Section 2: Medication Safety During Transitions of Care ...
32
Section 2: Medication Safety During Transitions of Care: Clinical Implications Acollection of tools for use by pharmacists in any caresetting. These tools are intended to assist inidentifying and focusing on key medication classes and disease states to optimize medication safety during transitions of care.
Transcript of Section 2: Medication Safety During Transitions of Care ...
Section 2:Medication Safety During Transitions
of Care: Clinical ImplicationsA collection of tools for use by pharmacists in any caresetting.These tools are intended to assist inidentifying and focusing on
key medication classes and disease states to optimize medication safety during transitions of care.
Section 2.5:Tools to Manage
Medications Safely
This section is divided into 8 Parts:
Section 2.5:Tools to Manage MedicationsSafely
Part 2.5.1 AnticoagulantsPart 2.5.2 HypoglycemicsPart 2.5.3 OpioidsPart 2.5.4 PsychotropicsPart 2.5.5 AntimicrobialsPart 2.5.6 Narrow Therapeutic IndexMedicationsPart 2.5.7 Anticholinergic/Sedation/Fall RiskMedicationsPart 2.5.8 Pharmacogenomics
Part 2.5.1: Anticoagulants
Anticoagulant Tools• University of Michigan Anticoagulation Toolkit
• considerations when selecting between warfarin vs.DOACs• updated to reflect 2016 CHESTGuidelines
Link: http://www.anticoagulationtoolkit.org/sites/default/files/toolkit_pdfs/toolkitfull.pdf• MAQI2 Anticoagulation Toolkit iPhone App (FREE)
• Includes CHADS-VASc and HAS-BLED calculators, warfarin dose adjustment calculator(based on RE- LY Trialalgorithm), and above University of Michigan AnticoagulationToolkit
• Resource: This link directs you to the ISMP Medication Safety Self Assessment® for Antithrombotic Therapyhttps://www.ismp.org/assessments/antithrombotic-therapy
• Resource: This link directs you to the ISMP Example of Health-Care Failure Mode and Effects Analysis (FMEA) for Anticoagulants
https://www.ismp.org/sites/default/files/attachments/2018-02/FMEAofAnticoagulants.pdf• Resource: This link directs you to the ISMP High-Alert Medication Feature: Anticoagulant Safety Takes Center Stage In 2007
https://www.ismp.org/resources/high-alert-medication-feature-anticoagulant-safety-takes-center-stage-2007• wŜǎƻdzNJŎŜΥ This link directs you to the IHI: Reduce Adverse Drug Events Involving Anticoagulants page: https://www.ihi.org/resources/Pages/Changes/ReduceAdverseDrugEventsInvolvingAnticoagulants.aspx
Part 2.5.2: Hypoglycemics
Hypoglycemics• 2018 ADA Standards of Care:
• Avoid insulin sliding scale• Have higher clinical targets in older adults• Diabetes Management in long-term care and skilled nursing
facilities Link: http://care.diabetesjournals.org/content/39/2/308• ADA Older Adults: Standards of Medical Care in Diabetes—2018
http://care.diabetesjournals.org/content/41/Supplement_1/S119 Society of Hospital Medicine: The Glycemic Control ImplementationGuide
Link: http://tools.hospitalmedicine.org/resource_rooms/imp_guides/GC/GC_Workbook.pdf
• Treating the Elderly Diabetic Patient: SpecialConsiderationsCitation: Kezerle L, Shalev L, Barski L. Treating the elderly diabetic patient: special considerations. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy. 2014;7:391-400. doi:10.2147/DMSO.S48898.
•
Part 2.5.3: Opioids

Opioid Prescribing• Nonpharmacologic therapy and nonopioid pharmacologic therapy preferredfor
chronic pain• Only use opioids if expected benefits outweighrisks
• When starting, use immediate-release at lowest effective dose at no greater quantitythanexpected duration of pain
• Continue only if clinically meaningful improvement in pain and function
• Discuss known risks with patient, evaluate risk factors and incorporate strategiesto mitigate risk• Refer to state prescription drug monitoringprogram (PDMP)• Consider urine drug testing before starting therapy and annually to assess for opioid misuse• Establish realistic goals with patient
• Avoid concurrent opioids andbenzodiazepines
Opioid Prescribing Resources• Interagency Guideline on Prescribing Opioids for Pain by Washington State Medical Directors
Group 2015 Link: http://www.agencymeddirectors.wa.gov/Files/2015AMDGOpioidGuideline.pdf
• Managing Pain in the Geriatric Patient, Journal of the American OsteopathicAssociation Link: http://jaoa.org/article.aspx?articleid=2093506
• CDC Guidelines for Prescribing Opioids in ChronicPainCitation: Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain —United States, 2016. MMWR Recomm Rep 2016;65(No. RR-1):1–49.Link: http://www.cdc.gov/drugoverdose/pdf/guidelines_factsheet-a.pdf
Summary of above CDCguidelines:Link: http://dx.doi.org/10.15585/mmwr.rr6501e1
• AMDA Clinical Practice Guidelines for Pain(Members only) Link:http://www.paltc.org/topic/pain-management
Opioid Dosing• Medscape Opioids Equivalents and Conversions
Link: http://emedicine.medscape.com/article/2138678-overview
• An 8 step approach to exchanging one opioid agent or rout of administration foranother (copyright)
Link: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1069064/
• Opiod Dose calculator (both opioid naïve and conversion calculator) Link: http://opioidcalculator.practicalpainmanagement.com
• Opioids converter program GlobalRPhLink: http://www.globalrph.com/narcoticonv.htm
jesse_000
Cross-Out
Pain Assessment• University of Iowa Assessing Geriatric Pain
• Tools for assessing and treating pain in cognitively intact and cognitively impairedLink: https://geriatricpain.org/pain-assessment
• AMDA guidelines Pain assessment in Assisted LivingLink: http://www.assistedlivingconsult.com/issues/01-03/ALC1-3_AMDAPain.pdf
Cancer Pain Treatment
• Carlson CL. Effectiveness of the World Health Organization cancer pain reliefguidelines: an integrative review. Journal of Pain Research.2016;9:515–34.
• Currow DC, Stevenson JP, Abernethy AP, et al. Prescribing in palliative care asdeath approaches. J Am Geriatr Soc.2007;55:590–5.
• Vargas-Schaffer G. Is the WHO analgesic ladder still valid? Can Fam Physician2010;56:514-7.
• Proposed new adaptation of WHO analgesicladder
Part 2.5.4: Psychotropics
Psychotropics and Dementia Overview• Assess patient for potentially modifiable contributors tosymptoms• Non-pharmacologic interventions arepreferred• Non-emergent antipsychotics should only be used for treatment of agitation in patients with
dementia when symptoms are severe, dangerous, and/or cause significant distress to patient• Discuss potential benefits and risks with patient, surrogate decision maker, and/or familyas appropriate
• When starting antipsychotic, use lowest effective dose astolerated• If patient experiences clinically significant side effect, review potential risks vs. benefits to determine if tapering and
discontinuing is indicated• If no clinically significant response after a 4-week trial of an adequate dose of antipsychotic, taper and discontinue• If adequate response, attempt to taper and discontinue should be made within 4 months unless patient experienced
recurrence of symptoms with prior attempts at tapering
• Do not use haloperidol as first-line agent in absence of delirium• Do not use long-acting injectable antipsychotic in absence ofchronic psychotic disorder
Psychotropics Resources• The American Psychiatric Association Practice Guideline on the Use of Antipsychotics to Treat Agitation or
Psychosis in Patients with DementiaCitation: Reus VI, Fochtmann LJ, Eyler AE, et al. Am J Psychiatry. 2016 May 1;173(5):543-6. Link: http://psychiatryonline.org/doi/pdf/10.1176/appi.books.9780890426807
• IA- ADAPT– Improving Antipsychotic Appropriateness in Dementia Patients: Training videos and pocket guides ontopics including antipsychotic prescribing guide, antipsychotic monitoring, delirium assessment and management,drugs that causedelirium, and algorithms for behavioral and psychological symptoms of dementia(BPSD).
Link: https://igec.uiowa.edu/ia-adapt
• Colorado Health Care Association and Center for Assisted Living: Guidelines for Reducing the Use ofAntipsychotic Medications in Nursing Homes, monitoring parameters for patients currently receivingpsychotropic medications, tips for a successful gradual dose reduction (GDR), and resources for compliance withCMS, and non-pharmacologic management of common behavioral disturbances in the elderly.
Link: https://www.cohca.org/wp-content/uploads/sites/170/2016/02/Guidelines-for-Reducing-the-Use-of-Antipsychotic-Medications-publication.pdf
Dementia: Cognitive Assessment Tools• Mini-Mental StatusExamination
• Citation: Folstein, M., Folstein, S.E., McHugh, P.R. (1975). “Mini-Mental State” aPractical Method for Grading the Cognitive State of Patients for the Clinician. Journal ofPsychiatric Research, 12(3); 189-198.
• Montreal Cognitive Assessment (MoCA)Test Link: http://www.mocatest.org/
• Alzheimer’s Association Cognitive AssessmentToolkit
Link: https://www.alz.org/media/Documents/cognitive-assessment-toolkit.pdf
Part 2.5.5: Antimicrobials
Antibiotic Stewardship Program(ASP)• ASP includes preauthorization and/or prospective review andfeedback
o Do not rely solely on didactic educationalmaterialso Target patients with specific infectiousdiseases
• Reduce the use of antibiotics associated with a high risk of c. difficile infection• Do not use antibiotic cycling• Use strategies that encourage prescribers to routinely review antibioticregimens
o Incorporate computerized clinical decision supporto Develop stratified antibiogramso Timely transition patients from IV to oralantibioticso Reduce antibiotic therapy to shortest effectiveduration
• In SNF, implement ASP to decrease unnecessary use ofantibiotics• Implement pharmacokinetic monitoring and adjustment programs for vancomycin• Use alternative dosing strategies for broad-spectrum beta-lactams• Monitor antibiotic use by days of therapy
o Measure cost based on prescriptions and administration (not purchasing data)• Provide clinical decision support for antibiotic use in terminally ill patients• Address fever and neutropenia management in hematology-oncology patients• Address prescribing of antifungals in immunocompromisedpatients
ASCP Antibiotic StewardshipResources
• Antibiotic Stewardship in Long-Term and Post-Acute Care Toolkit for facilitatingprograms in LTPACfacilities
• Provides guidance to initiate and sustainprogram• Incorporating into facility Quality Assurance Improvement Program(QAPI)• Ensures compliance with infection prevention regulations in CMS Requirementsof
Participation for Long-TermCare
Link: http://www.ascp.com/amstoolkit

Antibiotic Stewardship Resources
• Implementing an Antibiotic Stewardship Program: Guidelines by theInfectious Disease Society of America and the Society for HealthcareEpidemiology of America. Clin Infect Dis. 2016 May 15;62(10) :1197-202
Link to article: http://cid.oxfordjournals.org/content/62/10/1197.long
• PracticalAdvice
Antibiotic Stewardship Resources
• Algorithms promoting Antibiotic Stewardship in Long Term Caresetting
Link to article: https://www.jamda.com/article/S1525-8610(15)00728-8/abstract • CDC Core Elements for Antibiotic Stewardship in Long
TermCare
Link: http://www.cdc.gov/longtermcare/prevention/antibiotic-stewardship.html• Action Steps and Strategies to implementing antibiotic stewardship program inlong term
care Link: https://www.health.state.mn.us/diseases/antibioticresistance/hcp/index.html
Assessing Antibiotic Therapy• Global RPh Infectious Disease Empiric
Therapy Link:http:/ /www.globalrph.com/antibiotic.htm
• Global RPh Pathogenic BacteriaResourceLink: http://www.globalrph.com/bacterial-strains-anaerobic.htm
• Global RPh Aminoglycoside/Vancomycin Dosing by levelscalculator Link:
http://www.globalrph.com/dosebylevels.htm
Part 2.5.6: Narrow Therapeutic Index
Medications
Narrow Therapeutic Index (NTI) Medications
• General information about therapeutic drugmonitoring
Link: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2687654/
• Pharmacist letter lab monitoring chartCitation: Pl Detail-Document, Lab Monitoring for Common Medications. Pharmacist’s Letter/ Prescriber’s Letter. June 2014. (requires login)
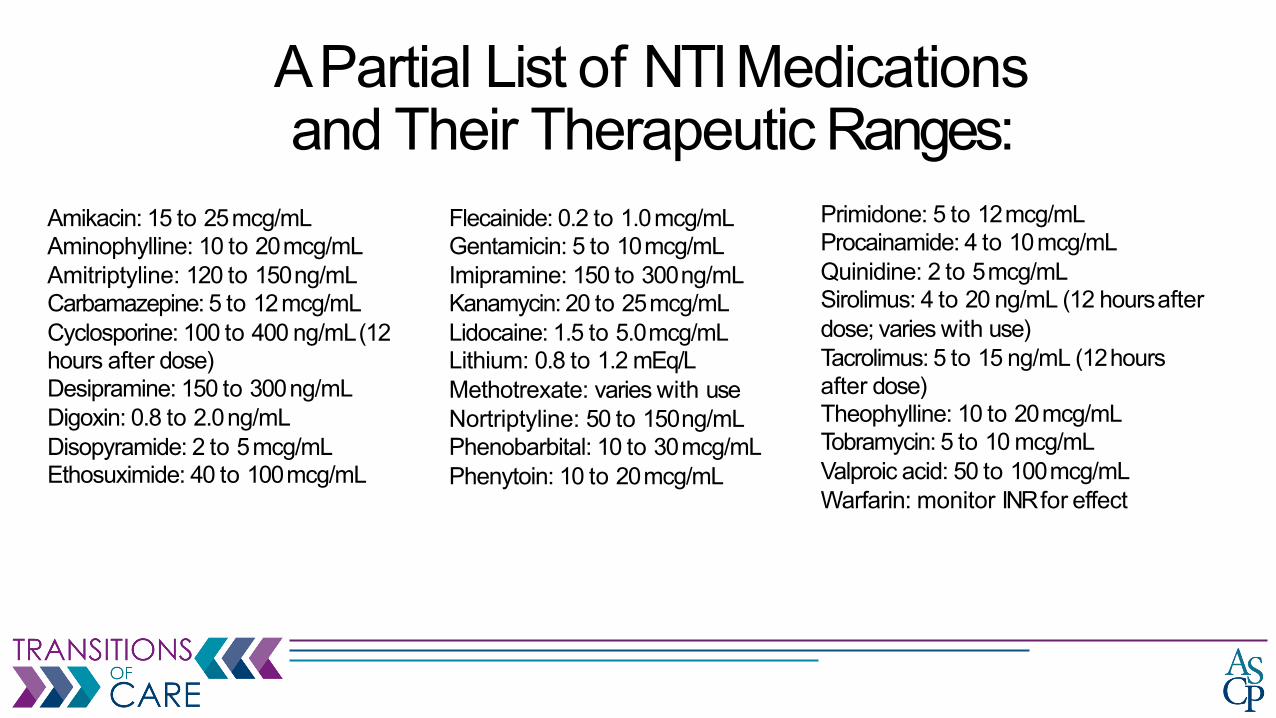
A Partial List of NTI Medications and Their Therapeutic Ranges:
Amikacin: 15 to 25mcg/mLAminophylline: 10 to 20mcg/mLAmitriptyline: 120 to 150ng/mLCarbamazepine: 5 to 12mcg/mLCyclosporine: 100 to 400 ng/mL(12 hours after dose)Desipramine: 150 to 300ng/mLDigoxin: 0.8 to 2.0ng/mLDisopyramide: 2 to 5mcg/mLEthosuximide: 40 to 100mcg/mL
Flecainide: 0.2 to 1.0mcg/mLGentamicin: 5 to 10mcg/mLImipramine: 150 to 300ng/mLKanamycin: 20 to 25mcg/mLLidocaine: 1.5 to 5.0mcg/mLLithium: 0.8 to 1.2 mEq/L Methotrexate: varies with use Nortriptyline: 50 to 150ng/mLPhenobarbital: 10 to 30mcg/mLPhenytoin: 10 to 20mcg/mL
Primidone: 5 to 12mcg/mLProcainamide: 4 to 10mcg/mLQuinidine: 2 to 5mcg/mLSirolimus: 4 to 20 ng/mL (12 hoursafter dose; varies with use)Tacrolimus: 5 to 15 ng/mL (12hours after dose)Theophylline: 10 to 20mcg/mLTobramycin: 5 to 10 mcg/mL Valproic acid: 50 to 100mcg/mL Warfarin: monitor INR for effect
Part 2.5.7: Anticholinergic/Sedation/Fall
RiskMedications
Anticholinergics• Anticholinergic medication list forpatients
• Pocket reference card in lay language, including common questions patients may haveLink: ƘǘǘLJǎΥκκƘŜNJŎŜΦLJdzōƭƛŎπƘŜŀƭǘƘΦdzƛƻǿŀΦŜŘdzκŜŘdzŎŀǘƛƻƴκ!ƴǘƛŎƘƻƭƛƴŜNJƎƛŎ/ŀNJŘΦLJŘŦ
• Anticholinergic cognitive burden scale• Developed by the Aging Brain Program of the Indiana University Center forAging
Research Link: https://americandeliriumsociety.org/files/ACB_Handout_Version_03-09-10.pdf • Journal of the American Medical Association article: The Anticholinergic Risk Scale and
Anticholinergic Adverse Effects in Older Persons: Linkhttps://jamanetwork.com/journals/jamainternalmedicine/fullarticle/414049
Tools to AssessSedation• Drug Burden Index
• Citation: Kouladjian L, Gnjidic D, Chen TF, et al. Drug Burden Index in orderadults:theoretical and practical issues. Clin Interv Aging.2014;9:1503-15.
• Link: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4166346/pdf/cia-9-1503.pdf• Citation: Dispennette R, Elliott D, Nguyen L, et al. Drug Burden Index score and
anticholinergic risk scale as predictors of readmission to the hospital. ConsultPharm.2014;29:158-68.
• Citation: Hilmer SN, Gnjidic D, Abernethy DR. Drug Burden Index for internationalassessment of the functional burden of medications in older people. JAm Geriatr Soc.2014 Apr; 62(4):791-2.
Tools for Fall Risk Assessment• Timed Up and Go Test (TUG) Assessment Tool
Link:https://www.cdc.gov/steadi/pdf/TUG_Test-print.pdf -and -Go-TUG.pdf
• Tinetti Balance AssessmentToolCitation: Tinetti ME, Williams TF, Mayewski R, Fall Risk Index for elderly patients based on number of chronic disabilities. Am J Med1986:80:429-434
• Gait score-12, balance score-16, combined score <18-high risk, 19-23-mod risk,>/=24-low risk
• Berg Balance ScaleLink: https://geriatrictoolkit.missouri.edu/Berg-Balance-Scale.doc
Part 2.5.8: Pharmacogenomics
Pharmacogenomics• Research on how specific genes for proteins affect individuals’ response to medications
• May impact medication safety and/oreffectiveness
• Genetic testing is a one-time test• Once genotype is known, prescribing can be adjusted to maximize therapeuticbenefit
• National Institutes of Health (NIH) pharmacogenomic dosingguidelines• Collation of dosing guidelines based ongenotype
Link: https://www.pharmgkb.org/view/dosing-guidelines.do
• Frequently askedquestions:Link: https://www.nigms.nih.gov/education/Pages/factsheet-pharmacogenomics.aspx