Britain 1851-1951 Britain 1851-1951 Liberal Reforms Introduction Higher History.

NATIONAL SERVICE
1
ROYAL ARMY DENTAL CORPS 1951-1953
by
Barry Brown
Colonel Frank McCarthy, senior dental officer, on inspection tour to Dental Centre,
Kaduna.
NATIONAL SERVICE
2
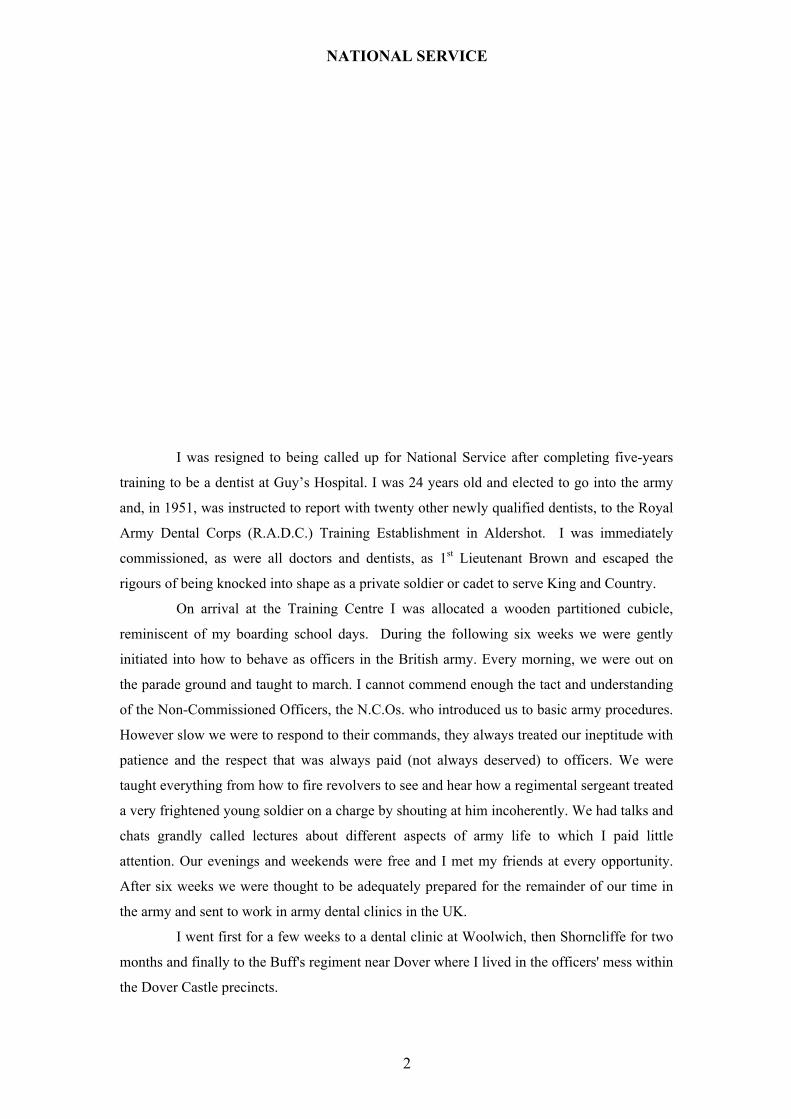
I was resigned to being called up for National Service after completing five-years
training to be a dentist at Guy’s Hospital. I was 24 years old and elected to go into the army
and, in 1951, was instructed to report with twenty other newly qualified dentists, to the Royal
Army Dental Corps (R.A.D.C.) Training Establishment in Aldershot. I was immediately
commissioned, as were all doctors and dentists, as 1st Lieutenant Brown and escaped the
rigours of being knocked into shape as a private soldier or cadet to serve King and Country.
On arrival at the Training Centre I was allocated a wooden partitioned cubicle,
reminiscent of my boarding school days. During the following six weeks we were gently
initiated into how to behave as officers in the British army. Every morning, we were out on
the parade ground and taught to march. I cannot commend enough the tact and understanding
of the Non-Commissioned Officers, the N.C.Os. who introduced us to basic army procedures.
However slow we were to respond to their commands, they always treated our ineptitude with
patience and the respect that was always paid (not always deserved) to officers. We were
taught everything from how to fire revolvers to see and hear how a regimental sergeant treated
a very frightened young soldier on a charge by shouting at him incoherently. We had talks and
chats grandly called lectures about different aspects of army life to which I paid little
attention. Our evenings and weekends were free and I met my friends at every opportunity.
After six weeks we were thought to be adequately prepared for the remainder of our time in
the army and sent to work in army dental clinics in the UK.
I went first for a few weeks to a dental clinic at Woolwich, then Shorncliffe for two
months and finally to the Buff's regiment near Dover where I lived in the officers' mess within
the Dover Castle precincts.

NATIONAL SERVICE
3
Unexpectedly, the surgeries at each of the three dental clinics in England where I
worked were inadequately equipped. What was worse for a newly qualified dentist was to be
told what treatment I was allowed and not allowed to do. I became completely dispirited with
the curtailment of my professional skills by senior officers who appeared more concerned
with my clothes and whether or not I saluted them correctly than with my clinical
competence.
While at Dover I received a copy of an urgent memorandum from The Secretary of
State, The War office, London, to the General Officer Commander-in Chief, Eastern
Command, dated 17th August 1951. It stated:
The under mentioned officer, R.A.D.C., is required for service overseas in
West Africa (Nigeria – disemplane Lagos).
Lieutenant W.A.B. Brown (415087) Gp. No. 51.05.
I look back in wonderment on my flight in 1951 by Dakota to West Africa. Today it
takes less than twelve hours to fly from Heathrow to Lagos, but it took us two and a half days
with two night stopovers and three extra stops to refuel. I presumed the army must have
found that flying personnel to their overseas postings was more economical than sending them
on a leisurely two-week sea trip in an Elder Dempster Line ship.
We flew across France and Spain and landed in Gibraltar for the night. Very early,
the following morning, we took off for Nigeria and flew across the Sahara. We touched down
at 9.0 a.m. in the desert to refuel at Aoulef which, we could see from the air had a runway, a
small administration building and one or two rectangular huts of dried mud located near an
oasis. We taxied up to the buildings where ladders were placed against the wings for the
technicians to access the plane’s petrol tanks. In the desert, petrol was stored in drums within
rectangular enclosures protected by dried mud walls, 18 inches thick and 5 feet high. There
was no roof and the drums were covered with sand. A Frenchman managed the airport with
the help of some of the villagers.
We refuelled again at Goa, memorable for its unbelievable heat, on the banks of the
river Niger before arriving in Kano in Northern Nigerian where we spent the night. We were
due to land at Lagos at noon with one stop on the way at the administrative and military town
of Kaduna where three of the passengers were due to alight and where we would take on more
fuel.
West Africa
When we landed at Kaduna airport and taxied towards the buildings, I saw among
the waiting officers a Royal Army Dental Corps badge and thought what a friendly gesture
that the dental officer at Kaduna had come to welcome me to Nigeria. I was soon put right as
to his intentions. He had orders for me to disembark at Kaduna. I produced my orders to say I
was to disembark at Lagos, but the plane’s senior army officer decided the new order was

NATIONAL SERVICE
4
more recent than mine. I collected my baggage and said farewell to my fellow passengers, a
mixed group of army personnel and a civilian, with whom I had established a nodding
acquaintance.
The dental officer, Captain Baxter, informed me that I was replacing him. He took
me straight on to what was destined to be my home for seventeen months. We travelled in an
army truck along a sandy road lined by mango trees. After a 15-minute drive, we abruptly
turned off the road where a signboard confirmed that we had arrived in the grounds of the 44
Military Hospital.
The hospital was isolated in its own grounds of fifty or more acres not far from the
Governor General’s house and within walking distance of the township to the southeast. The
administration block, the ward for nursing Europeans and the operating theatre were on the
southern side. The officers’ accommodation, the mess, nurses' quarters and a rather grand
house for the CO and his family were on the northern side. The mess and accommodation for
the British Non Commissioned Officers, B.N.C.Os., spread out to the east and an array of
buildings, including a mortuary, secure accommodation for patients requiring custodial care
and the Dental Centre were within easy reach. About a half-mile away further to the east
there were wards for the Nigerian soldiers and self-contained, on the far side of the camp,
were the African lines or living accommodation for the soldiers and their families. The very
flat and stark environment was softened by a number of very tall and majestic bombax trees,
numerous mango, papaya and butter trees and flaming acacias. Randomly planted in the
compound were frangipani shrubs and a variety of brilliant yellow flowering hibiscus and red
flowered bougainvillea shrubs. A variety of exotic and colourful birds, depending on the
season, flew in and out among the trees and shrubs. Lizards of various shapes, sizes and
colour scuttled busily around the buildings in pursuit of food. At night during the rainy season
frogs added their deep-throated croak. There were poisonous snakes, but we rarely saw them.
Captain David Baxter introduced me to my future life where I was to be responsible
for the dental health of 4,000 soldiers of the R.W.A.F.F. (Royal West African Frontier Force).
I was to live and sleep in a room, known as a gida, one of four in a block with a narrow
communal veranda. After breakfast, we did a tour of the hospital and at lunch I was
introduced to my future companions, all National Service officers, Keith Henley, medical
specialist, Peter Lewis, surgeon and Basil Bendeth, medical officer for the military families,
who all gave me a warm welcome. After lunch, much to my surprise, everyone retired to their
room for a snooze. No work was done after 1.0 p.m. except for emergencies and ward rounds.
During the rest of the day, David painstakingly described, instructed and warned me about the
future, advising me to take care that all things due to me would be received by me and all
things I should dispense, should be dispensed. Thomas, an African soldier, came later to me in

NATIONAL SERVICE
5
my gida to say I would be his master and he would be responsible for looking after my clothes
and room.
I was surprised to learn that only National Service personnel with an officer’s
commission were seconded to the Royal West African Frontier Force and that only regular
soldiers of the rank of sergeant and above were posted there. Life in the R.W.A.F.F. was to
be very different from anything I had so far experienced in the British Army.
Dentistry
On my first morning, Thomas, my batman, awakened me at 6.30 from a deep sleep
and I rose immediately with the usual enthusiasm of one waking up the first day amidst new
surroundings. Breakfast was fruit, orange or grapefruit, followed by two eggs, fried bread and
bacon, and rounded off by toast and marmalade. A Paludrine tablet, a preventive against
malaria, was put on everyone’s side plate and I took one every morning throughout my stay in
West Africa and escaped the debilitating disease. After breakfast, David took me across to the
Dental Centre, a three-minute walk from the gidas. I was introduced to Sgt. Tapp, a British
Non Commissioned Officer (B.N.C.O.) dental technician, Cpl. Sylvanos Oko who ran the
centre and Pte. Akujuobi, his assistant. The centre was a single storey 25-foot square building
divided to provide a spacious surgery and a smaller laboratory. A veranda served as a waiting
room.
Sgt. Tapp, Lt. Brown, Cpl. Sylvanos Oko and Pte. Akujuobi,

NATIONAL SERVICE
6
There were eight patients waiting to be seen: two African women, five African
soldiers and one B.N.C.O.. The two African women were wives of colonial workers, one in
the P.W.D. (Public Works Department) and the other a policeman. The Civilian dentist was
out of town and there was a reciprocal arrangement between the army and the civilian dentist
to stand in for each other.
The policeman’s wife at first refused to open her mouth. Her husband persuaded her
and, then, when he pointed to the offending tooth, she made a tentative bite at his finger,
calling forth a torrent of words from all assembled and a kick or two into the bargain from her
husband. The subsequent treatment was more easily given. It was a surprise introduction to
dentistry in Africa.
The following morning, the African woman whose husband had kicked her into
submission, came in smiling and obediently did all that she was told.
I couldn’t help noticing in the course of treating my African patients that the body
aroma they gave off was distinctive and unfamiliar, but as the days passed I noticed it less and
less and one day to my surprise, found that I was giving off the same smell. Eventually, I
discovered that all newcomers from Europe quickly developed this customary odour. I never
discovered the cause of the distinctive odour.
David returned to England a few days later and I was on my own, left to discover
how I would take care of the dental health of the soldiers and families of George VI’s Royal
West African Army Frontier Force. In Kaduna, I was responsible for two thousand men in
two battalions and several service corps. In Zaria, 50 miles to the north I had to look after one
thousand men and in Enugu, nearly 400 miles to the south, another thousand men. The
families of these soldiers were all entitled to treatment as well. I had a completely free hand
on how I organised my day’s work. My senior R.A.D.C. officer was stationed 700 miles away
in Accra in the Gold Coast. I soon learned that the only people from whom I could seek
advice were the ever-helpful medical National Service colleagues. In retrospect it is
interesting to reflect that nobody in the R.A.D.C. Command questioned that a dentist qualified
just over a year would be able to manage on his own, especially as the needs of the European
servicemen were just as complex in West Africa as they were back home. However, I soon
learned that my senior R.A.D.C. officer’s main preoccupation was how many fillings I did in
a month, which was paradoxical for I soon discovered after a few days of seeing African
patients that their dentitions were different from those of the Europeans and were to all intents
and purposes absolutely free of dental caries, the destructive process causing toothache and, if
untreated, to destruction of the tooth. Very few African soldiers needed any fillings for their
teeth. They had different dental requirements. This was such an obvious fact, I could never
understand why my superiors in Accra was always asking me to do more work. There simply

NATIONAL SERVICE
7
was not the demand for treatment of the kind that existed in the UK. refined carbohydrate, an
important factor in dental caries. The exceptions were the Africans cooking for Europeans
who evidently tasted and ate the refined sugar preparations cooked for their employers. But
another very important factor to account for the African soldiers’
The most obvious explanation for the difference was that their diet was free from
freedom from dental disease was that only Africans with perfect dentitions were recruited into
the army. So, my impression that the majority of Nigerians had caries-free dentitions was
based on an unrepresentative sample. There might have been a much higher caries incidence
in the population. The Africans soldiers on the other hand, compared with the British soldiers,
had a much higher incidence of disease arising from their gums, which led to the formation of
abscesses around the necks of the teeth. Treatment was quick and simple with an incision
made by a scalpel.
Africans had their own natural occurring toothbrush: chewing the ends of small
twigs from a particular tree caused the fibres of the twig to splay out just like a toothbrush.
There was no toothpaste, but I often saw Africans rubbing the fine silt from the riverside
round their teeth. Many Africans were just as obsessional about cleaning their teeth as the
Europeans.
The Africans frequently filed the opposing corners of their upper central incisor
teeth at an angle of 45º, to form, for aesthetic reasons, an inverted “V”. Little did they realise
the damage they were doing. The filing took away the outer protective enamel of the tooth
and exposed the underlying dentine leading to the tooth pulp or nerve as it is popularly called,
becoming infected and eventually to the "death" of the tooth. Subsequently an abscess
developed or a large invasive cyst, a sac-like cavity , formed in the bone round the apex or tip
of the root of the tooth. I treated these cysts by root filling the tooth and removing the lining
of the cyst. If I had to extract the tooth, I would replace it with a tooth on a small denture and
file the opposing corner of the artificial central incisor tooth to match the original filed tooth
As I have explained, there was very little restorative (filling of teeth) dentistry for
me to do. However, I extracted many structurally sound teeth because of very severe
periodontal disease, a condition that led to the destruction of most of the bone in which the
teeth were anchored. Their removal was a very simple procedure. Occasionally, however, a
molar tooth would have to be extracted because of a dental abscess arising from rare dental
decay and, in those cases, the supporting bone securing the teeth in their sockets would be
intact and extracting the tooth could entail an elaborate surgical technique.
Nigerians did not have impacted molar teeth that are so familiar in the UK, because
they usually had big enough jaws to accommodate all their teeth and, as well, their teeth are
reduced in size by wear caused by eating yams and cassava with associated grit. The wearing
away on these surfaces could be as much as a two to three millimetres per tooth, which was

NATIONAL SERVICE
8
equivalent to the whole length of a third molar from front to back, so making adequate room
to enable the third molar to erupt correctly into the mouth. A similar explanation would
account for dentitions in which four additional premolars, the next teeth in series teeth
forming behind the canines, developed and erupted and found enough space to function
normally.
One day a six-foot tall, robust looking soldier had to have a tooth extracted and after
I gave him his injection, he suddenly got up from the chair and said, “Sir, I have strong ju-ju
to protect me against the metal of my enemy’s weapons so, Sir, I’d like to take it off my belt. I
don’t want to damage your instruments.” He proceeded to remove a little leather sac tied with
a thong to his belt and I thanked him for his consideration.
Dental officers were allowed to do private practice but, as Kaduna had a
comparatively small population and there was a civilian dental officer already working in the
town, not many private patients came my way. However, one day, a very ragged African
wearing only tattered khaki shorts arrived at the Dental Centre saying he had heard of my
special dentures and wanted one to replace his front teeth. He had come 400 miles to see me.
At the conclusion of the treatment, assuming, because of his tattered clothes, he was a very
poor man, I asked for a very small fee. The man pulled out of his trouser pocket a very large
wad of notes and had come prepared to pay a substantial sum. He turned out to be a trader.
When the colonial dentist was away, civilians from Kaduna and the surrounding
villages would come to the Army Dental Centre for emergency treatment. They were usually
straightforward emergencies, but one day I was faced for the first time with a condition I
knew I could not treat. A woman in her fifties who spoke no English, and for whom Corporal,
Sylvanos, translated, said that the ju-ju doctor had blown white dust into her face and caused a
lump to grow in her mouth. She asked if could I get rid of it. I looked in her mouth where
there was a large irregular shaped swelling of the palate and back of the mouth. It was a
tumour of a kind I did not recognise. I had no alternative but to send her to the hospital and
hope somebody there could treat her. I never heard what happened to the lady and she still
remains to haunt me, reminding me how limited my skills were.
On another occasion a man dressed in a grey suit of coarse material, came with a
guard from the local prison for treatment. He was a murderer and due shortly to be hanged. I
found the episode eerie. I forget what treatment I had to administer, but have often reflected
on the paradox of this situation, especially as the man remained totally expressionless. I recall
at the time that some people in the hospital were interested, for professional reasons, in going
to watch how the hanging was carried out. I shiver to think of it now.
One of the trials with which I had to contend was the unreliable delivery of essential
materials for treating patients. In my first week at Kaduna, I discovered that there were no
more local anaesthetic cartridges, in spite of them having been ordered by my predecessor
NATIONAL SERVICE
9
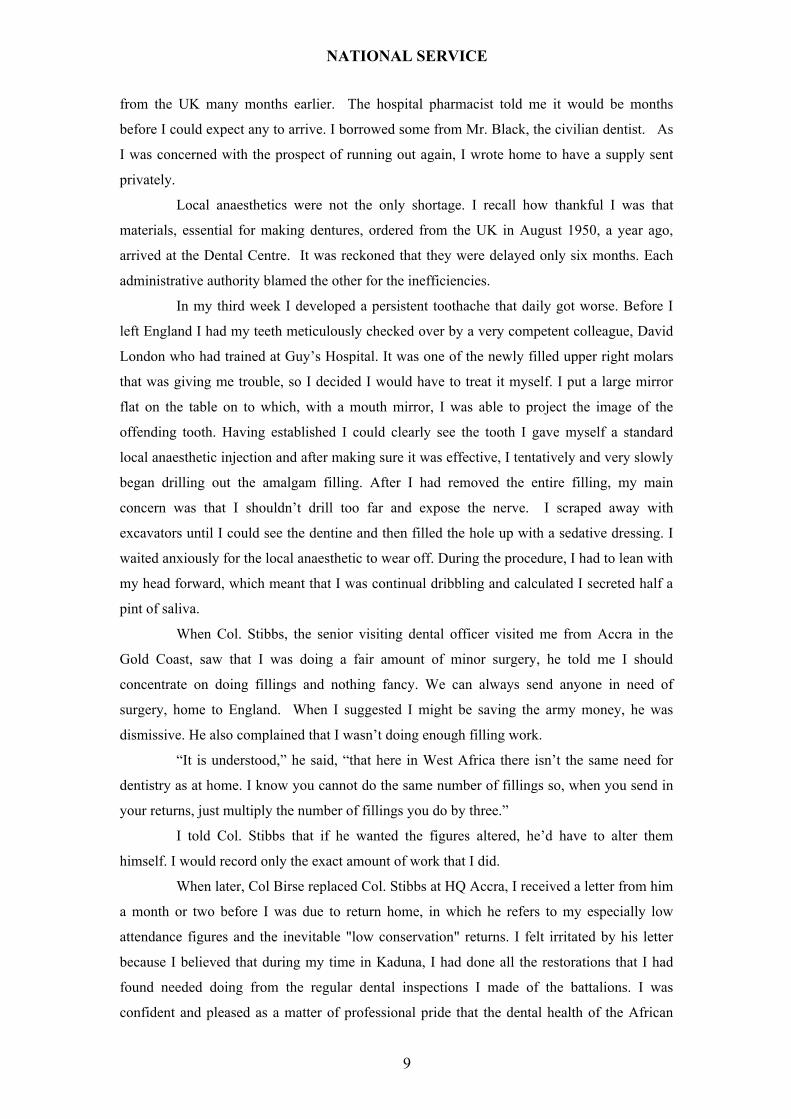
from the UK many months earlier. The hospital pharmacist told me it would be months
before I could expect any to arrive. I borrowed some from Mr. Black, the civilian dentist. As
I was concerned with the prospect of running out again, I wrote home to have a supply sent
privately.
Local anaesthetics were not the only shortage. I recall how thankful I was that
materials, essential for making dentures, ordered from the UK in August 1950, a year ago,
arrived at the Dental Centre. It was reckoned that they were delayed only six months. Each
administrative authority blamed the other for the inefficiencies.
In my third week I developed a persistent toothache that daily got worse. Before I
left England I had my teeth meticulously checked over by a very competent colleague, David
London who had trained at Guy’s Hospital. It was one of the newly filled upper right molars
that was giving me trouble, so I decided I would have to treat it myself. I put a large mirror
flat on the table on to which, with a mouth mirror, I was able to project the image of the
offending tooth. Having established I could clearly see the tooth I gave myself a standard
local anaesthetic injection and after making sure it was effective, I tentatively and very slowly
began drilling out the amalgam filling. After I had removed the entire filling, my main
concern was that I shouldn’t drill too far and expose the nerve. I scraped away with
excavators until I could see the dentine and then filled the hole up with a sedative dressing. I
waited anxiously for the local anaesthetic to wear off. During the procedure, I had to lean with
my head forward, which meant that I was continual dribbling and calculated I secreted half a
pint of saliva.
When Col. Stibbs, the senior visiting dental officer visited me from Accra in the
Gold Coast, saw that I was doing a fair amount of minor surgery, he told me I should
concentrate on doing fillings and nothing fancy. We can always send anyone in need of
surgery, home to England. When I suggested I might be saving the army money, he was
dismissive. He also complained that I wasn’t doing enough filling work.
“It is understood,” he said, “that here in West Africa there isn’t the same need for
dentistry as at home. I know you cannot do the same number of fillings so, when you send in
your returns, just multiply the number of fillings you do by three.”
I told Col. Stibbs that if he wanted the figures altered, he’d have to alter them
himself. I would record only the exact amount of work that I did.
When later, Col Birse replaced Col. Stibbs at HQ Accra, I received a letter from him
a month or two before I was due to return home, in which he refers to my especially low
attendance figures and the inevitable "low conservation" returns. I felt irritated by his letter
because I believed that during my time in Kaduna, I had done all the restorations that I had
found needed doing from the regular dental inspections I made of the battalions. I was
confident and pleased as a matter of professional pride that the dental health of the African

NATIONAL SERVICE
10
soldiers for whom I was responsible, was well under control. I was never once called out for
emergency treatment during my whole 18 months in West Africa. However, I could not
guarantee the same for the European military personnel, as it was mainly left to them and their
families to decide if they wanted treatment from me. Col. Birse wrote as follows:
I am new to this Command and am completely ignorant of local conditions and your
trials and tribulations, but I do ask you to do your utmost to step up these figures for fillings, it
will ease my burden somewhat and avoid some adverse criticism from the powers that be. It
may give you a lead to tell you that the other Dental Centres have brought their monthly
averages to over 100 conservations. To be perfectly frank, I see no reason why a daily average
of six fillings should not be maintained for every working day.
Anyway, do your utmost to increase the output. I regret having to make these
observations & especially so soon after my arrival, but I can assure you it is not from choice -
I get the unenviable task to do & must just do it.'
I wrote an immediate reply to explain why I was not able to increase the number of
conservations because I had already completed all the treatments that I had discovered were
needed. I could do nothing to persuade this officer that I had worked my best to look after the
dental health of those for whom I was responsible. By this time my eighteen months in
Nigeria was drawing to a close and I decided not to waste any more time justifying myself to
him. I later learned that when Col. Birse visited Kaduna after I had returned to England, my
regular army colleague, Fletcher Martin helped to give him a balanced view of my activities.
Unexpected Experiences
It is difficult to realise how monotonous our daily lives could be and what we were
prepared to do to break the routine. I never imagined that I could be persuaded to watch a post
mortem being performed by Keith, our consultant Medical Specialist, but I was. Basil the
Family medical Officer suggested at 4.15 p.m. that I should accompany him to see how Keith
was getting on and to ask if he needed any help. An African corporal had died at 2.30 p.m. of
suspected cancer of the liver. By 4.00 p.m. Keith was carrying out a post mortem. The
hospital mortuary was about 200 yards from our gidas. There were two entrance doors, one
marked African mortuary and at the opposite end, one marked European mortuary. So, even
in death, though most of the Africans were Christians or Muslims, the colour of our skins was
still important. We went into the African mortuary to find Keith working on the body with
two Africans looking on. Another African was tidying up and a B.N.C.O. Pathology
technician was assisting.
One of the Africans was a sergeant, a teacher, who had come to observe. The
pathetic look in his eyes recalled my own first visit to the mortuary at Guy's Hospital. I felt
then very much as he looked now. I hoped that he would see more post mortems and learn to

NATIONAL SERVICE
11
dissociate a human personality from the body that was being dissected before him.
One afternoon Keith warned me that he might want help in the operating theatre.
Basil was out on a call. He came back so there was no need for my assistance. Nevertheless, I
decided to familiarise myself with the routine. The theatre was large, with an adjoining
washing up or sterilising room. Petrol burners heated the sterilisers, not electricity as in the
Dental Centre and, I assumed this was because of the unreliability of the Kaduna electricity
supply. The anaesthetic machine was very primitive but adequate. The lighting and the
operating table looked functional.
A patient, a man about 40 was already on the operating table when I arrived. He had
been climbing into a lorry when a jeep pulled up too late, and crushed him against00 the
N.A.A.F.I. (Navy, Army, Air Force Institute) shop wall. He was now lying awake on the table
breathing very rapidly and occasionally saying something. I assumed, thou0gh I did not know,
that he was pre-medicated. He did not seem to feel the needle bein00g1 inserted into his vein
for the saline drip. It had been decided to open him up to inv1estig10at0e for a possible
perforation with a now superimposed peritonitis. At this stage I had en0ough and went to sit
out on the veranda steps.
I returned to the theatre to find that the patient's breathing had become irregular and
then Keith warned that he thought it was the end and within a minute or two the patient was
dead. There was a sudden silence in the theatre and the brake was released from the wheels of
the operating table. It was decided to do an immediate post mortem and so, after a slight
pause, we all made our way to the mortuary for the second time in three days.
There were other occasions when I was caught up in the professional anxieties of
my medical colleagues. We awoke one day knowing that two lives were at stake. The
condition of a B.N.C.O. from one of Kaduna’s battalions who had encephalitis was gradually
worsening. The other sick man was an African soldier with kidney failure. The health of these
two men was entirely in the hands of the National Service doctors and surgeon. They were
questioning among themselves why it was that they cared so much if they lost the B.N.C.O.,
but could not think the same way about the African. They concluded that it was a culturally
driven concern. Both soldiers were equally competent at their jobs. To my knowledge, there
was no senior regular army officer with whom they could share their anxiety. The CO, though
medically qualified worked as an administrator and rarely did any clinical work.
At 12.40 p.m. the B.N.C.O. was dead, by 1.30 p.m. his post-mortem was started, and
I was asked to write up the mortuary record. What had been a human personality, with all its
vast and variable reactions, was now just an object to be examined by the dispassionate
searching eyes of a pathologist. I can never understand how it is possible to harden oneself,
but one does: there is a dead body and the cause of death needs to be established. We spent
just under three hours in the mortuary with each body part being carefully examined and

NATIONAL SERVICE
12
where abnormality was found, a portion was put aside for microscopic examination.
One of the most traumatic experiences that could occur to an anaesthetist happened
while I was in West Africa. In one week, three Africans died under general anaesthetic. The
trilene used as the anaesthetic had degraded in the hot climate. We were all devastated by the
accidents. I am sure if the patients who had died, had been Europeans, there would have been
sensational headlines back in the U.K., but they were Africans. I wondered how the Africans
perceived these events.
Africans have their own array of diseases that, in the fifties, would have rarely been
found outside Africa. There were many unusual parasitical infections, which had specific
cures. We were always being alerted about bilharzias, a tropical flatworm, which was caught
from elements in its life cycle getting into water from where they could penetrate human skin.
There was another worm, which could grow several inches long. Every day it had to be drawn
from its location by rolling it slowly round a thin stick, which after every turn was re-affixed
to the skin by elastoplasts.
During my time in West Africa, several Europeans had what were called nervous
breakdowns or were on the verge of having one and would be sent back to England or in army
terms “boarded home”. There was one young National Service officer who had been
hospitalised in the European ward because of some bizarre episode. I remember listening
incredulously to him telling me how he had ordered a boat from England and was planning to
return home via Sahara underground waterways. He showed me maps where the waterways
were. He was so very convincing, I thought how interesting it would be to accompany him!
While I was in West Africa, I met several men who for one reason or another should
not have been posted to Africa. Obvious human considerations appeared to have been
overlooked. Never was this more tragically revealed than in the case of one National Service
medical officer with a reputation as a successful musical composer whose works had been
played in Liverpool. He arrived in Kaduna as if he had been totally unprepared for service
life, yet alone conditions in West Africa. For some never explained reason, he had even
missed the six weeks introductory course at the R.A.M.C. depot. It was suggested that this
was because he had an influential friend in the R.A.M.C. who was keen to help him remain in
a congenial environment near where he lived so that he could continue composing.
To my shame, one afternoon, when he wanted to talk, I was impatient with him
because I had al0ready found him a very demanding person. I broke the unspoken
understanding we had among ourselves that if anybody wanted to talk, one of us would listen.
A day or two later, the medical officer was called at the usual hour by his personal boy, but he
could not wake him. Capt. Lewis was called and alerted us all. The doctor’s gida door was
locked with the key in the keyhole. We got hold of a long cane to get the key out of the lock
to open the door from the outside. He was in a deep sleep and was raced over to the theatre to

NATIONAL SERVICE
13
be stomach pumped. An hour or two later Peter came back to tell us that he had died and it
looked as if he had taken his own life with a drug overdose. Later, a note was found to
confirm it.
There was the question of whether or not he should be buried in consecrated ground.
We awaited the coroner's verdict so the clergy could make a decision. Such refined
considerations seemed totally irrelevant to me. Bury the poor chap I thought, but without any
suggestion that the taking of his own life was an offence. I went to the funeral, as did most of
the officers on the station. The medical officer’s coffin draped by a flag was carried on a gun
carriage and he was accorded full military honours. When the gun carriage drew up at the
church door, there was a delay while the military photographer took several photographs. I
remember a brigadier who was standing near me say, "At least his parents will know we
buried him with full military honours.”
Other Responsibilities
Compared with the medical staff who were frequently called out at night and at
weekends, most of my responsibilities were during routine working day. For that reason it was
understood that the dental officer should be given other things to do, which I mainly accepted
and carried out.
One Monday, Part II orders, which gave instructions for the hospital staff and which
were displayed on a notice board, required a B.N.C.O and me to organise a PE test for thirty
or more African men of all ranks. I was reminded of my responsibilities first thing in the
morning by the B.N.C.O. sergeant enquiring what time we would assemble. We decided on
five o'clock and when I arrived at the ground, somebody had already marked out an 8-foot
long jump and 2 foot 6 inches tall, high jump. We lined the men up and carefully told them
what they had to do. The men jumped in turns. Towards the last of the jumps I thought I
recognised amongst them similarities with the familiar figures of my own school sports and
school gym: some were the very agile, others clumsy and incompetent. Their delighted
giggles when a jumping style was comical or a man failed to get over the jump were more
reminiscent of a third form classroom than soldiers in the army. After we had finished the
jumps, the men were lined up for a route march: officially it was laid down that 5 miles
should be walked in 1 hour. After half an hour I turned them round, assuming we had
completed two and a half miles or so. I was amused when they made the return journey in half
the time! The marchers sang as we went along. Usually one or two of them struck up a song,
which was followed by an answering chorus from the rest. The songs were familiar English
ones with only a few African songs, which seemed to be wordless, appearing to have rhythm
from repetition of a few notes.
I was appointed “Chop Master”, responsible for supervising the Officers’ Mess cook

NATIONAL SERVICE
14
and arranging the daily menus and assuring extra food was bought with money subscribed by
the mess members, so that we had a more varied diet than army rations alone allowed.
One day, I discovered from Part 1 Orders posted on the notice board that I had been
listed to take my turn on the rota with the B.N.C.Os. to supervise the care of a psychologically
disturbed African soldier. The man had to be forcibly restrained after, as the term was, he
went “bush”, meaning mad and started firing a gun off in all directions. I went to see the CO,
Col. McNeil and told him that I had no training in supervising mentally disturbed patients and
that it would be inappropriate for me to take on the responsibility. He told me that I would do
as he ordered. I told him that as the only dental officer in the command, I was there to look
after dental emergencies, and said that my responsibilities must first be towards any potential
patients, those for instance, I said, who might have broken jaws, choosing carefully the one
emergency that most doctors didn’t know how to manage. I was very polite and very firm, and
having had my say, left, imagining that would be the end of it - but no!
Later that day I was called to the CO’s private house, which adjoined the mess. He
looked out from his upstairs bedroom window, telling me that I was to be responsible for the
disturbed African. I said no I would not be, and repeated my arguments. Whereupon, he began
to shout and rage at me. When he had quietened down, I said that it had been made quite clear
to me in England before I came to West Africa what my responsibilities were to be and, one
of these, was always to be available for emergencies. I said that if he insisted that I went on
the rota, I would send a signal to the Deputy Assistant Director of Dental services in Accra, to
seek guidance. On hearing this Col. McNeil nearly fell out of the window gesticulating and
shouting at me, so I just walked away and left him. When my friend, Keith Henley, saw me,
he said I looked very white and angry and he seemed surprised I was so adamant in insisting
on my point of view. I anxiously awaited events. I assumed the CO sent a signal seeking
guidance on the limits of my responsibilities. I felt an important issue was at stake,
recognising that the moment I agreed to do open-ended non-dental tasks, there would be no
limit to the other demands made upon me and my successors. In a sense, I felt as the sole
representative of the R.A.D.C. with no immediate senior officer to whom to appeal that I had
to speak up. In the end I heard no more about the matter. Col. McNeil never admitted that he
might have been wrong but he did not forget.
One of the more asinine activities that army officers indulged in were "mess games",
the kind of high-spirited activities that adolescents enjoy. Even the Military Hospital mess had
on occasions to have a mess games night, usually when we were acting host to visiting
Regulars Army officers. On one of these occasions when Col. McNeil joined in the evening's
entertainments, we were arranged in teams and I was the third man locked in a column that
had to snake itself forward to the finishing line. Col. Mc Neil was two places behind me, a
fact I discovered when suddenly I felt a burning pain on the side of my neck, and looking

NATIONAL SERVICE
15
round saw the CO's outstretched arm with a lighted cigarette in his hand. There was nothing
that I could do and I just thought to myself what an idiot! Not long after we were involved in
another game and we had to crawl through a tunnel of legs. When I emerged from the end of
the tunnel, the CO was standing ready with a glass of whisky, which he sloshed into my face.
I was completely taken aback. Subsequently I’ve been assured by my retired Regular Army
friend that on a mess games night, I would have been in my rights, to slosh whisky back into
his face, but it would be the last thing I could imagine doing. My friend also thought that if I
had been in the wrong about my responsibilities, I would have heard a lot more about it.
Itinerant Dental Officer
As well as looking after the dental health of the battalions in Kaduna, I was
responsible for the R.W.A.F.F. training battalion at Zaria, 50 miles to the north by road and
the battalion stationed in Enugu about 400 miles away to the south by train. There were
between 800 to 1000 African soldiers and 30 European officers and B.N.C.Os. at each centre.
The big challenge we had was to take all the moveable dental equipment except the heavy
adjustable dental chair from Kaduna with us when we visited these battalions. We, also, took
along an old fashion pedal drill in case of a power failure. If I had to make dentures, we took
all the processing equipment as well. Cpl. Sylvanos Oko very competently, with the help of
Pte. Akujuobi, made sure everything was packed and I don’t ever remember anything being
overlooked.
I travelled to Zaria in the cab with the driver of a three-ton truck, with Sylvanos and
Akujuobi, with the dental equipment in the back of the truck. As we travelled northwards out
of Kaduna, the Macadam road ended and was replaced by a sun-baked clay and laterite
surfaced road, which caused, as we drove along, a long pinkish plume of dust to trail behind
us. For a few miles out of Kaduna the road was quite well maintained but the further we went
from Kaduna, the more it deteriorated and then, as we approached Zaria, it began to improve.
The road incongruously had all the familiar English traffic warning signs such as dangerous
bends. We crossed several small streams on single lane traffic bridges, which looked as if
they were temporary structures.
As we travelled north, the scenery imperceptibly changed, the trees that had
survived the bush fires were larger and there were many more termite anthills. They were all
shapes and sizes: short and tubby, large and fat, tall and shiny and small and shiny. They had
an irregular 4' to 6' wide base and could be 6' or more tall and looked to me like the kind of
city that would be found in the world of fairies.
On the approach to Zaria the road skirted round the old walled town. The wall,
which is a quarter to a half-mile in length, was constructed of mud, which, in many parts, had
crumbled away. Today, Zaria is a picturesque town occupied by the Hausas, ruled over by an

NATIONAL SERVICE
16
Emir who lives in a substantial palace. We drove past the European trading centres and after
a short journey came to the officers’ mess where I was allocated a circular mud bricked
walled building with a thatched roof and all modern conveniences.
In the time available it was impossible to check the dental health of 800 men with
the usual 20 minutes needed to make a proper examination. Even sitting a man in a dental
chair, adjusting the headrest and the light to look in his mouth and updating his dental chart
would take at least ten minutes. I soon realised that Africans very rarely had decayed or
missing teeth of the kind that prevailed in the Army in the U.K. and their teeth were usually
perfectly aligned and worn down, so that it was very easy to see any evidence of decay. So, I
devised a very simple procedure for examining the African battalions with the maximum of
speed and efficiency, which made sure that any serious dental problem was quickly identified
and treated.
The companies of the battalions were paraded in turn. I stood on a raised platform
wearing an operating gown and with the sun behind me. Sylvanos arranged for each soldier to
step forward in turn. When they stopped in front of me, they opened their mouths and with
two clean mirrors, I retracted their cheeks, and looked first round the lower teeth and then the
top ones. If any treatment was necessary, it was immediately obvious and I would call out to
Sylvanos what had to be done and the soldier was given an appointment to be treated by me
later.
On one occasion when I was doing a battalion dental inspection, the soldiers as they
stepped forward in answer to their names stamped their boots into the ground and swung their
arms into a smart salute, raising a great cloud of choking dust. I had to tell Sylvanos to stop
them and when they still persisted in saluting, I told him to tell them that the next man who
saluted me would be put on a charge! In all my time in the army I never did put a man on a
charge. I examined all the European personnel by separate appointments and treated them
immediately.
On one of my visits to Zaria, I went with the MO and a visiting French officer from
Port Lamis in an army utility van with an African driver to the walled city of Zaria.
Apparently this wall, which gave the place such an air of antiquity, was completed in 1880. It
had been constructed of sun-baked clay. After passing through the main entrance, we travelled
nearly a mile along a road with extensive sugar cane cultivations on either side before we
came to the town itself. We went into the market and got out to walk.
All types of food could be bought from young boys walking around carrying bowls
or trays balanced on their heads. Older boys and adults had their wares set out on rush mats
b0efore them. A section of the market was set-aside for the women and their goods. In another
part of the town we found a series of shallow wells in which a dark blue dye had been
prepared for colouring cloth. Wherever we went there were children of all ages running at

NATIONAL SERVICE
17
our heels, shouting and laughing.
It started to pour with rain and as we made our way back in the van, I noticed a
strange character standing quite alone in the middle of the market, quite oblivious of the rain.
He started to move towards us with a strange shuffling gait. His ankles were chained together
and the chain was joined to his hands. He came up to us with a vacant and harmless
expression on his face. He was mentally handicapped and our African driver explained that
there were no lunatic asylums in Nigeria so all mentally handicapped people were chained in
this way. On another occasion I saw a mentally disturbed woman wandering round naked and
unrestrained.
The furtherest battalion I had to visit was in Enugu, 400 miles or so to the south of
Kaduna. I received orders from Headquarters in Accra to undertake a dental inspection and to
take with me Sgt Tapp, the dental technician. He was a very skilled craftsman who single-
mindedly got on with his work. He was an independent and uncomplaining character.
Though Lagos, where the other dental officer in Nigeria was stationed, was only
250 miles west of Enugu, it was easier for me in Kaduna to travel by train the about 400 miles
south to Enugu. This can be best understood by looking at a map. The Niger flows diagonally
northwest to southeast between the lower one third and upper two thirds of the country. There
is no direct west to east road or rail link from Lagos because of the Niger delta, which
stretches nearly 300 mile along the coastline with numerous small tributaries flowing 50 or
more miles to the coast. A traveller from Lagos would have to travel north by train to Kaduna
crossing the Niger at Jebba and then take a train south from Kaduna to Enugu, crossing the
river Benue, a wide tributary of the Niger, at Makurdi. Where else in the world would you
have to travel 900 miles or so to link two coastal towns, which are only 250 miles apart?
We arrived at Kaduna station to find a very large and quite old looking steam train
waiting. Our nine crates of dental equipment had already been locked away in the guard’s
van. Sgt Tapp and I were to share a compartment and after we secured our tickets and seen all
was in order, we settled down for the 36-hour train ride. Sylvanos and Akujuobi had “seating
only” reservations on the train and yet thy needed to be as fre0sh and alert as I was to organise
the work when we got to Enugu
The compartment was similar to that found on an English sleeper train with bunk
beds. The windows were of dark glass and could be raised or lowered at will. For night use
there was a moveable wooden shutter with vents. By adjusting the window and shutter the
compartment temperature could be conveniently controlled with the help of a fan.
We stopped at stations throughout the night and I awoke to the chattering and
laughing of passengers talking to pass the time. We arrived at Kafanchan junction, 100 miles
to the south of Kaduna at 6.30 a.m. where we had to wait for three hours. It was a long time,
but I had already accepted that life went along at a slower pace in West Africa.

NATIONAL SERVICE
18
While having breakfast, I watched a constant trickle of men women and children
walking along the railway track with their loads of bananas, wood, yams and other vegetables.
They were very variably dressed. Some of the women who were pagans from the plateau
round Jos, wore only leaves held by a thong in front and a woven mat or an 18" long tail of
grass behind. Sometimes they wore both.
The train set off again at 9.30 just as we had finished breakfast, and Kafanchan
faded in the background. The scenery changed very slowly until we saw hills far away in the
distance. At times the train, barely moving faster then walking pace, climbed very slowly and
circuitously up into the hills. There were palms and banana trees, especially where there was
water, which were a welcome addition to the scenery. Birds were surprisingly rare, frightened
away by the noise and rumbling of the steam train, but on one occasion I saw a magnificent
red coloured cardinal bird.
We reached Enugu at 4.30 a.m. but we were not wakened until five for tea when we
were told that we had to wait until 6.30 before the train went off on its last lap to Port
Harcourt. It had been an extraordinary day and a half journey travelling, but I found that it had
passed rapidly and easily.
The battalion is located in a magnificent site overlooking a valley. The mess and the
MO's gida, which I shared with him, were superbly situated. I noticed what a large variety of
unfamiliar butterflies there were and how profuse were the flowering shrubs. Some had large
red horn shaped flowers and others bright yellow bellflowers. I was very happy and contented
that evening as I gazed over the wide basin-like valley to the hills three or four miles away.
At night in Enugu I heard a rhythm being played on an instrument that sounded
closely allied to the English xylophone, which every now and again was interrupted by a mass
beating of drums.
I had nine days in which to examine 900 men and carry out any treatment, so my
professional routine at Enugu was considerably different from that at Kaduna. I started work
punctually at 7.0 a.m. and hoped to have completed all the necessary inspections and
treatments by 9.0 a.m. when I joined my fellow officers for breakfast. By 10 o’clock, I was
down at the Medical Inspection room again, a half-mile walk from the mess and worked
through to lunchtime. I gave up my routine afternoon siesta and treated patients for an hour
and a half to two hours. The fact that I recall this, suggests that life must have become very
leisurely in Kaduna for R.A.D.C. officer Brown.
I never expected to visit the Gold Coast (Ghana) but Col. McCarthy, the chief dental
officer in army headquarters in Accra was suddenly taken seriously ill and flown home, and I
was transferred from Kaduna to replace him for a few weeks. In Accra there was some routine
dentistry to be done and examining of dental technicians for their trade tests. I was ordered to
undertake dental inspections of the battalions in Kumasi and Tamale, which hadn’t been done

NATIONAL SERVICE
19
for some time. I treated several European personnel who told me how difficult it had been to
get an appointment under Col. McCarthy. It was rumoured that he earned as much as £7,000 a
year in private practice. The trip was an unexpected bonus and helped to break the monotony
of my routine life in Kaduna.
One of the most striking buildings to be seen outside Accra overlooking the sea was
Christiansborg Castle, built by the Danes in the 17th century. It was a reminder of how, with
the discovery of the West African coast by the Portuguese in 1471, the land trading routes
across the Sahara gave way to the more accessible sea routes. The British bought
Christiansborg Castle from the Danes in 1850. It must have been an impregnable fort built on
the edge of the sea with a shaded courtyard and veranda facing to the north.
Accra was an important trading capital, but without a natural harbour. Ships
bringing imports anchored a mile off shore and loading and unloading was done by local craft.
The large skiff like boats were paddled out or sailed from the shore to bring the freight to
land. The men who manned these boats had very powerful physiques. Such primitive means
of unloading the ships necessarily restricted the nature of the imports. The port at Takoradi
and the more recently opened port at Tema will have dramatically influenced the trading
opportunities for Ghana.
Kumasi, 150 miles inland and north west of Accra, was the capital of the Ashanti
people. We travelled by train on a single-track line with selected places for trains to pass. The
track curved and climbed up from the coast and must have been quite an engineering feat to
build.
The officer's mess in Kumasi had been built specially by Prempeh, the last king of
Ashanti, for the Prince of Wales, the future Duke of Windsor’s visit in the twenties. It had
been built on top of 15-foot high concrete columns, leaving the ground level completely open
for the circulation of air. Medical opinion of the time was that this was the healthiest type of
building to minimise catching any of the dreaded fevers. The entrance to the building was
approached by a rather grand stone stairway, which led up into a substantial hallway.
There were back steps to the mess where walking towards them one morning, I was
confronted by a small green snake that had raised its body 9" off the ground into a
characteristic strike position. I carefully avoided it. I never discovered what species of snake it
was and whether its bite would have been fatal. People were very afraid of snakes and it was
reported that forty or so people a year died in the whole of British West Africa out of a
population approaching a hundred million people, but a moment's pause makes me question
that figure. Some parts of Africa were so remote, there would be little chance of a death from
a snakebite being reported.
I was in Kumasi during a bank holiday weekend and the mess was deserted. I had no
idea where everyone went. I settled down undisturbed and totally contented but must have

NATIONAL SERVICE
20
been mentally alert, as I was able to read the whole of Dostoevesky's Crime and Punishment.
Not far from the mess was a tropical grove where I discovered large and exotic
butterflies, reminding me of a Henri Rousseau tropical painting with a lurking tiger and a
coiled python. Someway to the south of Kumasi was a lake that looked as if it had once been a
vast opening to a long inactive volcano. It was described as a sacred lake and it was alleged
that all sorts of ritual activities took place, but I had no chance to look around for any
evidence of them. The basis for these frightening stories was the well-authenticated stories of
human sacrifices associated with the Ashanti kings whose authority was symbolically
represented by the golden stool, which was thought to contain the spirit or soul of the Ashanti
people.
Kumasi had a most unusual red brick fort built by the British in 1897. Many years
later, I learned that it had been designed and built by my father-in-law, Lt. Col. Charles
Vesey, who was in the Royal Engineers at the time of the Ashanti wars.
I travelled the 250 miles from Kumasi to Tamale in a 3-ton army truck. It was an
uneventful journey, apart from the crossing of the river Yeji by ferry and the driver quenching
his thirst with a pineapple. Once we were out of the tropical lushness of Kumasi, there was
nothing but shrubland with decreasing numbers of trees the further north we went. To relieve
my boredom, I persuaded the driver to let me drive. He was very reluctant to do so, as it was
against army regulations. We were always told that more officers were killed driving
themselves than from any other cause.
Tamale was one of the few towns of any size on the main road to the north east of
the Gold Coast. It appeared to me in 1952 as a remote small place. A battalion was stationed
here and I wondered what possible function it could serve. The atmosphere in the mess was
very tense. The regular officers sat at one end of the long communal table and the National
Service officers at the other. The medical officer and I sat between the two groups and were
able to talk to both. The clearly expressed view by some of the regulars was that they had
served their time in the war and now it was the turn of the National Service officers to get on
with the job. Some of the officers I met were seriously demoralised. My memory of Tamale's
mess is dominated by the drinking habits of some of the regulars. The station began its work
early in the morning, and by eleven o’clock most of the day's scheduled work was completed.
During the coffee break, several of the regular officers ordered their first gins, and one of
them, as soon as he had finished his drink, ordered a bottle of gin from the mess steward and
went off to his living quarters. We would not see him again for the rest of the day unless there
was a special function for him to attend. The medical officer said that before his coming to the
station, one officer had died from, and another had been very seriously ill with alcohol
poisoning. The previous medical officer had had a substantial thirst for beer and had
decorated the borders round the garden in front of the medical centre with empty beer bottles.

NATIONAL SERVICE
21
Though there were many intelligent and competent regular officers, there was a
general belief that some of them had been posted to West Africa because of some unspecified
misdemeanour and I met some who did not conform to the ways of a traditional British
officer. But there was also a feeling among some of the regulars that having to command
natives was an improper use of their skills and they very much resented their West African
posting.
The reservoir near the battalion's compound was home to some small crocodiles,
which could be seen at the water's edge. They grew to a couple of metres in length. Once a
year these ungainly looking creatures would move from the reservoir to an alternative pool on
the far side of the army compound, walking straight past the officers' mess to get there. It was
one of the big events of the year.
Tamale had few distractions. There was only the army there and there was very little
for them to do. I walked out occasionally, but it was only through the familiar bush in which
there were a few trees and shrubs and occasionally I would see an African village in the
distance. I saw a few farmers, but I never made any contact.
The African soldiers I treated had ready access to their own medicine men. On
several occasions they had complex attachments of wood and leather bound to their arms,
which were described to me as ju-ju to fend off some evil. At first, I was incredulous as to
what they believed, but in retrospect I am sure that many Africans might have found the
prevailing Christian beliefs equally incredible. Perhaps more surprising was the army's
readiness to allow the men to wear these intricately made constructions.
I was flown back with six others from Tamale to Accra in a light aircraft, which had
a coffin lid shaped door into the pilot's cabin, which caused me to smile sceptically to myself.
Nobody else seemed to notice, so I lived with my private fears of what it so aptly symbolised.
We landed at Kumasi to pick up passengers and to have a short break, when suddenly the pilot
looked out of the small hut, which served as the airport lounge and seeing huge black clouds
rapidly massing overhead, anxiously ordered, "Hurry up everyone, get back to the plane as
quickly as possible. We want to get out of here before that storm is upon us." We all ran, as
fast as we could, and for me significance of the cabin door's shape, became even more real. I
did not relax until we landed safely back at Accra.
Leisure
In England I avoided routine sports and at weekends confined myself to sailing
leisurely along the English coast, but in Kaduna I regularly played tennis with my colleagues
and subsequently played in the hospital hockey team against other Kaduna teams. I’m sure
these games played an important part in providing a competitive stimulus in the rather
confined and claustrophobic environment in which we lived. For me, participating in sports

NATIONAL SERVICE
22
was a way of life in West Africa. They compensated for my unexpected inability to
concentrate on reading and failure to remember what I read. I never found a satisfactory
explanation for this blank minded state but concluded that the brain had a way of lowering its
energy output to match the level of stimulus to which it was exposed.
Early on I had decided that I should participate in some major sporting activity and
polo seemed to be an unusual and promising pastime. However, I found it would be very
expensive but more to the point, one needed to have pretensions to a certain social style,
which I did not. Above all, I realised that to play polo, you needed to be a dedicated
horseman, which I was not.
However, several of the hospital staff had bought horses for casual riding. When
Ebony, one day, was brought round for Keith, he did not want to ride the animal and
suggested I should. I took him out beyond the area where the African soldiers and their
families lived. The road narrowed down to a single track along which walked an intermittent,
but endless, stream of Africans. The path curved and wandered between cultivated fields.
Some of the crops like guinea corn were 3 metres or higher reaching higher than myself
sitting on old Ebony's back. Other crops were trenched, very like potatoes. Hardly any
Europeans knew the names and, to explain why not, they would say, "The African doesn't
know nor does he care," which of course was nonsense.
After a half-mile or so I came to small settlement consisting of a cluster of mud
brick huts completely surrounded by a wall which, where it was not formed by the walls of
the huts themselves, was made of a high fence of dried guinea corn stalks. There were many
African men and women around and we exchanged smiles and greetings of ‘Sannu, Sannu’. I
continued along the path for a while beyond the village until I came to a stream, which Ebony
was reluctant to enter and, through which I would not force him, as it was very deep.
On one occasion in the cool of late afternoon, I played football at a small township
on the way to Gusau. The local football team had challenged the army. There were five
Europeans in our team and the rest were Nigerians, many of whom were natural athletes. The
whole town turned out for this spectacle. I had never played football seriously, but the
enthusiasts in our team overlooked my ignorance - just keep kicking the ball towards their
goal was their simple and repeated encouragement. We began to play in the latter part of the
afternoon. I cannot remember when I had last run so much. I was totally out of condition, but
what I remember more than anything about this game was that at half time when the whistle
blew, I was completely exhausted and simply sat down where I was on the dusty ground.
Immediately the townspeople of all ages surged on to the pitch and surrounded each of us,
staring down in amazement at our overheated reddened and sweating bodies. I felt as a fly
must feel when a hundred termites have clambered all over him, determined to kill and devour
him.

NATIONAL SERVICE
23
We were able to play hockey at the hospital only because of the drive and energy of
Capt. Fletcher Martin, R.A.M.C., always known as “Marty”, who had joined us at Kaduna as
a hospital administrator. He was in his forties, a mature person who had risen in the regular
army from the ranks, which might explain his intuitive perception of the officer class. He had
a healthy contempt for the airs and graces of the regular officers from whatever branch they
came, but kept his contempt to himself, never letting it interfere with his sense of duty. He
said that if the senior officer of the garrison invited him to a reception, he would have pleasure
in refusing but, not surprisingly, his claim was never put to the test. The army was far more
divided by internal class distinctions than I had suspected. Marty knew more about the way a
medical unit should be administered than any of the medically qualified administrators and he
always suspected there was a hidden agenda in their decision making He was a humble man
of complete integrity who worked continuously to improve the conditions of service for
everybody. The British non-commissioned officers respected and liked him while the
incompetent ones among them recognised that in him, they had met their match.
He believed that if a soldier committed an offence, then, any punishment should be
in some way beneficial to the culprit. I suspect that was the driving principle of his life:
whoever had dealings with Fletcher Martin, would have their lives in one way or another
enhanced by his insights. His philosophy was based on his own experience of life. He was not
obviously a religious man and yet his overall influence for the good was far more effective
than many of the self-centred padres I met.
Sport was very important to him and we regularly played tennis together. He was
not only keen on playing sport himself, but wanted everybody to join in. He achieved the near
impossible task of organising the construction of a hockey pitch on an indifferent piece of
ground. He used compacted termite anthills to produce a flat hard finished surface, managing
to do so with the minimum of labour and in a remarkably short time. It was Fletcher Martin
who had us all enthusiastically playing hockey.
Our hockey matches with the other units became seriously contested affairs. The
Africans joined in and they quickly became expert players. They were very fast runners and
had a remarkable eye for the ball. I was astonished by their natural athleticism and at the time
did not realise I was watching a phenomenon, which is now universally taken for granted. Our
sporting activities were the most effective way to cut across both the rank and racial barriers.
Two episodes I describe from hearsay are hardly sport, more like distractions
invented to pass time and relieve monotony. Most officers' messes had formal monthly
dining-in nights at which everyone dressed in formal mess kit. It was usual, after the meal was
eaten and the toasts proposed and drunk, for games to be played, some of which were of a
very dubious nature. On one occasion one of the battalions in Kaduna used its regimental
memorabilia swords in mock duels among its officers, and one of the swords entered the

NATIONAL SERVICE
24
mouth of one of the participants, piercing his cheek. He was brought into see the duty MO
who stitched him up and the episode was hushed up. A riskier pastime, depending on your
point of view, was firing shotguns blindly at each other in the pitch black of night. The
contestants would fire at each other from behind sandbagged positions set thirty or more yards
apart. There were never any reports of injury. I am not even sure what one had to do to win.
All these activities helped to pass the time and to displace our basic feelings of
futility and to give a slight emotional edge to our daily lives, preventing us from becoming too
lethargic and incidentally keeping us fit, but as a 24 year-old, fitness was not something I
particularly sought.
I took an active part in amateur dramatics and played two small parts as a clergyman
and an American police officer in Arsenic and Old Lace, which was performed in Kaduna and
Zaria. Looking at the photograph of the cast of 19 people, I can recognise only Keith Henley,
Capt. Hart and a woman teacher who was memorably gauche, but very well intentioned. I
saved for some years a review from the local press, which acknowledged my contributing
cameos. We often read plays at other people's house, including that of Col. McNeil, who
always before the respectable colonials of Kaduna behaved very civilly to his staff even
praising me, one day, for my performance. Who would have thought that such a fine
gentleman should also have had a nasty abusive side to his personality?
I had been an enthusiastic classical film fan in London and so was reluctant to go to
a film, “Pretty Babe”, but went because all the others were going. I thought, My God! Have I
descended to this level already? And yet I enjoyed the film and recorded that “I laughed like
a drain”. Thereafter, I never missed an opportunity to go to any of the films on offer.
When you think of our cinema, don’t imagine a padded seat Odeon cinema with
slow dimming lights. We sat in director style canvas chairs supplied by the N.A.A.F.I.
(Navy, Army Air Force Institutes) under a corrugated roof. Outhouses flanked the sides of the
“cinema” and when the moon was shining very brightly, it was difficult to see the picture
clearly. When it rained the corrugated roof let in a constant stream of water leaving little
islands of space with no chairs. The continual loud beating of the rain on the metal roof, made
it at times difficult to follow the dialogue and the screen glistened as it became wet.
The regular visits of the traders around teatime were an invaluable distraction and
most of us, in our time in Nigeria, spent many happy hours haggling with them. I often bought
goods with the excuse that I was getting a bargain. One day a trader had brought a large
snakeskin bag, which had a rather coarse skin. There always seemed to be flaws: either a
perforation in the skin or signs of patching to make up for shortage of skin. Prices (Nigerian l.
s. d.) varied considerably and I am recording them here for future reference.
Two iguana bags 11" x 9" £2. 10. 0.
One snake skin 11" x 9" £0. 15. 0.

NATIONAL SERVICE
25
Another trader who came produced all his wares, but for one small package. We
persuaded him to open it and found some ivory necklaces. One, with graded beads, the largest
3/4" across and the smallest, 1/4", caught my eye and so I asked, but with no intention of
buying, how much. £2.10 was an emphatic reply. I laughed at the exorbitant price. However I
continued to regard this necklace, whilst Keith was haggling over the price of another. When
Keith had a moment, he mentioned it was well worth a quid. Our trader must have been
hungry this day because slowly, slowly he cajoled me into buying, by finally reducing his
price to £1 and then the deed was done.
Many of the traders were clever and well informed men. Mamantow was a
particularly friendly man who liked to share a view. He found for me an African bow with
arrows. It stood about 5' high, was made from unidentified wood and strung with a leather
thong. The arrows were contained in a sheaf of 3" diameter made out of a hollow piece of
wood. The arrows were interesting. There was a head and a shaft with no flights. The shaft
was of bamboo into which the head was fixed. The opposite end was slotted so that it could be
fixed into the thong. The head was of metal with a point with two barbs about 1/2" long, each
directed backwards at an angle of 30°, which if they penetrated the skin would make the
arrow difficult to withdraw. Mamantow could shoot surprisingly accurately with the bow. I
bought it. The friendly old trader persuaded me at the same time to buy a mat. It was a good
colour and I had no regrets. I had felt exhausted before the trader arrived and after a half hour
of chat and bargaining, my energies were restored.
Summary
When I arrived in the unfamiliar world of Nigeria, I had an insatiable desire to
discover all I could about the people and the country, which was so different from the
England in which I had grown up. I had plenty of time available to explore because in Kaduna
we worked only from 8.00 until midday. However, I was told everyone took an afternoon
siesta and that I would be wise to follow suit, but while others slept I wandered around, read
and wrote but slowly my capacity for being continuously on the go diminished and only when
I was away from Kaduna visiting new places did my energy return. I would again explore in
the afternoon when I was free while the rest of the European world was dozing. I
subsequently learned that several Europeans had wagered that because of my hyperactivity, I
would not last my eighteen months and that I would have to be sent home with a nervous
breakdown, as some of my colleagues were.
We all wondered why we felt so enervated. We attributed it to the weather: its
sameness, its humidity and its heat, depending on the time of year. We blamed the lack of
food for our lethargy, for we were disinclined to eat in the hot weather. I suspected the lack of
adequate mental stimulus slowed my brain down to match the unchanging environment in

NATIONAL SERVICE
26
which I lived. It was easier to play tennis or hockey or cards than read a book. From an early
ambition to read a lot, I was reduced to reading less and less and ever more slowly. It was an
effort to get through a Leslie Charteris “Saint” book.
During the last few months of my stay in Nigeria, I was exhausted and had an
insatiable desire to sleep. I would sleep during the afternoon and was ready for bed at 9.30 in
the evening and found it a struggle to get up in the morning. As the weeks passed, I became
increasingly passive and docile so, by the end of my stay, I would not have been surprised if,
in looking in the mirror, I saw a cabbage winking his eye back at me. Remarkably I was
totally at peace with myself and could have imagined myself sitting quietly in a chair all day
watching the world go by as if it was nothing to do with me.
I want to pay a special tribute to Cpl. Sylvanos O. Oko for the effective running of
the dental centre in Kaduna. He was responsible for the efficient running of everything to do
with dentistry and the army wherever I had to work in Nigeria. He was a very intelligent,
rather serious person on whom I totally relied. He knew exactly how the army worked and
perfectly understood what everybody was entitled to and what was expected of them. I cannot
remember ever having a disagreement with him. I used to receive signals from Accra
headquarters telling me when I was to visit the different battalions outside Kaduna and I
trusted Sylvanos implicitly to organise the clinics, and arrange tours for dental inspections in
Zaria or Enugu. He would make sure that everything that had to be done was done and, with
the minimum of fuss, exercising a quiet but firm authority. More than anyone he freed my
routine working day from the expected frustrations.
He was particularly good at liaising with his fellows, and few people under-
estimated him. Quite apart from his role as an army man, he was Sylvanos the very likeable
human being. I perceived him more as a friend than a non-commissioned officer whose
judgement I respected. In a letter many years later, when I wanted his opinion about some of
the events I have recorded in this manuscript, he was quite clear that as far as he was
concerned, he was the corporal under orders from Capt. Brown. He wrote, 'In those days it
was a master and servant relationship. We hardly sat together to talk about life in Nigeria -
worth putting in a publication of value' (letter 22-3-91). He must have been a few years older
than me. Sylvanos was, I imagine, largely self-educated. If he had had the same educational
opportunities as us, he would have succeeded in anything he chose to do. He never expressed
any regrets. I am sure he had views on all of us, but he was a man of the utmost discretion. I
am still in correspondence with Sylvanos who is now over eighty years old. He has ten
children and signs himself Elder S. O. Oko.
Sylvanos exemplified completely for me the way the Nigerian soldier, though
completely respecting the differences in rank so dear to the traditional British, was always
able, given the chance, to reflect his own personality. I suppose in a sense it was because the

NATIONAL SERVICE
27
serving African soldiers were largely free from the feeling of inferiority that so pervaded the
British "Other Ranks" at the time. Many of the recruited soldiers were sons of village chiefs,
but I am not sure if Sylvanos had any official status at home.
After leaving the army, he joined the civil dental service as a technician and, has
only recently retired. I kept up a correspondence with him over the years and in 2006 spoke
with him on the phone.
Pte. Akujuobi also of the R.W.A.F.F. worked with me in the Dental Centre under
the guidance of Cpl. Oko throughout my stay in West Africa. He shared completely in
ensuring that our unit ran smoothly and efficiently, He was also of great help when I went on
an extended trip into rarely visited areas near Enugu. He was around 24 years old and a very
friendly person. He was always much more than Pte. Akujuobi and occasionally expressed
himself in a way his fellow Africans would understand but which was outside accepted
behaviour for a junior ranking soldier. Happily we were able to settle together the difficulties
he experienced without his loosing face.
The RADC and the Army
The impatience the National Service dentists had with their Regular Army
professional colleagues arose because many of us had already held junior hospital
appointments in teaching hospitals in which we had gained an array of experience in the latest
and most successful clinical procedures. We were enthusiastic and rather proud of our skills.
We soon discovered that many of the senior regular officers in the R.A.D.C. who controlled
us were often unimaginative administrators. What clinical work they did do often appeared to
be to a minimal standard. I concluded that it was this minimal clinical standard that enabled
them to tolerate poor working conditions and inadequate equipment for their junior staff.
What was worse, they expected us to work effectively in this run-down atmosphere. All that
the senior officers, under whom I worked, were concerned about, was how many fillings or
extractions I did in a day and whether or not I was on time for duty, dressed in the right
clothes. They actively discouraged our giving more than minimal treatment to National
Service men whether they were officers or other ranks. I was told that they would soon return
to civilian life and would be the responsibility of the National Health Service. If they were
interested in enhancing the reputation of the R.A.D.C., they had no idea how to harness our
expertise and enthusiasm. We quickly concluded that many of the regular R.A.D.C. officers
were dentists who would not have succeeded in civilian life and had chosen the easy option of
a service career. Because of the obsession with the number of fillings we did, it seemed to me
that the Royal Army Dental Corps in West Africa had got itself into a mess by years of
inaccurate reporting back to HQ in England of the amount of work that was being done.
There simply wasn’t enough work to justify a full time dental officer in Kaduna. As it was, I

NATIONAL SERVICE
28
travelled to Zaria for three days at a time and Enugu for three weeks and to Lagos and then to
Accra, Kumasi and Tamale for three months. If I could be spared away from Kaduna for all
those weeks and there was no dental crisis in Kaduna, it suggests that the dental requirements
were greatly over-estimated.
However, as critical as I maybe about my experience of the army, I gained useful
professional experience, but more than that, I gained from my time in Nigeria an incalculable
depth of knowledge and understanding about a country and its people, which has proved to be
an invaluable model with which to compare and contrast the British way of life.
The Regular Army was not always happy with having to deal with the National
Service conscripts particularly the older conscripts like myself. There was no use shouting at
us. We quickly found that many of the Senior Regular officers had no idea how to exercise
authority and, unless we thought their orders relating to professional matters made sense and
were in the interests of the patients, we ignored them.
However, I had the highest regard for the professional knowledge and skills of my
R.A.M.C. and R.A.D.C. National Service conscript colleagues. I suspect that the Regular
Army greatly benefited from having the services of many highly qualified National Service
doctors who in ordinary circumstances would never have thought of choosing the army for a
career.
It was often the casual meetings with civilian professional people: the vets,
geologists, district officers and the commercial people, working outside the restrictive
ambience of the army, who were free to practice their profession and follow their interests,
that emphasised the restrictive cocoon-like nature of life in the army. This condition is
understandable when one remembers that soldiers are trained to deal with cataclysmic events
in which their rare skills can be deployed. If one did not belong to that world, it was difficult
to share their values and ambitions. I was mainly cushioned from this realisation because I
lived and worked with fellow National Service professionals who collectively helped to
sustain the illusion that the army was not really anything to do with us.
Conclusion
My time as a National Service officer in the army was in many ways a rewarding
experience, introducing me while in West Africa to a world that I had only known in fiction. I
am especially grateful to the many soldiers in the Royal West African Army Frontier Force
who taught me so much about their country. As a Dental Officer I gained broad professional
insights that helped me to decide my future career. My survival in the army was very
dependent on the give and take and understanding that existed between my fellow National
Service officers and to a number of career soldiers, to all of whom, I say, a very grateful
“Thank You”. I was fortunate to travel extensively and experience so much of the rich and
NATIONAL SERVICE
29
varied cultures of West Africa. I was blessed in Kaduna with many friends with whom I spent
many happy hours. Some Regular Army officers were very helpful, but some of the senior
Regular Army Royal Army Dental officers that I came across perceived dentistry in a
different way from me and it was clear that their career ambitions were very different from
mine.
6th March 2008

NATIONAL SERVICE
30
Subsequent career
After leaving the army I decided to specialise in Orthodontics, and was fortunate
to have junior appointments in the Orthodontic Departments of King’s College Hospital and
the London Hospital from 1954 to 1957. Between 1957 and 1959 I worked on a research
programme at the Dental School of the University of Illinois. On returning, I was appointed
as a Senior Lecturer in Orthodontics at Queen’s University where I worked until 1964.
From then until 1970 I was a Senior Lecturer at the newly formed Dental School in Cardiff.
In 1970 I left clinical dentistry and taught Dental Anatomy to dental students, at King’s
College, University of London. I retired in 1987. Over the years I have posted several
publications on my website (www.wabbrown.co.uk).

NATIONAL SERVICE
31