Sanford I. Weill Professor of Metabolic Research Weill...
51
What’s New in Pharmacotherapy for Obesity Louis J. Aronne, MD, FACP, FTOS Sanford I. Weill Professor of Metabolic Research Weill Medical College of Cornell University Medical Director, Comprehensive Weight Control Center Division of Endocrinology, Diabetes, and Metabolism New York, NY
Transcript of Sanford I. Weill Professor of Metabolic Research Weill...

What’s New in
Pharmacotherapy for ObesityLouis J. Aronne, MD, FACP, FTOS
Sanford I. Weill Professor of Metabolic ResearchWeill Medical College of Cornell University
Medical Director, Comprehensive Weight Control CenterDivision of Endocrinology, Diabetes, and Metabolism
New York, NY

DisclosuresOwnership Interest:BMIQCardiometabolic Support NetworkGelesisMyos CorporationZafgen, Inc.
Board of Directors:Myos CorporationJamieson Laboratories
I am a consultant, speaker, advisor, or receive research support from:Aspire Bariatrics
Eisai Inc.
Enteromedics
Gelesis
GI Dynamics
Novo Nordisk
Pfizer
VIVUS Inc.
Zafgen Inc.
As faculty of Weill Cornell Medical College, we are committed to providing transparency for any and all external relationships prior to giving an academic presentation.


Gaps Between 2015 Obesity Pharmacology Guidelines and Actual Practice
If a patient’s response is effective (weight loss >5% of body weight at 3 mo) and safe, we recommend it be continued
If ineffective (weight loss <5% at 3 mo) or there are safety or tolerability issues, we recommend it be discontinued
J Clin Endocrinol Metab. 2015 Feb;100(2):342‐62.Pharmacological management of obesity: an endocrine Society clinical practice guideline.
Guideline Recommendations
Just under half (46%) of adults in the U.S. fit the criteria for use of anti‐obesity pharmacotherapy, but only 2% receive such treatment 1,2
1. Samaranayake NR, et al. Ann Epidemiol. 2012 May;22(5):349‐ 53. 2. Xia Y, et al. Obesity (Silver Spring). 2015 Aug;23(8):1721‐8.
Actual Practice
Less than one percent (0.7%) of eligible overweight or obese patients (n=1,835,541) received pharmacotherapy for weight lossThose who received it tended to be:• Heavier (BMI 33.6 vs. 31.3 kg/m2)• Younger (42 vs. 52 years)• Female (84.3 vs. 58.2% male)• Commercially insured (70.1 vs. 50.4%) • Used more antidepressants (30.8 vs. 14.1%)• Used more NSAIDs (21.7 vs. 12.0%) Zhang S, et al. Obes Sci Pract. 2016;doi:10.1002/osp4.46.
4

Gaps Between 2015 Obesity Pharmacology Guidelines and Actual Practice
If a patient’s response is effective (weight loss >5% of body weight at 3 mo) and safe, we recommend it be continued
If ineffective (weight loss <5% at 3 mo) or there are safety or tolerability issues, we recommend it be discontinued
J Clin Endocrinol Metab. 2015 Feb;100(2):342‐62.Pharmacological management of obesity: an endocrine Society clinical practice guideline.
Guideline Recommendations
Just under half (46%) of adults in the U.S. fit the criteria for use of anti‐obesity pharmacotherapy, but only 2% receive such treatment 1,2
1. Samaranayake NR, et al. Ann Epidemiol. 2012 May;22(5):349‐ 53. 2. Xia Y, et al. Obesity (Silver Spring). 2015 Aug;23(8):1721‐8.
Actual Practice
Less than one percent (0.7%) of eligible overweight or obese patients (n=1,835,541) received pharmacotherapy for weight lossThose who received it tended to be:• Heavier (BMI 33.6 vs. 31.3 kg/m2)• Younger (42 vs. 52 years)• Female (84.3 vs. 58.2% male)• Commercially insured (70.1 vs. 50.4%) • Used more antidepressants (30.8 vs. 14.1%)• Used more NSAIDs (21.7 vs. 12.0%) Zhang S, et al. Obes Sci Pract. 2016;doi:10.1002/osp4.46.
5

W E I L L . C O R N E L L . E D U
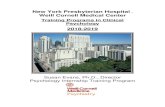
Pharmacotherapy Utilization: T2DM vs Obesity
Thomas, C et al Obesity (Silver Spring). 2016 Sep;24(9):1955-61. doi: 10.1002/oby.21533.:
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Obesity Type 2 Diabetes
U.S
. Adu
lt Po
pula
tion
(%)
Adults in the U.S.
Indicated Treated

W E I L L . C O R N E L L . E D U
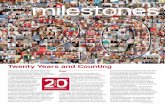
Uptake of SGLT 2s vs Ant i -Obesi ty Drugs
Title for Slide Deck 7
Prescriptions Dispensed, U.S., 2012-2015
74% Phentermine
18.6% new anti-obesity pharma
MARKETSHARE
• Thomas, C et al Obesity (Silver Spring). 2016 Sep;24(9):1955-61. doi: 10.1002/oby.21533.:

Prevalence of physicians, by medical specialty, prescribing phentermine, new anti‐obesity medications, and SGLTs U.S., 2012‐2015
Thomas CE, Mauer EA, Shukla AP, Rathi S, Aronne LJ.Obesity (Silver Spring). 2016 Sep;24(9):1955‐61. Source: Symphony Health Solutions PHAST Data Set
Obesity Pharmacology: Prescribers and Prescription Volume
% New Anti‐obesity Pharma by RegionU.S., 2012‐2015
Prescriptions Dispensed, U.S., 2012‐2015
74% Phentermine
18.6% new anti‐obesity pharma
MARKETSHARE
0
2500
5000
7500
10000
2013 2014 2015
Phentermine Qsymia Belviq Contrave Saxenda
TRx’s (000
)
7,5278,213
9,189
10.90% Compound Annual Growth Rate2
8

Case :
• A 52‐year‐old woman with obesity (BMI 38) presents with multiple comorbidities– Has a 7‐year history of T2DM and has gained a significant amount of weight
since being placed on insulin 6 months ago – Has remarkable medical history for atrial fibrillation, hypertension,
proteinuria, and sleep apnea
She was unable to lose weight after 6 months of improving her diet and increasing physical activity
T2DM: type 2 diabetes mellitus.

Interactions Among Hormonal and Neural Pathways1
AGRP: agouti‐related peptide; α‐MSH: α‐melanocyte‐stimulating hormone; GHSR: growth hormone secretagoguereceptor; INSR: insulin receptor; LepR: leptin receptor; MC4R: melanocortin‐4 receptor; NPY: neuropeptide Y; POMC: proopiomelanocortin; PYY: peptide YY; Y1R; neuropeptide Y1 receptor; Y2R: neuropeptide Y2 receptor.1. Apovian CM Aronne LJ Bessesen D et al. J Clin Endocrinol Metab. 2015;100:342‐362.

J Clin Invest. 2012 Jan 3;122(1):153‐62. doi: 10.1172/JCI59660. Epub 2011

Why Don’t People Just Lose Weight!
14% Weight Loss Produced Changes in 8 Hormones That Encourage Weight Regain
Might Need More Than One Drug
14% Weight Loss:Reduced IncreasedLeptin ‐ 65%Peptide YYCholecystokininInsulinAmylin
GhrelinPancreatic polypeptideGastric inhibitory polypeptide
Measures of appetite
10-week, lifestyle-based weight loss intervention in healthy overweight and obese adults (n=34) led to sustained elevations in appetite stimulating hormone(s) and decreases in appetite suppressing hormones
Sumithran P et al. N Engl J Med. 2011;365:1597-1604. 12NET RESULT OF THESE HORMONAL CHANGES is WEIGHT GAIN!

That’s why patients hit a weight loss plateau. Can you overcome it?
The same way you overcome hyperglycemia, or hypertension in someone who doesn’t respond
to a single agent.
Add more medication Key point : diet and behavior are like a medication – Low carb diets increase TEE
If that doesn’t work: Consider a procedure.
Key Point: Don’t give up

Shukla AP, Iliescu RG, Thomas CE, Aronne LJ. Food Order has a Significant Impact on Post–prandial Glucose Levels. Late Breaking Abstract. The Obesity Society’s 2014 Annual Scientific Meeting, Obesity Week. Boston, MA.
Bread firstVegs and chicken 15 min later
Vegs and chicken firstBread 15 min later
Good Advice:Protein and Vegs firstAUC glucose ‐73%

Antiobesity Agents and Their Mechanism of Action1
1. Apovian CM Aronne LJ Bessesen D et al. J Clin Endocrinol Metab. 2015;100:342‐362.

PHEN/TPM ER 7.5/46 Produces Greater Weight Loss thanPHEN 15 or TPM ER 92:
Combination Better Than 2x the Dose of Monotherapy
PHEN: phentermine; TPM: topiramate.1. Aronne LJ et al. Obesity. 2013;21:2163‐2171.

Weight Loss With Lorcaserin/Phentermine: Combination Produces Greater Weight Loss
N = 238
LOR: lorcaserin; IR: immediate release; QD: daily.1. Smith S et al. ObesityWeek 2014. Abstract 2053P.
a LOR/PHEN IR QD = LOR 10 mg BID + PHEN IR 15 mg QD; LOR/PHEN IR BID = LOR 10 mg BID + PHEN IR 15 mg BID; LOR + PHEN is not FDA approved for the treatment of obesity/overweight in the United States.
N = 238
3‐Month Safety Study

PHARMACOLOGICAL MANAGEMENT of
OBESITY: An Endocrine Society Clinical
Practice Guideline
January 15, 2015
. Apovian CM Aronne LJ Bessesen D et al. J Clin Endocrinol Metab. 2015;100:342‐

Pharmacotherapy for Obesity
a Mean weight loss in excess of placebo as percentage of initial body weight or mean kg weight loss over placebo.GABA: gamma‐aminobutyric acid; GLP‐1: glucagon‐like peptide‐1.
1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.
Drug Mechanism of Action Mean Weight Lossa Study Duration
Phentermine Norepinephrine‐releasing agent 3.6 kg 2 to 24 weeks
Diethylpropion Norepinephrine‐releasing agents 3.0 kg 6 to 52 weeks
Orlistat Pancreatic and gastric lipase inhibitor 2.9 to 3.4 kg(2.9 to 3.4%) 1 year
Lorcaserin 5HT2C receptor agonist 3.6 kg (3.6%) 1 year
Phentermine/topiramate
GABA receptor modulation (topiramate) plus norepinephrine‐releasing agent (phentermine)
6.6 kg (6.6%) (recommended dose)
8.6 kg (8.6%)(high dose)
1 year
Naltrexone bupropion
Reuptake inhibitor of dopamine and norepinephrine (bupropion) and opioid antagonist (naltrexone)
4.8% 1 year
Liraglutide GLP‐1 agonist 5.8 kg 1 year
19

Pharmacotherapy for Obesity:
a Mean weight loss in excess of placebo as percentage of initial body weight or mean kg weight loss over placebo.GABA: gamma‐aminobutyric acid; GLP‐1: glucagon‐like peptide‐1.1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.
Drug Mechanism of Action Mean Weight Lossa Study Duration
Phentermine resin Norepinephrine‐releasing agent 3.6 kg 2 to 24 weeks
Diethylpropion Norepinephrine‐releasing agents 3.0 kg 6 to 52 weeks
Orlistat Pancreatic and gastric lipase inhibitor
2.9 to 3.4 kg, 2.9% to 3.4% 1 year
Lorcaserin 5HT2C receptor agonist 3.6 kg, 3.6% 1 year
Phentermine/topiramate
GABA receptor modulation (topiramate) plus
norepinephrine‐releasing agent (phentermine)
6.6 kg (recommended
dose), 6.6%; 8.6 kg (high dose), 8.6%
1 year
Naltrexone bupropion
Reuptake inhibitor of dopamine and norepinephrine (bupropion)
and opioid antagonist (naltrexone)
4.8% 1 year
Liraglutide GLP‐1 agonist 5.8 kg 1 year

Common side effects of obesity treatmentsKey Point: Side Effects Guide Treatment
Drug Common Side EffectsPhentermine resin Headache, elevated BP, elevated heart rate, insomnia, dry
mouth, constipation, anxiety; palpitation, tachycardia, Diethylpropion
Orlistat Decreased absorption of fat‐soluble vitamins, steatorrhea, oily spotting, fecal urgency, oily evacuation, increased defecation
Lorcaserin Headache, nausea, dry mouth, dizziness, fatigue, constipationPhentermine/topiramate
Insomnia, dry mouth, constipation, paresthesia, dizziness, dysgeusia
Naltrexone bupropion Nausea, constipation, headache, vomiting, dizziness
Liraglutide Nausea, vomiting
1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.

Advantages and Disadvantages Associated With Weight‐Loss Medications1At present, prescribing is often based on cost and side effect profile
a Less weight loss = 2%‐3%; greater weight loss = >3%‐5%; robust weight loss = >5%. b Long‐term data is 1‐2 years.
1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.
Drug Advantages Disadvantages
Phentermine Inexpensive, greater weight lossa
Side‐effect profile, no long‐term datab
Topiramate/phentermine Robust weight lossa, long‐term data Expensive, teratogen
Lorcaserin Side‐effect profile, long‐term datab Expensive
Orlistat, prescription Nonsystemic, long‐term datab
Less weight lossa, side‐effect profile
Orlistat, over the counter Inexpensive Less weight lossa, side‐effect profile
Natrexone/bupropion Greater weight lossa, food addiction, long‐term datab
Side‐effect profile,mid‐level price range
Liraglutide Side‐effect profile, long‐term datab Expensive, injectable
22

Lorcaserin1
MAOI: monoamine oxidase inhibitor; SNRI: serotonin–norepinephrine reuptake inhibitor; SSRI: selective serotonin reuptake inhibitor.1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.
Action Mean Weight Lossa
Study Duration
Common Side Effects Contraindications
5HT2creceptor agonist
3.6 kg, 3.6% 1 year
Headache, nausea, dry mouth,
dizziness, fatigue, constipation
• Pregnancy and breastfeeding
• Use with caution:– SSRI, SNRI/MAOI– St. John’s wort– Triptans– Buproprion– Dextromethorphan
a Mean weight loss in excess of placebo as percentage of initial body weight or mean kg weight loss over placebo.

Weight Loss With Lorcaserin: BLOOM Trial1a
• Study patients: BMI 30‐45 or BMI 27‐30 with risk factors (hypertension, CVD, dyslipidemia, impaired glucose tolerance, or obstructive sleep apnea)
• At 1 year, 55.4% of patients receiving lorcaserin and 45.1% of patients receiving placebo remained in the trial
• Weight loss with lorcaserin (10 mg twice daily) vs placebo, 52 weeks
• Small but significant decreases in blood pressure in lorcaserin vs placebo groups
• Rates of headache and nausea greater in treatment vs placebo groups
ITT: intention‐to‐treat; LOCF: last observation carried forward.1. Smith SR et al. N Engl J Med. 2010;363:245‐256.
a Based on ITT‐LOCF analysis.
Weight Loss Lorcaserin(n = 1,538)
Placebo(n = 1,499) P
≥5% 47.5% 20.3% <.001
≥10% 22.6% 7.7% <.001
Mean weight loss 5.8 kg 2.2 kg <.001
24

Weight Loss With Lorcaserin: BLOOM Trial1a
• Study patients: BMI 30‐45 or BMI 27‐30 with risk factors (hypertension, CVD, dyslipidemia, impaired glucose tolerance, or obstructive sleep apnea)
• At 1 year, 55.4% of patients receiving lorcaserin and 45.1% of patients receiving placebo remained in the trial
• Weight loss with lorcaserin (10 mg twice daily) vs placebo, 52 weeks
• Small but significant decreases in blood pressure in lorcaserin vs placebo groups
• Rates of headache and nausea greater in treatment vs placebo groups
ITT: intention‐to‐treat; LOCF: last observation carried forward.1. Smith SR et al. N Engl J Med. 2010;363:245‐256.
a Based on ITT‐LOCF analysis.
Weight Loss Lorcaserin(n = 1,538)
Placebo(n = 1,499) P
≥5% 47.5% 20.3% <.001
≥10% 22.6% 7.7% <.001
Mean weight loss 5.8 kg 2.2 kg <.001

The Power of Obesity Treatment: Improvement in Multiple Risk
Factors:Lorcaserin
Lorcaserin FDA EMDAC26

Lorcaserin: Cardiometabolic Effects1
HDL: high‐density lipoprotein; LDL: low‐density lipoprotein; mITT: modified intention to treat.1. Aronne L et al. Postgrad Med. 2014;126:7‐18.
*P ≤ .001; ** P < .05; *** P < .001.

Lorcaserin: Those Who Lost ≥4.5% Total Body Weight by Week 12 Were Week 52 Responders1
Studies 009 and 011, mITT
mITT Lorcaserin BID Week 12 Completed Week 12 Completed Week 52
N = 3097 ≥4.5% weight loss 1369/3097 (44.2%) 1083/1369 (79.1%)
<4.5% weight loss 1168/3097 (37.7%) 680/1168 (58.2%)
BID: twice daily.1. Slide courtesy Dr. Steve Smith; May 10, 2012 FDA Advisory Committee Meeting.
Chan
ge, %
Key Point: if it doesn’t work, stop

Phentermine/Topiramate ER1
Action Mean Weight Lossa
Study Duration
Common Side Effects Contraindications
GABA receptormodulation
(topiramate) plus norepinephrine‐releasing agent (phentermine)
6.6 kg (recommended dose), 6.6%; 8.6 kg (high dose), 8.6%
1 year
Insomnia, dry mouth,
constipation,paresthesia, dizziness, dysgeusia
Pregnancy andbreastfeeding,
hyperthyroidism,glaucoma, MAOI,sympathomimetic
amines
ER: extended release.1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.
a Mean weight loss in excess of placebo as percentage of initial body weight or mean kg weight loss over placebo.

Weight Loss With Phentermine/Topiramate ER CONQUER Trial1a
Weight LossTopiramate/Phentermine
7.5 mg/46 mg Daily(n = 1,538)
Topiramate/Phentermine
15 mg/92 mg Daily(n = 981)
Placebo(n = 979) P
≥5% 62% 70% 21% <.001
≥10% 37% 48% 7% <.001
Mean weight loss 8.1 kg 10.2 kg 1.4 kg <.001
• Patients: BMI 27‐45 and ≥2 obesity‐related comorbidities (hypertension, dyslipidemia, type 2 diabetes, prediabetes, abdominal obesity)
• Weight loss, 56 weeks
• Dose‐related AEs: dry mouth, constipation, dysgeusia, paresthesia, insomnia, dizziness, anxiety, irritability, disturbance in attention
• Endpoint assessments were not available for 31% of participants
1. Gadde KM et al. Lancet. 2011;377:1341‐1352.
a Based on ITT‐LOCF analysis.30

Weight Loss With Phentermine/Topiramate ER: CONQUER Trial1a
Weight Loss
Topiramate/Phentermine7.5 mg/46 mg Daily
(n = 1,538)
Topiramate/Phentermine15 mg/92 mg Daily
(n = 981)
Placebo(n = 979) P
≥5% 62% 70% 21% <.001
≥10% 37% 48% 7% <.001
Mean weight loss 8.1 kg 10.2 kg 1.4 kg <.001
• Dose‐related AEs: dry mouth, constipation, dysgeusia, paresthesia, insomnia, dizziness, anxiety, irritability, disturbance in attention
• Endpoint assessments were not available for 31% of participants
• Patients: BMI 27‐45 and ≥2 obesity‐related comorbidities (hypertension, dyslipidemia, type 2 diabetes, prediabetes, abdominal obesity)
• Weight loss, 56 weeks
1. Gadde KM et al. Lancet. 2011;377:1341‐1352.
a Based on ITT‐LOCF analysis.

Phentermine/Topiramate ER: Cardiometabolic Effects1,2
• Significant dose‐related reductions in systolic and diastolic pressure in patients with hypertension
• Significant reductions in fasting glucose, HbA1c, and insulin in patients with prediabetes
• Significant improvements in lipid profiles in patients with hypertriglyceridemia
• Significant improvement in sleep apnea ‐ AHI2‐
AHI: apnea–hypopnea index .1. Gadde KM L et al. Lancet. 2011;377:1341‐1352. 2. Winslow DH et al. Sleep. 2012;35:1529‐1539.

Liraglutide1
ActionMean Weight Lossa
Study Duration
Common Side Effects Contraindications
GLP‐1 agonist 5.8 kg 1 year Nausea,
vomiting,
PancreatitisMedullary thyroidcancer history,
multiple endocrineneoplasia type 2
history
1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.
a Mean weight loss in excess of placebo as percentage of initial body weight or mean kg weight loss over placebo.

Liraglutide: Weight Loss Over 2 Years1
1. Astrup A et al. Int J Obes (Lond). 2012;36:843‐854.
All patients on liraglutide/placebo switched to liraglutide 2.4 mg at week 52, and then to
3.0 mg between weeks 70 and 96
Patients: BMI 30‐40 Weight loss: 104 weeks

Weight Loss With Liraglutide: SCALE Studies
1. Greenway FL et al. The Obesity Society Annual Meeting at ObesityWeek 2014 (ObesityWeek 2014). Abstract 3027‐OR. 2. Kushner FL et al. ObesityWeek 2014. Abstract 3030‐OR.
• Study patients: nondiabetic subjects with obesity and overweight with comorbidities
• Randomized 2:1 to liraglutide 3.0 mg (n = 2487) or placebo (n = 1244) as an adjunct to diet and exercise
SCALE: Obesity and Prediabetes1 SCALE: Diabetes2
• Study patients (n = 864): overweight or obese subjects with type 2 diabetes
• Randomized to liraglutide 3.0 mg or placebo as an adjunct to diet and exercise

Impact of Liraglutide on Cardiometabolic Effects and HRQL: SCALE Studies
FPG: fasting plasma glucose ; SF: short form.1. O’Neil P et al. 97th Annual Meeting of the Endocrine Society (ENDO 2015). Abstract SAT‐572. 2. Kushner FL et al. ObesityWeek 2014. Abstract 3030‐OR. 3. Blackman A et al. 50th Annual Meeting of the European Association for the Study of Diabetes (EASD 2014). Abstract OR‐184.
• Health‐related quality of life improved significantly with liraglutide 3 mg but not with 1.8 mg
SCALE: Obesity and Prediabetes: Subgroup Analysis1
SCALE: Diabetes2
• Reductions in FPG were greater with liraglutide vs placebo (−8.3 vs −2.8 mg/dL, respectively)
• Reduction in systolic blood pressure were greater with liraglutide vs placebo in both responders (−5.5 vs −3.4 mmHg, respec vely)
• Changes in overall physical health scores (SF‐36) were greater for liraglutidecompared with placebo (+4.3 vs +4.1, respectively)
SCALE: Sleep Apnea3
• Liraglutide 3 mg compared with placebo produced significant improvements in AHI

Naltrexone/Bupropion1
ActionMean Weight Lossa
Study Duration
Common Side Effects Contraindications
Reuptake inhibitor of
dopamine and norepinephrine (bupropion) and opioid antagonist (naltrexone)
4.8% 1 year
Nausea, constipation, headache,vomiting, dizziness
Uncontrolledhypertension,
seizuredisorders, anorexianervosa or bulimia,drug or alcohol
withdrawal, MAOI
1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.
a Mean weight loss in excess of placebo as percentage of initial body weight or mean kg weight loss over placebo.

Change in Body Weight With NB: COR‐II1
* P < .001 vs placebo at all time points.NB: naltrexone sustained‐release (SR) (32 mg/day) plus bupropion SR (360 mg/day). 1. Apovian CM et al. Obesity. 2013;21:935‐943.

Proportion of Participants Who Lost Weight With Naltrexone/Bupropion: COR‐II1
* P < .001 vs placebo at all time points.1. Apovian CM, et al. Obesity . 2013;21:935‐943.
39

Advantages and Disadvantages Associated With Weight‐Loss Medications1At present, prescribing is often based on cost and side effect profile
a Less weight loss = 2%‐3%; greater weight loss = >3%‐5%; robust weight loss = >5%. b Long‐term data is 1‐2 years.1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.
Drug Advantages Disadvantages
Phentermine Inexpensive, greater weight lossa
Side‐effect profile, no long‐term datab
Topiramate/phentermine Robust weight lossa, long‐term data Expensive, teratogen
Lorcaserin Side‐effect profile, long‐term datab Expensive
Orlistat, prescription Nonsystemic, long‐term datab
Less weight lossa, side‐effect profile
Orlistat, over the counter Inexpensive Less weight lossa, side‐effect profile
Natrexone/bupropion Greater weight lossa, food addiction, long‐term datab
Side‐effect profile,mid‐level price range
Liraglutide Side‐effect profile, long‐term datab Expensive, injectable
40

Advantages and Disadvantages Associated With Weight‐Loss Medications1At present, prescribing is often based on cost and side effect profile
Drug Advantages Disadvantages
Phentermine Inexpensive, greater weight lossa
Side‐effect profile, no long‐term datab
Topiramate/phentermine Robust weight lossa, long‐term data Expensive, teratogen
Lorcaserin Side‐effect profile, long‐term datab Expensive
Orlistat, prescription Nonsystemic, long‐term datab
Less weight lossa, side‐effect profile
Orlistat, over the counter Inexpensive Less weight lossa, side‐effect profile
Natrexone/bupropion Greater weight lossa, food addiction, long‐term datab
Side‐effect profile,mid‐level price range
Liraglutide Side‐effect profile, long‐term datab Expensive, injectable
a Less weight loss = 2%‐3%; greater weight loss = >3%‐5%; robust weight loss = >5%. b Long‐term data is 1‐2 years.1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.

74.585.1
65.8 6573
49.1
64.3
35.2 39 41
0.00
25.00
50.00
75.00
100.00
PHEN/TPM7.5/46
PHEN/TPM15/92
LOR 10 BID BUP/NAL32/360
LIR 3.0
Patie
nts, %
5% weight loss 10% weight loss
a Combined with lifestyle modification.
Odds of Reducing Body Weight by % Categories at 1 Year With Adjunctive Medication Among Those Who Complete Treatment
3

Slide 42
3 can you get rid of the references and make the picture biggerWeill Cornell Medical College, 2/2/2016

Questions you may have???
• Q: What medicine should I use for which patient?• A: Based on side effect profile and coverage
• Q: What about metformin?• A: It works
• Q: What do you use for drug‐induced weight gain?• A: Depends on the drug, how critical, what the MD prescribing it says

DPPOS – 10 year Follow‐Up Data
CONCLUSIONS: “Metformin used for diabetes prevention is safe and well tolerated. Weight loss is related to adherence to metformin and is durable for
at least 10 years of treatment”
Diabetes Prevention Program Research Group. Diabetes Care. 2012 Apr;35(4):731-7

Salpeter SR, et al. AJM 2008;121:149.
Metformin Reduces BMI

Metformin Reduces BMI in Non‐diabetics
Salpeter SR, et al. AJM 2008;121:149.

MAOI: monoamine oxidase inhibitor; SSRI: selective serotonin reuptake inhibitor.1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.
Category Drug Class Weight Gain Alternatives
Psychiatric agents
AntipsychoticClozapine, risperidone,olanzapine, quetiapine,
haloperidol, perphenazineZiprasidone, aripiprazole
Antidepressants/mood stabilizers: tricyclic antidepressants
Amytriptyline, doxepin,imipramine, nortriptyline,trimipramine, mirtazapine
Bupropiona, nefazodone,fluoxetine (short term), sertraline (<1 year)
Antidepressants/mood stabilizers: SSRIs
Fluoxetine?, sertraline?,paroxetine, fluvoxamine
Antidepressants/mood stabilizers: MAOIs Phenylzine, tranylcypromine
Lithium —
Neurologic agents Anticonvulsants Carbamazepine, gabapentin,
valproateLamotrigine?,
topiramatea, zonisamidea
Endocrinologicagents Diabetes drugs
Insulin (weight gain differs with type and regimen used),
sulfonylureas, thiazolidinediones, sitagliptin?, metiglinide
Metformina, acarbosea, miglitola, pramlintidea, edenatidea, liraglutidea
a Weight‐reducing.
Drugs Associated With Weight Gain and Suggested Alternatives1

Category Drug Class Weight Gain Alternatives
Gynecologic agents
Oral contraceptives
Progestational steroids, hormonal contraceptivescontaining progestational
steroids
Barrier methods, IUDs
Endometriosis treatment Depot leuprolide acetate Surgical methods
Cardiologic agents Antihypertensives α‐blocker?, β‐blocker?
ACE inhibitors?, calcium channel blockers?,
angiotensin‐2 receptor antagonists
Infectious disease agents Antiretroviral therapy Protease inhibitors —
GeneralSteroid hormones Corticosteroids, progestational
steroids NSAIDs
Antihistamines/ anticholinergics
Diphenhydramine?, doxepin?, cyproheptadine?
Decongestants, steroid inhalers
IUD: intrauterine device.1. Apovian CM et al. J Clin Endocrinol Metab. 2015;100:342‐362.
Drugs Associated With Weight Gain and Suggested Alternatives (Cont’d)1

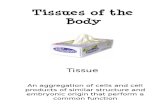
0% 5% 10% 15% 20% 25% 30% 35% Weight Loss
Treatment Gap in Mid‐BMI Range
Lap BandGastric Bypass
TreatmentGap
NOT EFFECTIVE
enoughfor many
people
Diet and Lifestyle& Drugs prior to 2012• Orlistat • Phentermine
TOO RISKY for many people
After Aronne L. FDA EMDAC 2010.
BPD
Sleeve gastrectomy
The gap is being filled
49

0% 5% 10% 15% 20% 25% 30% 35% Weight Loss
Treatment Gap in Mid‐BMI Range
Lap BandGastric Bypass
TreatmentGap
NOT EFFECTIVE
enoughfor many
people
Diet and Lifestyle& Drugs prior to 2012• Orlistat • Phentermine
TOO RISKY for many people
After Aronne L. FDA EMDAC 2010.
BPD
Sleeve gastrectomy
More Drug options:
LorcaserinLiraglutide
Combination Pharmacotherapy
Phen/topNalt/bup
Less Invasive Procedures
Vagal block therapyEndoscopic sleeve
More Drug options (2015):• Lorcaserin• Liraglutide
The gap is being filled
New drugs and devices can reduce weight and weight‐related comorbidities
50