Scientifically Sound Guidelines for THC in Food in...
75
Scientifically Sound Guidelines for THC in Food in Europe nova-Institute July 2015 Authors Luis Sarmento (nova-Institute), Michael Carus (nova-Institute), Dr med. Franjo Grotenhermen (nova-Institute), Daniel Kruse (Hempro Int. GmbH & Co. KG) with support from: Dr med. Dr phil. Gerhard Nahler (Clinical Investigation Support GmbH, Austria), Dr med. Eberhard Pirich (Public Relations, Information and Knowledge Management in Health Care, Austria), Prof. Dr Rudolf Brenneisen (University Bern, Switzerland), and Prof. Dr Giampaolo Grassi (CRA-CIN, Italy) nova-Institut GmbH Chemiepark Knapsack Industriestraße 300, 50354 Hürth Internet: www.nova-Institut.eu E-Mail: [email protected]
Transcript of Scientifically Sound Guidelines for THC in Food in...

Scientifically Sound Guidelines for THC in Food in Europe
nova-Institute July 2015
Authors Luis Sarmento (nova-Institute), Michael Carus (nova-Institute), Dr med. Franjo Grotenhermen (nova-Institute), Daniel Kruse (Hempro Int. GmbH & Co. KG) with support from: Dr med. Dr phil. Gerhard Nahler (Clinical Investigation Support GmbH, Austria), Dr med. Eberhard Pirich (Public Relations, Information and Knowledge Management in Health Care, Austria), Prof. Dr Rudolf Brenneisen (University Bern, Switzerland), and Prof. Dr Giampaolo Grassi (CRA-CIN, Italy)
nova-Institut GmbH Chemiepark Knapsack
Industriestraße 300, 50354 Hürth Internet: www.nova-Institut.eu
E-Mail: [email protected]
!

nova-Institute would like to thank all donors for making this report possible (in order of contribution size):
• The European Industrial Hemp Association (www.eiha.org)
• Hempro Int. GmbH & Co. KG (www.hempro.com)
• Canah International (www.canah.com/en)
• Nutiva (www.nutiva.com)
• HEMP SEED OIL EUROPE LTD (www.hempseedoil.eu)
• Hemp Factory GmbH (www.hempfactory.com)
• HempFlax B.V. (www.hempflax.com)
• UAB Agropro (www.agropro.lt/en/)
• HANF FARM GmbH (www.hanffarm.de) nova-Institute would like to thank the following people for additional support and feedback on this document (in alphabetic order): Prof. Dr med Jace Callaway
Dipl. Ing Sarah Jungkunz
Michael Verhoeckx

Executive summary
The main aim of this paper is to contribute to the development of scientifically sound delta 9-tetrahydrocanabinol (THC) guidance values for hemp foods at the European level that protect the consumer without unnecessarily compromising the market of hemp products. For this purpose, having identified a lack of European-wide guidance values, the European Industrial Hemp Association (EIHA) requested nova-Institute to evaluate and propose new scientifically derived values for THC content in hemp foods. The lack of guidelines can potentially undermine an industry that is currently growing at a two-digit rate globally. Furthermore, excessive restrictions may prevent consumer access to what has been dubbed by both scientific minds and diet experts, alike, as a ‘nutritional powerhouse’ due to its wide fatty acid range and easily digestible proteins (Leson 1999). In Europe, only three countries – Germany, Belgium and Switzerland – have applied guid-ance values or limits for THC in food products, which tend to differ in purpose and scope, leaving both suppliers and consumers vulnerable and misinformed, and potentially repre-senting extra regulatory costs. Therefore, EIHA has requested nova-Institute to evaluate and propose safe guidance values for the European Union in order to assure consumers’ protection and sustain the industry’s current growth rate. In order to better understand the impact of THC consumed orally in food, the European Commission requested the European Food Safety Agency (EFSA) to deliver a detailed risk assessment with regard to the risks for human health in relation to the presence of THC in milk. After a first statement by EFSA, in 2011, commented on by EIHA, the European Commission insisted on having a second more detailed and expanded statement, published in June 2015. Therefore, EFSA has contacted EIHA for details with regards to the impact of THC in organisms and its metabolic conversion in vivo, along with its distribution in the hemp plant and THC content in final hemp goods. EIHA commissioned this paper with the aim of contributing to the discussion on THC reg-ulatory values, by showcasing the current status of THC regulations around the globe and reviewing the most up to date scientific literature on the adverse effects of THC, to then derive new scientifically based values for total THC uptake per person per day. Total THC is composed of a factor of THC and the caboxylic acid of THC (THCA), which is naturally found in the leaves and flowers, and has no effect on the human body in its purest form but may be ‘activated’ (decarboxylated to THC) under certain circumstances, such as high heat or pressure. In Europe, one country stands out as having the most thorough guidance values, Germany; and two others, Switzerland and Belgium, as having actual scientifically based govern-ment-backed limits. The latter are considered safe for the consumer and friendly to the industry, while many consider the German safe, albeit too conservative. Outside of Europe, Canada stands out as it only has limits on THC at the hemp raw material level, rather than the common approach of THC in finished goods. To date, there have not been complaints from customers or government, to suggest that the Canadian limits for THC in hemp foods could be too high. This system is pragmatic and designed to help the industry. Its efficien-cy can also be partially attributed to the country’s administrative character that has a more homogeneous culture and experience implementing highly technical regulations.
The German guidelines are one of the most commonly used in Europe, particularly in member states that lack their own THC regulation. This is due to the fact that Germany is the biggest hemp market in Europe and has been the first EU member to regulate THC in

food goods. Therefore, this paper will follow the same methodology as before, in order to re-establish more sound European guidance values that previously suggested (for the Ger-man guidance values, please refer to section 3.1.2 German THC guidelines). For all pur-poses, when referring to THC, this paper will mean total THC unless noted otherwise.
After an extensive review of the literature on the topic of THC consumption and effects, a Lowest Observed Effect Level (LOEL) of 2.5 mg of THC intake per person twice daily was derived. Due to the fact that the oral consumption of THC results in its effects wearing off within 8 hours, a twice daily intake was put forward, taking into account 16 hours of awakened time (please see Figure 1, Section 5). Applying an uncertainty factor of 20, de-duced from a combination of inter-individual variations (5), higher vulnerability of foetus-es and neonates (2), and potential interference with other substances (2), an Acceptable Daily Intake (ADI) of 0.120 mg of THC per person twice daily was obtained as a result. Although data from human trials, using a No Observed Effect Level (NOEL), can result in lower values, this paper suggests an uncertainty factor of 20, due to the fact that a NOEL is not yet known. Currently, only a LOEL is derivable from scientific studies. Therefore, this paper recommends further studies to be done on the subject matter of NOEL of THC in order to reduce the uncertainty factor from 20 (based on LOEL) to potentially 10 (based on NOEL). The authors introduce the value of 20 as a reference and leave the uncertainty fac-tor open to future revision. The following table exposes the evolution of LOEL and uncer-tainty factors on THC in hemp food goods.
Table 1 Comparison of LOEL and uncertainty factor of THC in hemp food goods based on BgVV 1998, EFSA 2011 and 2015, and nova-Institute proposed values 2015
Once safely permissible oral THC doses and the uncertainty factor were determined, the corresponding maximum permissible THC concentrations in food had to be derived using consumption patterns for relevant hemp foods. While typical consumption habits served as a baseline, the consumption of quantities higher than average had to be considered as well. Since hemp-based foods may be consumed in strongly varying quantities, several catego-ries and their respective limits were established. A list of products according to the catego-ries created can be found in annex (Annex I). Food intake data were taken into account, based on existing consumption patterns (see section 7). The limit for each category is a function of the average consumption per category and the sum of all THC uptakes per food good. The sum of all categories should not surpass the Acceptable Daily Intake (ADI) of 0.120 mg twice daily. With the total consumption per product and its respective limit known at the end consumer level, recipes of the products were used to derive reference values for business to business trading of hemp intermediate goods.
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! Comparison of Lowest Observed Effect Level (LOEL) and
uncertainty factor values
LOEL (mg/kg) 2.5 2.5 2.5 5*Uncertainty factor 20-40 100 30 20**
BgVV 1998 EFSA 2011 EFSA 2015 nova Institut 2015
*!2.5!twice!daily **! Value! proposed! is! derived! from! solid! data! available! from! clinical! studies! with! cannabis! extracts! and! THC! in! humans.! Additional!uncertainty!factors!are!not! justified.!Even!lower! factors! could!be!possible;!however!due!to!methodologic!uncertainty!in! establishing!a!reasonable!uncertainty!factor,!the!proposed!value!is!open!for!evaluation!in!future.!Please!see!text!for!more!information.

The following table summarizes nova’s proposed guidance values derived from scientifi-cally sound THC effects. The results of the data collection on THC regulation around the world are also presented as means of comparison. The following proposal was accepted by an absolute majority of the present members at EIHA’s General Meeting of May 2015.
Table 2 Final nova-Institute/EIHA proposal for THC regulation in intermediate and final food goods per category, and equivalent values for listed countries (in mg/kg)
!
The following Table showcases the practical implications of the proposed values for ready-to-eat products on hemp raw and intermediate materials with regards to THC content. De-pending on the hemp food product and its recipe intermediates can also show higher THC levels – in this paper, only the guidance values for the ready-to-eat products are covered.
Table 3 List of THC reference values for hemp raw material and intermediates derived from nova-Institute/EIHA proposal on ready-to-eat products, based on selected recipes and consumption patterns. And guidance values and limits for selected countries.

This paper’s proposals allow for a clear understanding between expectations of consumers and responsibilities of traders at the European level. The guidance values proposed in this paper guarantee the availability of hemp to the consumers while safely protecting them from any undesirable side effects. This could result in potential expansion of the industry and yield direct and indirect investment and job creation.
Outlook and further research topics
This report identified important gaps when deriving reasonable guidance values for THC in food. Further research is mainly needed in: Methodology and evaluation of uncertainty factor, realistic consumption patterns of hemp food, and interaction of THC with other cannabinoids (especially CBD).

Table of contents
1! INTRODUCTION*.................................................................................................................................*9!2! SUMMARY*ON*HEMP*FOOD*PRODUCTS*...................................................................................*11!2.1! THE!VALUE!OF!HEMP!AS!FOOD!.....................................................................................................................!11!2.2! THE!HEMP!FOOD!MARKET!............................................................................................................................!12!2.3! THE!PRESENCE!OF!THC!IN!HEMP!FOODS!..................................................................................................!12!
3! THC*GUIDANCE*VALUES*AND*REGULATIONS*AROUND*THE*WORLD*.............................*15!3.1! THC!GUIDE!VALUES!AND!REGULATIONS!IN!EUROPE!..............................................................................!15!3.1.1! Switzerland/............................................................................................................................................../16!3.1.2! German/THC/guidelines/....................................................................................................................../17!3.1.3! United/Kingdom/...................................................................................................................................../24!3.1.4! The/Netherlands/...................................................................................................................................../24!3.1.5! Italy/............................................................................................................................................................../24!3.1.6! Austria/......................................................................................................................................................../25!3.1.7! Belgium/....................................................................................................................................................../25!
3.2! THC!GUIDANCE!VALUES!AND!REGULATIONS!IN!NONTEUROPEAN!COUNTRIES!...................................!26!3.2.1! Canada/......................................................................................................................................................./26!3.2.2! USA/.............................................................................................................................................................../28!3.2.3! Australia/and/New/Zealand/.............................................................................................................../29!
3.3! CONCLUSION!...................................................................................................................................................!32!4! EFSA*FEEDING*ISSUE*......................................................................................................................*34!4.1! BACKGROUND!.................................................................................................................................................!34!4.2! EFSA!2011!REPORT!.....................................................................................................................................!35!4.3! LATEST!ACTIVITY!...........................................................................................................................................!37!4.4! CONCLUSION!...................................................................................................................................................!37!
5! LITERATURE*REVIEW*ON*NO*OBSERVED*EFFECT*LEVEL*(NOEL),*LOWEST*OBSERVED*EFFECT*LEVEL*(LOEL)*AND*ACCEPTABLE*DAILY*INTAKE*(ADI)*......................*38!5.1! PHARMACOLOGICAL!BASIS!FOR!A!LOWEST!OBSERVED!EFFECT!LEVEL!(LOEL)!AND!NO!OBSERVED!EFFECT!LEVEL!(NOEL)!...........................................................................................................................................!40!5.2! CONCLUSION!...................................................................................................................................................!44!
6! THC*EFFECTS*ON*HUMAN*BIOLOGICAL*VARIATIONS*..........................................................*46!6.1! SENSITIVITY!OF!CHILDREN,!NEONATES!AND!FOETUSES!..........................................................................!46!6.2! GENETIC!VARIATION!IN!THE!GENES!ENCODING!CB!RECEPTORS!AND!METABOLIZING!ENZYMES!....!48!6.3! PHARMACOLOGICAL!BASIS!FOR!DERIVING!AN!ACCEPTABLE!DAILY!INTAKE!.......................................!49!6.4! CONCLUSION!...................................................................................................................................................!52!
7! NEW*PROPOSAL*ON*THC*GUIDELINES*FOR*DIFFERENT*HEMP*FOOD*PRODUCTS*....*54!8! DELTA*9ETHC*CONTENT*IN*CONSUMER*GOODS*DERIVED*FROM*THE*HEMP*PLANT*63!9! REFERENCES*.....................................................................................................................................*65!
0
nova-Institute 8 THC Guidelines for Food
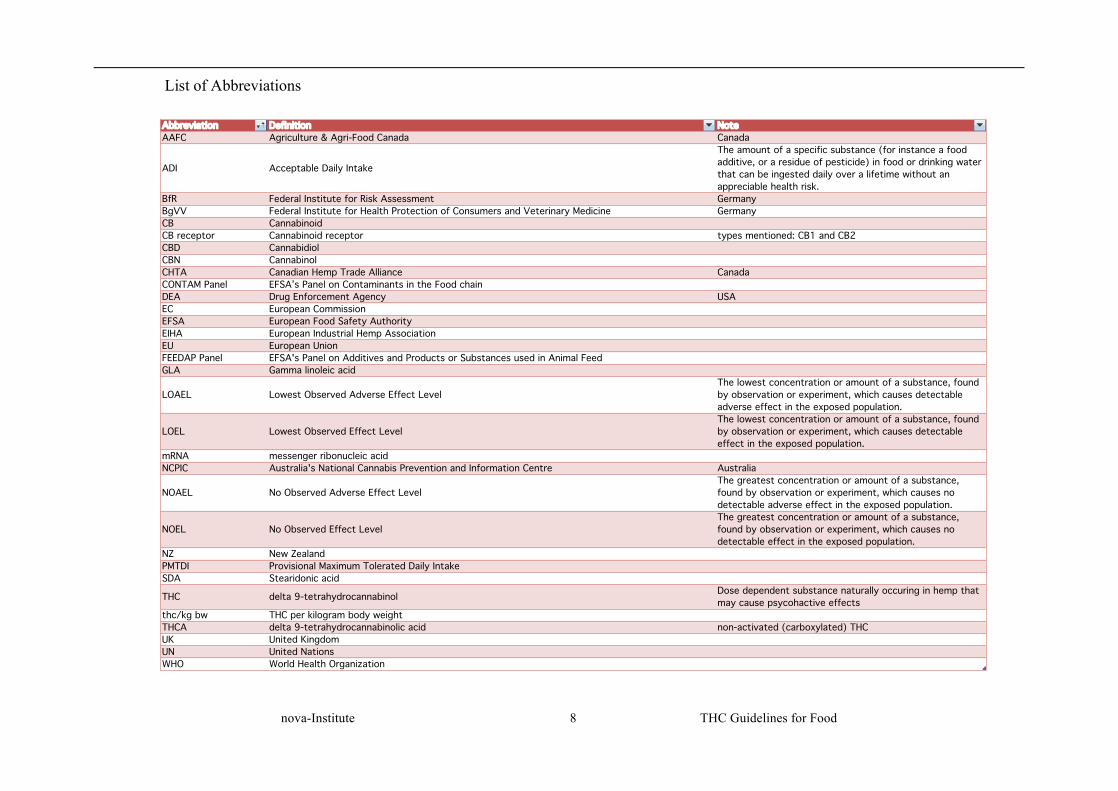
Abbreviation Definition NoteAAFC Agriculture & Agri-Food Canada Canada
ADI Acceptable Daily Intake
The amount of a specific substance (for instance a food additive, or a residue of pesticide) in food or drinking water that can be ingested daily over a lifetime without an appreciable health risk.
BfR Federal Institute for Risk Assessment GermanyBgVV Federal Institute for Health Protection of Consumers and Veterinary Medicine GermanyCB CannabinoidCB receptor Cannabinoid receptor types mentioned: CB1 and CB2CBD CannabidiolCBN Cannabinol CHTA Canadian Hemp Trade Alliance CanadaCONTAM Panel EFSA’s Panel on Contaminants in the Food chainDEA Drug Enforcement Agency USAEC European CommissionEFSA European Food Safety AuthorityEIHA European Industrial Hemp AssociationEU European UnionFEEDAP Panel EFSA's Panel on Additives and Products or Substances used in Animal FeedGLA Gamma linoleic acid
LOAEL Lowest Observed Adverse Effect LevelThe lowest concentration or amount of a substance, found by observation or experiment, which causes detectable adverse effect in the exposed population.
LOEL Lowest Observed Effect LevelThe lowest concentration or amount of a substance, found by observation or experiment, which causes detectable effect in the exposed population.
mRNA messenger ribonucleic acidNCPIC Australia's National Cannabis Prevention and Information Centre Australia
NOAEL No Observed Adverse Effect LevelThe greatest concentration or amount of a substance, found by observation or experiment, which causes no detectable adverse effect in the exposed population.
NOEL No Observed Effect LevelThe greatest concentration or amount of a substance, found by observation or experiment, which causes no detectable effect in the exposed population.
NZ New ZealandPMTDI Provisional Maximum Tolerated Daily IntakeSDA Stearidonic acid
THC delta 9-tetrahydrocannabinol Dose dependent substance naturally occuring in hemp that may cause psycohactive effects
thc/kg bw THC per kilogram body weightTHCA delta 9-tetrahydrocannabinolic acid non-activated (carboxylated) THCUK United KingdomUN United NationsWHO World Health Organization
List of Abbreviations
1 Introduction
nova-Institute 9 THC Guidelines for Food
1 Introduction
Delta-9-tetrahydrocannabinol (THC) is the most researched Cannabis component, as it is the main psychoactive ingredient of the cannabis plant. THC is a highly active pharmacological substance that shows, as a function of dose, effects on a multitude of organ systems and body functions. The physical toxicity is low for smoked marijuana in monkeys is surprisingly low (Ali et al., 1991). Tests to establish a lethal dose for THC in monkeys have been unsuccessful to date. Previously, the maximum adminis-tered dose of 9,000 mg/kg body weight did not result in the death of the monkeys (Thompson et al. 1973). This corresponds to a dose of 15 kilograms of drug Cannabis for a person weighing 70 kg, with an equivalent weight extrapolation. Aside from the temporary effects on cognition from high doses, such as loss of cognitive ability or drowsiness, beneficial effects at low doses were observed as well, e.g. antiemesis, immune-stimulating and neuroprotective effects (Sides 2015).
THC at high concentrations can cause adverse effects, the most relevant effects are those on mood and cognition (euphoria, fear, reduced cognitive functions) as well as on the cardiac circulation system (increase in cardiac frequency, changes in blood pressure). Since different parts of the hemp crop contain THC in different concentra-tions, products made from hemp, in particular food goods, made from hemp contain varying levels of THC. Processing methods may also influence THC occurrence in finished goods. Therefore, production and commercialization of hemp food products must be regulated so as to protect the consumer from potential unintended effects.
However, to date, there are still no THC guidance values for food at the European level. Derived from this lack of Europe-wide control, some member states have taken it upon themselves to draw guidelines on food products containing THC. Germany is among the states to do so. Although several member states also use the German non-binding guide values, the lack of legal strength of these guidelines leaves both traders and consumers, vulnerable.
The European Industrial Hemp Association (EIHA) represents hemp food producers in the EU and, with the public’s health in mind, proposes, through nova-Institute, a scientifically based regulation to give both the industry and consumers a safe frame-work.
In order to familiarize the reader with the current THC regulations around the world, this report first gives background information on the regulations in Germany and some other European countries, along with North America, Australia and New Zea-land. It also presents recent activities by the European Food Safety Authority (EFSA), which works for the EU Commission on THC limits for animal feed for meat and milk production.
This report next puts forward a comprehensive review of scientific literature on the topic of THC intoxication, in order to derive a Lowest Observed Effect Level (LOEL) and an Acceptable Daily Intake (ADI) of THC. The term ADI is related to substances that are deliberately added to food or unavoidable residues. It is derived from LOELs by applying an uncertainty factor.

1 Introduction
nova-Institute 10 THC Guidelines for Food
Finally, European-wide THC guide values for different hemp food goods such as hemp seed, hemp seed oil (hereon referred to as hemp oil), pasta, bread, snacks, and hemp-based beverages are recommended.
With this paper, nova-Institute provides a scientific base for legislation to be drafted on the regulation of THC in food goods at the national and European levels. EIHA contributes to the open discussion of THC in food with the aim of aiding the Commis-sion in establishing fair and scientifically based THC guidance values in food and feed goods across Europe, protecting consumers without compromising the market for hemp products unnecessarily.

1 Introduction
nova-Institute 11 THC Guidelines for Food
2 Summary on Hemp food products
Hemp (Cannabis sativa L.) is the common name for types of the cannabis plant used for industrial and food purposes around the world. It yields natural fibres, seeds and shives. Out of its main produces, seeds are commonly used in the feed and food in-dustry. Often hemp is cultivated and processed for multiple purposes, such as fibres, shives and seeds. There are significant health benefits associated with the consump-tion of seeds and its derivatives (i.e. hemp oil or seed meal cake) because of its well balanced fatty acid spectrum and high value proteins. The current market value of the hemp crop in Europe is steadily growing, following a two-digit world trend.
Due to the fact that hemp seeds contain trace amounts of delta-9-tetrahydrocannabinol (THC), the psychoactive ingredient that makes the cannabis plant sought after by rec-reational users, guidelines on THC values ought to be introduced. Scientifically sound guidance values would give room for an industry to flourish while protecting the con-sumer. The carboxylic acid of THC (THCA) is found naturally in the leaves and flowers, and has no effect on the human body in its purest form but may be ‘activated’ (decarboxylated to THC) under certain circumstances, such as high heat or pressure. This chapter will introduce the reader to the hemp plant, presenting its nutritional and market values, to then cover the issue of THC content in food goods in more detail.
2.1 The value of hemp as food
Hemp Seeds can be used whole (with shell), hulled (without shell) or pressed for its hemp oil. The pressing of hemp seed for oil generates, as a by-product, hemp seed cake, rich in protein and dietary fibre. Hemp oil can be used for food, feed or cosmet-ics (particularly skin applications) (Hempro International, personal communication 2014). Hemp seeds and its derivatives are considered of particular important nutri-tional value due to their “almost perfect” balance of the omega-3 and omega-6 essen-tial fatty acids plus the presence stearidonic acid (SDA) and gamma linoleic acid (GLA) (Manku 1990; Ross 1996; Science Daily 2014; Parker et al. 2003; Erasmus 1999; Simopoulos 2002; Ross et al. 2000; Lachenmeier and Walch 2005; Karimi and Hayatghaibi 2006; Gibb et al. 2005; Leizer et al. 2000, Callaway 2004, Callaway and Pate 2009). While most fatty acids in hempseed oil were already identified by the end of the 19th century (Von Hazura 1887), the presence of SDA in hempseed oil was not reported until just over a century later (Callaway et al. 1997a).
In a rare report on children who were of successively treated for tuberculosis with a traditional porridge, during the 1930s and 1940s in Czechoslovakia, in the absence of antibiotics (Sirek 1954). This report emphasized the importance of hempseed protein, and subsequent research over the years has since revealed the dietary significance of the omega-3 and -6 fatty acids that in hempseed oil.
A gross imbalance in the omega-3/6 ratio in the Western diet, with too much omega-6, is now considered an important contributor to the high occurrence of various in-flammatory, cardiovascular, skin and even mental disorders. As a balanced source of these fatty acids, hempseed oil and seeds can be used to help reduce their occurrence. The healthy ratio of omega-6 and omega-3 fatty acids, and the relatively high level of phytosterols in hempseed foods, makes them beneficial to health (Deferne and Pate 1996; Fenstrom 1999; Malini and Vanithakumari 1990). Clinical benefits on choles-
2 Summary on Hemp food products
1 Introduction
nova-Institute 12 THC Guidelines for Food
terol profiles have been shown for dietary hempseed oil in a double blind, randomized controlled trial (Schwab et al 2006). Dietary hempseed has been shown to be effective in treating patients with atopic dermatitis (eczema) in one clinical study that also used a double blind, randomized control design (Callaway et al. 2005).
Hemp seeds and its milled seed cake flour contain a high quality protein. It is easily digestible, and contains all essential amino acids in a balanced ratio that satisfies the protein needs of adults (Amerio 1998; Gibb et al. 2005; Erickson 2007; Hessle, Erik-son and Turner 2008; Callaway and Pate 2009). Commercially available protein flour and powders are high in protein and dietary fibre. They are used in shakes and smoothies, as well as for baking. 65% of the proteins in hemp foods are in the form of the globulin edestin. Edestin is considered by many to be the most easily digestible protein for mammals. The remaining 35% is albumin, yet another easily digestible protein (HempOil Canada, 2014).
2.2 The hemp food market
In Europe, during the year 2014 (based on seeds from the 2013 harvest) whole hemp seeds and derived hemp food and feed products are estimated to have had a total mar-ket size of €45 million a year. Of this, €15 million were generated from EU seeds and an additional €30 million were generated from imported seeds/oils (EIHA 2014). Due to its unique properties, particularly its environmental benefits and the high yield of natural technical fibres, hemp is a valuable crop for the bio-based economy.
Today hemp is a niche crop, cultivated on over 18,000 ha in the European Union (EI-HA 2014). Of these, over 10,000 hectares are located in France and 8,000 across 18 other countries within the European Union (EIHA 2014). Production is estimated to increase in Romania, Hungary, and the Baltic States. Currently, France, the Nether-lands, and Germany are big processors of hemp raw materials (EIHA 2014).
In Europe the total demand for hemp seed has been increasing over the years and was at about 18,000 metric tons in 2013. Estimates for 2014 saw the market reach 20,500 metric tonnes (EIHA 2014). Around 50% of this was covered by domestic production and ca. 50% by imports from China. Only a small share was cultivated organically, mainly used in the bio-food market (EIHA 2013). This was an increase from the 2008 values of 15,500 metric tonnes (FAOSTAT, 2013; Hempro 2014). The production of hemp seeds is predicted to rise with demand for human food doubling in the next 5 years, although animal feed will remain the main market share (Hempro 2014; EIHA 2014, nova-Institute 2014). This is due to the fact that some farm animals need lipids with a high share of omega-3 and omega-6 fatty acids for optimum development.
2.3 The presence of THC in hemp foods
Hemp plant parts used for food originate from varieties allowed for industrial cultiva-tion in Europe, which should not exceed 0.2% THC (in dry matter of the upper 1/3 of the crop) (Lachenmeier and Walch 2005; EU Commission 2008). The varieties of hemp legally allowed by the European Union can be found in Annex II of COMMIS-SION REGULATION (EC) No 145/2008 of 19 February 2008. From an average of 2,151 samples collected in Europe between 2006 and 2008, the average concentration of THC found was 0.075% (EFSA Scientific Opinion 2011), although samples in the
2 Summary on Hemp food products

1 Introduction
nova-Institute 13 THC Guidelines for Food
EU showed values ranged from 0.05% to 0.2% (El-Ghany 2002; Mechtler et al. 2004). The prescribed use of certified hemp planting seed by the EU and the increase of controls on manufacturers have obviously preserved low level of THC in EU food and feed products (Lachenmeier and Walch 2005).
Generally, all parts of the Cannabis plant can contain cannabinoids (Lachenmeier and Walch 2005). However, Australia's National Cannabis Prevention and Information Centre (NCPIC) (2011) has stated that the stalks and seeds have "much lower THC levels" than the flower, with the UN confirming that leaves can contain ten times less THC concentrates than the buds, and the stalks one hundred times less (UN 2009). The hemp seed itself, which is used for both food and feed, is almost free of THC but unavoidable contamination happens by contact between the shell (testa) and the flow-er or leaves of the plant. Only less than 2 µg/g for drug-type seeds and less than 0.5 µg/g for hemp-type seeds of THC is found in the kernel itself (internal area) (Ross et al. 2000; Lachenmeier and Walch 2005). THC concentration in seeds is a function of the type of seed and the extent of contamination of the seeds with plant debris (Lachenmeier and Walch 2005). When hempseeds are cleaned properly, no significant THC content being found (Hemphill, Turner and Mahlberg 1980; Ross et al. 2000; Karimi and Hayatghaibi 2006). In both North America and Europe, since 1998, a sig-nificant decline in THC concentrations has been reported in hempseed foods. This is due to the planting and importing of low THC strains and a more careful cleaning of the seed before processing (Leson et al. 2001).
In fresh, unprocessed hemp plants, THC mostly occurs in the form of its inactive car-boxylic acid: i.e. THC acid A (here onwards referred to simply as THCA). THCA is present at a rate of about 90% of the total THC, and is devoid of psychotropic effects (Dewey 1986). However, THCA can be decarboxylated, i.e. converted into its active form, usually with heat, to provide its biologically active product; THC. Decarboxyla-tion occurs primarily as a function of time, pressure, temperature and long exposure to light, for instance in food processing or when combusted. Thus, largely unprocessed foods, such as cold-pressed oils, do usually contain large fractions of the pharmaco-logically inactive THCA. THC can naturally accumulate even if THCA-containing material is not heated, with a half-life of between 35 and 91 days (depending on stor-age conditions and type of material this half-life can even be considerably longer), whereas THC degrades to cannabinol (CBN) at a half-life rate of only 24 to 26 months (Lindholst 2010).
In order to take into account the possibility of THCA converting into THC, previous guidance values have assumed total THC. The EU limits of 0.2% in the crop, for ex-ample, take both THC and THCA into account, at total THC value. The same applies for many food guidance values, including the widely used BgVV (German guidance values).
In order to calculate total THC, one adds the amount of THC found in a sample to the amount of THCA present after multiplying by a factor of 314/358 to correct for the different molar masses of the two compounds. In other words, even when transfor-mation was complete, only a part of THCA present in a sample (approximately 87.7% by weight) will be available as THC.
As an example:
2 Summary on Hemp food products

1 Introduction
nova-Institute 14 THC Guidelines for Food
If delta 9-THC were to be 0,28 mg/kg; and THCA were 0,91 mg/kg, the TOTAL THC would not be 1,19 mg/kg (= 0,28 + 0,91), but rather 0,28 + 0,91*314/358 = 1,08 mg/kg of product.
This paper will refer to total THC as THC unless noted otherwise.
The following chapter will showcase the current THC guidance values around the European continent and the world, in order to contextualize for the reader the current existing guide values in the food market and to show where there is room for im-provement.
2 Summary on Hemp food products
3 THC Guidance Values and Regulations around the World
nova-Institute 15 THC Guidelines for Food
3 THC Guidance Values and Regulations around the World
In Europe the total demand for hemp seed has been increasing over the years and was at about 18,000 metric tons in 2013. Estimates for 2014 see the market reaching 20,500 metric tons (EIHA 2014). It is estimated that the production of hemp seeds will rise, with demand for hemp food doubling (Hempro International 2014; EIHA 2014; nova-Institut 2014).
Canada is a major producer of hemp seeds (18,000 metric tonnes in 2011), which rep-resents a considerable increase of 6,500 metric tons in total since 2005. Almost all of the hemp produced in Canada is for the supply of seeds. There were about 44,000 ha of hemp farmed in Canada in 2014 and 18,300 metric tonnes were exported the same year (Hermann 2015). These tend to be used for human food, either as hulled seeds, hemp oil, or protein powder (Hempro International 2014).
With demand for hemp food goods estimated to grow fast in Europe and North Amer-ica by the end of the decade (EIHA 2013), regulations become an ever more pressing necessity. The following chapter will address current THC guide values in selected European nations, Canada, USA, and Australia, New Zealand. This will facilitate the understanding and comparison of THC regulatory systems worldwide. Chinese ex-ports have recently increased, with the volumes to Europe doubling in less than five years (Hempro International 2015, EIHA 2015)
3.1 THC guide values and Regulations in Europe
When hemp seeds were reintroduced for human consumption in the mid-1990s, it was not uncommon to find THC levels in excess of 100 ppm (i.e. > 100 mg THC/kg) in hemp oil from Chinese and European seeds. It was not until the mandatory farming of low-THC varieties combined with the cleaning of the seeds, that THC levels in oil from European producers were effectively reduced.
Currently European THC limits only exist for hemp cultivation. According to EU law, cultivating hemp is solely permitted if it contains less than 0.2% (or 2.000 ppm (mg/kg)) THC in the upper 1/3 of the mature crop (Council Regulation (EC) No 1420/98)
EU Regulations on General Food Law, which covers food during manufacture, prepa-ration or treatment, recognises
“…any product being extracted from or made on the basis of hemp can be considered as narcotic drugs in the meaning of the United Nations Convention on Narcotic Drugs (1961) and the United nations Convention of psychotic substances (1971). According to Article 2(g) of Regulation (EC) No 178/2002 (General Food Law), narcotic or psy-chotropic substances covered by the aforesaid conventions should not be considered as “food” and consequently, they should not be allowed to be incorporated into the food during manufacture, preparation or treatment.”
This separates the narcotic cannabis plant from hemp, one being penalized and the other permitted under certain controls. Member States that do not have specific THC regulations fall under EU and international law. However, food law is enforced at the

3 THC Guidance Values and Regulations around the World
nova-Institute 16 THC Guidelines for Food
discretion of individual Member States. The following sub-chapter will review the current status of hemp in several European countries.
Within the EU, foods containing hemp products are allowed in several countries in-cluding UK, Germany, Austria, Finland, but regulation is unclear in others (Food standards NZ 2012). The resulting lack or uncertainty in regulation in some countries leads traders to use the German guidance values as a reference point to limit legal liability. Yet, this makes it hard to bring hemp food goods to the market, unnecessari-ly limiting a growing industry.
This sub-chapter starts with the Swiss limits on THC, to then focus on the German case in more detail, the latter being the generic model for THC regulation in Europe. Finally, the sub-chapter will showcase THC guide values imposed by other EU mem-ber states.
3.1.1 Switzerland
Switzerland is a special case when it comes to THC in food, as it is one of the few countries that have limits in place, rather than guidance values. The values were de-rived with the aim of avoiding psychotropic effects.
Due to the fact that biologically relevant concentrations of THC were found in Swiss hemp foods in 1996, the Swiss government introduced legal limits for THC in oil and other foods made from hemp seeds. The high THC content found in oils and cow milk was the result of the improperly cleaned seeds of high-THC varieties being used (Lehmann et al. 1997). This pushed Switzerland to become the first country in the world to adopt THC limits in food (Grotenhermen et al. 1998; Hemp Food 2001).
Reviewing scientific studies, the Swiss government divided food goods in sub-sets according to daily average uptake and general THC prevalence (Table 4) (Russo 2013; EDI 2014). To maintain a certain flexibility for farmers to breed new strains, the THC limit for crops was set at 1% THC (Bundesamt für Gesundheit, Switzerland).
Table 4 THC limits for food goods in Switzerland. Source: Fremd-und-Inhaltsstoffverordnung, FIV 2014
!
Due to the impossibility of completely excluding liability by guidance values, the Swiss limits are considered by the industry as an acceptable alternative to any guid-ance values. To date, there has been no case of THC intoxication due to hemp food ingestion in Switzerland and no market distortion resulting from the regulation of

3 THC Guidance Values and Regulations around the World
nova-Institute 17 THC Guidelines for Food
THC in food. These limits are important as they help establish the upper threshold of governmentally set limits in THC-rich food goods. Although higher, the Swiss limits are scientifically sound, governmentally sponsored and formulated through a sound methodology.
3.1.2 German THC guidelines
The Federal Institute for Health Protection of Consumers and Veterinary Medicine (BgVV), which in 2003 came to include the Federal Institute for Risk Assessment (BFR)1, developed the German THC guidelines in the year 2000.
BgVV’s goal was to create a guidance value of THC per food good categories, in or-der to allow hemp in the food market but prevent adverse effects from excess inges-tion of hemp products. National consumption data were used to this effect to better classify each THC containing food category and its consumer uptake.
The first step taken by BgVV in the development of the guidelines was to establish an Acceptable Daily Intake (ADI) for THC. The ADI is the amount of a specific sub-stance (for instance a food additive, or a pesticide residue) in food or drinking water that can be ingested daily over a lifetime without a significant health risk. Daily limits are usually established for any food component or additive that is harmless in small doses but can have negative effects in larger amounts. It aimed at capping daily con-sumption of THC in order to avoid undesired secondary effects. ADI is calculated through establishing a Lowest Observed Effect Level (LOEL) that is then divided by an uncertainty factor.
Scientific literature tends to agree that a single dose of 2.5 mg of THC per person (70 kg body weight) per day can be regarded as a placebo. In rare cases, this dose rarely might cause mild psychotropic or psychomotor effects in humans such as ‘light head-edness’ (Please refer to Table 13 on side effects in the studies by Zajicek et al. (2003; 2005)). BgVV used this value as its LOEL per person.
Once a LOEL was established, an uncertainty factor was then applied. Uncertainty factors are a way to protect several subpopulations that are more vulnerable to a par-ticular substance effect. In the case of THC, this factor was determined to be 20. Di-viding the LOEL by the uncertainty factor resulted in an ADI of THC of 0.125 mg per person per day. As an added safety measure, this value was then rounded down to 0.120 mg per person per day. The following table (Table 5) summarizes this calcula-tion:
1 Bundesinstitut für Risikobewertung, www.bfr.bund.de

3 THC Guidance Values and Regulations around the World
nova-Institute 18 THC Guidelines for Food
Table 5 BgVV/SKLM THC-guidance values for hemp-based foodstuffs BgVV/SKLM THC-guidance values for hemp-based foodstuffs Male weighing 70 kg, 25-50 years old Lowest Observed Effect Level (LOEL) per person 2,5 mg THC/day/person divided by uncertainty factor of 20: Acceptable daily intake (ADI) of THC 0,125 mg THC/day * person rounded to: 0,120 mg THC/day/person
With a calculated ADI of THC of 0.120 mg calculated, the next step was to derive guidance values for specific food groups. For this purpose, BgVV used consumption patterns relevant to foods that may be partially or fully made out of hemp goods. The following table (Table 6) shows the German average consumption patterns for select-ed goods that may contain hemp. For simplicity purposes, several food groups were gathered in three food categories (column 1). The initial data were retrieved from an average annual consumption per capita of the German Federal government for the years 1994, 1995 and 1996 (column 4), and converted to daily uptake in column 5. An aggregated sum per category was calculated in column 6. Finally, these values were rounded up to create an extra layer of safety (column 7), in order to assure that any excessive consumption would not result in intoxication, due to the varying diets and quantities per serving.

3 THC Guidance Values and Regulations around the World
nova-Institute 19 THC Guidelines for Food
Table 6 Consumption data for years 1994, 1995 and 1996 for selected products. Source: BMELV 1997
Category
General food groups
Specific food goods
Annual Consump-tion
Daily consump-tion Total daily consumption
per category (g/day/capita)
(ml/day/capita)
Total daily consumption per category rounded
(kg/day/capita) (l/day/capita)
(German Federal Statistical Office) (kg/year/capita) (g/day/capita)
(l/year/capita) (ml/day/capita)
Oils Edible oil
· Including the quantities present in processed foods
12.1 (1996) 33 7* 0.007* · Olive oil · Other food oils
Finished food goods
Finished products, pastries, and non-perishable foodstuffs
· Waffles, biscuits
13.4 (1994) 37
472 0.5
· Chocolate, bars, nuts/seeds · Salty baked goods · Chocolate cream · Honey cake, gingerbread
Sweets · Sweets and others 7.3 (1996) 20
Meats · Sausage
36.5 (1996) 100 · Meat
Pastas · Pasta 4.8 (1995 and 1996) 13
Dairy Products · Yoghurt
25.5 (1995 and 1996)
· Cheese 70
Breads, rolls and Nuts · Breads and rolls
84.9 (1996) 232 · Nuts
Beverages
Alcoholic drinks
· Beer
169.6 (1996) 465
1155 1.2
· Wine · Sparkling Wine · Spirits
Tea · Black
25.5 (1996) 70 · Infusions
Non-alcoholic drinks · Refreshments
225.5 (1996) 620 · Fruit juices
* Value rounded due to culinary limitations of hemp oil

3 THC Guidance Values and Regulations around the World
nova-Institute 20 THC Guidelines for Food
Ready to eat solid food goods totalled 0.5 kg/day/person, while alcoholic and non-alcoholic beverages totalled 1.2 l/day/person. Even though the total daily consumption of oils reached 33 g/day/person, hemp oil has the limitation that it loses beneficial properties when heated. Therefore, a value of 7 g/day/person was adopted within which it could be used to replace other oils without losing properties.
With an Acceptable Daily Intake (ADI) of THC and a rounded daily consumption of certain grouped food goods, BgVV could now proceed with the calculation of the guidance values per category.
Each category’s guidance value multiplied by the average daily consumption per per-son yields the daily THC uptake per person per category. The sum of all categories of daily THC uptakes per person ought not to exceed the ADI of THC of 0.120 mg per person per day.
Taking hemp oil, a guidance value of 5 mg of THC per litre of product was estab-lished for pragmatic purposes, because several samples tended to average this amount, with no registered intoxication cases. Furthermore, the fat soluble character of THC made it too difficult to reduce its presence beyond this level, even after precautionary measures, such as seed cleaning, had been applied.
As previously mentioned, in order to calculate the daily THC uptake of hemp oil per person, one needs to multiply the daily THC guidance value of hemp oil per person by the average daily consumption of oil per person.
In other words, the daily THC uptake of hemp oil, per person, is: 5 (the guidance val-ue in mg/kg) multiplied by 0.007 kg (the average daily consumption), which equals 0.035 mg of daily-ingested THC per person. 0.035 mg is the total daily amount of THC one would ingest from oils if replacing 7 g of oil for hemp oil.
Applying this reasoning to beverages, BgVV established a daily guidance value of 0.005 mg of THC per kg, resulting in a maximum of 0.006 mg of THC being ingested daily per person through drinks (0.006 = 0.005 x 1.2). In other words, once more, if one were to replace all of one person’s daily consumed beverages by hemp-derived beverages, one would ingest a total of 0.006 mg of THC per day.
In order to keep the ingestion levels of THC below the THC ADI, the sum of all cate-gories of daily THC uptakes ought not exceed the limit of 0.120 mg per day per per-son.
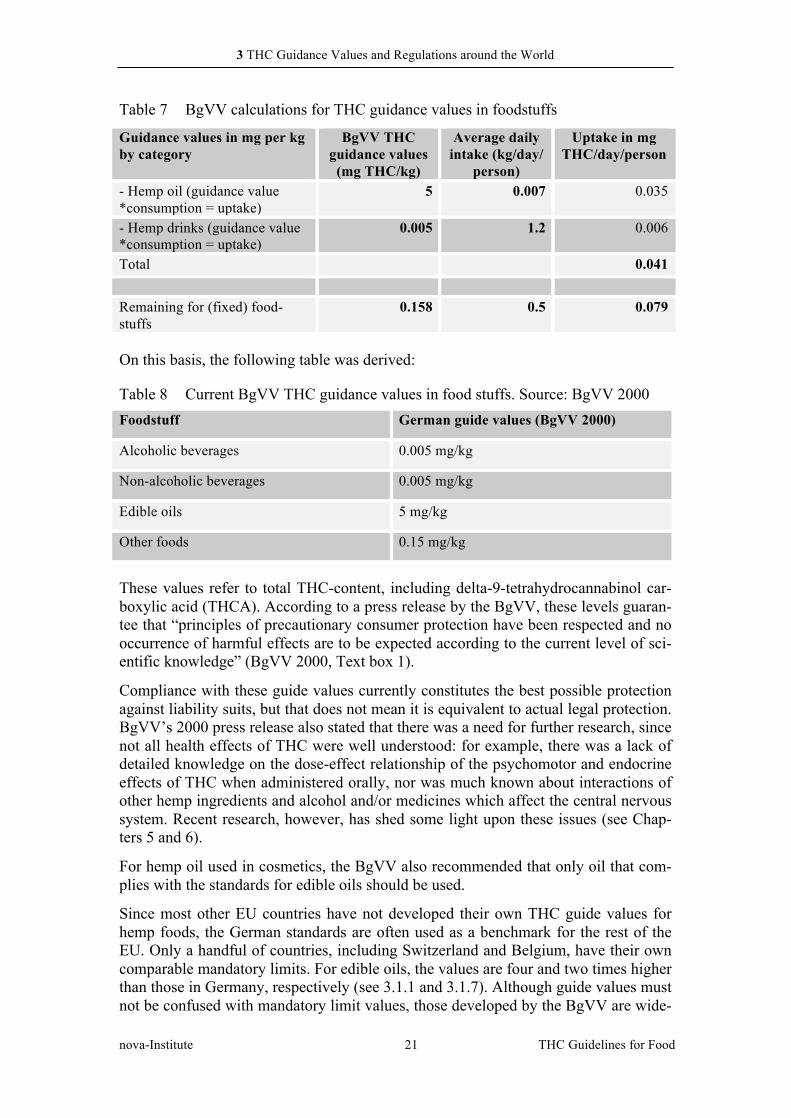
Finally, BgVV divided the difference between the sum of the daily THC uptake per person of both hemp oil and hemp beverages (0.041 mg) by the average daily intake of remaining food goods (0.5 kg), to reach the guidance value for all other food goods of 0.158 mg per person per day. This value was rounded down, as a safety precaution to 0.15 mg/kg. The following table (Table 7) summarizes the previous calculations:
3 THC Guidance Values and Regulations around the World
nova-Institute 21 THC Guidelines for Food
Table 7 BgVV calculations for THC guidance values in foodstuffs
Guidance values in mg per kg by category
BgVV THC guidance values
(mg THC/kg)
Average daily intake (kg/day/
person)
Uptake in mg THC/day/person
- Hemp oil (guidance value *consumption = uptake)
5 0.007 0.035
- Hemp drinks (guidance value *consumption = uptake)
0.005 1.2 0.006
Total 0.041
Remaining for (fixed) food-stuffs
0.158 0.5 0.079
On this basis, the following table was derived:
Table 8 Current BgVV THC guidance values in food stuffs. Source: BgVV 2000 Foodstuff German guide values (BgVV 2000)
Alcoholic beverages 0.005 mg/kg
Non-alcoholic beverages 0.005 mg/kg
Edible oils 5 mg/kg
Other foods 0.15 mg/kg
These values refer to total THC-content, including delta-9-tetrahydrocannabinol car-boxylic acid (THCA). According to a press release by the BgVV, these levels guaran-tee that “principles of precautionary consumer protection have been respected and no occurrence of harmful effects are to be expected according to the current level of sci-entific knowledge” (BgVV 2000, Text box 1).
Compliance with these guide values currently constitutes the best possible protection against liability suits, but that does not mean it is equivalent to actual legal protection. BgVV’s 2000 press release also stated that there was a need for further research, since not all health effects of THC were well understood: for example, there was a lack of detailed knowledge on the dose-effect relationship of the psychomotor and endocrine effects of THC when administered orally, nor was much known about interactions of other hemp ingredients and alcohol and/or medicines which affect the central nervous system. Recent research, however, has shed some light upon these issues (see Chap-ters 5 and 6).
For hemp oil used in cosmetics, the BgVV also recommended that only oil that com-plies with the standards for edible oils should be used.
Since most other EU countries have not developed their own THC guide values for hemp foods, the German standards are often used as a benchmark for the rest of the EU. Only a handful of countries, including Switzerland and Belgium, have their own comparable mandatory limits. For edible oils, the values are four and two times higher than those in Germany, respectively (see 3.1.1 and 3.1.7). Although guide values must not be confused with mandatory limit values, those developed by the BgVV are wide-

3 THC Guidance Values and Regulations around the World
nova-Institute 22 THC Guidelines for Food
ly accepted in practice and provide considerable (albeit limited) legal and planning conditions for producers.
Most products are likely to comply with the guide values. Only products containing a high number of hemp seeds and hemp seeds themselves may, at times, surpass the guidance values. This may also be the case in fat rich products, such as chocolates, since THC is fat-soluble.
A factor that plays a role in keeping the THC content in these products low is the cleaning process of the hemp seeds. The seeds themselves contain only traces of THC at the surface and the THC content in the oil mainly stems from contaminations from other plant particles. However, seed cleaning is not sufficient to keep the THC content of certain products under current guidance values, while it can also be deemed exces-sively cautious and strict.

3 THC Guidance Values and Regulations around the World
nova-Institute 23 THC Guidelines for Food
Text box 1: The original press release of the BgVV, 16.03.2000
Available at http://www.bfr.bund.de/cd/1309
“BgVV recommends guidance values for THC (tetrahydrocannabinol) in hemp-containing foods
Varieties of hemp which are low in narcotics can now be cultivated as useful industrial plants. Consequently, components of the hemp plant are increasingly being used to pro-duce foods. The constantly growing range of products takes in for instance hempseed and hemp oil as well as cakes, pastries and pasta products, confectionary, sausage products, herbal teas, lemonades and beers produced using hemp. In the opinion of the Federal Insti-tute for Health Protection of Consumers and Veterinary Medicine (BgVV) it is mainly the content of the diverse action, psychoactive delta-9-tetrahydrocannabinol (THC) or its precursor delta-9-tetrahydrocannabinol carboxylic acid which is decisive for the health assessment of these products.
Already in the past BgVV has recommended (Press Release 26/97) that the daily intake of THC in hemp-containing foods should not exceed 1-2 µg per kg body weight. Examinati-on of these studies confirmed this assessment which means that it is now the basis for the proposals elaborated by BgVV for THC values in foods. Assuming that average amounts of various hemp-containing products are consumed every day, the following THC guidance values were derived for foods:
5 µg/kg for non-alcoholic and alcoholic beverages
5000 µg/kg for edible oils
150 µg/kg for all other foods
The above values refer to ready-to-eat foods and apply to total THC including delta-9-tetrahydrocannabinol carboxylic acid. Compliance with this value means that the princip-les of precautionary consumer protection have been respected and no occurrence of harm-ful effects are to be expected according to the current level of scientific knowledge. Since the dose dependency of some effects of THC has not been clarified in a definitive manner, the proposed guidance values must be seen as temporary. They are meant as an orientation aid in food monitoring and for manufacturers.
The guidance values suggested by BgVV were confirmed in consultations of the Senate Commission of the German Research Society for the Assessment of Health Safety of Foods (SKLM). In this context, a need for research was identified on all these issues. For instance, there is a lack of more exact knowledge about the dose-effect relationship of the psychomotor and endocrine effects of THC when administered orally to human beings. Studies on impairment of psychomotor abilities are especially important given the rele-vance of these effects for traffic safety and safety at the workplace. In this context, exami-nations must also be undertaken of possible interaction with other hemp ingredients and with alcohol and/or medicines which affect the central nervous system in man.
A working group within BgVV is currently looking at the development of suitable stan-dardised analytical methods for the determination of total THC in various foods. After consultation with its Cosmetics Committee, BgVV also recommends that only hemp oil which complies with the above guidance value for edible oils should be used in cosme-tics.”

3 THC Guidance Values and Regulations around the World
nova-Institute 24 THC Guidelines for Food
3.1.3 United Kingdom
In the UK, the use of hemp in food is not regulated, at the moment, and it tends to be considered on a case-by-case basis. Factors considered include the amount of hemp present in the final product, the extent of use and anticipated intake. Cannabis is still considered a controlled drug and so the Home Office makes sure every product is subjected to review in order to clear its potential growth or commercialization as a narcotic. (Braham 2015)
Several types of products can be found on the market, including seeds and protein powders.
3.1.4 The Netherlands
Food containing hemp is sold and consumed in The Netherlands.
The Dutch authorities do not have any specific laws governing hemp in food and therefore follow EU laws and regulations. There are no maximum levels for THC in food for the Netherlands, no licensing requirements, no import restrictions and no THC-based controls on the seed.
This lack of regulation leaves several Dutch traders unsure about how to place their products in the market legally. This grey area also leaves suppliers vulnerable to pros-ecution, as they can be held solely responsible for the health effects of their food. Generally, Dutch companies use the German guidelines as a reference although cli-ents can be more flexible in some products, such as oils, than others, such as protein powder. The German guidelines do not protect traders from legal action.
The seeds from Cannabis plants are exempt from the Dutch Opium Act (European Monitoring Centre for Drugs and Drug Addiction 2014).
3.1.5 Italy
Italy allows hemp-based foods. THC levels are currently expected to be zero or the closest detectable value to zero, although this may be revised in the future. The Italian Health and Internal Affairs Ministries have been working with experts in an attempt to change the current tolerance level. However, changes in governments resulting from elections tend to slow the process down and render it unproductive or, at times, regressive as new governments want to restart the process from scratch.
Food goods derived from hemp seeds are allowed, although expected to contain no THC, due to the fact that THC is scheduled in the list of forbidden substances. Re-gardless of the zero-THC cap, hemp food goods containing THC can still be found, as some products are more tolerated than others, such as hemp oil. Seed and oil are cur-rently classified as supplements and used in the treatment of menstrual pains and skin care.
The position of ‘zero tolerance’ was taken only in a letter (Circolare) from the Health Ministry in 2009, to allow production and sale of hemp-based foods. However, the Circolare has been taken with a common sense approach from both control agencies and authorities (Assocanapa, 2015)
3 THC Guidance Values and Regulations around the World
nova-Institute 25 THC Guidelines for Food
If a company were to start selling hemp food goods, it is legally allowed to do so, although it runs the risk of being controlled by the police regarding THC-containing products. This is more frequent on hemp beer than other products, due to the per-ceived dangers of exposing vulnerable people (alcoholics) to yet another substance.
Local health authorities, fraud squads and import authorities have the responsibility of checking the THC level in food. At the border the checks are carried out on the doc-umentation, and samples may be taken for analysis. Plans for legislation include using the German guidelines. However, governments seem reluctant to approve them, as they may generate a boom in hemp farming and production of derived products. Fur-thermore, there are no strong local farming associations that can lobby the govern-ment and effectively defend more specific THC regulations.
Currently, production of hemp food goods in Italy is low and irregular (Grassi 2014). Producers and traders eagerly wait for clear, simpler and logical regulations in order to conduct their business (Assocanapa, 2015).
3.1.6 Austria
Austria permits the sale and consumption of foods containing hemp. There are no specific Austrian legal requirements for hemp foods, so Austria follows EU laws and regulations. The institution responsible for THC regulation is the Austrian Agency for Health and Food Safety or Österreichischen Agentur für Gesundheit und Ernährungssicherheit (AGES).
Based on the European General Food Law Regulation (EC) 178/2002 requiring food to be safe, Austria expects THC content in foods not to exceed 1-2 µg/kg bw/day, or 0.1 ppm per person per day, assuming an adult weighing 70 kg.
Austria has no direct experience with drug testing results but relies on a German study (Rosenstock 2004) where students were fed hemp chocolate, granola bars etc. which had quantifiable amounts of THC. Although large amounts were consumed and blood and urine samples were taken on an hourly basis no positive blood or urine results were obtained. Experiments involving considerable amounts of hemp tea produced similar results. The overall conclusion was that hemp-containing foodstuffs that meet German guidance values and are consumed in normal amounts do not lead to blood concentrations associated with effects or positive cannabis results in body fluids.
The Austrian Food Inspection Authorities are responsible for THC compliance in food. Hemp foods such as seeds, oil, butter, beer and chocolates are tested on a case-by-basis for THC content. Hemp tea is tested on a routine basis.
3.1.7 Belgium
Belgium permits the sale and consumption of hemp foods. Prior to the food being available for sale, it must be granted an exemption from the Belgian food regulations. Exemptions are granted on a case-by-case basis. To date these include: tea-based bev-erages, alcoholic beverages, oil, seeds, cookies, bread, veggie-burgers and flour.
For those foods where exemptions are granted the level of THC needs to be provided on a batch basis and maximum levels must not exceed the mandatory limits below.

3 THC Guidance Values and Regulations around the World
nova-Institute 26 THC Guidelines for Food
These provisions also apply to imported foods containing THC. The limits were es-tablished on a pragmatic basis and under a decent risk evaluation.
• Oil of seed: 10 mg/kg
• Seed and flour of seed: 5 mg/kg
• Other foods and drinks: 0.2 mg/kg
(FSANZ 2012)
Belgian authorities use batch testing for THC content to counteract the possibility of high-THC products getting into the food chain. In addition, any hemp production needs to comply with EU regulations and laws on type of seed used. Analysis reports must include batch number, the method of analysis and detection limit. (Geelen 2015)
Purchased seeds or oil certified as low-THC that are later used to make other products do not require subsequent THC testing. In other words, the THC-analysis that comes with the prime material can be used for the end product. (Geelen 2014)
3.2 THC guidance values and regulations in non-European countries
The US and Canada both established hemp and marijuana legislation early on. In 1938, mainly due to the 1937 US-led anti-cannabis legislation, the cultivation of both drug cannabis and industrial hemp were banned in Canada and the United States. ince 1994, a small number of Canadian companies, as well as Canadian universities and provincial governments started researching industrial hemp production and pro-cessing. Due largely to their initiative, in 1998 the 60-year ban was lifted in Canada and the commercial cultivation of hemp was authorized.
Today, hemp is enjoying a renaissance, with the global hemp market becoming a thriving, commercial success. In particular, a recent boom of the cannabis industry in North America has seen increasing demand for hemp goods. In the United States alone, estimated retail sales for hemp food and body care products were $620 million in 2014. The market percentage has increased from 7.3% (2011), to 16.5% (2012), to 24% (2013), to 21.2% in 2014 (HIA 2015).
Until recently, and although commercialised, hemp foods were not permitted for hu-man consumption in Australia and New Zealand. Exceptions to certain cannabis seeds and products (such as hemp oil in NZ) have recently been granted and hemp food-stuffs continue to be commercially available.
3.2.1 Canada
Canada was the second country to pass THC limits, after Switzerland, in 1998. How-ever, the limit does not refer directly to food, but to hempen raw and semi-finished products, such as hemp oil or flour. This allows further processed food goods contain-ing hempen semi-finished products to be produced without the need for THC testing.

3 THC Guidance Values and Regulations around the World
nova-Institute 27 THC Guidelines for Food
Products containing hemp are exempt from further regulation if they contain semi-finished or derivative hemp goods that were found to contain 10 mg or less THC per g (or 10 ppm or 0.001%). This regulation represents a de facto limit for the handling of hemp.
Producers and traders alike believe that this method is more efficient because it caps THC limits without interfering in the market. Guidelines, such as the German ones, are deemed too intrusive, costly and inefficient. There have been no cases of positive work place drug tests derived from this method. (Hermann 2015)
After the seeds are proved to be non-viable and contain less than 10 ppm, they are cleared for sale. All intact viable grains are deemed non-viable once they have been rendered so by the methods set-out in the Industrial Hemp Technical Manual, and they have been shown to be incapable of germination. These methods include steam heat, infra-red cooking processing and toasting. It is the responsibility of the proces-sor, not the supplier of the grain or the recipient of the oil or meal, to assure that tests are conducted after processing. Accredited laboratories must also be authorized to possess industrial hemp grain or seed. (Food Standards Australia and New Zealand 2012)
The THC limit for industrial hemp plants is 0.3% (3.000 ppm) of the dry weight of leaves and flowering parts. The THC levels in crops are usually regulated via an ap-proved cultivar list. Licensed individuals must have their crops tested for THC to veri-fy they are complying with the law.!Some!Canadian!cultivars!are!exempt!from!in5field!THC! testing! based! on! the!Canadian!Policy! on! the!Exemption! of! Industrial!Hemp!Varieties!from!THC!Testing!During!the!Growing!Season.!(Hermann!2014)
On the origin of the 0.3% THC level, Dr. Ernest Small, Principal Research Scientist at the Eastern Cereal and Oilseed Research Centre, in Ottawa, a section of Agriculture & Agri-Food Canada (AAFC), the Canadian federal government ministry of agriculture, commented that:
“this was simply a figure derived for taxonomic classification purposes to address infraspecific variation by recognizing just two groups – one obviously reflecting historical selection for “narcotic” kinds and the other historical selection for fibre kinds. However, while medical or risk considerations were not originally consid-ered in deriving the 0.3% level, it can be assumed that legislators and regulators adopting this criterion were more or less aware that a figure of 0.3% THC in the upper third of female plants was related to the practical level of 0.9% THC often considered minimal in marijuana to produce marketable marijuana (obviously a much higher level is required today), and that for practical purposes the figure of 0.3% was reasonable for allowing the industrial hemp industry to develop while controlling the narcotic industry.”
(Ernest Small, Private communication 2014)
Dr. Small also pointed out that “the THC level in plants should not be a critical con-sideration when the level in seed oil and seed oil products is in fact the critical issue for regulatory concern” (Ernest Small, Private communication 2014).
Canada emerges as a growing influence on global hemp production and trade, with an estimated plantation area of 43,911.52 ha in 2014 (Hermann 2015). This is an increase of 40% in surface area since 2013. Canada is estimated to have more than 50,000 ha of land used for hemp plantation by 2015 (Hempro International 2014).

3 THC Guidance Values and Regulations around the World
nova-Institute 28 THC Guidelines for Food
Under the leadership of the Canadian Hemp Trade Alliance (CHTA) regulatory re-view committee, the CHTA has asked for derivate testing to be eliminated.
3.2.2 USA
The United States has no regulations on THC in hemp foods. Technically, “zero-tolerance” (0% THC) is expected on imported hemp goods. However, products with proper HS codes are allowed to be imported, including those under the Canadian 10 ppm (0.001%) legislation.
Furthermore, the industry has established its own standards that are voluntary but have been widely adopted. The goal was primarily to avoid any issues with drug test-ing and false positives for cannabis. For this effect, in the early 2000s several North American companies got together to create “Test Pledge”, a voluntary regulatory agreement created by members of the industry. Pledge companies have made a com-mitment to implement quality control measures which limit the amount of trace resid-ual THC in hulled hemp nuts and oil, thus eliminating the risk of positive drug tests. Producers and processors of hemp oil and hulled hemp nuts must commission THC tests on each and every lot of hulled hemp nuts and oil, performed by a properly ac-credited laboratory following the official Health Canada protocol. All TestPledge dis-tribution and/or manufacturing companies downstream must obtain and keep copies of THC tests on each and every lot of hulled hemp nuts and oil that is bought, used and/or sold. It only covers hulled hemp nuts and hemp oil, as these are currently the most commonly consumed hemp products in the US market. Even Test Pledge prod-ucts containing 10 ppm or less have not caused employees to fail workplace drug tests; they have been allowed to be imported as a product and so the limit is seen somewhat as a reference. Higher THC values would still be accepted on the market and are commonly traded, with no known problems to the consumer.
The Drug Enforcement Agency (DEA) and Office of National Drug Control Policy (ONDCP) attacked hemp food and cosmetics, mainly on the thin pretext that such products interfere with their campaign to eliminate the use of psychoactive cannabis. Until 1998, when thoroughly cleaned seeds from Canada and the European Union became widely available, hemp oil containing more than 50 ppm of THC was often found in the market.
A study by a Canadian governmental research program (ARDI) and members of the hemp industry found that none of the 15 individuals who consumed up to 600 µg of THC per day were even close to producing a urine sample that was "confirmed posi-tive". This and similar findings have not kept the federal government from using past drug-test interference problems as a pretext to harass the hemp industry, particularly as other food goods, such as poppy seeds, are not pressured despite the fact that these may well interfere with current narcotics drug-testing.
Based on scientific research TestPledge requires that pledging companies achieve and commit to the following THC guidance values:
Hemp oil: 5.0 mg/kg
Hulled hemp nuts: 1.5 mg/kg
The more stringent THC limit in hulled hemp nut compared to oil was set because hulled hemp nuts are more palatable and may be eaten in larger quantities. THC guid-
3 THC Guidance Values and Regulations around the World
nova-Institute 29 THC Guidelines for Food
ance values for TestPledge were set low enough to allow for the extensive daily con-sumption of both hemp oil and hulled hemp nuts without any problems.
Production, transformation, and import of viable hemp seed or grain remain some-what restricted in the United States, where focus is usually on non-viability of import-ed seeds.
Although growing industrial hemp in the US is not strictly illegal, it requires a permit granted by the DEA to import viable hemp seed or grain and a state license to culti-vate in accordance with Sec. 7606 of the US Farm Bill of 2014. New federal legisla-tion has been put forward in order to provide states the right to manage the cultivation and regulating of hemp production.
Any product containing any quantity of THC or other cannabinoids, unless exempted by the Drug Enforcement Agency (DEA), is considered a schedule 1 drug under the US Controlled Substances Act (CSA). Exceptions are also made for goods listed in another schedule based on FDA-approved medical use. DEA exempted products are all hemp items that do not result in THC entering the human body: paper, rope, cloth-ing, animal feed mixtures, soaps and shampoos.
(Hermann 2014; HIA 2015; TestPledge 2014)
3.2.3 Australia and New Zealand
THC regulation in both Australia and New Zealand falls under the responsibility of Food Standards Australia New Zealand (FSANZ). Despite some state regulatory dif-ferences, Ministerial levels in both countries work very closely with regard to food standards.
Hemp foods are not permitted for human consumption in Australia and New Zealand under laws regulated by FSANZ: Standard 1.4.4 – Prohibited and Restricted Plants and Fungi in the Australia New Zealand Food Standards Code. The Code prohibits all species of cannabis from being added to food or sold as food in Australia and New Zealand. Hemp oil is the only exception, which has been permitted in NZ since 2002 under New Zealand Food (Safety) Regulations. Previous attempts to change the code to remove hemp from the list of Restricted Plants and Fungi have failed, including an application in 2002 cosponsored by the company Hemp Foods Australia. (http://www.foodstandards.gov.au/consumer/generalissues/hemp/Pages/default.aspx)
In 2012, FSANZ recommended that hemp be approved as a food source. The FSANZ report stated that:
“It was satisfied that low THC Hemp foods are safe for consumption when they con-tain no more than specified maximum levels (MLs) of THC. Foods derived from Hemp seeds may provide a useful dietary source of many nutrients and polyunsaturat-ed fatty acids, particularly omega-3 fatty acids. Hemp Foods have no psychoactive properties and therefore could not be detectable in drug tests. Hemp grows distinctive-ly different to Marijuana and would easily be detectable by drug enforcement agen-cies.” (Hemp Foods Australia 2014)
Standard 1.4.4 has been variously granted exceptions to certain Cannabis sativa seeds and products. Although illegal, they may be purchased to add to food if they contain 5 mg/kg of THC, “which is naturally present”, non-viable and hulled. Other products

3 THC Guidance Values and Regulations around the World
nova-Institute 30 THC Guidelines for Food
allowed in both countries and derived from hemp have different limits according to clause (2) of the document, and can be summarized as follows:
Table 9 THC guidance values in foodstuffs in Australia and New Zealand Food product THC guidance value (mg THC/kg) Seeds 5 Oil 10 Beverages 0.2 Any other substance extracted or derived from seeds
5
It is important to note that Cannabis sativa is allowed to contain no more than 0.5% THC in the leaves and flowering heads of the plants.
The NZ Ministry of Health has no health concerns about hemp seeds in food because hemp seeds do not contain any THC and are not psychoactive. The Ministry of Agri-culture and Forestry (MAF) agrees that the generic nutritional composition of low THC Cannabis sativa looks quite appealing as it has the potential to offer an alterna-tive source of alpha-linolenic acid in the food supply. (MAF 2011)
A proposal to change the current regulation was up for consideration at a meeting of the Forum in late January 2015.


3 THC Guidance Values and Regulations around the World
nova-Institute THC Guidelines for Food 32
3.3 Conclusion
Currently, only a few countries in Europe have established limits or guide values for THC in food goods. Due to the lack of Europe-wide control, some member states have taken it upon themselves to draw guidelines for food products containing THC. The Swiss case, with the highest limits recorded and solely aiming to avoid psychotropic effects, is an ex-ample of the upper boundaries currently applied in Europe. Due to the impossibility of completely excluding liability by guidance values, the Swiss limits are considered by the industry as an acceptable government approved alternative to any guidance values. The Netherlands is another country that stands out for its lack of regulation. Its liberal approach to THC-containing products may be a consequence of its recreational use market, a factor that is unique to this country.
On the other side of the spectrum are countries that expect a zero tolerance approach, alt-hough, practically speaking, this is rarely enforced.
Both the UK and Belgium judge food goods containing THC on a case-by-case basis, with the latter judging against its own THC limits.
The German threshold in food, commonly consulted as a non-binding reference, is the most widely used, regardless of its relatively conservative nature. The German Ministry of Health has demanded a “joint regulation for THC limits” at the EU level. However at the intra-national level, progress has been slow (Hellwig 1998).
Canada is unique in its THC limitations on hemp products due in that they are applied across the spectrum of raw and semi-finished hemp products with a single value: 10 ppm. The Canadian THC limits have proved their value in practice. On the one hand, producers have been able to comply with them through proper manufacturing practices. On the other hand, no incidents of side effects due to the consumption of hemp-based food have hitherto occurred following the adoption of the THC limit. This unique set of limits has stimulated a growing sector, revitalizing rural areas, and was expected to grow at a rate of 25% in 2013 alone (Department of Agricultural Economics, University of Kentucky, 2013; Hempro International 2014).
The United States, in contrast, has no regulations on THC in hemp foods. Technically, 0% or no THC is expected for hemp goods. The industry, however, has established its own standards that are voluntary and have been widely adopted. The goal was primarily to avoid any issues with drug testing and false positives for marijuana.
Finally, Australia and New Zealand have put in place regulations that are a direct result of the drug policy in these countries. In an attempt to limit the usage of drugs, restrictions were applied to both narcotic and non-narcotic cannabis products. Although certain limita-tions have been relaxed, hemp food goods remain a constrained market. Nevertheless, Ministries and Food Standards alike seem willing to promote a change to the current re-strictions.
This report continues by presenting the most recent call for the introduction of THC legis-lation, a case study of THC-rich milk products that entered the European single market from Switzerland. As we have just seen, Swiss THC limits for growing hemp are higher than those in the EU, making most Swiss hemp farmers non-compliant with EU hemp norms. With a lack of appropriate restrictions and regulations in the EU market for hemp

3 THC Guidance Values and Regulations around the World
nova-Institute THC Guidelines for Food 33
food goods, any food products processed from Swiss hemp will result in higher THC con-centrations than those in the EU.
After analysing the different policies presented above, this paper will opt to use the Ger-man guidelines, considered the most sound and consistent on the subject matter by many European nations. This allows for a scientifically reasoned THC amount in food goods, maintaining the safeguard of the public in mind. By applying guidance values in THC-containing hemp foods to an average per capita consumption of different food goods, the German guidelines bridge the industry’s and the consumer’s interests alike. This method-ology will be instructive to the European-wide guidelines proposed by this paper.

4 EFSA feeding issue
nova-Institute THC Guidelines for Food 34
4 EFSA feeding issue
4.1 Background
In the early 2000s, it came to the attention of the public that Swiss farmers had been feed-ing their cows flowers from cannabis plants containing high amounts of THC. The fibre hemp grown in Switzerland is subject to high THC limits and hence a lot of the traditional cultivars and varieties contained considerable amounts of THC. In fact Switzerland had been the only European Country where the cultivation of high-THC hemp was allowed and not further regulated. On February 3rd 2004, the local newspaper “La Broye” published an advert depicting a boy holding a bottle of milk. The text said “since my dad feeds hemp to the cows, my milk tastes even better” (NZZ 2005).
The advert was run by a company called SanaSativa, which was said to have around 60 Swiss farmers on its books (NZZ 2005). The Swiss authorities felt the need to check the claims and recognized that milk from cows fed with cannabis flowers could contain THC. The mandate to check THC levels in milk was given to Agroscope, the Swiss Federal Re-search Institute for Animal Production and Dairy Products. A literature review found a Pakistani study that had detected traces of a metabolite of THC in milk from buffalos that were fed wild hemp (Ahmad and Ahmad 1990). The non-hallucinogenic metabolite was found in 5 milk samples of the 10 animals tested. Additionally, a separate test presented by Agroscope found traces of THC in Swiss cows’ milk. The study dated back to 1998, in which pills with 625 mg pure THC were fed to cows, leading to milk with 0.017 mg THC per litre, 23 hours after dosing. Daniel Guidon, head of the department for security and quality, considered the findings enough to propose a ban of hemp as fodder to the Federal Assembly reasoning that not the amount of THC in milk but the perception of THC in so-ciety was crucial (NZZ 2005).
Restrictions were introduced on cultivable varieties, the last one to be banned being 'Fédo-ra 17'. To maintain a certain flexibility for farmers to breed new strains the limit was set at 1% THC.
Barbara Früh, fodder expert for Bio Suisse, the Swiss umbrella group for organic organiza-tions, stated that the scientific foundations for banning hemp from fodder were rather "lean". The 15-year-old Pakistani test was done with cannabis that contained high THC values, which is not considered hemp under EU regulations. She added that a better solu-tion would have been for both the Pakistani and Swiss case studies to undertake tests with hemp fodder containing a low amount of THC (NZZ 2005).
Additionally, farmers claimed that animals showed signs of better health and higher yield when fed cannabis plants, with most farmers also claiming it made the feeding process more affordable (NZZ 2005; BBC 2005). These claims were supported by SanaSativa, who added that the ban was not sufficiently supported by scientific research and therefore ille-gal (SanaSativa 2005). If confirmed, some of these claims could result in the drastic reduc-tion of antibiotic intake by cattle, one of the main causes of the development of antibiotic-resistant bacteria (WHO AMR 2014).
According to EU standards, none of plants in question are industrial hemp plants as their THC content exceeded the EU norm of 0.2%. Therefore, EIHA believes the results from these feeding regimes should not be related to animal feed derived from industrial hemp in the European Union.

4 EFSA feeding issue
nova-Institute THC Guidelines for Food 35
4.2 EFSA 2011 report
Nevertheless, a detailed risk assessment with regard to the risks for human health in rela-tion to the presence of THC in milk and other food of animal origins was requested by the European Commission and was performed by EFSA’s Panel on Contaminants in the Food chain (CONTAM) in 2011.
EFSA’s Panel on Additives and Products or Substances used in Animal Feed (FEEDAP) adopted a scientific opinion on the safety of hemp (cannabis genus) for use in animal feed:
– “EFSA Panel on Additives and Products or Substances used in Animal Feed (FEEDAP); Scientific Opinion on the safety of hemp (cannabis genus) for use as animal feed. EFSA Journal 2011, Vol. 9(3):2011. [41 pp] doi: 10.2903/j.efsa.2011. 2011. Availa-ble online: http://www.efsa.europa.eu/en/efsajournal/doc/4058.pdf - last accessed April 10, 2015].“
In spite of several of the different human exposure scenarios considered showing estimated exposure higher than the established PMTDI (Provisional Maximum Tolerable Daily In-take) of 0.4 µg/kg body weight, the conclusion was that, with regard to these previous find-ings, it is appropriate to consider the need to establish possible maximum levels for THC in milk and other food of animal origins in the framework of Council Regulation (EEC) No. 315/93 of February 8th 1993, which lays down Community procedures for contaminants in food. For that purpose a detailed risk assessment regarding the risks to human health in relation to the presence of THC in milk and other food of animal origins has been request-ed by the European Commission and will be performed by EFSA’s Panel on Contaminants in the Food chain (CONTAM).
The Terms of Reference of the Commission request were as follows:
In accordance with Article 29 (1) (a) of Regulation (EC) No. 178/2002, the Commission asks EFSA for a scientific opinion on the risks to human health related to the presence of THC in milk and other food of animal origins.
The scientific opinion should, inter alia, comprise the:
Evaluation of the toxicity of THC for humans, considering all relevant adverse acute and chronic health effects.
Estimation of the dietary exposure (chronic and acute dietary exposure) of the EU popula-tion to THC from milk and other food of animal origins, including the consumption pat-terns of specific (vulnerable) groups of the population (i.e. those with higher consumption, (young) children, pregnant women).
Assessment of the acute and chronic human health risks as the consequence of the presence of THC in milk and other food of animal origins, with particular attention to specific (vul-nerable) groups of the population (i.e. those with higher consumption, (young) children, pregnant women).
EFSA’s Panel on Additives and Products or Substances used in Animal Feed (FEEDAP) adopted a scientific opinion on the safety of hemp (cannabis sp.) for use in animal feed. EFSA suggested to put whole hemp plant-derived feed materials on the list of materials whose placing on the market or use for animal nutritional purposes is restricted or prohibit-

4 EFSA feeding issue
nova-Institute THC Guidelines for Food 36
ed and to introduce a maximum THC content of 10 mg/kg to hemp seed-derived feed ma-terials.
This suggestion was based on a LOEL (lowest observed effect level) of THC in humans of 0.04 mg THC/kg body weight (bw). By applying an uncertainty factor of 100, a PMTDI (provisional maximum tolerable daily intake) of 0.0004 mg/kg bw was derived.
Although the European Industrial Hemp Association (EIHA) welcomes the establishment of guidelines for THC concentrations in food and feed by the European Commission, EI-HA rebutted the values provided by EFSA in a statement released in May 2011. The publi-cation refused EFSA’s arguments on the basis that they were derived solely from animal studies.
“Toxicological data from animal studies can help to elucidate the toxicity of cannabinoids in humans. However, comparison of the data from studies on humans and animals reveals often considerable inconsistencies”.
Therefore, it suggested that, “wherever possible, a quantitative risk assessment should be based on data from human studies” (EIHA statement 2011).
EIHA refuted the notion that an uncertainty factor of 100 was indeed necessary. The value attempts to account for the differences between test animals and humans (factor of 10) and possible differences in sensitivity between humans (another factor of 10). However, EIHA believes that there are enough human-based studies on the effects of THC for an interspe-cies factor not to be needed and that most of the references on differences in human sensi-tivity lacked updated scientific knowledge.
Furthermore, EIHA did not see much scientific basis for a maximum tolerable daily intake to be provisional (PMTDI) since the toxicology of THC is very well investigated in hu-mans, compared to other toxins.
Usually, technical cleaning processes, commonly used processes for grain cleaning, direct-ly lower the total THC on the outer seed shell. By comparison, the Swiss fed their cows “hemp pellets”, which were actually produced from drug Cannabis, rather than non-drug Cannabis (i.e., hemp). These pellets had a total THC content ranging from 0.65% (or 6.50 mg/kg) to 1.7% (or 17.0 mg/kg), which is not within the legal definition of hemp in the EU. The drying process and pressure that was used to make these pellets certainly caused some transformation of THCA into THC. THC was, then, metabolized and detected in the cows’ milk. . In another experiment, pure THC was fed to cows, within also produced THC metabolites that were detected in the cows’ milk. This, however, would not have been the case if initial THC contents had been kept under EU regulations (0.2%) by using actual hemp. In the fresh plant, about 90% of the total THC is actually THCA and the can-nabinoid acid of THC (or THCA) are devoid of psychotropic effects (Dewey 1986). The typical ratio will range from 1:9 to 1:17 (Pitts 1992) in fresh plants, with 1:>20 registered in some cases, like Switzerland (Brenneisen 1984). So, animals that are fed fresh hemp (stalks, leaves, flowering seed heads, etc.) will mostly receive THCA and very little THC. This would mean very low (if any) amounts of THC in the animal and animal products. The production of THC from THCA is mainly a function of time. Increasing temperature, pressure or light by processing raw materials from hemp will also increase the production of THC from THCA.
The fact that in fresh, unheated hemp most of the total THC is still THCA is of crucial im-portance, as THCA is neither psychotropic nor is it converted into THC or other psychoac-tive metabolites in vivo. This is the case in both humans and animals (Wohlfahrt 2012;

4 EFSA feeding issue
nova-Institute THC Guidelines for Food 37
Jung et al. 2009). Considering the low percentage of total THC (sum of THCA and THC) available as THC, fresh hemp should not pose a problem as neither food nor feed.
4.3 Latest activity
After the first statement by EFSA, in 2011 and above presented, the European Commission insisted on having a second more detailed and expanded statement, due in 2015.
EFSA has contacted EIHA, along with other stakeholders, to gather information concern-ing THC metabolic conversion in live stock animals and the market structure of hemp in Europe, in particular with regard to feed and food. EIHA provided EFSA with this infor-mation on the 10th of October 2014.
In November 2014 a document containing the lab results of 50 samples of hemp food goods analysed for THC were provided to EFSA by EIHA.
At the date of printing of this paper, no further communication had taken place on this top-ic between the agency and the association.
With the last information gathered by EFSA in October/November 2014, the agency pub-lished its newest report in June 2015. The paper’s main focus is on metabolization of THC by cattle fed hemp feed, and its potential transfer to milk and meat. The document also suggests an uncertainty factor for THC of 30 and a LOEL of 2.5 mg of THC per kg (EFSA 2015).
Now that the document published, the Commission will hear stakeholders and other ex-perts to discuss EFSA’s recommendations in autumn 2015.
EIHA brings a contribution to the discussion with this report, with the aim of aiding the Commission in establishing fair and scientifically based THC guidance values in food and feed goods.
4.4 Conclusion
As stated above, the process of establishing European THC guidance values in feed started in 2011 with the European Commission’s request. The action was a consequence of THC being detected in milk of Swiss origin, after cows were fed silage made from drug Canna-bis, and not the EU permitted hemp varieties. Although EIHA welcomes regulation on this issue, it reiterates that the Swiss samples should not be considered hemp, because their high THC content exceeds EU norms.
A new report was published by EFSA in June 2015, after which a hearing in the European Commission is now expected to take place. This paper shares scientific information on the issue of THC in food and feed.
The next chapter of this paper will present a quantitative risk assessment that is based on data from human studies. This will allow for a sound guidance value to be delineated.

5 Literature Review on No Observed Effect Level (NOEL), Lowest Observed Effect Level (LOEL) and Acceptable Daily Intake (ADI)
nova-Institute THC Guidelines for Food 38
5 Literature Review on No Observed Effect Level (NOEL), Lowest Observed Effect Level (LOEL) and Acceptable Daily Intake (ADI)
Concepts such as “No Observed Effect Level (NOEL)”, "Lowest Observed Effect Level" (LOEL) and “Acceptable Daily Intake” (ADI) are commonly applied when developing standards intended to prevent undesired side effects from chemicals that are known, or suspected, to cause such effects. NOEL and LOEL are actual data points from human clin-ical or experimental animal studies. While NOEL is the highest data point at which there was not an effect, LOEL is the lowest data point at which there was an observed effect (Yuill 2015).
Contrary to No Observed Adverse Effect Level (NOAEL) and Low Observed Adverse Effect Level (LOAEL), NOELs and LOELs do not necessarily imply toxic or harmful ef-fects and may be used to describe beneficial or other measurable biological or pharmaco-logical effects of chemicals.
The term Acceptable Daily Intake (ADI) is used to describe safe daily intake of a sub-stance that may be deliberately added to food or an unavoidable residue (Herman and Younes 1999). It is calculate by multiplying the NOEL by an uncertainty factor.
In this paper, the guidance value for THC was not based on toxic effects (No Observed Adverse Effect Level, NOAEL) but on the Lowest Observed Effect Level (LOEL), which is a pharmacological effect. Such effects of THC are described in the literature as tempo-rary, mild to moderate psychomotor- or cognitive effects. These contrasts vastly with ad-verse (toxic) effects, which tend to be severe and chronic, such as neurotoxicity or canceri-genousity.
However, EFSA’S 2011 final proposal concluded that a Provisional Maximum Tolerable Daily Intake (PMTDI), commonly used for contaminants that may accumulate in the body (Herman and Younes 1999), was to be used. THC contrasts sharply with effects of e.g. methyl-mercury, which is neurotoxic and has a half-life ten times longer than THC; yet the TWI of methyl-mercury was set only slightly lower than that of THC (Nahler 2015). Therefore, EFSA labelled the relatively minor to intermediate health effects of THC intake at the same toxicity level as chemical substances like mercury, lead, and bisphenol A, which are known to have long lasting detrimental effects that far surpass those of THC. (See Table 11)

5 Literature Review on No Observed Effect Level (NOEL), Lowest Observed Effect Level (LOEL) and Acceptable Daily Intake (ADI)
nova-Institute THC Guidelines for Food 39
Table 11 Maximum Tolerated Daily Intake of THC proposed by EFSA vs. other sub-stances. Source: Nahler 2015
THC differs from non-specifically acting harmful chemicals in food in that it acts on com-pound-specific binding sites (cannabinoid receptors) on the surface of body cells. THC's mode of action provides an additional safety margin for two reasons:
1. As a rule, for the most harmful chemicals, when toxicity increases, the NOAEL corre-spondingly decreases with the duration of exposure. This fact must be taken into account when determining the safety margin. In the case of THC, however, the opposite applies. The effect of high THC doses decreases with increasing exposure due to the development of tolerance to THC by the receptors. Following the repeated ingestion of low THC doses no changes are expected on cannabinoid receptors, but also no increase of adverse effects.
2. Children are generally considered particularly sensitive to various harmful chemicals. Consequently, higher uncertainty factors are chosen to provide sufficient protection. How-ever, children have a significantly lower density of cannabinoid receptor sites. Thus, com-pared to adults, psychotropic effects occur only at higher THC doses. These assumptions

5 Literature Review on No Observed Effect Level (NOEL), Lowest Observed Effect Level (LOEL) and Acceptable Daily Intake (ADI)
nova-Institute THC Guidelines for Food 40
have been confirmed in clinical studies with THC in children and following the treatment of children with cannabinoid-based medicines.
Furthermore, it used to be the case that the majority of toxicological data for THC resulted from animal studies in which high doses were applied, as well as from cell studies (see Table 13, Chapter 6). For many of the potential health effects of THC, the NOEL and LOEL was found to vary. However, new data of THC effects on humans provides a sound basis for the exclusion of uncertainty with a high safety margin.
Cannabis is one of the most well studied plants on the planet. Yet the information above shows that the influence of THC on human subjects requires a more detailed understanding in order to establish guidance values for consumption guidance. The following chapter will use scientific evidence from research papers in order to adequately extrapolate a Lowest Observed Effect Level and a No Observed Adverse Effect Level. The evidence will be presented from a pharmacological point of view and will aid in understanding the vast and complex knowledge that science currently has on THC effects in humans.
5.1 Pharmacological basis for a Lowest Observed Effect Level (LOEL) and No Observed Effect Level (NOEL)
Several clinical studies, some of them large-scale, have been conducted in the past 10 years with oral THC or oral cannabis extracts with high concentrations of THC, further elucidat-ing the effects of THC in the human body (e.g. Zajicek et al. 2003, 2005; Wade et al. 2004; Rog et al. 2005; Strasser et al. 2006; Collin et al. 2007; Narang et al. 2008; Novotna et al. 2011). These studies add to the existing literature that aims to increase the understanding of THC effects in the human body. Therefore they ought to be used as the basis for the extrapolation of a LOEL and NOEL for THC.
Lucas & Laszlo (1980) found pronounced psychotropic reactions (anxiety, marked visual distortions) in patients undergoing cancer chemotherapy, which had received oral doses of 15 mg THC/m2 of body surface, corresponding to 25 mg THC for an average adult (body surface: 1.7 m2). A reduction to 5 mg THC/m2, about 8-10 mg THC, produced only mild reactions. In a study by Frytak et al. (1984), oral administration of 15 mg THC to 38 cancer patients caused psychotropic effects in 58% while 42% experienced no effects. Brenneisen et al. (1996) administered single oral doses of 10 or 15 mg THC to two patients. Physiolog-ical parameters (heart rate) and psychological parameters (concentration, mood) were not modified by administering THC. The authors suggest a threshold for psychotropic effects of 0.2-0.3 mg/kg bw. In a study with patients suffering from spasticity due to spinal cord injury by Hagenbach et al. (2007) patients tolerated daily doses of 15-60 mg oral THC. In some other cases, a single oral dose of 20 mg of THC caused symptoms like tachycardia, conjunctival irritations, “high feeling” or dysphoria within 1-4 hours in adults. (Lachenmeier and Walch 2005). The highest dose administered to a set of individuals was 210 mg/person/day, given over a period of 25 days. Not all subjects exposed had an Ad-verse Drug Reaction (ADR) to THC (Jones et al. 1976; Freinberg et al. 1975). It is clear, then, that THC has an exceptionally large safety range. However, these were the highest doses administered in experimental settings. The highest doses observed in clinical settings have been much higher, well above 1000 mg THC per day. For example in a study in Ja-maica researchers investigated the effects of cannabis in people consuming 20-30 g of Cannabis material with a mean THC concentration of 4% (Bowman 1973).
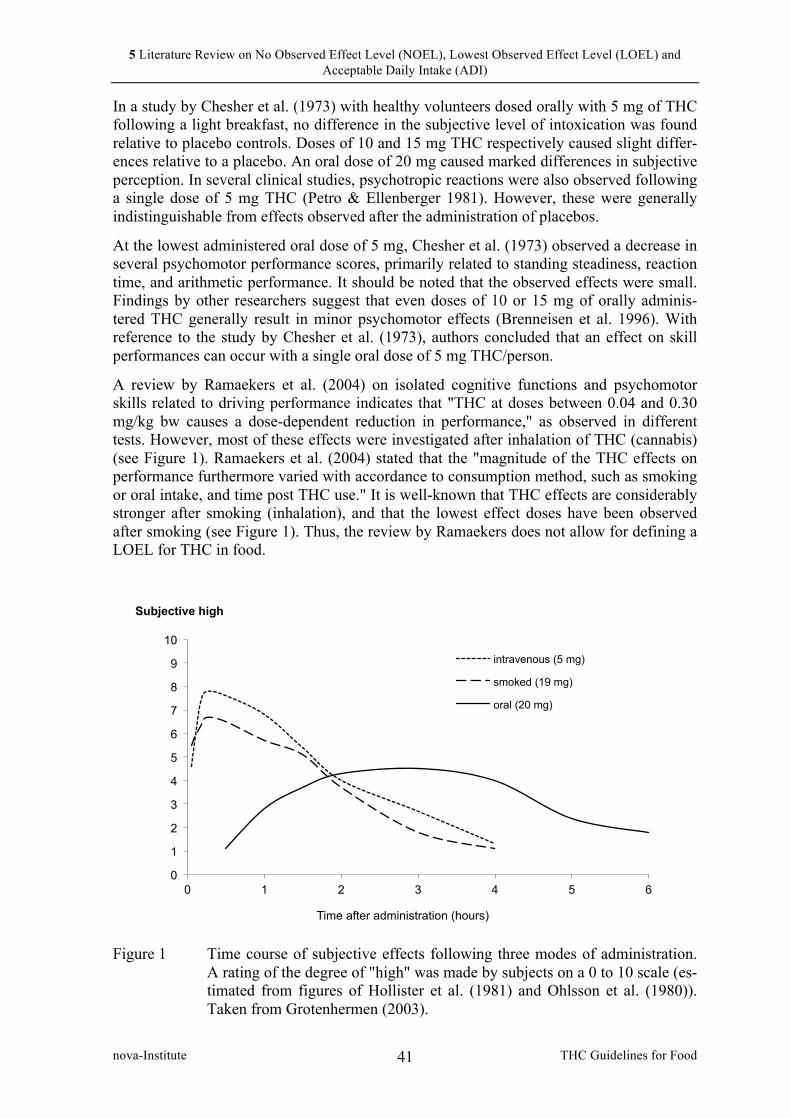
5 Literature Review on No Observed Effect Level (NOEL), Lowest Observed Effect Level (LOEL) and Acceptable Daily Intake (ADI)
nova-Institute THC Guidelines for Food 41
In a study by Chesher et al. (1973) with healthy volunteers dosed orally with 5 mg of THC following a light breakfast, no difference in the subjective level of intoxication was found relative to placebo controls. Doses of 10 and 15 mg THC respectively caused slight differ-ences relative to a placebo. An oral dose of 20 mg caused marked differences in subjective perception. In several clinical studies, psychotropic reactions were also observed following a single dose of 5 mg THC (Petro & Ellenberger 1981). However, these were generally indistinguishable from effects observed after the administration of placebos.
At the lowest administered oral dose of 5 mg, Chesher et al. (1973) observed a decrease in several psychomotor performance scores, primarily related to standing steadiness, reaction time, and arithmetic performance. It should be noted that the observed effects were small. Findings by other researchers suggest that even doses of 10 or 15 mg of orally adminis-tered THC generally result in minor psychomotor effects (Brenneisen et al. 1996). With reference to the study by Chesher et al. (1973), authors concluded that an effect on skill performances can occur with a single oral dose of 5 mg THC/person.
A review by Ramaekers et al. (2004) on isolated cognitive functions and psychomotor skills related to driving performance indicates that "THC at doses between 0.04 and 0.30 mg/kg bw causes a dose-dependent reduction in performance," as observed in different tests. However, most of these effects were investigated after inhalation of THC (cannabis) (see Figure 1). Ramaekers et al. (2004) stated that the "magnitude of the THC effects on performance furthermore varied with accordance to consumption method, such as smoking or oral intake, and time post THC use." It is well-known that THC effects are considerably stronger after smoking (inhalation), and that the lowest effect doses have been observed after smoking (see Figure 1). Thus, the review by Ramaekers does not allow for defining a LOEL for THC in food.
Figure 1 Time course of subjective effects following three modes of administration.
A rating of the degree of "high" was made by subjects on a 0 to 10 scale (es-timated from figures of Hollister et al. (1981) and Ohlsson et al. (1980)). Taken from Grotenhermen (2003).
0
1
2
3
4
5
6
7
8
9
10
0 1 2 3 4 5 6
Subjective high
Time after administration (hours)
intravenous (5 mg)
smoked (19 mg)
oral (20 mg)
5 Literature Review on No Observed Effect Level (NOEL), Lowest Observed Effect Level (LOEL) and Acceptable Daily Intake (ADI)
nova-Institute THC Guidelines for Food 42
With regard to repeated exposure of THC, two studies by Beal et al. (1995, 1997) have been referenced in which HIV patients received oral THC. The first study was a placebo controlled study with 139 patients who received either THC (2 x 2.5 mg/person daily) or a placebo for 42 days (Beal et al. 1995). The second study was an open, long-term study where patients received THC for 12 months (Beal et al. 1997). In the first study 25 of the 72 patients (about 35%) experienced effects. In the long-term study similar effects were observed. However, an open clinical study is not very useful for assessing psychotropic effects of THC since similar effects may be observed after placebo.
For instance, Strasser et al. (2006) investigated the effects of THC (2.5 mg twice daily) in cancer patients in a placebo controlled three-arm study with THC, a cannabis extract and a placebo. 243 patients were randomly assigned and 164 completed the six-week trial. In contrast to the study by Beal et al. (1995) with HIV patients, who received the same dose for the same period of time, no differences were observed between THC and placebo for THC-related effects. Thus, a THC dose of 2.5 mg twice daily may usually be regarded as a placebo dose concerning THC effects.
Later clinical studies abandoned the principle of administering fixed doses to patients in clinical studies, since only very few patients experience effects at a dose of 2.5 mg THC twice daily. Instead controlled clinical studies apply the principle of titrating the dose up to an individual effective dose.
The largest clinical study ever conducted with THC was a 15-week three-arm study on THC, a cannabis extract and placebo in patients with multiple sclerosis (Zajicek et al. 2003). Patients were offered the possibility to continue into a 12-month follow-up study, which was also a double-blind placebo-controlled study (Zajicek et al. 2005). In the short-term study 611 patients were evaluated; the long-term study evaluated 502 patients. In the short-term study doses were slowly increased up to the occurrence of side effects or until the maximum dose (10-25 mg THC/day depending on body weight) was reached. The maximum dose was 10 mg for participants with a body weight below 50 kg and 25 mg for those with a body weight above 89 kg. Mean daily doses after the dose finding phase for participants with a body weight of 50-69 kg was 11.5 mg (or 0.17-0.23 mg/kg bw) and for participants with a body weight of 70-89 kg 15.8 mg (or 0.18-0.23 mg/kg bw). Thus, mean daily tolerable doses were about 0.2 mg THC/kg bw.
Compared to the short-term study the long-term therapy with THC over a course of 12 months resulted in a dramatic reduction of adverse effects (Table 12). This may be due to the development of tolerance for some symptoms and the establishment of an individual tolerable dose for every patient. In the short-term study, doses were slowly increased until side effects appeared or the maximum daily dose was reached. Since several participants experienced psychotropic effects before reaching their maximum daily dose side effects were observed frequently. However, they were usually mild or moderate in intensity (Zajicek et al. 2003). In the long-term study by Zajicek et al. (2005) the incidence of side effects was no longer higher in the verum groups (THC and cannabis) compared to the placebo group except for the events "dizzy or light headedness" and "falls" (Table 12). In studies with THC taken by patients with HIV, similar observations of a reduction in fre-quency of side effects were made. While about 25% of patients reported a minor CNS-related adverse drug event during the first 2 weeks, only about 4% reported such an event during each of the following six weeks (Marinol prescribing information 2011).

5 Literature Review on No Observed Effect Level (NOEL), Lowest Observed Effect Level (LOEL) and Acceptable Daily Intake (ADI)
nova-Institute THC Guidelines for Food 43
Table 12 Side effects in the studies by Zajicek et al. (2003, 2005). Mean daily doses: about 0.2 mg/kg bw (see text for detailed information). Daily doses were 10-15 mg THC.
Adverse event Short-term study
(15 weeks)
Long-term study
(52 weeks)
THC Canna-bis
Placebo THC Canna-bis
Placebo
Dizzy or light-headedness 59% 50% 18% 8% 10% 2%
Sleep 35% 40% 33% 8% 8% 9%
Spasms or stiffness 34% 33% 33% 14% 15% 14%
Gastrointestinal tract 30% 37% 20% 9% 12% 7%
Miscellaneous 28% 30% 22% 7% 7% 7%
Pain 26% 24% 32% 10% 17% 10%
Dry mouth 26% 20% 7% 2% 1% 1%
Weakness or reduced mobility 25% 23% 20% 10% 12% 16%
Bladder 24% 26% 23% 10% 12% 15%
Infection 15% 16% 17% 9% 11% 11%
Tremor or lack of coordination 12% 10% 8% 5% 2% 2%
Depression or anxiety 10% 9% 8% 6% 6% 5%
Numbness or paraesthesia 9% 7% 7% 5% 4% 4%
Vision 6% 8% 2% 2% 2% 0%
MS-relapse or exacerbation *) - - - 5% 6% 6%
Falls *) - - - 4% 7% 3%
Memory or concentration *) - - - 2% 2% 1%
Other skin problems *) - - - 1% 5% 6%
Pressure sores *) - - - 0% 1% 3%
*) Not measured in the short-term study
Further clinical studies refer to the cannabis extract Sativex®. It has been approved as a medicinal drug in the UK, Spain, Germany, France, Canada, Denmark, Norway, Israel, Austria, Poland, Sweden, Italy, Finland, Switzerland and several other countries. CBD, another cannabinoid that is found in hemp, is known to reduce mainly psychological and psychomotor THC adverse effects. This is the reason why Sativex® has a 1:1 ratio of THC and CBD. One spray of the cannabis spray Sativex® contains 2.7 mg THC and 2.5 mg CBD, since this dose is expected to cause some effects in only very few patients. No ef-fects are expected below this dose and people usually experience some effects only after

5 Literature Review on No Observed Effect Level (NOEL), Lowest Observed Effect Level (LOEL) and Acceptable Daily Intake (ADI)
nova-Institute THC Guidelines for Food 44
higher doses (several sprays of the extract). In clinical practice physicians usually start with 1x1 (once daily), 2x1 (morning and evening) or 3x1 sprays (morning, lunch time, evening) corresponding to 2.7, 5.4 and 8.1 mg THC a day, respectively, which is increased thereafter up to the effective and tolerated dose (Koehler 2014).
In a large study with advanced cancer patients, researchers intended to evaluate the analge-sic efficacy and safety of Sativex® (Portenoy et al. 2012). Patients received either 1-4 sprays, 6-10 sprays or 11-16 sprays of Sativex® per day. 263 patients completed the study. Adverse events were dose-related and only the high-dose group receiving 29.7-43.2 mg THC (11-16 sprays with 2.7 mg THC each) compared unfavourably with placebo.
Medical use of THC is well tolerated over months and years. For example, Rog et al. (2007) conducted an open-label extension study following a controlled study with Sa-tivex® in patients suffering from neuropathic pain. The mean duration of open-label treat-ment was 463 days (median, 638 days; range, 3-917 days). In the 34 patients of this study reaching one year of treatment the mean number of sprays was 7.5 corresponding to 20.25 mg THC. Most patients experienced an adverse effect, which was usually mild even at higher doses, and overall the medication was well tolerated. In another long-term study with 161 patients mean treatment exposure was 334 days and patients on average sprayed 7.3 times per day (=19.71 mg THC) (Serpell et al. 2013). The authors noted that “no new safety concerns were identified with chronic Sativex® treatment, and serious AEs [adverse effects] were uncommon.” In another long-term study with Sativex® researchers conclud-ed: “Even after more than 2 years of use, no new safety/tolerability signals have emerged with Sativex®” (García-Merino et al. 2013).
In a study investigating driving ability of multiple sclerosis patients, participants received a mean dose of 5.1 sprays per day corresponding to 13.77 mg THC (Freidel et al. 2014). The authors concluded from their research: “Treatment of MS patients with Sativex® does not negatively impact driving ability and may improve moderate to severe treatment-resistant MS spasticity.”
5.2 Conclusion
According to the analysed literature, upwards of 15 mg THC for an average adult could be considered a high dosage, following the findings of Lucas & Laszlo (1980). High dosages involved pronounced psychotropic reactions in patients that had received the correspond-ing amount to 25 mg THC oral doses (Chesher et al. 1990) and participants experiencing marked differences in subjective perception after an oral dose of 20 mg.
Usually, single doses of 5-15 mg THC cause mild psychotropic effects (Lucas & Laszlo 1980; Petro & Ellenberger 1981; Chesher et al. 1990; Brenneisen et al. 1996; Brenneisen et al. 1996).
An acute dose of 2.5 mg THC (corresponding to 0.035 mg/kg bw assuming a body weight of 70 kg) may usually be regarded as a placebo dose, albeit this dose rarely may cause mild psychotropic or psychomotor effects in humans such as ‘light-headedness’. These effects tend to decrease with time, as the body builds up a tolerance to THC (Zajicek et al. 2003 and Zajicek et al. 2005). The method of administration causes direct variations in the inten-sity of the effects (Figure 1).
The effects of a single dose of THC typically last anywhere between 4-6 hours, some last-ing up to 8 hours after consumption in extreme cases (Lachenmeier and Walch 2005; Fig-

5 Literature Review on No Observed Effect Level (NOEL), Lowest Observed Effect Level (LOEL) and Acceptable Daily Intake (ADI)
nova-Institute THC Guidelines for Food 45
ure 1). Assuming that an average human being sleeps 8 hours a day, 16 hours of the day are spent awake. Thus, the ingestion of an oral dose of 2.5 mg of THC twice per day, equivalent to 5 mg taken over the course of a 24-hour period (or 16 waking hours), repre-sents a safe LOEL for any reduction in human performance to be felt as a consequence of THC consumption. The following chapter takes into account human biological diversity with regard to THC reaction, in order to establish a safe uncertainty factor.

6 THC effects on human biological variations
nova-Institute THC Guidelines for Food 46
6 THC effects on human biological variations
For several reasons, some humans may be more prone to suffer from THC side effects. Some subjects, such as children or pregnant women, are particularly vulnerable to general substances in food. Others may be carriers of genetic variations that could be responsible for undesired THC intolerance. Therefore, an appropriate scientific understanding of the effects of THC in vulnerable humans is crucial for extrapolating a safe uncertainty value to apply to the recommended THC guidance values. The following chapter will address this problem with new data on children, neonates and foetuses, along with genetic variations within the human population that may be responsible for undesirable THC effects. Finally, this chapter will present evidence why animal tests with THC are not a good source of sci-entific information for the determination of a scientifically sound uncertainty factor.
6.1 Sensitivity of children, neonates and foetuses
Children are considered particularly sensitive to many harmful chemicals. Consequently, higher uncertainty factors are defined to provide adequate protection. However, clinical studies have indicated that children are less sensitive to the effects of THC (Dalzell et al. 1986; Abrahamov et al. 1995). Two long-term longitudinal studies on children who were exposed to high levels of THC in utero, followed these children into adolescence and be-yond and examined effects of the exposure on cognitive and other performance (Porath et al. 2005; Goldschmidt et al. 2012). Both studies found subtle effects of cognitive perfor-mance, mainly on executive function, in later childhood and adolescence.
One study on cannabinoid receptor (CB-R) density (Glass et al. 1997) found a similar re-ceptor density in the human foetus and children compared to adults. However, other re-searchers have found that CB-R density increases fivefold from birth to adulthood in rats (Belue et al. 1995). In yet another study, low numbers of CB-R could be observed as early as the 14th week of gestation in humans (Biegon & Kerman 2001). CB-R density increased slowly but did not reach adult levels by the end of the 24th week.
Glass et al. (1997) found that foetal and neonatal human brains show patterns of CB-R distribution similar to those observed in the adult human brain. They found a similar densi-ty in several parts of the brain (neocortex, cerebellum) and a greater density in children in other parts (midbrain, basal ganglia). However, the authors admit some limitations of their study: “Due to the small numbers of cases available for the study, it is not possible to draw any definitive conclusions on the precise levels of CB-R binding within the developing brain. Also, since the foetal/neonatal and adult tissue was not processed together, consider-able care must be taken in comparing the results of the foetal/neonatal studies with the re-sults in the adult brains” (Glass et al. 1997).
Rodriguez de Fonseca et al. (1993) also found an increase in CB-R binding in rats between birth and day 30, this time followed by a slight decrease until adulthood (day 60 and later). Another group (McLaughlin et al. 1994) found that CB-R messenger ribonucleic acid (mRNA) is present at adult levels as early as postnatal day 3, while CB binding increased almost 50% with increasing age. The last study may explain some of the contradictions between the different studies since CB-R density may be high in infants and children while CB-R activity may be low.
With regard to studies on humans, Biegon & Kerman (2001) investigated the pre- and postnatal distribution of human brain CB-R type 1 using quantitative autoradiography with
6 THC effects on human biological variations
nova-Institute THC Guidelines for Food 47
[(3)H]CP55,940 as a ligand. Normal foetal brains (N = 8, gestational age 14-24 weeks) were obtained from voluntary abortions and were compared with normal adult human brains (N = 16, age 18-78). In the foetal human brain, low densities of THC-displaceable, region-specific binding could be observed as early as 14 weeks gestation. Receptor density increased slowly with gestational age but did not reach adult levels by the end of the se-cond trimester (24 weeks gestation). In addition, the distribution pattern in the foetal brains was markedly different from the adult pattern. The most striking difference was the very low density of binding in the foetal caudate and putamen. In contrast, the globus pallidus pars medialis has almost-adult levels of CB-R by 17-18 weeks gestation. The authors con-cluded, "The relatively low and regionally selective appearance of cannabinoid receptors in the foetal human brain may explain the relatively mild and selective nature of postnatal neurobehavioral deficits observed in infants exposed to cannabinoids in utero."
Furthermore, other clinical studies have shown that children tolerate much higher doses of THC than adults before side effects become significant (Dalzell et al. 1986; Abrahamov et al. 1995). In one study, eight children aged 3 to 10 who underwent chemotherapy orally received 18 mg delta-8-THC per square meter of body surface four times daily. Each child received an average of 60 doses, which caused only mild psychotropic side effects in two children and none in the other six. Thus, children with a body surface of 1.0 m2 received 18 mg THC four times daily. Assuming a body surface of 1.7 m2 for an adult, this corresponds to single doses of 30 mg and a daily dose of about 120 mg THC. Delta-8-THC is assumed to be somewhat less psychotropic than delta-9-THC, with a relative potency of approxi-mately 65% (Hollister & Gillespie 1973). Thus, a single 30 mg delta-8-THC dose corre-sponds to about 23 mg of delta-9-THC, a dose at which adults usually experience consid-erable psychotropic effects. Authors suggest that the lower CB-R type 1 density in children compared to adults may be responsible for the lower susceptibility of children to THC.
According to case reports of the Centre for Palliative Medicine and Paediatric Pain Thera-py of Saarland University (Germany), THC is an effective and well-tolerated medication in the treatment of different severe illnesses in children (Gottschling 2011). All children re-ceived a slowly increased dose starting with 0.1 mg/kg bw, which efficiently avoided ad-verse effects. Mean the THC dose was about 0.2 mg/kg bw in children suffering from spas-ticity and pain after finishing dose finding.
As a rule, with regard to pregnancy, foetuses tend to be particularly susceptible to toxins. In both humans and animals, transfer of THC to the vascular system of the foetus occurs across the placenta. The time course of the THC-concentration in foetal blood is strongly correlated to that of maternal blood, though foetal plasma concentrations were found to be lower compared to the maternal level in rats (Hutchings et al. 1989), in sheep (Abrams et al. 1985–1986), in dogs (Martin et al. 1977), and in monkeys (Bailey et al. 1987).
Following oral intake of THC by the mother, the ratio between foetal and maternal THC levels in plasma appear to be much lower—about one to ten—compared to intravenous and pulmonal THC administration, where foetal THC levels are about one third of the moth-er’s. This is likely due to the difference in metabolic pathways between oral, pulmonal (smoking), and intravenous administration. In a study on dogs, the brain of the foetus showed a THC concentration of one third of the mother’s concentration half an hour after intravenous administration (Martin et al. 1977). This relation was also maintained with multiple administrations, indicating that the maternal plasma THC and not the foetal tissue is the actual source for the foetal plasma THC. In a study on THC transfer following oral administration that was carried out with rats (Hutchings et al. 1989) two multiple-dose groups were administered either 15 or 50 mg/kg THC once daily during the last two weeks
6 THC effects on human biological variations
nova-Institute THC Guidelines for Food 48
of gestation. Although among the dams, plasma concentrations co-varied with dose, and multiple dosing produced higher concentrations than acute dosing among the foetuses, es-pecially at the high dose, both in the acute and the chronic dosing group, plasma concentra-tions were approximately 10% of those found in the dams.
However, an important difference between intravenous, pulmonal and oral intake must be restated as much lower maximal peak concentrations of THC are found following the oral route (please Figure 1, section 5.1). Inhalation of a single dose of 10–20 mg THC results in THC peak plasma concentration in the order of about 50–100 ng/ml, whereas the same oral dose results in a broader, less pronounced peak with maximum concentrations of typically 5 ng/ml (Grotenhermen 2003). This also results in a lower, broader THC peak in the foetal plasma. Since higher peak concentrations result in stronger effects for the same route of administration, it can be assumed that the foetus is less affected following oral ingestion, since oral and pulmonal routes of administration of the mother result in the same applica-tion route for the foetus, i.e. the blood vessels of the umbilical cord.
This indicates that the absence of cognitive effects in the children of mothers who used oral drug Cannabis in a Jamaican study (Dreher et al. 1994) may be due in part to the inef-ficient transfer or parental tolerance, and thus low foetal toxicity, of THC ingested by pregnant women. Pregnant women in Jamaica tend to use cannabis orally, while women in the USA and Canada, whose off-spring showed some cognitive impairment (see above) usually smoke the drug (Goldschmidt et al. 2012, Porath et al. 2005).
Therefore, although it is known from clinical studies that children tolerate higher doses of THC in relation to body weight compared to adults. This may be due to the lower density and different distribution of the CB-receptors (Biegon & Kerman 2001) or due to the fact that the receptors are in a way inactive or incapable of binding (McLaughlin et al. 1994). A possible higher susceptibility of foetuses and neonates leads us to conclude that an uncer-tainty factor of 2 should offer a sufficient safety margin. However, the use of other drugs in these studies may have influenced these results, and the levels of THC obtained from drug Cannabis are much higher than those found in hempseed food products.
6.2 Genetic variation in the genes encoding CB receptors and metabolizing enzymes
There is considerable inter-individual variation in the THC doses that result in pharmaco-logical effects. This may be due to variations in polymorphisms of the specific genes (CNR1 and CNR2) that encode the most well-defined CB-R, i.e. CB-R type 1 and 2, and polymorphisms in the enzymes that are mainly responsible for the metabolism of THC in the liver (mainly CYP2C9).
Sachse-Seeboth et al. (2009) investigated the impact of the CYP2C9 polymorphism on the pharmacokinetics of orally administered THC in 43 healthy volunteers. THC pharmacoki-netics did not differ by CYP2C9*2 allele status. However, the median area under the curve of THC was three-fold higher and that of the metabolite 11-nor-9-carboxy-THC was 70% lower in CYP2C9*3/*3 homozygotes than in CYP2C9*1/*1 homozygotes. CYP2C9*3 carriers also showed a trend toward increased sedation following administration of THC. They concluded that "the CYP2C9*3 variant may influence both the therapeutic and ad-verse effects of THC." Four of the 43 volunteers were carriers of the CYP2C9*3/*3 variant with a median maximum THC concentration in plasma of 6.3 ng/ml compared to a median of 2.7 ng/ml in carriers of CYP2C9*1/*1. It is reasonable to believe that some patients in

6 THC effects on human biological variations
nova-Institute THC Guidelines for Food 49
the large clinical studies conducted with THC in recent years were carriers of the CYP2C9*3/*3 and this fact might have been the reason that in some studies even doses of 2.5-5 mg twice daily may have caused psychotropic effects since these carriers may have presented with comparably higher THC concentrations in blood at these low doses com-pared to other patients. There is also considerably variation in systemic bioavailability after oral intake resulting in variation of pharmacological effects.
Since an uncertainty of any origin is already largely taken into consideration by choosing a low LOEL, this paper suggests an uncertainty factor of 5 for the small part of the popula-tion (6-10%) that potentially suffer from this genetic polymorphism.
6.3 Pharmacological basis for deriving an Acceptable Daily Intake
A large number of studies have been conducted that address neuroendocrine effects of THC. The following sub-chapter will prove human studies on the effects of THC in order for an Acceptable Daily Intake to be derived. This will prove that it is no longer necessary to mainly rely on studies with animals.
The University of Pittsburgh (PA, USA) has been conducting an epidemiological study over more than 20 years on over 700 children with mothers who used cannabis and other drugs during pregnancy. These children have been examined regularly since their birth and results have since been published in more than 20 papers (e.g. Scher et al. 1988; Gray et al. 2005; Day et al. 2006; Willford et al. 2010; Day et al. 2011). A somewhat smaller epide-miological study, involving about 300 children, has been on-going for more than 30 years at Carleton University in Ottawa, Canada, which greatly increased the amount of literature on THC effects on foetuses in humans (e.g. Fried 1980; Fried 1995; Smith et al. 2004; Fried et al. 2005). Both longitudinal studies allow a good understanding of the conse-quences of THC exposure by the inhalation of cannabis to the foetus and its consequences in later life. It is no longer necessary to rely on studies with rats, like Wenger et al. 1988.
In addition, the relevance to humans of animal studies, which found increased risk of still-birth and other adverse effects on the foetus following intraperitoneal injection of THC, is in principal highly questionable. No such effects have been found with humans after oral or pulmonal administration of much higher doses. The same applies to the reported impact of low THC doses on hormone levels in pregnant rats. There are several indications that the effects observed by Wenger and his colleagues should not be extrapolated to humans. E.g., in one of their studies (1989), intraperitoneal (i.p.) injection of 0.001 mg/kg THC during the 3rd week of pregnancy in rats caused a significant prolongation of pregnancy and 42% stillbirth cases. This contrasts strongly to studies in humans. There are many stud-ies of pregnancy outcome in users of cannabis. None of them reported any increase of still-births or prolonged pregnancy relative to controls who did not consume cannabis (see Ta-ble 13).
Wenger and his colleagues also reported significant alterations following very low doses of i.p. administered THC, including a reduced Luteinizing Hormone (LH) concentration after i.p. injection of 0.001 mg/kg THC over the 1st, 2nd or 3rd week of pregnancy in rats (Wenger et al. 1988). In contrast, Tyrey (1980) administered i.v. THC in doses of 0.0312 to 0.5 mg/kg to female ovariectomized rats and found no effects on LH secretion at the lowest dose of 0.0312 mg/kg and significant effects at 0.0625 mg/kg and higher. It is un-clear why an i.v. dose of 0.0312 mg/kg (corresponding to about 0.3 mg/kg oral THC with

6 THC effects on human biological variations
nova-Institute THC Guidelines for Food 50
regard to bioavailability) should cause no effects while a 0.001 mg/kg THC dose should cause effects. Considering this contradiction in findings, EIHA suggests to challenge the findings by Wenger and his colleagues until confirmed independently. It should be noted that the studies by Wenger et al. were conducted more than 20 years ago and no other re-search group has reproduced their findings since then.
Steger et al. (1990) found a significant decrease of LH and testosterone plasma levels fol-lowing doses of 0.1, 1.0 and 10 mg/kg THC in male rats. There was no dose-response rela-tionship; all doses were equally effective. However much higher THC doses than 0.1 mg/kg had no effect on testosterone levels in humans. E.g., Dax et al. (1989) investigated the effects on male chronic cannabis users by oral administration of 10 mg of THC three times per day or inhalation of 18 mg of THC three times per day for three days, following at least two weeks of abstinence. These conditions simulate routine cannabis drug use. The researchers did not find any alterations in plasma testosterone concentrations. Mendelson et al. (1978) could not detect any influence on testosterone levels in 27 cannabis users who had consumed an average of 54 cannabis cigarettes or 120 cannabis cigarettes over a peri-od of 21 days. In a National Institute on Drug Abuse (NIDA) Research Monograph, Men-delson et al. (1984) stated with regard to the effect of THC on female hormones:
“It is clear from the foregoing that THC consistently produces significant changes in pi-tuitary gonadal hormones, which are essential for normal reproductive function in ex-perimental animal models. The major unanswered question is: what is the relevance of these data for human females? There are often marked species differences even within animal models and the degree to which THC induced disruption of pituitary gonadal hormones in animals can be extrapolated to humans is an empirical question. Despite the predictive values (and relative economy) of studying drug effects in animals, the ul-timate significance of these findings can only be determined in human studies” (page 105).

6 THC effects on human biological variations
nova-Institute THC Guidelines for Food 51
Table 13 Selected discrepancies between animal and human data on THC Target effect Animal study Human study
Male plasma tes-tosterone hormone concentration
– 0.1 mg/kg oral THC resulted in decrease in male rats (Steger et al. 1991).
– 0.15 mg/kg oral THC three times daily did not cause an effect (Dax et al. 1989).
– 0.25 mg/kg inhaled THC three times daily did not cause an effect (Dax et al. 1989).
Male prolactin level in plasma
– Increase following 0.04 mg/kg THC intraperitoneally in rats (Daley et al. 1974).
– Decrease after 0.5 mg/kg oral THC in rats (Rodriguez De Fonseca et al. 1992).
– No change following about 0.6 mg/kg inhaled THC (Cone et al. 1986).
– Chronic cannabis users do not show any significant alteration in their prolactin levels (Vescovi et al. 1992, Cohen 1976).
Female luteinizing hormone (LH) concentration
– 0.0625 mg/kg intravenous THC caused a profound decrease in rats (Tyrey 1980).
– No change in LH level following about 0.3 mg/kg inhaled THC (Mendelson et al. 1985a).
– However, a light significant decrement (p < 0.02) was observed when the canna-bis was consumed during the luteal phase. Chronic users present a normal LH-level (Dornbush et al. 1978, Kolodny et al. 1979; Block et al. 1991).
Stillbirths – 0.001 mg/kg intraperitoneally THC resulted in 42% stillbirths (Wenger et al. 1989).
– No increased rate of stillbirths in any human study of female cannabis users.
Duration of preg-nancy
– 0.001 mg/kg intraperitoneally THC resulted in a prolonged duration of pregnancy (Wenger et al. 1989).
– Most human studies did not find any effect of cannabis use on duration of pregnancy (e.g., Hatch and Bracken 1986; Zuckerman et al. 1989; Shiono et al. 1995; Day et al. 1991).
– Some found a decreased length of gestation or a higher rate of premature births (Gibson et al. 1983; Fried et al. 1984; Sherwood et al. 1999).
Birth weight – 0.001 mg/kg intraperitoneally THC reduced birth weight in rats (Wenger et al. 1991)
– Chronic cannabis use (about 0.1 to 2.0 mg/kg inhaled THC) did not cause re-duced birth weight (Dreher et al. 1994; Shiono et al. 1995; several other studies).

6 THC effects on human biological variations
nova-Institute THC Guidelines for Food 52
6.4 Conclusion
Biological differences among humans allow for a better understanding of the regulatory guidance values of THC. Although some studies have found that human foetuses and chil-dren have the same amount of CB-R as adults (Glass et al. 1997), the majority of the litera-ture indicates that human foetuses and children have a smaller amount of CB-R in the brain, leading to a higher THC tolerance (Dalzell et al. 1986; Abrahamov et al. 1995; Belue et al. 1995; Biegon & Kerman 2001; Gottschling 2011).
Foetuses experience significant exposure to THC following maternal cannabis ingestion. However, due to different pharmacokinetics of oral and pulmonal THC, foetal exposure after oral THC intake by the mother, e.g., with hemp foods, will be lower compared to in-haled THC intake by the mother, e.g., by smoking cannabis cigarettes. Assuming a system-ic bioavailability of oral THC of about one third of that of inhaled THC (6-7% vs. 20%) and a foetus/mother plasma level ratio of 1:10, compared to 1:3 for inhaled THC, foetal exposure to THC ingested by the mother accounts for about 11% of the exposure caused by inhaling the same dose (see Table 14). In addition, oral ingestion by the mother results in a much lower maximum peak concentration compared to inhalation of the same dose, further reducing possible impact from THC. These differences in the transfer to the foetus between oral and inhalative uptake of THC thus provide an additional safety margin from potential teratogenic effects.
Table 14 Comparison of dose-specific foetal toxicity caused by maternal ingestion vs. inhalation of THC.
Inhalation (smoking a can-nabis cigarette)
Oral intake (hemp)
Systemic bioavailability 20% 6-7%*)
Ratio of ingested THC to THC systemically available
1/5 1/15
Ratio of THC concentration in foetal and maternal plasma
1/3 1/10
Overall'ratio' 1/15 1/150
*) An extensive first pass liver metabolism reduces oral bioavailability of THC, i.e. much of the THC is ini-tially metabolized in the liver before it reaches the sites of action. Ingestion of 20mg THC in a chocolate cookie (Ohlsson et al. 1980) and administration of 10mg dronabinol (synthetic THC) (Sporkert et al. 2001) resulted in a systemic bioavailability of 6 ± 3% (range: 4-12%) or 7 ± 3% (range: 2-14%) with a high interin-dividual variation.
Furthermore, it is reasonable to believe that some patients in the large clinical studies con-ducted with THC in recent years were carriers of the CYP2C9*3/*3 genotype and this fact might have been the reason that in some studies even doses of 2.5-5 mg twice daily may have caused psychotropic effects since these carriers may have presented with comparably higher THC concentrations in blood at these low doses compared to other patients.
Finally, toxicological data from animal studies can help to elucidate adverse effects of can-nabinoids in humans. However, comparison of the data from studies on humans and ani-mals has often revealed considerable inconsistencies. These may result from not only inter-

6 THC effects on human biological variations
nova-Institute THC Guidelines for Food 53
species differences, but also different routes of administration. Particularly, the suitability of the intraperitoneal route for extrapolation to oral and inhalative exposure has previously been questioned (Abel 1985). The findings by Wenger and his colleagues, which contradict findings from human studies applying much higher doses and using the more representa-tive oral or inhalative routes, are a case in point. Thus, wherever possible, a quantitative risk assessment should be based on data from human studies. EIHA suggests disregarding the results of Wenger and colleagues and relying instead on the extensive and available human data for THC.
Based on the previously stated scientific arguments, this paper suggests applying an uncer-tainty factor of 20. This value was deduced from three different factors that may affect the way THC works in the human body.
Firstly, large clinical studies have shown that there is considerable inter-individual varia-tion in susceptibility to THC and that some adults may experience slight psychotropic or psychomotor effects at twice a dose of 2.5 mg (or 0.07 mg/kg bw), while most individuals show only effects at considerably higher doses. This variation may be based on genetic polymorphisms of the genes encoding the cannabinoid receptors and the enzymes respon-sible for the metabolism of THC. We suggest an uncertainty factor of 5 since an uncertain-ty of any origin is already largely taken into consideration by choosing a low LOEL.'
Secondly,' since THC may easily cross the placenta to the foetus and the foetus may be more susceptible than children and adults, we suggest an uncertainty factor of 5 for a pos-sibly higher susceptibility of foetuses and neonates with still not fully developed drug me-tabolizing enzymes. It is known from clinical studies that children tolerate higher doses of THC in relation to body weight compared to adults. In addition, adverse effects from can-nabis on the foetus, which have been observed in epidemiological studies, are relatively low compared to other drugs. Therefore, an uncertainty factor of 2 should assure a suffi-cient safety margin.
Finally, although there is no hint at a measurable potentiation of THC effects with an oral dose of 2.5 mg twice daily by alcohol or other drugs, an uncertainty factor of 2 should as-sure a sufficient safety margin should this, in certain extreme cases, take place.
Although this paper suggests an uncertainty factor of 20, a value of 10 is commonly ap-plied to substances that have a strong scientific basis on human testing, rather than animal. Furthermore, there has been a wide range of uncertainty factors applied to THC by BgVV and EFSA, ranging from 20 – 100. These denote that security values for THC need further evaluation. Substances such as morphine, commonly found in poppy seeds, have a security factor of 3 (EFSA 2011a), in spite of morphine being considerably more harmful. There-fore, nova introduces the value of 20 extrapolated from medical data as a preliminary ref-erence and leaves the uncertainty factor open to future revision.
Based on the above, an acceptable daily intake (ADI) for orally ingested THC of 0.0035 mg/kg bw was deduced to provide protection from both acute and chronic effects in hu-mans.
Based on the literature reviewed and the values defined, the next chapter will put forward guidelines'for'THC'concentration'in'food.

7 New proposal on THC guidelines for different hemp food products
nova-Institute THC Guidelines for Food 54
7 New proposal on THC guidelines for different hemp food products
“The THC level in plants should not be a critical consideration when the level in seed oil and seed oil products is in fact the critical issue for regulatory concern” (Small 2014).
Following the literature review of the previous chapters (5 and 6), two aspects have to be considered relating to oral intake in food:
THC must be consumed in its free, non-carboxylated form in order to be biologically ac-tive. However, in fresh unprocessed hemp plants, THC occurs in the form of its inactive carboxylic acid, i.e. THC acid A (THCA-A). Fresh hemp is considered safer as THCA is not metabolised to THC and not psychotropic. It is decarboxylated, i.e. converted into its active form, primarily by heat during short period baking and other forms of food pro-cessing, and when smoked. Thus, largely unprocessed foods, such as cold-pressed oils, may often contain large fractions of pharmacologically inactive THCA. THCA does natu-rally decay to THC with a half-life of 35 and 91 days, whereas THC degrades to CBN only at a half-life rate of 24 to 26 months, effectively resulting in THC accumulating even if THCA-containing material is not heated (Lindholst 2010). THC guidelines tend to account for this process by measuring the total THC in a product.
The degree of THC absorption into the human intestines also depends on the physical and chemical properties of the carrier. Generally, lipophilic carriers, such as oil, increase ab-sorption. If THC is present in less fatty matrices, such as breads, pastries or drinks (hydro-philic environments) the bioavailability of THC is typically reduced by 50% (Grotenher-men 2014).
As described in chapter 3, certain countries expect a zero tolerance of THC in food goods based on US drug policy rather than health research practices. Not even toxic food contam-inants or pollutant (see Table 11, section 5), such as pesticides or heavy metals, are held to such limiting restrictions, and popular foods containing trace amounts of other natural drugs, such as morphine (in poppy seeds), are not a matter of official concern.
Therefore, there is demand for more scientifically accurate THC guidance values in food and beverages that can take into account both the consumer’s and the producer’s concerns, providing the former with more choices and the latter with room to develop the industry. This chapter will put forward new guidelines for food and beverages that contain THC.
From section 2.1, in Europe, one country stands out as having the most thorough guidance values, Germany, and two others, Switzerland and Belgium, as having actual scientifically based government-backed limits. The two sets of limits are considered safe to the consum-er and friendly to the industry.
The German guidelines are one of the most commonly used in Europe, particularly in Member States that lack their own values. Therefore, this paper will use its methodology, already generally accepted and considered one of the most sound, complete and consistent in the subject matter, in order to set new European guidance values (for the German guid-ance values, please refer to section 2.1.2.).
Applying the same methodology used by BgVV, the first step is to set a Lowest Observed Effect Level (LOEL) innocuous to health. An uncertainty factor is then applied, yielding

7 New proposal on THC guidelines for different hemp food products
nova-Institute THC Guidelines for Food 55
an Acceptable Daily Intake (ADI) of THC. The factor is a way to protect several subpopu-lations that are more vulnerable to the particular substance.
Following the German annual average consumption patterns, a daily average per product category is reached. The selected food category data will correspond to hemp products already existing on the market. THC guidance values are then put forward for each food category that, multiplied by the average daily intake, generate the uptake in mg of THC per person per day per category.
Finally, the sum of all categories’ uptakes ought not surpass the initial ADI of THC.
Acceptable Daily Intake (ADI) of THC
An ADI is the maximum allowed ingestion of THC by an individual in a day. This limit is usually expressed in mg of THC per kg of body weight.
First the placebo limit for acute psychotropic and physical effects from THC ingestion had to be determined from the literature. In the case of THC, the most relevant effects are those on mood and cognition (euphoria, fear, reduced cognitive functions) as well as on the car-diac circulation system (increase in cardiac frequency, changes in blood pressure).
Usually, single doses of 5-15 mg THC cause mild psychotropic effects (Lucas & Laszlo 1980; Petro & Ellenberger 1981; Chesher et al. 1990; Brenneisen et al. 1996).
As mentioned in Chapter 6, an acute dose of 2.5 mg THC (corresponding to 0.035 mg/kg bw assuming a body weight of 70 kg) may usually be regarded as a placebo dose, particu-larly as effects tend to be watered down with time, as the body builds up a tolerance to THC (Zajicek et al. 2003 and Zajicek et al. 2005). The effects of a single dose of THC typ-ically last anywhere between 4-6 hours, with some remaining up to 8 hours after consump-tion, in extreme cases (Lachenmeier and Walch 2005; please refer to Figure 1, section 5.1). Since nobody usually ingests all their food at once, the uptake of an oral dose of 2.5 mg of THC twice per day, equivalent to 5 mg taken over the course of a 24-hour period (or 16 waking hours), represents an appropriate and realistic minimum daily effect dose per per-son.
This paper suggests applying an uncertainty factor of 20. This value was deduced from three different factors that may affect the way THC is metabolized in the human body. As stated in chapter 6, the value of 20 results from a combination of inter-individual variations (5), higher vulnerability of foetuses and neonates (2), and potential interference with other substances (2). This value is still open to review in the future.
The following table exposes the evolution of LOEL and uncertainty factors on THC in hemp food goods.

7 New proposal on THC guidelines for different hemp food products
nova-Institute THC Guidelines for Food 56
Table 15 Comparison of LOEL and uncertainty factor of THC in hemp food goods based on BgVV 1998, EFSA 2011 and 2015, and nova-Institute proposed values 2015
Although this paper suggests an uncertainty factor of 20, a value of 10 is commonly ap-plied to substances that have a strong scientific basis on human testing, rather than animal. Therefore, nova introduces the value of 20 as a reference and leaves the uncertainty factor open to future revision.
Therefore, a dose of 2.5 mg twice daily divided by the uncertainty factor of 20 results in an ADI of 0.125 mg twice daily. In order to follow the same safety rounds as those applied by BgVV, the value of 0.125 mg twice daily will be dropped to 0.120 mg twice daily equal 0.240 mg per day for a 70kg human or 0.0035 mg/kg bw. The following table summarizes the previous calculations:
Table 16 nova’s ADI THC-guidance values for hemp-based foodstuffs nova THC-guidance values for hemp-based foodstuffs Male weighing 70 kg, 25-50 years old Lowest Observed Effect Level 2 x 2.5 mg THC/day/person divided by uncertainty factor of 20: Acceptable Daily Intake of THC 2 x 0.125 mg THC/day * person rounded to: 2 x 0.120 mg THC/day/person
Updated consumption patterns
The next step of the process is to calculate the guidance values for each individual ready-to-eat food group. Usual proceedings of this type take into account the average consump-tion of sub-products of a specific good that may contain the substance under study (i.e. consumption patterns of hemp products). This information was impossible to access due to data limitations. Therefore, using an annual consumption data for selected consumer goods for the years 2011 and 2012, an average daily consumption was calculated (columns 4 and 5, Table 17).
The specific food goods selected were picked for their availability on the market. Only consumer goods that are partially or fully made out of hemp were used for this calculation in an attempt to replace as many food goods as possible for products containing hemp (see column 3 on Table 17 for a detailed list of products). In this assumption, hemp products directly replace the German average consumption and their ingestion should not pass the
''''''''''''''''''''''''''''''''''''''''''''''''''''' Comparison of Lowest Observed Effect Level (LOEL) and
uncertainty factor values
LOEL (mg/kg) 2.5 2.5 2.5 5*Uncertainty factor 20-40 100 30 20**
BgVV 1998 EFSA 2011 EFSA 2015 nova Institut 2015
*'2.5'twice'daily **'Value'proposed'from'recent'solid'data'available'from'medical'applications'on'the'effects'of'THC'in'humans;'however'due'to'methodologic'uncertainty'in'establishing'a'reasonable'uncertainty'factor,'the'proposed'value'is'open'for'evaluation'in'future.'Please'see'text'for'more'information.

7 New proposal on THC guidelines for different hemp food products
nova-Institute THC Guidelines for Food 57
previously stated ADI of 0.120 mg of THC per person twice daily. Note that all consumer goods that are available for purchase tend to only be partially made out of hemp. This pa-per assumes that they are completely hemp-based, on a one to one ratio. This creates an extra layer of security for the consumer.
All food goods were grouped in five major ready-to-eat categories: Oils, High Volume foods: Proteins, High Volume foods: Carbohydrates, Low Volume foods, and Beverages (Column 1, Table 17).
As was the case with the German calculations, hemp oil could not replace all oil consump-tion. Although hemp oil is rich in several essential fatty acids, its consumption can only replace the use of raw fats (such as spreadable fats or oils for salad). Just like in the Ger-man guidance values, this sees the general consumption of oil change from the German average of 30.4 grams/person/day to 7 g/p/d. The difference includes, among others, cook-ing oils.
The second and third categories of food goods were created to distinguish the volume of food one tends to eat. Accordingly, ‘High volume’ goods is understood as all foodstuffs that comprise the major part of a diet, usually consumed in the form of meals, and is made up of proteins (meats and dairy analogues) and carbohydrates (cereals, bread, pasta); ‘Low Volume’ foods are all other food goods that do not comprise the major part of a diet, i.e. snacks and other food goods usually consumed in low amounts, such as chocolate bars or food supplements. While ‘High Volume’ foods: Protein yielded a total daily consumption of 466 g/p/d, ‘High Volume’ foods: Carbohydrates 308 g/p/d, and ‘Low Volume’ foods totalled 158 g/p/d.
The last category is Beverages. Once more, all drinks that could be made with hemp as an ingredient were chosen and their consumption included in the list. For more details please see Table 17 below. Beverages totalled approximately 1004 ml of daily consumption.

7 New proposal on THC guidelines for different hemp food products
nova-Institute THC Guidelines for Food 58
Table 17 Consumption data for the years 2011, 2012 for selected products. Source: BMELV 2012
* Value rounded due to culinary limitations of hemp oil ** Value extracted from Statista Inc. 2014
With an ADI and a rounded daily consumption of certain grouped final food goods, we can now proceed with the calculation of the guidance values per category.
Each category’s guidance value multiplied by the average daily consumption per person yields the daily THC uptake per person per category. Once more, the sum of all categories of daily THC uptakes per person should not pass the maximum allowed THC uptake of 0.120 mg of per person twice daily.
New proposed guidance values The limit for each category is a function of the average consumption per category and the sum of all THC uptakes per food good. The sum of all categories should not surpass ADI.
Considering the twice-daily ADI limit of 0.120 mg of THC per person, this paper created the following THC guidance values. The values were derived from the assumption that usually no one eats all their daily food all at once, allowing for a bigger margin of THC uptake without adverse effects (for more details, please see previous sections).
Even if a hemp enthusiast were to eat all possible range of hemp products available on the market at the usual daily consumption rate, the guidance values prevent the individual from being intoxicated with THC, by a safe margin of 3.96 µg of THC per person per day (Table 18).
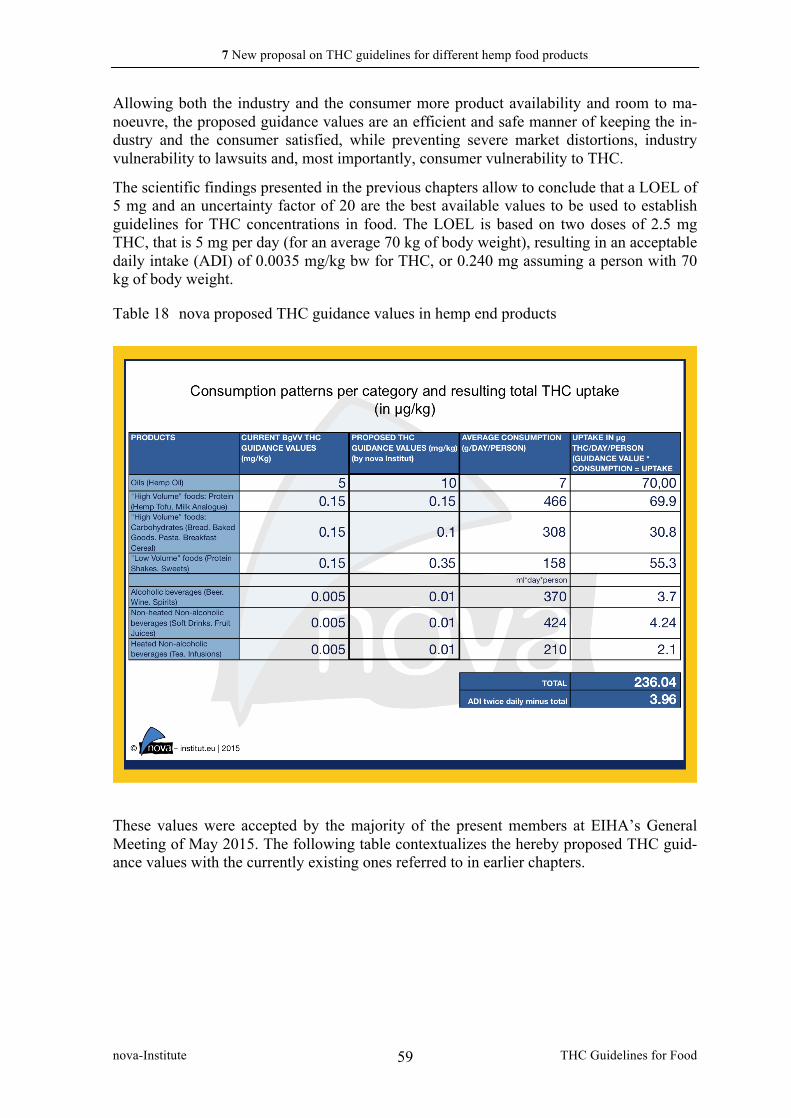
7 New proposal on THC guidelines for different hemp food products
nova-Institute THC Guidelines for Food 59
Allowing both the industry and the consumer more product availability and room to ma-noeuvre, the proposed guidance values are an efficient and safe manner of keeping the in-dustry and the consumer satisfied, while preventing severe market distortions, industry vulnerability to lawsuits and, most importantly, consumer vulnerability to THC.
The scientific findings presented in the previous chapters allow to conclude that a LOEL of 5 mg and an uncertainty factor of 20 are the best available values to be used to establish guidelines for THC concentrations in food. The LOEL is based on two doses of 2.5 mg THC, that is 5 mg per day (for an average 70 kg of body weight), resulting in an acceptable daily intake (ADI) of 0.0035 mg/kg bw for THC, or 0.240 mg assuming a person with 70 kg of body weight.
Table 18 nova proposed THC guidance values in hemp end products
'
These values were accepted by the majority of the present members at EIHA’s General Meeting of May 2015. The following table contextualizes the hereby proposed THC guid-ance values with the currently existing ones referred to in earlier chapters.

7 New proposal on THC guidelines for different hemp food products
nova-Institute THC Guidelines for Food 60
Table 19 Final nova-Institute/EIHA proposal for THC regulation in intermediate and final food goods per category, and equivalent values for listed countries (in mg/kg)
'
The suggested guidance values presented in Table 18 and Table 22 would only apply to final goods, and not on intermediate raw materials. This is already the norm with teas, where only the infused tea (i.e. tea herbs + water) is measured for THC and not the dry matter.
In order to understand the impacts of the proposed guidance values on the THC content of intermediate goods, the following table exposes a THC range resulting from selected reci-pes. Variations on recipes or the use of different products can result in different THC con-tent in the intermediate materials. These values are, therefore, to be used as reference for businesses that deal with raw and intermediate material trading or processing.

7 New proposal on THC guidelines for different hemp food products
nova-Institute THC Guidelines for Food 61
Table 20 Impact of proposed guidance values on hemp intermediate goods
' As previously stated, depending on the concentration on the final product, hemp intermedi-ate products could contain a range of THC per kg.
For the selected products and following the proposed guidance values on final goods, the amount of THC that may be contained in whole seeds, ranges from 5 to 7 mg/kg of raw material. Hulled hemp seeds may contain between 1.67 to 5 mg of THC per kg of raw ma-terial. Hemp protein may contain 3.5 mg/kg of THC and leaves can contain between 0.06 and 0.1 mg/kg of THC. As for flour, due to the fact that all products it is used for tend to be exposed to high temperatures (250°C for over 30 minutes), its THC content is not relevant as the molecule is denatured, assuring its breakdown and rendering it inactive. The values suggested for raw materials are intended as business to business trade reference. They should be seen as an industrial pledge for hemp ready-to-eat products to be safely produced within the guidance values proposed. EIHA recommends all its members to refer to these values.
The following table compares the practical implications of the proposed values on hemp raw materials with other countries.

7 New proposal on THC guidelines for different hemp food products
nova-Institute THC Guidelines for Food 62
Table 21 List of THC reference values for hemp raw material and intermediates derived from nova-Institute/EIHA proposal on ready-to-eat products, based on selected recipes and consumption patterns. And guidance values and limits for selected countries.
The next Chapter will see the analysis of some hemp food goods already on the market, for THC content in order to allow the reader to contextualize the values presented in this chap-ter.

8 Delta 9-THC content in consumer goods derived from the hemp plant
nova-Institute THC Guidelines for Food 63
8 Delta 9-THC content in consumer goods derived from the hemp plant
The tables below show the content of THC in hemp products available in Europe, divided into end consumer goods and raw food materials. The values, expressed in mg/kg show the levels of THC, THC acid and the total THC content of each product, along with the range of total THC. The data were calculated from lab tests provided by members of the Europe-an Industrial Hemp Association, analysis reports, data sheets of producers and publications (Jan, 2015).
These analyses found that the total THC content to be expected in end consumer goods is much lower than in raw food materials, ranging from 0.04 to 0.07 mg/kg in chocolate, and <0.1 mg/kg in hemp sesame bars and hemp bread (Table 22). This is due to the fact that other ingredients dissolve the concentration of cannabinoids in the product. The fat-soluble nature of THC results in higher concentrations on fat-rich products, such as chocolate, in comparison with bread or hemp sesame bars. Baked goods have trace concentrations of THC due to the fact that high oven temperatures, over baking time, destroy the THC mole-cule. All tested products fall within the guidance values proposed by this paper and gives the producer room to safely increase the hemp content in certain end consumer goods.
Table 22 THC levels in ready-to-eat products (in mg/kg), nova 2014 based on EIHA 2014 in mg/kg
Product Average THC
Average THCA
Average total THC
Range total THC
nb of data nova pro-posed val-
ues
Hemp-sesame-bars
< 0.1 < 0.1 < 0.1 < 0.1 - < 0.1
2 0.35
Hemp Bread
< 0.1 < 0.1 < 0.1 < 0.1 - < 0.1
2 0.1
Hemp chocolate bar
0.04 0.02 0.06 0.04 – 0.08 2 0.35
As mentioned, the higher value of total THC in some hemp products is, in part, due to the fat-soluble nature of the substance. Thus, products like hemp oils present higher total THC values than other defatted products, such as hemp flour or hemp powder (see Table 23). According to the values presented, hemp oil has a range of 0.025 to 12.4 mg of THC per kg of product. Total THC in whole hemp seeds range between <0.1 and 3.36, while hulled hemp seeds, hemp flour and hemp protein range between 1.1 – 6.14, 1.08 – 2.68 and 2.11 – 3.17, respectively. This means that the proposed guidance values in end products allow for intermediate goods to be traded at reasonable THC values without much interference on the market.

8 Delta 9-THC content in consumer goods derived from the hemp plant
nova-Institute THC Guidelines for Food 64
Table 23 THC levels in hemp food raw materials (in mg/kg), nova 2014 based on EIHA 2014
in mg/kg
Product((
Average(THC(
Average(THCA(
Average(total(THC(
Range((total(THC(
nb(of((data(
Reference(from(pro8posal(
Hemp'oil' 2.31' 2.64 4.47 0.025 – 12.4 51 10
Whole'Hemp'Seed'
2.8' 3.2 3.51 1.1 – 6.14 22 5
Hulled'Hemp'Seed'
1.04' 1.29 1.30 <0.1 - 3.36 45 2.5
Hemp'Powder'(Protein)'
0.66' 2.24 2.68 2.11 – 3.17 3 3.5
Hemp'Flour'
0.50' 0.96 1.685 1.08 – 2.68 3 N.A.
As mentioned in previous papers, the maximum THC content in current commercial hemp food products is ten to a hundred-fold lower than those found in studies of the 1990s (Alt 1997; Giroud et al. 1997; Lehmann et al., 1997; Mediavilla et al. 1997; Bosy and Cole 2000; Zoller et al. 2000). Lachenmeier and Walch (2005) believe that these levels of THC in hemp food no longer cause regulatory or health concerns. However, on-going quality control is needed to maintain low THC levels. This includes both the use of low THC vari-eties and proper seed cleaning.
This paper’s guidance values allow for products to be safe for end consumers while giving room for producers to market their goods without much market interference. The struck balance grants the consumer more product offer and the producer scientifically backed guidance on THC content.
The most promising product of cannabis cultivation is the seed and its derived products for utilization as food (Johnson 1999). Generally, the scientific community finds no health risks from the extremely low doses of THC present in hemp foods and body care products (Alt 1997; Giroud et al. 1997; Lehmann et al., 1997; Mediavilla et al. 1997; Bosy and Cole 2000; Zoller et al. 2000). The presented guidance values are a scientifically sound manner of protecting both the consumer and the industry.

9 References
nova-Institute THC Guidelines for Food 65
9 References
Abel EL. Effects of prenatal exposure to cannabinoids. NIDA Res. Monogr 1985;59:20-35. Abrahamov A, Abrahamov A, Mechoulam R. An efficient new cannabinoid antiemetic in
pediatric oncology. Life Sci. 1995;56(23-24):2097-102. Abrams RM, Cook CE, Davis KH, Niederreither K, Jaeger MJ, Szeto HH. Plasma delta-9-
tetrahydrocannabinol in pregnant sheep and fetus after inhalation of smoke from a marijuana cigarette. Alcohol Drug Res 1985-1986;6(5):361-9.
Agriculture and Agri-food Canada: Government of Canada. 2013. Industrial Hemp. http://www.agr.gc.ca/eng/industry-markets-and-trade/statistics-and-market-information/by-product-sector/crops/pulses-and-special-crops-canadian-industry/industrial-hemp/?id=1174595656066 – Last accessed April 10, 2015
Ahmad, G.R. & Ahmad, N., “Passive consumption of marijuana through milk: a low level chronic exposure to Delta-9-tetrahydrocannabinol (THC). Clinical Toxicology, 1990,28:2,255-260
Alt A., 1997: Lebensmittel auf Hanfbasis und deren forensische Bedeutung. In: GTFCh-Symposium 1997, Verlag Dr. Helm, Heppenheim, Germany.
Amerio, M., 1998: Chemical and nutritional evaluation of vegetable protein sources as possible dietary ingredients for sea bream (Sparus aurata). In: Vignali, C., Cas-telli, L., Fiorentini, L and Tibaldi, E., (Ed.), 8th International Symposium on Nutri-tion and Feeding in fish. Las Palmas De Gran Canaria, Spain, pp. 145
Assocanapa, 2015: Personal Communication.
Australia's National Cannabis Prevention and Information Centre (NCPIC) 2011: Cannabis Potency. National Cannabis Prevention and Information Centre. Retrieved 2011-12-13.
Bailey JR, Cunny HC, Paule MG, Slikker W Jr. Fetal disposition of delta 9-tetrahydrocannabinol (THC) during late pregnancy in the rhesus monkey. Toxicol Appl Pharmacol 1987;90(2):315-21.
BBC news. 20 July 2005. Farmers low at hemp ban for cows. Liechtenstein. http://news.bbc.co.uk/2/hi/europe/4699945.stm
Beal JE, Olson R, Lefkowitz L, Laubenstein L, Bellman P, Yangco B, Morales JO, Mur-phy R, Powderly W, Plasse TF, Mosdell KW, Shepard KV. Long-term efficacy and safety of dronabinol for acquired immunodeficiency syndrome-associated an-orexia. J Pain Symptom Manage 1997;14(1):7-14.
Beal JE, Olson R, Laubenstein L, Morales JO, Bellman P, Yangco B, Lefkowitz L, Plasse TF, Shepard KV. Dronabinol as a treatment for anorexia associated with weight loss in patients with AIDS. J Pain Symptom Manage 1995;10(2):89-97.
Belue RC, Howlett AC, Westlake TM, Hutchings DE. The ontogeny of cannabinoid recep-tors in the brain of postnatal and aging rats. Neurotoxicol Teratol 1995;17(1):25-30.
Biegon A, Kerman IA. Autoradiographic study of pre- and postnatal distribution of canna-binoid receptors in human brain. Neuroimage 2001;14(6):1463-8.

9 References
nova-Institute THC Guidelines for Food 66
BgVV 2000: BgVV recommends guidance values for THC (tetrahydrocannabinol) in hemp-containing foods. http://www.bfr.bund.de/en/presseinformation/2000/07/bgvv_recommends_guidance_values_for_thc__tetrahydrocannabinol__in_hemp_containing_foods-1309.html
Biegon A, Kerman IA. Autoradiographic study of pre- and postnatal distribution of canna-binoid receptors in human brain. Neuroimage 2001;14(6):1463-8.
Bohlmann, F. & Hoffmann, E. Cannabigerol-ähnliche verbindungen aus Helichrysum um-braculigerum. Phytochemistry, 1979, 18; 1371-1374
Bosy T.Z., Cole K.A., 2000: Consumption and quantitation of D9-tetrahydrocanna- binol in commercially available hemp seed oil products. Journal of Analytical Toxicol-ogy 24: 562-566
Bowman M, Pihl RO. Cannabis: psychological effects of chronic heavy use. A controlled study of intellectual functioning in chronic users of high potency cannabis. Psy-chopharmacologia 1973, 29(2):159-170.
Braham, Henry. 2015. Personal Communication Brenneisen R, Egli A, Elsohly MA, Henn V, Spiess Y. 1996: The effect of orally and rec-
tally administered delta 9- tetrahydrocannabinol on spasticity: a pilot study with 2 patients. International Journal of Clinical Pharmacology Therapeutics 1996, 34: 446–452.
Brenneisen, R. 1984 : Psychotrope Drogen. II. Bestimmung der Cannabinoide in Cannabis sativa L. und in Cannabisprodukten mittels Hochdruckflüssigkeitschroma-tographie (HPLC). Pharmaceutica Acta Helvetiae 59(9-10): 247-59.
Bundesinstitut für Risikobewertung 2015, www.bfr.bund.de Bundesministerium für Ernährung und Landwirtschaft (BMELV) 1994, 95, 96. 2011 and
2012. Consumption patterns in Germany. http://www.bmelv-statistik.de/ Bundesanzeiger 2001: Leitsätze für Speiseöle und Speisefette, Bundesanzeiger. No. 199.
October 24, 2001. Callaway JC, Tennilä T, Pate DW (1997). Occurrence of “omega-3” stearidonic acid (cis-
6,9,12,15-octadecatetraenoic acid) in hemp (Cannabis staiva L.) seed. Journal of the International Hemp Association 3(2): 61-63.
Callaway JC (2004). Hempseed as a nutritional resource: an overview. Euphytica 140: 65-72.
Callaway, JC, Schwab U, Harvimaa I, Halonen P, Mykkänen O, Hyvönen P & Järvinen T (2005). Efficacy of dietary hempseed oil in patients with atopic dermatitis. Journal of Dermatological Treatment 16: 87-94.
Callaway JC, Pate DW (2009). Hempseed Oil. Chapter 5, pp. 185-213 In: Gourmet and Health-Promoting Specialty Oils, Moreau RA and Kamal-Eldin A (Eds), AOCS Press, Urbana Il, ISBN 978-1-893997-97-4.
Callaway, J. 2014: Personal Communication. Carus, M. et al. 2008: Studie zur Markt- und Konkurrenzsituation bei Naturfasern und
Naturfaser-Werkstoffen (Deutschland und EU), In: Gülzower Fachgespräche, Band 26.

9 References
nova-Institute THC Guidelines for Food 67
Geelen, Joris. 2014. Personal Communication.
Chesher GB, Dahl CJ, Everingham M, Jackson DM, Marchant-Williams H, Starmer GA. The effect of cannabinoids on intestinal motility and their antinociceptive effect in mice. British Journal of Pharmacology, 1973, 49: 588–594
Dalzell AM, Bartlett H, Lilleyman JS. Nabilone: an alternative antiemetic for cancer chemotherapy. Arch Dis Child 1986;61(5):502-5.
Darshan, S.K. and Rudolph, I.L. 2000: Effect of fatty acids of w-6 and w-3 type on human immune status and role of eicosanoids. Nutrition, 16: 143-145
Deferne, J.L., & Pate, D.W. 1996: Hemp seed oil: A source of valuable essential fatty ac-ids. Journal of the International Hemp Association, 3: 4-7
Dewey, W.L. 1986: Cannabinoid pharmacology. Pharmacology Review 38 (2): 151-78.
Dreher MC, Nugent K, Hudgins R. Prenatal marijuana exposure and neonatal outcomes in Jamaica: an ethnographic study. Pediatrics 1994;93(2):254-60.
EFSA Panel on Additives and Products or Substances used in Animal Feed (FEEDAP) 2011: Scientific Opinion on the safety of hemp (Cannabis genus) for use as ani-mal feed. EFSA Journal 2011, 9(3). doi:10.2903/j.efsa.2011.2011. Available online: www.efsa.europa.eu/efsajournal
EFSA Panel on Contaminants in the Food Chain (CONTAM); Scientific Opinion on the risks for public health related to the presence of opium alkaloids in poppy seeds. EFSA Journal 2011a;9(11):2405. [150 pp.] doi:10.2903/j.efsa.2011.2405. Availa-ble online: www.efsa.europa.eu/efsajournal
EFSA CONTAM Panel (EFSA Panel on Contaminants in the Food Chain), 2015. Scien-tific Opinion on the risks for human health related to the presence of tetrahydro-cannabinol (THC) in milk and other food of animal origin. EFSA Journal 2015;13(6):4141, 125 pp. doi:10.2903/j.efsa.2015.4141. Available online: www.efsa.europa.eu/efsajournal
El-Ghany M.E.A., 2002: Molekulargenetische Diversität einer monözischen und einer diözischen Hanfsorte und Analyse des Fasergehaltes von verschiedenen Hanffor-men. Dissertation Martin-Luther-Universität, Halle-Wittenberg, Germany.
Erasmus, U. 1999: Fats that Heal, Fats that Kill. Alive books, Burnaby, British Columbia, Canada.
Erickson, M. 2007: Hempseed cake as protein feed for growing cattle. Student Report 128, 1-71.
European Commission. 2014. Plants: Plant variety catalogues & databases. http://ec.europa.eu/food/plant/propagation/catalogues/index_en.htm
EU Commission, Commission Regulations 2008: http://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32008R0145#ntr2-L_2008044EN.01000901-E0002 – Last accessed April 10, 2015
European Commission. 1998 Council Regulation (EC) No 1420/98 http://eur-lex.europa.eu/legal-content/EN/TXT/?qid=1414150819939&uri=CELEX:31998R1420 - Last ac-cessed April 10, 2015

9 References
nova-Institute THC Guidelines for Food 68
EUR-Lex, Access to European Union Law. 1998. COUNCIL REGULATION (EC) No 1420/98 amending Regulation (EEC) No 619/71 laying down general rules for granting aid for flax and hemp. http://eur-lex.europa.eu/legal-content/EN/TXT/?qid=1414150819939&uri=CELEX:31998R1420 – Last ac-cessed April 10, 2015
European Monitoring Centre for Drugs and Drug Addiction, Country legal profiles: The Dutch opium act. 2012. http://www.emcdda.europa.eu/html.cfm/index5174EN.html?pluginMethod=eldd.countryprofiles&country=NL – Last accessed April 10, 2015
FAOSTAT (Food Agricultural Organization of the United Nations) 2013: http://faostat3.fao.org/home/index.html#SEARCH_DATA in Economic Consid-erations for Growing Industrial Hemp: Implications for Kentucky’s Farmers and Agricultural Economy Department of Agricultural Economics, University of Ken-tucky July 2013
Feinberg, I., Jones R., Walker, J.M., Cleve, M.S., Cavness, B.A., March, J. Effects of high dosage delta-9-tetrahydrocannabinol on sleep patterns in man. Journal of Clinical Pharmacology and Therapeutics, 1975 April; 17(4): 458-66
Fenstrom, J.D. 1999: Effects of the dietary polyunsaturated fatty acids on neuronal func-tion. Lipids, 34: 161-9
Food Standards Australia New Zealand (FSANZ) 2012. http://www.foodstandards.gov.au/consumer/generalissues/hemp/Pages/default.aspx - Last accessed April 10, 2015
Freidel M, Tiel-Wilck K, Schreiber H, Prechtl A, Essner U, Lang M. Drug-resistant MS spasticity treatment with Sativex(®) add-on and driving ability. Acta Neurol Scand 2015;131(1):9-16.
García-Merino A. Endocannabinoid system modulator use in everyday clinical practice in the UK and Spain. Expert Rev Neurother 2013;13(3 Suppl 1):9-13.
Geelen, Joris. 2015. Personal Communication Geiwitz, J., Ad Hoc Committee on Hemp Risks, 2001: THC in Hemp Foods and Cosmet-
ics: The Appropriate Risk Assessment. January 15, 2001. Canada. Gerhard Nahler. 2015. Personal Communication
Gibb, D. J., Shah, M.A., Mir, P.S., McAllister, T.A. 2005: Effect of Full-fat Hemp Seed on Performance and Tissue Fatty Acids of Feedlot Cattle. Canadian Journal of Ani-mal Science, 85 (2005): 223-30
Giampaolo Grassi. 2014. Personal Communication
Giroud, C., Augsburger, M., Rivier, L., Mangin, P. 1997: Hemp tea versus hemp milk: subjective effects and elimination studies of THC and its main metabolite. In Pro-ceedings of the 35th TIAFT Meeting, Padova, Italy: 112-121
Glass M, Dragunow M, Faull RL. Cannabinoid receptors in the human brain: a detailed anatomical and quantitative autoradiographic study in the fetal, neonatal and adult human brain. Neuroscience 1997;77(2):299-318.
Goldschmidt, L, Richardson, G.A., Willford, J.A., Severtson, S.G., Day, N.L. School achievement in 14-year-old youths prenatally exposed to marijuana. Neurotoxi-cology and Teratology, 2012, 34(1):161-167

9 References
nova-Institute THC Guidelines for Food 69
Grotenhermen, F. 2014. Personal Communication.
Grotenhermen, F., & Carus, M. 2011: Statement by the EIHA on the study by EFSA on Scientific Opinion on the safety of hemp (Cannabis genus) for use as animal feed: 1-11.
Grotenhermen, F., Leson, G. Pless, P. 2001. Assessment of Exposure to and human health risk from THC and other cannabinoids in hemp foods. Leson Environmental Con-sulting, Berkeley, CA.
Grotenhermen, F., Karus, M., Lohmeyer, D. THC-Limits for Foods—A Scientific Study. nova Institute, Hürth, Germany, July 1998.
Hellwig 1998: personal communication July 3rd, 1998 (Federal Health Ministry, Bonn, Germany)
Hemphill, J.K., Turner, J.C., Mahlberg, P.G. 1980: Cannabinoid content of individual plant organs from different geographical strains of Cannabis sativa L. Journal of Natu-ral Products, 1980, 43:112-122
HempOil Canada 2014: Personal Communication
Hempro International. 2014: Various Publications, Personal Communication and lab mate-rial for hemp food goods.
Hemp Industries Assiciation (HIA). 2015. 2014 Annual Retail Sales for Hemp Products Estimated at $620 Million. http://thehia.org/PR/2015-03-12-PR-2014-Annual-Retail-Sales-for-Hemp-Products-Estimated-at-$620-Milli-li-on.html?utm_source=HIA+PR%3A+2014+Hemp+Product+Sales+Est.+%24620+Million&utm_campaign=PR-2014-hemp-sales&utm_medium=email – Last ac-cessed April 10, 2015
Hemp Foods Australia. 2014. Australian Hemp Legislation. http://www.hempfoods.com.au/australian-hemp-legislation/#.VFICcYvF-Es – Last accessed April 10, 2015
Hermann, Andrea. 2015. Personal Communication.
Herrman, J. L., & Younes, M. 1999: Background to the ADI/TDI/PTWI. Regulatory Toxi-cology and Pharmacology, 30(2 Pt 2):S109-13.
Hessle, A., Eriksson, M., Nadeau, E., Turner, T., & Johansson, B. 2008: Cold-pressed hempseed cake as a protein feed for growing cattle. Acta Agriculturae Scandina-vica, Section A - Animal Science, 58(3): 136-145
Hollister, L.E., Gillespie, H.K.. Delta-8- and delta-9-tetrahydrocannabinol. Clinical Phar-macology and Therapeutics 1973;14:353-357
Hutchings DE, Gamagaris Z, Miller N, Fico TA. The effects of prenatal exposure to delta-9-tetrahydrocannabinol on the rest-activity cycle of the preweanling rat. Neuro-toxicol Teratol 1989;11(4):353-6.
Jan, Guillaume. 2015. Personal Communication Johnson, P. 1999: Industrial hemp: a critical review of claimed potentials for Cannabis
sativa. TAPPI Journal 82: 113-123

9 References
nova-Institute THC Guidelines for Food 70
Jones, R.T., Benowitz, N., Bachman, J. Clinical studies of cannabis tolerance and depend-ence. Annals of the New York Academy of Sciences, December 1976, 282: 221-239
Jung, J., Meyer, M.R., Maurer, H.H., Neusüß, C., Weinmann, W., Auwärter, V. 2009: Studies on the metabolism of the Δ9-tetrahydrocannabinol precursor Δ9-tetrahydrocannabinolic acid A (Δ9-THCA-A) in rat using LC-MS/MS, LC-QTOF MS and GC-MS techniques. Journal of Mass Spectrometry, 2009, 44: 1423-1433
Karimi, I., Hayatghabi, H., & Urmia University (Iran) College of Veterinary Medicine. 2006: Effect of Cannabis Sativa L. Seed (Hempseed) on Serum Lipid and Protein Profiles of Rat. Pakistan Journal of Nutrition, 5 (6): 585-588
Koehler J, Feneberg W, Meier M, Pöllmann W. Clinical experience with THC:CBD oro-mucosal spray in patients with multiple sclerosis-related spasticity. Int J Neurosci 2014;124(9):652-6.
Lachenmeier, D.W., & Walch, S.G. 2005: Current Status of THC in German Hemp Food Products. Journal of Industrial Hemp, 10(2)(2005): 5-17
Lehmann, T., Sager, F., Brenneisen, R. 1997: Excretion of cannabinoids in urine after in-gestion of cannabis seed oil. Journal of Analytical Toxicology 21: 373-375
Leizer, C., Ribnicky, D., Poulev, A., Dushenkov, S., Raskin, I. 2000: The composition of hemp seed oil and its potential as an important source of nutrition. Journal of Nutraceuticals, Functional & Medical Foods 2: 35–53
Leson, G. 1999: Hemp Foods & Oils for Health, In: Pless, P., Roulac, J.W. (Eds.): Hemp Foods and Oils for Health. Hemptech Ltd, Sebastopol.
Lindholst, C. 2010: Long term stability of cannabis resin and cannabis extracts. Australian Journal of Forensic Sciences 2010, 42(3): 181-190
Lucas, V.S. & J. Laszlo. Delta-tetrahydrocannabinol for refractory vomiting induced by cancer chemotherapy. Journal of the American Medical Association 1980,243: 1241-1243
MAF, 2011. ‘THC hemp as food’. Ministry of Agriculture and Forestry (MAF) Australia New Zealand.
Malini, T., & Vanithakumari, G. 1990: Rat toxicity studies with b-sitosterol. Journal of Ethnopharmacology, 28: 221-234
Manku, M.S. 1990: Clinical biochemistry of essential fatty acids. In Omega-6-Essential Fatty Acids: Pathophysiology and Roles in Clinical Medicine, D.F. Horrobin, Ed. Alan R. Liss, New York, NY, 1990: 21-53
Martin BR, Dewey WL, Harris LS, Beckner JS. 3H-delta9-tetrahydrocannabinol distribu-tion in pregnant dogs and their fetuses. Res Commun Chem Pathol Pharmacol 1977;17(3):457-70.
McLaughlin CR, Martin BR, Compton DR, Abood ME. Cannabinoid receptors in develop-ing rats: detection of mRNA and receptor binding. Drug Alcohol Depend 1994;36(1):27-31.
Mechtler K., Bailer J., de Hueber K. 2004: Variations of D9-THC content in single plants of hemp varieties. Industrial Crops and Products 19: 19-24.

9 References
nova-Institute THC Guidelines for Food 71
Mediavilla, V., Derungs, R., Känzig, A., Mägert, A. 1997: Qualität von Hanfsamenöl aus der Schweiz. Agrarforschung 4: 449-451
Mendelson JH, Ellingboe J, Kuehnle JC, Mello NK. Effects of chronic marihuana use on integrated plasma testosterone and luteinizing hormone levels. J Pharmacol Exp Ther 1978;207(2):611-7.
Nahler, Gerhard. 2015. Personal Communication Nederlandse Associatie voor legale cannabis en haar stoffen als medicatie (NCSM) 2014.
http://www.ncsm.nl/english/what-is-medicinal-cannabis/active-ingredients - Last accessed April 10, 2015
Neue Zürcher Zeitung (NZZ). 13 February 2005. ‘No Grass for Cows’ (original: Kein Gras für Kühe). http://www.nzz.ch/aktuell/startseite/articleCLCNP-1.92799 original texts: “Seit Papa den Kühen Hanf verfüttert, schmeckt meine Milch noch besser” “Es geht um die Wahrnehmung der Leute. THC wird in Zusammenhang gebracht mit Kiffen”
nova Institut. 2000. http://www.naihc.org/hemp_information/content/nova_report/part1.html - Last accessed April 10, 2015
Novotna A, Mares J, Ratcliffe S, Novakova I, Vachova M, Zapletalova O, Gasperini C, Pozzilli C, Cefaro L, Comi G, Rossi P, Ambler Z, Stelmasiak Z, Erdmann A, Montalban X, Klimek A, Davies P; Sativex Spasticity Study Group. A random-ized, double-blind, placebo-controlled, parallel-group, enriched-design study of nabiximols* (Sativex(®) ), as add-on therapy, in subjects with refractory spastici-ty caused by multiple sclerosis. Eur J Neurol 2011;18(9):1122-31.
Ohlsson, A., Lindgren, J.E., Wahlen, A., Agurell, S., Hollister, L.E., Gillespie, H.K. Plas-ma delta-9 tetrahydrocannabinol concentrations and clinical effects after oral and intravenous administration and smoking. Clinical Pharmacology and Therapeu-tics, 1980, 8(3): 409-16
Pallesen, B. 2015. Personal Communication Parker, T.D., Adams, D.A., Zhou, K., Harris, M., Yu, L. 2003: Fatty acid composition and
oxidative stability of cold-pressed edible seed oils. Journal of Food Science, 68: 1240–1243
Pate, D.W. (1999). Hemp seed: A valuable food source. In: P. Ranalli (Ed.), Advances in hemp research. Haworth Press.
Petro, D.J., Ellenberger C., 1981. Treatment of human spasticity with delta 9-tetrahydrocannabinol. Journal of Clinical Pharmacology, 21: 413–16
Pitts, J.E., Neal, J.D., & Gough, T.A. 1992: Some features of Cannabis plants grown in the United Kingdom from seeds of known origin. Journal of Pharmacology, 44 (12): 947-51
Porath, A.J., Fried, P.A. 2005: Effects of prenatal cigarette and marijuana exposure on drug use among offspring. Neurotoxicology and Teratology, 2005 ,27(2):267-77
Portenoy RK, Ganae-Motan ED, Allende S, Yanagihara R, Shaiova L, Weinstein S, McQuade R, Wright S, Fallon MT. Nabiximols for opioid-treated cancer patients with poorly-controlled chronic pain: a randomized, placebo-controlled, graded-dose trial. J Pain 2012;13(5):438-49.

9 References
nova-Institute THC Guidelines for Food 72
Ramaekers JG, Berghaus G, van Laar M, Drummer OH. Dose related risk of motor vehicle crashes after cannabis use. Drug Alcohol Depend 4;73(2):109-19.
Robbins, L., Snell, W., Halich, G., Maynard, L., Dillon, C., & Spalding, D. 2013: Econom-ic Considerations for Growing Industrial Hemp: Implications for Kentucky's Farmers and Agricultural Economy. Department of Agricultural Economics, Uni-versity of Kentucky: 1-26
Rodríguez de Fonseca F, Ramos JA, Bonnin A, Fernández-Ruiz JJ. Presence of canna-binoid binding sites in the brain from early postnatal ages. Neuroreport 1993;4(2):135-8.
Rog DJ, Nurmikko TJ, Young CA. Oromucosal delta9-tetrahydrocannabinol/cannabidiol for neuropathic pain associated with multiple sclerosis: an uncontrolled, open-label, 2-year extension trial. Clin Ther 2007;29(9):2068-79.
Rosenstock: “Untersuchungen zu cannabishaltigen Lebensmitteln”, Medizinische Disserta-tion, Greifswald 2004
Ross, S.A., El-sohly, H.N., El-ashoury, E.A., El-sohly, M.A. 1996: Fatty acids of cannabis seeds. Phytochemical Analysis, 1996, 7:279-283
Ross, S., Mehmedic, Z., Murphy, T., & Elsohly, M. 2000: GC-MS Analysis of the To-tal 9-THC Content of Both Drug- and Fiber-Type Cannabis Seeds. Journal of Analytical Toxicology: (November-December 2000) 24 (8): 715-717.doi: 10.1093/jat/24.8.715.
Russo, E.B. 2013. Cannabis and Cannabinoids: Pharmacology, Toxicology, and Therapeu-tic Potential. The Haworth Integrative Healing Press®, NY.
SanaSativa® AG, Circular 8, “food hemp”, March 1, 2005. http://www.sanasativa.ch/index.php?option=com_content&task=view&id=45&Itemid=43&lang=de – Last accessed April 10, 2015
Schwab U, Callaway J, Erkkilä A, Gynther J, Uusitupa M, Järvinen T (2006). Effects of hempseed and flaxseed oils on the profile of serum lipids, serum total and lipopro-tein lipid concentrations and haemostatic. European Journal of Nutrition 45(8):470-7.
Science Daily 2014: http://www.sciencedaily.com/releases/2014/09/140917173041.htm - Last accessed April 10, 2015
Serpell MG, Notcutt W, Collin C. Sativex long-term use: an open-label trial in patients with spasticity due to multiple sclerosis. J Neurol 2013;260(1):285-95.
Sides, H. (2015, June 1). Science Seeks to Unlock Marijuana's Secrets - National Geo-graphic Magazine. Retrieved June 24, 2015, from http://ngm.nationalgeographic.com/2015/06/marijuana/sides-text
Simopoulos, A.P. 2002: The importance of the omega-6/omega-3 essential fatty acids. Bi-omedicine and Pharmacotherapy, 56: 365-379
Sirek, J. Importance of Hempseed in the Therapy of Tuberculosis. ACTA UNIVERSI-TASIS PALACKIANAE OLOMUCENSIS 1995 - TOM.VI.
Small, E. 2014. Personal Communication.

9 References
nova-Institute THC Guidelines for Food 73
Small, E., & Marcus, D. 2002: Hemp: A new crop with new uses for North America. In: J. Janick and A. Whipkey (eds.), Trends in new crops and new uses. ASHS Press, Alexandria, VA: 284–326
Sporkert F,. Pragst F,. Ploner C.J., Tschirch, A., Stadelmann, A.M. 2001: Pharmacokinetic investigation of delta-9-tetrahydrocannabinol and its metabolites after single ad-ministration of 10 mg Marinol in attendance of a psychiatric study with 17 volun-teers. Poster at the 39th Annual International Meeting, The International Associa-tion of Forensic Toxicologists, Prague, Czech Republic, August 26 - 30, 2001: 62
Stansbury, L. Hemp Industries Association. February 28, 2014. https://www.votehemp.com/PR/2014-02-28-hia_$581_million_annual_sales.html – Last accessed April 10, 2015
Steger RW, Murphy LL, Bartke A, Smith MS. Effects of psychoactive and nonpsychoac-tive cannabinoids on the hypothalamic-pituitary axis of the adult male rat. Phar-macol Biochem Behav 1990;37(2):299-302.
Cannabis-In-Cachexia-Study-Group, Strasser F, Luftner D, Possinger K, Ernst G, Ruhstaller T, Meissner W, Ko YD, Schnelle M, Reif M, Cerny T. Comparison of orally administered cannabis extract and delta-9-tetrahydrocannabinol in treating patients with cancer-related anorexia-cachexia syndrome: a multicenter, phase III, randomized, double-blind, placebo-controlled clinical trial from the Cannabis-In-Cachexia-Study-Group. J Clin Oncol 2006;24(21):3394-400.
Styrczewska, M., Kulma, A., Ratajczak, K., Amarowicz, R., Szopa, J. 2012: Cannabinoid-like anti-inflammatory compounds from flax fiber. Cellular & Molecular Biology Letters 2012, March 29, 17: 479-499
TestePledge 2014. http://www.testpledge.com/reasons.htm Thompson, G. R., Rosenkrantz, H., Schaeppi, U. H., Braude, M. C. 1973: Comparison of
acute oral toxicity of cannabinoids in rats, dogs and monkeys. Toxicology and Applied Pharmacology, 1973, 25: 363-372
Toyota, M., Shimamura, T., Ishii, H., Renner, M., Braggins, J., Asakawa, Y. 2002: New bibenzyl cannabinoid from the New Zealand liverwort Radula marginata. Chemi-cal and Pharmaceutical Bulletin (Tokyo), 2002, 50(10): 1390-1392
Tyrey L. delta 9-Tetrahydrocannabinol: a potent inhibitor of episodic luteinizing hormone secretion. J Pharmacol Exp Ther 1980;213(2):306-8.
United Nations 2009: Why Does Cannabis Potency Matter? United Nations Office on Drugs and Crime, June 29, 2009.
Von Hazura, K. Untersuchungen über die Hanfölsäure. Monatsh 1887, 8, 147–155.
Whiting, P., Robert F. Wolff, Sohan Deshpande, Marcello Di Nisio, Steven Duffy, Adrian V. Hernandez, J. Christiaan Keurentjes, Shona Lang, Kate Misso, Steve Ryder, Simone Schmidlkofer, Marie Westwood, Jos Kleijnen, (2015). Cannabinoids for Medical Use A Systematic Review and Meta-analysis. Journal of the American Veterinary Medical Association, 313(24), 1266-1267. doi:10.1001/jama.2015.6358
Wenger T, Croix D, Tramu G. The effect of chronic prepubertal administration of mari-huana (delta-9-tetrahydrocannabinol) on the onset of puberty and the postpubertal reproductive functions in female rats. Biol Reprod 1988;39(3):540-5.

9 References
nova-Institute THC Guidelines for Food 74
West, D. 1998: Hemp and Marijuana: Myths & Realities. North American Industrial Hemp Council. http://www.votehemp.com/PDF/myths_facts.pdf - Last accessed April 10, 2015
WHO AMR, 2014. Fact Sheet 194 Antimicrobial resistance. http://www.who.int/mediacentre/factsheets/fs194/en/ - Last accessed April 10, 2015
Wohlfahrt, A. 2012: Pharmacokinetik und Metabolismus von D9-Tetrahydrocannabinolsäure A im Menschen. Thesis, University Freiburg.
Yehuda, S., Rabinovitz, S., Carrasso, R.L., Mostofsky, D.I. 1996: Essential fatty acids preparation (SR-3) improves Alzheimer’s patients quality of life International Journal of Neuroscience, 87: 141-9
Youdim, K.A., Martin, A., Joseph, J.A. 2000: Essential fatty acids and the brain: Possible health implications. International Journal of Developmental Neuroscience, 18: 383-99
Yuill, Thomas. "Dose-response Relationship." The Encyclopedia of Earth. Boston Univer-sity - National Library of Medicine, 16 Sept. 2008. Web. 13 May 2015
Zajicek, J., Fox, P., Sanders, H., Wright, D., Vickery, J., Nunn, A., Thompson, A. 2003. Cannabinoids for treatment of spasticity and other symptoms related to multiple sclerosis (CAMS study): multicentre randomised placebocontrolled trial, on be-half of UK MS Research Group. Lancet.
Zajicek, J.P., Sanders, H.P., Wright, D.E., Vickery, P., Ingram, W., Reilly, S., Nunn, A., Teare, L., Fox, P., and Thompson, A. 2005. Cannabinoids in multiple sclerosis (CAMS) study: safety and efficacy data for 12 months follow up. Journal of Neu-rology, Neurosurgery & Psychiatry, 76: 1664–1669
Zoller, O., Rhyn, P., Zimmerli, B. 2000: High-performance liquid chromatographic deter-mination of D9-tetrahydrocannabinol and the corresponding acid in hemp contain-ing foods with special regard to the fluorescence properties of D9-tetrahydro- cannabinol. Journal of Chromatography A 872: 101-110

9 References
nova-Institute THC Guidelines for Food 75
Annex I List of some final products according to suggested categories:
nova%category% Product% Main%hemp%intermediate%good%
! ! !Oils! Oil! Oil!
! ! !"High!Volume"!foods:!Proteins!
Tofu!Meat!analogue!
seed!seed!
!Milk!analogue! seed!
!
Yoghurt!analogue!Ice!Cream!Puree!Pancake!Falafel!
seed!seed!seed!seed/flour!seed/flour!
! ! !"High!Volume"!foods:!CarbohyBdrates! Bread! seed/flour!
!Cake! seed/flour/oil!
!Cookies! seed/flour/bud!
!Pasta! flour!
!
Muesli!Bread!
seed!flour/seed!
! ! !"Low!Volume"!foods! Sweets! extract!
!Snak!bars!(cereal,!marzipan,!etc.)! seed!
!
Chocolates!Lollipops!Protein!Shakes!
seed!extract!protein!powder!
!
Vegetable!stock!Salt!!
leaves!leaves!!
Alcoholic!Beverages! Beer! extract/seed/leaves!
! ! !NonBheated!nonBalcoholic!beverages! Ice!tea! extract!
!Energy!drink! extract!
Heated!NonBalcoholic!beverages! Herbal!tea! extract/leaves!
!Fruit!tea! extract/leaves!
!Infusions! extract/leaves!
We do not include in this list products with medicinal or pharmaceutical claims. These products and others, such as food additives, require special regulations not covered in this document on food goods.