RS 210-Shoulder Anatomy.docx
7
Shoulder Anatomy Anatomy of shoulder and clavicle Rotator cuff o Responsible for stabilizing the shoulder during various movements o Consists of 4 primary muscles Supraspinatus- assists the deltoid muscle in abduction Infraspinatus- lateral rotation Teres minor- lateral rotation Subscapularis- medial rotation Various shoulder protocols o Protocol dependent on pt history Pain/pathology Hx of trauma Thoracic outlet syndrome o Projections may vary facility to facility AP interal AP external AP neutral AP oblique PA Scapular Y AP Scapular Y Inferosuperio axial Superinferio axial Apical AP Neer method o Pathology/ pain protocol Usually 2 AP positions AP with internal AP with external CR perp 1” inferior to coracoid AP Internal o Used to r/o bursitis, tendonitis, Hill-Sach’s defect Hill-sachs- trauma to shoulder, caused by anterior dislocation to humeral head o Moves the lesser tubercle inferomedial and into profile
Transcript of RS 210-Shoulder Anatomy.docx

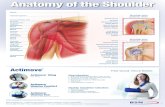
Shoulder Anatomy Anatomy of shoulder and clavicle Rotator cuff
o Responsible for stabilizing the shoulder during various movementso Consists of 4 primary muscles
Supraspinatus- assists the deltoid muscle in abduction Infraspinatus- lateral rotation Teres minor- lateral rotation Subscapularis- medial rotation
Various shoulder protocolso Protocol dependent on pt history
Pain/pathology Hx of trauma Thoracic outlet syndrome
o Projections may vary facility to facility AP interal AP external AP neutral AP oblique PA Scapular Y AP Scapular Y Inferosuperio axial Superinferio axial Apical AP Neer method
o Pathology/ pain protocol Usually 2 AP positions AP with internal AP with external CR perp 1” inferior to coracoid
AP Internalo Used to r/o bursitis, tendonitis, Hill-Sach’s defect
Hill-sachs- trauma to shoulder, caused by anterior dislocation to humeral head
o Moves the lesser tubercle inferomedial and into profile Neutral position of the arm will not move the lesser tubercle
AP Externalo Moves greater tubercle superiolateral and into profileo Palm upo Also visualize “Bankart lesions”
Anterior dislocation of the rim of the glenoid Sometimes do a 15 degree caudal angle to look for osteophyte in subacromial
space If you cannot get external rotation you can use Grashey if you cannot get arm Trauma Protocols

o Usually include AP (anatomical or neutral)o Then any of the following:
Glenoid (AP Oblique) Apical Oblqiue PA Scapular “Y” Inferosuperio axial Transthoracic
Glenoid (AP Oblique)o Patient is either AP with arm either anatomical or neutral positiono MSP is rotated 45 degrees towards the affected sideo CR is perp glenoid o Shows glenoid in profile and glenohumeral space
Greater tubercle in profile o When clavicle looks like a snake that means their obliqued to that side
When ribs elongated and more vertical than horizontal then turned
Not seeing face of glenoid Apical oblique
o Referred to as 45-45 o 45 degrees towards affected side o Position is same as AP Oblique but CR is directed @45 degrees caudalo Opens subacromial space, elongates the humeral head and neck o See glenoid in profile, glenohumeral space, and greater tubercle o Clavicle looks like dinosaur/ very vertical
Humeral head looks bitten off= Hill Sach’s defect PA Scapular “Y”
o Provides a lateral of the shoulder to r/o anterior/posterior dislocations
o Pt is PA with affected side towards the IRo Oblique shoulder 30-45 degrees towards
IRo CR is perp to mid scapula
Palpate superior angle of the scapula
Palpate distal tip of acromin Line them up so they are
perpendicular to IRo Coracoid should always be pointing
mediallyo Acromin lateral o Lesser tubercle should be seen free of
superimposition and pointing medially Scapular anterior dislocation
o 97% of all shoulder dislocations are anteriorly displaced

o 2% are posteriorly displacedo 1% are interiorly displaced
humeral head down low/ underneath glenoid AP Scapular “Y”
o PA scapular Y can be performed in the supine positiono The affected shoulder would be rotated 60 degrees away from the IRo 60 LPO would demonstrate the right shouldero 60 RPO would demonstrate the left shouldero AP “Y” would visualize all the same anatomy as the PA scapular “Y”
but with increased magnification= less detail Inferosuperio axial (Lawrence Method)
o Orthopedics’ choice of lateralo Relationship between humeral head and
glenoid o Can be done supine or seatedo If supine, arm is abducted 90 degrees and
externally rotatedo CR directed 15-20 degrees medially
Tube is directed horizontally o Build shoulder upo Supinate hand o Should be using a grid o Lesser tubercle is on top
When you supinate the hand you see lesser tubercle o Internal, Y, and inferosuperio axial
Seated Axillaryo Pt seated at the end of the tableo CR is directed distally at a 5-10 angle o Goes superiorly to inferiorly o Magnification with this projectiono Arm is pronanted
Transthoracic o Anterior/posterior displacement of the
shouldero Last resort because of heavy
superimposition of thoracic structureso Breathing technique (decrease mA and
increase exposure time) to blur lungs and vascular markings
o 3 seconds is a good amount of time in order to blur
Thoracic Outlet syndrome o Supraspinatus outlet syndrome or
impingement syndrome

o Requires positions/projections with caudal angles to better visualize subacromial space
o Attempting to visualize “osteophytes” extending from the inferior acromial surface
o Can also be performed to demonstrate subacromial bursitis Usual projections for TOS
o Apical APo Apical oblique (Garth)o Neer scap Yo Routine AP internal/external with 10 degree
caudal angle Apical AP
o PT is positioned similar to AP shoulder with arm in neutral
o 30 degree angle to open up subacromial space Apical oblique
o 45/45o Position same as AP/Garth
Neer Scapular “Y” o Pt is positioned similar to routine PA Scapulao 10-15 degree caudal angleo Open subacromial space
AP Scapulao PT positioned similar to AP shouldero Affected arm is abducted 90 degrees with hand in supinationo CR directed perpendicular and 2 inches medial to axillao Use breathing technique (3 seconds) or full exhalation to improve
visibility Image critique
o Humerus is horizontal o See much more of the scapula o See blurring of the lungs
Lateral Scapulao RAO/LAO affected side closest to receptoro Position is similar to “Y”o Instruct pt to place forearm and hand over posterior wristo Palpate vertebral and axiallary borders to ensure superimposition
Image critiqueo See border of scapula o Can see stellate FX
Occurs from blow to scapula Radiating fx lines in a star pattern
Clavicle

o FX to the clavicle usually occur due to falls on the outstretched hand, or direct blow
o Recognized as the most common injury associated with childbirth, and children in general
o Images more easily obtained in the upright, PA position whenever possible
PA Clavicleo Position affected side closest to receptoro Adjust shoulders to lie in the same transverse planeo CR perp to exit mid-shaft of clavicle o Must include S-C jointso Suspended exhalation
AP clavicle o Increase OID will result in increase magnification and decrease in
detail PA axial
o Projects clavicle superior to ribs/scapula Push clavicle up as much as you can
o Clavicle imaged horizontal placemento Position pt similar to PAo CR directed caudal, 25-30 degrees to exit the midshaft of the clavicle
Thinner pt require greater of an angleo All axial methods should employ full inhalation to further push
clavicle above ribs/scapulao You want full inhalation o PA= caudally
AP Axialso Same image can be obtained in the AP erect or recumbent positiono 2 methods can be used
CR directed 25-30 degrees cephalic Patient is positioned the same as a lordotic chest Thinner pt usually require the use of a 15 degree cephalic
angle to try to straighten out the clavicle a little more Acromioclavicular articulations
o Performed frequently in orthopedic officeso Done to demonstrate separation, dislocation of the AC jointo Evidenced by widening of the joint of one side vs the othero Radiographs of the shoulder should be performed/ reviewed prior to
these projections to r/o FX in the shoulder girdle AC joints
o Always performed bilateral for comparisono Images performed in AP Erect position
No weight With weights

o Minimum 10 pound weights provided- attached to wrists (do not allow pt to hold in hands)
o 72” SID with CR perp to MSP and 1 inch superior to jugular notcho Use routine AP shoulder technique @ 72”o Hypersthenic pt may require individual exposures