
Sdd C di D thiSudden Cardiac Death in Children and ...
72
S dd C di D th i S dd C di D th i Sudden Cardiac Death in Sudden Cardiac Death in Children and Adolescents Children and Adolescents Children and Adolescents Children and Adolescents Kristopher C mbermack MD Kristopher Cumbermack, MD Assistant Professor, Pediatrics Contemporary Pediatrics Contemporary Pediatrics May 19, 2011 1
Transcript of Sdd C di D thiSudden Cardiac Death in Children and ...
S dd C di D th iS dd C di D th iSudden Cardiac Death in Sudden Cardiac Death in Children and AdolescentsChildren and AdolescentsChildren and AdolescentsChildren and Adolescents
Kristopher C mbermack MDKristopher Cumbermack, MDAssistant Professor, Pediatrics
Contemporary PediatricsContemporary PediatricsMay 19, 2011
1
Faculty DisclosureFaculty DisclosureFaculty DisclosureFaculty Disclosure• No disclosures or conflicts of interestNo disclosures or conflicts of interest
ObjectivesObjectivesObjectivesObjectives• Recognize the common causes, riskRecognize the common causes, risk
factors of sudden cardiac death in children
• Discuss the diagnostic tools available to identify potential risk factorsy p
• Review potential interventionsp
3
TopicsTopicsTopicsTopics• Sudden Cardiac DeathSudden Cardiac Death• Congenital Heart Disease
Arrhythmias• Arrhythmias• Cardiomyopathies• Prevention• Role of the Primary Care Physiciano e o e a y Ca e ys c a
4
Sudden Death (SD)Sudden Death (SD)Sudden Death (SD)Sudden Death (SD)• Unexpected death in previously healthy• TraumaticMost common cause of SD in children~ 72 million in 1991: 21,367 SD (~30/100,000)
• Non-traumaticNon-cardiacSudden Cardiac Death (SCD) in childrenEstimates of 500/yr (0.8-6.2/100,000/yr)
5Rivara et al, Pediatrics 1996
Sudden Cardiac DeathSudden Cardiac DeathSudden Cardiac DeathSudden Cardiac Death• Abrupt (typically < 1 hr from event to death)Abrupt (typically 1 hr from event to death)• Unexpected
Cardiovascular etiology• Cardiovascular etiology• Absence of other fatal conditions
• Variety of mechanisms; often arrhythmiaa e y o ec a s s; o e a y a
6Zipes et al Circulation 1998
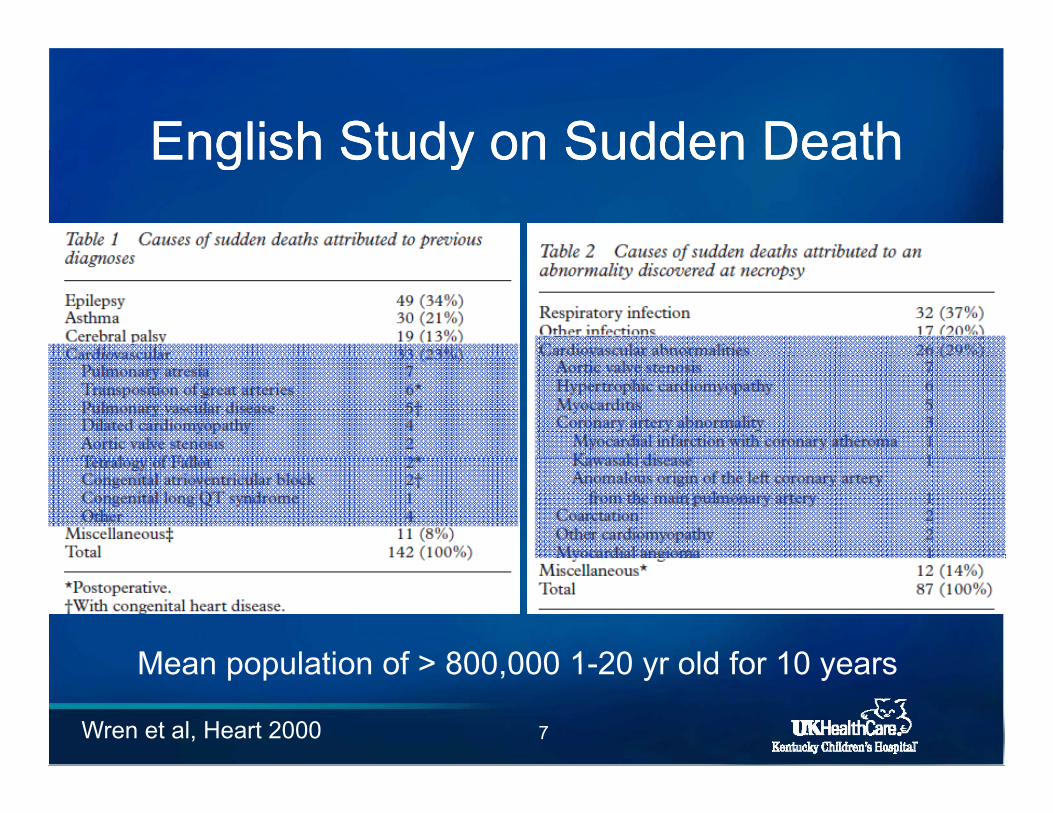
English Study on Sudden DeathEnglish Study on Sudden DeathEnglish Study on Sudden DeathEnglish Study on Sudden Death
Mean population of > 800 000 1 20 yr old for 10 years
7Wren et al, Heart 2000
Mean population of > 800,000 1-20 yr old for 10 years
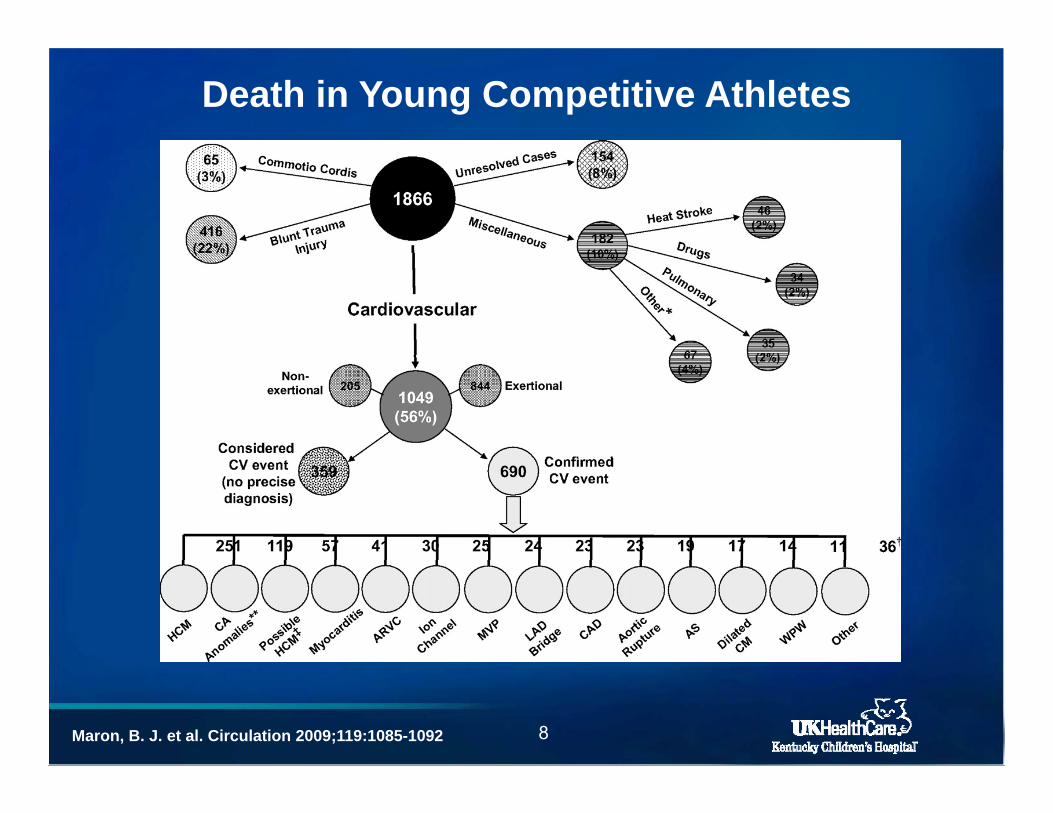
Death in Young Competitive Athletes
Maron, B. J. et al. Circulation 2009;119:1085-1092 8
TopicsTopicsTopicsTopics• Sudden Cardiac DeathSudden Cardiac Death• Congenital Heart Disease
Arrhythmias• Arrhythmias• Cardiomyopathies• Prevention• Role of the Primary Care Physiciano e o e a y Ca e ys c a
9
Congenital Heart DiseaseCongenital Heart DiseaseCongenital Heart DiseaseCongenital Heart Disease• Repaired CHDRepaired CHDTetralogy of FallotTransposition of the great arteriesTransposition of the great arteriesSingle ventricle s/p Fontan procedure
• Unrepaired CHDAortic stenosisAortic stenosisCoronary artery anomalies
10
Coronary Artery Origin Coronary Artery Origin AnomaliesAnomalies
• Left coronary artery from right aortic sinus• Right coronary artery from left aortic sinusg y y
• Incidence of 0 17 1 2%• Incidence of 0.17 – 1.2%
• 2nd most common cause of SCD in young athletes
11Davis et al, JACC 2001
Coronary Origin AnomaliesCoronary Origin AnomaliesCoronary Origin AnomaliesCoronary Origin Anomalies• Asymptomatic 70-80% y p
• Diagnostic testingNo physical exam findingsElectrocardiogram typically normalg yp yEchocardiographyEnsure reports comment on coronary originsEnsure reports comment on coronary origins
12Davis et al, JACC 2001
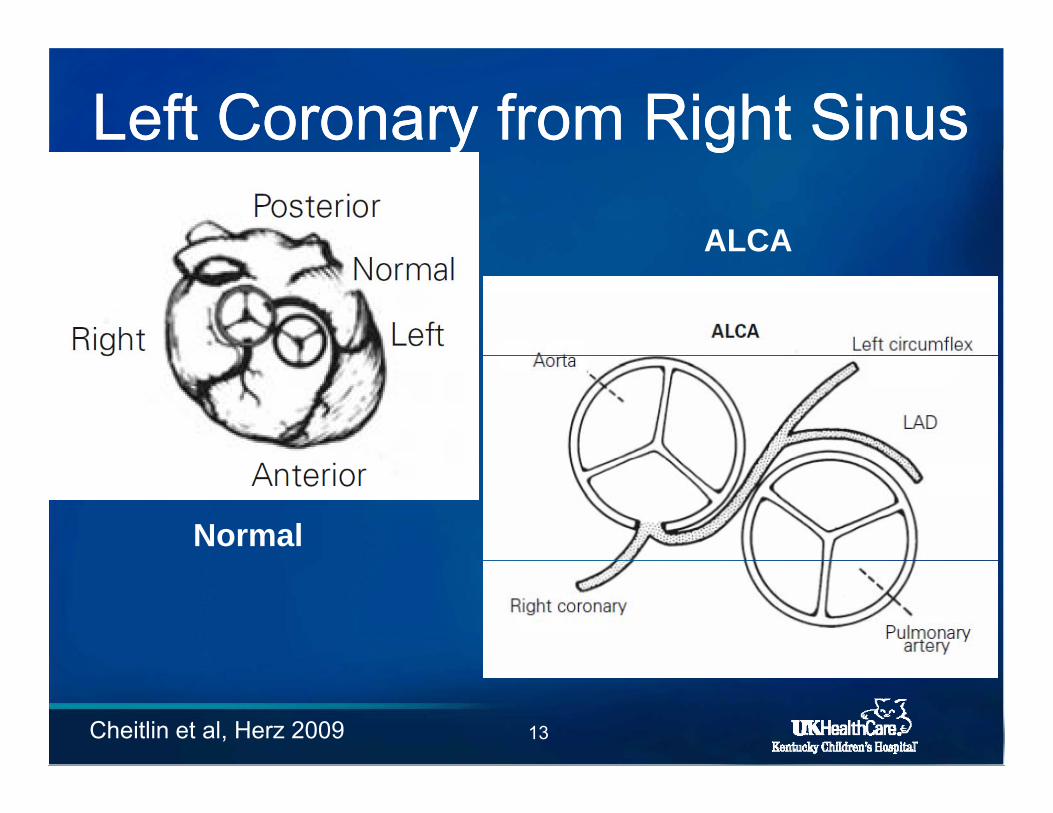
Left Coronary from Right SinusLeft Coronary from Right Sinusy gy gPosterior
ALCA
Anterior
Normal
Anterior
13Cheitlin et al, Herz 2009
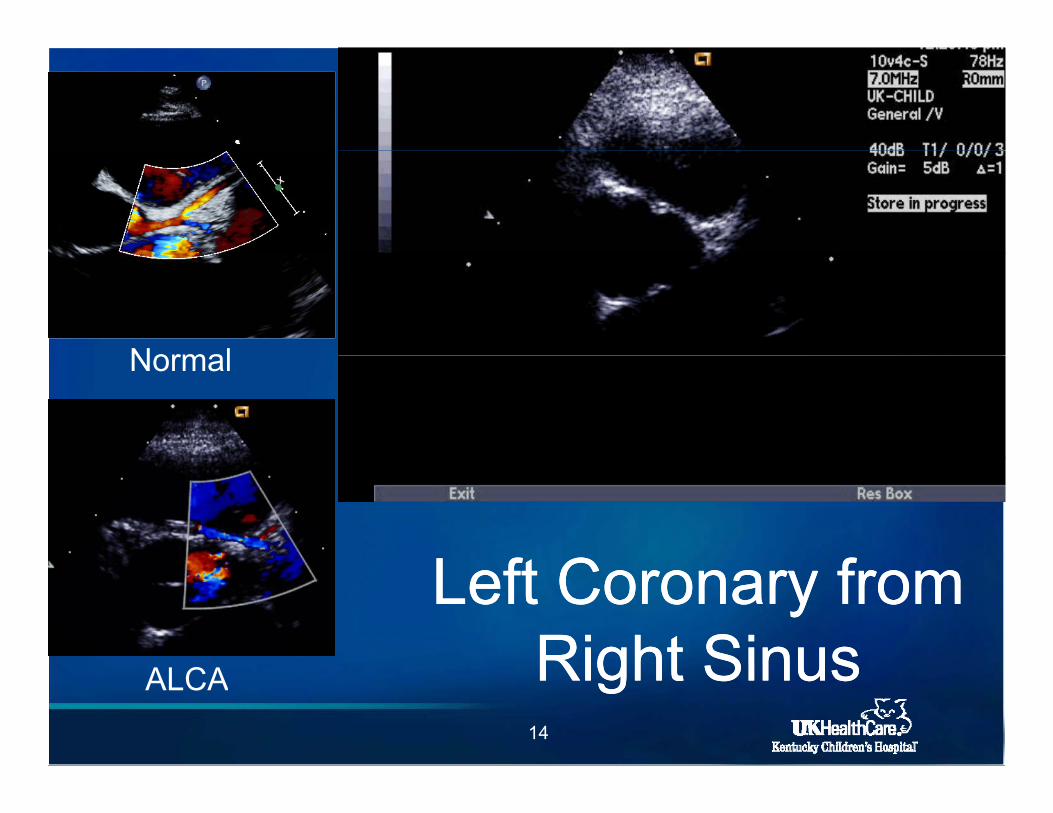
NormalNormal
L ft C fL ft C fLeft Coronary from Left Coronary from Right SinusRight Sinus
14
Right SinusRight SinusALCA
TreatmentTreatmentTreatmentTreatment
• Many recommend surgical interventionUnroofing procedureUnroofing procedure
C t d di t i l• Controversy depending on anatomical details due to limited data
15Frommelt et al, Pacing Clin EP, 2009
TopicsTopicsTopicsTopics• Sudden Cardiac Death OverviewSudden Cardiac Death Overview• Congenital Heart Disease
Arrhythmias• Arrhythmias• Cardiomyopathies• Prevention• Role of the Primary Care Physiciano e o e a y Ca e ys c a
16
Arrhythmias and SCDArrhythmias and SCDArrhythmias and SCDArrhythmias and SCD• Wolff-Parkinson-White SyndromeWolff Parkinson White Syndrome
• ChannelopathiespLong QT syndromeShort QT syndromeShort QT syndromeBrugada syndrome
• Catecholaminergic Polymorphic Ventricular Tachycardia (CPVT)Ventricular Tachycardia (CPVT)
17
WolffWolff--Parkinson White Parkinson White Syndrome (WPWS)Syndrome (WPWS)
• Prevalence of 0 07% in children• Prevalence of 0.07% in children
• Supraventricular tachycardia (SVT)• Supraventricular tachycardia (SVT)Re-entrant (80%)Atrial fibrillation (15 30%) atrial flutter (5%)Atrial fibrillation (15-30%), atrial flutter (5%)
• Symptoms of SVT• Symptoms of SVT PalpitationsSyncopeSyncope
18
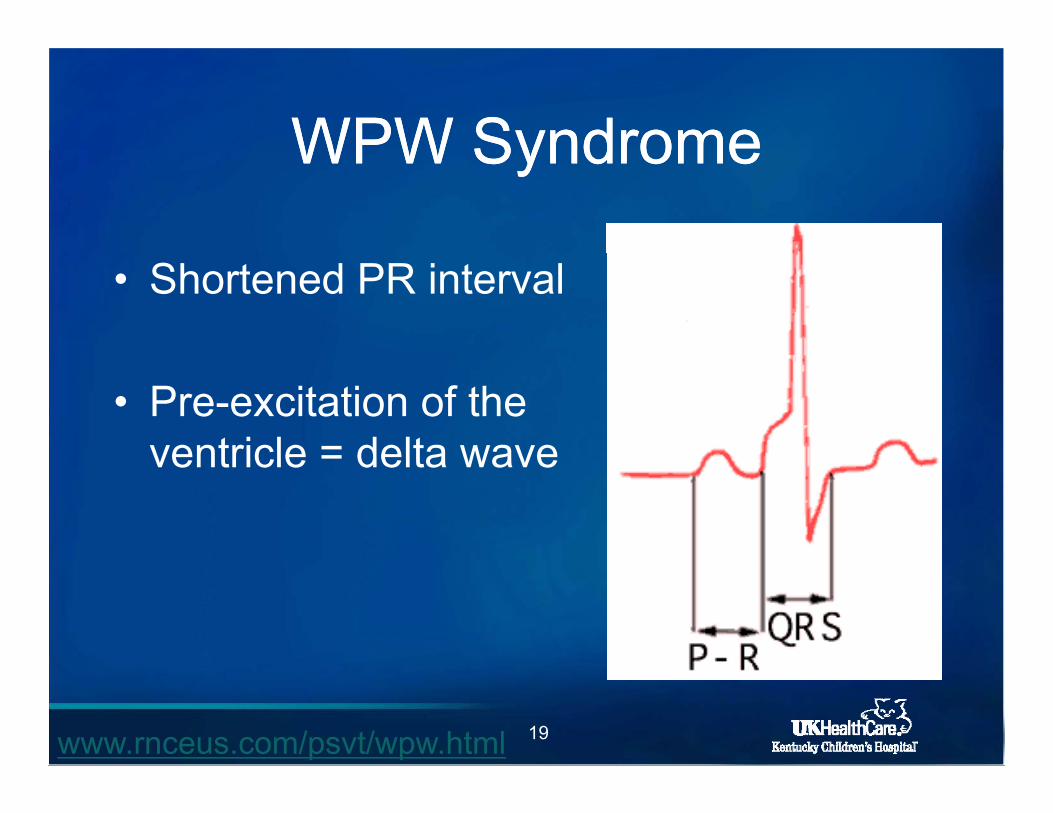
WPW SyndromeWPW SyndromeWPW SyndromeWPW Syndrome
• Shortened PR interval
• Pre-excitation of the ventricle = delta waveventricle = delta wave
19www.rnceus.com/psvt/wpw.html
WPW PatternWPW PatternWPW PatternWPW Pattern• ECG pattern of pre-excitation onlyECG pattern of pre excitation only
• Asymptomatic without SVTy p
• Higher incidence than true WPW syndromeg y
• Theoretical risk for SCD
• Evaluation, intervention not defined
20
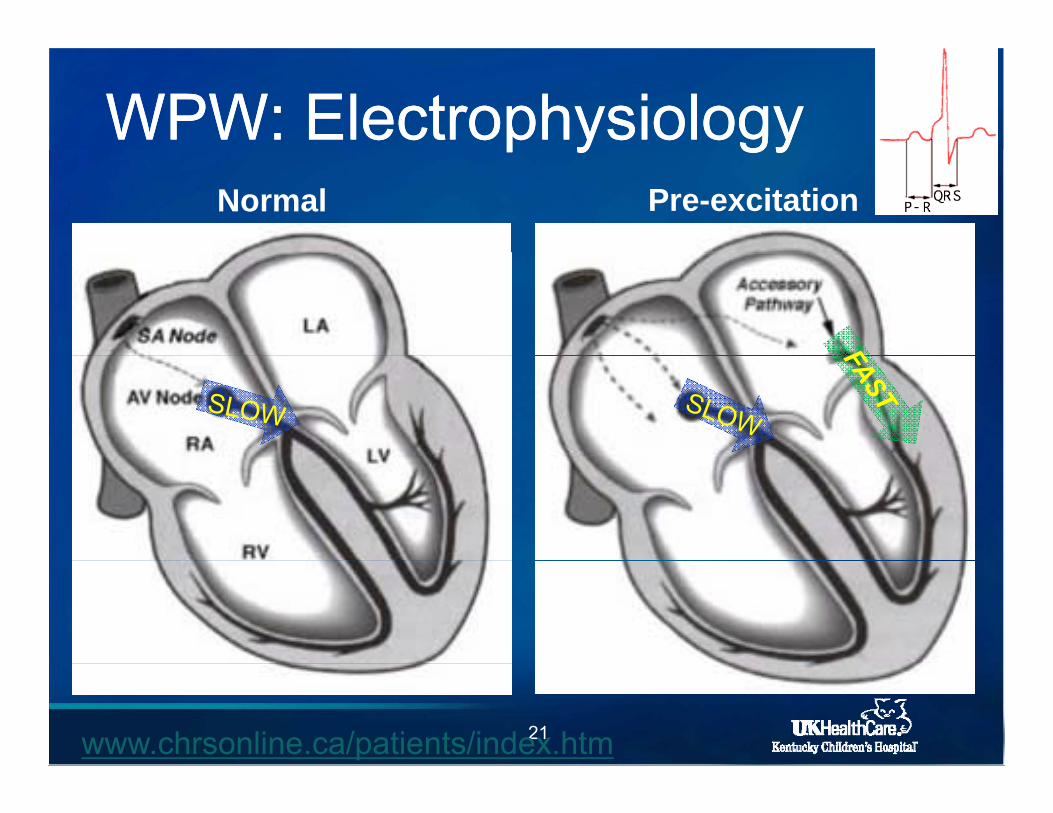
WPW: ElectrophysiologyWPW: Electrophysiologyp y gyp y gyNormal Pre-excitation
21www.chrsonline.ca/patients/index.htm
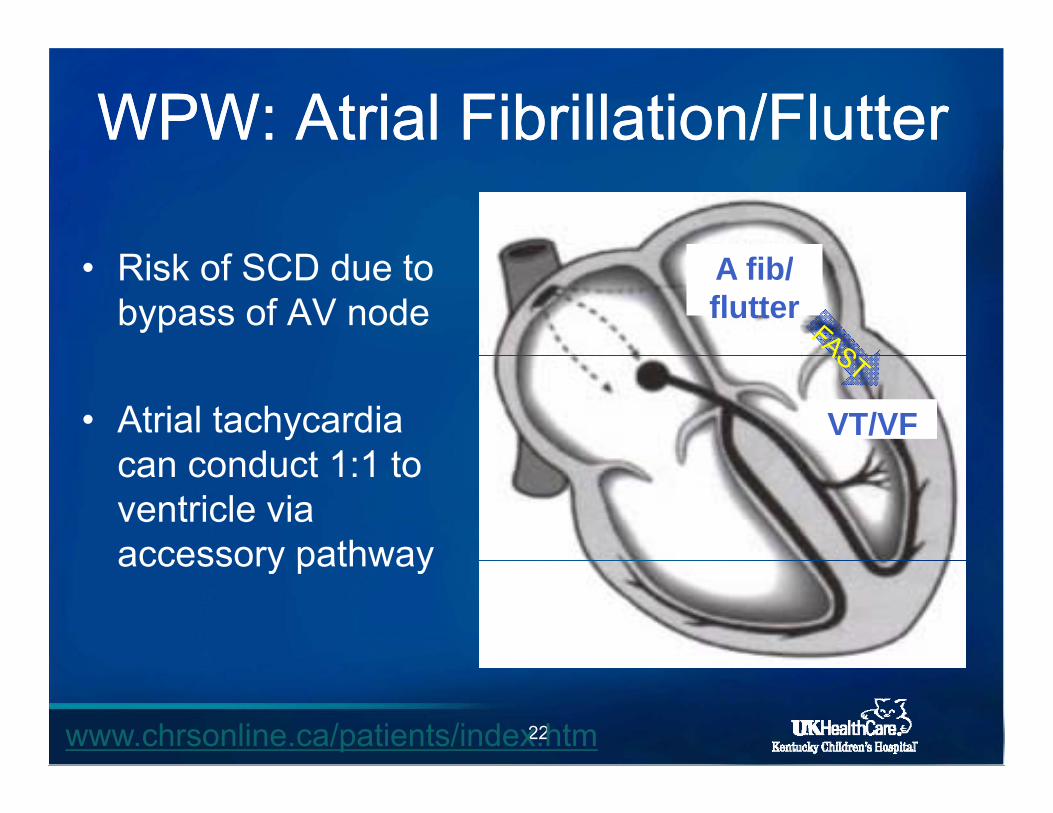
WPW: Atrial Fibrillation/FlutterWPW: Atrial Fibrillation/Flutter
• Risk of SCD due to bypass of AV node
A fib/flutter
• Atrial tachycardia can conduct 1:1 to
VT/VFcan conduct 1:1 to ventricle via accessory pathwayaccessory pathway
22www.chrsonline.ca/patients/index.htm
TreatmentTreatmentTreatmentTreatment• Digoxin is contraindicatedDigoxin is contraindicated
• Beta blocker
• Class IC (flecainide)
• Electrophysiology study (EPS)Risk stratificationAblation
23
Long QT Syndrome (LQTS)Long QT Syndrome (LQTS)Long QT Syndrome (LQTS)Long QT Syndrome (LQTS)• Prolongation of the QT intervalProlongation of the QT interval
• Genetic disorderMutations of ion channels affecting action
potentialpAutosomal dominantVariable expressionp
• Syncope, SCDy p ,
24
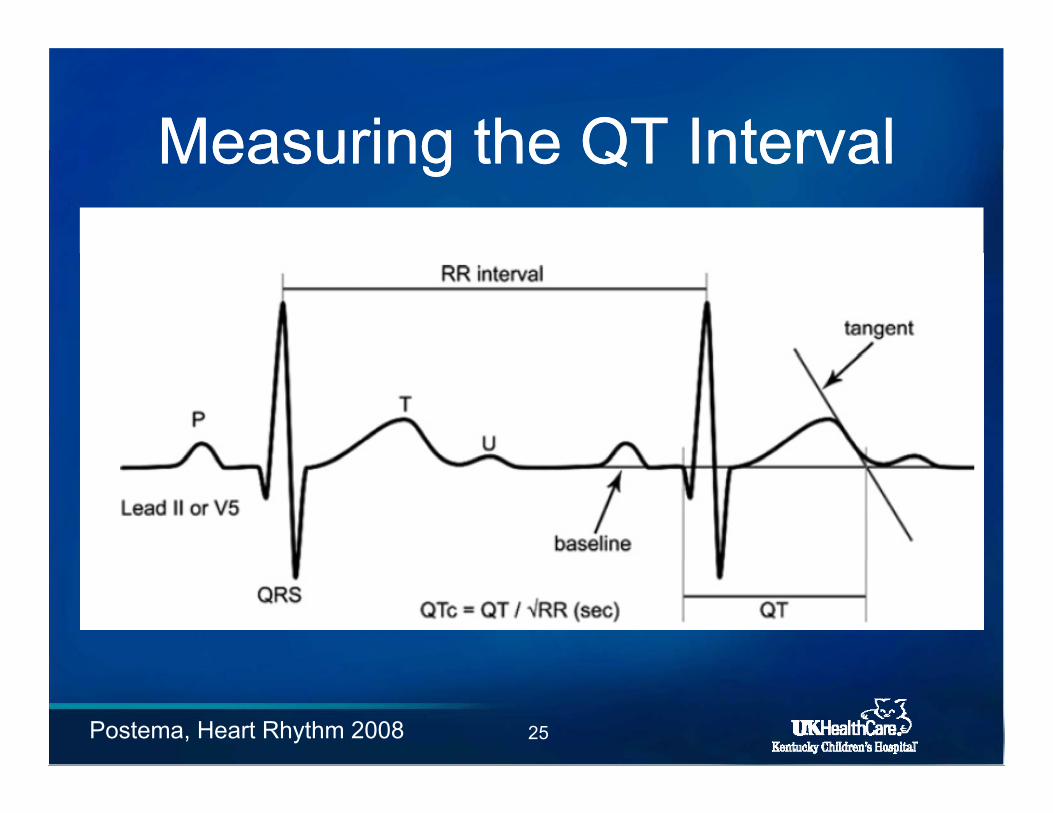
Measuring the QT IntervalMeasuring the QT IntervalMeasuring the QT IntervalMeasuring the QT Interval
25Postema, Heart Rhythm 2008
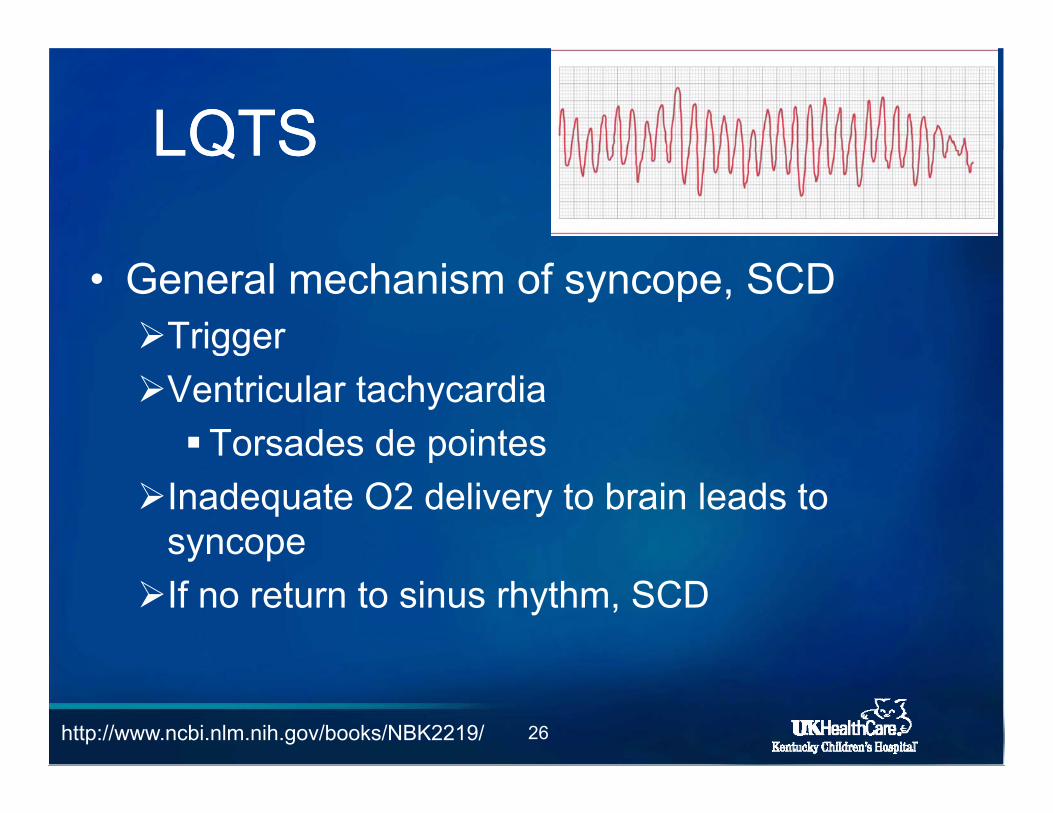
LQTSLQTSLQTSLQTS
• General mechanism of syncope, SCDTriggerggVentricular tachycardia Torsades de pointesp
Inadequate O2 delivery to brain leads to syncopey pIf no return to sinus rhythm, SCD
26http://www.ncbi.nlm.nih.gov/books/NBK2219/
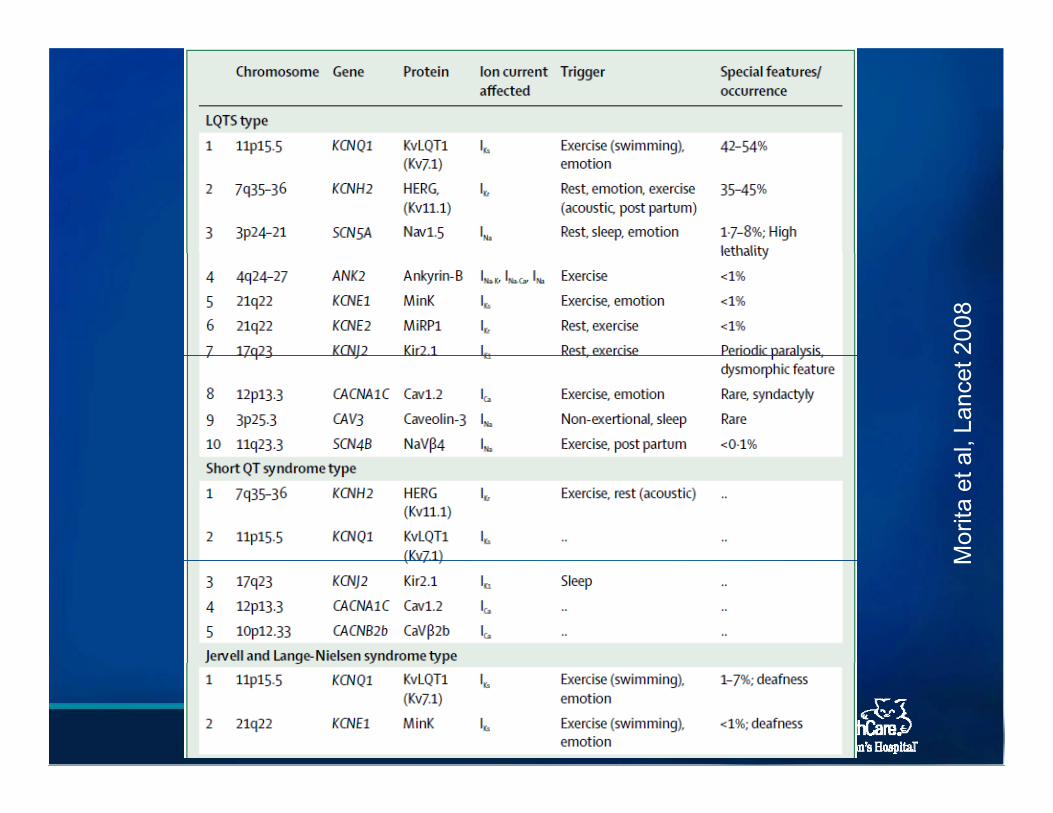
2008
al, L
ance
t M
orita
et a
M
27
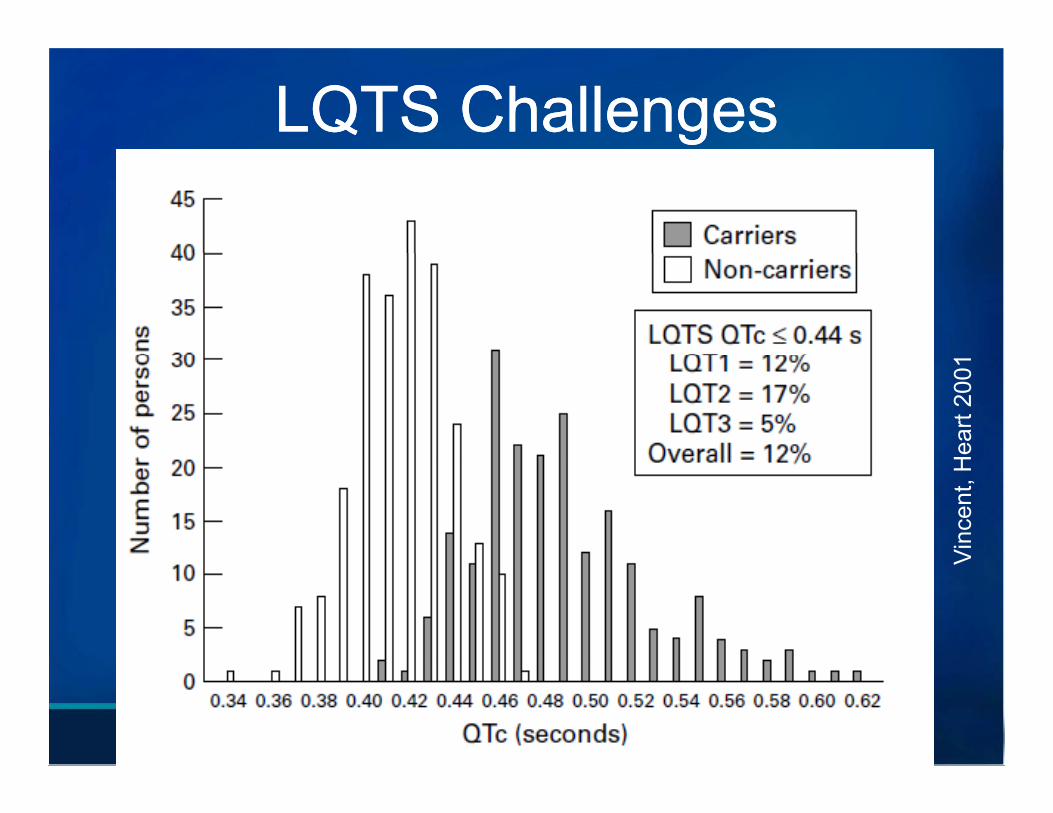
LQTS ChallengesLQTS Challenges
Hea
rt 20
01Vi
ncen
t, H
V
28
LQTS ChallengesLQTS ChallengesLQTS ChallengesLQTS Challenges• Overlap of QT interval in normal and LQTSOverlap of QT interval in normal and LQTS
populations
• Secondary QT prolongation can occur mimicking LQTS or expose true LQTSg p
• Variable phenotype for same genotypep yp g yp
• 1st symptom may be SCDy y
29
LQTS Treatment OptionsLQTS Treatment OptionsLQTS Treatment OptionsLQTS Treatment Options• Beta blockadeBeta blockadeMost effective in LQT1 with decreased
effectiveness in others
• Surgical denervation of the left cardiac gsympathetic nerve
• Automatic implantable cardioverter defibrillator (AICD)
30
Suspect LQTS?Suspect LQTS?Suspect LQTS?Suspect LQTS?• Assessment of family history risk factors• Assessment of family history, risk factors
• Restrict from exercise• Restrict from exercise
• Urgent referral to pediatric cardiologist• Urgent referral to pediatric cardiologist
• If QTc > 500 ms consider empiricIf QTc > 500 ms, consider empiric treatment with beta blocker
31
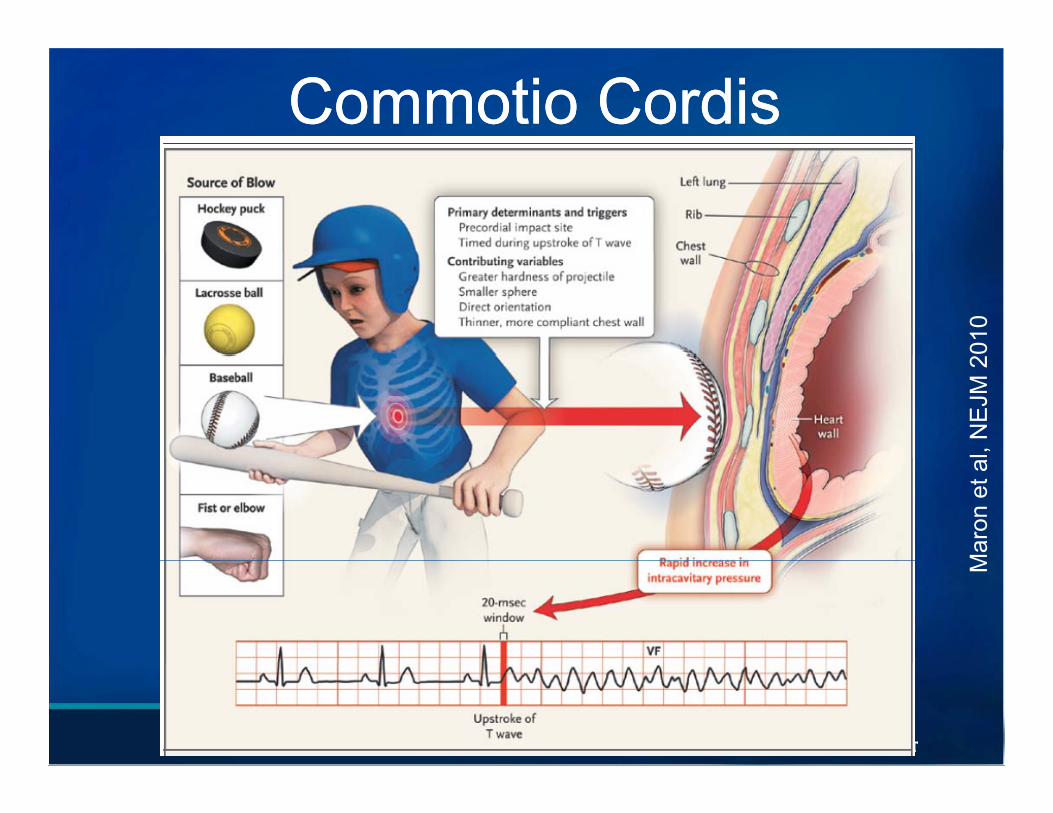
CommotioCommotio CordisCordis
010
l, N
EJM
2M
aron
et a
M
32
TopicsTopicsTopicsTopics• Sudden Cardiac DeathSudden Cardiac Death• Congenital Heart Disease
Arrhythmias• Arrhythmias• Cardiomyopathies• Prevention• Role of the Primary Care Physiciano e o e a y Ca e ys c a
33
CardiomyopathiesCardiomyopathiesCardiomyopathiesCardiomyopathies• Hypertrophic Cardiomyopathyyp p y p y• Dilated Cardiomyopathy• Restrictive Cardiomyopathy• Restrictive Cardiomyopathy• Myocarditis• Arrhythmogenic Right Ventricular
Cardiomyopathy/Dysplasia• Left ventricular non-compaction
34
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
• Most common cause of SCD in young athletes in US
• Autosomal dominantAutosomal dominantVariety of sarcomere genes (>20 identified)Variable phenotypic expressionVariable phenotypic expressionMay not develop until adulthood
35
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
• Prevalence of 1 in 500 adults
• 1-20 yr old incidence of death in undiagnosed HCMundiagnosed HCM1 in 1.35 million/0.74 per million person yrs
36Wren et al Heart 2000
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
• Thickened ventricular walls Absence of other causes of hypertrophyWithout ventricular dilationSymmetric or asymmetric
• Systolic function typically maintained• Abnormal diastolic function (relaxation)( )
HCM: Mechanism of SCDHCM: Mechanism of SCDHCM: Mechanism of SCDHCM: Mechanism of SCD• Left ventricular outflow tract obstructionLeft ventricular outflow tract obstruction
• Disarray of myocardial muscle fibersy y
• Promotes arrhythmogenesisy g
• VT/VF thought to play significant role even g p y gw/o left ventricular outflow tract obstruction
38
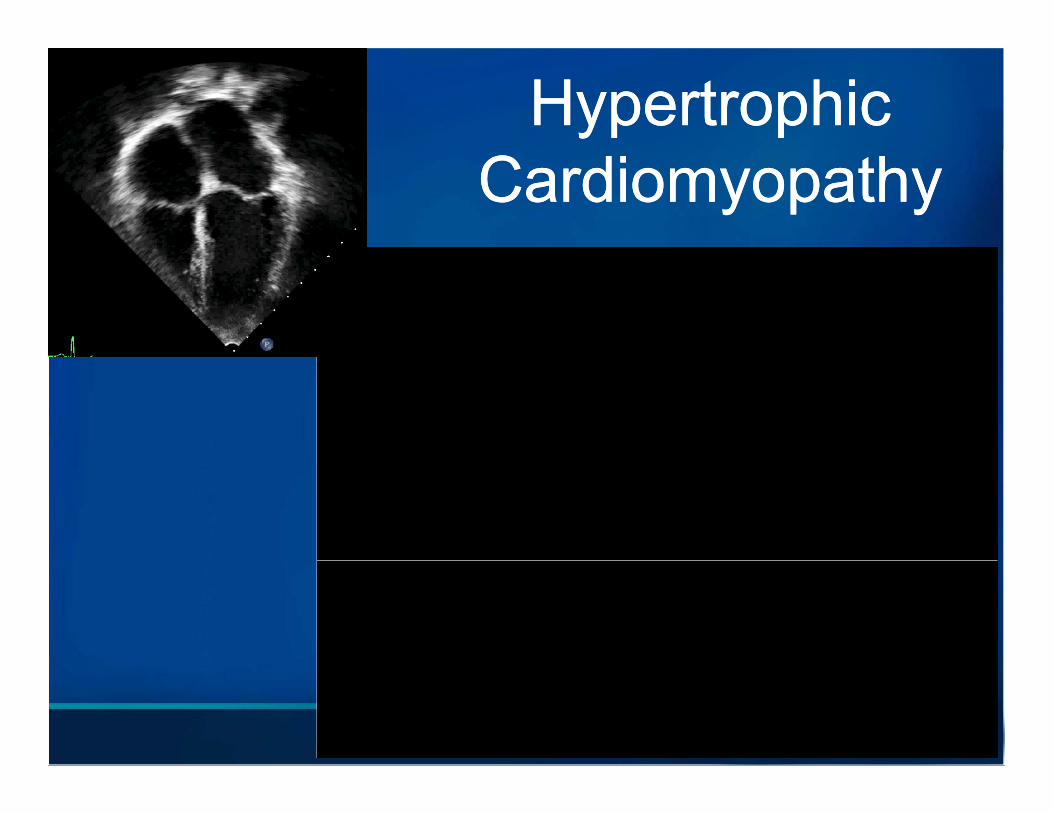
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
39
Athlete’s HeartAthlete’s HeartAthlete s HeartAthlete s Heart• Physiologic hypertrophyPhysiologic hypertrophy
• Exercise can cause cardiac remodelinggIncreased chamber sizeIncreased ventricular wall thicknessIncreased ventricular wall thickness
• Preserved systolic and diastolic functionese ed sys o c a d d as o c u c o
40
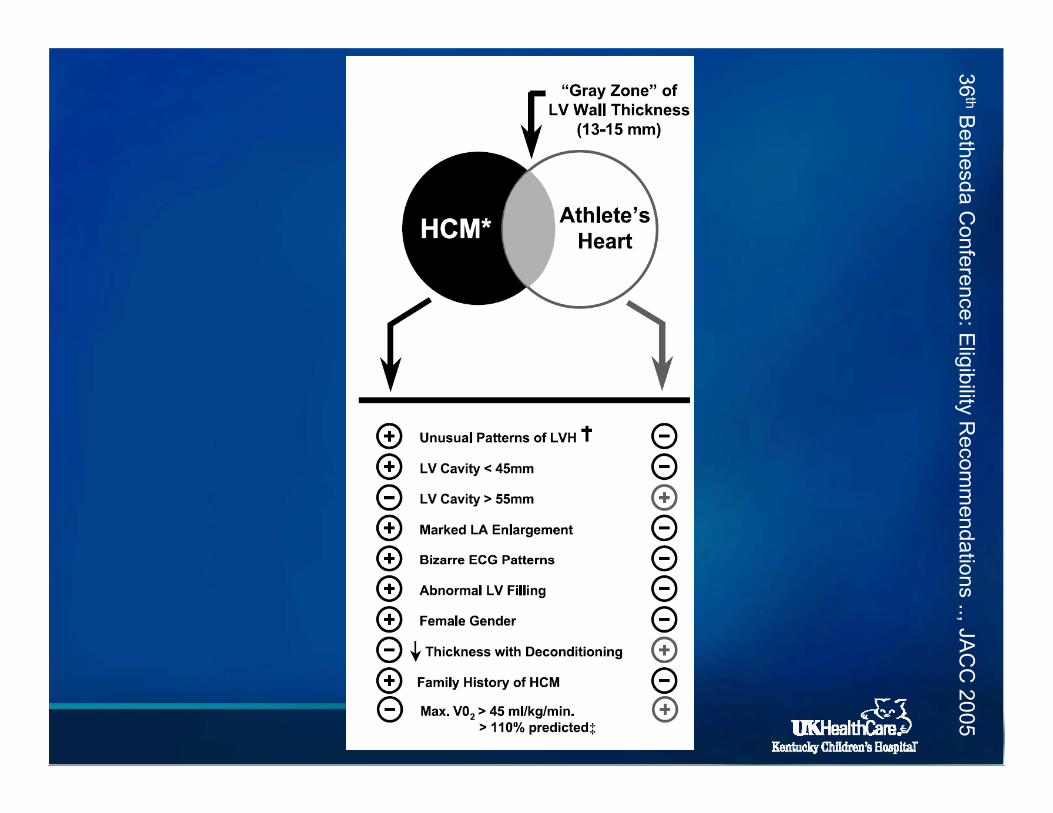
36thB
ethhesda Confference: E
ligibility Reccom
mendatiions .., JAC
41
CC
2005
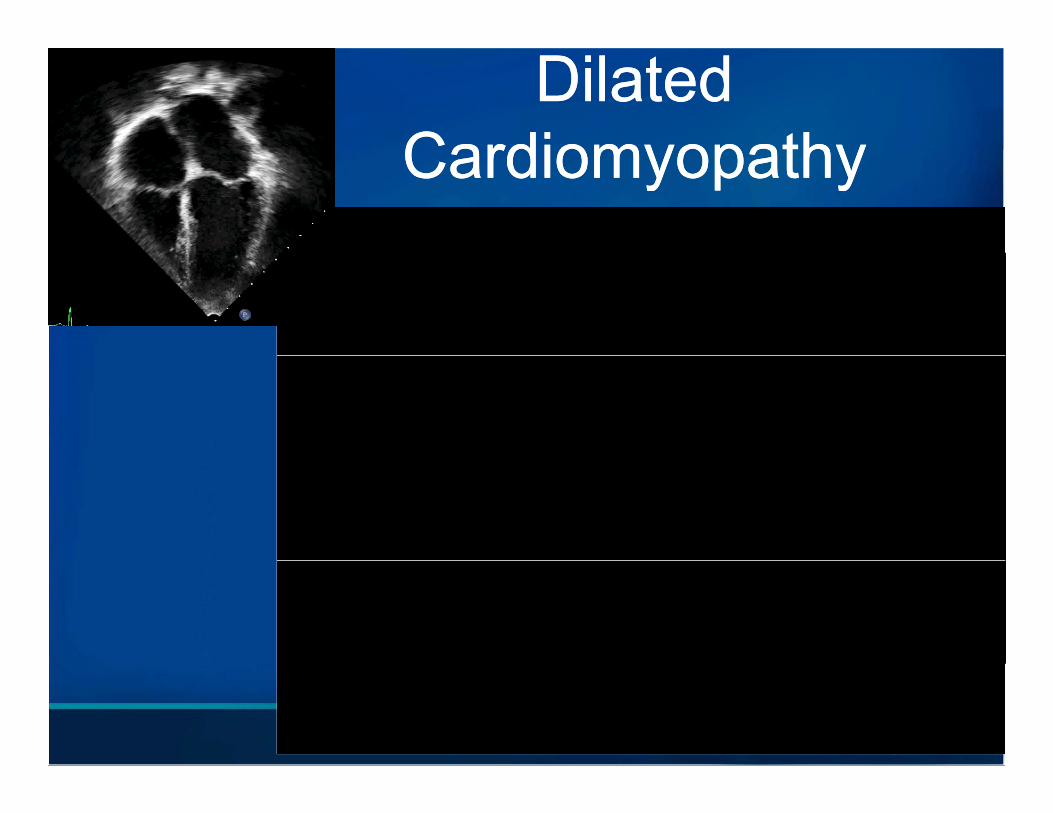
Dilated Dilated CardiomyopathyCardiomyopathyCardiomyopathyCardiomyopathy
42
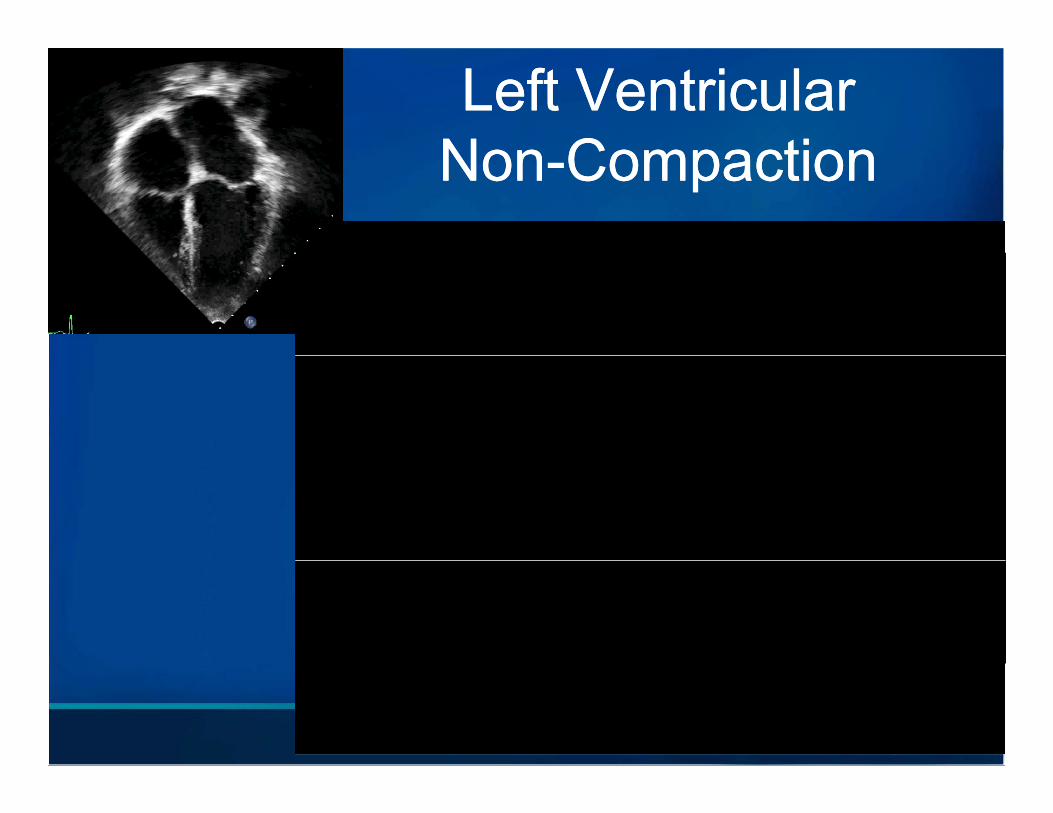
Left Ventricular Left Ventricular NonNon CompactionCompactionNonNon--CompactionCompaction
43
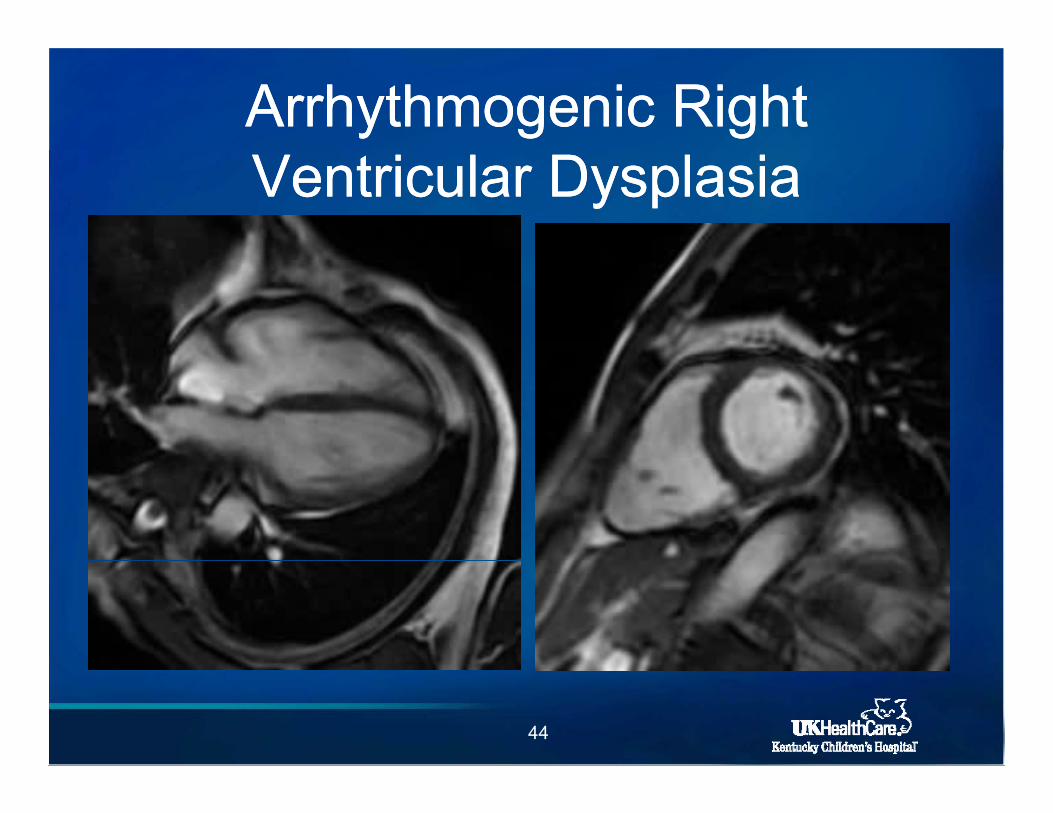
Arrhythmogenic Right Arrhythmogenic Right Ventricular DysplasiaVentricular Dysplasia
44
TopicsTopicsTopicsTopics• Sudden Cardiac DeathSudden Cardiac Death• Congenital Heart Disease
Arrhythmias• Arrhythmias• Cardiomyopathies• Prevention• Role of the Primary Care Physiciano e o e a y Ca e ys c a
45
Our ChallengeOur ChallengeOur ChallengeOur Challenge• SCD is incredibly rare• SCD is incredibly rare
• First symptom is often SCD or aborted SCDFirst symptom is often SCD or aborted SCD
• Identify children at risk for SCD in feasibleIdentify children at risk for SCD in feasible and cost-effective manner
• Provide a reasonable intervention to decrease riskdecrease risk
46
PreventionPreventionPreventionPrevention• Primary preventionPrimary preventionInterventions to decrease risk of initial SCD
• Secondary preventionI i d i k f bInterventions to decrease risk of subsequent
events
47
PrePre--participation Screeningparticipation ScreeningPrePre participation Screeningparticipation Screening• Identify young athletes with 7Identify young athletes with
cardiovascular abnormalities
on 2
007
• Controversy regarding extent of screening of athletes C
ircul
atio
screening of athletesMedical history and examECG?
et a
l, C
ECG?Echocardiogram? M
aron
48
Screening IssuesScreening IssuesScreening IssuesScreening Issues• Estimates of up to 10 million require
screening (high school > 5 million)
M t t ti ifi• Most asymptomatic or non-specific
C di l b liti 0 3% f• Cardiovascular abnormalities ~0.3% of athlete population
• Incidence of SCD in high school athletes 1/200 000~1/200,000 per year
49
AHA Recommendations for AHA Recommendations for S i f C titi Athl tS i f C titi Athl tScreening of Competitive AthletesScreening of Competitive Athletes
• 12 key elements 712 key elementsPersonal HistoryFamily History on
200
7
Family HistoryPhysical Examination
Circ
ulat
io
• Parental verification important• Repeated after 2 years et
al,
C
• Repeated after 2 years• Repeated prior to college athletics M
aron
50
Personal HistoryPersonal HistoryPersonal HistoryPersonal History• Exertional chest pain/discomfort 7Exertional chest pain/discomfort• Excessive exertional and unexplained
dyspnea/fatigue on 2
007
dyspnea/fatigue• Unexplained syncope/near syncope
f Circ
ulat
io
• Prior recognition of heart murmur• Elevated systemic blood pressure et
al,
CM
aron
51
Family HistoryFamily Historyy yy y• Premature death before age of 50 yrs due to
h t di i ≥ 1 l ti 7heart disease in ≥ 1 relative
• Disability from heart disease in close relative on 2
007
• Disability from heart disease in close relative < 50 yrs
Circ
ulat
io
• Presence of specific cardiac conditions in family members et
al,
CM
aron
52
Physical ExamPhysical ExamPhysical ExamPhysical Exam• Heart murmur 7Heart murmur
• Femoral pulses (coarctation) on 2
007
p ( )
• Physical stigmata of Marfan syndrome
Circ
ulat
io
y g y
• Brachial artery blood pressure et a
l, C
y p
Mar
on
53
• “At the discretion of the examiner,a positive response or finding in 20
07
a positive response or finding in any 1 or more of the 12 items may
cula
tion
be judged sufficient to trigger a referral for cardiovascular al
, Circ
evaluation.”
aron
et
Ma
Routine ECG Screening?Routine ECG Screening?Routine ECG Screening?Routine ECG Screening?• European Society of Cardiology and 7European Society of Cardiology and
International Olympic Committee recommend ECG screening on
200
7
recommend ECG screening• AHA does not endorse routine ECG;
remains at discretion of individual physician Circ
ulat
io
remains at discretion of individual physicianLow prevalenceLimited resources et
al,
C
Limited resourcesCosts ($2 billion/yr; $3.4 mill/prevented death)
Mar
on
55
Exercise Restriction GuidelinesExercise Restriction GuidelinesExercise Restriction GuidelinesExercise Restriction Guidelines
• Detailed recommendations for conditions at risk for SCD
56
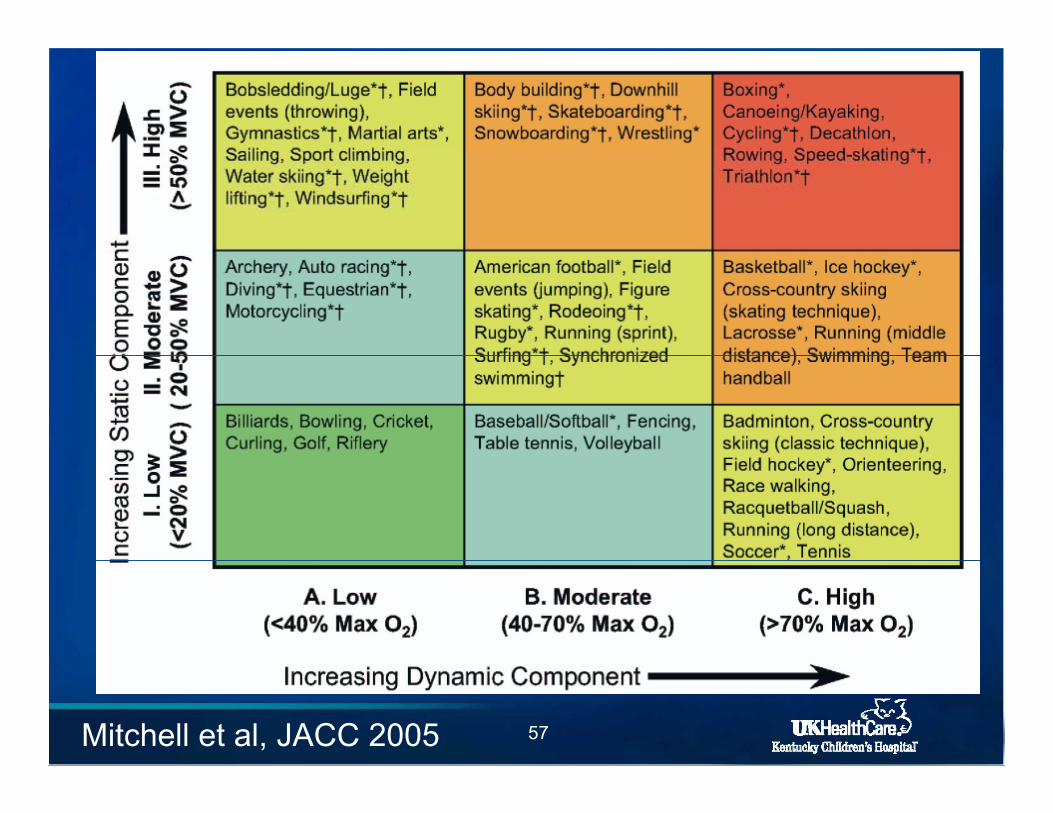
Exercise Restriction Exercise Restriction GuidelinesGuidelines
57Mitchell et al, JACC 2005
Competitive Sport RestrictionCompetitive Sport RestrictionCompetitive Sport RestrictionCompetitive Sport Restriction
R t i ti f ll t• Restriction from all sportsCoronary artery origin anomalyHypertrophic cardiomyopathyUntreated WPW syndrome
• Restricted to Class IARestricted to Class IALong QT syndromeAICDAICD
58
Primary PreventionPrimary Preventionyy• MedicationBeta blockade in LQT1
• AICDs/p congenital heart surgeryLQTSHCM
• EP study with ablationEP study with ablationWPW syndrome
• Surgical unroofing of anomalous coronary• Surgical unroofing of anomalous coronary59
Secondary PreventionSecondary PreventionSecondary PreventionSecondary Prevention• Competitive sports restrictionsCompetitive sports restrictions
• Medication
• AICD
• CPR training
• Automatic external defibrillators (AED)
60
Automatic External Automatic External Defibrillator (AED)Defibrillator (AED)
• Ventricular fibrillation is common final pathway to SCD in many cases
• Time to defibrillation is most important factor for survival in out of hospital VF
• Survival < 10% if > 10 minutes
61
AHA AED ProgramAHA AED ProgramAHA AED ProgramAHA AED Program• AED available within 5 minutesAED available within 5 minutesSchoolsOrganized SportsOrganized SportsTraining sitesArenas/StadiumsArenas/Stadiums
• CPR training for individuals involved at eachFi i i h• First activate emergency services, then initiate CPR and deploy AED
62
TopicsTopicsTopicsTopics• Sudden Cardiac DeathSudden Cardiac Death• Congenital Heart Disease
Arrhythmias• Arrhythmias• Cardiomyopathies• Prevention• Role of the Primary Care Physiciano e o t e a y Ca e ys c a
63
Role of the Primary Care Role of the Primary Care Ph i iPh i iPhysicianPhysician
• Clinical presentationClinical presentationExertional symptomsChest pain syncope dyspneaChest pain, syncope, dyspnea
Syncope Inconsistent w/ neurocardiogenic/vasovagal Inconsistent w/ neurocardiogenic/vasovagalOther etiology not found
Early fatigueEarly fatigue
64
Role of the Primary Care Role of the Primary Care PhysicianPhysician
• Family HistoryRecurrent syncopeRecurrent syncope
Unexplained sudden death, SCD, SIDS
Known cardiovascular entities associated with SCDwith SCD
65
Role of the Primary Care Role of the Primary Care PhysicianPhysician
• Physical ExamHarsh, systolic murmur at upper right sternal y pp g
border or click consistent w/ aortic stenosisValsalva maneuver or standing may
accentuate systolic murmur @ LLSB in HCMIrregular heart rateMarfan stigmata
66
Role of the Primary Care Role of the Primary Care PhysicianPhysician
• High index of suspicion
If b i ECG• If concerns, obtain ECG
• Err on initial restriction of sports• Err on initial restriction of sportsUtilize 36th Bethesda recommendations
• Refer to pediatric cardiology for further evaluationevaluation
67
AcknowledgementsAcknowledgementsAcknowledgementsAcknowledgements• Jason Grabham, RDCS, FASEJason Grabham, RDCS, FASE • Leslie Brashear, RDCS
Anil Attili MD• Anil Attili, MD• Douglas Schneider, MD• Thomas DiSessa, MD
68
Q ti ?•Questions?
69
ReferencesReferencesReferencesReferences• Azaouagh, A., et al., Arrhythmogenic right ventricular cardiomyopathy/dysplasia: a review and
update. Clin Res Cardiol, 2011. 100(5): p. 383-94. Antzelevitch, C., et al., Brugada syndrome: report of the second consensus conference: endorsed by the Heart Rhythm Society and the p y y yEuropean Heart Rhythm Association. Circulation, 2005. 111(5): p. 659-70.
• Berger, S., et al., Sudden cardiac death in children and adolescents: introduction and overview. Pediatr Clin North Am, 2004. 51(5): p. 1201-9.
• Cheitlin, M.D. and J. MacGregor, Congenital anomalies of coronary arteries: role in the pathogenesis of sudden cardiac death. Herz, 2009. 34(4): p. 268-79.
• Collura, C.A., et al., Left cardiac sympathetic denervation for the treatment of long QT syndrome and catecholaminergic polymorphic ventricular tachycardia using video-assisted thoracic surgery. Heart Rhythm, 2009. 6(6): p. 752-9.C d D t l C di l ti i ti i f titi thl t f• Corrado, D., et al., Cardiovascular pre-participation screening of young competitive athletes for prevention of sudden death: proposal for a common European protocol. Consensus Statement of the Study Group of Sport Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur Heart J, 2005. 26(5): p. 516-24.p y gy , ( ) p
• Davis, J.A., et al., Major coronary artery anomalies in a pediatric population: incidence and clinical importance. J Am Coll Cardiol, 2001. 37(2): p. 593-7.
• Fermini, B. and A.A. Fossa, The impact of drug-induced QT interval prolongation on drug discovery and development. Nat Rev Drug Discov, 2003. 2(6): p. 439-47.
70
ReferencesReferencesReferencesReferences• Frommelt, P.C., Congenital coronary artery abnormalities predisposing to sudden cardiac death.
Pacing Clin Electrophysiol, 2009. 32 Suppl 2: p. S63-6.• Maron, B.J., et al., Recommendations and considerations related to preparticipation screening
for cardiovascular abnormalities in competitive athletes: 2007 update: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: endorsed by the American College of Cardiology Foundation. Circulation, 2007. 115(12): p. 1643-4551643-455.
• Maron, B.J. and D.P. Zipes, Introduction: eligibility recommendations for competitive athletes with cardiovascular abnormalities-general considerations. J Am Coll Cardiol, 2005. 45(8): p. 1318-21.
• Maron, B.J., et al., Sudden death in young competitive athletes. Clinical, demographic, andMaron, B.J., et al., Sudden death in young competitive athletes. Clinical, demographic, and pathological profiles. JAMA, 1996. 276(3): p. 199-204.
• 36th Besthesda Conference: Eligibility Recommendations for Competitive Athletes with Cardiovascular Abnormalities . J Am Coll Cardiol, 2005
• Maron, B.J. and N.A. Estes, 3rd, Commotio cordis. N Engl J Med, 2010. 362(10): p. 917-27.g ( ) p• Maron, B.J., Sudden death in young athletes. N Engl J Med, 2003. 349(11): p. 1064-75.• Mitchell, J.H., et al., Task Force 8: classification of sports. J Am Coll Cardiol, 2005. 45(8): p.
1364-7.• Morita, H., J. Wu, and D.P. Zipes, The QT syndromes: long and short. Lancet, 2008. 372(9640): p y g ( )
p. 750-63.
71
ReferencesReferencesReferencesReferences• Napolitano, C. and S.G. Priori, Diagnosis and treatment of catecholaminergic polymorphic
ventricular tachycardia. Heart Rhythm, 2007. 4(5): p. 675-8.y y , ( ) p• Pignatelli, R.H., et al., Clinical characterization of left ventricular noncompaction in children: a
relatively common form of cardiomyopathy. Circulation, 2003. 108(21): p. 2672-8.• Postema, P.G., et al., Accurate electrocardiographic assessment of the QT interval: teach the
tangent. Heart Rhythm, 2008. 5(7): p. 1015-8 • Rivara, F.P. and D.C. Grossman, Prevention of traumatic deaths to children in the United
States: how far have we come and where do we need to go? Pediatrics, 1996. 97(6 Pt 1): p. 791-7.
• Rubart, M. and D.P. Zipes, Mechanisms of sudden cardiac death. J Clin Invest, 2005. 115(9): p. 2305-15.
• Towbin, J.A., et al., Incidence, causes, and outcomes of dilated cardiomyopathy in children. JAMA, 2006. 296(15): p. 1867-76.
• Vincent, G.M., Role of DNA testing for diagnosis, management, and genetic screening in long QT syndrome hypertrophic cardiomyopathy and Marfan syndrome Heart 2001 86(1): p 12 4QT syndrome, hypertrophic cardiomyopathy, and Marfan syndrome. Heart, 2001. 86(1): p. 12-4.
• Wren, C., J.J. O'Sullivan, and C. Wright, Sudden death in children and adolescents. Heart, 2000. 83(4): p. 410-3.
72


















