Selection, transition and progression – the role of the GMC Dr John Jenkins CBE Chair,...
37
Selection, transition and progression – the role of the GMC Dr John Jenkins CBE Chair, Postgraduate Board
-
Upload
sabrina-walker -
Category
Documents
-
view
216 -
download
2
Transcript of Selection, transition and progression – the role of the GMC Dr John Jenkins CBE Chair,...

Selection, transition and progression
– the role of the GMC
Dr John Jenkins CBEChair, Postgraduate Board

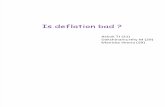
Selection, transition and progression are key elements of the education and training of doctors, for which the GMC has overall regulatory responsibility
Medical School
(4-6 years)
F1 year
(1 year)
F2 year
(1 year)
Specialty/GP training
(3-8 years)
Specialist/GP register (to retirement)
Provisional registration
Full registration
Certificate of completion of training (CCT)
SASG (specialty doctors)

Wider Context for the debate
GMC assuming responsibility for regulating all stages of medical education and training -
including undergraduate, foundation, specialty (including GP), continuing professional development
Increasing recognition of importance of selection, transition and progression throughout medical education and training
Implementation of Quality Improvement Framework

GMC Quality Improvement Framework

Quality Improvement Framework: Four elements
Approval against Standard
s

Education strategy 2011-2013
Setting and assuring standards,
and valuing education and training:
Ensure that the standards we set provide a framework for excellence and that we are proactive in maintaining compliance
Defining outcomes for education and
training:
Define clear outcomes which must be met by students and trainees on completion of different stages of training

Setting and assuring standards and valuing training
Alignment and review of standards – The Trainee Doctor
Valuing training (approval of trainers)
Developing a smarter evidence base
Consolidating quality visits and oversight

Defining outcomes for education and training
Tomorrows Doctors (2009)
Foundation Programme
Generic outcomes for specialty curricula
Routes to the Specialist and GP Registers

Education strategy 2011-2013
Working with partners and promotingfeedback and learning:
We will work with all those organisations, groups and individuals who have a stake in medical education and training. We will develop mechanisms to feedback what we have learned to encourage learning and improvement
Promoting effective selection,transition and progression:
Ensure there are clearer progressions between the stages of medical education and that risks associated with transitions are better managed

Promoting effective selection,transition and progression
Selection into medical school
Supporting disabled students and trainees
Transitions
Selection into specialty including GP training
Review of CPD

Roles in selection
UKFPO national eligibility
and recruitment
Medical school
Postgraduate deans, medical Royal Colleges
and Faculties – UK wide/ national and/or local depending on
specialty
Medical School Foundation Programme
Specialty / GP training
Appointment to career post
GMC sets standards and requirements

Student Selection – What we say now
Tomorrow’s Doctors 2009 states that:
Processes for student selection will be open, objective and fair (Paragraph 71)
Selection criteria will take account of the personal and academic qualities needed in a doctor as set out in Good Medical Practice and capacity to achieve the outcomes set out in Tomorrow’s Doctors (Paragraph 73)

Future role of GMC in selection?
Stronger assurance role
How effective are current methods of selection to medical school at assessing non-academic attributes of a good doctor?
Diversity in selection processes – is this justified and what is the impact?
How robust is the evidence to support current methods of selection to medical school?

Conclusion of seminar (June 2011)
The GMC has a significant role to play in:
(i) Promoting research
(ii) Evaluating current processes
(iii) Ensuring fairness and transparency
Issues for further debate :
(i) Better alignment of “inputs and outputs”
(ii) Minimising “waste”
(iii) Widening participation

GMC Education Strategy (2011-2013)
Key aim – Promoting effective selection, transition and progression:
‘In 2011 we will work with the Medical Schools Council and others to identify examples of good practice in relation to the selection of medical students, based on the best available evidence.’

PMETB report on selection into specialty training
There should be effective assurance of the assessment instruments and processes used in selection into specialty including GP training
The regulator should examine further the optimum way of assuring the assessment instruments and processes involved in selection into specialty, including GP training
In the examination to determine how best to achieve that assurance, statutory regulation should be considered

Education strategy 2011-2013
Setting and assuring standards,
and valuing education and training:
Ensure that the standards we set provide a framework for excellence and that we are proactive in maintaining compliance
The Trainee Doctor
Foundation and specialty, including GP training

Domain 4 – Recruitment, selection and appointment
Purpose - to ensure that the processes for entry into postgraduate training programmes are fair and transparent
Responsibility - postgraduate deans, medical Royal Colleges and Faculties, specialty associations,
UK Foundation Programme Office, local faculty and, through these, employers
Evidence - Deanery data, trainee surveys, national and local recruitment processes
Standard - Processes for recruitment, selection and appointment must be open, fair, and effective

Mandatory requirements
Candidates will be eligible for consideration for entry into specialty training if they:
(a) are a fully registered medical practitioner with the GMC or are eligible for any such registration
(b) hold a licence to practise or are eligible to do so
(c) are fit to practise
(d) are able to demonstrate the competences required to complete foundation training. This covers candidates who have completed foundation training, candidates who apply before completion and those who have not undertaken foundation training but can demonstrate the competences in another way

The selection process must:
(a) ensure that information about places on training programmes, eligibility and selection criteria and the application process is published and made widely available in sufficient time to doctors who may be eligible to apply
(b) use criteria and processes which treat eligible candidates fairly
(c) select candidates through open competition
(d) have an appeals system against non-selection on the grounds that the criteria were not applied correctly, or were discriminatory
(e) seek from candidates only such information (apart from information sought for equalities monitoring purposes) as is relevant to the published criteria and which potential candidates have been told will be required

The selection process
4.3 Selection panels must consist of persons who have been trained in selection principles and processes
4.4 Selection panels must include a lay person
4.5 There must be comprehensive information provided for those within postgraduate programmes about choices in the programme and how they are allocated
Foundation training mandatory requirement
4.6 The appointment process should demonstrate that foundation doctors are fit for purpose and able, subject to an appropriate induction and ongoing training, to undertake the duties expected of them in a supportive environment. The process should build on experiences gained at medical schools to support fitness for purpose in the working environment.

New elements of selection
Medical school – collaborative content (MSC); Prescribing skills assessment (MSC, BPS)
Improving Selection to the Foundation Programme project (ISFP) – educational performance measures; situational judgement tests
Specialty training – increasing move to national/UK wide recruitment
Award of CCT – exit assessments

GMC Education Strategy 2011 -2013
‘In 2011 we are considering whether research should be commissioned in relation to the discharge of our existing responsibilities to set standards for selection processes into specialty including GP training.’

The state of medical education and practice in the UK
“In the 2010 national survey of trainees, nearly 90% of those approaching the end of their training were confident about taking up a new role as a consultant or GP.”
However, there is also increasing recognition of the importance of transitions as “pressure points” for both patient safety and quality of training –
(i) graduation
(ii) entry to specialist training
(iii) CCT and appointment to substantive post

Medical schools need to ensure that graduatesare well prepared for clinical practice
“In our quality assurance visits (inspections) of medical schools (2005-10), we found inconsistencies and variation in the assessment policies and practices. This raises the question of whether all graduates have the same minimum standards of clinical competence.
There is evidence that, in the past, some medical graduates reported being unprepared for some of the practical skills required of them when they entered Foundation training.”
The state of medical education and practice in the UK, 2011

Transitions research - findings
Graduates looked forward to ‘being a doctor’ While communication is a strong area at graduation, F1s
were under-prepared for some complex communication tasks
Other clinical skills are well practised, but not in contexts which sufficiently mimic the clinical environment
Knowledge of non-clinical areas such as legal and ethical issues, and the operation of the NHS, was lacking at the start of F1
Prescribing a significant area of under-preparedness
Dr Jan Illing et al: How prepared are medical graduates to begin practice? (2008)

Transitions research - recommendations
Undergraduates’ preparedness will be improved by more experiential learning in clinical practice:
Ensure that placements have more structure and consistency Ensure that students are given a greater role in medical teams Establish fuller and more prescriptive guidelines on shadowing Specify the limits of the F1 role Address particular weaknesses in prescribing
Dr Jan Illing et al: How prepared are medical graduates to begin practice? (2008)

GMC Education Strategy 2011 -2013
We expect that the implementation of TD 2009 will do much to address past concerns about the preparedness of some graduates to enter the workplace. Nevertheless, we will continue to work closely with others to support the critical transition in responsibility from medical student to new doctor
In 2011 we will continue to contribute to groups established by MSC and MEE looking at, respectively, transitions and shadowing

Transfer of Information
Tomorrow’s Doctors 2009
‘While it is essential that the outcomes are achieved by all graduates, medical schools should also make arrangements so that their graduates’ areas of relative weakness are fed into their Foundation Programme portfolios so they can be reviewed by the educational supervisor.’
Medical Schools Council Transition Group – implementing TD (09) recommendations

GMC Education Strategy 2011 -2013
“We will prioritise the development and implementation of arrangements that ensure, for the protection of patients and in the educational interests of trainees, that appropriate information about graduates is shared between medical schools and their Foundation Programme educational supervisor.”

Future of GMC role in transition
Defining clear outcomes for each stage of training (medical school to F1; outcomes for F2; generic outcomes for specialty training)
Assuring local processes for sharing information
Assessing transition outcomes – shared evidence (including trainee survey)

Progression
Annual review of competence and progression for every trainee (ARCP)
Depends on requirements of curriculum and assessment system – usually includes specialty exams, workplace based assessment and feedback from supervisors and others

Progression issues
Clear trajectory of learning (level descriptors)
Robust and fair ARCP with triangulated evidence
Educational and clinical supervision and reports
“Workplace based assessments” - ? change in terminology and use (undergraduate and postgraduate)
Early identification of unsatisfactory progress, causes and remediation

Future GMC role in progression
Approval of Trainers project
Project to provide overview of current assessment systems
Review interaction between specialty exam pass rates and progression
Joint project with Deaneries to analyse progression trends in ARCP outcomes
Investigation of delivery of ARCP processes

Principles of better regulation
Development of the QIF was guided by the five principles for assessing and improving the quality of regulation:
• Proportionality - Regulators should only intervene when necessary. Remedies should be appropriate to the risk posed, and costs identified and minimised
• Accountability - Regulators must be able to justify decisions and be subject to public scrutiny
• Consistency - Government rules and standards must be joined up and implemented fairly
• Transparency - Regulators should be open, and keep regulations simple and user-friendly
• Targeting - Regulation should be focused on the problem and minimise side effects

Principles of better regulation
Working together
• Clear understanding of complementary roles and responsibilities
• Effective communication (including participation in each other’s structures and workstreams)

What is the GMC doing to improve training?
Clarifying the standards of training (for today’s healthcare) and education (for the challenges of tomorrow, including complexities, uncertainty and risk)
Securing an identified individual responsible and accountable for the quality of training delivered locally
Maximising the value of training time, including the experiential and environmental components
Aiming for excellence (building on competence and including confidence) in personal responsibility for the quality and safety of care, delivered in the context of team-based approach to management