R.Peterson-Return to Sports Participation and Discharge ...
68
Return to Sports Participation and Discharge Testing Richard Peterson DPT, OCS, SCS
Transcript of R.Peterson-Return to Sports Participation and Discharge ...
Return to Sports Participation
and Discharge Testing
Richard Peterson DPT, OCS, SCS
My Background
• Originally from Warren, PA
• Bachelors in Sport and Exercise Science,
Gannon University, Erie, PA
• Doctorate in Physical Therapy, University of
Southern California, Los Angeles, CA
• Orthopedic Physical Therapy Residency,
University of Southern California, Los Angeles,
CA
Disclosures
• I have nothing to Disclose

Objectives
• Discuss the components of functional testing
for lower extremity injuries
• Identify the criteria that athletes must meet to
return to their sport
• Describe strategies to transition between
formal rehabilitation and performance
training
Recognizing the current limitations
• Return to Sport (RTS) testing is common,
however, it is variable, not standardized, and
continuing to evolve

Why Do We Test?
• Return to Sport Testing is an important process with regards to readiness for participation in high level activities in order to decrease risk of re-injury or secondary injury
• Risk Factors for Injury: Previous Injury, Asymmetry, and Fatigue
– Following ankle sprains, up to 75% of individuals will suffer a recurrent sprain, with up to 70% of those patients developing chronic instability (Hubbard and Wikstrom 2010)
– 30% of patients with non-contact ACL tear could have a second ACL tear within 2 years, up to 6x more likely to have an ACL tear compared to healthy controls (Paterno 2014)

Who Do We Test?
• Elite Athletes, Recreational Athletes, Tactical Athletes (Military, Police, EMS)
• Post-Surgical Patients
– This is relatively common (not-standardized) area of Return to Sport Testing, especially in ACL-R Rehabilitation
• Non-Surgical Patients
– Muscle Strains
• Hamstring strains most common
– Sprains

RTS Decision Making
• Time vs. Medical Examination vs. Return to Sport Testing
– Clinical Exam Clearance with same relative risk when compared to Y-Bal/FMS, however, do not necessarily test/clear to same patients (Mayer et al. 2015)
– Recent researchers suggest that time may be most significant factor associated with re-injury/secondary injury (ACL-R), and advisable wait time up to 2 years (Paterno et al 2014)
– Generalizing data, desired LSI is at least 90% across the board

RTS Decision Making – Functional
Outcome Measures
• Hip
– Lower Extremity Functional Scale (LEFS), Hip Outcome Score (HOS), Harris Hip Score, Patient Specific Functional Scale (PSFS)
• Knee
– LEFS, Knee Outcome Score (KOS), International Knee Documentation Committee Subjective Knee Evaluation (IKDC), PSFS
• Foot/Ankle
– LEFS, Foot and Ankle Outcomes Questionnaire, PSFS

RTS Testing: What makes a good test?
• Reliable – the degree to which a test produces consistent results
• Reproducible – in the research, the methods described in such completeness that the study can be re-created exactly as done by original researchers
• Predictive of Injury
• Valid – it tests what it is supposed to
• Feasible – taking account cost, the test materials, space, time needed, as well as many other factors, is it possible for you to do?

Levels of Assessment: Return to Sport
Testing
• Clinical Examination
• Limb Symmetry Index (LSI) Testing
– Basic Functional/Early Clinical Tests
– Transitional Strength/Endurance/Technique
– Power/Control/Deceleration
• Endurance Testing
• Advanced Agility/Field Tests
• Re-integration into each facet of sport leading up to full clearance – On Field Progression

RTS Decision Making – Clinical Exam
• Goal prior to progressing to more rigorous RTS Testing is that the patient pass a Clinical Exam, with satisfactory scores in regards to:
– Pain
– Swelling
– Range of Motion/Flexibility
– Strength
– Gait
• Successful re-integration back to ADL
Limb Symmetry Index Testing
• Limb Symmetry Index (LSI) Testing
– Basic Functional/Early Clinical Tests
• Functional Movement Screen (FMS)
• Y-Balance/Star Excursion Balance Test (SEBT)
• Isokinetic Testing
– Transitional Strength/Endurance/Technique
• Vail Sport Cord Test
– Power/Control/Deceleration
• Hop Testing

Limb Symmetry Index Testing
• Limb Symmetry Index (LSI) Testing
– Basic Functional/Early Clinical Tests
• Functional Movement Screen (FMS)
• Y-Balance/Star Excursion Balance Test (SEBT)
• Isokinetic Testing
– Transitional Strength/Endurance/Technique
• Vail Sport Cord Test
– Power/Control/Deceleration
• Hop Testing

Functional Movement Screen
• Screening tool created by Cook et el. in 1997
• Goal to identify asymmetries which result in movement deficiencies
• Numerous Studies to demonstrate Reliability/Validity (Cook et al 1998, Teyhen et al 2012, Parenteau 2013)
• Consists of Seven Movement Patterns Graded from 0-3 Points (21 points possible)– 3/3 No Compensations
– 2/3 Able to Perform movement with Compensations
– 1/3 Unable to Perform Movement
– 0/3 Pain during attempted movement
• Cut-Off Score of 14/21

FMS

Y-Balance / SEBT
• Y-Balance Test derived from Star Excursion
Balance Test first described by Gary Gray in
1995
– SEBT: 8 Directions, 6 Practice Trials, 3
Measurements, 144 Repetitions
– Y-Balance: 3 Reaches, Anterior, Posterior-Medial,
and Posterior-Lateral
– Tests dynamic balance at the limits of stability

Lower Quarter Y-Balance
Posterior Medial Reach
Posterior Lateral ReachAnterior Reach
https://www.functionalmovement.com/Store/23/y-balance_test_kit

Lower Quarter Y-Balance
• Used to assess dynamic strength/balance at limits of stability
• Measures Limb Symmetry as well as Composite Score:– (Ant Reach + PM Reach + PL Reach) / 3x Limb Length x 100
• Different scores predictive for different populations
– Butler et al. established Composition Cut-Off of 89% for College Football Players
– Plisky et al. demonstrated Composition Cut-Off of 94% for High School Basketball Players

Lower Quarter Y-Balance
• 4cm Difference L/R Difference Anterior Reach
results in 2.5x increased risk for injury – Plisky
et al 2006
• Better Posterior-Lateral Reach decreases risk
for ankle sprains – de Noronha et al 2012

Isokinetic Testing
• Isokinetics have been around since 1950s
• Isokinetic Testing measures various factors of muscle activation/strength for a designated(set) speed of movement
• Data for nearly all body regions, with most proliferative area being the knee

Isokinetic Testing
• Common Velocities tested: 60/180/300 deg/sec
• Goal of at least 85-90% Symmetry
• Common Variables Evaluated:– Peak Torque (Most Common in literature per Davies et
al)
– Torque/Body Weight Ratio
– Angle Specific Torque
– Total Work
– Average Power
– Rate of Force Development
– Quadriceps/Hamstrings Ratio

Limb Symmetry Index Testing
• Limb Symmetry Index (LSI) Testing
– Basic Functional/Early Clinical Tests
• Functional Movement Screen (FMS)
• Y-Balance/Star Excursion Balance Test (SEBT)
– Transitional Strength/Endurance/Technique
• Vail Sport Cord Test
– Power/Control/Deceleration
• Hop Testing
Vail Sport Cord Test
• Functional Test that evaluates muscle strength, endurance, power, and movement quality
• Originally described by Garrison et al 2012
• 4 Components – Possible 54 Total Points - 46/54 Considered Passing Score (85%)– Single Leg Squat – 3 min – Possible 15 Points
– Lateral Bounding – 90 sec – Possible 15 Points
– Forward Jogging – 2 min – Possible 12 Points
– Backward Jogging – 2 min – Possible 12 Points
• **Also a Hip Version**

Vail Sport Cord Test
• Single Leg Squat (goal: 3 minutes)
• 1. Knee flexion angle between 30 and 60° Yes (1) No (0)
• 2. Patient performs repetitions without dynamic knee valgus *knee valgus = patella falls medial to the great toe
• Yes (1) No (0)3. Patient avoids locking knee during extension
• Yes (1) No (0)4. Patient avoids patella extending past the toe during knee flexion
• Yes (1) No (0)5. Patient maintains upright trunk during knee flexion
• Yes (1) No (0)Minute 1 ________ Minute 2 ________ Minute 3 ________
• Single Leg Squat Total Points: _______/15
• • If patient repeats error on 3 consecutive repetitions after correction, they are not eligible to receive a point for that particular standard (within each 1 minute timeframe).

Vail Sport Cord Test
• Lateral Bounding (goal: 90 seconds)
• 1. Knee flexion angle is 30° or greater during landing Yes (1) No (0)
• 2. Patient performs repetitions without dynamic knee valgus *knee valgus = patella falls medial to the great toe
• Yes (1) No (0)3. Patient performs repetitions within landing boundaries
• Yes (1) No (0)4. Landing phase does not exceed 1 second in duration
• Yes (1) No (0)
• 5. Patient maintains upright trunk during knee flexion Yes (1) No (0)
• 1st 30 sec ________ 2nd 30 sec _________ 3rd 30 sec ________ Lateral Bounding Total Points _______/15
• • If patient repeats error on 3 consecutive repetitions after correction, they are not eligible to receive a point for that particular standard (within each 30 second timeframe).

Vail Sport Cord Test
• Forward Jogging/Backward Jogging (goal: 2 minutes)
• 1. Knee flexion angle between 30 and 60° Yes (1) No (0)
• 2. Patient performs repetitions within landing boundaries Yes (1) No (0)
• 3. Patient performs repetitions without dynamic knee valgus * knee valgus = patella falls medial to the great toe
• Yes (1) No (0)
• 4. Patient avoids locking knee during extension Yes (1) No (0)
• 5. Landing phase does not exceed 1 second in duration Yes (1) No (0)
• 6. Patient maintains upright trunk during knee flexion
• Yes (1) No (0)Minute 1 ________ Minute 2 _________
• Forward Jogging Total Points ______/12
• Backward Jogging Total Points ______/12
• • If patient repeats error on 3 consecutive repetitions after correction, they are not eligible to receive a point for that particular standard (within each 1 minute timeframe).

Vail Hip Sport Cord Test
– Single Leg Squat – 3 min – Possible 6 Points
– Lateral Bounding – 100 sec – Possible 5 Points
– Diagonal Bounding – 100 sec – Possible 5 Points
– Forward Box Lunge – 2 min – Possible 4 Points
– 20 points Total
Limb Symmetry Index Testing
• Limb Symmetry Index (LSI) Testing
– Basic Functional/Early Clinical Tests
• Functional Movement Screen (FMS)
• Y-Balance/Star Excursion Balance Test (SEBT)
– Transitional Strength/Endurance/Technique
• Vail Sport Cord Test
– Power/Control/Deceleration
• Hop Testing

Hop Testing
• Noyes Hop Tests
– Single Leg Hop
– Single Leg Triple Hop
– Single Leg Triple Cross-
Over Hop
– 6 Meter Timed Hop
• Drop Jump (LESS)
• Tuck Jump
• Vertical Jump
• “Back in Action” Testing
Battery
• Functional Lower
Extremity Evaluation
(FLEE) Testing Battery
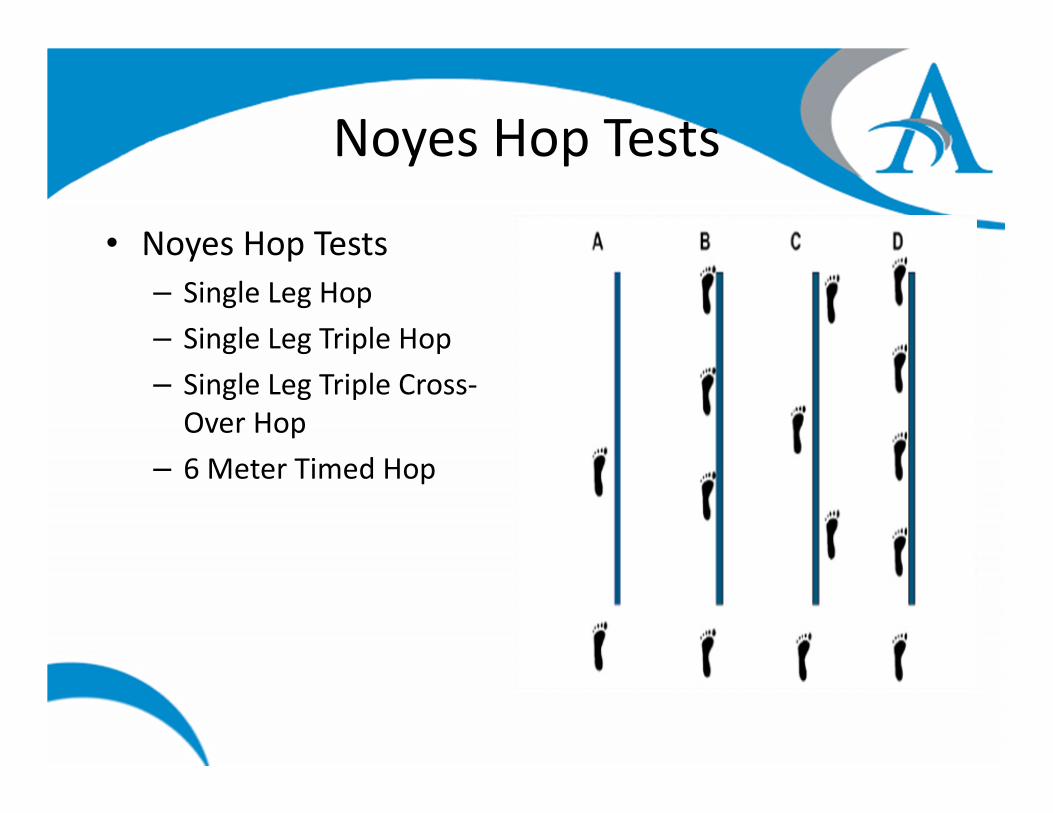
Noyes Hop Tests
• Noyes Hop Tests
– Single Leg Hop
– Single Leg Triple Hop
– Single Leg Triple Cross-
Over Hop
– 6 Meter Timed Hop

Noyes Hop Tests
• Single Leg Hop For Distance
– <85% Limb Symmetry found to be abnormal (ACL Deficiency), Noyes et al (1991)
– Munro and Herrington(2011) on Healthy Recreational Athletes
• 100% participants had LSI >90%
• 73% had LSI >95%
– Logersted et al. (2012)
• LSI of at least 89.3% found to be optimum

Noyes Hop Tests
• Triple Hop For Distance– <85% Limb Symmetry
found to be abnormal (ACL Deficiency), Noyes et al (1991)
– Munro and Herrington(2011) on Healthy Recreational Athletes
• 100% participants had LSI >90%
• 68% had LSI >95%
– Logersted et al. (2012)• LSI of at least 95.2% found
to be optimum

Noyes Hop Tests
• Cross Over Hop– <85% Limb Symmetry
found to be abnormal (ACL Deficiency), Noyes et al (1991)
– Munro and Herrington(2011) on Healthy Recreational Athletes
• 100% participants had LSI >90%
• 64% had LSI >95%
– Logersted et al. (2012)• LSI of at least 94.9% found
to be optimum
Noyes Hop Tests
• 6 Meter Timed Hop– <85% Limb Symmetry
found to be abnormal (ACL Deficiency), Noyes et al (1991)
– Munro and Herrington(2011) on Healthy Recreational Athletes
• 100% participants had LSI >90%
• 86% had LSI >95%
– Logersted et al. (2012)• LSI of at least 87.7% found
to be optimum

Hop Tests Continued
• Drop Jump (LESS)
• Tuck Jump
• Vertical Jump

Drop Jump – Landing Error Scoring
System
• Patient jumps from 30cm box, landing on both
feet at a distance ½ of their height way from the
box, then immediately performs a maximal
vertical jump
• Scored out of 19 Points - Higher Scores reflect
poor technique and indicate Higher Risk for Injury
• Valid, Reliable, Predictive (Padua 2009, 2015)
• Scores <5 Indicate Low Risk for ACL Injury (Fox et
al 2016)

LESS Scoring Sheet

LESS Demonstration Video

Tuck Jump
• Introduced by Myer et al in 2008 as a “Clinician Friendly Plyometric Assessment…”
• Patient performs repeated Tuck Jumps over the duration of 10 seconds, and is graded according to movement flaws that exist
• 10 potential flaws assessed, in addition to number of jumps per test– Higher score = more flaws present
• Conflicting data regarding reliability, with studies suggesting a steep learning curve with assessment – Video Analysis could be helpful in this area
• Useful test to help educate patient and guide treatment

Tuck Jump Assessment
Read et al. 2016
Vertical Jump• Used to Assess Lower Extremity Power
• Double Leg and Single Leg Jumping– Goal to achieve at least 85% LSI
• Petshnig et al. (1998) found that at 1 year out, only Single Leg Vertical Jump was found to be less than 85% LSI when Isokinetic testing, SL Hop for Distance, and SL Triple Hop for Distance were over 85% LSI– Utilized Jump Plate, 10 seconds of repeated jumping, with
instructions to have shortest possible amount of contact time
• Lee 2018 felt that LSI goal of 89% appropriate, with correlations to passing scores with SL Hop and Isokinetic Testing (peak extensor torque and extensor strength deficit)

Testing Batteries
• “Back In Action” Test Battery– Blend of tests which utilize technology to aide in risk
stratification, some of which are newly established tasks
• Functional Lower Extremity Evaluation – FLEE– Utilizes more established functional tests
• Kyritsis et al. “Six”– Likelihood of ACL graft rupture increased with patients not
meeting six clinical discharge criteria before return to sport and is associated with a four times greater risk of rupture (2016)
• Isokinetic Testing: Quadriceps deficit < 10% at 60 deg/sec)
• Noyes Hop Testing at least 90% LSI
• Running T-Test <11 Seconds
• Completed On-Field Sports Specific Rehab
“Back in Action” Test Battery
• Introduced by Hildebrandt et al. (2015)– Moderate to Good Reliability for each test
• Devoloped by CoRehab (Trento, Italy)
• Seven Functional Tests:– Two-Leg Stability Test
– One-Leg Stability Test
– Two-Leg Counter-Movement Jump
– One-Leg Counter-Movement Jump
– Plyometric Jumps
– Speedy Test
– Quick Feet Test
• Utilizing Data from Test, compiled results described on scale from ”Very Weak” to ”Very Good”

Speedy Jump testQuick Feet test

Functional Lower Extremity Evaluation
- FLEE• Described by Haitz et al in 2014
• Moderate to Excellent Test-Retest Reliability, High to Excellent Interrater Reliability (Haitz et al 2014)
• Test Battery Consisting of 8 Performance tests– 3 Sub Test Clusters: Control, Hop, Endurance
– Control Sequence:• Timed Lateral Step Down
• Timed Leap and Catch
– Hop Sequence:• Single Leg Hop for Distance
• Single Leg Triple Hop for Distance
• Single Leg Triple Cross-Over for Distance
• Single Leg 6 Meter Timed Hop
– Endurance Sequence:• Square Hop Test
• LEFT – Lower Extremity Functional Test (a cone agility test)
• Scores based on normative data as well as LSI

FLEE – Control Sequence
Timed Lateral Step Down
Timed Leap and Catch

FLEE
Brummit et al 2016
Noyes et al 1991 Caffrey et al 2009
FLEE – Hop Sequence /
Endurance Sequence
LEFT – Lower Extremity Functional Test

Endurance Testing
• Yo-Yo Endurance Test
(Beep Test)
– Developed by Danish
physiologist Jens Bangsbo
– Several testing variations,
all with normative data
• Cooper Test
– 2 Main Variations
• 12 Minute Run (Scored by
Distance)
• 1.5 Mile Run (Scored by
time)
Field Tests / Advanced Agility
• 40 Yard Dash– Usually patients have baseline of scores if they play football
• Pro Agility (5-10-5)– Popular test that measures pre-planned change of direction speed
• T-Test and Modified T-Test– Agility test that involves running forward, lateral shuffle, backward running, with changes in
directions
– Modified T-Test shortens distances, which can more helpful for sports which require short bursts (Tennis, Baseball Infielder)
• 3 Cone Agility – L-Test– Replaced Box Drill at NFL Combine
• Normative Data Available
• Illinois Agility– Forward running agility test with cutting
• Normative Data Available
• Barrow Test– Common Agility test used in soccer, forward running test with varying degrees of cutting
• Normative Data Available
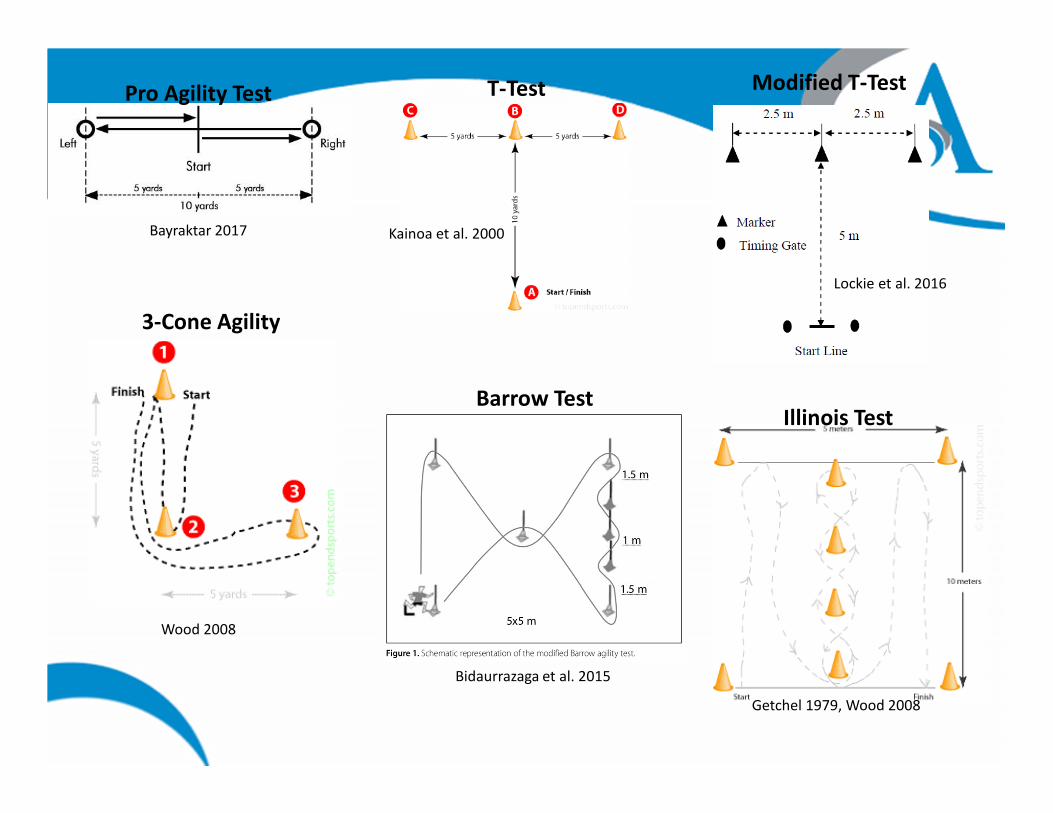
Kainoa et al. 2000Bayraktar 2017
Lockie et al. 2016
Bidaurrazaga et al. 2015
Wood 2008
Getchel 1979, Wood 2008
Pro Agility Test T-Test Modified T-Test
3-Cone Agility
Barrow TestIllinois Test

Hitting our Check-Points to Stay on
Track
• It is often helpful to decide upon Initial Evaluation which tests are going to be the most appropriate for your patients– Examples: Type of Injury, Surgical/Non-Surgical, Age, Sport,
Professional/Elite Youth/Recreational Levels, Previous Sport Testing (40YD, Yo-Yo Test, etc), Coach/ATC/Personal Trainer involvement, Insurance Limitations
• Based on those decisions, you can have pre-planned “check-points” in regards to what you want to test, and when (time point or functional criteria met)

Hitting our Check-Points to Stay on
Track• Often easier to plan check-points when surgical such as
with ACL-R– Example:
• 12 Weeks: Goal to pass clinical Exam, Perform FMS/Y-Balance to assess for impairments
• 4 Months: Isokinetic Testing initiated, If no isokinetic testing available, consider Vail Sport Cord Test, or “Control Sequence” of FLEE
• 4-6 Months: Hop testing
• 6-12 Months: Conditioning/Agility Testing
• This timeline of Check-Points will be significantly altered with non-contact such as lateral ankle sprain or a hamstring strain, especially when considering the degree of injury and whether or not they are in their primary season
Technology
• Recently, there has been a big push to move toward technologically assisted assessments due to the ability of technology to capture so much data in a short amount of time
• Examples include both wearable and external equipment:– Force Plates
– Accelerometers
– Motion Capture Cameras
• There are various companies which utilize technology and software to help risk stratify– ”CoRehab’s ‘Back in Action’”, 3-Planes Movement Specialists, Sparta Science
• There is also Risk Stratification Software which allows tester to enter data from tests performed– For example: Move 2 Perform
• Technology will play a big part in the future of Return to Sport Testing

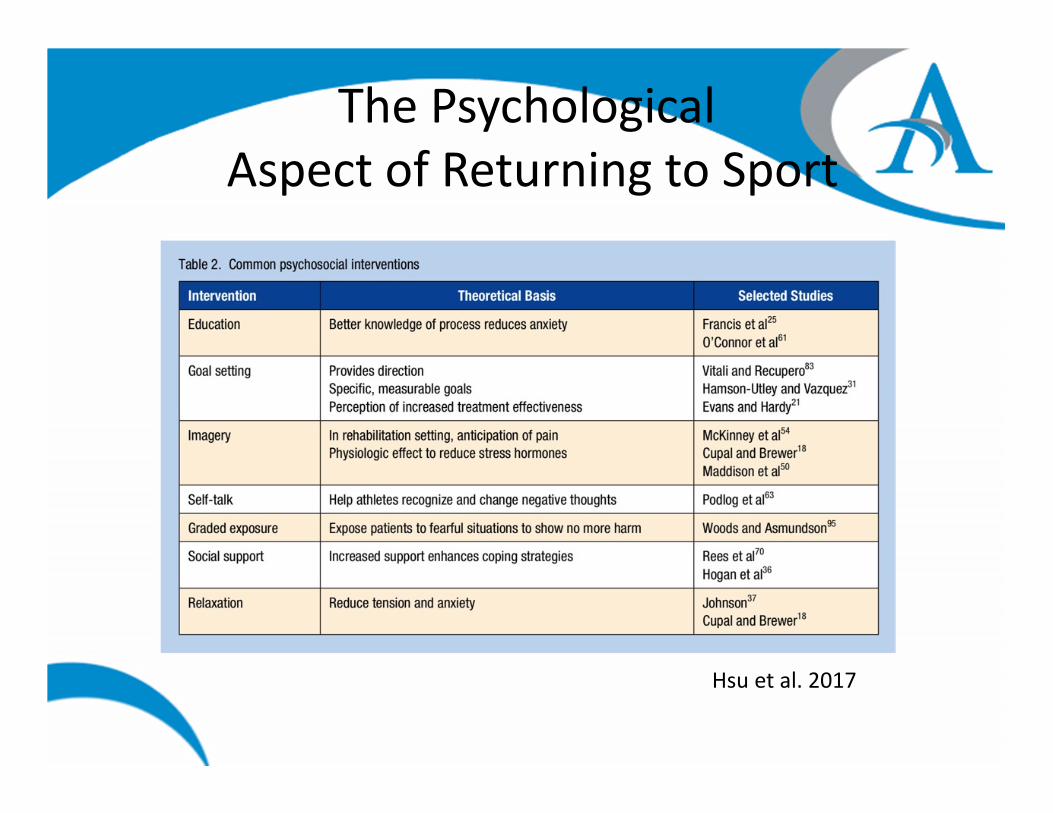
The Psychological
Aspect of Returning to Sport• Kinesiophobia – a primary psychosocial construct which
refers to the fear of movement/re-injury
• ”fear of reinjury can adversely result in both physiological (such as muscular guarding) and psychological changes (such as distraction and lack of trust in the injured site) that can affect rehabilitation outcomes..”
• Following ACL-R: fear of re-injury appears to be phase specific (depending on time-frame)– Inconsistent early on, but later in rehab, Increased fear is
associated with decreased Self-Reported Function
• Following Achilles Ruptures: Increased fear associated with decreased function
Hsu et al. 2017

The Psychological
Aspect of Returning to Sport
Hsu et al. 2017
The Psychological
Aspect of Returning to Sport
Hsu et al. 2017
Communication Between Professionals
with Return to Sport as Goal• Who are the Facilitators for Return to Sport Testing
– Physicians, Physical Therapists, Athletic Trainers, Coaches, Performance Coaches
• Excellent Communication between Facilitators is needed to help minimize the risk of returning a previously injured athlete back to performance– Physicians often want to know from the Rehab Professionals what the
patient’s clinical exam looks like, where they are in regards to functional demands, and whether there is limb symmetry
– Rehab Professionals often want to know from Physician where the patient stands in regards to tissue healing, and when functional tasks/tests can be performed, and then when they are comfortable with more impact related testing
– Performance Staff/Coaches often want to know from Rehab Professionals what they are “cleared” to do: Weightlifting, Conditioning, Skills, Non-Contact vs. Contact Practice, Live Competition

Transitioning from Formal
Rehabilitation to Performance Training• Using movement analysis in early stages of rehab can help guide
the patient’s motor programming as they move toward performance (if they demonstrate a movement dysfunction at a slower speed, you can bet that they demonstrate it at a faster speed, even if you can’t see it)
• Patients who are returning to high level sports must understand the underlying concepts of the exercises they are performing– Alignment and shock absorption with numerous variables
manipulated:• Single vs. Multiplanar, Loaded vs Unloaded, Speed, Amplitude, Acceleration vs
Deceleration, Multi-step exercises (Run, Cut, Jump combinations)
– From Simple Pre-planned moving toward Complex Reactive tasks

Examples of Early Movement Faults
�Sled Push – L LE: Extensor Thrust, Heel Drop, Hip Pop
↑Sled Pull – L LE: Decreased Knee Extension,
Shorter Stance Phase

Examples of Early Movement Faults
←Ladder “Icky” Shuffle - L LE: Dec Shock
absorption, Dec Eccentric knee flexion,
Inc Trunk Lean (Tibia/Trunk not parallel)
Hop and Stick – L LE: Dec Shock
absorption, Dec Eccentric knee flexion,
Inc Trunk Lean (Tibia/Trunk not parallel), →
Rapid Trunk Extension “Whip” to
generate momentum to return to
start

Take Home Points
• Return to Sport Testing/Screening is important for all injuries that result in time-loss, not just surgical cases
• In order to be ready to Return to Sport, the Athlete first needs to feel ready. In order to be Cleared for Return to Sport, they need to Provethey are ready
• Clusters of tests are more powerful than individual tests, and each test has a purpose. An appropriate cluster incorporates the tests most appropriate for each patient.

Take Home Points
• Clinicians should begin to decide early on which RTS Tests the patient should pass, so the treatment plan/direction can be reflected by those goals, and all appropriate communication between facilitators can be achieved
• Don’t miss an opportunity to improve a patient’s future performance training with appropriate coaching during rehab

Thank You!

References
• Beardsley C, Contreras B. The Functional Movement Screen: A Review. Strength & Conditioning Journal (Lippincott Williams & Wilkins). 2014;36(5):72.
• Bidaurrazaga-Letona I, Carvalho HM, Lekue JA, Badiola A, Figueiredo AJ, Gil SM. Applicability of an Agility Test in Young Players in the Soccer Field. Revista Brasileira de Medicina do Esporte. 2015;21(2):133.
• Bizzini M, Hancock D, Impellizzeri F. Suggestions from the field for return to sports participation following anterior cruciate ligament reconstruction: soccer. The Journal Of Orthopaedic And Sports Physical Therapy. 2012;42(4):304-312. doi:10.2519/jospt.2012.4005
• Butler RJ, Lehr ME, Fink ML, Kiesel KB, Plisky PJ. Dynamic balance performance and noncontact lower extremity injury in college football players. Sports Health. 2013;5:417-422
• CAFFREY E, DOCHERTY CL, SCHRADER J, KLOSSNER J. The Ability of 4 Single--Limb Hopping Tests to Detect Functional Performance Deficits in Individuals With Functional Ankle Instability. Journal of Orthopaedic & Sports Physical Therapy. 2009;39(11):799.
• Cook G, Burton L, Fields K, Kiesel K. The Functional Movement Screen. Danville, VA: Athletic Testing Services Inc, 1998
• Currie J, Ackland T, Ebert JR, et al. Comparison of the “Back in Action” Test Battery to Standard Hop Tests and Isokinetic Knee Dynamometry in Patients Following Anterior Cruciate Ligament Reconstruction. International Journal of Sports Physical Therapy. 2018;13(3):389-400. doi:10.26603/ijspt20180389
• Davies G, McCarty E, Provencher M, Manske R. ACL Return to Sport Guidelines and Criteria. Current Reviews in Musculoskeletal Medicine. 2017;10(3):307.
• Garrison JC, Shanley E, Thigpen C, Geary R, Osler M, DelGiorno J. The Reliability of the Vail Sport Test^TM^ as a Measure of Physical Performance Following Anterior Cruciate Ligament Reconstruction. International Journal of Sports Physical Therapy. 2012;7(1):20-30. http://proxy-s.mercer.edu/login?qurl=http%3a%2f%2fsearch.ebscohost.com%2flogin.aspx%3fdirect%3dtrue%26db%3drzh%26AN%3d104458365%26site%3deds-live%26scope%3dsite.
• Gokeler A, Welling W, Benjaminse A, Lemmink K, Seil R, Zaffagnini S. A critical analysis of limb symmetry indices of hop tests in athletes after anterior cruciate ligament reconstruction: A case control study. Orthopaedics & Traumatology, Surgery & Research: OTSR. 2017;103(6):947-951. doi:10.1016/j.otsr.2017.02.015.
• Gokeler A, Welling W, Zaffagnini S, Seil R, Padua D. Development of a test battery to enhance safe return to sports after anterior cruciate ligament reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy: Official Journal Of The ESSKA. 2017;25(1):192-199. doi:10.1007/s00167-016-4246-3.
• Gómez-Piqueras P, Sixto González-Víllora, María del Pilar Sainz de Baranda Andújar, Onofre R. Contreras-Jordán. Functional Assessment and Injury Risk in a Professional Soccer Team. Sports, Vol 5, Iss 1, p 9 (2017). 2017;(1):9. doi:10.3390/sports5010009.
• Gomez-Piqueras P, Gonzalez-Rubio J, de Baranda PS, Najera A. Use of functional performance tests in sports: Evaluation proposal for football players in the rehabilitation phase. Turkish Journal of Physical Medicine & Rehabilitation (2587-0823). 2018;64(2):148-154. doi:10.5606/tftrd.2018.1462

References
• Haitz K, Shultz R, Hodgins M, Matheson GO. Test-Retest and Interrater Reliability of the Functional Lower Extremity Evaluation. Journal of Orthopaedic & Sports Physical Therapy. 2014;44(12):947-954. doi:10.2519/jospt.2014.4809.
• Herbst, E, Wierer G, Fischer F, Gfoller P, Hoser, C, Fink, C. Functional assessments for anterior cruciate ligament reconstruction return to sport. Annals of Joint. 2017; 2:37(7). Doi: 10.21037/aoj.2017.06.13
• Hubbard, Tricia, Erik A Wikstrom. Ankle sprain: pathophysiology, predisposing factors, and management strategies. Open Access Journal of Sports Medicine, Vol 2010, Iss default, Pp 115-122 (2010). 2010;(default):115.
• Hildebrandt C, Müller L, Zisch B, Huber R, Fink C, Raschner C. Functional assessments for decision-making regarding return to sports following ACL reconstruction. Part I: development of a new test battery. Knee Surgery, Sports Traumatology, Arthroscopy: Official Journal Of The ESSKA. 2015;23(5):1273-1281. doi:10.1007/s00167-015-3529-4.
• Hoog P, Warren M, Smith CA, Chimera NJ. Functional Hop Tests and Tuck Jump Assessment Scores between Female Division I Collegiate Athletes Participating in High Versus Low Acl Injury Prone Sports: A Cross Sectional Analysis. International Journal of Sports Physical Therapy. 2016;11(6):945-953.
• Hsu C-J, Meierbachtol A, George SZ, Chmielewski TL. Fear of Reinjury in Athletes. Sports Health: A Multidisciplinary Approach. 2017;9(2):162.
• KLINE PW, JOHNSON DL, IRELAND ML, NOEHREN B. Clinical Predictors of Knee Mechanics at Return to Sport after ACL Reconstruction. Medicine & Science in Sports & Exercise. 2016;48(5):790.
• Kyritsis P, Bahr R, Landreau P, Miladi R, Witvrouw E. Likelihood of ACL graft rupture: not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. British Journal Of Sports Medicine. 2016;50(15):946-951.
• Lee DW, Yang SJ, Cho SI, Lee JH, Kim JG. Single-leg vertical jump test as a functional test after anterior cruciate ligament reconstruction. The Knee. 2018;25:1016-1026. doi:10.1016/j.knee.2018.07.014.
• Logerstedt D, Grindem H, Lynch A, et al. Single-legged hop tests as predictors of self-reported knee function after anterior cruciate ligament reconstruction: the Delaware-Oslo ACL cohort study. The American Journal Of Sports Medicine. 2012;40(10):2348-2356.
• Lynch TS, Bedi A, Larson CM. Athletic Hip Injuries. The Journal Of The American Academy Of Orthopaedic Surgeons. 2017;25(4):269-279. doi:10.5435/JAAOS-D-16-00171
• Munro AG, Herrington LC. Between-session reliability of four hop tests and the agility T-test. Journal of Strength & Conditioning Research (Lippincott Williams & Wilkins). 2011;25(5):1470-1477. doi:10.1519/JSC.0b013e3181d83335.
• Myer GD, Ford KR, Hewett TE. Tuck Jump Assessment for Reducing Anterior Cruciate Ligament Injury Risk. Athletic Therapy Today. 2008;13(5):39-44.
• Noronha M, França LC, Haupenthal A, Nunes GS. Intrinsic predictive factors for ankle sprain in active university students: A prospective study. Scandinavian Journal of Medicine & Science in Sports. 2013;23(5):541-547. doi:10.1111/j.1600-0838.2011.01434.x

References
• Noyes FR, Barber SD, Mangine RE. Abnormal lower limb symmetry determined by function hop tests after anterior cruciate ligament rupture. American Journal of Sports Medicine. 1991;19(5):513-518.
• Padua DA, Marshall SW, Boling MC, Thigpen CA, Garrett WE Jr., Beutler AI. The Landing Error Scoring System (LESS) is a valid and reliable clinical assessment tool of jump-landing biomechanics: The JUMP-ACL study. American Journal of Sports Medicine. 2009;37(10):1996-2002. doi:10.1177/0363546509343200.
• Padua DA, DiStefano LJ, Beutler AI, de la Motte SJ, DiStefano MJ, Marshall SW. The Landing Error Scoring System as a Screening Tool for an Anterior Cruciate Ligament Injury-Prevention Program in Elite-Youth Soccer Athletes. Journal of Athletic Training (Allen Press). 2015;50(6):589-595. doi:10.4085/1062-6050-50.1.10.
• PAMUKOFF DN, MONTGOMERY MM, CHOE KH, MOFFIT TJ, GARCIA SA, VAKULA MN. Bilateral Alterations in Running Mechanics and Quadriceps Function following Unilateral Anterior Cruciate Ligament Reconstruction. Journal of Orthopaedic & Sports Physical Therapy. 2018;48(12):960-967. doi:10.2519/jospt.2018.8170
• Parenteau GE, Gaudreault N, Chambers S, Boisvert C, Grenier A, Gagne G, Balg F. Functional movement screen test: A reliable screening test for young elite ice hockey players. Phys There Sport. 2013.
• PATERNO, M. V. et al. Clinical Factors That Predict a Second ACL Injury After ACL Reconstruction and Return to Sport: Preliminary Development of a Clinical Decision Algorithm. Orthopaedic Journal Of Sports Medicine, [s. l.], v. 5, n. 12, p. 2325967117745279, 2017.
• Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of Second ACL Injuries 2 Years After Primary ACL Reconstruction and Return to Sport. The American Journal Of Sports Medicine. 2014;42(7):1567-1573. doi:10.1177/0363546514530088.
• Petschnig R, Baron R, Albrecht M. The relationship between isokinetic quadriceps strength test and hop tests for distance and one-legged vertical jump test following anterior cruciate ligament reconstruction. Journal of Orthopaedic & Sports Physical Therapy. 1998;28(1):23-31.
• Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star excursion balance test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther. 2006;36(12):911
• Powell C, Jensen J, Johnson S. Functional Performance Measures Used for Return-to-Sport Criteria in Youth Following Lower-Extremity Injury. Journal of Sport Rehabilitation. 2018;27(6):581.
• Pratt KA, Sigward SM. Knee Loading Deficits During Dynamic Tasks in Individuals Following Anterior Cruciate Ligament Reconstruction. The Journal Of Orthopaedic And Sports Physical Therapy. 2017;47(6):411-419. doi:10.2519/jospt.2017.6912.
• READ PJ, OLIVER JL, DE STE CROIX MBA, MYER GD, LLOYD RS. Reliability of the Tuck Jump Injury Risk Screening Assessment in Elite Male Youth Soccer Players. Journal of Strength & Conditioning Research (Lippincott Williams & Wilkins). 2016;30(6):1510-1516. doi:10.1519/JSC.0000000000001260.
• Lina Schelin, Eva Tengman, Patrik Ryden, Charlotte Häger. A statistically compiled test battery for feasible evaluation of knee function after rupture of the Anterior Cruciate Ligament - derived from long-term follow-up data. PLoS ONE, Vol 12, Iss 5, p e0176247 (2017). (5):e0176247. doi:10.1371/journal.pone.0176247.

References
• Schmitt LC, Paterno MV, Ford KR, Myer GD, Hewett TE. Strength Asymmetry and Landing Mechanics at Return to Sport after Anterior Cruciate
Ligament Reconstruction. Medicine And Science In Sports And Exercise. 2015;47(7):1426-1434. doi:10.1249/MSS.0000000000000560.
• Sueyoshi T, Nakahata A, Emoto G, Yuasa T. Single-Leg Hop Test Performance and Isokinetic Knee Strength After Anterior Cruciate Ligament
Reconstruction in Athletes. Orthopaedic Journal Of Sports Medicine. 2017;5(11):2325967117739811. doi:10.1177/2325967117739811.
• Teyhen DS, Shaffer SW, Lorenson CL, Halfpap JP, Donofry DF, Walker MJ, Dugan JL, Childs JD. The functional movement screen: A reliability
study. JOSPT. 2012; 42:530-40.
• Valle X, L Tol J, Hamilton B, et al. Hamstring Muscle Injuries, a Rehabilitation Protocol Purpose. Asian Journal Of Sports Medicine.
2015;6(4):e25411. doi:10.5812/asjsm.25411.
• Wilke, C, Pfeiffer, L, Frobose, I. Return to Sports after Lower Extremity Injuries: Assessment of Movement Quality. Health. 2017(9) 1416-1426.
Doi:10.4236/health.2017.910104
• Zaffagnini S, Grassi A, Serra M, Marcacci M. Return to sport after ACL reconstruction: how, when and why? A narrative review of current
evidence. Joints. 2015;3(1):25-30.