Salivary glands
99
SALIVARY GLANDS & SALIVA AS A DIAGNOSTIC AID
-
Upload
sinnygoel -
Category
Health & Medicine
-
view
166 -
download
2
Transcript of Salivary glands

SALIVARY GLANDS&
SALIVA AS A DIAGNOSTIC AID
Introduction
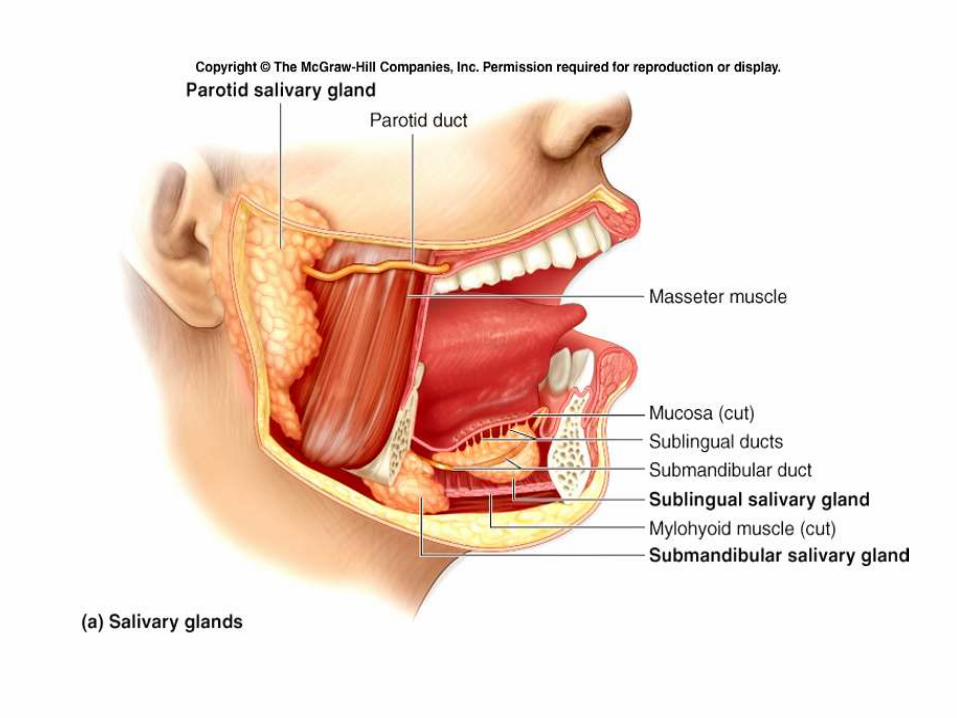
The paired parotid, submandibular, and sublingual glands are referred to as the major salivary glands;
Each is anatomically, histologically, and functionally unique.
The minor salivary glands are submucosal clusters of salivary tissue present in the oral cavity, paranasalsinuses, pharynx, and upper respiratory tract.
It has been estimated that more than 750 minor salivary gland clusters are present.
Embryogenesis• All salivary glands -common embryogenesis- local
proliferations of surface epithelium into theunderlying mesenchyme- similar anatomicstructure.
• Secretory/parenchymal tissues arise from theseproliferations - of ectodermal origin for the majorsalivary glands and of either ectodermal orendodermal origin (depending upon theanatomic location) for the minor salivary glands.
• Stroma -mesodermal origin and an additionalcomponent of neural crest.

• Parotid anlagen -first to develop (4-6th wk)
• Submandibular gland anlagen- 6th wk
• Sublingual gland anlagen- 7-8th wk
• Minor salivary glands –do not start to develop until late in the 12th wk of intrauterine life.

• Epithelial buds enlarge, elongate, and branch, the last process being induced by the mesenchymesurrounding the epithelium.
• Then canalization process results from a differential in the mitotic rate- completed prior to the development of lumina in the terminal buds -develop into the acini.
• epithelial cells lining the ducts, tubules, and acinithen differentiate.

• Surrounding the acini are- myoepithelial cells that reach their peak density by the 24th wk in the submandibular glands 25th wk in the parotid glands
• Interaction of the salivary gland parenchymaland stromal elements with the ANS is necessary for salivary development and function,
– as sympathetic nerve stimulation leads to acinardifferentiation,
– parasympathetic is important for overall glandular growth.

• In the parotid glands, – ducts are canalized by the 10th wk– terminal buds by 16th wk – secretions commence in 18th wk
• In the submandibular glands, – acini start to differentiate by -12th fetal week. – Serous secretory activity starts at 16th fetal week, – increases until the 28th wk, and then diminishes.
• These serous secretions contribute to the amniotic fluids, and contain amylase and possibly nerve and epidermal growth factors.
• The mucous acini develop postnatally. The mucosal minor salivary glands are not morphologically mature until the twenty-fifth fetal week.

• Although the parotid anlagen are the first to emerge, they become ‘‘encapsulated’’ only after the submandibular and sublingual glands have become encapsulated.
• Thus, at the completion of embryogenesis, the parotid glands have lymph nodes and lymphatic channels within the gland’s capsule, while the submandibular and sublingual glands do not.
• In addition, salivary epithelial cells can be included within the intraparotid and periparotid lymph nodes (MALT) during their process of encapsulation.
• These LNs supply all the major salivary glands with IgAproducing plasma cells that are important components of mucosa-based immunity.
• This special embryogenesis of the parotids and their LNs play a role in the development of Warthin’s tumors

Parotid Gland
• Largest
• Palpable superficial portion .
• Fascia –SLDCF,
– densest over lateral and inferior aspects,
– filmy or incomplete over medial surface
• Fascial extensions- subdivide the gland into lobules.

Space of the Parotid Gland
• SLDCF splits to enclose the parotid gland.
• the parotid gland cannot be shelled out, leaving behind a real compartment with strong fascialboundaries.
• However, conceptually, this space encloses the parotid gland, the parotid lymph nodes, and portions of the external carotid artery and the posterior facial or retromandibular vein

• Weight: 14-28 g (adult male)
• Measures: 5.8 cm craniocaudally and 3.4 cm ventrodorsally.
• Female-slightly smaller.
• ∼80% is superficial to the masseter, ramus, angle.
• rarely extends cranially to the zygoma.
• Superficial parotid lies below and anterior to theexternal auditory canal and mastoid tip,
• extending caudally to angle of mandible.
• deep aspect (∼20%) extends medially throughstylomandibular tunnel
• Present b/w posterior edge of ramus and anteriorborders of the sternocleidomastoid muscle and theposterior belly of the digastric muscle.
• Stylomandibular ligament separates it from thesubmandibular gland.
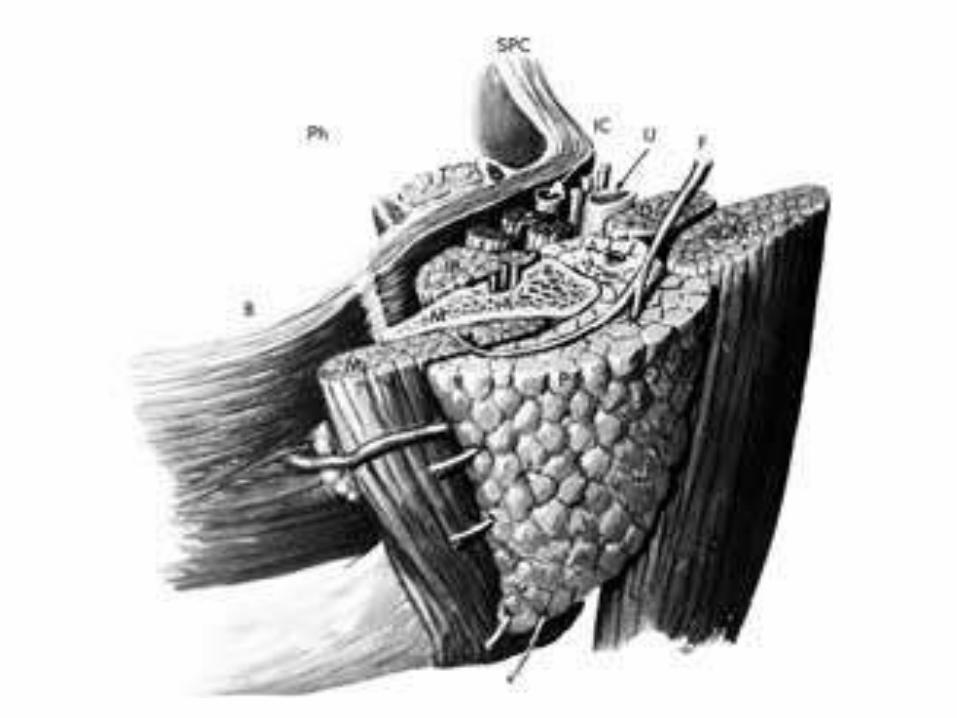
• Despite the commonly used terminology, there is actually no anatomic division into separate superficial and deep parotid lobes, a nomenclature based on the facial nerve as a reference plane within the gland.
• However, anatomically correct terminology in which the mandible has become the reference point is gaining popularity.

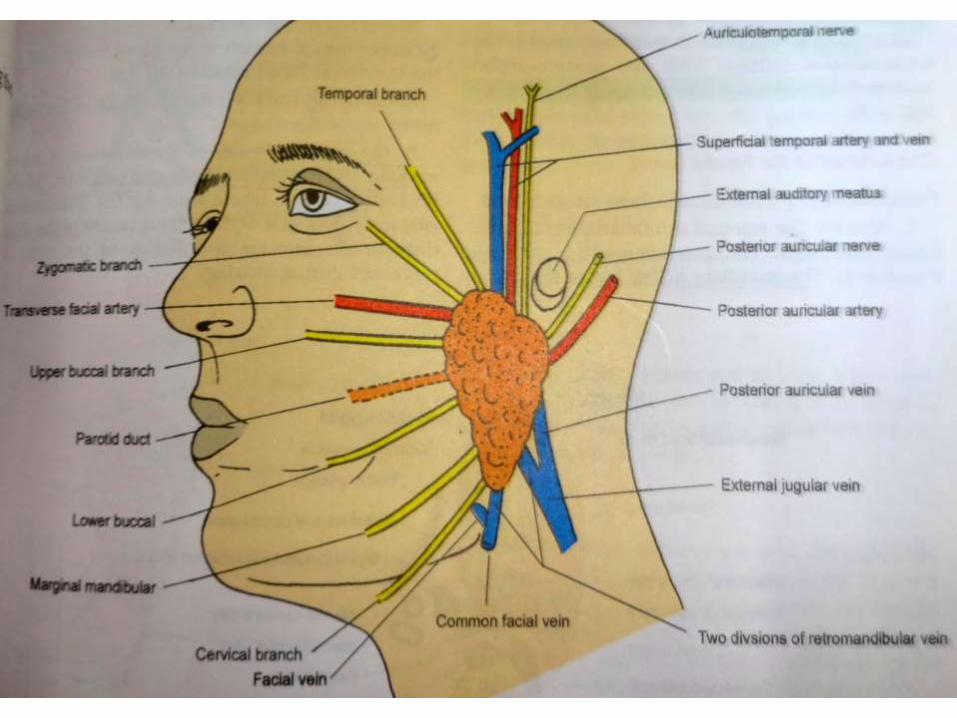
• Main trunk of the facial nerve exits the skull base via stylomastoid foramen, immediately producing three small branches: the posterior auricular, posterior digastric, and stylohyoidnerves.
• Courses laterally around the styloid process, superficial to the posterior belly of digastric.

• Distal to this, it pierces the posterior capsule ofthe parotid gland.
• Continues within the gland lateral to theposterior facial vein (retromandibular vein) andthe more medially situated external carotidartery.
• It then divides via variable anatomic patterns intothe temporal, zygomatic, buccal, mandibular, andcervical branches.

• parotid ductal organization has an arborizingor tree-like branching pattern.
• As one traces proximally from the main parotid duct (Stensen’s duct) toward the terminal acini, the ducts become progressively smaller, with more numerous branches


• Histologically, the main excretory ducts can be seen to lead into the – striated ducts (columnar) – the intercalated ducts (cuboidal epithelium surrounded by
myoepithelial cells), – and the terminal acini.
• In the adult, the parotid acini are purely serous; it is only in the neonatal period that some mucous cells are found.
• Sebaceous elements may be uncommonly found in the parotid gland and are thought to explain the sebaceous differentiation that may be seen in some salivary tumors.
• Parotid parenchyma has abundant adipose tissue, adipose to glandular tissue of 1;1.
• The parotid intercalated ducts are long and thin compared to the submandibular gland.
• The sublingual gland has the shortest and widest intercalated ducts.
• These variations in intercalated duct morphology may be related to the types of secretions in each of these glands.
• Stensen’s duct- 7 cm long;
• Course: anterior parotid-over the masseter and buccalfat pad- abruptly courses medially- pierce the buccinator muscle (90° angle)- obliquely and inferiorly for a short distance between the buccinator and oral mucosa- buccal mucosa, opposite the second upper molar.
• An accessory parotid duct may join Stensen’s duct as the latter passes over the masseter muscle.
• Accessory parotid tissue is present in about 20% of the population, usually about 6 mm anterior to the main parotid gland, adjacent to Stensen’s duct.

• Lies cranial to stensen’s duct, with only one excretory duct entering stensen’s duct.
• There may be multiple accessory glands, each with its own primary drainage into Stensen’s duct.
• The parotid gland contains 3 to 32 (average, 20) intraglandular lymph nodes interconnected by a plexus of lymphatics that drain the ipsilateral upper and midfacialskin.
• The palatine tonsil also drains into the parotid lymph nodes.
• parotid lymph nodes drain primarily into internal jugular chain (level IIA) and also into the upper spinal accessory chain (level IIB).
• The parotid is innervated from the sympathetic plexus on the carotid artery,
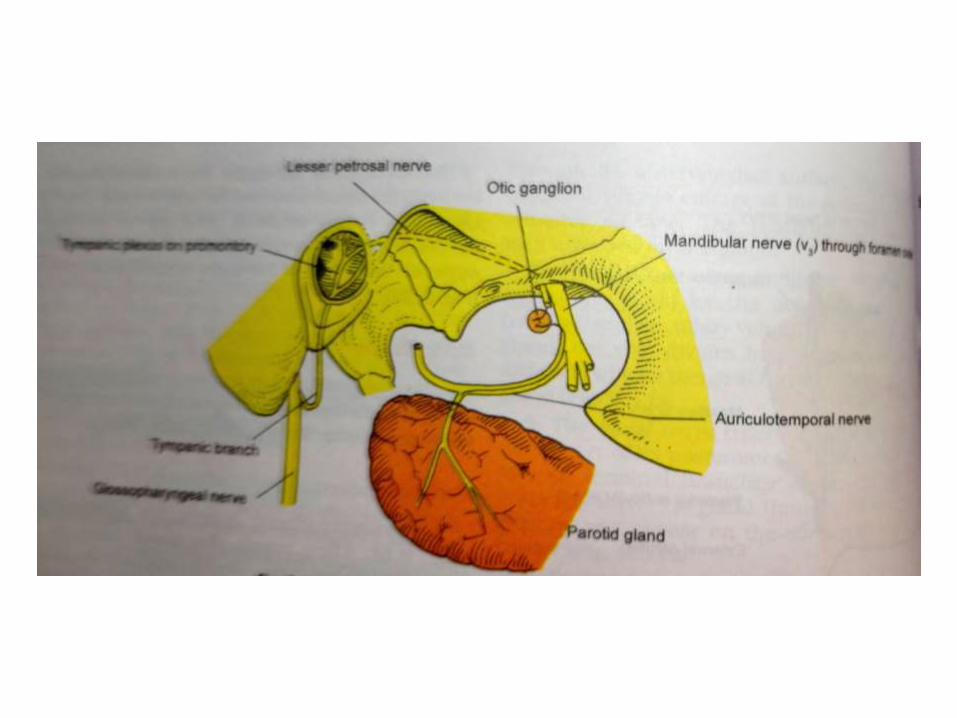
• parasympathetic innervation- glossopharyngealnerve via auriculotemporal n.
• parasympathetic fibers may also be contributed via the facial nerve through the otic ganglion.
• sympathetic nerves- vasoconstriction,
• Parasympathetic - secretion.
Proper surgical planning requires that the surgeon be informed as to whether a parotid mass is limited to the superficial gland or extends to the deep portion of the gland.
If a parotid mass extends into the parapharyngeal space, its size is important, as such a mass will require one of several modifications of the standard surgical parotidectomy for successful extirpation without violation of the tumor capsule.
The surgical modifications vary, depending on tumor size, from simple anterior dislocation of the temporomandibularjoint (TMJ), to an angle mandibulotomy, to a midline mandibular split with dislocation of the TMJ.
If the deep neck mass can be shown not to be of parotid gland origin, a lateral neck or submandibular approach is used.
Blood supply
• facial and external carotid arteries,
• richer vascular supply to the ductal than the acinar system.
• blood flow is parallel, but in opposite direction to the salivary flow.




Submandibular Gland
• Second largest salivary gland,
• Weight: 10- 15 g (1/2 parotid).
• occupies most of the submandibular triangle;
• folded around the free edge of the mylohyoid
– referred to as being divided into superficial and deep lobes.

Submandibular Gland• Superficial portion bounded
– anteriorly and inferiorly by the anterior belly of the digastric muscle,
– posteriorly by posterior belly of the digastric and stylohyoid muscles,
– laterally by lower border of the mandible and the medial pterygoid muscle .
• Posteriorly, it is separated from the parotid gland by– stylomandibular ligament.
• The floor or deep surface of the submandibulartriangle– formed by the mylohyoid and hyoglossus muscles.
Space of the Submandibular Gland
• This space can’t be considered a real space in the sense that the submaxillary gland can be easily shelled out of it, leaving the SLDCF behind as a capsule.
• Instead, the septa of the gland are continuous with the capsule.

Submandibular Space
• Overall, this space is the volume described within the mandibulararch, limited above by the mucosa in the floor of the mouth and caudally by the SLDCF as it extends from the hyoid bone to the mandible.
• Divided into an upper and a lower portion by the mylohyoid muscle
• Submandibular gland lies partially above and partially below its dorsal edge.
• In fact, the upper and lower portions of the submandibular space communicate freely with each other around dorsal margin of the mylohyoid muscle.
• Also free communication between the left and right sides of this space.
• Cranial portion of the submandibular space is often called the sublingual space. – filled with loose connective tissue that surrounds both sublingual glands
and their ducts, the lingual and hypoglossal nerves, the lingual arteries, and the smaller or deep portion of each submandibular gland along with its hilum and Wharton’s duct.
• On either side, the lower or caudal portion of the submandibularspace is usually referred to as the submaxillary space, and the larger superficial portion of the submandibular gland and its lymph nodes lie within its loose connective tissue.
• The facial artery and vein as well as the digastric muscle are also in each submandibular space.
• The submental triangle and the submandibular triangles of the neck are the superficial landmarks that correspond to the region of this space
• Superficial portion- SLDCF, platysma, anterior facialv., marginal mandibular n. runs adjacent to thegland.
• The anterior facial vein- useful imaging landmark to help determine if a mass arises within or adjacent to the submandibular gland.
– A lesion arising within the gland will never be separated from the gland by this vein.
– If the vein separates the mass and the gland, the lesion may have originated from submandibular lymph nodes (level IB) or the adjacent soft tissues.



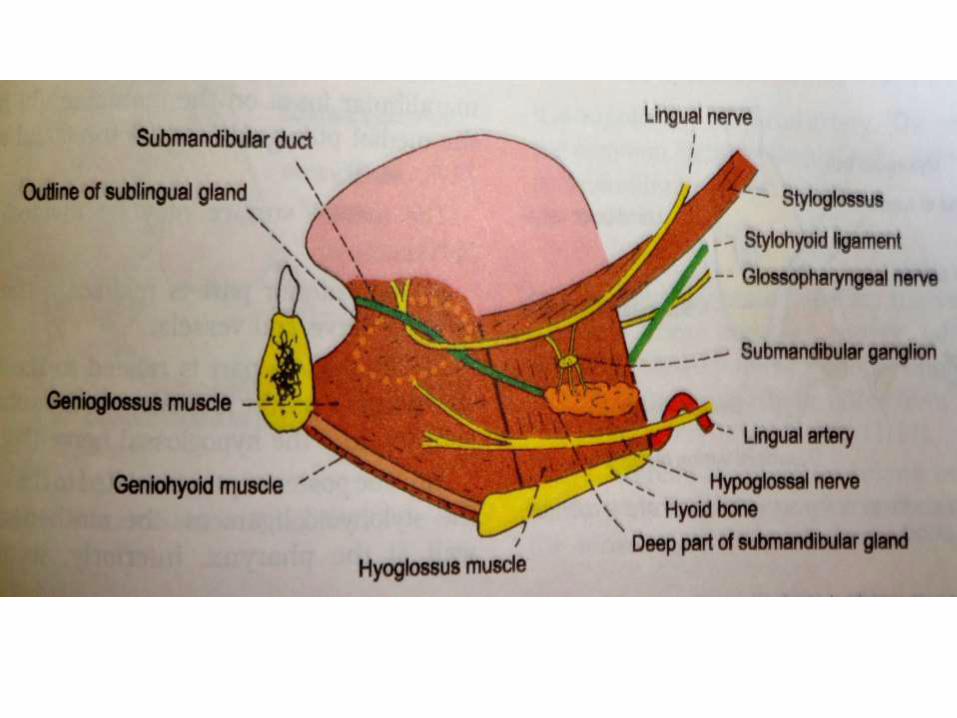
• lingual nerve and submandibular ganglion are superficial (lateral) to the gland,
• hypoglossal nerve with its accompanying vein lies deep to it.
• Wharton’s duct- 5 cm long, with thinner walls than Stensen’s duct.
Submandibular Gland

• Along this course, the duct is angled atapproximately 45° to both the sagittal and axialplanes.
• It terminates within the sublingual papilla in theanterior floor of the mouth.
• As the duct courses upward, the lingual nervewinds around it, first laterally, then inferiorly, andfinally medially
Submandibular Gland

Submandibular gland
• Serous acini (90%), with a mucinous acinar component (10%).
• Adipose tissue is not a significant component of the glandular parenchyma, as it is in the parotid.
• Arterial supply- branches of external maxillary and lingual arteries.
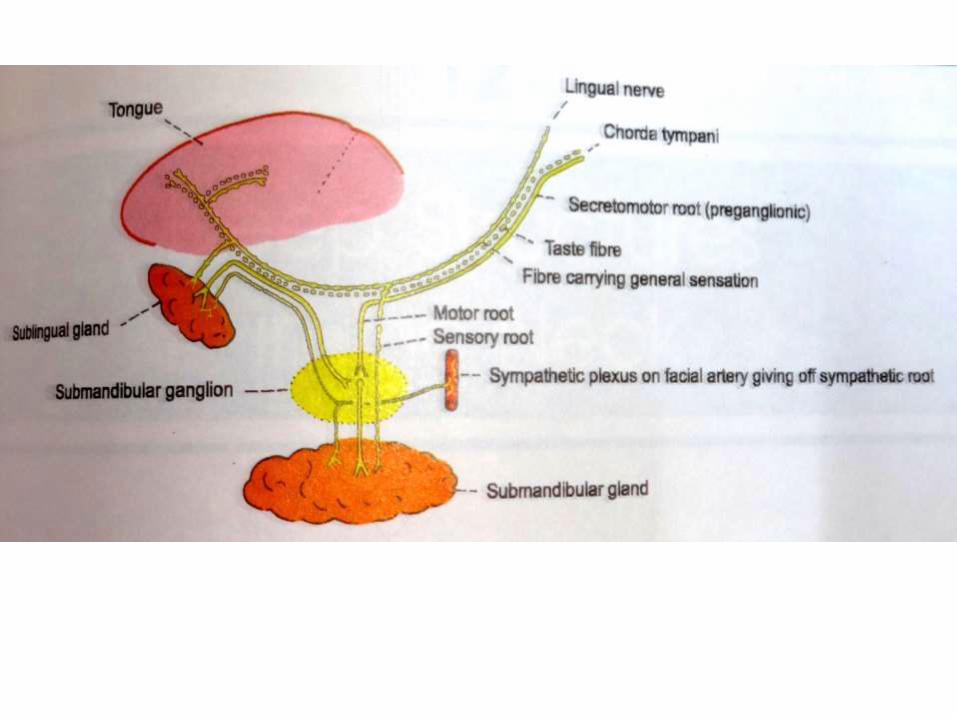
• Sympathetic innervation - carotid plexus, • parasympathetic innervation- facial nerve and possibly the
glossopharyngeal nerves via the chorda tympani nerve and the submandibular ganglion.
• Glandular lymphatic drainage - submandibular nodes (level I).

Sublingual Gland
• The sublingual gland is the smallest of the major salivary glands,
• about half the size of the submandibular gland,
• weighing only about 2 g, measuring about 2.5 cm
• shaped like a flattened almond

Sublingual Gland
• Lies submucosally against the sublingual depression of the lingual mandibular surface, – adjacent to the symphysis, – on the mylohyoid muscle.
• The lingual nerve and Wharton’s duct separate the medial sublingual gland contour from the genioglossus muscle.
• no well-defined capsule
• composed entirely of mucinous acini.

Sublingual Gland
• There are about 20 individual small ducts (the ducts of Rivinus), most of which open independently into the floor of the mouth along the sublingual papilla and fold.
• Occasionally some of these ducts fuse to form Bartholin’s duct, which in turn opens into Wharton’s duct.
• The sublingual innervation is identical to that of the submandibular gland.
• The gland’s lymph drains into the submental and submandibular lymph nodes (level I).

Minor Salivary Glands
• within the submucosa of the oral cavity, palate, paranasal sinuses, pharynx, larynx, trachea, and bronchi.
• concentrated in the buccal, labial, palatal, and lingual regions.
• The gingivae, anterior hard palate, and true vocal cords have relatively sparse concentrations of MSG.
Minor Salivary Glands
• MSG acini are either entirely mucinous (e.g., hard palate) or mixedseromucous glands (e.g. sinonasal, oral).
• The acinar clusters lead to intercalated ducts, striated ducts, and excretoryducts that terminate as mucosal pores.
• The autonomic secretory function of the upper aerodigestive tract MSG iscontrolled by the following ganglia:
– Sphenopalatine (pterygopalatine) ganglia, located near the sphenopalatineforamina of the medial pterygopalatine fossae, innervate the paranasal sinuses,nasal cavity, portions of the palate, and the uppermost pharynx;
– Otic ganglia, located along the medial aspect of the mandibular nerves below theskull base, innervate the buccal mucosa;
– Submandibular ganglia, innervate the floor of the mouth and the anteriortongue; and finally, the pharyngeal plexus innervates the pharynx

MICROSTRUCTURE
• The structure of the salivary glands is similar to other exocrine glands, comprising a series of secretory units (acinar cells) clustered around a central lumen.
• These acini comprise the terminal or secretory end-piece of the gland, situated farthest from the oral cavity.
• They are supported by the myoepithelial cells and a basement membrane.
• From each acinus the secretions pass to a series of interconnected ducts before passing out through the major salivary duct into the oral cavity.
MICROSTRUCTURE
• Each acinus comprises a series of polygonal cells on a basement membrane around a central ductal lumen.
• The acinar cells are classified histologicallyinto two types – serous cells and mucous cells according to their appearance after staining with eosin and heamatoxylin (histochemicalterm rather than a functional).
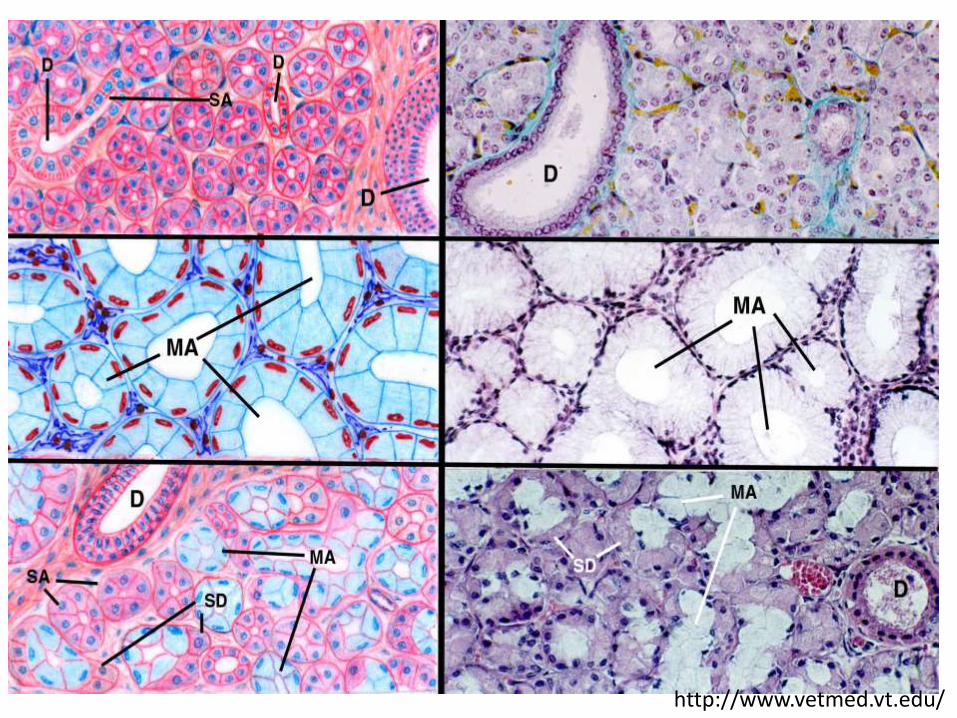
http://www.vetmed.vt.edu/
Serous Cells
• Stain blue; make up most of the acini of the parotid glandand of von ebner.
• Large, polygonal.
• Nucleus lying towards the basement membrane.
• Contain extensive endoplasmic reticulum andmitochondria,
• In the luminal portion of the cells are granules and vacuoleswhich fill up during resting periods but discharge byexocytosis on stimulation, some of these contain amylase.
• secretion more serous than other glands

Mucous cells • Predominantly pink – staining cells.
• Staining properties resemble those of other cells elsewhere which produce mucoid substances,
• Since the secretions of these cells are viscous and rich in protein – carbohydrate complex, they have been referred to as mucous cells.
• The acinar cells of the submandibular and sublingual glands are said to comprise mucous cells. The general form and appearance of mucous cells is not dissimilar to that of serous cells.
• Mucous cells show more areas of smooth parallel cisternaeand have larger secretory vacuoles.
DUCTS
Intercalated duct cells • The secretions pass from the acinus to a short
intercalated duct: the duct cells tend to be cuboidal, they have large central nucleus and many mitochondria and little endoplasmic reticulum.
• The duct lining cells are closely interdigitated.
• Contain zymogen granules, which may contribute to stable changes in salivary composition.


DUCTSStriated duct cells • The intercalated duct then pass abruptly into another short but wide,
striated duct, the striated duct are lined by cells which are much more columnar than the cells of the intercalated duct.
• The cells have marked cellular membrane interdigitations projecting towards the lumen.
• Striated ducts actively resorb sodium ions from the primary acinarsecretion, with the associated capillaries then transporting the ions away from the glands into systemic circulation.
• These striated ducts then pass abruptly into two epithelial cell layered excretory ducts and finally to the stratified squamous epithelial cell lined terminal duct.
• Although these latter excretory ducts resorb electrolytes from the primary secretion, they are probably less efficient than the stratified duct lining cells.

Myoepithelial cells
• Constrict the acini and ducts to facilitate salivary flow.
• Nucleus lies in a broader part of the cell and is surrounded by mitochondria and strands of endoplasmic reticulum.
• Remainder of the cells contain- myofibrils.
SALIVA
• Three major glands and about 400 minor glands located within theoral cavity produce saliva.
• A healthy adult : 500–1,500 mL saliva/day at a rate of approximately0.5 mL/min.
• Multitude of functions: maintaining homeostasis; promotingwound healing; lubricating the oral cavity; facilitating mineralizationof dental surfaces; digesting carbohydrates by salivary α-amylase;digesting lipids via salivary lipase; and facilitating chewing,speaking, swallowing, and taste perception.
• Help maintain oral hygiene by clearing and inhibiting growth ofmicroorganisms.

MECHANISM OF SALIVARY SECRETION
• Stimulation of secretomotor nerves- release of neurotransmitters- act on membrane receptor sites on the acinar cells to stimulate secretion.
Formation of the acinar fluid• The acinar fluid consists of water, ions, small
molecules, synthesized by the cells.
• This fluid arises from the interstitial fluid, which in turn arises from the blood in the capillaries.
MECHANISM OF SALIVARY SECRETION
• The acinar cells behave as if freely permeable to lipid-soluble substances and water, but much less permeable to other molecules. – Entry of glucose and amino–acids probably occurs by
active transport, their concentration in acinar fluid is low.
• The ions of the acinar fluid are broadly similar to those of interstitial fluid.
• Sodium and chloride concentration are similar to those of plasma
MECHANISM OF SALIVARY SECRETION
• Active transport of these two ions at the luminalmembrane is the major factor producing an osmoticforce to speed water movement through the acinarcells.
• Potassium is lost from the acinar cells to the acinarfluid on stimulation and high acinar potassium levelmay arise from a cell membrane permeability whenexposed to acetylecoline.
• Synthesis of salivary proteins occurs at theribosomes and the proteins pass into the cisternaeof the endoplasmic reticulum ; to be secreted fromthe cell surface by exocytosis.

MODIFICATIONS OF THE ACINAR FLUID
Modification in the intercalated duct :
• Involved in the initial secretion; though histologically they do not resemble secretorycells.
• It is possible that the loss of potassium from the gland which occurs on stimulation may take place here as well as in the acinar cells.
MODIFICATIONS OF THE ACINAR FLUID
Modification in the striated duct :
• transformed from an isotonic, or slightly, hypertonic fluid, with ionic concentration similar to plasma, to a hypotonic fluid, with low sodium and chloride concentration.
MODIFICATIONS OF THE ACINAR FLUID
• Sodium is actively transported across the cell -concentration gradiant increases- luminal fluid, resulting in diffusion of sodium into the cells from the lumen.
• The active transport of sodium is linked with active transport of potassium in the opposite direction and also with passive diffusion of chloride to maintain the electrochemical balance.
MODIFICATIONS OF THE ACINAR FLUID
• Bicarbonate is actively secreted to the lumen in this part of the gland. The cells behave as if largely impermeable to water, so that although salts are conserved in the area, water is not resorbed and a hypotonic secretion results.
• Stimulation either of sympathetic or parasympathetic nerves causes activation of the duct cells.
• Resting transmembrane potential of cells of the striated ducts is around – 80 mv On stimulation of the glands, the transmembrane potential on the luminal side of the cells becomes much less negative (around –20 mv).
Modification in the distal excretory ducts
• In the distal part of the excretory ducts partial re-equilibration of saliva with plasma occurs and concentration of ions return from extreme values to more plasma like concentrations.

CONTROL OF SECRETION• Controlled by a salivary center composed of nuclei in the medulla but
there are specific triggers for this secretion.
Afferent pathways (stimuli)
Local factors• The act of chewing, the sensation of taste, the irritation of the
mucous membrane - reflexly produce salivation.
• The fibers carrying sensations of taste and touch are carried in the same nerves carrying the secretomotor fibers – i.e., the chordatympani fibers in the lingual nerve (which originate in the facial nerve) from the anterior 2/3rd of the tounge and glossophargneal nerve from the poterior 1/3 of tounge.
• The sensation of smell and sight from the nose and eyes are carried by the 1st and 2nd cranial nerves respectively.
Psychic stimuli
• The sight of food, talking about or the noise of food preparation are sufficient to activate the conditioned reflexes (influenced by higher centers, ex: hypothalamus.)
Stimulation from other organs
• Esophageal irritation causes reflex salivation, although gastric irritation leads to increased salivation as a component of the nausea / vomiting reflex.

Central control
• The afferent stimuli reach the brain and spinal cord and are finally integrated in the cell bodies of the preganglionic secretomotorneurons- Where efferent secretomotor impulses are generated.
• Cell bodies of parasympathetic neurons- in the nuclei of facial and glossophsyngeal nerves.
• The area which gives salivary response on stimulation is termed ‘nucleus salivatorius’. The nucleus salivatorius has been divided into two components.
– Superior salivary nucleus : stimulations of which causes secretion of submandibular and sublingual glands.
– Inferior salivary nucleus : stimulation causes secretion of parotid glands.
• cell bodies of the sympathetic nervous system - in the lateral columns of the first five thoracic nerves.
• The secretomotor cell-bodies, in addition receive inputs, both excitatory and inhibitory, from other parts of the brain.
• Hypothalamic activity is also associated with salivary responses.
THE EFFERENT PATHWAY • The flow of saliva is controlled entirely by
nervous stimuli.
• Control exerted mainly by parasympathetic, butalso by sympathetic stimuli.
• Parasympathetic fibers to the submandibular andsublingual glands arise from the superior salivarynucleus in the medulla as nervous intermedins -geniculate ganglion - descend through the facialN.- chorda tympani- lingual N. - submandibualarganglion- secretory and dialatory fibers to glands.
THE EFFERENT PATHWAY • The parasympathetic fibers to the parotid gland arise from
the inferior salivatory nucleus (dorsal nucleus of the IX nerve) in the medulla- descend through glossophargneal N. - tympanic branch -tympanic plexus -lesser superior petrosal nerve -otic ganglion- post ganglionic fibers- parotid gland through the auriculotemporal nerve to supply it with secretory and dilator fibers.
• The sympathetic fibers to all these glands synapse in the superior cervical ganglion- postganglionic fibers- pass along the walls of the arteries and supply all the salivary glands.
• The sympathetic fibers end in the serous gland or the serous part of the mixed gland and supply vasoconstrictor fibers to the vessels of the glands and myoepitheilial cells of the ducts.
Diagnostic Uses of Saliva• Human saliva harbors proteins, lipids, RNA,
DNA, and some 700 microbial species.
• A biofluid for early disease detection andprognosis, risk stratification, and monitoringtreatment response.
• Used for diagnosis and prognosis of oral,head, and neck cancers, periodontal diseases,diabetes, and autoimmune disorders.
Other diagnostic uses
• Biomarkers identified in saliva for detecting early-stage pancreatic cancer.– UCLA Newsroom. Researchers find biomarkers in saliva for detection of early-stage pancreatic cancer. Available at the UCLA
Newsroon online. (Accessed August 2012).
• Soluble c-erbB-2Her2/neu levels in saliva may be useful in detecting and monitoring recurrence of breast cancer.– Streckfus CF, Mayorga-Wark O, Arreola D, et al. Breast cancer related proteins are present in saliva and are modulated
secondary to ductal carcinoma in situ of the breast. Cancer Invest 2008;26:159–67.
• Salivaomics is an open-access database that containssalivaomics-based studies and includes information onthe biology, diagnostic potential, pharmacogenomics,and pharmacoproteomics of saliva.

Saliva Proteome
• Human saliva is a plasma ultra filtrate and containsproteins either synthesized in situ in the salivary glandsor derived from blood.
• It contains biomarkers derived from serum, gingivalcrevicular fluid, and mucosal transudate.
• To date, researchers have identified 2,340 proteins inthe salivary proteome, of which 20–30% are also foundin blood,– an encouraging indicator for the clinical utility of saliva as a
diagnostic fluid.• Bandhakavi S, Stone MD, Onsongo G, et al. A dynamic range compression and three-dimensional peptide
fractionation analysis platform expands proteome coverage and the diagnostic potential of whole saliva. JProteome Res 2009;8:5590–600.

Saliva Proteome
• In contrast to the plasma proteome, in which 99% of the totalprotein content is contributed by 22 highly abundant proteins,the 20 most abundant proteins in human whole saliva (WS)constitute only 40% of the protein content.
• This composition suggests that detecting biomolecules of clinicalsensitivity and specificity in saliva should be feasible and easierthan in blood.
• Unlike the plasma proteome, however, the WS proteome is highlysusceptible to a variety of physiological and biochemicalprocesses, such as salivary protein modifications occurring in themouth that are catalyzed by host and bacterial derived enzymes.Such modifications also could present unique challenges forclinical saliva proteomics.
• The dynamic range of proteins in saliva isanother challenge.
• α-amylase- present at mg/mL conc.
• IL-6 and IL-8 only pg/mL.
• This disparity highlights the importance ofdeveloping tools and strategies for detectinglow abundance proteins having clinicalrelevance in saliva.
Saliva Proteome

• How molecules are transported from blood intosaliva- important for successful use of saliva as adiagnostic fluid.
• Lipophilic molecules such as steroid hormonespassively diffuse into saliva, while water andelectrolytes pass through the pores of acinar cells.
• Various peptides in blood move through proteinchannels, and large proteins are transported viapinocytosis .
Saliva Proteome
Yang Foo JY, Wan Y, Kostner K, et al. NT-ProBNP levels in saliva and its clinical relevance to heart failure. [Epub] PLoS One October 31, 2012
Commercially Available Saliva Tests
• Two U.S. companies were early pioneers of oral diagnostics: Epitope, Inc. and Saliva Diagnostic Systems, Inc.
– They both commercialized saliva collection devices in the early 1990s,
– In 1996 FDA approved Epitope’s Orasure HIV test, the first test that used oral fluid to test for an infectious disease.
• Recently FDA (2012) has approved first over-the-counter salivary HIV test that allows people to test themselves in the privacy of their homes for the HIV virus. – The OraQuick HIV test, which takes only 15 minutes from start to
finish, detects the presence of HIV antibodies in saliva via mouth swab.
Commercially Available Saliva Tests
• Several companies have commercial tests to detect drugs-of-abuse ina spit sample, including Cozart Biosciences, Securetec, and Mavand.
• Some of these companies send their kits via regular mail tocustomers, allowing individuals to collect their own saliva either in acup or with a swab and send the sample to lab for analysis.
• Other tests target DNA in saliva. Canada-based DNA Genotek wasthe first company to commercialize a broad range of saliva collectiontools for genotyping based on PCR, microarrays, and sequencing.
– My PerioPath is a DNA test that determines the risk of periodontalinfections by detecting bacterial pathogens in saliva.
– OraRisk HPV is a salivary test that determines an individual’s risk ofdeveloping HPV-related oral cancers.• It identifies various HPV genotypes, including HPV 8, 11, 16, and 18.

Emerging Clinical Applications
• Other applications of salivary diagnostics are emerging, includingfor the detection of
• cardiovascular disease– Yang Foo JY, Wan Y, Kostner K, et al. NT-ProBNP levels in saliva and its clinical relevance to heart failure. [Epub] PLoS One
October 31, 2012.
• and head and neck cancer– Ovchinnikov DA, Cooper MA, Pandit P, et al. Tumour-suppressor gene promoter hypermethylation in saliva of head and neck
cancer patients. Transl Oncol 2012;5:321–6.
• Salivary C-reactive protein (CRP) levels can be used as a biomarkerto differentiate patients with ischemic heart disease from healthycontrols .
• Salivary endothelin conc and natriuretic peptide- to assess heartfailure.
Roadblocks to Advancement
• Analytes in saliva are usually present at only 0.1–0.001 of the levels found in blood;
– Therefore, very sensitive detection technology is required.
• Lack of information about reference ranges of molecules in saliva within a healthy control population.
• To be clinically useful, there must be reliablecorrelations between levels of the targetsubstance in saliva and in blood or plasma.
– Ex: salivary diagnostics are not well suited tomeasure glucose levels because blood and salivarylevels of glucose are poorly correlated.
Roadblocks to Advancement
• Contamination of saliva with blood – falsepositive result.– Bleeding after brushing or flossing occurs frequently/
high false-positive rates.
• Research also is needed on how levels ofmolecules vary diurnally.– salivary growth hormone levels are higher in the
morning than during the day, which could also be thecase for other biomarkers.
Roadblocks to Advancement
• Lack of standardized saliva collection methods
• OraSure saliva collection device detectshepatitis C virus with greater sensitivity thanthe Salivette device .
Roadblocks to Advancement
•Judd A, Parry J, Hickman M, et al. Evaluation of a modified commercial assay in detecting antibody to hepatitis C virus in oral fluids and dried blood spots. J Med Virol 2003;71:49–55.
What Does the Future Hold?
• As our knowledge of the biomolecules present in salivagrows, the potential applications for oral and systemicdisease diagnosis will expand.
• While the scientific link between salivary biomarkersand oral diseases is clear,– more studies are needed to delineate the mechanisms by
which saliva reflects other systemic diseases.
• Furthermore, before saliva can become widelyrecognized as a reliable diagnostic fluid,– need to understand a number of important variables.
What Does the Future Hold?
• First, we need to define the normal biological variability ofbiomolecules in saliva,– diurnal rhythms,– inter- and intra-subject variation,– Age– gender effects.
• Influence of diet, medication, smoking, alcohol, and physical activitystatus may also influence levels of biomolecules in saliva.
• Variations caused by saliva sampling, handling, and storage conditionsand analytical techniques.
• Since the salivary proteome is sensitive to both extrinsic and intrinsicfactors,– analyte reference ranges needs to be carefully documented.
• Salivary diagnostics has enormous potential forthe future,– but we need to lay a solid scientific foundation in
the present in order to realize that potential.
• Non-invasive tests for detecting breast cancer,viral, and bacterial diseases, cardiovascular andmetabolic diseases, and general nutritionaldeficiencies could make a tremendous impacton global health.
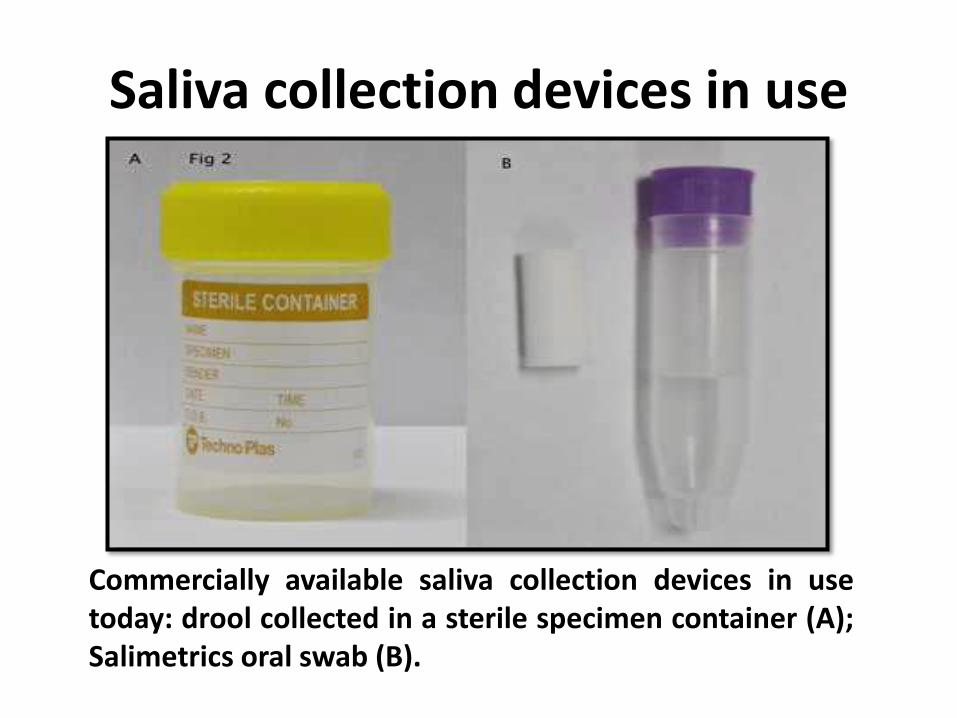
Commercially available saliva collection devices in usetoday: drool collected in a sterile specimen container (A);Salimetrics oral swab (B).
Saliva collection devices in use

Salivette cotton and synthetic device (C); Greiner Bio-One saliva collection system (D)

OriGene DNA collection device (E); and DNASal collection device (F).

Advantages and Disadvantages of Saliva as a Diagnostic Fluid

THANK YOU