
How Exceptional is New York as an Immigrant City? Nancy Foner.
SARWER-FONER AND OTHERS: PHENELZINE IN DEPRESSION 991
DEPRESSIVE STATES AND DRUGS.II.-THE STUDY OF PHENELZINEDIHYDROGEN SULFATE (NARDIL)IN OPEN PSYCHIATRIC SETTINGS*
G. J. SARWER-FONER, M.D.,tE. K. KORANYI, M.D.,+
A. M1ESZAROS, M.D.§ and H. GRAUER, M.D.,4iMontreal
BETA phenylethylhydrazine dihydrogen sulfate, apowerful inhibitor of monoamine oxidase,1 knowvncommercially as Nardil,1f was assessed in the opeiipsychiatric wards of Queen Mary Veterans Hospital,in selected patients of the geriatric unit at Ste.Anne's Veterans Hospital and Mount Sinai Sana-torium, and in selected outpatients of the PsychiatricDrug Clinic at the Jewish General Hospital, Mont-real, from July 1958 to June 1959.Twelve of these were inpatients of the psychiatric
section of Ste. Anne's (geriatric unit); 22 were
inpatients at Queen Mary Veterans Hospital, Mont-real; 5 were inpatients at Mount Sinai Sanatorium,Prefontaine; and 18 were outpatients from thePsychiatric Drug Clinic at the Jewish GeneralHospital. Three other outpatients completed theseries. Thus 60 patients formed this series, of whom39 were inpatients and 21 were outpatients (46were male, 14 were female).
Selection of patients: No suicidal or markedlyagitated patients were selected for our series. Inthe open hospital settings, or in the drug clinicor general outpatient department, it is not feasibleto attempt treatment of this type of patient withdrugs. This point of view has been elaboratedelsewhere.2-5 Research design was essentially thatdescribed for our other drug projects investigatingalleged antidepressive drugs.For the inpatients at Q.M.V.H., screening tests
for toxicity were done before the administration ofthe drug and then on a weekly basis. These were
the usual screening tests previously described,2' 3, 5 7
and consisted of determination of hoemogram, pro-thrombin time, serum proteins, albumin/globulinratio, and bilirubin, direct and indirect van denBergh reaction, cephalin-cholesterol flocculation,and fasting blood sugar, and a complete urineanalysis.The research design, the selection of patients
and the manner in which the observations are madeand charted have been described in detail else-
*Fromi the Departnment of Psychiatry, Queen Alary VeteransHospital, Jewish General Hospital, Ste. Anne's Veterans Hos-pital an(d McGill university Faculty of Medicine, Montreal,Qtue.tConsultant in I'sychiatry, Director of Psychliatric Reseairch,Queen Mary Veterans Hospital; Lecturer in Psychiatry, MIc(illt'niversity Factulty of Medicine; Assistant I'sychiatr ist. JewishGeneral Hospital, MIontreal.$Aesearc(h scientist in Psychiatry, Queen Mary Veterans Hos-pital, Montreal.§StaiffPsychiatist, Ste. Anne's-Veteralns Hospi al, Ste-Anne-
de-flellevue, P.Q.1TResearch Fellow in Psychiatry, Queen Mary Veterans Hos-
pital, Mlontreal.IlStipplied through the cour-tesy of D'. H S. Dunhamii, MedicalDirectoi', Wtarner-Chilcott Laboratories, Canada.
where.2' 3' 5' 7 The drug treatment team \vhich super-vises this work has also been commented upon.3 5
Psychotherapy continued for all patients. Thereasons for this have been amply elaborated on inprevious publications.2 3' 5-9 The high doctor-patientratio, the ward setting and orientation of the wardstructure have also been set forth in detail.2' 5Our comments on the nature of depression, and
on the need to understand the feelings of thepatient, his psychodynamic level and his individual-ized reactions may be read elsewhere in detail.' 1
It will suffice here to mention the following:each patient should be studied as a person againsthis own set of current difficulties and against histotal background.
In a largely open hospital setting, and in thepsychiatric drug clinic of the J.G.H., as well as in a
general outpatient setting, the majority of patientsseen with depressive disorders have deeply rootedconflicts over loss of love, attention and prestige,and at the same time are often avidly seeking thereturn of such gratifications. They have thereforemarked oral, dependent needs, and their conflictsover passivity and receiving are often great. It mustbe kept in mind that the majority of such patientsusually do well in supportive psychotherapy andrelationship therapy, where the therapeutic situa-tion gratifies many of the abovementioned needs.The necessity therefore of differentiating betweenpatients who are remitting from their illness becauseof the abovementioned factors and those who are
responding to the specific effects of a drug becomesof considerable theoretical importance. Two factorsother than the psychodynamics and evolution ofthe patient's illness are of considerable help inassessing this. These are: (a) the "pharmacologicalprofile" of the drug and the specific-patient-responseto it (if any), and (b) the time relationship be-tween the presence of this specific "pharmacologicalprofile" and the remission of the depressive ill-ness.3-5' 9I11 All the other information on the inter-personal relations of the patient, the changes in histhinking, feeling, mood, affect, use of muscularenergy and channelling of his various drives (actiontendencies) as manifested in psychotherapy and inhis daily behaviour, are used to help evaluate thefirst two factors mentioned.2-5 +' 8' ' 15 1"
Orality, passivity-dependency and depression.-Many of these patients have problems of loneli-ness 17,19 and feelings of abandonment. Providedthe physician takes care of these problems, thepatients nay tend to do well in hospital or inoffice pr-actice over a period of time. These patientsmay differ in regard to their ability to respond tohuman contact in a short period of time from manvof the cases more commonly seen with psvchoticdepression in mental hospitals referred to by manyof our colleagues as the group of so-called "endo-genous depressions". It is most important to accentthis point because the results obtained in our handsin our studies2 5-9' 19 were always by a combina-tion of psychotherapy, care and support, plus
Canad. M. A. J.Dec. 15, 1959, vol. 81
992 SARWER-FONER AND OmBERS: PHENELZINE IN DEPREsSION Canad. M. A. J.Dec. 15,1959, vol. 81
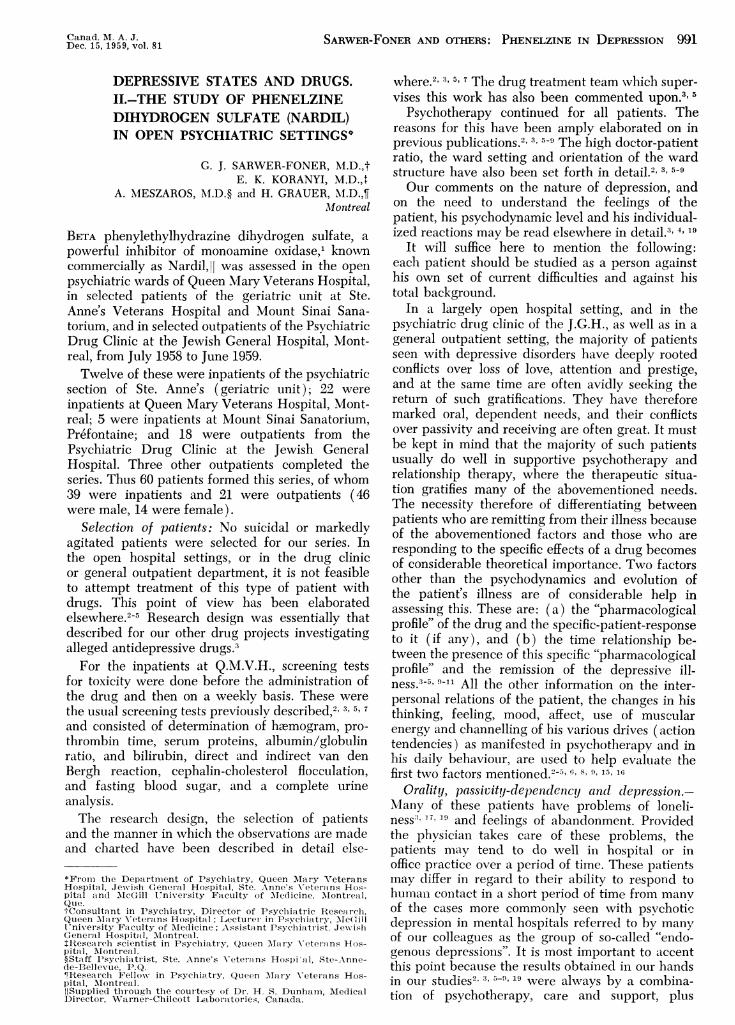
TABLE I.-DIAGNOSTIC CATEGORIES
Inpatients Outpatients
Schizophrenic reactions.............................schizo-affective type .......... ............ 2paranoid type with dependent features...... 1chronic residual type with dependent features 2
Anxiety reactions..................................in a mental defective (moderate) I.Q. 67-
with dependent features ............... 1in a passive-dependent personality with de-
pendent features .......... ............ 1Chronic brain syndromes............................
with epilepsy and dependent features ....... 1with cerebral arteriosclerosis and dependent
features ..... 4with Korsakoff's syndrome ................ 1with parkinsonism .......... ............. 1with bilateral cortical atrophy ............. 1with chronic hypoxia ..................... 1
Psychotic depressions.Chronic.
Manic-depressive reactions.depressed .
Schizoid pereonalities with depressive features.Depressive reactions.
in passive-dependent personality........... 9in passive-dependent personality with
advanced pulmonary tuberculosis........ 1in passive-dependent personality with
duodenal ulcer ........................ 1in passive-dependent personality with
marked obesity ............. .......... 1in obsessive-compulsive personality with
depressive features .......... .......... 5
5 Schizophrenic reactions ..............................schizophrenia, affective type with dependent
features ........................... 1paranoid type with dependent features...... 1
2 Anxiety reactions ...................................in a passive-dependent personality with
dependent features
9 Chronic brain syndrome.
2
1
317
Total ..;.................................. 39
administration of a drug to a patient-populationlargely consisting of oral, passive-dependent people.Many of the total therapeutic outcomes cannottherefore be directly attributed to the action ofthe drug only.Crude data.-Table I shows the diagnostic cate-
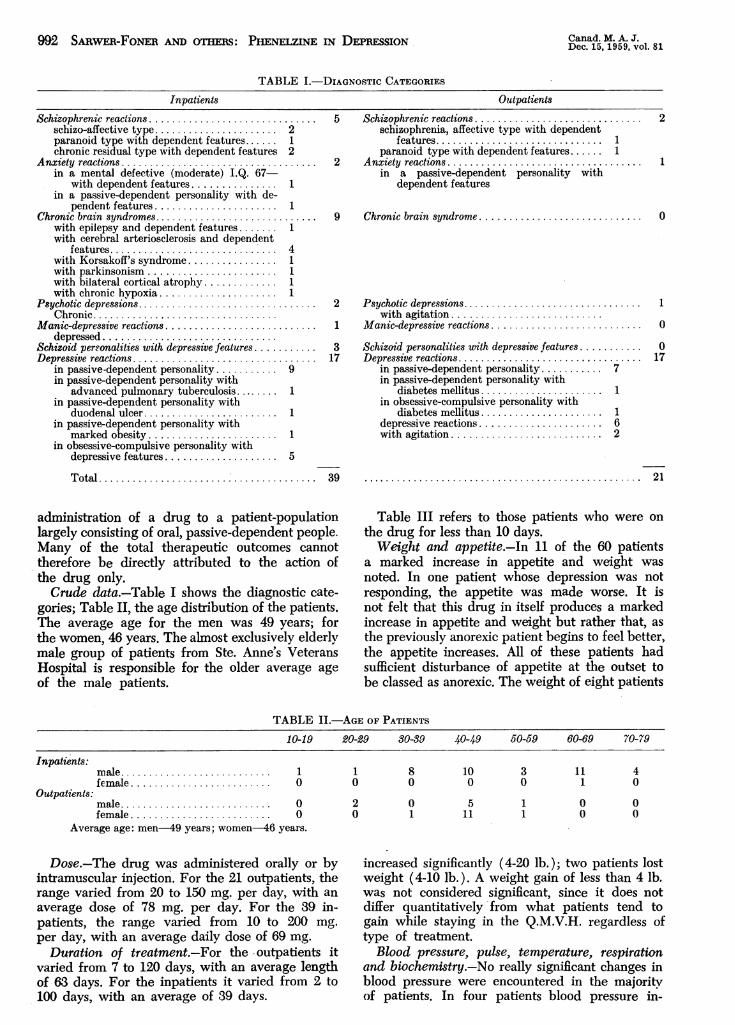
gories; Table II, the age distribution of the patients.The average age for the men was 49 years; forthe women, 46 years. The almost exclusively elderlymale group of patients from Ste. Anne's VeteransHospital is responsible for the older average ageof the male patients.
Psychotic depressions..............................with agitation..........................
Manic-depressive reactions..........................
Schizoid personalities with depressive features ...........Depressive reactions................................
in passive-dependent personality........... 7in passive-dependent personality with
diabetes mellitus ........... ........... 1in obsessive-compulsive personality with
diabetes mellitus ........... ........... 1depressive reactions .......... ............ 6with agitation ................ ........... 2
2
1
0
1
0
017
...................... ............... ..................21
Table III refers to those patients who were onthe drug for less than 10 days.Weight and appetite.-In 11 of the 60 patients
a marked increase in appetite and weight wasnoted. In one patient whose depression was notresponding, the appetite was made worse. It isnot felt that this drug in itself produces a markedincrease in appetite and weight but rather that, asthe previously anorexic patient begins to feel better,the appetite increases. All of these patients hadsufficient disturbance of appetite at the outset tobe classed as anorexic. The weight of eight patients
TABLE II.-AGE OF PATIENTS
10-19 20-29 30-39 40-49 50-59 60-69 70-79
Inpatients:
Outpatients:
male...........................female .........................
male ..0female ..0
Average age: men-49 years; women-46 years.
Dose.-The drug was administered orally or byintramuscular injection. For the 21 outpatients, therange varied from 20 to 150 mg. per day, with anaverage dose of 78 mg. per day. For the 39 in-patients, the range varied from 10 to 200 mg.per day, with an average daily dose of 69 mg.
Duration of treatment.-For the .outpatients itvaried from 7 to 120 days, with an average lengthof 63 days. For the inpatients it varied from 2 to100 days, with an average of 39 days.
1 1 8 10 3 11 40 0 0 0 0 1 0
2 0 5 10 1 11 1
o oo 0
increased significantly (4-20 lb.); two patients lostweight (4-10 lb.). A weight gain of less than 4 lb.was not considered significant, since it does notdiffer quantitatively from what patients tend togain while staying in the Q.M.V.H. regardless oftype of treatment.
Blood pressure, pulse, temperature, respirationand biochemistry.-No really significant changes inblood pressure were encountered in the majoritvof patients. In four patients blood pressure in-

SARwER-FONER AND OTHERS: PHENELZINE IN DEPRESSION 993
TABLE III. PATIENTS ON DRUG FOR 10 DAYS OR LESS
Case
18 Patient began to feel better after two weeks of hospitali-zation and one week of the drug. Insisted on returningto work, since he was "beginning to feel better". Dis-charged home. On drug for seven days.
19 On drug for eight days; had begun to feel better, but hisphysician felt that he would recover more quickly withECT. Drug therefore discontinued.*
24 On drug for five days; physician felt that patient wouldrecover more quickly with ECT. Drug discontinued.*
29 After receiving drug for four days, the patient com-plained of increased inner drive, anxiety and restless-ness. Physician discontinued the drug and gave thepatient subcoma insulin.*
33 Had shown such considerable improvement within aweek that the physician felt the drug was no longernecessary.
43 Needed medical investigation for an organic illness.Drug was discontinued for this reason.
46 Outpatient stopped taking the drug without consultingthe physician because it made her "dizzy".
*Our research design did not permit a patient to receive anorganic adjuvant such as ECT or insulin as well as the drugand remain a part of the series.
creased, in two of them by 15-25 mm. Hg; in onecase the blood pressure fell, and this was a patientwho was "made tired", "weak", and showed anxietyand insomnia. The pulse rate increased in threeand fell in two; respiration did not alter signifi-cantly. We therefore feel that no significant changesin blood pressure, pulse or respiration resultedfor the majority of patients, and that one cannotnecessarily attribute the increase in blood pressureto the effect of the drug. Nevertheless some patientswho became hypomanic or manic did tend toshow an increase in blood pressure. It wouldtherefore seem t-hat in select cases this drug iscapable of producing fairly intense stimulationand a blood pressure rise will be seen in some ofthese patients, as well as an increase in pulse rate.Only one patient had a significant fall in bloodpressure in this series, but the literature reportsothers who did show postural hypotension.'3There were no significant changes in the bio-
chemical findings and no evidence of toxicity inour screening tests in this series.
TABLE IV.-SIDE EFFECTS*Dizziness ....................................
Indigestion .................Bitter taste in mouth........................Weaknesst, tiredness, tremulousness ...........Drowsiness ..................................Insomnia ....................................
Impotence ...................................Subjective sensation of muscular stiffness.Developed hypomanic reactions$t..............Developed manic reactions-
(after 30 days of drug orally)..............
6 patients4 "
1 patient6 patients2 "1 patient1 "1 "4 patients
1 patient
*Only those reactions which were severe enough to causemarked subjective discomfort to the patient were classed asside effects.
tOne of the patients who complained of weakness, tirednessand tremulousness also displayed marked sweating and palpita-tions.
+Three of the hypomanic reactions developed graduallywhile the drug was administered; in one case (No. 5), however,it developed rapidly after the patient had received it by theintramuscular route for 14 days.
Side effects.-Table IV lists the side effects. Sixpatients complained of dizziness. Three patientswere made markedly drowsy; four complained ot
indigestion. Those receiving the drug by intra-muscular injection complained of a burning sensa-
tion for a few moments after the injection; no
induration, abscess or swelling developed. Thepatients who complained of indigestion had a
feeling of the presence of gas, burning, or
constipation. One patient (Case 59) said the drugrendered him impotent, after 63 days of adminis-tration. He nevertheless felt that on the whole thedrug had helped him with his depression. Onewho became manic complained of sleeplessness,and another said that he felt tired, sweaty andweak. A total of six patients was made markedlyweak, tired and tremulous; one of them also ex-
perienced palpitations and sweating.Changes in major symptoms.-The shifts of
major symptoms described here are those seen inany patient recovering from a depression whileunder any form of treatment. In this setting theyoccurred with psychotherapy and phenelzinetherapy in a group composed of passive-dependent,orally deprived patients with neurotic depressions.Those who improved showed a significant
change in the following: withdrawal and apathy,with a resulting increase in activity in 27 cases;mood, happier and more cheerful in 25 cases;interpersonal relations and object relationships weremarkedly improved in 24 cases. By the latter ismeant the way in which they related to otherpeople, to their doctor, to nurses and to themselves.A feeling of a more pleasant, and at the same timeincreased, inner drive was seen which was usuallyassociated with an increase in energy available forexternal activities and events. In other words, theopposite of psychomotor retardation was witnessedin 25 patients who improved. They showedamelioration of mood and an increase in the energyavailable for reality testing and for external rela-tionships, with improvement in object relationshipsand in their interpersonal relationships.
Six patients experienced marked tiredness,sleepiness and increased fatigue. One of thesecomplained of an inner tremulousness; anotherpatient complained of an increase in "inner tension",but without becoming hypomanic or manic. Fivepatients showed an increase in anxiety while on
the drug.One patient became manic and four patients be-
came hypomanic, one of these after 14 days ofintramuscular injections. Another became manicafter 30 days of drug administration orally. Thusone sees in the selected case the stimulating effectof this drug. It has the capacity to increase energyand inner affective drive, and thus to improveobject relationships as the available energy forrenewed object relationships becomes accessible tothe patient. The manic and hypomanic episodes infive patients and the increase in anxiety withoutother evidence of hypomania, although with feelings
Canad. M. A. J.Dec. 15, 1959, vol. 81

994 SARWER-FONER AND OTHERS: PHENELZINE IN DEPRESSION
of increased inner tension and drive, in six otherpatients are further evidence of its stimulatingeffects. No other behavioural reactions or serioustoxic reactions were noted in this series.
Subjectively 33 patients felt that they were
"helped" by the drug. For one of these, even
though he felt "helped", further treatment in an-
other setting was necessary. In this last patient,the pharmacological effects of the drug were presentand helpful, but the total therapeutic outcome forthe period of hospital stay described was not goodenough to relieve his symptoms sufficiently, andfurther treatment in a closed setting was foundnecessary. Table V analyses the cases which were
TABLE V.-PATIENTS "NOT HELPED" OR "MADE WORSE"WHILE ON THE DRUG
Thirteen patients did not show sufficient change in theirdepressive symptomatology to be considered "helped". Nine ofthese had received adequate doses of the drug, and over asufficient time for it to act, while four others were given aninsufficient dosage.
Case 15-Did not show alleviation of depressive sympto-matology. This was a schizophrenic patient with residualdepressive symptoms who had been hospitalized in a closedsetting for 39 years.
In the case of five patients they either were given the drugfor an insufficient length of time or had received a dose ofdrug, early in our experience with it, insufficient for adequatepharmacological action, or had the drug discontinued for otherreasons. (Cases 43, 46, 29, 24 and 19-dealt with in TableIII.)
Two patients exhibited the typical pharmacologicalactivity of this drug and had the target symptoms alleviated.The total therapeutic outcome however did not allow us toconsider them as "helped" despite the "good" effect on targetsymptoms.
Case 6-Became manic and was "made worse".Cases 5, 30, 1, 23-Became hypomanic and were "made
worseCase 13-Showed a steady worsening of his depressive
illness.
Thus: 23 patients were "helped".21 patients were "not helped".6 patients were."made worse".
"not helped" or were "made worse". Twenty-onepatients felt they were "not helped". Three ofthese had received an inadequate dosage of thedrug; six had either an inadequate dosage or didnot receive it for a length of time sufficient topermit adequate pharmacological effects to occur.
One other patient who felt that he was "nothelped" had the target symptoms controlled butexpected the drug to do much more than this.Six patients were "made worse"; four of thesebecame hypomanic and one, manic. The depressionof the remaining patients continued to worsen whileon the drug.Evidence of pharmacological profile.-The earliest
evidence for onset of drug action was obtainedafter two to six days. This occurred in the minorityof patients, but when present was crystal-clear.In many patients, although the pharmacologicaleffects of the drug were present by then, therewas no necessary fundamental change in the de-pression for two to six weeks after this. Oftensome alleviation of the depressed state had begunin this time, although full-scale remission had not
Canad. M. A. J.Dec. 15, 1959, vol. 81
been reached. The concept of George H.Alexander'0 is important in this regard. He feltthat, in the treatment of a depressed state with anorganic agent, any improvement occurring afterthe first month of such treatment with an inpatienthospital group might be due to a natural remission.Because of this, one should regard with suspicionall "good" results in depressive states that areproduced after many weeks or months of adminis-tration of an alleged anti-depressant drug in aninpatient setting. In our patients, who were mainlya passive-dependent, orally deprived group suffer-ing largely from neurotic depressions, the additionalfactors of care and human attention operatingover a period of time played an important rolein therapy. Therefore, in order to be able to linkimprovement specifically to the effects of a drug,one must be able to relate it in terms of timerelationships to the occurrence of the pharmaco-logical effect of the drug, and to the patient's re-action to this effect. Further, the improvement mustoccur in a short period of time and bear a one-to-onerelationship to the drug effect, before one canattribute improvement to it. For patients in ourseries who took longer than four weeks to improve,this was therefore difficult to do.3-"' ,15 16 Mostpatients who improved began to show improvementwithin one month of treatment. In most cases, therewas agreement between staff and patients as towho were helped or not helped. The exceptionshave already been discussed.
Transference effects2' 3. 6- and reality factors3' 6-
enter into the action of all drugs, and more parti-cularly with drugs given to passive-dependentpatients, in a most important way. We feel thatthese factors more than otitweigh the pharmaco-logical effects of the drugs in the majority oftypes of patients we have dealt with suffering fromdepressive illness. Examples of this are quoted inother publications.3 6
Sainz,14 for example, felt that phenelzine did notproduce as good results with reactive depressionsas with the "endogenous" group and recommendedit mainly for the latter. We feel that reality affect-provoking factors are always of prime importancein determining the clinical state of the patient, andthat the overriding effect of these, at least in thetype of patient seen in our studies, is more im-portant than the drug effect in most patients.3The manner in which the patient is treated, andwhat is offered to the patient, or the modalitiesin which he can be permitted either to improve orget worse (in hospital, in an open or closed setting,with support and psychotherapy; hospital and psy-chotherapy plus drug treatment; hospital plusdrug treatment; office supporting visits; office psy-chotherapy plus drug) help channel the ways inwhich improvement takes place. It must be remem-bered in this regard that even considering all thatwe offer the patient in the way of treatment, it isstill the patient who gets well or doesn't. Thetreatment is still nonspecific in the sense of a

Dec. 15, 1959, vol. 81 SARWER-FONER AND OTHERS: PHENELZINE IN DEPRESSION 995
specific antibiotic. In psychiatry the patient usesour help to help himself recover. Bleuler's18comments about the need for humility in thephysician as to his own therapeutic specificity(although made about the treatment of schizo-phrenia) seem to the authors to apply equallywell to all psychiatric conditions. The patient doesthe work and gets better; the physician helps himdo this. This applies even to those most funda-mental and real changes produced in a patient bypsychoanalysis.
CONCLUSIONS
Phenylethylhydrazine dihydrogen sulfate orphenelzine (Nardil) is a useful adjuvant to psycho-therapy in treatment of selected types of depressiveillness dealt with in this paper (that is, largelyneurotic or reactive depressions treated in an opensetting as outpatients, or in private practice).
Pharmacologically, phenylethylhydrazine dihy-drogen sulfate has some sympatheticomimeticpotential. In the occasional cases its stimulanteffects can be marked.
Phenelzine exhibited onset of pharmacologicalactivity within two to six days, characterized bybetter sleep, by a feeling of fatigue and weaknessin many, and sometimes by dizziness and tremu-lousness. As its action continued, usually withinone month, some tendency for increased motoractivity, improved mood, better relationship todoctors, patients and nurses, increased feeling ofinner drive (action tendencies), better appetite,and improved sleep when these were previouslyimpaired, was seen. In our series this was seenin 42 of the 60 patients. Only 33 of these wereclassed as "helped" in terms of the total therapeuticoutcome. It must be remembered in regard to thetotal therapeutic outcome that improvement oc-curred in the patients in this series with the use ofboth psychotherapy and phenelzine and, further,that the majority in this series were oral, passive-dependent patients largely suffering from neuroticdepressions.
Certain sensitive patients can become manic orhypomanic while on this drug.By intramuscular administration its action is
rapid and more pronounced than by the oral route.A burning sensation, without induration or abscessformation, is produced at the site of the injectionfor a few minutes.
Serious toxic effects were absent in this series.The blood pressture can be raised to a considerabledegree in the occasional patient (four patients inthis series). Caution is therefore indicated inpersons with an impaired cardiovascular system.One patient showed a fall in blood pressure of10 mm. Hg, with development of anxiety and in-somnia, and others have been known to developpostural hypotension.13The most frequent side effects were dizziness,
weakness, fatigue or tremulousness, sometimes with
palpitations and sweating; drowsiness, indigestion,the development of hypomanic or manic reactions,increases in blood pressure and sometimes in pulserate. Less frequent are insomnia, a sense of mus-cular stiffness, sexual impotence (one case in thisseries), hypotension and constipation. Side effectswere not prominent in the majority of patients.The doses used in this series were relatively high,
and considerably exceeded the 45 mg. daily recom-mended by the makers for initial therapy (averagefor inpatients, 69 mg. and for outpatients, 78 mg.daily).
Althouglh no toxic effects on hepatic functionwere seen in this series, the fact that othier mono-amine oxidase inlhibitors have occasionally pro-duced severe hepatic reactions should inspire closesurvey of hepatic function.The need to treat every patient as an individutal,
and avoid dependence on the chemical action of an"anti-depressant" alone, is again stressed.3-3 8,19This applies to all anti-depressant drugs.
We wish to thank Drs. MI. Aronovitch and M. Grossmanof Mount Sinai Sanatorium for their co-operation.
Drs. Rashid, Dardi, Adler, Chester, Lemieuix, Hanjeck,A. M. Marcus, Beland and Mackay contributed observationsto this study. We wish to express our appreciation to them,and lastly but by no means least, to thank the nursingstaff of the four hospitals for their very valuable observa-tions and collaboration.We wish to express our gratitude to Dr. H. S. Dunham
and the Warner-Chilcott Laboratories for their collabora-tion and support of our research program.
AddressesG. J. Sarwer-Foner, E. K. Koranyi,613 Cote St-Antoine Rd., 4631 Sherbrooke St. W.,Westmount, P.Q. Westmount, P.Q.
A. M. Meszaros, H. Grauer,Ste. Anne's Veterans Hospital, 900 Sherbrooke St. W.,Ste-Anne-de-Bellevue, P.Q. Montreal, P.Q.
REFERENCES
1. CHESSIN, M. et al.: Ann. New York Aced. Sc. (in press3).2. SARWER-FONER, G. J. AND OGLE, w.: Canad. Ml. A. J., 73:
187, 1955.3. SARWEPR-FONER, G. J. et al.: Canad. Serv. BI. J., 15: 359,
1959.4. Idema: Ann. New York Acad. Sc., 80: 789, 1959.5. Idem: On a methodology of testing and clinical applica-
tions of the neuroleptic drugs in psychiatry. Read atMohawrk Valley Neuropsychiatric Society Meeting,Marcy, N.Y., Oct. 20, 1958. Psychiat. Quart. (in press).
6. Idem: Transference and non-speciflc drug effects in theu-ze of the trannmillizing driLus and thoir infl,'enee onaffect, In: Research in affects, Psychiatric ResearchReport No. 8, American Psychiatric Association, 1957,p. 153.
7. SARWER-FONER. Gr. J. AND KORANYI, E. K.: Canead. M.A. J., 77: 450, 1957.
8. SARWF:P,-FONER. (4. .1. Theoretical aspects of the m1odiwes ofactioni, In: Psychoplharnmacology frontiers, edited byN. S. Kline, Little, Brow-n & Com-lpany, Boston, 1959,p. 295.
9. SARWER-FONER, G. J. AND KORANYI, E. K.: Transferencoeffects, the attitude of the treating physician andcounter-transference in the use of the neurolepticdirugs, In: The dynamics of psychiatric cdrug therapy,edited by G. J. Sarwer-Foner, Charles C Thomi-as,Publisher, Springfleld, Ill., 1959.
10. ALEXANDER, G. H.: J. Nerv. & Ment. Dis., 99: 922, 1944.11. LEMERE. F.: Amn. J. Psyc7i at.. 116: 258, 1959.12. KING, P. D. : Ibid., 116: 64, 1959.13. SAIUNDERs, 5. C. et al.: Ibvid., 116: 71, 1959.14. SAINz, A\.: Aanq. Newc York Aced. Sc., 80: 780, 1959.15. LI.xN, BC. L. : Amw. J. Psychiet., 116: 97, 1959.16. SHERMTAN. L. J.: Ibid., 116: 208, 1959.17. FROMMA-REICHMTANN, F.: Psychiatry, 22: 1, 195,9.

996 FORTIER AND SIMARD: CHLORQUINALDOL IN PIATPRCS Dec. 15, 159, vol. 81
18. BLEULER, E.: Dementia praecox or the group of schizo-phrenias, International Universities Press, Inc., NewYork, 1950.
19. KERENYI, A., KORANYI, E. K. AND SARWER-FONER, G. J.:Depressive states and drugs. III. The use of methyl-phenidate (Ritalin) in open psychiatric settings. Inpreparation.
RE'SUAlELe sulfate bi-hydrogene de ph6nylethylhydrazine est un
adjuvant utile en psychiatrie dans le traitement de caschoisis de depression (nevroses, depressions par reaction).Au point de vue pharmacologique ce compose possedecertaines affinites sympathicomimetiques et peut memequelquefois se comporter comme un puissant stimulant. Seseffets se manifestent entre deux et six jours apr'es sonadministration par un sommeil plus profond, une sensationde fatigue ou meme faiblesse et quelquefois du tremble-ment et des etourdissements. Apres environ un mois laplupart des malades ressentent un besoin d'activite motriceaccrue, manifestent une meilleure humeur, offrent unrapport plus riche avec le therapeute et les infirmieres et
voient sourdre en eux-memes un regain d'energie. Ceseffets se sont manifestes chez 42 des 60 malades soustraitement. Le medicament cependant n'a vraiment con-tribue 'a I'amelioration therapeutique que chez 33 d'entreeux, car ces malades ont aussi regu de la psychotherapie.La plupart d'entre eux etaient des nevroses a tendanceorale, deprimes, passifs et 'a charge.
Lorsqu'administre par voie intramusculaire le phenyl-ethylhydrazine a une action plus rapide et plus prononceeque par voie orale. Le malade ressent une sensation debrulement sans induration ou abces 'a l'endroit de l'injectionpendant quelques minutes. Aucun effet toxique serieux nefut note au cours de la presente 6etude. Quelques sujetsa, sensibilite particuliere peuvent cependant verser dans lamanie ou 1'hypomanie. La tension arterielle augmentLeconsiderablement chez certains malades, presentant ainsiune contre-indication 'a son usage gen;eralise; d'autres, parcontre, ont souffert d'hypotension posturale. La posologiemoyenne fut de 69 mg. dans quelques cas et de 78 mg. dansd'autres, doses qui depassent beaucoup celle recommandeepar les fabriquants.
CHLORQUINALDOL (STEROSAN)-HYDROCORTISONE IN SKINDISORDERS OF INFANTS
PROF. DE LA BROQUERIE FORTIER andROCH SIMARD,* Quebec City, Que.
TOPICAL MEDICATION continues to occupy an im-portant place in dermatological therapy, and inrecent years potent new topically active bacterio-static and fungistatic agents have been added tothe dermatological armamentarium. Their extensionto include the peediatric dermatoses is a logicaldevelopment.
Several authors1-8 have clinically investigatedthe use of chlorquinaldol (Sterosan) in derma-tology. Recently, Robinson and Hollander9 reportedthe marked effectiveness of chlorquinaldol in thetreatment of various skin conditions includingeczema and desquamative or exfoliative erythro-dermia. One of us recently reported on the use ofchlorquinaldol''11 in infantile eczema.
It was not long after the introduction of hydro-cortisone that this agent was also investigated indermatology. Sulzberger and Witten12 in 1952published the results of their research on the useof "Compound F" or hydrocortisone acetate incertain localized dermatoses, and in 1953, Sidi,Bourgeois-Gavardin and Plas of Paris, France,'3undertook the study of this agent in eczema. Inthe United States, Lubowe16 and Pace'7 publishedthe results of their study of its use in a variety ofdermatological conditions. The present paper re-views our experience, over a two-year period, inthe use of a combined chlorquinaldol-hydrocorti-
*Paediatric Service, HOpital de l'Enfant Jesus, Quebec.Cet article est publi-6 en frangais dans l'Union Medicale duCa,nada. N.D.L.R.
sone preparation* in the treatment of eczema andother infantile dermatoses.
CLINICAL MATERIALThe following list gives the ages and dermat-
ological lesions in 36 children who received un-questionable benefit from chlorquinaldol-hydro-cortisone treatment:
Eczema:Dry or weeping ......................... 11 casesImpetiginized ........................... 6
Desquamative and exfoliative erythrodermia..... 10 "Pyodermia.................................... 4Gluteal erythema ............................. 5
It is particularly interesting to note the ages ofthe children at the time therapy was initiated(Table I).
RESULTS1. EczemaIt was noted that chlorquinaldol-hydrocortisone
was particularly effective in producing rapid relieffrom pruritus in this condition. Reduction of thepruritic factor in eczema is important in preventingythe scratching which contributes to the chronicityof the lesion. Pertinent data in some of these casesare noted below.
CASE 1.-Andre L., 7% months: Admitted to hospitalMay 29, 1957, for impetiginized eczema. The babyweighed 7.4 lb. at birth and had been artificially fed.Weaning was without incident.
At the age of 4 months small reddish blotches ap-peared on the face and soon spread to the cheeks, chin,forehead and the external parts of the ears. A fewweeks later, identical lesions appeared on the legs
*The combination of chlorquinaldol and hydrocortisone (chlor-quinaldol 3% and hydrocortisone 1%) is marketed as Stero-san-hydrocortisone by Geigy Pharmaceuticals.


















