Salivary glands cancer
25
Salivary Glands Cancer By Osama El-Zaafarany
-
Upload
osama-elzaafarany -
Category
Health & Medicine
-
view
782 -
download
3
description
some clinical notes about types and management of salivary gland malignancy..
Transcript of Salivary glands cancer
Salivary Glands Cancer
By
Osama El-Zaafarany
Epidemiology • Salivary gland neoplasms account for 6% of H&N
cancers (35% are malignant).
• Less than 0.3% of all malignancies.
• Approximately 80% of all salivary gland neoplasms originate in the parotid.
• The male-to-female ratio for malignant salivary gland tumors is 0.6.
• About 25% of parotid, 40% of submandibular, and
75% of sublingual gland tumors are malignant.

Etiology • Lifestyle: Cigarette smoking has a strong association
with Warthin’s tumor, a benign tumor of the parotid gland
• Occupational: Hairdressers, rubber manufacturing, exposure to metal in the plumbing industry and nickel compounds, and woodworking in the automobile industry
• Ethnic: Inuit men and women have the highest incidence rate of salivary gland cancer in the world, primarily from an excess of lymphoepithelial carcinomas
• Ionizing radiation: (including 131l): risk factor mostly for mucoepidermoid carcinomas and Warthin’s tumors. An increased risk has also been observed for adenocarcinomas among Hodgkin lymphoma survivors.
• Epstein-Barr virus: lymphoepithelial carcinomas
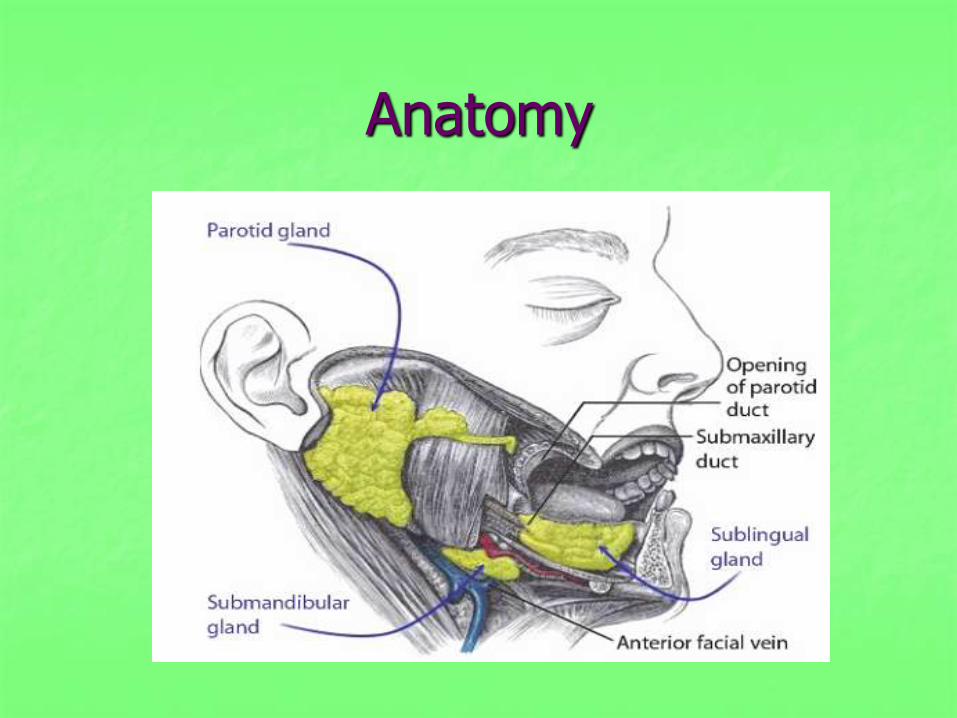
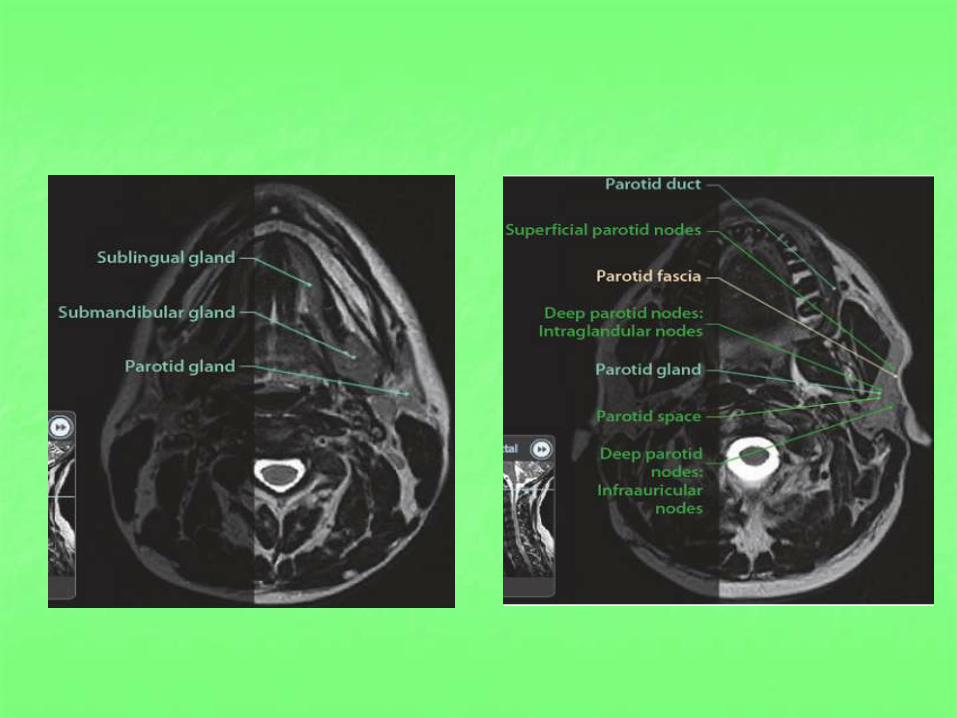
Anatomy

Pathology
WHO 2005 classification of malignant salivary epithelial tumors
Natural History • Mucoepidermoid carcinoma is the most common
malignant diagnosis (33%), followed by adenoid cystic carcinoma (24%), polymorphous low-grade adenocarcinoma, carcinoma ex pleomorphic adenoma.
• Mucoepidermoid carcinoma has higher incidence for LNs metas.
• Adenoid cystic carcinoma: 25-50 % distant metas.
PNI.
Needs adjuvant RTx.
Not respond to Taxol.
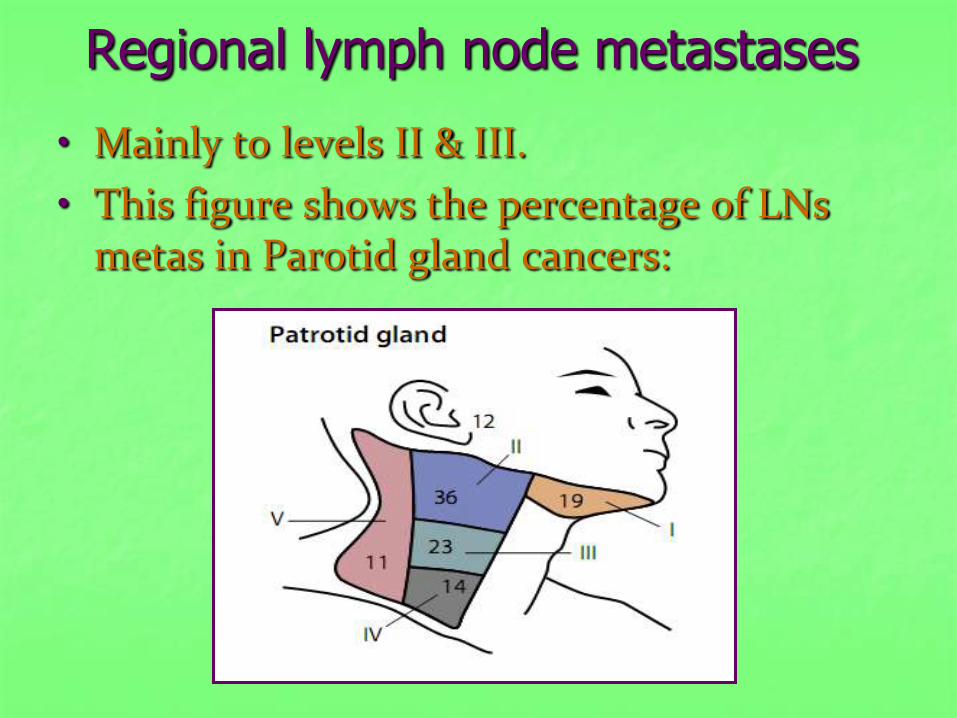
Regional lymph node metastases
• Mainly to levels II & III.
• This figure shows the percentage of LNs metas in Parotid gland cancers:

Risk of positive neck nodes according to summation of scores and site:

Workup
• H&P with bimanual palpation. Carefully examine cranial nerves and for trismus.
• CT and/or MRI of head and neck.
• PET scan is still investigational for salivary gland cancers.
• Fine-needle aspiration biopsy.
• Chest X-ray.
• Dental evaluation prior to the start of RT.
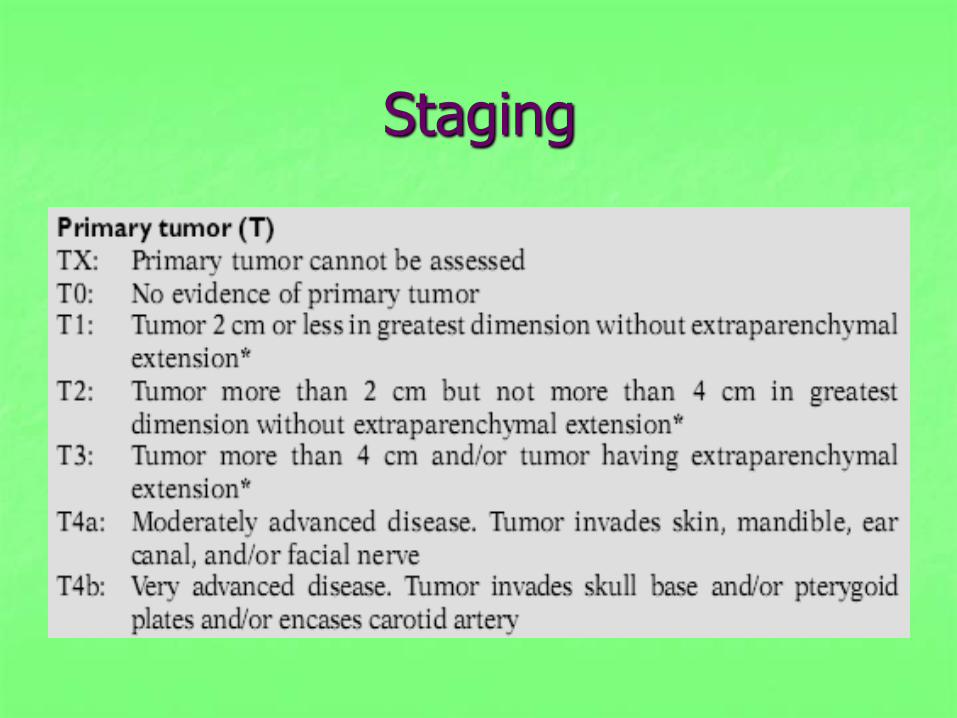
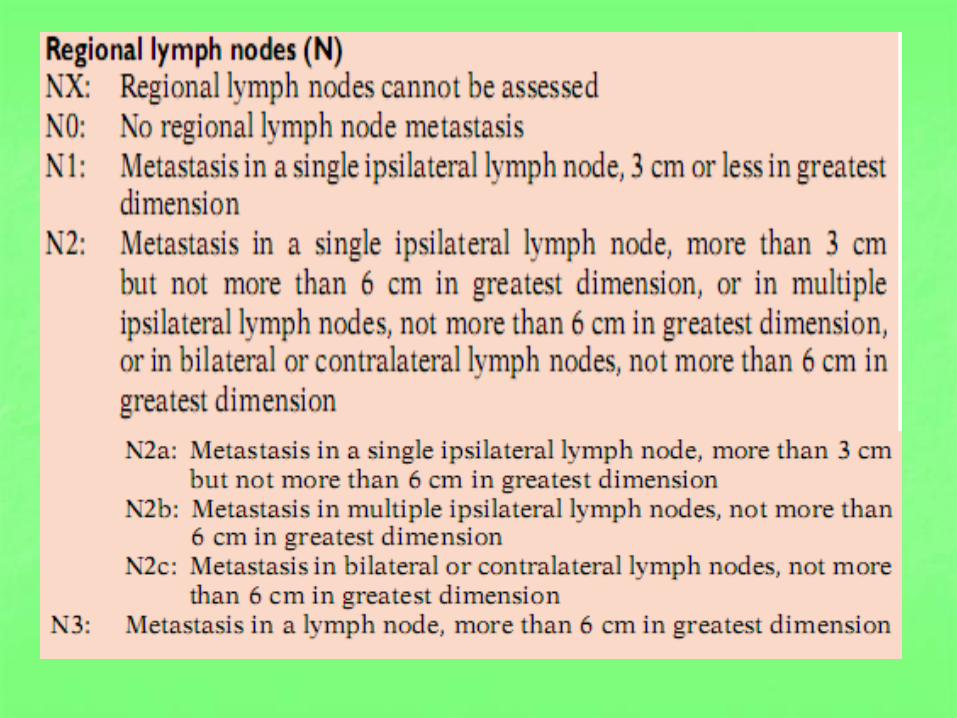
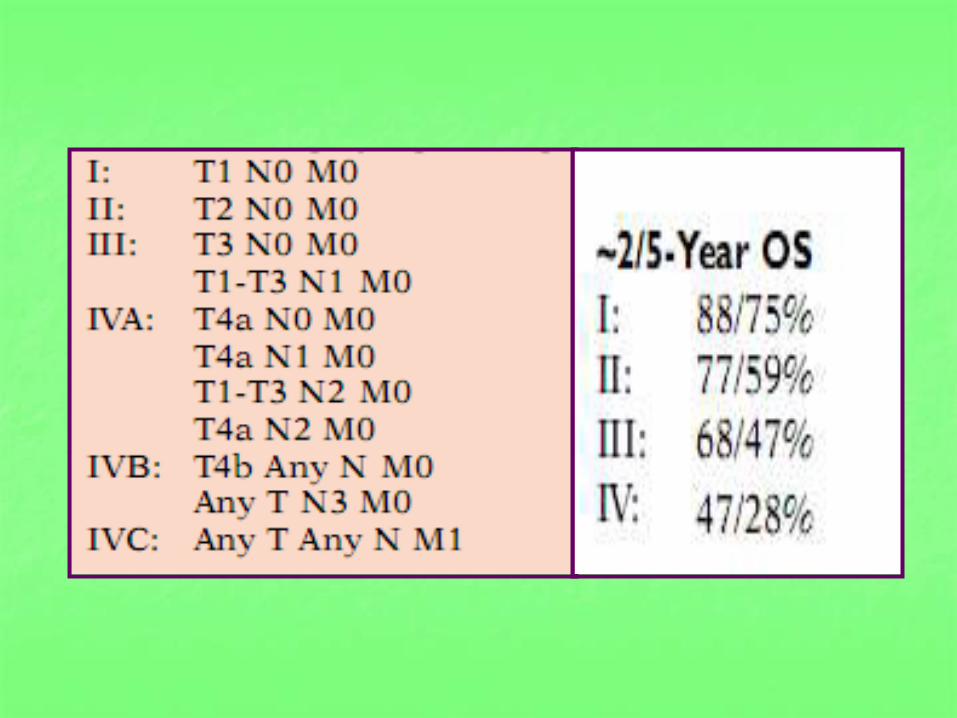
Staging

Treatment Recommendations
• Surgery forms the mainstay of defnitive treatment for salivary gland malignancies.
• Complications of surgery include facial nerve dysfunction and Frey’s syndrome; (gustatory flushing, sweating, auriculotemporal syndrome(.
• Superfcial parotidectomy can generally be performed for: low-grade parotid tumors.
T1–T2 superficial parotid lobe tumors without facial nerve invasion.
• Neck dissection recommended for: clinically +ve LNs.
high-grade tumors.

• Indications for post-op RT are currently controversial as there is no randomized data analyzing the role of post-op RTx.
• Consider post-op RTx for: PNI. close/+ve margins. high-grade tumors. T3-4 tumors. +ve LNs. +ve Vascular invas.
• RT alone (definitive) is indicated for medically inoperable and unresectable tumors.
• LC rates with RTx alone range from 20-80%.
• Neutron therapy may achieve better LC for unresectable or inoperable tumors.
• Brachytherapy or intraoperative RT can be considered for recurrent tumors.
• IMRT reduces mean doses to normal structures and allows dose-escalation to tumor.
RTx dose
• Post-op RT :
-ve margins: 60–63 Gy at 1.8–2 Gy/fx
+ve margins: 66 Gy at 1.8–2 Gy/fx
for gross residual disease: 70 at 1.8–2 Gy/fx
• RT alone (definitive): 70 at 1.8–2 Gy/fx
• Elective neck RT: 50–54 Gy at 1.8–2 Gy/fx. Ipsilat.
Levels I-II-III.
For tumors > 4cm include levels IV, V.
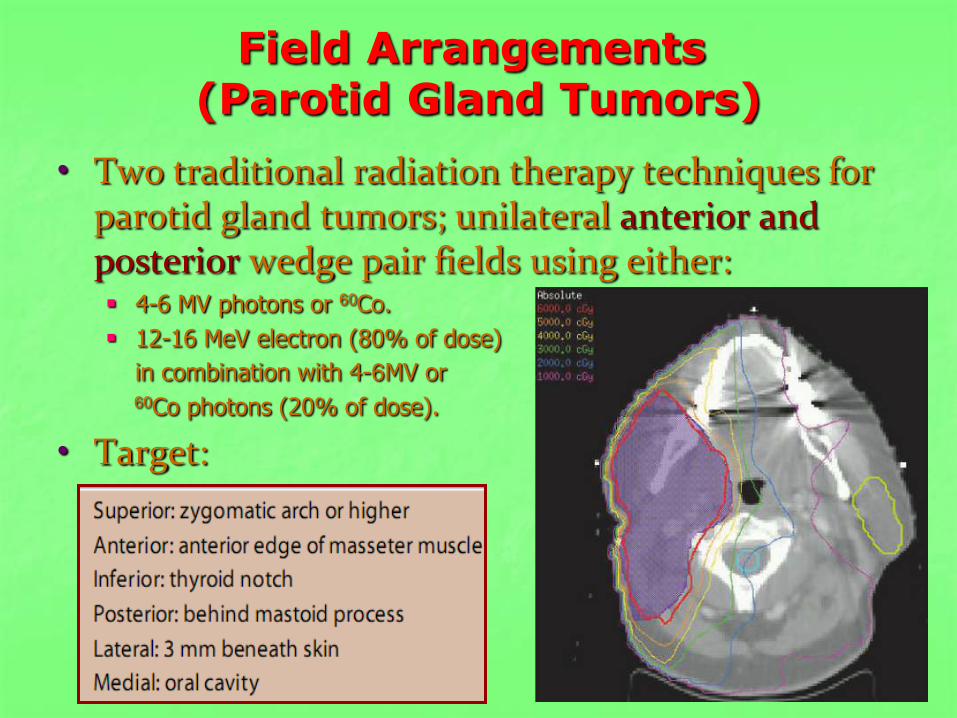
Field Arrangements (Parotid Gland Tumors)
• Two traditional radiation therapy techniques for parotid gland tumors; unilateral anterior and posterior wedge pair fields using either: 4-6 MV photons or 60Co.
12-16 MeV electron (80% of dose)
in combination with 4-6MV or 60 Co photons (20% of dose).
• Target:
Metastatic disease
• CAP regimen: cyclophosphamide (500 mg/m2), doxorubicin (Adriamycin; 50 mg/m2), and cisplatin (Platinol; 50 mg/m2) on first day of a 28-day regimen.
• The objective response rates to chemotherapy are modest, ranging from 15 to 50%, and lasting from 6 to 9 months.
• Paclitaxel 200 mg/m2 every 21 days (no response in adenoid cystic carcinoma)
• Targeted therapy may prove useful in the future as some histologies express EGFR, C-kit, and/or HER-2

Evidence
Role of adjuvant RTx: Dutch Head and Neck Cooperative Group (NWHHT), 2005:

Role of neutron RTx:
University of Washington, 2003:
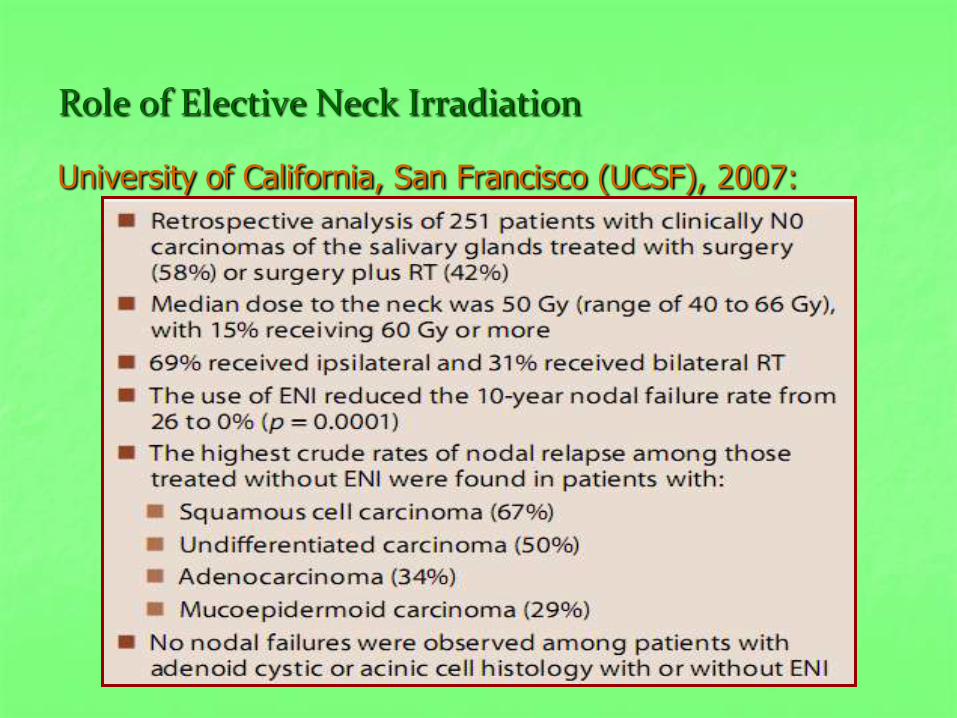
Role of Elective Neck Irradiation
University of California, San Francisco (UCSF), 2007:
Follow-Up
• H&P:
every 1–3 months for 1 year.
every 2–4 months for second year.
every 4–6 months for years 3–5.
annually thereafter.
• Regular head imaging with MRI and CXR as indicated.
• TSH every 6–12 months if neck irradiated.