
Scaling-up of RTI services at Wardha District Using RTI Syndromic Approach Method MS. GUNJAN KINNU...
36
Scaling-up of RTI services at Wardha District Using RTI Syndromic Approach Method MS. GUNJAN KINNU CEO, ZP, WARDHA
-
Upload
helena-carpenter -
Category
Documents
-
view
221 -
download
2
Transcript of Scaling-up of RTI services at Wardha District Using RTI Syndromic Approach Method MS. GUNJAN KINNU...

Scaling-up of RTI services at Wardha District Using RTI Syndromic Approach
Method
MS. GUNJAN KINNU CEO, ZP, WARDHA

Discussion
Reproductive tract infections- Public health importance.
Cross-sectional study at PHC Zadshi RTI program in Wardha district.

RTI-STI- Global situation- Burden of diseases in adults by sex (WHO 1990) - Female Male
Maternal causesHIVSTI
TuberculosisRespiratory infectionMotor vehicle injuries
AnaemiaDepressive disorders
Homicide and violenceWar
Self inflicted injuriesAlcohol dependence
20% 15% 10% 5% 0% 5% 10% 15% 20%

Public Health Importance of RTIPublic Health Importance of RTI
1. As a cause of infertility and other serious gynecological complications in 1. As a cause of infertility and other serious gynecological complications in womenwomen
2. Facilitates transmission and acquisition of HIV 2. Facilitates transmission and acquisition of HIV
3. Take up a great deal of health providers’ and patient’s time and money and 3. Take up a great deal of health providers’ and patient’s time and money and repeated infections may take up a large proportion of individual’s health repeated infections may take up a large proportion of individual’s health budgetbudget
4. Uncontrolled Epidemic spread4. Uncontrolled Epidemic spread
5. Preventable 5. Preventable
6. As a cause of infection in newly-born babies. May cause premature death in 6. As a cause of infection in newly-born babies. May cause premature death in babiesbabies

1. RTI-STI causing Infertility and other gyn. complications-
Gonorrhoea and Chlamydia infections 10-40% women develop PID
PID
20% result in Infertility 9% result in Ectopic pregnancy
Infertility- social side
Social stigma
Women mostly suffer consequences of being ‘Infertile’ (may not be allowed to participate in some social functions).
Takes up a large portion of family health budget

2. HIV and RTI
-Strong evidence indicates that both ulcerative and non-ulcerative RTI promote HIV transmission.
-Available data leave little doubt that RTI, both endogenous and sexually transmitted, facilitate HIV transmission through direct, biological mechanisms

Current situation- HIV in Maharashtra
Wardha Proximal to high prevalence districts

3. Financial constrains-
For patients-
Costly medical Bills
Loss of daily wages
Private hospitals –more costly
Takes up a large proportion of monthly earnings.

Types of RTI
• Endogenous Infections– e.g. Candida albicans and bacterial vaginosis
• Sexually Transmitted Infections (STI)– e.g. gonorrhoea, syphilis, herpes
• Iatrogenic infections– e.g. Staphylococcus aureus, Pseudomonas

RTI services provided at primary health centre.
1) Regular OPD services
2) Referral of patients to civil hospital or Rural Hospital.

Regular OPD services in PHC-
Approximately10-20 patients are treated monthly(MIS report).
No record available in OPD register/ treatment cards
No partner management in required cases.
Improper treatment in many patients
No Follow-up

Referral to rural/civil hospital No data/record of such patients Financial burden for patients No follow-up.

Cross-sectional study
Objectives-
To Identify the capacity of Wardha district to detect, diagnose and treat Reproductive Tract infections, within available resources.
To interpret and suggest interventions for emerging RTIs

Cross-Sectional Study
Method- Phase I 1) Meeting was conducted for sensitizing the staff about the magnitude
of RTI problem
2) Questionnaire was prepared to assess the burden of RTI and perception about it in population.
3) Training of staff about the survey was conducted in second meeting and sample size of 10% of all houses in PHC area was selected.
4) House to house survey was conducted and all person in reproductive age group were interviewed. Specific questions were asked about RTI confidentially. Camp date was informed to all suspected cases. Patients were requested to attend camp with partners.

Staff Meeting

Survey at Yelakeli-

Cross-Sectional Study
Method -Phase II Camps were organized at sub-center level All symptomatic patients were diagnosed and
treated using WHO guidelines Partner management in required cases was
done and patients were motivated to complete treatment.
Health education regarding menstrual hygiene and safe sexual practices was given.

Treatment Camps at sub-center

Examination room
Cross-sectional study
Method Phase III Repeat survey was conducted for treated
patients to note symptomatic relief and cure rate.
Those still symptomatic were again examined, second Pap Smear was taken and patients will be treated according to results.

Results
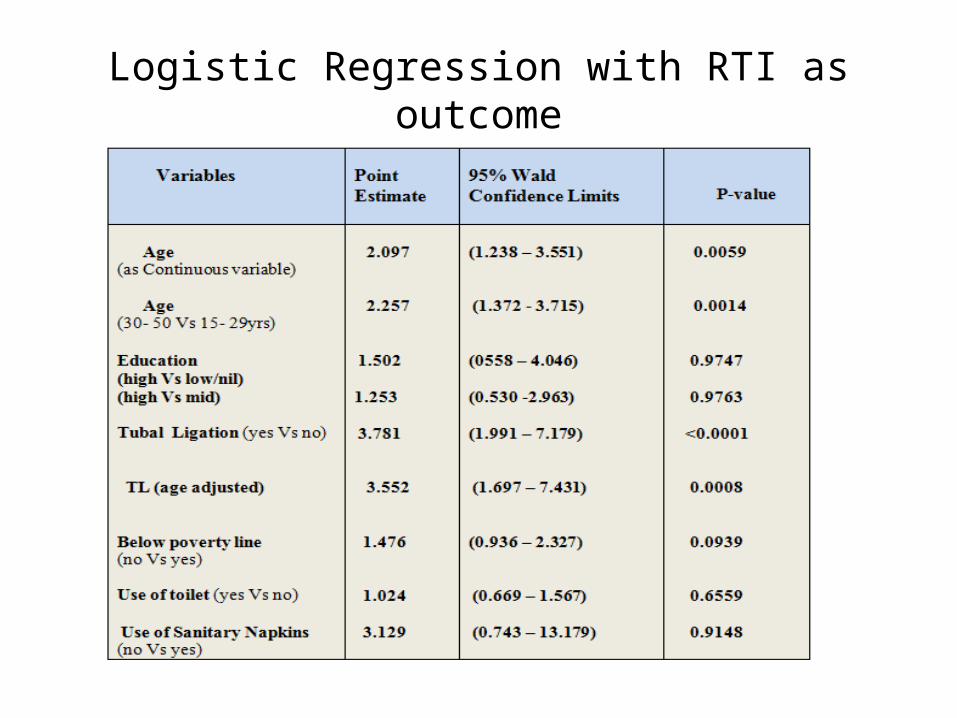
Logistic Regression with RTI as outcome
Results
• Among all people increasing age is significantly associated with increased odds of RTI. With every 5 years increase in age, the odds are increasing by 1.1.
• Compared to the younger age group (15-29y), RTI is significantly associated with 2.2 times increased odds of getting infection in people in older age group (30-50y).
• People with low education (nil or primary) are 1.5 times more likely to get infection compared to those who are high educated (grade12 or more) even people
• Females who had already done tubal ligation are 3.7times more likely to get RTI as compared to those who have not undergone the TL.

Results
Sub-center wise patient detection
Pap-smear

Results Pap-smear
Endogenous infections like Candida and bacterial vaginosis were found in (40.29%) patients.
Sexually transmitted infections like HPV , chronic cervicitis and Trichomonas were found in 59.70% of total pap smears.
Shift in trend from endogenous infection to STD

Estimated Capacity of Wardha District34,260 RTI Cases
EXPLAIN

RTI program Wardha district

Protocol designed for Scaling-up the participation of RTI patients.
Integration of RTI control into primary care as a routine activity.
Comprehensive RTI case management using WHO Syndromic Management Guidelines
Specific services for vulnerable
populations and those at higher risk for RTI

Integration of RTI services into primary healthcare
ANMs should fill at least 15 RTI detection forms weekly from the targeted population during routine home visits. Suspected patients should be invited at sub-center for diagnosis and treatment.
MO must organize weekly diagnostic and treatment camps at sub-center level.

Data management and analysis-

At sub-center camp-
ANM should Identify the syndrome Antibiotic treatment for the RTI syndrome should be
given. Partner management should be done in all required
cases. Pap smear should be taken of patients more than 35
yrs. Educate the patient about medicine compliance, risk
reduction, safe sexual practices, menstrual hygiene. Provide Condoms. Follow-up after 7 days of treatment completion. Refer patient to higher center if no relief.

Comprehensive case management with WHO syndromic-management method

Advantages
• Efficient
• Sensitive
• No need to refer patients to Laboratory investigations.
• Cost-effective.
• Treatment is given at first visit, avoiding unnecessary return visits

Disadvantages-
- Overtreatment.
- May not cover asymptomatic infection.
- Errors in disease treatment.
- Confidentiality issues
- Limited male participation
- Unmarried women- Stigma



















