
Script # 12 .. Bone disorders 4
24
1
Transcript of Script # 12 .. Bone disorders 4

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 1/24
1

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 2/24
2
Part one : By Osama Yousef
Before we start talking about Paget‟s disease of bone, you have to know the
following things :
Osteoclast Bone resorption .
Osteoblast Bone deposition.
Paget‟s disease of bone is of unknown etiology, there are hypothesis about the
etiology of this disease, but most of the cases are of unknown etiology.
Normally there is a balance between the activity of bone deposition and bone
resorption and this is called normal bone remolding, but in Paget‟s disease of bone
this balance is not kept. We have excessive or abnormal : bone resorption or in
other words : Osteoclast function , either it is excessive ; hyperosteoclast function
or abnormal .
In Paget‟s disease of bone there are three overlapping phases :
1. The first phase is called “Predominantly osteolytic phase “: there is excessive
osteoclast activity (or excessive bone resportion) in this stage the radiograph
will be radiolucent (more black in color).
2. The second phase will be a mix between osteolytic (bone resorption ) and
osteoblastic ( bone deposition ) , all of which are taking place at the same time.

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 3/24
3
3. The third phase is the “Sclerotic phase or Osteosclerotic bone“ where the
osteoblastic activity is the predominant and the bone becomes osteoscleraotic
the bone will show the following signs in this stage :
Dense, hard , brittle, easily fractured upon extraction and with low blood
supply, all of these signs might lead to osteomaliets and bone infectionwhich will be discussed in later occasions
The first phase and second phase, we will have excessive bleeding because of
increases of vascularity in the marrow spaces, in fact we have too much vascularity
the patient might have heart failure. The second phase could be also considered as
a vascular phase. So the complications of the first and second phase is excessive
bleeding and hemorrhage after extraction due to high vsacularity
Deformity of bones will occur in the first and second phases. In the third phase it‟llfix the deformity and make it dense or; sclerotic.
It should be noted that Paget‟s disease of bone is a chronic disease .
The disease is most common in areas such as United kingdom, Australia and
North America, in fact in England because they wear hats, the patient will
complain about their hats are getting smaller in size, but what‟s actually happing is
that their skulls are getting bigger!
We are going to talk about the sgins of Paget‟s disease in different areas of the
human body .
The effects on the bones can be summed up as follows :
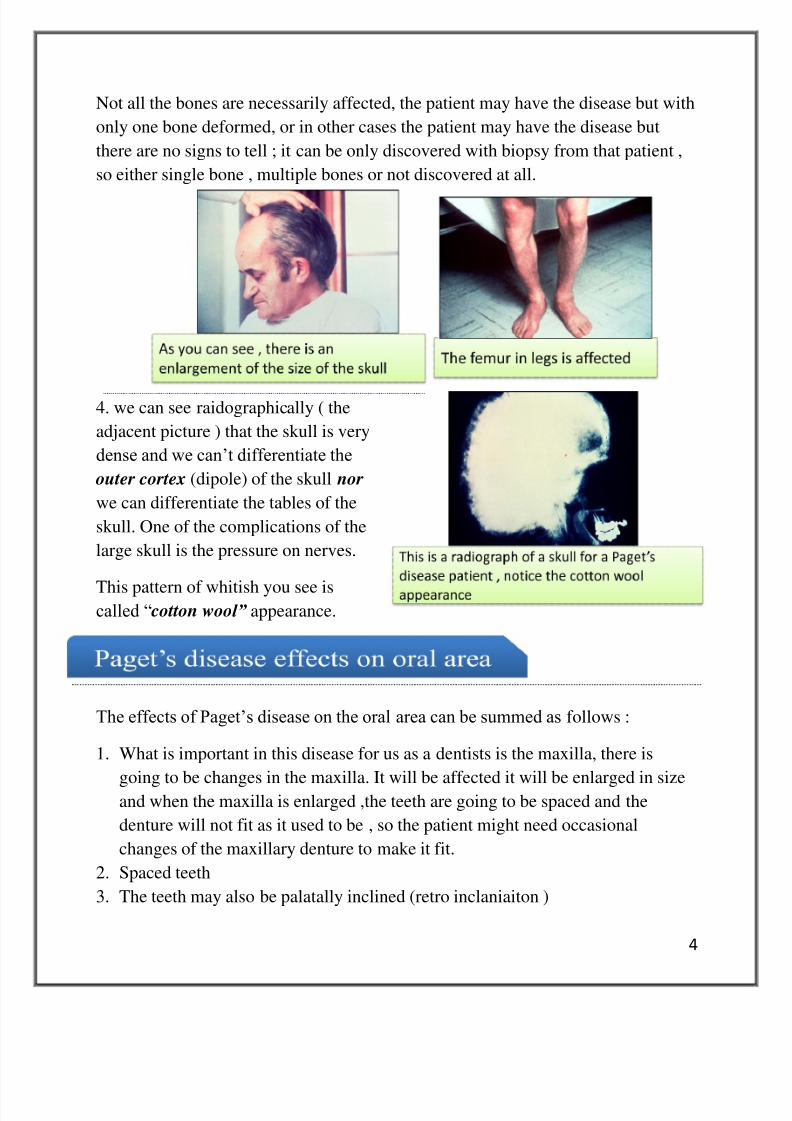
1. There is bony deformity, the head becomes large.
2. The femur in legs will have curved apperance
3. the sacrum in the vertebral column is also affected (giving the bend
appearance).
8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 4/24
4
Not all the bones are necessarily affected, the patient may have the disease but with
only one bone deformed, or in other cases the patient may have the disease but
there are no signs to tell ; it can be only discovered with biopsy from that patient ,
so either single bone , multiple bones or not discovered at all.
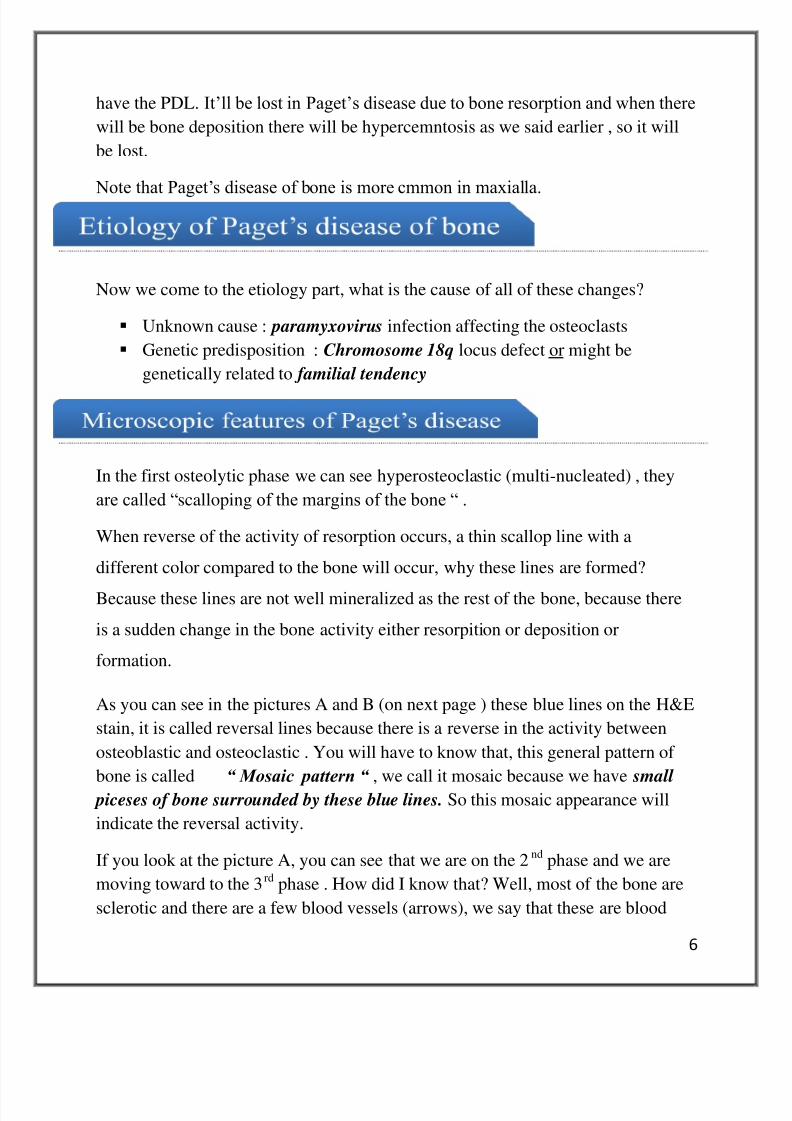
4. we can see raidographically ( the
adjacent picture ) that the skull is very
dense and we can‟t differentiate the
outer cortex (dipole) of the skull nor
we can differentiate the tables of the
skull. One of the complications of the
large skull is the pressure on nerves.
This pattern of whitish you see iscalled “ cotton wool” appearance.
The effects of Paget‟s disease on the oral area can be summed as follows :
1. What is important in this disease for us as a dentists is the maxilla, there is
going to be changes in the maxilla. It will be affected it will be enlarged in sizeand when the maxilla is enlarged ,the teeth are going to be spaced and the
denture will not fit as it used to be , so the patient might need occasional
changes of the maxillary denture to make it fit.
2. Spaced teeth
3. The teeth may also be palatally inclined (retro inclaniaiton )

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 5/24
5
4. hypercemntosis and the ankylosis , ankylosis as you already know is the fusion
between cementum and bone without PDL space .
5. We also might have root resorption , which will occur mainly in the first phase .
6. We also might have Post-extraction hemorrhage and More prone to infection in
sclerotic phase as we said earlier.
7. Widening of the alveolar ridges
8.Abnormal occlusion
Due to hypercemntosis and ankylosis in Paget‟s disease , there might be surgical
complications because the tooth won‟t come out easily.
9. Loss of the lamina dura in teeth , what is the lamina dura ? It is the compact
bone or dense bone it appears radiographically as white lines surroding the teeth,
these white lines have spaces between them and the root and within this space we
8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 6/24
6
have the PDL. It‟ll be lost in Paget‟s disease due to bone resorption and when there
will be bone deposition there will be hypercemntosis as we said earlier , so it will
be lost.
Note that Paget‟s disease of bone is more cmmon in maxialla.
Now we come to the etiology part, what is the cause of all of these changes?
Unknown cause : paramyxovirus infection affecting the osteoclasts
Genetic predisposition : Chromosome 18q locus defect or might be
genetically related to familial tendency
In the first osteolytic phase we can see hyperosteoclastic (multi-nucleated) , they
are called “scalloping of the margins of the bone “ .
When reverse of the activity of resorption occurs, a thin scallop line with a
different color compared to the bone will occur, why these lines are formed?
Because these lines are not well mineralized as the rest of the bone, because there
is a sudden change in the bone activity either resorpition or deposition or
formation.
As you can see in the pictures A and B (on next page ) these blue lines on the H&E
stain, it is called reversal lines because there is a reverse in the activity between
osteoblastic and osteoclastic . You will have to know that, this general pattern of
bone is called “ Mosaic pattern “ , we call it mosaic because we have small
piceses of bone surrounded by these blue lines. So this mosaic appearance will
indicate the reversal activity.
If you look at the picture A, you can see that we are on the 2nd
phase and we are
moving toward to the 3rd
phase . How did I know that? Well, most of the bone are
sclerotic and there are a few blood vessels (arrows), we say that these are blood

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 7/24
7
vessels because if you look closer you can see endothelial lining. You should note
that determining the phases is a hard thing, because often they are overlapping.
Increased serum alkaline phosphatase this reflects the bone resorption or
deposition
Serum calcium and phosphorus occasionally increased usually within
normal limits. (There is change in the calcium/phosphor but they are in the
normal range) .
In order to treat Paget‟s disease patient we have to stop the osteoclastic activity,
and we do this by giving Calcitonin and diphosphonates .

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 8/24
8
Paget‟s disease is usually not fetal, but it creates lesions inside the bones and these
lesions might lead to increased incidence of malignant neoplasms , most common
type of the malignat complications is osteosarcoma. Note that the incidence for
this is <1%.
You should also remember the default sings of paget‟s disease of bone which we
discussed earlier as, skull enlargement and the maxilla denture problems related to
this disease which may count also as complactions.
Question : “Are each phase of the three phases with a fixed timing “ ? the answer
was : “ no , they have no specific timing , they are overlapping but the leastduration would be the first phase “.
Question:” You said that Paget‟s disease affects the maxilla; does it affect the
mandi ble as well?” Yes it does, but the maxilla rate is greater and it is more
commonly involved, it depends on which bone the disease choose to infect .
As we said, one of the complications of Paget‟s disease is the lesions that are
inside the bone , looking at this picture which phase is this picture indicating ? it is
the first because we have too many osteoclasts activity and scalloped border of the
bone. ( picture of gaint cell lesion , next page )
The doctor said that we have already talked about central giant granuloma and we
have already compared it with hyper-para-thyrodism , honestly she just passed the
slides without talking too much about it , it is up to you if you want to study it or
not.

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 9/24

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 10/24
10
It is not common in children and it is not of developmental cause , in the past they
thought that it had a developmental connection to it , but it turned out not to be ,
because if it were developmental how come we can‟t see it more in children .
Some say it increases in size because of masticatory function, especially patients of
burixsm habit , but if you think about it there isn‟t much of muscles movement
going on the palate so it is just one of the theories , other causes is unknown of
why it changes in size . But burixsim habit has a link to it.
This change in size due to the muscles pull might be more evident in the torus
mandibularis , which will be discussed next .
It is found at the lingual aspect, present above the mylohyoid line , it is found in
90% bilateral . Note that torus palatinus is more common than torus mandibularis
They are neither benign nor malignant tumors so they are not tumors at all! , still
their significance comes from:
The denture of the patient will not fit propbley as it used to be.

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 11/24
11
The dentist might not understand what are the
raidopacity that are present (look the x-ray). The
dentist might be confused with the diagnoses,
until he meets the patient and discover these
toruies , see picture A.
They occur in the Buccal aspect of the alveolar
bone and mainly on the maxillary teeth, people
with “gum smile “will be more concerned than
normal people because these Buccal exostoses
will be more shown .
What you have to do is only reassurance you
have to explain to them that these are just
developmental changes and there is absolutely
no need to worry, if they are too much worried,
and then you can make a surgical removal for
them.
Like the Buccal exostosis we can also have palatal
exostosis (picture), they may occur palatal to the last
molar area.

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 12/24
12
We also have Subpontine exostosis which is after extraction of the tooth and
constriction of a denture or a bridge there might be exostotic mass, why it formed
there? Well maybe because it is reactive in the space provided by the denture or
bridge.~ note this exostosis is not mentioned in the book.
It is composed of dense compact bone (look picture),
you can notice the few bone marrow spaces. Most of
the time the histopathology is dense compact bone.
Dense bone island is of idopathic cause ,
you may see that the tooth is, not havinglow grade infection ,it is not carious and the
bone is not cemnto-ostasis dysplisa because
it is not surrondeed by raidolucent area , it
is not causing bone expanison so in this
case you call it dense bone islnad or bone
scar , as the scars in the skin.
It might not be fused to the root or it might be fused to the root , looking at the
picture above the doctor asked to give some dignoses for it . Some answered that it
might be hypercemntosis the dr said no because hypercemntosis occuer in the root
surface and the hypercemntosis will still show the PDL space , unlike the picture.
Others said concrescence , again the dr said no because in the concrescence you
can‟t find dense bone areas within the bone itself , the concrescence is just fusion
of the roots between adjacent teeth with cemntum , here if you take a look you

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 13/24

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 14/24
14
It is a true benging tumor of bone meaning that it will keep enlarging in size slowly
with time, it is usually not multiple like the Buccal exstosis and not present in the
midline of the palate nor the above the mylohyoid line . It is usually found at the angle of the mandible.
It could be sub periosteal (immediately below the perotisum) or diffused within
the bone (central ). The ostoemoa may be compact or cancellous bone .
Looking at picture A, what is this mass? Is it soft tissue ? No , it is a bony mass
, that is found at the angle of the mandible and if you look at the radiograph you
can notice that it is a bony mass , it is denser than the bone , so it is osteomoa.
It requires surgical removal because it is continuosaly growing , unlinke buccal
exoseosis they don‟t require surgical treatment expect when denture
constriaction or cosmatic reasons.
Looking at picture B, what do you think this disease is if you knew it is
continuously enlarging its size. Is it osteoma or Buccal exostosis ? The answer is
osteomoa because it is continuously enlarging in size and because it is found as a
single proturbrance , Buccal exosteosis is found multiple and not only one.
But if the osteoma are multiple in a single patient we should think about Gardner
syndrome (we discussed gardner syndrome in the middle exam material, we said
that gadrnder syndrome had a relation with multiple supernumerary teeth).

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 15/24
15
The patients of this syndrome will have premalagenit adenomas of the colon, and
100% of those patients will have adenocarcinoma of the intestine .
What shall we do for these patients ? Actually they cut their colon as prohylaxis
to make sure they don’t get the worse case which is the adecnocarcinoma of the
intestine.
It is Autosomal dominenet
Polyposis coli marked tendency for malignant change
Fibrous tumors
Sebacous cysts of the skin
Multiple impacted and supernumerary teeth
Looking at the picture A , you can see we have two
osteomoma , so this person might have Gardner syndrome ,
so genetic analysis is important for this patient .
Looking at picture B , you can notice that the osteomia is
not below the bone it is actually wihtin the bone so it is of
central type. It looks also cancilous bone , not very dense.
A student asked a question “ from picture B , sometimes we
might get confiused between exosteosis and osteomoa “ .
The answer was as follows : “ No , this is osteomia because
of two things :
1. In oral pathology we don‟t have a single exososs
apperaing at the angle of the mandbile
2. The angle of the mandbile is a common place for
osteoma

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 16/24
16
A student asked another question “ The buccl exosteosis looks simillar to what we
saw in the ginvial cysts “ . The answer was “ during the clinc trial , upon palpation
the cyst will show fluid materials , while the osteoma will be a bony mass ; will not
show fluid “.
It is a true benign slow growing tumor of bone that consists of mature bone.
It is more frequent in the mandible than the maxilla.
It may arise as Sub periosteal or central.
Multiple osteomas is a feature of Gardner Syndrome.
With this we finished talking about osteoma .
Is a benign tumor but locally aggressive.
It may destroy the cortical plates of bone,
and may reach big sizes and cause fracture to
the mandible.
Histologically ,, Osteoblastoma are totally
different from Osteoma…. The doctor didn't talk
about these differences.
Microscopically, may be confused with
Osteosarcoma because it has active cells
within it.
Clinically and radiographically may look like Cementoblastoma. But thedifference is that Osteoblastoma is separated from the cementum of the root.

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 17/24
17
Is a Benign tumor of cementum
It is well demarcated from the surrounding
bone It is fused with the cementum of the root.
It's increasing in size because it's a true
tumor of bone.
Dense lesion that has mixed radiolucent
and radiopaque according to the activity of the
cells, with a surrounding radiolucent line.
*** In the adjacent picture, Well defined
rounded radilucent small area between the roots of mandibular premolarsis Mental Foramena !!
Is a malignant tumor of bone
The malignant cells in it are osteoblast .
** The normal product of osteoblast is bone, the immature bone is called
woven bone, and the matrix of this immature bone is called osteoid ,which
is not well mineralized yet.
It will have malignant osteoblast that will form osteoid which will be
malignant, too.
Most common primary malignant tumor in jaws.
*** Primary tumors come from the bone itself, but Secondary tumors
come from metastasis NOT from the bone itself and it may come from
the oral epithelium in the oral cavity.
8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 18/24
18
The age of onset is around 30 a little bit later than osteosarcoma in other
long bone in the body ,
May be central, or may start from under the periosteom which is easier to
be diagnosed.
The mandible will have better prognosis, because the maxilla may have
many marrow spaces that the osteosarcoma may spread through them easily
and early .
Ostoesarcoma may increase in paget's deiseas of bones.
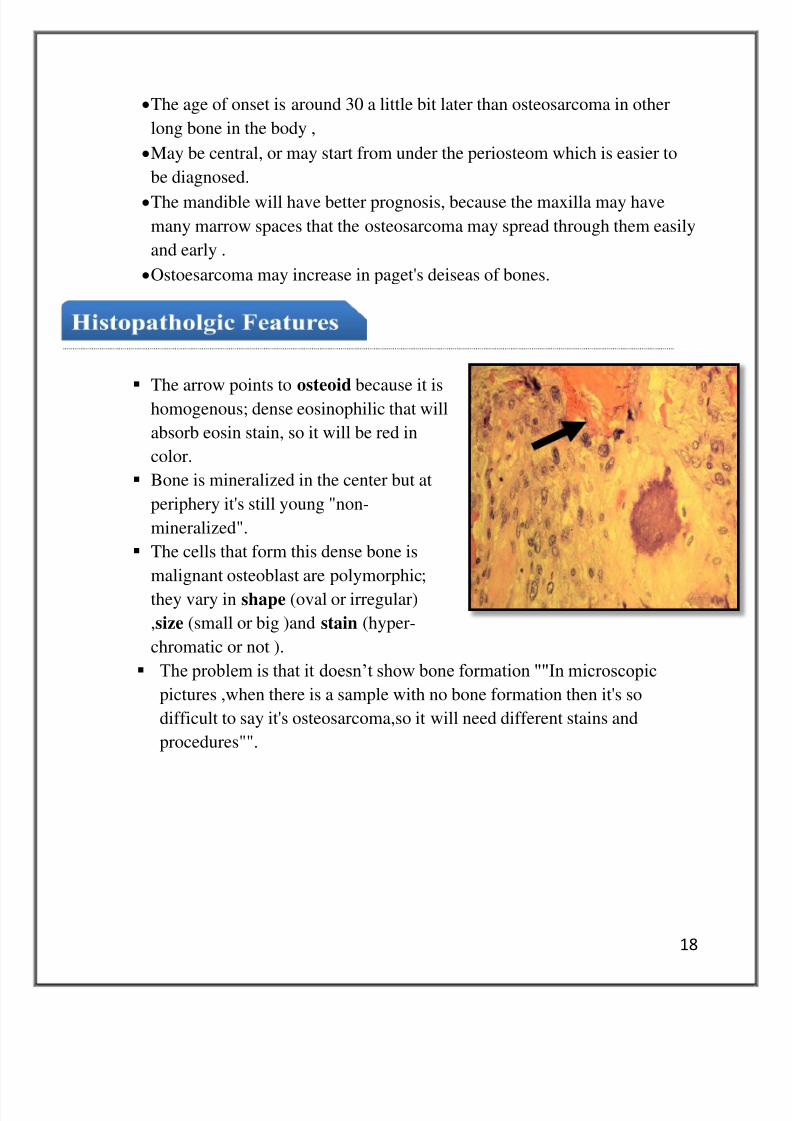
The arrow points to osteoid because it ishomogenous; dense eosinophilic that will
absorb eosin stain, so it will be red in
color.
Bone is mineralized in the center but at
periphery it's still young "non-
mineralized".
The cells that form this dense bone is
malignant osteoblast are polymorphic;
they vary in shape (oval or irregular)
,size (small or big )and stain (hyper-
chromatic or not ).
The problem is that it doesn‟t show bone formation ""In microscopic
pictures ,when there is a sample with no bone formation then it's so
difficult to say it's osteosarcoma,so it will need different stains and
procedures"".

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 19/24
19
Malignant tumors are rapidly
growing, therefore they don‟t give
time to the body to form a welldefined corticated region; ill-defined
radiolucent region.
This lesion will eat everything (the
roots, the bone).
It may perforate through the cortex
causing expansion of the bone.
May go inside PDL causing
symmetrical widening.
It may go out the soft tissue and
produce rapidly enlargement lesion
with ulceration later on, because the
epithelium will be thin which a
secondary manifestation is and mastication of the above teeth will allow
the enlargement, it fells bony.
The lesion may be radiopaque or radiolucent or mixed according to the
amount of osteoid that will be formed within the lesion; if it has more
bone radiobaque but if it has less bone then it will be radiolucent.
Swelling Pain, toothache because the tumor may press on the nerves and it
will resorb teeth.
Loose or displaced teeth Bleeding Paresthesia because of pressure on nerves

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 20/24
20
*** Sun-ray pattern: due to formation of bony trabeculae in perpendicular
angle to the bone .It is present only in 25% of all patients and it may present in
other lesions.
**Not unique to osteosarcoma**
Early signs: localized symmetrical widening
of PDL because it is easy to go through them.
Treatment: Surgery, radiation thereby or
chemotherapy.
***If the whole lesion was like this
then it will appear radiolucent.
End of part two

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 21/24
21
Part three : By Ali Al-Qudsi
Chondrosarcoma is a tumor of chondroblasts (cartiallage producing cells),
classified as a primary bone tumor, due to remnants of cartilage in the jaw
(Mandible = Head of the condyle / Maxilla = Close to the anterior part of the
maxilla).
Product of chondrobalsts = Chondroid
Chondrosarcoma = Malignant, Chondroma = Benign.
The more common of the two is the malignant form (Chondrosarcoma).
The chondroid matrix appearance
is not completely pink/eosophillic
it appears a mix of eosniphillic
and basophilic, the
chondoroblasts themselves are
found in their lacuna but they are
Pleomorphic (varying size),
Mulit-loculated, can Be Bi-
nucleated, (highly cellular &
Contains plump cells).
The appearance of Chondroma (benign form) closely resembles that of the
chondrosarcoma except a few differences, mainly No bi-nucleation, no
Hyperchromatism and minimal pleomorphisim (picture A in next page )

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 22/24
22
Chondrosarcomas/Chondromas can appear
radiographically as radio-opaque, radio-
lucent or mixed depending on the amountof chondroids found in the lesion. These
chondroids may later ossify (turn into
bone) with time which makes it difficult to differentiate between Chondrosarcomas
and Osteosarchomas microscopically (each has a different treatment, therefore it‟s
critical to differentiate between the two.
Mandibular lesions have a better prognosis (less dangerous)
Chondrosarcomas are less aggressive than other sarcomas (slower growth
rate).
Plasma cells (found in bone marrow) may become cancerous leading to
a condition known as multiple myelomas (malignant tumor/neoplasm of plasma
cells), may be present as a Single
lesion/Multiple lesions. Multiple myeloma ismost common in elderly patients, a common
symptom of multiple myelomas is sever bone
pain, upon radiographic investigation the
patients skull appears to have „a punched out
appearance’ (present as well defined well
rounded radiolucencies). Multiple myeloma may
affect several bones (skull, vertebral column,
mandible and other bones).
The product of plasma cells are immunoglobulins (IgG, IgA, IgE…)
A single lesion of defected plasma cells is called Plasma-Cytoma

8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 23/24
23
Upon protein investigation of blood there will be a peak/spike in one of the
blood proteins due to monoclonal proliferation of the plasma cells. This
protein is the M Spike/Para-protein (M in relation to myeloma) this M
spike represents the increase in the number of IGs.
Malignant tumors are usually accompanied by rapid
growth and destruction accumulating in both bone and
soft tissue. Radiographically the lesions appear Ill-
Defined leading to a radiographical feature called
„floating in air teeth’ (teeth appear to be unsupported
at all- very common in Langerhan Cell Disease) due
to the destruction in bone (the tooth is only supported
by abnormal soft tissue- hardly any bone left).
The most commonly affected bones are the
Skull, Vertebrae, Sternum and Pelvis; however
it‟s possible that the only clinical manifestation
is lower back pain.
Electrophoresis to search for „M Spike Protein‟
Bence-Jones Proteins- light protein chains that may leak out in the urine
(present in 50% of the cases)
Blood may contain Increase in Calcium (due to increased bone resorption)
Amyloidosis (Protein presence in tissue of chronic diseases) leads to
Macroglossia or swelling.
Sharply demarcated punched out radiolucencies (diploe of the skulls are
evident- lost in Paget‟s disease)
8/3/2019 Script # 12 .. Bone disorders 4
http://slidepdf.com/reader/full/script-12-bone-disorders-4 24/24
24
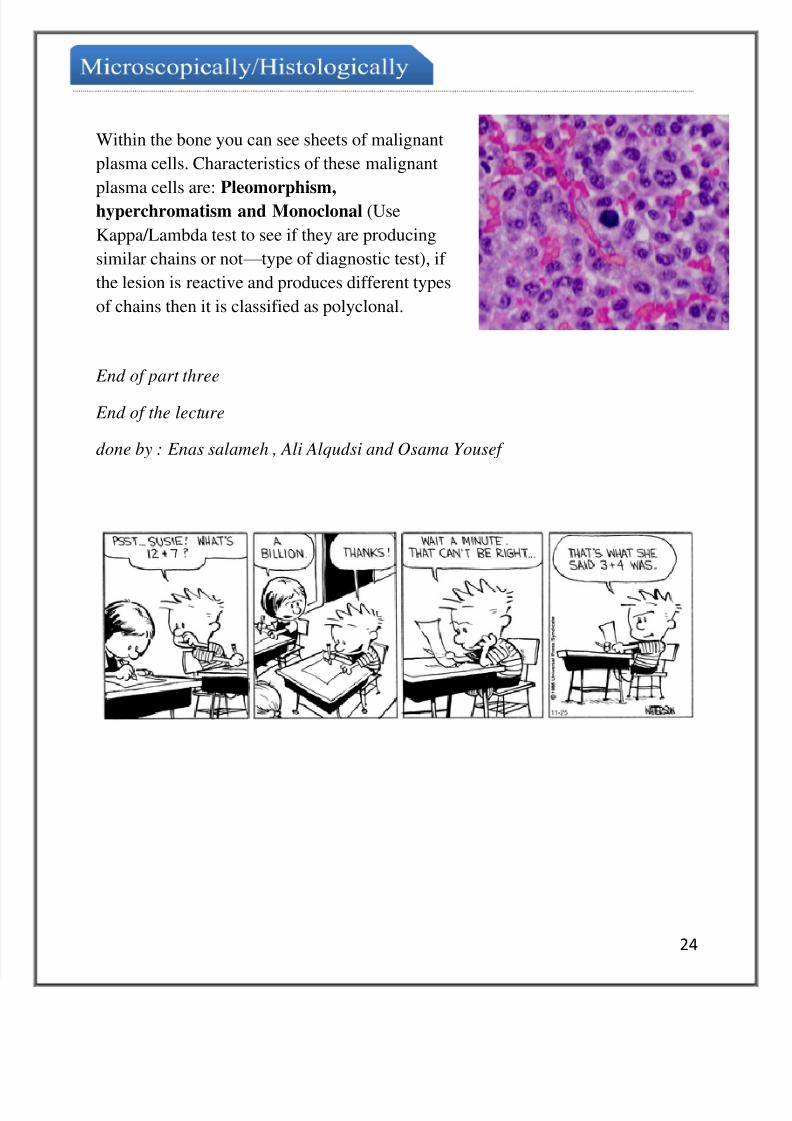
Within the bone you can see sheets of malignant
plasma cells. Characteristics of these malignant
plasma cells are: Pleomorphism,hyperchromatism and Monoclonal (Use
Kappa/Lambda test to see if they are producing
similar chains or not — type of diagnostic test), if
the lesion is reactive and produces different types
of chains then it is classified as polyclonal.
End of part three
End of the lecture
done by : Enas salameh , Ali Alqudsi and Osama Yousef


















