
Selective Leuco-depletion of Blood Products Dr. Sangeeta Pathak Sr. Consultant & Head-Blood Bank.
32
Selective Leuco- depletion of Blood Products Dr. Sangeeta Pathak Sr. Consultant & Head-Blood Bank
-
Upload
dylan-gravely -
Category
Documents
-
view
214 -
download
0
Transcript of Selective Leuco-depletion of Blood Products Dr. Sangeeta Pathak Sr. Consultant & Head-Blood Bank.

Selective Leuco-depletion of Blood Products
Dr. Sangeeta PathakSr. Consultant & Head-Blood
Bank

Whether all cellular components should have their white cells reduced
in number remains controversial*
*Vamvakas EC. White blood cell containing allogeneic blood transfusion, postoperative infection & mortality: A meta analysis of observational “before & after” studies. Vox Sang 2004;86:111-19

Objective
In which circumstances would you recommend/not recommend the use of leucocyte depleted blood products?– Able to answer the question regarding
leucocyte depleted blood products.– Finances!

Definition
Leucocyte depleted blood products must contain
<0.5x109 leucocytes per unit red cells or adult therapeutic
dose of platelets.

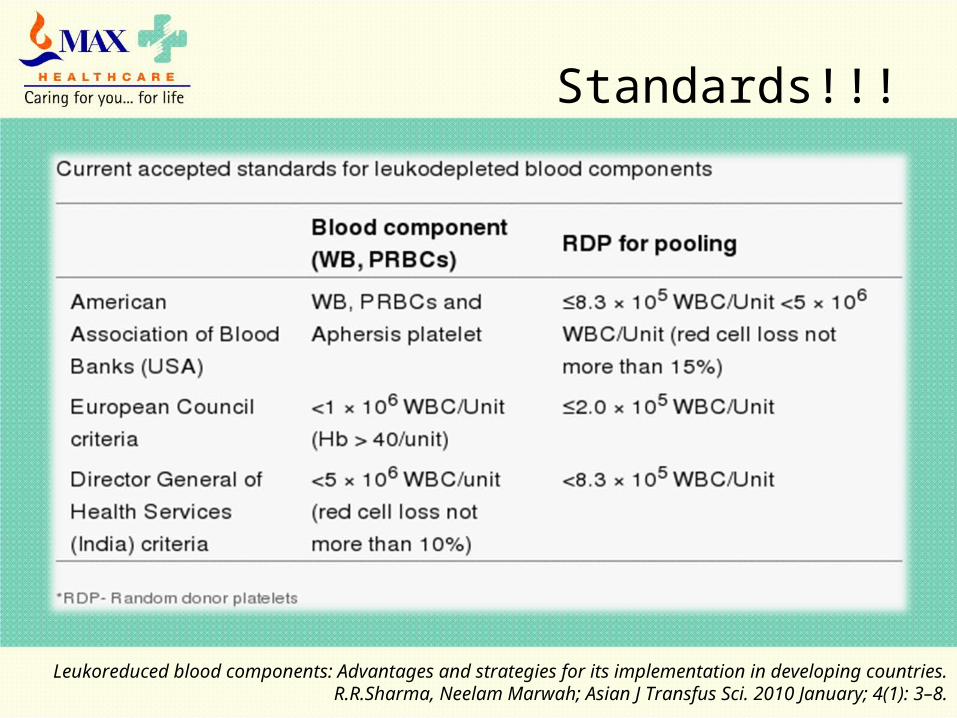
Keeping in view the variability of leukocyte numbers in the component and the leuko-reduction method, the leukocyte content in a blood component unit should be less than 5 × 106/unit after leuko-reduction (3 log reduction 99.9%) with a minimum of 85% red cell recovery in 95% of the units tested, as per the standards of the American Association of Blood Banks.
The European council guidelines are a little more stringent in terms of residual leukocyte content and require it to be less than 1 × 106/unit.
The Numbers!!!!
Leukoreduced blood components: Advantages and strategies for its implementation in developing countries. R.R.Sharma, Neelam Marwah; Asian J Transfus Sci. 2010 January; 4(1): 3–8.

Current Scenario Worldwide…
http://ijtm.in/view_article.php?id=14
In recent years BCT has witnessed opposing trends in the area of Leuco-depletion
– Forced implementation
• National Blood Services:
– UK National Blood Service
– American Red Cross

• Nearly all of Europe & Canada have implemented leucocyte reduction in all cellular component - termed Universal leucocyte reduction
• It has not been mandated by the FDA in the United State & the most recent survey data indicate that –– 72% of red cells – 40% of whole derived platelet– Nearly all apheresis plateletare leucocyte reduced*.
*US Department of Health and Human Services. The 2007 National Blood Collection and Utilization Survey Report. Washington, DC:DHHS, 2008

• Oct 2000, the University Health Consortium concluded that the available evidence was insufficient to recommend universal leucocyte reduction.
• In contrast, the US Blood Safety & Availability Committee recommended in Jan 2001 that universal leucocyte reduction be implemented as “soon as feasible”.
• Adoption of universal leucocyte reduction remains a hotly debated topic*.
*Vamvakas EC, Blajchman MA. Universal WBC reduction: The case for and against. Transfusion 2001;41:691 - 712

In developing countries like India, cost is the major hurdle for use of universal leuco-depletion of blood products and its usage thus remains controversial and limited !!!
Indian Scenario!!!!
http://ijtm.in/view_article.php?id=14
Leukoreduced blood components: Advantages and strategies for its implementation in developing countries. R.R.Sharma, Neelam Marwah; Asian J Transfus Sci. 2010 January; 4(1): 3–8.
Standards!!!

Practical aspects
• To achieve residual count less than specified, process should be completed with in 48 hours form collection of the donor unit.
• Quality should be assured by monitoring the components for 100% compliance.

Transfusion-transmitted pathogen associated primarily or solely with leucocyte
Pathogen Leucocyte subtype
Viruses Cytomegaloviruses Mainly monocytes
possibly small amount in granulocyte
Human T-cell T-Lymphocyteleukemia virusesI and II
Human Herpes Virus & B-Lymphocytes Epstein-Barr Virus B-Lymphocytes
BacteriaYersinia enterocolitica Granulocytes
PrionsLeucocyte involvement Unknown
Transfusion Microbiology by John A.J.Barbara Marcela Contreras

Little evidence suggests a serious clinical disadvantage of leucocytes
reduction.
Disadvantages??????
Disadvantages:
• The Technology is Expensive
• There are three documented disadvantages.
Are they there???? If any???

1st Disadvantage!!!
• Filtration results in a substantial loss of the therapeutic blood element intended for Transfusion.
• The VATS* found that patients randomly assigned to the leucocytes reduction arm received a statistically smaller mass of red cells.
• It is unclear whether this actually results in additional red cells transfusion.
*Collier AC, Kalish LA, Bush MP et al. Leucocytes reduced red cells transfusion in patients with anemia & HIV virus infection. The Viral activation transfusion study – a randomized controlled trial. JAMA 2001;285:1592-601.

1st Disadvantage!!!
• This problem may be particularly important if filtration is combined with other manipulations, such as preparation of RBC’s by the buffy coat removal technique, preparation of washed platelet concentrates, or pathogen inactivation techniques.
2nd Disadvantage!!!
• Bedside leucocytes reduction has been associated with hypotensive reactions, especially among recipients treated with ACE inhibitors*.
• As blood passes through negatively charged filters, contact activation occurs.
• The activation, in turn, causes generation of short lived vasoactive proteins such as bradykinin, leading to hypotension.
*Cyr M, Eastland T, Blais C, et al. Bradykinin metabolism and hypotensive transfusion reactions. Transfusion 2001;41:136-50

2nd Disadvantage!!!Takahashi et al.
some filters
(Associated with
production of )
Bradykinin
(during filtration of) platelet concentrate
Bradykinin increased from
37pg/mL 6794pg/mL
(if ACE inhibitor added)
36000pg/mL
(because ACE inhibitor also inhibits the kininases responsible
for the breakdown of bradykinin.) These reactions led to recommendations to use pre-storage leukocyte reduced components to eliminate this complication.

Recently, these reactions were reported in a patient taking ACE inhibitor, despite the fact that the Blood was pre-storage leucocyte reduced; an inherited defect in kinin metabolism was suspected*.
1. Patient taking ACE inhibitor and 2. Patients with inherited deficiencies of kininases
more susceptible to the hypotensive effects of administered bradykinin.
2nd Disadvantage!!!
*Arnold DM, Molinaro G, Warkentin TE, et al. Hypotensive transfusions reactions can occur with blood products that are leukoreduction before storage. Transfusion 2004;44:1361-6.
3rd Disadvantage!!!
Reports of allergic reactions characterized by
– acute conjunctivitis,
– Pain at the site of blood infusion*, or
– Sudden onset of pain and
– Hypertension**
have been observed in some patients undergoing transfusion of LR blood.
*Podlosky LR, Boskov LK. Infusion site pain related to bedside leucoreduction filters(letter). Transfusion 1995;35:362
**Haley NR, Sledge LS, Gibble J, et al. an unusual transfusion reaction pattern to leucocyte reduced red cells. Transfusion 2000;40(suppl):40s

3rd Disadvantage!!!
• Although these events appear to occur in a very small proportion of patients who undergo transfusion.
• The study highlight that even low-frequency adverse consequences attributed to leucocyte filtration will affect growing numbers of patients as the technology becomes more widely used.

Disadvantage – Cost!!!
The major argument against leucodepletion is the cost of white cell removal.
Leucocyte depletion adds a significant cost to each transfusion episode.
Buffy coat removal costs approximately $2 per unit whilst second and third generation filters cost between $15-$60 per RCC or platelet transfusion.
Thus leucodepletion must be shown to be cost effective.
This means that their influence on patient clinical outcome must be shown to be of sufficient benefit to warrant the cost of treating all eligible patients within defined categories.
Not useful in…
a) Fresh frozen plasma (FFP) and cryoprecipitate transfusion - as these blood components are prepared with least cellular contamination and hence do not require leucodepletion.
b) Prevention of transfusion associated graft versus host disease (TAGVHD) - Gamma irradiation is the method of choice for prevention of TAGVHD.
c) Transfusion associated acute lung injury (TRALI) - is due to the leucocyte antibodies present in donor plasma and leucodepletion is not useful in prevention of TRALI.
http://ijtm.in/view_article.php?id=14

Future Evaluation
The role of leucodepletion is a complex one and its ultimate place in transfusion is yet to be determined.
Health care professionals now have a responsibility to ensure that new modalities of treatment produce a clearly definable benefit to the patients in whom they are used.
Cost is but one factor that must be assessed, but it is no longer appropriate to recommend new and expensive techniques such as leucodepletion without well documented evidence of its efficacy.
Future Evaluation
This approach has been recently affirmed by the Royal College of Physicians of Edinburgh who held a consensus conference on leucodepletion.
There is likely to be a considerable amount of information published on this topic over the next few years and the role of leucodepletion will need to be regularly reassessed in the light of results from the relevant clinical trials.

Study!!!
• Using an analytical decision model a cost-effectiveness analysis was conducted in a Hospital in Queensland in 2007.
• This study has concluded that cost effectiveness is not an influential factor in policy decision regarding quality and safety initiatives in the Australian Blood sector.
• The same hospital implemented Universal Leucodepletion in 2008.

• A prospective RCT of leucocyte reduction in a major academic medical centre failed to demonstrate a difference in in-hospital mortality, hospital length of stay, or other secondary outcomes*.
• Other RCTs in HIV-infected patients** and trauma patient *** failed to show a benefit in patient outcomes.
• A “before & after” study of the effects of adopting universal leucoreduction in Canada reported that the unadjusted hospital mortality rates declined from 7.03% to 6.19% (p<0.04)****
*Dzik S, Anderson JK, O’Neill M, et al. A prospective, randomized clinical trail of universal WBC reduction. Transfusion 2002;42:1114-22.
**Collier AC, Kalish LA, Busch MP, et al. Leucocyte-reduced red blood cell transfusions in patients with anemia and human immunodeficiency virus infection: The viral activation transfusion study-a randomized controlled
trial. JAMA 2001;285:1592-601.***Nathens AB, Nester TA, Rubenfeld GD, et al. The effcts of leucoreduced blood transfusion on risk following
injury: A randomized controlled trial. Shock 2006;26:342-7.****Hebert PC, Fergusson D, Blajchman MA, et al. Clinical Outcomes following institution of the Canadian
universal leucoreduction program for red cells transfusions. JAMA 2003;289:1941-9

• There was no difference in serious nosocomial infections, although post-transfusion fevers and antibiotic use did decrease.
• A similar analysis of Canadian data in premature neonates found no difference in primary outcomes: nosocomial bacteremia and neonatal intensive care unit mortality*. Improvement in some secondary clinical outcomes were reported.
• These two studies must be interpreted with caution, however, because of their retrospective design and potential bias from confounders.
*Fergusson D, Hebert PC, Lee SK, et al. Clinical outcomes following institutions of universal leucoreduction of blood transfusions for premature infants. JAMA 2003;289:19560-6
• When viewed in the context of the negative RCTs noted above, adoption of universal leucocyte reduction cannot be justified on the basis of available scientific evidence.
Other considerations such as• logistics, • public policy, • public perception and • mechanisms for funding leucocyte reduction all play a role in making a final decision regarding
adoption of universal leucocyte reduction.
Deterrents !!!
• High cost to blood services and hospitals. • Increase space requirements.• Equipments to be purchased. • More staff to be recruited and trained.
Universal leucodepletion: Cost/Benefit Analysis; Marcela Contreras Gac Méd Méx Vol. 140, Suplemento No. 3, 2004

References!!!
• ROSSI’S – Principles of Transfusion Medicine IVth Edition, Leucocytes-reduced blood components, 2009;16:242-3
• AABB Technical Manual – 16th Edition, Hemotherapy Decisions and their Outcomes, 2008;20:576-6



















