Salient Periodontal Issues for the Modern Biologic Orthodontist
17
Salient Periodontal Issues for the Modern Biologic Orthodontist Leena Palomo, Juan Martin Palomo, and Nabil F. Bissada The term synergy refers to the interaction between many agents acting in concert to create an effect greater than the sum of the separate parts; in other words the whole is greater than the sum of the parts. This definition helps one understand the biologic basis of periodontal orthodontic relation- ships in either therapy or disease. Synergistic collaborative treatment be- tween the specialists also helps develop the harmony that results in less damage to both components of the periodontium, the soft tissue “gingival unit” around the crown, and the “attachment apparatus” that connects the root to bone. Orthodontists should recognize possible periodontal risks to patients undergoing orthodontic treatment and any “damage” to the peri- odontium or enlargement of the gingiva is often an inevitable and reversible side effect. The goal is to minimize any harmful effects as any good surgeon seeks to minimize an inevitable scar. This is best done by interdisciplinary collaboration in controlling infection with chemicals, erupting teeth through keratinized gingiva, empowering patients with modern regenerative sur- gery, and using orthodontic therapy to minimize the amount of bone that is removed during periodontal osseous surgery. Thus, with synergistic collab- oration, orthodontic therapy can enhance periodontal health and periodon- tal therapy can enhance the orthodontic outcome. (Semin Orthod 2008;14: 229-245.) © 2008 Published by Elsevier Inc. T he term synergy refers to two or more dis- tinct influences or agents acting together to create an effect greater than that predicted by knowing only the separate effects of the individ- ual agents; in other words the whole is greater than the sum of the parts, as a symphony is more than the arithmetic sum of each instrument’s performance. This definition is applicable to the classic relationship between orthodontic and pe- riodontic specialties in treating patients. Under- standing the biologic basis of periodontal surgi- cal procedures, recent advancements in tissue engineering, and research development can yield more productive clinical endpoints than ever before. Making the most of what these two specialties offer each other begins with the iden- tification of periodontal problems that could become more complicated during orthodontic therapy and, conversely, those that could benefit from orthodontic therapy. The Question as to Whether Orthodontic Therapy Contributes to Periodontal Disease The periodontium consists of two parts: the “gin- gival unit,” the gingival margin to the most coro- nal connective tissue fiber attached to the osseous crest and the remainder of the periodontium, the periodontal ligament (PDL), alveolus to Diplomate, American Board of Periodontics, Assistant Professor of Periodontics, Director of Predoctoral Periodontics, School of Dental Medicine, Case Western Reserve University, Cleveland, OH. Diplomate, American Board of Orthodontics, Associate Professor of Orthodontics, Craniofacial Imaging Center—Director, School of Dental Medicine, Case Western Reserve University, Cleveland, OH. Professor and Chairman of Periodontics, School of Dental Med- icine, Case Western Reserve University, Cleveland, OH. Address correspondence to Nabil F. Bissada, DDS, MSD, Case Western University, School of Dental Medicine, 10900 Euclid Ave- nue, Cleveland, OH 44106. Phone: (216) 368-6757; Fax: (216) 368-3204; E-mail: [email protected] © 2008 Published by Elsevier Inc. 1073-8746/08/1404-0$30.00/0 doi:10.1053/j.sodo.2008.07.002 229 Seminars in Orthodontics, Vol 14, No 4 (December), 2008: pp 229-245
-
Upload
ahmed-tarek-el-shanawany -
Category
Documents
-
view
26 -
download
4
description
Salient Periodontal Issues for the ModernBiologic OrthodontistSeminars in Orthodontics, Vol 14, No 4 (December), 2008: pp 229-245
Transcript of Salient Periodontal Issues for the Modern Biologic Orthodontist

SBL
Ttkuttp
oM
oD
i
Wn3
alient Periodontal Issues for the Moderniologic Orthodontist
eena Palomo, Juan Martin Palomo, and Nabil F. Bissada
The term synergy refers to the interaction between many agents acting in
concert to create an effect greater than the sum of the separate parts; in
other words the whole is greater than the sum of the parts. This definition
helps one understand the biologic basis of periodontal orthodontic relation-
ships in either therapy or disease. Synergistic collaborative treatment be-
tween the specialists also helps develop the harmony that results in less
damage to both components of the periodontium, the soft tissue “gingival
unit” around the crown, and the “attachment apparatus” that connects the
root to bone. Orthodontists should recognize possible periodontal risks to
patients undergoing orthodontic treatment and any “damage” to the peri-
odontium or enlargement of the gingiva is often an inevitable and reversible
side effect. The goal is to minimize any harmful effects as any good surgeon
seeks to minimize an inevitable scar. This is best done by interdisciplinary
collaboration in controlling infection with chemicals, erupting teeth through
keratinized gingiva, empowering patients with modern regenerative sur-
gery, and using orthodontic therapy to minimize the amount of bone that is
removed during periodontal osseous surgery. Thus, with synergistic collab-
oration, orthodontic therapy can enhance periodontal health and periodon-
tal therapy can enhance the orthodontic outcome. (Semin Orthod 2008;14:
229-245.) © 2008 Published by Elsevier Inc.
crsceyestbtf
TOP
Tgnc
he term synergy refers to two or more dis-tinct influences or agents acting together
o create an effect greater than that predicted bynowing only the separate effects of the individ-al agents; in other words the whole is greater
han the sum of the parts, as a symphony is morehan the arithmetic sum of each instrument’serformance. This definition is applicable to the
Diplomate, American Board of Periodontics, Assistant Professorf Periodontics, Director of Predoctoral Periodontics, School of Dentaledicine, Case Western Reserve University, Cleveland, OH.
Diplomate, American Board of Orthodontics, Associate Professorf Orthodontics, Craniofacial Imaging Center—Director, School ofental Medicine, Case Western Reserve University, Cleveland, OH.
Professor and Chairman of Periodontics, School of Dental Med-cine, Case Western Reserve University, Cleveland, OH.
Address correspondence to Nabil F. Bissada, DDS, MSD, Caseestern University, School of Dental Medicine, 10900 Euclid Ave-
ue, Cleveland, OH 44106. Phone: (216) 368-6757; Fax: (216)68-3204; E-mail: [email protected]
© 2008 Published by Elsevier Inc.1073-8746/08/1404-0$30.00/0
tdoi:10.1053/j.sodo.2008.07.002
Seminars in Orthodontics, Vol 14, No
lassic relationship between orthodontic and pe-iodontic specialties in treating patients. Under-tanding the biologic basis of periodontal surgi-al procedures, recent advancements in tissuengineering, and research development canield more productive clinical endpoints thanver before. Making the most of what these twopecialties offer each other begins with the iden-ification of periodontal problems that couldecome more complicated during orthodonticherapy and, conversely, those that could benefitrom orthodontic therapy.
he Question as to Whetherrthodontic Therapy Contributes toeriodontal Disease
he periodontium consists of two parts: the “gin-ival unit,” the gingival margin to the most coro-al connective tissue fiber attached to the osseousrest and the remainder of the periodontium,
he periodontal ligament (PDL), alveolus to2294 (December), 2008: pp 229-245

wsttml
otettrfiggcticpHpofphsosAacbh
dcimcdptosoifop
pebcootcmae
M
Usdafafmpdatatos
poamapfoplmdnas
pb
v
230 Palomo, Palomo, and Bissada
hich it is attached and root elements. Thisecond major anatomical unit is referred to ashe “attachment apparatus” on which is basedhe term “attachment loss.” The latter term is
ore appropriate than the ambiguous “boneoss” when referring to periodontitis.
Maintaining a healthy periodontal status inrthodontic patients is a perennial and ubiqui-ous challenge to most orthodontists, and thentrance of an increasing number of adults intohe orthodontic treatment population increaseshe risk of iatrogenic periodontal damage. Manyesearchers worldwide have investigated the ef-ects of fixed orthodontic appliances on patientsn relation to periodontal attachment loss andingivitis.1-6 Most periodontal challenges areingival since fixed appliances can indirectlyontribute to an exacerbation of any inflamma-ion. Chronic inflammation is generally revers-ble on appliance removal or following patientompliance with standard periodontal recall ap-ointments and personal oral hygiene regimens.owever, chronic inflammation can cause fibro-lasia in most areas of the human body and theral cavity is no exception. Orally that is mani-est as permanent gingival hyperplasia known asostorthodontic gingival enlargement. Gingivalyperplasia is difficult to differentiate becauseuperficial fibrosis mimics gingival health so therthodontists should actively investigate the pos-ibility of pernicious damage. Alexander, andtack and others7-9 suggested that orthodonticppliance removal leads to similar periodontalonditions as those present before treatment,ut their conclusions beg a larger question ofyperplasia and gingival pocket management.
Although most problems are gingival, it isifficult to ignore the findings of Hamp andoworkers10 who found that “in conclusion, dur-ng a long-term period of active orthodontic treat-
ent with fixed appliances a slight but signifi-ant loss of periodontal support was observedespite the establishment and maintenance ofroper oral hygiene standards.” The word “long-
erm” is emphasized. An excellent review of peri-dontal bacteriology has been authored by Loe-che and Grossman,11 which suggests that therthodontist should always be prepared for the
ndividual patient who does not conform to pro-essional instructions that should ensure peri-dontal health. Contemporary commercial em-
hasis on esthetics, “invisible” appliances, and iractice management, however, have somewhatclipsed the biological imperatives that form theasis of orthodontic care and protect the clini-ian from untoward destructive side effects. Inne very real sense the sciences of osteology andrthopedics, as integral parts of all orthodonticooth movement (OTM), can never be seriouslyonsidered irrelevant to any orthodontic treat-ent. They can only be ignored. This article
ims to make that science understandable andasily incorporated into daily practice.
echanisms of Tissue Damage
nfestooned orthodontic bands are particularlyuspect as possibly complicating factors jeopar-izing interproximal periodontal support, andt the present time “special periodontallyriendly bands” are being designed in researchnd design laboratories. These challenging ef-ects of band impingement may directly compro-
ise local resistance related to subgingivalathogens in susceptible patients and result inamage to both interproximal gingival tissuesnd alveolar crestal bone in a manner similar tohat produced by faulty crown margins. Diedrichnd coworkers12 observed apical migration ofhe junctional epithelium and defects in orth-dontic cemented bands in 85% of the subjectstudied.
Årtun and Urbye (1998)5 suggest that theeriodontal damage witnessed in their study ofrthodontic patients is corroborated by others13
nd, beyond the well known mechanisms of trau-atic occlusion, that periodontal support might
lso be damaged during tooth intrusion whereatients have active periodontitis or gingival in-ection significant enough to convert to peri-dontal disease. In these kinds of susceptibleatients a screening examination for the inter-
eukin (IL) family of inflammatory mediatorsay be wise. The details of genetic screening,
iscussed elsewhere in this issue, study the ge-etic potential of exaggerated immunologic re-ctions of host response to bacterial challengeuch a those that recruit IL-1�.14,15
Although such tests may not be specific foreriodontitis it has been associated with a num-er of serious health problems.16
Thus, where available, an assessment of ele-ated inflammatory mediator may be prudent, as
t represents some of the latest scientific at-
trleofb
ciatscclgoo
epttimWweaflem
nloapgs
tciefiwaapm
sct“iaadsfsecpfudcu
opawsawcmbibccisaTpndtb
iscorpt
231Salient Periodontal Issues
empts that eclipse gross clinical observation oradiographs in its ability to clarify systemic etio-ogic elements of periodontal health and dis-ase. This enhances the value of care to orth-dontic patients or their parents who are payingor the “best” modern orthodontics with a strongiologic rationale.
C-reactive protein (CRP) has also been asso-iated with both cardiovascular disease and oralnfection.17 Noack and coworkers18 have notedn increase in CRP levels in periodontitis pa-ients with severity of the disease even where age,moking, body mass index, triglycerides, andholesterol have been statistically eliminated asonfounding variables. Also, there are elevatedevels of CRP associated with infection with sub-ingival organisms often associated with peri-dontal disease, including a number of notori-us periodontal pathogens.
Therefore, for orthodontists who are inter-sted in distinguishing themselves as an integralart of the health care profession, any evalua-
ion of genetic susceptibility and systemic healthhreats associated with the infection can mean-ngfully enhance their orthodontic treatment as
ore than merely minor cosmetic adornment.hile the details and validity are still beingorked out at major research centers, the mod-rn orthodontist may wish to remain educatedbout emerging oral tests of gingival crevicularuid (GCF) to assess systemic health and dis-ases that relate to easily diagnosed genetic poly-orphisms.The etiology of periodontal problems may
ot simply rely on exaggerated host immuno-ogic reactions. Mattingly and coworkers19 andthers20-22 reflect the view that long-term fixedppliances can contribute to unfortunate butredictable qualitative alterations in the subgin-ival bacterial biofilms that become progres-ively periodontopathic with time.
One cannot make the airtight claim thathere is absolutely unequivocal proof of causalonnection among all orthodontic patients andnevitable contributions to periodontitis. How-ver, the same can be said of orthodontic bene-ts. We cannot claim that orthodontic treatmentill universally guarantee a more productive lifend self-esteem. So to dismiss periodontal dam-ge by reasoning that it is a minor event in mostatients is fallacious. Extrapolations and com-
on sense must prevail at this point in the ab- oence of absolute proof that microbiologicalhanges of crevicular fluid components provehat orthodontic fixed appliances singularlycause” periodontitis to worsen. At this point, asn many multifactorial causal systems, it remainst most a “risk factor” and quality-of-life issue justs much as physiologic dental alignment. Theegree to which any orthodontist seeks to per-onally protect his or her patient from all riskactors is a matter of individual preference andtyle of practice. Sufficient circumstantial dataxist, however, to convince the modern biologi-ally oriented orthodontist to at least inform theatient of the possibility of risk in a formal in-ormed consent document and ensure that reg-lar prophylaxis is maintained. Once that isone, the contributions to periodontal health byonscientious orthodontic therapy are virtuallyndeniable.
On a practical level it seems that an absencef bleeding on probing is a better forecastingarameter of health than bleeding on probing is
predictor of progressive disease. In otherords, an absence of bleeding on probing, de-
pite the pocket depth can justifiably be used astest of “healthy gums.” On the other hand,
hile bleeding on probing is certainly an indi-ation of infection of the gingivae, it is one ofany risk factors associated with progressive
one loss due to periodontitis. However, the tests not spontaneous bleeding or even bleeding onrushing and flossing. That elicits only superfi-ial disease, one that contributes significantly toaries and marginal decalcification. The best tests “bleeding on probing” elicited by stroking theulci with a flexible plastic periodontal probe atcomfortable range of force between 10 to 20 g.hose orthodontic patients who present withersistent bleeding on such probing should beotified that they are “at risk” and that prudenceictates a more intensive regimen of periodontalherapy than those who present with little or noleeding on probing.
Since bleeding swollen gingiva is ubiquitousn the orthodontic population universal cautionhould be employed and supportive periodontalare recommended routinely as an integral partf orthodontic therapy.23,24 Boyd and Baum-ind25 and others26,27 have pointed out the im-ortance of a full-mouth examination, six sites per
ooth, for a comprehensive description of peri-
dontal status in orthodontic patients. Thus, it is
scnaotrewe
s
eesctdwpovpptanowcvm
baagpcw
rns
T
Simtidgffstfeit
adlmsatcofhs
iwaptntpdpa(otp
232 Palomo, Palomo, and Bissada
till not clear if these circumstantial data of perni-ious effects of orthodontic therapy might perma-ently influence the susceptibility to periodontalttachment loss in healthy patients undergoingrthodontic treatment, but it is certainly nothinghat can be ethically or scientifically ignored. Theesponsibility, however, should be shared, and del-gation to trained, competent ancillary personnelith educational talents is very effective under gen-ral supervision by the orthodontist.
The words of Sanders give us an excellentummation of the pertinent literature:
Orthodontic bodily tooth movement into plaque-induced in-frabony defects can be successfully performed, provided thatthe periodontal lesion is eliminated before tooth movement isbegun and that excellent oral hygiene is maintained. Al-though there is no unfavorable effect on the level of connec-tive tissue attachment under these optimal conditions, nei-ther does there appear to be a gain in soft-tissue attachment.On the other hand, if subgingival plaque and periodontaldisease are not controlled before and during orthodontictreatment, an accelerated loss of attachment may result.28
This is particularly sage advice when recentvidence suggests that popular methods of non-xtraction therapy, rapid palatal expansion, pere may cause a reduction in the amount of buc-al periodontal bone support.29 The conclusionhat seems most logical is that some periodontalamage may occur, particularly in those patientsho exhibit poor oral hygiene during fixed ap-liance therapy, but the contribution of orth-dontic care is generally minor, occasionally se-ere enough to justify periodontal therapy andrevalent enough to indicate concomitant sup-ortive periodontal therapy as a routine preven-
ive tactic during fixed appliance therapy. It isdvisable that professional scaling and root plan-ing, where indicated, be performed by a peri-dontist and alternated with restorative dentistsho can also provide prophylactic measures foraries control, for example, sealants, fluoridearnish, and with alternating recalls every 3onths with the periodontist.With the trend toward the use of bonded
racket by orthodontists, removal of arch wiresnd brackets for restorative care is understand-ble, but routine removal of arch wires for sub-ingival scaling and root planing does not ap-ear to be necessary. Fixed appliance removalan also risk orthodontic relapse and interfere
ith expedient tooth movement. Therefore, moutine appliance removal every 3 months is notecessary and should be requested only underpecifically difficult circumstances.
reating the Infected Patient
ince the human mouth is impossible to steril-ze, the orthodontist should consider all patients
ore or less “infected.” This begs many ques-ions of management given that one cannot eas-ly distinguish between benign commensal resi-ents, those that limit their damage to theingival unit, and more virulent pathogenicorms. As universal precautions are employedor OSHA requirements, “universal caution”hould be employed with all orthodontic pa-ients and every patient should be (1) informedor the risks of periodontal damage and (2)xplicitly encouraged to participate in “formalnitial therapy” before and during all orthodon-ic treatment with fixed appliances.
The classic relationship between periodontitisnd orthodontics lies in managing plaque-in-uced infection with different degrees of viru-
ence. The key in delivery of appropriate treat-ent is distinguishing reversible gingivitis from
elf-perpetuating and progressive periodontitis,n infection that requires the diagnostic andherapeutic abilities and interventions of a clini-ian. Therapy for both is aimed at the reductionf etiologic factors that damage tissue directlyrom bacterial toxins and indirectly due to theost’s destructively excessive inflammatory re-ponse.
Bone loss is the hallmark of periodontitis. Itnvolves loss of the “attachment apparatus” ofhich bone is a part and may or may not bemenable to regeneration depending on theattern of destruction and an individual pa-ient’s biologic capacity for regeneration. Withotable exceptions, children and adolescents
end to develop gingivitis (hypertrophic or hy-erplastic) without massive loss of attachmenturing orthodontic therapy when compliance isoor. Zachrisson and Alnaes30,31 noted decadesgo that although periodontal attachmentbone) loss is not a common threat to the orth-dontic patient on average, some individual pa-ients may show some pernicious damage to theeriodontal attachment.
In fact, the patient with root resorption of 3
m is less compromised than the patient with
mt
1fdpsid(tb
tctieaDnmspmtopdthis
cabfvlataarrtdbtc
cddtootdia(nimngtccmt
edmWpmacanedsimgjgdl
dapaotcs
233Salient Periodontal Issues
arginal bone loss due to the conic nature ofhe root form.
Interestingly individual patients in the 13- to8-year-old age group may harbor infection andrank periodontal attachment loss patterns thato not conform to the norm. Significantly, Cap-elli and coworkers32 noted that 25.7% of thetudents in a study of Hispanic patients exhib-ted early-onset periodontitis (EOP) with 1.7%iagnosed as localized juvenile periodontitisLJP). This fact alone should alert orthodontistshat the teenage populations may not be able toe treated with impunity.
Encouraging is the report of Johal and Lee33
hat simple modifications in orthodontic proto-ols can ameliorate any iatrogenic damage thathreatens the clinical outcome. Simple support-ve care, if not ensuring against periodontal sideffects, at least can allow patients to modulateny pernicious effects with supportive care.iedrich and coworkers12 noted that the con-ective tissue attachment damage at the ce-ento-enamel junction of banded teeth was so
everely damaged on the mesial surface and theocket epithelium proliferated toward the apex,eaning progression from established gingivitis
o an initial periodontal lesion. It is these kindsf individual problems that most experiencedractitioners guard against, because statisticalata and general trends do not necessarily cap-
ure the entire domain of private practice co-orts especially when data are pooled or exper-
mental selection bias (eg, dental students asubjects) occurs in the research.
Moreover, although it may be comforting toonsider that orthodontic patients are, “on aver-ge,” less prone to problems, averages may note of significance to the individual patient. In-ormed patient consent and awareness of risksersus rewards are strongly advised. Attachmentoss in an adolescent with bleeding on probingnd the presence of bacteria that can invadeissue may have serious systemic implications,nd treating without informing both parentsnd patient is untenable in light of modernesearch data on oral bacteriology and diseaseesearch in cardiovascular disease. Ironically,reating adult patients may be less risky becauseisease is more prevalent and less obscure andoth clinicians and patients are likely aware ofhe patient’s medical condition. This is espe-
ially true of patients who smoke tobacco or are tompromised with systemic conditions such asiabetes, connective tissue disorders, endocrineisorders, neutrophil abnormalities, HIV, andhose with a family history of dentures or peri-dontitis. Therefore, a comprehensive orth-dontic diagnosis that includes assessment ofhe periodontal foundation is the critical step inetermining an appropriate treatment plan for
ndividual cases. Attachment loss cannot be di-gnosed simply by even the best radiographseg, a full series of films using a parallel tech-ique with a superimposed 1-mm grid on bitew-
ngs and periapical exposures), which essentiallyeasure trabecular patterns of the endosteum,
ot the medullary bone where periodontitis be-ins. This is because radiographs underestimatehe degree of attachment (bone) loss unless it isorrelated with periodontal probing below theontact point. Likewise line angle probingisses incipient lesions that initiate the destruc-
ive process apical to the col.Attachment loss may actually begin during
ruption of permanent teeth into an arch lengtheficiency and may produce permanent attach-ent loss even before full eruption according toaerhaug.34 Lest the orthodontist becomes too
reoccupied with periodontal problems, weust remember that orthodontic therapy gener-
lly helps more than it hurts. Apparently, ac-ording to Waerhaug,34 arch length deficienciesnd distortion of contact point/embrasure formearly always ensure at least some gingival pock-ting where crowding (arch length deficiencies)rive plaques subgingivally. Moreover trauma as-ociated with faulty bracket position, partial bond-ng, and untoward trauma during individual tooth
ovement can drive supragingival plaque subgin-ivally to initiate pathological changes in the sub-
acent attachment apparatus. Some evidence sug-ests that trauma per se may create qualitativeeterioration of subgingival biofilm to more viru-
ent bacterial profiles.The mechanism of accelerated periodontal
estruction around teeth with occlusal traumand increased mobility remains unclear. Oneossible mechanism is that tooth mobility cre-tes a subgingival environment conducive tovergrowth by periodontal pathogens. One au-horitative study compared the subgingival mi-roflora in mobile and nonmobile teeth of 35upportive therapy adult patients and 15 un-
reated adults with periodontitis. Grant and
cttpercp
mdtiTspttao
p
cptimpmIhraorgfegcnipr
F(mtm
234 Palomo, Palomo, and Bissada
oworkers35 found that pockets around mobileeeth harbored significantly higher propor-ions of known periodontal pathogens thanockets with nonmobile teeth. These research-rs suggested that tooth mobility may pose aisk for periodontal breakdown due to an in-reased subgingival occurrence of specificeriodontal pathogens.
This potential brings up a practical issue forost practicing orthodontists. Since a great
egree of task delegation keeps orthodonticreatment affordable, task delegation may benadequate supervision of disease activity.hus delegation to a general dental supervi-
ion or periodontal specialist may be the mostrudent course. A simultaneous “tandemreatment” with conventional fixed applianceherapy and standard nonsurgical “initial ther-py” emerges as the optimal protocol for mostrthodontic patient groups.
The monitoring should involve recordingrobing pocket depth in even seemingly mild
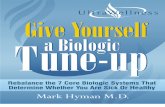
igure 1. (A) Probing at static points such as line anB) A common error is not advancing the probe farore accurately detect defects, the periodontal probe
he clinician to follow the attachment around the too
ay be necessary to “walk” the probe underneath the contaases because a mere 5-mm interproximalocket on the mesial of a maxillary first molar
hreatens to produce horizontal progressionnto the trifurcation rendering treatment
ore problematic with a relatively poorerrognosis. A Michigan O probe with Williamsarkings (Hu-Friedy Manufacturing, Chicago
L) is recommended because its precise scoringelps ensure accuracy. The actual probing forcearely needs to be more than 20 to 25 g of force,force generated by little more than the weightf the probe itself (�17 g) (Fig 1). It is critical toealize that gingival recession, zone of attachedingiva, attachment level of some infrabony de-ects entirely within the medullary bone mayscape diagnosis in periapical or bitewing radio-raphs. However, if the diagnosis is made by aollaborating professional, the orthodontisteed only provide a screening examination, cal-
brate probing accuracy with the comanagingrofessional, and inform the patient of potentialisks and then concentrate on the biomechani-
may miss defects that are not located in those areas.gh interproximally and under the contact point. Towalked” along the junctional epithelium. This allowsd reach the depth of the pocket. A slight angulation
glesenou
is “th an
ct point. (Color version of figure is available online.)

cedstt
hdsmpltpbomtif
otttcttrmbIgtootcmmet
T
Oiisib
ccni
tscttcitcrwmdaiacpv
mfbttdmfgaifaetfipco
G
Oaofi
235Salient Periodontal Issues
al protocol. This kind of shared responsibilitynsures that periodontal pockets (pathologicallyeepened sulci) will be managed as well as pos-ible. Ultimately it is the patient’s responsibilityo assume treatment risks on well-informed writ-en consent.
It is important to understand some of theistology of the pocket to understand health andisease (Fig 2). The area of the pocket, theo-called forefront of the “periodontal lesion,” isost vulnerable because it is bounded by hyper-
lastic epithelium, which is not keratinized. Thisack of stratum corneum has given rise to theheory that the gingival sulcus is a susceptibleoint of entry to subjacent connective tissue andone and even influences the spread of micro-rganisms’ toxins into the systemic environ-ent. This is why periodontitis has not escaped
he attention of the medical community, whichs taking a renewed interest in the systemic ef-ects of chronic untreated oral infection.36
The junctional epithelium, apical to the basef the clinical pocket, forms the attachment be-ween tooth and gingiva. The apical extent ofhis epithelium is thinner, just a few cell layershick, has two basal laminas, one to attach toonnective tissue and the other to attach toooth surface. These “functional” epithelial cellsurn over every 4 to 6 days and play a significantole in breakdown of the periodontal attach-ent. Healing of these cells is known as “repair
y long functional (or junctional) epithelium.”n contrast, “new attachment” procedures or “re-eneration” of periodontal attachment refers tohe restoration of an entirely new tissue complexf cementum, ligament fibers, and bone previ-usly destroyed by disease. The nuance is impor-ant because a long junctional epithelial (notonnective tissue) attachment to the root canimic regeneration of a new periodontal attach-ent when viewed clinically by an inexperi-
nced clinician. Disease can look like health tohe untrained eye.
reatment Options and Rationale
nce periodontitis is diagnosed two major modal-ties of care have proven effective. The first is anti-nfective treatment. The goal is to stop the progres-ion of disease by minimizing the amount andnfluence of a primary etiologic element, that is,
acterial plaque biofilms. This is often elusive be- Gause the natural communal aggregations of mi-robes that form on all wet surfaces appear to theaked eye identical to virulent bacteria-laden flu-
ds of the mouth and the surface of the tooth.The second major objective is regenerative
herapy to restore structures that have been de-troyed by disease with new attachment: bone,ementum, and periodontal ligament. Initialherapy is directed at the reduction of oral bac-eria and associated calcified deposits and non-alcified biofilm. Good home care is stressed tomprove oral hygiene and plaque scores are usedo quantify the extent of the improvement. Lo-al irritating factors like calculus and defectiveestorations are removed. Orthodontic archires and brackets usually need not be re-oved, depending on extent and severity of
isease. Removal of calculus and biofilms ischieved by hand, sonic, ultrasonic, or piezonstruments. Topical antibacterial agents, withctive ingredients such as chlorhexidine diglu-onate or triclosan (5-chloro-2-(2,4-dichloro-henoxy)phenol), help to reduce supragingi-al bacterial plaque.37
However, the problem is that topical liquidsay not reach the subgingival environment ef-
ectively, even when delivered under pressure,ecause they do not remain in close contact withhe root surface for long enough periods ofime. There is protection by the architecture ofental plaque, a dynamic bacterial biofilm “com-unity” that has formidable microbiologic de-
ense mechanisms. Treating the surface of theingiva only “masks” deeper disease. Profession-lly controlled delivery of solids or gels, however,s effective because these materials remain activeor a long period of time. The latter chemicalgents, deep inside periodontal pockets, are veryffective, according to Drisko,38 and althoughhe process is more time consuming than super-cial brushing, the outcomes confirm the hy-otheses of other experts in the field that theyan be an effective means of maintaining peri-dontal health.39-41
ingival Hyperplasia
vergrowth of tissue during orthodontic ther-py is also a threat to periodontal health and isften more pernicious because its fibrotic super-cial appearance can mimic health42 (Fig 3).
ingival enlargement (see Waldrop elsewhere in
236 Palomo, Palomo, and Bissada
Figure 2. Illustration showing what is measured us-ing a periodontal probe. (A) Healthy environmentshowing a sulcus, also known as periodontal pocketif infected and/or pathologically deepened; (B)due to gingivitis, the value measured may indicate a“deep” pocket, but there is not bone loss present.This is also known as pseudopocket. (C) Illustrationshowing both attachment and bone loss, and whatcould be measured as a “deep” pocket. Even thoughthe linear depth may be lower in this situation thanin the previous, the bone loss present categoricallyindicates a worse prognosis. (Color version of figureis available online.)

thpcmtie
M
Igcibttcsttrpfosgf
urflamtmbhowbpTngttssnepsdgpc
rtvpatfwttMttmt
trcai
Fpiarcadtci
237Salient Periodontal Issues
his issue) not only complicates the patient’s oralygiene, and creates esthetic and functionalroblems, but by increasing the depth of thelinical pocket, creates an environment for pre-ature definitive attachment loss (periodonti-
is) in susceptible patients and can thereforenterfere with the diagnosis of more serious dis-ase closer to the alveolar bony crest.
anaging Patients at Risk
n patients with active periodontal disease, pro-ressively resorbing bone, the threat of compli-ations is more imminent but does not categor-cally contraindicate OTM. Initial therapy maye followed by surgical treatment to improveissue topography by surgical osteoplasty/ostec-omy or guided tissue regeneration (GTR). Thehoice of treatment plan depends on factorsuch as plaque score, width of the zone of kera-inized tissue, and osseous architecture. The ex-ent of the osseous surgery and predictability ofegeneration depend on the extent and mor-hology of the osseous defect (Fig 4). There-ore, a well-orchestrated leveling and aligningf teeth can actually minimize the need forurgical bone removal during periodontal sur-ery and enhance bone development through
igure 3. Inflammatory overgrowth. The gingiva im-inges on the clinical crown. Chronic inflammation
n humans often leads to fibroplasia and permanentlteration in form, that is, clinical hyperplasia, whichequires surgical treatment. Even though hyperplasiareates a “pseudopocket,” the depth is conducive tottachment loss and should not be trivialized. Clinicalistinctions between pseudopocketing and true at-
achment loss are often impossible and the prudentlinician plans for the worst. (Color version of figures available online.)
orced eruption. a
Some two-walled defects with shallow cratersp to 4 mm may be corrected with minor boneemoval (ostectomy) and an apically positionedap. For deeper bone defects, however, newdvances in tissue engineering can be used toanage three-walled defects that are deeper
han 4 mm, some hemiseptal defects, and someolar furcation defects with limited tooth mo-
ility. Currently, bone grafts using autogenouslyarvested bone, allografts, such as mineralizedr demineralized freeze-dried bone, with orithout a resorbable or nonresorbable mem-rane, are commonly used with a high degree ofredictability in the treatment of periodontitis.he bone graft generally serves as a scaffold forative bone growth and the introduction ofrowth factors can generate new bone, even ec-opically in animals, by a process of osteoinduc-ion (creating bone de novo). How, specifically,urgical mechanisms of osteoinduction relateynergistically with bone created by OTM hasot yet been clearly defined. Nonetheless discov-ries in tissue and genetic engineering are mostromising and can add an exciting new dimen-ion to the daily practice of dentofacial orthope-ics. Clinicians who incorporate periodontal sur-ery with orthodontic therapy might treat newatients who would otherwise avoid orthodonticare.
The purpose of the resorbable and non-esorbable tissue membranes is to exclude epi-helial ingrowth into the bony defect and pro-ide space between the mucoperiosteal flap anderiodontal bony lesion to protect osteogenesisnd new attachment to the root. If gingival epi-helium and connective tissue can be delayedrom migrating into the defect during earlyound healing, reconstruction of the periodon-
al tissues can progress from pluripotent cells ofhe periodontal ligament and alveolar bone.
embranes and bone grafting materials are of-en used together to reduce micromovement ofhe graft and are well-accepted modalities to
aintain the alveolar crestal bone height andhickness.
In the past, prudence dictated that periodon-ists delay orthodontic tooth movement until theegenerated tissues were mature. However, re-ent clinical research by Wilcko and Fergusonnd coworkers (see Wilcko and coworkers in thisssue) have shown that tooth movement through
healing graft is not only safe but may actually

238 Palomo, Palomo, and Bissada
Figure 4. Bone loss analysis based on mor-phology. (A) One-wall defect, (B) two-walldefect, and (C) three-wall defect. More wallscontribute to an improved prognosis for re-generation. (Color version of figure is avail-able online.)

eortibro
G
RmmMostrsmi
manccsch
iac“oactamitptdtgps
nm
ctsectwiaca2t
giTgefooc(AbttcgFsaflbElawtrv
etto(
239Salient Periodontal Issues
nhance the orthodontic clinical outcome andbviate any need for tooth extraction. The “pe-iodontally accelerated osteogenic orthodon-ics” protocol (PAOO) presents a most promis-ng frontier for future interdisciplinary synergyetween the specialties of orthodontics and pe-iodontists. (PAOO is a trademark of Wilck-dontics, Inc., Erie, PA.)
ingival Reconstructive Procedures
econstructive surgery is performed on abnor-al structures that may be congenital, develop-ental, results of trauma, infection, or disease.ucogingival surgery (often referred to as “peri-
dontal plastic surgery”) is an example of recon-tructive surgery available to orthodontic pa-ients. The goal of mucogingival procedures is toestore periodontal health through the recon-truction of lost hard and soft tissue. Improve-ent of esthetics is another goal of the mucog-
ngival procedures.Whether the nature of periodontal attach-
ent (regenerated attachment apparatus versuslong junctional epithelium or both) has a sig-ificant impact on the clinical result is not yetlearly defined in the literature and cannot beonfirmed in each patient because of ethicaltrictures; that is, the nature of the attachmentan only be confirmed by experimenting on liveumans.
Tooth malposition, alveolar bone dehiscence,mpinging restorative or orthodontic appliances,nd chronic infection are all risk factors thatontribute to mucogingival lesions known asgingival stripping” or “runners” in the clinicalrthodontic terminology.43 While the lesion mayppear during orthodontic tooth movement nolear correlation has been demonstrated be-ween tooth position and gingival dehiscencend may represent one of the most unfortunateisconceptions in the field of orthodontics.44 It
s important to realize that in adolescents orransitional dentition patients, a “precocious”assive eruption, compared with adjacent re-
arded passive eruption, may mimic true gingivalehiscence. This is easily diagnosed by palpating
he cemento-enamel junction (CEJ). If the gin-ival margin is at the CEJ and palpable with arobe, the lesion is a kind of “pseudo reces-
ion,” and if sufficient connective tissue thick- cess lies at the cervix of the tooth, no treat-ent is needed.True gingival recession and bony dehis-
ences, however, are a constant threat that seemo be minimized by a thick buccolingual dimen-ion of alveolar bone. Where this is absent andxtraction therapy is contraindicated due to fa-ial profile esthetics, the PAOO procedure in-roduced by Wilcko and coworkers45 serves as aell-founded alternative to orthognathic surgery
n some cases. What is particularly encouragingbout PAOO is that it lends greater stability thanonventional orthodontic biomechanics while itccelerates the tooth movement rates by at least00% with both outcome quality and periodon-al impunity.
However, a simple prophylactic soft tissue gin-ival augmentation may be reasonable especiallyn patients with thin periodontal biotype.46,47
reatment of gingival recession by soft tissuerafting for complete root coverage requires ad-quate vascular supply. This may be obtainedrom the subjacent underlying bone and peri-dontal ligament and from the gingival flapverlying the graft. The early surgeries for rootoverage employed laterally positioned flapLPF), rotational flaps, and repositioned flaps.n average of 67% root coverage can be attainedy LPF. Free gingival grafts evolved from a desireo expand the zone of keratinized tissue tohicker ones with greater predictability for rootoverage. Root coverage expected from free gin-ival grafts was estimated to be 69% of the root.ree gingival grafts have a single source of bloodupply from the underlying bone, periosteum,nd periodontal ligament. Coronally positionedap procedure advances tissue already presenty a distance equal to the extent of recession.xisting papillae are deepithelialized and over-
apped by the newly created gingival tissue. Anverage of 61% root coverage can be achievedith the main limitation being the zone of kera-
inized tissue that is present. If the existing ke-atinized tissue is limited, the potential to ad-ance a flap is also limited.
Recently, with the development of tissuengineering, enamel matrix derivative appliedo coronally positioned flap has been reportedo enhance root coverage to a mean coveragef 86% of the root.48 Enamel matrix derivativeEMD) is a resorbable, implantable material
onsisting of hydrophobic enamel matrix pro-
tbpiapcsofndd
grt(haTeebtOhasr(taet
pesttchmdoacwFcr
setmimStmwtatct
V
WspsocsiTdod
Fmpottia
240 Palomo, Palomo, and Bissada
eins extracted from a developing porcine em-ryo. When applied in a gel form to the ex-osed root, the protein assembles into an
nsoluble three-dimensional matrix. New bonend periodontal ligament formation are re-orted using EMD.48 An average of 98% defectoverage is obtained because of the dual bloodupply from the underlying periosteum andverlying flap. Since reflecting a flap inter-eres to some extent with the vascular beds, aewer, no-flap, tunnel preparation has beeneveloped to slide connective tissue graft un-erneath the overlying flap.
Over the last few decades, connective tissuerafting has expanded the possibilities for cor-ecting mucogingival defects. With the advent ofissue engineering, guided tissue regenerationGTR), to a mean coverage of 86% of the root,as also been employed for root coverage usingbioabsorbable or nonresorbable membrane.
he membrane is sutured into place to preventpithelial ingrowth. The membrane is then cov-red completely with a coronally positioned flapecause an exposed membrane is often subjecto infection and may compromise the results.ne benefit of this technique is that the GTRas the potential to regenerate new bone. Andvantage of GTR is that there is no need for aecond surgical site to obtain donor tissue. Moreecently, the use of acellular dermal matrixADM) was introduced to substitute connectiveissue grafting. ADM is harvested from cadaversnd treated to remove all cells but preserve thextracellular matrix including vascular struc-ures.
A short clinical crown is another estheticroblem in orthodontic patients. Altered passiveruption is when a tooth has reached the occlu-al plane and the gingival margin, is at the junc-ion between the cervical and middle thirds ofhe clinical crown or in the coronal third of thelinical crown in the absence of inflammation,ypertrophy, or hyperplasia of the gingiva. Thisay give the appearance of excessive gingival
isplay. Gingival overgrowth, associated withrthodontic therapy and poor plaque control,lso results in the appearance of short clinicalrowns (Fig 5). These conditions are treatedith a flap procedure instead of a gingivectomy.lap surgery is actually less morbid and allowsomplete visualization of any need for osseous
esection. Sometimes altered passive eruption of toft tissue is accompanied by arrested activeruption and the crest of the alveolus is coronalo the CEJ. In such situations simple gingivecto-
ies will fail because they do not attend to anmmutable biological width, a fundamental
echanism of spatial periodontal homeostasis.everal parameters such as zone of keratinizedissue, location of alveolar crest relative to ce-
ento-enamel junction (CEJ), and biologicidth of attachment apparatus are used to de-
ermine surgical treatment modality. Lasers arelso reported to have similar effects as tradi-ional scalpel gingivectomy, without hemostasisomplications, but are not shown superior to theraditional method.49
isualizing and Exposing Impacted Teeth
hen a permanent tooth fails to erupt, a recon-tructive procedure may serve to surgically ex-ose the anatomical crown of the tooth.46,47 Thishould be done without compromising peri-dontal support. Often damage can occur whenanines are erupted through infected mucosa ortainless steel ligatures are used to “lasso” thempacted tooth at its cemento-enamel junction.he primary goal of modern periodontal proce-ures is to expose the crown to place an orth-dontic bracket, while minimizing periodontalefect on adjacent teeth. The best way to protect
igure 5. Altered passive eruption, reversible inflam-atory enlargement, and permanent gingival hyper-
lasia are three modes of gingival enlargement. Theyften coexist and may be impossible to distinguish inhe clinical situation. Professional collaboration is of-en needed to make the fine distinctions necessary forndividual patient care. (Color version of figure isvailable online.)
he erupting tooth is to erupt it within a wide

ztcAam
bctditcdt
ttmplasce
OP
Otp
Fcir
241Salient Periodontal Issues
one of keratinized tissue. The best way to keephe tooth in keratinized tissue is to use an api-ally positioned flap or to use a gingival graft.fter the surgery the rate of eruption may beccelerated and orthodontic adjustments can beade biweekly.Determining the most suitable flap design
efore surgery is very subjective due to the diffi-ulty in determining the exact tooth location inhe alveolus. A conventional two-dimensional ra-iograph with inherent distortion makes locat-
ng the unerupted tooth inaccurate. An innova-ion rapidly gaining popularity in the 21stentury is cone beam CT (CBCT). The three-imensional CBCT scan provides the exact loca-
ion of the unerupted tooth (Fig 6). It provides a
igure 6. Sagittal views using CBCT technology of a pentral area. The image clearly shows lack of contactmage also shows that access through the palate woul
emoval of the deciduous teeth.hree-dimensional image without the distortionhat is present in a panoramic radiograph. This
odern imaging simplifies presurgical flap designlanning and allows for smaller incisions and flaps,
ess anesthetic, a more rapid surgical procedure,nd less postoperative discomfort. Using CBCT forurgical exposure of impacted teeth is particularlyost effective when pretreatment records have alsomployed CBCT imaging.
rthodontic Solutions to Periodontalroblems
rthodontic treatment to correctly positioneeth before placing dental implants or beforeeriodontal reconstruction must be offered, as
t presenting with supernumerary teeth in the upperdamage from part of the supernumerary teeth. Thebably be an efficient approach without the need for
atienand
d pro

i(lorttpdttcatbtitpfpmamsasa
fittoptapm
Fl equi
F(ss
242 Palomo, Palomo, and Bissada
ndicated, to each patient seeking treatmentFig 7). Orthodontic treatment can reduce theikelihood of unnecessary or excessive removalf healthy bone by leveling and aligning teeth toestore alveolar crest topology. Appropriatereatment planning is essential. Orthodonticreatment is needed to achieve and maintaineriodontal health. An example is where aeep dental bite that impinges on periodontalissues may result in trauma to the periodon-ium. Histologically the latter will show ahronic inflammatory infiltrate, ulceration,nd incomplete keratinization. Prevention ofhis type of situation is indicated. In addition,y correcting severe malocclusions, local fac-ors contributing to periodontitis may be elim-nated (Figs 8, 9). For example, plaque reten-ive contact relationships that may lead tolaque induced inflammation, and traumarom interfering occlusal contact, which in theresence of inflammation can lead to attach-ent loss, can be corrected. Orthodontics can
lso utilize equilibration (occlusal adjust-ent) techniques to reshape form where po-
itional changes cannot be corrected or wherenterior esthetics are a function of incisal edgehape, not only malalignment. The functional
igure 7. Male patient (17-year-old), with congenitaower incisors. This is an example of treatment that r
lignment of teeth beyond their static esthetic a
orm is underestimated as a method of direct-ng occlusal forces along the long axis of theooth to improve periodontal architecture ando improve tooth position relative to the alve-lar housing. Changing the location of mal-osed teeth within the alveolus can increase
he width and thickness of keratinized tissuend axial loading strengthens the cribriformlate when primary occlusal trauma reducesobility.
issing permanent upper lateral incisors, and threeres multidisciplinary coordination.
igure 8. Use of a temporary anchorage deviceTAD) is a more modern alternative to orthognathicurgery that could aid in the intrusion of the posterioregment of the maxilla. (Color version of figure is
lly m
vailable online.)

drccoctctatptffpiaoaog
C
Apmccsdssbebvapitoel
243Salient Periodontal Issues
In certain clinical situations, vertical bonyefects may be corrected by orthodonticallyepositioning teeth. Similarly, in restorativeases where, due to the extent of decay, arown impinges on the needed biologic widthf gingival attachment to tooth, and surgicalrown lengthening is not practical, orthodon-ic extrusion of the tooth can be used to re-reate biologic width. Caution in the restora-ion of the tooth is needed in these situations,s crown-to-root ratio ideally should be lesshan 1:1 to try to ensure a good long-termrognosis, even though this is a relative objec-ive. Many teeth with severely shortened rootsunction well when both functional and para-unctional forces are equilibrated to a mutualrotected schema. Similarly, in cases where
mplant therapy is planned, and there is notdequate vertical height of bone, forced orth-dontic extrusion can be a means of attainingdequate alveolar ridge height. However, with-ut an appreciation of microtrauma the lon-
evity of the implant is jeopardized. conclusions
ttaining optimal outcomes in daily clinicalractice may involve bringing the expertise ofore than one dental specialty. This requires
oordination, communication, and sometimesompromise. Modern technology allows easierpecialty interaction. Biology provides the fun-amental basis, while technology provides theeamless vehicle needed in everyday clinicalynergy. The new orthodontist who wishes touild a career that is uniquely compatible withmerging sciences of the new century woulde wise to consult the Web for a plethora ofaluable insights, policies and, even in thebsence of hard unequivocal data, review re-orts that may assist in providing information
nto periodontally sound dentofacial and den-oalveolar orthopedics. The best local sourcef data is an experienced, responsible andnlightened periodontist. In this regard, col-egial humility is no vice and orthodontic over-
igure 9. Use of indirect anchorage from a tempo-ary anchorage device (TAD). (A) TAD with crossead (RMO Inc., Denver, CO) placed as far away asossible from the working area. (B) A wire is bent toassively go through the TAD and touch the tooth toe used as source of absolute anchorage, and (C)he wire in bonded to both tooth and TAD. Thisooth now can be used as a source of absolute an-horage, with horizontal force vectors, more familiaro clinicians, and easier to control and predict.Color version of figure is available online.)
Frhppbttct(
onfidence is no virtue in interdisciplinary en-

dcm
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
244 Palomo, Palomo, and Bissada
eavors. Indeed, token but disingenuousollaboration is the worst because it onlyasks disease and misleads patients.50-52
eferences1. Gomes SC, Varela CC, da Veiga SL, et al: Periodontal
conditions in subjects following orthodontic therapy. Apreliminary study. Eur J Orthodont 29:477-481, 2007
2. Dubey R, Jalili VP, Garg S: Oral hygiene and gingivalstatus in orthodontics patients. J Pierre Fauchard Acad7:43-54, 1993
3. Huser M, Baehni P, Lang R: Effects of orthodontic bandson microbiologic and clinical parameters. Am J OrthodDentofacial Orthop 97:213-218, 1990
4. Skold-Larsson K, Lindberg T, Twetman S, et al: Effect ofa triclosan-containing dental gel on the levels of prosta-glandin I2 and interleukins-1 beta in gingival crevicularfluid from adolescents with fixed orthodontic appli-ances. Acta Odont Scand 61:193-196, 2003
5. Årtun J, Urbye KS: The effect of orthodontic treatmenton periodontal bone support in patients with advancedloss of marginal periodontium. Am J Orthodont Dento-facial Orthop 93:143-148, 1998
6. Årtun J, Spadafora AT, Shapiro PA: A 3-year follow-upstudy of various types of orthodontic canine-to-canineretainers. Eur J Orthodont 19:501-509, 1997
7. Alexander SA: Effects of orthodontic attachments on thegingival health of permanent second molars. Am JOrthod Dentofacial Orthop 100:337-340, 1991
8. Waldrop T: Gummy smiles: The challenge of gingivalexcess: prevalence and guidelines for clinical manage-ment. Sem Orthod 14:260-271, 2008
9. Atack NE, Sandy JR, Addy M: Periodontal and microbio-logical changes associated with the placement of orthodon-tic appliances: a review. J Periodontol 67:78-85, 1996
0. Hamp S-E, Lundström F, Nyman S: Periodontal condi-tions in adolescents subjected to multiband orthodontictreatment with controlled oral hygiene. Eur J Orthodont4:77-86, 1982
1. Loesche WJ, Grossman NS: Periodontal disease as aspecific, albeit chronic, infection: diagnosis and treat-ment. Clin Microbiol Rev 14:727-752, 2001
2. Diedrich P, Rudzki-Janson I, Wehrbein H, et al: Effectsof orthodontic bands on marginal periodontal tissuehuman species. J Orofac Orthop 62:146-156, 2001
3. Ericsson I, Thilander B, Lindhe J, et al: The effects oforthodontic tilting movements on the periodontal tis-sues of infected and non-infected dentitions in dogs.J Clin Periodontol 4:278-293, 1977
4. Hou L-T, Cheing-Meei Liu C-M, Liu B-Y, et al: Interleu-kin-1�, clinical parameters and matched cellular-his-topathologic changes of biopsied gingival tissue fromperiodontitis patients. J Periodontal Res 38:247-254,2003
5. Kornman KS, Crane A, Wang HY, et al: The interleu-kin-1 genotype as a severity factor in adult periodontaldisease. J Clin Periodontol 24:72-77, 1997
6. Greenstein G, Hart TC: Clinical utility of a genetic sus-ceptibility test for severe chronic periodontitis: a critical
evaluation. J Am Dent Assoc 133:452-459, 20027. Ridker PM, Rifai N, Rose L, et al: Comparison of C -reactive protein and low-density lipoprotein cholesterollevels in the prediction of first cardiovascular events.N Eng J Med 347:1557-1565, 2002
8. Noack B, Genco RJ, Trevisan M, et al: Periodontal infec-tions contribute to elevated systemic C-reactive proteinlevel. J Periodontol 72:1221-1227, 2001
9. Mattingly JA, Sauer GJ, Yancey JM, et al: Enhancement ofStreptococcus mutans colonization by direct bonded orth-odontic appliances. J Dent Res 62:1209-1211, 1983
0. Perinetti G, Paolantonio M, Serra E, et al: Site-specificsubgingival colonization by Actinobacillus actinomycetem-comitans in orthodontic patients. Am J Orthodont Dento-facial Orthop 115:423-428, 1999
1. Sallum EE, Nover D, Klein M, et al: Clinical and microbi-ologic changes after removal of orthodontic appliances.Am J Orthod Dentofacial Orthop 126:363-366, 2004
2. Perinetti G, Paolantonio M, Serra E, et al: Longitudinalmonitoring of subgingival colonization by Actinobacillus ac-tinomycetemcomitans, and crevicular alkaline phosphataseand aspartate aminotransferase activities around orthodon-tically treated teeth. J Clin Periodontol 31:60-67, 2004
3. Lang NP, Adler R, Joss A, et al: Absence of bleeding onprobing. An indicator of periodontal stability. J ClinPeriodontol 17:714-721, 1990
4. Lang NP, Joss A, Orsanic T, et al: Bleeding on probing.a predictor for the progression of periodontal disease?J Clin Periodontol 13:590-596, 1986
5. Boyd RL, Baumrind S: Periodontal considerations in theuse of bonds or bands on molars in adolescents andadults. Angle Orthod 62:117-126, 1992
6. Kingman A, Albandar JM: Methodological aspects ofepidemiological studies of periodontal diseases. Peri-odontol 2000 29:11-30, 2002
7. Susin C, Kingman A, Albandar JM: Effect of partialrecording protocols on estimates of prevalence of peri-odontal disease. J Periodontol 76:262-267, 2005
8. Sanders NL: Evidence-bases care in orthodontics andperiodontics: a review of the literature. J Am Dent Assoc130:521-527, 1999
9. Garib DG, Henriques JFC, Guilherme-Janson G, et al:Periodontal effects of rapid maxillary expansion withtooth-tissue-borne and tooth-borne expanders: a com-puted tomography evaluation. Am J Orthod DentofacialOrthop 129:749-758, 2006
0. Zachrisson BU, Alnaes L: Periodontal condition in orth-odontically treated and untreated individuals. I. Loss ofattachment, gingival pocket depth and clinical crownheight. Angle Orthod 43:402-411, 1993
1. Zachrisson BU, Alnaes L: Periodontal condition in orth-odontically treated and untreated individuals. II. Alveo-lar bone loss: radiographic findings. Angle Orthod 44:48-55, 1994
2. Cappelli DP, Ebersole JL, Kornman KS: Early-onset pe-riodontitis in Hispanic-American adolescents associatedwith A. actinomycetemcomitans. Community Dent OralEpidemiol 22:116-121, 1994
3. Johal AS, Lee RT: The periodontal-orthodontic inter-face: a simple solution to a difficult problem. Br J Orth-
odont 25:95-99, 1998
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
245Salient Periodontal Issues
4. Waerhaug J: Eruption of teeth into crowded position,loss of attachment and downgrowth of subgingivalplaque. Am J Orthod 78:453-459, 1980
5. Grant DA, Grant DA, Flynn MJ, et al: Periodontal micro-biota of mobile and non-mobile teeth. J Periodontol66:386-90, 1995
6. Tonetti MS, D’Aiuto F, Nibali L, et al: Treatment ofperiodontitis and endothelial function. N Engl J Med356:911-920, 2007
7. Bruhn G, Netuschil L, Richter St., et al: Effect of toothpaste containing triclosan on dental plaque, gingivitis,and bleeding on probing an investigation in periodon-titis patients over 28 weeks Clin Oral Invest. 6(2):124-127, 2002
8. Drisko C: The use of locally-delivered doxycycline in thetreatment of periodontitis. Clinical results. J Clin Peri-odontol 25:947-952, 1998
9. Garrett S, Johnson L, Drisko CH, et al: Two multicenterstudies evaluating locally delivered doxycycline hyclate,placebo control, oral hygiene, and scaling and root plan-ing in the treatment of periodontitis. J Periodontol 70:490-503, 1999
0. Goodson JM: Pharmacokinetic principles controlling ef-ficacy of oral therapy. J Dent Res 68(Spec Issue):1625-1632, 1989
1. Goodson JM, Cugini MA, Kent RL, et al: Multi-centerevaluation of tetracycline fiber therapy. (II) Clinical re-sponse. J Periodont Res 26:371-379, 1991
2. Wennstrom JL: Mucogingival therapy. Ann Periodontol
1:671-701, 19963. Stetler KJ, Bissada NF: Significance of the width of keratin-ized gingival on the periodontal status of teeth with sub-marginal restorations. J Periodontol 58:696-700, 1987
4. Djeu G, Hayes C, Zawaideh S: Correlation between man-dibular central incisor proclination and gingival reces-sion during fixed appliance therapy. Angle Orthod 72:238-245, 2002
5. Wilcko WM, Wilcko T, Bouquot JE, et al: Rapid orth-odontics with alveolar reshaping: two case reports ofdecrowding. Int J Periodont Rest Dent 21:9-19, 2001
6. Cobb CM: Lasers in periodontics: a review of literature.J Periodontol 77:545-564, 2006
7. Kokich VG, Matthews DP: Surgical and orthodonticmanagement of impacted teeth. Dent Clin North Am37:181-204, 1993
8. The American Academy of Periodontology. Oral recon-structive and corrective considerations in periodontaltherapy (Academy report, informational paper). J Peri-odont 76:1588-1600, 2005
9. Cobb CM. Lasers in Periodontics: a review of literature.J Periodont 77(4):545-564, 2006
0. Kouraki E, Bissada NF, Palomo J, et al: Gingival enlarge-ment and resolution during and after orthodontic treat-ment. NY State Dent J 71:34-37, 2005
1. Coatoan GW, Behrents RG, Bissada NF: The width ofkeratinized gingiva during orthodontic treatment: itssignificance and impact on periodontal status J Peri-odontol 52:307-313, 1981
2. Greenwell H, Bissada NF, Dodge JR: Disease masking: ahazard of nonsurgical periodontal therapy. Periodontal
Insights 5:14-19, 1998