Screening for Child and Adolescent Depression in Primary Care … · 2011-11-10 · REVIEWARTICLE...
22
DOI: 10.1542/peds.2008-2415 2009;123;e716-e735 Pediatrics Selvi B. Williams, Elizabeth A. O'Connor, Michelle Eder and Evelyn P. Whitlock Systematic Evidence Review for the US Preventive Services Task Force Screening for Child and Adolescent Depression in Primary Care Settings: A http://www.pediatrics.org/cgi/content/full/123/4/e716 located on the World Wide Web at: The online version of this article, along with updated information and services, is rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2009 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk publication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly . Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.org Downloaded from
Transcript of Screening for Child and Adolescent Depression in Primary Care … · 2011-11-10 · REVIEWARTICLE...

DOI: 10.1542/peds.2008-2415 2009;123;e716-e735 Pediatrics
Selvi B. Williams, Elizabeth A. O'Connor, Michelle Eder and Evelyn P. Whitlock Systematic Evidence Review for the US Preventive Services Task Force
Screening for Child and Adolescent Depression in Primary Care Settings: A
http://www.pediatrics.org/cgi/content/full/123/4/e716located on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2009 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

REVIEW ARTICLE
Screening for Child and Adolescent Depression inPrimary Care Settings: A Systematic Evidence Reviewfor the US Preventive Services Task ForceSelvi B. Williams, MD, MPH, Elizabeth A. O’Connor, PhD, Michelle Eder, PhD, Evelyn P. Whitlock, MD, MPH
Center for Health Research, Kaiser Permanente, Portland, Oregon; Oregon Evidence-Based Practice Center, Portland, Oregon
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
CONTEXT.Depression among youth is a disabling condition that is associated withserious long-term morbidities and suicide.
OBJECTIVE. To assess the health effects of routine primary care screening for majordepressive disorder among children and adolescents aged 7 to 18 years.
METHODS.Medline, the Cochrane Central Registry of Controlled Trials, PsycInfo, theCochrane Database of Systematic Reviews, recent systematic reviews, experts, andbibliographies from selected studies were the data sources. The studies selected werefair- and good-quality (on the basis of US Preventive Services Task Force criteria)controlled trials of screening and treatment (selective serotonin reuptake inhibitorand/or psychotherapy), diagnostic accuracy studies, and large observational studiesthat reported adverse events. Two reviewers quality-graded each article. One re-viewer abstracted relevant information into standardized evidence tables, and asecond reviewer checked key elements.
RESULTS.We found no data describing health outcomes among screened and un-screened populations. Although the literature on diagnostic screening test accuracyis small and methodologically limited, it indicates that several screening instrumentshave performed fairly well among adolescents. The literature on treatment efficacy ofselective serotonin reuptake inhibitors and/or psychotherapy is also small but in-cludes good-quality randomized, controlled trials. Available data indicate that selec-tive serotonin reuptake inhibitors, psychotherapy, and combined treatment areeffective in increasing response rates and reducing depressive symptoms. Not allspecific selective serotonin reuptake inhibitors, however, seem to be efficacious.Selective serotonin reuptake inhibitor treatment was associated with a small absoluteincrease in risk of suicidality (ie, suicidal ideation, preparatory acts, or attempts). Nosuicide deaths occurred in any of the trials.
CONCLUSIONS. Limited available data suggest that primary care–feasible screening toolsmay accurately identify depressed adolescents and treatment can improve depressionoutcomes. Treating depressed youth with selective serotonin reuptake inhibitors maybe associated with a small increased risk of suicidality and should only be consideredif judicious clinical monitoring is possible. Pediatrics 2009;123:e716–e735
MAJOR depressive disorder (MDD) is a debilitating condition that has beenincreasingly recognized among youth, particularly adolescents. The preva-
lence of current or recent depression among children is 3% and among adolescentsis 6%.1 The lifetime prevalence of MDD among adolescents may be as high as 20%.2–4
Adolescent-onset MDD is associated with an increased risk of death by suicide,suicide attempts, and recurrence of major depression by young adulthood.5–7 MDD isalso associated with early pregnancy, decreased school performance, and impairedwork, social, and family functioning during young adulthood.6–8 Despite the significant public health burden of MDD,studies have indicated that the majority of depressed youth do not receive any type of treatment.9–11
Mass screening in primary care could help clinicians identify missed cases and increase the proportion of depressedchildren and adolescents who initiate appropriate treatment. It could also help clinicians to identify cases earlier inthe course of disease. Depression-screening tools have been developed that are feasible for use in primary caresettings.12 Current, reliable data describing screening practices for pediatric depression, however, are not available. In
www.pediatrics.org/cgi/doi/10.1542/peds.2008-2415
doi:10.1542/peds.2008-2415
KeyWordsdepression, primary care, screening,treatment, children, adolescents
AbbreviationsMDD—major depressive disorderSSRI—selective serotonin reuptakeinhibitorFDA—Food and Drug AdministrationUSPSTF—US Preventive Services TaskForceKQ—key questionDARE—Database of Abstracts of Reviewsof EffectsCDSR—Cochrane Database of SystematicReviewsAHRQ—Agency for Healthcare Researchand QualityPHQ-A—Patient Health Questionnaire forAdolescentsBDI-PC—Beck Depression Inventory-Primary Care VersionSDQ—Strengths and DifficultiesQuestionnaireRCT—randomized, controlled trialCI—confidence intervalRD—risk differenceSRE—suicide-related adverse eventRR—relative riskTADS—Treatment for Adolescents WithDepression StudyCBT—cognitive behavioral therapyIPT-A—interpersonal psychotherapy foradolescentsCCRCT—Cochrane Collaboration Registryof Clinical Trials
Accepted for publication Aug 11, 2008
Address correspondence to Selvi B. Williams,MD, MPH, Center for Health Research, KaiserPermanente, 3800 N Interstate Ave, Portland,OR 97227. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005;Online, 1098-4275); published in the publicdomain by the American Academy ofPediatrics
e716 WILLIAMS et al. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

1 study from the past decade, providers in communityhealth centers reported screening 64% of patients butdocumented screening for only 3%.13 Providers in ahealth maintenance organization estimated screening anaverage of 46% of their patients.14 These data, however,may overestimate how often primary care clinicians ac-tually screen for depression among pediatric popula-tions. Data based on direct observation or providerand/or patient report after specific clinical encounterswould be more reliable.
For mass screening to be effective, it would be neces-sary for delivered treatments to be effective in improvingpatients’ depression and alleviating suffering morequickly than no treatment. Trials demonstrating the ef-ficacy of drug treatments and time-limited psychother-apies among pediatric populations were first publishedduring the 1990s.15 Presently, fluoxetine, a selective se-rotonin reuptake inhibitor (SSRI), is the only pharma-cologic agent that the US Food and Drug Administration(FDA) has approved for the treatment of pediatric MDD.In 2004, however, the FDA released a black-box warn-ing about suicidality and antidepressant use in pediatricpatients. There have been numerous subsequent publi-cations discussing this issue, including the publication ofthe findings from the FDA meta-analyses evaluating riskof suicidality among 4582 pediatric patients treated withantidepressants.16
Among depressed youth identified in primary care,the majority seem to start treatment.17–19 During 1998,for example, 69.7% of youth with visits in primary carefor newly identified episodes of depression were eitherseen by a mental health specialist or received 1 or moredispensings of psychotropic medication in a health main-tenance organization during the subsequent 30 to 90days.17 Similarly, data from the National AmbulatoryMedical Care Survey (NAMCS) and the outpatient com-ponent of the National Hospital Ambulatory MedicalCare Survey (NHAMCS) showed that of adolescent pri-mary care visits in which depression was reported, anti-depressants were prescribed 52% of the time, and 68%of the visits included psychotherapy or counseling.18
In 2002, the US Preventive Services Task Force(USPSTF) concluded that there was insufficient evidence torecommend for or against routine screening of childrenor adolescents for depression (I recommendation).20 Atthe time of that review, no controlled trials of screeningamong child or adolescent populations were available.15
Likewise, relatively few studies of diagnostic accuracy,particularly in primary care settings or among children,were available. Furthermore, only 2 trials of SSRIsamong pediatric patients with MDD had been published.Our objective was to systematically assess the evidenceon screening for MDD among average-risk child andadolescent primary care populations to assist the USPSTFin updating its 2002 recommendation. We have summa-rized the evidence for the benefits and harms of screen-ing, the accuracy of primary care–feasible screeningtests, and the benefits and risks of treating depression byusing psychotherapy and/or SSRIs among patients aged7 to 18 years. The Oregon Evidence-Based Practice Cen-ter conducted the review, and the full evidence report is
available at www.preventiveservices.ahrq.gov. This arti-cle summarizes the report’s findings.
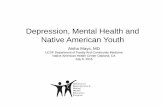
METHODSWe developed an analytic framework (Fig 1) and 5 keyquestions (KQs), by using USPSTF methods21, to guideour literature search. For all KQs, we searched for sys-tematic reviews, meta-analyses, and evidence-basedguidelines on depression screening, treatment, or asso-ciated harms in children and adolescents in the Databaseof Abstracts of Reviews of Effects (DARE), the CochraneDatabase of Systematic Reviews (CDSR), Medline, andPsycINFO from 1998 to May 2006. We also conducted aseries of literature searches through May 2007 for eachKQ (detailed in Appendix 1) and reviewed the searchresults for applicability to all KQs. Articles were alsoobtained from outside experts and through reviewingbibliographies of other relevant articles and systematicreviews. In addition to these searches for published tri-als, we searched pharmaceutical company and federalagency trial registries for unpublished trials of SSRIs. Allsearches were limited to articles in English. Inclusionand exclusion criteria specific to each question are de-tailed in Appendices 2 and 3.
Two investigators independently reviewed all ab-stracts for KQs 4 and 5. The initial search for KQs 1through 3 produced a very high yield (3418 abstracts).Therefore, we used a modified approach to reviewingthese abstracts as described in Appendix 2. Two investi-gators evaluated abstracts against a set of inclusion/ex-clusion criteria, including independent review using de-sign-specific quality criteria based on the USPSTFmethods, supplemented by National Institute for Healthand Clinical Excellence22 criteria for quality of systematicreviews (Appendix 4). Two investigators critically ap-praised all studies excluded for quality reasons. Datafrom included studies were abstracted into evidence ta-bles by 1 investigator and checked by another investiga-tor. Details of our quantitative synthesis approach andrationale are described in detail in Appendix 2. We iden-tified numerous recent systematic evidence reviews rel-evant to our KQs.16,23–40 Our approach to incorporatingthese reviews is described in Appendix 2.
We worked with 4 USPSTF liaisons at key pointsthroughout the review process to develop and refine theanalytic framework and KQs and to resolve issuesaround scope and approach. Research was funded by theAgency for Healthcare Research and Quality (AHRQ)under a contract to support the work of the USPSTF.AHRQ staff provided oversight for the project, includingreviewing the draft report and assisting in the externalreview of the draft evidence synthesis.
RESULTS
KQ1: Does Screening for Depression Among Children andAdolescents in the Primary Care Setting Improve HealthOutcomes?No trials were found that examined health outcomes ofdepression-screening programs in youth.
PEDIATRICS Volume 123, Number 4, April 2009 e717. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

KQ1a: Does Screening Increase the Proportion of PatientsIdentifiedWith and/or Treated for Depression?No trials were found that examined whether screeningled to an increased proportion of children or adolescentsidentified with and/or treated for depression.
KQ2: Are Depression-Screening Instruments for Children andAdolescents Accurate in Identifying Depression in PrimaryCare or School-Based Clinics?The overall body of evidence describing the accuracy ofdepression-screening instruments for children and ado-lescents is limited both in quantity and quality. Availableevidence applies mostly to adolescents. We identified 9relevant fair-quality studies4,41–51 that reported the accu-racy of 6 different depression-screening instruments (Ta-ble 1). Two of the studies were conducted in primarycare or school-based health clinics, 1 study was con-ducted in a community sample, and 6 were conducted inschool population samples (not through school healthclinics). Most studies restricted study samples to adoles-cents aged 12 years or older.
The performance characteristics of screening testswere quite varied across the studies. Sensitivity rangedfrom 18% to 100%, and specificity ranged from 38% to97%. This wide variation may be a result of the largenumber of instruments that was tested and the greatamount of heterogeneity across the populations in-cluded. The multiple differences between trials (includ-ing lack of replicating results for most of the tools stud-ied) make generalizations difficult. Another important
limitation is that all studies had methodologic flaws,including nonrandom selection, excessive delays be-tween screening and diagnostic interviews, high levels ofattrition, poor reporting of methods or attrition, smallsamples, or using a less-than-ideal reference standard.No single study stood out as being of good quality.
Sensitivity in the 2 primary care studies41,42 rangedfrom 73% for the Patient Health Questionnaire for Ad-olescents (PHQ-A) to 91% for the Beck Depression In-ventory-Primary Care Version (BDI-PC). Specificityranged from 91% (BDI-PC) to 94% (PHQ-A). The prev-alence of MDD among the 2 study samples was 9% to11%, yielding positive predictive values of 56% for bothtests and negative predictive values of 97% to 99% inthese 2 primary care samples. Because both studies ex-amined only adolescents, no information was found thatis directly applicable to screening younger children pre-senting to primary care.
Studies that involved younger children tended tohave poorer performance.43,49,50 The single study thatinvolved a community sample reported sensitivitiesranging from 33% to 63% for the Strengths and Diffi-culties Questionnaire (SDQ), examining various combi-nations of child, parent, and teacher report with 2 dif-ferent age ranges. The 33% sensitivity in the SDQ forchild-only report in those aged 11 to 15 years improvedto 63% when both parent and child reports were used.Sensitivity for those aged 5 to 10 years (parent reportonly) was 53%.
Clinical populations
Children and adolescents 7–18 y of age
(average risk)
Screening
2
Harms of screening
Patients identified with and/or treated for depression
Pharmacotherapy and/or psychotherapy
4
1
Treatment of depression -Remission -Improved depressive symptoms -Quality of life, global functioning -Improvement in comorbid disorders, change in health status, reduction in physical complaints -Suicidality, death 5
Adverse effects of treatment
1a
3
Key Questions: Screening and Treatment for Depression in Children and Adolescents
1. Does screening for depression among children and adolescents in the primary care setting improve health outcomes?
1a. Does screening increase the proportion of patients identified with and/or treated for depression?
2. Are depression screening instruments for children and adolescents accurate in identifying depression in primary care or school-based clinics?
3. What are the harms of screening?
4. Does the treatment of depression (SSRIs and/or psychotherapy) among screen-detected children and adolescents identified in primary care or comparable populations improve health outcomes?
5. What are the adverse effects of treatment?
FIGURE 1Analytic framework.
e718 WILLIAMS et al. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

KQ3: What Are the Harms of Screening?No studies were found that examined harms of depres-sion-screening programs in youth.
KQ4: Does Treatment of Depression (SSRIs and/orPsychotherapy) Among Screen-Detected Children andAdolescents Identified in Primary Care or ComparablePopulations Improve Health Outcomes?We identified 18 fair- or good-quality randomized, con-trolled trials (RCTs) that reported health outcomesamong children or adolescents with MDD treated withSSRIs,52–65 psychotherapy,55–58,66–74 or both an SSRI andpsychotherapy55–58 (Table 2). These trials evaluated theshort-term efficacy of 5 different SSRIs against placebo-control conditions, 10 different group or individuallydelivered psychotherapies compared with control condi-tions, and combined therapy (cognitive behavioral psy-chotherapy and an SSRI). Two of these trials were con-ducted in community or school-based clinical settings(both good-quality RCTs),55,72 and the remainder wereconducted in academic research centers or in schools.The majority (6 of 9) of SSRI trials included children asyoung as 8 years old in their study samples. In contrast,the majority of trials that tested psychotherapy interven-tions included only adolescents aged 12 to 14 years andolder. Only 2 psychotherapy trials included 9- or 10-year-olds, and no completed trials included childrenaged 7 or 8 years.
Nine of the SSRI or psychotherapy trials were rated asgood quality according to USPSTF criteria, and 9 were of
fair quality. Good-quality trials typically used a multi-gated screening procedure, including a clinical assess-ment, to identify depressed participants, measured out-comes through blinded clinical assessments (and oftenalso self-reported depression symptoms), and analyzedintention-to-treat populations, most often by usingLOCF (last-observation-carried-forward) data to replacemissing values. Depression outcomes were reported after8 to 12 weeks of SSRI treatment or 4 to 16 weeks ofpsychotherapy. No controlled data were available forlonger-term outcomes. The definition of treatment re-sponse differed among trials.
Across the 9 SSRI trials, response rates among treat-ment and placebo groups varied considerably. Of thepatients in treatment groups, 36% to 69% met responsecriteria at postintervention follow-up, compared with24% to 59% of patients in placebo-control groups. Wecalculated that the pooled absolute risk difference (RD)in the response rate between treatment and interventiongroups was 12% (95% confidence interval [CI]: 7–16;random-effects analysis) for the 9 SSRI trials, indicatinghigher response rates among those treated with SSRIs(Fig 2). When considering individual SSRIs, fluoxetineand citalopram both yielded statistically significanthigher response rates. Data from meta-analyses of effi-cacy among children and adolescents analyzed sepa-rately in a recent systematic review by Bridge et al26 in2007 suggested that overall, SSRIs were less effectiveamong children. When restricting the analysis to onlyfluoxetine trials, however, results were similar for both
TABLE 1 Depression Screening Instrument Accuracy Summary for Current MDD (KQ2)
Study No. CompletingScreen andDiagnosticInterview
Instrument Age, Rangeor Mean, y
Sensitivity,%
Specificity,%
PPV,%
NPV,%
USPSTFStudyQualitya
Primary care samplesJohnson et al41 (2002) 241c PHQ-A-positive 13–18 73 94 56 97 FairWinter et al42 (1999)b 100 BDI-PC � 4 12–17 91 91 55.6 98.8 Fair
Community samplesGoodman et al43 (2003) 7984 SDQ-positive 5–10 54 (p) NR NR NR Fair
11–15 33 (c) NR NR NR11–15 44 (p) NR NR NR11–15 63 (c and p) NR NR NR
School samplesCanals et al44–46 (2001, 1997, and 1995) 290 BDI � 11 17–18 90 86 20 99.5 Fair
BDI � 16 90 96 47 99.6Barrera and Garrison-Jones47 (1988)b 49 BDI � 11 12–17 100 77 NR NR Fair
BDI � 16 100 93 NR NRWhitaker et al4 (1990)b 356 BDI � 16 14–17 77 65 NR NR FairRoberts et al48 (1991)b 1704 BDI � 11 16.6 84 81 10 99.5 Fair
CES-D � 24 84 75 8 99Garrison et al49,50 (1991 and 1990)b 332 CES-D � 22 11–15 18 (male) 83 (male) 9 NR Fair
83 (female) 77 (female) 25 NRCES-D � 12 11–15 85 (male) 49 (male) 13 NR
84 (female) 38 (female) 11 NRPatton et al51 (1999) 170 CIS-R-positive 15.7 18 97 49 91 Fair
p indicates parent; c, child; NR, not reported; CES-DC, Center for Epidemiological Studies-Depression Scale for Children; CES-D, Center for Epidemiological Studies-Depression Scale; CIS-R,Revised Clinical Interview Schedule.a USPSTF quality criteria are described in Appendix 4.b Included in the 2002 USPSTF report.20c Four-hundred three patients completed screen and diagnostic interviews, but 162 patients were excluded because of a time lag between screen and interview.
PEDIATRICS Volume 123, Number 4, April 2009 e719. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

TABL
E2
Characteristicsof
RCTs
ofDep
ressionTreatm
entinCh
ildrenan
dAdo
lescen
ts(KQ4)
Reference
Interven
tion
Age
Rang
e,y
No.of
Patien
tsRa
ndom
lyAssigne
d
Leng
thof
Interven
tion
,wk
Respon
seCriteria
Respon
seRa
teRisk
Differen
ce,%
(95%
CI)orP
USPSTF
Qualitya
Treatm
entG
roup
ControlG
roup
SSRIs
Emslieetal
52,54(1997)
IG:fluo
xetin
e;CG
:placebo
7–17
968
CGI-I
�2
27/48(56%
)16/48(33%
)23
(4to
42)
Fair
Emslieetal
53,54(2002)
IG:fluo
xetin
e;CG
:placebo
8–17
219
9�30%decrease
inCD
RS-R
71/109
(65%
)54/101
(54%
)12
(�2to
25)
Fair
TADS5
5–58(2004)
IG1:fluoxetine;CG
:placebo
12–17
221
12CG
I-I�
266/109
(61%
)39/112
(35%
)26
(13to
39)
Good
Kelleretal59
(2001)
IG:paroxetine;CG
:placebo
12–18
180b
8HAM
-D�8or
�50%
redu
ctionfrom
baseline
60/90(67%
)48/87(55%
)12
(�3to
26)
Good
Berard
etal
60(2006)
IG:paroxetine;CG
:placebo
13–18
286
12�50%decrease
inMAD
RS107/177(61%
)53/91(58%
)2(�
10to
15)
Good
Emslieetal
61(2006)
IG:paroxetine;CG
:placebo
7–17
206
8CG
I-I�
249/101
(49%
)46/100
(46%
)3(�
11to
16)
Good
Wagneretal62
,63
(2003)c
IG:sertraline;CG
:placebo
6–17
376
10�40%decrease
inadjusted
CDRS-R
127/185(69%
)105/179(59%
)Good
Wagneretal64
(2004)
IG:citalopram
;CG:placebo
7–17
178
8CD
RS-Rscore
�28
32/89(36%
)20/85(24%
)12
(�1to
26)
Fair
Wagneretal65
(2006)
IG:escitalopram
;CG:placebo
6–17
268
8CG
I-I�
281/129
(63%
)69/132
(52%
)11
(�1to
22)
Good
Psycho
therapy
Interventio
nsClarke
66(1999)
IG1:grou
pCB
T;IG2:grou
pCB
T�
parent;CG:w
aitlist
14–18
123
8Nolong
ermeetin
gDSM
-III-R
criteria
for2
wkbasedon
LIFE
clinicalinterview
IG1:24/37(64.9%
);IG2:
22/32(68.8%
)13/27(48.1%
)�.05(IG
1andIG2
combinedvs
CG)
Good
Kahn
andKehle6
7
(1990)
IG1:grou
pCB
T;IG2:grou
prelaxatio
n;IG3:individu
alself-mod
eling;CG
:waitlist
10–14
686–8
Moved
from
dysfun
ctionaltofunctio
nal
BIDscore
IG1:13/17(76%
);IG2:11/17
(65%
);IG3:10/17(59%
)3/17
(18%
)NR
Fair
Lewinsohn
68(1990)
IG1:grou
pCB
T;IG2:grou
pCB
T�
parent;CG:w
aitlist
14–18
697
Nolong
ermeetin
gDSM
-III-R
criteria
basedon
K-SA
DS-E
IG1:42.9%;IG2:47.6%
5.3%
�.01(IG
1andIG2
combinedvs
CG)
Fair
Starketal
69(1987)
IG1:grou
pself-control;IG2:
grou
pbehavioralprob
lem
solving;CG
:waitlist
9–12
295
CDI�
13IG1:7/9(78%
);IG2:6/10
(60%
)1/9(11%
)NR
Fair
Rosello
70(1999)
IG1:individu
alIPT;IG2:
individu
alCB
T;CG
:waitlist
13–17
7112
CDI�
17IG1:82%;IG2:59%
NR
NR
Fair
Mufson7
1(1999)
IG1:individu
alIPT-A;CG
:clinicalmon
itorin
g12–18
4812
HRSD
�6CG
I-S75%;20/21
(95.5%
)46%;7/11(61.5%
).04;
�.001
Fair
Mufsonetal
72(2004)
IG1:individu
alIPT-A;CG
:treatm
entasu
sual
12–18
6416
HAM
D�
617/34(50%
)10/29(34%
)NR
Good
Diamon
detal
73
(2002)
IG1:attachment-based
family
therapy;CG
:waitlist
13–17
3212
Nolong
ermeetin
gcriteria
forM
DDon
K-SA
DS-P
13/16(81%
)7/15
(47%
).04
Good
Ackerson
74(1998)
IG1:cogn
itive
bibliotherapy;
CG:w
aitlist
14–18
304
NR
NR
NR
NA
Fair
TADS5
5–58(2004)
IG2:individu
alCB
T;CG
:placebo
�clinical
mon
itorin
g
12–17
223
12CG
Iimprovem
entscoreof1
or2
43.2%(95%
CI:34–52)
34.8%(95%
CI:26–44)
.20
Good
Psycho
therapyandSSRI
TADS5
5–58(2004)
IG3:individu
alCB
T�
fluoxetine;CG
:placebo
�clinicalmon
itorin
g
12–17
209
12CG
Iimprovem
entscoreof1
or2
71%(95%
CI:62–80)
34.8%(95%
CI:26–44)
Good
IGindicatesinterventiongrou
p;CG
,con
trolgrou
p;CG
I-I,ClinicalGlobalImpression
-Improvem
entScale;CDRS-R,Children’sD
epressionRatin
gScale-Revised;HAM
-D,Ham
ilton
Ratin
gScaleforD
epression;MAD
RS,M
ontgom
ery-AsbergDepressionRatin
gScale;DSM
-III-R
,Diagnostic
andStatisticalManualofM
entalD
isorders,Third
Edition,Revised;LIFE,Lon
gitudinalIntervalFollowup
Evaluatio
n;BID,BellevueIndexof
Depression;K-SA
DS-E,Kidd
ie-ScheduleforAffectiveDisordersandSchizoph
renia-
Epidem
iologicaleditio
n;HRSD,Ham
ilton
Ratin
gScaleforD
epression;CG
I-S,ClinicalGlobalImpression
-Severity
ofIllness;NR,no
treported;K-SA
DS-P,Kidd
ie-ScheduleforA
ffectiveDisordersandSchizoph
renia-PresentV
ersion
.aUSPSTFqu
ality
criteria
aredescrib
edinAp
pend
ix4.
bAn
additio
nal95patientsw
ererand
omlyassign
edto
imipraminetreatm
ent.
cTw
oseparateRC
Tswerepo
oled
bystud
yauthorsa
ndrepo
rted
in1pu
blication.
e720 WILLIAMS et al. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

children (RD: 21% [95% CI: 4–37]) and adolescents(RD: 20% [95% CI: 7–33]). These results were statisti-cally significant for both groups.
Nine of the 10 psychotherapy trials found that treatedpatients had higher short-term response rates or agreater reduction in depression symptoms after inter-ventions compared with a variety of control conditions.Two studies included children aged 9 or 10 years, andboth reported that mean clinician-rated depressionscores improved more among treated patients than con-trol group patients. No trials included children aged 7 or8 years.
One trial tested the effect of psychotherapy plus anSSRI (fluoxetine) compared with a placebo-control con-dition.55–58 Among adolescents treated with the combi-nation therapy, 71% (95% CI: 62–80) achieved re-sponse criteria compared with 34.8% (95% CI: 26–44)of placebo-control patients. This trial did not include anypatients younger than 12 years.
KQ5: What Are the Adverse Effects of Treatment?Data describing the adverse effects of SSRIs wereavailable from the 9 RCTs included for KQ4, for whichwe calculated pooled absolute RDs for suicide-relatedadverse events (SREs) using data for a subset of trialsincluded in the Bridge et al review.26 SREs includesuicidal ideation (ie, passive thoughts about wantingto be dead or active thoughts about killing oneself, notaccompanied by preparatory behavior), suicide at-tempts, or preparatory actions toward imminent sui-cidal behavior (eg, a person tries to hang himself orherself but is prevented from doing so by a familymember). Data were also available from 4 other meta-analyses that calculated the pooled relative risk (RR)or RD of SREs on the basis of outcomes assessed byusing blinded suicidology experts16,26,27 or includedother serious adverse events in addition to SREs.40 Inaddition, data from large retrospective cohort or case-control studies provided observational data describingrisk of suicidality, suicide death, and manic conver-
sion.75–78 Previous systematic reviews and meta-anal-yses did not exclude trials on the basis of qualitycriteria, and some did not report any quality-ratingprocedure or results. In contrast, we were able toreview published results from all currently completedtrials and analyze them in detail by using our typicalUSPSTF quality-rating criteria. We excluded 2 SSRItrials because of poor methodologic quality.79,80 Au-thors of previous reviews have also used varying in-clusion and exclusion criteria (eg, MDD trials only,SSRIs only) and have used both fixed-effects and ran-dom-effects approaches to meta-analyses, as well asBayesian methods of meta-analyses. The random-ef-fects and Bayesian approaches assume additionalsources of trial-related variation across studies andtypically produce RR estimates that are smaller inmagnitude and wider in CI. The FDA researchers usedfixed-effects methods, validated by results of hetero-geneity tests, to calculate the more conservative esti-mate. Meta-analyses also differed in terms of calculat-ing RR or RD. The FDA analysis focused on RR and,therefore, could not include data from 4 trials (non-SSRI MDD trials) that did not include serious adverse-event outcomes in either group.
Most conservative estimates from the FDA analysisindicate that treating any pediatric population withantidepressants for any indication doubles the RR of aSRE (RR: 1.95 [95% CI: 1.28 –2.98]).16 The absoluteRD between intervention and control populations inthat report was 1% (95% CI: 1–2). Published meta-analyses did not report the pooled RD among SSRItrials for treating pediatric MDD, considering datafrom all currently available completed trials (includinga recently published trial of escitalopram65). We cal-culated the pooled RD of those trials that were of atleast fair or good quality and found an absolute RD of1% (95% CI: 0 –2; Fig 3). In total, even the mostconservative estimates indicate that the risk of suicid-ality may increase absolutely by 1% or 2%. No suicidedeaths occurred in any of the trials.
Review : KQ4 SSRIsComparison: 01 SSRI vs placebo Outcome: 01 Response rate
RD (Random) t,hgieW RD (Random)Placebo tnemtaerT ydutSIC %59 % IC %59 n/N n/N bcategoryus ro
Emslie et al52,54 (1997) 27/48 16/48 5.66 0.23 [0.04 to 0.42]
Keller et al59 (2001) 60/90 48/87 9.57 0.11 [-0.03 to 0.26]
Emslie et al61 (2006) 49/101 46/100 10.13 0.03 [-0.11 to 0.16]
Wagner et al64 (2004) 32/89 20/85 10.57 0.12 [-0.01 to 0.26]
Emslie et al53,54 (2002) 71/109 54/101 10.87 0.12 [-0.02 to 0.25]
TADS55-58 (2004) 66/109 39/112 11.53 0.26 [0.13 to 0.38]
Berard et al60 (2006) 107/177 53/91 11.97 0.02 [-0.10 to 0.15]
Wagner et al65 (2006) 81/129 69/132 12.77 0.11 [-0.01 to 0.22]
Wagner et al62-63 (2003) 127/185 105/179 16.92 0.10 [0.00 to 0.20]
Total (95% CI) 1037 935 100.00 0.12 [0.07 to 0.16]
Total events: 620 (treatment), 450 (placebo)Test for heterogeneity: χ² = 10.05, df = 8 (P = .26), I² = 20.4%Test for overall effect: z = 4.63 (P < .00001)
-0.50 -0.25 0.00 0.25 0.50
Favors control Favors treatment
FIGURE 2Response to SSRIs to treat MDD in RCTs including children and adolescents (KQ4).
PEDIATRICS Volume 123, Number 4, April 2009 e721. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

Data from observational studies have provided con-flicting results regarding the relationship between an-tidepressant use and suicide attempts and death.75–77
An important limitation of observational studies is theinability to control for confounding by the indication.One additional cohort study found that antidepressantuse was associated with an increased risk of conver-sion from a unipolar depressive disorder to a bipolardisorder.78
The Treatment for Adolescents With DepressionStudy (TADS) was the only trial that reported adverseeffects of combined SSRI and psychotherapy treat-ment.55,56 The SRE rate among the cognitive behav-ioral therapy (CBT) plus fluoxetine group was 6%compared with 4% in the placebo-control group. Re-sults were not statistically different, but the study wasnot designed to have power to detect a difference ofthis magnitude.
Results for all KQs are summarized in Table 3.
DISCUSSIONWe found no studies that directly examined the healthoutcomes of screening children and adolescents for de-pression. Therefore, we cannot say whether the use ofsystematic screening improves identification, treatment,and outcomes of depression over standard identificationmethods. Although some screening instruments seem tohave better performance characteristics than others, it isdifficult to say the degree to which differences are causedby the quality of the instrument or the characteristics ofthe population or study. None of the instruments havebeen studied in large numbers of patients from a varietyof settings, including studies by investigators other thanthose who developed the questionnaires. Of primaryimportance to this review, 2 primary care studies re-ported sensitivities of 73% and 91% and specificities of91% and 94% in instruments developed for primarycare (the PHQ-A and BDI-PC). Both of these studiesexamined only adolescents, so no information wasfound that is directly applicable to younger children.
More data were reported in other settings using a varietyof instruments, some including younger children (al-though most were at least 10 years old). In these studies,sensitivities ranged from 18% to 100% and specificitiesranged from 38% to 97% and differed depending onwhat instrument, cutoff score, and informant source wasused. Data describing the accuracy of using depression-screening instruments in younger children remain verylimited. Only 1 study included children younger than 10and reported generally poor sensitivity and did not re-port specificity. We found no studies that examinedpotential harms of systematic, standardized screening fordepression in any setting. Theoretical harms are similarto those that have been discussed for suicide-screeningprograms.81 Until systematic depression screening istested in a controlled manner, however, actual harms topatients or costs to health care systems, relative to un-detected and untreated depression, cannot be measured.
The quantity of efficacy data from RCTs of interven-tions to treat pediatric MDD is also quite limited, partic-ularly when compared with the large body of evidencesupporting efficacy among adults. Despite this limitationin quantity, however, good-quality RCTs have been con-ducted to test SSRIs and psychotherapies among pediat-ric populations and provide evidence that efficaciousinterventions are available, although long-term effectsare not known. Meta-analyses have consistently foundthat fluoxetine is efficacious for treating pediatric popu-lations. Fluoxetine has been studied among both chil-dren and adolescents aged 7 to 17 years and is the onlydrug that is approved by the FDA for treating MDDamong youth. Available age-stratified meta-analysis re-sults indicate that fluoxetine is efficacious for both chil-dren and adolescents. The absolute RD is �20% for bothage groups, which would mean that �5 children oradolescents with MDD would need to be treated withfluoxetine for 1 to benefit. When combining data fromtrials of all SSRIs for treating MDD in youth, we foundthat patients treated with an SSRI were more likely toshow a response to treatment than patients treated with
Review : KQ5 SSRIsComparison: 01 SSRI vs placebo Outcome: 06 Suicid ideation or behavior rate
RD (Random) t,hgieW D (Random)R lortnoC tnemtaerT ydutSIC %59 % IC %59 n/N n/N bcategoryus ro
Emslie et al52,54 (1997) 2/48 2/48 2.62 0.00 [-0.08 to 0.08]
Emslie et al53,54 (2002) 6/109 6/110 4.56 0.00 [-0.06 to 0.06]
TADS55-58 (2004) 9/109 2/112 5.06 0.06 [0.01 to 0.12]
Keller et al59 (2001) 4/93 1/88 7.47 0.03 [-0.02 to 0.08]
Berard et al60 (2006) 6/180 2/95 10.60 0.01 [-0.03 to 0.05]
Wagner et al64 (2004) 1/93 2/85 10.90 -0.01 [-0.05 to 0.03]
Emslie et al61 (2006) 2/104 1/102 14.88 0.01 [-0.02 to 0.04]
Wagner et al62-63 (2003) 5/189 2/184 20.57 0.02 [-0.01 to 0.04]
Wagner et al65 (2006) 1/131 2/133 23.35 -0.01 [-0.03 to 0.02]
Total (95% CI) 1056 957 100.00 0.01 [0.00 to 0.02]
Total events: 36 (Treatment), 20 (Control)Test for heterogeneity: χ² = 8.40, df = 8 (P = .40), I² = 4.7%Test for overall effect: z = 1.27 (P = .20)
-0.50 -0.25 0.00 0.25 0.50
Treated: lower risk Treated: higher risk
FIGURE 3Suicidal ideation or behavior risk in children or adolescents treated with SSRIs for MDD (KQ5).
e722 WILLIAMS et al. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

TABL
E3
Summaryof
Eviden
ceQua
lityAccording
toKQ
KQNo.of
Stud
ies
Design
Limitations
Consistency
App
licab
ility
OverallQuality
Summaryof
Find
ings
1Non
e—
——
——
—1a
Non
e—
——
——
—2
9Screeningaccuracy
stud
ies
usingavalid
reference
standard
Youn
geragesp
oorly
represented,majority
ofstud
iesinscho
olsettings,few
instruments
exam
ined
in�1
stud
y
Fair
Fair;2stud
iescon
ducted
inprimarycaresettings,1
incommun
itysetting,6
inscho
olsettings
Fair
Twoinstrumentsdemon
stratedgo
odsensitivityand
specificityinprimarycaresettings
inadolescents;
only1stud
y(in
acommun
itysetting)includ
edchildren
�10
yofage,andthemajority
includ
edadolescents�
12y;thelargenu
mberof
instrumentsandheterogeneity
insamples
and
settings
makes
generalizationacrossstud
ies
difficultandmay
explainthewiderang
eof
performance
characteristicsreported(sensitivity
rang
edfrom
18%to
100%
andspecificityrang
edfrom
38%to
97%)
3Non
e—
——
——
—4
SSRIs
9RC
TsNolong
-termou
tcom
es;
trialsexclud
edpatientsw
ithmany
comorbiddisorders
Fair
Fair;primarily
cond
uctedin
research
orspecialty
settings
Good(3fair,6go
od)
SSRIusersh
adhigh
errespon
seratesthanthose
taking
placebomedication,with
anabsoluteRD
betweentreatm
entand
controlgroup
sof12%
(95%
CI:7–16);fluo
xetin
eandcitalopram
both
yieldedstatisticallysign
ificant
high
errespon
serates;datafrom
meta-analyses
ofefficacyam
ong
childrenandadolescentsa
nalyzedseparately
sugg
estedthatSSRIsw
erelesseffectiveam
ong
children
Psycho
therapy
10RC
TsNodataforages7
–8;
limiteddataforages
9–10;sho
rt-term
outcom
eson
ly
Good
Fair;on
ly2trialsin
commun
ityclinics
Fair(6fair,4go
od)
Mosto
fthe
psycho
therapytrialsfoun
dthattreated
patientsh
adhigh
errespon
serateso
rrem
ission
rateso
ragreaterreductio
nindepression
symptom
safterinterventio
nscomparedwith
avarietyofdiffe
rent
typeso
fcon
trolcond
ition
sSSRIandpsycho
therapy
combined
1RC
TSing
lestud
yNA
Good
Fair(1go
od-qualityRC
T)Co
mbinedfluoxetineandindividu
alCB
Tgrou
pshow
edarespon
serateof71%vs
35%inthose
taking
placeboandreceivingweeklyclinical
mon
itorin
g5
SSRIs
17RC
Ts,m
eta-analyses,
coho
rtstud
ies,case-
controlstudy
Inadequatepo
werto
assesssuicidality
Fair
Fair
Fair
Even
themostcon
servativeestim
ates
indicatethat
theriskofsuicidality
may
increase
absolutelyby
1%or2%
Psycho
therapy
Non
e—
——
——
—
PEDIATRICS Volume 123, Number 4, April 2009 e723. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

placebo pills. These pooled results, however, must beinterpreted with caution. Baseline response rates amongplacebo-treated patients were quite variable across thetrials, and some individual SSRIs do not seem to beefficacious. Furthermore, not all SSRIs have been eval-uated in pediatric clinical trials. One good-quality trialconducted in community clinics also evaluated com-bined therapy with fluoxetine plus individual CBT andfound that nearly 3 of 4 patients responded to combinedtherapy, in contrast with only 1 in 3 who responded inthe placebo group.55 These results indicate that 2 to 3adolescents would need to be treated with combinedCBT plus fluoxetine therapy for 1 adolescent to benefitfrom the therapy. Results of psychotherapy trials indi-cate that a variety of psychotherapy types are efficaciousamong adolescents, including group CBT and interper-sonal psychotherapy (IPT-A).
The most conservative estimates from the final resultsof the FDA analyses indicate that treating youth withantidepressants leads to a 2% absolute increase in risk ofexperiencing either suicidal ideation or behavior.16 Nosuicide deaths occurred during these trials. When dataare pooled for individual drugs, they have not yieldedstatistically significant increases in suicide-related out-comes. That lack of statistically significant effects, how-ever, may be a result of lack of power. For fluoxetine,6% (17 of 287) of treated patients and 4% (11 of 289) ofplacebo-control patients experienced either suicidal ide-ation or behavior during a trial, yielding an absolute RDof 2%. This result, however, was not statistically signif-icant.
On the basis of the estimate of increased absolute riskof 2%, for 1 patient to develop suicidality attributable toantidepressant therapy, �50 patients would need to betreated. Authors of several meta-analyses have arguedthat additional sources of heterogeneity must be incor-porated to more accurately assess the true risk of eitherefficacy or harms. The FDA analyses used fixed-effectsmodels to calculate RDs and risk ratios. In contrast,Bridge et al used a random-effects model that incorpo-rated additional sources of within and between meta-analysis trial heterogeneity. They found that the abso-lute RD was 1% and that the number needed to harmwas 112. In either case, available data indicate that apatient is more likely to benefit from treatment than todevelop suicidality. Nevertheless, suicidality is an ex-tremely serious condition and could translate, theoreti-cally, into an increased risk of suicide death (current trialdata are insufficient to address this issue). As a result, theoverall balance of risk and benefit of treatment withantidepressants is not yet clear.
Data are also currently insufficient to determine therole of combined treatment (SSRI plus psychotherapy)on SREs. The TADS was the only RCT included in thisreview that evaluated combined therapy.55 SREs wereless common among patients treated with combinedtherapy (fluoxetine and CBT; 5.6%), compared withfluoxetine alone (8.3%) but more common than amongpatients in the placebo-control group (3.6%) These dif-ferences, however, were not statistically significant. Thetrial was not powered sufficiently to detect differences of
these magnitudes. Therefore, it is uncertain whethercombined therapy would lead to a slight increase insuicidality compared with placebo if more data fromlarger numbers of patients were available. The additionalTADS safety results reported by Emslie et al56 in 2006indicate that the suicidality results vary depending onhow it is measured. Two recent comparative efficacytrials compared combined therapy with SSRI treatmentalone, and neither found statistically significant differ-ences between groups for suicidality measures.82,83 Thedecision to treat an individual pediatric patient with anantidepressant should be based on the clinical situationand guidelines from mental health specialists. Thus,careful consideration must be given to how closely apatient will be able to be monitored, either through theclinical setting or at home, after initiating a therapy.Harms of psychotherapy have not been systematicallyreported in trials in the past. Recently, Bridge et al84
highlighted the importance of assessing suicidality atbaseline and during follow-up assessments in trials ofpsychotherapy.
This review focuses on MDD and does not addressevidence to support screening or treatment for dysthy-mia, minor depression, or other psychiatric disorders inchildren and adolescents. Research addressing MDD inchildren and adolescents is less comprehensive than thatfor adults. Unlike the adult literature, no research hasdirectly evaluated the benefits of screening for depres-sion in children and adolescents in primary care. There isalso a more limited volume of research on screeninginstruments, on pharmacologic or psychotherapeutictreatments, and on community treatment patterns inchildren and adolescents, compared with research indepressed adults. Research is particularly limited onscreening instruments and treatments appropriate forchildren aged 10 years and younger.
There are many important areas that have not yetbeen studied. Future research in this area should in-clude:
● large-scale RCTs (or well-controlled clinical trials) ofprimary care or health care system depression-screen-ing programs documenting health outcomes, includ-ing harms, and rates of diagnosis and treatment initi-ation to guide clinicians in depression-screeningprograms for children and adolescents;
● descriptive epidemiologic studies describing the prev-alence of MDD (diagnosed and undiagnosed, treatedand untreated) in children and adolescents in primaryhealth care settings according to age, gender, and race/ethnicity;
● trials comparing depression treatment adherence andoutcomes (including benefits achieved and harmsavoided or increased) from depression collaborativecare management approaches compared with usualclinical care;
● analyses of predictors of treatment that may be rele-vant to the implementation and sustainability of in-terventions in primary care, such as patient treatment
e724 WILLIAMS et al. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

preference or level of provider training needed fordelivering effective interventions;
● comparative effectiveness of pharmacologic and non-pharmacologic treatments for MDD in children andadolescents, particularly those at high risk for suicid-ality or nonadherence to pharmacotherapy; and
● observational outcomes studies of risks for longer-term outcomes, including mania precipitation, withuse of antidepressants, particularly SSRIs.
CONCLUSIONSAlthough no trials of screening for pediatric MDD wereidentified, very limited available data suggest that pri-mary care–feasible screening tools have been reasonablyaccurate in identifying depressed adolescents. Studiesare needed to assess whether these findings can be rep-licated by other research groups in larger studies thatinclude patients from a variety of primary care settings.Data are also limited regarding treatment of MDDamong youth, but evidence from RCTs, including someeffectiveness trials, have indicated that available treat-ments are effective in improving depression outcomesamong adolescents. Thus, it is possible that screeningamong adolescents could lead to increased detection ofdepression, earlier detection of depression, and greateror earlier improvement in depression symptoms than ifpatients had never been screened.
Data describing screening among children are inade-quate. Effects of treatment among children also need tobe understood better, because data indicate that age is amodifier of treatment effects. Treatment of depressedyouth with SSRIs is associated with a small increased riskof suicidality and, therefore, should only be considered ifjudicious clinical monitoring is possible. Specific treat-ment should be based on individual patients’ needs andon mental health treatment guidelines.
ACKNOWLEDGMENTSPrepared by the Oregon Evidence-Based Practice Centerunder contract No. 290-02-0024, task order No. 1 fromthe AHRQ.
We are grateful for the feedback and guidance pro-vided by the experts who reviewed our full evidencereport: Amy Cheung, MD; Greg Clarke, PhD; Lisa Sharp,PhD; Karen Wagner, MD, PhD; Robin Weersing, PhD;and Craig Whittington, PhD. We also acknowledge theUSPSTF liaisons for guidance. We thank Daphne Plaut,MLS, Kevin Lutz, MFA, and Sarah Zuber, MSW, forassistance in the preparation of this article.
REFERENCES1. Jane Costello E, Erkanli A, Angold A. Is there an epidemic of
child or adolescent depression? J Child Psychol Psychiatry. 2006;47(12):1263–1271
2. Lewinsohn PM, Rohde P, Seeley JR. Major depressive disorderin older adolescents: prevalence, risk factors, and clinical im-plications. Clin Psychol Rev. 1998;18(7):765–794
3. Cheung A. Canadian community health survey: major depres-sive disorder and suicidality in adolescents. Healthc Policy. 2006;2(2):76–89
4. Whitaker A, Johnson J, Shaffer D, et al. Uncommon troubles inyoung people: prevalence estimates of selected psychiatric dis-orders in a nonreferred adolescent population. Arch Gen Psychi-atry. 1990;47(5):487–496
5. Shaffer D, Gould MS, Fisher P, et al. Psychiatric diagnosis inchild and adolescent suicide. Arch Gen Psychiatry. 1996;53(4):339–348
6. Weissman MM, Wolk S, Goldstein RB, et al. Depressed adoles-cents grown up. JAMA. 1999;281(18):1707–1713
7. Fergusson DM, Woodward LJ. Mental health, educational, andsocial role outcomes of adolescents with depression. Arch GenPsychiatry. 2002;59(3):225–231
8. Keenan-Miller D, Hammen CL, Brennan PA. Health outcomesrelated to early adolescent depression. J Adolesc Health. 2007;41(3):256–262
9. Kessler RC, Olfson M, Berglund PA. Patterns and predictors oftreatment contact after first onset of psychiatric disorders. Am JPsychiatry. 1998;155(1):62–69
10. Kessler RC, Walters EE. Epidemiology of DSM-III-R majordepression and minor depression among adolescents andyoung adults in the National Comorbidity Survey. Depress Anx-iety. 1998;7(1):3–14
11. Leaf PJ, Alegria M, Cohen P, et al. Mental health service use inthe community and schools: results from the four-communityMECA Study. Methods for the Epidemiology of Child andAdolescent Mental Disorders Study. J Am Acad Child AdolescPsychiatry. 1996;35(7):889–897
12. Sharp LK, Lipsky MS. Screening for depression across thelifespan: a review of measures for use in primary care settings.Am Fam Physician. 2002;66(6):1001–1008
13. Klein JD, Allan MJ, Elster AB, et al. Improving adolescentpreventive care in community health centers. Pediatrics. 2001;107(2):318–327
14. Halpern-Felsher BL, Ozer EM, Millstein SG, et al. Preventiveservices in a health maintenance organization: how well dopediatricians screen and educate adolescent patients? Arch Pe-diatr Adolesc Med. 2000;154(2):173–179
15. Pignone MP, Gaynes BN, Rushton JL, et al. Screening for Depres-sion. Rockville, MD: Agency for Healthcare Research andQuality; 2002. i-D-83
16. Hammad TA, Laughren T, Racoosin J. Suicidality in pediatricpatients treated with antidepressant drugs. Arch Gen Psychiatry.2006;63(3):332–339
17. DeBar LL, Clarke GN, O’Connor E, Nichols GA. Treated prev-alence, incidence, and pharmacotherapy of child and adoles-cent mood disorders in an HMO. Ment Health Serv Res. 2001;3(2):73–89
18. Ma J, Lee KV, Stafford RS. Depression treatment during out-patient visits by U.S. children and adolescents. J Adolesc Health.2005;37(6):434–442
19. Olfson M, Gameroff MJ, Marcus SC, Waslick BD. Outpatienttreatment of child and adolescent depression in the UnitedStates. Arch Gen Psychiatry. 2003;60(12):1236–1242
20. US Preventive Services Task Force. Screening for depression:recommendations and rationale. Ann Intern Med. 2002;136(10):760–764
21. Harris RP, Helfand M, Woolf SH, et al. Current methods of theUS Preventive Services Task Force: a review of the process.Am J Prev Med. 2001;20(3 suppl):21–35
22. National Institute for Health and Clinical Excellence. The Guide-lines Manual. London, United Kingdom: National Institute forHealth and Clinical Excellence; 2006
23. Stein RE, Zitner LE, Jensen PS. Interventions for adolescentdepression in primary care. Pediatrics. 2006;118(2):669–682
24. Zuckerbrot RA, Jensen PS. Improving recognition of adoles-cent depression in primary care. Arch Pediatr Adolesc Med. 2006;160(7):694–704
PEDIATRICS Volume 123, Number 4, April 2009 e725. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

25. Weisz JR, McCarty CA, Valeri SM. Effects of psychotherapy fordepression in children and adolescents: a meta-analysis. PsycholBull. 2006;132(1):132–149
26. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and riskfor reported suicidal ideation and suicide attempts in pediatricantidepressant treatment: a meta-analysis of randomized con-trolled trials. JAMA. 2007;297(15):1683–1696
27. Kaizar E, Greenhouse J, Seltman H, Kelleher K. Do antidepres-sants cause suicidality in children? A Bayesian meta-analysis.Clin Trials. 2006;3(2):73–90; discussion 91–98
28. Mosholder AD, Willy M. Suicidal adverse events in pediatricrandomized, controlled clinical trials of antidepressant drugsare associated with active drug treatment: a meta-analysis.J Child Adolesc Psychopharmacol. 2006;16(1–2):25–32
29. Mann JJ, Emslie G, Baldessarini RJ, et al. ACNP Task Forcereport on SSRIs and suicidal behavior in youth. Neuropsychop-harmacology. 2006;31(3):473–492
30. Medicines and Healthcare Products Regulatory Agency. Selectiveserotonin reuptake inhibitors (SSRIs): overview of regulatorystatus and CSM advice relating to major depressive disorder(MDD) in children and adolescents—summary of clinicaltrials. 2003. Available at: www.mhra.gov.uk/Safetyinformation/Safetywarningsalertsandrecalls/Safetywarningsandmessagesformedicines/CON019494. Accessed January 30, 2009
31. National Institute for Clinical Excellence. Depression in Childrenand Young People: Identification and Management in Primary, Com-munity and Secondary Care. Northhamptonshire, UnitedKingdom: British Psychological Society; 2005
32. Wohlfarth TD, van Zwieten BJ, Lekkerkerker FJ, et al. Anti-depressants use in children and adolescents and the risk ofsuicide. Eur Neuropsychopharmacol. 2006;16(2):79–83
33. March JS, Klee BJ, Kremer CM. Treatment benefit and the riskof suicidality in multicenter, randomized, controlled trials ofsertraline in children and adolescents. J Child Adolesc Psycho-pharmacol. 2006;16(1–2):91–102
34. Committee on Safety of Medicines. Report of the CSM ExpertWorking Group on the Safety of Selective Serotonin ReuptakeInhibitor Antidepressants. 2004. Available at: www.mhra.gov.uk/SafetyInformation/Safetywarningsalertsandrecalls/Safetywarningsandmessagesformedicines/CON1004259.Accessed Jan-uary 30, 2009
35. Dubicka B, Hadley S, Roberts C. Suicidal behaviour in youthswith depression treated with new-generation antidepressants:meta-analysis. Br J Psychiatry. 2006;189:393–398
36. Apter A, Lipschitz A, Fong R, et al. Evaluation of suicidalthoughts and behaviors in children and adolescents takingparoxetine. J Child Adolesc Psychopharmacol. 2006;16(1–2):77–90
37. Safer DJ, Zito JM. Treatment-emergent adverse events fromselective serotonin reuptake inhibitors by age group: Childrenversus adolescents. J Child Adolesc Psychopharmacol. 2006;16(1–2):159–169
38. Cheung AH, Emslie GJ, Mayes TL. Review of the efficacy andsafety of antidepressants in youth depression. J Child PsycholPsychiatry. 2005;46(7):735–754
39. Whittington CJ, Kendall T, Fonagy P, Cottrell D, Cotgrove A,Boddington E. Selective serotonin reuptake inhibitors in child-hood depression: systematic review of published versus un-published data. Lancet. 2004;363(9418):1341–1345
40. Wallace AE, Neily J, Weeks WB, Friedman MJ. A cumulativemeta-analysis of selective serotonin reuptake inhibitors in pe-diatric depression: did unpublished studies influence theefficacy/safety debate? J Child Adolesc Psychopharmacol. 2006;16(1–2):37–58
41. Johnson JG, Harris ES, Spitzer RL, Williams JB. The patienthealth questionnaire for adolescents: validation of an instru-
ment for the assessment of mental disorders among adolescentprimary care patients. J Adolesc Health. 2002;30(3):196–204
42. Winter LB, Steer RA, Jones-Hicks L, Beck AT. Screening formajor depression disorders in adolescent medical outpatientswith the Beck Depression Inventory for Primary Care. J AdolescHealth. 1999;24(6):389–394
43. Goodman R, Ford T, Simmons H, Gatward R, Meltzer H. Usingthe Strengths and Difficulties Questionnaire (SDQ) to screenfor child psychiatric disorders in a community sample. Int RevPsychiatry. 2003;15(1–2):166–172
44. Canals J, Blade J, Carbajo G, Domenech-Llaberia E. The BeckDepression Inventory: psychometric characteristics and useful-ness in nonclinical adolescents. Eur J Psychol Assess. 2001;17(1):63–68
45. Canals J, Domenech E, Carbajo G, Blade J. Prevalence ofDSM-III-R and ICD-10 psychiatric disorders in a Spanish pop-ulation of 18-year-olds. Acta Psychiatr Scand. 1997;96(4):287–294
46. Canals J, Marti-Henneberg C, Fernandez-Ballart J, DomenechE. A longitudinal study of depression in an urban Spanishpubertal population. Eur Child Adolesc Psychiatry. 1995;4(2):102–111
47. Barrera M Jr, Garrison-Jones CV. Properties of the Beck De-pression Inventory as a screening instrument for adolescentdepression. J Abnorm Child Psychol. 1988;16(3):263–273
48. Roberts RE, Lewinsohn PM, Seeley JR. Screening for adoles-cent depression: a comparison of depression scales. J Am AcadChild Adolesc Psychiatry. 1991;30(1):58–66
49. Garrison CZ, Addy CL, Jackson KL, McKeown RE, Waller JL.The CES-D as a screen for depression and other psychiatricdisorders in adolescents. J Am Acad Child Adolesc Psychiatry.1991;30(4):636–641
50. Garrison CZ, Jackson KL, Marsteller F, McKeown R, Addy C. Alongitudinal study of depressive symptomatology in youngadolescents. J Am Acad Child Adolesc Psychiatry. 1990;29(4):581–585
51. Patton GC, Coffey C, Posterino M, Carlin JB, Wolfe R, BowesG. A computerised screening instrument for adolescentdepression: population-based validation and application to atwo-phase case-control study. Soc Psychiatry Psychiatr Epidemiol.1999;34(3):166–172
52. Emslie GJ, Rush AJ, Weinberg WA, et al. A double-blind,randomized, placebo-controlled trial of fluoxetine in childrenand adolescents with depression. Arch Gen Psychiatry. 1997;54(11):1031–1037
53. Emslie GJ, Heiligenstein JH, Wagner KD, et al. Fluoxetine foracute treatment of depression in children and adolescents: aplacebo-controlled, randomized clinical trial. J Am Acad ChildAdolesc Psychiatry. 2002;41(10):1205–1215
54. Mayes TL, Tao R, Rintelmann JW, et al. Do children andadolescents have differential response rates in placebo-controlled trials of fluoxetine? CNS Spectr. 2007;12(2):147–154
55. March J, Silva S, Petrycki S, et al. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents withdepression: Treatment for Adolescents With Depression Study(TADS) randomized controlled trial. JAMA. 2004;292(7):807–820
56. Emslie G, Kratochvil C, Vitiello B, et al. Treatment for Adoles-cents With Depression Study (TADS): safety results. J Am AcadChild Adolesc Psychiatry. 2006;45(12):1440–1455
57. March JS, Silva S, Petrycki S, et al. The Treatment for Adoles-cents With Depression Study (TADS): long-term effectivenessand safety outcomes [published correction appears in Arch GenPsychiatry. 2008;65(1):101]. Arch Gen Psychiatry. 2007;64(10):1132–1143
58. Kennard B, Silva S, Vitiello B, et al. Remission and residualsymptoms after short-term treatment in the Treatment of Ad-
e726 WILLIAMS et al. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

olescents With Depression Study (TADS). J Am Acad ChildAdolesc Psychiatry. 2006;45(12):1404–1411
59. Keller MB, Ryan ND, Strober M, et al. Efficacy of paroxetine inthe treatment of adolescent major depression: a randomized,controlled trial. J Am Acad Child Adolesc Psychiatry. 2001;40(7):762–772
60. Berard R, Fong R, Carpenter DJ, Thomason C, Wilkinson C. Aninternational, multicenter, placebo-controlled trial of parox-etine in adolescents with major depressive disorder. J ChildAdolesc Psychopharmacol. 2006;16(1–2):59–75
61. Emslie GJ, Wagner KD, Kutcher S, et al. Paroxetine treatmentin children and adolescents with major depressive disorder: arandomized, multicenter, double-blind, placebo-controlledtrial. J Am Acad Child Adolesc Psychiatry. 2006;45(6):709–719
62. Wagner KD, Ambrosini P, Rynn M, et al. Efficacy of sertralinein the treatment of children and adolescents with major de-pressive disorder: two randomized controlled trials. JAMA.2003;290(8):1033–1041
63. Donnelly CL, Wagner KD, Rynn M, et al. Sertraline in childrenand adolescents with major depressive disorder. J Am AcadChild Adolesc Psychiatry. 2006;45(10):1162–1170
64. Wagner KD, Robb AS, Findling RL, Jin J, Gutierrez MM, Hey-dorn WE. A randomized, placebo-controlled trial of citalopramfor the treatment of major depression in children and adoles-cents. Am J Psychiatry. 2004;161(6):1079–1083
65. Wagner KD, Jonas J, Findling RL, Ventura D, Saikali K. Adouble-blind, randomized, placebo-controlled trial of escitalo-pram in the treatment of pediatric depression. J Am Acad ChildAdolesc Psychiatry. 2006;45(3):280–288
66. Clarke GN RP. Cognitive-behavioral treatment of adolescentdepression: efficacy of acute group treatment and booster ses-sions. J Am Acad Child Adolesc Psychiatry. 1999;38(3):272–279
67. Kahn J, Kehle T. Comparison of cognitive-behavioral, relax-ation, and self-modeling interventions for depression amongmiddle-school students. School Psychol Rev. 1990;19(2):196–211
68. Lewinsohn P. Cognitive-behavioral treatment for depressedadolescents. Behav Ther. 1990;21:385–401
69. Stark KD, Reynolds WM, Kaslow NJ. A comparison of therelative efficacy of self-control therapy and a behavioral prob-lem-solving therapy for depression in children. J Abnorm ChildPsychol. 1987;15(1):91–113
70. Rossello J. The efficacy of cognitive-behavioral and interper-sonal treatments for depression in Puerto Rican adolescents. JConsult Clin Psychol. 1999;67(5):734–745
71. Mufson L. Efficacy of interpersonal psychotherapy for de-pressed adolescents. Arch Gen Psychiatry. 1999;56(6):573–579
72. Mufson L, Dorta KP, Wickramaratne P, Nomura Y, Olfson M,Weissman MM. A randomized effectiveness trial of interper-sonal psychotherapy for depressed adolescents. Arch Gen Psy-chiatry. 2004;61(6):577–584
73. Diamond GS, Reis BF, Diamond GM, Siqueland L, Isaacs L.Attachment-based family therapy for depressed adolescents: atreatment development study. J Am Acad Child Adolesc Psychia-try. 2002;41(10):1190–1196
74. Ackerson J. Cognitive bibliotherapy for mild and moderateadolescent depressive symptomatology. J Consult Clin Psychol.1998;66(4):685–690
75. Valuck RJ, Libby AM, Sills MR, Giese AA, Allen RR. Antide-pressant treatment and risk of suicide attempt by adolescentswith major depressive disorder: a propensity-adjusted retro-spective cohort study. CNS Drugs. 2004;18(15):1119–1132
76. Søndergård L, Kvist K, Andersen PK, Kessing LV. Do antide-pressants precipitate youth suicide? A nationwide pharmaco-epidemiological study. Eur Child Adolesc Psychiatry. 2006;15(4):232–240
77. Olfson M, Marcus SC, Shaffer D. Antidepressant drug therapyand suicide in severely depressed children and adults: a case-control study. Arch Gen Psychiatry. 2006;63(8):865–872
78. Martin A, Young C, Leckman JF, Mukonoweshuro C, Rosen-heck R, Leslie D. Age effects on antidepressant-induced manicconversion. Arch Pediatr Adolesc Med. 2004;158:773–780
79. Simeon JG, Dinicola VF, Ferguson HB, Copping W. Adolescentdepression: a placebo-controlled fluoxetine treatment studyand follow-up. Prog Neuropsychopharmacol Biol Psychiatry. 1990;14(5):791–795
80. von Knorring AL, Olsson GI, Thomsen PH, Lemming OM,Hulten A. A randomized, double-blind, placebo-controlledstudy of citalopram in adolescents with major depressive dis-order. J Clin Psychopharmacol. 2006;26(3):311–315
81. Pena JB, Caine ED. Screening as an approach for adolescentsuicide prevention. Suicide Life Threat Behav. 2006;36(6):614–637
82. Goodyer I, Dubicka B, Wilkinson P, et al. Selective serotoninreuptake inhibitors (SSRIs) and routine specialist care with andwithout cognitive behaviour therapy in adolescents with majordepression: randomised controlled trial. BMJ. 2007;335(7611):142
83. Melvin GA, Tonge BJ, King NJ, Heyne D, Gordon MS, KlimkeitE. A comparison of cognitive-behavioral therapy, sertraline,and their combination for adolescent depression. J Am AcadChild Adolesc Psychiatry. 2006;45:1151–1161
84. Bridge JA, Barbe RP, Birmaher B, Kolko DJ, Brent DA. Emer-gent suicidality in a clinical psychotherapy trial for adolescentdepression. Am J Psychiatry. 2005;162(11):2173–2175
85. US Preventive Services Task Force. Screening for Suicide Risk:Recommendation and Rationale. Rockville, MD: Agency forHealthcare Research and Quality; 2004
86. Compton SN, March JS, Brent D, Albano AM, Weersing R,Curry J. Cognitive-behavioral psychotherapy for anxiety anddepressive disorders in children and adolescents: an evidence-based medicine review. J Am Acad Child Adolesc Psychiatry. 2004;43(8):930–959
87. Cuijpers P, van Straten A, Smits N, Smit F. Screening and earlypsychological intervention for depression in schools: system-atic review and meta-analysis. Eur Child Adolesc Psychiatry.2006;15(5):300–307
88. DerSimonian R, Laird N. Meta-analysis in clinical trials. ControlClin Trials. 1986;7(3):177–188
PEDIATRICS Volume 123, Number 4, April 2009 e727. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

APPENDIX 1 Search Strategies
Systematic reviews and meta-analysesDatabases: DARE, the CDSR, Medline, PsycINFO, 1998–2006
1. Search “depression” or “depressive disorder” or “depression,postpartum” or “depressive disorder, major” or “dysthymic disorder” or“seasonal affective disorder”; limits, all child: 0–18 years, English,publication date from 1998–2006
2. Search 1 and systematic.sb3. Search depression.ti.ab. or depressed.ti.ab. or depressive.ti.ab4. Search child.ti.ab or children.ti.ab. or adolescen*.ti.ab. or teen.ti.ab. orteens.ti.ab. or teenage*.ti.ab.
5. Search 3 and 46. Search 5 and (publisher.sb. or in process.sb.)7. Search 6 and systematic.sb.8. Search 6 and (meta-analysis.ti.ab. or medline.ti.ab. or systematic*.ti.ab.or search*.ti.ab.)
9. Search 7 or 810. Search 7 or 8 limits: English, Publication date from 1998–200611. Search 2 or 10
Screening outcomes, screening accuracy, and screening adverse effects (KQs1–3)
Databases: Medline, PsycINFO, Cochrane Central Register of Controlled Trials1998–2006
1. Depressive disorder/2. Depressive disorder, major/3. Depression/4. depress$.ti,ab.5. 1 or 2 or 3 or 46. Mass screening/7. screen$.ti,ab.8. case finding.ti,ab.9. casefinding.ti,ab.10. child$ depression inventory$.ti,ab.11. child$ depression scale$.ti,ab.12. child$ depression rating scale$.ti,ab.13. child$ self-report rating scale$.ti,ab.14. “mood and feelings questionnaire$”.ti,ab.15. reynold$ child$ depression.ti,ab.16. reynold$ adolesc$ depression.ti,ab.17. kutcher$ adolesc$.ti,ab.18. “depression scale for children$”.ti,ab.19. Beck Depression Inventory$.ti,ab.20. Center for Epidemiologic Studies Depression Scale$.ti,ab.21. 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19or 20
22. 5 and 2123. Limit 22 to (“child �6 to 12 years�” or “adolescent �13 to 18 years�”)24. children$.ti,ab.25. childhood.ti,ab.26. teen.ti,ab.27. teens.ti,ab.28. teenage$.ti,ab.29. pediatric$.ti,ab.30. paediatric$.ti,ab.31. adolescen$.ti,ab.32. boys.ti,ab.33. girls.ti,ab.34. youth.ti,ab.35. youths.ti,ab.36. child.ti,ab.37. 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 3638. 22 and 3739. 23 or 3840. Limit 39 to English language41. Limit 40 to year � “1998–2006”
APPENDIX 1 Continued
Treatment efficacy (KQ4)Databases: Medline, PsycINFO, Cochrane Central Register of Controlled TrialsSSRIs: 2004–2006; psychotherapy: 1998–20061. Depressive disorder/2. Depressive disorder, major/3. Depression/4. depress$.ti. or (depression or depressive or depressed).ab.5. 1 or 2 or 3 or 46. Antidepressive agents, second-generation/7. Serotonin uptake inhibitors/8. Antidepressive agents/9. antidepressant$.ti,ab.10. antidepressives.ti,ab.11. antidepressive agent$.ti,ab.12. antidepressive drug$.ti,ab.13. selective serotonin reuptake inhibitor$.ti,ab.14. ssri.ti,ab.15. ssris.ti,ab.16. Fluoxetine/17. fluoxetine.ti,ab.18. prozac.ti,ab.19. Fluvoxamine/20. fluvoxamine.ti,ab.21. luvox.ti,ab.22. Paroxetine/23. paroxetine.ti,ab.24. paxil.ti,ab.25. Sertraline/26. sertraline.ti,ab.27. zoloft.ti,ab.28. Citalopram/29. citalopram.ti,ab.30. celexa.ti,ab.31. escitalopram.ti,ab.32. lexapro.ti,ab.33. 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or32
34. Psychotherapy/35. Psychotherapy, brief/36. Psychotherapy, group/37. psychotherap$.ti,ab.38. Cognitive therapy/39. (cognitive adj (therap$ or treatment$ or intervention$)).ti,ab.40. Behavior therapy/41. (behavio$ adj (therap$ or treatment$ or intervention$)).ti,ab.42. interpersonal therap$.ti,ab.43. interpersonal intervention$.ti,ab.44. Self-help groups/45. self help.ti,ab.46. Family therapy/47. family support.ti,ab.48. parent$ education.ti,ab.49. Parents/ed �education�50. Counseling/51. Directive counseling/52. counsel$.ti,ab.53. Problem solving/54. problem solving.ti,ab.55. 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46or 47 or 48 or 49 or 50 or 51 or 52 or 53 or 54
56. 5 and 3357. Limit 56 to year � “2004–2006”58. 5 and 5559. Limit 58 to year � “1998–2006”
e728 WILLIAMS et al. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

APPENDIX 1 Continued
60. 57 or 5961. Limit 60 to (“child �6 to 12 years�” or “adolescent �13 to 18 years�”)62. children$.ti,ab.63. child.ti,ab.64. childhood.ti,ab.65. teen.ti,ab.66. teens.ti,ab.67. teenage$.ti,ab.68. pediatric$.ti,ab.69. paediatric$.ti,ab.70. adolescen$.ti,ab.71. boys.ti,ab.72. girls.ti,ab.73. youth.ti,ab.74. youths.ti,ab.75. 62 or 63 or 64 or 65 or 66 or 67 or 68 or 69 or 70 or 71 or 72 or 73 or 7476. 60 and 7577. 61 or 7678. Limit 77 to (clinical trial or controlled clinical trial or randomized,controlled trial)
79. Clinical trials/or controlled clinical trials/or randomized, controlledtrials/
80. Double-blind method/or random allocation/or single-blind method/81. random$.ti,ab.82. 79 or 80 or 8183. 77 and 8284. 78 or 8385. Limit 84 to English language86. Limit 85 to news87. 85 not 86
Treatment adverse effects (KQ5)Databases: Medline, PsycINFO, Cochrane Central Register of Controlled TrialsSSRIs: 2004–2006; Psychotherapy: 1990–20061. Depressive disorder/2. Depressive disorder, major/3. Depression/4. depress$.ti. or (depression or depressive or depressed).ab.5. 1 or 2 or 3 or 46. Antidepressive agents, second-generation/7. Serotonin uptake inhibitors/8. Antidepressive agents/9. antidepressant$.ti,ab.10. antidepressives.ti,ab.11. antidepressive agent$.ti,ab.12. antidepressive drug$.ti,ab.13. selective serotonin reuptake inhibitor$.ti,ab.14. ssri.ti,ab.15. ssris.ti,ab.16. Fluoxetine/17. fluoxetine.ti,ab.18. prozac.ti,ab.19. Fluvoxamine/20. fluvoxamine.ti,ab.21. luvox.ti,ab.22. Paroxetine/23. paroxetine.ti,ab.24. paxil.ti,ab.25. Sertraline/26. sertraline.ti,ab.27. zoloft.ti,ab.28. Citalopram/29. citalopram.ti,ab.30. celexa.ti,ab.31. escitalopram.ti,ab.32. lexapro.ti,ab.
APPENDIX 1 Continued
33. 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or32
34. 1 or 3 or 435. 33 and 3436. Limit 35 to year � “2004–2006”37. Psychotherapy/38. Psychotherapy, brief/39. Psychotherapy, group/40. psychotherap$.ti,ab.41. Cognitive therapy/42. (cognitive adj (therap$ or treatment$ or intervention$)).ti,ab.43. Behavior Therapy/44. (behavio$ adj (therap$ or treatment$ or intervention$)).ti,ab.45. interpersonal therap$.ti,ab.46. interpersonal intervention$.ti,ab.47. Self-help groups/48. self help.ti,ab.49. Family therapy/50. family support.ti,ab.51. parent$ education.ti,ab.52. Parents/ed �education�53. Counseling/54. Directive counseling/55. counsel$.ti,ab.56. Problem solving/57. problem solving.ti,ab.58. 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49or 50 or 51 or 52 or 53 or 54 or 55 or 56 or 57
59. 5 and 5860. Limit 59 to year � “1990–2006”61. 36 or 6062. Limit 61 to (“child (6 to 12 years)” or “adolescent (13 to 18 years)”)63. children$.ti,ab.64. child.ti,ab.65. childhood.ti,ab.66. teen.ti,ab.67. teens.ti,ab.68. teenage$.ti,ab.69. pediatric$.ti,ab.70. paediatric$.ti,ab.71. adolescen$.ti,ab.72. boys.ti,ab.73. girls.ti,ab.74. youth.ti,ab.75. youths.ti,ab.76. 63 or 64 or 65 or 66 or 67 or 68 or 69 or 70 or 71 or 72 or 73 or 74 or 7577. 61 and 7678. 62 or 7779. harm$.ti,ab.80. (adverse effects or chemically induced or drug effects or mortality orpoisoning or toxicity).fs.
81. adverse effect$.ti,ab.82. adverse event$.ti,ab.83. adverse reaction$.ti,ab.84. Adverse drug reaction reporting systems/85. Drug toxicity/86. Drug hypersensitivity/87. Death/88. death.ti,ab.89. death$.ti,ab.90. Suicide/91. Suicide, attempted/92. suicide.ti,ab.93. suicidal$.ti,ab.
PEDIATRICS Volume 123, Number 4, April 2009 e729. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

APPENDIX 1 Continued
94. mania.ti,ab.95. manic episode$.ti,ab.96. overdos$.ti,ab,mh.97. self damag$.ti,ab.98. self injur$.ti,ab.99. self injurious behavior/100. self inflict$.ti,ab.101. 79 or 80 or 81 or 82 or 83 or 84 or 85 or 86 or 87 or 88 or 89 or 90 or 91or 92 or 93 or 94 or 95 or 96 or 97 or 98 or 99 or 100
102. 78 and 101103. Antidepressive agents, second-generation/ae, po, to �adverse effects,poisoning, toxicity�
104. Serotonin uptake inhibitors/ae, po, to �adverse effects, poisoning,toxicity�
105. Fluoxetine/ae, po, to �adverse effects, poisoning, toxicity�106. Fluvoxamine/ae, po, to �adverse effects, poisoning, toxicity�107. Paroxetine/ae, po, to �adverse effects, poisoning, toxicity�108. Sertraline/ae, po, to �adverse effects, poisoning, toxicity�109. Citalopram/ae, po, to �adverse effects, poisoning, toxicity�110. 103 or 104 or 105 or 106 or 107 or 108 or 109111. Limit 110 to year � “2004–2006”112. Limit 111 to (“child �6 to 12 years�” or “adolescent �13 to 18 years�)”113. 111 and 76114. 112 or 113115. 102 or 114116. Limit 115 to English language117. Limit 116 to humans118. Limit 116 to animals119. 118 not 117120. 116 not 119121. Limit 120 to news122. 120 not 121
APPENDIX 2 DetailedMethods
Literature Search StrategyFor all KQs, we used existing systematic evidence reviews and meta-analyses
to the extent possible and supplemented with primary systematicliterature searches bridging the time period covered by the previousreview. Results are presented in a cumulative fashion, incorporating therelevant studies from the previous review. For all KQs, we initially searched forsystematic reviews,meta-analyses, and evidence-based guidelines ondepression screening, treatment, or associated harms in children andadolescents in the DARE, the CDSR,Medline, and PsycINFO from1998 throughMay 2006. Subsequent searches specific to each KQ supplemented evidencefound in the search of reviews andmeta-analyses. Two reviewersindependently examined all searches for relevance to all KQs.
For KQs 1 through 3 (addressing screening outcomes, accuracy, and harms),our preliminary search yielded no systematic reviews or meta-analysesthat met our inclusion criteria. Therefore, we conducted a primaryliterature search for depression screening in children and adolescents inprimary care to cover the time period since the previous USPSTF review(1998 through May 2007) in Medline, PsycINFO, and the CochraneCollaboration Registry of Clinical Trials (CCRCT) without restrictions onstudy designs. Search terms are listed in Appendix 1.
For KQ4, the preliminary search yielded 1 systematic review38 and 1 meta-analysis40 of SSRI treatment efficacy and adverse effects in children andadolescents that covered the years through 2004. We used these reviewsas source documents and bridged their searches for SSRI treatment andharms. Therefore, for KQ4, we searched for RCTs/controlled clinical trials ofpsychotherapy and SSRI treatment in children and adolescents in Medline,PsycINFO, and the CCRCT in 2 separate searches covering 1998 throughMay 2007 for psychotherapy and 2004 through May 2007 for SSRIs.
For KQ5, we searched for adverse effects of SSRIs and psychotherapeutictreatment, without restrictions on study designs, in 2 separate searches
APPENDIX 2 Continued
covering 1990 through May 2007 for psychotherapy and 2004 throughMay 2007 for SSRIs. Our search period for adverse effects of psychotherapybegan in 1990, because harms of treatment were not addressed in theprevious USPSTF report.
Articles were also obtained from outside experts and through reviewingbibliographies of other relevant articles and systematic reviews. Inaddition to these searches for published trials, the following sources weresearched for unpublished trials of SSRIs: Robert Wood JohnsonFoundation; Computer Retrieval of Information on Scientific Projects;NARSAD: The Mental Health Research Association;ClinicalStudyResults.org; Current Controlled Trials; GlaxoSmithKlineClinical Trial Register; ClinicalTrials.gov; Eli Lilly and Company Clinical TrialRegistry; Australian Clinical Trials Registry; NovartisClinicalTrials.com;Bristol-Myers Squibb Clinical Trial Registry; International Federation ofPharmaceutical Manufacturers and Associations Clinical Trials Portal;Drugs@FDA; European Medicines Agency; and Education ResourcesInformation Center.
Inclusion and Exclusion CriteriaWe developed the following set of inclusion/exclusion criteria that wereapplied to the KQs. Additional exclusion criteria are specified in Appendix 3.
PopulationsThis review addresses children and adolescents aged 7 to 18 years of age inthe United States and other similarly developed Westernized populations(defined as being at a human development index of �0.90). Currentlyavailable screening tools are reported to be appropriate for children aged7 years and older.12 Furthermore, the prevalence of depression amongchildren younger than 6 years is estimated to be less than 1%; thus, thepredictive value of a positive test is likely to be low.
PopulationsWith Risk FactorsWe addressed the prevalence of depression among populations with riskfactors through a contextual question and also captured studies thatevaluated screening and treatment among populations with riskfactors. We examined studies conducted among populations with thefollowing clinically relevant risk factors recommended by experts whoreviewed the work plan for this review: children of depressed parents,previous personal history of a major depressive episode, chronicmedical conditions with high prevalence among primary carepopulations (eg, asthma), substance abuse, and acute negative lifeevents. After reviewing the evidence for depression screening andtreatment in populations with risk factors, the USPSTF decided that thereview should not address screening and treatment in high-riskpopulations separately because of the lack of relevant studies. In ourdiscussion of this review, however, we did consider this evidence inrelation to our findings’ applicability to these high-risk populations. Wedid not examine primary epidemiologic studies that identified riskfactors for childhood depression. We excluded studies that focused onpatients with bipolar disorder or with psychotic disorders, includingpsychotic depression, as well as patients with severe medicalconditions (eg, cancer) that may have interfered with the performanceof screening tools or treatment or were not generally represented inprimary care populations. We also excluded studies that focused onidentifying parental depression, including postpartum maternaldepression.
DiseasesThis report includes studies that focused on MDD or depression nototherwise specified, as defined by Diagnostic and Statistical Manual ofMental Disorders, Fourth Edition criteria. We also included studies that useda predetermined cutoff on a screening test to define major depression. Wedid not address screening or treatment of dysthymia or minor depressionor prevention of depression. We did not address screening specifically forsuicide prevention, which has been addressed by a separate USPSTFrecommendation.12
e730 WILLIAMS et al. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

APPENDIX 2 Continued
SettingsWe included studies conducted in primary care or in school-based clinics. In
addition, we included studies conducted in non–clinic-based settings (eg,church or after-school programs) if they were conducted in populationsthat were comparable to primary care patients. For KQs 4 and 5, whichevaluate treatment efficacy and adverse effects, we included trials thatwere conducted in outpatient mental health clinic settings, but thesesettings were excluded for KQs 1 through 3. This report does not addressdepression screening or treatment in incarcerated populations, drugtreatment programs, inpatient settings, or residential settings.
Screening InterventionsThis review includes only studies of screening instruments that are feasiblefor primary care settings. Specifically, a screening tool should take nolonger than 15 minutes to complete if delivered before clinician andpatient face-to-face contact (eg, in the waiting room or in the examinationroom before clinician entrance) and no longer than 5 minutes or 5questions if used during the face-to-face visit. More general mental healthscreening tools were included if they had a depression module or werebeing used to identify depressive illness and related outcomes.
Treatment InterventionsWe included studies of pharmacologic interventions that evaluated SSRIs:fluoxetine, fluvoxamine, paroxetine, sertraline, citalopram, andescitalopram. We excluded studies of tricyclic antidepressants (which werefound to be ineffective among children and adolescents in the previousreview), monoamine oxidase inhibitors (MAOIs), and electroconvulsivetherapy or other interventions that are not primary care–feasible orreferable. We also excluded atypical antidepressants, because they are notcurrently approved by the FDA for treating depression among children oradolescents and are not expected to be approved in the near future. Thisreport includes studies that evaluated the following types ofpsychotherapeutic interventions: CBT, IPT, pure or guided self-help, familysupport, and parental education. The scope of this review does not includehealth systems approaches to depression treatment such as collaborativecare interventions; however, we considered these areas in the discussionof our findings.
OutcomesWe included the following outcomes if they were reported at 6 weeks’follow-up time or later. The primary health outcomes of interest wereremission from depression, improved depressive symptoms, andrecurrence of depression. Additional outcomes of interest included qualityof life, global functioning, psychosocial functioning, educationalachievement, unplanned pregnancy, substance abuse, improvement incomorbid disorders, change in health status, and reduction in physicalcomplaints. For harms, we focused on death, other serious psychiatricevents (such as hospitalization, suicidal ideation, and suicide attempts),triggering symptoms of mania, and discontinuation of medicationresulting from adverse events.
Study DesignsFor KQs 1 and 4, which address outcomes of screening and treatment, weincluded RCTs, controlled clinical trials, systematic reviews, and meta-analyses. We excluded noncomparative study designs and comparativeeffectiveness studies. For psychotherapy trials, we included studies withno treatment, placebo pill, or wait-list control groups. We also acceptedclinical monitoring as a control group if there was significantly lessinteraction time compared with the intervention arm(s) and it wasrestricted to nontherapeutic content. Nondirective supportivepsychotherapy was considered to be a treatment group unless it wasdescribed as being significantly less intense (in total minutes of contact)than that in the intervention arm(s).
For KQ 2, addressing the accuracy of screening, we included studies ofdiagnostic accuracy that reported sensitivity and specificity compared withan independently assessed criterion standard for MDD or depression not
APPENDIX 2 Continued
otherwise specified within 2 months of the screening test. For KQs 3 and 5,evaluating the harms of screening and treatment, we used evidence fromRCTs preferentially, then well-designed non-RCTs and high-qualityobservational studies with sample sizes of at least 1000.
QualityWe excluded studies that met criteria for “poor” quality in the USPSTF design-specific criteria (Appendix 4).
LanguageWe excluded non–English-language abstracts and articles.
Article Review and Data AbstractionWe reviewed a total of 4979 abstracts and 444 complete articles for all KQs(Appendix 5). Although we conducted 3 searches to cover depressionscreening, depression treatment efficacy, and depression treatmentharms, we reviewed all abstracts for potential inclusion for any of the KQs.Two investigators independently reviewed all abstracts for KQs 4 and 5.The search for KQs 1 through 3 produced a very high yield (3418 abstracts).Therefore, we used a modified approach to reviewing these abstracts. Oneinvestigator reviewed all the abstracts for KQs 1 through 3. A secondinvestigator independently reviewed all abstracts from the CCRCT search,the 500 most recently published abstracts from both Medline andPsycINFO, and every fifth abstract in the remaining set for Medline andPsycINFO, representing an additional random subset of 20% that weredually reviewed. Therefore, 1562 (46%) of the 3418 screening abstractswere dually reviewed for inclusion or exclusion. There were a total of 22(1.4%) discrepancies between the 2 reviewers for the 1562 dual-reviewedabstracts. None of these 22 abstracts were included in the final review;therefore, we feel confident that no relevant articles were missed byhaving a second investigator dual review only a subset of the abstracts.
Two investigators independently reviewedarticlesagainst inclusion/exclusioncriteriaspecific foreachKQandmarkedarticles forexclusionas soonasanexclusioncriterionwasmet. Includedstudies thatmetall criteriawere then independentlyrated forqualityby2 investigatorsbyusing theUSPSTF’s studydesign-specificcriteria supplementedbyNational Institute forHealthandClinical Excellencecriteria forqualityassessment22 (Appendix4). TheMethodsWorkGroupof theUSPSTFhasdefineda3-category ratingof “good,” “fair,” and“poor”onthebasisofthesecriteria. Ingeneral, agoodstudymeetsall criteriawell.A fair studydoesnotmeet,or it isnotclear that itmeets, at least1criterion,buthasnoknown importantlimitation thatcould invalidate its results.Apoor studyhas important limitations.Articleswere ratedasgood, fair, orpoorbyeach rater, anddisagreementsweresettledbyconsensus. Studies that receivedapoorfinalquality ratingwereexcluded fromthe review.Listingsofexcludedarticles foreachKQ,alongwith thereason forexclusion, are in the full evidence reportwhich isavailableatwww.preventiveservices.ahrq.gov (AppendixC,TablesC1,C3,C4,C6, andC9).Allexclusioncriteriaare listed inAppendix3.
We identifiednumerous recent systematicevidence reviews thatexaminedtheefficacyofSSRIs for treatingMDDinyouthand includedbothpublishedandunpublishedresults.26,31,38–40We includedresults fromthemost recentlypublishedgood-quality systematicevidence reviewofantidepressantefficacybyBridgeetal.26Numeroussystematicevidence reviewsandmeta-analysesevaluating theefficacyofpsychotherapy for treatingdepression inyouthhavealsobeenpublishedrecently. These reviewsonlypartiallyoverlappedwithour inclusionandexclusioncriteriaandcouldnotdirectlyanswer thescopeofourKQs.Therefore,weusedthe5most recentlypublishedsystematicevidence reviewsas supplementalsources for identifying trials relevant for this report.23,25,31,86,87 Numerous recentsystematic evidence reviewsand regulatoryagency reports have alsosynthesized available data fromRCTs to estimatewhether excess risk ofsuicide-related events (SRE) occurs among depressed children or adolescentstreatedwith SSRIs or atypical antidepressants.16,26–40 For this report, weincluded themost recently published reviews that used suicide-relatedoutcome SRE data thatwere blindly classified by suicidology experts atColumbia University (requested by the FDADivision of NeuropharmacologicalDrug Products).16,26,27 (Only 1 of these reports incorporated a recentlypublished trial of escitalopram.26)
PEDIATRICS Volume 123, Number 4, April 2009 e731. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

APPENDIX 2 Continued
There are 4 systematic reviews/meta-analyses and 31 studies (reported in 39articles) included in this review. We found no studies for KQs 1, 1a, and 3.For KQ2, we found 9 studies reported in 12 articles, 5 of which wereincluded in the previous USPSTF report. KQ4 includes 1 systematic reviewand 18 trials reported in 22 articles, 3 of which were included in theprevious USPSTF report, and KQ5 includes 4 meta-analyses and 13 trialsreported in 17 articles, none of which were included in the previousUSPSTF report because harms were not addressed. One primary reviewerabstracted relevant information such as study setting, population,screening method, and outcomes into standardized evidence tables foreach included article. A second reviewer checked the abstracted data foraccuracy and completeness. These tables are in Appendix C, Tables C2,C5, C7 and C8, of the full evidence report (available at www.preventiveservices.ahrq.gov).
Data SynthesisWe found no data for KQs 1, 1a, and 3. Data synthesis for KQ2 was qualitative,because heterogeneity in the instruments, samples, and settings studieddid not allow for quantitative syntheses. For psychotherapy trials includedin KQs 4 and 5, we did not conduct meta-analyses because of theheterogeneity of the interventions. Instead, we qualitatively summarizedour findings in the results text and summary tables. For evidence on theefficacy and adverse effects of SSRIs (KQ4 and 5), binary outcome data forresponse rate and SREs were pooled across the trials that met our inclusionand exclusion criteria. We used a recent good-quality systematic review(Bridge et al26) as a source of outcome data for response rate and SRE.Bridge et al used SRE data that were based on the blinded review ofoutcomes by suicidology experts from Columbia University (the same dataused in analyses by the FDA). For newer trials, the authors usedmethodology similar to that in the Columbia University review. We quality-rated all individual trials and compared all data for response outcomesagainst outcomes reported in published versions of individual trials.This review revealed no discrepancies. We could not analyze the datafor SRE, because the FDA provided these outcomes to Bridge et al.Heterogeneity tests were performed on outcome results. Authors ofprevious meta-analyses of these data argued that fixed-effect modelsare not appropriate for this body of literature.26,27 Commentators onthese previous meta-analyses, however, have argued that using thisapproach is appropriate for adverse-event outcomes because the trialsare already biased toward finding null effects resulting from lack ofsystematic measurement of adverse events, underreporting outcomes,and measurement error.
We agree with the assessment by Bridge et al that these trials are likely tohave heterogeneity across studies not accounted for by observedcovariates. We used a random-effects model (method of DerSimonian andLaird88) to calculate the pooled RD. Random-effects approaches generallyyield lower risk estimates and wider CIs (yielding more-conservativeestimates of efficacy and less-conservative estimates of adverse events). Toincorporate more conservative estimates of adverse events into thereview, we included results frommeta-analyses using fixed-effects models.We conducted sensitivity analyses recalculating pooled RDs by using afixed-effects model to understand how this difference in approach wouldaffect results. We focused on the RD, instead of RR, because the data aremore directly applicable to comparing risks and benefits (ie, calculatingand comparing numbers needed to treat or harm). All meta-analyses wereconducted by using RevMan 4.2 software (Cochrane Collaboration.Available at www.cc-ims.net/RevMan.).
External Review ProcessThe USPSTF appointed 3 liaisons to guide the scope and reporting of thisreview. The work plan for the review was sent to 5 experts on childhoodmental health, whomwe asked to comment on the general proposedapproach, scope of the review, and adequacy of the identified questions.In addition, 5 outside experts provided feedback on a draft version of thisevidence synthesis.
APPENDIX 3 Exclusion Criteria for KQsExclusion criteria applied to all KQsPopulationFocuses on adults (�18 y old) or children aged 0–6 or does not report
pediatric outcomes separatelyFocuses on patients with severe medical illnesses (eg, cancer), bipolar
disorder, or psychotic disorderFocuses on identifying or treating maternal depression (eg, during
pregnancy or after delivery)Focuses on identifying or treating parental depressionConducted in population that is not comparable to primary care (eg, high-
risk conditions not prevalent in primary care populations)Focuses on patients with minor depression or dysthymia or does not present
MDD outcomes separatelyConducted exclusively in high-risk populationsConducted in non-Westernized population
SettingNot conducted in primary care, school-based clinics, or other setting with
primary care–comparable population (ie, church or after-schoolprogram)
Conducted with inpatients or those in residential treatment or drugtreatment programs
Conducted with incarcerated populationsDesignEditorialsLettersNoncomparative studiesNonsystematic reviewsOpinionsComparative effectiveness studiesAbstracts
QualityDoes not meet quality criteriaNo relevant outcomesPrecedes search periodArticle covered by an included systematic reviewSystematic review used as source document onlyNon-English
Additional exclusion criteria specific to each KQKQ1: Does screening for depression among children and adolescents in the
primary care setting improve health outcomes?RelevanceDoes not focus on screening and treatment of depressionReports on test that is not relevant to or feasible in primary care settingFocuses on screening for suicide risk
SettingConducted in outpatient mental health clinic
QualityOnly short-term health outcomes �6 wk are reported
KQ2: Are depression screening instruments for children and adolescents accurate inidentifying depression in primary care or school-based clinics?
RelevanceDoes not focus on depression screeningDoes not use a credible reference standard or reports on test that is notrelevant to or feasible in primary care setting
Focuses on screening for suicide riskSettingConducted in outpatient mental health clinic
APPENDIX 2 Continued
USPSTF InvolvementThis research was funded by the AHRQ under a contract to support thework of the USPSTF. The authors worked with 3 USPSTF liaisons at keypoints throughout the review process to develop and refine the scope,analytic framework, and KQs; to resolve issues around the reviewprocess; and to finalize the evidence synthesis. The AHRQ had no rolein study selection, quality assessment, or synthesis, although AHRQstaff provided project oversight, reviewed the draft evidence synthesis,and distributed the initial evidence report for external review ofcontent by outside experts, including representatives of professionalsocieties and federal agencies. The final published systematic evidencereview was revised on the basis of comments from these externalreviewers.
e732 WILLIAMS et al. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

APPENDIX 3 ContinuedDesignDoes not report sensitivity and specificity compared with an
independently assessed criterion standard for MDD or depression nototherwise specified within 2 mo of the screening test
KQ3: What are the harms of screening?RelevanceDoes not focus on harms of depression screeningFocuses on screening for suicide risk
SettingConducted in outpatient mental health clinic
KQ4: Does the treatment of depression (SSRIs and/or psychotherapy) amongscreen-detected children and adolescents identified in primary care orcomparable populations improve health outcomes?
RelevanceDoes not focus on depression treatmentFocuses on efficacy of tricyclic antidepressants, atypical antidepressants,
MAOIs, electroconvulsive therapy, or other medications/proceduresthat are not primary care–feasible or referable
Focuses on treatment comparison, matching, or fine-tuningExamination of nondemographic modifiers (eg, genetics, personality
characteristics)Focuses on prevention of depression (either universal or among
populations with risk factors)Focuses on health systems approach to depression treatment such as
collaborative care interventions
APPENDIX 4 Quality Rating Criteria
Design USPSTF Quality Rating Criteriaa National Institute for Health and ClinicalExcellence Methodology Checklistsb
Systematic reviews andmeta-analyses
Comprehensiveness of sources considered/search strategy used The study addresses an appropriate and clearlyfocused question
Standard appraisal of included studies A description of the methodology used is includedValidity of conclusions The literature search is sufficiently rigorous to
identify all the relevant studiesRecency and relevance are especially important for systematic reviews Study quality is assessed and taken into account
There are enough similarities between the studiesselected to make combining them reasonable
Case-control studies Accurate ascertainment of cases The study addresses an appropriate and clearlyfocused question
Nonbiased selection of cases/controls with exclusion criteria appliedequally to both
The cases and controls are taken from comparablepopulations
Response rate The same exclusion criteria are used for both casesand controls
Diagnostic testing procedures applied equally to each group What percentage of each group (cases andcontrols) participated in the study?
Measurement of exposure accurate and applied equally to each group Comparison is made between participants andnonparticipants to establish their similarities ordifferences
Appropriate attention to potential confounding variables Cases are clearly defined and differentiated fromcontrols
Is it clearly established that controls are noncases?Measures have been taken to prevent knowledgeof primary exposure influencing caseascertainment
Exposure status is measured in a standard, valid,and reliable way
The main potential confounders are identified andtaken into account in the design and analysis
Have CIs been provided?
APPENDIX 3 ContinuedSettingIntervention not primary care–feasible or widely available for primary care
referralDesignControl group is not significantly less interaction time compared with
intervention arm or has therapeutic content, including nondirectivesupportive therapy
QualityOnly short-term health outcomes �6 wk are reported
KQ5: What are the adverse effects of treatment?RelevanceDoes not focus on harms of depression treatmentFocuses on harms of tricyclic antidepressants, atypical antidepressants,
MAOIs, electroconvulsive therapy, or other medications/proceduresthat are not primary care–feasible or referable
Focuses on treatment comparison, matching, or fine-tuningExamination of nondemographic modifiers (eg, genetics, personality
characteristics)Focuses on harms of prevention of depression (either universal or among
populations with risk factors)SettingFocuses on harms of intervention that is not primary care–feasible or
widely available for primary care referralDesignHigh-quality observational study with a sample size of �1000
PEDIATRICS Volume 123, Number 4, April 2009 e733. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

APPENDIX 4 Continued
Design USPSTF Quality Rating Criteriaa National Institute for Health and ClinicalExcellence Methodology Checklistsb
All relevant outcomes are measured in a standard,valid, and reliable way
What percentage of the individuals or clustersrecruited into each treatment arm of the studydropped out before the study was completed?
All the subjects are analyzed in the groups towhich they were randomly allocated (oftenreferred to as intention-to-treat analysis)
When the study is carried out at �1 site, resultsare comparable for all sites
Cohort studies Initial assembly of comparable groups uses consideration of potentialconfounders with either restriction or measurement for adjustmentin the analysis; consideration of inception cohorts
The study addresses an appropriate and clearlyfocused question
Maintenance of comparable groups (includes attrition, crossovers,adherence, contamination)
The 2 groups being studied are selected fromsource populations that are comparable in allrespects other than the factor underinvestigation
Important differential loss to follow-up or overall high loss to follow-up The study indicates howmany of the people askedto take part did so, in each of the groups beingstudied
Measurements: equal, reliable, and valid (includes masking of outcomeassessment)
The likelihood that some eligible subjects mighthave the outcome at the time of enrollment isassessed and taken into account in the analysis
Clear definition of the interventions What percentage of individuals or clustersrecruited into each arm of the study droppedout before the study was completed?
All important outcomes considered Comparison is made between full participants andthose lost to follow-up, according to exposurestatus
The outcomes are clearly definedThe assessment of outcome is made blind toexposure status
When blinding was not possible, there is somerecognition that knowledge of exposure statuscould have influenced the assessment ofoutcome
The measure of assessment of exposure is reliableEvidence from other sources is used todemonstrate that the method of outcomeassessment is valid and reliable
Exposure level or prognostic factor is assessedmore than once
The main potential confounders are identified andtaken into account in the design and analysis
Have CIs been provided?Diagnostic accuracystudies
Screening test relevant, available for primary care, adequatelydescribed
The nature of the test being studied is clearlyspecified
Study uses a credible reference standard, performed regardless of testresults
The test is compared with an appropriate goldstandard
Reference standard interpreted independently of screening test When no gold standard exists, a validatedreference standard is used as a comparator
Handles indeterminate result in a reasonable manner Patients for testing are selected either as aconsecutive series or randomly from a clearlydefined study population
Spectrum of patients included in study The test and gold standard are measuredindependently (blind) of each other
Sample size The test and gold standard are applied as closetogether in time as possible
Administration of reliable screening test Results are reported for all patients who areentered into the study
e734 WILLIAMS et al. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

APPENDIX 5 Search Results and Article Flow
Articles reviewed for KQ1 n = 19
Articles reviewed for KQ4 n = 244
Articles excluded for KQ4 n = 221
Articles excluded for KQ1 n = 19
Articles included for KQ1 n = 0
Articles included for KQ4 n = 23
(18 studies + 1 systematic evidence
review)
Articles reviewed for KQ5 n = 162
Articles excluded for KQ5 n = 141
Articles included for KQ5 n = 21
(13 studies + 4 meta-analyses)
Abstracts reviewed
N = 4979
Total articles reviewed
n = 444
Articles reviewed for KQ3 n = 9
Articles excluded for KQ3 n = 9
Articles included for KQ3 n = 0
Articles reviewed for KQ2 n = 95
Articles excluded for KQ2 n = 83
Articles included for KQ2 n = 12
(9 studies)
Articles reviewed from outside sources
n = 96
APPENDIX 4 Continued
Design USPSTF Quality Rating Criteriaa National Institute for Health and ClinicalExcellence Methodology Checklistsb
RCTs Initial assembly of comparable groups uses adequate randomization,including first concealment and whether potential confounders weredistributed equally among groups
The study addresses an appropriate and clearlyfocused question
Maintenance of comparable groups (includes attrition, crossovers,adherence, contamination)
The assignment of subjects to treatment groups israndomized
Important differential loss to follow-up or overall high loss to follow-up An adequate concealment method is usedMeasurements: equal, reliable, and valid (includes masking of outcomeassessment)
Subjects and investigators are kept “blind” abouttreatment allocation
Clear definition of the interventions The treatment and control groups are similar atthe start of the trial
All important outcomes considered The only difference between groups is thetreatment under investigation
Hierarchy of researchdesigna
I Properly conducted randomized controlled trial (RCT)II-1: Well designed controlled trial without randomizationII-2: Well-designed cohort or case-control analytic studyII-3: Multiple time series with or without the intervention;
dramatic results from uncontrolled experimentsIII: Opinions of respected authorities, based on clinical
experience; descriptive studies or case reports; reports ofexpert committees
A prediagnosis is made and reported
a See reference 21.b See reference 22.
PEDIATRICS Volume 123, Number 4, April 2009 e735. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from

DOI: 10.1542/peds.2008-2415 2009;123;e716-e735 Pediatrics
Selvi B. Williams, Elizabeth A. O'Connor, Michelle Eder and Evelyn P. Whitlock Systematic Evidence Review for the US Preventive Services Task Force
Screening for Child and Adolescent Depression in Primary Care Settings: A
& ServicesUpdated Information
http://www.pediatrics.org/cgi/content/full/123/4/e716including high-resolution figures, can be found at:
References
http://www.pediatrics.org/cgi/content/full/123/4/e716#BIBLat: This article cites 81 articles, 26 of which you can access for free
Citations
eshttp://www.pediatrics.org/cgi/content/full/123/4/e716#otherarticlThis article has been cited by 2 HighWire-hosted articles:
Subspecialty Collections
http://www.pediatrics.org/cgi/collection/office_practice Office Practice
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be found online:
. Provided by University Of Pittsburgh, HSLS on July 29, 2010 www.pediatrics.orgDownloaded from