SciAm PsychotherapyonTrial

of 8
-
Upload
katarzyna-cwiek -
Category
Documents
-
view
220 -
download
0
Transcript of SciAm PsychotherapyonTrial
-
8/13/2019 SciAm PsychotherapyonTrial
1/8
In the past half a century psy -chotherapy research has blos-somed, with thousands of stud-ies conrming its positive effectsfor a wide array of clinical prob-lems, including depression, anxi-ety, eating disorders and sexual dys-func tion. Yet in recent years, intensecontroversy over whether and how toput these ndings into practice has erupt-ed, further widening the scientist-practitionergap, the deep gulf that has separated many re-searchers and psychotherapists for decades.
The current debate centers on the growing use ofempirically supported therapies, or ESTs, which are spe-cic therapies for specic problems for example, depression
( FREUD at 150 ) The Future of Psychotherapy
Psychotherapyon Trial
42 SCIENTIFIC AMERICAN MIND Apri l /May 2 0 0 6
A N D Y W A R H O L F O U N D A T I O N C o r
b i s
-
8/13/2019 SciAm PsychotherapyonTrial
2/8
Empirically supported therapies
seek to bring the power of research-proven techniques to the therapists
ofce. So why are they controversial?By Hal Arkowitz and Scott O. Lilienfeld
www.sc i ammi n d .co m S CIE NT IF IC AM E RICAN M IND 43
and bulimia that meet certain criteria (such as agiven number of well-designed studies showingpositive effects) for treatment efcacy. Proponentshave welcomed ESTs for their clear guidelines onwhat works for patients and their explicit manualsprescribing administration of treatment. Criticshave sharply questioned ESTs on a number ofgrounds, namely, whether their research base isadequate, whether their one-size-ts-all approachcan address the needs of individual patients, andwhether their focus should be primarily alleviationof symptomatic distress or changes in underlyingdispositions and vulnerabilities.
The debates resolution bears important im-plications for treatments that psychotherapy pa-tients seek and receive. A survey of nearly 10,000adults published in 2005 showed that one out offour Americans meets the criteria for a diagnosisof a psychological disorder in any given year and
that slightly less than half of all people in the U.S.will suffer from a psychological disorder over thecourse of their lifetimes [see Half Are Men-tally Ill, by Jamie Talan, Head Lines; ScienticAmerican Mind, Vol. 16, No. 3; 2005].
Before we wrote this article, one of us (Ar-kowitz) had been highly critical of ESTs (thoughnot of placing psychotherapy on a more scien-tic basis). The other one of us (Lilienfeld) hadbeen a strong advocate of ESTs. Ultimately wefound considerable common ground on manypoints regarding the proper role of research ininforming clinical practice. In this feature, wehope to offer a modest step toward reconcilingopposing views on ESTs.
Laying the GroundworkFifty years ago the foundations of modern
psychotherapy research were just being laid. One
-
8/13/2019 SciAm PsychotherapyonTrial
3/8
participant at a 1950 conference was being onlypartially facetious when he commented: Psy-chotherapy is an undened technique applied tounspecied problems with unpredictable out-comes. For this technique we recommend rigor -ous training.
Just two years later an eminent British psy-chologist named Hans Eysenck questioned thescientic basis of talk therapy in a landmark pa-perasserting that it was no more effective thanthe absence of treatment. Researchers soon roseto Eysencks challenge, and thousands of studiesover the ensuing decades demonstrated conclu-sively that psychotherapy does help many pa-tients. But which are the most effective therapiesand for which problems? Further studies soughtanswers.
In 1995 a task force of a division of theAmerican Psychological Association (APA),chaired by Boston University psychologist Da-
vid H. Barlow, issued the rst of several reportsthat set forth initial criteria for ESTs, along withlists of therapies that met those criteria. Thecurrent task force list is widely used today, es-pecially in university settings in which futureclinical psychologists are educated [ see box on
page 47 ].We should note that the list tells only wheth-
er a treatment has been found to work in con-trolled studies but not necessarily in clinicalpractice outside the laboratory. Most experi-ments have examined cognitive-behavioraltherapy; psychoanalytic, humanistic and inte-grative methods have received less research at-tention [ see box on page 48 ]. If a treatment isabsent from the list, it means one of two things:either studies have shown that the treatmentdoes not work, or it has not been tested and,therefore, we do not know whether or not itworks. Most of the more than 500 brands of G E
T T Y I M A G E S
44 SCIENTIFIC AMERICAN MIND Apri l /May 2 0 0 6
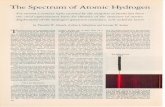
A variety of factors can lead unwary clinicians and researchers to conclude thata useless psychotherapy is in fact effective. These factors help to explain whypsychotherapy research is necessary.
Spontaneous remission Some psychotherapy clients may become betteron their own
Placebo effects Improvement results from the mere expectationof improvement
Regression to the mean Extreme scores tend to become less extremeover time
Initial misdiagnosis Some clients diagnosed with a mentaldisorder may either have no disorder at all orhave a milder disorder
Multiple-treatment interference Clients often obtain other types of treatmentat the same time
Demand characteristics Some clients may report what they believe theirtherapists want to hear, resulting in overly positivereports of improvement
Selective attrition Clients who do not benet from treatment maytend to drop out of psychotherapy, leaving onlythose clients who do benet
Effort justication Clients may feel a need to rationalize the time,energy and money they have expendedin psychotherapy
How We Can Be Fooled
-
8/13/2019 SciAm PsychotherapyonTrial
4/8
psychotherapy are not on the EST list , becausethey fall in the second category.
The Case for ESTsAdvocates have advanced three major argu-
ments in favor of a list of efcacious therapies forspecific disorders: it protects patients against
fringe psychotherapies, it empowers mental healthconsumers to make appropriate choices for theircare, and it aids in training future therapists.
First, in recent years consumers have beenbeset by a seemingly endless parade of fad thera-pies of various stripes [ see box on page 49 ]. De-spite scant scientic support or sometimes out-
right debunking some fringe treatments con-tinue to be used widely. For example, surveys ofdoctoral-level therapists in the 1990s indicatedthat about one quarter regularly employed twoor more recovered-memory techniques. Facili-tated communication, discredited by scienticresearch in the 1990s, is still popular in somecommunities. Counselors who administer crisisdebrieng number in the thousands; in the after-math of the September 11 terrorist attacks, onecrisis-debriefing outfit in Atlanta alone dis-patched therapists to 200 companies. All thesetreatments have been found to be ineffective oreven harmful. Some studies have discovered thatcrisis debrieng, for example, increased the riskof post-traumatic stress disorder in trauma-ex-posed individuals. The EST list makes it harderfor practitioners who administer these and otherquestionable techniques to claim that they areoperating scientically.
Second, the EST list benets patients becauseby providing them with information regardingwhich treatments have been proven to work, itputs them in a better position to make goodchoices for their care. Like the Food and DrugAdministrations list of approved medications,the EST list performs a quality-control function.It serves a similar purpose for managed care or-ganizations and health care agencies, which wantto make scientically informed decisions aboutwhich treatments should and should not bereimbursed. By placing the burden of proof on atreatments proponents to show that it is efca-cious, the EST list helps to ensure that therapies
promoted to the general public have met basicstandards.
Third, the EST list can improve the educationand training of graduate students in clinical psy-chology, social work and other mental healthelds. The sprawling psychotherapy research lit-erature is often confusing and contradictory;
without such a list, novice clinicians have no clearresearch guidance concerning which treatmentsto administer and which to avoid.
The Case against ESTs
Critics have responded with four concerns:EST research ndings may not apply to psycho-
therapy as practiced in the real world; the listmay be biased toward cognitive-behavioral ther-apies; the EST view of psychotherapy is narrow;and techniques emphasized by such lists may notbe the key ingredients of therapeutic change.
First, critics have attacked ESTs for both thescience underlying their empirical support andtheir applicability to clinical practice. The moveto worship at the altar of these scientic treat-ments has been destructive to clients in practice,because the methods tell you very little abouthow to read the real and complex people whoactually come in for therapy, said psychiatristGlen O. Gabbard of the Baylor College of Medi-cine in a 2004 New York Times article.
To satisfy requirements for good research,which seeks to eliminate any variables that couldconfound the results, investigators must sacricea great deal of what practicing psychotherapistsbelieve is important. EST manuals often sharplyconstrain therapists exibility to tailor the treat-ments to clients needs, resulting in a one-size-ts-all approach. Researchers reject up to 90 percentof subjects who are initially recruited, in the nameof ensuring a pure group with the diagnosis ofinterest. As a result, participants in these studiestypically represent only a small percentage ofthose who might be seen in actual practice.
The all-or-none nature of the EST list also hasbeen criticized. By categorizing treatments as ei-ther empirically supported or not, the list omitspotentially useful information, such as the de-gree of efcacy of different EST therapies. Fur-ther, many of the ESTs have modest or even rela-
www.sc i ammi n d .co m S CIE NT IF IC AM E RICAN M IND 45
Many therapies leave clients slightly better or not helpedat all. Can we call them empirically supported ?( )
-
8/13/2019 SciAm PsychotherapyonTrial
5/8
46 SCIENTIFIC AMERICAN MIND Apri l /May 2 0 0 6
tively weak effects. That is, they leave many cli-ents slightly improved or not helped at all, witha high l ikelihood of relapse. Is it reasonable tocall such therapies empirically supported?
In 2001 psychotherapy researchers DrewWesten, now at Emory University, and CatherineM. Novotny, now at the Department of Veterans
Affairs Medical Center in San Francisco, pub-lished an analysis of a large number of efcacystudies for depression and some anxiety disorders.Most of the therapies they examined were variantsof cognitive-behavioral therapy. Their ndings re-vealed a glass that is both half-full and half-empty.
On the positive side, they learned that 51 percentof depressed clients and 63 percent of those withpanic disorder were signicantly better or no lon-ger had symptoms. But the glass seems emptier ifwe recognize that many patients who had im-proved still exhibited symptoms at the end oftreatment and that others were not helped at all. Ifwe include people who dropped out of therapy, thesuccess percentages plunge considerably. In addi-tion, follow-up studies reveal high rates of relapse.For example, only 37 percent of those depressedclients who completed treatment remained im-proved one to two years later.
Second, some critics have argued that ESTtherapies are biased in favor of cognitive-behav-ioral techniques. Reviews of research on psycho-analytic and humanistic therapies suggest posi-tive effects broadly comparable to those of cogni-tive-behavioral therapies. Although less researchhas been conducted on these therapies than oncognitive-behavioral therapy, their underrepre-sentation on EST lists raises questions of bias.
Third, ESTs focus almost exclusively on symp -toms and distress to the exclusion of other impor-tant factors that lead people to seek therapy.These considerations include predispositions, vul-nerabilities and personality characteristics thatoften persist after the symptoms are gone. Manypsychotherapists believe that it is important to fo-
cus on these types of problems in therapy, in orderto enhance the quality of the clients life and helpreduce the chances of a relapse. The emphasis ofESTs on standardized techniques similarly ignoresnot only the uniqueness of individuals but also thesalutary power of the therapist-client relationship.
Fourth, the techniques emphasized by the ESTlist may not be what produces change in manycases. Most studies comparing the efcacy of twoor more therapies find that they all do aboutequally well. This surprising result is termed the
Dodo Bird verdict, after the Dodo Bird in Al-ices Adventures in Wonderland, who declares(following a race) that everybody has won andall must have prizes. Psychotherapy researchersintensely debate the meaning of the Dodo Birdverdict. Some argue that actual important differ-ences exist among therapies but that problemswith study design have masked them. Such prob-lems include small samples and the limited rangeof therapies that have been compared. It is alsopossible that although average outcomes of vari-ous therapies may not differ, some clients may dobetter with one therapy, whereas other clientsmay do better with another.
Still other researchers have accepted theDodo Bird verdict and attempted to account forit. One explanation suggests that therapeuticchange is caused more by common factors thattherapies share rather than by specic techniques.Such factors include instilling hope and provid-ing a believable theoretical rationale with associ-ated therapeutic rituals, which can make cli-ents feel that they are taking positive action tosolve their problems. This perspective also em-phasizes the healing power of the therapist-patient relationship.
Future DirectionsThe EST movement has succeeded in placing
the importance of evidence-based practice
The EST movement has placed evidence-based practice squarely on the agenda of clinical psychology.( )
(The Authors)HAL ARKOWITZ and SCOTT O. LILIENFELD hope to bring some insights to
the contentious discussion surrounding empirically supported therapies.
Arkowitz, associate professor of psychology at the University of Arizona,
has served as editor of the Journal of Psychotherapy Integration. He hasreceived two awards from the Arizona State Psychological Association for
distinguished contributions to the practice of psychology and distinguished
contributions to the science of psychology. Lilienfeld, associate professor
in the department of psychology at Emory University, is former president
of the Society for a Science of Clinical Psychology and editor of ScienticReview of Mental Health Practice.
-
8/13/2019 SciAm PsychotherapyonTrial
6/8
www.s ciammind .com SCIENTIFIC AMERICAN MIND 47
squarely on the agenda of clinical psychology.Because EST lists have many inherent problems,however, they may prove more useful as a cata-lyst for helping the eld move toward scienti-cally informed practice than they will be as thenal word.
Several promising proposals recently have at-tempted to rene or replace ESTs in ways that re-tain their emphasis on science-based practice. Onecomes from the work of University of New Mex-ico psychologist William R. Miller. Miller con-
structed a list of all researched therapies for alco-holism, ranking them by the quality of the re-search and magnitude of the effects. His methodprovides access to all relevant information aboutall therapies studied, not just those that meet theall-or-none criteria for inclusion on the EST list.
Others have suggested that we seek empiri-cally based principles of change rather thanempirically supported therapies. For example,repeated exposure to feared objects and events isa central principle underlying most effective G E
T T Y I M A G E S
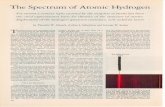
Below are selected therapies deemed empirically supported by the AmericanPsychological Association Division 12 Commit tee.
THERAPY AND PROBLEM DESCRIPTION OF THERAPY
Behavior therapyfor depression
Monitor and increase positive daily activities Improve communication skills Increase assertive behaviors Increase positive reinforcement for
nondepressed behaviors Decrease negative life stresses
Cognitive-behavior therapyfor depression
Teach clients to identify, reevaluate andchange overly negative thinking associatedwith depressed feelings
Conduct between-session experiments to testthoughts for accuracy
Monitor and increase daily activities
Interpersonal therapyfor depression
Help clients identify and resolve interpersonaldifculties associated with depression
Cognitive-behavior therapyfor bulimia
Teach ways to prevent binge eating and createalternative behaviors
Develop a plan for a regular pattern of eating Support skills to deal with high-risk situations
for binge eating and purging Modify att itudes toward eating and ones
physical appearance
Cognitive-behavior therapyfor panic disorder
Induce panic attacks during sess ions to helpclients perceive them as less dangerous(to reassure them that they will not, forexample, go crazy or die)
Introduce breathing retraining to preventhyperventilation
Control exposure to situations that triggerpanic attacks
Research-Supported Therapies
-
8/13/2019 SciAm PsychotherapyonTrial
7/8
48 SCIENTIFIC AMERICAN MIND Apri l /May 2 0 0 6
G E T T Y I M A G E S
More than 500 brands of psychotherapy exist. Below is a sampler.
TYPE OF THERAPY SUBTYPESVIEW OF CLINICALPROBLEMS
THERAPYSTRATEGIES
Cognitive-behavior BehaviorCognitive
Result fromdysfunctional learningand thinking
Encourage and teachnew behaviors; teachpeople to challenge andcorrect dysfunctionalthinking
Psychoanalytic Classic FreudianObject relationsSelf-psychologicalRelational
Conscious orunconsciouspsychologicalconicts; problems inself-regulation ofemotions andimpulses; problematicways of thinking andfeeling about the selfand others
Help make unconsciousprocesses and conictsconscious; encourageexamination ofproblematicinterpersonal patternsin and out of therapy;teach understanding ofhow these patternsdeveloped but are nolonger adaptive in thepresent; work to correctthese patterns as theyare manifested in thetherapy relationship
Humanistic-experiential
Client-centeredGestaltProcess-experientialExistential
Result from obstaclesto the innate growth(self-actualization)processes of beinghuman
Support the clientsexperience ofunderstanding, caringand empathy, leading tochanged views of theself; introduceexercises to provideopportunities thatincrease awareness offeelings and thatfacilitate change
Integrative Theoretical integration:Integrating two or more
therapies
Systematic eclecticism:Selecting and matchingtreatment to the personand problem
Common factors:Combining the factorsthat different therapiesshare
Incorporate all majorpsychotherapies and
ways of understandingclinical problems
Draw from any existingtherapy approaches
Major Approaches to Psychotherapy
-
8/13/2019 SciAm PsychotherapyonTrial
8/8
www.s ciammind .com SCIENTIFIC AMERICAN MIND 49
treatments for anxiety disorders. Therapists canderive many ways of exibly implementing a
principle of change to t clients without beingconstrained by a specic technique or manual. Ina similar vein, others have recently suggested thatwe focus on empirically supported relationshipfactors, such as therapist empathy and warmth.But there is not yet sufcient agreement concern-ing which change or relationship principlesshould qualify as empirically supported.
Another alternative to ESTs was proposed bya committee appointed by past APA presidentRonald F. Levant. The concept, which is calledevidence-based practice, has been widely em-
braced in many areas of medicine. In its 2005policy statement, the APA committee denedevidence-based practice as the integration ofthe best available research with clinical expertisein the context of patient characteristics, culture,and preferences.
The term best available research is muchbroader than evidence based on psychotherapystudies alone. It encompasses research across theentire eld of psychology, including personality,psychopathology and social psychology. Clini-cal expertise relates to therapist competenciesthat are not tied directly to research but that arebelieved to promote positive therapeutic out-comes. These capabilities inform the ability toform therapeutic relationships with clients andto devise and implement treatment plans. Finally,inclusion of client characteristics, culture andpreferences points to the importance of tailoringtreatments to individuals.
Although this APA report is a noble effort tograpple with some of the controversies, its long-term impact remains unclear. Many EST propo-nents have been dissatised with the recommen-dation to employ the best available research asbeing so vague, at least compared with the spec-icity of ESTs, as to be of little value. Many ESTadvocates have also objected to the inclusion ofclinical expertise in a definition of evidence-based practice.
Given the shortcomings of ESTs and the ex-isting alternatives to them, it is clear that theeld is just beginning to incorporate science-based practice. Nevertheless, we can begin to seethe broad outlines of promising positions thatare less dogmatic than earlier ones. Such trends
may help assuage the legitimate concerns of bothresearchers and practitioners. Ultimately we be-lieve that the eld must move beyond a narrowdenition of ESTs toward views that bridge thegap between researchers and practitioners. Afterall, whatever their differences may be, arent allclinical psychologists seeking better ways to helptroubled people feel happier and live enrichinglives? M
Energy therapiesPurport to treat clients anxiety disordersby manipulating their invisible energy elds
Recovered-memory techniquesSuggestive methods (such as hypnosis,guided imagery, keeping journals) designedto unearth memories of early child abuse
Rebirthing therapiesClaimed to treat adolescents and youngerchildrens anger by forcing them to reenactthe trauma of birth
Facilitated communicationSaid to allow mute autistic children to typesentences on a computer keyboardwith the aid of an assistant who guidestheir hand movements
Crisis debriengIntended to ward off post-traumatic stressdisorder in trauma victims by stronglyencouraging them to process theemotions and memories associated withthe anxiety-provoking event, evenif they do not feel ready to do so
Therapies to Avoid?A selective sampling of treatments for whichthere is scant scientic support.
(Further Reading)The Great Psychotherapy Debate: Models, Methods, and Findings.Bruce E. Wampold. Lawrence Erlbaum Associates, 2001.Evidence-Based Practices in Mental Health: Debate and Dialogue onthe Fundamental Questions. Edited by John C. Norcross, L. E. Beutler andR. F. Levant. American Psychological Association Press, 2005.
We begin to see the outlines of positions that may assuage the concerns of researchers and practitioners.( )