Gender Mainstreaming in Rural Connectivity Investment Program

of 6
Upload
zeeshan-shahCategory
view
215download
07/22/2019 Rural District Health Office Data Connectivity and eHealth Record System
1/6
Abstract - Primary healthcare in rural and remote areas is
one of the biggest concerns especially for people in
developing nations. According to recent report by World
Health Organization, almost 800 women die every day due
to complications during childbirth. This is mainly because
of many factors which include poverty, lack of availability
of trained staff, distance etc. Providing quality health care
services in these geographically less connected areas withpoor infrastructure is a huge problem. Moreover, sudden
outbreak of epidemic diseases affects these people more
than those living in urban areas due to absence of proper
and timely medical aid, making them the most suffers. The
rapid growth and accessibility of mobile phones and
success stories of systems using Interactive Voice Response
and Short Message Service especially among low income
groups and illiterate people in different domains has
motivated us to combat these issues. Addressing the
challenges using such systems is simpler and accessible,
because these solutions are based on the technology that
we are using regularly. Validation of the proposed solution
by NGOs, Institutes, and Health Centers etc. working inRural Health has proved to very useful and effective.
Proposed solution doesnt need any special power
requirements. Moreover, the cost of implementation is
very minimal as we would be using Open Source Software
for the same.
I ndex TermseHealth, Global Health, ICTD, IVRS,
mHealth, Mobile Information System, Public Health, SMS,
Tele Medicine
I. INTRODUCTIONProviding access to primary healthcare services to peopleespecially those living in remote and rural areas is a majorconcern for any developing nation. Proper medical aid,availability of trained medical staff, doctors especially at thetime of exigencies etc. are among the distant dreams forpeople living in these regions. Patients suffering fromtuberculosis, malaria etc. who need regular monitoring,expectant mothers who dont have access to pre and post natal
care are major sufferers because of the unavailability of thebasic health facilities.This work is a part of Young Professional Project Contest 2013 for IEEE Global
Humanitarian Technology Conference 2013 and is sponsored by IEEE & USAID.
Moreover, many people suffering from various diseases arenot even properly diagnosed due to lack of facilities andconsequently dont get a chance to get proper medical aid.In fact people living in rural and remote regions are considered tobe at higher risk as they have lower life expectancy andstigmatized social status. This is because of the geographicallocation, which is the main hurdle in setting up the basic
facilities which are required for the functioning of a properhealth care system.
Though one cant fill the void created due to the unavailability
of doctors but recent advancement in technologies can act as amediator in building a bridge between the patients and thelimited medical staff available in rural and remote areas.
Various studies have shown that the unprecedented and deeppenetration of mobile phones can be used as a viable mediumof communication between patients and health workers.
According to The International Telecommunication Union
(ITU) [5] there are 6.8 billion mobile subscribers in 2013, with89% of them in the developing nations. The rapidly growingmobile phone penetration has the potential to impact variousaspects of life in developing countries like commerce, health,agriculture, education than just changing the way wecommunicate. Cell phone usage for the purpose of health isgrowing rapidly as it gives an unprecedented opportunity toconnect people. The rapid growth of mobile coverage anddeep penetration of cell phones especially in the developingregions giving rise to different mobile health projects whichare being deployed in various places where no health carefacilities were available earlier [5-7]. Also, for most of thepeople in rural and remote regions, its true that they haveaccess to cell phones as compared to health workers who canhelp them with basic healthcare facilities.
Platforms based on Automated Interactive Voice ResponseSystem (IVRS) and Short Message Service (SMS) have beenfound to be very useful and beneficial especially for lowincome groups and populations in rural and remote areas [1-4].
Many applications in different domains have been successfullybuilt and deployed using IVRS and SMS. Many applicationsin different domains have been successfully built and
Proposal for Rural District Health Office DataConnectivity & eHealth Record System
Piyush Aggarwal Matthew Imhoff Ray Gorman Vincent Mosoti([email protected])([email protected]) ([email protected]) ([email protected])
Chandramouli Sharma Prabhav Nr Nitesh Jangir Zeeshan Shah([email protected]) ([email protected]) ([email protected]) ([email protected])
7/22/2019 Rural District Health Office Data Connectivity and eHealth Record System
2/6
deployed using IVRS & SMS [1-4]. Collecting feedback frombeneficiaries, soliciting information etc. are few exampleswhere this has been used. In the healthcare sector as well,people in different parts of the world have also startedexploring the usage of these platforms. CHW, NGOs etc. areusing such systems to alarm patients about their medications,to provide post hospitalization follow-ups etc [11-15]. Thesuccess stories of these systems motivated us to explore the
usage of these systems in the context of rural and remoteareas.
One of the key challenges in rural healthcare is also the littlestandardization of data-sets and processes. Also, there is verylow or no collaboration exists between health workers andprofessionals, which otherwise may provide a morecoordinated process of delivering rural healthcare. Self-sustainability is another key issue in providing thecomprehensive solution.
II. PROBLEM
Getting a proper, timely and quality medical aid is the basicneed, but a large part of the population especially indeveloping nations is deprived of it. Many lose their livesbecause their routine illness could not be treated timely andwithout getting the initial screening, there are chances ofbecoming it chronic.
Take the case of Maternal and Child Health (MCH), womendie every year from lack of access to proper care duringpregnancy, which is totally preventable by providing propernutrition, skilled care before, during and after childbirth andemergency obstetric care. Out of total, 99% of maternal deathsoccur in the developing nations and is higher among womenliving in rural areas and poorer communities and as onlyalmost 50% of expectant mothers in developing regions haveaccess to the recommended minimum antenatal care facilities.The main reason of this high mortality is the lack ofavailability of basic health services [9].
It is not fair for a woman to die because of giving birth or
giving life to another human being. Its not acceptable. Sadly,
women and children die of causes that can be prevented,
quoted by President of Tanzania, Jakaya Kikwete [10].
Another prevailing problemworldwide is HIV. It continues tobe a major global health concern issue and have taken morethan 25 million lives in the last three decades.69% of all
people infected with HIV are living in Sub-Saharan Africa.
Similar is the case with Tuberculosis (TB) [9], which is thesecond greatest killer worldwide after HIV. Over 95% of TBdeaths occur in low and middle income countries. Adherenceto TB treatment is both difficult and critical as the diseasecarries a high mortality rate if not treated, and breaks in therecommended regimen can lead to multi drug resistance.
Most of the lives can be prevented and deaths are avoidable,as the solutions to prevent such incidents are well known. To
prevent such incidents, any patient needs access to qualityhealth care like pre and post natal care before, during and afterchildbirth in case of MCH. In case TB, the majority of casescan be cured when medicines are provided and taken properlyand regularly.
There are many reasons as why such basic facilities are notaccessible to people in the developing world. Most common
reasons are poverty, distance, lack of awareness, lack ofskilled health workers etc.
In fact, improving maternal health and reducing maternalmortality ratio by 75% is 5th Millennium Development Goalset by United Nation [8].Similarly, the problem of diseases like Malaria, Diabetes etc.are huge which affects millions of people across the globe [9].
Many of these deadly conditions are relatively simple to treat,prevent or contain. A system using the available technologieswhich people use in their daily lives regularly could be used totackle and address these issues.
III. SOLUTIONWith this proposal, we aim to propose a solution to provide a
low cost health care service using IVRS and SMS based
platforms for mending the gap between medical help seeker
and provider.
A. Pre-RequisitesHeath care at remote and rural area is of concern to people andtherefore many systems have been designed and areimplemented at various locations and at different levels. Here,we assume that for each family to access the service, theymust own or have access to a text based cell phone and amobile subscription. Also, users must live in a region wherethey have access to network coverage. For SMS based system,itll require patients at least to read and write, so in that case,
they must also be semi-literate.
B. Work FlowA system is envisaged where each patient at remote and rurallocation are connected to Central Medical Facility Unit(CMU) via Community Health Centre (CHC) of their
community. The Central Medical Facility Unit is located insome urban area where the access of doctors and othernecessary facilities can be easily fetched at the time of need,and it will be connected with each Community Health Centre.
The connectivity could be a cloud based service or locallyhosted service, depending on the availability of the internetaccess at Community Health Centre.
Each patient will be registered with their basic demographicinformation along with their Mobile Number, which would be
7/22/2019 Rural District Health Office Data Connectivity and eHealth Record System
3/6
their unique identity at the Community Health Centre in theircommunity, which is connected to the Central MedicalFacility Unit. Patient can register themselves by just sending aSMS/calling on IVR or any Local Health Worker inCommunity Health Centre can also register them.
CMU and CHC will felicitate the registration process and thiscould be through SMS, IVR or Mobile Applications etc.
As mobile number serves are unique identification key,therefore, in the cases of relocation of existing users, which isthe case with migrant workers especially, the system wouldallow unique identification. The mobile number registeredearlier with the system will be able to recognize and retrievethe previous history of the patient and transfer it tocorresponding Community Health Centre.
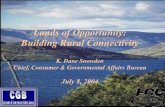
Figure (1): Block Diagram of Work Flow
The system is designed to serve the patients of community.The main/important features of the system out of many others,which can solve most prevailing problems are:
I. Important UpdatesII. Reminders
Feedback in Real Time & Buddy SystemIII. Inquires
Important Updates
Here patient will receive regular updates via Voice Calls andText Messages. It could be basic updates on maternal andchild health, vaccinations routines, immunizations, risk factorsetc. Also automated IVR Calls and SMSs will be sent asupdates to the patients to inform them about their upcomingappointments. Patients will also be notified about the healthcamps or workshops as and when they are organized.
For e.g. to promote maternal and child health the proposedIVRS/SMS platforms can be used by sending regular relevanthealth information to expectant mothers (they need to pre-register with their details) for pre & post natal care addressingtopics like labor signs, prenatal care, nutrition, diet, variousmilestones etc from local facilities. Information can alsoinclude common questions about new-born care, vaccinationsetc. We believe skilled care along with the required timely
information before, during and after childbirth can save thelives of women and new-born babies.
In order to provide useful information, a woman can registerherself or someone on her behalf can do this with theirexpected date of delivery.Access to tips on quality family planning and sexual andreproductive health care will also improve the situation.
Reminders
One of the major problems in case of TB & other relateddiseases are adherence to medications which if not followedcan lead to Multi Drug Resistance which is more fatal.
It is well known fact that people forget to take medicineespecially when they start recovering. But at that timemedicine is very crucial and leads to fatal relapse of thediseases. These platforms can be used to send regularreminders in form of SMS or Voice Calls.
Follow up applications and Buddy Systems can be also used tofor this purpose
Similarly, IVRS/SMS based systems can be used to monitordrug for any other diseases like Malaria, HIV etc.
Feedback in Real Time & Buddy System
Patients getting medication reminders have to respond in realtime to confirm when they take the medications. Until thepatient confirms, constant reminders will be sent and evenafter 5 (Variable), if patient doesnt confirm, Buddy System
will be used. In Buddy System, a reminder to other concernedfamily member (Buddy) will be sent so that they canphysically monitor the situation and ask patient to takemedications. Itll also introduce apressure and might help incompliance and adherence.
Patients suffering from TB, Malaria, HIV etc. can be sent such
reminders to take medications and for follow-ups visits.
Inquires
In case any patient seeks medical advice or need any medicalinformation, they can easily call or send SMS any time to aspecific number from their registered mobile number with thedescription. Call will be recorded and SMS would be stored inthe inbox, which is accessible by Health Workers to reply.Health Workers can appropriately answer to the problems andthey will have the facility to either call back the patientdirectly, can also send SMS or can record his response through
Community
Community HealthCentre (CHC)
Call or SMS to Register/Ask QueriesResponse via
SMS or Call
CHWs MonitoringEmergency Messages
Central
MedicalUnit
(CMU)
CHC & CMU areconnected via
Cloud/SMS
7/22/2019 Rural District Health Office Data Connectivity and eHealth Record System
4/6
IVRS. Patient will receive the SMS that his query has beenanswered and he can call back to listen to the response.
Also, patient can also listen to the response in future also bycalling at the same number from their registered mobilenumber. This will also give insight into the most commonqueries people have.
Emergency Situation
In case of emergency situations like sudden outbreak of somedisease, natural disasters etc. the system can alert localresidents with suggestion/precautions which can bebroadcasted on registered numbers as SMS or IVR Calls tosafeguard and protect them. Patients can also call the IVRNumber or send SMS to retrieve such information in suchsituations.
In fact, studies have shown that the uptime of IVR Systems isaround 99.9% during disasters. US airlines fielded 350,000more calls than a usual day before Hurricane Sandy. Suchusage serves itself as a validation for the effect of IVR
Systems for disasters.
In case of emergency at patients end, they can call or sendSMS with a specific code to the same number, which will bemonitored 24x7 by the Health Workers and will inform theconcerned personnel on duty to take immediate action. It canhelp CMU and patient to get timely, appropriate medical helpby reducing the time that elapses between a medicalemergency and reaching medical aid.
IV. TECHNOLOGYIVRS/SMS
The Automated IVRS and SMS based services have beenproviding the solutions to automate systems by reducing thehuman intervention for more than a decade now in variousfields. Platforms based on such technologies are easy to use,require low cost to set up and are easily deployable.
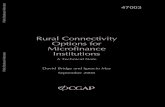
Figure (2): IVRS Work Flow
Figure (2) explains the complete IVR flow of the proposedsystem. It has been designed with menu options to keep itsimple for use and to avoid any confusion for people who arenot used to such interfaces. The IVR systems can be builtusing open software like Asterisk, FreeSwitch, FreedomFoneetc.
Figure (3) describes the work flow of SMS part of the
solution. They can be built using solutions like Frontline SMS,Rapid SMS etc. to reduce the implementation the running cost.
Figure (3): SMS Work Flow
These could be a cloud based or locally hosted service. Allthis data thus collected will be uploaded to a central hub viathe use of Delay Tolerant Network or SMS or other availableplatforms.
Data-Sets
For a higher level of collaboration between CHC, it isrecommended to have a standardized data set for information.
According to the health officials, as of now, there is a largeamount of variation among these medical records. This isbecause there is no unique pattern in which one Health Centrerecords the data. Also the mode of recording is manual atsome place and some places it is electronic. The IVR and SMSSystems would allow a first level of data-set standardization.
This standardization will help in making the systemsystematic. The data thus collected can be used to analyze andmonitor different situations like number of patients sufferingfrom specific diseases, number of patients under treatment,number of children being born, number of expecting womenetc. It will help in understanding the trends or patterns (ifexist) to design and provide the requited relief measureswherever necessary.
Data Security
Data collected as part of the project is very important and thehosted applications will be protected and will require acomplete authorization in order to access the restrictedinformation. Data at CHC will only be shared with CMU andnot among themselves and only authorized personnel at CMUwill have access to it. However, these regulations can be
7/22/2019 Rural District Health Office Data Connectivity and eHealth Record System
5/6
different as per the government regulations in the area ofdeployment.
Power
As the CMU will be at located at an urban location where the
power would be available therefore this system can be
deployed anywhere without power crunch. At CMU, there will
be a simple laptop/desktop which would be running the systemand will require a very minimal power to operate. Therefore
power generation is not an essential discussion point for this
project.
Cost
To pilot a project at any CHC, the cost of the project can be
divided into two parts, Capital Expenditure (CapEx) and
Operational Expenditure (OpEx). To set up the system and
make it running for a single channel IVRS, it would cost
around $6,000. As far as the operational cost is concerned it
would be approximately around $10,000 annually. This
includes the cost one telephone line which would be used formaking outbound calls and sending text messages,
maintenance and internet charges (if available) etc. Salaries of
the people serving, rent etc. is not included in this plan.
S.No.
Budget Head Cost ($) Description
1. CapEx 6,000 Its a non-recurringcost, includes the
complete setting up ofone CHC unit withsingle channel IVR
which is connected to
CMU2. OpEx (Per
Annum)10,000 It is recurring cost,
includes maintenance,telephone line, internet
etc.
V. CONCLUSIONOur proposed IVRS/SMS based system is an honest effort intackling one of worlds global grand challenges of healthcare.
We have focused on keeping it simple with an easy to useinterface and focusing on the technology that people regularlyuse in their day to day lives with the hope to reach out to manymore people.
The rural healthcare system can stand to benefit from theemerging low cost easily deployable technologies with a wideacceptance rate among populations. The proposed system isdesigned to be a low cost solution to serve the people atremote areas in useful and benefit ways.
Here each Phone Call & SMS will be automated butmonitored so that the human intervention can be minimizedand help can be provided 24x7.
We carried out meetings with Healthcare Professionals,Doctors, CHWs, NGOs staffers working in the field with anaim to understand the problem of people on the ground face.These meetings made it clear that the medical personal did not
feel strongly about the medical data-set and procedurestandardization for the different use cases. It was realizedthere was significant value if the system could be implementedproperly. Authors are in active talks with All India Institute ofMedical Science (AIIMS) and All India Institute of Hygieneand Public Health to pilot the project at their end.
To realize this, we need to partner with organizations, NGOs,SHGs working in the domain of healthcare at different levels.If our system can provide the timely help in case of emergencyand save peoples life in exigency we will feel system hasserved its purpose.
REFERENCES
1. Z Koradia, P Aggarwal, Phonepeti: A First Look atthe Role of IVR Systems in Community RadioStations, Microsoft Tech Vista, Jan12, Kolkata
2. Piyush Aggarwal et al., A Case Study on the Use ofIVR Systems by Visually Impaired People, ACMDEV, Jan13, Bangalore
3. Kisitu Bruce, Interactive Voice Responses (IVR) toshare Agricultural Information on Mobile Phones,
Available: http://apf-uganda.ning.com/profiles/blogs/interactive-voice-responses-ivr-to-share-agricultural-information
4. Z Koradia, P Aggarwal et al., Gurgaon Idol: Asinging competition over Community Radio andIVRS,ACM DEV, Jan13, Bangalore
5. ICT Facts & Figures, Available:http://www.itu.int/en/ITU-D/Statistics/Documents/facts/ICTFactsFigures2013.pdf,ITU13
6. Abhinav Anand, Veljko Pejovic, David L. Johnson,Elizabeth M. Belding, Village Cell: Cost Effective
Cellular Connectivity in Rural Areas,ICTD127. Joanne Riebschleger, Social Workers Suggestions
for Effective Rural Practice, Families in Society:
The Journal of Contemporary Social Services07
8. Millennium Development Goals, Fact Sheet,Available:http://www.un.org/millenniumgoals/pdf/Goal_5_fs.pdf,UN13
9. World Health Organization, Available:http://www.who.int/en/
10. Mobile Alliance for Maternal Action, July13Available:http://mobilemamaalliance.org/sites/default/files/1749-MAMA-Spotlight-July-v4-TC%5B2%5D.pdf
http://apf-uganda.ning.com/profiles/blogs/interactive-voice-responses-ivr-to-share-agricultural-informationhttp://apf-uganda.ning.com/profiles/blogs/interactive-voice-responses-ivr-to-share-agricultural-informationhttp://apf-uganda.ning.com/profiles/blogs/interactive-voice-responses-ivr-to-share-agricultural-informationhttp://www.itu.int/en/ITU-D/Statistics/Documents/facts/ICTFactsFigures2013.pdfhttp://www.itu.int/en/ITU-D/Statistics/Documents/facts/ICTFactsFigures2013.pdfhttp://www.itu.int/en/ITU-D/Statistics/Documents/facts/ICTFactsFigures2013.pdfhttp://www.un.org/millenniumgoals/pdf/Goal_5_fs.pdfhttp://www.un.org/millenniumgoals/pdf/Goal_5_fs.pdfhttp://www.who.int/en/http://mobilemamaalliance.org/sites/default/files/1749-MAMA-Spotlight-July-v4-TC%5B2%5D.pdfhttp://mobilemamaalliance.org/sites/default/files/1749-MAMA-Spotlight-July-v4-TC%5B2%5D.pdfhttp://mobilemamaalliance.org/sites/default/files/1749-MAMA-Spotlight-July-v4-TC%5B2%5D.pdfhttp://mobilemamaalliance.org/sites/default/files/1749-MAMA-Spotlight-July-v4-TC%5B2%5D.pdfhttp://mobilemamaalliance.org/sites/default/files/1749-MAMA-Spotlight-July-v4-TC%5B2%5D.pdfhttp://mobilemamaalliance.org/sites/default/files/1749-MAMA-Spotlight-July-v4-TC%5B2%5D.pdfhttp://www.who.int/en/http://www.un.org/millenniumgoals/pdf/Goal_5_fs.pdfhttp://www.un.org/millenniumgoals/pdf/Goal_5_fs.pdfhttp://www.itu.int/en/ITU-D/Statistics/Documents/facts/ICTFactsFigures2013.pdfhttp://www.itu.int/en/ITU-D/Statistics/Documents/facts/ICTFactsFigures2013.pdfhttp://www.itu.int/en/ITU-D/Statistics/Documents/facts/ICTFactsFigures2013.pdfhttp://apf-uganda.ning.com/profiles/blogs/interactive-voice-responses-ivr-to-share-agricultural-informationhttp://apf-uganda.ning.com/profiles/blogs/interactive-voice-responses-ivr-to-share-agricultural-informationhttp://apf-uganda.ning.com/profiles/blogs/interactive-voice-responses-ivr-to-share-agricultural-information7/22/2019 Rural District Health Office Data Connectivity and eHealth Record System
6/6
11. Manjeet Singh Chalga, Development of an ICTBased Support System for improving Health Care,
IJCSE, ISSN: 0975-3397 Vol. 3 No. 5May1112. Tucker JA, Blum ER, Xie L, Roth DL, Simpson CA,
Interactive voice response self-monitoring to assessrisk behaviors in rural substance users living withHIV/AIDS,PubMed12
13. Innovative Support to Emergency Diseases andDisaster, Available:http://instedd.org/14. John Quinn, Health Information TechnologyArchitecture vs Semantic Interoperability,
Bellagio,July0815. Innovative Mobile Solution for Social Change,
Available:http://projects.texttochange.org/
http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://instedd.org/http://projects.texttochange.org/http://projects.texttochange.org/http://instedd.org/http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964http://www.ncbi.nlm.nih.gov/pubmed/21311964