Downloaded From - Niti... · Downloaded From - Visit For More Books -

6JClin Pathol 1995;48:456-462
Light scatter characteristics of blast cells inacute myeloid leukaemia: association withmorphology and immunophenotype
M B Vidriales, A Orfao, M C Lopez-Berges,M A Garcia, J Galende, J F San Miguel
M Gonzalez, A L6pez-Macedo,
AbstractAims-To analyse the forward scatter/sidescatter (FSC/SSC) distribution of acutemyeloblastic leukaemia (AML) blast cellsin order to assess whether it correlateswith their morphology, immuno-phenotype, and clinical and biologicaldisease characteristics.Methods-FSCISSC patterns were es-tablished upon taking into account thelocalisation of the residual T lymphocytesin the FSC/SSC dot plot as an internalbiological standard. One hundred andseventy one newly diagnosed AMLpatients were analysed and five differentFSC/SSC patterns were established.These five patterns could be grouped intotwo major categories taking into accountthe FSC/SSC distribution of normal cellsin a bone marrow aspirate: immaturepatterns (1 and 2) and mature patterns(3, 4, and 5). These FSC/SSC patternswere correlated with different clinicaland biological characteristics of AMLpatients.Results-No significant associations weredetected in relation to the clinical andhaematological disease characteristicsand the prognosis of these patients. Bycontrast there was a significant correlationbetween the FSC/SSC pattern of the AMLblast cells and the FAB classification. Anincreased reactivity for the antigens as-sociated with myeloid differentiation suchas CD13, CD33, CD11b, CD15, CD14,CD4, CD56, and/or CD16 was detectedamong cases showing a mature FSCISSCpattern (3, 4, and 5), both in the wholeseries and even within each of the FABAML subtypes. By contrast, the reactivityfor the CD34 precursor cell associated an-tigen was higher among those cases dis-playing an immature FSC/SSC pattern,this being observed even within each FABsubgroup.Conclusions-The FSC/SSC pattern dis-tribution of AML blast cells not onlyprovides an additional objective and re-productible system for the classification ofthese leukaemias but it may also representa connection between the FAB mor-phological groups and the immuno-phenotypic classification ofAML patients.(J7 Clin Pathol 1995;48:456-462)
Keywords: Acute myeloblastic leukaemia, light scatter,immunophenotype, morphology.
The French-American-British CooperativeGroup (FAB) classification,'2 which is basedon both morphological and cytochemical cri-teria, is the most widely accepted and usedclassification for the acute leukaemias. How-ever, this classification has received criticismfrom several sources, mainly because of dis-crepancies among different observers.3`6 Thishas led other groups to propose alternativeclassifications, some of which include cyto-genetic and immunophenotypic criteria.79At present, immunophenotypic studies on
patients with acute myeloblastic leukaemia(AML) frequently combine the use of mono-clonal antibodies and flow cytometry. Twotypes of index can be measured: that relatedto the light scatter, and that associated withthe presence of fluorochromes in a cell.'01'Measurements of the low angle forward lightscatter (FSC) and the orthogonal light scatter(SSC) have been shown to provide informationabout cell size, asymmetry, and viability, as wellas on the internal complexity of the cell.'0"1Thus the combination of these two light scatterindices allows the identification of differentleucocyte subpopulations in both peripheralblood and bone marrow.'0-12 Analysis of AMLblast cells combining monoclonal antibodiesand flow cytometry may therefore provide in-formation not only on the phenotypic char-acteristics of the blast cells but also on theirFSC/SSC features. Up to now no account hasbeen taken of the distribution pattern ofAMLblast cells according to their light scatter prop-erties in most immunophenotypical studies onAML patients. This is probably because it hasbeen shown that there is no absolute correlationbetween this morphological information ob-tained using flow cytometry and the FAB clas-sification.12The aim of the present study was to analyse
the FSC/SSC distribution of AML blast cellsin order to assess whether or not it correlateswith their morphology, immunophenotype,and clinical and biological disease char-acteristics.
MethodsPATIENTSOne hundred and seventy one untreatedpatients with de novo AML diagnosed ac-cording to the FAB criteria'2 were included inthe study.
Patients under 65 years old and older patientsin otherwise good physical health were treated
Servicio deHematologia, HospitalClinico Universitario,Paseo de SanVincente, 37007Salamanca, SpainM B VidrialesM C Lopez-BergesM GonzalezM A GarciaJ GalendeJ F San Miguel
Servicio General deCitometria,Universidad deSalamanca,Salamanca, SpainA Orfao
Becaria del JNICT,PortugalA L6pez-MacedoCorrespondence to:Dr Jesus F San Miguel.Accepted for publication:24 September 1994
456
on May 20, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.48.5.456 on 1 May 1995. D
ownloaded from

Light scatter characteristics in AML
according to a standard protocol which in-cluded daunorubicin (60 mg/m2 for three days)and Ara-C (200 mg/M2 for seven days). Thecriteria of Ellison et al'3 were used to ascertainthe achievement of complete remission.
IMMUNOLOGICAL PHENOTYPEFor the immunophenotypic characterisation ofthe AML blast cells a panel of monoclonalantibodies (Mab) was used: the specificity ofthese Mab has been described elsewhere.71415This panel included markers against the differ-ent myeloid lineages, as well as several Mabfor precursor cells and other markers directedagainst lymphoid T, B, and natural killer (NK)cell linages. All cases were tested for at leastone specific Mab for all the different cell line-ages, using double and triple staining pro-cedures. The Mab used were: FMC56 (CD9);3C5, HPCA-1, HPCA-2 (CD34); anti-HLA-DR; My7, Leu M7 (CD13); My9, Leu M9(CD33); Leu 15 (CD11b); Leu MI (CD15),Leu M3 (CD 14); anti-glycophorin A; anti-transferrin receptor (CD71); anti-GPIIIa(CD61);J15 (CD41); AN51, FMC25 (CD42);anti-TdT; Leu 12 (CD 19); Leu 9 (CD7); Leu5b (CD2); Leu 4 (CD3); Leu 3a (CD4); Leu2 (CD8); Leu 19 (CD56); Leu llc (CD16).
Analysis of cell reactivity with the differentMab combinations was performed on an FAC-Scan flow cytometer (Becton Dickinson),equipped with an argon ion laser tuned at488 nm and 15 mW. Results were analysed forat least 4000 cells per test, using the LYSIS-IIand PAINT-A-GATE software programs (BectonDickinson). An antigen was considered to bepositive when at least 15% of the blast cellsexpressed this marker. Erythroblasts were ex-cluded from the analysis gate used for the M6leukaemia blast cells.
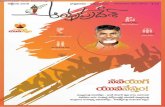
FSC/SSC PATTERNSIn all patients included in the present studythe FSC/SSC distribution pattern of the blastcells was recorded and analysed. Five differentFSC/SSC patterns were established upon tak-ing into account the localisation of the residualT lymphocytes in the FSC/SSC dot plot as aninternal biological standard (fig 1), where theT lymphocytes are represented by red dots.In all groups, blast cells usually displayed ahomogeneous distribution with respect to theFSC/SSC patterns observed in both normalperipheral blood and bone marrow samples. Inpattern 1, blast cells displayed a low FSC andSSC, with a distribution that overlapped that
*3: VPA8594050,.. . .........._-
#3: .JAP6443050 #3: JL1 1584050
* I*
- 50 100 150FSC-H\FSC-Height. --->
C, ._.
eni
C,)I-
C- _
250 0 50FSC --->
U-)
Cu.
-c-
C-,
I X
IJC
-C.
CiD
1,0.0. 150 2-0I-i 60, 1 58'Ia6, 250I-r-W-He-, Ight .-,--. . . I
50 100 150 200FSC-H',FSC-Heigh t --- >
#3: MFS3588050
CD
&~~&
C t
0 50FSC --->
#3: ADT372 1050
CIIC
100 150 200
CU.
0 50 100 150 200 250FSC -->
Blue dots: T lymphocytes
Figure I Classification of light scatter patterns in acute myeloblastic leukaemia.
CUC4.-
r,.
II
"I
I
-CO
-4-tl
0 250
II
C)
_- f--,- -, ,,tI~ '- 5- -II T*.. I..
,Iv m .- - . .-- .- r---. .- .,--.--. . . .
457
250
I
on May 20, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.48.5.456 on 1 May 1995. D
ownloaded from

Vidriales, Orfao, LDpez-Berges, Gonzdlez, LUpez-Macedo, Garcia, et al
Table 1 Clinical characteristics of acute myeloblastic leukaemia cases according to the FSCISSC pattern of blast cells
FSC/SSC pattern
1 2 3 4 5(n = 34) (n = 43) (n = 9) (n = 56) (n = 29) p
Sex M 62 66 60 43 59NSF 38 34 40 57 41
Age* 62 (13), 62 61 (20), 64 57 (23), 56 56 (19), 59 59 (16), 61 NS
Hepatomegaly 13 26 44 42 27 0 04
Splenomegaly 13 26 0 27 17 NS
Lymph nodes 16 22 44 28 24 NS
Other infiltration 7 8 22 20 26 NS
Results expressed as percentages. *Mean (SD), median.
Table 2 Biological features of acute myeloblastic leukaemia cases according to the FSC/SSC pattern of blast cells
FSCISSC pattern
1 2 3 4 5(n = 34) (n = 43) (n = 9) (n = 56) (n = 29) p
Hb (g/dl) 7-8 (2-1) 8 5 (2 0) 9 8 (3 0) 9-1 (2-2) 8-6 (2 3) NS8 1 85 87 94 8-1
Leucocytes 22 (34) 45 (60) 35 (48) 54 (69) 26 (38) 0 02( x 109/1) 37 21 18 30 12
Platelets 54 (46) 57 (42) 68 (58) 65 (58) 48 (43) NS( x 09'/1) 36 43 50 48 28
Peripheral blood blast 54 (35) 61 (28) 64 (30) 64 (27) 49 (29) NScells (%) 56 67 72 73 51
Bone marrow blast 76 (21) 82 (15) 79 (14) 80 (13) 80 (16)cells (%) 83 87 83 82 85 NS
LDH (lUll) 610 (349) 1380 (1258) 1071 (1013) 1134 (1011) 930 (797) NS500 752 648 839 770
Results expressed as mean (SD) and median.
ofresidual T lymphocytes. In the cases includedas pattern 2, blast cells accumulated in a FSC/SSC region corresponding to that of myeloidCD34 + precursor cells in normal bone marrowsamples, displaying a slightly higher FSC anda similar or slightly higher SSC than that ofTlymphocytes. Thus in pattern 2, blast cellsappeared as a prolongation of the T lympho-cytes in the FSC/SSC dot plots (fig 1). Pattern3 was characterised by having an FSC identicalto that ofT lymphocytes and a heterogeneousSSC always higher than that of T cells. Blastcells ofthe cases classified as pattern 4 displayedidentical FSC/SSC characteristics to those ofmonocytes. In pattern 5, blast cells were clearlyseparated from the T cells because they dis-played both a higher FSC and a greater SSC.These five FSC/SSC patterns were groupedinto two major groups: mature cases (patterns
Table 3 Relationship between the FSCISSC patterns of acute myeloblastic leukaemiaand FAB classification
FSC/SSC pattern
1 2 3 4 5FAB classification (n = 34) (n= 43) (n = 9) (n = 56) (n -29)MO (n=5) 20 60 0 20 0M1 (n=24) 38 42 4 12 4M2 (n=36) 14 33 11 31 11M3 (n=25) 28 4 4 24 40M4 (n=28) 0 28 11 46 14M5 (n=43) 18 9 0 52 21M6 (n=4) 50 25 0 0 25M7 (n=4) 50 50 0 0 0
Results expressed as percentages. p=0 0002.
3, 4, and 5) and immature cases (patterns1 and 2). The latter were identified accordingto the FSC/SSC characteristics of CD34 +normal cells that were considered to be rep-resentative of an "immature pattern". Thispopulation was determined using a doublestaining for CD34/CD45 and their FSC/SSClight scatter that was investigated using thePAINT-A-GATE PLUS software program.
STATISTICAL METHODSThe X2 test (BMDP 4F software program)16 wasused to estimate differences among completerecovery rates; to establish the statistical sig-nificance of the differences between clinical,haematological, and immunophenotypicalcharacteristics either the analysis of variance(ANovA) or the Kruskal-Wallis tests (BMDP 3Ssoftware program)'6 was used. Survival curveswere plotted according to the method ofKaplanand Meier and comparison between curves wasperformed using the Breslow and Mantel-Coxtests (BMDP 1L software program).'6 Valuesare given as mean (SD).
ResultsTable 1 shows the distribution of patients ac-cording to the FSC/SSC pattern of their blastcells. The most frequent FSC/SSC pattern wasnumber 4 (33%), while pattern 3 was the leastcommon one (5%); similar frequencies wereobserved for pattern 1 (20%), pattern 2 (25%),
458
on May 20, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.48.5.456 on 1 May 1995. D
ownloaded from

Light scatter characteristics in AML
Table 4 Ml acute myeloblastic leukaemia (AML) cases:phenotypic features of blast cells according to their FSCISSC distribution pattern
Immature (1 and 2) Mature (3, 4, and 5)(n = 19) (n = 5) p
CD33 44 (31) 73 (19) 0 0579% 100%
CD13 59 (28) 79 (19) 01895% 100%
CD11b 13 (12) 33 (20) 0 0541% 80%
CD15 17 (22) 25 (16) 0.1937% 75%
CD14 2 (3) 5 (2)0-040% 0%
CD4 9 (20) 33 (36) 0 1922% 75%
CD56 3 (5) 1 NS8% 0%
CD16 2 (4) 6 NS8% 0%
HLA-DR 62 (29) 67 (24) NS78% 100%
CD34 39 (32) 7 (9) 0 1172% 33%
Results expressed as mean (SD) of positive blast cells andpercentage of positive AML cases.
and pattern 5 (17%). Upon grouping the FSC/SSC patterns into mature and immature, al-most half of the patients were included in eachgroup (55% and 45%, respectively). On thebasis of "visual" criteria, three different ob-servers analysed and classified the patients ac-
cording to the FSC/SSC pattern of their blastcells; the concordance between them was 86%.The clinical and biological characteristics of
the AML patients according to their FSC/SSCcharacteristics are shown in tables 1 and 2. Nomajor differences were observed between them,with the exception of a higher incidence of
Table 5 M2 acute myeloblastic leukaemia (AML) cases:
phenotypic features of blast cells according to their FSCISSC distribution pattern
Immature (1 and 2) Mature (3, 4, and 5)(n=17) (n= 19) p
CD33 77 (21) 78 (26) NS
94% 89%
CD13 55 (30) 66 (28) NS88% 89%
CD11b 18 (24) 24 (30) NS
44% 44%
CD15 23 (25) 38 (35) NS
47% 63%
CD14 1 (2) 12 (26) 0-050% 16%
CD4 23 (22) 39 (33) 0-1656% 68%01
CD56 20 (32) 25 (34) NS
38% 39%
CD16 1 (0) 7 (18) NS
0% 11%
HLA-DR 34 (30) 60 (33) 0 02
65% 70%
CD34 45 (38) 26 (35) NS
64% 44%
Results expressed as mean (SD) of positive blast cells andpercentage of positive AML cases.
Table 6 M3 acute myeloblastic leukaemia (AML) cases:phenotypic features of blast cells according to their FSCISSC distribution pattern
Immature (1 and 2) Mature (3, 4, and 5)(n= 8) (n = 17) p
CD33 84 (9) 90 (7) 0-06100% 100%
CD13 69 (17) 85 (16) 0 01100% 93%
CD11b 10 (21) 9 (17) NS13% 13%
CD15 29 (25) 21 (27) NS62% 41%
CD14 2 (3) 2 (8) NS0% 0% N
CD4 27 (31) 21 (25) NS50% 43%
CD56 17 (35) 9 (24) NS20% 10%
CD16 0 (0) 0 (0) NS0% 0%
HLA-DR 15 (24) 9 (15) NS25% 18%
CD34 27 (35) 13 (23) NS37% 22%
Results expressed as mean (SD) of positive blast cells andpercentage of positive AML cases.
hepatomegaly in those cases displaying eitherpattern 3 or pattern 4 (p = 0 04) and a greaterperipheral blood white cell count in pattern 4patients (p = 0 02).Upon comparing the distribution of the
different FAB morphological subgroups in eachof the FSC/SSC patterns, a statistically sig-nificant correlation (p = 0 0002) was detectedbetween the two classifications (table 3). Eightypercent of the MO and Ml AML cases dis-played immature FSC/SSC patterns (patterns1 and 2) while M2 and M3 cases showed aheterogeneous distribution, 40% of the M3
Table 7 M4 acute myeloblastic leukaemia (AML) cases:phenotypic features of blast cells according to their FSCISSC distribution pattern
Immature (2) Mature (3, 4, and 5)(n = 8) (n= 20) p
CD33 64 (32) 74 (24) NS87% 95%
CD13 78 (15) 75 (16) NS100% 100%
CD11b 18 (24) 48 (34) 0 0333% 83%
CD15 19 (19) 45 (35) 0-0850% 65%
CD14 5 (5) 33 (31) 0-0313% 60%
CD4 26 (27) 46 (36) 0.1957% 75%
CD56 0 (0) 39 (32) 0 0050% 70%
CD16 1 (2) 17 (27)0% 30%~~1 .1
HIA-DR 66 (22) 67 (21) NS100% 100%
CD34 50 (32) 26 (26) 0 1180% 60%
Results expressed as mean (SD) of positive blast cells andpercentage of positive AML cases.
459
on May 20, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.48.5.456 on 1 May 1995. D
ownloaded from

Vidriales, Orfao, L6pez-Berges, Gonzailez, L6pez-Macedo, Garcia, et al
Table 8 M5 acute myeloblastic leukaemia (AML) cases:phenotypic features of blast cells according to their FSCISSC distribution pattern
Immature (1 and 2) Mature (3, 4, and 5)(n= 12) (n=31) p
CD33 42 (31) 78 (29) 0 000975% 94%
CD13 66 (17) 72 (32) 0 1092% 84%
CD1lb 25 (23) 61 (36) 0 0164% 79%
CD15 15 (27) 51 (39) 127% 67%
CD14 17 (32) 34 (32) 02317% 58%
CD4 35 (27) 60 (30) 000675% 90%
CD56 26 (39) 39 (39) 02840% 60%
CD16 0 (0) 29 (25) 0-0020% 68%
HLA-DR 80 (18) 79 (24) NS100% 91%
CD34 49 (32) 18 (22) 0 0980% 38%
Results expressed as mean (SD) of positive blast cells andpercentage of positive AML cases.
100
75.
a.
25
0 8 16 24 32Months
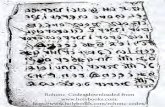
Figure 2 Survival curves of the different FSCISSC pattern groups ofAML patients.Mantel-Cox p= 0 49; Breslow p= 0 94.
40)0)
0L)a.
32Months
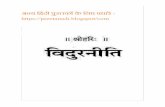
Figure 3 Survival curves of the FSCISSC pattern 5 v the rest in AML patients.Mantel-Cox p= 0 43; Breslow p= 0-68.
leukaemias corresponding to the mature pat-tern 5. Forty six percent of the M4 patients,52% of all M5 patients, and 81% of the M5bpatients were included in pattern 4. Moreover,73% of the M4 patients and 72% of the M5patients had mature FSC/SSC patterns (pat-terns 3, 4, and 5). By contrast, most of the M6(75%) and all of the M7 AML cases displayedeither pattern 1 or pattern 2.We also analysed whether or not the FSC/
SSC pattern of blast cells within each FABsubtype correlated with cell differentiation, asshown by the expression of distinct cell surfacemarkers. Upon grouping our patients into im-mature and mature FSC/SSC cases, importantphenotypic differences were detected for eachmorphological subtype; these are shown intables 4-8. Both M6 and M7 leukaemias wereexcluded from the analysis since in the presentseries few cases were included in either of theseFAB subtypes. Statistically significant differ-ences between Ml cases with immature ormature FSC/SSC patterns were detected forantigens CD33 (44(SD 31) v 73(19); p = 0 05),CDllb (13(12) v 33(20); p=0 05), and CD14(2(3) v 6(2); p=0 04) (table 4). RegardingM2 leukaemias, a lower expression of antigensCD14 (1(2) v 12(26); p=0 05) and HIA-DR(34(30) v 26(35); p=0 02) was detected inpatients with an immature FSC/SSC pattern(table 5). In the M3 AML cases with an im-mature FSC/SSC pattern, a lower reactivity forthe CD13 antigen (69(17) v 85(16); p=0 01)was detected (table 6). In addition, M4 caseswith an immature FSC/SSC pattern showed alower reactivity for antigens CD1 lb (18(24) v48(34); p=0 03), CD14 (5(5) v 33(31); p=0-03), and CD56 (0(0) v 39(32); p=0005)(table 7). Likewise, AML patients classified asM5 leukaemias with an immature light scatterpattern had a significantly lower reactivity forantigens CD33 (42(31) v 78(29); p=00009),CD11b (25(23) v 61(36); p=001), CD15(15(27) v 61(39); p=0 01), CD4 (35(27) v60(30); p=0 006), and CD16 (0(0) v 29(25);p = 0 002) (table 8). No statistically significantdifferences were detected for the expression ofother antigens analysed, although the ex-pression ofthe CD34 antigen was always higherin the cases in which cells displayed an im-mature FSC/SSC pattern (tables 4-8). Re-garding the analysis of the prognostic impactof the FSC/SSC pattern of the leukaemic blastcells, no statistically significant differences weredetected with respect to either the completeremission rate (pattern 1: 74%; pattern 2: 70%;pattern 3: 80%; pattern 4: 70%; pattern 5:80%) or survival, although the patients withFSC/SSC pattern 5 had a slightly better out-come (figs 2 and 3).
DiscussionThe morphological classification ofAML pro-posed by the FAB group is limited to subjectiveinterpretation, and the degree of agreementobtained between different observers, even ex-perts, is usually lower than 70%.3561718 Theseproblems have led several groups to proposealternative classifications, incorporating other
460
I 1
on May 20, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.48.5.456 on 1 May 1995. D
ownloaded from

Light scatter characteristics in AML
aspects, such as the morphological, immuno-logical, and cytogenetic (MIC)9 and im-munophenotypic7 classifications of AML.Flow cytometry provides information on
both the immunophenotype and the mor-phology associated characteristics of blast cells,as assessed by their FSC/SSC properties.'0"'To the best of our knowledge, there has onlybeen one attempt to group AML patients ac-cording to the light scatter properties of theleukaemic cells. 2 In that studyAML cases weredivided into nine different categories that weregrouped into three different FSC/SSC patterns,and their correlation with the FAB classificationwas analysed.
In the present paper the light scatter char-acteristics of 171 newly diagnosed AMLpatients were analysed. In contrast to normalperipheral blood or bone marrow samples,leukaemic specimens showed quite a homo-geneous FSC/SSC distribution. This is re-lated to the monomorphic morphology dis-played by leukaemic compared with normalsamples. When examining the FSC/SSC dis-tribution of normal bone marrow cells,'9 a cor-relation between the light scatter properties ofthe leukaemic blast cells and that of normalmyeloid cells can be established. Five differentFSC/SSC patterns were determined by takingthe FSC/SSC of the residual T lymphocytesas a reference. These five patterns could begrouped into two major categories: (1) im-mature patterns: cases displaying FSC/SSCpatterns that overlap those of normal myeloidprecursor cells (patterns 1 and 2); and (2)mature patterns: those in which leukaemic cellsaccumulate in regions corresponding to moremature monocytic (pattern 4) or granulocyticcells (patterns 3, 4, and 5). The existence of aclear cutoff between T lymphocytes and blastcells would allow a good discrimination be-tween the two groups of patients. Interestingly,a high reproducibility (86%) was found in thepresent study for this classification, even whenonly a subjective interpretation of the FSC/SSC dot plots was performed and the valuesof the arbitrary unit (channel) for these cellpopulations were not considered.Upon grouping the AML patients according
to the FSC/SSC pattern of their blast cells nomajor differences were observed regarding theclinical and biological disease characteristics ofthe different groups, with the exception ofhigher mean peripheral blood white cell countsin pattern 4, and a high frequency of hep-atomegaly in patterns 3 and 4. This is probablybecause of the higher incidence of monocyticleukaemias detected in this group. In addition,no significant differences in prognosis weredetected among the different groups, althoughthere was a slightly better survival rate inpatients displaying pattern 5. This was probablyrelated to the high incidence ofM3 leukaemiaswithin this FSC/SSC pattern. By contrast, therewas a significant correlation between the FSC/SSC pattern of the AML blast cells and theFAB morphology classification. In this sense,the morphologically undifferentiated cases (MOand M1 cases) were associated with an im-mature FSC/SSC pattern, while cases dis-
playing more mature morphological charac-teristics (M2, M3, M4, and M5 leukaemias)showed a higher incidence ofmature FSC/SSCpatterns. However, several FSC/SSC patternscan be found in each FAB morphological sub-type. The present results indicate that the FSC/SSC pattern of blast cells to a large extentreflects the morphological and immunologicaldifferentiation associated features of myeloidcells. Accordingly upon analysing the im-munological characteristics of the immatureversus the mature FSC/SSC patterns, our res-ults showed that this classification of AMLcases largely reflects cell differentiation alongthe monocytic and granulocytic cell lineagesand may explain some of the discrepanciesdetected among the morphological and pheno-typic characteristics ofAML blast cells. In thissense, an increased reactivity for the antigensassociated with myeloid differentiation, suchas CD13, CD33, CD1lb, CD15, CD14, CD4,CD56, and CD16, was detected among casesshowing a mature FSC/SSC pattern, both inthe whole series and even within each of theAML FAB subtypes. By contrast, the reactivityfor the CD34 precursor cell associated antigen,even within each FAB subgroup, was higheramong the cases with an immature FSC/SSCpattern.
In summary, our results indicate that theFSC/SSC pattern distribution of AML blastcells provides not only additional objective in-formation for the classification of these leuk-aemias but may also represent the connectionbetween the FAB morphological groups andthe immunophenotypic classification of AMLpatients.
This work was supported by institutional grant from the Com-isi6n Interministerial de Ciencia y Tecnologia (CICYT SAF92/0041).
1 Bennett JM, Catovsky D, Daniel MT, Flandrin G, GaltonDAG, Gralnick HR, et al. (FAB group). Criteria for thediagnosis of acute leukemia ofmegakaryocyte lineage. AnnIntern Med 1985;103:626-9.
2 Bennett JM, Catovsky D, Daniel MT, Flandrin G, GaltonDAG, Gralnick HR, et al. Proposed revised criteria forthe classification of acute myeloid leukemia: a report ofthe French-American-British Cooperative Group. AnnIntern Med 1985;103:620-4.
3 Argyle JC, Benjamin DR, Lampking B, Hammond D. Acutenonlymphocytic leukemia of childhood. Inter-observervariability and problems in the use of the FAB clas-sification. Cancer 1989;63:295-301.
4 Bain BJ. Acute leukaemia. In: Leukaemia diagnosis. A guide tothe FAB classification. London: Gower Medical Publishing,1990:1-43.
5 Dick FR, Armitage JO, Bums CP. Diagnostic concurrence inthe subclassification ofadult acute leukemia using French-American-British criteria. Cancer 1982;49:916-20.
6 Head DR, Cerezo L, Savage RA, Craven CM, Bickers JN,Hartsock R, et al. Institutional performance in applicationof FAB classification of acute leukemia. The SouthwestOncology Group experience. Cancer 1985;55:1979-86.
7 San Miguel JF, Gonzalez M, Cafnizo MC, Anta JP, Zola H,L6pez Borrasca A. Surface marker analysis in acute my-eloid leukaemia and correlation with FAB classification.Br 7 Haematol 1986;64:547-60.
8 San Miguel JF, Ojeda E, Gonzalez M, Orfao A, CafiizoMC, Sanchez I, et al. Prognostic value of immunologicalmarkers in acute myeloid leukemia. Leukemia 1989;3:108-11.
9 Second MIC Cooperative Study Group. Morphologic, im-munologic and cytogenetic (MIC) working classificationof the acute myeloid leukaemias. Br J Haematol 1988;68:487-94.
10 Orfao A, Ruiz Arguelles A. Citpmetria de flujo y su apli-caci6n en hematologia. In: Lopez Borrasca A, ArochaPirango CL, Campos Guerra C, Parreira A, Pavlosky S,Ruiz-Arguelles G, San Miguel JF, eds. Enciclopedia dehematologia iberoamericana, vol 1. Salamanca: EdicionesUniversidad de Salamanca, 1992:161-75.
11 Orfao A, Gonzalez M, Ciudad J, Lopez-Berges C, LopezA, San Miguel JF, et al. Aplicaciones de la citometria de
461
on May 20, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.48.5.456 on 1 May 1995. D
ownloaded from

Vdriales, Orfao, Lopez-Berges, Gonzdlez, Lopez-Macedo, Garcia, et al
flujo en el diagn6stico Hematologico. Biol Clin Hematol1992;14:193-203.
12 Terstappen LW, Konemann S, Safford M, Loken MR,Zurlutter K, Buchner T, et al. Flow cytometric char-acterization ofacute myeloid leukemia. Part 1. Significanceof light scattering properties. Leukemia 1991;5:315-21.
13 Ellison RR, Holland JF, Weil M, et al. Arabinosyl cytosine;a useful agent in the treatment of acute leukemia in adults.Blood 1968;32:507-23.
14 San Miguel JF, Hernandez JM, Gonzalez-Sarmiento R,Gonzalez M, Sanchez I, Orfao A, et al. Acute leukemiaafter primary myelodysplastic syndrome: immuno-phenotypic, genotypic and clinical characteristics. Blood1991;78:768-72.
15 Vidriales MB, Orfao A, Gonzalez M, Hernandez JM, L6pez-Berges MC, Garcia MA, et al. Expression of NK andlymphoid-associated antigens in blast cells of acute my-
eloblastic leukemia. Leukenia 1993;7:2026-9.
16 Dixon WJ. (Biomedical-Data Package): Statistical software.Berkeley, California: University of California, 1983.
17 Castoldi GL. Reliability of conventional cytological clas-sification: experience of GIMEMA and EORTC. Pro-ceedings of the XII Meeting of the International Societyof Hematology (European and African division), Vienna,1993:16 (Abstract).
18 Terstappen LW, Safford M, Unterhalt M, Konemann S,Zurlutter K, Piechotka K, et al. Flow cytometric char-acterization of acute myeloid leukemia: IV. Comparisonto the differentiation pathway of normal hematopoieticprogenitors cells. Leukemia 1992;6:993-1000.
19 Loken MR, Civin CI, Shah VO, Fackler MF, Segers-NoltenI, Terstappen LW. Flow cytometric characterization oferythroid, lymphoid and monomyeloid lineages in normalhuman bone marrow. In: Laerum OD, Bjerknes R, eds.Flow cytonmetry in hematology. London: Academic Press,1992:31-40.
462
on May 20, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.48.5.456 on 1 May 1995. D
ownloaded from