Seminar Pedo Ppt
98
-
Upload
siti-mutia-chairunnissa-dipawinangun -
Category
Documents
-
view
238 -
download
0
Transcript of Seminar Pedo Ppt


To give you important and useful information regarding swallowing
and speech


SPEAKER #1KIKI


a series of coordinated muscular contraction that moves a bolus of food from oral cavity through the esophagus to the stomach
Okeson, 2008



1.Degrees of fineness of the food
2.Intensity of the taste extracted
3.Degree of lubrication of the bolus
Practice : To appreciate the mechanism of masseter muscleStep : 1. Patient’s position: sit up straight 2. Clinicians: prependicular 3. Ask the patient to swallowing the saliva 4. Please stay attention to the symmetry ofResult: Muscle function (+) Symmetry Muscle function (-) Asymmetry

ConclusionFrom now on, please getting information of patient’s swallowing.
SPEAKER #2MEITY

What Are They?Clinical Examination

Medilexocon.com
• Somatic Swallow:swallowing pattern with muscular contractions and uses the teeth for mandibular stability that appear to be under control of the person
• Visceral Swallow:immature swallowing pattern of an infant or older person with tongue thrust, resembling peristaltic, and wavelike

What Are They?
Clinical Examination

• Ask your patients to swallow her/his saliva, if there’s no tongue trust SOMATIC SWALLOW
• Ask your patients to swallow her/his saliva, if there’s tongue trust VISCERAL SWALLOW

Highlight:As a clinician, we must know what type of swallowing our patient has.

SPEAKER #3NATASHA
EXPLORATION
THE IMPORTANCE

Swallowing patterns evolve as a changes adapted in the form of food, an increase in activity of muscle mastication, and the first molar tooth eruption.
Pinkham, 1999

The transition generally occurs in children aged 3-10 years.
Normal adult swallowing pattern obtained at age 4 ½ to 5 years, so that the pattern of infantile swallowing may transition to adult swallowing pattern completely at 8 years old.
Pinkham, 1999

EXPLORATION
THE IMPORTANCE

LACK OF TOOTH SUPPORT AS A RESULT POOR TOOTH POSITION OR ARCH RELATIONSHIP MAY RESULT NO TRANSITION FROM INFANTILE SWALLOW TO ADULT SWALLOW.
Okeson, 2008

OVERRETENTION OF THE INFANTILE SWALLOW CAN RESULT IN LABIAL DISPLACEMENT OF THE ANTERIOR TEETH BY THE POWERFUL TONGUE MUSCLE.
THIS MAY PRESENT CLINICALLY AS AN ANTERIOR OPEN BITE. Okeson, 2008

EssenceAs a clinician, we should aware about the relation between occlusion and swallowing.

SPEAKER #4REVINI

The Time
The Power The Importance

Average tooth contact during swallowing is 683 msec. This is more then 3 times longer than mastication.
Okeson, 2008
The Time
The Power The Importance

The force applied the teeth during swallowing is 66.5 pounds, is 7.8 pounds more than mastication.
Okeson, 2008

The Time
The Power The Importance
When the mandible is braced, it is brought into a some what posterior or retruded position. If the teeth do not fit together well in this position, an anterior slide occurs to the intercuspal position.
Okeson, 2008

Bottom LineAs a clinician, we should know that the normal time of swallowing is less than 1 seconds.

SPEAKER #5SITI

Anatomy
The Importance

www. Crossfitsouthbay.com
Anatomy

Anatomy
The Impotance

The Importance
• the sensory input from the trigeminal nerve synapse in the spinal V nucleus
• it’s also important to appreciate that the most caudal region of the spinal tract nucleus extends inferiorly into the region where the upper cervical nerves enter the spinal cord (CN I – V)Okeson,
2008

Getting to know
The Mechanism The Factors

The Factors
• Quality of the intercuspal position will determine position mandible during swallowing, not retruded relationship with fossa.• Muscle engrams and reflex activity maintain closure of the mandible into the intercuspal position
Okeson, 2008
PRACTICE
1. Patient sit up straight and relax
2. Ask the patient to swallow3. Notice the cheek while
swallowing
To Evaluate Mastication Muscle

RESULT
- Masseter muscle pressing towards the midline and the cheek muscle should not move at all
- If left or right cheek bulging
PRACTICE

Conclusion• As the clinician, please be
familiar with mastication muscle on your patient

SPEAKER #6ELFIRA

What is it?
The Process
What is it?
Oral phase of swallowing where the tongue cups to position the food, fluid or saliva for swallowing
www.beckmannoralmotor.com

What is it?
Okeson, 2008

What is it?
The Process

The Process
• Selective parting of bolus by tongue• Bolus placed on dorsum of the tongue• Tongue pressed lightly against the hard palate• Lips are sealed, teeth brought together• Reflex contraction in the tongue, pressed bolus backward, transferred to pharynx
Okeson, 2008

PRACTICE
1. Patient sit up straight and relax
2. Ask the patient to swallow3. Notice the lips while
swallowing
To evaluate first stage of swallowing

RESULT
- Lips are sealed while swallowing
- Lips are not sealed while swallowing
PRACTICE

Bottom Line• As the clinician, please be
familiar with first stage of swallowing on your patient

SPEAKER #7NADIA

Getting to know
The Mechanism

Getting To Know
Second Stage of Deglutition : occurs when bolus reaches the area of palatoglossal folds. It is also known as the pharyngeal phase of swallowing.
www.ouhsc.edu

Second Stage of Deglutitionis under involuntary neuromuscular control which is stimulated by posterior tongue movement and stimulation of pharyngeal mucosa that stimulated the swallowing reflex.
www.ouhsc.edu
Getting To Know

Getting to know
The Mechanism

Okeson, 2008
The Mechanism

Okeson, 2008
The Mechanism

www.ouhsc.edu
The sequential steps to pharyngeal phase of swallowing are:1.Velum elevating to contact posterior pharyngeal wall and block upward movement of bolus into nasopharynx 2.Elevation of the larynx and hyoid bone toward base of tongue, bringing a passive flipping over of the epiglottis to cover the glottis 3.Contraction of pharyngeal constrictor muscles from superior to inferior direction4.Relaxation of the upper esophageal sphincter to allow passage of bolus into esophagus
The Mechanism

Practice: to appreciate any abnormalities of
second stage deglutition1. Sit up straight and relax2. Ask the patient to swallow his/
her saliva

Result:• Patient can swallow the saliva easily
and the swallowing lasts less than 2 second → NORMAL
• Patient has difficulty in swallowing and it lasts longer than 2 second → SWALLOWING DISORDER

Essence:From now on, let’s start paying close attention to the way patients swallow.

SPEAKER #8RIMA

Clinical Examination

The third stage of swallowing consist of passing the bolus through the length of the esophagus and into the stomach.
Okeson, 2008
?
Clinical Examination

Peristaltic waves carry the bolus down the esophagus. The waves take 6 to 7 seconds to carry the bolus through the length of the esophagus.
Okeson, 2008
The process
Clinical Examination
Practice: to appreciate the clinical examination of
esophagus phase Lets swallowing
Result :Normal → feel no obstacle in esophagusProblem feel an obstacle in esophagus
Clinical Examination

Important point:As a clinician, please be aware if there is an obstacle while patient’s swallowing

Swallowing occurs 590 times during 24-hour•146 cycles during eating•394 cycles between meals while awake•50 cycles during sleep
Okeson, 2008
Frequency of swallowing

SPEAKER #9LULU
SPEECHPart 1: Introduction

SPEECHPart 1: Introduction
Speech is the third major function of the masticatory system and occurs when a volume of air is forced from the lungs by the diaphragm through the larynx and oral cavity.
Okeson, 2008
What is it ?

SPEECHPart 1: Introduction

Controlled contraction and relaxation of the vocal cords create a sound with the desired pitch
Okeson, 2008
The Importance

SPEECHPart 1: Introduction

The HumanHuman have ability to form
intricate sound using vowels and consonantsThe Animal
Animal don’t have ability to produce as many as distinguishable sounds because of simpler anatomy
The Difference
www.linkedin.com
Bottom Line:As a clinician, please be aware about articulation speech of the patient

SPEAKER #10NINASPEECH
Part 2: Articulation of Sound (I)

The importance Assorted Sound
SPEECHPart 2: Articulation of Sound
(I)
By varying the relationship of the lips and the tongue to the palate and teeth, one can produce a variety of sounds. Okeson,
2008

The importance Assorted Sound
SPEECHPart 2: Articulation of Sound
(I)

OKESON, 2008

As a clinician, we should be aware if the patient can’t spell obviously

SPEAKER #11ERWINA
SPEECHPart 3: Articulation of Sound
(II)

The importance The Mechanism
SPEECHPart 3: Articulation of Sound
(II)

A combination of the anatomic structures can also be use to form many of these sounds.
Okeson, 2008

The importance The Mechanism
SPEECHPart 3: Articulation of Sound
(II)

• The tongue touches the maxillary th sound.
• The lower lip touches the incisal edges of the maxillary teeth f and v sounds.
• The posterior portion of the tongue rises to touch the soft palate k or g
The MechanismThe Mechanism
calleteach.wordpress.com

Important point:As a clinician we should aware about combination of the anatomic structures that use to form many of these sounds.

SPEAKER #12DINAR
SPEECHPart 4: The Role of Occlusion

SPEECHPart 4: The Role of Occlusion

Okeson, 2008
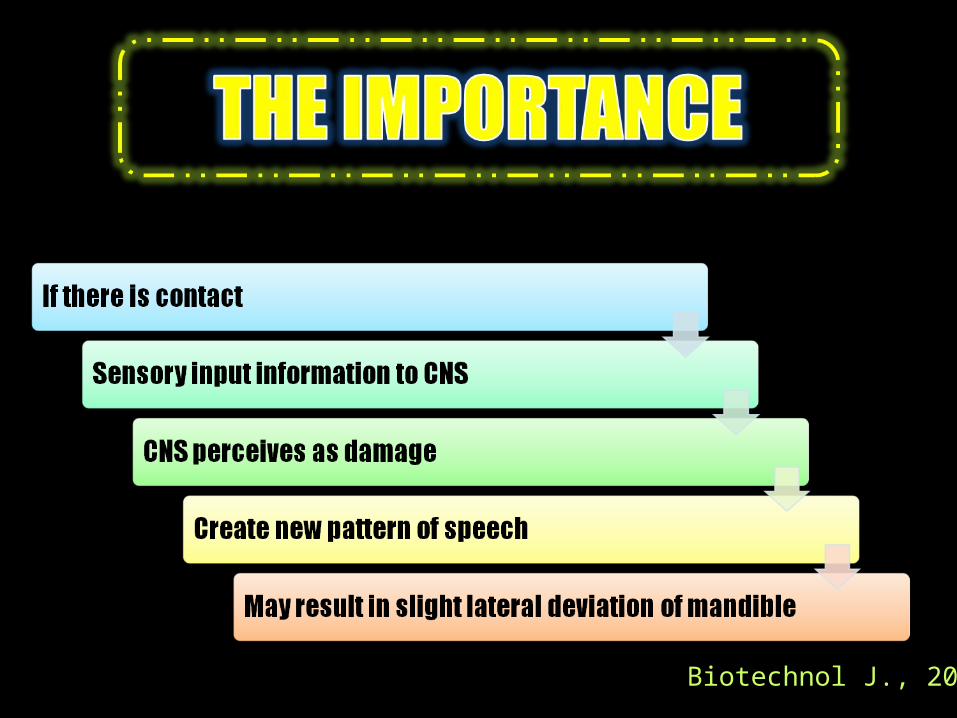
Biotechnol J., 2006
HighlightAs a clinician, we should give advice to our patient/parent to keep their teeth healthy.