SEDENTARY BEHAVIOUR PROFILING IN BREAST CANCER … · Dr. Catherine Sabiston. There is not enough...
91
SEDENTARY BEHAVIOUR PROFILING IN BREAST CANCER SURVIVORS AND IMPLICATIONS FOR MENTAL HEALTH by Jason Lacombe A thesis submitted in conformity with the requirements for the degree of Masters of Science Exercise Sciences University of Toronto © Copyright by Jason Lacombe 2015
Transcript of SEDENTARY BEHAVIOUR PROFILING IN BREAST CANCER … · Dr. Catherine Sabiston. There is not enough...

SEDENTARY BEHAVIOUR PROFILING IN BREAST CANCER SURVIVORS AND IMPLICATIONS FOR
MENTAL HEALTH
by
Jason Lacombe
A thesis submitted in conformity with the requirements for the degree of Masters of Science
Exercise Sciences University of Toronto
© Copyright by Jason Lacombe 2015
ii
Sedentary behavior profiling in breast cancer survivors and implications
for mental health
Jason Lacombe
Masters of Science
Exercise Sciences University of Toronto
2015
Abstract
Background: Symptoms of depression remain under diagnosed but highly prevalent in breast
cancer survivors (BCS). Reducing sedentary behaviour (SED) during the early survivorship
period may be a strategy for treating clinical depression in survivors.
Methods: One hundred and eighty-seven BCS provided baseline demographic, medical, and
SED/physical activity data. Depression was reported three months later. Multiple dimensions of
SED were identified and examined in cluster analysis. The association between cluster
membership and depression was assessed using logistic regression.
Results: Two SED groups were identified representing higher and lower SED. High SED cluster
BCS’s were significantly older, heavier, less physically active, less educated, and were more
likely to have undergone lymph/axial node dissection. In the logistic regression model cluster
membership was a significant predictor of clinical depression.
Conclusions: Reducing dimensions of SED during the early survivorship period could protect
from clinical depression symptoms.
Key Words: Sedentary behaviour, physical activity, breast cancer survivors, depression
iii
Acknowledgments
I would like to first acknowledge and express my sincerest gratitude to my supervisor,
Dr. Catherine Sabiston. There is not enough room in this document to even begin to express how
much I appreciate everything that you have done for me over these past two years. I have learned
so much under your supervision, and your willingness to provide countless hours of time to help
me with this thesis is greatly appreciated.
Next, I would like to acknowledge the support from my committee members and say
thank you for all your help.
Dr. Faulkner: you were the first mentor that I ever had in academia. I have learned so
much from you, and continue to learn and be inspired by your work. I am grateful for everything
that you have done for me.
Dr. Jones: I first met you in the third year of my undergraduate studies and I can
truthfully say that you are the reason that I am passionate about studying physical activity and
sedentary behavior in breast cancer survivors. When I first started a research placement with you
in September 2011, I was lost. I did not know what I was interested in, nor did I know what I
wanted to do once I graduated from Kinesiology. You opened my eyes and provided me with the
opportunity to work with breast cancer patients. Through working with these wonderful women,
I developed a passion for the doing the research that I am doing today.
Dr. Trinh: Over the past two years you have been a terrific mentor! I learned so much
about research and academia from you. In addition, I really enjoyed going on multiple coffee
breaks (tea for you)! Whenever I was stressed I would come upstairs and no matter what time it
was, or how busy you were, you would make time for me. You were always able to offer great
guidance and support! Thank you so much!
Finally, I would like to say thank you to my family! You have always supported me and
been there for me when I needed you.
iv
Table of Contents
Abstract……………………………………………………………………………………………i
Acknowledgements………………………………………………………………………………iv
List of Tables…………………………………………………………………………………….vii
List of Appendices………………………………………………………………………………viii
CHAPTER 1………………………………………………………...…………………………….1
Introduction……………..…………………………………………………………………1
CHAPTER 2………………………………………………………………………………………5
Literature Review.....………………………………………………………........................5
Cancer Survivorship ………………………………………………………………………5
Life After Cancer Moving On……………………………………………………………..8
Mental Health in Breast Cancer Survivors: Depression…………………………………10
Physical Activity and Breast Cancer ………………………………………………….....13
Sedentary Behaviour …………………………………………………………………….15
CHAPTER 3……………………………………………………………………………………..23
Manuscript Title Page...………………………………………………………………….23
Abstract...…………………………………………………………………………….…..24
Introduction………………………………………..………..……………………………25
Methods………………………………………………………...………………………...29
v
Results……………………………………………………………………………………35
Discussion……………………………………………………………………..................38
CHAPTER 4……………………………………………………………………………………..48
Conclusions and Future Directions………………………………………………………48
References ………………………………………………………………….....................52
TABLES………..………………………………………………………………..........................72
APPENDICIES………………………………………………………………………………..…78

vi
List of Tables
Table 1: Baseline demographic, medical, sedentary and physical activity descriptives for
participants
Table 2: SITT variables by cluster membership
Table 3: Bivariate correlations by sedentary behaviour cluster membership variables and
self-report/objective moderate-to-vigorous physical activity
Table 4: Bivariate correlations between cluster membership variables and continuous
depression
Table 5: MANOVA and chi square examining medical, demographic and weight status
variables by cluster membership
Table 6: Logistic regression of main Study variables predicting clinical depression
vii
List of Appendices
Appendix A: Sedentary Behaviour Definitions
Appendix B: Descriptive statistics comparing 500 minute accelerometer wear-time and 600
minute accelerometer wear-time
Appendix C: Bivariate correlations comparing 500 minute accelerometer wear-time and 600
minute accelerometer wear-time
Appendix D: Sedentary behaviour frequency (S in the SITT principle) and interruptions (I in
the SITT principle), time (T in the SIIT principle) and type (T in the SITT
principle) using objective and self-report data
Appendix E: Bivariate correlations between demographic and medical covariates
Appendix F: Bivariate correlations between objective sedentary behaviour and measures of
weight status
Appendix G: Bivariate correlations between self-report sedentary behavior and measures of
weight status

1
Chapter 1 Introduction
One in nine Canadian women will be diagnosed with breast cancer in their lifetime making
breast cancer the most common female cancer diagnosis in women (Canadian Cancer Society,
2013). In conjunction with this, the number of breast cancer survivors (BCS) continues to
increase, with the 5-year survival rate being estimated between 80 and 95% (Coleman et al.,
2011). Unfortunately, cancer survival is associated with increased risk of death from noncancer
causes and poorer overall health (Baade, Fritschi, & Eakin, 2006; Lynch, Dunstan, Vallance, &
Owen, 2013). Moreover, cancer survivors are also at risk of developing many long-term
psychological and physiological complications from the disease itself and/or the cancer treatment
profile (Howard-Anderson, Ganz, Bower, & Stanton, 2012; Zainal, Nik-Jaafar, Baharudin,
Sabki, & Ng, 2013). Fortunately, physical activity (PA) has been consistently reported to
alleviate physical and mental health challenges among breast cancer survivors (Brunet, Sabiston,
& Meterissian, 2011; Courneya et al., 2005; Schmitz et al., 2010). Despite this, few BCS engage
in sufficient PA to gain the associated health benefits. Estimates ranging from 50 to 90% of BCS
are not achieving the American College of Sports Medicine (ACSM; (Schmitz et al., 2010))
recommended 150 minutes of moderate-to-vigorous physical activity (MVPA) per week
(Blanchard, Courneya, & Stein, 2008; Lynch et al., 2010; Schmitz et al., 2010). Given the low
levels of MVPA reported and measured among BCS, and challenges associated with uptake and
adherence to MVPA, it may be that other related behaviours need to be targeted to help improve
mental and physical health in this population. Sedentary behaviour is related to, but a distinct
health behaviour from MVPA. Researchers have found relationships between SED and a host of
physical and mental health problems among healthy adults, including having a direct influence
on bone mineral content, vascular health, metabolism and poorer quality of life (Hamer,

2
Coombs, & Stamatakis, 2014; Tremblay, Colley, Saunders, Healy, & Owen, 2010; Wilmot et al.,
2012). While there is limited overall evidence on the health implications of SED among cancer
survivors, high volumes of SED are independently associated with chronic disease-related risk
factors such as central adiposity, elevated blood glucose and insulin as well as poorer physical
functioning and general health in cancer survivors (George et al., 2014; Lynch et al., 2013).
Thus, a new cancer survivorship research agenda is needed to focus on sedentary behaviour
(SED) (Lynch et al., 2013).
SED is defined as any waking behaviour characterized by a low-energy expenditure (i.e.,
≤1.5 resting metabolic equivalents) while in a sitting or reclining posture (Tremblay, 2013).
Researchers on SED have proposed using the SITT principle to describe participant’s SED
(Tremblay et al., 2010). Specifically, SITT refers to Sedentary behaviour frequency (number of
bouts of a certain duration); Interruptions in sedentary behaviour (e.g., getting up from one’s
desk while at work; Healy et al., 2008); Time (the duration of total sitting time); and Type (mode
of sedentary behaviour). As such, SED is multidimensional health behaviour. To date, there is no
evidence of understanding SED using the SITT principle amongst BCS. Thus, one aim of this
current study is to examine and describe the SITT variables in a sample of BCS.
While research on SED is in its infancy, SED has been shown to have a direct influence
on bone mineral content, vascular health, and metabolism among healthy adults (Tremblay et al.,
2010). Increased SED is also associated with increased cancer risk (Matthews et al., 2012). At
this time, there is limited overall evidence on the health implications of SED among cancer
survivors. Nonetheless, it is important to recognize that SED is a distinct entity from PA with
independent and qualitatively different effects on physical function, metabolism, and health
outcomes, which must be treated separately from a lack of PA (Hamilton, Hamilton, & Zderic,

3
2004; Hamilton, Healy, Dunstan, Zderic, & Owen, 2008; Sallis, Owen, & Fotheringham, 2000;
Tremblay et al., 2010). To date, some hypothesized biological mechanisms have been proposed
to better understand the association between SED and various health outcomes. For example,
Lynch (2010) proposed a framework to better understand these complex relationships. Within
this framework and the well-established evidence that SED is independently associated with
central adiposity, elevated blood glucose/insulin, and a number of cardiometabolic outcomes,
Lynch believes that a bidirectional relationship between SED and metabolic attributes exist
which are then responsible for cancer progression. The strongest evidence exists to support a
bidirectional relationship between SED and adiposity when compared to other metabolic
attributes (i.e., sex hormones, inflammation, vitamin D; Lynch, 2010). Using Lynch’s (2010)
proposition, SED may be linked to physical and mental health problems among BCS. Depression
is a prominent mental health factor for BCS that may be linked to SED.
Symptom reporting of depression is a common comorbidity associated with cancer
survival (Harrington, Hansen, Moskowitz, Todd, & Feuerstein, 2010), and is thought to be
under-reported in BCS with an estimated 10-25% of women reporting depression (Burgess et al.,
2005; Qiu et al., 2012; Zainal et al., 2013). Depression is an important mental health factor to
reduce because it has been linked to cardiac mortality, stroke, hypertension, heart disease, type 2
diabetes, anxiety disorders, insomnia and cancer (Archer et al., 2012; Black, Markides, & Ray,
2003; Eaton, Armenian, Gallo, Pratt, & Ford, 1996; Jonas & Lando, 2015; Kim et al., 2009;
Ladwig, Röll, Breithardt, Budde, & Borggrefe, 1994; Mendes de Leon et al., 1998; Penninx et
al., 1998, 2001). The associations between some SED facets and depression in BCS have been
studied with mixed results (Rogers, Markwell, Courneya, McAuley, & Verhulst, 2011; Trinh,
Amireault, Lacombe, & Sabiston, 2015). In a cross-sectional study examining daily sitting time
and fatigue and depression, rural living survivors had a significant increase in fatigue with
4
increased SED but no association between depression and increased SED (Rogers et al., 2011).
Furthermore, Trinh and colleagues (2015) found a MVPA by SED interaction effect such that
lower MVPA and higher SED were associated with higher pain, fatigue, and depression in a
sample of BCS. Based on these findings, there may be some association between specific SED
facets and depression. However, researchers have not explored all dimensions of SED and the
link to depression.
Thus, this study has three objectives. The first objective is to better understand the SED
profile of BCS using the SITT principle. Along with this first objective, the multiple dimensions
of SED will be examined as grouping factors to classify survivors based on their SED. The
second objective is to examine personal and cancer-specific factors that distinguish the clusters
of SED. The third objective is to examine the association between SED and depression among
BCS.

5
Chapter 2 Review of Literature
One in nine Canadian women will be diagnosed with breast cancer in their lifetime
(Canadian Cancer Society, 2013). In 2013, 12,200 new cases of breast cancer in Canada were
reported, and breast cancer continues to be the most common cancer diagnosis in women
(Canadian Cancer Society, 2013). Breast cancer is most prevalent in females aged 50 to 69 years
(52% of diagnoses), with 30% of cases being in women over the age of 69 years (Canadian
Cancer Society, 2013). Despite this, early detection strategies and better treatment opportunities
have led to a substantial increase in the number of breast cancer survivors (BCS) with five-year
survival rates estimated between 80 and 95% (Coleman et al., 2011). Moreover, the female
breast cancer mortality rate has been steadily declining since the mid-1980’s (Canadian Cancer
Society, 2013). A number of hypotheses have been proposed as to why this downward trend is
being observed, but at present, it appears that increased mammography screening (Shields &
Wilkins, 2009) and the use of more effective therapies following surgery (Edwards et al., 2005;
Mariotto, 2002) are the two factors most responsible for the decline. As a result, in recent years
there has been an emphasis placed on the importance of the survivorship period and both the
physiological and psychosocial outcomes for women treated for breast cancer (Lynch et al.,
2013; Lynch, 2010).
Cancer Survivorship
In 1985, Dr. Mullan, a cancer survivor and physician, wrote the first paper in the New
England Journal of Medicine introducing the term “survivor” to describe cancer patients
(Mullan, 1985). A widespread belief of cancer survival at this time was that once an individual
was treated for cancer they were either “cured” or “living with overt or covert disease”
(Feuerstein, 2007; Mullan, 1985). Based on discussions with other cancer survivors and his

6
personal experience, Mullan believed that survivorship was not this binary experience but
instead a process and far more complex experience, he termed “survival” (Feuerstein, 2007;
Mullan, 1985). Furthermore, Mullan was the first to suggest that, “survivorship should be studied
as a phenomenon in itself rather than a by-product or afterthought of basic research or cancer
treatment” (Feuerstein, 2007). Mullan suggested that survival should be divided into three
distinct phases (Ristovski-Slijepcevic & Bell, 2014). First, a survivor enters the acute survival
period, which is immediately following diagnosis and is focused on surviving treatment
(Ristovski-Slijepcevic & Bell, 2014). Next, a survivor enters the extended survival period, which
is the period after treatment completion and focuses on dealing with the physical and
psychological consequences of treatment (Ristovski-Slijepcevic & Bell, 2014). Finally, a
survivor enters the permanent survival phase, where recurrence seems unlikely, and the survivor
focuses on the long-term effects of treatment (Ristovski-Slijepcevic & Bell, 2014). Building off
the work by Mullan, Aziz (2002) noted that survivorship needs to account for both late and long-
term effects of cancer and not just the effects of primary treatment on the well-being and health
of survivors. While the National Coalition for Cancer Survivorship (NCCS) defined a cancer
survivor as any person diagnosed with cancer, from the time of initial diagnosis until his or her
death (Khan, Rose, & Evans, 2012), it is important to examine survivorship in phases when
targeting health behaviours given the unique experiences that occur during treatment compared
to post-treatment. This definition is also extended out from the patient themselves to the family
and social support network surrounding the patient (Khan et al., 2012). In the current study, BCS
are studied in the ‘extended survivor’ phase of the survivorship trajectory (Ristovski-Slijepcevic
& Bell, 2014).
Approximately 90% of women in developed countries, such as Canada, are expected to
survive cancer for at least five years (Canadian Cancer Society, 2013). As such, women with a

7
history of breast cancer are the largest group of cancer survivors (Canadian Cancer Society,
2013). Unfortunately, cancer survival is associated with decrements in health status and
increased risk of death from noncancer causes (Baade et al., 2006; Lynch et al., 2013). The
burden of cancer survival includes premature death from comorbid chronic diseases, such as,
type 2 diabetes and cardiovascular disease (Demark-Wahnefried Pinto, & Gritz, 2006; Lynch et
al., 2013) and generally increased susceptibility to chronic diseases. Additionally, those who are
cancer-free for a minimum of 5 years after their diagnoses may be at a risk of developing long-
term psychological complications from the disease itself and/or the treatments such as
radiotherapy, chemotherapy, mastectomy (Howard-Anderson et al., 2012; Zuraida-Zinal et al.,
2013). For example, Deimling and colleagues (2005) showed that one-third of long-term
survivors (5 + years) reported worries about cancer reoccurrence, worries about developing a
second cancer, and worries that symptoms they experience on a daily basis may be from cancer.
Additionally, cancer-related worries significantly predicted depression and anxiety.
Many BCS experience long-term chronic physical symptoms as a result of the
multifaceted sequelae of breast cancer (Alfano et al., 2007). The period of survival after active
treatment is completed brings a number of unique physical health challenges (Baade et al., 2006;
Alfano et al., 2007; Lynch et al., 2013). These physical symptoms include: fatigue (Barton-
Burke, 2006; Bowen, Alfano, McGregor, Kuniyuki, Bernstien, & Meeske, et al, 2007), hormone-
related symptoms (Carpenter & Andrykowski, 1999; Ganz, Desmond, Leedham, Meyerowitz, &
Wyatt, 1998), chronic pain and sensation’s in the arm or breast that was treated (Erickson,
Pearson, Ganz, Adams, & Kahn, 2001), and sexual dysfunction (Ganz et al., 2002; Kornblith,
Herndon, Weiss, Zhang, Zuckerman, & Rosenberg, et al, 2003; Alfano et al., 2007). These
symptoms are common with fatigue and pain estimated to effect one-third of all survivors
(Kornblith et al., 2003; Bower, Ganz, Desmond, Bernaards, Rowland, Meyerowitz, et al., 2006;

8
Alfano et al., 2007) and sexual dysfunction estimated to effect 20-30% of all survivors
(Kornblith et al., 2003; Alfano et al., 2007). Symptoms that are commonly reported as a result of
undergoing hormone-replacement therapy include vasomotor complaints (sweats, hot flashes,
palpitations), urinary problems, vaginal dryness, and cognitive/mood changes (Carpenter et al.,
1999; Alfano et al., 2007). Although this thesis will focus on psychological symptom reporting,
specifically depression, chronic physical symptoms can serve as a continuous reminder of cancer
and thus result in significant psychological morbidity, including depression, for as much as 20
years post-treatment (Deimling et al., 2002; Kornblith et al., 2003; Alfano et al., 2007). Physical
activity has been shown to consistently improve many of these physical and psychological
symptoms in healthy adults (Alfano et al., 2007; Lynch et al., 2013), however how these
symptoms are associated with SED remains understudied, and inconclusive in BCS.
Life After Cancer Moving On Dataset
To date, 10 research articles have been published using the “Life After Breast Cancer:
Moving On” dataset. This comprehensive longitudinal study examines the physical,
psychological and behavioural activities/symptoms of female breast cancer survivors.
Topics examined using this dataset include:
1. The role of physical activity as a potential mediator between pain and mental health
(Sabiston, Brunet, & Burke, 2012);
2. PA and psychological health explored using Basic Psychological Needs Theory (Mack,
Meldrum, Wilson & Sabiston 2013);
3. The role of social support and stress in examining changes in post-traumatic growth and
subjective well-being (McDonough, Sabiston, & Wrosch, 2015);

9
4. Investigating the relationship between self-presentation process and physical activity
(Brunet, Sabiston, & Gaudreau, 2012);
5. Examining PA and SED using objective measures during the early survivorship period
(Sabiston, Brunet, Vallance, & Meterissian, 2014);
6. Systemic inflammation and the role of goal disengagement and health-related self-
protection (Castonguay, Wrosch, & Sabiston, 2014);
7. Identification and prediction of PA trajectories (Brunet, Amireault, Chaiton, & Sabiston,
2014);
8. Examining how being self-determined increases physical activity and well-being (Brunet,
Burke, & Sabiston, 2013);
9. Validating the Godin-Shephard Leisure-Time PA questionnaire using accelerometry
(Amireault, Godin, Lacombe, & Sabiston, 2015); and
10. Interactions between PA and SED as they relate to physical and psychological health
(Trinh, Amireault, Lacombe, & Sabiston, 2015).
Worth noting; a recent cross-sectional baseline examination using self-report measures of
pain, fatigue and depression, as well as, objective PA and SED found that lower levels of MVPA
and higher levels of SED significantly predicted higher levels of fatigue (p <.001), but not higher
levels of pain (p = .06) or depression (p = .08) (Trinh et al., 2015). When higher levels of MVPA
and higher levels of SED were explored, no association with these symptoms existed (Trinh et
al., 2015). This study provided an important examination into the potential interactive effect
between SED and PA in BCS and how this interaction may be associated with symptom
reporting pain, fatigue and depression. To expand and examine a different research question this
thesis will use a prospective study design opposed to a cross-sectional research design as is seen
in this work. In addition, a cut-off score to indicate clinical depression using a valid measure will
10
be used opposed the continuous measure of depression. The measure of depression is different
(i.e., Trinh et al. reported on dysphoria using the Profile of Mood States compared to the current
study using the Centers for Epidemiological Studies – Depression measure). Moreover,
additional participant data will be added and examined, and all data will be extracted from raw
data and re-cleaned using stringent criteria. Finally, this thesis will focus only on SED, using
both self-report and objective measures and thus will not examine the interactive effect of PA
and SED as is seen in the Trinh and colleagues (2015) study.
Mental health in BCS: Depression
There is a number of different definitions of depression in the literature and the most
commonly used diagnostic criteria tool for clinical depression is that of the Diagnostic and
Statistical Manual of Mental Disorders (DSM, 2013) The DSM criteria required to be diagnosed
with major depressive disorder is as follows:
1. Depressed mood or a loss of interest or pleasure in daily activities for more than 2 weeks,
2. Mood represents a change from the person’s baseline,
3. Impaired function: social, occupational or educational,
4. Specific symptoms of at least 5 of the 8 following,
i) depressed mood or irritable
ii) decreased interest or pleasure
iii) significant weight change (5%) or change in appetite
iv) change in sleep
v) change in activity
vi) fatigue or loss of energy
11
vii) guilt/worthlessness
viii) decreased concentration
ix) suicidality (DSM, 2013).
In Western societies, yearly incidence rates of depression for adults are between 3%-5%
with an estimated 17% of people experiencing depression in their lifetime (Andrews, Henderson,
& Hall, 2001; Blazer, Kessler, McGonagle, & Swartz, 1994; Krogh, Nordentoft, Sterne, &
Lawlor, 2011; Lépine, Gastpar, Mendlewicz, & Tylee, 1997; Spaner, Bland, & Newman, 1994).
Moreover, the World Health Organization estimates that unipolar depression is the fourth leading
cause of burden and years lost in healthy adults, with major depression accounting for 12% of all
total years lived with disability (Krogh et al., 2011; Ustün, Ayuso-Mateos, Chatterji, Mathers, &
Murray, 2004). To date, depression is under reported in BCS, with prevalence varying between
10% and 25% (Burgess et al., 2005; Qiu et al., 2012; Zainal et al., 2013). In a recent systematic
review of BCS, Zainal and colleagues (2013) concluded that depression has not been studied
adequately and reported that prevalence varies across the extreme of 1-56% depending on how it
is defined. This is mainly due to the number of different measurement instruments that have been
validated to assess depression in cancer survivors. From this systematic review, Zainal and
colleagues (2013) recommended that the Center for Epidemiological Studies Depression Scale
(CES-D;(Radloff, 1977)), which is a self-report questionnaire, deriving questions from the DSM
is a valid and reliable screening tool for BCS.
There are number of possible biological and psychological mechanisms to explain how
reducing SED and increasing PA might act as an antidepressant (Krogh et al., 2011). In animal
models, increasing PA has led to an increase in neurogenesis (Bjørnebekk, Mathé, & Brené,
2005) and increased levels of serotonin (Gomez-Merino, Béquet, Berthelot, Chennaoui, &

12
Guezennec, 2001), resulting in an antidepressant response (Krogh et al., 2011). When examining
non-biological mechanisms, studies have shown that depressed individuals who exercise
regularly might receive positive feedback/compliments from other individuals who exercise with
them, resulting in increased self-esteem or as a diversion from negative feelings and thoughts
(Krogh et al., 2011; Nolen-Hoeksema & Morrow, 1993). Alternatively, regular exercise in 24
BCS’s has led to a decrease in depression and potential therapeutic effect (Segar et al., 1998).
Among BCS, depression has been correlated with a number of demographic characteristics, such
as, age (Burgess et al., 2005), income level (Casso, Buist, & Taplin, 2004), and education status
(Casso et al., 2004). Furthermore, depression is associated with cancer or treatment (Casso et al.,
2004), symptoms, such as pain (Casso et al., 2004; Kim et al., 2008), and a number of
psychosocial factors, including social support, hopelessness/helplessness, and loss of control
(Bardwell et al., 2006; Kim et al., 2008). Long term effects associated with depression include
cancer treatment, specifically chemotherapy, sexual dysfunction, infertility, menopause-
associated health problems such as cardiovascular disease, and osteoporosis (Azim, de
Azambuja, Colozza, Bines, & Piccart, 2011; Lorizio et al., 2012; Zainal et al., 2013). Moreover,
patients can be prescribed tamoxifen, a drug used for treatment of breast cancer, which has also
been associated with increased risk for depression (Lorizio et al., 2012; Zuraida-Zinal et al.,
2013). Furthermore, inactive and highly sedentary cancer survivors may also be at risk for
depression (Roshanaei-Moghaddam, Katon, & Russo, 2009). Nonetheless, reviews of the
association between physical activity and depression in healthy adults suggest that there is a
protective effect of being physically active on the risk for developing depression (Teychenne and
colleagues (2010); Mammen & Faulkner (2013)). As such, it may be of interest to study the
protective effects of behaviours such as physical activity and sedentary behaviour among BCS to
help reduce the risk for, and burden associated with, depression symptoms.

13
Physical Activity and Breast Cancer
Regular moderate-intensity PA, such as brisk walking, has been shown to be associated
with diminished treatment side effects, enhanced quality of life (Courneya et al., 2005; Lynch,
Cerin, Owen, Hawkes, & Aitken, 2008), and prolonged survival (Haydon, Macinnis, English, &
Giles, 2006; Holmes, Chen, Feskanich, Kroenke, & Colditz, 2005; Meyerhardt et al., 2006).
Furthermore, a systematic review by Speck and colleagues (2010) found that regular PA
decreased depression and reduced fatigue in BCS and, a recent meta-analysis also found that
higher PA levels were correlated with reduced breast cancer mortality and overall mortality in
BCS (Ballard-Barbash et al., 2012). Overall, there is a myriad of positive benefits associated
with PA participation among BCS that have physiological (e.g., improved cardiovascular
function, aerobic fitness, blood pressure, etc.), psychological (e.g., reduced depression, anxiety,
improved body image, etc.), and social (e.g., improved connectedness, support, etc.)
underpinnings (Sabiston & Brunet, 2011).
In spite of the positive outcomes associated with PA, and research that has demonstrated
it is feasible, safe, and effective, a large number of survivors are not meeting physical activity
guidelines recommended to achieve a number of health benefits (Schmitz et al., 2010; Speck et
al., 2010). The American College of Sports Medicine (ACSM; (Schmitz et al., 2010)) has a set of
exercise guidelines specifically designed for individuals with cancer, suggesting that cancer
survivors should aim to complete at least 150 minutes of moderate-to-vigorous physical activity
(MVPA) per week. Specifically, cancer survivors should strive to increase aerobic exercise to 3-
5 times per week and also introduce resistance training into their regime 2-3 times per week, and
flexibility exercises should be done daily. Unfortunately, BCS report lower PA levels compared
to a sample of females without cancer (Ballard-Barbash et al., 2012), and are generally quite

14
inactive with rates ranging from 50 to 90% of women not meeting recommended PA levels of
150 minutes of MVPA each week (Blanchard et al., 2008; Lynch et al., 2010). In the first study
to describe PA using objective measures, Lynch and colleagues (2010) found that after 7 days of
monitoring, BCS (n= 111) spent 31.5% of their day engaged in light activities and only 0.5% of
their day engaged in MVPA. Similarly, a recent imputation-based approach comparing estimates
of activity level amongst BCS (n=398) and healthy controls (n=1120) found that, on average,
BCS spent 31.1% in light activity and 2.6% in MVPA (Phillips et al., 2015). Trinh and
colleagues (2015) also reported low PA of less than 2% of the day spent in MVPA in a sample of
BCS. Notwithstanding these poor rates of PA among BCS, the healthy adult population is no
better. Generally, adults spend less than 5% of their waking hours engaged in MVPA and 25% of
their time engaged in light activities (Healy, Wijndaele, et al., 2008; Matthews et al., 2012).
Light-intensity activities make up the majority of time where older adults find
themselves exercising, spending more time in daily light PA than any other age group (Buman et
al., 2010). Interestingly, when PA and physiological changes/health outcomes are studied across
different intensities (light, moderate and vigorous), a curvilinear relationship is observed for a
variety of diseases with the steepest gradient observed at the lowest end of activity (Powell,
Paluch, & Blair, 2011). This suggests that something is better than nothing and given the large
proportion of older adults who fall into the lowest end of the PA scale, relatively small increases
in daily PA will bring substantial health benefits, even if one does not meet the recommended
daily guidelines (Matthews et al., 2008; Powell et al., 2011; Troiano et al., 2008). In older adults,
easy walking is reported as the most common light PA (Buman et al., 2010; Westerterp, 2008). A
recent meta-analysis examining walking and all-cause mortality, reported that daily walking for
3 hours/week at 3 kilometres/hour results in a 20% risk reduction of all-cause mortality (M
Hamer & Chida, 2008; Woodcock, Franco, Orsini, & Roberts, 2011). In addition, replacing

15
sedentary time with equal amounts 30 minutes/day with light PA yields better physical health
and well-being overall (Buman et al., 2010).
Given the low levels of physical activity reported and measured among BCS, there is a
gap in the understanding of this health behaviour. It is likely that there is too much emphasis on
higher intensity PA at the expense of better understanding other related health behaviours.
Sedentary behaviour (SED) is related to, but distinct health behaviour from MVPA that has only
been recently introduced as an independent behaviour that may have unique health outcomes.
Sedentary Behaviour
Lynch and colleagues (2013) suggested that a new cancer survivorship research agenda is
needed to focus on sedentary behaviour (SED). Sedentary behaviour is defined as any waking
behaviour characterized by a low-energy expenditure (i.e., ≤1.5 resting metabolic equivalents)
while in a sitting or reclining posture (Tremblay, 2013). Researchers have advocated that SED
should be identified as a distinct behaviour from PA with independent and qualitatively different
effects on physical function, metabolism, and health outcomes (Hamilton et al., 2004, 2008;
Sallis et al., 2000; Tremblay et al., 2010). Unfortunately, at this point in time there are no
published guidelines pertaining to SED for adults regardless of health status.
Definition and measurement of SED. Similar to the FITT formula used to study PA
(Frequency, Intensity, Time (duration), and Type of activity), Tremblay and colleagues (2010)
propose using the SITT formula to describe participant’s SED. This acronym corresponds to the
following:
• Sedentary behaviour frequency (number of bouts of a certain duration);
• Interruptions in sedentary behaviour (e.g., getting up from one’s desk while at work;

16
Healy et al., 2008);
• Time (the duration of total sitting time); and
• Type (mode of sedentary behaviour, e.g., sitting at one’s desk, TV viewing, or
driving a car).
Methods used to assess SED using the SITT require the use of both self-report
questionnaires to assess aspects related to Type and Time, and objective tools to assess SED
frequency, Interruptions, and Time. In a systematic review of SED in longitudinal studies, Thorp
and colleagues (2011) recommended the use of device-based measures to provide a clear
understanding of the impact of SED. One method to measure objective SED is to use an
accelerometer. An accelerometer is a device that measures movement of the body in space and
also the individual’s intensity, duration, frequency, and patterns of movement (Tremblay et al.,
2010). Additionally, the inclinometer feature on some accelerometers can indicate whether a
participant is standing, sitting or lying down when the device is worn at the hip. At this time, the
ActiGraph GT3X remains one of the best accelerometers to measure both PA and SED and the
GT3X is an improvement from the previous biaxial, antero-posterior GT1M accelerometer
(Hänggi, Phillips, & Rowlands, 2013). Furthermore, the inclusion of the inclinometer on the
GT3X allows researchers to accurately measure individuals SED (Hänggi et al., 2012). This is
supported by a plethora of recent studies, which have concluded that triaxial accelerometers are
more sensitive than uniaxial and biaxial accelerometers (Coleman et al., 2011; Eston, Rowlands,
& Ingledew, 1998; Trost, Mciver, & Pate, 2005). In a recent report by Verloigne and colleagues
(2012), the authors concluded that accelerometry should be used when studying the possible
effect of SED on health. These researchers sampled 672 children and assessed their sedentary
time using both accelerometry and self-report. Importantly, these authors showed that self-
reported TV and computer time did not effectively reflect total sedentary time compared to

17
accelerometers (Verloigne et al., 2012). Despite these findings, it appears that the best method of
assessing SED is using a combined approach similar to the SITT principle outlined above
(Prince, Saunders, Gresty, & Reid, 2014). For example, when self-report time in SED is
compared to objectively measured SED, only a low to moderate correlation is observed
(Saunders, Prince, & Tremblay, 2011). However, there are stronger associations among
construct-specific associations such as when specific domains of self-reported SED (i.e., TV
viewing) are compared with objective measures of SED (Healy et al., 2011; Saunders et al.,
2011).
SED and health outcomes. While research on SED is in its infancy, in the general
population, SED has been shown to have a direct influence on bone mineral content, vascular
health, and metabolism among healthy adults (Tremblay et al., 2010). Furthermore, a systematic
review of prospective studies (n= 19) examining adult SED and health outcomes found that there
is moderate evidence for a positive association between SED (time spent sitting) and risk for
type 2 diabetes (Proper, Singh, Van Mechelen, & Chinapaw, 2011). Additionally, strong
evidence appears to exist linking SED to all-cause and cardiovascular disease mortality and there
is also evidence of significant associations between SED and overall cancer mortality (Matthews
et al., 2012). Moreover, a systematic review of longitudinal studies (n= 48) between 1996-2011
found a consistent relationship between SED and weight gain from childhood to adulthood
(Thorp et al., 2011). Both of these reviews are supported by a recent systematic review of 24
studies, which also found strong evidence that increased SED is related to all-cause mortality
risk in older adults (Rezende, Rodrigues Lopes, Rey-López, Matsudo, & Luiz, 2014). This
review also found moderate evidence that SED is related to obesity, waist circumference, and
metabolic syndrome (Rezende et al., 2014). Unfortunately, a criticism of these reviews and the
literature to date is that self-report measures of SED tend to be used. For example, of the 48

18
studies included in the Thorp and colleagues review, 46 of these studies used a self-report
measure of SED. Furthermore, many of the studies reviewed focus on a unidimensional SED
construct with little regard to the potential different dimensions as defined using the SITT
principle. As such, there is value in studying the potential multiple dimensions of SED using
objective measures such as inclinometers and accelerometers. Finally, there are few studies
focused on cancer survivors.
At this time the majority of work done pertaining to SED has been completed in children
and adolescents. In these groups there are clear SED guidelines (Tremblay et al., 2011) and
research on various bout and break lengths has been completed, whereby frequently breaking
SED may be a more important overall measure then examining specific bout lengths (Carson &
Janssen, 2011; Cliff et al., 2014; Travis John Saunders et al., 2013). In adults using the NHANES
survey data from 2003-2006, adults reported on average 92.5 breaks (interruptions) and a higher
number of breaks in SED was associated with better C-reactive protein (immune function)
outcomes and waist circumference (Healy, Matthews, Dunstan, Winkler, & Owen, 2011). In a
cross-sectional study of 197 overweight/obese women, researchers collected length of bouts of
SED lasting ≥ 10, ≥ 30 and ≥ 60 minutes as well as the mean length of breaks as different
measures of SED (Baruth, Sharpe, Hutto, Wilcox, & Warren, 2013). On average, women spent
544.1 minutes per day engaged in sedentary pursuits (Baruth et al., 2013). Furthermore, many
women engaged in multiple bouts lasting ≥ 10 and ≥ 30 minutes, however a great deal of data
was not recorded when ≥ 60 minutes bouts were considered, meaning that participants did not
have a large number of SED bouts lasting 60 minutes or longer. Thus, it would appear that when
choosing appropriate bout lengths to use in analysis for women, one should not include 60-
minute bout lengths but instead focus on 10 and 30 minute bout lengths.

19
SED and BCS. Researchers have shown that BCS spend an average of 66 to nearly 80%
of their day sedentary, primarily sitting (Lynch et al., 2013; Phillips et al., 2015; Trinh,
Amireault, et al., 2015). Compared with women and men over 60 years of age from the National
Health and Nutrition Examination Survey (NHANES) population, both breast and prostate
cancer survivors spent less time physically active (light, moderate, and vigorously active) and
more time sedentary, compared to non-cancer controls (Lynch et al., 2013). Using
accelerometers with 14 hours of wear-time per day, survivors accumulated approximately 9.5
hours of daily sedentary time (Lynch et al., 2013). This is slightly more time spent in SED
compared to data from the NHANES survey that found in the general population adults over the
age of 20 years spend approximately 8.4 hours/day sedentary (Healy et al., 2011). These findings
are supported by a recent report by Brunet and colleagues (2014) which followed 177 BCS
during a yearlong period following completion of primary treatment. Objective measures of
sedentary time and MVPA were collected using the ActiGraph GT3X accelerometer. In this
group, survivors spent 78% of their waking hours engaged in SED and only 2% of their day
engaged in MVPA (Brunet et al., 2014). Moreover, a recent study of 398 BCS (Mage = 56.95
years) reported that BCS spent 66.4% of their waking hours engaged in SED (Phillips et al.,
2015). In addition, BCS’s SED remained relatively stable over the 12-month period, and when
trends were observed, these trends were more pronounced in women who were overweight
(Brunet et al., 2014).
Importantly, to date, no work has examined specifically how different bout lengths of
SED might impact physical and/or psychological health symptoms in cancer survivors. While
there is limited overall evidence on the health implications of SED among cancer survivors, high
volumes of SED in this clinical population are independently associated with chronic disease-
related risk factors such as central adiposity, elevated blood glucose and insulin (Lynch et al.,
20
2013). The most detailed systematic review of SED and cancer to date was conducted by Brigid
Lynch (2010). Lynch reviewed all available literature pertaining to SED and cancer and
identified 11 articles that examined the association between SED and cancer risk. One study was
focused on breast cancer risk, whereby the authors assessed SED using TV viewing time and
found null findings between both weekday and weekend viewing time with cancer risk (Mathew
et al., 2009). Overall, at this time there is a lack of SED interventions examining potential
associations with mental health variables in clinical populations such as women diagnosed and
treated for breast cancer.
Specifically related to mental health outcomes in BCS, two American studies and one
Canadian study have considered the associations between SED and mental health. Cross-
sectional work (n=483) examining daily sitting time and fatigue, as well as, depression found
that rural living survivors had a significant increase in fatigue with increased SED but no
association between depression and increased SED (Rogers et al., 2011). Prospective analysis of
710 BCS from the HEAL study found time spent engaged in SED was not associated with
quality of life or fatigue (George et al., 2012). Finally, a recent study of 195 BCS found MVPA
by SED had a significant interaction effect when examining associations with pain, fatigue, and
depression (Trinh, Amireault, et al., 2015). However, in women with lower levels of MVPA,
simple slopes analysis showed that high levels of SED significantly predicted higher levels of
fatigue, and higher levels of depression. Moreover, these associations between SED and health
outcomes were not observed when higher levels of MVPA were considered (Trinh et al., 2015).
Researchers have also suggested that depression and SED have a bidirectional relationship,
however, much more research needs to be conducted (Roshanaei-Moghaddam et al., 2009). For
example, the causality mechanism that links SED and depression remains unknown.
21
To date, no studies have explored the association between SED and clinical depression in
BCS using a validated depression screening tool (Andresen, Malmgren, Carter, & Patrick, 1994)
and this research is imperative. Breast cancer remains the most common cancer diagnosis in
women, with survival estimates increasing every year (Canadian Cancer Society, 2013). With
survivors living longer, much more research needs to be conducted examining how certain
common co-morbidities (i.e., depression) can be reduced through easy to implement, cost-
effective, behavioural change interventions such as reducing SED. Psychosocial researchers have
identified SED as one of the top 10 most important research topics to examine in the field of
physical activity and cancer survivorship (Courneya, Rogers, Campbell, Vallance, &
Friedenreich, 2015) and this prospective study will begin to provide recommendations for SED
and clinical depression in BCS.
Thus, this study has three main research objectives. The first objective is to better
understand the SED profile of BCS using the SITT principle. Along with this first objective, the
multiple dimensions of SED will be examined as grouping factors to classify survivors based on
their SED. The second objective is to examine personal and cancer-specific factors that
distinguish the clusters of SED. Based on previous research with SED and more prominently
with PA, it is expected that age, weight status, and potentially some cancer-related variables such
as treatments endured will be important factors differentiating the SED clusters. It is
hypothesized that those who are most SED will be older and have a higher body mass index
(BMI ( Demark-Wahnefried et al., 2001; Kroenke, Chen, Rosner, & Holmes, 2005; Patterson,
Cadmus, Emond, & Pierce, 2010). Furthermore, women who have undergone surgical removal
of the axillary lymph node have been shown to be less active than those who have not (Sagen,
Kåresen, & Risberg, 2009) and undergoing chemotherapy or radiation therapy during treatment
can make survivors less active due to high levels of fatigue (Demark-Wahnefried, Hars, et al.,

22
1997; Irwin et al., 2003). As a result it was hypothesized that these demographic/medical and
treatment outcomes may be associated with increased SED. The third objective is to examine the
association between SED and depression among BCS during the early survivorship period. This
time period is generally understudied and can be a good time to intervene and teach new health
behaviours (Brunet et al., 2014). It is hypothesized that those reporting higher SED, as measured
through cluster membership and those with the highest SED facets, will be significantly
associated with higher depression.

23
Chapter 3 Thesis Manuscript
Profiling sedentary behaviour in breast cancer survivors: Links with depression during the
early survivorship period
Jason Lacombe, BKIN Faculty of Kinesiology and Physical Education,
University of Toronto, 55 Harbord Street, Toronto, Ontario, Canada, M5S 2W6
Guy Faulkner, PhD Faculty of Kinesiology and Physical Education,
University of Toronto, 55 Harbord Street, Toronto, Ontario, Canada, M5S 2W6
Jennifer Jones, PhD Associate Director, ELLICSR,
Princess Margaret Cancer Centre
Linda Trinh, PhD Faculty of Kinesiology and Physical Education,
University of Toronto, 55 Harbord Street, Toronto, Ontario, Canada, M5S 2W6
Catherine Sabiston, PhD (Corresponding Author) Faculty of Kinesiology and Physical Education,
University of Toronto, 55 Harbord Street, Toronto, Ontario, Canada, M5S 2W6
Email: [email protected]
ACKNOWLEDGEMENTS:
This study was funded by a Canadian Institutes of Health (CIHR) Research Operating Grant (grant#186128) awarded to CMS. During the time of data analysis, LT was supported by a research trainee award from the Kidney Cancer Research Network of Canada (KCRNC). JL was supported by a Sir Frederick Banting and Charles Best Canada Graduate Scholarship-Master’s from CIHR and the Psychosocial Oncology Research Training Program (PORT)-Master’s. GF hold a CIHR Applied Public Health Chair. CMS holds a Canada Research Chair in Physical Activity and Mental Health.

24
ABSTRACT
Background: Symptoms of depression remain under diagnosed but highly prevalent in breast
cancer survivors (BCS). Reducing sedentary behaviour (SED) during the early survivorship
period may be a strategy for treating clinical depression in survivors.
Methods: One hundred and eighty-seven BCS provided baseline demographic, medical, and
SED/physical activity data. Depression was reported three months later. Multiple dimensions of
SED were identified and examined in cluster analysis. The association between cluster
membership and depression was assessed using logistic regression.
Results: Two SED groups were identified representing higher and lower SED. High SED cluster
BCS’s were significantly older, heavier, less physically active, less educated, and were more
likely to have undergone lymph/axial node dissection. In the logistic regression model cluster
membership was a significant predictor of clinical depression.
Conclusions: Reducing dimensions of SED during the early survivorship period could protect
from clinical depression symptoms.

25
INTRODUCTION
Breast cancer continues to be the most diagnosed and prevalent cancer in women,
affecting approximately one in nine Canadian females (Canadian cancer society, 2013).
Fortunately, five-year survival rates are estimated to be between 80-95% (Coleman et al., 2011).
Although the number of breast cancer survivors (BCS) is increasing each year, cancer survival is
associated with an increased risk of psychological and physiological complications from the
disease itself and/or the treatment experienced (Howard-Anderson et al., 2012; Zainal et al.,
2013). Specifically, BCS tend to be sedentary, overweight/obese and older (Demark-Wahnefried
et al., 2001; Kroenke, Chen, Rosner, & Holmes, 2005; Patterson et al., 2010). Furthermore, a
diagnosis of breast cancer increases risk for mental health problems such as depression (Fann et
al., 2008). Depression is one of the most common comorbidities associated with cancer survival
(Harrington et al., 2010), and may be under-reported in BCS with an estimated 10 to 25% of
survivors reporting depression (Burgess et al., 2005; Fann et al., 2008; Qiu et al., 2012; Zainal et
al., 2013). Identifying factors that help protect from the deleterious mental health challenges
among BCS is an important public health agenda.
Physical activity (PA) has been consistently shown to alleviate many physical and mental
health challenges among BCS (Courneya et al., 2005; Sabiston & Brunet, 2011; Speck et al.,
2010), including but not limited to, diminished treatment side effects, enhanced quality of life
(Courneya et al., 2005; Lynch et al., 2008), and prolonged survival (Haydon et al., 2006; Holmes
et al., 2005; Meyerhardt et al., 2006). Moreover, compared to those women who do not exercise
regularly, active BCS are significantly less depressed (Segar et al., 1998). Notwithstanding these
findings, BCS are inactive with 50-90% of survivors not meeting healthy activity guidelines
(Blanchard et al., 2008; Lynch et al., 2010, 2013; Speck et al., 2010). Specifically, the American

26
Cancer Society (Rock et al., 2012) and the American College of Sports Medicine (Schmitz et al.,
2010) recommend PA guidelines of 150 minutes of moderate-to-vigorous physical activity
(MVPA), 75 minutes weekly of vigorous aerobic physical activity and muscle-strengthening
exercises 2 times per week. Given the low levels of PA among BCS, and that PA behaviours
only occur during a fraction of one’s day, it may be more effective to intervene with other health
risk behaviours (Lynch et al., 2013). Specifically, Lynch and colleagues (2013) have proposed a
research agenda to highlight the importance of targeting sedentary behaviour.
Sedentary behaviour (SED) is defined as any waking behaviour characterized by a low-
energy expenditure (i.e., ≤1.5 resting metabolic equivalents) while in a sitting or reclining
posture (Tremblay, 2013). Importantly, SED is a distinct entity from PA with independent and
qualitatively different effects on physical function, metabolism, and health outcomes (Hamilton
et al., 2004, 2008; Sabiston, Brunet, Vallance, & Meterissian, 2014; Trinh et al., 2015).
Sedentary behaviour has been shown to have a direct influence on bone mineral content, vascular
health, and metabolism among healthy adults (Tremblay et al., 2010) and high SED is also
associated with increased cancer risk (Matthews et al., 2012). To best define and study SED,
Tremblay and colleagues (2010) propose using a SITT principle. SITT refers to Sedentary
behaviour frequency (number of bouts of a certain duration); Interruptions in sedentary
behaviour (e.g., getting up from one’s desk while at work; Healy et al., 2008); Time (the
duration of total sitting time); and Type (mode of sedentary behaviour) of SED (Tremblay et al.,
2010). This combined approach to measuring SED allows researchers to use both traditional self-
report tools and objective measures of SED/PA to capture a complete picture of individuals daily
SED. In addition, using SITT, researchers are also able to study breaks/interruptions in SED.
Independent of levels of MVPA and total SED, breaks in SED has been shown to be beneficial
for adults BMI, waist circumference, levels of triglycerides and fasting blood glucose levels

27
(Healy et al., 2008). To date, no studies have examined all the SITT principle variables in cancer
survivors. The way in which SED is operationalized is important for targeted efforts aimed at
decreasing SED among BCS.
Using more generalized assessments of SED rather than a multidimensional approach
such as SITT, BCS spend 66-79% of their waking hours engaged in sedentary pursuits versus
only 1-3% of their day engaged in higher intensity PA (Lynch et al., 2010; Phillips et al., 2015;
Sabiston et al., 2014; Trinh, Amireault, et al., 2015; Wrosch & Sabiston, 2013). Unfortunately,
the majority of past research on SED has used self-report measures. For example, of the 48
studies included in the Thorp and colleagues review, 46 of these studies used a self-report
measure of SED. Self-report measures of SED may times do not paint a complete picture. A
recent study comparing objective accelerometer SED and self-report SED in 317 Australian
adults found that after 7 days of monitoring (500 minutes/day wear time for a minimum of 4
days), the self-report estimate of SED was 13% less time sitting than accelerometer estimates
(Celis-Morales et al., 2012). Furthermore, many of the studies reviewed focus on a
unidimensional SED construct with little regard to the potential different dimensions as defined
using the SITT principle. As such, there is value in studying the potential multiple dimensions of
SED using objective measures such as inclinometers and accelerometers. Both self-report
measures and objective measures used on their own have limitations, such as, recall bias for self-
report measures and the ability to only capture time in SED and not type of SED for objective
measures, however when combined using the SITT principle researchers should be able to
capture a more complete understanding of daily SED.
In preliminary evidence, researchers have reported a mix of findings linking SED and
mental health outcomes among cancer survivors. Rogers and colleagues (2011) conducted a

28
cross-sectional study with 483 rural-living BCS and reported increased fatigue, but not
depression, with higher SED. In a study of 195 BCS, Trinh and colleagues (2015) found a
MVPA by SED interaction effect such that low levels of MVPA and high levels of SED
significantly predicted higher levels of fatigue and depression and a trend for increased pain.
These associations between SED and health outcomes were not observed when higher levels of
MVPA were considered (Trinh, Amireault, et al., 2015). Combined, the evidence from emerging
studies demonstrates a possible protective effect of SED on depression. However, researchers
have only explored total SED as either time spent sitting or total time spent in SED with little
regard to the number and length of time in SED, type of SED, and number of breaks from SED.
As such, a multidimensional approach to the study of SED is needed to classify BCS and explore
links to health outcomes. Finally, studying SED as it relates to cancer survivorship has been
identified as one of the 10 most important research questions related to PA and cancer
survivorship, and exploring this question can potentially improve the lives of many cancer
survivors each year (Courneya et al., 2015).
Thus, this study has three objectives. The first objective is to better understand the SED
profile of BCS using the SITT principle. Along with this first objective, the multiple dimensions
of SED will be examined as grouping factors to classify survivors based on their SED. The
second objective is to examine personal and cancer-specific factors that distinguish the clusters
of SED. Based on previous research with SED and more prominently with PA, it is expected that
age, weight status, and potentially some cancer-related variables such as treatments endured will
be important factors differentiating the SED clusters. It is hypothesized that those who are most
SED will be older and have a higher BMI (Demark-Wahnefried et al., 2001; Kroenke, Chen,
Rosner, & Holmes, 2005; Patterson et al., 2010). Furthermore, women who have undergone
surgical removal of the axillary lymph node have been shown to be less active than those who

29
have not (Sagen, Kåresen, & Risberg, 2009) and undergoing chemotherapy or radiation therapy
during treatment can make survivors less active due to high levels of fatigue (Demark-
Wahnefried, Hars, et al., 1997; Irwin et al., 2003). As a result it was hypothesized that these
demographic/medical and treatment outcomes may be associated with increased SED. The third
objective is to examine the association between SED and depression among BCS during the
early survivorship period. This time period is generally understudied compared to the phases of
diagnosis and treatment and can be a good time to intervene and teach new health behaviours
(Brunet et al., 2014). It is hypothesized that those reporting higher SED, as measured through
cluster membership and those with the highest SED facets, will be significantly associated with
higher depression.
METHODS
Study Population
This study is part of a larger and on-going trial exploring the natural developmental
changes in lifestyle behaviours of BCS (Life After Breast Cancer: Moving On). Specifically,
participants who were diagnosed and had undergone treatment for breast cancer were recruited
through advertisements and oncologist referrals from various local medical clinics and hospitals
in Montreal, Quebec. Participants were screened for study eligibility using the following
inclusion criteria: (1) at least 18+ years of age; (2) 0–20 weeks post primary treatment (i.e.,
surgery, chemotherapy, radiation therapy) for stage I to III breast cancer; (3) first cancer
diagnosis; (4) able to provide written informed consent and read/speak in English or French; and
(5) reported no health concerns which prevent them from engaging in PA. The appropriate
university and hospital research ethics committees approved the study protocol, and all
participants provided written informed consent before starting data collection.

30
Procedures
Once screened for eligibility and the completion of the consent process, women visited
the Health Behaviour and Emotion laboratory to complete a baseline questionnaire, have height,
weight, and waist circumference measured, and to receive an accelerometer to wear for seven
days to assess PA and SED. Depression data was collected during the second data collection
three months after baseline, which equated to approximately 6 months after completion of
systemic treatment and approximately one year post treatment. This period of time was targeted
to capture the early transient survivorship period in BCS because it is a good time to intervene
and teach new health behaviours, consistent with the teachable moment hypothesis (Brunet et al.,
2014).
Measures
Data were collected using a combination of reliable and valid self-report and objective measures.
Demographics and Medical Variables. Women self-reported their demographic and
medical history including questions on age in years, ethnicity, education level, income, stage of
cancer, cancer treatments, time since diagnosis and time since treatment. Measures of weight, to
nearest kilogram (kg), height, to nearest .01 cm, and waist circumference, to nearest .01 cm were
taken by a trained research assistant during the first laboratory visit. These measures were used
to calculate body mass index (BMI, measured as weight divided by height in meters squared)
which was a continuous variable and also examined as a categorical variable based on healthy
(<24.9 kg/m2), and being overweight/obese (≥ 25.0 or more kg/m2 (Flegal, Carroll, Kuczmarski,
& Johnson, 1997). Waist circumference was defined as a continuous variable and categorical
based on an established cut-point of greater than 88 centimeters for women representing
overweight (National Institutes Of Health, 1998), and waist-to-height ratio (WHRT) was
31
assessed as waist circumference in centimeters divided by height in centimeters for a total value
and a categorical variable with a cut-point of 0.50 established to be “unhealthy = > 0.50” or
healthy for women with WHRT of less than 0.50 (Ashwell, Gunn, & Gibson, 2012).
Sedentary Behaviour and Physical Activity. Objective SED was assessed using GT3X+
accelerometers (Actigraph, Pensicola, Florida). Participants wore the accelerometer on their hip
during waking hours for a 7-day period, except for periods of bathing/showering or other water
activities. Data were downloaded in 60-second epochs and converted to mean counts per minute
to estimate daily minutes SED as <100 counts•minute-1, adjusted for non-wear time
operationalized as at least 60 minutes of consecutive zeroes with the allowance of 2-minute
intervals of non-zeroes (Troiano et al., 2008). Data were analyzed if there were no extreme
counts (> 20,000) and if data are available for at least 500 minutes on 4 or more days (Celis-
Morales et al., 2012; Trinh et al., 20151).
Using the sedentary analysis tool within the ActiGraph software, participants’ bouts of
SED (10, 15, 20 and 30 minutes), breaks, total time and average time engaged in SED were
calculated and a minimum 5-minute breaks of SED were used as the default. This enabled the
assessment of each participant’s Sedentary behaviour frequency, Interruptions, and objective
Time spent in SED. The 10 and 30 minute bouts used in the main analysis was based on findings
reported by (Baruth et al., 2013) suggesting these are valuable and meaningful bout lengths.
The Type of SED and an additional Time measure was assessed using self-report items.
1 Some researchers have used 600 minutes for minimum wear time (Healy et al., 2011). However, this level may be inappropriate for clinical samples. Therefore, a comparison of the descriptive statistics for 500 and 600 minimum wear time was conducted (See Appendix B) and bivariate correlations were calculated (See Appendix C). Given the findings, the 500 wear time was used for the current study.

32
Participants were asked to report number of times per week and average duration per session of
SED using the question: “during a typical week (7-day period), how many times on average do
you participate in sedentary activity (no effort) (e.g., TV/video watching, video/computer games,
computer use) and for how long”. This question was modeled after common items used to assess
PA among cancer survivors (Amireault, Godin, Lacombe, & Sabiston, 2015; Godin, 2011).
Participants also completed questions on the amount of time (number of times and average
duration) spent engaged in television viewing, computer use and reading for pleasure per week to
get at type of SED. In the absence of validated SED questionnaires among cancer survivors,
these questions were drawn from the Sedentary Behaviour Questionnaire (SBQ) which has been
found to be a valid and reliable tool to use in adults (Rosenberg et al., 2010). For the current
study and consistent with SED analyses, participants’ total television time and computer time
were summed to create a screen-time variable (Stamatakis, Hamer, & Dunstan, 2011; Sugiyama,
Healy, Dunstan, Salmon, & Owen, 2008). A list of detailed definitions of the various SED
variables used in the current study is presented in Appendix A. Cluster membership SED
variables included: 1) self-report SED; 2) screen-time; 3) reading; 4) average number of 10
minute bouts; 5) average time in 10 minute bouts; 6) average number of 30 minute bouts; 7)
average time in 30 minute bouts; 8) objective SED; and 9) average length of breaks. For a
detailed descriptive analysis of all SITT principle variables see Appendix D.
PA was assessed using accelerometers and total minutes of PA were calculated using
mean counts per minute to estimate daily minutes of light (100-2019 counts•minute-1), moderate
(2200-5998 counts•minute-1) and vigorous (> 5998 counts•minute-1) PA based on established
cut-points (Troiano et al., 2008), while controlling for the number of days the accelerometer was
worn. For the current study, and consistent with guidelines (Schmitz et al., 2010) time spent in
moderate and vigorous PA was combined to create a MVPA variable. Self-report PA was
33
assessed using the Godin-Shephard Leisure Time Exercise Questionnaire (GSLTEQ; Godin,
2011). The GSLTEQ is easily administered and asks participants to recall the past 7-days of PA
which they participated in. The GSLTEQ is a 4-item questionnaire with the first 3 questions
assessing participants PA mild, moderate and strenuous PA frequency during a typical week
lasting more than 15 minutes (Amireault et al., 2015; Godin, 2011). Again, consistent with
previous research, guidelines, and the objective assessment of PA, participants’ moderate and
strenuous PA scores were summed to create an MVPA variable.
Depression. Depression symptoms were assessed using the 10-item Center for
Epidemiological Studies Depression Scale ((CES-D; Andresen, Malmgren, Carter, & Patrick,
1994)) approximately three months following the baseline assessment. Adapted from the CES-D
20, the CES- D 10 has 10 items assessing depression symptoms experienced in the last week
(sample question “I felt depressed”) reported on a 4-point (0-3) Likert-type scale ranging from
“Rarely or none of the time [< 1 day]” to “all of the time [5-7 days]”. Higher scores on the CES-
D scale represent higher levels of reporting of symptoms of depression; with a total score range
possible of 0 to 30. Consistent with previous reports (Andresen et al., 1994), a score ≥ 10 was
used to screen participants with depressive symptomology related to clinical depression in the
current study.
Data Analyses
Preliminary Data Analysis. All quantitative data analysis was conducted using the
Statistical Package for the Social Sciences version 21 (SPSS Inc., Chicago, IL). In addition, the
wear time validation and sedentary analysis tools were used in Actigraph to input and clean data.
Inspection of statistical outliers and examination of statistical assumptions for analysis of
variance and regression analyses were conducted. Missing data for all items were explored using

34
frequency distributions. Means and standard deviations were computed and reported for all
continuous study variables, and frequencies were explored among dichotomous variables.
Pearson (and where appropriate Spearman Rho) correlation coefficients were calculated to
explore relationships among all study variables.
Main Analyses. To examine potential groupings of BCS based on the multiple facets of
SED, cluster analysis was conducted. Specifically, the facets of SED included average number of
10 minute bouts of SED, average time in 10 minute bouts of SED, average number of 30 minute
bouts of SED, average time in 30 minute bouts of SED, daily average time in SED breaks, self-
report SED, average screen-time, average time spent reading and accelerometer SED average.
All these results are presented in minutes per day. Based on cluster analysis guidelines (Hair,
Anderson, Tatham, & Black, 1998; Ullrich-French & Cox, 2009), multiple approaches to cluster
analysis were used to accurately assess the stability of the outcome and identify the appropriate
number of clusters. First, a hierarchical cluster-analysis using Ward’s linkage method and
squared Euclidean distance was conducted to determine the appropriate number of clusters
represented by the data (Ullrich-French & Cox, 2009). Second, a k-means (nonhierarchical)
cluster analysis was conducted using simple Euclidean distance in which the specific number of
clusters was specified based on the hierarchical cluster solution (Ullrich-French & Cox, 2009). A
preliminary multivariate analysis of variance (MANOVA) was tested to examine all SED
variables across cluster membership.
Following the cluster membership analysis, an additional MANOVA with follow-up
univariate tests was conducted to examine significant differences across the clusters on
continuous demographic, personal, and medical variables. In the current study, age, time since
diagnosis and time since treatment, body mass index, waist circumference, waist-to-height ratio,

35
and both self-report and objectively assessed MVPA were tested. Chi-square tests were
conducted to examine differences in percentage of women reporting on categorical variables
including ethnicity, marital status, and type of treatment of lymph/axillary node dissection,
lumpectomy, single mastectomy, double mastectomy, reconstructive surgery, chemotherapy,
radiotherapy, hormonal therapy, and cancer stage. If there were significant differences observed
across cluster membership (i.e., p <.05), variables were then used as covariates in follow-up
analyses.
To test the association between SED cluster membership and depression three months
later, a stepwise logistic regression analysis was completed while controlling for significant
variables identified in the MANOVA/ANOVA and chi-square analyses.
RESULTS
Overall, 187 women provided complete self-report and objective data for the study (92%
of total sample). Women were on average 55 years of age (SD = 11), and predominantly married,
white, highly educated, and were stage I or II cancer survivors (see Table 1). Women had an
average BMI of 26.25 (SD = 5.7) kg/m2, and were approximately 10 months (SD = 3.4) since
being diagnosed for breast cancer and 3 months (SD = 2.3) since completing their last treatment.
Based on accelerometer data, participants spent approximately 8.8 hours of their waking
hours a day sedentary and 25 minutes engaged in MVPA. This differed from self-report SED
where BCS reported that only around 2.5 hours of their day were spent engaged in any SED and
approximately 24 minutes a day engaged in MVPA. Surprisingly when specific types of SED
were considered, women reported spending almost 6 hours per day engaged in screen-time
activities and just less than 2 hours per day spent reading (see Table 2). Using the CES-D 10,
36
31.1% of our sample reported a score of ≥ 10, which places individuals at a risk for clinical
depression.
Pearson and/or Spearman Rho bivariate correlations were used to test relationships
among SED variables that were entered in the cluster membership and self-report/objective
MVPA (Table 3) and cluster membership variables and depression (Table 4). The inter-
correlation of MVPA (self-report and objective) was significant (p<.001). Lower self-report
MVPA was significantly associated with higher numbers of 10-minute bouts, objective SED, and
decreased number of breaks. Lower levels of MVPA as measured with accelerometer was
significantly associated with higher self-report and objective SED, higher screen-time, higher
number of 10 and 30 minute bouts, higher average time in 10 minute bouts and lower number of
breaks. As supplementary analyses, Pearson bivariate correlations were also calculated to
examine relationships among demographic and medical variables (Appendix E), objective
(accelerometer-measured) SED and weight status (Appendix F), and self-report SED and weight
status (Appendix G).
Hierarchical cluster analysis was conducted using self-report SED, screen-time, reading,
objective SED time, average number of 10- and 30-minute bouts, average time in 10- and 30-
minute bouts, and average time in SED breaks. The nine SED variables were standardized for
use in the cluster analyses (Ullrich-French and Cox, 2009). Ward’s linkage method and squared
Euclidean distance as a similarity measure was complete to attempt to assess the most stable and
appropriate number of cluster groups (Ullrich-French and Cox, 2009). These findings led to a
recommended 2-cluster solution based on the creation of a high SED group and low SED group.
Next, a non-hierarchical cluster using Euclidean distance as a similarity measure was conducted
specifying two cluster groups. K-means cluster solution confirmed two clusters that were
37
subsequently examined and described as a low SED and a high SED group. The MANOVA
model testing significant differences in SED variables across cluster membership was significant,
F (1,185) = 44.11, p<.001, η2 = .69. Participants in the high SED cluster spent significantly more
time engaged self-report SED η2 = .16; F (1,185)= 34.23, p<.001, screen-time activities η2 =
.67; F (1,185)= 380.56, p<.001, average time in 10 minute bouts η2 = .04; F (1,185)=7.70,
p<.05, and average number of 30 minute bouts η2 = .03; F (1,185)=3.34, p<.05 compared to
participants in the low SED cluster.
To examine cluster membership differences by personal and cancer-specific variables,
the main MANOVA model was significant, F (8,185) = 4.82, p<.001, η2 =.17. The high SED
group was significantly older (F (1, 185) = 6.56, p = <.05, partial η2 = .03), heavier based on
BMI (F (1, 185) = 7.11, p = <.05; partial η2 = .04), had a larger waist circumference (F (1, 185) =
17.64, p = <.001, partial η2 = .09), higher waist-to-height ratio (F (1, 185) = 12.40, p = <.001,
partial η2 = .06), were less active (self-report MVPA F (1, 185) = 4.07, p = <.05, partial η2 = .03
and objective MVPA F (1, 185) = 16.38, p = <.001, partial η2 = .08) compared to those in the
low SED cluster (see Table 5). In addition, women in the high SED group were significantly (p
< 0.05) more likely to be less educated [X2(1) = 11.86], had undergone lymph or axillary node
dissection [X2 (1) = 5.21], overweight [X2 (1) = 4.00], have a waist-to-height ratio >0.50 [X2 (1) =
4.00], and have a waist circumference > 88cm [X2 (1) = 11.09]. These results are presented in
Table 5.
A stepwise logistic regression analysis was conducted to predict symptom reporting of
clinical depression (i.e., scores of > 10 on the CES-D) for BCS three months after baseline,
controlling for age, education, lymph/axillary node dissection, being overweight, self-report
MVPA and objective MVPA based on the results presented above. In the final model, objective

38
MVPA (OR = 0.97, 95%CI = .95 to 0.99) and cluster membership (OR = 0.46, 95%CI = 0.22 to
0.98) were significant predictors of clinical depression suggesting that high MVPA and being in
the low SED cluster were protective of self-report symptoms of depression (see Table 6).
DISCUSSION
Owning to recent advances in the operational definition of SED and the possible
independent health effects of SED among BCS, the purpose of this study was threefold. First it
was an aim to explore and describe sedentary behaviour facets among women with breast cancer
and examine how sedentary behaviours cluster. Second personal demographic and cancer-
specific differences on the clustering of SED were explored, and third, the association between
SED clusters and depression was tested, independent of PA. The focus of this work was on
women who were recently finished treatments for breast cancer because this is an important time
in the survivorship trajectory for making health behaviour changes (Brunet et al., 2014). Overall,
it was found that BCS were highly sedentary, spending the majority of their waking hours
engaged in sedentary pursuits. Women who were highly SED were more likely to be overweight,
older, less educated and had undergone surgical removal of the lymph/axillary node. In addition,
the results from the logistic regression revealed that after controlling for significant
demographic/medical and PA variables, cluster membership was a significant predictor of
clinical depression among BCS such that high SED was a risk factor of depression.
The current study is the first to examine the SITT principle in cancer survivors and how
this combined approach using objective and self-report SED measurement can be used to
identify SED frequency, interruptions, time, and type of SED. In the current study, average
number and time in 10-minute bouts, average number and time in 30-minute bouts, average time
in SED breaks, objective SED, self-report SED, screen-time and time spent reading were used to
39
represent the different facets of SITT. There are few to no studies reporting on these multiple
facets of SED, however a common measure used has been total time spent in SED – defined as
less than 100 counts per minute using accelerometers (Lynch et al., 2010; Trinh, Amireault, et
al., 2015). In the current sample, 64% of BCS waking hours were spent engaged in SED pursuits
and 3% of the time was spent engaged in MVPA. This is consistent with national survey
estimates of BCS, where 66% of their waking hours were spent sedentary and 1% of time
engaged in MVPA (Lynch, 2010). Moreover, a recent study of 398 BCS (Mage = 56.95 years)
reported that BCS spent 66.4% of their waking hours engaged in SED and only 2.6% engaged in
MVPA (Phillips et al., 2015). In the first representative population objective measure of
sedentary time, Matthews and colleagues (2008) found that adults over the age of 60 spend
approximately 60% of their waking hours engaged in SED (Matthews et al., 2008). In addition,
women aged 50-59 years spent 7.74 waking hours a day (~56% of the day) engaged in SED and
this differed from women over the age of 60 who spent on average 8.60 waking hours a day
(~62% of the day) engaged in SED (Matthews et al., 2008). These estimates are similar to
Australian objective population data which has shown adults spend on average 58% of their
waking hours sedentary (average age 53.3 years; (Healy et al., 2007)). Given these empirical
results coupled with the findings from the current study, it may be that BCS are more SED (or at
least as sedentary) as healthy adults. Furthermore, based on the cluster membership data in the
current study, there is a group of BCS who are likely targets for SED interventions. Specifically,
women in the high SED cluster reported significantly more SED time, screen-time, average time
spent in 10-minute bouts and average number of 30-minute bouts compared to women in the low
SED group. The biggest discrepancy in cluster membership was seen in screen-time, where
participants in the high SED group reported approximately 9 hours a day engaged in screen-time
activities versus under 4 hours a day spent in screen-time activities observed for the low SED
40
group. As such, screen time may be an early intervention target for women with breast cancer
who are recently finished systemic treatments. Specifically, drawing on a recent qualitative study
for men with prostate cancer, it may be important to help BCS add breaks to their SED screen
time using mobile technology such as alarms that remind them to stand up (Trinh et al., 2015).
While this is a novel study exploring the SITT principle in cancer survivors, the results of
the cluster analysis demonstrate that the SITT variables tend to function similarly such that they
grouped into high and low clusters. In addition, most objective and self-report SED variables
were significantly correlated together, however when individually compared to depression, no
significant associations were found. Researchers are urged to further tease out the uniqueness of
the different facets of SED, especially among clinical samples. Future work should examine how
all SITT principle variables are related and the implications of assessing the different facets of
SED on the health and well-being of BCS. Examining the correlation coefficients, most SED
variables were directly associated with decreased length of breaks. Given that breaks are times in
the day when the participants are not sedentary, these findings may allude to a replacement
proposition such that PA replaces time spent sedentary (Owen, Healy, Matthews, & Dunstan,
2010). Researchers have shown that simply replacing SED with light intensity PA has a number
of independent health benefits and when compared against all other intensities of PA, a switch
from no activity (SED) to light activity has the greatest overall health benefit (Powell, Paluch &
Blair, 2011). Future work should begin to examine in more detail the association and interaction
between SED and light PA in BCS. Numerous studies have shown that breaking SED routinely
and replacing this behaviour with PA have number of unique health benefits, including improved
insulin responses and better resting blood pressure (Dunstan et al., 2012; Larsen et al., 2014;
Barr-Anderson et al., 2011). Transitioning from SED to light PA exhibits health benefits
irrespective of a change in the volume of MVPA (Powell et al., 2011). In addition, a recent
41
systematic examining non-vigorous PA and all-cause mortality found that the largest health
benefit observed was from moving from SED to light PA (Woodcook, Franco, Orsini & Roberts,
2011). Thus, it is recommended that researchers begin to focus on the transition between SED
and light PA rather than focus solely on MVPA. Older adults and BCS spend the majority of
their day engaged in SED and light PA opposed to approximately 2% of their day engaged in
MVPA (Powell et al., 2011; Lynch et al., 2013). This research could have public health and
clinical ramifications that are as important or even more important that promoting the many
benefits of regular MVPA.
Furthermore, the results of the cluster membership in the current study take into account
both self-report and objective measures of SED. To date, the knowledge of the effects of SED
has been driven predominantly by self-report assessments. Among healthy adults, self-report
SED has been consistently linked with a number of negative disease-related outcomes. Using
time spent sitting, adults with the longest time SED were more at risk for total mortality and
cardiovascular morbidity and mortality regardless of PA (Katzmarzyk, Church, Craig, &
Bouchard, 2009; Patel et al., 2010; van der Ploeg, Chey, Korda, Banks, & Bauman, 2012). In a
population sample, screen-time as measured as a combination of television viewing and screen-
based activities was related to heightened risk of mortality and cardiovascular disease
independent of PA level (Stamatakis et al., 2011). Regardless of these findings, self-report
measures may be subject to bias. For example, a recent study comparing objective accelerometer
SED and self-report SED in 317 Australian adults found that after 7 days of monitoring (500
mins/day wear time for a minimum of 4 days), the self-report estimate of SED was 13% less time
sitting than accelerometer estimates (Celis-Morales et al., 2012). In addition, these adults self-
reported spending 7.5 hours/day engaged in SED versus accelerometer derived estimates of
almost 9 hours/day engaged in SED (Celis-Morales et al., 2012). In the current study, there was

42
also a discrepancy between self-report SED/PA and accelerometer derived SED/PA with a nearly
300 minute difference between objective time spent SED and self-report SED time.
Discrepancies in self-report and objective assessment of health behaviours are commonly
reported and are likely based on social desirability, inability to self-monitor behaviours, lack of
knowledge of what constitutes the behaviour (Brunet et al., 2011; Motl, McAuley, & DiStefano,
2005; Patterson et al., 2010; Sabiston et al., 2014). Thus, person-centered analyses such as the
one used here allows one to capture subtle differences in SED using both objective and
subjective measurement, and may be a valuable way to continue to assess SED.
Based on the results of this study, high SED was associated with a number of important
demographic, personal and medical variables. Of particular relevance is the link between SED
and weight status indicators. High SED was significantly associated with higher levels of BMI,
waist circumference and waist-to-height ratio. Being overweight and highly SED combined
could potentially increase BCS’s risk profile for a host of other health problems (Healy et al.,
2011; Owen, Healy, Matthews, & Dunstan, 2010; Tremblay et al., 2010). Older BCS were also
more likely to be in the high SED group. This finding is consistent with previous reports
suggesting that age is a common predictor of low levels of PA among BCS (Fontein et al., 2013).
Nonetheless, the benefit of engaging in PA may be even greater in older BCS compared to
younger BCS (Fontein et al., 2013). Thus, health care practitioners should be encouraging
women to reduce their SED and increase their PA at any intensity that feels comfortable across
the lifespan. In addition, SED cluster membership was associated with having had undergone
surgical removal of the axillary lymph node. Traditionally BCS have been told not to perform
upper body exercises following surgical removal of the axillary lymph node due to the belief that
this exercise would worsen the lymphedema (Kwan, Cohn, Armer, Stewart, & Cormier, 2011).
While this myth has been dispelled by a number of researchers (Ganz, 1999; Kwan et al., 2011;

43
Markes, Brockow, & Resch, 2006; Rockson, 1998; Schmitz et al., 2010; Young-McCaughan &
Arzola, 2007), many oncologists, nurses, physiotherapists, and rehabilitation scientists may
continue instruct patients to restrict their daily PA (Sagen et al., 2009) and few discuss PA with
their patients (Karvinen, DuBose, Carney, & Allison, 2010). Thus, like age, health care-
practitioners should encourage BCS to reduce their SED and increase their PA even if they have
undergone this procedure.
Not surprisingly, women in the high SED cluster were also significantly less physically
active. In addition women who spent more time sedentary were less likely to break SED which
can be used as a proxy for physical activity. These findings are common and consistent in adults
and clinical populations such as cancer survivors (Celis-Morales et al., 2012; Gordon-Larsen,
Nelson, & Popkin, 2004; Healy, Dunstan, et al., 2008; Katzmarzyk et al., 2009; Lynch et al.,
2013) As such, there is a constant message that both SED and PA are needed targets in cancer
care. In addition, researchers have begun to tease out the importance of separating SED from
physical inactivity and examining how SED and levels of PA produce unique metabolic profiles
independently (Owen et al., 2010; Tremblay et al., 2010). For example, researchers have
demonstrated that participants can be both sedentary and physically inactive, but also sedentary
and physically active, and these profiles have significantly different metabolic outcomes (Owen
et al., 2010). The ‘active couch potato’ is classified as an individual highly sedentary but also
meeting national physical activity guidelines (Owen et al., 2010). This differs from an inactive
couch potato who is both highly sedentary and highly inactive. The results of the current study
were purposefully limited to define the multiple facets of SED, while controlling for MVPA in
analyses. However, there are multiple ways of exploring the combination of SED and PA that
should be explored among BCS.

44
In the current study, SED cluster membership significantly predicted clinical depression
three months after baseline and approximately six months after completion of systemic
treatments. In clinical populations, researchers employing cross-sectional designs have
demonstrated depressed individuals live a more sedentary lifestyle (Roshanaei-Moghaddam et
al., 2009; Weyerer & Kupfer, 1994). Moreover, although only limited work has been done
examining SED and depression in BCS, the current findings are consistent with evidence that
high levels of SED were associated with depressive mood assessed as dysphoria (Trinh et al.,
2015). Nonetheless, when levels of MVPA were assessed independently and in interaction with
SED, women with high levels of MVPA were more protected from dysphoria (Trinh et al.,
2015). In the current study, both SED (assessed as cluster membership) and MVPA were
significant predictors of depression three months later. As such, it is important to continue to
study both PA and SED to best understand mental health outcomes. It is also important to
identify the unique and combined mechanisms that may explain the association between SED,
MVPA, and depression. There are a number of proposed possible linkages that should be
examined. For example, it may be the intensity and frequency of PA combined with low SED
that improve mental health outcomes through neurobiological influences such as monoamine
availability and increased neurotropic factors (Rot, Mathew, & Charney, 2009). Also, PA
opportunities, but not SED, may enhance self-efficacy and self-concept which could explain the
association to depression (Dishman et al., 2006). Furthermore, the associations may be explained
in part by immune functioning such that high SED and low PA are related to poorer immune
function which exacerbates health conditions including depression (Ballard-Barbash et al., 2012;
Lynch, 2010). Lynch’s (2010) model also explored the existing literature on a number of
metabolic markers and how these markers influence the relationship between SED and cancer.
These include inflammation, sex hormones (androgen/estrogen/sex hormone binding globulin),
45
vitamin D and metabolic dysfunction (insulin/glucose). It is possible that these metabolic
markers might also influence the relationship between SED and depression. Thus, future work
should study these markers both independently and concomitantly to explore if and how they
might influence the direction of relationship between SED and depression.
In the current study, the participants were BCS considered in the “extended survivorship”
period (Ristovski-Slijepcevic & Bell, 2014). This is an important time for survivorship outcomes
and could be a possible time for intervention (Demark-Wahnefried, 2005). Furthermore, more
than 88% of breast cancer patients are surviving for 5 years or more after being diagnosed
(Canadian Cancer Society, 2013) and that there is a high prevalence of depression in BCS, which
means it is imperative to explore how behavioural changes such as reducing SED might
influence the sequeale caused by cancer and its related physical, social and psychological
symptoms. Interventions reducing SED represent a cost-effective and non-pharmaceutical
strategy to potentially combat many negative health outcomes among cancer survivors (Lynch et
al., 2013). Given the low levels of MVPA reported and measured among BCS, and challenges
associated with uptake and adherence to regular physical activity, targeting SED may be more
feasible and realistic in this population. A recent qualitative study exploring SED and the
perceptions of SED in prostate cancer survivors found that men would enjoy a web-based/mobile
application to reduce SED and these men were not able to differentiate between the differences
of SED and inactivity (Trinh, Arbour-nicitopoulos, et al., 2015). To the best of our knowledge
this qualitative work has yet to be done in BCS and qualitative work like this could help
researchers identify the best and most effective ways to reduce SED and increase PA in BCS.
Future work could aim to identify what mobile and web-based applications BCS may prefer for
changing SED patterns and how these applications can be best introduced into their daily lives.
46
Although the findings from this prospective cohort study offer exciting findings related to
SED and depression in BCS, the results need to be considered with some limitations. The sample
was a convenience sample of BCS with the majority of women being early stage cancer
survivors, highly educated, and white. As a result, these women are not reflective of all BCS, and
future work should examine the replicability in other groups (e.g., nonwhite, low education,
stage III BCS). Nonetheless, the sample characteristics are similar to the characteristic of many
studies exploring factors related to PA in BCS (Brunet et al., 2014). Second, cluster analysis is a
person-centered approach to understanding SED. This analysis renders the current findings to be
sample specific and thus may limit the generalizability of results. However, this approach
enabled a comprehensive understanding of multiple facets of SED simultaneously in light of no
detailed guidelines for understanding SED behaviours in BCS. Also, the use of SITT principle to
operationalize SED has not been used among cancer survivors and these findings should be
replicated. While specific justifiable facets were included in the current study to represent each
of the SITT elements, it is clear that there are a number of additional facets of SED that were not
studied in the current analysis that may also have clinical, practical, and/or theoretical
implications. Finally, although the cut-point for clinical depression was consistent with
recommendations (Andresen et al., 1994), the original CES-D measure was tested for clinical
ramifications and thus replication of these findings with similar cut-points are needed.
Notwithstanding the limitations, this study offers important preliminary evidence that
high SED as measured through a combination of self-report and objective measures may be
related to symptoms of clinical depression during the early survivorship period. Based on these
findings, it is important to encourage BCS to reduce SED to attenuate symptoms of depression.
Introducing health promotion messages encouraging survivors to reduce SED might represent an
easier to follow and more effective tool then instructing survivors to increase daily MVPA,

47
wherefew BCS currently meet the recommended PA guidelines. At the individual level, reducing
SED represents a cost-effective and non-pharmaceutical tool, which could potentially reduce
symptoms of depression. A large number of BCS are currently not active enough to gain health
benefits (Lynch et al., 2010), so promoting reductions in SED, where individuals spend a large
portion of their day, could lead to tremendous benefits, which are probably not limited to
reducing symptoms of depression. From a public health perspective, using health messaging to
inform all survivors about the potential benefits of reducing SED could prove to be an effective
tool that could improve the quality and quantity of life among BCS (Lynch et al., 2013). Also,
reducing symptoms of depression and other negative symptoms associated with cancer survival
through promoting reductions in SED could potentially reduce the financial commitment
required to treat co-morbities associated with cancer survival. Based on our findings and
previous work, the early survivorship period represents an important time to introduce health
behaviour change messaging (Brunet et al., 2014) and can potentially exhibit positive changes to
the lives of the many women living with a diagnosis of breast cancer.

48
Chapter 4 Conclusions and Future Directions
This thesis had three main objectives. The first goal was to better understand the SED
profile of BCS using the SITT principle. Along with this first objective, the multiple dimensions
of SED were examined by grouping survivors based on their SED into a high and low SED
group. The preliminary modeling demonstrated that the two clusters were significantly different
on age, level of education, weight-status, PA and having undergone surgical removal of the
lymph/axillary node.
The second objective was to examine personal and cancer-specific factors that distinguish
the groups of SED. Based on previous research with SED and more prominently with PA, it was
expected that age, weight status, and potentially some cancer-related variables would be
important factors differentiating the SED groups. It was hypothesized that high SED would be
associated with being older and have a higher BMI (Demark-Wahnefried et al., 2001; Kroenke,
Chen, Rosner, & Holmes, 2005; Patterson et al., 2010). Furthermore, we hypothesized that those
women who had undergone chemotherapy, radiation and/or had undergone surgical removal of
the axillary lymph node would be highly SED (Harvie, Campbell, Baildam, & Howell, 2004;
Rockson, 1998; Sagen et al., 2009). Based on MANOVA, ANOVA and chi-square results we
confirmed that SED was significantly associated with age, weight status measures, education and
lymph/axillary node dissection but not with chemotherapy or radiation.
Finally, the third objective was to examine the association between SED and depression
among BCS over time. It was hypothesized that cluster membership would significantly predict
symptom reporting consistent with clinical depression. We confirmed this hypothesis through
completing a logistic regression analysis while controlling for a number of significant
demographic, medical and PA covariates. These findings are exciting because they are the first

49
study in cancer survivor’s to explore various SED facets and examine how these relate to
depression however insufficient evidence has accumulated to draw strong conclusions between
SED and depression. Future work should explore this potential relationship in more detail as well
as the direction of this relationship.
Practically, reducing SED and depression should be given important priority by BCS.
Psychosocial oncology researchers have identified SED as one of the most important issues to
consider in PA and cancer survivorship, and exploring this question in more detail can
potentially improve the lives of the many cancer survivors (Courneya et al., 2015). In addition,
compared to MVPA, targeting SED may be a more feasible, realistic, cost-effective for the ever-
increasing number of BCS’s (Gardiner, Eakin, Healy, & Owen, 2011; Lynch et al., 2013). In the
current study of a convenience sample of BCS, the women spent on average 8.8 hours/day
engaged in SED during their waking hours. This corresponds to 64% of one’s waking hours
engaged in SED. Displacing SED and replacing this behaviour with light intensity PA will lead
to a myriad of positive physical and psychological health outcomes (Owen et al., 2012). The
current analysis only began to explore the number of different ways that SED can be measured
through using the SITT principle. Future work should identify the appropriate bout length, break
length and number of breaks required to most effectively reduce symptoms of depression and
also experience a number of additional physical and psychological health benefits. Until this
work can be done, researchers first need to agree on operational definitions of SED, beginning
with adults in general and in clinical populations afterwards (i.e., cancer survivors). From a
clinical perspective, researchers should begin to tease out the impact that different facets of SED
have on both physical and psychological health of adults and clinical populations. Before doing
this work it is imperative to create detailed SED guidelines, which provide recommendations on
the appropriate dose and frequency of daily SED. In addition, these guidelines should also

50
instruct to adults on how often to break SED and for how long they should break SED in order to
receive health benefits. Doing this work will help clinician’s and survivors to better understand
SED and continue to dispel the myth that SED is synonymous with physical inactivity. As of
2013, there are 12,200 new cases of breast cancer in Canada reported annually, and breast cancer
continues to be the most common cancer diagnosis in women (Canadian Cancer Society, 2013).
From a research perspective, a criticism from systematic reviews regarding current SED
measurement is heterogeneity of measurement across studies (Lynch, 2010). Thus in addition to
having operational definitions of SED, researchers should also validate and agree on an
established set of procedures to use when conducting studies and randomized controlled trials
amongst BCS. Based on the directions of the current study, it may be of value to study and assess
SED using the SITT principle in BCS because it allows the researcher to capture multiple facets
of SED using both objective and self-report measures of SED.
Furthermore, it may be of research importance for researchers to direct attention at
developing and testing nomological frameworks explaining the association between SED, PA,
and both physical and mental health outcomes. To accomplish this goal, mechanisms linking
these lifestyle behaviours to health outcomes such as depression need to be tested. There are a
number of proposed possible mechanisms including the type, intensity and frequency of PA and
SED, effects of these features of lifestyle behaviours on neurobiology (including monoamine
availability, neurotrasmitters, and neurotropic factors) and immune function, metabolic
dysfunction, and increases in self-efficacy and mastery (Rot et al., 2009)(Dishman et al.,
2006)(Ballard-Barbash et al., 2012; Lynch, 2010). Lynch’s (2010) model may offer a starting
point for the testing of mechanisms and the development of theoretical or conceptual frameworks
that best explain the association between SED, PA, and health. Researchers are encouraged to
51
design prospective studies to examine proposed associations, and to examine manipulations in
the SED and PA behaviours using randomized controlled trials among BCS.
In conclusion, breast cancer is most prevalent in females aged 50 to 69 years (52% of
diagnoses) and five-year survival rates are now estimated between 80 and 95% (Coleman et al.,
2011). With an ever increasing number of survivors and with survivors living longer, the time is
now for public health researchers, clinicians and policy makers to beginning to explore the
impact the modifiable factors such as reducing SED and increasing daily PA have on the
physical and psychological health of BCS’s. In conclusion, efforts to explore SED and how this
potential negative health behaviour might be linked with various mental health outcomes are of
immediate concern. However, before effective interventions can be tested, researchers first need
to generate a clear and concise set of guidelines for SED beginning in adults and then within
clinical populations. Once these tasks have been completed, researchers are next encouraged to
test the framework suggested by Lynch (2010) and explore if these relationships continue to hold
when different demographic (i.e., ethnicity) and medical variables (i.e., stage of cancer) of BCS
are considered. Overall, this is the first study to explore SED in BCS using the SITT principle
and the first study to examine SED as a predictor clinical depression.

52
References
Alfano, C.M., Smith, A.W., Irwin, M.L., Bowen, D.J., Sorensen, B, Reevem B.B.,…&
McTiernan, A. (2007). Physical activity, long-term symptoms, and physical health-related
quality of life among breast cancer survivors: A prospective analysis. Journal of Cancer
Survivorship, 1(2), 116-128.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders
(5th ed., text rev). Washington, D.C: Author.
Amireault, S., Godin, G., Lacombe, J., & Sabiston, C. M. (2015). Validation of the Godin-
Shephard Leisure-Time Physical Activity Questionnaire classification coding system using
accelerometer assessment among breast cancer survivors. Journal of Cancer Survivorship.
http://doi.org/10.1007/s11764-015-0430-6
Andresen, E. M., Malmgren, J. A., Carter, W. B., & Patrick, D. L. (1994). Screening for
depression in well older adults: evaluation of a short form of the CES-D (Center for
Epidemiologic Studies Depression Scale). American Journal of Preventive Medicine, 10(2),
77–84. http://doi.org/10.4236/health.2013.53A078
Andrews, G., Henderson, S., & Hall, W. (2001). Prevalence, comorbidity, disability and service
utilisation: Overview of the Australian National Mental Health Survey. British Journal of
Psychiatry, 178(FEB.), 145–153. http://doi.org/10.1192/bjp.178.2.145
Archer, J., Bower, P., Gilbody, S., Lovell, K., Richards, D., Gask, L., … Coventry, P. (2012).
Collaborative care for depression and anxiety problems. The Cochrane Database of
Systematic Reviews, 10(10), CD006525. http://doi.org/10.1002/14651858.CD006525.pub2
Ashwell, M., Gunn, P., & Gibson, S. (2012). Waist-to-height ratio is a better screening tool than
waist circumference and BMI for adult cardiometabolic risk factors: Systematic review and
meta-analysis. Obesity Reviews, 13(3), 275–286. http://doi.org/10.1111/j.1467-
789X.2011.00952.x
Association, A. P. (2013). DSM 5. American Journal of Psychiatry.
http://doi.org/10.1176/appi.books.9780890425596.744053

53
Azim, H. A., de Azambuja, E., Colozza, M., Bines, J., & Piccart, M. J. (2011). Long-term toxic
effects of adjuvant chemotherapy in breast cancer. Annals of Oncology : Official Journal of
the European Society for Medical Oncology / ESMO, 22(9), 1939–1947.
http://doi.org/10.1093/annonc/mdq683
Aziz, N. M. (2002). Cancer survivorship research: challenge and opportunity. The Journal of
Nutrition, 132(11 Suppl), 3494S–3503S.
Baade, P. D., Fritschi, L., & Eakin, E. G. (2006). Non-cancer mortality among people diagnosed
with cancer (Australia). Cancer Causes & Control : CCC, 17(3), 287–97.
http://doi.org/10.1007/s10552-005-0530-0
Ballard-Barbash, R., Friedenreich, C. M., Courneya, K. S., Siddiqi, S. M., McTiernan, A., &
Alfano, C. M. (2012). Physical activity, biomarkers, and disease outcomes in cancer
survivors: a systematic review. Journal of the National Cancer Institute, 104(11), 815–40.
http://doi.org/10.1093/jnci/djs207
Bardwell, W. A., Natarajan, L., Dimsdale, J. E., Rock, C. L., Mortimer, J. E., Hollenbach, K., &
Pierce, J. P. (2006). Objective cancer-related variables are not associated with depressive
symptoms in women treated for early-stage breast cancer. Journal of Clinical Oncology :
Official Journal of the American Society of Clinical Oncology, 24(16), 2420–2427.
http://doi.org/10.1200/JCO.2005.02.0081
Barr-Anderson, D.J., AuYoung, M., Whitt-Glover, M.C., Glenn, B.A., & Yancey, A.K. (2011).
Integration of short bouths of physical activity into organizational routine. American Journa
of Preventative Medicine, 40(1), 76-93.
Baruth, M., Sharpe, P. A., Hutto, B., Wilcox, S., & Warren, T. Y. (2013). Patterns of sedentary
behavior in overweight and obese women. Ethnicity & Disease, 23(3), 336–42. Retrieved
from
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3761397&tool=pmcentrez&ren
dertype=abstract
Barton-Burke, M. (2006). Cancer-related fatigue and sleep disturbances. American Journal of
Nursing, 106(3), 72-77.

54
Buman, M.P., Hekler, E.B., Haskell, W.L., Pruitt, L., Conway, T.L., Cain, K.L.,…& King, A.C.
(2010). Objective light-intensity physical acitivity associations with rated health in older
adults. American Journal of Epidemiology, 172(10), 1155-1165.
Black, S. A., Markides, K. S., & Ray, L. A. (2003). Depression predicts increased incidence of
adverse health outcomes in older Mexican Americans with type 2 diabetes. Diabetes Care,
26(10), 2822–2828. http://doi.org/10.2337/diacare.26.10.2822
Blanchard, C. M., Courneya, K. S., & Stein, K. (2008). Cancer survivors’ adherence to lifestyle
behavior recommendations and associations with health-related quality of life: Results from
the American Cancer Society's SCS-II. Journal of Clinical Oncology, 26(13), 2198–2204.
http://doi.org/10.1200/JCO.2007.14.6217
Blazer, D. G., Kessler, R. C., McGonagle, K. A., & Swartz, M. S. (1994). The prevalence and
distribution of major depression in a national community sample: the National Comorbidity
Survey. American Journal of Psychiatry, 151, 979–986.
Bower, J.E., Ganz, P.A., Desmond, K.A., Bernaards, C., Rowland, J.H., Meyerowitz, B.E., &
Belin, T.R. (2006). Fatigue in long-term breast carcinoma survivors: A longitudinal
investigation. Cancer, 106(4), 751-8.
Brunet, J., Burke, S.M., & Sabiston, C.M. (2013). The benefits of being self-determined in
promoting physical activity and affective well-being among women recently treated for
breast cancer. Pyscho-Oncology, 22(10), 2245-2252.
Brunet, J., Sabiston, C.M., & Gaudreau, P. (2014). A prospective investigation of the
relationship between self-presentation processes and physical activity in women treated for
breast cancer. Health Psychology, 33(3), 205-13.
Brunet, J., Amireault, S., Chaiton, M., & Sabiston, C. M. (2014). Identification and prediction of
physical activity trajectories in women treated for breast cancer. Annals of Epidemiology,
24(11), 837–842. http://doi.org/10.1016/j.annepidem.2014.07.004
55
Brunet, J., Sabiston, C. M., & Meterissian, S. (2011). Physical Activity and Breast Cancer
Survivorship: Evidence-Based Recommendations. American Journal of Lifestyle Medicine,
6(3), 224–240. http://doi.org/10.1177/1559827611421460
Buman, M. P., Hekler, E. B., Haskell, W. L., Pruitt, L., Conway, T. L., Cain, K. L., … King, A.
C. (2010). Objective light-intensity physical activity associations with rated health in older
adults. American Journal of Epidemiology, 172(10), 1155–1165.
http://doi.org/10.1093/aje/kwq249
Burgess, C., Cornelius, V., Love, S., Graham, J., Richards, M., & Ramirez, A. (2005).
Depression and anxiety in women with early breast cancer: five year observational cohort
study. BMJ (Clinical Research Ed.), 330(7493), 702.
http://doi.org/10.1136/bmj.38343.670868.D3
Canada, S. (2013). Canadian Cancer Statistics Special topic : Liver cancer, 1–114.
Carson, V., & Janssen, I. (2011). Volume, patterns, and types of sedentary behavior and cardio-
metabolic health in children and adolescents: a cross-sectional study. BMC Public Health,
11, 274. http://doi.org/10.1186/1471-2458-11-274
Carpenter, J.S., & Andrykowski, M.A. (1999). Menopausal symptoms in breast cancer survivors.
Oncology Nursing Forum, 26(8), 1311-1317.
Casso, D., Buist, D. S. M., & Taplin, S. (2004). Quality of life of 5-10 year breast cancer
survivors diagnosed between age 40 and 49. Health and Quality of Life Outcomes, 2, 25.
http://doi.org/10.1186/1477-7525-2-25
Castonguay, A.L., Wrosch, C., & Sabiston, C.M. (2014). Systemic inflmmation among breast
cancer survivors: The roles of goal-disengagment capacities and health-related self-
protection. Pyscho-Oncology, 23(8), 878-85.
Castonguay, A.L., Crocker, P.R.E., Hadd, V., McDonough, M.H., & Sabiston, C.M. (2015).
Linking physical self-worth to posttraummatic growth in a sample of physically active
breast cancer survivors. Journal of Applied Biobehavioral Research, 20(2), 53-70.

56
Celis-Morales, C. A., Perez-Bravo, F., Ibañez, L., Salas, C., Bailey, M. E. S., & Gill, J. M. R.
(2012). Objective vs. self-reported physical activity and sedentary time: Effects of
measurement method on relationships with risk biomarkers. PLoS ONE, 7(5).
http://doi.org/10.1371/journal.pone.0036345
Cliff, D. P., Jones, R. A., Burrows, T. L., Morgan, P. J., Collins, C. E., Baur, L. A., & Okely, A.
D. (2014). Volumes and bouts of sedentary behavior and physical activity: Associations
with cardiometabolic health in obese children. Obesity, 22(5).
http://doi.org/10.1002/oby.20698
Coleman, M. P., Forman, D., Bryant, H., Butler, J., Rachet, B., Maringe, C., … Richards, M. A.
(2011). Cancer survival in Australia, Canada, Denmark, Norway, Sweden, and the UK,
1995-2007 (the International Cancer Benchmarking Partnership): an analysis of population-
based cancer registry data. Lancet, 377(9760), 127–38. http://doi.org/10.1016/S0140-
6736(10)62231-3
Courneya, K. S., Friedenreich, C. M., Quinney, H. A., Fields, A. L. A., Jones, L. W., Vallance, J.
K. H., & Fairey, A. S. (2005). A longitudinal study of exercise barriers in colorectal cancer
survivors participating in a randomized controlled trial. Annals of Behavioral Medicine : A
Publication of the Society of Behavioral Medicine, 29(2), 147–53.
http://doi.org/10.1207/s15324796abm2902_9
Courneya, K. S., Rogers, L. Q., Campbell, K. L., Vallance, J. K., & Friedenreich, C. M. (2015).
Top 10 Research Questions Related to Physical Activity and Cancer Survivorship. Research
Quarterly for Exercise and Sport, 86(2), 107–116.
http://doi.org/10.1080/02701367.2015.991265
Deimling, G.T., Kahana, B., Bowman, K.F., & Schaefer, M.L. (2002). Cancer survivorship and
psychological distress in later life. Psychooncology, 11(6), 479-494.
Deimling, G. T., Sterns, S., Bowman, K. F., & Kahana, B. (2005). The health of older-adult,
long-term cancer survivors. Cancer Nursing, 28(6), 415–424.
http://doi.org/10.1300/J077v20n04_05
57
Demark-Wahnefried, W., Hars, V., Conaway, M., Havlin, K., Rimer, B., McElveen, G., &
Winer, E. (1997). Reduced rates of metabolism and decreased physical activity in breast
cancer patients receiving adjuvant chemotherapy. Am J Clin Nutr, 65(5), 1495–1501.
Retrieved from http://ajcn.nutrition.org/content/65/5/1495.abstract
Demark-Wahnefried, W., Peterson, B. L., Winer, E. P., Marks, L., Aziz, N., Marcom, P. K., …
Rimer, B. K. (2001). Changes in weight, body composition, and factors influencing energy
balance among premenopausal breast cancer patients receiving adjuvant chemotherapy.
Journal of Clinical Oncology, 19(9), 2381–2389.
Demark-Wahnefried, W., Pinto, B. M., & Gritz, E. R. (2006). Promoting health and physical
function among cancer survivors: potential for prevention and questions that remain.
Journal of Clinical Oncology : Official Journal of the American Society of Clinical
Oncology, 24(32), 5125–31. http://doi.org/10.1200/JCO.2006.06.6175
Dishman, R. K., Hales, D. P., Pfeiffer, K. A., Felton, G. A., Saunders, R., Ward, D. S., … Pate,
R. R. (2006). Physical self-concept and self-esteem mediate cross-sectional relations of
physical activity and sport participation with depression symptoms among adolescent girls.
Health Psychology : Official Journal of the Division of Health Psychology, American
Psychological Association, 25(3), 396–407. http://doi.org/10.1037/0278-6133.25.3.396
Dunstan, D.W., Shaw, J.E., Kingwell, B.A., Bertovic, D.A., Larsen, R., Zimmet, P.Z.,…&
Owen, N. (2012). Breaking up prolonged sitting reduces postprandial glucose and insulin
responses. Diabetes Care, 35, 976-83.
Eaton, W. W., Armenian, H., Gallo, J., Pratt, L., & Ford, D. E. (1996). Depression and risk for
onset of type II diabetes. A prospective population-based study. Diabetes Care, 19(10),
1097–1102. http://doi.org/10.2337/diacare.19.10.1097
Edwards, B. K., Brown, M. L., Wingo, P. A., Howe, H. L., Ward, E., Ries, L. A. G., … Pickle,
L. W. (2005). Annual report to the nation on the status of cancer, 1975-2002, featuring
population-based trends in cancer treatment. Journal of the National Cancer Institute,
97(19), 1407–27. http://doi.org/10.1093/jnci/dji289

58
Erickson, V.S., Pearson, M.L., Adams, J., & Kahn, K.L. (2001). Arm edema in breast cancer
patients. Journal of the National Cancer Institute, 93(2), 96-11.
Eston, R. G., Rowlands, A. V, & Ingledew, D. K. (1998). Validity of heart rate, pedometry, and
accelerometry for predicting the energy cost of children’s activities. Journal of applied
physiology (Bethesda, Md. : 1985) (Vol. 84).
Fann, J. R., Thomas-Rich, A. M., Katon, W. J., Cowley, D., Pepping, M., McGregor, B. A., &
Gralow, J. (2008). Major depression after breast cancer: a review of epidemiology and
treatment. General Hospital Psychiatry, 30(2), 112–126.
http://doi.org/10.1016/j.genhosppsych.2007.10.008
Feuerstein, M. (2007). Defining cancer survivorship. Journal of Cancer Survivorship, 1(1), 5–7.
http://doi.org/10.1007/s11764-006-0002-x
Flegal, K. M., Carroll, M. D., Kuczmarski, R. J., & Johnson, C. L. (1997). Overweight and
obesity in the United States: prevalence and trends, 1960–1994. International Journal of
Obesity, 22(1), 39–47. http://doi.org/10.1038/sj.ijo.0800541
Fontein, D. B. Y., de Glas, N. A., Duijm, M., Bastiaannet, E., Portielje, J. E. A., Van de Velde,
C. J. H., & Liefers, G. J. (2013). Age and the effect of physical activity on breast cancer
survival: A systematic review. Cancer Treatment Reviews.
http://doi.org/10.1016/j.ctrv.2013.03.008
Ganz, P. A. (1999). The quality of life after breast cancer - solving the problem of lymphedema.
New England Journal of Medicine, 340(5), 383–5.
Ganz, P.A., Desmond, K.A., Leedham, B., Rowland, J.H., Meyerowitz, B.E., & Belin, T.R.
(2002). Quality of life in long-term, diseass-free survivors of breast cancer: A follow-up
study. Journal of the National Cancer Institute, 94(1), 39-49.
Gardiner, P. A., Eakin, E. G., Healy, G. N., & Owen, N. (2011). Feasibility of reducing older
adults’ sedentary time. American Journal of Preventive Medicine, 41(2), 174–177.
http://doi.org/10.1016/j.amepre.2011.03.020

59
George, S. M., Alfano, C. M., Groves, J., Karabulut, Z., Haman, K. L., Murphy, B. A., &
Matthews, C. E. (2014). Objectively measured sedentary time is related to quality of life
among cancer survivors. PLoS ONE, 9(2). http://doi.org/10.1371/journal.pone.0087937
Godin, G. (2011). The Godin-Shephard Leisure-Time Physical Activity Questionnaire. Health &
Fitness Journal of Canada, 4(1), 18–22.
Gordon-Larsen, P., Nelson, M. C., & Popkin, B. M. (2004). Longitudinal physical activity and
sedentary behavior trends: Adolescence to adulthood. American Journal of Preventive
Medicine, 27(4), 277–283. http://doi.org/10.1016/j.amepre.2004.07.006
Hair, J. F., Anderson, R. E., Tatham, R. L., & Black, W. C. (1998). Multivariate Data Analysis.
International Journal of Pharmaceutics (Vol. 1).
http://doi.org/10.1016/j.ijpharm.2011.02.019
Hamer, M., & Chida, Y. (2008). Walking and primary prevention: a meta-analysis of prospective
cohort studies. British Journal of Sports Medicine, 42(4), 238–243.
http://doi.org/10.1136/bjsm.2007.039974
Hamer, M., Coombs, N., & Stamatakis, E. (2014). Associations between objectively assessed
and self-reported sedentary time with mental health in adults: an analysis of data from the
Health Survey for England. BMJ Open, 4(3), e004580. http://doi.org/10.1136/bmjopen-
2013-004580
Hamilton, M. T., Hamilton, D. G., & Zderic, T. W. (2004). Exercise physiology versus inactivity
physiology: an essential concept for understanding lipoprotein lipase regulation. Exercise
and Sport Sciences Reviews, 32(4), 161–166. http://doi.org/10.1097/00003677-200410000-
00007
Hamilton, M. T., Healy, G. N., Dunstan, D. W., Zderic, T. W., & Owen, N. (2008). Too little
exercise and too much sitting: Inactivity physiology and the need for new recommendations
on sedentary behavior. Current Cardiovascular Risk Reports, 2(4), 292–298.
http://doi.org/10.1007/s12170-008-0054-8
60
Hänggi, J. M., Phillips, L. R. S., & Rowlands, A. V. (2013). Validation of the GT3X ActiGraph
in children and comparison with the GT1M ActiGraph. Journal of Science and Medicine in
Sport, 16(1), 40–44. http://doi.org/10.1016/j.jsams.2012.05.012
Harrington, C. B., Hansen, J. a., Moskowitz, M., Todd, B. L., & Feuerstein, M. (2010). It’s Not
Over When It's Over: Long-Term Symptoms in Cancer Survivors—A Systematic Review.
The International Journal of Psychiatry in Medicine, 40(2), 163–181.
http://doi.org/10.2190/PM.40.2.c
Harvie, M. N., Campbell, I. T., Baildam, A., & Howell, A. (2004). Energy balance in early breast
cancer patients receiving adjuvant chemotherapy. Breast Cancer Research and Treatment,
83(3), 201–210. http://doi.org/10.1023/B:BREA.0000014037.48744.fa
Haydon, A. M. M., Macinnis, R. J., English, D. R., & Giles, G. G. (2006). Effect of physical
activity and body size on survival after diagnosis with colorectal cancer. Gut, 55(1), 62–7.
http://doi.org/10.1136/gut.2005.068189
Healy, G. N., Dunstan, D. W., Salmon, J., Cerin, E., Shaw, J. E., Zimmet, P. Z., & Owen, N.
(2007). Objectively measured light-intensity physical activity is independently associated
with 2-h plasma glucose. Diabetes Care, 30(6), 1384–1389. http://doi.org/10.2337/dc07-
0114
Healy, G. N., Dunstan, D. W., Salmon, J., Cerin, E., Shaw, J. E., Zimmet, P. Z., & Owen, N.
(2008). Breaks in sedentary time. Diabetes Care, 31(4), 661–666.
http://doi.org/10.2337/dc07-2046
Healy, G. N., Matthews, C. E., Dunstan, D. W., Winkler, E. A. H., & Owen, N. (2011).
Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 200306. European
Heart Journal, 32(5), 590–597. http://doi.org/10.1093/eurheartj/ehq451
Healy, G. N., Wijndaele, K., Dunstan, D. W., Shaw, J. E., Salmon, J., Zimmet, P. Z., & Owen,
N. (2008). Objectively measured sedentary time, physical activity, and metabolic risk the
Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Diabetes Care, 31(2), 369–
371. http://doi.org/10.2337/dc07-1795

61
Holmes, M. D., Chen, W. Y., Feskanich, D., Kroenke, C. H., & Colditz, G. A. (2005). Physical
activity and survival after breast cancer diagnosis. JAMA : The Journal of the American
Medical Association, 293(20), 2479–86. http://doi.org/10.1001/jama.293.20.2479
Howard-Anderson, J., Ganz, P. A., Bower, J. E., & Stanton, A. L. (2012). Quality of life, fertility
concerns, and behavioral health outcomes in younger breast cancer survivors: A systematic
review. Journal of the National Cancer Institute. http://doi.org/10.1093/jnci/djr541
Ibrahim, E.M., & Al-Homaidh, A. (2011). Physical activity and survival after breast cancer
diagnosis: Meta-analysis of published studies. Medical Oncology, 28(3), 753-65.
Irwin, M. L., Crumley, D., McTiernan, A., Bernstein, L., Baumgartner, R., Gilliland, F. D., …
Ballard-Barbash, R. (2003). Physical activity levels before and after a diagnosis of breast
carcinoma: The health, eating, activity, and lifestyle (HEAL) study. Cancer, 97(7), 1746–
1757. http://doi.org/10.1002/cncr.11227
Jonas, B. S., & Lando, J. F. (2015). Negative affect as a prospective risk factor for hypertension.
Psychosomatic Medicine, 62(2), 188–196. http://doi.org/10.1097/00006842-200003000-
00006
Karvinen, K. H., DuBose, K. D., Carney, B., & Allison, R. R. (2010). Promotion of physical
activity among oncologists in the United States. The Journal of Supportive Oncology, 8(1),
35–41.
Katzmarzyk, P. T., Church, T. S., Craig, C. L., & Bouchard, C. (2009). Sitting time and mortality
from all causes, cardiovascular disease, and cancer. Medicine and Science in Sports and
Exercise, 41(5), 998–1005. http://doi.org/10.1249/MSS.0b013e3181930355
Khan, N. F., Rose, P. W., & Evans, J. (2012). Defining cancer survivorship: A more transparent
approach is needed. Journal of Cancer Survivorship, 6(1), 33–36.
http://doi.org/10.1007/s11764-011-0194-6
Kim, J.-M., Stewart, R., Kim, S.-W., Yang, S.-J., Shin, I.-S., & Yoon, J.-S. (2009). Insomnia,
depression, and physical disorders in late life: a 2-year longitudinal community study in
Koreans. Sleep, 32(9), 1221–1228.
62
Kim, S. H., Son, B. H., Hwang, S. Y., Han, W., Yang, J.-H., Lee, S., & Yun, Y. H. (2008).
Fatigue and depression in disease-free breast cancer survivors: prevalence, correlates, and
association with quality of life. Journal of Pain and Symptom Management, 35(6), 644–55.
http://doi.org/10.1016/j.jpainsymman.2007.08.012
Kornblith, A.B., Herndon, J.E., Weiss, R.B., Zhang, C., Zuckerman, E.L., Rosenberg, S.,…
(2003). Long-term adjustment of survivors of early-stage breast carcinoma, 20 years after
adjuvant chemotherapy. Cancer, 98(4), 679-689.
Kroenke, C. H., Chen, W. Y., Rosner, B., & Holmes, M. D. (2005). Weight, weight gain, and
survival after breast cancer diagnosis. Journal of Clinical Oncology : Official Journal of the
American Society of Clinical Oncology, 23(7), 1370–1378.
http://doi.org/10.1200/JCO.2005.01.079
Krogh, J., Nordentoft, M., Sterne, J. a C., & Lawlor, D. a. (2011). The effect of exercise in
clinically depressed adults: systematic review and meta-analysis of randomized controlled
trials. The Journal of Clinical Psychiatry, 72(4), 529–538.
http://doi.org/10.4088/JCP.08r04913blu
Kwan, M. L., Cohn, J. C., Armer, J. M., Stewart, B. R., & Cormier, J. N. (2011). Exercise in
patients with lymphedema: A systematic review of the contemporary literature. Journal of
Cancer Survivorship. http://doi.org/10.1007/s11764-011-0203-9
Larsen, R.N., Kingwell, B.A., Sethi, P., Cerin, E., Owen, N.,…Dunstan, D.W. (2014). Breaking
up prolonged sitting reduces resting blood pressure in overweight/obese adults. Nutrition,
Metabolism, & Cardiovaascular Diseases, 24(9), 976-82.
Ladwig, K. H., Röll, G., Breithardt, G., Budde, T., & Borggrefe, M. (1994). Post-infarction
depression and incomplete recovery 6 months after acute myocardial infarction. Lancet,
343(8888), 20–23. http://doi.org/10.1016/S0140-6736(94)90877-X
Lépine, J. P., Gastpar, M., Mendlewicz, J., & Tylee, A. (1997). Depression in the community:
the first pan-European study DEPRES (Depression Research in European Society).
International Clinical Psychopharmacology, 12(1), 19–29.

63
Lorizio, W., Wu, A. H. B., Beattie, M. S., Rugo, H., Tchu, S., Kerlikowske, K., & Ziv, E. (2012).
Clinical and biomarker predictors of side effects from tamoxifen. Breast Cancer Research
and Treatment, 132(3), 1107–1118. http://doi.org/10.1007/s10549-011-1893-4
Lynch, B. M. (2010). Sedentary behavior and cancer: a systematic review of the literature and
proposed biological mechanisms. Cancer Epidemiology, Biomarkers & Prevention : A
Publication of the American Association for Cancer Research, Cosponsored by the
American Society of Preventive Oncology, 19(11), 2691–709. http://doi.org/10.1158/1055-
9965.EPI-10-0815
Lynch, B. M., Cerin, E., Owen, N., Hawkes, A. L., & Aitken, J. F. (2008). Prospective
relationships of physical activity with quality of life among colorectal cancer survivors.
Journal of Clinical Oncology : Official Journal of the American Society of Clinical
Oncology, 26(27), 4480–7. http://doi.org/10.1200/JCO.2007.15.7917
Lynch, B. M., Dunstan, D. W., Healy, G. N., Winkler, E., Eakin, E., & Owen, N. (2010).
Objectively measured physical activity and sedentary time of breast cancer survivors, and
associations with adiposity: findings from NHANES (2003-2006). Cancer Causes &
Control : CCC, 21(2), 283–8. http://doi.org/10.1007/s10552-009-9460-6
Lynch, B. M., Dunstan, D. W., Vallance, J. K., & Owen, N. (2013). Don’t take cancer sitting
down: a new survivorship research agenda. Cancer, 119(11), 1928–35.
http://doi.org/10.1002/cncr.28028
Mack, D.E., Meldrum, L.S., Wilson, P.M., & Sabiston, C.M. (2013). Physical activity and
psychological health in breast cancer survivors: An application of basic psychological needs
theory. Applied Psychology: Health and Well-Being, 5(3), 369-88.
Mammen, G., & Faulkner, G. (2013). Physical activity and the prevention of depression: A
systematic review of prospective studies. American Journal of Preventive Medicine, 45(5),
649–657. http://doi.org/10.1016/j.amepre.2013.08.001
Mariotto, A. (2002). Trends in Use of Adjuvant Multi-Agent Chemotherapy and Tamoxifen for
Breast Cancer in the United States: 1975-1999. CancerSpectrum Knowledge Environment,
94(21), 1626–1634. http://doi.org/10.1093/jnci/94.21.1626
64
Markes, M., Brockow, T., & Resch, K. L. (2006). Exercise for women receiving adjuvant
therapy for breast cancer. The Cochrane Database of Systematic Reviews, (4), CD005001.
http://doi.org/10.1002/14651858.CD005001.pub2
Matthews, C. E., Chen, K. Y., Freedson, P. S., Buchowski, M. S., Beech, B. M., Pate, R. R., &
Troiano, R. P. (2008). Amount of time spent in sedentary behaviors in the United States,
2003-2004. American Journal of Epidemiology, 167(7), 875–881.
http://doi.org/10.1093/aje/kwm390
Matthews, C. E., George, S. M., Moore, S. C., Bowles, H. R., Blair, A., Park, Y., … Schatzkin,
A. (2012). Amount of time spent in sedentary behaviors and cause-specific mortality in US
adults. American Journal of Clinical Nutrition, 95(2), 437–445.
http://doi.org/10.3945/ajcn.111.019620
McDonough, M.H., Sabiston, C.M., Wrosch, C. (2013). Predicting changes in posttraumatic
growth and subjective well-being among breast cancer survivors: The role of social support
and stress. Pyschosocial-Oncology, 23(1), 114-20.
Mendes de Leon, C. F., Krumholz, H. M., Seeman, T. S., Vaccarino, V., Williams, C. S., Kasl, S.
V, & Berkman, L. F. (1998). Depression and risk of coronary heart disease in elderly men
and women: New Haven EPESE, 1982-1991. Established Populations for the
Epidemiologic Studies of the Elderly. Archives of Internal Medicine, 158(21), 2341–2348.
Meyerhardt, J. A., Heseltine, D., Niedzwiecki, D., Hollis, D., Saltz, L. B., Mayer, R. J., …
Fuchs, C. S. (2006). Impact of physical activity on cancer recurrence and survival in
patients with stage III colon cancer: findings from CALGB 89803. Journal of Clinical
Oncology : Official Journal of the American Society of Clinical Oncology, 24(22), 3535–41.
http://doi.org/10.1200/JCO.2006.06.0863
Motl, R. W., McAuley, E., & DiStefano, C. (2005). Is social desirability associated with self-
reported physical activity? Preventive Medicine, 40(6), 735–739.
http://doi.org/10.1016/j.ypmed.2004.09.016
Mullan, F. (1985). Seasons of survival: Reflections of a physcian with cancer. New England
Journal of Medicine, (313), 270–273.

65
National Institutes Of Health. (1998). Clinical guidelines on the identification, evaluation, and
treatment of overweight and obesity in adults: the evidence report. Obesity Research, 6,
51S–209S.
Owen, N., Healy, G. N., Matthews, C. E., & Dunstan, D. W. (2010). Too much sitting: the
population health science of sedentary behavior. Exercise and Sport Sciences Reviews,
38(3), 105–113. http://doi.org/10.1097/JES.0b013e3181e373a2
Patel, A. V., Bernstein, L., Deka, A., Feigelson, H. S., Campbell, P. T., Gapstur, S. M., … Thun,
M. J. (2010). Leisure time spent sitting in relation to total mortality in a prospective cohort
of US adults. Am J Epidemiol, 172, 419–29. http://doi.org/10.1093/aje/kwq155
Patterson, R. E., Cadmus, L. a, Emond, J. a, & Pierce, J. P. (2010). Physical activity, diet,
adiposity and female breast cancer prognosis: a review of the epidemiologic literature.
Maturitas, 66(1), 5–15. http://doi.org/10.1016/j.maturitas.2010.01.004
Penninx, B. W., Beekman, A. T., Honig, A., Deeg, D. J., Schoevers, R. A., van Eijk, J. T., & van
Tilburg, W. (2001). Depression and cardiac mortality: results from a community-based
longitudinal study. Archives of General Psychiatry, 58(3), 221–227.
http://doi.org/10.1001/archpsyc.58.3.221
Penninx, B. W., Guralnik, J. M., Pahor, M., Ferrucci, L., Cerhan, J. R., Wallace, R. B., & Havlik,
R. J. (1998). Chronically depressed mood and cancer risk in older persons. Journal of the
National Cancer Institute, 90(24), 1888–1893. http://doi.org/10.1093/jnci/90.24.1888
Phillips, S. M., Dodd, K. W., Steeves, J., McClain, J., Alfano, C. M., & McAuley, E. (2015).
Physical activity and sedentary behavior in breast cancer survivors: New insight into
activity patterns and potential intervention targets. Gynecologic Oncology.
http://doi.org/10.1016/j.ygyno.2015.05.026
Powell, K. E., Paluch, A. E., & Blair, S. N. (2011). Physical activity for health: What kind? How
much? How intense? On top of what? Annual Review of Public Health, 32, 349–365.
http://doi.org/10.1146/annurev-publhealth-031210-101151

66
Prince, S. A., Saunders, T. J., Gresty, K., & Reid, R. D. (2014). A comparison of the
effectiveness of physical activity and sedentary behaviour interventions in reducing
sedentary time in adults: A systematic review and meta-analysis of controlled trials. Obesity
Reviews. http://doi.org/10.1111/obr.12215
Proper, K. I., Singh, A. S., Van Mechelen, W., & Chinapaw, M. J. M. (2011). Sedentary
behaviors and health outcomes among adults: A systematic review of prospective studies.
American Journal of Preventive Medicine, 40(2), 174–182.
http://doi.org/10.1016/j.amepre.2010.10.015
Qiu, J., Yang, M., Chen, W., Gao, X., Liu, S., Shi, S., & Xie, B. (2012). Prevalence and
correlates of major depressive disorder in breast cancer survivors in Shanghai, China.
Psycho-Oncology, 21(12), 1331–7. http://doi.org/10.1002/pon.2075
Radloff, L. S. (1977). The CES-D Scale: A Self Report Depression Scale for Research in the
General. Applied Psychological Measurement, 1, 385–401.
http://doi.org/10.1177/014662167700100306
Rezende, L. F. M. de, Rodrigues Lopes, M., Rey-López, J. P., Matsudo, V. K. R., & Luiz, O. do
C. (2014). Sedentary behavior and health outcomes: an overview of systematic reviews.
PloS One, 9(8), e105620. http://doi.org/10.1371/journal.pone.0105620
Ristovski-Slijepcevic, S., & Bell, K. (2014). Rethinking assumptions about cancer survivorship.
Canadian Oncology Nursing Journal, 24(3), 166–168.
http://doi.org/10.5737/1181912x243166168
Rock, C. L., Doyle, C., Demark-Wahnefried, W., Meyerhardt, J., Courneya, K. S., Schwartz, A.
L., … Gansler, T. (2012). Nutrition and physical activity guidelines for cancer survivors.
CA: A Cancer Journal for Clinicians, 62(4), 243–74. http://doi.org/10.3322/caac.21142
Rockson, S. G. (1998). Precipitating factors in lymphedema: myths and realities. Cancer, 83(12
Suppl American), 2814–2816.
Rogers, L. Q., Markwell, S. J., Courneya, K. S., McAuley, E., & Verhulst, S. (2011). Physical
activity type and intensity among rural breast cancer survivors: Patterns and associations

67
with fatigue and depressive symptoms. Journal of Cancer Survivorship, 5(1), 54–61.
http://doi.org/10.1007/s11764-010-0160-8
Rosenberg, D. E., Norman, G. J., Wagner, N., Patrick, K., Calfas, K. J., & Sallis, J. F. (2010).
Reliability and validity of the Sedentary Behavior Questionnaire (SBQ) for adults. Journal
of Physical Activity & Health, 7(6), 697–705.
Roshanaei-Moghaddam, B., Katon, W. J., & Russo, J. (2009). The longitudinal effects of
depression on physical activity. General Hospital Psychiatry, 31, 306–315.
http://doi.org/10.1016/j.genhosppsych.2009.04.002
Rot, M. A. H., Mathew, S. J., & Charney, D. S. (2009). Neurobiological mechanisms in major
depressive disorder. CMAJ. http://doi.org/10.1503/cmaj.080697
Sabiston, C. M., & Brunet, J. (2011). Reviewing the Benefits of Physical Activity During Cancer
Survivorship. American Journal of Lifestyle Medicine, 6(2), 167–177.
http://doi.org/10.1177/1559827611407023
Sabiston, C.M., Brunet, J., & Burke. (2012). Pain, movement and mind. Does physical activity
mediate the relationship between pain and mental health among survivors of breast cancer?
Journal of Clinical Pain, 28, 489-495.
Sabiston, C. M., Brunet, J., Vallance, J. K., & Meterissian, S. (2014). Prospective examination of
objectively assessed physical activity and sedentary time after breast cancer treatment:
Sitting on the crest of the teachable moment. Cancer Epidemiology Biomarkers and
Prevention, 23(7), 1324–1330. http://doi.org/10.1158/1055-9965.EPI-13-1179
Sagen, A., Kåresen, R., & Risberg, M. A. (2009). Physical activity for the affected limb and arm
lymphedema after breast cancer surgery. A prospective, randomized controlled trial with
two years follow-up. Acta Oncologica (Stockholm, Sweden), 48(8), 1102–1110.
http://doi.org/10.3109/02841860903061683
Sallis, J. F., Owen, N., & Fotheringham, M. J. (2000). Behavioral epidemiology: a systematic
framework to classify phases of research on health promotion and disease prevention.
68
Annals of Behavioral Medicine : A Publication of the Society of Behavioral Medicine,
22(4), 294–8. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11253440
Saunders, T. J., Prince, S. A., & Tremblay, M. S. (2011). Clustering of children’s activity
behaviour: the use of self-report versus direct measures. The International Journal of
Behavioral Nutrition and Physical Activity. http://doi.org/10.1186/1479-5868-8-48
Saunders, T. J., Tremblay, M. S., Mathieu, M. È., Henderson, M., O’Loughlin, J., Tremblay, A.,
& Chaput, J. P. (2013). Associations of sedentary behavior, sedentary bouts and breaks in
sedentary time with cardiometabolic risk in children with a family history of obesity. PLoS
ONE, 8(11). http://doi.org/10.1371/journal.pone.0079143
Schmitz, K. H., Courneya, K. S., Matthews, C., Demark-Wahnefried, W., Galvão, D. A., Pinto,
B. M., … Schwartz, A. L. (2010). American college of sports medicine roundtable on
exercise guidelines for cancer survivors. Medicine and Science in Sports and Exercise.
http://doi.org/10.1249/MSS.0b013e3181e0c112
Segar, M. L., Katch, V. L., Roth, R. S., Garcia, A. W., Portner, T. I., Glickman, S. G., …
Wilkins, E. G. (1998). The effect of aerobic exercise on self-esteem and depressive and
anxiety symptoms among breast cancer survivors. Oncology Nursing Forum, 25(1), 107–
113.
Shields, M., & Wilkins, K. (2009). An update on mammography use in Canada. Health Reports,
20(3), 7–19. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/19813435
Spaner, D., Bland, R. C., & Newman, S. C. (1994). Epidemiology of psychiatric disorders in
Edmonton. Major depressive disorder. Acta Psychiatrica Scandinavica. Supplementum,
376, 7–15.
Speck, R. M., Courneya, K. S., Mâsse, L. C., Duval, S., & Schmitz, K. H. (2010). An update of
controlled physical activity trials in cancer survivors: a systematic review and meta-
analysis. Journal of Cancer Survivorship : Research and Practice, 4(2), 87–100.
http://doi.org/10.1007/s11764-009-0110-5

69
Stamatakis, E., Hamer, M., & Dunstan, D. W. (2011). Screen-Based Entertainment Time, All-
Cause Mortality, and Cardiovascular Events. Journal of the American College of
Cardiology. http://doi.org/10.1016/j.jacc.2010.05.065
Sugiyama, T., Healy, G. N., Dunstan, D. W., Salmon, J., & Owen, N. (2008). Joint associations
of multiple leisure-time sedentary behaviours and physical activity with obesity in
Australian adults. The International Journal of Behavioral Nutrition and Physical Activity,
5, 35. http://doi.org/10.1186/1479-5868-5-35
Swartz, A.M., Squires, L., & Strath, S.J. (2011). Energy expenditure of interruptions to sedentary
behaviour. International Journal of Behavioural Nutrition and Physical Activity, 8(69), 1-7.
Teychenne, M., Ball, K., & Salmon, J. (2010). Sedentary behavior and depression among adults:
a review. International Journal of Behavioral Medicine, 17(4), 246–54.
http://doi.org/10.1007/s12529-010-9075-z
Thorp, A. A., Owen, N., Neuhaus, M., & Dunstan, D. W. (2011). Sedentary behaviors and
subsequent health outcomes in adults: A systematic review of longitudinal studies,
19962011. American Journal of Preventive Medicine, 41(2), 207–215.
http://doi.org/10.1016/j.amepre.2011.05.004
Tremblay, M. S. (2013). Letter to the Editor: Standardized use of the terms “sedentary” and
“sedentary behaviours.” Mental Health and Physical Activity, 6(1), 55–56.
http://doi.org/10.1016/j.mhpa.2012.06.001
Tremblay, M. S., Colley, R. C., Saunders, T. J., Healy, G. N., & Owen, N. (2010). Physiological
and health implications of a sedentary lifestyle. Applied Physiology, Nutrition, and
Metabolism = Physiologie Appliquee, Nutrition et Metabolisme, 35(6), 725–740.
http://doi.org/10.1139/H10-079
Tremblay, M. S., Leblanc, A. G., Janssen, I., Kho, M. E., Hicks, A., Murumets, K., … Duggan,
M. (2011). Canadian sedentary behaviour guidelines for children and youth. Applied
Physiology, Nutrition, and Metabolism = Physiologie Appliquee, Nutrition et Metabolisme,
36(1), 59–64; 65–71. http://doi.org/10.1139/H11-012

70
Trinh, L., Amireault, S., Lacombe, J., & Sabiston, C. M. (2015). Physical and psychological
health among breast cancer survivors : interactions with sedentary behavior and physical
activity.
Trinh, L., Arbour-nicitopoulos, K. P., Sabiston, C. M., Alibhai, S. M., Jones, J. M., Berry, S. R.,
… Faulkner, G. E. (2015). A Qualitative Study Exploring the Perceptions of Sedentary
Behavior in Prostate Cancer Survivors Receiving Androgen-Deprivation Therapy, 42(4),
398–406. http://doi.org/10.1188/15.ONF.398-406
Troiano, R. P., Berrigan, D., Dodd, K. W., Mâsse, L. C., Tilert, T., & Mcdowell, M. (2008).
Physical activity in the United States measured by accelerometer. Medicine and Science in
Sports and Exercise, 40(1), 181–188. http://doi.org/10.1249/mss.0b013e31815a51b3
Trost, S. G., Mciver, K. L., & Pate, R. R. (2005). Conducting accelerometer-based activity
assessments in field-based research. In Medicine and Science in Sports and Exercise (Vol.
37). http://doi.org/10.1249/01.mss.0000185657.86065.98
Ullrich-French, S., & Cox, A. (2009). Using cluster analysis to examine the combinations of
motivation regulations of physical education students. Journal of Sport & Exercise
Psychology, 31(3), 358–379.
Ustün, T. B., Ayuso-Mateos, J. L., Chatterji, S., Mathers, C., & Murray, C. J. L. (2004). Global
burden of depressive disorders in the year 2000. The British Journal of Psychiatry : The
Journal of Mental Science, 184, 386–392. http://doi.org/10.1192/bjp.184.5.386
Van der Ploeg, H. P., Chey, T., Korda, R. J., Banks, E., & Bauman, A. (2012). Sitting Time and
All-Cause Mortality Risk in 222 497 Australian Adults. Archives of Internal Medicine.
http://doi.org/10.1001/archinternmed.2011.2174
Verloigne, M., Van Lippevelde, W., Maes, L., Yıldırım, M., Chinapaw, M., Manios, Y., … De
Bourdeaudhuij, I. (2012). Levels of Physical Activity and Sedentary Time among 10 to 12
year-old Boys and Girls across 5 European countries using Accelerometers: an
Observational Study within the ENERGY Project. The International Journal of Behavioral
Nutrition and Physical Activity, 9(1), 34. http://doi.org/10.1186/1479-5868-9-34
71
Wang, J.C.K., & Biddle, S.J.H. (2001). Young people's motivational profiles in physi1-cal
acitivity: A cluster analysis. Journal of Sport & Exercise Psychology, 23(1), 1-22
Westerterp, K. R. (2008). Physical activity as determinant of daily energy expenditure.
Physiology & Behavior, 93(4-5), 1039–1043. http://doi.org/10.1016/j.physbeh.2008.01.021
Weyerer, S., & Kupfer, B. (1994). Physical exercise and psychological health. Sports Med, 17,
108–116.
Wilmot, E. G., Edwardson, C. L., Achana, F. A., Davies, M. J., Gorely, T., Gray, L. J., …
Biddle, S. J. H. (2012). Sedentary time in adults and the association with diabetes,
cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia,
55(11), 2895–2905. http://doi.org/10.1007/s00125-012-2677-z
Woodcock, J., Franco, O. H., Orsini, N., & Roberts, I. (2011). Non-vigorous physical activity
and all-cause mortality: Systematic review and meta-analysis of cohort studies.
International Journal of Epidemiology, 40(1), 121–138. http://doi.org/10.1093/ije/dyq104
Wrosch, C., & Sabiston, C. M. (2013). Goal adjustment, physical and sedentary activity, and
well-being and health among breast cancer survivors. Psycho-Oncology, 22(3), 581–9.
http://doi.org/10.1002/pon.3037
Young-McCaughan, S., & Arzola, S. M. (2007). Exercise Intervention Research for Patients
With Cancer on Treatment. Seminars in Oncology Nursing, 23(4), 264–274.
http://doi.org/10.1016/j.soncn.2007.08.004
Zainal, N. Z., Nik-Jaafar, N. R., Baharudin, A., Sabki, Z. A., & Ng, C. G. (2013). Prevalence of
depression in breast cancer survivors: a systematic review of observational studies. Asian
Pacific Journal of Cancer Prevention : APJCP, 14(4), 2649–56. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/23725190
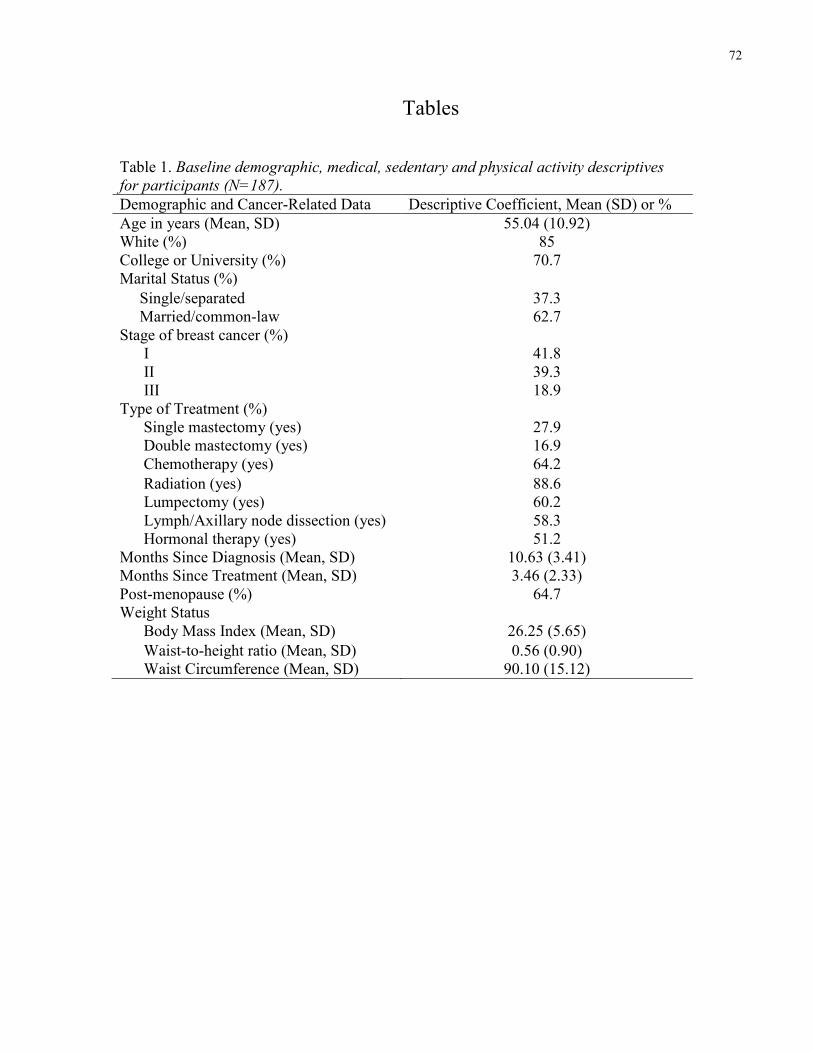
72
Tables
Table 1. Baseline demographic, medical, sedentary and physical activity descriptives
for participants (N=187).
Demographic and Cancer-Related Data Descriptive Coefficient, Mean (SD) or % Age in years (Mean, SD) 55.04 (10.92) White (%) 85 College or University (%) 70.7 Marital Status (%) Single/separated 37.3 Married/common-law 62.7 Stage of breast cancer (%) I 41.8 II 39.3 III 18.9 Type of Treatment (%) Single mastectomy (yes) 27.9 Double mastectomy (yes) 16.9 Chemotherapy (yes) 64.2 Radiation (yes) 88.6 Lumpectomy (yes) 60.2 Lymph/Axillary node dissection (yes) 58.3 Hormonal therapy (yes) 51.2 Months Since Diagnosis (Mean, SD) 10.63 (3.41) Months Since Treatment (Mean, SD) 3.46 (2.33) Post-menopause (%) 64.7 Weight Status Body Mass Index (Mean, SD) 26.25 (5.65) Waist-to-height ratio (Mean, SD) 0.56 (0.90) Waist Circumference (Mean, SD) 90.10 (15.12)

73
Table 2. SITT variables by cluster membership (n=187). Variable Cluster One
n=64 (M, SD) Cluster Two
n=123 (M, SD) Total
N = 187 (M, SD)
Average number of 10 min bouts 102.28 (22.98) 98.59 (23.86) 99.85 (23.57) Average time in 10 min bouts 23.18 (3.13) 21.86 (3.06) 22.31 (3.14)* Average number of 30 min bouts 22.26 (9.39) 19.10 (9.13) 20.18 (9.32)* Average time in 30 min bouts 47.70 (5.76) 46.13 (5.45) 46.67 (5.59) Average time in SED breaks 33.94 (9.98) 35.17 (10.23) 34.75 (10.14) Self-report SED 195.20 (105.54) 115.14 (78.74) 142.54 (96.38)** Screen-time 572.43 (127.09) 233.12 (104.75) 349.25 (196.79)** Reading 115.37 (77.89) 102.38 (71.96) 106.82 (74.09) Objective SED 539.27 (87.41) 521.83 (88.87) 527.80 (88.53) **. Univariate model significant at the .001 level (2-tailed). *. Univariate model significant at the .05 level (2-tailed).

74
Table 3. Bivariate correlations by sedentary behaviour cluster membership variables and self-report/objective
moderate-to-vigorous physical activity (n=187). Variable 1 2 3 4 5 6 7 8 9 10
1. Self-report MVPA
2. Objective MVPA .45**
3. Self-report SED -.10 -.16*
4. Screen-time -.12 -.28** .37**
5. Reading .02 -.12 .08 .10
6. Avg number 10 minute bouts -.17* -.24** .18* .12 .09
7. Avg time per 10 minute bouts .06 -.24** .26** .23** .17* .23**
8. Avg number of 30 minute bouts -.08 -.31** .22** .19** .18* .67** .81**
9. Avg time per 30 minute bouts .12 -.03 .21** .16* .10 -.04 .64** .29**
10. Objective SED -.15* -.28** .19* .10 .14 .84** .46** .75** .16*
11. Average time of SED breaks .15* .18* -.13 -.05 -.11 -.75** -.11 -.45** .09 -.83**
**. Correlation is significant at the 0.01 level (2-tailed). *. Correlation is significant at the 0.05 level (2-tailed).

75
Table 4. Bivariate correlations between cluster membership variables and continuous depression
(n=187).
Variable 1 2 3 4 5 6 7 8 9
1. Depression
2. Self-report SED .13
3. Screen-time .15 .37**
4. Reading -.03 .08 .10
5. Avg number of 10 minute bouts
.02 .18* .12 .09
6. Avg time per 10 minute bouts .05 .26** .23** .17* .23**
7. Avg number of 30 minute bouts
.05 .22** .19** .18* .67** .81**
8. Avg time per 30 minute bouts -.05 .21** .16* .10 -.04 .64** .29**
9. Avg time in SED breaks .03 -.13 -.05 -.11 -.75** -.11 -.45** .09
10. Objective SED -.02 .19* .10 .14 .84** .46** .75** .16* -.83**
**. Correlation is significant at the 0.01 level (2-tailed).
*. Correlation is significant at the 0.05 level (2-tailed).

76
Table 5. MANOVA and chi square examining medical, demographic and weight status
variables by cluster membership (n=187). Variable Total
(n=187) Cluster 1 (n=64) Cluster 2 (n=123)
Age (M, SD) 54.44 (10.85)* 57.22 (11.16) 53.00 (10.44) BMI (M, SD) 26.24 (5.60)* 27.73 (5.90) 25.46 (5.30) Waist circumference (M, SD) 90.17 (15.41)** 96.45 (16.68) 86.90 (13.66) Waist-to-height ratio (M, SD) .56 (.09)** .59 (.09) .54 (.09) LTEQ MVPA (M, SD) 23.75 (24.26)* 18.83 (20.50) 26.31 (25.71) Objective MVPA (M, SD) 25.21 (18.28)** 18.00 (13.88) 28.96 (19.20) Time since diagnosis (M, SD) 10.73 (3.35) 10.59 (3.49) 10.81 (3.29) Time since treatment (M, SD) 3.47 (2.32) 3.19 (2.17) 3.61 (2.39) University (% yes) 51.2 ** 32.8 59.3 White ethnicity (% yes) 85.1 85.9 84.6 Lymph/axillary node dissection (% yes) 57.7* 46.9 64.2 Lumpectomy (% yes) 60.2 65.6 59.3 Single mastectomy (% yes) 27.9 23.4 28.5 Double mastectomy (% yes) 16.9 14.1 16.3 Reconstructive surgery (% yes) 7.0 3.1 8.9 Chemotherapy (% yes) 64.2 62.5 65.9 Radiotherapy (% yes) 88.6 92.2 87.8 Hormonal therapy (% yes) 51.2 48.4 51.2 BMI overweight (% yes) 50.2* 60.9 45.5 Waist circumference over 88 cm (% yes) 53.2** 70.3 44.7 Waist-to-height ratio (% yes) 72.1* 81.3 67.5 Married (% yes) 64.2 59.4 69.1 Cancer stage 1 or 2 (% yes) 81.1 23.4 18.7 Post-menopausal (% yes) 64.7 71.9 57.7 *Indicates significance at the .05 level. **Indicates significance at the .001 level.

77
Table 6. Logistic regression of main Study variables predicting clinical
depression (n=187). Variable β SE OR 95% CI University Education 0.02 0.38 1.02 0.49-2.13 Age (years) -0.02 0.02 0.98 0.95-1.02 Lymph/axillary node dissection 0.60 0.38 1.82 0.87-3.82 Overweight -0.03 0.37 0.98 0.47-2.02 Self-report MVPA 0.00 0.01 1.00 0.99-1.02 Objective MVPA -0.03 0.01 0.97* 0.95-0.99 SED cluster membership -0.77 0.39 0.46* 0.22-0.98 *Indicates significance at the .05 level. **Indicates significance at the .001 level.
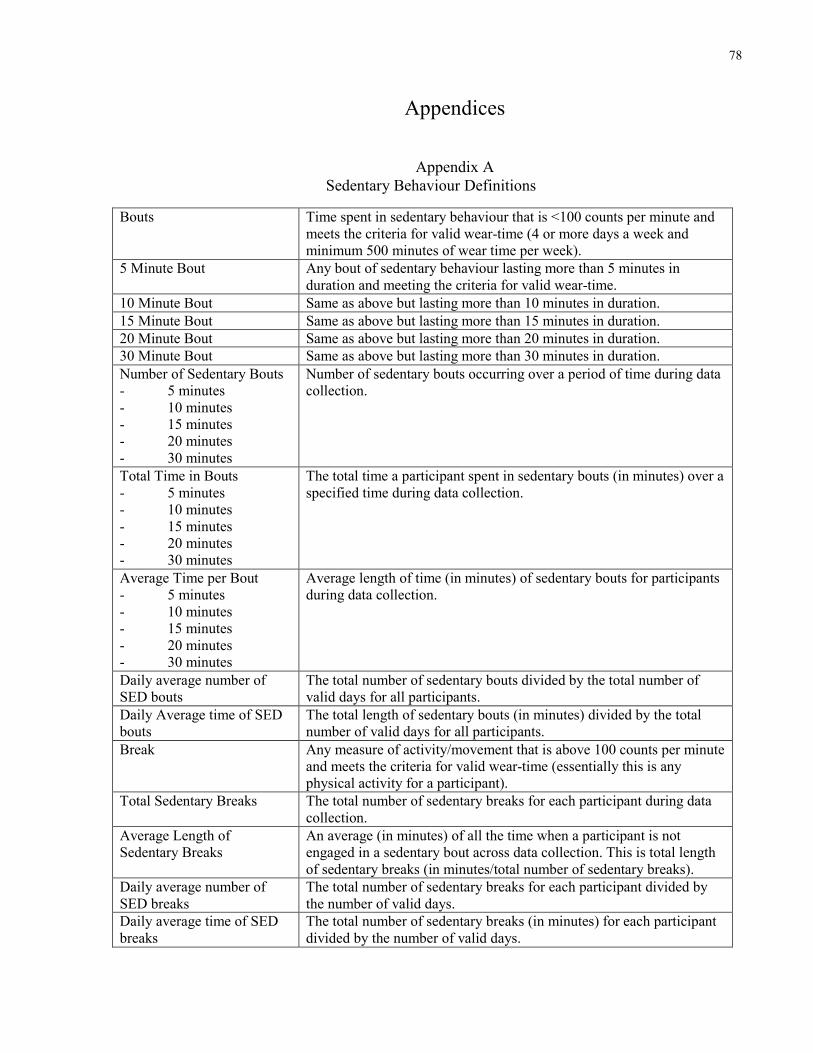
78
Appendices
Appendix A Sedentary Behaviour Definitions
Bouts Time spent in sedentary behaviour that is <100 counts per minute and meets the criteria for valid wear-time (4 or more days a week and minimum 500 minutes of wear time per week).
5 Minute Bout Any bout of sedentary behaviour lasting more than 5 minutes in duration and meeting the criteria for valid wear-time.
10 Minute Bout Same as above but lasting more than 10 minutes in duration. 15 Minute Bout Same as above but lasting more than 15 minutes in duration. 20 Minute Bout Same as above but lasting more than 20 minutes in duration. 30 Minute Bout Same as above but lasting more than 30 minutes in duration. Number of Sedentary Bouts - 5 minutes - 10 minutes - 15 minutes - 20 minutes - 30 minutes
Number of sedentary bouts occurring over a period of time during data collection.
Total Time in Bouts - 5 minutes - 10 minutes - 15 minutes - 20 minutes - 30 minutes
The total time a participant spent in sedentary bouts (in minutes) over a specified time during data collection.
Average Time per Bout - 5 minutes - 10 minutes - 15 minutes - 20 minutes - 30 minutes
Average length of time (in minutes) of sedentary bouts for participants during data collection.
Daily average number of SED bouts
The total number of sedentary bouts divided by the total number of valid days for all participants.
Daily Average time of SED bouts
The total length of sedentary bouts (in minutes) divided by the total number of valid days for all participants.
Break Any measure of activity/movement that is above 100 counts per minute and meets the criteria for valid wear-time (essentially this is any physical activity for a participant).
Total Sedentary Breaks The total number of sedentary breaks for each participant during data collection.
Average Length of Sedentary Breaks
An average (in minutes) of all the time when a participant is not engaged in a sedentary bout across data collection. This is total length of sedentary breaks (in minutes/total number of sedentary breaks).
Daily average number of SED breaks
The total number of sedentary breaks for each participant divided by the number of valid days.
Daily average time of SED breaks
The total number of sedentary breaks (in minutes) for each participant divided by the number of valid days.
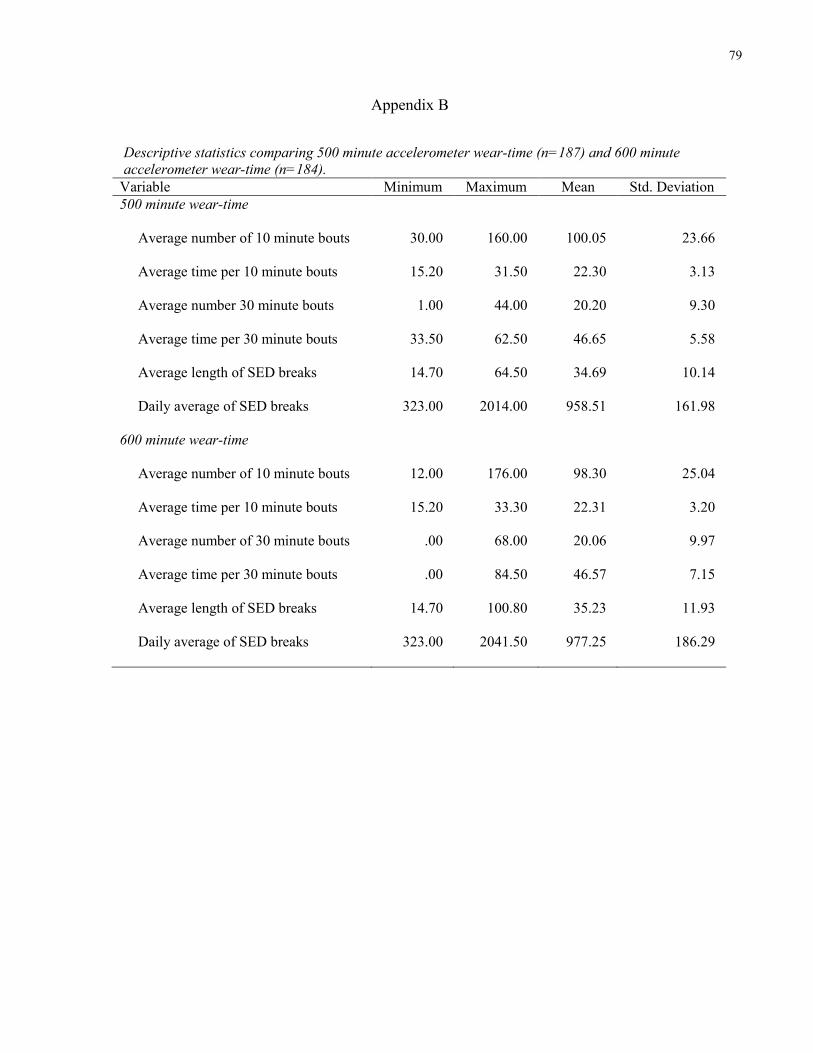
79
Appendix B
Descriptive statistics comparing 500 minute accelerometer wear-time (n=187) and 600 minute
accelerometer wear-time (n=184).
Variable Minimum Maximum Mean Std. Deviation 500 minute wear-time
Average number of 10 minute bouts 30.00 160.00 100.05 23.66
Average time per 10 minute bouts 15.20 31.50 22.30 3.13
Average number 30 minute bouts 1.00 44.00 20.20 9.30
Average time per 30 minute bouts 33.50 62.50 46.65 5.58
Average length of SED breaks 14.70 64.50 34.69 10.14
Daily average of SED breaks 323.00 2014.00 958.51 161.98
600 minute wear-time
Average number of 10 minute bouts 12.00 176.00 98.30 25.04
Average time per 10 minute bouts 15.20 33.30 22.31 3.20
Average number of 30 minute bouts .00 68.00 20.06 9.97
Average time per 30 minute bouts .00 84.50 46.57 7.15
Average length of SED breaks 14.70 100.80 35.23 11.93
Daily average of SED breaks 323.00 2041.50 977.25 186.29
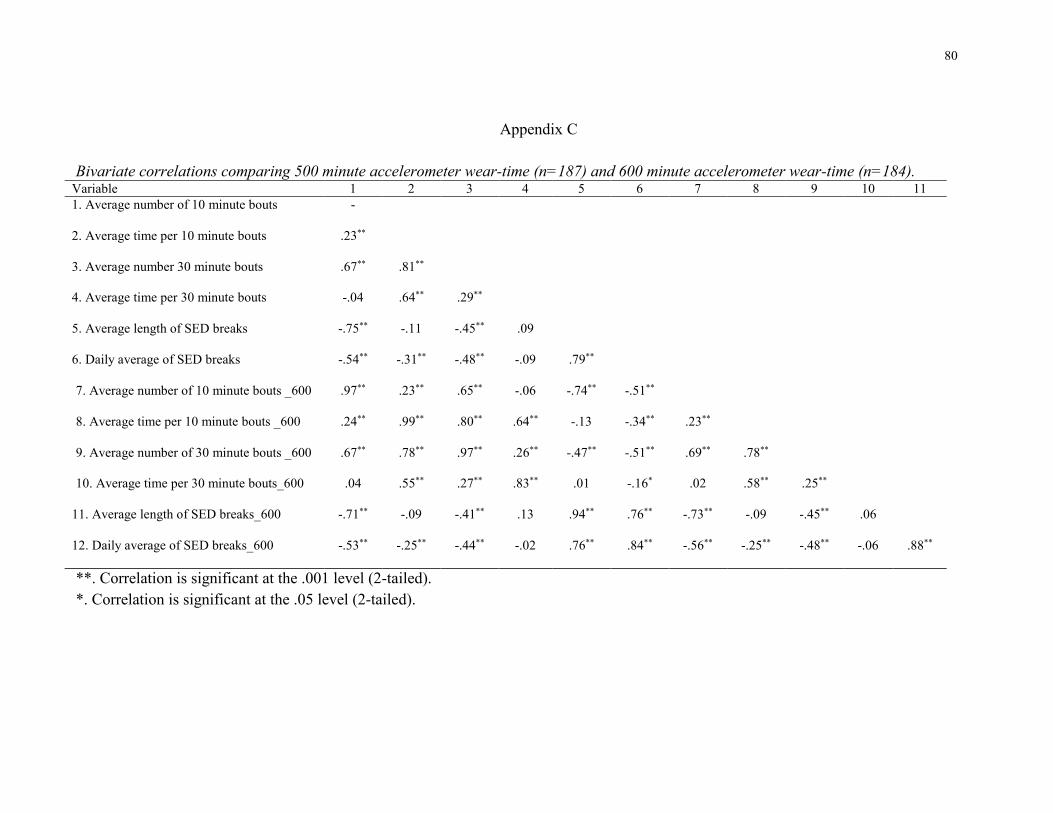
80
Appendix C
Bivariate correlations comparing 500 minute accelerometer wear-time (n=187) and 600 minute accelerometer wear-time (n=184). Variable 1 2 3 4 5 6 7 8 9 10 11 1. Average number of 10 minute bouts -
2. Average time per 10 minute bouts .23**
3. Average number 30 minute bouts .67** .81**
4. Average time per 30 minute bouts -.04 .64** .29**
5. Average length of SED breaks -.75** -.11 -.45** .09
6. Daily average of SED breaks -.54** -.31** -.48** -.09 .79**
7. Average number of 10 minute bouts _600 .97** .23** .65** -.06 -.74** -.51**
8. Average time per 10 minute bouts _600 .24** .99** .80** .64** -.13 -.34** .23**
9. Average number of 30 minute bouts _600 .67** .78** .97** .26** -.47** -.51** .69** .78**
10. Average time per 30 minute bouts_600 .04 .55** .27** .83** .01 -.16* .02 .58** .25**
11. Average length of SED breaks_600 -.71** -.09 -.41** .13 .94** .76** -.73** -.09 -.45** .06
12. Daily average of SED breaks_600 -.53** -.25** -.44** -.02 .76** .84** -.56** -.25** -.48** -.06 .88**
**. Correlation is significant at the .001 level (2-tailed). *. Correlation is significant at the .05 level (2-tailed).

81
Appendix D
Sedentary behaviour frequency (S in the SITT principle) and interruptions (I in the SITT
principle), time (T in the SIIT principle) and type (T in the SITT principle) using objective
and self-report data (n=187). Variable Minimum Maximum Mean Std. Deviation SED frequency/interupptions Avg number of 10 minute bouts 30.00 160.00 100.0479 23.66077 Avg time in 10 minute bouts 15.20 31.50 22.2989 3.13242 Avg number of 15 minute bouts 7.00 129.00 61.1755 18.19050 Avg time in 15 minute bouts 19.90 40.80 29.0000 3.80777 Avg number of 20 minute bouts 3.00 108.00 41.2074 14.73272 Avg time in 20 minute bouts 24.30 47.50 34.9686 4.43063 Avg number of 30 minute bouts 1.00 44.00 20.2048 9.29992 Avg time in 30 minute bouts 33.50 62.50 46.6500 5.58132 Avg time SED Breaks 14.70 64.50 34.6947 10.13974 Time/Type Objective SED 321.00 778.14 528.19 88.46 LTEQ SED .00 432.00 144.82 98.55 Screen-time .00 898.00 348.77 195.85 Reading .00 315.00 108.24 73.47 * NOTE: all values are presented in minutes/day.

82
Appendix E
Bivariate correlations between demographic and medical covariates (n=187). Variable 1 2 3 4 5 6 7 8 9 10 11 12 13 14 1. Age -
2. Income .05
3. Marital status .29** -.09
4. Education -.17* .04 -.11
5. Lymph/axillary node -.13 -.06 -.02 .07
6. Lumpectomy .09 .07 .04 .05 -.04
7. Single mastectomy .04 .09 -.06 .01 .04 -.49**
8. Double mastectomy -.28** .01 -.13 .11 .01 -.37** -.16*
9. Reconstructive surgery -.17* -.04 .05 .003 .04 -.14 -.04 .45**
10. Chemotherapy -.36** -.02 -.19** .10 .22** -.16* .09 .25** .16*
11. Radiotherapy .14 .03 .11 -.08 -.09 .19** -.09 -.38** -.33** -.27**
12. Hormone therapy -.06 .14 -.11 .20** -.03 .02 -.04 .18* .03 .04 -.04
13. Time since diagnosisa -.21** -.02 -.13 -.05 .20** -.02 .06 .10 .09 .39** .10 .05
14. Time since treatmenta .07 -.01 -.02 -.04 -.02 .06 .01 -.07 .01 -.13 -.04 .06 .36**
15. Cancer stage -.23** .11 -.16* .16* .18** -.14* .06 .21** -.05 .44** -.05 .03 .31** -.09
**. Correlation is significant at the .001 level (2-tailed). *. Correlation is significant at the .05 level (2-tailed). aRefers to time in months.

83
Appendix F
Bivariate correlations between objective sedentary behaviour and measures of weight status (n=187). Variable 1 2 3 4 5 6 7 8 9 10 11 12 13 14
1. Body mass index -
2. Waist circumference .72**
3. Waist-to-height ratio .84** .87**
4. Average number of 10 min bouts .09 .06 .10
5. Average time in 10 min bouts .09 .14 .10 .23**
6. Average number of 15 min bouts .06 .08 .08 .92** .49**
7. Average time in 15 min bouts .13 .13 .12 .14 .94** .32**
8. Average number of 20 min bouts .08 .12 .18 .84** .64** .96** .48**
9. Average time in 20 min bouts .08 .06 .06 .06 .85** .21** .94** .31**
10. Average number of 30 min bouts .09 .14 .12 .67** .81** .83** .71** .90** .59**
11. Average time in 30 min bouts .09 .00 .02 -.04 .64** .07 .73** .16* .80** .29**
12. Average length of SED breaks -.01 .02 -.02 -.75** -.11 -.67** -.02 -.59** .02 -.45** .09
13. Daily average time in SED breaks .00 -.03 -.03 -.54** -.31** -.56** -.20** -.55** -.16* -.48** -.09 .79**
14. Objective SED .10 .06 .10 .84** .46** .85** .37** .81** .30** .75** .16* -.83** -.61**
15. Percent time SED .13 .11 .11 .73** .52** .80** .38** .80** .29** .75** .12 -.69** -.55** .82**
**. Correlation is significant at the .001 level (2-tailed). *. Correlation is significant at the .05 level (2-tailed).

84
Appendix G
Bivariate correlations between self-report sedentary behavior and measures of weight status (n=187). Variable 1 2 3 4 5 1. Body mass index -
2. Waist circumference .72**
3. Waist-to-height ratio .84** .87**
4. LTEQ SED .14* .24** .21**
5. LTEQ Screen-time .18* .28** .25** .37**
6. LTEQ Reading .01 -.02 .02 .08 .10
**. Correlation is significant at the .001 level (2-tailed). *. Correlation is significant at the .05 level (2-tailed).