S4 ch14 toxic_responsesofthekidney
24
CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY Rick G. Schnellmann Cell Volume and Ion Homeostasis Cytoskeleton and Cell Polarity Mitochondria Lysosomes Ca 2 Homeostasis Phospholipases Endonucleases Proteinases SPECIFIC NEPHROTOXICANTS Heavy Metals Mercury Cadmium Chemically Induced 2u -Globulin Nephropathy Halogenated Hydrocarbons Chloroform Tetrafluoroethylene Bromobenzene Mycotoxins Therapeutic Agents Acetaminophen Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) Aminoglycosides Amphotericin B Cyclosporine Cisplatin Radiocontrast Agents FUNCTIONAL ANATOMY Renal Vasculature and Glomerulus Proximal Tubule Loop of Henle Distal Tubule and Collecting Duct PATHOPHYSIOLOGIC RESPONSES OF THE KIDNEY Acute Renal Failure Adaptation Following Toxic Insult Chronic Renal Failure SUSCEPTIBILITY OF THE KIDNEY TO TOXIC INJURY Incidence and Severity of Toxic Nephropathy Reasons for the Susceptibility of the Kidney to Toxicity Site-Selective Injury Glomerular Injury Proximal Tubular Injury Loop of Henle/Distal Tubule/Collecting Duct Injury Papillary Injury ASSESSMENT OF RENAL FUNCTION BIOCHEMICAL MECHANISMS/MEDIATORS OF RENAL CELL INJURY Cell Death Mediators of Toxicity Cellular/Subcellular and Molecular Targets The functional integrity of the mammalian kidney is vital to total body homeostasis, as the kidney plays a principal role in the ex- cretion of metabolic wastes and in the regulation of extracellular fluid volume, electrolyte composition, and acid–base balance. In addition, the kidney synthesizes and releases hormones, such as renin and erythropoietin, and metabolizes vitamin D 3 to the active 1,25-dihydroxy vitamin D 3 form. A toxic insult to the kidney there- fore could disrupt any or all of these functions and could have pro- found effects on total-body metabolism. Fortunately, the kidneys are equipped with a variety of detoxification mechanisms and have considerable functional reserve and regenerative capacities. Nonetheless, the nature and severity of the toxic insult may be such that these detoxification and compensatory mechanisms are over- whelmed, and renal failure ensues. The outcome of renal failure can be profound; permanent renal damage may result, requiring chronic dialysis treatment or kidney transplantation. FUNCTIONAL ANATOMY Gross examination of a sagittal section of the kidney reveals three clearly demarcated anatomic areas: the cortex, medulla, and papil- la (Figs. 14-1 and 14-2). The cortex constitutes the major portion of the kidney and receives a disproportionately higher percent- age (90 percent) of blood flow compared to the medulla (~6 to 10 percent) or papilla (1 to 2 percent). Thus, when a blood-borne toxicant is delivered to the kidney, a high percentage of the material will be delivered to the cortex and will have a greater opportunity to influence cortical rather than medullary or papil- lary functions. However, medullary and papillary tissues are ex- posed to higher luminal concentrations of toxicants for prolonged periods of time, a consequence of the more concentrated tubular fluid and the more sluggish flow of blood and filtrate in these regions. 491 Copyrighted Material Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com
-
Upload
yasir-iqbal-chaudhry -
Category
Documents
-
view
47 -
download
1
Transcript of S4 ch14 toxic_responsesofthekidney

CHAPTER 14
TOXIC RESPONSES OF THEKIDNEY
Rick G. Schnellmann
Cell Volume and Ion HomeostasisCytoskeleton and Cell PolarityMitochondriaLysosomesCa2� HomeostasisPhospholipasesEndonucleasesProteinases
SPECIFIC NEPHROTOXICANTS
Heavy MetalsMercuryCadmium
Chemically Induced �2u-Globulin NephropathyHalogenated Hydrocarbons
ChloroformTetrafluoroethyleneBromobenzene
MycotoxinsTherapeutic Agents
AcetaminophenNonsteroidal Anti-Inflammatory Drugs (NSAIDs)AminoglycosidesAmphotericin BCyclosporineCisplatinRadiocontrast Agents
FUNCTIONAL ANATOMY
Renal Vasculature and GlomerulusProximal TubuleLoop of HenleDistal Tubule and Collecting Duct
PATHOPHYSIOLOGIC RESPONSES OF THE KIDNEY
Acute Renal FailureAdaptation Following Toxic InsultChronic Renal Failure
SUSCEPTIBILITY OF THE KIDNEY TO TOXICINJURY
Incidence and Severity of Toxic NephropathyReasons for the Susceptibility of the Kidney to
ToxicitySite-Selective InjuryGlomerular Injury Proximal Tubular InjuryLoop of Henle/Distal Tubule/Collecting Duct InjuryPapillary Injury
ASSESSMENT OF RENAL FUNCTION
BIOCHEMICAL MECHANISMS/MEDIATORS OFRENAL CELL INJURY
Cell DeathMediators of ToxicityCellular/Subcellular and Molecular Targets
The functional integrity of the mammalian kidney is vital to totalbody homeostasis, as the kidney plays a principal role in the ex-cretion of metabolic wastes and in the regulation of extracellularfluid volume, electrolyte composition, and acid–base balance. Inaddition, the kidney synthesizes and releases hormones, such asrenin and erythropoietin, and metabolizes vitamin D3 to the active1,25-dihydroxy vitamin D3 form. A toxic insult to the kidney there-fore could disrupt any or all of these functions and could have pro-found effects on total-body metabolism. Fortunately, the kidneysare equipped with a variety of detoxification mechanisms and haveconsiderable functional reserve and regenerative capacities.Nonetheless, the nature and severity of the toxic insult may be suchthat these detoxification and compensatory mechanisms are over-whelmed, and renal failure ensues. The outcome of renal failurecan be profound; permanent renal damage may result, requiringchronic dialysis treatment or kidney transplantation.
FUNCTIONAL ANATOMY
Gross examination of a sagittal section of the kidney reveals threeclearly demarcated anatomic areas: the cortex, medulla, and papil-la (Figs. 14-1 and 14-2). The cortex constitutes the major portionof the kidney and receives a disproportionately higher percent-age (90 percent) of blood flow compared to the medulla (~6 to 10 percent) or papilla (1 to 2 percent). Thus, when a blood-bornetoxicant is delivered to the kidney, a high percentage of the material will be delivered to the cortex and will have a greater opportunity to influence cortical rather than medullary or papil-lary functions. However, medullary and papillary tissues are ex-posed to higher luminal concentrations of toxicants for prolongedperiods of time, a consequence of the more concentrated tubularfluid and the more sluggish flow of blood and filtrate in these regions.
491
2996R_ch14_491_514 4/12/01 10:22 AM Page 491
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

492 UNIT 4 TARGET ORGAN TOXICITY
The functional unit of the kidney, the nephron, may be con-sidered in three portions: the vascular element, the glomerulus, andthe tubular element.
Renal Vasculature and Glomerulus
The renal artery branches successively into interlobar, arcuate, andinterlobular arteries (Fig. 14-1). The last of these give rise to theafferent arterioles, which supply the glomerulus; blood then leavesthe glomerular capillaries via the efferent arteriole. Both the affer-ent and efferent arterioles, arranged in a series before and after theglomerular capillary tuft, respectively, are ideally situated to con-trol glomerular capillary pressure and glomerular plasma flow rate.Indeed, these arterioles are innervated by the sympathetic nervoussystem and contract in response to nerve stimulation, angiotensinII, vasopressin, endothelin, prostanoids, and cytokines, affectingglomerular pressures and blood flow. The efferent arterioles drain-ing the cortical glomeruli branch into a peritubular capillary net-work, whereas those draining the juxtamedullary glomeruli form acapillary loop, the vasa recta, supplying the medullary structures.These postglomerular capillary loops provide an efficient arrange-ment for delivery of nutrients to the postglomerular tubular struc-tures, delivery of wastes to the tubule for excretion, and return
of reabsorbed electrolytes, nutrients, and water to the systemiccirculation.
The glomerulus is a complex, specialized capillary bed com-posed primarily of endothelial cells that are characterized by an at-tenuated and fenestrated cytoplasm, visceral epithelial cells char-acterized by a cell body (podocyte) from which many trabeculaeand pedicles (foot processes) extend, and a glomerular basementmembrane (GBM), which is a trilamellar structure sandwiched be-tween the endothelial and epithelial cells (Fig.14-3). A portion ofthe blood entering the glomerular capillary network is fractionated
Figure 14-1. Schematic of the human kidney showing the major bloodvessels and the microcirculation and tubular components of eachnephron. [From Guyton AC, Hall JE (eds): Textbook of Medical Physi-ology. Philadelphia: Saunders, 1996, p 318, with permission.]
Figure 14-2. Schematic of short- and long-looped nephrons and the col-lecting system.
A medullary ray is delineated by a dashed line within the cortex. (1) Re-nal corpuscle including Bowman’s capsule and the glomerulus; (2) proxi-mal convoluted tubule; (3) proximal straight tubule; (4) descending thinlimb; (5) thin ascending limb; (6) thick ascending limb; (7) macula densa,located within the final portion of the thick ascending limb; (8) distal con-voluted tubule; (9) connecting tubule; (9*) connecting tubule of the jux-tamedullary nephron, which forms an arcade; (10) cortical collecting duct;(11) outer medullary collecting duct; (12) inner medullary collecting duct.[From Kriz W: Standard nomenclature for structures of the kidney. Am JPhysiol 254:F1–F8, 1988, with permission.]
2996R_ch14_491_514 4/16/01 10:09 AM Page 492
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY 493
into a virtually protein-free and cell-free ultrafiltrate, which passesthrough Bowman’s space and into the tubular portion of thenephron. The formation of such an ultrafiltrate is the net result ofthe Starling forces that determine fluid movement across capillarybeds—that is, the balance between transcapillary hydrostatic pres-sure and colloid oncotic pressure (Maddox and Brenner, 1991). Fil-tration is therefore favored when transcapillary hydrostatic pres-sure exceeds plasma oncotic pressure. An additional determinantof ultrafiltration is the effective hydraulic permeability of theglomerular capillary wall, in other words, the ultrafiltration coef-ficient (Kf), which is determined by the total surface area availablefor filtration and the hydraulic permeability of the capillary wall.Consequently, chemically induced decreases in glomerular filtra-tion rate (GFR) may be related to decreases in transcapillary hy-drostatic pressure and glomerular plasma flow due to increased af-ferent arteriolar resistance or to decreases in the surface areaavailable for filtration, resulting from decreases in the size and/ornumber of endothelial fenestrae or detachment or effacement offoot processes.
Although the glomerular capillary wall permits a high rate offluid filtration (approximately 20 percent of blood entering theglomerulus is filtered), it provides a significant barrier to the trans-glomerular passage of macromolecules. Experiments using a vari-ety of charged and neutral tracers have established that this barrierfunction is based on the ability of the glomerulus to act as a size-selective and charge-selective filter (Brenner et al., 1977). In gen-eral, the filtration of macromolecules is inversely proportional tothe molecular weight of a substance; thus, small molecules, such
as inulin (MW 5500), are freely filtered, while large molecules,such as albumin (MW 56,000 to 70,000), are restricted. Filtrationof anionic molecules tends to be restricted compared to that of neu-tral or cationic molecules of the same size. These permselectiveproperties of the glomerulus appear to be directly related to the physi-cochemical properties of the different cell types within the glomeru-lus (Kanwar et al., 1991). In particular, charge-selective propertiesof the glomerulus appear to be related to the anionic groups of theGBM coupled with the anionic coating of the epithelial and en-dothelial cells (Fig. 14-3). These highly anionic components pro-duce electrostatic repulsion and hinder the circulation of polyan-ionic macromolecules, thereby markedly retarding passage of thesemolecules across the filtration barrier. Toxicants that neutralize orreduce the number of fixed anionic charges on glomerular struc-tural elements therefore will impair the charge- and/or size-selective properties of the glomerulus, resulting in urinary excre-tion of polyanionic and/or high-molecular-weight proteins.
Proximal Tubule
The proximal tubule consists of three discrete segments: the S1
(pars convoluta), S2 (transition between pars convoluta and parsrecta), and S3 (the pars recta) segments (Fig. 14-2). The S1 seg-ment is the initial portion of the proximal convoluted tubule andis characterized by a tall brush border and a well-developed vac-uolar lysosomal system. The basolateral membrane is extensivelyinterdigitated and many long mitochondria fill the basal portion ofthe cell, characteristic of Na�-transporting epithelia. The S2 seg-ment comprises the end of the convoluted segment and the initialportion of the straight segment. These cells possess a shorter brushborder, fewer apical vacuoles and mitochondria, and less basolat-eral interdigitation compared to the S1 cells. The S3 segment com-prises the distal portion of proximal segments and extends to thejunction of the outer and inner stripe of the outer medulla. The S3
cells have a well-developed brush border but fewer and smallerlysosomes and mitochondria than S1 and S2 cells.
The formation of urine is a highly complex and integratedprocess in which the volume and composition of the glomerularfiltrate is progressively altered as fluid passes through each of thedifferent tubular segments. The proximal tubule is the workhorseof the nephron, as it reabsorbs approximately 60 to 80 percent ofsolute and water filtered at the glomerulus. Toxicant-induced in-jury to the proximal tubule therefore will have major consequencesto water and solute balance. Water reabsorption is through a pas-sive iso-osmotic process, driven primarily by Na� reabsorption,mediated by the Na�,K�-ATPase localized in the basolateralplasma membrane. In addition to active Na� reabsorption, the prox-imal tubule reabsorbs other electrolytes, such as K�, HCO3
�, Cl�,PO4
3�, Ca2�, and Mg2�. The proximal tubule contains numeroustransport systems capable of driving concentrative transport ofmany metabolic substrates, including amino acids, glucose, andcitric acid cycle intermediates. The proximal tubule also reabsorbsvirtually all of the filtered low-molecular-weight proteins by spe-cific endocytotic protein reabsorption processes. In addition, smalllinear peptides may be hydrolyzed by peptidases associated withthe proximal tubular brush border. An important excretory func-tion of the proximal tubule is secretion of weak organic anions andcations by specialized transporters that drive concentrative move-ment of these ions from postglomerular blood into proximal tubu-lar cells, followed by secretion into tubular fluid. Toxicant-induced
Figure 14-3. A. Schematic of the ultrastructure of the glomerular cap-illaries. B. Cross section of the glomerular capillary membrane with thecapillary endothelium, basement membrane, and epithelium podocytes.[From Guyton AC, Hall JE, 1996, p 32, with permission.]
2996R_ch14_491_514 4/12/01 10:22 AM Page 493
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

494 UNIT 4 TARGET ORGAN TOXICITY
interruptions in the production of energy for any of these activetransport mechanisms or the function of critical membrane-boundenzymes or transporters can profoundly affect proximal tubular andwhole-kidney function.
The different segments of the proximal tubule exhibit markedbiochemical and physiologic heterogeneity (Goldstein, 1993). Forexample, filtered HCO3
�, low-molecular-weight proteins, aminoacids, and glucose are primarily reabsorbed by the S1 segment.Transport capacities for these substances in the S2 and S3 segmentsare appreciably less; for example, glucose reabsorption in the S2
and S3 segments is about 50 percent and 10 percent of that in theS1 segment, respectively. In contrast, the principal site of organicanion and cation secretion is in the S2 and S1/S2 segments, re-spectively. Oxygen consumption, Na�,K�-ATPase activity, andgluconeogenic capacity are greater in the S1 and S2 segments thanin the S3 segment. Catabolism and apical transport of glutathione(GSH) occurs to a much greater extent in the S3 segment, wherethe brush-border enzyme �-glutamyltranspeptidase (GGT) is pres-ent in greater amounts. Chemically induced injury to distinct prox-imal tubular segments therefore may be related in part to their seg-mental differences in biochemical properties (see “Site-SelectiveInjury,” below).
Loop of Henle
The thin descending and ascending limbs and the thick ascendinglimb of the loop of Henle are critical to the processes involved inurinary concentration (Fig. 14-2). Approximately 25 percent of thefiltered Na� and K� and 20 percent of the filtered water are reab-sorbed by the segments of the loop of Henle. The tubular fluid en-tering the thin descending limb is iso-osmotic to the renal inter-stitium; water is freely permeable and solutes, such as electrolytesand urea, may enter from the interstitium. In contrast, the thin as-cending limb is relatively impermeable to water and urea, and Na�
and Cl� are reabsorbed by passive diffusion. The thick ascendinglimb is impermeable to water, and active transport of Na� and Cl�
is mediated by the Na�/K�-2Cl� cotransport mechanism, with theenergy provided by the Na�,K�-ATPase. The relatively high ratesof Na�,K�-ATPase activity and oxygen demand, coupled with themeager oxygen supply in the medullary thick ascending limb, arebelieved to contribute to the vulnerability of this segment of thenephron to hypoxic injury. The close interdependence betweenmetabolic workload and tubular vulnerability has been demon-strated, revealing that selective damage to the thick ascending limbin the isolated perfused kidney can be blunted by reducing tubularwork and oxygen consumption (via inhibition of the Na�,K�-ATPase with ouabain) or by increasing oxygen supply (via provi-sion of an oxygen carrier, hemoglobin) (Brezis and Epstein, 1993).Conversely, increasing the tubular workload (via the ionophore am-photericin B) exacerbates hypoxic injury to this segment (Breziset al., 1984).
Distal Tubule and Collecting Duct
The macula densa comprises specialized cells located between theend of the thick ascending limb and the early distal tubule, in closeproximity to the afferent arteriole (Fig. 14-2). This anatomicarrangement is ideally suited for a feedback system whereby a stim-ulus received at the macula densa is transmitted to the arteriolesof the same nephron. Under normal physiologic conditions, in-creased solute delivery or concentration at the macula densa trig-
gers a signal resulting in afferent arteriolar constriction leading todecreases in GFR (and hence decreased solute delivery). Thus, in-creases in fluid/solute out of the proximal tubule, due to impairedtubular reabsorption, will activate this feedback system, referred toas tubuloglomerular feedback (TGF) and resulting in decreases inthe filtration rate of the same nephron. This regulatory mechanismis viewed as a powerful volume-conserving mechanism, designedto decrease GFR in order to prevent massive losses of fluid/elec-trolytes due to impaired tubular reabsorption. Humoral mediationof TGF by the renin-angiotensin system has been proposed, andevidence suggests that other substances may be involved. The dis-tal tubular cells contain numerous mitochondria but lack a well-developed brush border and an endocytotic apparatus characteris-tic of the pars convoluta of the proximal tubule. The early distaltubule reabsorbs most of the remaining intraluminal Na�, K�, andCl� but is relatively impermeable to water.
The late distal tubule, cortical collecting tubule, and medullarycollecting duct perform the final regulation and fine tuning of uri-nary volume and composition. The remaining Na� is reabsorbedin conjunction with K� and H� secretion in the late distal tubuleand cortical collecting tubule. The combination of medullary andpapillary hypertonicity generated by countercurrent multiplicationand the action of antidiuretic hormone (vasopressin, ADH) serveto enhance water permeability of the medullary collecting duct.Agents that interfere with ADH synthesis, secretion, or actiontherefore may impair concentrating ability. Additionally, becauseurinary concentrating ability is dependent upon medullary and pap-illary hypertonicity, agents that increase medullary blood flow mayimpair concentrating ability by dissipating the medullary osmoticgradient.
Table 14-1 illustrates the efficiency of the nephrons in the con-servation of electrolytes, substrates, and water and excretion of ni-trogenous wastes (urea).
PATHOPHYSIOLOGIC RESPONSESOF THE KIDNEY
Acute Renal Failure
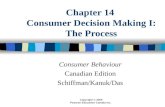
One of the most common manifestations of nephrotoxic damageis acute renal failure (ARF), characterized by an abrupt decline inGFR with resulting azotemia. Any decline in GFR is complex andmay result from prerenal factors (afferent arteriolar constriction,hypovolemia, insufficient cardiac output, obstruction of renalarteries), postrenal factors (ureteral or bladder obstruction), and in-trarenal factors (tubular epithelial cell death/loss, tubular obstruc-tion) resulting in back-leak, glomerular nephritis, and tubulointer-stitial nephritis (Fig. 14-4). Figure 14-5 illustrates the pathwaysthat lead to diminished GFR following chemical exposure. As dis-cussed above, pre- and postrenal factors can lead to decreased GFR.If a chemical causes tubular damage directly, then tubular casts cancause tubular obstruction, increased tubular pressure, and decreasedGFR. The tubular damage may result in epithelial cell death/loss,leading to back-leak of glomerular filtrate and a decrease in GFR.If a chemical causes intrarenal hemodynamic alterations that leadto vasoconstriction, the resulting medullary hypoxia may cause tu-bular damage and/or decreases in perfusion pressure, glomerularhydrostatic pressure, and GFR. Finally, a chemical may disruptglomerular function, resulting in decreased glomerular ultrafiltra-tion and GFR. Table 14-2 provides a partial list of chemicals thatproduce ARF through these different mechanisms. Importantly, in
2996R_ch14_491_514 4/12/01 10:22 AM Page 494
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY 495
most instances ARF is a consequence of tubular damage and/or in-creased renal vascular resistance.
The maintenance of tubular integrity is dependent on cell-to-cell and cell-to-matrix adhesion; these interactions are mediated inpart by integrins and cell adhesion molecules (Fig. 14-6). It hasbeen hypothesized that after a chemical or hypoxic insult, adhe-sion of non–lethally damaged, apoptotic, and oncotic cells to the
basement membrane is compromised, leading to their detachmentfrom the basement membrane and appearance in the tubular lumen(Goligorksy et al., 1993). Morphologically, such an event wouldlead to gaps in the epithelial cell lining, potentially resulting inback-leak of filtrate and diminished GFR. These detached cells mayaggregate in the tubular lumen (cell-to-cell adhesion) and/or ad-here or reattach to adherent epithelial cells downstream, resulting
Table 14-1Filtration, Reabsorption, and Excretion Rates of Different Substances by the Kidneys*
FILTERED, REABSORBED, EXCRETED, REABSORBED,meq/24 h meq/24 h meq/24 h %
Glucose (g/day) 180 180 0 100Bicarbonate (meq/day) 4,320 4,318 2 �99.9Sodium (meq/day) 25,560 25410 150 99.4Chloride (meq/day) 19,440 19260 180 99.1Water (L/day) 169 167.5 1.5 99.1Urea (g/day) 48 24 24 50Creatinine (g/day) 1.8 0 1.8 0
*Glomerular filtration rate: 125 mL/min � 180 L/24h.
Figure 14-4. Mechanisms of reduction of the glomerular filtration rate (GFR).
A. GFR depends on four factors: (1) adequate blood flow to the glomerulus; (2) adequate glomerular capillarypressure; (3) glomerular permeability; and (4) low intratubular pressure. B. Afferent arteriolar constriction de-creases GFR by reducing blood flow, resulting in diminished capillary pressure. C. Obstruction of the tubularlumen by cast formation increases tubular pressure; when tubular pressure exceeds glomerular capillary pres-sure, filtration decreases or ceases. D. Back-leak occurs when the paracellular space between cells increases andthe glomerular filtrate leaks into the extracellular space and bloodstream [From Molitoris BA, Bacallao R: Patho-physiology of ischemic acute renal failure: Cytoskeletal aspects, in Berl T, Bonventre JV (eds): Atlas of Dis-eases of the Kidney. Philadelphia: Current Medicine, 1999, p 13.5, with permission.]
2996R_ch14_491_514 4/12/01 10:22 AM Page 495
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

496 UNIT 4 TARGET ORGAN TOXICITY
in tubular obstruction. Further, the loss of expression of integrinson the basolateral membrane may be responsible for the exfolia-tion of tubular cells, and the redistribution of integrins from thebasolateral to the apical membrane facilitates adhesion of detachedcells to the in situ epithelium.
Other studies have indicated that leukocyte adhesion mole-cules play a critical role in ARF, possibly because of the ability ofactivated leukocytes to release cytokines and reactive oxygenspecies (ROS), resulting in capillary damage/leakage, which maylead to the vascular congestion often observed in ARF. Bonventreand colleagues have demonstrated that treatment of rats with ei-ther monoclonal antibodies against the integrins, CD11a andCD11b, or a monoclonal antibody against ICAM-1 (a ligand forCD11a) conferred significant protection against renal ischemic in-jury (Kelly et al., 1994; Rabb et al., 1994), suggesting a criticalrole for leukocyte–endothelial adhesion in the pathophysiology ofischemic ARF.
Whereas chemically induced ARF can be initiated by proxi-mal tubular cell injury, nephrotoxicants also may inhibit cellularproliferation and migration, thereby delaying renal functional re-covery. For example, Leonard et al. (1994) demonstrated that cis-platin impaired tubular regeneration resulting in prolonged renaldysfunction, effects that were in contrast to the regenerative re-sponse and renal functional recovery following tobramycin-induced nephrotoxicity. Using an in vitro model, Counts et al.(1995) reported that following mechanically induced injury to aproximal tubular monolayer, proliferation and migration were in-hibited by the heavy metal HgCl2, the mycotoxin fumonisin B1,and dichlorovinyl-L-cysteine (DCVC), suggesting that nephrotox-icants may inhibit/delay the regenerative process.
Adaptation Following Toxic Insult
Fortunately, the kidney has a remarkable ability to compensate fora loss in renal functional mass. Micropuncture studies have re-vealed that following unilateral nephrectomy, GFR of the remnant
Renal vasoconstriction Prerenal azotemia
GFR
Increased tubular pressure
“Back-leak” of glomerular filtrateTubular obstruction
Intratubularcasts
Functionalabnormalities
Tubular damage
Exposure
to
nephrotoxicant
Intrarenal factors Persistent medullary hypoxia
Physical constrictionof medullary vessels
Glomerularhydrostatic
pressure
Hemodynamicalterations
Intrarenalvasoconstriction
Glomerular factors
Obstruction Postrenal failure
Glomerular ultrafiltration
Perfusion pressureEfferent toneAfferent tone
Figure 14-5. Mechanisms that contribute to decreased GFR in acute re-nal failure.
After exposure to a nephrotoxicant, one or more mechanisms may con-tribute to a reduction in the GFR. These include renal vasoconstriction re-sulting in prerenal azotemia and obstruction due to precipitation of a drugor endogenous compound within the kidney. Intrarenal factors include di-rect tubular obstruction and dysfunction resulting in tubular back-leak andincreased tubular pressure. Alterations in the levels of a variety of vasoac-tive mediators may result in decreased renal perfusion pressure or efferentarteriolar tone and increased afferent arteriolar tone, leading to in decreasedglomerular hydrostatic pressure. [Schnellmann RG, Kelly KJ: Pathophysi-ology of nephrotoxic acute renal failure, in Berl T, Bonventre JV (eds): At-las of Diseases of the Kidney. Philadelphia: Current Medicine, 1999, p 15.4,with permission.]
Table 14-2Mechanisms of Chemically Induced Acute Renal Failure
PRERENAL VASOCONSTRICTION CRYSTALLURIA
Diuretics Nonsteroidal anti- SulfonamidesInterleukin-2 inflammatory drugs MethotrexateAngiotensin-converting Radiocontrast agents Acyclovir
enzyme inhibitors Cyclosporine TriamtereneAntihypertensive Tacrolimus Ethylene glycol
agents Amphotericin B Protease inhibitors
TUBULAR TOXICITY ENDOTHELIAL INJURY GLOMERULOPATHY INTERSTITIAL NEPHRITIS
Aminoglycosides Cyclosporine Gold MultipleCisplatin Mitomycin C PenicillamineVancomycin Tacrolimus Nonsteroidal anti-Pentamidine Cocaine inflammatory drugsRadiocontrast agents Conjugated estrogensHeavy metals QuinineHaloalkane- and
Haloalkene-cysteineconjugates
2996R_ch14_491_514 4/12/01 10:22 AM Page 496
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY 497
kidney increases by approximately 40 to 60 percent, an effect as-sociated with early compensatory increases in glomerular plasmaflow rate and glomerular hydraulic pressure. Compensatory in-creases in single-nephron GFR are accompanied by proportionateincreases in proximal tubular water and solute reabsorption;glomerulotubular balance is therefore maintained and overall renalfunction appears normal by standard clinical tests. Consequently,chemically induced changes in renal function may not be detecteduntil these compensatory mechanisms are overwhelmed by signif-icant nephron loss and/or damage.
There are a number of cellular and molecular responses to anephrotoxic insult. After a population of renal cells are exposed toa toxicant, a fraction of the cells will be severely injured and un-dergo cell death by apoptosis or oncosis (see below) (Fig. 14-7).Those cells that are nonlethally injured may undergo cell repairand/or adaptation, which contribute to the structural and functional
recovery of the nephron (Fig. 14-8). In addition, there is a popu-lation of cells that are uninjured and may undergo compensatoryhypertrophy, cellular adaptation, and cellular proliferation. At thistime there is little evidence for a stem cell in the kidney; conse-quently, it is thought that renal cells undergo dedifferentiation, pro-liferation, migration, and differentiation. The cellular proliferationand compensatory hypertrophy contribute to the structural andfunctional recovery of the nephron. Growth factors delivered to re-nal epithelial cells from local and systemic sources may help or-chestrate the proliferative response of the nephron. Several growthfactors—such as epidermal growth factor (EGF), insulin-likegrowth factor-1 (IGF-1), hepatocyte growth factor (HGF), fibrob-last growth factors, and transforming growth factors � and � havebeen implicated in proximal tubular regeneration (Hammerman andMiller, 1994). Interestingly, exogenous administration of EGF,HGF, or IGF-1 accelerates renal repair following ischemic-, gen-
Figure 14-6. After injury, alterations can occur in the cytoskeleton and in the normal distribution of mem-brane proteins such as Na�,K�-ATPase and �1 integrins in sublethally injured renal tubular cells.
These changes result in loss of cell polarity, tight junction integrity, and cell-substrate adhesion. Lethally injuredcells undergo oncosis or apoptosis, and both dead and viable cells may be released into the tubular lumen. Ad-hesion of released cells to other released cells and to cells remaining adherent to the basement membrane mayresult in cast formation, tubular obstruction, and further compromise the GFR. [Schnellmann RG, Kelly KJ:Pathophysiology of nephrotoxic acute renal failure, in Berl T, Bonventre JV (eds): Atlas of Diseases of the Kid-ney. Philadelphia: Current Medicine, 1999, p 15.5, with permission.]
2996R_ch14_491_514 4/12/01 10:22 AM Page 497
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

498 UNIT 4 TARGET ORGAN TOXICITY
tamicin-, bromohydroquinone-, and/or HgCl2-induced ARF. How-ever, it is not clear which endogenous growth factors are requiredfor tubular regeneration.
Two of the most notable cellular adaptation responses are met-allothionein induction (see “Cadmium,” below) and stress proteininduction. Heat-shock proteins (Hsps) and glucose-regulated pro-teins (Grps) are two examples of stress protein families that are in-duced in response to a number of pathophysiologic states such asheat shock, anoxia, oxidative stress, toxicants, heavy metal expo-sure, and tissue trauma. The distribution of individual stress pro-teins varies between different cell types in the kidney and withinsubcellular compartments (Goering et al., 2000). These proteinsare believed to play an important housekeeping role in the main-tenance of normal protein structure and/or the degradation of dam-aged proteins and thereby to provide a defense mechanism againsttoxicity and/or for the facilitation of recovery and repair. Hsp in-duction in renal tissue has been demonstrated following renal is-chemia (Van Why et al., 1992; Enami et al., 1991) and treatmentwith nephrotoxicants such as gentamicin (Komatsuda et al., 1993),haloalkane cysteine conjugates (Chen et al., 1992), and HgCl2(Goering et al., 1992). Interestingly, proximal tubular Hsps havebeen identified as molecular targets of the reactive metabolites ofthe haloalkane cysteine conjugate tetrafluoroethyl-L-cysteine(TFEC) (Bruschi et al., 1993), an effect that could alter the nor-mal housekeeping functions of the proximal tubule and thereby po-tentially contribute to and exacerbate TFEC nephrotoxicity. Grp78is an endoplasmic reticulum stress protein, and recent evidenceshows that Grp78 is induced following a cellular stress (Halleck etal., 1997). Prior induction of Grp78 in a renal cell line rendered
cells tolerant to a subsequent TFEC exposure. These findings sug-gest that cellular adaptation is an importance response to renal cellinjury and death.
Chronic Renal Failure
Progressive deterioration of renal function may occur with long-term exposure to a variety of chemicals (e.g., analgesics, lithium,cyclosporine). It is generally believed that progression to end-stagerenal failure is not simply a function of the primary renal insultper se but rather is related to secondary pathophysiologic processestriggered by the initial injury. The progression of chronic renal dis-ease, for example, has been postulated by Brenner and colleagues(1982) to be a consequence of the glomerular hemodynamic re-sponse to renal injury. That is, following nephron loss, there areadaptive increases in glomerular pressures and flows that increasethe single-nephron GFR of remnant viable nephrons. Althoughthese compensatory mechanisms serve to maintain whole-kidneyGFR, evidence has accumulated to suggest that, with time, thesealterations are maladaptive and foster the progression of renal fail-ure. Focal glomerulosclerosis eventually develops and may lead totubular atrophy and interstitial fibrosis. Consequently, glomeru-losclerosis in these nephrons will perpetuate the cycle of trigger-ing further compensatory increases in the hemodynamics of lessdamaged nephrons, contributing, in turn, to their eventual destruc-tion. Although the underlying mechanisms are not precisely known,compensatory increases in glomerular pressures and flows of theremnant glomeruli may result in mechanical damage to the capil-laries due to increased shear stress on the endothelium and dam-age to the glomerular capillary wall, leading to altered permeabil-ities, and mesangial thickening due to increased transcapillary fluxand local deposition of macromolecules (Dunn et al., 1986). Other
Nephrotoxic insultto the nephron
Cellularproliferation
Cellularrepair
Cellularadaptation
Compensatoryhypertrophy
Re-epithelialization Cellular adaptation
Differentiation
Structural and functional recovery of the nephron
Uninjured cells Injured cells Cell death
Figure 14-7. The response of the nephron to a nephrotoxic insult.
After a population of cells is exposed to a nephrotoxicant, the cells respond;ultimately the nephron recovers function or, if cell death and loss are ex-tensive, nephron function ceases. Terminally injured cells undergo celldeath through oncosis or apoptosis. Cells injured sublethally undergo re-pair and adaptation in response to the nephrotoxicant. Cells not injured andadjacent to the injured area may undergo dedifferentiation, proliferation,migration or spreading, and differentiation. Cells not injured may also un-dergo compensatory hypertrophy in response to the cell loss and injury. Fi-nally the uninjured cells also may undergo adaptation in response to anephrotoxicant exposure. [Schnellmann RG, Kelly KJ: Pathophysiology ofnephrotoxic acute renal failure, in Berl T, Bonventre JV (eds): Atlas of Dis-eases of the Kidney. Philadelphia: Current Medicine, 1999, p 15.4, withpermission.]
Figure 14-8. Inhibition and repair of renal proximal tubule cellular func-tions after exposure to the model oxidant t-butylhydroperoxide.
Approximately 25 percent cell loss and marked inhibition of mitochon-drial function, active Na� transport, and Na�-coupled glucose transport occurred 24 h after oxidant exposure. The activity of the brush-border mem-brane enzyme �-glutamyl transferase (GGT) was not affected by oxidantexposure. Cell proliferation and migration or spreading was complete byday 4, whereas active Na� transport and Na�-coupled glucose transportdid not return to control levels until day 6. These data suggest that selec-tive physiologic functions are diminished after oxidant injury and that a hi-erarchy exists in the repair process. [Schnellmann RG, Kelly KJ: Patho-physiology of nephrotoxic acute renal failure, in Berl T, Bonventre JV (eds):Atlas of Diseases of the Kidney. Philadelphia: Current Medicine, 1999, p15.6, with permission.]
2996R_ch14_491_514 4/12/01 10:22 AM Page 498
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY 499
factors likely to play a role in the pathogenesis of chronic renalfailure include growth promoters and inhibitors, increased extra-cellular matrix deposition, ROS, lipid accumulation, and tubuloin-terstitial injury.
SUSCEPTIBILITY OF THE KIDNEYTO TOXIC INJURY
Incidence and Severity ofToxic Nephropathy
A wide variety of drugs, environmental chemicals, and metals cancause nephrotoxicity (Table 14-2). A large 1-year survey of all pa-tients with ARF admitted to nephrology units revealed that in 18percent, ARF was considered to be drug-induced (Kleinknecht etal., 1986; Fluery et al., 1990). Nephrotoxicity is a recognized clin-ical liability of certain classes of drugs; in particular, antibioticsrepresent the major class of nephrotoxic drugs, followed byangiotensin-converting enzyme inhibitors, glafenin (a Europeananalgesic), nonsteroidal anti-inflammatory drugs (NSAIDs), andradiocontrast media. Approximately 70 percent of the patients pre-senting with drug-induced ARF were nonoliguric; the pathologicfindings revealed acute tubular necrosis in 60 percent. Approxi-mately 50 percent recovered completely. A myriad of risk factorsappear to contribute to the incidence/severity of ARF, including ge-netic/hereditary factors, volume depletion, septic shock, hypoten-sion, multiple chemical insults, age, diabetes, and preexisting re-nal disease. The consequences of ARF can be profound, aspermanent renal damage may result and dialysis or renal trans-plantation may be required.
Chronic renal failure leading to end-stage renal failure hasbeen associated with long-term abuse of analgesics. The incidenceof analgesic nephropathy has been reported to be as high as 20 to25 percent in certain countries (e.g., Switzerland). Other agents—such as lithium, cyclosporine, NSAIDs, lead, and cadmium—mayproduce chronic tubulointerstitial nephropathy with progressiveloss of renal function.
Reasons for the Susceptibility of theKidney to Toxicity
The unusual susceptibility of the mammalian kidney to the toxiceffects of noxious chemicals can be attributed in part to the uniquephysiologic and anatomic features of this organ. Although the kid-neys constitute only 0.5 percent of total body mass, they receiveabout 20 to 25 percent of the resting cardiac output. Consequently,any drug or chemical in the systemic circulation will be deliveredto these organs in relatively high amounts. The processes involvedin forming a concentrated urine also serve to concentrate potentialtoxicants in the tubular fluid. As water and electrolytes are reab-sorbed from the glomerular filtrate, chemicals in the tubular fluidmay be concentrated, thereby driving passive diffusion of toxicantsinto tubular cells. Therefore, a nontoxic concentration of a chem-ical in the plasma may reach toxic concentrations in the kidney.Progressive concentration of toxicants along the nephron may re-sult in intraluminal precipitation of relatively insoluble compounds,causing ARF secondary to tubular obstruction. Finally, renal trans-port, accumulation, and metabolism of xenobiotics contribute sig-nificantly to the susceptibility of the kidney (and specific nephronsegments) to toxic injury (see “Site-Selective Injury,” below).
In addition to intrarenal factors, the incidence and/or severityof chemically induced nephrotoxicity may be related to the sensi-tivity of the kidney to circulating vasoactive substances. For ex-ample, nephrotoxicity due to NSAIDs is known to result in ARFif patients are suffering from hypotension, hypovolemia, and/orcardiac insufficiency (Brezis et al., 1991). Under these conditions,vasoconstrictors such as angiotensin II or vasopressin are increased.Normally, the actions of high circulating levels of vasoconstrictorhormones are counterbalanced by the actions of increased va-sodilatory prostaglandins; thus, renal blood flow (RBF) and GFRare maintained. However, when prostaglandin synthesis is sup-pressed by NSAIDs, RBF declines markedly and ARF ensues, dueto the unopposed actions of vasoconstrictors. Another example ofpredisposing risk factors relates to the clinical use of angiotensin-converting enzyme (ACE) inhibitors, such as captopril (De Jongand Woods, 1998). Captopril has been reported to produce ARF inpatients with severe hypertension, due either to bilateral renal ar-tery stenosis or to renal artery stenosis in a solitary kidney. Underthese conditions, glomerular filtration pressure is dependent on an-giotensin II–induced efferent arteriolar constriction. ACE in-hibitors will block this vasoconstriction, resulting in a precipitousdecline in filtration pressure and ARF.
Site-Selective Injury
Many nephrotoxicants have their primary effects on discrete seg-ments or regions of the nephron. For example, the proximal tubuleis the primary target for most nephrotoxic antibiotics, antineo-plastics, halogenated hydrocarbons, mycotoxins, and heavy met-als, whereas the glomerulus is the primary site for immune com-plexes, the loop of Henle/collecting ducts for fluoride ions, and themedulla/papilla for chronically consumed analgesic mixtures. Thereasons underlying this site-selective injury are complex but canbe attributed in part to site-specific differences in blood flow, trans-port and accumulation of chemicals, physicochemical properties ofthe epithelium, reactivity of cellular/molecular targets, balance ofbioactivation/detoxification reactions, cellular energetics, and/orregenerative/repair mechanisms.
Glomerular Injury
The glomerulus is the initial site of chemical exposure within thenephron, and a number of nephrotoxicants produce structural in-jury to this segment. In certain instances, chemicals alter glomeru-lar permeability to proteins by altering the size- and charge-selective functions. Both puromycin aminonucleoside anddoxorubicin target glomerular epithelial cells, resulting in changesin size and charge selectivity and proteinuria. The decrease incharge selectivity is thought to result from a decrease in negativelycharged sites, while the loss of size selectivity is thought to resultfrom focal detachment of podocytes from the glomerular basementmembrane.
Cyclosporine, amphotericin B, and gentamicin are examplesof chemicals that impair glomerular ultrafiltration without signifi-cant loss of structural integrity and decrease GFR. AmphotericinB decreases GFR by causing renal vasoconstriction and decreas-ing the glomerular capillary ultrafiltration coefficient (Kf), an ef-fect probably mediated through the endothelial cells. Because of its polycationic nature, the aminoglycoside gentamicin in-teracts with the anionic sites on the endothelial cells, decreas-ing Kf and GFR. Finally, cyclosporine not only causes renal
2996R_ch14_491_514 4/12/01 10:22 AM Page 499
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

500 UNIT 4 TARGET ORGAN TOXICITY
vasoconstriction and vascular damage but is injurious to theglomerular endothelial cell.
Chemically induced glomerular injury may also be mediatedby extrarenal factors. Circulating immune complexes may betrapped within the glomeruli; binding of complement, attraction ofneutrophils, and phagocytosis may result. Neutrophils andmacrophages are commonly observed within glomeruli in mem-branous glomerulonephritis, and the local release of cytokines andreactive oxygen species (ROS) may contribute to glomerular in-jury. Heavy metals (e.g., HgCl2, gold, cadmium), hydrocarbons,penicillamine, and captopril can produce this type of glomerularinjury. A chemical may function as a hapten attached to some na-tive protein (e.g., tubular antigens released secondary to toxicity)or as a complete antigen—particularly if it is sequestered withinthe glomerulus via electrostatic interactions—and elicit an anti-body response. Antibody reactions with cell-surface antigens (e.g.,GBM) lead to immune deposit formation within the glomeruli, me-diator activation, and subsequent injury to glomerular tissue.Volatile hydrocarbons, solvents, and HgCl2 have been implicatedin this type of glomerulonephritis.
Proximal Tubular Injury
The proximal tubule is the most common site of toxicant-inducedrenal injury. The reasons for this relate in part to the selective ac-cumulation of xenobiotics into this segment of the nephron. Forexample, in contrast to the distal tubule, which is characterized bya relatively tight epithelium with high electrical resistance, theproximal tubule has a leaky epithelium, favoring the flux of com-pounds into proximal tubular cells. More importantly, tubular trans-port of organic anions and cations, low-molecular-weight proteinsand peptides, GSH conjugates, and heavy metals is localized pri-marily if not exclusively to the proximal tubule. Thus, transport ofthese molecules will be greater in the proximal tubule than in othersegments, resulting in proximal tubular accumulation and toxicity.Indeed, segmental differences in transport and accumulation ap-pear to play a significant role in the onset and development of proximal tubular toxicity associated with certain drugs such asaminoglycosides, �-lactam antibiotics, and cisplatin; environ-mental chemicals such as ochratoxin, haloalkene S-conjugates,d-limonene, and 2,4,4-trimethylpentane; and metals such as cad-mium and mercury. Although correlations between proximal tubu-lar transport, accumulation, and toxicity suggest that the site oftransport is a crucial determinant of the site of toxicity, transportis unlikely to be the sole criterion. For example, the S2 segment isthe primary site of transport and toxicity of cephaloridine, and sev-eral lines of evidence suggest a strong correlation between thetransport, accumulation, and nephrotoxicity of this antibiotic. How-ever, when a variety of cephalosporins are considered, the rank or-der of accumulation does not follow the rank order of nephrotox-icity; for example, renal cortical concentrations of the potentnephrotoxicant cephaloglycin are comparable to those of the rela-tively nontoxic cephalexin. These data suggest that site-specifictransport and accumulation are necessary but not sufficient to causeproximal tubular toxicity of cephalosporins. Once taken up and se-questered by the proximal tubular cell, the nephrotoxic potentialof these drugs ultimately may be dependent upon the intrinsic re-activity of the drug with subcellular or molecular targets.
In addition to segmental differences in transport, segmentaldifferences in cytochrome P450 and cysteine conjugate �-lyase ac-tivity also are contributing factors to the enhanced susceptibility of
the proximal tubule. Both enzyme systems are localized almost ex-clusively in the proximal tubule, with negligible activity in theglomerulus, distal tubules, or collecting ducts. Thus, nephrotoxic-ity requiring P450 and �-lyase–mediated bioactivation will mostcertainly be localized in the proximal tubule. Indeed, the site ofproximal tubular bioactivation contributes at least in part to theproximal tubular lesions produced by chloroform (via cytochromeP450) and by haloalkene S-conjugates (via cysteine �-lyase).
Finally, proximal tubular cells appear to be more susceptibleto ischemic injury than are distal tubular cells. Therefore, the prox-imal tubule likely will be the primary site of toxicity for chemi-cals that interfere with renal blood flow, cellular energetics, and/ormitochondrial function.
Loop of Henle/Distal Tubule/CollectingDuct Injury
Chemically-induced injury to the more distal tubular structures,compared to the proximal tubule, is an infrequent occurrence. Func-tional abnormalities at these sites manifest primarily as impairedconcentrating ability and/or acidification defects. Drugs that havebeen associated with acute injury to the more distal tubular struc-tures include amphotericin B, cisplatin, and methoxyflurane. Eachof these drugs induces an ADH-resistant polyuria, suggesting thatthe concentrating defect occurs at the level of the medullary thickascending limb and/or the collecting duct. However, the mecha-nisms mediating these drug-induced concentrating defects appearto be different. Amphotericin B is highly lipophilic and interactswith lipid sterols such as cholesterol, resulting in the formation oftransmembrane channels or pores and disrupting membrane per-meability (Bernardo and Branch, 1997). Thus, amphotericin effec-tively transforms the tight distal tubular epithelium into one that isleaky to water and ions and impairs reabsorption at these sites. Themechanisms mediating cisplatin-induced polyuria are not com-pletely understood, but the first phase is responsive to vasopressinand inhibitors of prostaglandin synthesis (Safirstein and Defray,1998). The second phase is not responsive to vasopressin orprostaglandin synthesis inhibitors but is associated with decreasedpapillary solute content. Methoxyflurane nephrotoxicity is associ-ated with the inhibitory effects of the metabolite fluoride on soluteand water reabsorption (Jarnberg, 1998). Fluoride inhibits sodiumchloride reabsorption in the thick ascending limb and inhibitsADH-mediated reabsorption of water, possibly due to disruptionin adenylate cyclase.
Papillary Injury
The renal papilla is susceptible to the chronic injurious effects ofabusive consumption of analgesics. The intial target is themedullary interstitial cells, followed by degenerative changes inthe medullary capillaries, loops of Henle, and collecting ducts(Bach, 1997). Although the exact mechanisms underlying selectivedamage to the papilla by analgesics are not known, the intrarenalgradient for prostaglandin H synthase activity has been implicatedas a contributing factor. This activity is greatest in the medulla andleast in the cortex, and the prostaglandin hydroperoxidase compo-nent metabolizes phenacetin to reactive intermediates capable ofcovalent binding to cellular macromolecules. Other factors maycontribute to this site-selective injury, including high papillary con-centrations of potential toxicants and inhibition of vasodilatoryprostaglandins, compromising renal blood flow to the renal
2996R_ch14_491_514 4/12/01 10:22 AM Page 500
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY 501
medulla/papilla and resulting in tissue ischemia. The lack of ani-mal models that mimic the papillary injury observed in humanshas limited mechanistic research in this area (Schnellmann, 1998).
ASSESSMENT OF RENALFUNCTION
Evaluation of the effects of a chemical on the kidney can be ac-complished using a variety of both in vivo and in vitro methods.Initially, nephrotoxicity can be assessed by evaluating serum andurine chemistries following treatment with the chemical in ques-tion. The standard battery of noninvasive tests includes measure-ment of urine volume and osmolality, pH, and urinary composition(e.g., electrolytes, glucose, protein). Although specificity is oftenlacking in such an assessment, urinalysis provides a relatively easyand noninvasive assessment of overall renal functional integrity andcan provide some insight into the nature of the nephrotoxic insult.
For example, chemically induced increases in urine volume ac-companied by decreases in osmolality may suggest an impairedconcentrating ability, possibly via a defect in ADH synthesis, re-lease, and/or action. To determine whether the impaired concen-trating ability is due to an altered tubular response to ADH, con-centrating ability can be determined before and after an exogenousADH challenge. Glucosuria may reflect chemically induced de-fects in proximal tubular reabsorption of sugars; however, becauseglucosuria also may be secondary to hyperglycemia, measurementof serum glucose concentrations also must be evaluated. Urinaryexcretion of high-molecular-weight proteins, such as albumin, issuggestive of glomerular damage, whereas excretion of low-molecular-weight proteins, such as �2-microglobulin, suggestsproximal tubular injury (Fig. 14-9). Urinary excretion of enzymeslocalized in the brush border (e.g., alkaline phosphatase, �-glu-tamyl transferase) may reflect brush-border damage, whereas uri-nary excretion of other enzymes (e.g., lactate dehydrogenase) may
Figure 14-9. Mechanism of glomerular and tubular proteinuria.
In the healthy kidney, low-molecular-weight proteins are filtered by the glomerulus and reabsorbed by an en-docytic mechanism to form an endosome (EL), which in turn fuses with lysosomes (L), where proteins are ca-tabolized to their constituent amino acids (aa) (upper left). Following proximal tubular injury, formation and in-ternalization of endocytotic vesicles may be impaired, resulting in decreased reabsorption and increased urinaryexcretion of low-molecular-weight proteins (upper right). In mold, glomerular injury, high-molecular-weightproteins, such as albumin, that traverse the glomerular barrier may be taken up by the proximal tubule (bottomleft); however, with severe glomerular injury, proximal tubular transport of albumin is saturated, resulting in al-buminuria (bottom left). [Goldstein RS, Schnellmann RG: Toxic responses of the kidney, in Klaassen CD (ed):Casarett & Doull’s Toxicology. New York: McGraw-Hill, 1996, with permission.]
2996R_ch14_491_514 4/12/01 10:22 AM Page 501
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

502 UNIT 4 TARGET ORGAN TOXICITY
reflect more generalized cell damage. Enzymuria is often a tran-sient phenomenon, as chemically induced damage may result in anearly loss of most of the enzyme available. Thus, the absence ofenzymuria does not necessarily reflect an absence of damage.
GFR can be measured directly by determining creatinine orinulin clearance. Creatinine is an endogenous compound releasedfrom skeletal muscle at a constant rate under most circumstances.Further, it is completely filtered with limited secretion. Inulin is anexogenous compound that is completely filtered with no reab-sorption or secretion. Following the injection of inulin, inulin serumand urinary concentrations and urine volume are determined overtime. If creatinine is being used, then serum and urinary creatinineconcentrations and urine volume are determined over time. Crea-tinine or inulin clearance is determined by the following formula:
Inulin clearance (mL/min) �
inulin concentration in urine (mg/L) urine volume (mL/min)Inulin concentration in serum (mg/L)
Indirect markers of GFR are serial blood urea nitrogen (BUN)and serum creatinine concentrations. However, both serum creati-nine and BUN are rather insensitive indices of GFR; a 50 to 70percent decrease in GFR must occur before increases in serum cre-atinine and BUN develop (Fig. 14-10). Chemically induced in-creases in BUN and/or serum creatinine may not necessarily re-flect renal damage but rather may be secondary to dehydration,hypovolemia, and/or protein catabolism. These extrarenal eventsshould be taken into consideration in evaluating BUN/serum cre-atinine as potential endpoints of renal toxicity and/or when corre-lating these endpoints with renal histopathology.
Histopathologic evaluation of the kidney following treatmentis crucial in identifying the site, nature, and severity of the nephro-toxic lesion. Assessment of chemically induced nephrotoxicitytherefore should include urinalysis, serum clinical chemistry, andhistopathology to provide a reasonable profile of the functional andmorphologic effects of a chemical on the kidney. Further, infor-
mation on the biotransformation and toxicokinetics of the chemi-cal should be used to direct further in vivo and in vitro studies; inparticular, what metabolites are found in the kidney and what arethe concentrations of parent compound and metabolites in the kid-ney over time.
Once a chemical has been identified as a nephrotoxicant invivo, a variety of in vitro techniques may be used to elucidate un-derlying mechanisms. Tissue obtained from naive animals may beused in the preparation of isolated perfused kidneys, kidney slices,isolated suspensions of renal tubules, cells or subcellular or-ganelles, primary cultures of renal cells, and established renal celllines. For example, freshly prepared isolated perfused kidneys, kid-ney slices, and renal tubular suspensions and cells exhibit thegreatest degree of differentiated functions and similarity to the invivo situation. However, these models have limited lifespans of 2to 24 h. In contrast, primary cultures of renal cells and establishedrenal cell lines exhibit longer life spans (�2 weeks), but—by com-parison to the in vivo condition—exhibit differentiated functionsand similarity to a lesser degree; this is particularly true of im-mortalized renal cell lines. The reader is referred to several excel-lent reviews for further details on the utility and limitations of thesepreparations (Tarloff and Kinter, 1997; Ford, 1997). Such ap-proaches may be used to distinguish between an effect on the kid-ney due to a direct chemical insult and one caused by extrarenaleffects such as extrarenally generated metabolites, hemodynamiceffects, immunologic effects, and so forth. Care must be taken toensure that the cell type affected in the in vitro model is the sameas that affected in vivo. In addition, concentrations of thenephrotoxicant to be used in in vitro preparations must be compa-rable to those observed in vivo, as different mechanisms of toxic-ity may be operative at concentrations that saturate metabolic path-ways or overwhelm detoxification mechanisms. Once a mechanismhas been identified in vitro, the postulated mechanism must betested in vivo. Thus, appropriately designed in vivo and in vitrostudies should provide a complete characterization of the bio-chemical, functional, and morphologic effects of a chemical on thekidney and an understanding of the underlying mechanisms in thetarget cell population(s).
BIOCHEMICALMECHANISMS/MEDIATORS OF
RENAL CELL INJURY
Cell Death
In many cases, renal cell injury may culminate in cell death. Ingeneral, cell death is thought to occur through either oncosis orapoptosis (Levin et al., 1999). The morphologic and biochemicalcharacteristics of necrosis and apoptosis are very different. Apop-tosis is a tightly controlled, organized process that usually affectsscattered individual cells. The organelles retain integrity while cellvolume decreases. Ultimately, the cell breaks into small fragmentsthat are phagocytosed by adjacent cells or macrophages withoutproducing an inflammatory response. In some cases DNA frag-mentation occurs through an endonuclease-mediated cleavage ofthe DNA at internucleosomal linker regions, which can be visual-ized as a ladder-like pattern following agarose gel electrophoresis.In contrast, oncosis often affects many contiguous cells; the or-ganelles swell, cell volume increases, and the cell ruptures withthe release of cellular contents, followed by inflammation. Withmany toxicants, lower but injurious concentrations produce cell
Figure 14-10. Relationships among glomerular filtration rate, serum cre-atinine, and blood urea nitrogen concentrations in the determination ofrenal function.
In general, approximately 50 percent of renal function must be lost beforeserum creatinine or blood urea nitrogen increases. [From Tarloff JB, Kinter LB: In vivo methodologies used to assess renalfunction, in Sipes IG, McQueen CA, Gandolfi AJ (eds): ComprehensiveToxicology. Vol 7. Oxford, England: Elsevier, 1997, pp 99–120, with per-mission.]
2996R_ch14_491_514 4/12/01 10:22 AM Page 502
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY 503
death through apoptosis (Fig. 14-11). As the concentration of thetoxicant increases, oncosis plays a predominant role. However, be-cause apoptosis is an ATP-dependent process, for those toxicantsthat target the mitochondrion, oncosis may be the predominantpathway with only limited apoptosis occurring. In general, whilenephrotoxicants produce cell death through apoptosis and oncosis,it is likely that the degree of oncosis leads to renal failure.
Mediators of Toxicity
A chemical can initiate cell injury by a variety of mechanisms(Fig. 14-12). In some cases the chemical may initiate toxicity dueto its intrinsic reactivity with cellular macromolecules. For exam-ple, amphotericin B reacts with plasma membrane sterols, in-creasing membrane permeability; fumonisin B1 inhibits sphinga-nine (sphingosine) N-acyltransferase; and Hg2� binds to sulfhydrylgroups on cellular proteins. In contrast, some chemicals are nottoxic until they are biotransformed to a reactive intermediate. Bi-ologically reactive intermediates, also known as alkylating agents,are electron-deficient compounds (electrophiles) that bind to cel-lular nucleophiles (electron-rich compounds) such as proteins andlipids. For example, acetaminophen and chloroform are metabo-lized in the mouse kidney by cytochrome P450 to the reactiveintermediates, N-acetyl-p-benzoquinonimine and phosgene, re-spectively (see “Chloroform” and “Acetaminophen,” below). Thecovalent binding of the reactive intermediate to critical cellularmacromolecules is thought to interfere with the normal biologicalactivity of the macromolecule and thereby initiate cellular injury.In other instances, extrarenal biotransformation may be requiredprior to the delivery of the penultimate nephrotoxic species to theproximal tubule, where it is metabolized further to a reactive in-termediate.
Finally, chemicals may initiate injury indirectly by inducingoxidative stress via increased production of ROS, such as super-oxide anion, hydrogen peroxide, and hydroxyl radicals. ROS canreact with a variety of cellular constituents to induce toxicity. For
example, ROS are capable of inducing lipid peroxidation, whichmay result in altered membrane fluidity, enzyme activity, and mem-brane permeability and transport characteristics; inactivating cel-lular enzymes by directly oxidizing critical protein sulfhydryl oramino groups; depolymerizing polysaccharides; and inducing DNAstrand breaks and chromosome breakage. Each of these eventscould lead to cell injury and/or death. Oxidative stress has beenproposed to contribute, at least in part, to the nephrotoxicity asso-ciated with ischemia/reperfusion injury, gentamicin, cyclosporine,cisplatin, and haloalkene cysteine conjugates (Chen et al., 1990;Groves et al., 1991; Ueda et al., 2001).
While nitric oxide is an important second messenger in a num-ber of physiologic pathways, recent studies suggest that in the pres-ence of oxidative stress, nitric oxide can be converted into reactivenitrogen species that contribute to cellular injury and death. Forexample, in the presence of superoxide anion, nitric oxide can betransformed into peroxynitrite (ONOO�), a strong oxidant and ni-trating species (Pryor and Squadrito, 1995). Proteins, lipids, andDNA are all targets of peroxynitrite. The primary evidence for arole of peroxynitrite in renal ischemia/reperfusion injury is theformation of nitrotyrosine-protein adducts and the attenuation ofrenal dysfunction through the inhibition of the inducible form ofnitric oxide synthase (Ueda et al., 2001).
Figure 14-11. The general relationship between oncosis and apoptosisafter nephrotoxicant exposure.
For many toxicants, low concentrations primarily cause apoptosis and on-cosis occurs principally at higher concentrations. When the primary mech-anism of action of the nephrotoxicant is ATP depletion, oncosis may be thepredominant cause of cell death, with limited apoptosis occurring. [Schnell-mann RG, Kelly KJ: Pathophysiology of nephrotoxic acute renal failure,in Berl T, Bonventre JV (eds): Atlas of Diseases of the Kidney. Philadel-phia: Current Medicine, 1999, p 15.6, with permission.]
High-affinity bindingto macromolecules
Toxicant
Biotransformation
Reactive intermediate Redox cycling
Covalent bindingto macromolecules
Increased reactiveoxygen species
Damage to criticalmacromolecules
Oxidative damage tocritical macromolecules
Cell injury
Cell repair Cell death
Altered activity ofcritical macromolecules
Figure 14-12. Covalent and noncovalent binding versus oxidative stressmechanisms of cell injury.
Nephrotoxicants are generally thought to produce cell injury and deaththrough one of two mechanisms, either alone or in combination. In somecases the toxicant may have a high affinity for a specific macromoleculeor class of macromolecules that results in altered activity (increase or de-crease) of these molecules and cell injury. Alternatively, the parent nephro-toxicant may not be toxic until it is biotransformed into a reactive inter-mediate that binds covalently to macromolecules and, in turn, alters theiractivity, resulting in cell injury. Finally, the toxicant may increase reactiveoxygen species in the cells directly, after being biotransformed into a re-active intermediate or through redox cycling. The resulting increase in re-active oxygen species results in oxidative damage and cell injury. [Schnell-mann RG, Kelly KJ: Pathophysiology of nephrotoxic acute renal failure,in Berl T, Bonventre JV (eds): Atlas of Diseases of the Kidney. Philadel-phia: Current Medicine, 1999, p 15.7, with permission.]
2996R_ch14_491_514 4/16/01 10:09 AM Page 503
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

504 UNIT 4 TARGET ORGAN TOXICITY
Cellular/Subcellular andMolecular Targets
A number of cellular targets have been identified to play a role incell death. It is generally thought that an intracellular interaction(e.g., an alkylating agent or ROS with a macromolecule) initiatesa sequence of events that leads to cell death. In the case of onco-sis, a “point of no return” is reached in which the cell will die re-gardless of any intervention. The idea of a single sequence of eventsis probably simplistic for most toxicants, given the extensive num-ber of targets available for alkylating species and ROS. Rather,multiple pathways, with both distinct and common sequences ofevents, may lead to cell death.
Cell Volume and Ion Homeostasis
Cell volume and ion homeostasis are tightly regulated and are crit-ical for the reabsorptive properties of the tubular epithelial cells.Toxicants generally disrupt cell volume and ion homeostasis by in-teracting with the plasma membrane and increasing ion perme-ability or by inhibiting energy production. The loss of ATP, for ex-ample, results in the inhibition of membrane transporters thatmaintain the internal ion balance and drive transmembrane ionmovement. Following ATP depletion, Na�,K�-ATPase activity de-creases, resulting in K� efflux, Na� and Cl� influx, cell swelling,and ultimately cell membrane rupture. Miller and Schnellmann(1993, 1995) have proposed that ATP depletion in rabbit renal prox-imal tubule segments initially results in K� efflux and Na� influxfollowed by a lag period before Cl� influx occurs. Cl� influx oc-curs during the late stages of cell injury produced by a diversegroup of toxicants and does not appear to be due to currently char-acterized renal Cl� transporters. Cl� influx may be a trigger forcell swelling, because decreasing Cl� influx decreased cellswelling and cell death, and inhibition of cell swelling decreasedcell lysis but not Cl� influx. Meng and Reeves (2000) have re-ported similar findings using hydrogen peroxide as the toxicant andLLC-PK1 cells.
Cytoskeleton and Cell Polarity
Toxicants may cause early changes in membrane integrity such asloss of the brush border, blebbing of the plasma membrane, or al-terations in membrane polarity. These changes can result fromtoxicant-induced alterations in cytoskeleton components andcytoskeletal–membrane interactions, or they may be associatedwith perturbations in energy metabolism or calcium and phospho-lipid homeostasis. Marked changes in the polarity of tubular ep-ithelium occur following an ischemic insult. Under control condi-tions, the tubular epithelial cell is polarized with respect to certaintransporters and enzymes. During in vivo ischemia and in vitroATP depletion there is a dissociation of Na�,K�-ATPase from theactin cytoskeleton and redistribution from the basolateral mem-brane to the apical domain in renal proximal tubule cells (Moli-toris, 1997). The redistribution of this enzyme has been postulatedto explain decreased Na� and water reabsorption during ischemicinjury.
Mitochondria
Many cellular processes depend on mitochondrial ATP and thusbecome compromised simultaneously with inhibition of respira-
tion. Conversely, mitochondrial dysfunction may be a consequenceof some other cellular process altered by the toxicant. Numerousnephrotoxicants cause mitochondrial dysfunction (Schnellman andGriner, 1994). For example, following an in vivo exposure, HgCl2altered isolated renal cortical mitochondrial function and mito-chondrial morphology prior to the appearance of tubular necrosis(Weinberg et al., 1982a). Furthermore, HgCl2 produced similarchanges in various respiratory parameters when added to isolatedrat renal cortical mitochondria (Weinberg et al., 1982b). Differenttoxicants also produce different types of mitochondrial dysfunc-tion. For example, pentachlorobutadienyl-L-cysteine initially un-couples oxidative phosphorylation in renal proximal tubular cellsby dissipating the proton gradient, while TFEC does not uncoupleoxidative phosphorylation but rather inhibits state 3 respira-tion by inhibiting sites I and II of the electron transport chain(Schnellmann et al., 1987, 1989; Wallin et al., 1987; Hayden andStevens, 1990).
Whether toxicants target mitochondria directly or indirectly,it is clear that mitochondria play a critical role in determiningwhether cells die by apoptosis or oncosis. The mitochondrial per-meability transition (MPT) is characterized by the opening of ahigh-conductance pore that allows solutes of 1500 molecularweight to pass (Lemasters, 1999). It is thought that the MPT oc-curs during cell injury and ultimately progresses to apoptosis ifsufficient ATP is available or oncosis if ATP is depleted. Further,the release of cytochrome c following the MPT plays a key role inactivating downstream caspases and executing apoptosis.
Lysosomes
Lysosomes are key subcellular targets of aminoglycosides, un-leaded gasoline, and d-limonene and are believed to induce cellu-lar injury via rupture and release of lysosomal enzymes and toxi-cants into the cytoplasm following excessive accumulation ofreabsorbed toxicant(s) and lysosomal overload. �2u-Globulin isnormally reabsorbed in the proximal tubule and degraded in thelysosomes. �2u-Nephropathy occurs in male rats when compoundssuch as d-limonene and constituents of unleaded gasoline bind to�2u-globulin, inhibiting normal lysosomal degradation and result-ing in the accumulation of �2u-globulin in the proximal tubule. Thesize and number of lysosomes increase and a characteristic protein-droplet morphology is observed. Ultimately, this leads to single-cell necrosis and regenerative hyperplasia.
The aminoglycosides also induce lysosomal dysfunction fol-lowing tubular reabsorption of aminoglycosides and accumulationin lysosomes (Fig. 14-13). The size and number of lysosomes in-crease and electron-dense lamellar structures called myeloid bod-ies appear. The myeloid bodies contain undegraded phospholipidsand are thought to occur through the inhibition of lysosomal hy-drolases and phospholipases by the aminoglycosides.
Ca2� Homeostasis
Ca2� is a second messenger and plays a critical role in a varietyof cellular functions. The distribution of Ca2� within renal cells iscomplex and involves binding to anionic sites on macromoleculesand compartmentation within subcellular organelles. The criticalcellular Ca2� pool for regulation is the free Ca2� present in thecytosol. The concentration of this pool is approximately 100 nMand is maintained at this level against a large extracellular/intra-cellular gradient (10,000:1) by a series of pumps and channels lo-
2996R_ch14_491_514 4/12/01 10:22 AM Page 504
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY 505
cated on the plasma membrane and endoplasmic reticulum (ER).Because the proximal tubular cells reabsorb approximately 50 to60 percent of the filtered load of Ca2�, they must maintain low cy-tosolic Ca2� concentrations during a large Ca2� flux.
Sustained elevations or abnormally large increases in cytoso-lic free Ca2� can exert a number of detrimental effects on the cell.For example, an increase in cytosolic free Ca2� can activate a num-ber of degradative Ca2�-dependent enzymes, such as phospholi-pases and proteinases, and can produce aberrations in the structureand function of cytoskeletal elements. While the precise role ofCa2� in toxicant-induced injury remains unclear, release of ERCa2� stores may be a key step in initiating the injury process andincreasing cytosolic free Ca2� concentrations. For example, priordepletion of ER Ca2� stores protects renal proximal tubules fromextracellular Ca2� influx and cell death produced by mitochondr-ial inhibition and hypoxia (Waters et al., 1997b). Mitochondria areknown to accumulate Ca2� in lethally injured cells through a low-affinity, high-capacity Ca2� transport system. While this systemplays a minor role in normal cellular Ca2� regulation, under inju-rious conditions the uptake of Ca2� may facilitate ROS formationand damage.
Phospholipases
Phospholipase A2 (PLA2) consists of a family of enzymes that hy-drolyze the acyl bond at the sn-2 position of phospholipids, re-sulting in the release of arachidonic acid and lysophospholipid. Theenzymes within this family have different biochemical character-istics, substrate preferences, and Ca2� dependencies. PLA2 acti-vation has been suggested to play a role in various forms of cellinjury through a variety of mechanisms (Cummings et al., 2000a).A supraphysiologic increase in PLA2 activity could result in theloss of membrane phospholipids and consequently impair mem-brane function. The increase in PLA2 activity may be secondaryto an increase in cytosolic Ca2�, because some PLA2 enzymestranslocate to membranes following increases in cytosolic freeCa2�. Cell membranes are rich with polyunsaturated fatty acids
and as such are susceptible to lipid peroxidation. Peroxidized lipidsare predisposed to degradation by PLA2, resulting in increasedPLA2 activity and the formation of peroxidized arachidonic acidmetabolites and lysophospholipids. Lysophospholipids can be toxicto cells and alter membrane permeability characteristics and un-couple mitochondrial respiration. Furthermore, the eicosanoidproducts of arachidonic metabolism are chemotactic for neu-trophils, which also may contribute to tissue injury.
The actual role of PLA2 in renal cell injury has been contro-versial, as it is unclear whether changes in PLA2 are a cause orconsequence of cell injury or death (Cummings et al., 2000a). Fur-ther difficulties arise because inhibitors of PLA2 are not very se-lective. However, Sapirstein et al. (1996) showed that cytosolicCa2�-dependent PLA2 (cPLA2) contributed to oxidant-induced on-cosis by overexpressing cPLA2 or secretory PLA2 in LLC-PK1 cellsand demonstrating that cells overexpressing cPLA2 were more sus-ceptible to H2O2 toxicity, whereas overexpression of sPLA2 didnot increase H2O2 toxicity. In contrast, Cummings et al. (2000b)demonstrated that inhibition of Ca2�-independent PLA2 (iPLA2)potentiates t-butylhydroperoxide-induced oncosis in rabbit renalproximal tubular cells. Thus, the role of PLA2s in oncosis dependsupon the PLA2 isoform and stimulus of injury. While the role ofPLA2s in renal cell apoptosis has received minimal attention, it hasbeen reported that inhibition of iPLA2 decreases cisplatin-inducedproximal tubular cell apoptosis (Cummings et al., 2000c).
Endonucleases
Endonucleases have been suggested to play a role in renal cell on-cosis and apoptosis. Endonuclease activation with the associatedDNA cleavage producing a “ladder” pattern following gel ele-crophoresis is a well-characterized response of apoptosis. In thiscase, the observed DNA cleavage is a very late event in the apop-totic process. Ueda et al. (1995) reported DNA damage and the ac-tivation of an endonuclease in rat renal proximal tubules undergo-ing oncosis following hypoxia/reoxygenation. In contrast, DNAcleavage producing a “ladder” pattern was not observed following
Figure 14-13. Renal handling of aminoglycosides: (1) glomerular filtration, (2) binding to the brush-bordermembranes of the proximal tubul, (3) pinocytosis, and (4) storage in the lysosomes. [From De Broe ME: Re-nal injury due to environmental toxins, drugs, and contrast agents, in Berl T, Bonventre JV (eds): Atlas ofDiseases of the Kidney. Philadelphia: Current Medicine, 1999, p 11.4, with permission.]
2996R_ch14_491_514 4/12/01 10:22 AM Page 505
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

506 UNIT 4 TARGET ORGAN TOXICITY
in vitro exposure of rabbit proximal tubules to mitochondrial in-hibitors, the oxidant t-butylhydroperoxide, or the calciumionophore ionomycin (Schnellmann et al., 1993). These studiessuggest that endonuclease activation may occur during apoptosisand oncosis, but that endonuclease activation does not uniformlyoccur following renal cell injury.
Proteinases
Supraphysiologic activation of proteinases could disrupt normalmembrane and cytoskeleton function and lead to cell death. Onesource of proteinases is the lysosomes, where proteins are normallydegraded by acid hydrolases. Under conditions of cell injury, thelysosomal membrane could rupture, releasing hydrolases into thecytosol to degrade susceptible proteins. However, several studiessuggest that proximal tubular cell death does not necessarily in-volve lysosomal rupture (Weinberg, 1993). For example, a varietyof cysteine and serine proteinase inhibitors were ineffective in protecting rabbit renal proximal tubules from antimycin A,tetrafluoroethyl-L-cysteine, bromohydroquinone, and t-butylhy-droperoxide (Schnellmann and Williams, 1998). Only E64 demon-strated any cytoprotective properties following exposure to an-timycin A and TFEC, and the cytoprotection was not associatedwith the inhibition of lysosomal cysteine proteinases. These resultssuggest that nonlysosomal cysteine proteinases play an importantrole in cell death.
The calpains, calcium-activated neutral proteinases, are likelycandidates for a role in cell death because they are cysteine pro-teinases; they are activated by calcium; and they have cytoskeletalproteins, membrane proteins, and enzymes as substrates. For ex-ample, calpain activity increased in rat proximal tubules subjectedto hypoxia, and calpain inhibitors were cytoprotective (Edelsteinet al., 1996). Further, Schnellmann and coworkers (Waters et al.,1997a) showed that calpain inhibitors with different mechanismsof action decreased cell death produced by a variety of toxicants,suggesting that calpains may play an important role in the cell deathproduced by a diverse range of toxicants. The mechanisms and tar-gets of calpains in cell injury remain to be determined.
Caspases are another class of cysteine proteinases that play arole in renal cell death. A number of caspases have been identifiedin the rat kidney (e.g. caspases 1, 2, 3, and 6), and rat kidneys sub-jected to ischemia/reperfusion injury exhibit differential expressionof caspases with marked increases in caspases 1 and 3 (Kaushal etal., 1998). Treatment of LLC-PK1 cells with cisplatin resulted incaspase 3 activation and apoptosis (Zhan et al., 1999). While thecaspase cascade is clearly integral in the initiation and executionof apoptosis, the role of different caspases in chemically inducedrenal injury requires additional experimentation.
SPECIFIC NEPHROTOXICANTS
Heavy Metals
Many metals—including cadmium, chromium, lead, mercury, plat-inum, and uranium—are nephrotoxic. It is important to recognizethat the nature and severity of metal nephrotoxicity varies with re-spect to its form. For example, salts of inorganic mercury producea greater degree of renal injury and a lesser degree of neurotoxic-ity than do organic mercury compounds, an effect that has beenassociated with the greater degree of lipophilicity of organic mer-cury compounds (Conner and Fowler, 1993; Zalups and Lash,
1994). In addition, different metals have different primary targetswithin the kidney. For example, potassium dichromate primarilyaffects the S1 and S2 segments of the proximal tubule, while mer-curic chloride affects the S2 and S3 segments (Zalups and Lash,1994).
Metals may cause toxicity through their ability to bind tosulfhydryl groups. For example, the affinity of mercury forsulfhydryl groups is very high and is about ten orders of magni-tude higher than the affinity of mercury for carbonyl or aminogroups (Ballatori, 1991). Thus, metals may cause renal cellular injury through their ability to bind to sulfhydryl groups of criti-cal proteins within the cells and thereby inhibit their normal function.
Mercury Humans and animals are exposed to elemental mercuryvapor, inorganic mercurous and mercuric salts, and organic mer-curic compounds through the environment. Administered elemen-tal mercury is rapidly oxidized in erythrocytes or tissues to inor-ganic mercury, and thus the tissue distribution of elemental andinorganic mercury is similar. Due to its high affinity for sulfhy-dryl groups, virtually all of the Hg2� found in blood is bound tocells, albumin, other sulfhydryl containing proteins, glutathione,and cysteine.
The kidneys are the primary target organs for accumulationof Hg2�, and the S3 segment of the proximal tubule is the initialsite of toxicity. As the dose or duration of treatment increases, theS1 and S2 segments may be affected. Renal uptake of Hg2� is veryrapid with as much as 50 percent of a nontoxic dose of Hg2� foundin the kidneys within a few hours of exposure. Considering the factthat virtually all of the Hg2� found in blood is bound to an endogenous ligand, it is likely that the luminal and/or basolater-al transport of Hg2� into the proximal tubular epithelial cell is through cotransport of Hg2� with an endogenous ligand such as glutathione, cysteine, or albumin, or through some plasma membrane Hg2�-ligand complex. Current evidence indicates thatat least two mechanisms are involved in the proximal tubular uptake of Hg2� (Fig. 14-14) (Zalups, 1997). One mechanism ap-pears to involve the apical activity of �-glutamyltranspeptidase (�-GT) and a neutral amino acid transporter. Basolateral membranetransport is likely to be mediated by the organic anion transportsystem.
The acute nephrotoxicity induced by HgCl2 is characterizedby proximal tubular necrosis and ARF within 24 to 48 h after ad-ministration (Zalups, 1997). Early markers of HgCl2-induced re-nal dysfunction include an increase in the urinary excretion ofbrush-border enzymes such as alkaline phosphatase and �-GT, sug-gesting that the brush border may be an initial target of HgCl2.Subsequently, when tubular injury becomes severe, intracellular en-zymes such as lactate dehydrogenase and aspartate aminotrans-ferase increase in the urine. As injury progresses, tubular reab-sorption of solutes and water decreases and there is an increase inthe urinary excretion of glucose, amino acids, albumin, and otherproteins. Associated with the increase in injured proximal tubulesis a decrease and progressive decline in the GFR. For example,GFR was reduced 35 percent in rats within 6 h of HgCl2 adminis-tration and continued to decline to 32 percent and 16 percent ofcontrols at 12 and 24 h, respectively (Eknoyan et al., 1982). Thereduction in GFR results from the glomerular injury, tubular in-jury, and/or vasoconstriction. Interestingly, there is an early de-crease in RBF secondary to the vasoconstriction. RBF may returnto normal within 24 to 48 h, while GFR continues to decline. If
2996R_ch14_491_514 4/12/01 10:22 AM Page 506
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY 507
the decline in renal function is not too severe, the remaining prox-imal tubular cells undergo a proliferative response and renal func-tion returns over time.
As stated above, inorganic mercury has a very high affinityfor protein sulfhydryl groups, and this interaction is thought to playan important role in the toxicity of mercury at the cellular level.Changes in mitochondrial morphology and function are very earlyevents following HgCl2 administration, supporting the hypothesisthat mitochondrial dysfunction is an early and important contrib-utor to inorganic mercury–induced cell death along the proximaltubule. Other studies have suggested that oxidative stress plays animportant role in HgCl2-induced renal injury. For example, Fuk-ino and colleagues (1984) observed increased thiobarbituricacid–reactive substances, a marker of lipid peroxidation, in renalcortical homogenates following HgCl2 administration, suggestingthat oxidative stress did occur. Recent studies by Lund and cowork-ers (1993) showed that mitochondria isolated from rats treated withHgCl2 exhibited elevated hydrogen peroxide formation and thuswere a possible source of ROS. Finally, HgCl2 increases intracel-lular free calcium in primary cultures of rabbit renal tubular cells(Smith et al., 1987) and may activate a variety of degradative path-ways that contribute to proximal tubular injury.
Several animal studies have shown that chronic exposure toinorganic mercury results in an immunologically mediated mem-branous glomerular nephritis secondary to the production of anti-bodies against the glomerular basement membrane and the depo-sition of immune complexes (Zalups, 1997).
Cadmium Chronic exposure of nonsmoking humans and animalsto cadmium is primarily through food and results in nephrotoxic-ity (Kido and Nordberg, 1998). In the workplace, inhalation of cad-mium-containing dust and fumes is the major route of exposure.Cadmium has a half-life of greater than 10 years in humans andthus accumulates in the body over time. Approximately 50 percentof the body burden of cadmium can be found in the kidney. Cad-mium produces proximal tubule dysfunction (S1 and S2 segments)and injury characterized by increases in urinary excretion of glu-cose, amino acids, calcium, and cellular enzymes. This injury mayprogress to a chronic interstitial nephritis.
Numerous studies have tried to identify markers to predict thenephrotoxic effects of cadmium in humans. These include but arenot limited to urinary cadmium, calcium, amino acids, albumin,�2-microglobulin, N-acetyl-�-D-glucosaminidase, and retinol-binding protein concentrations. Lauwerys and coworkers (1994)have suggested that cadmium concentrations in the urine greaterthan 5 and 2 nmol/mmol creatinine for adult male workers and thegeneral population, respectively, are associated with tubulardysfunction.
A very interesting aspect of cadmium nephrotoxicity is therole metallothioneins (Klaassen et al., 1999). Metallothioneins area family of low-molecular-weight, cysteine-rich metal-binding pro-teins that have a high affinity for cadmium and other heavy met-als. In general, the mechanism by which metallothionein is thoughtto play a role in cadmium and heavy metal toxicity is through itsability to bind to a heavy metal and thereby render it biologicallyinactive. This assumes that the unbound or “free” concentration ofthe metal is the toxic species. Metallothionein production can beinduced by low, nontoxic concentrations of metals. Subsequently,animals challenged with a higher dose of the metal will not exhibittoxicity compared to naive animals.
Following an oral exposure to CdCl2, Cd2� is thought to reachthe kidneys both as Cd2� and as a Cd2�-metallothionein complexformed and released either from intestinal cells or hepatocytes. TheCd2�-metallothionein complex is freely filtered by the glomerulusand is reabsorbed by the proximal tubule. Inside the tubular cellsit is thought that lysosomal degradation of the Cd2�-metallo-thionein results in the release of “free” Cd2�, which, in turn, in-duces renal metallothionein production. Once the renal metalloth-ionein pool is saturated, “free” Cd2� initiates injury. Themechanism by which Cd2� produces injury at the cellular level isnot clear; however, low concentrations of Cd2� have been shownto interfere with the normal function of several cellular signal trans-duction pathways, including inositol triphosphate, cytosolic freeCa2�, and protein kinase C (Beyersmann et al., 1994; Smith et al.,1989).
Chemically Induced �2u-GlobulinNephropathy
A diverse group of chemicals—including unleaded gasoline,d-limonene, 1,4-dichlorobenzene, tetrachloroethylene, decalin, andlindane—cause �2u-globulin nephropathy or hyaline dropletnephropathy (Lehman-McKeeman, 1997). This nephropathy oc-curs in male rats, is characterized by the accumulation of proteindroplets in the S2 segment of the proximal tubule, and results insingle-cell necrosis, the formation of granular casts at the junctionof the proximal tubule and the thin loop of Henle, and cellular re-generation. Chronic exposure to these compounds results in pro-
Figure 14-14. Cellular transport of Hg2�.
Proximal tubular uptake of inorganic mercury is thought to be the result ofthe transport of Hg2� conjugates [e.g., diglutathione-Hg2� conjugate(GSH-Hg-GSH), dicysteine-Hg2� conjugate (CYS-HG-CYS)]. At the lu-minal membrane, GSH-Hg-GSH is metabolized by �-GT and a dipeptidaseto form CYS-HG-CYS. CYS-HG-CYS may be taken up by an amino acidtransporter. At the basolateral membrane, Hg2�-conjugates appear to betransported by the organic anion transporter. Uptake of Hg2�-protein con-jugates by endocytosis may play a minor role in the uptake of Hg2�. (Cour-tesy of Dr. R.K. Zalups.) [Schnellmann RG, Kelly KJ: Pathophysiology ofnephrotoxic acute renal failure, in Berl T, Bonventre JV (eds): Atlas of Dis-eases of the Kidney. Philadelphia: Current Medicine, 1999, p 15.7, withpermission.]
2996R_ch14_491_514 4/16/01 10:09 AM Page 507
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

508 UNIT 4 TARGET ORGAN TOXICITY
gression of these lesions and ultimately in chronic nephropathy.With compounds such as unleaded gasoline, chronic exposure re-sults in an increased incidence of renal adenomas/carcinomas bynongenotoxic mechanisms.
As the name implies, the expression of this nephropathy re-quires the presence of the �2u-globulin protein. �2u-Globulin issynthesized in the liver of male rats and is under androgen con-trol. Due to its low molecular weight (18.7 kDa), �2u-globulin isfreely filtered by the glomerulus with approximately half beingreabsorbed via endocytosis in the S2 segment of the proximaltubule. Many of the compounds that cause �2u-globulin nephropa-thy bind to �2u-globulin in a reversible manner and decrease theability of lysosomal proteases in the proximal tubule to breakdown�2u-globulin (see above). This results in the accumulation of �2u-globulin in the proximal tubule with an increase in the size andnumber of lysosomes and the characteristic protein-droplet mor-phology. A proposed mechanism of �2u-globulin nephropathy isthat cellular necrosis secondary to lysosomal overload leads to asustained increase in cell proliferation, which, in turn, results inthe promotion of spontaneously or chemically initiated cells toform preneoplastic and neoplastic foci (Lehman-McKeeman,1997; Melnick, 1992).
�2u-Globulin nephropathy appears to be sex- and species-specific. That is, it occurs in male rats but not female rats and inmale or female mice, rabbits, or guinea pigs because they do notproduce �2u-globulin (Lehman-McKeeman, 1997). Furthermore, itdoes not occur in male Black Reiter rats that lack �2u-globulin.Considering the diversity of compounds that cause �2u-globulinnephropathy and renal tumors and the fact that humans are exposedto these compounds regularly, the question arises whether humansare at risk for �2u-globulin nephropathy and renal tumors when ex-posed to these compounds. Current data suggest that humans arenot at risk because (1) humans do not synthesize �2u-globulin, (2)humans secrete less proteins in general and in particular less low-molecular-weight proteins in urine than the rat; (3) the low-molecular-weight proteins in human urine are either not relatedstructurally to �2u-globulin, do not bind to compounds that bind to�2u-globulin, or are similar to proteins in female rats, male BlackReiter rats, rabbits, or guinea pigs that do not exhibit �2u-globulinnephropathy; and (4) mice excrete a low-molecular-weight urinaryprotein that is 90 percent homologous to �2u-globulin, but they donot exhibit �2u-globulin-nephropathy and renal tumors followingexposure to �2u-globulin-nephropathy–inducing agents.
Halogenated Hydrocarbons
Halogenated hydrocarbons are a diverse class of compounds andare used extensively as chemical intermediates, solvents, and pes-ticides. Consequently, humans are exposed to these compounds notonly in the workplace but also through the environment. Numer-ous toxic effects have been associated with acute and chronicexposure to halogenated hydrocarbons, including nephrotoxicity(Elfarra, 1997). The three examples provided below illustrate theimportance of biotransformation in the nephrotoxicity of halo-genated hydrocarbons.
Chloroform Chloroform produces nephrotoxicity in a variety ofspecies, with some species being more sensitive than others. Theprimary cellular target is the proximal tubule, with no primary dam-age to the glomerulus or the distal tubule. Proteinuria, glucosuria,and increased blood urea nitrogen levels are all characteristic of
chloroform-induced nephrotoxicity. The nephrotoxicity producedby chloroform is linked to its metabolism by renal cytochromeP450 and the formation of a reactive intermediate that binds co-valently to nucleophilic groups on cellular macromolecules. Cy-tochrome P450 biotransforms chloroform to trichloromethanol,which is unstable and releases HCl to form phosgene. Phosgenecan react with (1) water to produce 2 HCl + CO2, (2) two mole-cules of glutathione to produce diglutathionyl dithiocarbonate, (3)cysteine to produce 2-oxothizolidine-4-carboxylic acid, or (4) cel-lular macromolecules to initiate toxicity. The sex differences ob-served in chloroform nephrotoxicity appear to be related to differ-ences in renal cytochrome P450 isozyme contents. For example,castration of male mice decreased renal cytochrome P450 and chlo-roform-induced nephrotoxicity (Smith et al., 1984). Likewise,testosterone pretreatment of female mice increased cytochromeP450 content and rendered female mice susceptible to the nephro-toxic effects of chloroform. Cytochrome P450 isozyme 2E1 is pres-ent in male mice and expressed in female mice treated with testos-terone (Lock and Reed, 1997). Thus, these isozymes may play arole in chloroform-induced nephrotoxicity.
Tetrafluoroethylene Tetrafluoroethylene is metabolized in theliver by GSH-S-transferases to S-(1,1,2,2-tetrafluoroethyl)-glutathione. The GSH conjugate is secreted into the bile and smallintestine where it is degraded to the cysteine S-conjugate (TFEC),reabsorbed, and transported to the kidney. The mercapturic acidmay also be formed in the small intestine and reabsorbed. Alter-natively, the glutathione conjugate can be transported to the kid-ney and biotransformed to the cysteine conjugate by �-GT and adipeptidase located on the brush border (Fig. 14-15). The mercap-turic acid is transported into the proximal tubule cell by the or-ganic anion transporter while cysteine conjugates are transportedby the organic anion transporter and the sodium-independent L andT transport systems. The cysteine S-conjugate of these compoundsis thought to be the penultimate nephrotoxic species. Followingtransport into the proximal tubule, which is the primary cellulartarget for haloalkenes and haloalkanes, the cysteine S-conjugate isa substrate for the cytosolic and mitochondrial forms of the en-zyme cysteine conjugate �-lyase. In the case of the N-acetyl-cysteine S-conjugate, the N-acetyl group must be removed by adeacetylase for it to be a substrate for cysteine conjugate �-lyase.The products of the reaction are ammonia, pyruvate, and a reac-tive thiol that is capable of binding covalently to cellular macro-molecules. There is a correlation between the covalent binding ofthe reactive thiol of the cysteine conjugate with renal protein andnephrotoxicity. Hayden and colleagues (1991) and Bruschi andcoworkers (1993) have shown that biotransformation of TFEC re-sults in difluorothioamidyl-L-lysine-protein adducts in mitochon-dria and that two of the targeted proteins may belong to the heat-shock family of proteins. Hayden and colleagues (1992) have also shown that halogenated thioamide adducts of phosphatidyl-ethanolamine are formed in mitochondria following cysteine conjugate �-lyase biotransformation of TFEC.
The nephrotoxicity produced by haloalkenes is characterizedmorphologically by proximal tubular necrosis, primarily affectingthe S3 segment, and functionally by increases in urinary glucose,protein, cellular enzymes, and BUN. Following in vivo and in vitroexposures to TFEC, the mitochondrion appears to be a primary tar-get. In rabbit renal proximal tubules and isolated mitochondria,there is a marked decrease in state 3 respiration (respiration asso-ciated with maximal ATP formation) following TFEC exposure
2996R_ch14_491_514 4/12/01 10:22 AM Page 508
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY 509
(Groves et al., 1993). Furthermore, the decrease in mitochondrialfunction occurs prior to the onset of cell death. Oxidative stressmay also play a contributing role in TFEC-induced cell death be-cause lipid peroxidation products were formed prior to the onsetof cell death, and antioxidants and iron chelators decreased cyto-toxicity (Chen et al., 1990; Groves et al., 1991).
Bromobenzene In addition to their hepatotoxic effects, bro-mobenzene and other halogenated benzenes also produce nephro-toxicity. The biotransformation of these compounds, like that ofthe haloalkenes, is critical for the expression of the nephrotoxic-ity. In a series of studies, Lau and Monks demonstrated that bro-mobenzene must be oxidized by hepatic cytochrome P450 to bro-mophenol and then further oxidized to bromohydroquinone (BHQ)(Lau and Monks, 1997). BHQ is conjugated to glutathione, form-ing 2-bromo-bis(glutathione-S-yl)hydroquinone and three posi-tional isomers of 2-bromo-(glutathione-S-yl)hydroquinone. Thediglutathione conjugate is approximately a thousandfold more po-tent than bromobenzene in producing nephrotoxicity, while it pro-duces the same morphologic changes in the S3 segment andincreases the amount of protein, glucose, and cellular enzymes inthe urine. The glutathione conjugates of BHQ are substrates for re-nal �-GT activity and may ultimately be converted to cysteine andN-acetyl-cysteine conjugates of BHQ. Lau and Monks (1997) haveproposed a sequence of pathways for the renal disposition of 2-bromo-bis(cystein-S-yl)hydroquinone and 2-bromo-(cystein-yl)hydroquinones and identified possible toxic reactive intermedi-ates. While the mechanisms by which these compounds produceproximal tubular cell death remains to be determined, experiments
using LLC-PK1 cells as a model suggest that ROS play an im-portant role.
Mycotoxins
The nephrotoxicity of two mycotoxins, ochratoxin A and citrinin,found on a variety of cereal grains have been studied extensivelyand reviewed by Berndt (1993). Citrinin administration to rats mayresult in either anuric renal failure and death or nonoliguric renalfailure with complete recovery within 8 days. In contrast, ochra-toxin A produces renal dysfunction only after repeated injectionsof small doses—a condition characterized by glucosuria, ketonuria,proteinuria, and polyuria. One or both of these mycotoxins havebeen implicated in Balkan nephropathy in humans, although thedata to support this are less than clear.
Fumonisins (mycotoxins produced by the fungus Fusariummoniliforme and other Fusarium species) are commonly found oncorn and corn products and produce nephrotoxicity in rats and rab-bits (Bucci et al., 1998). Histologic examination of the kidney re-vealed disruption of the basolateral membrane, mitochondrialswelling, increased numbers of clear and electron-dense vacuoles,and apoptosis in proximal tubular cells at the junction of the cor-tex and medulla. Changes in renal function included increased urinevolume, decreased osmolality, and increased excretion of low- andhigh-molecular-weight proteins. The fumonisins are structurallysimilar to sphingoid bases and are thought to produce their toxic-ity through the inhibition of sphinganine (sphingosine) N-acyl-transferase. Inhibition of this enzyme results in an increase in theratio of free sphinganine to free sphingosine and a decrease in com-plex sphingolipids. However, the mechanism by which these sphin-golipid alterations results in cell death is unknown.
Therapeutic Agents
Acetaminophen Large doses of the antipyretic and analgesicacetaminophen (APAP) are commonly associated with hepatoxic-ity. However, large doses of APAP can also cause nephrotoxicityin humans and animals. APAP nephrotoxicity is characterized byproximal tubular necrosis with increases in BUN and plasma cre-atinine; decreases in GFR and clearance of paraaminohippurate;increases in the fractional excretion of water, sodium, and potas-sium; and increases in urinary glucose, protein, and brush-borderenzymes. There appears to be a marked species difference in thenature and mechanism of APAP nephrotoxicity (Emeigh Hart etal., 1994; Tarloff, 1997). Morphologically, the primary targets inthe mouse kidney are the S1 and S2 segments of the proximal tubule,while in the rat kidney the S3 segment is the target. In the mouse,renal cytochrome P450 2E1 has been associated with APAP bio-transformation to a reactive intermediate, N-acetyl-p-amino-benzoquinoneimine, that arylates proteins in the proximal tubuleand initiates cell death. Two of the proteins that are targets of N-acetyl-p-amino-benzoquinoneimine are a selenium-binding proteinand a glutamine synthetase (Emeigh Hart et al., 1994; Tarloff,1997). However, the mechanism by which protein adducts initiateproximal tubular cell death and ultimately nephrotoxicity remainsto be determined. While renal cytochrome P450 plays a role inAPAP activation and nephrotoxicity, glutathione conjugates ofAPAP may also contribute to APAP nephrotoxicity. Evidence forthis pathway was provided by experiments in which �-GT or or-ganic anion transport was inhibited and APAP-induced nephrotox-icity decreased (Emeigh Hart et al., 1990).
Figure 14-15. Renal tubular uptake and metabolism of GSH conjugates.
(1) Intracellular formation of GSH conjugates (R-SG) catalyzed by renalGSH S-transferase(s); (2) Secretion of the R-SG into the lumen; (3) �-GT-mediated catabolism of R-SG and formation of the corresponding S-cysteinylglycine conjugate; (4) formation of the corresponding cysteineconjugate (R-Cys); (5) Na�-coupled transport of R-Cys into the renal prox-imal tubular cell; (6) Na�-coupled transport of RSG across the basolateralmembrane; (7) Na�-coupled transport of R-Cys across the basolateral mem-brane; (8) Na�-coupled and probenecid-sensitive transport of the mercap-turate (R-NAC) across the basolateral membrane; (9) secretion R-NAC intothe lumen; (10) deacetylation of R-NAC to R-Cys and (11) acetylation ofR-Cys to R-NAC; (12) reactive thiol formation via �-lyase; (13) bindingof the reactive thiol to cellular macromolecules and initiation of cell injury.[Schnellmann RG, Kelly KJ: Pathophysiology of nephrotoxic acute renalfailure, in Berl T, Bonventre JV (eds): Atlas of Diseases of the Kidney.Philadelphia: Current Medicine, 1999, p 15.7, with permission.]
2996R_ch14_491_514 4/12/01 10:22 AM Page 509
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

510 UNIT 4 TARGET ORGAN TOXICITY
In contrast to its effects in the mouse, a critical and early stepin APAP nephrotoxicity in the rat is the conversion of APAP topara-aminophenol (PAP) (Tarloff, 1997). PAP is also a metaboliteof phenacetin and aniline and is a known toxicant to the S3 seg-ment of the proximal tubule in the rat. The steps following PAPformation and the expression of nephrotoxicity are less clear. PAPor a metabolite must be further oxidized to a benzoquinoneimineor other oxidized reactive intermediate for nephrotoxicity to occur,and there is an association between covalent binding of a PAPequivalent to renal protein and nephrotoxicity. Although glu-tathione conjugates of PAP have been isolated from rats treatedwith PAP and have been shown to be nephrotoxic when adminis-tered, the exact role they play in PAP nephrotoxicity is not clear.For example, inhibition of �-GT or organic anion transport did notameliorate PAP-induced nephrotoxicity (Anthony et al., 1993;Fowler et al., 1993), while bile duct cannulation and GSH deple-tion partially attenuated PAP-induced nephrotoxicity (Gartland etal., 1990).
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) NSAIDssuch as aspirin, ibuprofen, naproxen, and indomethacin are exten-sively used as analgesics and anti-inflammatory agents and pro-duce their therapeutic effects through the inhibition ofprostaglandin synthesis. At least three different types of nephro-toxicity have been associated with NSAID administration (Bach,1997; Tarloff, 1997; Whelton and Watson, 1998). ARF may occurwithin hours of a large dose of a NSAID, is usually reversible uponwithdrawal of the drug, and is characterized by decreased RBF andGFR and by oliguria. When the normal production of vasodilatoryprostaglandins is inhibited by NSAIDs, vasoconstriction inducedby circulating catecholamines and angiotensin II are unopposed,resulting in decreased RBF and ischemia.
In contrast, chronic consumption of NSAIDs and/or APAP(�3 years) results in an often irreversible form of nephrotoxicityknown as analgesic nephropathy (Bach, 1997; Elseviers and DeBroe, 1998). The incidence of analgesic nephropathy varies widelyin the western world, ranging from less than 1 to 18 percent of pa-tients who present with end-stage renal disease requiring dialysis.The primary lesion in this nephropathy is papillary necrosis withchronic interstitial nephritis (see above). Initial changes are to themedullary interstitial cells and is followed by degenerative changesto the medullary loops of Henle and medullary capillaries. Themechanism by which NSAIDs produce analgesic nephropathy isnot known but may result from chronic medullary/papillary is-chemia secondary to renal vasoconstriction. Other studies have sug-gested that a reactive intermediate is formed in the cells that, inturn, initiates an oxidative stress or binds covalently to critical cel-lular macromolecules.
The third albeit rare type of nephrotoxicity associated withNSAIDs is an interstitial nephritis (Tarloff, 1997; Whelton andWatson, 1998) characterized by a diffuse interstitial edema withinfiltration of inflammatory cells. Patients normally present withelevated serum creatinine and proteinuria. If NSAIDs are discon-tinued, renal function improves in 1 to 3 months.
Aminoglycosides The aminoglycoside antibiotics are so namedbecause they consist of two or more amino sugars joined in a gly-cosidic linkage to a central hexose nucleus. While they are drugsof choice for many gram-negative infections, their use is primarilylimited by their nephrotoxicity. The incidence of renal dysfunctionfollowing aminoglycoside administration ranges from 5 to 25 per-
cent but seldom leads to a fatal outcome (Cojocel, 1997; De Broe,1999; Verpooten et al., 1998).
Renal dysfunction by aminoglycosides is characterized by anonoliguric renal failure with reduced GFR and an increase inserum creatinine and BUN. Polyuria is an early event followingaminoglycoside administration and may be due to inhibition ofchloride transport in the thick ascending limb (Kidwell et al., 1994).Within 24 h, increases in urinary brush-border enzymes, gluco-suria, aminoaciduria, and proteinuria are observed. Histologically,lysosomal alterations are noted initially, followed by damage to thebrush border, endoplasmic reticulum, mitochondria, and cyto-plasm, ultimately leading to tubular cell necrosis. Interestingly, pro-liferation of renal proximal tubule cells can be observed early af-ter the onset of nephrotoxicity.
Aminoglycosides are highly polar cations; they are almost ex-clusively filtered by the glomerulus and excreted unchanged. Fil-tered aminoglycosides undergo proximal tubular reabsorption bybinding to anionic phospholipids in the brush border, followed byendocytosis and sequestration in lysosomes of the S1 and S2 seg-ments of the proximal tubules (Fig. 14-13). Basolateral membranebinding and uptake also may occur, but this is a minor contribu-tion to the total proximal tubular uptake of aminoglycosides. Theearliest lesion observed following clinically relevant doses ofaminoglycosides is an increase in the size and number oflysosomes. These lysosomes contain myeloid bodies, which areelectron-dense lamellar structures containing undergraded phos-pholipids. The renal phospholipidosis produced by the aminogly-cosides is thought to occur through their inhibition of lysosomalhydrolases, such as sphingomyelinase and phospholipases. Whilephospholipidosis plays an important role in aminoglycosidenephrotoxicity, the steps between the phospholipid accumulationin the lysosomes and tubular cell death are less clear. One hy-pothesis suggests that the lysosomes become progressively dis-tended until they rupture, releasing lysosomal enzymes and highconcentrations of aminoglycosides into the cytoplasm (Fig. 14-13).The released lysosomal contents can interact with various mem-branes and organelles and trigger cell death. Another mechanismof aminoglycoside nephrotoxicity includes a decrease in Kf andGFR (see above).
Amphotericin B Amphotericin B is a very effective antifungalagent whose clinical utility is limited by its nephrotoxicity(Bernardo and Branch, 1997). Renal dysfunction associated withamphotericin B treatment is dependent on cumulative dose and isdue to both hemodynamic and tubular effects. Amphotericin Bnephrotoxicity is characterized by ADH-resistant polyuria, renaltubular acidosis, hypokalemia, and either acute or chronic renalfailure. Amphotericin B nephrotoxicity is unusual in that it impairsthe functional integrity of the glomerulus and of the proximal anddistal portions of the nephron.
Amphotericin B administration is associated with decreasesin RBF and GFR secondary to renal arteriolar vasoconstriction oractivation of TGF. In animals, the calcium channel blocker vera-pamil blocks the acute amphotericin B–induced renal vasocon-striction, suggesting that the vasoconstriction may be mediatedthrough increased calcium levels in vascular smooth muscle cells(Tolins and Raij, 1988). However, verapamil did not completelyblock the acute decrease in GFR, suggesting that the decrease inGFR is not exclusively due to vasoconstriction. Thus, renal vaso-constriction is an important component in amphotericin B–inducedchronic renal failure.
2996R_ch14_491_514 4/12/01 10:22 AM Page 510
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY 511
Some of the renal tubular cell effects of amphotericin B aredue to the ability of this polyene to bind to cholesterol in the plasmamembrane and form aqueous pores. In the presence of amphotericinB, cells of the turtle and rat distal tubule do not produce a normalnet outward flux of protons due to an increase in proton perme-ability (Steinmetz and Husted, 1982; Gil and Malnic, 1989). Thisresults in impaired proton excretion and renal tubular acidosis. Thehypokalemia observed with amphotericin B may be due to an in-crease in luminal potassium ion permeability in the late distaltubule and the cortical collecting duct and the loss of potassiumions in the urine.
Cyclosporine Cyclosporine is an important immunosuppressiveagent and is widely used to prevent graft rejection in organ trans-plantation. Cyclosporine is a fungal cyclic polypeptide and acts byselectively inhibiting T-cell activation. Nephrotoxicity is a criticalside effect of cyclosporine, with nearly all patients who receive thedrug exhibiting some form of nephrotoxicity. Clinically, cy-closporine-induced nephrotoxicity may manifest as (1) acute re-versible renal dysfunction, (2) acute vasculopathy, and (3) chronicnephropathy with interstitial fibrosis (Mason and Moore, 1997;Dieperink et al., 1998).
Acute renal dysfunction is characterized by dose-related de-creases in RBF and GFR and increases in BUN and serum creati-nine. These effects are lessened by reducing the dosage or by ces-sation of therapy. The decrease in RBF and GFR is related tomarked vasoconstriction induced by cyclosporine; and it is proba-bly produced by a number of factors, including an imbalance invasoconstrictor and vasodilatory prostaglandin production. In par-ticular, increased production of the vasoconstrictor thromboxaneA2 appears to play a role in cyclosporine-induced ARF. Endothe-lin may contribute to constriction of the afferent arteriole becauseendothelin receptor antagonists inhibit cyclosporine-induced vaso-constriction (Lanese and Conger, 1993). While a number of stud-ies have explored possible direct effects of cyclosporine on tubu-lar cells, it is still not clear whether a direct effect of cyclosporineon tubular cells plays a role in the nephrotoxicity.
Acute vasculopathy or thrombotic microangiopathy is a ratherunusual nephrotoxic lesion that affects arterioles and glomerularcapillaries, without an inflammatory component, following cy-closporine treatment. Hyaline and/or fibroid changes, often withfibrinogen deposition, is observed in arterioles, while thrombosiswith endothelial cell desquamation affects the glomerular capillar-ies (Racusen and Solez, 1993). The pathogenesis of this lesion ispoorly understood. While the characteristics of this lesion differfrom the vascular changes of acute rejection, a variety of factorsmay contribute to this lesion in the clinical transplant setting.
Long-term treatment with cyclosporine can result in chronicnephropathy with interstitial fibrosis. Modest elevations in serumcreatinine and decreases in GFR occur along with hypertension,proteinuria, and tubular dysfunction. Histologic changes are pro-found; they are characterized by arteriolopathy, global and seg-mental glomerular sclerosis, striped interstitial fibrosis, and tubu-lar atrophy. These lesions may not be reversible if cyclosporinetherapy is discontinued and may result in end-stage renal disease.While the mechanism of chronic cyclosporine nephropathy is notknown, vasoconstriction probably plays a contributing role. Stud-ies by Wang and Salahudeen (1994, 1995) indicated that rats treatedwith cyclosporine and an antioxidant lazaroid for 30 days exhib-ited increased GFR and RBF and less tubulointerstitial fibrosis andlipid peroxidation than rats treated with cyclosporine alone, sug-
gesting that oxidative stress plays a role in cyclosporine nephro-toxity in rats. The marked interstitial cell proliferation and in-creased procollagen secretion that occurs following cyclosporineadministration may contribute to the interstitial fibrosis (Racusenand Solez, 1993).
Tacrolimus (FK-506) is a new immunosuppressive agent thatexhibits nephrotoxicity. At this time, the degree and incidence ofnephrotoxicity and morphologic changes associated withtacrolimus exposure are similar to that exhibited with cyclosporine,suggesting similar modes of toxic action.
Cisplatin Cisplatin is a valuable drug in the treatment of solidtumors, with nephrotoxicity limiting its clinical use. The kidney isnot only responsible for the majority of cisplatin excretion but isalso the primary site of accumulation (Wolfgang and Leibbrant,1997; Safirstein and Defray, 1998). The effects of cisplatin on thekidney are several, including acute and chronic renal failure, renalmagnesium wasting, and polyuria.
ARF—characterized by decreases in RBF and GFR, enzy-muria, �2-microglobulinuria, and inappropriate urinary losses ofmagnesium—was identified in early clinical trials of cisplatin. Al-though the primary cellular target associated with ARF is the prox-imal tubule S3 segment in the rat, in humans the S1 and S2 seg-ments, distal tubule, and collecting ducts can also be affected. Thechronic renal failure observed with cisplatin is due to prolongedexposure and is characterized by focal necrosis in numerous seg-ments of the nephron without a significant effect on the glomeru-lus. Considerable effort has been expended in the development ofmeasures to prevent cisplatin nephrotoxicity. These efforts includethe use of extensive hydration and mannitol diuresis and thedevelopment of less nephrotoxic platinum compounds such ascarboplatin.
The mechanism by which cisplatin produces cellular injury isnot known but may involve metabolites of cisplatin. Interestingly,the trans isomer of cisplatin is not nephrotoxic even though simi-lar concentrations of platinum are observed in the kidney afterdosing. Thus, it is not the platinum atom per se that is responsiblefor the toxicity but rather the geometry of the complex or a metabo-lite. The antineoplastic and perhaps the nephrotoxic effects of cis-platin may be due to its intracellular hydrolysis to the reactivemono-chloro-mono-aquo-diammine-platinum or diaquo-diammine-platinum species and the ability of these metabolites to alkylatepurine and pyrimidine bases.
In vitro studies using primary cultures of mouse proximal tu-bular cells revealed that the type of cell death produced by cis-platin is dependent on the concentration (Lieberthal et al., 1996).At cisplatin concentrations less than 100 �M, the primary form ofcell death is apoptosis. As the concentration increases above 100�M, a greater percentage of the cells die by oncosis. Using rabbitrenal proximal tubule cells, Courjault et al. (1993) showed thatwhile DNA synthesis, protein synthesis, glucose transport, Na�,K�-ATPase activity, and cell viability were all inhibited by cis-platin, DNA synthesis was the most sensitive. These results sug-gest that cisplatin may produce nephrotoxicity through its abilityto inhibit DNA synthesis as well as transport functions. The lackof complete return of renal function following cisplatin treatmentin vivo may result from the interference of cisplatin with the nor-mal proliferative response that occurs after injury.
Radiocontrast Agents Iodinated contrast media are used for theimaging of tissues, with two major classes of compounds currently
2996R_ch14_491_514 4/12/01 10:22 AM Page 511
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

512 UNIT 4 TARGET ORGAN TOXICITY
in use. The ionic compounds, diatrizoate derivatives, are (1) ion-ized at physiologic pH, (2) not significantly bound to protein,(3) restricted to the extracellular space, (4) almost entirely elim-inated by the kidney, and (5) freely filtered by the glomerulusand neither secreted nor reabsorbed. These agents have a veryhigh osmolality (�1200 mOsm/L) and are potentially nephro-toxic, particularly in patients with existing renal impairment, di-
abetes, or heart failure or who are receiving other nephrotoxicdrugs. The newer contrast agents (e.g., iotrol, iopamidol) are non-ionic owing to the addition of an organic side chain, their low os-molality, and their lower nephrotoxicity. The nephrotoxicity ofthese agents is due to both hemodynamic alterations (vasocon-striction) and tubular injury (via ROS) (Bakris, 1997; Porter andKremer, 1998).
REFERENCES
Anthony ML, Beddell CR, Lindon JC, Nicholson JK: Studies on the ef-fects of L(aS,5S)-a-amino-3-chloro-4,5-diphydro-5-isoxazoleaceticacid (AT-125) on 4-aminophenol-induced nephrotoxicity in the Fis-cher 344 rat. Arch Toxicol 67:696–705, 1993.
Bach PH: The renal medulla and distal nephron toxicity, in Sipes IG,McQueen CA, Gandolfi AJ (eds): Comprehensive Toxicology. Vol 7.Oxford, England: Elsevier, 1997, pp 279–298.
Bakris GL: The pathogenesis and prevention of radiocontrast-induced re-nal dysfunction, in Sipes IG, McQueen CA, Gandolfi AJ (eds): Com-prehensive Toxicology. Vol 7. Oxford, England: Elsevier, 1997, pp547–566.
Ballatori N: Mechanisms of metal transport across liver cell plasma mem-brane. Drug Metab Rev 23:83–132, 1991.
Bernardo JF, Branch RA: Amphotericin B, in Sipes IG, McQueen CA, Gan-dolfi,AJ (eds): Comprehensive Toxicology. Vol 7. Oxford, England:Elsevier, 1997, pp 475–494.
Berndt WO: Effects of selected fungal toxins on renal function, in HookJB, Goldstein RS (eds): Toxicology of the Kidney, 2d ed. New York:Raven Press, 1993, pp 459–475.
Beyersmann D, Block C, Malviya AN: Effect of cadmium on nuclear pro-tein kinase C. Environ Health Perspect Suppl 3:177–180, 1994.
Brenner BM, Bohrer MP, Baylis C, Deen WM: Determinants of glomeru-lar permselectivity: Insights derived from observations in vivo. Kid-ney Int 12:229–237, 1977.
Brenner BM, Meyer TH, Hotstetter TH: Dietary protein intake and the pro-gressive nature of kidney disease: The role of hemodynamically me-diated glomerular injury in the pathogenesis of glomerular sclerosisin agina, renal ablation and intrinsic renal disease. N Engl J Med307:652–659, 1982.
Brezis M, Epstein FH: Pathophysiology of acute renal failure, in Hook JB,Goldstein RS (eds): Toxicology of the Kidney, 2d ed. New York: RavenPress, 1993, pp 129–152.
Brezis M, Rosen S, Epstein FH: Acute renal failure, in Brenner BM, Rec-tor FJ (eds): The Kidney, 4th ed. Philadelphia, Saunders, 1991, pp 993–1061.
Brezis M, Rosen S, Silva P: Transport activity modifies thick ascend-ing limb damage in isolated perfused kidney. Kidney Int 25:65–72,1984.
Bruschi SA, West K, Crabb JW, et al: Mitochondrial HSP60 (P1 protein)and a HSP-70 like protein (mortalin) are major targets for modifica-tion during S-(1,1,2,2-tetrafluorethyl)-L-cysteine induced nephrotoxi-city. J Biol Chem 268:23157–23161, 1993.
Bucci TJ, Howard PC, Tolleson WH, et al: Renal effects of fumonisin my-cotoxins in animals. Toxicol Pathol 26:160–164, 1998.
Chen Q, Jones TW, Brown PC, Stevens JL: The mechanism of cysteineconjugate cytotoxicity in renal epithelial cells. J Biol Chem265:21603–21611, 1990.
Chen Q, Yu K, Stevens JL: Regulation of the cellular stress response byreactive electrophiles: The role of covalent binding and cellular thiolsin transcriptional activation of the 70-kDa heat shock protein gene bynephrotoxic cysteine conjugates. J Biol Chem 267:24322–24327,1992.
Cojocel C: Aminoglycoside nephrotoxicity, in Sipes IG, McQueen CA,
Gandolfi AJ (eds): Comprehensive Toxicology. Vol 7. Oxford, Eng-land: Elsevier, 1997, pp 495–524.
Conner EA, Fowler BA: Mechanisms of metal-induced nephrotoxicity, inHook JB, Goldstein RS (eds): Toxicology of the Kidney, 2d ed. NewYork: Raven Press, pp 437–457, 1993.
Counts RS, Nowak G, Wyatt RD, Schnellmann RG: Nephrotoxicants inhi-bition of renal proximal tubule cell regeneration. Am J Physiol269:F274–F281, 1995.
Courjault F, Leroy D, Coquery I, Toutain H: Platinum complex–induceddysfunction of cultured renal proximal tubule cells. Arch Toxicol67:338–346, 1993.
Cummings BS, McHowat J, Schnellmann RG: Phospholipase A2s in cellinjury and death. J Pharmacol Exp Ther 294(3):793–799, 2000a.
Cummings, BS, McHowat J, Schnellmann RG: Inhibition of a microsomalCa2�-independent phospholipase A2 increases oxidant-induced apop-tosis in renal proximal tubular cells. Toxicol Sci 54:404, 2000b.
Cummings, BS, McHowat, J, Schnellmann, RG: Inhibition of a microso-mal Ca2�-independent phospholipase A2 decreases cisplatin-inducedapoptosis in renal proximal tubular cells. J Am Soc Nephrol 11:599A,2000c.
De Broe ME: Renal injury due to environmental toxins, drugs, and con-trast agents, in Berl T, Bonventre JV (eds): Atlas of Diseases of theKidney. Philadelphia: Current Medicine, 1999, pp 11.2–11.14.
De Jong PE, Woods LL: Renal injury from angiotensin I converting en-zyme inhibitiors, in DeBroe ME, Porter GA, Bennett AM, VerpootenGA (eds): Clinical Nephrotoxicants, Renal Injury from Drugs andChemicals. The Netherlands: Kluwer, 1998, pp 239–250.
Dieperink H, Perico N, Nielsen FT, Remuzzi G: Cyclosporine/tacrolimus(FK-506), in DeBroe ME, Porter GA, Bennett AM, Verpooten GA(eds): Clinical Nephrotoxicants, Renal Injury from Drugs and Chem-icals. The Netherlands: Kluwer, 1998, pp 275–300.
Dunn RB, Anderson S, Brenner B: The hemodynamic basis of progressiverenal disease. Semin Nephrol 6:122–138, 1986.
Eknoyan G, Bulger RE, Dobyan DC: Mercuric chloride-induced acute re-nal failure in the rat: I. Correlation of functional and morphologicchanges and their modification by clonidine. Lab Invest 46:613–620,1982.
Elfarra AA: Halogenated hydrocarbons, in Sipes, IG, McQueen, CA, Gan-dolfi, AJ (eds): Comprehensive Toxicology. Vol 7. Oxford, England:Elsevier, 1997, pp 601–616.
Elsevier MM, DeBroe ME: Analgesics, in DeBroe ME, Porter GA, BennettAM, Verpooten GA (eds): Clinical Nephrotoxicants, Renal Injury fromDrugs and Chemicals. The Netherlands: Kluwer, 1998, pp 189–202.
Emeigh Hart SG, Wyand DS, Khairallah EA, Cohen SD: A role for the glu-tathione conjugate and renal cytochrome P450 in acetaminophen(APAP) induced nephrotoxicity in the CD-1 mouse. Toxicologist11:57, 1990.
Emeigh Hart SGE, Beierschmitt WP, Wyand DS, et al: Acetaminophennephrotoxicity in CD-1 Mice. I. Evidence of a role for in situ activa-tion in selective covalent binding and toxicity. Toxicol Appl Pharma-col 126:267–275, 1994.
Enami A, Schwartz JH, Borkan SC: Transient ischemia or heat stress in-
2996R_ch14_491_514 4/16/01 10:09 AM Page 512
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 14 TOXIC RESPONSES OF THE KIDNEY 513
duces a cytoprotectant protein in rat kidney. Am J Physiol 260:F479–F485, 1991.
Fluery D, Vanhille P, Pallot JL, Kleinknecht D: Drug-induced acute renalfailure: A preventable disease linked to drug misuse. Kidney Int38:1238, 1990.
Ford SM: In vitro toxicity systems, in Sipes IG, McQueen CA, GandolfiAJ (eds): Comprehensive Toxicology. Vol 7. Oxford, England: Else-vier, 1997, pp 121–142.
Fowler LM, Foster JR, Lock EA: Effect of ascorbic acid, acivicin andprobenecid on the nephrotoxicity of 4-amino-phenol in the Fischer344 rat. Arch Toxicol 67:613–621, 1993.
Fukino H, Hirai M, Hsueh YM, Yamane Y: Effect of zinc pretreatment onmercuric chloride–induced lipid peroxidation in the rat kidney. Toxi-col Appl Pharmacol 73:395–401, 1984.
Gartland KPR, Eason CT, Bonner FW, Nicholson JK: Effects of biliarycannulation and buthionine sulphoximine pretreatment on the nephro-toxicity of para-aminophenol in the Fischer 344 rat. Arch Toxicol64:14–25, 1990.
Georing, PL: Mercury induces regional and cell-specific stress protein ex-pression in rat kidney. Toxicol Sci 53:447–457, 2000.
Gil FZ, Malnic G: Effect of amphotericin B on renal tubular acidificationin the rat. Pflugers Arch 413:280–286, 1989.
Goering PL, Fisher BR, Chaudhary PP, Dick CA: Relationship betweenstress protein induction in rat kidney by mercuric chloride and nephro-toxicity. Toxicol Appl Pharmacol 113:184–191, 1992.
Goldstein RS: Biochemical heterogeneity and site-specific tubular injury,in Hook JB, Goldstein RS (eds): Toxicology of the Kidney, 2d ed. NewYork: Raven Press, 1993, pp 201–248.
Goligorsky MS, Lieberthal W, Racusen L, Simon EE: Integrin receptors inrenal tubular epithelium: New insights into pathophysiology of acuterenal failure. Am J Physiol 264:F1–F8, 1993.
Groves CE, Hayden PJ, Lock EA, Schnellmann RG: Differential cellulareffects in the toxicity of haloalkene and haloalkane cysteine conju-gates to rabbit renal proximal tubules. J Biochem Toxicol 8:49–56,1993.
Groves CE, Lock EA, Schnellmann RG: The role of lipid peroxidation inrenal proximal tubule cell death induced by haloalkene cysteine con-jugates. J Toxicol Appl Pharmacol 107:54–62, 1991.
Halleck MM, Liu H, North J, Stevens JL: Reduction of trans-4,5-dihydroxy-1,2-dithiane by cellular oxidoreductases activates gadd153/chop an dgrp78 transcription and induces cellular tolerance in kidneyepithelial cells. J Biol Chem 272:21760–21766, 1997.
Hammerman MR, Miller SB: Therapeutic use of growth factors in renalfailure. J Am Soc Nephrol 5:1–11, 1994.
Hayden PJ, Stevens JL: Cysteine conjugate toxicity, metabolism and bind-ing to macro-molecules in isolated rat kidney mitochondria. Mol Phar-macol 37:468–476, 1990.
Hayden PJ, Welsh CJ, Yang Y, et al: Formation of mitochondrial phospho-lipid adducts by nephrotoxic cysteine conjugate metabolites. ChemRes Toxicol 5:231–237, 1992.
Hayden PJ, Yang Y, Ward AJ, et al: Formation of diflourothionoacetyl-pro-tein adducts by S-(1,1,2,2-tetrafluoroethyl)-L-cysteine metabolites:Nucleophilic catalysis of stable lysyl adduct formation by histidineand tyrosine. Biochemistry 30:5935–5943, 1991.
Jarnberg P: Renal toxicity of anesthetic agents, in DeBroe ME, Porter GA,Bennett AM, Verpooten GA (eds): Clinical Nephrotoxicants, Renal In-jury from Drugs and Chemicals. The Netherlands: Kluwer, 1998, pp413–418.
Kanwar YS, Liu ZZ, Kashihara N, Wallner EI: Current status of the struc-tural and functional basis of glomerular filtration and proteinuria.Semin Nephrol 11:390–413, 1991.
Kaushal GP, Singh AB, Shah SV: Identification of gene family cf caspasesin rat kidney and altered expression in ischemia-reperfusion injury.Am J Physiol 274:F587–F595, 1998.
Kelly KJ, Williams WW, Colvin RB, Bonventre JV: Antibody to intercel-lular adhesion molecule 1 protects the kidney against ischemic injury.Proc Natl Acad Sci USA 91:812–816, 1994.
Kido T, Nordberg G: Cadmium-induced renal effects in the general envi-ronment, in DeBroe ME, Porter GA, Bennett AM, Verpooten GA (eds):Clinical Nephrotoxicants, Renal Injury from Drugs and Chemicals.The Netherlands: Kluwer, 1998, pp 345–362.
Kidwell DT, KcKeown JW, Grider JS, et al: Acute effects of gentamicinon thick ascending limb function in the rat. Eur J Pharmaco EnvironToxicol Pharmacol Section 270:97–103, 1994.
Klaassen, CD, Liu, J, Choudhuri, S. Metallothionein: An intracellular pro-tein to protect cadmium toxicity. Ann Rev Pharmacol Toxicol 39:267–294, 1999.
Kleinknecht D, Fillastre JP: Clinical aspects of drug-induced tubular necro-sis in man, in Bertani T, Remuzzi G, Garrattini S (eds): Drugs andKidney. New York: Raven Press, 1986, pp 123–136.
Komatsuda A, Wakui H, Satoh K, et al: Altered localization of 73-kilodaltonheat shock protein in rat kidneys with gentamicin–induced acute tu-bular injury. Lab Invest 68:687–695, 1993.
Lanese DM, Conger JD: Effects of endothelin receptor antagonist oncyclosporine-induced vasoconstriction in isolated rat renal arterioles.J Clin Invest 91:2144–2149, 1993.
Lau SS, Monks TJ: Bromobenzene nephrotoxicity: A model of metabo-lism-dependent toxicity, in Sipes IG, McQueen CA, Gandolfi AJ (eds):Comprehensive Toxicology: Vol 7, Oxford, England: Elsevier, 1997,pp 617–632.
Lauwerys RR, Bernard AM, Roels HA, Buchet JP: Cadmium: Exposuremarkers as predictors of nephrotoxic effects. Clin Chem 40:1391–1394, 1994.
Lehman-McKeeman LD: �2u-globulin nephropathy, in Sipes, IG, Mc-Queen, CA, Gandolfi, AJ (eds): Comprehensive Toxicology. Vol 7. Ox-ford, England: Elsevier, 1997, pp 677–692.
Leiberthal W, Triaca V, Levine J: Mechanisms of death induced by cisplatinin proximal tubular epithelial cells: Apoptosis vs. necrosis. Am J Phys-iol 270:F700–F708, 1996.
Lemasters JJ, Qian T, Bradham CA, et al: Mitochondrial dysfunction in thepathogenesis of necrotic and apoptotic cell death. J Bioenerg Bio-membr 31:305–319, 1999.
Leonard I, Zanen J, Nonclercq D, et al: Modification of immunoreactiveEGF and EGF receptor after acute tubular necrosis induced by to-bramycin or cisplatin. Ren Fail 16(5):583–608, 1994.
Levin S, Bucci TJ, Cohen SM, et al: The nomenclature of cell death: Rec-ommendations of an ad hoc committee of the society of toxicologicpathologists. Tox Pathol 27:484–490, 1999.
Lock EA, Reed CJ: Renal xenobiotic metabolism, in Sipes IG, McQueenCA, Gandolfi AJ (eds): Comprehensive Toxicology. Vol 7. Oxford,England: Elsevier, 1997, pp 77–98.
Lund BO, Miller DM, Woods JS: Studies in Hg(II)-induced H2O2 forma-tion and oxidative stress in vivo and in vitro in rat kidney mitochon-dria. Biochem Pharmacol 45:2017–2024, 1993.
Maddox DA, Brenner BM: Glomerular ultrafiltration, in Brenner BM, Rec-tor FC (eds): The Kidney, 4th ed. Philadelphia: Saunders, 1991, pp205–244.
Mason J, Moore LC: Cyclosporine, in Sipes IG, McQueen CA, GandolfiAJ (eds): Comprehensive Toxicology. Vol 7. Oxford, England: Elsevier,1997, pp 567–582.
Melnick R: An alternative hypothesis on the role of chemically inducedprotein droplet (�2u-globulin) nephropathy in renal carcinogenesis.Reg Toxicol Pharmacol 16:111–125, 1992.
Meng X, Reeves WB: Effects of chloride channel inhibitors on H2O2-induced renal epithelial cell injury. Am J Physiol Renal Physiol278:F83–F90, 2000.
Miller GW, Schnellmann RG: Cytoprotection by inhibition of chloridechannels: The mechanism of action of glycine and strychnine. Life Sci53:1211–1215, 1993.
Miller GW, Schnellmann RG: Inhibitors of renal chloride transport do notblock toxicant-induced chloride influx in the proximal tubule. ToxicolLett 76:179–184, 1995.
Molitoris BA: Alterations in surface membrane composition and fluidity:role in cell injury, in Sipes IG, McQueen CA, Gandolfi AJ (eds):
2996R_ch14_491_514 4/12/01 10:22 AM Page 513
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

514 UNIT 4 TARGET ORGAN TOXICITY
Comprehensive Toxicology. Vol 7. Oxford, England: Elsevier, 1997,pp 317–328.
Porter GA, Kremer D: Contrast associated nephropathy: presentation,pathophysiology, and management, in DeBroe ME, Porter GA, Ben-nett AM, Verpooten GA (eds): Clinical Nephrotoxicants, Renal Injuryfrom Drugs and Chemicals. The Netherlands: Kluwer, 1998, pp 317–332.
Pryor WA, Squadrito GL: The chemistry of peroxynitrite: A product fromthe reaction of nitric oxide with superoxide Am J Physiol 268:L699–L722, 1995.
Rabb H, Mendiola CC, Dietz J, et al: Role of CD11a and CD11b in is-chemic acute renal failure in rats. Am J Physiol 267:F1052–F1058,1994.
Racusen LC, Solez K: Nephrotoxicity of cyclosporine and other im-munotherapeutic agents, in Hook JB, Goldstein RS (eds): Toxicologyof the Kidney, 2d ed. New York: Raven Press, 1993, pp 319–360.
Safirstein R, Deray G: Anticancer, cisplatin/carboplatin, in DeBroe ME,Porter GA, Bennett AM, Verpooten GA (eds): Clinical Nephrotoxi-cants, Renal Injury from Drugs and Chemicals. The Netherlands:Kluwer, 1998, pp 261–272.
Sapirstein A, Spech RA, Witzgall R, et al: Cytosolic phospholipase A2
(PLA2) but not secretory PLA2, potentiates hydrogen peroxide cyto-toxicity in kidney epithelial cells. J Biol Chem 271(35):21505–21513,1996.
Schnellmann RG: Analgesic nephropathy in rodents. J Toxicol EnvironHealth, Part B 1:81–90, 1998.
Schnellmann RG, Cross TJ, Lock EA: Pentachlorabutadienyl-L-cysteine un-couples oxidative phosphorylation by dissipating the proton gradient.Toxicol Appl Pharmacol 100:498–505, 1989.
Schnellmann RG, Griner RD: Mitochondrial mechanisms of tubular injury,in Goldstein RS (ed): Mechanisms of Injury in Renal Disease and Tox-icity. Boca Raton, FL: CRC, 1994, pp 247–265.
Schnellmann RG, Lock EA, Mandel LJ: A mechanism of S-(1,2,3,4,4-pen-tachloro-1,3-butadienyl)-L-cysteine toxicity to rabbit renal proximaltubules. Toxicol Appl Pharmacol 90:513–521, 1987.
Schnellmann RG, Swagler AR, Compton MM: Absence of endonucleaseactivation in acute cell death in renal proximal tubules. Am J Physiol265:C485–C490, 1993.
Schnellmann RG, Williams SW: Proteases in renal cell death: Calpains me-diate cell death produced by diverse toxicants. Ren Fail 20(5):679–686, 1998.
Smith JB, Dwyer SD, Smith L: Cadmium evokes inositol polyphosphateformation and calcium mobilization. J Biol Chem 256:7115–7118,1989.
Smith JH, Maita K, Sleight SD, Hook JB: Effect of sex hormone status onchloroform nephrotoxicity and renal mixed function oxidases in mice.Toxicology 30:305–316, 1984.
Smith MW, Ambudkar IS, Phelps PC, et al: HgCl2-induced changes in cy-tosolic Ca2� of cultured rabbit renal tubular cells. Biochem BiophysActa 931:130–142, 1987.
Steinmetz PR, Husted RF: Amphotericin B toxicity for epithelial cells, inPorter GA (ed): Nephrotoxic Mechanisms of Drugs and Environmen-tal Toxins. New York, London: Plenum, 1982, pp 95–98.
Tarloff JB: Analgesics and nonsteroidal anti-inflammatory drugs, in SipesIG, McQueen CA, Gandolfi AJ (eds): Comprehensive Toxicology. Vol7. Oxford, England: Elsevier, 1997, pp 583–600.
Tarloff JB, Kinter LB: In vivo methodologies used to assess renal function,in Sipes IG, McQueen CA, Gandolfi AJ (eds): Comprehensive Toxi-cology. Vol 7. Oxford, England: Elsevier, 1997, pp 99–120.
Tolins JP, Raij L: Adverse effect of amphotericin B administration on re-nal hemodynamics in the rat. Neurohumoral mechanisms and influ-ence of calcium channel blockade. J Pharmacol Exp Ther 245:594–599, 1988.
Ueda N, Mayeux PR, Baglia R, Shah SV: Oxidant mechanisms in acuterenal failure, in Molitoris BA, Finn W (eds): Acute Renal Failure: ACompanion to Brenner’s and Rector’s The Kidney. St. Louis: Saun-ders, 2001. In press.
Ueda N, Walker PD, Hsu SM, Shah SV: Activation of a 15-kDa endonu-clease in hypoxia/reoxygenation injury without morphologic featuresof apoptosis. Proc Natl Acad Sci USA 92:7202–7206, 1995.
Van Why SK, Friedhelm H, Ardito T, et al: Induction and intracellular lo-calization of HSP-72 after renal ischemia. Am J Physiol 263:F769–F775, 1992.
Verpooten GA, Tulkens PM, Bennett WM: Aminoglycosides and van-comycin, in DeBroe ME, Porter GA, Bennett AM, Verpooten GA(eds): Clinical Nephrotoxicants, Renal Injury from Drugs and Chem-icals. The Netherlands: Kluwer, 1998, pp 105–120.
Wallin A, Jones TW, Vercesi AE, et al: Toxicity of S-pentachorobutadienyl-L-cysteine studied with isolated rat renal cortical mitochondria. ArchBiochem Biophys 258:365–372, 1987.
Wang C, Salahudeen AK: Cyclosporine nephrotoxicity: Attenuation by anantioxidant-inhibitor of lipid peroxidation in vitro and in vivo. Trans-plantation 58:940–946, 1994.
Wang C, Salahudeen AK: Lipid peroxidation accompanies cyclosporinenephrotoxicity: effects of vitamin E. Kidney Int 47:927–934, 1995.
Waters SL, Sarang SS, Wang KKW, Schnellmann RG: Calpains mediatecalcium and chloride influx during the late phase of cell injury. J Phar-macol Exp Ther 283:1177–1184, 1997a.
Waters SL. Wong JK. Schnellmann RG. Depletion of endoplasmic reticu-lum calcium stores protects against hypoxia- and mitochondrialinhibitor–induced cellular injury and death. Biochem Biophys ResCommun 240:57–60, 1997b.
Weinberg JM: The cellular basis of nephrotoxicity, in Schrier RW,Gottschalk CW (eds): Diseases of the Kidney, 5th ed. Vol 2. Boston,Toronto, London: Little, Brown, 1993, pp 1031–1097.
Weinberg JM, Harding PG, Humes HD: Mitochondrial bioenergetics dur-ing the initiation of mercuric chloride-induced renal injury: I. Directeffects of in vitro mercuric chloride on renal cortical mitochondrialfunction. J Biol Chem 257:60–67, 1982b.
Weinberg JM, Harding PG, Humes HD: Mitochondrial bioenergetics dur-ing the initiation of mercuric chloride-induced renal injury: II. Func-tional alterations of renal cortical mitochondria isolated after mercuricchloride treatment. J Biol Chem 257:68–74, 1982a.
Whelton A, Watson AJ: Nonsteroidal anti-inflammatory drugs: effects onkidney interstitial nephritis, in DeBroe ME, Porter GA, Bennett AM,Verpooten GA (eds): Clinical Nephrotoxicants, Renal Injury fromDrugs and Chemicals. The Netherlands: Kluwer, 1998, pp 203–216.
Wolfgang GHI, Leibbrant MEI: Antineoplastic agents, in Sipes IG,McQueen CA, Gandolfi AJ (eds): Comprehensive Toxicology. Vol 7.Oxford, England: Elsevier, 1997, pp 525–546.
Zalups RK: Renal toxicity of mercury, in Sipes IG, McQueen CA, Gan-dolfi AJ (eds): Comprehensive Toxicology. Vol 7. Oxford, England: El-sevier, 1997, pp 633–652.
Zalups RK, Lash LH: Advances in understanding the renal transport andtoxicity of mercury. J Toxicol Environ Health 42:1–44, 1994.
Zhan Y, van de Water B, Wang Y, Stevens JL: The roles of caspase-3 andbcl-2 in chemically induced apoptosis but not necrosis of renalepithelial cells. Oncogene 18:6505–6512, 1999.
2996R_ch14_491_514 4/12/01 10:22 AM Page 514
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com