
Sentinel Event Alert The Joint Commission ://€¦ · Sentinel Event Alert The Joint Commission ......
40
1 Sentinel Event Alert The Joint Commission http://www.jointcommission.org/SentinelEvents/SentinelEventAlert/ Issue 41, September 24, 2008 Preventing errors relating to commonly used anticoagulants Reports of accidental deaths and overdosing due to the improper use of anticoagulant drugs have received significant public attention. Anticoagulants have been identified as one of the top five drug types associated with patient safety incidents in the United States.(1 ) In the United Kingdom, anticoagulants are one of the classes of drugs commonly associated with fatal medication errors. (2 ) The Joint Commission’s Sentinel Event Database includes 446 medication-related sentinel events (9.3 percent of all events) reported from January 1997 through December 2007, with 7.2 percent (32) of these involving anticoagulants; of those, two-thirds (21) involve heparin* (see sidebar for more data). According to the United States Pharmacopeia MEDMARX database, a total of 59,316 medication errors related to anticoagulants were reported to the MEDMARX program from 2001 to 2006 (these data do not include errors involving heparin lock flush). Nearly 60 percent of these errors reached the patient and nearly 3 percent resulted in harm or death. Performance error (e.g., administration) is the most common cause of adverse events relating to anticoagulant medications. The anticoagulants cited most frequently in medication error reports are unfractionated heparin, warfarin and enoxaparin (classified as low molecular weight heparin, LMWH)*, according to MEDMARX and a hospital study. (3 ) These are also the most commonly used anticoagulants and the focus of this Alert. According to MEDMARX, in 2005, enoxaparin errors were associated with four patient deaths and two cases of permanent harm. Other anticoagulant errors have been associated with the concurrent use of heparin and enoxaparin and with argatroban and lepirudin. Contributing factors Patients under consideration for receiving anticoagulant drugs must be carefully screened for contraindications and drug interactions. While receiving anticoagulants, patients must be monitored closely to ensure effectiveness and to prevent side effects or overdosing. Heparin and warfarin in particular have narrow therapeutic ranges and a high potential for complications (4 ), so there is a greater risk of patient harm. (5 ) The following factors contribute to medication errors involving anticoagulants: • Lack of standardization for the naming, labeling and packaging of anticoagulants creates confusion. For example, heparin flush syringes have been confused with LMW heparin syringes. In addition, other, lesser-known anticoagulant drug names exist (e.g., enoxaparin, dalteparin, tinzaparin) and are used less commonly, which can result in duplicate medication orders and erroneous dosing. • Keeping current with different dosing regimens for various patient populations, newer assay methods, the expanding lists of drug interactions, and the potential reversal strategies can be a challenge for providers— especially those who infrequently prescribe or administer anticoagulants. (6 ) • The specific and individualized instructions and monitoring information (for example, dose adjustments, lab values, changing patient condition) that accompany the prescribing and administration of anticoagulants may fail to get documented or communicated during transfers and hand-offs. (7 ) • Neonates and other pediatric patients are problematic to treat, specifically because the medications are formulated and packaged primarily for adults. (8 )
Transcript of Sentinel Event Alert The Joint Commission ://€¦ · Sentinel Event Alert The Joint Commission ......

1
Sentinel Event Alert The Joint Commission http://www.jointcommission.org/SentinelEvents/SentinelEventAlert/
Issue 41, September 24, 2008
Preventing errors relating to commonly used anticoagulants Reports of accidental deaths and overdosing due to the improper use of anticoagulant drugs have received significant public attention. Anticoagulants have been identified as one of the top five drug types associated with patient safety incidents in the United States.(1) In the United Kingdom, anticoagulants are one of the classes of drugs commonly associated with fatal medication errors. (2)
The Joint Commission’s Sentinel Event Database includes 446 medication-related sentinel events (9.3 percent of all events) reported from January 1997 through December 2007, with 7.2 percent (32) of these involving anticoagulants; of those, two-thirds (21) involve heparin* (see sidebar for more data). According to the United States Pharmacopeia MEDMARX database, a total of 59,316 medication errors related to anticoagulants were reported to the MEDMARX program from 2001 to 2006 (these data do not include errors involving heparin lock flush). Nearly 60 percent
of these errors reached the patient and nearly 3 percent resulted in harm or death. Performance error (e.g., administration) is the most common cause of adverse events relating to anticoagulant medications.
The anticoagulants cited most frequently in medication error reports are unfractionated heparin, warfarin and enoxaparin (classified as low molecular weight heparin, LMWH)*, according to MEDMARX and a hospital study. (3) These are also the most commonly used anticoagulants and the focus of this Alert. According to MEDMARX, in 2005, enoxaparin errors were associated with four patient deaths and two cases of permanent harm. Other anticoagulant errors have been associated with the concurrent use of heparin and enoxaparin and with argatroban and lepirudin.
Contributing factors
Patients under consideration for receiving anticoagulant drugs must be carefully screened for contraindications and drug interactions. While receiving anticoagulants, patients must be monitored closely to ensure effectiveness and to prevent side effects or overdosing. Heparin and warfarin in particular have narrow therapeutic ranges and a high potential for complications (4), so there is a greater risk of patient harm. (5) The following factors contribute to medication errors involving anticoagulants:
• Lack of standardization for the naming, labeling and packaging of anticoagulants creates confusion. For example, heparin flush syringes have been confused with LMW heparin syringes. In addition, other, lesser-known anticoagulant drug names exist (e.g., enoxaparin, dalteparin, tinzaparin) and are used less commonly, which can result in duplicate medication orders and erroneous dosing.
• Keeping current with different dosing regimens for various patient populations, newer assay methods, the expanding lists of drug interactions, and the potential reversal strategies can be a challenge for providers—especially those who infrequently prescribe or administer anticoagulants. (6)
• The specific and individualized instructions and monitoring information (for example, dose adjustments, lab values, changing patient condition) that accompany the prescribing and administration of anticoagulants may fail to get documented or communicated during transfers and hand-offs. (7)
• Neonates and other pediatric patients are problematic to treat, specifically because the medications are formulated and packaged primarily for adults. (8)

2
Risk reduction strategies
Health care organizations that dispense or administer anticoagulant medications can prevent errors relating to anticoagulants by implementing specific risk reduction strategies. Since the management of anticoagulants is interdisciplinary, any risk strategies should be implemented by all staff who manage anticoagulants, which can include physicians, nurses, pharmacists, dieticians, and case managers. Specific guidelines regarding anticoagulant management have been developed by the United Kingdom’s National Patient Safety Agency, (2) the Institute for Safe Medication Practices, (9) and the Institute for Healthcare Improvement. (10) These guidelines stress improving staff communication and access to information; implementing close pharmacy oversight and involvement; and enhancing patient education. Research shows there is a significant reduction in the risk of thromboembolic events and death among patients who manage their anticoagulation therapy compared with those who rely solely on their doctor to monitor their treatment. (11,12) In addition, organizations may consider:
• Implementing a pharmacist-managed anticoagulation service. In addition to helping discharged patients receiving warfarin therapy, this service can assist staff caring for patients on all types of anticoagulants. (13,14,15)
• Implementing or using, when available, computerized provider order entry (CPOE) and/or bar coding technology. Pharmacy can use bar coding to replenish regular anticoagulant medication stock or automated dispensing cabinets. (16)
Existing Joint Commission requirements
• Standard MM 7.10: The organization develops processes for managing high-risk or high-alert medications. Elements of performance include identifying these medications and developing and implementing processes for procuring, storing, ordering, transcribing, preparing, dispensing, administering, and monitoring them.
• National Patient Safety Goal 3E: Reduce the likelihood of patient harm associated with the use of anticoagulant therapy. Targeted for full implementation by January 1, 2009, the requirement has a one-year phase-in period during 2008 that includes defined milestones (see the EPs at: http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/).
• National Patient Safety Goal 8: Accurately and completely reconcile medications across the continuum of care. Related requirements were revised based on feedback obtained from a Medication Reconciliation Summit convened in late 2007 and are effective January 1, 2009. These requirements include the communication of the reconciled list during transfer or discharge, and modified medication reconciliation processes.
Other Joint Commission suggested actions
For all anticoagulants:
1. Perform an organizational-wide risk assessment for anticoagulant therapy. (17) 2. Use best practices or evidence-based guidelines regarding the use of anticoagulants. (4) 3. Establish organization-wide dose limits on anticoagulants and screen all
orders for exceptions (i.e., require a confirmatory override by the physician). 4. Clearly label or otherwise differentiate syringes and other containers used for anticoagulant drugs. 5. Clarify all anticoagulant dosing for pediatric patients. 6. Promptly re-evaluate patients whose anticoagulant is being held for a procedure. The re-evaluation should include
an assessment of the need to reorder anticoagulant therapy. 7. Hospitals and ambulatory facilities (both hospital-owned/-managed and independent ambulatory care providers)
should provide timely communication of all anticoagulant-associated lab values to the provider or the person managing the anticoagulation therapy.

3
8. Under the supervision of clinical staff, educate and assist inpatients who require anticoagulant drugs to practice administering their own medications. This will help reduce the risk of errors after discharge. For heparin:
9. Consolidate and limit the number of institutional unfractionated heparin dosing nomograms. (18, 19) For all heparin medication orders (inpatient and outpatient), require prescribers to include the calculated dose and the dose per weight (e.g. milligrams per kilogram) or body surface area to facilitate an independent double-check of the calculation by a pharmacist, nurse or both. Note: For morbidly obese patients, the standard nomograms may not be accurate.
10. Before the start of a heparin infusion and with each change of the container or rate of infusion, require an independent double check of the drug, concentration, dose calculation, rate of infusion, pump settings, line attachment and patient identity.
11. Use heparin flush only for central lines and eliminate heparin flush of peripheral intravenous lines. (20) Stock and use only pre-filled syringes commercially prepared at set unit doses for flush solutions.
12. Identify patients with heparin-induced antibodies and heparin-induced thrombocytopenia (HIT) to avoid life-threatening events from heparin exposure. (21)
13. Dispense only preservative-free heparin to neonates and build an alert to pharmacists with this directive into order entry systems. For warfarin:
14. Consider reports of INRs greater than three and episodes of vitamin K administration as possible indicators of warfarin-associated adverse drug events and take immediate steps to address these events. (7)
15. Do not automatically discontinue warfarin according to automatic stop policies without verifying the drug’s indication and contacting the prescriber.
* All the medications are named by their generic names; they may be better known by brand names.
References
(1) The Joint Commission: High-alert medications and patient safety. Sentinel Event Alert #11, November 19, 1999. Available online: http://www.jointcommission.org/SentinelEvents/SentinelEventAlert/sea_11.htm (accessed 4/11//08)
(2) Cousins D, et al: Risk assessment of anticoagulation therapy. National Patient Safety Agency, January 2006. Available online: http://www.npsa.nhs.uk/patientsafety/alerts-and-directives/alerts/anticoagulant/ (accessed 4/16/08)
(3) Fanikos J, et al: Medication errors associated with anticoagulant therapy in the hospital. American Journal of Cardiology, 2004, 94:532-535
(4) Vats, V, et al: Survey of hospitals for guidelines, policies, and protocols for anticoagulants. American Journal of Health-System Pharmacy, 1203-120. Available for purchase online: http://www.ajhp.org/cgi/content/abstract/64/11/1203 (accessed 4/16/08)
(5) Lohr, LK: Improving the safety of heparin therapy. Orthopedics, April 2004, 27(4): 384-385
(6) Dager, WE, et al: Implementing anticoagulation management by pharmacists in the inpatient setting. American Journal of Health-System Pharmacy, 2007, 1071-1079. Available for purchase online: (accessed 4/16/08)
(7) Haig KM, et al: SBAR: A shared mental model for improving communication between clinicians. Joint Commission Journal of Quality and Patient Safety, 32(3):167-175
4
(8) The Joint Commission: Preventing pediatric medication errors. Sentinel Event Alert #39, April 1, 2008. Available online: http://www.jointcommission.org/SentinelEvents/SentinelEventAlert/sea_39.htm (accessed 4/16/08)
(9) Cohen MR, et al: High-alert medications: safeguarding against errors. Part IV, Chapter 14, Medication Errors, 2007, Washington DC, American Pharmacists Association
(10) Institute for Healthcare Improvement: Reduce adverse drug events involving anticoagulants. 2006. Available online: (accessed 4/16/08)
(11) Heneghan, C, et al: Self-monitoring of oral anticoagulation: A systematic review and metal-analysis. The Lancet, 2006, 367(9508): 412
(12) Couris R. et al: Development of a self-assessment instrument to determine daily intake and variability of dietary vitamin K. Journal of the American College of Nutrition, 2000, 19(6):801-806
(13) Hartis CE, et al: Use of specific indicators to detect warfarin-related adverse events. American Journal of Health-System Pharmacy, 2005, 62(16):1683-1688
(14) Locke C, et al: Reduction in warfarin adverse events requiring patient hospitalization after implementation of a pharmacist-managed anticoagulation service. Pharmacotherapy, 2005, 25:685-689
(15) Witt DM, et al: Effect of a centralized clinical pharmacy anticoagulation service on the outcomes of anticoagulation therapy. Chest, 2005, 127(5):1515-22
(16) National Coordinating Council for Medication Error Reporting and Prevention: Recommendations to Enhance Accuracy of Dispensing Medications, March 19, 1999. Available online: http://www.nccmerp.org/council/council1999-03-19.html
(17) Institute for Safe Medication Practices: 2005 ISMP Medication Safety Self-Assessment® for Antithrombotic Therapy in Hospitals. Available online: https://www.ismp.org/selfassessments/asa2006/Intro.asp (accessed 4/16/08)
(18) Oyen LJ, et al: Effectiveness of a computerized system for intravenous heparin administration: using information technology to improve patient care and patient safety. American Heart Hospital Journal, 2005, 3(2):75-81
(19) Oertal L, et al: Unfractionated heparin: a nursing dilemma. Pharmacotherapy, 2004, 24:156S-160S
(20) American Society of Health-System Pharmacists: ASHP Therapeutic Position Statement on the Institutional Use of 0.9% Sodium Chloride Injection to Maintain Patency of Peripheral Indwelling Intermittent Infusion Devices. American Journal of Health-System Pharmacy, 2006; 63:1273–5. Available online: http://www.ashp.org/s_ashp/docs/files/BP07/TPS_NaCl.pdf (accessed 4/16/08)
(21) Mims MP, et al: Acute cardiorespiratory collapse from heparin: a consequence of heparin-induced thrombocytopenia. European Journal of Haematology, 2004, 72:366-369
Other resources Wilson, K, et al: Preventing medication errors with smart infusion technology. American Journal of Health-System Pharmacy, 2004, 61:177-183
American Society of Health-System Pharmacists: ASHP Therapeutic Position Statement on the Use of the International Normalized Ratio System to Monitor Oral Anticoagulant Therapy. American Journal of Health-System Pharmacy, 1995, 52(5)529-531. Available online: http://www.ashp.org/DocLibrary/BestPractices/TPS_INR.aspx (accessed 4/16/08)

5
American Society of Health-System Pharmacists: ASHP Therapeutic Position Statement on Antithrombotic Therapy in Chronic Atrial Fibrillation. American Journal of Health-System Pharmacy, 1998, 55:376–81. Available online: http://www.ashp.org/s_ashp/docs/files/BP07/TPS_Antithrombotic.pdf (accessed 4/16/08)
American Society of Health-System Pharmacists: ASHP Therapeutic Position Statement on the Use of Low-Molecular-Weight Heparins for Adult Outpatient Treatment of Acute Deep-Vein Thrombosis. American Journal of Health-System Pharmacy, 2004, 61:1950–5. Available online: http://www.ashp.org/s_ashp/docs/files/BP07/TPS_LMWH.pdf (accessed 4/16/08
Number of Reported Sentinel Events Related to Anticoagulants (1997-2007)
Drug Involved Heparin 21Warfarin 6 Enoxaparin 3 Unknown* 2 Outcome (# of patients 34*) Death 28Loss of function 6 Settings Hospital 29Emergency Department 1 Long Term Care 2 Cause of Event Wrong drug 3 Wrong dose 7 Improper monitoring 9 Pump malfunction/error 5 Given without order 2 Not reordered 2 Unknown 4 * one event affected three patients

Institute for Healthcare Improvement: Reduce Adverse Drug Events Involving Anticoagulants
Log In/RegisterContact UsSite Map
More Search Options
Home > Topics > Patient Safety > Medication Systems > Changes
Programs
TopicsImprovementLeading System ImprovementChronic ConditionsCritical CareDeveloping CountriesEnd Stage Renal DiseaseFlowHealthcare-Associated InfectionsHealth Professions EducationHIV/AIDSLast Phase of LifeMedical-Surgical CareOffice PracticesPatient-Centered CarePatient SafetySafety: GeneralMedication SystemsHow to ImproveMeasuresChangesImprovement StoriesToolsResourcesLiteratureFAQs
Reducing Harm from FallsSurgical Site InfectionsPerinatal CareReducing MortalityReliability
Community
Workspace
Results
Products
About Us
Reduce Adverse Drug Events Involving Anticoagulants
Medications for anticoagulation have many benefits, but also many risks. Careful monitoring of laboratory values is essential to maintaining the balance between under-coagulation, which can result in development of clots, and over-coagulation, which increases the risk of bleeding and hemorrhage. Dosages require adjustments, sometimes frequently, but adjustments must be made carefully and with a variety of data in mind, including laboratory values for coagulation and renal function, diet, clinical condition, weight, and age. The use of standardized practices in the hospital setting can greatly reduce the chances of an adverse event from anticoagulants. Patients taking anticoagulants often continue taking the medications after they leave the hospital, so care providers must communicate ample information during the inpatient period and give proper patient education for self-management.
Changes for ImprovementUse Guidelines or Pre-Printed Orders for Vitamin K
Implement Weight-Based Heparin Protocols
Use Programmable Pumps and Independent Double-Checks for IV Anticoagulants
Develop a Warfarin Dosing Service or Clinic
Use Alarm Devices to Ensure Consistent Anticoagulant Dosing
Use Pre-Mixed Heparin Solutions
Provide Coagulation Test Results Within Two Hours or at Bedside
Use Dosing Charts for Heparin
Prepare All Heparin Doses and Solutions in the Hospital Pharmacy
Continue to Use Anticoagulation Flowsheets after Discharge
Implement Patient-Directed Administration of Warfarin
Educate Patients to Manage Warfarin Therapy at Home
Develop Weekly Dosing Regimens for Anticoagulants
Titrate Anticoagulant Doses
Eliminate Heparin Flush of Peripheral Intravenous Lines
Standardize International Normalized Ratio Testing Equipment
Adjust Anticoagulants with Thrombolytics and G2b/3A Inhibitors
Use Anticoagulation Flowsheets
Use Low Molecular Weight Heparin (LMWH)
Eliminate the Use of Heparin Solution with Arterial Lines
Allow Pharmacists to Manage an Anticoagulant Service
High-Risk ADEs per 1,000 Doses
Percent of Patients Receiving a Specific High-Risk Medication with a Related ADE
How-to Guide: Prevent Harm from High-Alert Medications developed as part of IHI's 5 Million Lives Campaign
Post your comments about this item.
View All Comments Post Your Comments
Your Privacy | Terms of Use/Legal | © Institute for Healthcare Improvement
http://www.ihi.org/IHI/Topics/PatientSafety/MedicationSyste...ges/Reduce+Adverse+Drug+Events+Involving+Anticoagulants.htm3/11/2009 8:35:29 AM

Institute for Healthcare Improvement: Develop a Warfarin Dosing Service or Clinic
Log In/RegisterContact UsSite Map
More Search Options
Home > Topics > Patient Safety > Medication Systems > Changes > Individual Changes
Programs
TopicsImprovementLeading System ImprovementChronic ConditionsCritical CareDeveloping CountriesEnd Stage Renal DiseaseFlowHealthcare-Associated InfectionsHealth Professions EducationHIV/AIDSLast Phase of LifeMedical-Surgical CareOffice PracticesPatient-Centered CarePatient SafetySafety: GeneralMedication SystemsHow to ImproveMeasuresChangesImprovement StoriesToolsResourcesLiteratureFAQs
Reducing Harm from FallsSurgical Site InfectionsPerinatal CareReducing MortalityReliability
Community
Workspace
Results
Products
About Us
Reduce Adverse Drug Events Involving Anticoagulants:
Develop a Warfarin Dosing Service or Clinic
A dosing service or clinic for patients taking warfarin can be a place where physicians, nurses, or pharmacists can provide consistent management of therapy and response. Many patients on warfarin see more than one physician, and it may not always be clear who is managing the warfarin therapy. Plus, physicians have varying amounts of experience managing patients on warfarin. Patients and physicians can both benefit from a dosing service or clinic, which helps to ensure consistency of care, timely evaluation of laboratory results, and prompt response to patients’ anticoagulant needs. The service or clinic can significantly reduce the risk of adverse drug events and improve satisfaction for patients and clinicians.
Tips
● Ensure that all information about a patient’s lab results, dose changes, and responses to therapy is regularly communicated to his or her physician.
● Manage the service or clinic using a nurse practitioner who can adjust doses as needed and communicate the changes to the appropriate physicians.
● Have a nurse or pharmacist, rather than a physician, manage the clinic using your organization’s anticoagulant guidelines or protocols so physicians will not need to be contacted for dose changes.
● Develop a mechanism to identify inpatients that are newly started on warfarin so they can be referred to the service or clinic while still in the hospital.
● Provide patient education about warfarin at the dosing service or clinic to make patients more knowledgeable about managing their therapy at home.
Reduce Adverse Drug Events Involving Anticoagulants
Allow Pharmacists to Manage an Anticoagulant Service
Educate Patients to Manage Warfarin Therapy at Home
Implement Patient-Directed Administration of Warfarin
Post your comments about this item.
View All Comments Post Your Comments
Your Privacy | Terms of Use/Legal | © Institute for Healthcare Improvement
http://www.ihi.org/IHI/Topics/PatientSafety/MedicationSyste...dualChanges/Develop+a+Warfarin+Dosing+Service+or+Clinic.htm3/11/2009 8:36:12 AM
Institute for Healthcare Improvement: Medication Systems
Log In/RegisterContact UsSite Map
More Search Options
Home > Topics > Patient Safety > Medication Systems
Programs
TopicsImprovementLeading System ImprovementChronic ConditionsCritical CareDeveloping CountriesEnd Stage Renal DiseaseFlowHealthcare-Associated InfectionsHealth Professions EducationHIV/AIDSLast Phase of LifeMedical-Surgical CareOffice PracticesPatient-Centered CarePatient SafetySafety: GeneralMedication SystemsHow to ImproveMeasuresChangesImprovement StoriesToolsResourcesLiteratureFAQs
Reducing Harm from FallsSurgical Site InfectionsPerinatal CareReducing MortalityReliability
Community
Workspace
Results
Products
About Us
Improving Medication Safety at Metropolitan Hospital
Successful improvement efforts generally have two valuable pay-offs: the end result and the learning gained along the way. Such is the case at Metropolitan Hospital (Grand Rapids, Michigan, USA) where adverse drug events (ADEs) on admission have been virtually eliminated, and a whole new approach to problem solving is now described as “a way of life.”
Campaign How-to Guides
● How-to Guide: Prevent Adverse Drug Events (Medication Reconciliation)
How-to Guide: Prevent Harm from High-Alert Medications
Medication Systems Content
How to Improve Tools
Measures Resources
Changes Literature
Improvement Stories FAQs
Case for ImprovementChangesAdvisorsDiscussion Groups
Trigger Tool for Measuring Adverse Drug Events
The use of "triggers," or clues, to identify adverse drug events (ADEs) is an effective method for measuring the overall level of harm from medications in a health care organization. This Trigger Tool provides instructions for conducting a retrospective review of patient records using triggers to identify possible ADEs.
Learn More
Your Privacy | Terms of Use/Legal | © Institute for Healthcare Improvement
http://www.ihi.org/IHI/Topics/PatientSafety/MedicationSystems/3/11/2009 8:36:26 AM

National Patient Safety | Joint Commission
http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/3/11/2009 8:37:37 AM
HOME | SEARCH | CONTACT US | SITE MAP | CAREERS | NEWSROOM | QUALITY CHECK
“Do Not Use” ListEisenberg AwardHospitals, Language, and CultureInfection ControlNational Patient Safety GoalsSolutionsSpeak UpUniversal Protocol
Home > Patient Safety > National Patient Safety Goals
National Patient Safety Goals
2009 National Patient Safety Goals
Click on the links below to access the goals and renumbering by program.
● Ambulatory Health Care
● Behavioral Health Care
● Critical Access Hospital
● Disease-Specific Care
● Home Care
● Hospital
● Laboratory
● Long Term Care & Medicare/Medicaid Certification-Based Long Term Care
● Office-Based Surgery
2009 Additional Resources
● Medication reconciliation National Patient Safety Goal to be reviewed, refined
● 2009 FAQs about the NPSGs and the Universal Protocol
● Facts about the NPSGs
● 2009 NPSG PowerPoint Presentation
● Request for Review of an Alternative Approach to a National Patient Safety Goal Requirement
● Easy-to-read versions of the 2009 NPSGs for the public
For more information, contact the Standards Interpretation Group at (630) 792-5900 or via the online question form.
Additional Resources
● Look-alike/sound-alike drug list *
● Official "Do Not Use" Abbreviations List *
● Implementation Tips for Eliminating Dangerous Abbreviations
● Introduction to the NPSGs
● Compliance Data
*Requires Adobe Reader
Past Goals
● 2008 NPSGs
● 2007 NPSGs
● 2006 NPSGs
● 2005 NPSGs
● 2004 NPSGs
● 2003 NPSGs
Accreditation Programs | Certification Programs | Quality Check | Achieve the Gold Seal | LibraryStandards | Patient Safety | Performance Measurement | Sentinel Event | Public Policy | SearchContact Us | Site Map | Careers | Newsroom | About Us © 2009 The Joint Commission, All Rights Reserved

2009 Hospital National Patient Safety Goals | Joint Commission
http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/09_hap_npsgs.htm3/11/2009 8:37:46 AM
HOME | SEARCH | CONTACT US | SITE MAP | CAREERS | NEWSROOM | QUALITY CHECK
Printer-Friendly
“Do Not Use” ListEisenberg AwardHospitals, Language, and CultureInfection ControlNational Patient Safety GoalsSolutionsSpeak UpUniversal Protocol
Home > Patient Safety > National Patient Safety Goals
National Patient Safety Goals 2009 National Patient Safety GoalsHospital Program
●
Chapter Outline
●
2009 National Patient Safety Goals Manual Chapter
●
2009 National Patient Safety Goals - Renumbering
● History Tracking Report 2009 -2008
● History Tracking Report 2008 -2009
The Goals include improvements emanating from the Standards Improvement Initiative, including the new numbering system and minor language changes for consistency. The new numbering format was designed to enable sorting electronically (for the new E-ditions of the manuals) and to accommodate the addition of new requirements. Under the new numbering system, each requirement is assigned a six-digit number that designates its place in the chapter.
Accreditation Programs | Certification Programs | Quality Check | Achieve the Gold Seal | LibraryStandards | Patient Safety | Performance Measurement | Sentinel Event | Public Policy | SearchContact Us | Site Map | Careers | Newsroom | About Us © 2009 The Joint Commission, All Rights Reserved

Accreditation Program: Hospital
National Patient Safety Goals
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
Goal 1
Improve the accuracy of [patient] identification.
NPSG
NPSG.01.01.01
Use at least two [patient] identifiers when providing care, treatment, and services.
Wrong-[patient] errors occur in virtually all stages of diagnosis and treatment. The intent for this goal is two-fold: first, to reliably identify the individual as the person for whom the service or treatment is intended; second, to match the service or treatment to that individual.
Rationale for NPSG.01.01.01
Elements of Performance for NPSG.01.01.01
C Prior to any specimen collection, medication administration, transfusion, or treatment, the hospital actively involves the patient and, as needed, the family in the identification and matching process. When active patient involvement is not possible or the patient’s reliability is in question, the hospital will designate the caregiver responsible for identity verification. Note: The involvement of a single caregiver is acceptable as long as the other components of patient identification are satisfied.
1.
C Two patient identifiers are used when administering medications, blood, or blood components.2.
A Two patient identifiers are used when collecting blood samples and other specimens for clinical testing.3.
C Two patient identifiers are used when providing other treatments or procedures.4.
A The patient’s room number or physical location is not used as an identifier. (See also MM.05.01.09, EPs 8 and 11)5.
A Containers used for blood and other specimens are labeled in the presence of the patient.6.
Page 2 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations
Accreditation Program: Hospital Chapter: National Patient Safety Goals
NPSG.01.03.01
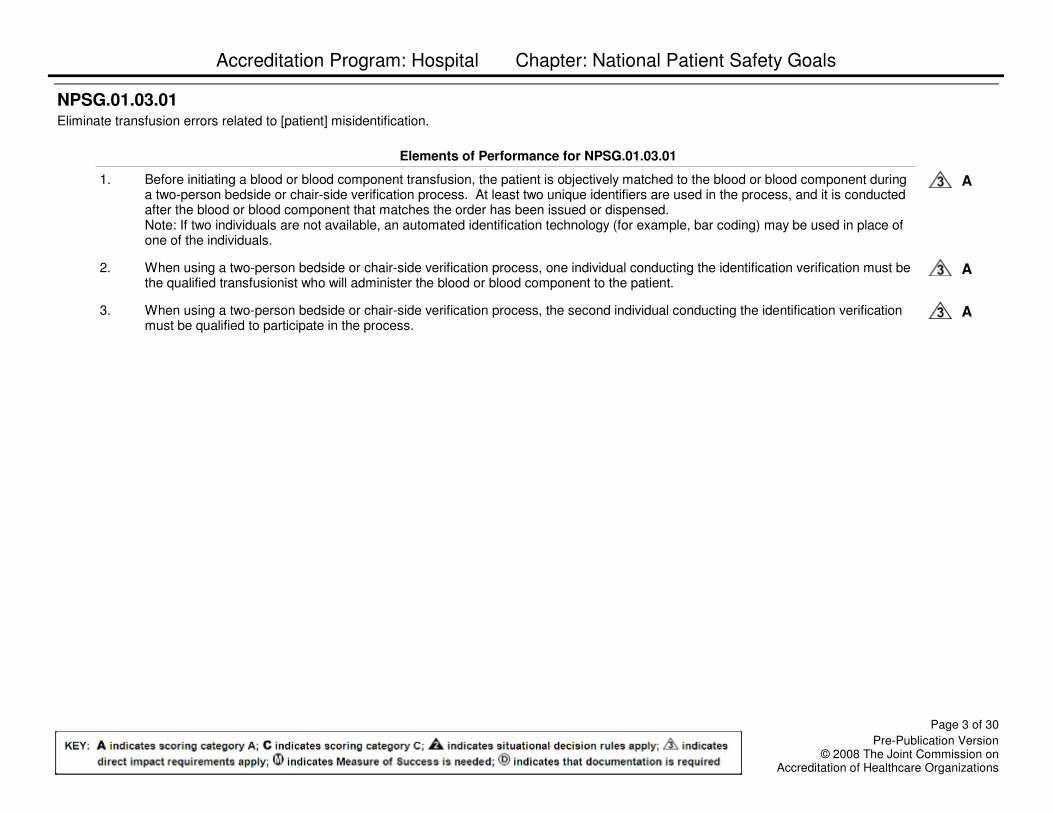
Eliminate transfusion errors related to [patient] misidentification.
Elements of Performance for NPSG.01.03.01
A Before initiating a blood or blood component transfusion, the patient is objectively matched to the blood or blood component during a two-person bedside or chair-side verification process. At least two unique identifiers are used in the process, and it is conducted after the blood or blood component that matches the order has been issued or dispensed. Note: If two individuals are not available, an automated identification technology (for example, bar coding) may be used in place of one of the individuals.
1.
A When using a two-person bedside or chair-side verification process, one individual conducting the identification verification must be the qualified transfusionist who will administer the blood or blood component to the patient.
2.
A When using a two-person bedside or chair-side verification process, the second individual conducting the identification verification must be qualified to participate in the process.
3.
Page 3 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
Goal 2
Improve the effectiveness of communication among caregivers.
NPSG
NPSG.02.01.01
For verbal or telephone orders or for telephone reporting of critical test results, the individual giving the order or test result verifies the complete order or test result by having the person receiving the information record and "read back" the complete order or test result.
Ineffective communication is the most frequently cited root cause for sentinel events. Effective communication that is timely, accurate, complete, unambiguous, and understood by the recipient reduces error and results in improved [patient] safety.
Rationale for NPSG.02.01.01
Elements of Performance for NPSG.02.01.01
C The individual receiving the information writes down the complete order or test result or enters it into a computer.1.
C The individual receiving the information reads back the complete order or test result.2.
C The individual who gave the order or test result confirms the information that was read back.3.
Page 4 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
NPSG.02.02.01
There is a standardized list of abbreviations, acronyms, symbols, and dose designations that are not to be used throughout the [organization].
Elements of Performance for NPSG.02.02.01
A The hospital develops a standardized list of abbreviations, acronyms, symbols, and dose designations that are not to be used throughout the hospital.
1.
A The current list of abbreviations, acronyms, symbols, and dose designations not to be used includes the following:- U,u- IU - Q.D., QD, q.d., qd - Q.O.D., QOD, q.o.d, qod- Trailing zero (X.0 mg) - Lack of leading zero (.X mg)- MS- MSO4- MgSO4Note: A trailing zero may be used only when required to demonstrate the level of precision of the value being reported, such as for laboratory results, imaging studies that report the size of lesions, or catheter/tube sizes. It may not be used in medication orders or other medication-related documentation.
2.
C The hospital implements the “do not use” list of abbreviations, acronyms, symbols, and dose designations and applies it to all orders and all medication-related documentation that is handwritten or entered as free text into a computer.
3.
A The hospital does not include any abbreviations, acronyms, symbols, and dose designations identified as not to be used on preprinted forms.
4.
Page 5 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
NPSG.02.03.01
The [organization] measures, assesses, and, if needed, takes action to improve the timeliness of reporting and the timeliness of receipt of critical tests and critical results and values by the responsible licensed caregiver.
Elements of Performance for NPSG.02.03.01
A The hospital defines critical tests and critical results and values.1.
A The hospital defines the acceptable length of time between the ordering of critical tests and reporting the results of these tests, whether normal or abnormal.
2.
A The hospital defines the acceptable length of time for reporting the results of routine tests with critical abnormal values or findings.3.
A The hospital defines the acceptable length of time between the availability of critical tests and critical results and values and receipt by the responsible licensed caregiver.
4.
A The hospital collects data on the timeliness of reporting critical test results and critical results and values from routine tests.5.
A The hospital assesses the data on the timeliness of reporting critical test results and critical results and values from routine tests and determines whether a need for improvement exists.
6.
A The hospital takes appropriate action to improve the timeliness of reporting critical test results and critical results and values from routine tests and measures the effectiveness of those actions.
7.
Page 6 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
NPSG.02.05.01
The [organization] implements a standardized approach to hand-off communications, including an opportunity to ask and respond to questions.
Health care has numerous types of [patient] hand-offs, including, but not limited to, nursing shift changes; physician transfer of complete responsibility for a [patient]; physician transfer of on-call responsibility; acceptance of temporary responsibility for staff leaving the unit for a short time; anesthesiologist report to post-anesthesia recovery room nurse; nursing and physician hand-off from the emergency department to inpatient units, different hospitals, nursing homes, and home health care; and critical laboratory and radiology results sent to physician offices. The primary objective of a hand-off is to provide accurate information about a [patient]'s care, treatment, and services; current condition; and any recent or anticipated changes. The information communicated during a hand-off must be accurate in order to meet [patient] safety goals.
Rationale for NPSG.02.05.01
Elements of Performance for NPSG.02.05.01
C The hospital’s process for effective hand-off communication includes the following: Interactive communication that allows for the opportunity for questioning between the giver and receiver of patient information.
1.
C The hospital's process for effective hand-off communication includes the following: Up-to-date information regarding the patient’s condition, care, treatment, medications, services, and any recent or anticipated changes. (See also NPSG.08.01.01, EP 4)
2.
C The hospital’s process for effective hand-off communication includes the following: A method to verify the received information, including repeat-back or read-back techniques.
3.
A The hospital’s process for effective hand-off communication includes the following: An opportunity for the receiver of the hand-off information to review relevant patient historical data, which may include previous care, treatment, and services.
4.
C Interruptions during hand-offs are limited to minimize the possibility that information fails to be conveyed or is forgotten.5.
Page 7 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
Goal 3
Improve the safety of using medications.
NPSG
NPSG.03.03.01
The [organization] identifies and, at a minimum, annually reviews a list of look-alike/sound-alike medications used by the [organization] and takes action to prevent errors involving the interchange of these medications.
Elements of Performance for NPSG.03.03.01
A The hospital identifies a list of look-alike/sound-alike medications used by the hospital. The list includes a minimum of 10 look-alike/sound-alike medication combinations selected from the tables of look-alike/sound-alike medications posted on The Joint Commission Web site at http://www.jointcommission.org.
1.
A The hospital reviews the list of look-alike/sound-alike medications at least annually.2.
A The hospital takes action to prevent errors involving the interchange of the medications on the list of look-alike/sound-alike medications.
3.
Page 8 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
NPSG.03.04.01
Label all medications, medication containers (for example, syringes, medicine cups, basins), or other solutions on and off the sterile field.
Medications or other solutions in unlabeled containers are unidentifiable. Errors, sometimes tragic, have resulted from medications and other solutions removed from their original containers and placed into unlabeled containers. This unsafe practice neglects basic principles of medication management safety yet has been routine in many organizations.
The labeling of all medications, medication containers, and solutions is a risk reduction activity consistent with safe medication practices. This practice addresses a recognized risk point in the safe administration of medications in perioperative and other procedural settings.
Rationale for NPSG.03.04.01
Elements of Performance for NPSG.03.04.01
A Medications and solutions both on and off the sterile field are labeled even if there is only one medication being used.1.
A Labeling occurs when any medication or solution is transferred from the original packaging to another container.2.
A Medication or solution labels include the medication name, strength, amount (if not apparent from the container), expiration date when not used within 24 hours, and expiration time when expiration occurs in less than 24 hours.
3.
C All medication or solution labels are verified both verbally and visually by two qualified individuals whenever the person preparing the medication or solution is not the person who will be administering it.
4.
A No more than one medication or solution is labeled at one time.5.
A Any medications or solutions found unlabeled are immediately discarded.6.
C All original containers from medications or solutions remain available for reference in the perioperative or procedural area until the conclusion of the procedure.
7.
A All labeled containers on the sterile field are discarded at the conclusion of the procedure.8.
C At shift change or break relief, all medications and solutions both on and off the sterile field and their labels are reviewed by entering and exiting personnel.
9.
Page 9 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
NPSG.03.05.01
Reduce the likelihood of [patient] harm associated with the use of anticoagulant therapy.Note: This requirement applies only to [organization]s that provide anticoagulant therapy and/or long-term anticoagulation prophylaxis (for example, atrial fibrillation) where the clinical expectation is that the [patient]’s laboratory values for coagulation will remain outside normal values. This requirement does not apply to routine situations in which short-term prophylactic anticoagulation is used for venous thrombo-embolism prevention (for example, related to procedures or hospitalization) and the clinical expectation is that the [patient]’s laboratory values for coagulation will remain within, or close to, normal values.
Anticoagulation therapy poses risks to patients and often leads to adverse drug events due to complex dosing, requisite follow-up monitoring, and inconsistent [patient] compliance. The use of standardized practices for anticoagulation therapy that include [patient] involvement can reduce the risk of adverse drug events associated with the use of heparin (unfractionated), low molecular weight heparin, and warfarin.
Rationale for NPSG.03.05.01
Elements of Performance for NPSG.03.05.01
A The hospital implements a defined anticoagulation management program to individualize the care provided to each patient receiving anticoagulant therapy.
1.
A To reduce compounding and labeling errors, the hospital uses only oral unit dose products, pre-filled syringes, or pre-mixed infusion bags when these types of products are available. Note: For pediatric patients, pre-loaded syringe products should only be used if specifically designed for children.
2.
C The hospital uses approved protocols for the initiation and maintenance of anticoagulant therapy appropriate to the medication used, to the condition being treated, and to the potential for medication interactions.
3.
A For patients starting on warfarin, a baseline International Normalized Ratio (INR) is available, and for all patients receiving warfarin therapy, a current INR is available and is used to monitor and adjust this therapy.
4.
C When dietary services are provided by the hospital, the service is notified of all patients receiving warfarin and responds according to its established food/medication interaction program.
5.
A When heparin is administered intravenously and continuously, the hospital uses programmable infusion pumps in order to provide consistent and accurate dosing.
6.
A The hospital has a written policy that addresses baseline and ongoing laboratory tests that are required for heparin and low molecular weight heparin therapies.
7.
C The hospital provides education regarding anticoagulant therapy to prescribers, staff, patients, and families.Note: Patient/family education includes the importance of follow-up monitoring, compliance issues, dietary restrictions, and potential for adverse drug reactions and interactions.
8.
Page 10 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
A The hospital evaluates its anticoagulation safety practices, takes appropriate action to improve its practices, and measures the effectiveness of those actions on a regular basis.
9.
Page 11 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
Goal 7
Reduce the risk of health care associated infections.
NPSG
NPSG.07.01.01
Comply with current World Health Organization (WHO) hand hygiene guidelines or Centers for Disease Control and Prevention (CDC) hand hygiene guidelines.
Compliance with the WHO or CDC hand hygiene guidelines will reduce the transmission by staff to [patient]s of infectious agents, thereby decreasing the incidence of health care–associated infections.
Rationale for NPSG.07.01.01
Elements of Performance for NPSG.07.01.01
C The hospital complies with current World Health Organization (WHO) or Centers for Disease Control and Prevention (CDC) hand hygiene guidelines. Note: Hospitals are required to comply with 1A, 1B, and 1C of the WHO or CDC guidelines.
1.
NPSG.07.02.01
Manage as sentinel events all identified cases of unanticipated death or major permanent loss of function related to a health care–associated infection.
A significant percentage of [patient]s who unexpectedly die or suffer major permanent loss of function have health care–associated infections. These unanticipated deaths and injuries meet the definition of a sentinel event and, therefore, are required to undergo a root cause analysis. The root cause analysis should attempt to answer the following questions: Why did the [patient] acquire an infection? Why did the [patient] die or suffer permanent loss of function?
Rationale for NPSG.07.02.01
Elements of Performance for NPSG.07.02.01
C The hospital manages all identified cases of unanticipated death or major permanent loss of function associated with a health care–associated infection as sentinel events (that is, the hospital conducts a root cause analysis).
1.
A The root cause analysis addresses the management of the patient before and after the identification of infection.2.
Page 12 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
NPSG.07.03.01
Implement evidence-based practices to prevent health care–associated infections due to multidrug-resistant organisms in acute care hospitals. Note 1: This requirement applies to, but is not limited to, epidemiologically important organisms such as methicillin-resistant Staphylococcus aureus (MRSA), Clostridium difficile (CDI), vancomycin-resistant Enterococci (VRE), and multiple drug-resistant gram negative bacteria.Note 2: This requirement has a one-year phase-in period that includes defined expectations for planning, development, and testing (milestones) at three, six, and nine months in 2009, with the expectation of full implementation by January 1, 2010.
[Patient]s continue to acquire health care–associated infections at an alarming rate. Risks and [patient] populations, however, differ between [organization]s. Therefore, prevention and control strategies must be tailored to the specific needs of each [organization] based on its risk assessment. The elements of performance for this requirement are designed to help reduce or prevent health care–associated infections from epidemiologically important multidrug-resistant organisms (MDROs).
Note: Hand hygiene, contact precautions, as well as cleaning and disinfecting [patient] care equipment and the [patient]’s environment are essential strategies for preventing the spread of health care–associated infections. Hand hygiene is addressed in NPSG.07.01.01. Contact precautions for [patient]s with epidemiologically significant multidrug-resistant organisms (MDROs) are covered in IC.02.01.01, EP 3. Cleaning and disinfecting [patient] care equipment are addressed in IC.02.02.01.
Rationale for NPSG.07.03.01
Elements of Performance for NPSG.07.03.01
A As of April 1, 2009, the hospital’s leadership has assigned responsibility for oversight and coordination of the development, testing, and implementation of NPSG.07.03.01.
1.
A As of July 1, 2009, an implementation work plan is in place that identifies adequate resources, assigned accountabilities, and a time line for full implementation of NPSG.07.03.01 by January 1, 2010.
2.
A As of October 1, 2009, pilot testing in at least one clinical unit is under way, for the requirements in NPSG.07.03.01.3.
A As of January 1, 2010, the elements of performance in NPSG.07.03.01 are fully implemented across the hospital.4.
C As of January 1, 2010, conduct periodic risk assessments for multidrug-resistant organism acquisition and transmission. (See also IC.01.03.01, EPs 1-5)
5.
C As of January 1, 2010, based on the results of the risk assessment, the hospital educates staff and licensed independent practitioners about health care–associated infections, multidrug-resistant organisms, and prevention strategies at hire and annually thereafter. Note: The education provided recognizes the diverse roles of staff and licensed independent practitioners and is consistent with their roles within the hospital. (See also HR.01.05.03, EP 4)
6.
Page 13 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
C As of January 1, 2010, the hospital educates patients, and their families as needed, who are infected or colonized with a multidrug-resistant organism about health care–associated infection strategies.
7.
A As of January 1, 2010, the hospital implements a surveillance program for multidrug-resistant organisms based on the risk assessment.
8.
A As of January 1, 2010, the hospital measures and monitors multidrug-resistant organism prevention processes and outcomes including the following:- Multidrug-resistant organism infection rates using evidence-based metrics- Compliance with evidence-based guidelines or best practices- Evaluation of the education program provided to staff and licensed independent practitioners
9.
A As of January 1, 2010, the hospital provides multidrug-resistant organism surveillance data to key stakeholders, including leaders, licensed independent practitioners, nursing staff, and other clinicians.
10.
C As of January 1, 2010, the hospital implements policies and practices aimed at reducing the risk of transmitting multidrug-resistant organisms that meet regulatory requirements and are aligned with evidence-based standards (for example, the Centers for Disease Control and Prevention (CDC) and/or professional organization guidelines).
11.
A As of January 1, 2010, when indicated by the risk assessment, the hospital implements a laboratory-based alert system that identifies new patients with multidrug-resistant organisms. The alert system may be either manual or electronic or a combination of both of these methods.Note: The alert system may use telephones, faxes, pagers, automated and secure electronic alerts, or a combination of these methods.
12.
A As of January 1, 2010, when indicated by the risk assessment, the hospital implements an alert system that identifies readmitted or transferred multidrug-resistant organism-positive patients. Note: The alert system information may exist in a separate electronic database or may be integrated into the admission system. The alert system may be either manual or electronic or a combination of both.
13.
Page 14 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
NPSG.07.04.01
Implement best practices or evidence-based guidelines to prevent central line–associated bloodstream infections. Note 1: This requirement covers short- and long-term central venous catheters and peripherally inserted central catheter (PICC) lines. Note 2: This requirement has a one-year phase-in period that includes defined expectations for planning, development, and testing (“milestones”) at three, six, and nine months in 2009, with the expectation of full implementation by January 1, 2010.
Elements of Performance for NPSG.07.04.01
A As of April 1, 2009, the hospital’s leadership has assigned responsibility for oversight and coordination of the development, testing, and implementation of NPSG.07.04.01.
1.
A As of July 1, 2009, an implementation work plan is in place that identifies adequate resources, assigned accountabilities, and a time line for full implementation of NPSG.07.04.01 by January 1, 2010.
2.
A As of October 1, 2009, pilot testing in at least one clinical unit is under way for the requirements in NPSG.07.04.01.3.
A As of January 1, 2010, the elements of performance in NPSG.07.04.01 are fully implemented across the hospital.4.
C As of January 1, 2010, the hospital educates health care workers who are involved in these procedures about health care–associated infections, central line–associated bloodstream infections, and the importance of prevention. Education occurs upon hire, annually thereafter, and when involvement in these procedures is added to an individual’s job responsibilities.
5.
C As of January 1, 2010, prior to insertion of a central venous catheter, the hospital educates patients and, as needed, their families about central line–associated bloodstream infection prevention.
6.
C As of January 1, 2010, the hospital implements policies and practices aimed at reducing the risk of central line–associated bloodstream infections that meet regulatory requirements and are aligned with evidence-based standards (for example, the Centers for Disease Control and Prevention (CDC) and/or professional organization guidelines).
7.
A As of January 1, 2010, the hospital conducts periodic risk assessments for surgical site infections, measures central line–associated bloodstream infection rates, monitors compliance with best practices or evidence-based guidelines, and evaluates the effectiveness of prevention efforts.
8.
A As of January 1, 2010, the hospital provides central line–associated bloodstream infections rate data and prevention outcome measures to key stakeholders including leaders, licensed independent practitioners, nursing staff, and other clinicians.
9.
C As of January 1, 2010, use a catheter checklist and a standardized protocol for central venous catheter insertion.10.
C As of January 1, 2010, perform hand hygiene prior to catheter insertion or manipulation.11.
Page 15 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
C As of January 1, 2010, for adult patients, do not insert catheters into the femoral vein unless other sites are unavailable.12.
C As of January 1, 2010, use a standardized supply cart or kit that is all inclusive for the insertion of central venous catheters.13.
C As of January 1, 2010, use a standardized protocol for maximum sterile barrier precautions during central venous catheter insertion.14.
C As of January 1, 2010, use a chlorhexidine-based antiseptic for skin preparation during central venous catheter insertion in patients over two months of age, unless contraindicated.
15.
A As of January 1, 2010, use a standardized protocol to disinfect catheter hubs and injection ports before accessing the ports.16.
A As of January 1, 2010, evaluate all central venous catheters routinely and remove nonessential catheters.17.
Page 16 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
NPSG.07.05.01
Implement best practices for preventing surgical site infections. Note: This requirement has a one-year phase-in period that includes defined expectations for planning, development, and testing (“milestones”) at three, six, and nine months in 2009, with the expectation of full implementation by January 1, 2010.
Elements of Performance for NPSG.07.05.01
A As of April 1, 2009, the hospital’s leadership has assigned responsibility for oversight and coordination of the development, testing, and implementation of NPSG.07.05.01.
1.
A As of July 1, 2009, an implementation work plan is in place that identifies adequate resources, assigned accountabilities, and a time line for full implementation of NPSG.07.05.01 by January 1, 2010.
2.
A As of October 1, 2009, pilot testing in at least one clinical unit is under way, for the requirements in NPSG.07.05.01.3.
A As of January 1, 2010, the elements of performance in NPSG.07.05.01 are fully implemented across the hospital.4.
A As of January 1, 2010, the hospital educates health care workers involved in surgical procedures about health care associated infections, surgical site infections, and the importance of prevention. Education occurs upon hire, annually thereafter, and when involvement in surgical procedures is added to an individual’s job responsibilities.
5.
C As of January 1, 2010, prior to all surgical procedures, the hospital educates patients, and their families as needed, who are undergoing a surgical procedure about surgical site infection prevention.
6.
C As of January 1, 2010, the hospital implements policies and practices aimed at reducing the risk of surgical site infections that meet regulatory requirements and are aligned with evidence-based standards (for example, the Centers for Disease Control and Prevention (CDC) and/or professional organization guidelines). (See also UP.01.03.01, EP 5)
7.
A As of January 1, 2010, the hospital conducts periodic risk assessments for surgical site infections, selects surgical site infection measures using best practices or evidence-based guidelines, monitors compliance with best practices or evidence-based guidelines, and evaluates the effectiveness of prevention efforts.
8.
A As of January 1, 2010, measurement strategies follow evidence-based guidelines, and surgical site infection rates are measured for the first 30 days following procedures that do not involve inserting implantable devices and for the first year following procedures involving implantable devices.
9.
A As of January 1, 2010, the hospital provides surgical site infection rate data and prevention outcome measures to key stakeholders, including leaders, licensed independent practitioners, nursing staff, and other clinicians.
10.
Page 17 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
C As of January 1, 2010, antimicrobial agents for prophylaxis used for a particular procedure or disease are administered according to evidence-based standards and guidelines for best practices.- Administer intravenous antimicrobial prophylaxis within one hour before incision (two hours are allowed for the administration of vancomycin and fluoroquinolones). - Discontinue the prophylactic antimicrobial agent within 24 hours after surgery (within 48 hours is allowable for cardiothoracic procedures).Footnote: See Joint Commission core measures at http://www.jointcommission.org/PerformanceMeasurement.
11.
A As of January 1, 2010, when hair removal is necessary, the hospital uses clippers or depilatories. Note: Shaving is an inappropriate hair removal method.
12.
Page 18 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations
Accreditation Program: Hospital Chapter: National Patient Safety Goals
Goal 8
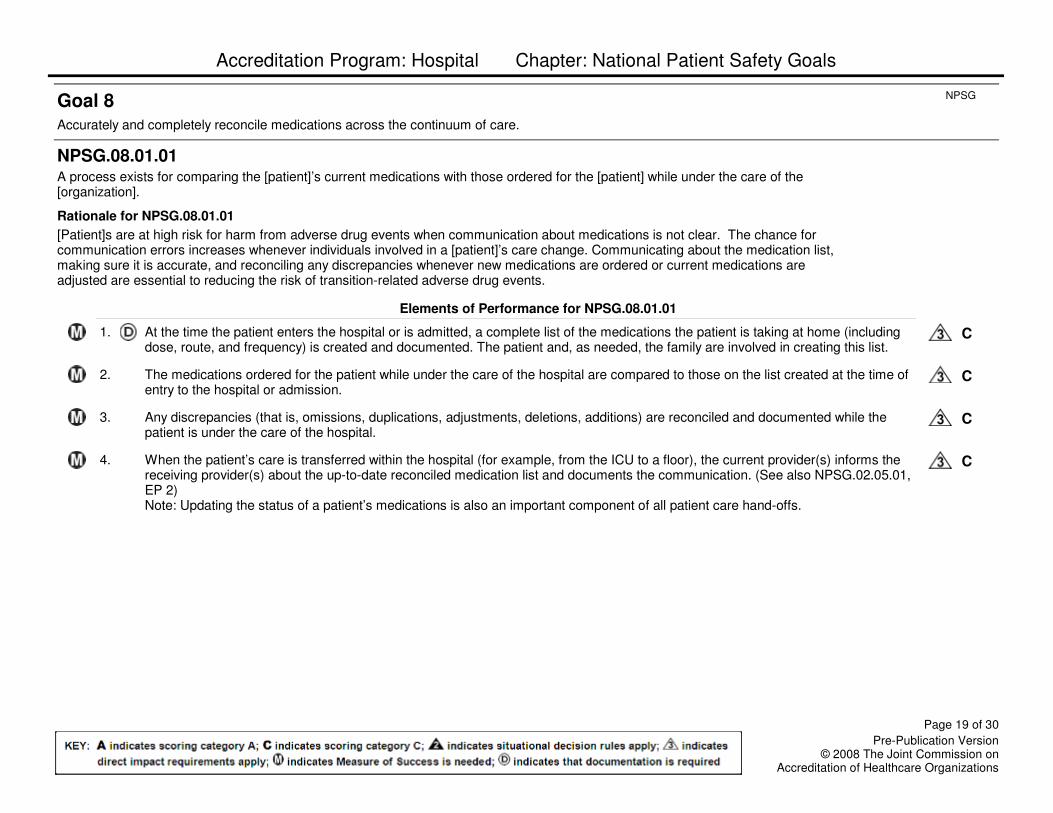
Accurately and completely reconcile medications across the continuum of care.
NPSG
NPSG.08.01.01
A process exists for comparing the [patient]’s current medications with those ordered for the [patient] while under the care of the [organization].
[Patient]s are at high risk for harm from adverse drug events when communication about medications is not clear. The chance for communication errors increases whenever individuals involved in a [patient]’s care change. Communicating about the medication list, making sure it is accurate, and reconciling any discrepancies whenever new medications are ordered or current medications are adjusted are essential to reducing the risk of transition-related adverse drug events.
Rationale for NPSG.08.01.01
Elements of Performance for NPSG.08.01.01
C At the time the patient enters the hospital or is admitted, a complete list of the medications the patient is taking at home (including dose, route, and frequency) is created and documented. The patient and, as needed, the family are involved in creating this list.
1.
C The medications ordered for the patient while under the care of the hospital are compared to those on the list created at the time of entry to the hospital or admission.
2.
C Any discrepancies (that is, omissions, duplications, adjustments, deletions, additions) are reconciled and documented while the patient is under the care of the hospital.
3.
C When the patient’s care is transferred within the hospital (for example, from the ICU to a floor), the current provider(s) informs the receiving provider(s) about the up-to-date reconciled medication list and documents the communication. (See also NPSG.02.05.01, EP 2)Note: Updating the status of a patient’s medications is also an important component of all patient care hand-offs.
4.
Page 19 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
NPSG.08.02.01
When a [patient] is referred to or transferred from one [organization] to another, the complete and reconciled list of medications is communicated to the next provider of service, and the communication is documented. Alternatively, when a [patient] leaves the [organization]’s care to go directly to his or her home, the complete and reconciled list of medications is provided to the [patient]’s known primary care provider, the original referring provider, or a known next provider of service. Note: When the next provider of service is unknown or when no known formal relationship is planned with a next provider, giving the [patient] and, as needed, the family the list of reconciled medications is sufficient.
The accurate communication of a [patient]’s reconciled medication list to the next provider of service reduces the risk of transition-related adverse drug events. The communication enables the next provider of service to receive thorough knowledge of the [patient]’s medications and to safely order/prescribe other medications that may be needed. This communication is especially important at transitions in care when a [patient] is referred or transferred from one organization to another.
Rationale for NPSG.08.02.01
Elements of Performance for NPSG.08.02.01
C The patient’s most current reconciled medication list is communicated to the next provider of service, either within or outside the hospital. The communication between providers is documented.
1.
C At the time of transfer, the transferring hospital informs the next provider of service how to obtain clarification on the list of reconciled medications.
2.
NPSG.08.03.01
When a [patient] leaves the [organization]’s care, a complete and reconciled list of the [patient]’s medications is provided directly to the [patient] and, as needed, the family, and the list is explained to the [patient] and/or family.
The accurate communication of the [patient]’s medication list to the [patient] and, as needed, the family, reduces the risk of transition-related adverse drug events. A thorough knowledge of the [patient]’s medications is essential for the [patient]’s primary care provider or next provider of service to manage the subsequent stages of care for the [patient].
Rationale for NPSG.08.03.01
Elements of Performance for NPSG.08.03.01
C When the patient leaves the hospital’s care, the current list of reconciled medications is provided and explained to the patient and, as needed, the family. This interaction is documented.Note: Patients and families are reminded to discard old lists and to update any records with all medication providers or retail pharmacies.
1.
Page 20 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
NPSG.08.04.01
In settings where medications are used minimally, or prescribed for a short duration, modified medication reconciliation processes are performed. Note: This requirement does not apply to [organization]s that do not administer medications. It may be important for health care organizations to know which types of medications their [patient]s are taking because these medications could affect the care, treatment, and services provided.
A number of [patient] care settings exist in which medications are not used, are used minimally, or are prescribed for only a short duration. This includes areas such as the emergency department, urgent and emergent care, convenient care, office-based surgery, outpatient radiology, ambulatory care, and behavioral health care. In these settings, obtaining a list of the [patient]’s original, known, and current medications that he or she is taking at home is still important; however, obtaining information on the dose, route, and frequency of use is not required.
Rationale for NPSG.08.04.01
Elements of Performance for NPSG.08.04.01
C The hospital obtains and documents an accurate list of the patient’s current medications and known allergies in order to safely prescribe any setting-specific medications (for example, intravenous contrast media, local anesthesia, antibiotics) and to assess for potential allergic or adverse drug reactions.
1.
C When only short-term medications (for example, a preprocedure medication or a short-term course of an antibiotic) will be prescribed and no changes are made to the patient's current medication list, the patient and, as needed, the family are provided with a list containing the short term medication additions that the patient will continue after leaving the hospital. Note: This list of new short term medications is not considered to be part of the original, known, and current medication list. When patients leave these settings, a list of the original, known, and current medications does not need to be provided, unless the patient is assessed to be confused or unable to comprehend adequately. In this case, the patient’s family is provided both medication lists and the circumstances are documented.
2.
C In these settings, a complete, documented medication reconciliation process is used when: Any new long-term (chronic) medications are prescribed.
3.
C In these settings, a complete, documented medication reconciliation process is used when: There is a prescription change for any of the patient’s current, known long-term medications.
4.
C In these settings, a complete, documented medication reconciliation process is used when: The patient is required to be subsequently admitted to an organization from these settings for ongoing care.
5.
C When a complete, documented, medication reconciliation is required in any of these settings, the complete list of reconciled medications is provided to the patient, and their family as needed, and to the patient’s known primary care provider or original referring provider or a known next provider of service.
6.
Page 21 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
Goal 9
Reduce the risk of [patient] harm resulting from falls.
NPSG
NPSG.09.02.01
The [organization] implements a fall reduction program that includes an evaluation of the effectiveness of the program.
Falls account for a significant portion of injuries in hospitalized patients, long term care residents, and home care recipients. In the context of the population it serves, the services it provides, and its environment of care, the [organization] should evaluate the [patient]’s risk for falls and take action to reduce the risk of falling as well as the risk of injury, should a fall occur. The evaluation could include a [patient]’s fall history; review of medications and alcohol consumption; gait and balance screening; assessment of walking aids, assistive technologies, and protective devices; and environmental assessments.
Rationale for NPSG.09.02.01
Elements of Performance for NPSG.09.02.01
A The hospital establishes a fall reduction program.1.
C The fall reduction program includes an evaluation appropriate to the patient population, settings, and services provided.2.
A The fall reduction program includes interventions to reduce the patient’s fall risk factors.3.
C Staff receive education and training for the fall reduction program.4.
C The hospital educates the patient and, as needed, the family on the fall reduction program and any individualized fall reduction strategies.
5.
A The hospital evaluates the fall reduction program to determine the effectiveness of the program. Note: Outcome indicators such as decreased number of falls and decreased number and severity of fall-related injuries could be used.
6.
Page 22 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
Goal 13
Encourage [patient]s’ active involvement in their own care as a [patient] safety strategy.
NPSG
NPSG.13.01.01
Identify the ways in which the [patient] and his or her family can report concerns about safety and encourage them to do so.
Communication with the [patient] and family about all aspects of care, treatment, and services is an important characteristic of a culture of safety. When the [patient] knows what to expect, he or she is more aware of possible errors and choices. The [patient] can also be an important source of information about potential adverse events and hazardous conditions.
Rationale for NPSG.13.01.01
Elements of Performance for NPSG.13.01.01
C The patient and family are educated on available reporting methods for concerns related to care, treatment, and services and patient safety issues.
1.
C The hospital provides the patient with information regarding infection control measures for hand hygiene practices, respiratory hygiene practices, and contact precautions according to the patient’s condition. The information is discussed with the patient and his or her family members on the day the patient enters the hospital or as soon as possible (for example, within 24–48 hours). The patient’s understanding of this information is evaluated and documented. (See also PC.02.03.01, EP 25) Note: The information provided to the patient may be in any form of media.
2.
C For surgical patients, the hospital describes the measures that will be taken to prevent adverse events in surgery. Examples include, but are not limited to, patient identification practices, prevention of surgical infections, and marking of the procedure sites. The patient’s understanding is evaluated and documented. (See also PC.02.03.01, EP 25) Note: The information provided to the patient may be in any form of media.
3.
C The hospital encourages patients and their families to report concerns about safety.4.
Page 23 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
Goal 15
The organization identifies safety risks inherent in its [patient] population.
NPSG
NPSG.15.01.01
The [organization] identifies [patient]s at risk for suicide.Note: This requirement only applies to psychiatric hospitals and patients being treated for emotional or behavioral disorders in general hospitals.
Suicide of a care recipient while in a staffed, round-the-clock care setting is a frequently reported type of sentinel event. Identification of individuals at risk for suicide while under the care of or following discharge from a health care organization is an important step in protecting these at-risk individuals.
Rationale for NPSG.15.01.01
Elements of Performance for NPSG.15.01.01
C The risk assessment includes identification of specific patient factors and environmental features that may increase or decrease the risk for suicide.
1.
C The hospital addresses the patient’s immediate safety needs and most appropriate setting for treatment.2.
C The hospital provides information such as a crisis hotline to individuals at risk for suicide and their family members.3.
Page 24 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
Goal 16
Improve recognition and response to changes in a patient’s condition.
NPSG
NPSG.16.01.01
The [organization] selects a suitable method that enables health care staff members to directly request additional assistance from a specially trained individual(s) when the [patient]’s condition appears to be worsening.
A significant number of critical inpatient events are preceded by warning signs prior to the event. A majority of [patient]s who have cardiopulmonary or respiratory arrest demonstrate clinical deterioration in advance. Early response to changes in a [patient]’s condition by a specially trained individual(s) may reduce cardiopulmonary arrests and [patient] mortality.
Rationale for NPSG.16.01.01
Elements of Performance for NPSG.16.01.01
A The hospital selects an early recognition and response method most suitable for its needs and resources.1.
A The hospital develops criteria for calling additional assistance to respond to a change in the patient’s condition or a perception of change by the staff, the patient, and/or family.
2.
C Based on the hospital’s criteria, staff seek additional assistance when they have concerns about a patient’s condition.3.
C The hospital encourages the patient and family to seek assistance when the patient’s condition worsens.4.
C Formal education for urgent response policies and practices is conducted with the staff and licensed independent practitioners who may request assistance and those who may respond to those requests.
5.
A The hospital measures cardiopulmonary arrest, respiratory arrest, and mortality rates before and after implementation of an early intervention plan.
6.
A The hospital evaluates its early intervention program and any underlying organizational system issues, takes appropriate action to improve its intervention system, and measures the effectiveness of those actions on a regular basis.Note: Hospitals are not required to create “rapid response teams” or “medical emergency teams” in order to meet this goal. The existence of these types of teams does not mean that all of the elements of performance are automatically achieved.
7.
Page 25 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations
Accreditation Program: Hospital Chapter: National Patient Safety Goals
Universal Protocol
The organization meets the expectations of the Universal Protocol.
NPSG
UP.01.01.01
Conduct a preprocedure verification process.
The preprocedure verification is an ongoing process of information gathering and verification, beginning with the decision to perform a procedure, continuing through all settings and interventions involved in the preprocedure preparation of the [patient], up to and including the time-out just before the start of the procedure.
The purpose of the preprocedure verification process is to make sure that all relevant documents and related information or equipment are:- Available prior to the start of the procedure.- Correctly identified, labeled, and matched to the [patient]’s identifiers.- Reviewed and are consistent with the [patient]’s expectations and with the team’s understanding of the intended [patient], procedure, and site.
Missing information or discrepancies are addressed before starting the procedure.
Rationale for UP.01.01.01
Elements of Performance for UP.01.01.01
A Verification of the correct person, correct site, and correct procedure occurs at the following times: - At the time the procedure is scheduled- At the time of preadmission testing and assessment- At the time of admission or entry into the facility for a procedure, whether elective or emergent- Before the patient leaves the preprocedure area or enters the procedure room- Anytime the responsibility for care of the patient is transferred to another member of the procedural care team, (including the anesthesia providers) at the time of, and during, the procedure- With the patient involved, awake and aware, if possible
1.
A When the patient is in the preprocedure area, immediately prior to moving the patient to the procedure room, a checklist (for example, paper, electronic, or other medium such as a wall-mounted whiteboard) is used to review and verify that the following items are available and accurately matched to the patient:- Relevant documentation (for example, history and physical, nursing assessment, and pre-anesthesia assessment)- Accurately completed, and signed, procedure consent form- Correct diagnostic and radiology test results (for example, radiology images and scans, or pathology and biopsy reports) that are properly labeled- Any required blood products, implants, devices, and/or special equipment for the procedure
2.
Page 26 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
UP.01.02.01
Mark the procedure site.
Marking the procedure site allows staff to identify without ambiguity the intended site for the procedure.
Rationale for UP.01.02.01
Elements of Performance for UP.01.02.01
C For all procedures involving incision or percutaneous puncture or insertion, the intended procedure site is marked. The marking takes into consideration laterality, the surface (flexor, extensor), the level (spine), or specific digit or lesion to be treated.Note: For procedures that involve laterality of organs, but the incision(s) or approaches may be from the midline or from a natural orifice, the site is still marked and the laterality noted.
1.
C The procedure site is initially marked before the patient is moved to the location where the procedure will be performed and takes place with the patient involved, awake and aware, if possible.
2.
C The procedure site is marked by a licensed independent practitioner or other provider who is privileged or permitted by the hospital to perform the intended surgical or nonsurgical invasive procedure. This individual will be involved directly in the procedure and will be present at the time the procedure is performed. Note: Final confirmation and verification of the site mark takes place during the time-out.
3.
A The method of marking the site and the type of mark is unambiguous and is used consistently throughout the hospital.4.
C The site marking has the following characteristics:- It is made at or near the procedure site or the incision site. Other nonprocedure site(s) are not marked unless necessary for some other aspect of care. - It includes, preferably, the surgeon’s or proceduralist’s initials, with or without a line representing the proposed incision. - It is made using a marker that is sufficiently permanent to remain visible after completion of the skin prep and sterile draping. Adhesive site markers are not to be used as the sole means of marking the site.- It is positioned to be visible after the patient has his or her skin prepped, is in his or her final position, and sterile draping is completed.
5.
C For spinal procedures, in addition to pre-operative skin marking of the general spinal region, special intraoperative radiographic techniques are used for marking the exact vertebral level.
6.
Page 27 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
A A defined, alternative process is in place for patients who refuse site marking or who cannot easily be marked under the following conditions: - For cases in which it is technically or anatomically impossible or impractical to mark the site (mucosal surfaces, perineum, premature infants), an alternative method for visually identifying the correct side and site is used. For example, the hospital may place a temporary, unique wrist band on the side of the procedure containing the patient’s name, and use a second identifier for the intended procedure and site.- For minimal access procedures that intend to treat a lateralized internal organ, whether percutaneous or through a natural orifice, the intended side is indicated by a mark at or near the insertion site, and remains visible after completion of the skin prep and sterile draping.- For interventional procedure cases for which the catheter/instrument insertion site is not predetermined (for example, cardiac catheterization, pacemaker insertion). - For teeth, the operative tooth name(s) and number are indicated on documentation or the operative tooth (teeth) is marked on the dental radiographs or dental diagram. The documentation, images, and/or diagrams are available in the procedure room before the start of the procedure. - For premature infants, for whom the mark may cause a permanent tattoo.
7.
Page 28 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
UP.01.03.01
A time-out is performed immediately prior to starting procedures.
The purpose of the time-out immediately before starting the procedure is to conduct a final assessment that the correct [patient], site, positioning, and procedure are identified and that, as applicable, all relevant documents, related information, and necessary equipment are available.
The time-out is consistently initiated by a designated member of the team and includes active communication among all relevant members of the procedure team. It is conducted in a standardized fail-safe mode (that is, the procedure is not started until all questions or concerns are resolved).
Rationale for UP.01.03.01
Elements of Performance for UP.01.03.01
A The time-out is conducted prior to starting the procedure and, ideally, prior to the introduction of the anesthesia process (including general/regional anesthesia, local anesthesia, and spinal anesthesia), unless contraindicated.
1.
A The time-out has the following characteristics:- It is standardized (as defined by the hospital). - It is initiated by a designated member of the team. - It involves the immediate members of the procedure team including the proceduralist(s), the anesthesia providers, the circulating nurse, the operating room technician, and other active participants as appropriate for the procedure, who will be participating in the procedure at its inception.- It involves interactive verbal communication between all team members, and any team member is able to express concerns about the procedure verification.- It includes a defined process for reconciling differences in responses.
2.
A During the time-out, other activities are suspended, to the extent possible without compromising patient safety, so that all relevant members of the team are focused on the active confirmation of the correct patient, procedure, site, and other critical elements.
3.
A When two or more procedures are being performed on the same patient, a time-out is performed to confirm each subsequent procedure before it is initiated.
4.
Page 29 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations

Accreditation Program: Hospital Chapter: National Patient Safety Goals
A The time-out addresses the following: - Correct patient identity- Confirmation that the correct side and site are marked- An accurate procedure consent form- Agreement on the procedure to be done- Correct patient position- Relevant images and results are properly labeled and appropriately displayed- The need to administer antibiotics or fluids for irrigation purposes (See also NPSG.07.05.01, EP 7)- Safety precautions based on patient history or medication use
5.
C The completed components of the Universal Protocol and time-out are clearly documented.6.
Page 30 of 30
Pre-Publication Version© 2008 The Joint Commission on
Accreditation of Healthcare Organizations


















