
Ruma's simons foundation talk 112809 final
57
From the Brigham to Bayalpata Ruma Rajbhandari MD MPH Global Health Equity Resident Brigham and Women’s Hospital
-
Upload
nyayahealth -
Category
Health & Medicine
-
view
703 -
download
3
description
Transcript of Ruma's simons foundation talk 112809 final

From the Brigham to Bayalpata
Ruma Rajbhandari MD MPHGlobal Health Equity Resident
Brigham and Women’s Hospital

Outline
• Personal background/GHE residency• Nick Simons Institute—Rural Staff Support
Program• Nyaya Health/Bayalpata Hospital

Personal Background• Born in Kathmandu• Social Action Volunteers• Yale University, Molecular Biology• World Health Organization, National TB Program• Harvard Medical School, Harvard AIDS Institute in Botswana• Patan Hospital/ Nick Simon’s Institute of Rural Health Care
Training• Brigham and Women’s Hospital, Global Health Equity
Residency Program• Nyaya Health, Bayalpata Hospital, Achham

Global Health Equity Residency
• Doris and Howard Hiatt residency in Global Health Equity
• Paul Farmer, Jim Kim, Partners in Health• Extra year of internal medicine residency• Clinical experiences at PIH sites: Haiti,
Rwanda, Lesotho• 3rd and 4th year: Nick Simons Institute/Nyaya
Health

Outline
• Personal background/GHE Residency• Nick Simons Institute—Rural Staff Support
Program• Nyaya Health/Bayalpata Hospital

Background situation
• Wide gaps between urban and rural health care in Nepal– Rural U5 mortality: 84/1000– Urban U5 mortality: 47/1000
• Doctor density drops 30-fold (96% of doctors in Nepal work in Kathmandu valley (<10% of the population lives there)
• Skilled birth attendance drops 4-fold from Kathmandu to rural Nepal

CEOC District
2008 Reality 13/ 67
District Hospitals
Comprehensive Emergency Obstetric Care
Source: MoHP Family Health Division

Nick Simons Institute of Rural Health Care Training
• Established in 2006 with a mission to train and support skilled, compassionate rural health care workers through:– the development and provision of quality training
programs – support for rural health care workers in order to
foster their productivity and retention– scholarships for health care leaders, particularly
MDGPs

Involvement with NSI
• Harvard School of Public Health project (October 2005)– “Train to retain”– Increasing the number of rural family practitioners– Rural Health Care Workers conference

Rural Staff Support Program
• Study of actual staffing patterns at district hospitals– 56% doctors present on full-time basis throughout
the previous 12 months• Rural Staff Support Program (May 2007)– Part of NSI’s second mission to support rural
health care workers– Composed of the 6Cs

6 C’s
Communication
Connection withLarger HospitalChildren’s
Education
Captained byMDGP Doctor
Continuing Medical Education
CommunityGovernance

Rural Staff Support Hospitals

RSSP: Developing a way forward
– May 2007– To find lessons that NSI could learn from similar
programs e.g. NSMP, UNICEF– What is feasible, what will work and what won't?
What else should the RSSP program include? Is RSSP a good use of NSI's resources?

Site visits and interviews
• Site Visits and interviews at district hospitals– Gorkha District Hospital– Lamjung Community Hospital: Tripartite agreement between
MoHP, local NGO and HDCS– Dolakha District Hospital, Jiri– TEAM Hospital, Dadeldhura: Christian mission hospital– Bajhang District Hospital, Chainpur – Bayalpata Hospital, Accham: at the time, non-functional
hospital– Su-joon Hospital, Doti: Korean mission hospital– Dadeldhura District Hospital


Rural Staff Support Program
• Training must go hand-in-hand with health care service delivery.
• Allows NSI to directly impact the delivery of health care
• Hands-on “laboratory” for NSI

Infrastructure support• Well trained staff need
proper equipment to do the things they are trained to do
• Detailed needs assessment in each pilot district, initially focusing on obstetric care
• Creating an "enabling environment" for the MDGP doctor and other staff

Community based health care
• Initial focus of RSSP is on the district hospital (supply side)
• Community-based health care (demand side) important
• Partners in Health: community health workers are key

Progress of RSSP
• Gulmi: MDGP doctor, functioning OR• Bajhang: MDGP doctor within the next 6
months• Jiri: MDGP in the next year• Future projects– Site standardization– Monitoring and evaluation

Outline
• Personal background/GHE residency• Nick Simons Institute—Rural Staff Support
Program• Nyaya Health/Bayalpata Hospital




Nyaya Health
24
501(c)(3) organization founded in 2006 Public-private partnership with Nepali Ministry
of Health & Population (2009) Managed by a volunteer Board of Directors and
paid Nepali staff Over 99% of all funds used directly in Nepal
Mission: To expand healthcare capacity in rural NepalTo develop a scalable model of healthcare delivery in resource-poor settings throughout the world

Building Healthcare Infrastructure: Clinical Facilities Development
Sanfe Bagar Health Center: Before
Sanfe Bagar Health Center: After25
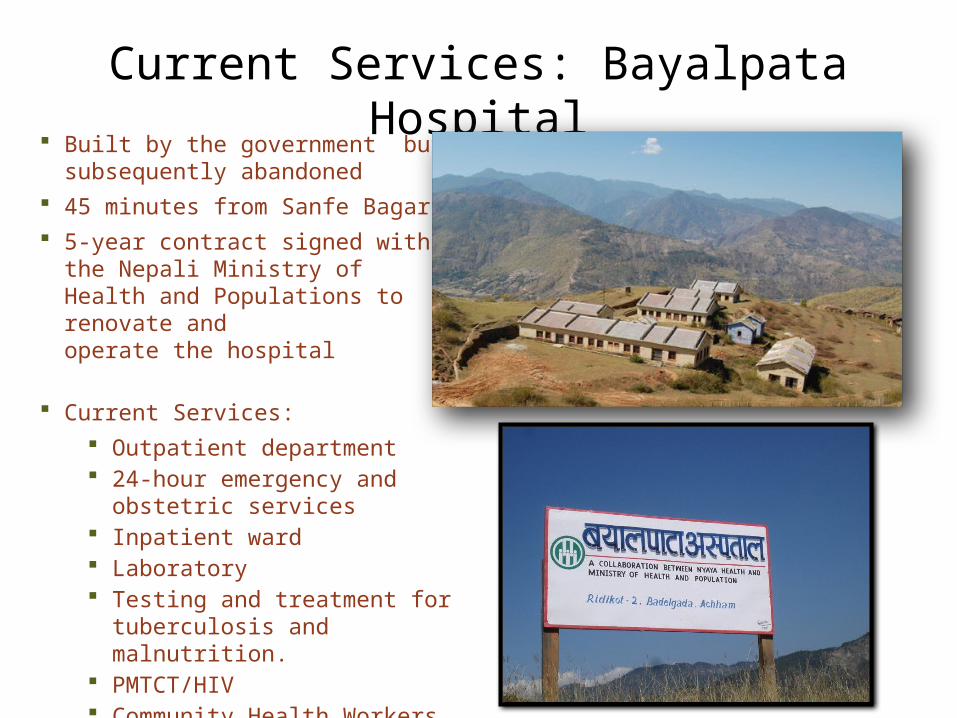
Current Services: Bayalpata Hospital Built by the government but
subsequently abandoned 45 minutes from Sanfe Bagar 5-year contract signed with the Nepali
Ministry of Health and Populations to renovate and operate the hospital
Current Services: Outpatient department 24-hour emergency and obstetric
services Inpatient ward Laboratory Testing and treatment for
tuberculosis and malnutrition. PMTCT/HIV Community Health Workers (CHWs)

Staff Recruitment• Focus on local talent• Salaries on par with the
Nepali government • Opportunities for career
advancement
27





Recurrent themes
• Severe gender inequality• Difficulty of life in the hills/ Natural “disasters”• Acceptance of death• Difficulty of referrals

Severe Gender Inequality
– Girls not counted among children – Taking a son for further treatment/referral but not
a daughter– Pica/geophagy (eating mud)severe iron
deficiency– Literacy 1996 2001
Literacy rate of 6+ years %
23.9 33.8
Male 45.3 54.1Female 5.5 6.0

parti

In the

Illegal abortion of female fetuses “I have seven girls. I had one boy but he died when he was very
young. I’ve been to Dhangadi two times before but both times they were girls and I got rid of them.”
If it was a boy, she would keep it. If it was a girl, she would abort.
Last year, when she had gone to Dhangadi, she and her husband spent almost Rs. 40,000 on medical treatment. In the Indian town of Paliya which borders Dhangadi, she underwent three ultrasound examinations to try to see the sex of the baby before it was finally confirmed that it was a girl. The rest of the money was spent on a D&C to abort the female fetus, along with travel and room and board.


Difficulty of life in the hills: Natural “disasters”
• Difficulty of life in the hills– 1-2 hour walk to the hospital considered
convenient– Patients carried on the back in a doko or on
stretcher for days to reach the hospital– Mangalsen trip—10 hours
• Natural “disasters”– Damage from a single day of rain – No electricity, no supplies, no water





Natural disasters

Storm damage

Referrals
• What disease/ill health means for a family especially when they have to be referred– Jeep ride to Nepalgunj/TEAM Hospital– Cost of medicines, hospital bed, operation, room
and board– Treating a simple illness means going into major
debt


Death of a 4 year old
A 4 year old girl was brought into Bayalpata Hospital ED at approximately 10:30am on 11/6/09 with fever and loss of consciousness by her uncle.

Mortality Review
• Lack of community health care and education • lack of ICU level care in Achham• difficulties of referral

Successes


Develop a Scalable Model • Developing a scalable model is central to
building the field of global health delivery• Nyaya Health uses several tools:
– Wiki– Blog– Data monitoring and evaluation– Open-access clinical and financial data
51

Developing a Scalable Model: Data Monitoring
Effective healthcare driven by data monitoring and evaluation
Collaboration between Nepal- and US-based data team is critical: Monthly uploading and analysis Public access to enhance
collaboration and transparency in the global health community
Revision of programmatic design and protocols according to regular data evaluation
Rigorous attention to patient privacy
http://wiki.nyayahealth.org/DataManagement
52

Developing a Scalable Model: Financial Transparency
• Nyaya’s wiki offers ready accessibility to:• Line-by-line expenditures• Month-by-month budgets
summaries• Accounts balances
– Benefits• More engaged donors• Organizational culture of honesty
and openness• More effective management
http://wiki.nyayahealth.org/Budget
53

CME program
• NSI Mid-level practicum
• CME for mid-level health workers at Bayalpata
• Interactive lectures tailored for mid-levels
• Dubbed in Nepali• Lectures from 3-4pm
three times/week

Nyaya Health: Future Plans• Furnishing/renovation• X-Ray services • Surgical capacity (C-sections)• Larger community health worker network• Expanded energy systems• HIV treatment center
55

nyaya_documentary08 - Shortcut.lnk

Thank you
• Mark Zimmerman• Nick Simons Institute• Jim and Marilyn Simons• Nyaya Health• Bayalpata Hospital staff and patients• Global Health Equity Residency


















