
Selective Dorsal Rhizotomy Manchester dosal rhizotomy mr andrew... · • Another diagnosis with...
5
1 Selective Dorsal Rhizotomy Andrew Roberts - Oswestry 9 th May 2012 Brain Injury Increased Tone Abnormal Posture Contracture Bony Deformity Birth Maturity Brain Injury Increased Tone Abnormal Posture Contracture Bony Deformity Birth Maturity SDR Physiotherapy ITB Orthopaedics SDR Only Reduces Spasticity Quantum of Benefit ∝ Extent & Severity of Spasticity What’s the Objective? • Spasticity • Discomfort • Contracture • Surgery • QoL • Walking
Transcript of Selective Dorsal Rhizotomy Manchester dosal rhizotomy mr andrew... · • Another diagnosis with...

1
Selective Dorsal Rhizotomy
Andrew Roberts - Oswestry
9th May 2012
Brain Injury
Increased Tone
Abnormal Posture
Contracture
Bony Deformity
Birth Maturity
Brain Injury
Increased Tone
Abnormal Posture
Contracture
Bony Deformity
Birth MaturityS
DR
Ph
ysio
thera
py
ITB
Orth
opae
dic
s
SDR Only Reduces Spasticity
Quantum of Benefit ∝∝∝∝ Extent & Severity of Spasticity
What’s the Objective?
• ���� Spasticity
• �Discomfort
• �Contracture
• � Surgery
• �QoL
• �Walking

2
Selection Criteria – Cole et al 2007
The Good
• Insufficient intensity of spasticity
• Insufficient extent of spasticity
The Bad
• Insufficient selective motor control
• Insufficient extensor strength
• Insufficient potential for rehabilitation
• Too heavy
• Too late to usefully alter evolving disability
The Ugly
• Dystonia
• Ataxia
• Not CP
– HSP
– Neuro metabolic disorders
Good
Ugly
Bad
17
1
513
441
The Mix

3
ControlImpaired
Too Deformed
Too Weak
1
7
3
4*20
The Bad (n = 50)
13
8Too Old
Uncooperative
*
The Ugly
Don’t Offer SDR to…
• Too good to benefit
• Another impairment that would limit improvement
• Another diagnosis with neurology other
than pure spasticity
• Those not selected were not “failures” –
they just needed something else.
Pathway (1 of 2)
• Referral
• Clinical Assessment– Physiotherapy
– Orthopaedic
– Neurology
• Gait assessment– Kinematics
– EMG
– Energy consumption
Pathway (2 of 2)
• Functional assessment– SATCo
– GMFCS
• Orthopaedic Imaging– L Spine
– Hips
• Neuro Imaging– Brain
– Whole spine

4
Outcome Assessments
• Spasticity
• Weight across centiles
• MRC Strength
• Degrees of contracture
• Walking Speed M/S
• Energy consumption Ml/Kg/M
• Physiological Cost Index Extra Beats/M
• Gillette Gait Index
• Gross motor Function Measure
Weight Change After SDR
100
0
10
20
30
40
50
60
70
80
90
Speed =
0.17
Speed =
0.24
Speed =
0.27
Speed =
0.28
Speed =
0.47
Speed =
0.65
Speed =
0.67
Speed =
0.72
Speed =
0.72
Speed =
0.91
Speed =
0.96
Speed =
0.99
Speed =
1.12
Weight
(Centiles) G
ain
Lo
ss
Scoliosis After SDREpidural Obliteration
Long Term Issues
• Walking
• Sexual function
• Comfort
• Orthopaedic Surgery
5
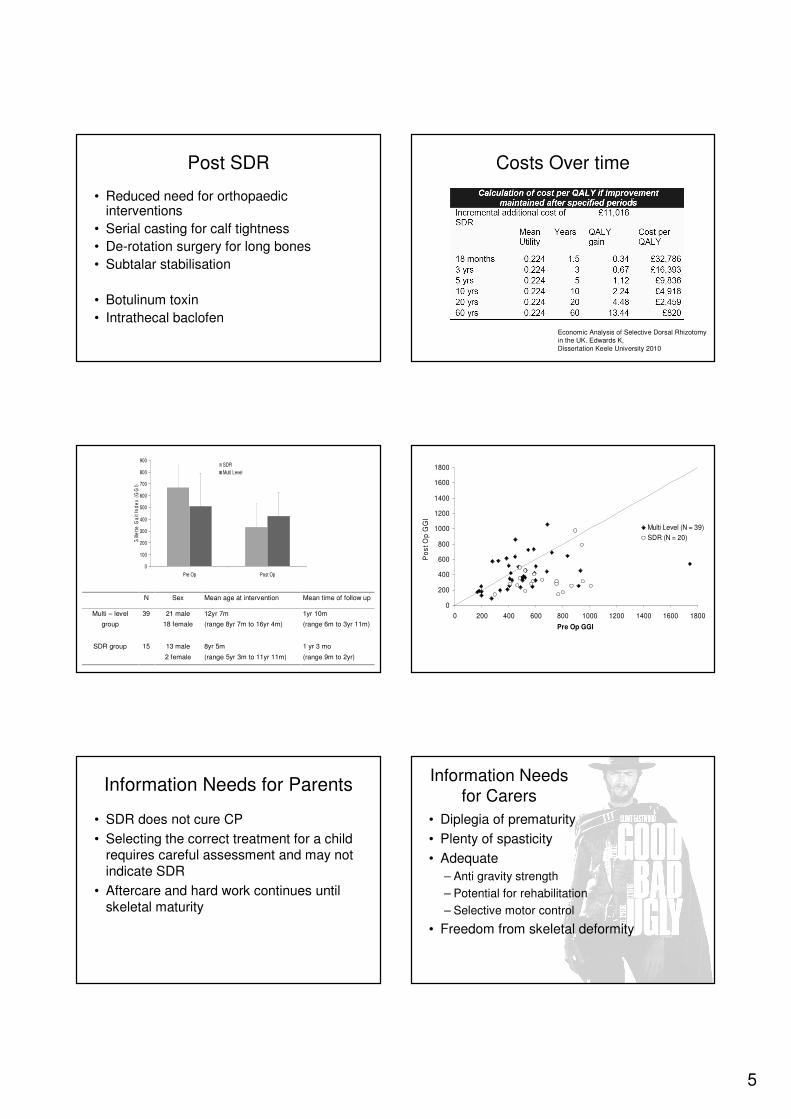
Post SDR
• Reduced need for orthopaedic interventions
• Serial casting for calf tightness
• De-rotation surgery for long bones
• Subtalar stabilisation
• Botulinum toxin
• Intrathecal baclofen
Costs Over time
Economic Analysis of Selective Dorsal Rhizotomy
in the UK. Edwards K,
Dissertation Keele University 2010
N Sex Mean age at intervention Mean time of follow up
Multi – level
group
39 21 male
18 female
12yr 7m
(range 8yr 7m to 16yr 4m)
1yr 10m
(range 6m to 3yr 11m)
SDR group 15 13 male
2 female
8yr 5m
(range 5yr 3m to 11yr 11m)
1 yr 3 mo
(range 9m to 2yr)
0
100
200
300
400
500
600
700
800
900
Pre Op Post Op
Gill
ett
e G
ait
Ind
ex
(G
GI)
SDR
Multi Level
0
200
400
600
800
1000
1200
1400
1600
1800
0 200 400 600 800 1000 1200 1400 1600 1800
Pre Op GGI
Po
st
Op
GG
I
Multi Level (N = 39)
SDR (N = 20)
Information Needs for Parents
• SDR does not cure CP
• Selecting the correct treatment for a child requires careful assessment and may not
indicate SDR
• Aftercare and hard work continues until
skeletal maturity
• Diplegia of prematurity
• Plenty of spasticity
• Adequate
– Anti gravity strength
– Potential for rehabilitation
– Selective motor control
• Freedom from skeletal deformity
Information Needs
for Carers














![Medulloblastoma: [Print] - eMedicine Neurology · emedicine.medscape.com eMedicine Specialties > Neurology > Pediatric Neurology Medulloblastoma George I Jallo, MD, Associate Professor](https://static.fdocuments.in/doc/165x107/5d472c3c88c993527c8b60e5/medulloblastoma-print-emedicine-neurology-emedicinemedscapecom-emedicine.jpg)



