Sensitivity and Specificity of Hemodynamic Criteria in the Diagnosis ...
12
Sensitivity and Specificity of Hemodynamic Criteria in the Diagnosis of Acute Right Ventricular Infarction JOSE LOPEZ-SENDON, M.D., ISABEL COMA-CANELLA, M.D., AND CARLOS GAMALLO, M.D. SUMMARY To test the sensitivity and specificity of hemodynamic criteria for acute right ventricular in- farction (RVI), two groups of patients with anatomically proved acute myocardial infarction and hemo- dynamic monitoring were studied. Group A included 22 patients with acute RVI and group B, 38 with infarc- tion confined to the left ventricle. In both groups, the closest relation between right atrial and pulmonary capillary pressures (RAP and PCP), as well as the presence of a severe noncompliant pattern (SNCP), were studied. A SNCP was defined as a y descent deeper than the x descent in RAP. RAP was equal to or higher than PCP in 10 patients from group A and in none from group B. In group B, a significant relation was found between RAP and PCP (r = 0.777, y = 0.43x + 0.18) (p < 0.05), and the 95% confidence limits could be calculated. Above these limits, a closer relation between RAP and PCP was only found in patients with RVI. However, six patients with RVI showed an RAP/PCP relation within 95% confidence limits of group B (sen- sitivity 72.7%, specificity 100%). A SNCP was present in 12 patients with RVI and only in one without RVI (p < 0.01) (sensitivity 54.5% and specificity 97.4%). When either criterion is present (close relation between RAP and PCP or SNCP), a high sensitivity (81.8%) and specificity (97.4%) can be achieved in the diagnosis of acute RVI. RIGHT VENTRICULAR INFARCTION often represents an interesting diagnostic and therapeutic challenge. Its diagnosis is based on clinical, hemo- dynamic, echocardiographic and radionuclide data.'-18 The anatomic diagnosis of right ventricular necrosis can only be made by demonstrating an anomalous myocardial uptake of technetium pyrophos- phate,10' 12, 17, 19 but there is an incidence of false- positive interpretations20 and usually right ventricular infarction is first suspected at bedside when hemodynamic alterations suggesting primary right ventricular dysfunction are present.'-6, 9, 11-14, 18 This situation is termed ischemic right ventricular dysfunc- tion."8 The finding of a right atrial pressure equal to or greater than the left ventricular filling pressure has been suggested as the characteristic hemodynamic profile of right ventricular infarction,3 and this diagnosis has been confirmed in some patients at necropsy.3 8, 8, 11, 14, 18 This strict criterion is probably very specific,21 but the amount of hemodynamic data from patients with right ventricular infarction con- firmed by autopsy is too small to permit definitive con- clusions about its sensitivity. Moreover, the hemo- dynamics in patients in whom the diagnosis of acute right ventricular infarction was established at necrop- sy have not been reported. Isner and Roberts21 per- formed such an investigation, but hemodynamic studies were performed in only four patients with biventricular infarction, two of whom had an old right ventricular infarction. We studied patients with a postmortem anatomic diagnosis of acute myocardial infarction in whom hemodynamic monitoring had been performed. We From the Coronary Care Unit, Servicio de Coronariopatias, Ciudad Sanitaria La Paz, Universidad Aut6noma de Madrid, Madrid, Spain. Address for correspondence: J. Lopez-Sendon, M.D., Unidad Coronaria, Ciudad Sanitaria La Paz, Madrid-34, Spain. Received February 28, 1980; revision accepted December 3, 1980. Circulation 64, No. 3, 1981. analyzed the hemodynamic alterations that may help to increase accuracy in the diagnosis of right ven- tricular infarction. Materials and Methods Sixty-one patients with acute myocardial infarction confirmed at postmortem examination in whom hemodynamic monitoring had been performed were studied. All had been admitted to the coronary care unit between August 1977 and December 1979. Patients with valvular heart disease, cardiomyopathy, pericardial disease or cardiac surgery were excluded. Two groups were defined, based on the presence of acute right ventricular necrosis found at the post- mortem examination. Group A included 22 patients with acute right ventricular necrosis. Group B in- cluded 38 patients without acute right ventricular necrosis. The remaining patient, without acute right ventricular necrosis, had evidence of an old posterior right ventricular infarction and was therefore excluded from a statistical evaluation. Anatomic Study Transverse sections of the heart were incubated in triphenyl tetrazolium chloride solution22 to label or identify the necrotic areas and were then examined microscopically to make the histologic diagnosis of acute myocardial infarction. The extent of right ven- tricular necrosis was classified according to the method of Isner and Roberts21: grade I = necrosis of less than 50% of the right ventricular posterior wall; grade II = necrosis limited to but involving more than 50% of the posterior wall; grade III = necrosis of the posterior wall and less than 50% of the anterolateral wall; and grade IV = necrosis of the right ventricular posterior wall and more than 50% of the anterolateral wall. We also added a grade V: involvement of a por- tion of the anterolateral wall without posterior wall necrosis. The lungs were also examined to investigate the presence of chronic obstructive pulmonary disease and pulmonary embolism. 515 by guest on April 7, 2018 http://circ.ahajournals.org/ Downloaded from
-
Upload
truongquynh -
Category
Documents
-
view
225 -
download
2
Transcript of Sensitivity and Specificity of Hemodynamic Criteria in the Diagnosis ...

Sensitivity and Specificity of Hemodynamic Criteriain the Diagnosis of Acute Right Ventricular InfarctionJOSE LOPEZ-SENDON, M.D., ISABEL COMA-CANELLA, M.D., AND CARLOS GAMALLO, M.D.
SUMMARY To test the sensitivity and specificity of hemodynamic criteria for acute right ventricular in-farction (RVI), two groups of patients with anatomically proved acute myocardial infarction and hemo-dynamic monitoring were studied. Group A included 22 patients with acute RVI and group B, 38 with infarc-tion confined to the left ventricle. In both groups, the closest relation between right atrial and pulmonarycapillary pressures (RAP and PCP), as well as the presence of a severe noncompliant pattern (SNCP), were
studied. A SNCP was defined as a y descent deeper than the x descent in RAP. RAP was equal to or higherthan PCP in 10 patients from group A and in none from group B. In group B, a significant relation was foundbetween RAP and PCP (r = 0.777, y = 0.43x + 0.18) (p < 0.05), and the 95% confidence limits could becalculated. Above these limits, a closer relation between RAP and PCP was only found in patients with RVI.However, six patients with RVI showed an RAP/PCP relation within 95% confidence limits of group B (sen-sitivity 72.7%, specificity 100%). A SNCP was present in 12 patients with RVI and only in one without RVI (p< 0.01) (sensitivity 54.5% and specificity 97.4%). When either criterion is present (close relation between RAPand PCP or SNCP), a high sensitivity (81.8%) and specificity (97.4%) can be achieved in the diagnosis of acuteRVI.
RIGHT VENTRICULAR INFARCTION oftenrepresents an interesting diagnostic and therapeuticchallenge. Its diagnosis is based on clinical, hemo-dynamic, echocardiographic and radionuclide data.'-18The anatomic diagnosis of right ventricular necrosiscan only be made by demonstrating an anomalousmyocardial uptake of technetium pyrophos-phate,10' 12, 17, 19 but there is an incidence of false-positive interpretations20 and usually right ventricularinfarction is first suspected at bedside whenhemodynamic alterations suggesting primary rightventricular dysfunction are present.'-6, 9, 11-14, 18 Thissituation is termed ischemic right ventricular dysfunc-tion."8The finding of a right atrial pressure equal to or
greater than the left ventricular filling pressure hasbeen suggested as the characteristic hemodynamicprofile of right ventricular infarction,3 and thisdiagnosis has been confirmed in some patients atnecropsy.3 8, 8, 11, 14, 18 This strict criterion is probablyvery specific,21 but the amount of hemodynamic datafrom patients with right ventricular infarction con-firmed by autopsy is too small to permit definitive con-clusions about its sensitivity. Moreover, the hemo-dynamics in patients in whom the diagnosis of acuteright ventricular infarction was established at necrop-sy have not been reported. Isner and Roberts21 per-formed such an investigation, but hemodynamicstudies were performed in only four patients withbiventricular infarction, two of whom had an old rightventricular infarction.We studied patients with a postmortem anatomic
diagnosis of acute myocardial infarction in whomhemodynamic monitoring had been performed. We
From the Coronary Care Unit, Servicio de Coronariopatias,Ciudad Sanitaria La Paz, Universidad Aut6noma de Madrid,Madrid, Spain.
Address for correspondence: J. Lopez-Sendon, M.D., UnidadCoronaria, Ciudad Sanitaria La Paz, Madrid-34, Spain.
Received February 28, 1980; revision accepted December 3, 1980.Circulation 64, No. 3, 1981.
analyzed the hemodynamic alterations that may helpto increase accuracy in the diagnosis of right ven-tricular infarction.
Materials and Methods
Sixty-one patients with acute myocardial infarctionconfirmed at postmortem examination in whomhemodynamic monitoring had been performed werestudied. All had been admitted to the coronary careunit between August 1977 and December 1979.Patients with valvular heart disease, cardiomyopathy,pericardial disease or cardiac surgery were excluded.Two groups were defined, based on the presence of
acute right ventricular necrosis found at the post-mortem examination. Group A included 22 patientswith acute right ventricular necrosis. Group B in-cluded 38 patients without acute right ventricularnecrosis. The remaining patient, without acute rightventricular necrosis, had evidence of an old posteriorright ventricular infarction and was therefore excludedfrom a statistical evaluation.
Anatomic StudyTransverse sections of the heart were incubated in
triphenyl tetrazolium chloride solution22 to label oridentify the necrotic areas and were then examinedmicroscopically to make the histologic diagnosis ofacute myocardial infarction. The extent of right ven-tricular necrosis was classified according to themethod of Isner and Roberts21: grade I = necrosis ofless than 50% of the right ventricular posterior wall;grade II = necrosis limited to but involving more than50% of the posterior wall; grade III = necrosis of theposterior wall and less than 50% of the anterolateralwall; and grade IV = necrosis of the right ventricularposterior wall and more than 50% of the anterolateralwall. We also added a grade V: involvement of a por-tion of the anterolateral wall without posterior wallnecrosis. The lungs were also examined to investigatethe presence of chronic obstructive pulmonary diseaseand pulmonary embolism.
515
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 64, No 3, SEPTEMBER 1981
TABLE 1. Anatomic and Hemodynamic Findings in Group A (n = 22)Relation between
Myocardial necrosis Lung Low Interventions orPt Acute LV Acute RV Old LV disease output Initial clinical events
1 P + IVS II - COPD Yes 8/16 Dextran +
2 P+IVS
3 P+IVS
4 P+IVS
5 P+IVS
6 A+P+IVS7 A+P+IVS8 P+IVS
9 A+P+IVS10 P+IVS11 P+IVS12 P+IVS
13 P+IVS
14 A+IVS15 A+P+IVS16 P +IVS
17 A+P+IVS18 A+IVS19 P+IVS20 A + IVS21 A+P+IVS22 P +IVS
II
III
I
IVS COPD + APE
- CPE
I
IIIII
IIIII
- CPE- COPDP COPD + CPEA -
II
V _I _
II -
II AV P+IVSIV
IIIII
- COPD
- COPD
Yesdopamine
17/34 Dextran +nitroprusside
Yes 15/10 Dextran +dopamine
Yes 14/20 Dextran +dopamine
Yes 6/7 Dextran +dopamine
Yes 14/16 DextranYes 18/38 NitroprussideYes 10/31 Dextran +
nitroprussideYes 13/25 NitroprussideNo 16/28 NitroprussideNo 11/14 DextranYes 9/35 Dextran +
nitroprussideYes 12/19 Dextran +
dopamineYesYes
10/2515/22 AVB
Yes 13/17 IVSR +nitroprusside
Yes 19/40 NitroprussideNo 9/20 FurosemideYesYesYesYes
6/2812/2212/2113/25
DopamineAVB
DextranAVB
*InternittentAbbreviations: LV = left ventricle; RV = right ventricle; RAP = right atrial pressure; PCP = pulmonary capillary pressure;
P = posterior; A = anterior; IVS = interventricular septum; COPD = chronic obstructive pulmonary disease; APE = acutepulmonary embolism; CPE = chronic pulmonary embolism; IVSR =interventricular septal rupture; AVB = atrioventricularblock; PH = pulmonary hypertension; I, II, III, IV, V location of right ventricular infarction (see text); Timing = time ofdiagnostic finding.
Hemodynamic Study
Right-heart hemodynamic monitoring was per-formed in all patients for 1-10 days. At admission, aSwan-Ganz thermodilution catheter was inserted intothe pulmonary trunk through a right antecubital vein.Right atrial (RAP), pulmonary trunk (PTP) andpulmonary capillary (PCP) pressures were recordedwith a Hewlett Packard 1280 transducer on a
Siemens-Elema Mingograph 34. The RAP wave formwas carefully analyzed. The term "tsevere non-
compliant pattern" was used when RAP showed an M
or W wave form with the y descent deeper than the x,
and "mild noncompliant pattern" when the y descentwas equal to the x.18 Cardiac output was determinedby thermodilution on an Edwards 9500 computer. In
every case, at least three successive determinationswere made, and the average value was calculated andstandardized for body surface area to cardiac index.A severe low-output syndrome was defined as a car-
diac index lower than 2.2 1/min2 with evidence ofreduced tissue perfusion, such as mental impairmentand oliguria or anuria. A complete hemodynamicevaluation was made at least every 8 hours. One to 40hemodynamic studies were performed per patient(mean 13 ± 9).
Interventions
Volume loading with Dextran-40 was performed inevery patient with a basal PCP lower than 18 mmHg.18 Other interventions included i.v. administration
516 CIRCULATION
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from

HEMODYNAMIC CRITERIA FOR ACUTE RV INFARCTION/Lopez-Sendon et al.
TABLE 1. (Continued)RAP and PCP Noncompliant pattern
Closest Indicative InterventionsRAP/PCP of RVI or clinical(mm Hg) RAP ' PCP timing Type events Timing22/22 22/22 1st day Severe Dextran 1st day*
22/22 22/22 1st day Mild AVB Initial*
20/20 26/22 Initial Severe - Initial
23/23 26/23 Initial Severe - Initial
19/19 22/20 2nd day Severe - Initial
27/27 28/23 Initial Severe - Initial18/30 - 1st day* Severe PH Initial*9/15 - -
12/15 - 2nd day*10/15 - - Severe PH lst day*23/23 24/23 Initial Mild Dextran 3rd day*15/15 15/15 1st day Mild Dextran 1st day
21/21 24/22 1st day Severe - Initial
10/25 - -20/22 - Initial* Severe AVB 3rd day*13/13 13/13 Initial
12/20 - - Severe PH 3rd day*5/10 - -5/16 - -14/17 - Ist day Severe AVB lst day*15/17 - 1st day - - -15/16 - lst day* Severe AVB lst day*
of diuretics or inotropic or vasoactive drugs.Special attention was given to the initial relation-
ship between RAP and PCP levels and to the pres-ence of a noncompliant pattern in the RAP waveform, as well as to the relation between these measure-ments after therapeutic interventions or clinicalevents.
Statistical AnalysisAll statistical analyses were performed considering
the initial determinations and those which showed theclosest relation (minimal difference) between RAPand PCP levels. Fisher's exact test was applied toevaluate the difference in incidence of hemodynamicand anatomic data in each group. A gaussian distribu-tion of RAP and PCP was demonstrated in bothgroups by the Kolmogorov-Smirnov test. The Pear-son's correlation coefficient between RAP and PCPwas calculated as well as the regression equation, itsS, (standard error of the estimate) and the 95% con-fidence limits for each set of data.
Results
Anatomic Findings
The locations of acute or healed myocardialinfarction and pulmonary lesions for each patient arelisted in tables 1 and 2. In group A, both right and leftventricular free walls and the interventricular septumwere involved in all patients. The incidence of acuteleft posterior myocardial infarction was higher ingroup A (19 patients, 86.4%) than in group B (13patients, 34.2%) (p < 0.01). The incidence of leftanterior myocardial infarction was lower in group A(nine patients, 40.9%) than in group B (31 patients,81.6%) (NS). Acute interventricular septal necrosiswas found in all group A patients, and in 31 (81.6%) ofgroup B patients (NS). The incidence of chronic ob-structive pulmonary disease or pulmonary thrombo-embolism, both well-known causes of right ventricu-lar dysfunction, was similar in group A (eight pa-tients, 36.4%) and group B (13 patients, 34.2%) (NS).
517
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 64, No 3, SEPTEMBER 1981
TABLE 2. Anatomic and Hemodynamic Findings in Group B (n - 38)Relation between RAP and PCP Noncompliant pattern
LVmyocardial Interventions Interventionsnecrosis Lung Low or clinical Closest or clinical
Pt Acute Old disease output Initial events RAP/PCP Type events Timing1 A 4- TV - - Yes 12/20 - 12/20 - - -1 r I 1 L V W
2 A+P+IVS3 A+IVS
4 P+IVS5 P6 A+IVS7 A + IVS8 A9 A+IVS10 A+IVS11 A+P+IVS12 A + IVS13 A+IVS
14 A+P+IVS15 A+IVS16 A+IVS17 A+IVS18 A+IVS19 A+IVS20 A21 A+IVS22 A + IVS23 A+P+IVS24 P25 A26 A + IVS27 A + IVS28 P +IVS29 A+P+IVS30 A+IVS31 P +IVS32 A + IVS33 A34 A+IVS35 A+P+IVS36 P+IVS37 A38 P+IVSAbbreviations: Se
- COPDA IJO -L &/ ws-/&Ik
Yes 17/31 Dextran 12/25Yes 10/33 Nitroprusside 11/22
+ dextran- - Yes 5/12 - 5/12- COPD +APE Yes 3/7 - 3/7- - No 22/50 Nitroprusside 2/14- COPD No 10/32 Tamponade 21/22- - Yes 14/29 - 14/29- - No 7/10 - 7/10- - Yes 12/20 - 12/20P - No 8/26 Nitroprusside 4/15- COPD No 8/20 - 8/20- COPD + CPE Yes 11/30 Furosemide 9/25
+ digoxin- - Yes 16/33 - 16/33- - No 8/26 Nitroprusside 7/20- - Yes 10/26 AVB 12/28- CPE Yes 8/20 Tamponade 20/20- COPD Yes 11/18 Tamponade 18/20- - Yes 7/15 Tamponade 18/18
P +IVS - Yes 20/35 Nitroprusside 10/20- COPD Yes 13/30 Nitroprusside 6/15- COPD No 12/30 - 12/30- APE Yes 11/23 - 11/23- COPD No 20/42 Prazosin 5/15- - Yes 7/20 Dopamine 0/10- - Yes 12/20 - 12/20P - No 8/23 Prazosin 5/12A - Yes 12/28 Nitroprusside 8/19- COPD Yes 12/30 Nitroprusside 6/18- - No 7/25 Nitroprusside 4/10- - No 15/45 Nitroprusside 8/23- COPD Yes 10/28 - 10/28
A + IVS - Yes 12/31 - 12/31A + IVS - Yes 20/40 Nitroprusside 12/22- - Yes 15/31 Nitroprusside 12/21- - Yes 11/18 - 11/18P - Yes 14/33 Nitroprusside 9/23- - Yes 9/19 - 9/19
,e table 1.
Hemodynamic Data
The incidence of severe low-output syndrome wasvery high in both group A (19 patients, 86.4%) andgroup B (27 patients, 71.1%), with no statisticaldifference between the groups.
Relationship ofRAP and PCPInitial RAP and PCP values and measurement after
interventions or relevant clinical events are shown intables 1 and 2. Initial determinations of RAP andPCP values at admission and before treatment are
Mild AVB 2nd day*
Mild 1st day*
Severe PH 3rd day*
518 CIRCULATION
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from

HEMODYNAMIC CRITERIA FOR ACUTE RV INFARCTION/Lopez-Sendon et al.
A A AMI with RVI n=22
o B AMI without RVI n=38
0 0 0
A C A0
A CC C
00
C CAC C ACO
A
C 03C
FIGURE 1. Relation between right atrialpressure (RAP) and pulmonary capillarypressure (PCP) at admission and beforetreatment. AMI = acute myocardial infarc-tion; R VI = right ventricular infarction.
PCP mmHg
represented in figure 1. A more significant correlationcould be demonstrated between these values in groupB (r = 0.824,p < 0.01) than in group A (r = 0.42 1,p< 0.05), but no difference could be demonstratedbetween groups because of the wide dispersion ingroup A.The minimum difference (closest relation) between
RAP and PCP values recorded during thehemodynamic profile evolution of each patient isshown in figure 2A. Usually, RAP was closer to PCPin both groups when left ventricular failure was notpresent or when PCP was reduced after therapeutic in-terventions such as administration of i.v. nitro-prusside or furosemide.
In group A, the RAP was equal to or higher thanthe PCP at some point in 10 patients. In six this oc-curred after dextran or dextran plus dopamine infu-sion, in one after nitroprusside administration, in twoafter dextran plus nitroprusside and in the otherthroughout the entire duration of the hemodynamic
monitoring. In seven patients, RAP values were 1-5mm Hg lower than PCP values. This relation wasobserved after relief of pulmonary congestion withnitroprusside or furosemide in three patients, coincid-ing with atrioventricular block in another threepatients and after dextran administration in one. Infive of these patients the RAP was greater than 10 mmHg. In the remaining five patients from group A, thedifference between RAP and PCP was greater than 5mm Hg throughout hemodynamic monitoring.
In group B, RAP was usually lower than PCP. Theexceptions were four patients with left ventricular rup-ture in whom RAP approached or equaled PCP valuesafter cardiac tamponade. In these patients, the closestrelation between RAP and PCP recorded before car-diac tamponade was considered for the statisticalanalysis. In only two patients without cardiac tam-ponade were RAP values found to reach 1-5 mm Hgbelow PCP values. RAP levels in both were less than10 mm Hg and the difference between RAP and PCP
35-
30-
25 -
20-
RAPmm Hg
15 -
10
5
a %0 5 io 15 2o
PCP mm Hg
RAPmm Hg
35.
30-
25
20-
15-
10
b25 30 35
r = 0.683
A y= 0.86x - 0,681,968SX = 8.88
r = 0o777
B y = 043x +0,18
196Syx 4,45
FIGURE 2. (A) Closest relation between right atrial pressure (RAP) and pulmonary capillary pressure (PCP) in groups A andB. AMI = acute myocardial infarction; R VI = right ventricular infarction. (B) Linear regression equation and 95% (± 1.96Sy. x) confidence interval.
RAPmm Hg
519
0
CAA 03
0 C
A A AMI with RVI n=22
o B AMI without RVI n=38
As-A
C 00
A C A C CA 0 00
/o 0 CC C
o o0 o
0
0
A
,B
10 15 20
PCP mm,Hg25 30 35
.~~~ ~ ~ ~ . . . .
A
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 64, No 3, SEPTEMBER 1981
increased when RAP exceeded 10 mm Hg.When the hemodynamic measurements showing the
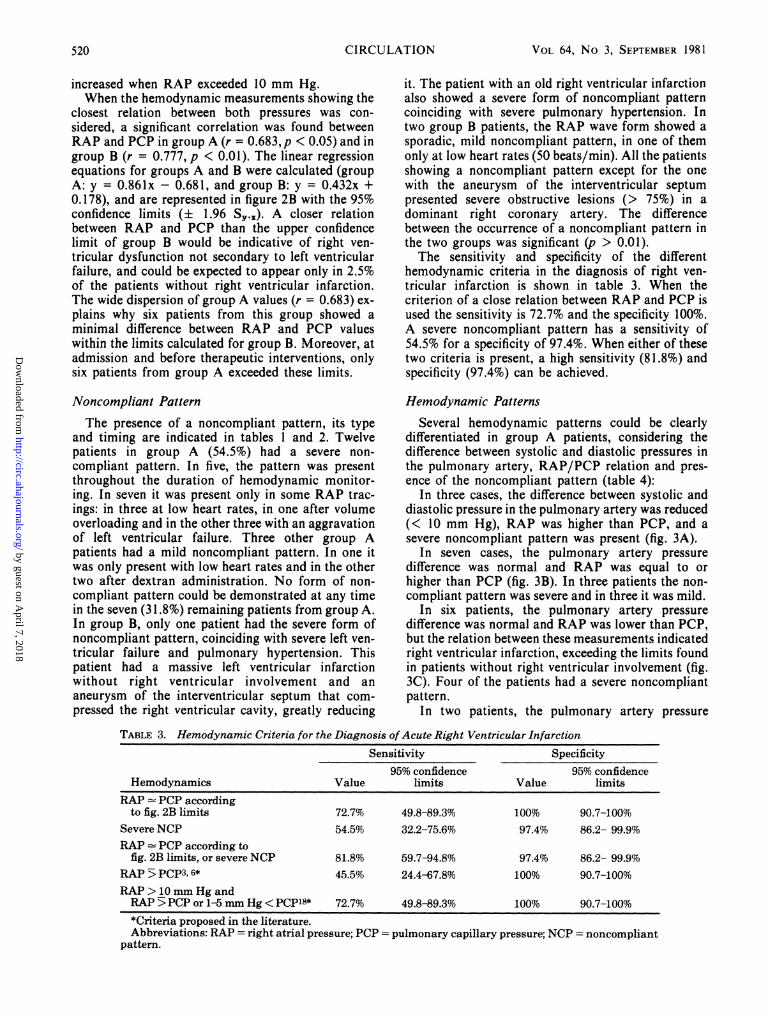
closest relation between both pressures was con-sidered, a significant correlation was found betweenRAP and PCP in group A (r = 0.683,p < 0.05) and ingroup B (r = 0.777, p < 0.01). The linear regressionequations for groups A and B were calculated (groupA: y = 0.861x - 0.681, and group B: y = 0.432x +0.178), and are represented in figure 2B with the 95%confidence limits (+ 1.96 S,). A closer relationbetween RAP and PCP than the upper confidencelimit of group B would be indicative of right ven-tricular dysfunction not secondary to left ventricularfailure, and could be expected to appear only in 2.5%of the patients without right ventricular infarction.The wide dispersion of group A values (r = 0.683) ex-plains why six patients from this group showed aminimal difference between RAP and PCP valueswithin the limits calculated for group B. Moreover, atadmission and before therapeutic interventions, onlysix patients from group A exceeded these limits.
Noncompliant Pattern
The presence of a noncompliant pattern, its typeand timing are indicated in tables 1 and 2. Twelvepatients in group A (54.5%) had a severe non-compliant pattern. In five, the pattern was presentthroughout the duration of hemodynamic monitor-ing. In seven it was present only in some RAP trac-ings: in three at low heart rates, in one after volumeoverloading and in the other three with an aggravationof left ventricular failure. Three other group Apatients had a mild noncompliant pattern. In one itwas only present with low heart rates and in the othertwo after dextran administration. No form of non-compliant pattern could be demonstrated at any timein the seven (31.8%) remaining patients from group A.In group B, only one patient had the severe form ofnoncompliant pattern, coinciding with severe left ven-tricular failure and pulmonary hypertension. Thispatient had a massive left ventricular infarctionwithout right ventricular involvement and an
aneurysm of the interventricular septum that com-pressed the right ventricular cavity, greatly reducing
it. The patient with an old right ventricular infarctionalso showed a severe form of noncompliant patterncoinciding with severe pulmonary hypertension. Intwo group B patients, the RAP wave form showed asporadic, mild noncompliant pattern, in one of themonly at low heart rates (50 beats/min). All the patientsshowing a noncompliant pattern except for the onewith the aneurysm of the interventricular septumpresented severe obstructive lesions (> 75%) in adominant right coronary artery. The differencebetween the occurrence of a noncompliant pattern inthe two groups was significant (p > 0.01).The sensitivity and specificity of the different
hemodynamic criteria in the diagnosis of right ven-tricular infarction is shown in table 3. When thecriterion of a close relation between RAP and PCP isused the sensitivity is 72.7% and the specificity 100%.
A severe noncompliant pattern has a sensitivity of54.5% for a specificity of 97.4%. When either of thesetwo criteria is present, a high sensitivity (81.8%) andspecificity (97.4%) can be achieved.
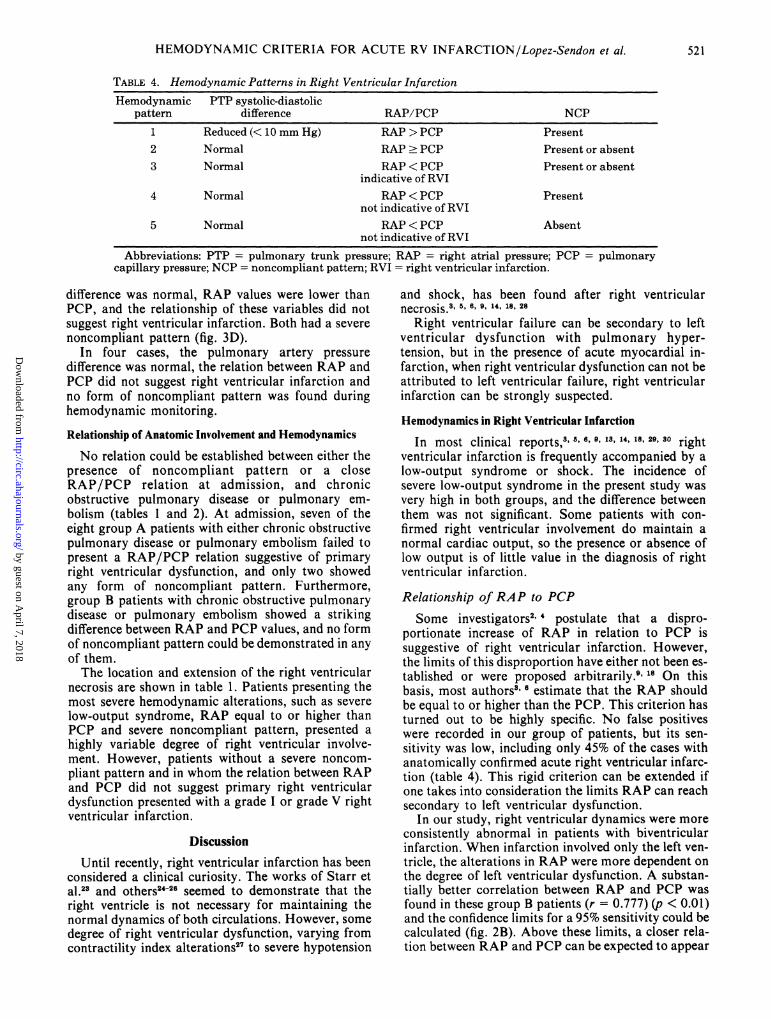
Hemodynamic Patterns
Several hemodynamic patterns could be clearlydifferentiated in group A patients, considering thedifference between systolic and diastolic pressures inthe pulmonary artery, RAP/PCP relation and pres-ence of the noncompliant pattern (table 4):
In three cases, the difference between systolic anddiastolic pressure in the pulmonary artery was reduced(< 10 mm Hg), RAP was higher than PCP, and asevere noncompliant pattern was present (fig. 3A).
In seven cases, the pulmonary artery pressuredifference was normal and RAP was equal to orhigher than PCP (fig. 3B). In three patients the non-compliant pattern was severe and in three it was mild.
In six patients, the pulmonary artery pressuredifference was normal and RAP was lower than PCP,but the relation between these measurements indicatedright ventricular infarction, exceeding the limits foundin patients without right ventricular involvement (fig.3C). Four of the patients had a severe noncompliantpattern.
In two patients, the pulmonary artery pressure
TABLE 3. Hemodynamic Criteria for the Diagnosis of Acute Right Ventricular Infarction
Sensitivity Specificity95% confidence 95% confidence
Hemodynamics Value limits Value limitsRAP - PCP according
to fig. 2B limits 72.7% 49.8-89.3% 100% 90.7-100%Severe NCP 54.5% 32.2-75.6% 97.4% 86.2- 99.9%RAP - PCP according to
fig. 2B limits, or severe NCP 81.8% 59.7-94.8% 97.4% 86.2- 99.9%RAP >; PCP3,6* 45.5% 24.4-67.8% 100% 90.7-100%RAP> 10 mm Hg andRAP 5>PCP or 1-5 mm Hg <PCP18* 72.7% 49.8-89.3% 100% 90.7-100%*Criteria proposed in the literature.Abbreviations: RAP = right atrial pressure; PCP = pulmonary capillary pressure; NCP = noncompliant
pattern.
520 CIRCULATION
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from
HEMODYNAMIC CRITERIA FOR ACUTE RV INFARCTION/Lopez-Sendon et al.
TABLE 4. Hemodynamic Patterns in Right Ventricular Infarction
Hemodynamic PTP systolic-diastolicpattern difference RAP/PCP NCP
1 Reduced (< 10 mm Hg) RAP > PCP Present2 Normal RAP > PCP Present or absent3 Normal RAP < PCP Present or absent
indicative of RVI4 Normal RAP < PCP Present
not indicative of RVI5 Normal RAP < PCP Absent
not indicative of RVIAbbreviations: PTP = pulmonary trunk pressure; RAP = right atrial pressure; PCP = pulmonary
capillary pressure; NCP = noncompliant pattern; RVI = right ventricular infarction.
difference was normal, RAP values were lower thanPCP, and the relationship of these variables did notsuggest right ventricular infarction. Both had a severenoncompliant pattern (fig. 3D).
In four cases, the pulmonary artery pressuredifference was normal, the relation between RAP andPCP did not suggest right ventricular infarction andno form of noncompliant pattern was found duringhemodynamic monitoring.
Relationship of Anatomic Involvement and Hemodynamics
No relation could be established between either thepresence of noncompliant pattern or a closeRAP/PCP relation at admission, and chronicobstructive pulmonary disease or pulmonary em-bolism (tables 1 and 2). At admission, seven of theeight group A patients with either chronic obstructivepulmonary disease or pulmonary embolism failed topresent a RAP/PCP relation suggestive of primaryright ventricular dysfunction, and only two showedany form of noncompliant pattern. Furthermore,group B patients with chronic obstructive pulmonarydisease or pulmonary embolism showed a strikingdifference between RAP and PCP values, and no formof noncompliant pattern could be demonstrated in anyof them.The location and extension of the right ventricular
necrosis are shown in table 1. Patients presenting themost severe hemodynamic alterations, such as severelow-output syndrome, RAP equal to or higher thanPCP and severe noncompliant pattern, presented ahighly variable degree of right ventricular involve-ment. However, patients without a severe noncom-pliant pattern and in whom the relation between RAPand PCP did not suggest primary right ventriculardysfunction presented with a grade I or grade V rightventricular infarction.
DiscussionUntil recently, right ventricular infarction has been
considered a clinical curiosity. The works of Starr etal.23 and others24-26 seemed to demonstrate that theright ventricle is not necessary for maintaining thenormal dynamics of both circulations. However, somedegree of right ventricular dysfunction, varying fromcontractility index alterations27 to severe hypotension
and shock, has been found after right ventricularnecrosis.38 5 6, 9, 14, 18, 28
Right ventricular failure can be secondary to leftventricular dysfunction with pulmonary hyper-tension, but in the presence of acute myocardial in-farction, when right ventricular dysfunction can not beattributed to left ventricular failure, right ventricularinfarction can be strongly suspected.
Hemodynamics in Right Ventricular Infarction
In most clinical reports,3' 5, 6, 9, 13, 14, 18, 29, 30 rightventricular infarction is frequently accompanied by alow-output syndrome or shock. The incidence ofsevere low-output syndrome in the present study wasvery high in both groups, and the difference betweenthem was not significant. Some patients with con-firmed right ventricular involvement do maintain anormal cardiac output, so the presence or absence oflow output is of little value in the diagnosis of rightventricular infarction.
Relationship of RAP to PCP
Some investigators2 4 postulate that a dispro-portionate increase of RAP in relation to PCP issuggestive of right ventricular infarction. However,the limits of this disproportion have either not been es-tablished or were proposed arbitrarily.9' 18 On thisbasis, most authors3' 6 estimate that the RAP shouldbe equal to or higher than the PCP. This criterion hasturned out to be highly specific. No false positiveswere recorded in our group of patients, but its sen-sitivity was low, including only 45% of the cases withanatomically confirmed acute right ventricular infarc-tion (table 4). This rigid criterion can be extended ifone takes into consideration the limits RAP can reachsecondary to left ventricular dysfunction.
In our study, right ventricular dynamics were moreconsistently abnormal in patients with biventricularinfarction. When infarction involved only the left ven-tricle, the alterations in RAP were more dependent onthe degree of left ventricular dysfunction. A substan-tially better correlation between RAP and PCP wasfound in these group B patients (r = 0.777) (p < 0.01)and the confidence limits for a 95% sensitivity could becalculated (fig. 2B). Above these limits, a closer rela-tion between RAP and PCP can be expected to appear
521
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from

CIRCULATION
only in 2.5% of the patients without right ventricularinfarction. For practical purposes, RAP must begreater than PCP when PCP is below 10 mm Hg, canbe 4 mm Hg below PCP when PCP reaches 15 mmHg, may be 7 mm Hg lower than PCP when PCP ex-ceeds 20 mm Hg, and can be as much as 14 mm Hglower than PCP when PCP exceeds 30 mm Hg. Usingthese criteria, the sensitivity of diagnosis in right ven-tricular infarction reaches 73% and the specificity
VOL 64, No 3, SEPTEMBER 1981
remains 100% (table 3).In a previous report,18 we stated that for the
diagnosis of right ventricular dysfunction, factors tobe considered include an RAP above 10 mm Hg andeither greater than, equal to or 1-5 mm Hg lower thanPCP. This criterion has been proved to be accurate forthe diagnosis of acute right ventricular infarction, andno false positives have been observed in this series(table 3).
522
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from

HEMODYNAMIC CRITERIA FOR ACUTE RV INFARCTION/Lopez-Sendon et al.
Alterations in Right Ventricular Compliance
The presence of a noncompliant pattern in the rightheart with a pressure wave form in right-heart cavitiessimilar to that observed in constrictive pericarditis andrestrictive myocardiopathies has already beendescribed in right ventricular infarction, and probablyis representative of the limited expansion of thedamaged myocardium.'8 In the present study, the sen-sitivity of the severe form of noncompliant patternwas found to be 54.5%. In the course of acute myocar-dial infarction, this severe form of noncompliantpattern is a highly specific sign of right ventricular in-farction (table 4) and may be the only hemodynamicsign leading to suspicion of right ventricular involve-ment when left ventricular dysfunction predominates,in which case a close relation between RAP and PCPwould be no longer evident.When either of the two criteria is present, a close
relation between RAP and PCP or a severe non-compliant pattern, sensitivity increases to 81.8% andspecificity remains close to 100% (table 3). Some casesare nevertheless overlooked because all the proposedcriteria refer to ischemic right ventricular dys-function, a condition that may be absent in somepatients with right ventricular infarction. One mustconsider that the patients we studied were by defini-tion (autopsy) particularly ill; therefore, more surviv-ing patients would present a less significant degree ofright ventricular dysfunction,"9 and in these samepatients the sensitivity of the proposed criteria wouldbe lower.
Effect of StressIschemic right ventricular dysfunction can some-
times only be manifest under cardiac interventionssuch as epinephrine administration,27 volume load-ing4 6', 18' 27 or rapid atrial pacing.27 According to thediagnostic criteria herein proposed, only six (27.3%)group A patients showed an RAP/PCP relationshipindicative of right ventricular infarction at the firsthemodynamic evaluation. Three stress conditionshave proved to be of great value in demonstratingright ventricular dysfunction clearly not secondary toleft ventricular failure (table 1).
Volume LoadingIn six group A patients, a close relation between
RAP and PCP indicative of right ventricular infarc-tion was observed only after dextran administration.In three patients, a noncompliant pattern was alsoobserved in these same conditions. Volume loading is
especially interesting in patients with low RAP andPCP values, because in this situation in both groups ofpatients the relationship between these two measure-ments is similar (fig. 2B).
Left Ventricular FailureIn two group A patients with left ventricular dys-
function and passive pulmonary hypertension, thesevere form of noncompliant pattern was observedonly with aggravation of left ventricular failure. Onlyone similar case in the absence of right ventricular in-volvement was found in group B. On the other hand,when left ventricular failure was present, a closer rela-tion between RAP and PCP was always observed inboth groups after the administration of i.v. vaso-dilators or diuretics with the consequent reduction ofPCP values. That is, while producing a severe non-compliant pattern, a close relation between RAP andPCP is prevented by the development of pulmonarycapillary hypertension.
Bradycardia
Bradycardia is an interesting spontaneous stresssituation in right ventricular infarction. Probably, lowheart rate acutely aggravates right ventricularischemia in patients with a critical obstructive lesionof the right coronary artery, producing an acute reduc-tion in right ventricular contractility and compliance.Bradycardia is poorly tolerated in patients with rightventricular infarction and decreased compliance, anda significant decrease in cardiac output may beobserved, perhaps as the result of an ineffective Frank-Starling mechanism. A close relation between RAPand PCP or a severe noncompliant pattern wasobserved only during low heart rates in three patientsfrom group A. In group B, bradycardia was followedby neither of these two hemodynamic patterns, exceptin one patient presenting a severe right coronaryartery stenosis, in whom a mild form of non-compliant pattern appeared at low heart rates (50beats/min).
Hemodynamic Patterns
In this study, a wide hemodynamic profile wasobserved, and several hemodynamic patterns could bedistinguished in biventricular infarction. The pres-ence of one or the other is probably related to therelative degree of right and left ventricular dysfunctionin each patient (table 4).
In the most severe form of dysfunction, the rightventricle practically does not generate pressure, as in-dicated by a reduced difference between the systolic
FIGURE 3. Hemodynamic patterns in acute right ventricular infarction. (A) Type 1. Pulmonary trunkpressure (PTP) is reduced, right atrial pressure (RAP) is higher than pulmonary capillary pressure (PCP)and severe noncompliant pattern is present. (B) Type 2. The PTP difference is normal and RAP exceedsPCP. In this patient, a severe noncompliant pattern is present. (C) Type 3. PTP difference is normal, andRAP is slightly lower than PCP. In this patient, the noncompliant pattern is absent. (D) Type 4. PCP ishigher than RAP and a severe noncompliant pattern is the only finding to suspect right ventricular infarc-tion.
523
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 64, No 3, SEPTEMBER 1981
and diastolic pulmonary pressures. RAP is higherthan PCP and closely resembles pulmonary trunkpressure. In this situation, low-output syndrome andsevere noncompliant pattern are invariably present,and' the RAP is higher than PCP3 (fig. 3A).
In the more common and perhaps characteristicpattern, the right ventricle generates pressure with anormal difference between systolic and diastolicpulmonary pressures, and RAP equals or exceedsPCP (fig. 3B). In these patients, low-output syndromeand noncompliant pattern are very common.Some patients show an RAP slightly below the PCP
for which many authors8 6 have chosen to exclude thediagnosis of right ventricular infarction (fig. 3C).However, the relation between these two measure-ments is suggestive of right ventricular infarction ac-cording to the limits' presented in this study.
In some patients, the diagnosis of right ventricularinfarction is only supported by the presence of a non-compliant pattern (fig. 3D). In th-ese patients, the closerelation between RAP and PCP characteristic ofischemic right ventricular dysfunction is lost, probablybecause the dysfunction of the left ventricle is moresevere than that of the right ventricle.Another pattern occurs, particularly when right
ventricular necrosis is small (grade I) or involves onlythe anterior wall of the right ventricle (grade V). Inthis situation, primary right ventricular dysfunction isabsent, and the hemodynamic diagnosis of right ven-tricular infarction is impossible. This situation isprobably more frequent in survivors"9 and thediagnosis of right ventricular involvement may be oflittle practical importance.
Relation Between Anatomic Involvement and Hemodynamics
No definite conclusions can be drawn as to therelation between the extent of right ventricularnecrosis and the functional impairment, because aprecise quantification of right ventricular necrosis wasnot made; the classification proposed by Isner andRoberts21 is only semiquantitative and does not takeinto account the necrosis extent from apex to base. Webelieve that severe right ventricular dysfunction maycoexist with variable degrees of right ventricular in-volvement. Conversely, all patients with normal rightventricular function had a small right ventricular in-farction. Right ventricular ischemia may have con-tributed to the functional impairment in patients withgrade I right ventricular infarction, and the involve-ment of the anterior wall of the right ventricle has lit-tle significance in right ventricular dynamics.
Differential Diagnosis
The specificity for biventricular infarction using anyof the aforementioned criteria found in the literature is
very high (table 3). However, the diagnosis is basedupon predominant right ventricular dysfunction,which is not pathognomonic for this condition, andmust only be reached once other causes of right ven-tricular failure, such as pulmonary embolism, chronic
obstructive pulmonary disease, interventricular septalrupture or cardiac tamponade, have been ruled out.Chronic obstructive pulmonary disease or
pulmonary embolism can produce right ventriculardysfunction, so s'ome authors have excluded patientswith this condition in the diagnosis of right ventricularinfarction. However, for RAP to increase, severepulmonary hypertension must be present, a situationin which a gradient between diastolic pulmonarypressure and PCP would be noticeable..'A severe noncompliant pattern, on the other hand,
has been described in myocardiopathy, constrictivepericarditis,32 after right ventriculotomy,33 in cases ofsevere tricuspid regurgitation,3' and in valvular heartdisease with atrial fibrillation.3' It is always absent incardiac tamponade.32
In the' present study, a severe intermittent noncom-pliant pattern was found in a patient without rightventricular involvement. In this patient, who presentedwith severe pulmonary hypertension secondary to leftventricular failure, an aneurysm of the inter-ventricular septum that almost completely obliteratedthe right ventricular cavity was found at necropsy. It isreasonable to suppose that during maximal left ven-tricular filling pressure elevation, the right ventricularcavity became nearly occluded, leading to a situationof severe impairment of right ventricular compliance.To our knowledge, no similar case has been reported,but such a cause of noncompliant pattern must betaken into account when considering the differentialdiagnosis of right ventricular infarction in the pres-ence of severe left ventricular failure.
AcknowledgmentWe gratefully acknowledge the assistance of Jorge Seoane, M.D.,
from the Internal Medicine Department, Ciudad Sanitaria La Paz,Madrid, Espania, in performing the statistical analysis. We are alsograteful to the nursing staff of the Coronary Care Unit for theircollaboration in the care of the patients.
References1. AI-Sadir J, Falicov R, Zahavi I, Brooks M, Resnekov L: Right
ventricular dysfunction in acute inferior myocardial infarction.(abstr) Circulation 48 (suppl lV): IV-59, 1973
2. Gomez G, Fresch D, Grismer J: Hemodynamic and echo-cardiographic correlation of right ventricular dysfunction inacute myocardial infarction. (abstr) Clin Res 21: 420, 1973
3. Cohn JN, Guiha NH, Broder M, Limas C: Right ventricular in-farction. Am J Cardiol 33: 209, 1974
4. Rackley CE, Russell RO: Right ventricular function in acutemyocardial infarction. Am J Cardiol 33: 927, 1974
5. Rotman M, Ratliff NB, Hanley J: Right ventricular infarction:a hemodynamic diagnosis. Br Heart J 36: 941, 1974
6. Rigo P, Murray M, Taylor DR, Weisfeldt ML, Kelly DT,Strauss HW, Pitt B: Right ventricular dysfunction detected bygated scintiphotography in patients with acute inferior myocar-dial infarction. Circulation 52: 268, 1975
7. Zone DD, Bot RE: Right ventricular infarction with tricuspidinsufficiency and chronic right heart failure. Am J Cardiol 37:445, 1976
8. Pitt B, Strauss HW: Myocardial perfusion imaging and gatedcardiac blood pool scanning. Clinical application. Am J Cardiol37: 445, 1976
9. Daubert JD, Deplace C, Bourdonnec C, Pony JC, Gouffault J:
524 CIRCULATION
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from

HEMODYNAMIC CRITERIA FOR ACUTE RV INFARCTION/Lopez-Sendon et al.
L'infarctus du ventriciile droit. 1. Diagnostic hemody-namique-correlations anatomiques. Arch Mal Coeur 70: 243,1977
10. Marcus ML, Kerber RE: Present status of the 99g technetiumpyrophosphate infarct scintigram. Circulation 56: 335, 1977
11. Raabe DS, Chester AC: Right ventricular infarction. Chest 73:96, 1978
12. Sharpe N, Botvinick E, Shames DM, Schiller NB, Massie BM,Chatterjee K, Parmley WW: The noninvasive diagnosis of rightventricular infarction. Circulation 57: 483, 1978
13. Lorell B, Leinbach RC, Pohost GM, Gold HK, Dinsmore RE,Hutter AM, Pastore JO, DeSanctis RW: Right ventricular in-farction. Clinical diagnosis and differentiation from cardiactamponade and pericardial constriction. Am J Cardiol 43: 456,1979
14. Coma-Canella I, Lopez-Send6n J, Gamallo C: Low output syn-drome in right ventricular infarction. Am Heart J 98: 613, 1979
15. Coma-Canella I, Lopez-Sendon J: Infarto de ventriculoderecho. Rev Esp Cardiol 32: 287, 1979
16. Cohn JN: Right ventricular infarction revisited. Am J Cardiol43: 666, 1979
17. Botvinick EM, Shames DM: Nuclear Cardiology. ClinicalApplications. Baltimore, Williams and Wilkins, 1979, pp 100,143
18. Coma-Canella 1, Lopez-Send6n J: Ventricular compliance inischemic right ventricular dysfunction. Am J Cardiol 45: 555,1980
19. Wackers FJT, Lie KI, Sokole EB, Res J, van der Schoot IB,Durrer D: Prevalence of right ventricular involvement in in-ferior wall infarction assessed with myocardial imaging withthallium 201 and technetium-99m pyrophosphate. Am J Car-diol 42: 358, 1978
20. Ahmad M, Dubiel JP, Logan KW, Verdon TA, Martin RH:Limited clinical diagnostic specificity of technetium 99m stan-nous pyrophosphate myocardial imaging in acute myocardialinfarction. Am J Cardiol 39: 50, 1977
21. Isner JM, Roberts WC: Right ventricular infarction complicat-ing left ventricular infarction secondary to coronary heart dis-ease. Am J Cardiol 42: 885, 1978
22. Lie JT, Pairolero PC, Holley KE, Titus JL: Macroscopicenzyme-mapping verification of large homogeneous experimen-tal myocardial infaretus of predictable size and localization indogs. J Thorac Cardiovasc Surg 69: 599, 1975
23. Starr J, Jeffers WA, Meade RH: The absence of conspicuousincrements of venous pressure after severe damage to the rightventricle in the dog with a discussion of the relationship betweenclinical congestive failure and heart disease. Am Heart J 26:291, 1943
24. Bakos AC: The question of the function of the right ventricularmyocardium: an experimental study. Circulation 1: 724, 1943
25. Rodbard S, Wagner D: By-passing the right ventricle. Proc SocExp Biol Med 71: 69, 1949
26. Kagan A: Dynamic responses of the right ventricle followingextensive damage by cauterization. Circulation 5: 816, 1952
27. Brooks H, Al-Sadir J, Schwartz J, Rich B, Harper P, Res-nekov L: Biventricular dynamics during quantitated anterosep-tal infarction in the porcine heart. Am J Cardiol 36: 765, 1975
28. Guiha NH, Limas C, Cohn JN: Predominant right ventriculardysfunction after right ventricular destruction in the dog. Am JCardiol 33: 254, 1974
29. Jensen DP, Goolsby JP, Oliva PB: Hemodynamic patternresembling pericardial constriction after acute inferior myocar-dial infarction with right ventricular infarction. Am J Cardiol42: 858, 1978
30. Ratliff NB, Hackel DB: Combined right and left ventricular in-farction: pathogenesis and clinico-pathologic correlations. AmJ Cardiol 45: 217, 1980
31. McIntyre RM, Sasahara A: Respuesta ventricular y hemo-dinamica al embolismo pulmonar. Prog Enf Cardiovasc 15:239, 1975
32. Shabetai R, Fowler NO, Guntheroth WG: The hemodynamicsof cardiac tamponade and constrictive pericarditis. Am J Car-diol 26: 480, 1970
33. Kirklin JW, Rarp RB: The Tetralogy of Fallot, from a SurgicalPoint of View. Philadelphia, WB Saunders, 1970
34. Cairns KB, Kloster FE, Bristow JD, Lees MH, Griswold HE:Problems in the hemodynamic diagnosis of tricuspid insufficien-cy. Am Heart J 75: 173, 1968
525
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from

J Lopez-Sendon, I Coma-Canella and C Gamalloventricular infarction.
Sensitivity and specificity of hemodynamic criteria in the diagnosis of acute right
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1981 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.64.3.515
1981;64:515-525Circulation.
http://circ.ahajournals.org/content/64/3/515the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on April 7, 2018
http://circ.ahajournals.org/D
ownloaded from