Sciatic nerve block Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software...
26
Sciatic nerve block Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics PhD (physio) Mahatma Gandhi Medical college and research institute , puducherry India
-
Upload
rudolf-floyd -
Category
Documents
-
view
227 -
download
1
Transcript of Sciatic nerve block Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software...

Sciatic nerve block
Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip.
Software statisticsPhD (physio)
Mahatma Gandhi Medical college and research institute , puducherry India
Indications
• one of the largest nerve trunks in the body• Combined with other blocks for anaesthesia • Analgesia for ankle fractures • Transport analgesia • Trauma analgesia

Volume
• 20 – 25 ml is adequate • Volume problem ??• But absorption is less quick• Motor block – 0.5 % or 0.25 % bupivacaine

Anatomy
• L 4 to S3 roots • roots of the sacral plexus form on the anterior
surface of the lateral sacrum • assembled into the sciatic nerve on the
anterior surface of the piriformis muscle• sciatic nerve exits the pelvis, is joined by the
posterior cutaneous nerve of the thigh

Anatomy
• posterior to the obturator internus, the gemelli, and the quadratus femoris. At this point, these nerves are anterior to the gluteus maximus.
• equidistant from the ischial tuberosity and the greater trochanter.
• continues downward through the thigh to lie along the posteromedial aspect of the femur. At popleteal fossa, divides to tibial and common peroneal nerves

Anatomy

Anatomy

Anatomy – lateral view

Classic technique ( Labat )
• The patient is positioned laterally, with the side to be blocked nondependent.
• The nondependent leg is flexed and its heel placed against the knee of the dependent leg The anesthesiologist is positioned to allow insertion of the needle

Needle Puncture
• A line is drawn from the posterior superior iliac spine to the midpoint of the greater trochanter.
• Perpendicular to the midpoint of this line, another line is extended caudomedially for 5 cm.
• The needle is inserted through this point



Technique
• 22-gauge, 10- to 12-cm needle is inserted,• The needle should be directed through the
entry site toward an imaginary point where the femoral vessels course under the inguinal ligament
• Paraesthesia or motor response. • Bone hits . Go towards trochanter but not
more than 2 cm

Anterior technique( BECK)
• supine patient • leg in neutral position• a line should be drawn from the anterior
superior iliac spine to the pubic tubercle. Another line should be drawn parallel to this line from the midpoint of the greater trochanter inferomedially,

Anterior Approach

Technique
• At the point,the perpendicular line crosses the more caudal line,
• a 22-gauge, 12-cm needle is inserted so that it contacts the femur at its medial border. Once the needle has contacted the femur, it is redirected slightly medially to slide off the medial surface of the femur.
• Then paraesthesia , 20-25 ml.

Parasacral sciatic nerve block (Mansour):
• Line from p.s.i.spine to ischial tuberosity
• 6 cm caudad • Perpendicular needle
insertion 5-7 cm • Bone , slip caudad,• get nerve stimulation –
dorsiflex foot

Raj approach
• patient supine• hip and knee flexed to
90°, • the greater trochanter
and ischial tuberosity are marked. A line is drawn
• intermuscular groove between the adductors and the hamstrings marked

Ischianagi’s approach, lateral midfemoral
• Supine • Posterior to posterior
border of greater trochanter
• Needle directed medially
• Cant position- ideal technique

Problems
• Dysaesthesias• Failure because of the necessity of combined
blocks

Ultrasound guided block

USG probe
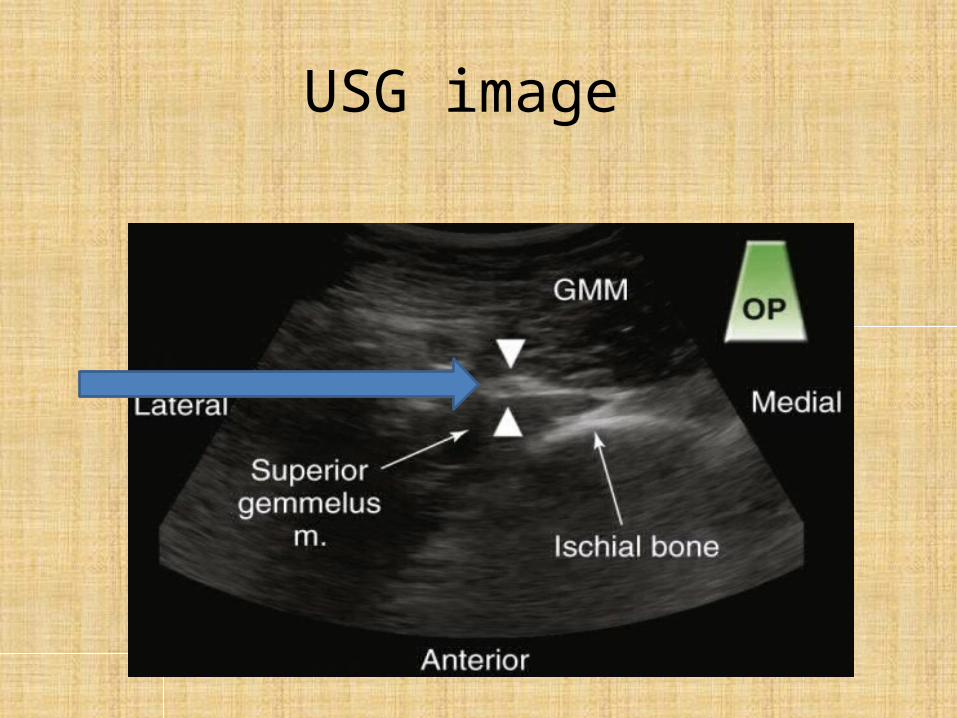
USG image

USG image

Before and after LA

Thank you all