
Routine Ordering of Primary Pathology Examinations in Canada
15
1 Routine Ordering of Primary Pathology Examinations in Canada 1 Routine Ordering of Primary Pathology Examinations in Canada Issue 46 October 2014 Context Human tissues removed during a biopsy or surgical procedure are typically sent to a pathology laboratory for diagnostic examination and testing. The pathologist’s findings and diagnosis are documented in a pathology report, which is then made available to the requesting physician. Decisions regarding which specimens are submitted to the pathology laboratory for examination may be directed by established and/or documented procedures at the provincial and territorial, regional, or institutional levels, or by clinician judgment. Some tissues are routinely sent for primary pathology examination (i.e., an initial diagnostic examination) even if there is minimal or no suspicion of a clinically significant abnormality. For the purpose of this Environmental Scan, “routine primary examination” refers to one of two scenarios: when primary pathology examinations of human tissue specimens are mandated by regulation, protocols, policies, standard operating procedures, etc.; or in clinical situations (defined by a particular population, condition, setting, or tissue) in which treating-physicians routinely requisition pathology examinations that would not otherwise be directed by regulation, protocols, policies, or standard operating procedures, and in which there is minimal or no suspicion of a clinically significant abnormality. Experts have suggested that there may be suboptimal use of pathology laboratory resources related to primary pathology examinations. In the case of a mandated routine examination, there is concern that existing regulations or policies may not provide sufficient criteria regarding specimen types and clinical situations for which submission to the pathology laboratory is necessary. In the case of routine physician-driven pathology requests, the concern relates to the potential for the treating physician to misinterpret or to deviate from policies or guidance around when pathology examination is required. For example, requesting physicians may submit surgical specimens irrespective of documented policies or suspicion of abnormality because of concerns about liability, patient requests, or financial incentives. They may also be faced with organizational or time constraints that hinder greater selectivity in pathology submissions based on the level of clinical suspicion. Another issue voiced by pathologists for both routine examination scenarios is the potential for lack of clarity regarding the level or detail of pathology assessment required (for example, gross versus microscopic examination) when these tissue specimens are received. This Environmental Scan will attempt to shed light on current practices related to routine pathology examinations in Canada by examining existing legislation and policies, as well as a survey of Canadian pathologists. Objectives The objectives of this Environmental Scan are to describe the drivers of routine primary pathology examinations of human tissue specimens in Canada and to identify potential opportunities for optimization in this area. The Environmental Scan addresses two questions: 1. What are the Canadian regulations and policies for sending surgically removed human tissues to a laboratory for primary
Transcript of Routine Ordering of Primary Pathology Examinations in Canada

1
Routine Ordering of Primary Pathology Examinations in Canada 1
Routine Ordering of Primary Pathology Examinations in Canada
Issue 46 October 2014
Context
Human tissues removed during a biopsy or surgical procedure are typically sent to a pathology laboratory for diagnostic examination and testing. The pathologist’s findings and diagnosis are documented in a pathology report, which is then made available to the requesting physician. Decisions regarding which specimens are submitted to the pathology laboratory for examination may be directed by established and/or documented procedures at the provincial and territorial, regional, or institutional levels, or by clinician judgment. Some tissues are routinely sent for primary pathology examination (i.e., an initial diagnostic examination) even if there is minimal or no suspicion of a clinically significant abnormality. For the purpose of this Environmental Scan, “routine primary examination” refers to one of two scenarios:
when primary pathology examinations of human tissue specimens are mandated by regulation, protocols, policies, standard operating procedures, etc.; or
in clinical situations (defined by a particular population, condition, setting, or tissue) in which treating-physicians routinely requisition pathology examinations that would not otherwise be directed by regulation, protocols, policies, or standard operating procedures, and in which there is minimal or no suspicion of a clinically significant abnormality.
Experts have suggested that there may be suboptimal use of pathology laboratory resources related to primary pathology examinations. In the case of a mandated routine examination, there is concern that
existing regulations or policies may not provide sufficient criteria regarding specimen types and clinical situations for which submission to the pathology laboratory is necessary. In the case of routine physician-driven pathology requests, the concern relates to the potential for the treating physician to misinterpret or to deviate from policies or guidance around when pathology examination is required. For example, requesting physicians may submit surgical specimens irrespective of documented policies or suspicion of abnormality because of concerns about liability, patient requests, or financial incentives. They may also be faced with organizational or time constraints that hinder greater selectivity in pathology submissions based on the level of clinical suspicion. Another issue voiced by pathologists for both routine examination scenarios is the potential for lack of clarity regarding the level or detail of pathology assessment required (for example, gross versus microscopic examination) when these tissue specimens are received. This Environmental Scan will attempt to shed light on current practices related to routine pathology examinations in Canada by examining existing legislation and policies, as well as a survey of Canadian pathologists.
Objectives
The objectives of this Environmental Scan are to describe the drivers of routine primary pathology examinations of human tissue specimens in Canada and to identify potential opportunities for optimization in this area. The Environmental Scan addresses two questions: 1. What are the Canadian regulations and
policies for sending surgically removed human tissues to a laboratory for primary

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 2
pathology examination, and how much detail or direction do they provide?
2. Are there clinical situations in which surgeons or treating-physicians routinely requisition pathology examinations, even though the likelihood of clinically significant abnormalities is very low and examination is not mandated by regulations, policy, or protocols?
Findings
This Environmental Scan is not intended to provide a comprehensive review of the topic. Results are based on a limited literature search, communication with key informants, and a survey. Nine provincial or territorial regulations and five regional or local policies regarding surgical specimen submission to the pathology laboratory were identified and included in this Environmental Scan. No relevant regulations or policies applicable to Quebec or Newfoundland and Labrador were identified. The survey (as circulated, Appendix 1) was developed in consultation with key informants in multiple jurisdictions, and its purpose was to inquire about the regulations, policies, and practices applicable to Canadian anatomic pathology laboratories. The survey was not conducted in Yukon, the Northwest Territories, or Nunavut because CADTH was informed that any surgical specimens from these regions would be sent to other jurisdictions for pathology examination. Thirty clinical experts in the field of pathology from 10 provinces were invited to participate in the survey; 10 individual or aggregate responses were received, representing British Columbia, Alberta, Manitoba, and Nova Scotia. In addition, two in-person interviews were held with key informants in Ontario. Key informants and
survey respondents included directors of pathology, department heads, and managers responsible for laboratories in urban tertiary care centres and community hospitals. This report is based on information gathered as at June 2014.
Provincial and Territorial Regulations
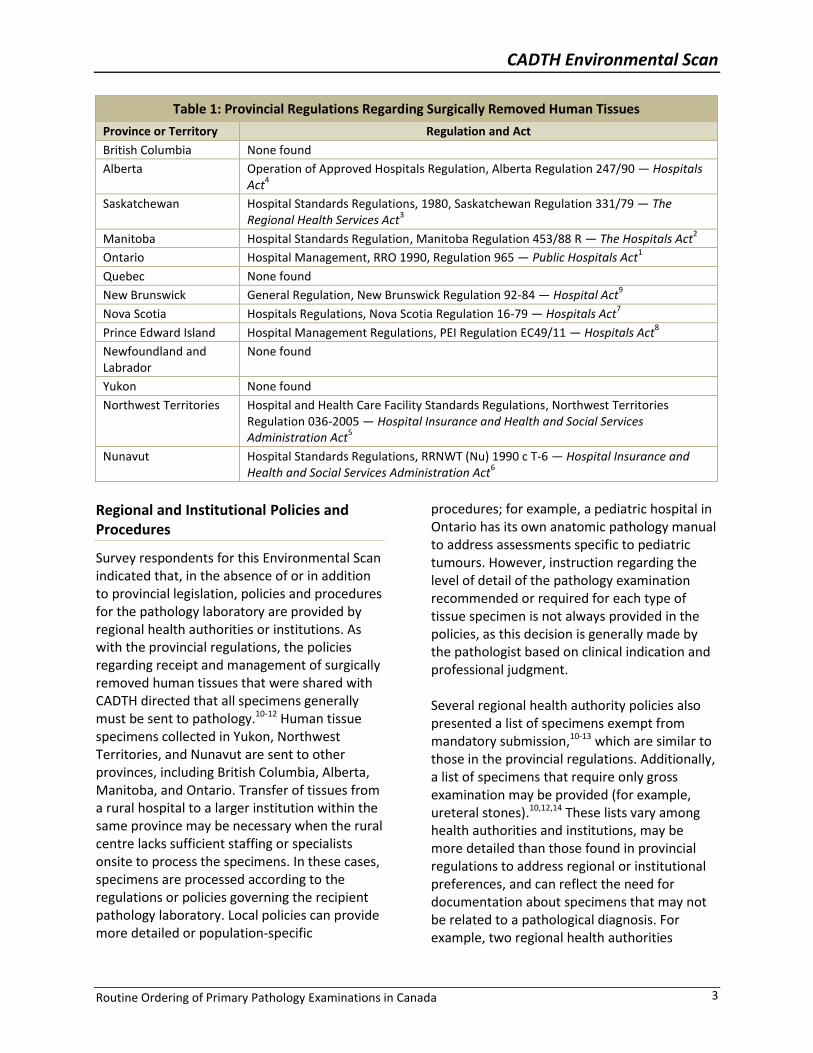
Provincial or territorial regulations outlining the requirement for human tissues removed by surgery or curettage to be sent to a laboratory for examination were identified for all provinces and territories except British Columbia, Quebec, Newfoundland and Labrador, and Yukon (Table 1). Most regulations include either a list of specimens that may be exempt from mandatory examination unless otherwise directed by the surgeon1-6 (Appendix 2, Table A3), or a statement that allows for the Ministry or local institutions to create their own documented policies for tissues exempt from examination.7,8 Specimens commonly listed as exempt include fingers,1-6 hernial sacs,2-6 hemorrhoids,1,3,5,6 prepuces,1-4 teeth,1-6 toes,1-3,5,6 and tonsils.1-6
Specifics regarding the level of pathology examination and testing (that is, gross versus histological examination) to be performed on surgical specimens submitted to the laboratory are provided in regulations from Saskatchewan,3 New Brunswick,9 and Nova Scotia.7 Although all hospitals must adhere to the requirements of their respective provincial or territorial legislation, these regulations are generally broad and allow for institutional protocols to provide more detailed criteria for the level of examination required for each type of human tissue specimen.
CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 3
Table 1: Provincial Regulations Regarding Surgically Removed Human Tissues
Province or Territory Regulation and Act
British Columbia None found
Alberta Operation of Approved Hospitals Regulation, Alberta Regulation 247/90 ― Hospitals Act
4
Saskatchewan Hospital Standards Regulations, 1980, Saskatchewan Regulation 331/79 ― The Regional Health Services Act
3
Manitoba Hospital Standards Regulation, Manitoba Regulation 453/88 R ― The Hospitals Act2
Ontario Hospital Management, RRO 1990, Regulation 965 ― Public Hospitals Act1
Quebec None found
New Brunswick General Regulation, New Brunswick Regulation 92-84 ― Hospital Act9
Nova Scotia Hospitals Regulations, Nova Scotia Regulation 16-79 ― Hospitals Act7
Prince Edward Island Hospital Management Regulations, PEI Regulation EC49/11 ― Hospitals Act8
Newfoundland and Labrador
None found
Yukon None found
Northwest Territories Hospital and Health Care Facility Standards Regulations, Northwest Territories Regulation 036-2005 ― Hospital Insurance and Health and Social Services Administration Act
5
Nunavut Hospital Standards Regulations, RRNWT (Nu) 1990 c T-6 ― Hospital Insurance and Health and Social Services Administration Act
6
Regional and Institutional Policies and Procedures
Survey respondents for this Environmental Scan indicated that, in the absence of or in addition to provincial legislation, policies and procedures for the pathology laboratory are provided by regional health authorities or institutions. As with the provincial regulations, the policies regarding receipt and management of surgically removed human tissues that were shared with CADTH directed that all specimens generally must be sent to pathology.10-12 Human tissue specimens collected in Yukon, Northwest Territories, and Nunavut are sent to other provinces, including British Columbia, Alberta, Manitoba, and Ontario. Transfer of tissues from a rural hospital to a larger institution within the same province may be necessary when the rural centre lacks sufficient staffing or specialists onsite to process the specimens. In these cases, specimens are processed according to the regulations or policies governing the recipient pathology laboratory. Local policies can provide more detailed or population-specific
procedures; for example, a pediatric hospital in Ontario has its own anatomic pathology manual to address assessments specific to pediatric tumours. However, instruction regarding the level of detail of the pathology examination recommended or required for each type of tissue specimen is not always provided in the policies, as this decision is generally made by the pathologist based on clinical indication and professional judgment. Several regional health authority policies also presented a list of specimens exempt from mandatory submission,10-13 which are similar to those in the provincial regulations. Additionally, a list of specimens that require only gross examination may be provided (for example, ureteral stones).10,12,14 These lists vary among health authorities and institutions, may be more detailed than those found in provincial regulations to address regional or institutional preferences, and can reflect the need for documentation about specimens that may not be related to a pathological diagnosis. For example, two regional health authorities

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 4
require gross examination of foreign materials that may have medico-legal implications (for example, bullets and prosthetic devices or implants with suspected defects).10,12
Laboratory Accreditation Programs
Apart from provincial and territorial, regional, or institutional policies, a laboratory will also typically be governed by an accreditation program that formally certifies laboratories that are compliant with established quality and safety standards. Accreditation signifies that the laboratory is competent to perform the tasks described within the scope of the accreditation.15 By driving quality standards, participation in an accreditation program influences laboratory practices, including the receipt and handling of tissue specimens after surgical removal. Accreditation Canada is an independent, not-for-profit organization that accredits health care and social service organizations, including medical laboratories,16 through its Biomedical Laboratory Services Standards.17 Two provinces with medical laboratories that follow Accreditation Canada are Nova Scotia18 and Prince Edward Island.19 Additional examples of laboratory accreditation programs applicable to anatomic pathology are summarized in Table 2. Several medical laboratory accreditation programs are offered through the provincial College of Physicians and Surgeons (Table 2). Some of these programs have chosen to adopt the College of American Pathologists (CAP) Laboratory Accreditation Program standards. The CAP Laboratory Accreditation Program’s Anatomic Pathology Checklist outlines standards regarding processes in pathology laboratories, including routine examination of surgically removed tissues.20 The checklist contains the specification that, if certain specimens are deemed to be exempt from submission to pathology or microscopic examination, then an institutional policy
containing a list of such exemptions must exist. Any such policies must be developed by the appropriate medical staff or committees and do not override a clinician’s request for examination of the surgical specimen. Notably, the CAP checklist does not provide specific protocols for the conduct of gross or microscopic examination for particular specimen types, but it instead requires that institutions provide policies and manuals to instruct pathology examination, and that gross and microscopic examinations be performed by qualified and competent professionals.20 The College of Physicians and Surgeons of British Columbia’s Diagnostic Accreditation Program (DAP)21 and the College of Physicians and Surgeons of Saskatchewan’s Laboratory Quality Assurance Program (LQAP)22 developed their own guidelines, although the DAP standards are very similar to the CAP Anatomic Pathology Checklist. Somewhat unique to accreditation standards, the LQAP Laboratory Guidelines contain a specific list of surgical specimens that are exempt from gross and/or microscopic examination in general or on a discretionary basis, unless requested by the attending physician.23 DAP provides mandatory accreditation services in the province of British Columbia.21 Much like the CAP accreditation checklist, the DAP Laboratory Medicine Accreditation Standards describe a number of criteria that must be met by accredited laboratories in each discipline, including Anatomic Pathology.24 The Gross Pathology standards (AP 1.0-1.4) within the DAP standards require the laboratory to have guidelines regarding the submission of tissue to the laboratory, exemptions from mandatory tissue submission, requirements for all submitted tissue to undergo gross examination by a pathologist or qualified delegate, and specimens exempt from microscopic examination.24

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 5
Table 2: Accreditation Programs for Anatomic Pathology Laboratories
Province(s) Program Standards or Guidelines
British Columbia CPSBC: DAP21
Accreditation Standards 2010: Laboratory Medicine
24
Alberta CPSA: ALQEP25
Anatomic Pathology Checklist, CAP Accreditation Program
20
Saskatchewan CPSS: LQAP22
Laboratory Guidelines, 201423
Manitoba CPSM: MANQAP26
Manitoba Laboratory Standards, 2014
27
Ontario, New Brunswick, Newfoundland and Labrador
QMP-LS: OLA 15189PLUS15
Provides accreditation to the international standard, ISO 15189:2012 Medical laboratories — Requirements for quality and competence
28
British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, Quebec
CAP Laboratory Accreditation Program29
Anatomic Pathology Checklist20
ALQEP = Alberta Laboratory Quality Enhancement Program; CAP = College of American Pathologists; CPSA = College of Physicians and Surgeons of Alberta; CPSBC = College of Physicians and Surgeons of British Columbia; CPSM = College of Physicians and Surgeons of Manitoba; CPSS = College of Physicians and Surgeons of Saskatchewan; DAP = Diagnostic Accreditation Program; LQAP = Laboratory Quality Assurance Program; MANQAP = Manitoba Quality Assurance Program; OLA = Ontario Laboratory Accreditation; QMP-LS = Quality Management Program − Laboratory Services.
Clinical Practices Influencing Routine Pathology Examination
Most survey respondents indicated that “routine primary pathology examinations,” as defined in this Environmental Scan, represent 76% to 100% of the workload of their pathology laboratories. However, there were varying perceptions regarding the frequency of specimen examination for which the likelihood of clinically significant abnormalities is very low and examination is not mandated by regulations, policy, or protocols. Some respondents reported that, in certain clinical situations (defined by a particular population, condition, or tissue), surgeons or treating-physicians routinely requisition a pathology examination for most if not all cases that would not normally require such examination based on the established clinical criteria and policies. Furthermore, most of the provided examples of such cases are already listed as specimens exempt from mandatory primary pathology examination within the respondents’ provincial regulations or policies (for example, normal
placenta, tonsils and adenoids in young patients, hernia sacs, digits from traumatic amputation, prepuces, and normal fractured bone). This may reflect a lack of awareness or recall by requesting physicians of the full list of specimens that are typically exempt from primary pathology examination according to existing regulations or policies. Other specimens that survey respondents thought should be exempt from pathology examinations in their region (for example, material from liposuctions and prosthetic devices) were in fact listed as specimens that are either exempt from submission to pathology or only subject to gross examination in another health authority’s policy. One province’s survey response reported that pathology laboratories receive several specimen types for pathology examination despite being on exemption lists (for example, hernial sacs, scar tissue, fingers, and toes), and each of these specimen types constitute less than 1% to 3% of total cases received by the laboratory. However, it was also stated that most clinicians in this region are aware of the exemption and will only

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 6
submit such specimens to pathology if the results of the examination are relevant to patient care. For those survey respondents from this province and other provinces who believe that specimens are being sent to pathology without clinical indication, the reasons behind this were suspected to be unclear criteria for tissue submission, lack of clinician knowledge of and/or adherence to established criteria for tissue submission, and a lack of clear guidance for follow-up of patients with previous tissue pathology (for example, colonic biopsies for follow-up of colon polyps). Placentas from normal pregnancies were regarded by pathologists in multiple jurisdictions as tissue specimens that, contrary to current practice, do not warrant routine pathology examination. Interestingly, normal placentas are on the exempt tissues lists within one provincial regulation2 and multiple regional health authority policies.10-13 Survey respondents in one province estimated that placentas represent up to 10% of all cases that receive gross and microscopic examination in their laboratories, even though in most cases the baby and mother are healthy and it is believed that the pathology report will have little to no impact on clinical care. For example, placentas are reportedly sent to pathology based on perceived abnormal appearance, when they typically meet all normal criteria according to pathology standards. These survey respondents suggested that the criteria for placenta submission need to be reviewed and that clinician education may improve implementation of the criteria. One institution contacted for this Environmental Scan reported that it provides pathology examinations of placentas based on submission criteria (maternal, fetal, and placental indications) that the pathology department developed in concert with clinicians. It receives placenta specimens from a number of external sites, and retains the option to send back placentas that do not
adhere to its clinical criteria for placental microscopic examination. More than half of the survey respondents reported having no issues at their institutions related to unnecessary tissue submission to pathology; they indicated that they are satisfied with the state of their local policies and procedures. These respondents largely attributed this success to collaborations between hospital pathology and surgical departments regarding which specimens should be submitted to pathology for examination and which clinical indications warrant microscopic examination, and to the discouraging of specimen submission purely for documentation purposes. Respondents from Western Canada reported that such collaborations at the institutional and/or regional level were initiated approximately 10 to 20 years ago and have significantly improved consistency in receipt of tissues for clinically indicated pathology examinations. One survey respondent also indicated that in Alberta there was no further need for pathology laboratory practice optimization due to Alberta Health Services’ recent two-year review of all anatomic pathology quality programs. The Eastern Ontario Regional Laboratory Association (EORLA), an organization responsible for the operation of 19 hospital-based clinical laboratories in the region, is also attempting to standardize its laboratory protocols.30 The goal of standardizing laboratory operations, including those related to anatomic pathology, is to reduce unnecessary or duplicate test requests and reduce the inefficient use of laboratory resources.31 Of note, the survey respondents who were satisfied with their respective policies and practices for routine primary pathology examination were not aware of any factors other than clinical indication that influence the decision to submit surgical specimens to the pathology laboratory.

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 7
Conclusion
Provincial and territorial regulations, regional and institutional guidelines and policies, and laboratory accreditation standards direct the submission of surgically removed human tissues to pathology laboratories in Canada. These documents offer high-level instruction and best practices but leave room for clinical expertise and judgment to inform which pathology examinations to perform and what level of examination is required. The specimen types exempt from pathology examinations varied across the regulations (Appendix 2, Table A3) and policies available to CADTH. There may be benefit in increased communication between jurisdictions to update and align policies and practices related to routine pathology examinations for optimal consistency across Canada, and to ensure that such policies are based on the best available evidence regarding clinical utility. Indeed, it was suggested by at least two survey respondents that standard indications for biopsies and clear definitions of what specimens should and should not be sent to pathology would help to optimize resources in pathology laboratories. Physicians have the discretion to order a pathology examination for any human tissue, regardless of whether the type of tissue specimen sent to pathology is on an exemption list. Thus, when tissue is sent to pathology along with a requisition, a primary examination is typically performed. This can lead to suboptimal resource use in pathology laboratories if the requesting physician is not aware of or compliant with the relevant pathology policies and regulations. However, the expressed need for pathology laboratory optimization efforts varied across survey responses; fewer than half of the survey respondents indicated such a need. Those who indicated a need for optimization reported that their laboratories routinely received specimens that were typically exempt from pathology examination (for example, tonsils, hernial sacs, and digits from traumatic amputations) and/or for which a
pathologist’s examination is not clinically indicated (for example, normal placentas). Lack of standardized indications for biopsies and clear surgical specimen submission criteria, and inconsistent adherence to pathology submission criteria by requesting physicians, were also noted as factors that may drive suboptimal pathology requisitions. Respondents indicating that no further optimization efforts were required reported success in streamlining the pathology submission process with the surgical care pathway. They recommended regular, ongoing interdepartmental communication and internal review to identify and address existing or new pathology laboratory concerns. Changing the practice by which tissues are sent for pathology examination, and the level of examination required, is a complex undertaking that likely requires effective interdepartmental coordination and, in some instances, changes to how pathology services are remunerated. Given the small survey sample size and the lack of publicly available information, it is unknown how generalizable the survey responses are within and across jurisdictions. As well, the extent to which there is a need for the optimization of policies and practices for routine primary pathology examinations is unclear, although it is evident from the survey that some institutions may benefit from such initiatives.
References
1. Ontario Ministry of the Attorney General. Hospital management. R.R.O. 1990, Regulation 965 [Internet]. In: Public Hospitals Act. Ottawa: Canadian Legal Information Institute; 2013 [cited 2014 Jun 13]. Available from: http://canlii.ca/t/523tl.
2. Manitoba Department of Justice. Hospital Standards Regulation, Manitoba Regulation 453/88 R [Internet]. In: The Hospitals Act. Ottawa: Canadian Legal Information Institute; 2003 [cited 2014 Jun 13]. Available from: http://canlii.ca/t/k7jk.

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 8
3. Government of Saskatchewan. Hospital Standards Regulations, 1980, Saskatchewan Regulations 331/79 [Internet]. In: Hospital Standards. Ottawa: Canadian Legal Information Institute; 2014 [cited 2014 Jun 13]. Available from: http://canlii.ca/t/525sf.
4. Government of Alberta. Operation of Approved Hospitals Regulation, Alberta Regulation 247/1990 [Internet]. In: Hospitals Act. Ottawa: Canadian Legal Information Institute; 2012 [cited 2014 Jun 13]. Available from: http://canlii.ca/t/51x7s.
5. Northwest Territories Department of Justice. Hospital and Health Care Facility Standards Regulations, NWT Regulation 036-2005 [Internet]. In: Hospital Insurance and Health and Social Services Administration Act. Ottawa: Canadian Legal Information Institute; 2012 [cited 2014 Jun 13]. Available from: http://canlii.ca/t/51xbn.
6. Nunavut Department of Justice. Hospital Insurance and Health Social Services Administration Act. Hospital Standards Regulations, RRNWT (Nu) 1990 c T-6 [Internet]. Ottawa: Canadian Legal Information Institute; 2006. [cited 2014 Jul 18]. Available from: http://canlii.ca/t/kh4c
7. Nova Scotia Department of Justice. Hospital regulations. Nova Scotia Regulation 16/79 [Internet]. In: Hospitals Act. Ottawa: Canadian Legal Information Institute; 2007 [cited 2014 Jun 13]. Available from: http://canlii.ca/t/jmlj.
8. Prince Edward Island Legislative Counsel Office. Hospital management regulations, PEI Regulation EC49/11 [Internet]. In: Hospitals Act. Ottawa: Canadian Legal Information Institute; 2011 [cited 2014 Jun 13]. Available from: http://canlii.ca/t/l0zt.
9. New Brunswick Office of the Attorney General. General Regulation, New Brunswick Regulation 92-84 [Internet]. In: Hospital Act (O.C. 92-508). Ottawa: Canadian Legal Information Institute; 2009 [cited 2014 Jun 13]. Available from: http://canlii.ca/t/jw1r.
10. Vancouver Coastal Health, VCH Regional Laboratory Medicine. Procedure: submission of tissue specimens to VCHA pathology laboratories. v.2. Vancouver: Vancouver Coastal Health; 2011 Jan. (Submission of Tissue Specimens to Anatomic Pathology; LTR9480).
11. Winnipeg Regional Health Authority, Clinical / Program Services. Pathology specimens (management of) - acute care setting. Winnipeg: Winnipeg Regional Health Authority; 2012 Feb. (110.220.070).
12. PHC medical staff rules [Internet]. Vancouver: Providence Health Care; 2011 Nov 24. [cited 2014 Jun 13]. Available from: http://medstaff.providencehealthcare.org/media/PHC%20Med%20Staff%20Rules%20Revision%20Nov%202011.pdf
13. Vancouver Island Health Authority, VIHA Laboratory Medicine, Pathology & Medical Genetics. RJH exempt samples. 1.1. Victoria (BC): Vancouver Island Health Authority; 2008 Jun 23. (AP Accessions; AP ACC 80 160 A).
14. Vancouver Island Health Authority, VIHA Laboratory Medicine, Pathology & Medical Genetics. Gross only samples. 1.0. Victoria (BC): Vancouver Island Health Authority; 2012 Nov 23. (APH Grossing; APH GRO 80 180A).
15. Institute for Quality Management in Healthcare. OLA 15189PLUS™ accreditation [Internet]. November 2013 Version 16. Toronto: Quality Management Program -- Laboratory Services; 2013 Dec 4. [cited 2014 Jun 25]. Available from: http://www.qmpls.org/Portals/0/OLA/PDFs/Master%20-%20OLA%20Program%20Information.pdf
16. Accreditation Canada [Internet]. Ottawa: Accreditation Canada. SCC and Accreditation Canada join forces to offer health care and medical laboratory communities accreditation to ISO15189; 2013 Mar 13 [cited 2014 Jul 15]. Available from: http://www.accreditation.ca/scc-and-accreditation-canada-join-forces-offer-health-care-and-medical-laboratory-communities
http://medstaff.providencehealthcare.org/media/PHC%20Med%20Staff%20Rules%20Revision%20Nov%202011.pdf
http://medstaff.providencehealthcare.org/media/PHC%20Med%20Staff%20Rules%20Revision%20Nov%202011.pdf

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 9
17. Accreditation Canada [Internet]. Ottawa: Accreditation Canada. Biomedical laborary services; 2013 [cited 2014 Jun 25]. Available from: http://www.accreditation.ca/biomedical-laboratory-services
18. Capital Health [Internet]. Halifax (NS): Capital Health. Accreditation profile: Department of pathology and laboratory medicine; 2010 Jun 23 [cited 2014 Jul 15]. Available from: http://www.cdha.nshealth.ca/media-centre/news/accreditation-profile-department-pathology-and-laboratory-medicine
19. Accreditation Canada. Accreditation Report: Health PEI [Internet]. Charlottetown (PE): HealthPEI; 2013 Oct 11. [cited 2014 Jul 15]. Available from: http://www.healthpei.ca/photos/original/hpei_acredrpt13.pdf
20. College of American Pathologists. CAP anatomic pathology checklist [Internet]. Northfield (IL): The College; 2011 Nov 7. [cited 2014 Jul 8]. Available from: http://www.cap.org/apps/docs/education/OnlineCourseContent/2011/LAP/Resources/Checklists/AP.pdf
21. Diagnostic Accreditation Program [Internet]. Vancouver: College of Physicians and Surgeons of British Columbia. About us; 2014 [cited 2014 Jun 25]. Available from: http://www.dap.org/Default.aspx?p=1
22. College of Physicians and Surgeons of Saskatchewan [Internet]. Saskatoon (SK): CPSS. Laboratory quality assurance program; 2013 [cited 2014 Jun 25]. Available from: http://www.cps.sk.ca/CPSS/Programs_and_Services/Laboratory_Quality_Assurance.aspx?LabQualityCCO=1
23. College of Physicians and Surgeons of Saskatchewan, Laboratory quality assurance program. Laboratory guidelines [Internet]. 2014 edition. Saskatoon (SK): CPSS; 2014. [cited 2014 Jun 25]. Available from: http://www.cps.sk.ca/Documents/Programs%20and%20Services/Laboratory%20Quality%20Assurance/Policies%20and%20Guidelines/2014%20Laboratory%20Guidelines.pdf
24. Diagnostic Accreditation Program, College of Physicians and Surgeons of British Columbia. Accreditation standards 2010: laboratory medicine [Internet]. Vancouver (BC): Diagnostic Accreditation Program; College of Physicians and Surgeons of British Columbia; 2010. [cited 2014 Jun 25]. Available from: http://www.dap.org/CmsFiles/file/Standards/2010%20Laboratory%20Standards%20TM%20Update%2022%20July%202013/Laboratory%20Medicine%20Standards%202010%2022%20July%202013.pdf
25. College of Physicians and Surgeons of Alberta. Alberta laboratory quality enhancement program [Internet]. Edmonton: The College. Overview; 2014 [cited 2014 Jun 25]. Available from: http://www.cpsa.ab.ca/Services/Quality_of_Care_Main/ALQEP/Alqep_Overview.aspx
26. College of Physicians and Surgeons of Manitoba [Internet]. Winnipeg: The College. The Manitoba quality assurance program (MANQAP); 2012 [cited 2014 Jun 25]. Available from: http://cpsm.mb.ca/manqap
27. College of Physicians and Surgeons of Manitoba. Manitoba laboratory standards [Internet]. Version 2. Winnipeg: The College; 2014 Mar. [cited 2014 Jun 25]. Available from: http://cpsm.mb.ca/cjj39alckF30a/wp-content/uploads/Laboratory_Standards_March_2014_Approved.pdf
28. Technical Committee ISO/TC 212, Clinical laboratory testing and in vitro diagnostic test systems. ISO 15189:2012 Medical laboratories -- Requirements for quality and competence [Internet]. 3rd ed. Geneva: International Organization for Standardization; 2012. [cited 2014 Jul 15]. Available from: http://www.iso.org/iso/catalogue_detail?csnumber=56115

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 10
29. College of American Pathologists. CAP [Internet]. Northfield (IL): The College. About the CAP laboratory accreditation program; 2014 Mar 12 [cited 2014 Jun 25]. Available from: http://www.cap.org/apps/cap.portal?_nfpb=true&cntvwrPtlt_actionOverride=%2Fportlets%2FcontentViewer%2Fshow&_windowLabel=cntvwrPtlt&cntvwrPtlt%7BactionForm.contentReference%7D=laboratory_accreditation%2Faboutlap.html&_state=maximized&_pageLabel=cntvwr
30. Eastern Ontario Regional Laboratory Association. EORLA [Internet]. Ottawa: The Association. EORLA: About us; 2012 [cited 2014 Jul 15]. Available from: http://www.eorla.ca/about-us
31. Dark Daily [Internet]. Spicewood (TX): The Dark Report. Canadian province of Ontario makes progress on standardizing EORLA's 19 clinical pathology laboratories; 2010 Nov 8 [cited 2014 Jul 9]. Available from: http://www.darkdaily.com/canadian-province-of-ontario-makes-progress-on-standardizing-eorlas-19-clinical-pathology-laboratories-1105

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 11
APPENDIX 1: SURVEY OF ROUTINE PRIMARY PATHOLOGY REVIEW OF HUMAN TISSUES IN CANADA
Target audience: Directors of pathology.
Purpose: This survey will help inform CADTH’s customers (i.e., decision-makers and stakeholders within the publicly funded health care system) about policies and practices related to routine diagnostic pathology review of surgically removed human tissues in Canadian laboratories. For the purposes of this survey, ‘routine review’ refers to two possible scenarios: 1) when primary pathology review of tissue
specimens is directed by regulation, protocols, policies, standard operating procedures, etc.; or
2) clinical situations (defined by a particular population, condition, setting, or tissue) in which treating physicians requisition pathology review for most if not all cases that would not otherwise be directed by regulation, protocols, policies, or standard operating procedures.
The intent is to publish the information provided by respondents in an aggregated form; names of survey respondents and hospitals will not be reported. Unless otherwise communicated, the Province/Territory and
hospital setting (e.g., urban, rural, or remote location and type of practice) will be published. Please share any documentation regarding regulation, policies, protocols, and standard operating procedures related to routine primary pathology review so that we can extract relevant details (e.g., list tissues subject to/exempt from pathology review). In summarizing these documents for our report, we will respect any confidentiality requirements that are communicated to us. Survey Questions 1. Please provide some information about
yourself and briefly describe the clinical setting of your pathology laboratory by completing the table below.
2. For your setting, please describe or provide the regulation, policies, protocols, or standard operating procedures that determine when a diagnostic pathology review is required for surgically removed human tissues.
If not providing the document, please complete the table for each regulation, policy, protocol, or standard operating procedure.
Table A1: Description of Clinical Setting
Professional Title
Departments you are responsible for within your facility/setting
Location of laboratory (e.g. urban, rural, remote)
Type of clinical practice housing the laboratory (e.g. community hospital, tertiary care centre, etc.)
Does your lab conduct primary pathology review of tissue specimens? If not, where are the specimens sent for this review?

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 12
Table A2: Description of Regulation, Policy, Protocol, Standard Operating Procedure
Title of Document
Level of Policy (regional, hospital, provincial,
other)
Does it provide inclusion and/or exclusion
criteria for tissues to be sent to pathology?
Does it provide direction on the level of
review required (e.g., gross examination,
microscopic examination, IHC testing) for the
removed tissues?
3. Based on your experience, are there clinical situations (defined by a particular population, condition, setting, or tissue) in which surgeons or treating physicians routinely requisition pathology review for most if not all cases, even though the likelihood of clinically significant abnormalities is very low and review is not mandated by regulations, policy, protocols, or standard operating procedures? If so, what are some examples? Please provide as much detail as possible, including condition/patient population, tissue, degree of examination requested (e.g., gross examination, microscopic examination, IHC testing), and how often these requests are made by clinicians (i.e., rarely, moderately, or frequently).
4. Approximately what proportion of the total pathology workload in your setting is attributable to routine tissue review as defined in this survey?
0-10%
11-25%
26-50%
51-75%
76-100%
5. Describe any other factors that affect tissue submissions for pathology review or the level of pathology review completed (e.g., fee-for-services incentives, private sector impact, remote clinic location, etc.).
6. Do you feel that policies and/or practices regarding routine primary pathology review (as defined in this survey) could be updated to better utilize lab resources? If so, what are some areas that you think need to be addressed?

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 13
APPENDIX 2: SPECIMENS EXEMPT FROM PRIMARY PATHOLOGY EXAMINATION
Table A3: Specimens on Exempt Specimen Lists Within Provincial/Territorial Regulations
Specimen Type Alberta4 Saskatchewan
3 Manitoba
2 Ontario
1 Northwest
Territories5
Nunavut6
Adenoids Xa
Xb
Amputation stumps ― secondary
X X
Arm X X X X
Blood clots X
Bone fragments and ligaments
X X
Bony ossicles (ears) X X
Cartilage, external ear (plastic)
X X
Finger X X X X X X
Fingernail X X
Foot X X X X
Foreign bodies (including bone plates, nails, and screws)
X X
Frenum X X
Hand X X X X
Hemorrhoid X X X X
Hernial sac X X X X X
Hydrocele sac X X
Intervertebral disc X X
Leg X X X X
Meningocele sac X X
Nasal septa when removed for obstruction only
X X
Optic lens X X X
Placenta X
Prepuce X X Xb
X
Ribs removed incidental to chest surgery
X X
Scar tissue X X
Semilunar cartridges
X X
Tendon segments removed incidental to orthopedic procedures
X X

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 14
Table A3: Specimens on Exempt Specimen Lists Within Provincial/Territorial Regulations
Specimen Type Alberta4 Saskatchewan
3 Manitoba
2 Ontario
1 Northwest
Territories5
Nunavut6
Toe X X X X X X
Toenail X X X
Tonsil Xa
X Xb
X X X
Tooth X X X X X X
Vaginal wall fragments (plastic repair)
X X
Varicocele X X
Vein strippings X X
aPatients under 40 years of age.
bPatients under 25 years of age.

CADTH Environmental Scan
Routine Ordering of Primary Pathology Examinations in Canada 15
Cite as: Pitre, E. Routine Ordering of Primary Pathology Examinations in Canada. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2014. (Environmental Scan; Issue 46). The contribution of name is acknowledged for his guidance and work in the review process.
***************** CADTH takes sole responsibility for the final form and content of this environmental scan. The statements and conclusions in this environmental scan are those of CADTH. Production of this report is made possible by financial contributions from Health Canada and the governments of Alberta, British Columbia, Manitoba, New Brunswick, Newfoundland and Labrador, Northwest Territories, Nova Scotia, Nunavut, Prince Edward Island, Saskatchewan, and Yukon. The Canadian Agency for Drugs and Technologies in Health takes sole responsibility for the final form and content of this report. The views expressed herein do not necessarily represent the views of Health Canada or any provincial or territorial government.
***************
Disclaimer: The Environmental Scanning Service is an information service for those involved in planning and providing health care in Canada. Environmental Scanning Service responses are based on a limited literature search and are not comprehensive, systematic reviews. The intent is to provide information on a topic that CADTH could identify using all reasonable efforts within the time allowed. Environmental Scanning Service responses should be considered along with other types of information and health care considerations. The information included in this response is not intended to replace professional medical advice nor should it be construed as a recommendation for or against the use of a particular health technology. Readers are also cautioned that a lack of good quality evidence does not necessarily mean a lack of effectiveness, particularly in the case of new and emerging health technologies for which little information can be found but that may in future prove to be effective. While CADTH has taken care in the preparation of the report to ensure that its contents are accurate, complete, and up to date, CADTH does not make any guarantee to that effect. CADTH is not liable for any loss or damages resulting from use of the information in the report. Copyright: This report contains CADTH copyright material. It may be copied and used for non-commercial purposes, provided that attribution is given to CADTH. Links: This report may contain links to other information available on the websites of third parties on the Internet.
Canadian Agency for Drugs and Technologies in Health (CADTH) 600-865 Carling Avenue, Ottawa, Ontario K1S 5S8


















