Sample Tax Return (Level 1) COVER PAGE
4
Sample Tax Return (Level 1) COVER PAGE The next pages contain the sample tax return. PLEASE NOTE: With multiple preparers creating the same return with the same info will only generate errors. • You will need to enter a fake SSN than what is on the sample return (at least the last 4) • You will need to enter a fake phone number than what is on the sample return • Please choose a “BANK PRODUCT CHECK” when you get to the e-file section so you will learn the process of all screens • You will also need to enter a fake driver’s license, issue date & expiration date: Brand new preparers will not have access to actually transmit and seasoned preparers will have access: IMPORTANT: ALL PREPARERS CHOOSE “SAVE AND EXIT” ON THE FINAL SCREEN AND DO NOT TRANSMIT. PLEASE WHEN ANSWERING THE REFUND QUESTION IN THE QUIZ, USE THE REFUND BEFORE FEES.
Transcript of Sample Tax Return (Level 1) COVER PAGE

Sample Tax Return (Level 1) COVER PAGE
The next pages contain the sample tax return.
PLEASE NOTE:
With multiple preparers creating the same return with the same info will
only generate errors.
• You will need to enter a fake SSN than what is on the sample return
(at least the last 4)
• You will need to enter a fake phone number than what is on the
sample return
• Please choose a “BANK PRODUCT CHECK” when you get to the e-file
section so you will learn the process of all screens
• You will also need to enter a fake driver’s license, issue date &
expiration date:
Brand new preparers will not have access to actually transmit and
seasoned preparers will have access:
IMPORTANT: ALL PREPARERS CHOOSE “SAVE AND EXIT” ON THE
FINAL SCREEN AND DO NOT TRANSMIT.
PLEASE WHEN ANSWERING THE REFUND QUESTION IN THE QUIZ,
USE THE REFUND BEFORE FEES.

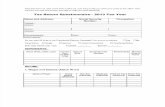
Client Interview Sheet
VALID ID – CANNOT BE EXPIRED (Make copy of ID for file)
Taxpayer Name__________________________________ SSN _________________________DOB_______________
Phone___________________ Cell Phone # __________________ Email ____________________________________
Spouse Name____________________________________ SSN ________________________ DOB_______________
Phone___________________ Cell Phone # __________________ Email ____________________________________
Address________________________________________________ City, State, Zip____________________________
Marketplace Insurance (1095A present) ____________ OR Private/Employer Insurance (1095B or C present) ____________
PLEASE COMPLETE BOXES BELOW
Dependent Name SSN Relationship DOB
Type of Insurance
Daycare Expense (Form 2441)
Did you receive 2020 Stimulus?
YES OR NO Amount?
Filing Status
Single ____
MFJ ____
MFS ____
HOH ____
Q-W ____
PLEASE MARK WHAT YOU CAN
PROVIDE IF REQUESTED BY IRS and
initial next to that form
Residency of Qualifying Child (ren)
▪ No qualifying child
▪ School records or statement _____
▪ Landlord or property management statement _____
▪ Health care provider statement_____
▪ Medical records_____
▪ Child care provider records_____
▪ Placement agency statement_____
▪ Social service records or statement_____
▪ Place of worship statement_____
▪ Indian tribal official statement_____
▪ Employer statement_____
▪ Other (specify)
PLEASE INITIAL NEXT TO WHAT
YOU CAN PROVIDE IRS SHOULD
THEY REQUEST PROOF
Disability of Qualifying Child (ren)
▪ No disabled child
▪ Doctor statement_____
▪ Other health care provider statement_____
▪ Social services agency or program statement_____
▪ Other (specify)
If a Schedule C is included with this return, which
documents or other information, if any, can you
provide “if requested by IRS” to confirm the
existence of the business and to figure the
amount of Schedule C income and expenses
reported on the return? Check all that apply. Keep
a copy of any documents you can provide.
Documents or Other Information
▪ No Schedule C
▪ Business license_____
▪ Forms 1099_____
▪ Records of gross receipts provided by taxpayer_____
▪ Taxpayer summary of income_____
▪ Records of expenses provided by taxpayer_____
▪ Taxpayer summary of expenses_____
▪ Bank statements_____
▪ Reconstruction of income and expenses_____
▪ Other (specify)
Signature of Taxpayer: _______________________________________
Signature of Spouse: _________________________________________
Date: ______/______/_______
Head of Household Filing Status
Can provide documents proving you are unmarried and provided more
than half of the cost of keeping up a home for the year for a qualified
person, PLEASE INITIAL THAT YOU CAN PROVIDE IF REQUESTED BY IRS
____________
Examples (Divorce decree, separation agreement or documents verifying your
spouse did not live with you during the last 6 months of the year)
Examples (Rent receipts, Utility bills, Grocery receipts, Upkeep & Repair bills,
and other household bills)
Have you had any EIC/CTC disallowed or
reduced in a prior year? YES OR NO
Sample Return
User
Typewritten text
Sample Return 400-88-9876 8/19/98
User
Typewritten text
X
User
Typewritten text
N/A
User
Typewritten text
549 Market Street Chatsworth,GA 30705
User
Typewritten text
No
User
Typewritten text
Mary Return 400-22-4321 Dtr. 4/2/19
User
Typewritten text
1700.00 & 1200.00
User
Oval
User
Typewritten text
SR
User
Typewritten text
SR
User
Typewritten text
SR
User
Line
User
Line
User
Line
User
Line
User
Oval
User
Typewritten text
Through Employer

ADDITIONAL NOTES
Taxpayer Signature__________________________________ Date __________________
Spouse Signature ___________________________________ Date___________________
Sample Return
User
Typewritten text
Where is your daughters' dad? Will he try to claim her on his tax return?
User
Typewritten text
She lives with me fulltime and he gets her every other weekend, so he won't be claiming her.

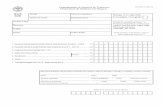
a Employee’s social security number
OMB No. 1545-0008
Safe, accurate, FAST! Use
Visit the IRS website at www.irs.gov/efile
b Employer identification number (EIN)
c Employer’s name, address, and ZIP code
d Control number
e Employee’s first name and initial Last name Suff.
f Employee’s address and ZIP code
1 Wages, tips, other compensation 2 Federal income tax withheld
3 Social security wages 4 Social security tax withheld
5 Medicare wages and tips 6 Medicare tax withheld
7 Social security tips 8 Allocated tips
9 10 Dependent care benefits
11 Nonqualified plans 12a See instructions for box 12Co d e
12bCo d e
12cCo d e
12dCo d e
13 Statutory employee
Retirement plan
Third-party sick pay
14 Other
15 State Employer’s state ID number 16 State wages, tips, etc. 17 State income tax 18 Local wages, tips, etc. 19 Local income tax 20 Locality name
Form W-2 Wage and Tax Statement 2020Copy B—To Be Filed With Employee’s FEDERAL Tax Return. This information is being furnished to the Internal Revenue Service.
Department of the Treasury—Internal Revenue Service
User
Typewritten text
400-88-9876
User
Typewritten text
27839.14
User
Typewritten text
1293.25
User
Typewritten text
30942.74
User
Typewritten text
30942.74
User
Typewritten text
1918.45
User
Typewritten text
448.67
User
Typewritten text
D
User
Typewritten text
3103.60
User
Typewritten text
DD
User
Typewritten text
14593.40
User
Typewritten text
X
User
Typewritten text
58-1111111
User
Typewritten text
Training W2
User
Typewritten text
411 Apple Street McIntosh, FL 32664
User
Typewritten text
Sample Return
User
Typewritten text
549 Market Street
User
Typewritten text
Chatsworth, GA 30705
User
Typewritten text
GA
User
Typewritten text
581111111
User
Typewritten text
27839.14
User
Typewritten text
683.26