Selection of an Ideal Disinfectant William A. Rutala, Ph.D., M.P.H. Director, Hospital Epidemiology,...
85
Selection of an Ideal Disinfectant William A. Rutala, Ph.D., M.P.H. Director, Hospital Epidemiology, Occupational Health and Safety, UNC Health Care; Research Professor of Medicine and Director, Statewide Program for Infection Control and Epidemiology, University of North Carolina at Chapel Hill, NC, USA
-
Upload
crystal-porter -
Category
Documents
-
view
214 -
download
0
Transcript of Selection of an Ideal Disinfectant William A. Rutala, Ph.D., M.P.H. Director, Hospital Epidemiology,...

Selection of an Ideal Disinfectant
William A. Rutala, Ph.D., M.P.H.Director, Hospital Epidemiology, Occupational Health
and Safety, UNC Health Care; Research Professor of Medicine and Director, Statewide Program for Infection Control and Epidemiology, University of
North Carolina at Chapel Hill, NC, USA
Disclosure: Clorox

LECTURE OBJECTIVES
Review the role of the environment in transmission of nosocomial pathogens
Review the properties of an ideal disinfectant Review the key considerations for selecting the
ideal disinfectant Kill Claims Kill and wet-contact time Safety Ease of use Other factors

DISINFECTION AND STERLIZATION
EH Spaulding believed that how an object will be disinfected depended on the object’s intended use. CRITICAL - objects which enter normally sterile tissue or the
vascular system or through which blood flows should be sterile.
SEMICRITICAL - objects that touch mucous membranes or skin that is not intact require a disinfection process (high-level disinfection [HLD]) that kills all microorganisms but high numbers of bacterial spores.
NONCRITICAL -objects that touch only intact skin require low-level disinfection.


Processing “Noncritical” Patient Care Objects
Classification: Noncritical objects will not come in contact with mucous membranes or skin that is not intact.
Object: Can be expected to be contaminated with some microorganisms.
Level germicidal action: Kill vegetative bacteria, fungi and lipid viruses.
Examples: Bedpans; crutches; bed rails; EKG leads; bedside tables; walls, floors and furniture.
Method: Low-level disinfection

Low-Level Disinfection for “Noncritical” Objects
Exposure time > 1 minGermicide Use ConcentrationEthyl or isopropyl alcohol 70-90%Chlorine 100ppm (1:500
dilution)Phenolic UDIodophor UDQuaternary ammonium UDImproved hydrogen peroxide 0.5%, 1.4%______________________________________________________UD=Manufacturer’s recommended use dilution

LECTURE OBJECTIVES
Review the role of the environment in transmission of nosocomial pathogens
Review the properties of an ideal disinfectant Review the key considerations for selecting the
ideal disinfectant Kill Claims Kill and wet-contact time Safety Ease of use Other factors

ENVIRONMENTAL CONTAMINATION LEADS TO HAIs
There is increasing evidence to support the contribution of the environment to disease transmission
This supports comprehensive disinfecting regimens (goal is not sterilization) to reduce the risk of acquiring a pathogen from the healthcare environment/equipment


KEY PATHOGENS WHERE ENVIRONMENTIAL SURFACES PLAY A ROLE IN TRANSMISSION
MRSA VRE Acinetobacter spp. Clostridium difficile Norovirus Rotavirus SARS

ENVIRONMENTAL CONTAMINATION ENVIRONMENTAL CONTAMINATION ENDEMIC AND EPIDEMIC MRSAENDEMIC AND EPIDEMIC MRSA
Dancer SJ et al. Lancet ID 2008;8(2):101-13

ENVIRONMENTAL SURVIVAL OF KEY PATHOGENS ON HOSPITAL SURFACES
Pathogen Survival Time
S. aureus (including MRSA) 7 days to >12 months
Enterococcus spp. (including VRE) 5 days to >46 months
Acinetobacter spp. 3 days to 11 months
Clostridium difficile (spores) >5 months
Norovirus (and feline calicivirus) 8 hours to >2 weeks
Pseudomonas aeruginosa 6 hours to 16 months
Klebsiella spp. 2 hours to >30 months
Adapted from Hota B, et al. Clin Infect Dis 2004;39:1182-9 andKramer A, et al. BMC Infectious Diseases 2006;6:130

Thoroughness of Environmental Cleaning
Carling et al. Am J Infect Control. 2013;41:S20-S25
0
20
40
60
80
100
HEHSG HOSP
IOWA HOSP
OTHER HOSP
OPERATING ROOMS
NICUEMS VEHICLES
ICU DAILY
AMB CHEMO
MD CLINIC
LONG TERM
DIALYSIS
%
DAILY CLEANING
TERMINAL CLEANING
Cle
aned
Mean = 32%
>110,000 Objects

Mean proportion of surfaces disinfected at terminal cleaning is ~30%

FREQUENCY OF ACQUISITION OF MRSA ON GLOVED HANDS AFTER CONTACT WITH SKIN AND ENVIRONMENTAL SITES
No significant difference on contamination rates of gloved hands after contact with skin or environmental surfaces (40% vs 45%; p=0.59)
Stiefel U, et al. ICHE 2011;32:185-187

TRANSMISSION MECHANISMS INVOLVING THE SURFACE ENVIRONMENT
Rutala WA, Weber DJ. In:”SHEA Practical Healthcare Epidemiology” (Lautenbach E, Woeltje KF, Malani PN, eds), 3rd ed, 2010.

ACQUISITION OF MRSA ON HANDS AFTER CONTACT WITH ENVIRONMENTAL SITES

TRANSFER OF MRSA FROM PATIENT OR ENVIRONMENT TO IV DEVICE AND TRANSMISSON OF PATHOGEN

EVALUATION OF HOSPITAL ROOM ASSIGNMENT AND ACQUISITION OF CDI
Study design: Retrospective cohort analysis, 2005-2006
Setting: Medical ICU at a tertiary care hospital
Methods: All patients evaluated for diagnosis of CDI 48 hours after ICU admission and within 30 days after ICU discharge
Results (acquisition of CDI) Admission to room previously
occupied by CDI = 11.0% Admission to room not previously
occupied by CDI = 4.6% (p=0.002)
Shaughnessy MK, et al. ICHE 2011;32:201-206

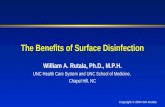
Increased Risk of Acquisition of HA Pathogen from Prior Room Occupant~120%
0 0.5 1 1.5 2 2.5 3 3.5 4
MDR Acinetobacter (Nseir S, 2011)
C. diff (Shaughnessy M, 2011)
VRE^ (Drees M, 2008)
MDR Pseudomonas (Nseir S, 2011)
VRE (Huang S, 2006)
VRE* (Dress M, 2008)
MRSA (Huang S, 2006)
* Prior room occupant infected; ^Any room occupant in prior 2 weeks infected

ALL “TOUCHABLE” (HAND CONTACT) SURFACES SHOULD BE WIPED WITH
DISINFECTANT
“High touch” objects only recently defined (no significant differences in microbial contamination of different surfaces)
and “high risk” objects not epidemiologically defined.


FREQUENCY (mean) OF HCP CONTACT FOR SURFACES IN AN ICU (N=28) AND WARD (N=24)
ICU WARD
Huslage K, Rutala WA, Sickbert-Bennett E, Weber DJ. ICHE 2010;31:850-853

MICROBIAL BURDEN ON ROOM SURFACES AS A FUNCTION OF FREQUENCY OF TOUCHING
Surface Prior to CleaningMean CFU/RODAC (95% CI)
Post Cleaning (mean)Mean CFU/RODAC (95% CI)
High 71.9 (46.5-97.3) 9.6Medium 44.2 (28.1-60.2) 9.3Low 56.7 (34.2-79.2) 5.7
The level of microbial contamination of room surfaces is similar regardless of how often they are touched both before and after cleaning
Therefore, all surfaces that are touched must be cleaned and disinfected
Huslage K, Rutala WA, Weber DJ. ICHE. 2013;34:211-212

Thoroughness of Environmental CleaningCarling et al. Am J Infect Control. 2013;41:S20-S25
0
20
40
60
80
100
HEHSG HOSP
IOWA HOSP
OTHER HOSP
OPERATING ROOMS
NICUEMS VEHICLES
ICU DAILY
AMB CHEMO
MD CLINIC
LONG TERM
DIALYSIS
%
DAILY CLEANING
TERMINAL CLEANING
Cle
aned
Mean = 32%
>110,000 Objects

ENVIRONMENTAL CONTAMINATION LEADS TO HAIsSuboptimal Cleaning
There is increasing evidence to support the contribution of the environment to disease transmission
This supports comprehensive disinfecting regimens (goal is not sterilization) to reduce the risk of acquiring a pathogen from the healthcare environment

Quality Improvement

MONITORING THE EFFECTIVENESS OF CLEANINGCooper et al. AJIC 2007;35:338
Visual assessment-not a reliable indicator of surface cleanliness
ATP bioluminescence-measures organic debris (each unit has own reading scale, <250-500 RLU)
Microbiological methods-<2.5CFUs/cm2-pass; can be costly and pathogen specific
Fluorescent marker

SURFACE EVALUATION USING ATP BIOLUMINESCENCE
Swab surface luciferace tagging of ATP Hand held luminometer
Used in the commercial food preparation industry to evaluate surface cleaning before reuse and as an educational tool for more than 30 years.

MONITORING THE EFFECTIVENESS OF CLEANINGCooper et al. AJIC 2007;35:338
• Visual assessment-not a reliable indicator of surface cleanliness
• ATP bioluminescence-measures organic debris (each unit has own reading scale, <250-500 RLU)
• Microbiological methods-<2.5CFUs/cm2-pass; can be costly and pathogen specific
• Fluorescent marker-transparent, easily cleaned, environmentally stable marking solution that fluoresces when exposed to an ultraviolet light (applied by IP unbeknown to EVS, after EVS cleaning, markings are reassessed)

Fluorescent Marking Solution

Target After Marking

Target Enhanced

TERMINAL ROOM CLEANING: DEMONSTRATION OF IMPROVED CLEANING
Evaluated cleaning before and after an intervention to improve cleaning
36 US acute care hospitals Assessed cleaning using a
fluorescent dye Interventions
Increased education of environmental service workers
Feedback to environmental service workers
†Regularly change “dotted” items to prevent targeting objects
Carling PC, et al. ICHE 2008;29:1035-41

LECTURE OBJECTIVES
Review the role of the environment in transmission of nosocomial pathogens
Review the properties of an ideal disinfectant Review the key considerations for selecting the
ideal disinfectant Kill Claims Kill and wet-contact time Safety Ease of use Other factors

PROPERTIES OF AN IDEALSURFACE DISINFECTANT
Broad spectrum Fast acting Remains wet Not affected by environmental
factors Nontoxic Surface compatibility Persistence
Easy to use Acceptable odor Economical Solubility Stability Cleaner Nonflammable
Rutala WA, Weber DJ. Infect Control Hosp Epidemiol 2014;35:855-865

PROPERTIES OF AN IDEALSURFACE DISINFECTANT
Broad spectrum Should have a wide antimicrobial spectrum, including kill claims for
all pathogens that are common causes of HAIs and outbreaks Fast acting
Should have a rapid kill and short kill/contact time listed on the label Remains wet
Should keep surfaces wet long enough to meet listed kill/contact times with a single application or meet wet times recommended by evidence-based guidelines (60 seconds)
Rutala WA, Weber DJ. Infect Control Hosp Epidemiol 2014;35:855-865

PROPERTIES OF AN IDEALSURFACE DISINFECTANT
Not affected by environmental factors Should be active in the presence of organic matter (e.g., blood, sputum,
feces) and compatible with soaps, detergents, and other chemicals encountered in use
Nontoxic Should not irritating to the user, visitors, and patients. Should not induce
allergic symptoms (especially asthma and dermatitis). The toxicity ratings for disinfectants are danger, warning, caution, and none. Ideally choose products with the lowest toxicity rating.
Surface compatibility Should be proven compatible with common healthcare surfaces and devices
Rutala WA, Weber DJ. Infect Control Hosp Epidemiol 2014;35:855-865

PROPERTIES OF AN IDEALSURFACE DISINFECTANT
Persistence Should have sustained antimicrobial activity or residual antimicrobial effect
on the treated surface Easy to use
Should be available in multiple forms, such as wipes (large and small), sprays, pull tops, and refills; directions for use should be simple and contain information about personal protective equipment as required
Acceptable odor Should have an odor deemed acceptable by users and patients
Solubility Should be soluble in water
Rutala WA, Weber DJ. Infect Control Hosp Epidemiol 2014;35:855-865

PROPERTIES OF AN IDEALSURFACE DISINFECTANT
Economical Costs should not be prohibitively high but when considering the costs of a
disinfectant one should also consider product capabilities, cost per compliant use, etc.
Stability Should be stable in concentrate and use dilution
Cleaner Should have good cleaning properties
Nonflammable Should have a flash point above 150oF
Rutala WA, Weber DJ. Infect Control Hosp Epidemiol 2014;35:855-865

LOW-LEVEL DISINFECTION FOR NONCRITICAL EQUIPMENT AND SURFACES
Exposure time > 1 minGermicide Use Concentration
Ethyl or isopropyl alcohol 70-90%Chlorine 100ppm (1:500
dilution)Phenolic UDIodophor UDQuaternary ammonium UDImproved hydrogen peroxide 0.5%, 1.4%____________________________________________________UD=Manufacturer’s recommended use dilution

LOW-LEVEL DISINFECTION FOR NONCRITICAL EQUIPMENT AND SURFACES
Exposure time > 1 minGermicide Use Concentration
Ethyl or isopropyl alcohol 70-90%Chlorine 100ppm (1:500
dilution)Phenolic UDIodophor UDQuaternary ammonium UDImproved hydrogen peroxide (HP) 0.5%, 1.4%____________________________________________________UD=Manufacturer’s recommended use dilution

BACTERICIDAL ACTIVITY OF DISINFECTANTS (log10 reduction) WITH A CONTACT TIME OF 1m WITH/WITHOUT FCS.
Rutala et al. ICHE. 2012; 33:1159-61
Organism 0.5% IHP 0.5% HP HP Cleaner-Dis 1.4% IHP
1.4% HP 3.0% HP QUAT
MRSA >6.6 <4.0 >6.5 <4.0 <4.0 5.5
VRE >6.3 <3.6 >6.1 <3.6 <3.6 4.6
MDR-Ab >6.8 <4.3 >6.7 <4.3 <4.3 >6.8
MRSA, FCS
>6.7 NT >6.7 NT <4.2 <4.2
VRE, FCS >6.3 NT >6.3 NT <3.8 <3.8
MDR-Ab, FCS
>6.6 NT >6.6 NT <4.1 >6.6
Improved hydrogen peroxide is significantly superior to standard HP at same concentration and superior or similar to the QUAT tested

Hospital Privacy Curtains(pre- and post-intervention study; sampled curtain, sprayed “grab area” 3x
from 6-8” with 1.4% IHP and allowed 2 minute contact; sampled curtain)

Decontamination of Curtains with Activated HP (1.4%)Rutala, Gergen, Weber. Am J Infect Control. 2014;42:426-428
CP for: Before DisinfectionCFU/5 Rodacs (#Path)
After DisinfectionCFU/5 Rodacs (#Path)
% Reduction
MRSA 330 (10 MRSA) 21*(0 MRSA) 93.6%
MRSA 186 (24 VRE) 4* (0 VRE) 97.9%
MRSA 108 (10 VRE) 2* (0 VRE) 98.2%
VRE 75 (4 VRE) 0 (0 VRE) 100%
VRE 68 (2 MRSA) 2* (0 MRSA) 97.1%
VRE 98 (40 VRE) 1* (0 VRE) 99.0%
MRSA 618 (341 MRSA) 1* (0 MRSA) 99.8%
MRSA 55 (1 VRE) 0 (0 MRSA) 100%
MRSA, VRE 320 (0 MRSA, 0 VRE) 1* (0 MRSA, 0 VRE) 99.7%
MRSA 288 (0 MRSA) 1* (0 MRSA) 99.7%
Mean 2146/10=215 (432/10=44) 33*/10=3 (0) 98.5%
* All isolates after disinfection were Bacillus sp; now treat CP patient curtains at discharge with IHP

How About “Green” Products?
Today, the definition of green is unregulated It can mean:
Sustainable resources/plant-based ingredients Free of petrochemicals Biodegradable No animal testing Minimal carbon footprint Traded fairly
It can, but does not always mean “safer”

Efficacy of “Green” Products to Inactivate MDR Pathogens
Rutala, Gergen, Weber. Unpublished results. 2013
No measurable activity against A. baumannii, A. xyloxidans, Burkholderia cenocepacia, K. pneumoniae, MRSA and P. aeruginosa, VRE, Stenotrophomonas maltophilia

Transfer of C. difficile Spores by Nonsporicidal Wipes
Cadnum et al. ICHE 2013;34:441-2
Detergent/nondisinfectant-nonsporicidal wipes transfer or spread microbes/spores to adjacent surfaces; disinfectants inactivate microbes

LOW-LEVEL DISINFECTION FOR NONCRITICAL EQUIPMENT AND SURFACES
Exposure time > 1 minGermicide Use Concentration
Ethyl or isopropyl alcohol 70-90%Chlorine 100ppm (1:500
dilution)Phenolic UDIodophor UDQuaternary ammonium UDImproved hydrogen peroxide 0.5%, 1.4%____________________________________________________UD=Manufacturer’s recommended use dilution

Quaternary ammonium compounds (e.g., didecyl dimethyl ammonium bromide, dioctyl dimethyl ammonium
bromide)Rutala, Weber. Am J Infect Control 2013;41:S36-S41
Advantages Bactericidal, fungicidal, virucidal
against enveloped viruses (e.g., HIV)
Good cleaning agents EPA registered Surface compatible Persistent antimicrobial activity
when undisturbed Inexpensive (in dilutable form) Not flammable
Disadvantages Not sporicidal In general, not tuberculocidal and
virucidal against non-enveloped viruses
High water hardness and cotton/gauze can make less microbicidal
A few reports documented asthma as result of exposure to benzalkonium chloride
Affected by organic matter Multiple outbreaks ascribed to
contaminated benzalkonium chloride

Sodium HypochloriteRutala, Weber. Am J Infect Control 2013;41:S36-S41
Advantages Bactericidal, tuberculocidal, fungicidal,
virucidal Sporicidal Fast acting Inexpensive (in dilutable form) Not flammable Unaffected by water hardness Reduces biofilms on surfaces Relatively stable (e.g., 50% reduction in
chlorine concentration in 30 days) Used as the disinfectant in water
treatment EPA registered
Disadvantages Reaction hazard with acids and ammonias Leaves salt residue Corrosive to metals (some ready-to-use
products may be formulated with corrosion inhibitors)
Unstable active (some ready-to-use products may be formulated with stabilizers to achieve longer shelf life)
Affected by organic matter Discolors/stains fabrics Potential hazard is production of
trihalomethane Odor (some ready-to-use products may be
formulated with odor inhibitors). Irritating at high concentrations.

AlcoholRutala, Weber. Am J Infect Control 2013;41:S36-S41
Advantages
Bactericidal, tuberculocidal, fungicidal, virucidal
Fast acting Non-corrosive Non-staining Used to disinfect small surfaces
such as rubber stoppers on medication vials
No toxic residue
Disadvantages Not sporicidal Affected by organic matter Slow acting against non-enveloped viruses
(e.g., norovirus) No detergent or cleaning properties Not EPA registered Damage some instruments (e.g., harden
rubber, deteriorate glue) Flammable (large amounts require special
storage) Evaporates rapidly making contact time
compliance difficult Not recommended for use on large surfaces Outbreaks ascribed to contaminated alcohol

PhenolicsRutala, Weber. Am J Infect Control 2013;41:S36-S41
Advantages Bactericidal, tuberculocidal,
fungicidal, virucidal Inexpensive (in dilutable
form) Non-staining Not flammable EPA registered
Disadvantages Not sporicidal Absorbed by porous
materials and irritate tissue Depigmentation of skin
caused by certain phenolics Hyperbilirubinemia in infants
when phenolic not prepared as recommended

Improved Hydrogen PeroxideRutala, Weber. Am J Infect Control 2013;41:S36-S41
Advantages Bactericidal, tuberculocidal,
fungicidal, virucidal Fast efficacy Easy compliance with wet-contact
times Safe for workers (lowest EPA
toxicity category, IV) Benign for the environment Surface compatible Non-staining EPA registered Not flammable
Disadvantages More expensive than most
other disinfecting actives Not sporicidal at low
concentrations

LECTURE OBJECTIVES
Review the role of the environment in transmission of nosocomial pathogens
Review the properties of an ideal disinfectant Review the key considerations for selecting the
ideal disinfectant Kill Claims Kill and wet-contact time Safety Ease of use Other factors

Key Considerations for Selecting the Ideal Disinfectant for Your Facility
Rutala, Weber. Infect Control Hosp Epidemiol. 2014;35:855-865
Consideration Question to Ask Score (1-10)
Kill Claims Does the product kill the most prevalent healthcare pathogens
Kill Times and Wet-Contact Times
How quickly does the product kill the prevalent healthcare pathogens. Ideally, contact time greater than or equal to the kill claim.
Safety Does the product have an acceptable toxicity rating, flammability rating
Ease-of-Use Odor acceptable, shelf-life, in convenient forms (wipes, spray), water soluble, works in organic matter, one-step (cleans/disinfects)
Other factors Supplier offer comprehensive training/education, 24-7 customer support, overall cost acceptable (product capabilities, cost per compliant use, help standardize disinfectants in facility)
Note: Consider the 5 components shown, give each product a score (1 is worst and 10 is best) in each of the 5 categories, and select the product with the highest score as the optimal choice (maximum score is 50).

SELECTION OF THE IDEAL SURFACE DISINFECTANTKill Claims
Disinfectants used in hospitals should be EPA registered Hospital disinfectant must show activity against Salmonella,
Pseudomonas and S. aureus Label are very specific about their kill claims (1-10 min
contact time) Does the product kill the most prevalent healthcare
pathogens including those that Cause most HAIs Cause most outbreaks Are of concern in your facility



MOST PREVALENT PATHOGENS CAUSING HAI
Most prevent pathogens causing HAI (easy to kill) S. aureus (15.6%) E. coli (11.5%) Coag neg Staph (11.4%) Klebsiella (8.0%) P. aeruginosa (8.0%) E. faecalis (6.8%) C. albicans (5.3%) Enterobacter sp. (4.7%) Other Candida sp (4.2%)
Common causes of outbreaks and ward closures (relatively hard to kill) C. difficile spores Norovirus Rotavirus Adenovirus

Middle East Respiratory Syndrome-CoronavirusMERS-CoV

New and Emerging PathogensMERS-CoV, Ebola, Enterovirus D68
Will likely not have an EPA-registered disinfectant on the market to kill it
Manufacturers may not make claims about emerging pathogens without EPA approval, which may take 18-24 months for new pathogens
Until an EPA-approved claim is available, users may refer to the hierarchy of microbial susceptibility to select the appropriate disinfectant
For example, an EPA claim against poliovirus could be used for MERS-CoV as well as inactivation data of coronavirus

Decreasing Order of Resistance of Microorganisms to Disinfectants/Sterilants
PrionsBacterial spores (C. difficile)
MycobacteriaSmall, non-enveloped viruses (noro, polio, EV-D68)
Fungal sporesGram-negative bacilli (Acinetobacter)
Vegetative fungi and algaeLarge, non-enveloped viruses
Gram-positive bacteria (MRSA, VRE)Enveloped viruses (Ebola, MERS-CoV)
Most Resistant
Most Susceptible

Inactivation of Coronavirus by Disinfectants/Antiseptics and Survival on Surfaces
Sattar, Springthorpe, Karim, Loro. Epidemiol Infect 1989;102:493 3 log10 reduction in 1m by 2% glut, 70% alcohol, 1% PI, phenolic, and
5,000 ppm chlorine Hulkower, Casanova, Rutala, Weber, Sobsey. Am J Infect Control
2011;39:401 2 log10 reduction in 1m by phenolic (use-dilution), OPA, 70% ethanol,
62% ethanol, 71% ethanol
Disinfectants and antiseptics effective in 1min

Decreasing Order of Resistance of Microorganisms to Disinfectants/Sterilants
PrionsBacterial spores (C. difficile)
MycobacteriaSmall, non-enveloped viruses (noro, polio, EV-D68)
Fungal sporesGram-negative bacilli (Acinetobacter)
Vegetative fungi and algaeLarge, non-enveloped viruses
Gram-positive bacteria (MRSA, VRE)Enveloped viruses (Ebola, MERS-CoV)
Most Resistant
Most Susceptible

GUIDELINE FOR THE PREVENTION OF NOROVIRUS OUTBREAKS IN HEALTHCARE, HICPAC, 2011
Avoid exposure to vomitus or diarrhea. Place patients with suspected norovirus on Contact Precautions in a single room (lB) Continue Precautions for at least 48 hours after symptom resolution (lB) Use longer isolation times for patients with comorbidities (ll) or <2 yrs (ll)
Consider minimizing patient movements within a ward (ll) Consider restricting movement outside the involved ward unless essential (ll) Consider closure of wards to new admissions (ll)
Exclude ill personnel (lB) During outbreaks, use soap and water for hand hygiene (lB) Clean and disinfect patient care areas and frequently touched surfaces
during outbreaks 3x daily using EPA approved healthcare product (lB) Clean surfaces and patient equipment prior to disinfection. Use product
with an EPA approved claim against norovirus (lC)
MacCannell T, et al. http://www.cdc.gov/hicpac/pdf/norovirus/Norovirus-Guideline-2011.pdf

Decreasing Order of Resistance of Microorganisms to Disinfectants/Sterilants
PrionsBacterial spores (C. difficile)
MycobacteriaSmall, non-enveloped viruses (noro, polio, EV-D68)
Fungal sporesGram-negative bacilli (Acinetobacter)
Vegetative fungi and algaeLarge, non-enveloped viruses
Gram-positive bacteria (MRSA, VRE)Enveloped viruses (Ebola, MERS-CoV)
Most Resistant
Most Susceptible

C. difficile EPA-Registered Products
• List K: EPA’s Registered Antimicrobials Products Effective Against C. difficile spores, April 2014
• http://www.epa.gov/oppad001/list_k_clostridium.pdf
• 34 registered products; most chlorine-based, some HP/PA-based

Key Considerations for Selecting the Ideal Disinfectant for Your Facility
Rutala, Weber. Infect Control Hosp Epidemiol. 2014;35:855-865
Consideration Question to Ask Score (1-10)
Kill Claims Does the product kill the most prevalent healthcare pathogens 10, 8Kill Times and Wet-Contact Times
How quickly does the product kill the prevalent healthcare pathogens. Ideally, contact time greater than or equal to the kill claim.
Safety Does the product have an acceptable toxicity rating, flammability rating
Ease-of-Use Odor acceptable, shelf-life, in convenient forms (wipes, spray), water soluble, works in organic matter, one-step (cleans/disinfects)
Other factors Supplier offer comprehensive training/education, 24-7 customer support, overall cost acceptable (product capabilities, cost per compliant use, help standardize disinfectants in facility)
Note: Consider the 5 components shown, give each product a score (1 is worst and 10 is best) in each of the 5 categories, and select the product with the highest score as the optimal choice (maximum score is 50).

SELECTION OF THE IDEAL SURFACE DISINFECTANTKill and Wet-Contact Time
How quickly does the product kill the prevalent healthcare pathogens?
Does the product keep surfaces visibly wet for the kill times listed on its label?

Kill Times for Most Prevalent Pathogens
Each disinfectant requires a specific time it must remain in contact with the microbe to achieve disinfection. This is known as the kill time or contact time
Some disinfectants may have a kill time for bacteria of 1m, which means bacteria in label disinfected in 1m
Other low-level disinfectants, often concentrated formulas require dilution, are registered by the EPA with contact time of 10m
Such a long contact time is not practical

CONTACT TIMES FOR SURFACE DISINFECTION
Follow the EPA-registered contact times, ideally Some products have achievable contact times for
bacteria/viruses (30 seconds-2 minutes) Other products have non-achievable contact times
If use a product with non-achievable contact time Use >1 minute based on CDC guideline and scientific
literature Prepare a risk assessment
http://www.unc.edu/depts/spice/dis/SurfDisRiskAssess2011.pdf

Key Considerations for Selecting the Ideal Disinfectant for Your Facility
Rutala, Weber. Infect Control Hosp Epidemiol. 2014;35:855-865
Consideration Question to Ask Score (1-10)
Kill Claims Does the product kill the most prevalent healthcare pathogens
Kill Times and Wet-Contact Times
How quickly does the product kill the prevalent healthcare pathogens. Ideally, contact time greater than or equal to the kill claim.
10, 8
Safety Does the product have an acceptable toxicity rating, flammability rating
Ease-of-Use Odor acceptable, shelf-life, in convenient forms (wipes, spray), water soluble, works in organic matter, one-step (cleans/disinfects)
Other factors Supplier offer comprehensive training/education, 24-7 customer support, overall cost acceptable (product capabilities, cost per compliant use, help standardize disinfectants in facility)
Note: Consider the 5 components shown, give each product a score (1 is worst and 10 is best) in each of the 5 categories, and select the product with the highest score as the optimal choice (maximum score is 50).

SELECTION OF THE IDEAL SURFACE DISINFECTANTSafety
Does the product have an acceptable toxicity rating (danger, warning, caution, none)?
Does the product have an acceptable flammability rating?
Is a minimum level of personal protective equipment required?
Is the product compatible with the common surfaces in your facility?

Key Considerations for Selecting the Ideal Disinfectant for Your Facility
Rutala, Weber. Infect Control Hosp Epidemiol. 2014;35:855-865
Consideration Question to Ask Score (1-10)
Kill Claims Does the product kill the most prevalent healthcare pathogens
Kill Times and Wet-Contact Times
How quickly does the product kill the prevalent healthcare pathogens. Ideally, contact time greater than or equal to the kill claim.
Safety Does the product have an acceptable toxicity rating, flammability rating
10, 9
Ease-of-Use Odor acceptable, shelf-life, in convenient forms (wipes, spray, surface area wet for 1-2m; wipe not torn easily or fall apart), water soluble, works in organic matter, one-step (cleans/disinfects)
Other factors Supplier offer comprehensive training/education, 24-7 customer support, overall cost acceptable (product capabilities, cost per compliant use, help standardize disinfectants in facility)
Note: Consider the 5 components shown, give each product a score (1 is worst and 10 is best) in each of the 5 categories, and select the product with the highest score as the optimal choice (maximum score is 50).

SELECTION OF THE IDEAL SURFACE DISINFECTANTEase of Use
Is the product odor acceptable? Does the product have an acceptable shelf life? Does the product come in convenient forms to meet your
facility’s needs (refills, sprays, liquids; surface area wet for 1-2m; wipe not torn easily or fall apart)?
Does the product work in the presence of organic matter? Is the product water soluble? Does the product clean and disinfect in a single step? Are the directions for use simple and clear?

DISINFECTANTS ANDHEALTHCARE PERSONNEL SAFETY
Environmental (Low Level) disinfectants: Risks Skin irritation (dermatitis) Allergies (including asthma) Rarely reported in US
Environmental disinfectants: Protection for HCP Proper PPE by HCP (gloves, gowns) Training for proper use and disposal
Training and PPE minimize risk

Occupational Exposures to Disinfectants at UNC Health Care
In regard to skin or respiratory irritation and allergies in HCP, most studies refer to glutaraldehyde or formaldehyde; these products are not recommended for use on noncritical surfaces
Surface disinfection in US generally accomplished by QUAT, phenolic, improved HP and chlorine
We are evaluating all chemical exposures for ten years (2003-2012, ~9500 employees) and have rarely seen an employee in OHS with chronic respiratory complaint related to a low-level disinfectant (~30M persons days of exposure [Weber, Rutala, Consoli. 2013. Unpublished data])
Need well-designed immunologic evaluations of randomly selected HCP and controls, not case series without controls

Key Considerations for Selecting the Ideal Disinfectant for Your Facility
Rutala, Weber. Infect Control Hosp Epidemiol. 2014;35:855-865
Consideration Question to Ask Score (1-10)
Kill Claims Does the product kill the most prevalent healthcare pathogens
Kill Times and Wet-Contact Times
How quickly does the product kill the prevalent healthcare pathogens. Ideally, contact time greater than or equal to the kill claim.
Safety Does the product have an acceptable toxicity rating, flammability rating
Ease-of-Use Odor acceptable, shelf-life, in convenient forms (wipes, spray), water soluble, works in organic matter, one-step (cleans/disinfects)
10, 7
Other factors Supplier offer comprehensive training/education, 24-7 customer support, overall cost acceptable (product capabilities, cost per compliant use, help standardize disinfectants in facility)
Note: Consider the 5 components shown, give each product a score (1 is worst and 10 is best) in each of the 5 categories, and select the product with the highest score as the optimal choice (maximum score is 50).

SELECTION OF THE IDEAL SURFACE DISINFECTANTOther Factors
Does the supplier offer comprehensive training and ongoing education, both in person and virtual?
Does the supplier offer 24-7 customer support? Is the overall cost of the product acceptable (considering
product capabilities, cost of infections that may be prevented, and cost per compliant use?
Can the product help standardize disinfectants in your facility?

Key Considerations for Selecting the Ideal Disinfectant for Your Facility
Rutala, Weber. Infect Control Hosp Epidemiol. 2014;35:855-865
Consideration Question to Ask Score (1-10)
Kill Claims Does the product kill the most prevalent healthcare pathogens
Kill Times and Wet-Contact Times
How quickly does the product kill the prevalent healthcare pathogens. Ideally, contact time greater than or equal to the kill claim.
Safety Does the product have an acceptable toxicity rating, flammability rating
Ease-of-Use Odor acceptable, shelf-life, in convenient forms (wipes, spray), water soluble, works in organic matter, one-step (cleans/disinfects)
Other factors Supplier offer comprehensive training/education, 24-7 customer support, overall cost acceptable (product capabilities, cost per compliant use, help standardize disinfectants in facility)
10, 7
Note: Consider the 5 components shown, give each product a score (1 is worst and 10 is best) in each of the 5 categories, and select the product with the highest score as the optimal choice (maximum score is 50).

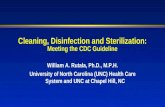
Key Considerations for Selecting the Ideal Disinfectant for Your Facility
Rutala, Weber. Infect Control Hosp Epidemiol. 2014;35:855-865
Consideration Question to Ask Score (1-10)
Kill Claims Does the product kill the most prevalent healthcare pathogens 10, 8Kill Times and Wet-Contact Times
How quickly does the product kill the prevalent healthcare pathogens. Ideally, contact time greater than or equal to the kill claim.
10, 8
Safety Does the product have an acceptable toxicity rating, flammability rating
10, 9
Ease-of-Use Odor acceptable, shelf-life, in convenient forms (wipes, spray), water soluble, works in organic matter, one-step (cleans/disinfects)
10, 7
Other factors Supplier offer comprehensive training/education, 24-7 customer support, overall cost acceptable (product capabilities, cost per compliant use, help standardize disinfectants in facility)
10, 7
50, 39
Note: Consider the 5 components shown, give each product a score (1 is worst and 10 is best) in each of the 5 categories, and select the product with the highest score as the optimal choice (maximum score is 50).

LECTURE OBJECTIVES
Review the role of the environment in transmission of nosocomial pathogens
Review the properties of an ideal disinfectant Review the key considerations for selecting the
ideal disinfectant Kill Claims Kill and wet-contact time Safety Ease of use Other factors

Selection of the Ideal DisinfectantConclusions
Disinfection of noncritical environmental surfaces/equipment is an essential component of Infection prevention
Disinfection should render surfaces and equipment free of pathogens in sufficient numbers to cause human disease
While the perfect disinfecting agent may not exist, a careful process of selection and use are necessary to reduce harm to patients and staff
When determining the optimal disinfecting product, consider the 5 components (kill claims/time, safety, ease of use, others)
Select the product with the highest score as the best choice for your healthcare facility

THANK YOU!www.disinfectionandsterilization.org