sease Journal of · 0 1 007 9 1218,8406 Research Article Open Access - 102 091 ¢...
3
Volume 1 • Issue 2 • 1000108 J Cardiovasc Dis Diagn ISSN: 2329-9517 JCDD, an open access journal Research Article Open Access Hong et al., J Cardiovasc Dis Diagn 2013, 1:2 DOI: 10.4172/2329-9517.1000108 Case Report Open Access Introduction Parachute Mitral Valve (PMV) is a rare congenital cardiac defect characterized by focalized attachment of the chordae tendinae of both leaflets to a single papillary muscle [1]. It may occur as an isolated lesion or part of a Shone’s anomaly in infants and young children [2]. Not much is known about PMV in adults [3]. ere have been reports of complete Atrioventricular Septal Defects (AVSD) associated with PMV in children, but a partial or transitional-type AVSD [4]. A combination of 2- (2D) and 3-dimensional (3D) transesophageal echocardiography (TEE) is essential to guide these complex surgical procedures in children and, more rarely, in adults [5]. Case Description A 55-year-old white male with new onset of atrial fibrillation, leſt hemiparesis, and a subsequent myocardial infarction presented for elective AVSD repair and coronary artery bypass graſt. His medical history was also significant for peripheral neuropathy, Charcot-Marie- Tooth disease, diabetes mellitus, and hyperlipidemia. Transthoracic Echocardiography (TTE) revealed what appeared to be an AVSD with a large ostium primum Type Atrial Septal Defect (ASD) component and a restrictive Ventricular Septal Defect (VSD). e shunt across the ASD was predominantly leſt to right with a leſt mitral valve cleſt and preserved ventricular systolic function. Cardiac catheterization demonstrated coronary artery disease. Aſter an uneventful anesthesia induction, the patient was placed on Cardiopulmonary Bypass (CPB) under mild hypothermic conditions. Intraoperative TEE confirmed the preoperative diagnosis of AVSD. 3D TEE further revealed the leaflets to be very primitive and thickened with no evidence of VSD (Figure 1). e right and leſt Atrioventricular Valves (AVV) were on the same plane, confirming the AVSD anatomy, and the direction of the right AVV regurgitation was toward and through the large primum ASD. e anterior mitral leaflet was larger and the cleſt was oriented so that it pointed toward the septum and right ventricle (Figure 2). ere was a mild mitral regurgitation through the cleſt. e aortic valve was wedged between the leſt and right AVV. ere was no evidence of leſt heart outflow obstruction. Further examination revealed a single papillary muscle with all the primary chordae originating from and supplying the leſt AVV structure (Figure 3). e chordae tendinae were short and thick. ey were oriented in a posterior-to-anterior direction and converged on a centrally placed, single papillary muscle. e surgeon’s direct visual inspection confirmed these findings. e surgical team decided against closing the cleſt as planned based on concerns that this could result in mitral stenosis in the future. e primum ASD was closed with a piece of bovine pericardial patch. Once the coronary bypass graſting was completed, the patient was successfully separated from CPB with milrinone and epinephrine infusions. TEE performed aſter CPB revealed complete closure of the ASD. ere was trace leſt AVV and mild right AVV regurgitation. Aſter an uneventful clinical course, the patient was discharged to a rehabilitation center five days aſter surgery. Discussion Pre- and intraoperative anatomical and structural delineation of the mitral valves and subvalvular apparatus are paramount to achieving successful and durable repair. Intraoperative TEE has a significant impact on both the surgical care and anesthetic management of the patient [6]. ere are several 2D but few 3D echocardiographic reports *Corresponding author: Associate Professor, Cardiothoracic and Intensive Care Division, Department of Anesthesiology and Perioperative Medicine, Georgia Regents University, 1120 Fifteenth Street, Augusta, Georgia 30912-2700, USA; Tel: 706-721-9895; E-mail: [email protected] Received April 06, 2013; Accepted April 27, 2013; Published May 06, 2013 Citation: Hong T (2013) Intraoperative 2- and 3-Dimensional Transesophageal Echocardiographic Guidance for Cardiovascular Surgery in a Patient with a Single Papillary Muscle “Parachute Valve”. J Cardiovasc Dis Diagn 1: 108. doi:10.4172/2329-9517.1000108 Copyright: © 2013 Hong T. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Intraoperative 2- and 3-Dimensional Transesophageal Echocardiographic Guidance for Cardiovascular Surgery in a Patient with a Single Papillary Muscle “Parachute Valve” Tao Hong 1 * Mohsen Karimi 2 , Vinayak Kamath 2 , Manuel Castresana 3 1 Associate Professor, Cardiothoracic and Intensive Care Division, Department of Anesthesiology and Perioperative Medicine, Georgia Regents University, USA 2 Department of Surgery, Georgia Regents University, USA 3 Department of Perioperative Medicine and Anesthesiology, Georgia Regents University, USA Inferior Superior 0 0 180 VR 12Hz Live 3D 3D 26% 3D 40dB Right LV LA Left 9cm 51 bpm Figure 1: Midesophageal 4-chamber view of 3D transesophageal echocardiography showing primitive and thickened atrioventricular valves. The mitral and tricuspid valves are on the same plane. Most of the atrial septal defect (ASD) and the superior aspect of the atrial septum (AS) are included in this 3D image. The mitral cleft is visible through the ASD. Right Atrium(RA); Right Ventricle (RV); Left Atrium (LA); Left Ventricle (LV); Mitral Valve (MV); Tricuspid Valve (TV). Journal of Cardiovascular Diseases & Diagnosis J o u r n a l o f C a r d i o v a s c u l a r D i s e a s e s & D i a g n o s i s ISSN: 2329-9517
Transcript of sease Journal of · 0 1 007 9 1218,8406 Research Article Open Access - 102 091 ¢...
-
Volume 1 • Issue 2 • 1000108J Cardiovasc Dis DiagnISSN: 2329-9517 JCDD, an open access journal
Research Article Open Access
Hong et al., J Cardiovasc Dis Diagn 2013, 1:2 DOI: 10.4172/2329-9517.1000108
Case Report Open Access
IntroductionParachute Mitral Valve (PMV) is a rare congenital cardiac defect
characterized by focalized attachment of the chordae tendinae of both leaflets to a single papillary muscle [1]. It may occur as an isolated lesion or part of a Shone’s anomaly in infants and young children [2]. Not much is known about PMV in adults [3]. There have been reports of complete Atrioventricular Septal Defects (AVSD) associated with PMV in children, but a partial or transitional-type AVSD [4]. A combination of 2- (2D) and 3-dimensional (3D) transesophageal echocardiography (TEE) is essential to guide these complex surgical procedures in children and, more rarely, in adults [5].
Case DescriptionA 55-year-old white male with new onset of atrial fibrillation, left
hemiparesis, and a subsequent myocardial infarction presented for elective AVSD repair and coronary artery bypass graft. His medical history was also significant for peripheral neuropathy, Charcot-Marie-Tooth disease, diabetes mellitus, and hyperlipidemia. Transthoracic Echocardiography (TTE) revealed what appeared to be an AVSD with a large ostium primum Type Atrial Septal Defect (ASD) component and a restrictive Ventricular Septal Defect (VSD). The shunt across the ASD was predominantly left to right with a left mitral valve cleft and preserved ventricular systolic function. Cardiac catheterization demonstrated coronary artery disease.
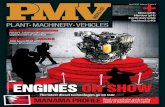
After an uneventful anesthesia induction, the patient was placed on Cardiopulmonary Bypass (CPB) under mild hypothermic conditions. Intraoperative TEE confirmed the preoperative diagnosis of AVSD. 3D TEE further revealed the leaflets to be very primitive and thickened with no evidence of VSD (Figure 1). The right and left Atrioventricular Valves (AVV) were on the same plane, confirming the AVSD anatomy, and the direction of the right AVV regurgitation was toward and through the large primum ASD. The anterior mitral leaflet was larger and the cleft was oriented so that it pointed toward the septum and right ventricle (Figure 2). There was a mild mitral regurgitation through the cleft. The aortic valve was wedged between the left and right AVV. There was no evidence of left heart outflow obstruction. Further examination revealed a single papillary muscle with all the primary chordae originating from and supplying the left AVV structure (Figure 3). The chordae tendinae were short and thick. They were oriented in a posterior-to-anterior direction and converged on a centrally placed, single papillary muscle. The surgeon’s direct visual inspection confirmed these findings. The surgical team decided against closing the cleft as planned based on concerns that this could result in mitral stenosis in the future.
The primum ASD was closed with a piece of bovine pericardial patch. Once the coronary bypass grafting was completed, the patient was successfully separated from CPB with milrinone and epinephrine
infusions. TEE performed after CPB revealed complete closure of the ASD. There was trace left AVV and mild right AVV regurgitation. After an uneventful clinical course, the patient was discharged to a rehabilitation center five days after surgery.
DiscussionPre- and intraoperative anatomical and structural delineation of
the mitral valves and subvalvular apparatus are paramount to achieving successful and durable repair. Intraoperative TEE has a significant impact on both the surgical care and anesthetic management of the patient [6]. There are several 2D but few 3D echocardiographic reports
*Corresponding author: Associate Professor, Cardiothoracic and Intensive CareDivision, Department of Anesthesiology and Perioperative Medicine, GeorgiaRegents University, 1120 Fifteenth Street, Augusta, Georgia 30912-2700, USA;Tel: 706-721-9895; E-mail: [email protected]
Received April 06, 2013; Accepted April 27, 2013; Published May 06, 2013
Citation: Hong T (2013) Intraoperative 2- and 3-Dimensional Transesophageal Echocardiographic Guidance for Cardiovascular Surgery in a Patient with a Single Papillary Muscle “Parachute Valve”. J Cardiovasc Dis Diagn 1: 108. doi:10.4172/2329-9517.1000108
Copyright: © 2013 Hong T. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Intraoperative 2- and 3-Dimensional Transesophageal Echocardiographic Guidance for Cardiovascular Surgery in a Patient with a Single Papillary Muscle “Parachute Valve”Tao Hong1* Mohsen Karimi2, Vinayak Kamath2, Manuel Castresana3
1Associate Professor, Cardiothoracic and Intensive Care Division, Department of Anesthesiology and Perioperative Medicine, Georgia Regents University, USA2Department of Surgery, Georgia Regents University, USA3Department of Perioperative Medicine and Anesthesiology, Georgia Regents University, USA
Inferior
Superior
0 0 180VR 12Hz
Live 3D3D 26%3D 40dB
Right
LV
LA
Left
9cm
51 bpm
Figure 1: Midesophageal 4-chamber view of 3D transesophageal echocardiography showing primitive and thickened atrioventricular valves. The mitral and tricuspid valves are on the same plane. Most of the atrial septal defect (ASD) and the superior aspect of the atrial septum (AS) are included in this 3D image. The mitral cleft is visible through the ASD. Right Atrium(RA); Right Ventricle (RV); Left Atrium (LA); Left Ventricle (LV); Mitral Valve (MV); Tricuspid Valve (TV).
Journal of Cardiovascular Diseases & DiagnosisJourn
al o
f Car
diovas
cular Diseases &Diagnosis
ISSN: 2329-9517
-
Citation: Hong T (2013) Intraoperative 2- and 3-Dimensional Transesophageal Echocardiographic Guidance for Cardiovascular Surgery in a Patient with a Single Papillary Muscle “Parachute Valve”. J Cardiovasc Dis Diagn 1: 108. doi:10.4172/2329-9517.1000108
Page 2 of 3
Volume 1 • Issue 2 • 1000108J Cardiovasc Dis DiagnISSN: 2329-9517 JCDD, an open access journal
of AVSD [7-8]. While 2D echocardiography provides clearer pictures, 3D TEE enables better visualization to determine the mechanism and site of AVV regurgitation. The combination of 2D and 3D real-time TEE has been shown to improve diagnostic accuracy from 40.4% to 65.4% [5]. In our case, the intraoperative TEE findings changed the surgical plan, potentially averting the adverse effects of mitral stenosis including heart failure, stroke, arrhythmia, and endocarditis.
PMV is caused by the defective delamination of the anterior and posterior parts of the trabecular ridge between the 5th and 19th weeks of gestion [9]. The underdeveloped chordae tendinae decrease mobility of the valve leaflets and reduce the mitral orifice. The narrowing of the interchordal spaces results in a smaller secondary mitral orifice, thus causing mitral inflow obstruction. The degree of stenosis is progressive and dependent on the tethering of the leaflets and reduction of the distal orifice. Most patients present during infancy with mitral stenosis of varying severity, or, less frequently, mitral regurgitation [10]. The
outcome is generally poor because of the multiple surgeries required to attain hemodynamic stability.
Adult PMV is an exceedingly uncommon condition. Only nine cases were identified in a nearly 50-year period (1960-2008) [3]. Of those nine, seven were male and five had isolated PMV. In contrast to PMV in the pediatric population, concomitant cardiac abnormalities are uncommon in adults.
Ours may be the first report of a transitional-type AVSD with an adult PMV and a cleft mitral valve. This is perhaps also one of the oldest patients with primum ASD to remain asymptomatic for so long. We speculate that the anomalous right AVV regurgitation through the primum ASD balanced the left-to-right shunt. Further, the cleft of the mitral valve provided additional space for the mitral orifice, thus preventing mitral stenosis in this adult PMV. Had we not discovered the single papillary muscle, the mitral valve cleft would have been closed as planned, eventually causing stenosis, because the only remaining blood flow from the left atrium to the left ventricle would been through the interchordal spaces.
This case demonstrates the importance of 2D and 3D TEE imaging in helping to select the proper surgical intervention of adult patients requiring complex congenital cardiac repairs.
Acknowledgement
Special thanks to Ms. Nadine Odo for her excellent work in the manuscript editing.
Right
rimum ASD
Left
Posterior
Anterior
0 10 180VR 3Hz
Live 3D3D 37%3D 40dB
6cm
56 bpm
Figure 2: 3D view of mitral valve cleft and wedge aortic valve. It is asurgeon’s view. Tricupid Valve (TV) can partially visible through the primum ASD. Right ventricular outflow (RVO) track is behind the aortic valve (AoV). Parts of Left atrial appendage (LAA) and left ventricle (LV) are visible.
FR 54Hz10cm
2D600%C50P OffGen
0 10 180
M4
JPEG
48 bpmPATT:37.OCTEET:37.BC
LA
P
G
R
Figure 3: Modified deep transgastric long-axis view demonstrating the relationship between the single papillary muscle (P) and mitral valve. The TEE probe was positioned between the deep transgastric and 4-chamber views.
Video 1:
Video 2:
-
Citation: Hong T (2013) Intraoperative 2- and 3-Dimensional Transesophageal Echocardiographic Guidance for Cardiovascular Surgery in a Patient with a Single Papillary Muscle “Parachute Valve”. J Cardiovasc Dis Diagn 1: 108. doi:10.4172/2329-9517.1000108
Page 3 of 3
Volume 1 • Issue 2 • 1000108J Cardiovasc Dis DiagnISSN: 2329-9517 JCDD, an open access journal
References
1. Madu EC, D’Cruz IA (1997) The vital role of papillary muscles in mitral andventricular function: echocardiographic insights. Clin Cardiol 20: 93-98.
2. Prunier F, Furber AP, Laporte J, Geslin P (2001) Discovery of a parachutemitral valve complex (Shone’s anomaly) in an adult. Echocardiography 18: 179-182.
3. Hakim FA, Kendall CB, Alharthi M, Mancina JC, Tajik JA, et al. (2010) Parachute mitral valve in adults-a systematic overview. Echocardiography 27: 581-586.
4. Sawazaki M, Tomari S, Izawa N, Tateishi N (2012) A single papillary musclewith chordal rupture in an adult. Interact Cardiovasc Thorac Surg 15: 920-921.
5. Willens HJ, Hendel RC, Qin JX, Ma C, Keith K, et al. (2011) Effect of performing real time three-dimensional transesophageal echocardiography in addition totwo-dimensional transesophageal echocardiography on operator diagnosticconfidence. Echocardiography 28: 235-242
6. Shanewise JS, Vezina DP, Cahalan MK (2005) Comprehensive and abbreviated
intraoperative TEE examination. In: RM Savage and S Aronson (eds), Comprehensive textbook of intraoperative transesophageal echocardiography. Philadelphia: Lippincott Williams and Wilkins 81-93.
7. Cheng HL, Huang CH, Tsai HE, Chen MY, Fan SZ, et al. (2012) Intraoperative assessment of partial atrioventricular septal defect with a cleft mitral valve byreal-time three-dimensional transesophageal echocardiography. Anesth Analg114: 731-734.
8. Mamaladze V, Capdeville M, Navia J, Vivacqua A (2011) Parachute-likeasymmetric mitral valve associated with mitral valve cleft and atrial septaldefect in an adult. J Cardiothorac Vasc Anesth 25: 1106-1108.
9. Oosthoek PW, Wenink AC, Wisse LJ, Gittenberger-de Groot AC (1998)Development of the papillary muscles of the mitral valve: morphogeneticbackground of parachute-like asymmetric mitral valves and other mitral valveanomalies. J Thorac Cardiovasc Surg 116: 36-46
10. Schaverien MV, Freedom RM, McCrindle BW (2004) Independent factorsassociated with outcomes of parachute mitral valve in 84 patients. Circulation109: 2309-2313.
http://www.ncbi.nlm.nih.gov/pubmed/9034636http://www.ncbi.nlm.nih.gov/pubmed/9034636http://www.ncbi.nlm.nih.gov/pubmed/11262544http://www.ncbi.nlm.nih.gov/pubmed/11262544http://www.ncbi.nlm.nih.gov/pubmed/11262544http://www.ncbi.nlm.nih.gov/pubmed/20608957http://www.ncbi.nlm.nih.gov/pubmed/20608957http://www.ncbi.nlm.nih.gov/pubmed/22859513http://www.ncbi.nlm.nih.gov/pubmed/22859513http://www.ncbi.nlm.nih.gov/pubmed/21276077http://www.ncbi.nlm.nih.gov/pubmed/21276077http://www.ncbi.nlm.nih.gov/pubmed/21276077http://www.ncbi.nlm.nih.gov/pubmed/21276077http://www.ncbi.nlm.nih.gov/pubmed/22344238http://www.ncbi.nlm.nih.gov/pubmed/22344238http://www.ncbi.nlm.nih.gov/pubmed/22344238http://www.ncbi.nlm.nih.gov/pubmed/22344238http://www.ncbi.nlm.nih.gov/pubmed/21093291http://www.ncbi.nlm.nih.gov/pubmed/21093291http://www.ncbi.nlm.nih.gov/pubmed/21093291http://www.ncbi.nlm.nih.gov/pubmed/9671895http://www.ncbi.nlm.nih.gov/pubmed/9671895http://www.ncbi.nlm.nih.gov/pubmed/9671895http://www.ncbi.nlm.nih.gov/pubmed/9671895http://www.ncbi.nlm.nih.gov/pubmed/15117833http://www.ncbi.nlm.nih.gov/pubmed/15117833http://www.ncbi.nlm.nih.gov/pubmed/15117833
TitleCorresponding authorIntroductionCase Description DiscussionAcknowledgementFigure 1Figure 2Figure 3Video 1Video 2References