
Saving newborn lives: roles for Healthcare Professionals · -Post-abortion care, TOP where legal-ST...
27
Saving newborn lives: roles for Healthcare Professionals Dr. Joy Lawn MB BS, MRCP, MPH Saving Newborn Lives/ Save the Children Funded through the Bill & Melinda Gates Foundation PMNCH Healthcare Professionals Workshop Blantyre, Malawi, November 2007
Transcript of Saving newborn lives: roles for Healthcare Professionals · -Post-abortion care, TOP where legal-ST...

Saving newborn lives: roles for Healthcare Professionals
Dr. Joy Lawn MB BS, MRCP, MPHSaving Newborn Lives/ Save the ChildrenFunded through the Bill & Melinda Gates Foundation
PMNCH Healthcare Professionals WorkshopBlantyre, Malawi, November 2007

1. Saving newborns?
2. Scaling up effective interventions – coverage and quality
3. Healthcare professionals and quality of care– what works?
Outline

Source: Graph Lawn JE et al 4 million neonatal deaths- where? When? Why? Lancet 2005. Data updated 2007 for progress until 2005 using UN data
79
300
50
100
150
200
250
1960 1970 1980 1990 2000 2010
Mor
talit
y ra
te p
er 1
000
birt
hs
Global mean under 5 mortality rate Global mean neonatal mortality rateGlobal mean neonatal mortality rate
Target for
MDG-432
Almost 40% of under-5 deaths are neonatalalmost 4 million each year
No measureable change in early neonatal mortality
Global progress for child survival: MDG4
To accelerate progress towards MDG 4 reducing deaths in the first month and especially the first week of life, is key – and this links closely with
maternal health and MDG 5

Progress to MDG 4 in Africa?
41
164
0
100
200
300
1960 1970 1980 1990 2000 2010
Mor
talit
y pe
r 1,
000
birt
hs
.
Neonatal Mortality RateUnder 5 Mortality Rate
Infant Mortality Rate
MDG 4 target for
2015
Source: Lawn JE, Kerber K Opportunities for Africa’s Newborns. PMNCH, 2006
New hope for reducing under five deaths! BUT average annual rate of reduction < 1% (1990 to 2005)To meet MDG 4 requires > 8% av annual reduction (2006 to 2015)
Progress must increase ALMOST TEN FOLD – how can the data help us to see where
acceleration is most needed?

WHERE?Neonatal Mortality burden in countries
SASI Group and M. Newman 2006
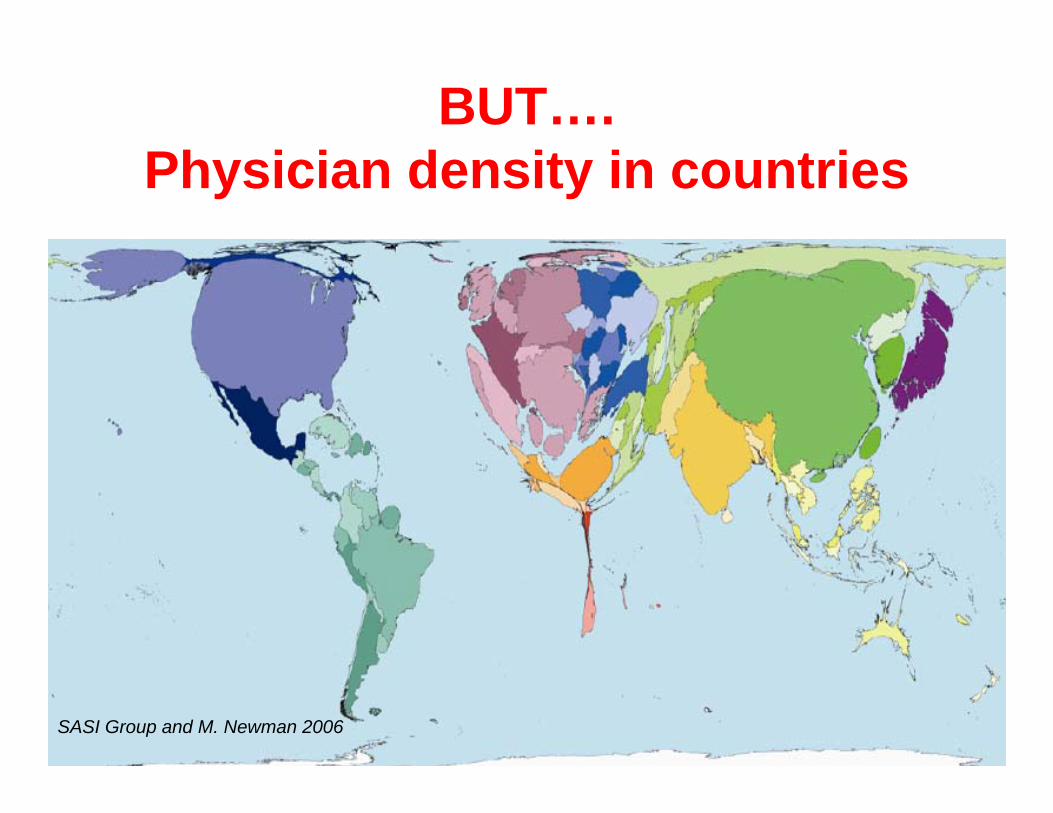
BUT….Physician density in countries
SASI Group and M. Newman 2006

When?Birthday is the riskiest day of life
Up to 50%of neonatal
deaths are in the first 24 hours
75% of neonatal deaths are in
the first week –3 million deaths
Source: Lawn JE et al Lancet 2005 Based on analysis of 47 DHS datasets (1995-2003) 10 048 neonatal deaths)
Birth and first week is key: yet coverage of care is lowest
for mothers and babies Over 50 million women deliver
at home every year
Crucial time for midwives, obstetricians
and paediatricians to be an effective
team especially as very few
neonatologists in Africa

Neonatal deaths and equity in Nigeria
DHS data analysis, published in Opportunities for Africa’s newborns, Lawn JE, Kerber KJ eds 2006
Neonatal mortality rate (per 1000 live births)
Income quintile
23
Highest income quintile
59
Lowest income quintile
If all the families in Nigeria received the same care as the richest, then NMR would be halved:127, 000 fewer newborn deaths each yearHCPs can play a crucial role in both advocating
for care for the poorest families, but also advancing this in policy and action
4 million neonatal deaths:
Scaling up effective interventions – coverage
and quality

Preterm, 25%
Asphyxia, 24%
Tetanus, 6%
Diarrhoea, 4%
Congenital, 6%
Other, 7%
Sepsis/ pneumonia,
28%
Infections
39%
Source: Opportunities for Africa’s Newborns, 2006. Based on vital registration for one country and updated modeling using the CHERG neonatal methods for 45 African countries using 2004 birth cohort, deaths and predictor variables.
WHY?1.2 million African newborns deaths
3 causes account for 88%
of neonatal deaths

Reaching 90% of women and babies with 16 proven interventions delivered through
packages could reduce neonatal mortality by up to 67% saving up to 2.7 million deaths per year
The Lancet Neonatal Survival series (2005)LI
VES
Additional cost of providing these interventions isUS$ 4.1 billion annually or $0.96 per capita
70% of costs benefit mothers & older childrenCO
ST

Coverage along the continuum of care is low
6942
830
65
0
25
50
75
100
Antenatal care(at least one
visit)
Skilledattendant at
birth
Postnatal carewithin 2 days
for homebirths*
Exclusivebreastfeeding
<6 months
DPT3vaccination
Cove
rage
(%) f
or 4
6 co
untr
ies
in
sub-
Saha
ran
Afric
a
The days of highest risk for mother and childhave the lowest coverage of care
* Postnatal care is only measured for home births in most Demographic and Health Surveys.Source: Opportunities for Africa’s Newborns, inputs from 28 African DHS from 1998-2005

MaternalSeries2006 Repro-
ductiveHealthSeries2006
Proliferating interventions and proliferating Lancet series..
Child develop
ment series 2007
Newborn 2005
Child 2003
Over 190 single
interventions listed
Need to package the interventions and strengthen existing programmatic platforms to reach families.
A paradigm shift to MNCH continuum of care
Nutrition series

ChildhoodNewborn/postnatalPre-pregnancy Pregnancy
Fam
ily/c
omm
unity
Out
reac
h/ou
tpat
ient
Clin
ical
Pr
imar
y /
Firs
t re
ferr
al
Ref
erra
lDelivery of interventions
Source: Lawn JE DCP chapter adapted for Lancet neonatal series executive summary
Birth

ChildhoodNewborn/postnatalPre-pregnancy Pregnancy
Fam
ily/c
omm
unity
Out
reac
h/ou
tpat
ient
Clin
ical
Pr
imar
y /
Firs
t re
ferr
al
Ref
erra
l
ANTENATAL CARE
- 4-visit focused package
- IPTp and ITN for malaria
- PMTCT for HIV/AIDS
POSTNATAL CARE–Promotion of healthy behaviours
–Early detection and referral of complications–Extra care of LBW babies–PMTCT for HIV
–Knowledge newborn care and breastfeeding
–Emergency preparedness
–Healthy home care including: promotion of exclusive breastfeeding, hygienic cord/skin care, keeping the baby warm, danger sign recognition and careseeking for illness
–Where referral is not available consider case management for pneumonia malaria, neonatal sepsis
–Where skilled care is not available, clean delivery and immediate newborn care including hygiene, warmth and early initiation of breastfeeding
–Adolescent and pre-pregnancy nutrition
–-Education
–Prevention of HIV and STIs
Integrated MNCH packages in the continuum of care
PREVENTIVE CHILD CARE
–Immunisations
–Malaria ITN
–Nutrition
–Care of children with HIV including cotrimoxazole
Source: Kerber KJ, Lawn JE et al Lancet in press
CHILDBIRTH CARE
–Emergency obstetric care
–Skilled obstetric care and immediate newborn care (hygiene, warmth, breastfeeding) and resuscitation, PMTCT
EMERGENCY NEWBORN AND CHILD CARE - Integrated management of childhood illness (IMNCI)
–Extra care of preterm babies including kangaroo mother care
–Emergency care of sick newborns
–Care of children with HIV
- Post-abortion care, TOP where legal
- STI case mx
REPRODUCTIVE HEALTH CARE
- Family planning
- Prevention & management of STI & HIV
- Folic acid
Birth
Childbirth care
Antenatal care
Adol-escenthealth
Postnatal care
Child health care

ChildhoodNewborn/postnatalPre-pregnancy Pregnancy
Fam
ily/c
omm
unity
Out
reac
h/ou
tpat
ient
Clin
ical
Pr
imar
y /
Firs
t re
ferr
al
Ref
erra
l
ANTENATAL CARE
- 4-visit focused package
- IPTp and ITN for malaria
- PMTCT for HIV/AIDS
POSTNATAL CARE–Promotion of healthy behaviours
–Early detection and referral of complications–Extra care of LBW babies–PMTCT for HIV
–Knowledge newborn care and breastfeeding
–Emergency preparedness
–Healthy home care including: promotion of exclusive breastfeeding, hygienic cord/skin care, keeping the baby warm, danger sign recognition and careseeking for illness
–Where referral is not available consider case management for pneumonia malaria, neonatal sepsis
–Where skilled care is not available, clean delivery and immediate newborn care including hygiene, warmth and early initiation of breastfeeding
–Adolescent and pre-pregnancy nutrition
–-Education
–Prevention of HIV and STIs
Reality for the delivery of integrated care
PREVENTIVE CHILD CARE
–Immunisations
–Malaria ITN
–Nutrition
–Care of children with HIV including cotrimoxazole
Source: Lawn JE DCP chapter adapted for Lancet neonatal series executive summary
CHILDBIRTH CARE
–Emergency obstetric care
–Skilled obstetric care and immediate newborn care (hygiene, warmth, breastfeeding) and resuscitation, PMTCT
EMERGENCY NEWBORN AND CHILD CARE - Integrated management of childhood illness (IMNCI)
–Extra care of preterm babies including kangaroo mother care
–Emergency care of sick newborns
–Care of children with HIV
- Post-abortion care, TOP where legal
- STI case mx
REPRODUCTIVE HEALTH CARE
- Family planning
- Prevention & management of STI & HIV
- Folic acid
Birth
Childbirth care
Postnatal care
Antenatal care
Adol-escenthealth
Child health care
Sick baby and child care in
hospital
Antenatal care
Emergency obstetricand neonatal care
Skilled attendance
IMCI
Behaviour Change and community mobilisation, community IMCI
PMTCT of HIV
Malaria programmes
Familyplanning
Adol-escent & school
programs
RoutinePostnatal
care
Nutrition programmes
Behaviour change and community mobilisation, community IMCI
Routinepostnatal
care

Ingredients for quality of care• Health system components (HARDWARE)
– Staff: numbers and skill mix, – Sites: infrastructure and equipment– Supplies: drugs and disposables
• Quality improvement process (SOFTWARE)– Norms, standards – Guidelines, training (nb preservice) and supervision– Review: audit including mortality review– Accountability for action (audit loop), and
rewards/motivation
Multiple approaches to quality improvement QI, QAP, TQM, PDQ, CORE……
Similar ingredients and process yet each like a separate sect!

4 million neonatal deaths:
Roles for HCPs in improving quality of care to save newborn lives –
what works?
HCPs and newborns
IPA and SNL joint initiativeGlobal movement for paediatricians to
advocate and act for newborn survival and health
• Obstetricians
• Paediatricians
• Midwives• Nurses• Other cadres can also play a key role
especially with HR crisis – eg extension workers such as HEWs and HSAs

• Assess the situation and act– Provide technical support for national planning and for
public health policy (standards, norms and guidelines) and use/adapt guides such as:• Hospital Pocket book (WHO, CAH)• Managing Newborn problems (WHO, MPS)• IMCI young infant algorithm (WHO, CAH)• Essential newborn care and Kangaroo mother care (
• Audit deaths and quality of care
• Advocate and promote and accountability– Better facilities, better supplies, better access
especially for the poorest– Promote and enable appropriate community
involvement and care
• Applied research
What can HCPs do?

69% 54% 59% 10% 11% 11%0%
25%
50%
75%
100%
Antenatalcare (at least
1 visit)
Antenatalcare (4visits)
TetanusToxoid
IPTp (malaria)
PMTCT forHIV (mother
dose)
PMTCT forHIV (baby
dose)
Cov
erag
e
.
Missed opportunity
Improving quality in existing high coverage packages eg Antenatal care
Source: Opportunities for Africa’s Newborns, Lawn JE, Kerber KJ eds 2006

Use Audit Eg. Perinatal audit in South Africa
• Facility-based mortality audit using standard format and free software (Perinatal Problem Identification Programme (PPIP))
• Each site meets for regular perinatal mortality review with all team members
• Data used for: – local quality improvement – national database held by Medical Research Council, with 3 yearly
publication linked to National and Provincial Departments of Health
• Started in October 1999, now includes 164 sites covering ~20% ofthe national births
• As of 2005 also have child audit - Child PIP
Source: Saving Babies V: Fifth perinatal care survey of South Africa (2003 to 2005) www.ppip.co.za

Avoidable causes of perinatal death (21,525 perinatal deaths, 2003 – 2005)25% have a defined avoidable cause
Source: Saving Babies V: Fifth perinatal care survey of South Africa (2003 to 2005) www.ppip.co.za
35%Inadequate intrapartum fetal monitoring / delaysInadequate neonatal management plan / delaysAntenatal steroids not given
Personnel & practices
19%Delay in transport Inadequate facilities/equipmentStaff not enough or not correctly trained or rotated too oftenLaboratory facilities/tests not available egsyphilis
Policy & admin
38%No antenatal careDelay in careseeking for danger signs
Patient & family
% of avoid-able deaths
ExamplesWhere in system?
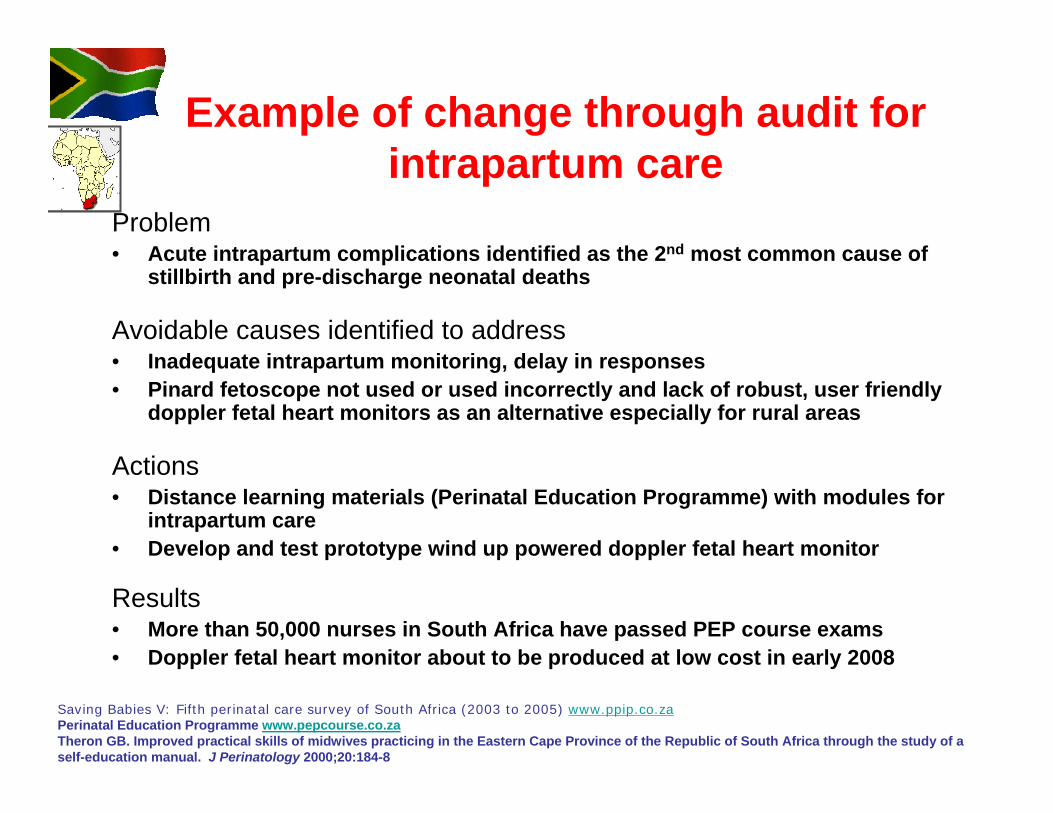
Example of change through audit for intrapartum care
Problem• Acute intrapartum complications identified as the 2nd most common cause of
stillbirth and pre-discharge neonatal deaths
Avoidable causes identified to address• Inadequate intrapartum monitoring, delay in responses• Pinard fetoscope not used or used incorrectly and lack of robust, user friendly
doppler fetal heart monitors as an alternative especially for rural areas
Actions• Distance learning materials (Perinatal Education Programme) with modules for
intrapartum care• Develop and test prototype wind up powered doppler fetal heart monitor
Results• More than 50,000 nurses in South Africa have passed PEP course exams• Doppler fetal heart monitor about to be produced at low cost in early 2008
Saving Babies V: Fifth perinatal care survey of South Africa (2003 to 2005) www.ppip.co.zaPerinatal Education Programme www.pepcourse.co.zaTheron GB. Improved practical skills of midwives practicing in the Eastern Cape Province of the Republic of South Africa through the study of a self-education manual. J Perinatology 2000;20:184-8

Newspaper headline August 2007
Influence public knowledge about quality of care
Happy result – Paediatricians, Save the
Children and others worked with
government to run a newspaper
supplement on Kangaroo Mother Care as
a simple, low cost solution

Everyone has a role to play…Ambassador Mongella, President of the Pan-African Parliament, 2006
“As government officials to lead
As policy makers to guarantee essential interventions and equity
As partners and donors to support programmes
As health workers to provide
Let us all play our part!
Source: Opportunities for Africa’s Newborns, Lawn JE, Kerber KJ eds 2006

Zikomo kwambiri! Asante sana, Ye dewaesepii! Danke! Merci beaucoup! Obligado!
Thank you !


















