Ronald J. Pekala , V. K. Kumar , Ronald Maurer Nancy ... · 292 Suggestiblity, Expectancy, and...
28
291 American Journal of Clinical Hypnosis Copyright © 2010 by the American Society of Clinical Hypnosis 52:4, April 2010 Suggestibility, Expectancy, Trance State Effects, and Hypnotic Depth: II. Assessment via the PCI-HAP Ronald J. Pekala 1 , V. K. Kumar 2 , Ronald Maurer 1 , Nancy Elliott-Carter 1 , Edward Moon 1 , Karen Mullen 1 Address correspondences and reprint requests to: Ronald J. Pekala Coatesville VA Medical Center, Coatesville, PA Biofeedback Clinic (116B) Coatesville VA Medical Center Coatesville, PA 19320 [email protected] Abstract This study sought to determine if self-reported hypnotic depth (srHD) could be predicted from the variables of the Phenomenology of Consciousness Inventory - Hypnotic Assessment Procedure (PCI-HAP) (Pekala, 1995a, 1995b; Pekala & Kumar, 2007; Pekala et al., 2010), assessing several of the processes theorized by researchers to be associated with hypnotism: trance (altered state effects), suggestibility, and expectancy. One hundred and eighty participants completed the PCI-HAP. Using regression analyses, srHD scores were predicted from the PCI-HAP pre-hypnotic and post-hypnotic assessment items, and several other variables. The results suggested that the srHD scores were found to be a function of imagoic suggestibility, expectancy (both estimated hypnotic depth and expected therapeutic efficacy), and trance state and eye catalepsy effects; effects that appear to be additive and not (statistically) interactive. The results support the theorizing of many investigators concerning the involvement of the aforementioned component processes with this particular aspect of hypnotism, the self-reported hypnotic depth score. Keywords: Altered states of consciousness, consciousness, expectancy, hypnosis, hypnotic depth, hypnotism, psychophenomenology, suggestibility, trance.
Transcript of Ronald J. Pekala , V. K. Kumar , Ronald Maurer Nancy ... · 292 Suggestiblity, Expectancy, and...

291
American Journal of Clinical Hypnosis Copyright © 2010 by the American Society of Clinical Hypnosis52:4, April 2010
Suggestibility, Expectancy, Trance State Effects, and HypnoticDepth: II. Assessment via the PCI-HAP
Ronald J. Pekala1, V. K. Kumar2, Ronald Maurer1, Nancy Elliott-Carter1, Edward Moon1, Karen Mullen1
Address correspondences and reprint requests to:Ronald J. PekalaCoatesville VA Medical Center, Coatesville, PABiofeedback Clinic (116B)Coatesville VA Medical CenterCoatesville, PA [email protected]
AbstractThis study sought to determine if self-reported hypnotic depth (srHD)could be predicted from the variables of the Phenomenology ofConsciousness Inventory - Hypnotic Assessment Procedure (PCI-HAP)(Pekala, 1995a, 1995b; Pekala & Kumar, 2007; Pekala et al., 2010),assessing several of the processes theorized by researchers to beassociated with hypnotism: trance (altered state effects), suggestibility,and expectancy. One hundred and eighty participants completed thePCI-HAP. Using regression analyses, srHD scores were predicted fromthe PCI-HAP pre-hypnotic and post-hypnotic assessment items, andseveral other variables. The results suggested that the srHD scores werefound to be a function of imagoic suggestibility, expectancy (bothestimated hypnotic depth and expected therapeutic efficacy), and trancestate and eye catalepsy effects; effects that appear to be additive andnot (statistically) interactive. The results support the theorizing ofmany investigators concerning the involvement of the aforementionedcomponent processes with this particular aspect of hypnotism, theself-reported hypnotic depth score.
Keywords: Altered states of consciousness, consciousness, expectancy,hypnosis, hypnotic depth, hypnotism, psychophenomenology,suggestibility, trance.

292
Suggestiblity, Expectancy, and Trance State Effects 2
IntroductionA prior paper (Pekala, Kumar, Maurer, Elliott-Carter, Moon, & Mullen, 2010) reviewed
the relationships among trance or altered state effects, suggestibility, and expectancy. Theseare variables that many hypnosis researchers and theorists (Barber, 2000; Cardeña, 2005;Kihlstrom, 2003, 2005; Kirsch, 1985, 1991; Lynn & Kirsch, 2006; Schumaker, 1991;Weitzenhoffer, 2002; among others) have posited to be important in understanding thenature of hypnotism. In an integrative review, Holroyd (2003) suggested altered state effectsand imagination/suggestibility combine with expectancy to account for how individualsunderstand hypnotism.
As mentioned in our prior article (Pekala et al., 2010) Holroyd’s model (2003) ofhypnotism can be operationally defined with aspects of the model quantified and estimatedusing the PCI-HAP (Phenomenology of Consciousness Inventory: Hypnotic AssessmentProcedure; Pekala, 1995a, 1995b; Pekala & Kumar, 2000, 2007). The PCI-HAP is aphenomenologically based hypnotic assessment instrument that is used to assess hypnoticresponsivity for this predominantly phenomenological perspective. It includes a pre- andpost-assessment along with completion of the PCI (an instrument that measures 12 majorand 14 minor dimensions of consciousness; Pekala, 1982, 1991b) embedded within the PCI-HAP. The PCI is retrospectively completed in reference to a sitting quietly period embeddedin a hypnotic induction protocol after the deinduction.
The PCI-HAP generates: (a), a pHGS (predicted Harvard Group Scale) score or“hypnoidal state” score (Pekala & Nagler, 1989) that may be construed as a “general measureof trance” (Pekala & Kumar, 2000, p. 112). The hypnoidal state score, we believe, is lessprone to distortion via demand characteristics (Orne, 1962) and response sets (Wagstaff,Cole, & Brunas-Wagstaff, 2008) than typical self-report hypnotic depth measures, due to thenature of the phenomenology that the hypnoidal state score is measuring (see below).
In addition to the hypnoidal state score, the PCI-HAP assessment protocol also includesa measure of “imagoic suggestibility” that is assessed via an imagery vividness dream item.Imagoic suggestibility is an aspect of imagination and fantasy as defined by Sheehan (1979), or“imaginative suggestibility” as defined by Kirsch and Braffman (2001): “requests to experiencean imaginary state of affairs as if it were real” (p. 59). (Imagoic suggestibility we conceive as oneaspect of imaginative suggestibility since the latter may include additional aspects.)
The PCI-HAP includes self-report measures of two types of expectancy: pre-hypnoticestimated hypnotic depth and pre- and post-hypnotic therapeutic efficacy. The post-assessment form also assesses responses to several other items: a finger response item, aneye catalepsy item, and a “fell asleep” item. In addition to the above, the PCI-HAP EXCELprogram (which is used to generate a 5-page report concerning the client’s hypnotic talents),generates raw and percentile scores for the various (sub)dimensions mapped by the PCI.
The PCI-HAP also allows participants to estimate their hypnotic depth in the spiritof LeCron (1953) via a self-reported Hypnotic Depth (srHD) score. Over 20 years agoLaurence and Nadon (1986) suggested that the elucidation of “hypnotic depth is a complextask involving the interaction of experiential, cognitive and contextual variables” (p. 215).Weitzenhoffer (2002) in his classic paper, “Scales, scales, and more scales,” noted thathypnotic depth scores are “lacking in solid evidence” (p. 214). In contrast, and in support ofself-report depth scales, Wagstaff et al. (2008) suggested that depth scales may serve as auseful alternative to conventional suggestion-based tests of hypnotizability. The presentstudy helps operationalize Laurence and Nadon’s (1986) “experiential, cognitive, andcontextual variables” to better understand self-reported hypnotic depth.
293
Pekala, et al.
The Present InvestigationThe purpose of this investigation was to determine how well self-reported hypnotic
depth could be predicted from altered state effects, suggestibility, and expectancy (measuredvia PCI-HAP), variables implicated in hypnotism by many hypnosis theorists and researchers.Barnier and McConkey (2003) (see also Sheehan and McConkey, 1982) have argued “thatthere are multiple cognitive pathways to compelling hypnotic experiences” (p. 298) withsome individuals using a “constructive” or “deliberate, strategic, effortful, reflective, analytic”(p. 298) style, while others, a “concentrative” or “intuitive, automatic, effortless, impulsive,primitive” style (p. 298). In a somewhat different vein Woody and McConkey (2003) suggestedthat “different responses require different combinations of underlying component abilities”(p. 316), and different individuals, or the same individuals at different times, may use “two ormore different sets of components (which) are each sufficient to produce a particular hypnoticresponse and thus represent alternative ways to pass a particular item” (p. 317).
Hence we asked how are imagoic suggestibility, altered state effects, and expectancyrelated to the perception of one’s subsequent self-reported hypnotic depth. Although thePCI-HAP does not include all the component processes defined by Woody, Barnier, andMcConkey (2005) in their “multiple hypnotizabilities” article, we believe the imagoicsuggestibility item taps an aspect of their perceptual-cognitive factor; the eye catalepsy itemtaps an aspect of their motor challenge factor; and the hypnoidal state score taps an aspectof their “general hypnotizability” factor.
Additionally, the study attempted to replicate the results of Pekala, Kumar, Maurer,Elliott-Carter, and Moon (2006), wherein hypnotic depth was predicted from an earlier versionof the PCI-HAP that did not include the expectancy variables. Pekala et al. (2006) found thatimagoic suggestibility and altered state effects (as assessed by the hypnoidal state score)accounted for most of the variance associated with participants’ self-reported hypnoticdepth. Because the srHD score provides a general measure of the participant’s self-perceivedhypnotic responsivity, this measure may serve an important function in clinical situations. Ifindividuals do not believe they were “hypnotized,” how motivated will they be to usehypnotism and self-hypnosis to help them with their particular symptom(s)?
This study also sought to replicate the results obtained in Pekala et al. (2006)wherein a correlation of .57 was found between the srHD score and the pHGS score, and anr of .72 was obtained between the srHD score and imagoic suggestibility. This earlier studyadded some support for the use of hypnotic depth scores, in contradiction to Weitzenhoffer’s(2002) conclusion that hypnotic depth scores are “lacking in solid evidence” (p. 214), butconsistent with the theorizing of Wagstaff et al. (2008).
Method
ParticipantsTwo hundred and twenty three participants from two Substance Abuse Residential
Rehabilitation Treatment Programs (SARRTPs) initially matriculated into two slightly differentstudies on relapse prevention which included completion of the PCI-HAP. Both studiesused the same design with one major difference - the first study paid the participants for afollow-up interview (n = 120), the second study (n = 103) did not. The pre-assessment formwas added part way through Study 1 and was used throughout Study 2.
Informed consent was procured; and participation was voluntary. The study wasreviewed and approved by the hospital IRB and R&D committees. Eliminating participants
294
Suggestiblity, Expectancy, and Trance State Effects 2
with a reliability index (RI)1 of greater than 2.30 on the PCI, to control for unreliable responses,resulted in 180 participants. Using only those participants who completed all pre- and post-assessment forms resulted in a final n of 123.
MaterialsParticipants took part in a study on relapse prevention for which they completed a
variety of questionnaires before discharge. One of those involved the hypnotic assessmentprocedure (PCI-HAP) described below (Pekala, 1995a, 1995b, 2002; Pekala & Kumar, 2000,2007; Pekala et al., 2010).
The PCI-HAP2 consists of a pre-assessment, a hypnotic induction, and a post-assessment (debriefing). For the pre-assessment, participants report whether they experiencedhypnotism before and if so, how hypnotizable they felt they were at that time. They also areasked to estimate their subsequent level of hypnotic depth on a “1” to “10” scale (estimatedhypnotic depth). Additionally, participants are told to visualize themselves in a hot tub andestimate the vividness of their kinesthetic and visual imagery. Finally, they are told toestimate (on a “1” to “10” scale) how helpful the hypnotic session was going to be for theirproblems and concerns.
The hypnotic induction consists of a “body scan” (progressive relaxation butwithout the tensing), and a “mind calm:” counting back from “10” to “1” while the mindbecomes more calm and empty. After the mind calms, participants are asked to go on vacationin their mind and experience a hypnotic dream. After this mental vacation (the imagoicsuggestibility item) participants are asked to raise their left index finger (the finger raisingitem) to obtain a measure as to whether they may have fallen asleep, or been unresponsive,at this point in time.
Participants are subsequently told that their eyes are “heavy like lead” and are askedto try to open their eyes (the eye catalepsy item). Participants are then told to sit quietly and“just continue to experience the state you are in right now.” After the 2-minutes sitting quietlyperiod, participants are asked to pause for 15 seconds and make a mental note of what theywere experiencing during that time. Participants are then counted out of the induction.
After deinduction, subjects subsequently complete the 53-item PCI in reference tothe 2-minute sitting quietly period during the hypnotic induction and the debriefingquestionnaire. The 53 items of the PCI assess subjective experiences across 12 majordimensions and 14 minor dimensions. These (sub)dimensions are: altered state of awareness,altered experience (body image, time sense, perception, unusual meaning), volitional control,self-awareness, rationality, internal dialogue, positive affect (joy, sexual excitement, andlove), negative affect (anger, sadness, and fear), imagery (amount and vividness), attention(direction and absorption), memory and arousal.
The PCI has been found to be reliable and valid for mapping phenomenologicalexperiences in response to such stimulus conditions as eyes open and closed sitting quietly,hypnotism, progressive relaxation, breathing, drumming and trance postures, and even firewalking (Forbes & Pekala, 1993, 1996; Maurer, Kumar, Woodside, & Pekala, 1997; Pekala &Levine, 1981, 1982; Pekala & Wenger, 1983; Pekala, Steinberg, & Kumar, 1986; Pekala & Ersek,1992/93; Woodside, Kumar, & Pekala, 1997). The PCI has been found especially useful inmapping the subjective states associated with hypnotism and it has been shown to haveadequate construct/criterion validity (Barnes, Lynn, & Pekala, 2009; Forbes & Pekala, 1993;Kumar & Pekala, 1988, 1989; Kumar, Pekala, & Marcano, 1996; Hand, Pekala, & Kumar, 1995;Kumar, Pekala, & McCloskey, 1999; Pekala, 1991a, 2002; Pekala, Forbes, & Contriasani, 1988;

295
Pekala, et al.
Pekala & Kumar, 1984,1986, 1987, 1989; Pekala, Steinberg, & Kumar, 1986) for measuringsubjective experiences associated with hypnotism.
After completing the PCI, the participant completes a debriefing form rating thevividness of their imagery in reference to going “on a vacation somewhere to a beautifulplace and having a very relaxing and very wonderful time;” rating on a “1” to “10” intensityscale the vividness of their imagery, letting “1” = “just a thought, no image at all” and “10,”“as real and vivid as actually being there.” The debriefing form also asks whether participantsopened their eyes during the eye catalepsy item (“1” = opened eyes; “2” = did not openeyes), if they raised their finger when asked to do so (“1” = raised finger ; “2” = did not raisefinger), and their self-report as to whether they fell asleep on a 4-point scale: “1” = fell asleep;“4” = did not fall asleep.3
The finger response and the fell asleep items were included in the PCI-HAP todetermine if participants, especially in a group setting, may have become unresponsiveduring the hypnotism. An item near the end of the debriefing form asks the participantsabout their hypnotic depth: “On a ‘1’ to ‘10’ scale, how hypnotized do you feel that youbecame? Let ‘1’ = ‘not hypnotized at all,’ and let ‘10’ = ‘the most hypnotized that you canimagine.’” This item measures a participant’s self-reported hypnotic depth (srHD). Anadditional item also asks how helpful hypnotism is going to be to help them with their“problems, issues, and concerns” (post-hypnotic therapeutic efficacy).
ProcedureParticipants were seen for two counterbalanced assessment/treatment sessions
spaced about a week a part. Participants were paid $10 for their participation in either study.Participants were paid $10 for a follow-up interview in Study 2; no such remuneration wasgiven in Study 1.
The first half of each session consisted of assessment with either the PCI-HAP, ora questionnaire that asked about anxiety, anger, beliefs, etc. Part way through the first studythe pre-assessment form was added to the PCI-HAP. The pre-assessment form was usedwith all subjects for Study 2. The second half of each session consisted of treatment: eitherself-hypnosis training for anxiety/anger reduction and relapse prevention, or self-hypnotictraining for self-esteem and serenity enhancement. For the purposes of this paper only thePCI-HAP results are addressed.
ResultsThe following section reviews the results starting first with preliminary analyses,
and then correlational and regression analyses to address the several purposes of the study.Anova analyses were also computed to supplement the regression analyses.
Preliminary AnalysesSince data came from two studies, MANOVAs were completed to determine if there
were significant differences across the variables as a function of Studies (1 and 2) and Order(first or second session – since the two sessions were counterbalanced). This preliminaryanalysis was done to determine if the two data sets could be combined to obtain a largersample size. Dependent variables included in the analyses were: srHD, imagoic suggestibility,hypnoidal state, finger response, eye catalepsy, negative effects, fell asleep, pre-hypnoticestimated hypnotic depth, pre- and post-hypnotic therapeutic expectancy, and pre-hypnoticvisual and kinesthetic imagery vividness. There was neither a significant main effect for

296
Suggestiblity, Expectancy, and Trance State Effects 2
Study, Wilks’ Lambda = 0.87, F (12, 108) = 1.30, p = .22; nor for Order, Wilks’ Lambda = 0.91,F (12, 108) = 0.85, p = .60. The interaction between Study and Order was also not significant,Wilks’ Lambda = 0.89, F (12, 108) = 1.15, p = .33.
Because the assessment of expectancy was an important part of the current study andthe pre-assessment form measured both pre-hypnotic estimated depth (“how deeply hypnotizeddo you expect to be when we try to hypnotize you today?”), and pre-hypnotic expected therapeuticefficacy (“how helpful do you think self-hypnosis training is going to be to help you with yourproblems, issues, or concerns?”), separate 2 (Order) x 2 (Prior Hypnotism) ANOVAs were alsocomputed for these two variables with Order and Prior Hypnotism (“Have you ever tried to behypnotized before: Yes or No,” - an item on the pre-assessment form) as the independent variables.For pre-hypnotic estimated hypnotic depth there were neither significant main effects for Order,F (1, 120) = 2.17, p = .14, nor Prior Hypnotism, F (1, 120) = .14, p = .80; nor was the interactionsignificant, F (1, 120) = .60, p = .60. For pre-hypnotic expected therapeutic efficacy, the maineffects for Order, F (1, 120) = 3.32, p = .07, and Prior Hypnotism, F (1, 120) = .03, p = .87) were notsignificant; nor was the interaction significant, F (1, 120) = 1.52, p = .22. Due to the aforementionednonsignificant MANOVA and ANOVA results, the data from the two studies were pooled for allsubsequent analysis.
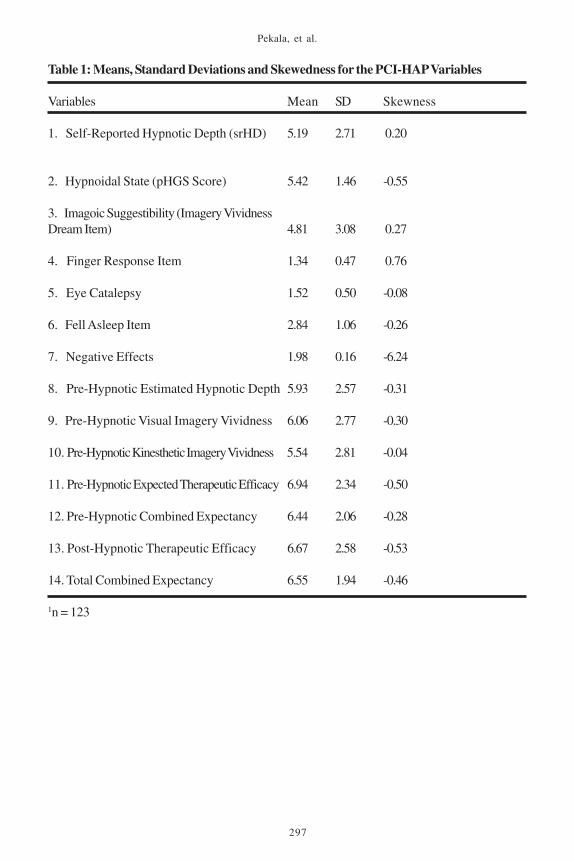
Descriptive Statistics and Correlational AnalysesTable 1 lists the means and standard deviations of the variables of interest in the study.
Table 2 lists the correlation matrix for the following scores: srHD , PCI pHGS (hypnoidal state),imagery vividness dream item (imagoic suggestibility), and the other PCI-HAP pre-assessment andpost-assessment items. A pre-hypnotic combined expectancy score was computed averaging thepre-hypnotic estimated hypnotic depth score and the pre-hypnotic therapeutic efficacy score, aswas a total combined expectancy score (which was the average of the pre-hypnotic combinedexpectancy score and the post-hypnotic therapeutic efficacy score).
The highest correlation obtained with the srHD score was imagoic suggestibility (r = .68,p < .001). The next highest correlations were with total combined expectancy (r = .62), post-hypnotic therapeutic efficacy (r = .53), and pre-hypnotic combined expectancy (r = .51). Thiswas followed by the hypnoidal state (r = .48) score, and the eye catalepsy item (r = .45). Pre-hypnotic estimated hypnotic depth (r = .43), pre-hypnotic expected therapeutic efficacy (r =.41), and pre-hypnotic kinesthetic (r = .35) and visual (r = .34) imagery were also significantlycorrelated (p < .001) with the srHD score (see Table 2).
Regression Analyses
Preliminary Assumption Testing.Preliminary analyses were completed to check if the data were in accord with the
assumptions of linearity, normality, and homoscedasticity of the independent variables4 requiredfor the regression analyses. Visual inspection of the data suggested that the assumptions oflinearity and homoscedasticity were met for all variables. Table 1 shows the skewness for allthe variables. All variables4 had a skewness of less than an absolute value of about .60(average absolute value of .39), suggesting relative normality for the independent variablesused in the regression analyses. Visual inspection of the distributions suggested that thedistributions of the variables were relatively mesokurtic (Newton & Rudestam, 1999). Henceno data transformations were deemed necessary on the aforementioned variables.
297
Pekala, et al.
Table 1: Means, Standard Deviations and Skewedness for the PCI-HAP Variables
Variables Mean SD Skewness
1. Self-Reported Hypnotic Depth (srHD) 5.19 2.71 0.20
2. Hypnoidal State (pHGS Score) 5.42 1.46 -0.55
3. Imagoic Suggestibility (Imagery VividnessDream Item) 4.81 3.08 0.27
4. Finger Response Item 1.34 0.47 0.76
5. Eye Catalepsy 1.52 0.50 -0.08
6. Fell Asleep Item 2.84 1.06 -0.26
7. Negative Effects 1.98 0.16 -6.24
8. Pre-Hypnotic Estimated Hypnotic Depth 5.93 2.57 -0.31
9. Pre-Hypnotic Visual Imagery Vividness 6.06 2.77 -0.30
10. Pre-Hypnotic Kinesthetic Imagery Vividness 5.54 2.81 -0.04
11. Pre-Hypnotic Expected Therapeutic Efficacy 6.94 2.34 -0.50
12. Pre-Hypnotic Combined Expectancy 6.44 2.06 -0.28
13. Post-Hypnotic Therapeutic Efficacy 6.67 2.58 -0.53
14. Total Combined Expectancy 6.55 1.94 -0.46
1n = 123

298
Suggestiblity, Expectancy, and Trance State Effects 2
Tabl
e 2:
Pea
rson
Cor
rela
tion
Mat
rix
for
the
PC
I-H
AP
Var
iabl
es1
Var
iabl
es1
23
45
67
89
1011
1213
1. S
elf-
Rep
orte
d1.
00H
ypno
tic D
epth
(srH
D)
2. H
ypno
tic S
tate
.482
1.00
(pH
GS)
Sco
re(.5
73 )
3. Im
agoi
c Su
gges
tibili
ty.6
8.3
61.
00(I
mag
ery
Viv
idne
ss(.7
2)(.4
5)D
ream
Item
)
4. F
inge
r Res
pons
e It
em.0
6-.0
7.1
41.
00(.2
0)(.0
8)(.1
9)
5. E
ye C
atal
epsy
Item
.45
.30
.34
-.25
1.00
(.15)
(.30)
(.08)
(-.2
6)
6. F
ell A
slee
p It
em.1
2.3
5.0
5-.2
9.1
91.
00(.0
8)(.2
7)(.0
6)(-
.32)
(.18)
7. N
egat
ive
Eff
ects
-.13
-.04
-.03
.00
-.05
.02
1.00
8. P
re-H
ypno
tic.4
3.1
9.3
4.1
8.2
1-.0
1-.2
31.
00E
stim
ated
Hyp
notic
Dep
th
9. P
re-H
ypno
tic V
isua
l.3
4.2
0.2
8.1
5.2
5.0
5-.0
9.4
21.
00Im
ager
y V
ivid
ness

299
Pekala, et al.
Tabl
e 2
cont
inue
d
Var
iabl
es1
23
45
67
89
1011
1213
10.
Pre-
Hyp
notic
.35
.19
.34
.15
.18
.00
-.12
.42
.83
1.00
Kin
esth
etic
Imag
ery
Viv
idne
ss
11.
Pre-
Hyp
notic
.41
.35
.22
.13
.21
.07
-.18
.41
.46
.48
1.00
Exp
ecte
d T
hera
peut
icE
ffic
acy
12.
Pre-
Hyp
notic
.51
.32
.34
.19
.25
.04
-.25
.86
.52
.53
.82
1.00
Com
bine
d E
xpec
tanc
y
13.
Post
-Hyp
notic
.53
.40
.30
.10
.27
.00
-.13
.22
.31
.27
.43
.38
1.00
Exp
ecte
d T
hera
peut
icE
ffic
acy
14.
Tota
l Com
bine
d.6
2.4
3.3
8.1
7.3
2.0
2-.2
1.6
0.4
9.4
7.7
2.7
9.8
7E
xpec
tanc
y
1 n =
123
2 r >
.18
(p <
.05)
; r >
.24
(p <
.01)
; and
r >
.29
(p <
.001
)3 C
orre
latio
ns in
par
enth
eses
repr
esen
t cor
rela
tions
from
an
earl
ier s
tudy
that
wer
e re
port
ed in
Pek
ala
et a
l., 2
006.

300
Suggestiblity, Expectancy, and Trance State Effects 2
Main Regression Analyses.Several stepwise regression analyses were completed using forward regression and an
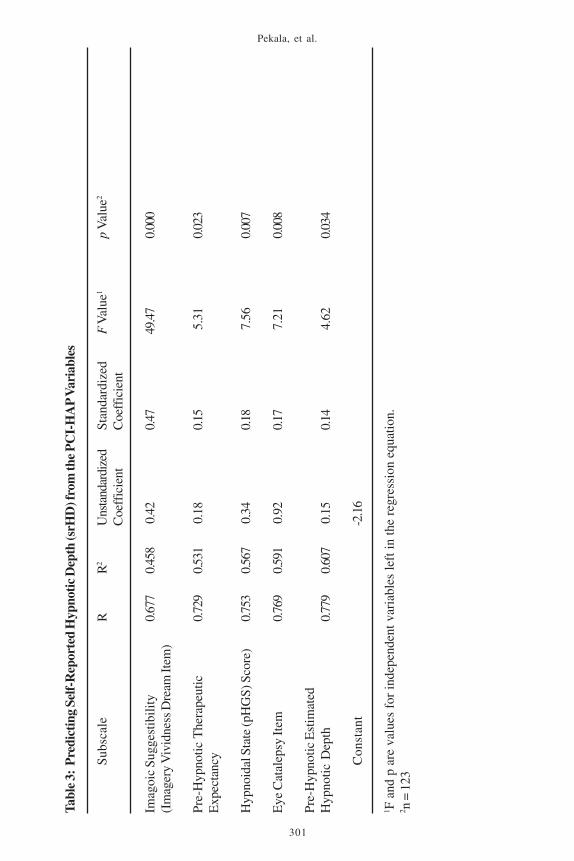
alpha-to-enter and leave of .15, the default value (Wilkinson, 1998). The first regression analysisattempted to predict the srHD scores from the PCI-HAP pre-assessment and post-assessmentvariables including the hypnoidal state score (but not including the post-hypnotic therapeuticefficacy score or any combined expectancy scores). Stepwise regression analyses generated amultiple R of .78 (R2 =.61) in predicting self-reported hypnotic depth. Left in the regressionequation were (standardized regression coefficients are in parentheses): imagoic suggestibility(vividness of the hypnotic dream) (.47); hypnoidal state (altered state trance effects) (.18); eyecatalepsy effects (.17); and pre-hypnotic expectancies concerning both estimated hypnotic depth(.14); and therapeutic expectancy (.15) (See Table 3.) (Single interactions were also assessed forall pairs of variables left in the regression equation. None were significant.)
Because partial regression coefficients partial out the variance associated with theother variables entered into the regression equation, they indicate “with a good deal ofconfidence, whether specific predictors make contributions to the criterion that are unrelatedto the contributions made by the other variables” (Grimm & Yarnold, 1995, p. 41), henceallowing for a comparison of “the relative contributions of each predictor to the overalleffect” (p. 41) of the variance accounted for by the regression. The aforementioned resultssuggest that of the 61% of the variance accounted for by the regression analysis much ofthat effect was due to imagoic suggestibility (the imagery vividness dream item). The twoexpectancy items (estimated hypnotic depth and expected therapeutic efficacy) togetherwith the hypnoidal state score and the eye catalepsy item accounted for the rest.
Another set of regression analyses were completed (see Table 4) identical to thefirst set of regression analyses mentioned above, but substituting the pre-hypnotic combinedexpectancy score for the pre-hypnotic estimated hypnotic depth and the pre-hypnotic expectedtherapeutic efficacy scores and adding in post-hypnotic therapeutic expectancy to the list ofindependent variables. The post-hypnotic therapeutic efficacy variable was not used previouslyin the regression equation, because as with self-reported hypnotic depth, it was one of the lastvariables that the participants were asked to estimate during the post-assessment, and hence, canbe conceived as more of an outcome or attributional (see below) variable than a predictor variable.Left in the regression equation were: imagoic suggestibility, hypnoidal state, pre-hypnotic combinedexpectancy, the eye catalepsy item, and also post-hypnotic therapeutic efficacy for an R of .80 andan R2 of .65 (see Table 4). Single interactions were also assessed for all pair of variables left in theregression equation. None of the interactions were found to be significant.
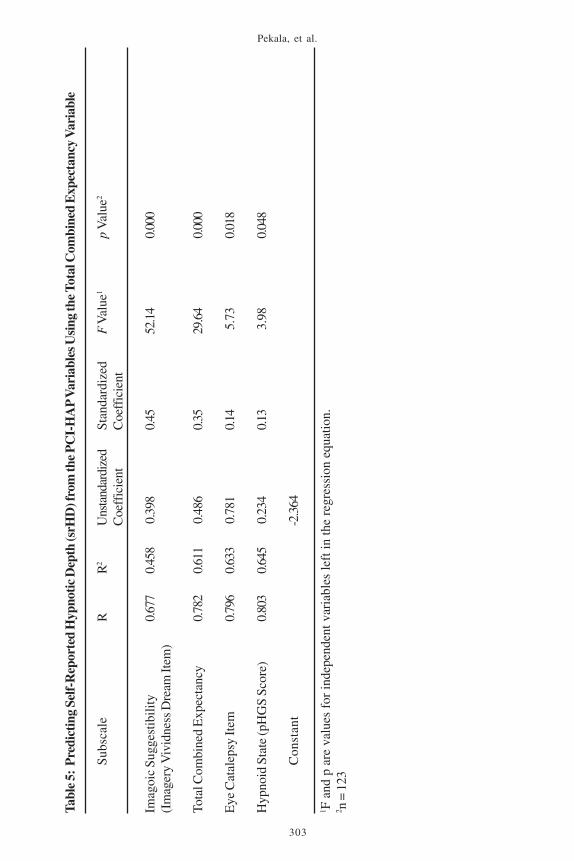
The final set of regression analyses used the aforementioned variables, but nowthe total combined expectancy score was substituted for the pre-hypnotic combinedexpectancy score and the post-hypnotic therapeutic efficacy score. In the regression equationwere: imagoic suggestibility, total combined expectancy, hypnoidal state, and the eyecatalepsy item for an R of .80 and an R2 of .65 (see Table 5). (Single interactions were alsoassessed for all pair of variables left in the regression equation. None of the interactionswere found to be significant.) Imagoic suggestibility accounted for the largest percentage ofthe relative variance, followed by total combined expectancy, with the eye catalepsy item andthe hypnoidal state score accounting for smaller percentages.
ANOVA Analyses and Visual Depiction of the Results.To visually illustrate for the reader the additive (and statistically noninteractive)
301
Pekala, et al.
Tabl
e 3:
Pre
dict
ing
Self-
Rep
orte
d H
ypno
tic D
epth
(srH
D) f
rom
the
PC
I-H
AP
Var
iabl
es
Sub
scal
eR
R2
Uns
tand
ardi
zed
Stan
dard
ized
F V
alue
1p
Val
ue2
Coe
ffic
ient
Coe
ffic
ient
Imag
oic
Sugg
estib
ility
0.67
70.
458
0.4
20.
4749
.47
0.00
0(I
mag
ery
Viv
idne
ss D
ream
Item
)
Pre-
Hyp
notic
The
rape
utic
0.72
90.
531
0.1
80.
15 5
.31
0.02
3E
xpec
tanc
y
Hyp
noid
al S
tate
(pH
GS)
Sco
re)
0.75
30.
567
0.3
40.
18 7
.56
0.00
7
Eye
Cat
alep
sy It
em0.
769
0.59
1 0
.92
0.17
7.2
10.
008
Pre-
Hyp
notic
Est
imat
edH
ypno
tic D
epth
0.77
90.
607
0.1
50.
14 4
.62
0.03
4
Con
stan
t-2
.16
1 F a
nd p
are
val
ues
for
inde
pend
ent v
aria
bles
left
in th
e re
gres
sion
equ
atio
n.2 n
= 1
23

302
Suggestiblity, Expectancy, and Trance State Effects 2
Tabl
e 4:
Pre
dict
ing
Self-
Rep
orte
d H
ypno
tic D
epth
(srH
D) f
rom
the
PC
I-H
AP
Var
iabl
es U
sing
the
Pre
-Hyp
notic
Com
bine
d E
xpec
tanc
y an
d th
eP
ost-
Hyp
notic
The
rape
utic
Exp
ecta
ncy
Var
iabl
es
Sub
scal
eR
R2
Uns
tand
ardi
zed
Stan
dard
ized
F V
alue
1p
Val
ue2
Coe
ffic
ient
Coe
ffic
ient
Imag
oic
Sugg
estib
ility
0.67
70.
458
0.3
970.
4550
.88
0.00
0(I
mag
ery
Viv
idne
ss D
ream
Item
)
Post
-Hyp
notic
The
rape
utic
0.75
70.
574
0.2
340.
2313
.04
0.00
0E
ffic
acy
Pre-
Hyp
notic
Com
bine
d0.
783
0.61
4 0
.255
0.19
9.6
30.
002
Exp
ecta
ncy
Eye
Cat
alep
sy It
em0.
797
0.63
5 0
.782
0.14
5.6
10.
020
Hyp
noid
Sta
te (p
HG
S Sc
ore)
0.80
40.
647
0.2
360.
13 3
.97
0.04
9
Con
stan
t-2
.138
8
1 F a
nd p
are
val
ues
for
inde
pend
ent v
aria
bles
left
in th
e re
gres
sion
equ
atio
n.2 n
= 1
23
303
Pekala, et al.
Tabl
e 5:
Pre
dict
ing
Self-
Rep
orte
d H
ypno
tic D
epth
(srH
D) f
rom
the
PC
I-H
AP
Var
iabl
es U
sing
the T
otal
Com
bine
d E
xpec
tanc
y V
aria
ble
Sub
scal
eR
R2
Uns
tand
ardi
zed
Stan
dard
ized
F V
alue
1p
Val
ue2
Coe
ffic
ient
Coe
ffic
ient
Imag
oic
Sugg
estib
ility
0.67
70.
458
0.3
980.
4552
.14
0.00
0(I
mag
ery
Viv
idne
ss D
ream
Item
)
Tota
l Com
bine
d E
xpec
tanc
y0.
782
0.61
1 0
.486
0.35
29.6
40.
000
Eye
Cat
alep
sy It
em0.
796
0.63
3 0
.781
0.14
5.7
30.
018
Hyp
noid
Sta
te (p
HG
S Sc
ore)
0.80
30.
645
0.2
340.
13 3
.98
0.04
8
Con
stan
t-2
.364
1 F a
nd p
are
val
ues
for
inde
pend
ent v
aria
bles
left
in th
e re
gres
sion
equ
atio
n.2 n
= 1
23

304
Suggestiblity, Expectancy, and Trance State Effects 2
nature of the regression results, the variables of hypnoidal state, imagoic suggestibility, andpre-hypnotic combined expectancy, were divided into three groups of low, medium, and highscorers. For hypnoidal state, groups consisted of lows (scores of 4.5 or less; n = 27),mediums (4.5 to 6.5; n = 49), and highs (greater than or equal to 6.5; n = 47). For imagoicsuggestibility, groups consisted of lows (4.5 or less; n = 37), mediums (4.5 to 6.0; n = 57), andhighs (greater than or equal to 6.0; n = 29). For pre-hypnotic combined expectancy, groupsconsisted of lows (less than 5.5; n = 43), mediums (5.5 to 8.0; n = 48), and highs (greater thanor equal to 8.0; n = 32). For the eye catalepsy item 59 participants opened their eyes; 64 didnot. (Separate ANOVAs were computed for Hypnoidal State by Expectancy, and also ImagoicSuggestibility by Eye Catalepsy so as to not visually complicate depiction of the results.)
A 3 (Hypnoidal State Group) by 3 (Pre-Hypnotic Combined Expectancy Group) ANOVAwas completed with self-reported hypnotic depth as the dependent variable. Significant maineffects were found for Hypnoidal State, F (2, 114) = 12.53, p < .001, and Expectancy, F (2, 114)= 12.52, p < .001. The interaction, F (4, 114) = 0.64, p = .64, was not significant. Figure 1illustrates the main effects. A 2 (Eye Catalepsy: pass/fail) by 3 (Imagoic Suggestibility) ANOVAwas also completed with self-reported hypnotic depth as the dependent variable. Significantmain effects were found for Eye Catalepsy, F (1, 117) = 13.58, p < .001, and Imagoic Suggestibility,F (2, 117) = 15.19, p < .001. The interaction F (2, 117) = 0.93, p = .40), was not significant.Figure 2 illustrates the main effects. Figures 1 and 2 illustrate the additive nature of therelationships between the srHD score and the aforementioned PCI-HAP variables.
Figure 1: Self-Reported Hypnotic Depth as a Function of Hypnoidal State and Pre-HypnoticCombined Expectancy

305
Pekala, et al.
Discussion
Correlational ResultsThe results of the present study, with correlations of .68 and .48 between self-
reported hypnotic depth, and imagoic suggestibility and hypnoidal state, respectively,replicated results of an earlier study by Pekala at al. (2006) which found slightly higher rs of.72 and .57 among the three variables. When looking at the pre-assessment variables (notassessed in the earlier, Pekala et al. 2006, study), four pre-assessment variables (estimatedhypnotic depth, visual and kinesthetic imagery vividness, and expected therapeutic efficacy)were all significantly correlated with the srHD score (rs of .34 and above, p < .001).
The significant correlation of .48 between the PCI hypnoidal state score and theself-reported hypnotic depth score suggests that these two items are measuring overlapping(sharing 23% of the variance), yet differing, constructs. This interpretation is supported byconsidering differences in the magnitude of the correlations of hypnoidal state and hypnoticdepth with imagoic suggestibility: .36 between hypnoidal state and imagoic suggestibilitybut .68 between srHD and imagoic suggestibility. Whereas the self-reported hypnotic depthscore has 46% of the variance in common with imagoic suggestibility, the hypnoidal statescore has only 13% of the variance in common with imagoic suggestibility.
Regression Results Trance state effects, imagoic suggestibility, and expectancy can be operationally
defined and measured with the PCI-HAP. These are concepts that various authors andtheorists (Barber, 2000; Brown & Fromm, 1986; Cardeña, 2005; Holroyd 2003; Kirsch, 1991,1997; Weitzenhoffer, 2002) have hypothesized to be related to hypnotism. This study examinedtheir utility in predicting self-reported hypnotic depth scores.
Figure 2: Self-Reported Hypnotic Depth as a Function of Imagoic Suggestibility and EyeCatalepsy Effects

306
Suggestiblity, Expectancy, and Trance State Effects 2
Standardized coefficients allow us to determine the relative contribution made tothe criterion by partialling out the contributions made by the other variables, hence permittingcomparison of the relative contribution of each predictor to the overall effect. (Standardcoefficients can add up to less, or more, than 100%. Hence, standard coefficients need to beexamined in reference to each other, and the coefficient does not necessarily indicate theexact percentage of variance accounted for.)5
Imagoic suggestibility accounted for the largest percentage of the relative varianceacross the various regression analyses, suggesting that imagoic suggestibility is a majorcomponent in people’s judgments of their hypnotic depth with the PCI-HAP. These resultssupport the theorizing (among others) of Holroyd (2003), Barber (2000), Weitzenhoffer (2002),Lynn and colleagues (Lynn & Rhue, 1986, 1988; Lynn & Sherman, 2000), Sheehan (1979), andKirsch and Braffman (1999, 2001) concerning the importance of fantasy and imagery, and hence,suggestibility6 (Schumaker, 1991) in understanding hypnotic depth as experienced by participants.
Pre-hypnotic expectancy, both estimated hypnotic depth and expected therapeuticefficacy, considered separately or together, accounted for a significant amount of the variancein the hypnotic depth scores, suggesting that the participant’s pre-hypnotic expectanciesare relevant to their experience of hypnotic depth. This result supports the theorizing ofBarber (2000), Kirsch (1985, 2000), Erickson (Erickson, Rossi, & Rossi, 1976), Holroyd (2003),and many clinicians concerning the importance of having a positive expectancy (Hammond,1990) in reference to the experience of hypnotism.
Trance state effects (the pHGS scores) were left in the regression equation regardlessof which types of regression analysis was done, supporting the theorizing (among others) ofHolroyd (2003), Barber (2000), Weitzenhoffer (1989), Hilgard (1965), Cardeña (2005), Barabaszand Watkins (2005), and Kihlstrom (1997) concerning the importance of alterations inexperience and consciousness in self-reported hypnotic depth. Loss of motor control, asevinced by the eye catalepsy item (the motor challenge item), was also left in the regressionequation. This effect supports the theorizing of Woody, Barnier, and McConkey (2005) whosuggested that hypnotism consists of a general factor and several component factors.
Current research looked at one particular aspect of “hypnotism,” the self-reportedhypnotic depth score. This score can be regarded as an attribution (see below) that participantswere asked to make in response to their experience of the PCI-HAP. Because it is a differentconstruct from hypnotic susceptibility, it is unknown to what extent the results would besimilar when assessing for susceptibility, as measured by the Harvard (Shor & Orne, 1962) ,the Stanford C, (Weitzenhoffer & Hilgard, 1962), or the HIP (Hypnotic Induction Profile;Spiegel & Spiegel, 2004), or the component processes of hypnotizability, as defined byWoody, Barnier, and McConkey (2005).
However, a study using the Harvard Group Scale (Mohl, Kumar, & Pekala, 2007)found that the a self-report hypnotic depth score correlated .67 with the total Harvard GroupScale score, and .73 with the hypnoidal state score obtained (from the PCI) in reference to theHarvard Group Scale. These results suggest some generalizability of the results of thepresent investigation with a different study. Another study (Barnes, Lynn, & Pekala, 2009)that used the PCI in reference to the Harvard Scale found a correlation of .62 between theHarvard Group Scale score and the hypnoidal state score, thus supporting the utility of thepHGS score as a measure of hypnotic responsivity.
307
Pekala, et al.
Attributions, Self-Reported Hypnotic Depth, and Component Processes.“Attributions are inferences that people draw about the causes of events, others’ behavior,
and their own behavior” (Weiten, 2001, p. 659). Self-reported hypnotic depth can be seen as anattribution concerning how much individuals felt they were “hypnotized.” To the extent that thereare various component processes associated with being hypnotized, individuals will utilize thoseprocesses that they feel were activated to determine the degree to which they felt hypnotized.
The present study is in strong support of Brown and Fromm’s (1986) observationthat participants feel more deeply hypnotized to the extent that they were responsive to thesuggestions and believed that there were alterations in their subjective experience. Higherscores on the imagoic suggestibility item were associated with the greatest percentage of therelative variance in predicting hypnotic depth and passing of the eye catalepsy item also hada significant impact on the feeling of being hypnotized. Expectancies further “color” theresults, predisposing one to view events consistent with that expectancy (Kirsch, 2000).Also remaining in the regression analyses were trance state effects.
Because post-hypnotic expected therapeutic efficacy is also an attribution thatparticipants make in response to their experience of being hypnotized, it was not added tothe earlier regression equation (see Table 3). When it was added (see Table 4) it remained inthe regression equation, along with pre-hypnotic combined expectancy, imagoic suggestibility,hypnoidal state, and the eye catalepsy item, resulting in a slight increase in the multiple R (.72to .80), with a resulting R2 of .65. Kirsch (1991, 2000) suggested that post-hypnoticexpectancies can be quite important in understanding hypnotism. Hence, the current resultssuggest that such post-hypnotic expectancies account for part of the effect, for substancedependent individuals, in determining how hypnotized they felt they became.
When using the total combined expectancy score (averaging across the two pre-hypnotic expectancy items and the post-hypnotic expectancy item), almost two-thirds of thevariance is again being accounted for by the regression equation (R2 = .65). In this equation(see Table 5), by far the greatest amount of the relative variance (as assessed by the standardizedregression equations) is associated with the vividness of the hypnotic dream, followed byexpectancy, with passage of the eye catalepsy item and the hypnoidal state effects accountingfor the rest. Both Holroyd (2003) and Woody, Barnier, and McConkey (2005) suggest thatdifferent factors or abilities are involved or combine in determining hypnotic responsivity. Thelack of interactions between the variables left in the regression equations suggests that theseeffects are additive and not (statistically) interactive, at least as assessed by the PCI-HAP forthe aforementioned regression analyses, which are illustrated by Figures 1 and 2.
Even though pre-hypnotic estimated hypnotic depth correlated .41 with pre-hypnoticexpected therapeutic efficacy (see Table 2), both were included in the regression equation ofTable 3. This suggests that each variable is assessing a somewhat different aspect ofexpectancy. Future research will need to more fully explore both pre-hypnotic estimatedhypnotic depth and pre-hypnotic expected therapeutic efficacy.
The correlation between post-hypnotic therapeutic efficacy and self-reportedhypnotic depth was .53 (see Table 2), and post-hypnotic therapeutic efficacy was a significantpredictor in the regression analyses depicted in Table 4. These results are quite consistentwith Kirsch’s earlier research: “postinduction expectancies were very highly correlated withboth behavioral (r = .55) and subjective (r = .64) measures of responsiveness” (1991, p. 458).The fact that post-hypnotic therapeutic efficacy remained in the regression equation (seeTable 4) along with the combined pre-hypnotic expectancies, suggest that both variables aretapping somewhat different constructs.

308
Suggestiblity, Expectancy, and Trance State Effects 2
When the pre-hypnotic combined expectancy score was averaged with the post-hypnotictherapeutic efficacy score, the correlation between self-reported hypnotic depth and total combinedexpectancy is now .62, and the standardized coefficient for this variable from the regressionanalyses (see Table 5) is .35. These results suggest that expectancy (as averaged across the pre-and post-hypnotic expectancy variables) is accounting for a major portion of the relative variancein predicting hypnotic depth. The authors are unaware of any previous research that assessedexpectancies (concerning both estimated hypnotic depth and therapeutic efficacy) in a highlymotivated clinical sample, let alone a study that generated an estimate of trance state effects. Thepresent methodology allows for such effects to be quantified and statistically assessed.
Limitations of the Current Study
Assessment of “Easy Suggestions.”The PCI-HAP was devised to be a predominantly state-based measure of subjective
experience associated with hypnotism (Pekala, 1995a, 1995b; Pekala & Kumar, 2000, 2007;Pekala et al., 2010). It is different from the typical cognitive/behavioral measures of hypnoticsusceptibility/suggestibility (such as the Harvard or the Stanford C) that are much more “trait”focused, although they are also prone to “state” effects (Kumar, Pekala, & Cummings, 1996), asthe socio-cognitive theorists have demonstrated. As opposed to assessing “how hypnotizablea person may be,” the PCI-HAP assesses “hypnotic responsivity” at a particular moment intime across several domains: imagoic suggestibility, hypnoidal state, and expectancy.
Woody, in a personal communication (April, 2008), pointed out that the PCI-HAPmeasures hypnotic depth based on “a small set of quite easy suggestions (e.g., no cognitivedistortions, negative hallucinations, etc.),” and hence it maps a rather narrow spectrum of the“hypnotic universe.” For this reason, it may be missing other aspects of hypnotic responsivityhad more difficult suggestions been used, such as those from the Stanford, Form C. Had moredifficult items been used, then the combined expectancy score may not have been associatedwith as much of the relative variance (as quantified by the standardized regression coefficient), aswas found to be the case. The PCI-HAP was developed to be a relatively easy instrument toassess hypnotic responsivity, and more difficult items were avoided, so as not to develop anegative reactance of clients/research participants, or a “no set” (Hammond, 1990), as clients orresearch participants are first introduced to hypnotism. Consequently, it is unknown to whatextent the results of the present study would replicate had more difficult suggestions been part ofthe PCI-HAP. This is definitely an area for additional research.
We believe the PCI-HAP is most likely tapping the “more easy” factor of hypnoticresponsivity, as defined in Woody, Drugovi, and Oakman’s (1997) two component model ofhypnotic performance. Other researchers (Kallio & Revonsuo, 2003, 2005) have suggestedthat the “essence” of hypnotism lies in understanding the very highly hypnotizableparticipant, the hypnotic virtuoso. Because the present study included participants acrossthe wide range of hypnotic responsivity, not only was the importance of altered state effectswith very high susceptibles not adequately addressed, but such effects with more difficultitems, such as those on the Stanford C, were also unaddressed.
Use of the Harvard Group Scale of Hypnotic Susceptibility.The Harvard Group Scale was used as the criterion measure of hypnotizability in generating
the hypnoidal state score. The Stanford Hypnotic Susceptibility Scale: Form C(Weitzenhoffer and Hilgard, 1962) is usually considered the “gold standard” (Kihlstrom, 2008, p. 31)

309
Pekala, et al.
for measuring such susceptibility. Consequently, the Harvard, due to its lower ceiling and the lackof more difficult cognitive items, suggests that it is probably not accessing to the fullest extent the“latent trait factor” hypothesized by Benham, Woody, Wilson, and Nash (2006) to underliehypnotizability. We agree that this is very likely the case, and developing an additional measure ofhypnoidal state, possibly using the Stanford C (Weitzenhoffer & Hilgard, 1962), or the Waterloo-Stanford Group C (WSGC) Scale of Hypnotic Susceptibility (Bowers, 1993), appears warranted.
However, a study has been published with the PCI in reference to both the Harvardand the Stanford scales (Hand, Pekala, & Kumar, 1995). Using the unstandardized regressioncoefficients obtained with the Harvard this regression equation was multiplied by the same(sub)dimensions raw scores that were obtained during a sitting quietly period during theStanford. The Pearson r between this Stanford pHGS score and the actual Stanford Scaletotal score was .86 (p < .0001).7 This suggested to the authors that the “phenomenologicalexperiences during the Harvard and the Stanford are similar” (Hand et al., 1995, p. 131), andadds some support for the construct validity of the hypnoidal state score.
Possible Circularity in Measuring Hypnotic Depth: The Hypnoidal State versus the Self-Reported Hypnotic Depth Score.
An important issue to address concerns the possible “circularity” of trying to measurehypnotic depth via the self-reported hypnotic depth and also the hypnoidal state scores. Webelieve that the hypnoidal state score is assessing a different aspect of “hypnotic depth” than theself-reported hypnotic depth score, although they are significantly correlated (r = .48, p = .001).
The PCI was completed immediately after the hypnotic induction and before thecompletion of the debriefing questionnaire. Subjects were asked to complete the PCI inventoryin reference to their subjective experience during the two-minute sitting quietly period nearthe end of the hypnotism. To the extent that participants did this reliably and validly, the PCI(sub)dimension results should accurately reflect what participants were experiencing at thistime. (Because subjects who were unreliable at doing this were eliminated we know that theresulting subjects were reliable at introspection.)
Over 30 years ago Nisbett and Wilson (1977) suggested that introspective accessis “not sufficient to produce generally correct or reliable reports” (p. 233). Smith and Miller(1978), in their rebuttal, suggested that assessment of cognitive processing may not be asinaccessible as Nisbett and Wilson indicate. Nisbett and Wilson may be partially correctwhen relating individuals’ attributions to their actions, but when asked to describe, not thereasons (the why), but the content (the what), of their subjective experience, people aremuch more accurate, as Ericsson and Simon (1980), Lieberman (1979), Kukla (1983), andSinger and Kolligian (1987) have demonstrated (Pekala, 1991a; Pekala & Cardeña, 2000).
Because we are using a composite index of subjects’ experiences to generate thehypnoidal state score, it represents a means of assessing subjects’ phenomenologicalexperiences during the sitting quietly period near the end of the hypnotism. The procedureallows us to estimate the “trance state” associated with hypnotism at that particular point intime, provided subjects accurately remember their experience, and then rate that experiencein reference to the PCI reliably. We have shown elsewhere (Pekala, 1991a, Pekala & Kumar,2000, 2007) that such assessment of phenomenological experience is valid in predicting stateeffects in response to hypnotism and other stimulus conditions provided the methodologicalguidelines for such retrospective phenomenological assessment are followed.
The results of this and our prior studies provide encouraging results that the hypnoidalstate score (although needing more replication and validation) may further our understanding of
310
Suggestiblity, Expectancy, and Trance State Effects 2
the nature of hypnotism. However, because depth of trance may be quite variable throughout thesession we do not know how this level of trance compares with that level of trance during thehypnotic dream or the eye catalepsy item or for that matter, throughout the induction.
The srHD score is, in contrast, an attribution that individuals make in trying to estimateand summarize the nature of their hypnotic depth after their hypnotic experience. As Brown andFromm (1986) and Tart (1970, 1979) have hypothesized, self-reported hypnotic depth appears to bea function of several variables. The aforementioned regression analyses are one means of trying todetermine how subjects try to make that attribution. The present study’s results suggest thatseveral variables (as assessed by the PCI-HAP) contribute to produce that attribution: pre- andpost-hypnotic expectancies, suggestibility, passage/failure of the eye catalepsy item, and hypnoidalstate effects. Those contributions appear to be additive and not statistically interactive. However,because of the nature of stepwise statistical regression (Newtown & Rudstam, 1999), although thepresent study replicated results of a prior study (Pekala et al., 2006), the present study is also in needof additional replication, especially concerning the expectancy variables.
The Use of Step-wise Regression Analysis.Step-wise regression analysis was chosen instead of simultaneous or hierarchical
regression (Newton & Rudestam, 1999) so we could let the data “speak for themselves,” so tospeak, without any a priori theorizing about which variables should be accounting for more ofthe variance. When “the goal is to maximaze R2” and determine the best subset of independentvariables “to predict the criterion to a high degree of accuracy” (Newton & Rudestram, 1999, p. 253),then step-wise regression is the multiple regression procedure to use. However, this model “isatheoretical, and the results tend to ‘overfit’ the data because they take advantages of chancerelationships in the sample” (1999, p. 254). Hence, the results need to be replicated and cross-validated with other samples and across other laboratories.
Context and Sensitization Effects. It is quite likely that various context effects were operative during this study.8 The pre-
assessment form asked participants to estimate their hypnotic depth and the possible effectivenessof hypnotism. This may well have sensitized participants to the importance of expectancy in thestudy, and hence, possibly inflated the correlations that were obtained. Adding additional “filler”items to the pre-assessment form may be one way to reduce such an effect.
Participants completed the PCI in reference to a sitting quietly period embedded in thePCI-HAP induction protocol. Various items of the PCI ask about alterations in consciousnessand experience, which may likewise have sensitized participants to the importance of such effects.Additionally, even the act of introspection may influence the results obtained, since introspectionabout subjective experience, especially concerning altered state effects, may affect the reportedresults, as Hunt and Chefurka (1976) suggested over 30 years ago.
Most importantly, the nature of the contents of consciousness associated with a particularstimulus condition are partly a function of the context in which they are assessed (Pekala, 1980,1991a). This was also echoed over 100 years ago by the structural introspectionists:
In 1907 Angell attacked the “more extreme and ingenuous conceptions ofstructural psychology” as the result of “an unchastened indulgence inwhat we may call the ‘state of consciousness’ doctrine” (p. 64); a doctrine thatyielded introspective data “dependent upon the particular exigencies andconditions which called them forth“(p. 67). (Pekala & Wenger, 1983, p. 251-252)

311
Pekala, et al.
Because what a person experiences during a short stimulus interval will be partly afunction of the context and instructional set given to the person, slightly different instructionsand/or stimulus context effects may yield differing introspective reports. Hence the need tobe cognizant of such effects and how they may influence the reported results especially inreference to the instructional sets of the present investigation. Much more research isneeded concerning this retrospective phenomenological approach to mapping and quantifyingsubjective experience (Pekala, 1980, 1991a; Pekala & Kumar, 2000, 2007) to better determinethe nature and extent of such context and sensitization effects.
General Limitations of the Instrument. The PCI-HAP includes several single items mapping particular responses, i.e., the
imagoic suggestibility score, the eye catalepsy, the finger response items, etc. Because it isimpossible to measure the internal consistency of a scale composed of a single item, thissuggests a major limitation of the instrument. More similar items were not added because thePCI-HAP was developed to be used in a private practice setting where time is at a premium.Future research may want to add additional similar items to better assess the internalconsistency reliability of these particular response items.
Replication of the present study’s results using a similar regression analysis approachwith a very similar study methodology with substance dependent individuals has been completed(Pekala & Maurer, 2010). The present study’s regression results were replicated with a differentsubject group using a very similar design suggesting that the lack of internal consistency reliabilityfor the aforementioned variables did not affect replication, i.e., very similar Rs were generated whensimilar regression analyses were completed. However, it is unknown to what extent these resultsmight generalize to other types of populations such as college students, or in different stimulusenvironments, or with different instructional sets, etc. Future research is needed.
The PCI is completed in reference to a short sitting quietly period embedded in the PCI-HAP.Because the PCI and predecessor instruments were developed to assess subjective experiencesassociated with a short stimulus interval (Pekala, 1980; Pekala, 1991a), the PCI is a “state” assessmentinstrument (as opposed to the “trait” nature of the Harvard or the Stanford C). The PCI is assessingthe fleeting and variable contents of mind or consciousness, which functionalists, such as Angell(1907) and James (1890/1950), pointed out over a 100 years ago, are quite evanescent. Hence, thetest-retest reliabilities of the PCI (sub)dimensions are not as high as one would anticipate with theusual trait instruments that social scientists are accustomed to using.9
Although no test-retest data is available on the PCI (sub)dimensions, test-retest reliabilities,in reference to an eyes closed sitting quietly period, are available with a predecessor to the PCI, the PCQ(Phenomenology of Consciousness Questionnaire; Pekala, 1980; Pekala & Levine, 1981, 1982), whichhas many similar (sub)dimensions. Pearson rs averaged .43 across all PCQ major dimensions;considerably lower than the .70 usually deemed adequate for trait scales (Nunnally, 1976).
Hence, the nature of the stimulus context and setting, the instructional set, andeven the mood of the person immediately before testing can influence the phenomenologicalresults obtained with the PCI. More research needs to be completed using the PCI inreference to various instructional sets and context variables associated with particular stimulusconditions to better determine the reliability and validity of this approach for quantifying subjectiveexperiences. Methodological and statistical issues related to assessing such subjective experiencescan be found in Pekala (1991a), Pekala and Cardeña (2000), and Pekala and Kumar (2007). Theinterested reader is also referred to: a) the interpretive manual (Pekala, 2009b)2 that was developedfor using the PCI-HAP, which reviews some of these limitations in more detail, especially from a

312
Suggestiblity, Expectancy, and Trance State Effects 2
References
Angell, J. (1907). The province of functional psychology. The Psychological Review, 14, 61-91.Barabasz, A., & Watkins, J. G. (2005). Hypnotherapeutic techniques: 2E. New York: Brunner-Routledge.Barber, T. X. (2000). A deeper understanding of hypnosis: Its secrets, its nature, its essence.
American Journal of Clinical Hypnosis, 42, 208-272.Barnes, S. M., Lynn, S. J., & Pekala, R. J. (2009). Not all hypnotic suggestibility scales are
created equal: Individual differences in behavioral and subjective responses.Consciousness and Cognition, 18, 255-265.
Barnier, A. J., & McConkey, K.M. (2003). Hypnosis, human nature, and complexity: Integratingneuroscience approaches into hypnosis research. International Journal of Clinicaland Experimental Hypnosis, 51, 282-308.
Benham, G., Woody, E. Z., Wilson, K. S., & Nash, M. R. (2006). Expect the unexpected: Ability,attitude and responsiveness to hypnosis. Journal of Personality and SocialPsychology, 91, 342-350.
clinical perspective; and b) a PowerPoint (Pekala, 2009b)10 presentation, which reviews how thisempirical phenomenological approach to consciousness can help us better understand hypnotism,including the constraints and limitations of such an approach.
Hypnotism and Alice in Wonderland: Towards an Integrated UnderstandingAlice in Wonderland (Carroll, 1960) fell down the rabbit hole, an abyss probably as
confusing to Alice as hypnotism is to us. During a subsequent competition described in thenovel, all participants were proclaimed to have won, and all were given prizes, highlightingthe importance each participant had in the competition. Many researchers and clinicians toonumerous to mention should all be commended for jumping into the rabbit hole!
The self-reported hypnotic depth score does indeed appear to be an attribution thatis a function of several component processes, as many have theorized concerning hypnotism.Because some participants will make attributions concerning their level of hypnotic depth dueto the vivid imagery experienced; others, due to their inability to open their eyes when asked todo so; and/or others, due to their subjective experiences of hypnotism, all colored by expectancy,it may not be surprising that hypnotism over the last two centuries has been defined to beeverything from animal magnetism and altered states of consciousness, to “only” imaginationor suggestion. Different suggestions, using different hypnotic assessments/interventions,and/or different contexts across participants of differing hypnotic responsivity, would likewisebe deemed to alter attributions, and hence what it means for the individual to be hypnotized.
In addition, we believe that the mystery of hypnotism, and how it relates to thealtered states of consciousness debate (Kallio & Revonsuo, 2003, 2005), can be more fullydeciphered using the aforementioned phenomenological methodology (Pekala, 1980, 1991a;Pekala & Cardeña, 2000; Pekala & Kumar, 2000, 2007), in conjunction with traditional cognitive/behavioral methodologies employing the Harvard, the Stanford C, and the HIP. Theprovocative debates seen in our field (Frischholz, 2000; Hammond, 1998; Kihlstrom, 2003,2005; Lynn, Kirsch, Knox, Fassler, & Lilienfeld, 2007, Lynn & Sherman, 2000) attests to thetremendous complexity associated with this most fascinating of enigmas. Perhaps suchdebates will eventually engender an equally provocative, but integrated, theoreticalunderstanding of that mystery we call hypnotism.
313
Pekala, et al.
Bowers, K. S. (1993). The Waterloo-Stanford Group C (WSGC) Scale of HypnoticSusceptibility: Normative and comparative data. International Journal of Clinicaland Experimental Hypnosis, 41, 35-46.
Brown, D. P., & Fromm, E. (1986). Hypnotherapy and hypnoanalysis. Hillsdale, NJ: LawrenceErlbaum Associates.
Cardeña, E. A. (2005). The phenomenology of deep hypnosis: Quiescent and physicallyactive. International Journal of Clinical and Experimental Hypnosis, 53, 1-12.
Carroll, L. (1960). Alice in wonderland. New York: Books, Inc.Erickson, M. H., Rossi, E. L., & Rossi, S. I. (1976). Hypnotic realities: The induction of
clinical hypnosis and forms of indirect suggestion. New York: Irvington Publishers.Ericsson, K. A., & Simon, H. A. (1980). Verbal reports as data. Psychological Review, 87, 215-251.Forbes, E., & Pekala, R. J., (1993). Predicting hypnotic susceptibility via a phenomenological
approach. Psychological Reports, 73, 1251-1256.Forbes, R. J., & Pekala, R. J. (1996). Types of hypnotically (un)susceptible individuals as a
function of phenomenological experience: A partial replication. Australian Journalof Clinical and Experimental Hypnosis, 24, 92-109.
Frischholz, E. J. (2000). What is hypnosis? American Journal of Clinical Hypnosis, 42, 174.Grimm, L. G., & Yarnold, R. R. (1995). Reading and understanding multivariate statistics.
Washington, DC: American Psychological Association.Hammond, D. C. (1990). Handbook of hypnotic suggestions and metaphors. New York: W.
W. Norton & Company.Hammond, D. C. (1998) Guest editorial - The need for clinically relevant research. American
Journal of Clinical Hypnosis, 41, 2-9.Hand, J., Pekala, R. J., & Kumar, V. K. (1995). Prediction of Harvard and Stanford Scale scores
with a phenomenological instrument. Australian Journal of Clinical andExperimental Hypnosis, 23, 124-134.
Hilgard, E. R. (1965). The experience of hypnosis. New York: Harcourt Brace Jovanovich.Holroyd, J. (2003). The science of meditation and the state of hypnosis. American Journal
of Clinical Hypnosis, 46, 109-128.Hunt, H. T., & Chefurka, C. M. (1976). A test of the psychedelic model of altered states of
consciousness. Archives of General Psychiatry, 33, 867-876.James, W. (1890/1950).The principles of psychology, Vols. 1 and 2. New York: Dover Press.Kallio, S., & Revonsuo, A. (2003). Hypnotic phenomena and altered states of consciousness:
Multilevel framework of description and explanation. Contemporary Hypnosis, 20, 111-164.Kallio, S., & Revonsuo, A. (2005). Altering the state of the altered state debate: Reply to
commentaries. Contemporary Hypnosis, 22, 46-55.Kihlstrom, J. F. (1997). Convergence in understanding hypnosis? Perhaps, but not so fast.
International Journal of Clinical and Experimental Hypnosis, 45, 324-332.Kihlstrom, J. (2003). The fox, the hedgehog, and hypnosis. International Journal of Clinical
and Experimental Hypnosis, 51, 166-189.Kihlstrom, J. F. (2005). Is hypnosis an altered state of consciousness or what? Contemporary
Hypnosis, 2, 34-38.Kihlstrom, F. F. (2008). The domain of hypnosis, revisited. In M. R. Nash & A. J. Barnier
(Eds.). The Oxford handbook of hypnosis: Theory, research, and practice. (pp. 21-52). London: Oxford University Press.
Kirsch, I. (1985). Response expectancy as a determinant of experience and behavior. AmericanPsychologist, 40, 1189-1202.
314
Suggestiblity, Expectancy, and Trance State Effects 2
Kirsch, I. (1991). The social learning theory of hypnosis. In S. J. Lynn & J. W. Rhue (Eds.).Theories of hypnosis: Current models and perspectives (pp. 439-465). New York: Guilford.
Kirsch, I. (1997). Suggestibility or hypnosis: What do our scales really measure? InternationalJournal of Clinical and Experimental Hypnosis, 45, 212-225.
Kirsch, I. (2000). The response set theory of hypnosis. American Journal of ClinicalHypnosis, 42, 274-292.
Kirsch, I., & Braffman, W. (1999). Correlates of hypnotizability: The first empirical study.Contemporary Hypnosis, 16, 224-230.
Kirsch, I., & Braffman, W. (2001). Imaginative suggestibility and hypnotizability. CurrentDirections in Psychological Science, 10, 57-61.
Kukla, A. (1983). Toward a science of experience. Journal of Mind and Behavior, 4, 231-246.Kumar, V. K., & Pekala, R. J. (1988). Hypnotizability, absorption, and individual differences in
phenomenological experience. International Journal of Clinical and ExperimentalHypnosis, 36, 17-22.
Kumar, V. K., & Pekala, R. J. (1989). Variations in phenomenological experience as a functionof hypnosis and hypnotic susceptibility: A replication. British Journal ofExperimental and Clinical Hypnosis, 6, 17-22.
Kumar, V. K., Pekala, R. J., & Cummings, J. (1996). Trait factors, state effects, and hypnotizability.International Journal of Clinical and Experimental Hypnosis, 44, 232-249.
Kumar, V. K., Pekala, R. J., & Marcano, G. (1996). Hypnotizability, dissociativity, andphenomenological experience. Dissociation, 9, 143-153.
Kumar, V. K., Pekala, R. J., & McCloskey, M. (1999). Phenomenological state effects duringhypnosis: A cross-validation of findings. Contemporary Hypnosis, 16, 9-22.
Laurence, J. R., & Nadon, R. (1986). Reports of hypnotic depth: Are they more than merewords? International Journal of Clinical and Experimental Hypnosis, 34, 215-233.
LeCron, L. M. (1953). A method of measuring the depth of hypnosis. Journal of Clinical andExperimental Hypnosis, 1, 4-7.
Lieberman, D. A. (1979). Behaviorism and the mind: A (limited) call for a return to introspection.American Psychologist, 34, 319-333.
Lynn, S. J., & Kirsch, (2006). Essentials of clinical hypnosis: An evidence-based approach.Washington, DC: American Psychological Association.
Lynn, S. J., Kirsch, I., Knox, J., Fassler, O., & Lilienfeld, S.O. (2007). Hypnosis and neuroscience:Implications for the altered state debate. In G. A. Jamieson (Ed.). Hypnosis and consciousstates: The cognitive neuroscience perspective (pp. 143-165). London: Oxford University Press.
Lynn, S. J., & Rhue, J. W. (1986). The fantasy prone person: Hypnosis, imagination, andcreativity. Journal of Personality and Social Psychology, 51, 404-408.
Lynn, S. J., & Rhue, J. W. (1988). Fantasy proneness: Hypnosis, developmental antecedents,and psychopathology. American Psychologist, 43, 35-44.
Lynn, S. J., & Sherman, S. J. (2000). The clinical importance of sociocognitive models ofhypnosis: Response set theory and Milton Erickson’s strategic interventions.American Journal of Clinical Hypnosis, 42, 294-315.
Maurer, R. L., Kumar, V. K., Woodside, L. N., & Pekala, R. J. (1997). Phenomenologicalexperience in response to monotonous drumming and hypnotizability. AmericanJournal of Clinical Hypnosis, 40, 130-146.
Mohl, J. C. , Kumar, V. K., & Pekala, R. J., (2007, August). The desire to be hypnotized:Intrinsic versus extrinsic motivation. Paper presented at the Annual Meeting of theAmerican Psychological Association, San Francisco, CA.

315
Pekala, et al.
Newton, R. R., & Rudstam, K. E. (1999). Your statistical consultant: Answers to your dataanalysis questions. London: Sage Publications.
Nisbett, R. E., & Wilson, T. D. (1977). Telling more than we can know: Verbal reports onmental processes. Psychological Review, 84, 231-259.
Nunnally, J. C. (1967). Psychometric theory. New York: McGraw-Hill.Orne, M. T. (1962). On the social psychology of the psychological experiment: With particular
reference to demand characteristics and their implications. American Psychologist, 17, 776-783.Pekala, R. J. (1980). An empirical-phenomenological approach for mapping consciousness
and its various “states.” (Doctoral dissertation, Michigan State University, 1980).44 (University Microfilm No. 82-02, 489)
Pekala, R. J. (1982). The phenomenology of consciousness inventory. Thorndale, PA:Psychophenomenological Concepts. (Now published by Mid-Atlantic EducationalInstitute. See Pekala, 1991b).
Pekala, R. J. (1991a). Quantifying consciousness: An empirical approach. New York: Plenum Press.Pekala, R. J. (1991b). The Phenomenology of Consciousness Inventory. West Chester, PA:
Mid-Atlantic Educational Institute.Pekala, R.J. (1995a). A short unobtrusive hypnotic induction for assessing hypnotizability
level: I. Development and research. American Journal of Clinical Hypnosis, 37, 271-283.Pekala, R. J. (1995b). A short unobtrusive hypnotic induction for assessing hypnotizability:
II. Clinical case reports. American Journal of Clinical Hypnosis, 37, 284-293.Pekala, R. J. (2002). Operationalizing “trance.” II. Clinical application using a
psychophenomenological approach. American Journal of Clinical Hypnosis, 44, 241-255.Pekala, R. J. (2009a, October). The puzzles and perplexities of hypnotism: How
phenomenology can help. Keynote address given at the Annual Meeting of theSociety for Clinical and Experimental Hypnosis, Reno, Nevada.
Pekala, R. J. (2009b, October). Therapist’s Manual: Interpretation of the Phenomenology ofConsciousness Inventory: Hypnotic Assessment Procedure (PCI-HAP).Unpublished manual.
Pekala, R. J. & Cardeña, E. (2000). Methodological issues in the study of altered states ofconsciousness and anomalous experiences. In E. Cardeña, S. J. Lynn, and S. Krippner(Eds.). Varieties of anomalous experience. (pp. 47-82). Washington, DC: AmericanPsychological Association.
Pekala, R. J., & Ersek, B. (1992/93). Fire walking versus hypnosis: A preliminary studyconcerning consciousness, attention, and fire immunity. Imagination, Cognition,and Personality, 12, 207-229.
Pekala, R. J., Forbes, E., & Contriasani, P. (1988). Hypnoidal effects associated with severalstress management strategies. Australian Journal of Clinical and ExperimentalHypnosis, 16, 121-132.
Pekala, R. J., & Kumar, V. K. (1984). Predicting hypnotic susceptibility by a self-reportphenomenological state instrument. American Journal of Clinical Hypnosis, 27, 114-121.
Pekala, R. J., & Kumar, V. K. (1986). The differential organization of the structures of consciousnessduring hypnosis and a baseline condition. Journal of Mind and Behavior, 7, 515-539.
Pekala, R. J., & Kumar, V. K. (1987). Predicting hypnotic susceptibility by a self-reportphenomenological state instrument. American Journal of Clinical Hypnosis, 30, 57-65.
Pekala, R. J., & Kumar, V. K. (1989). Patterns of consciousness during hypnosis: Relevanceto cognition and individual differences. Australian Journal of Clinical andExperimental Hypnosis, 17, 1-20.

316
Suggestiblity, Expectancy, and Trance State Effects 2
Pekala, R. J., & Kumar, V. K. (2000). Operationalizing “trance.” I. Rationale and research usinga psychophenomenological approach. American Journal of Clinical Hypnosis, 43, 107-135.
Pekala, R. J., & Kumar, V. K. (2007). An empirical-phenomenological approach to quantifyingconsciousness and states of consciousness: With particular reference tounderstanding the nature of hypnosis. In G. Jamieson (Ed.). Towards a cognitive-neuroscience of hypnosis and conscious states: A resource for researchers,students, and clinicians. (pp. 167-194). London: Oxford University Press.
Pekala, R. J., Kumar, V. K., & Marcano, G. (1996). Hypnotic types: A partial replicationconcerning phenomenal experience. Contemporary Hypnosis, 12, 194-200.
Pekala, R. J., Kumar, V. K., & Maurer, R. (2009, October). The Phenomenology of ConsciousnessInventory: Hypnotic Assessment Procedure (PCI-HAP): Administrator’s Manual.Unpublished manual.
Pekala, R. J., Kumar, V. K., Maurer, R., Elliott-Carter, N., & Moon, E. (2006). “How deeplyhypnotized did I get?” Predicting self-reported hypnotic depth from aphenomenological assessment instrument. International Journal of Clinical andExperimental Hypnosis, 54, 316-339.
Pekala, R. J., Kumar, V. K., Maurer, R., Elliott-Carter, N., Moon, E., & Mullen, K. (2010).Suggestibility, Expectancy, Trance State Effects, and Hypnotic Depth: I. Implicationsfor Understanding Hypnotism. American Journal of Clinical Hypnosis, 52, 271-286.
Pekala, R. J. & Levine, R. L. (1981). Mapping consciousness: Development of an empirical-phenomenological approach. Imagination, Cognition, and Personality: TheScientific Study of Consciousness, 1, 29-47.
Pekala, R. J., & Levine, R. L. (1982). Quantifying states of consciousness via an empirical-phenomenological approach. Imagination, Cognition, and Personality: TheScientific Study of Consciousness, 2, 51-71.
Pekala, R. J., & Maurer, R. (2010). Self-reported hypnotic depth, suggestibility, expectancy,and trance state effects: A replication. Paper accepted for presentation at AmericanPsychological Association Annual Convention in San Diego, CA.
Pekala, R. J., & Nagler, R. (1989). The assessment of hypnoidal states: Rationale and clinicalapplication. American Journal of Clinical Hypnosis, 31, 231-236.
Pekala, R. J., Steinberg, J., & Kumar, V. K. (1986). Measurement of phenomenological experience:Phenomenology of Consciousness Inventory. Perceptual and Motor Skills, 63, 983-989.
Pekala, R. J., & Wenger, C. F. (1983). Retrospective phenomenological assessment: Mappingconsciousness in reference to specific stimulus conditions. Journal of Mind andBehavior, 4, 247-274.
Schumaker, J. F. (Ed.). (1991). Human suggestibility: Advances in theory, research, andapplication. New York: Routledge.
Sheehan, P. W. (1979). Hypnosis and the processes of imagination. In E. Fromm & R, E. Shor(Eds.) Hypnosis: Developments in research and new perspectives, (2nd ed., pp.381-411). New York: Aldine.
Sheehan, P. W., & McConkey, K. M. (1982). Hypnosis and experience: The exploration ofphenomena and process. Hillsdale, NJ: Lawrence Erlbaum.
Shor , R. E. , & Orne, E. C. (1962). The Harvard Group Scale of Hypnotic Susceptibility. PaloAlto, CA: Consulting Psychologists Press.
Singer J. L., & Kolligian, J. Jr. (1987). Personality: Developments in the study of privateexperience. Annual Review of Psychology, 38, 533-574.

317
Pekala, et al.
Smith, E., & Miller, F. (1978). Limits on perception of cognitive processes: A reply to Nisbettand Wilson. Psychological Review, 85, 355-362.
Spiegel, H., & Spiegel, H. (2004). Trance and treatment: Clinical uses of hypnosis. (2nd ed.)Washington, DC: American Psychiatric Press.
Tart, C. T. (1970). Self-report scales of hypnotic depth. International Journal of Clinical andExperimental Hypnosis, 18, 105-125.
Tart, C. T. (1979). Measuring the depth of an altered state of consciousness with particularreference to self-report scales of hypnotic depth. In E. Fromm & R. E. Shor (Eds.), Hypnosis:Developments in research and new perspectives (2nd ed., pp. 567-601). New York: Aldine.
Wagstaff, G. F., Cole, J. C., & Brunas-Wagstaff, J. (2008). Measuring hypnotizability: Thecase for self-report depth scales and normative data for the Long Stanford Scale.International Journal of Clinical and Experimental Hypnosis, 56, 119-142.
Weiten, W. (2001). Psychology: Themes and variations (5th Ed.). New York: Brooks Cole.Weitzenhoffer, A. M. (1989). The practice of hypnotism: Volume 1: Traditional and semi-
traditional techniques and phenomenology. New York: John Wiley and Sons.Weitzenhoffer, A. M. (2002). Scales, scales, and more scales. American Journal of Clinical
Hypnosis, 44, 209-220.Weitzenhoffer, A. M., & Hilgard, E. (1962). Stanford Hypnotic Susceptibility Scale: Form C.
Palo Alto, CA: Consulting Psychologists Press.Wilkinson, L. (1998). SYSTAT. Evanston, IL: SYSTAT.Woodside, L. N., Kumar, V. K., & Pekala, R. J. (1997). Monotonous percussion drumming and trance
postures: A controlled evaluation of phenomenological effects. Anthropology ofConsciousness, 8, 69-87.
Woody, E. Z., Barnier, A. J., & McConkey, K. M. (2005). Multiple hypnotizabilities:Differentiating the building blocks of hypnotic response. PsychologicalAssessment, 17, 200-211.
Woody, E. Z., Drugovic, M., & Oakman, J. M. (1997). A reexamination of the role ofnonhypnotic suggestibility in hypnotic responding. Journal of Personality andSocial Psychology, 72, 399-407.
Woody, E. Z., & McConkey, K. M. (2003). What we don’t know about the brain and hypnosis,but need to: A view from the Buckhorn Inn. International Journal of Clinical andExperimental Hypnosis, 51, 309-338.
Footnotes
This research is partially based on two $5,000 grants received from the Veterans AdministrationStars and Stripes (VISN4) Healthcare Network. This paper is based, in part, on a presentationgiven at the Annual Meeting of the American Society of Clinical Hypnosis and the Society ofClinical and Experimental Hypnosis in Dallas, Texas, January, 2007. The authors wish tothank the staff of wards 39A and 39B of the Coatesville VA Medical Center for their supportin doing this research. The authors also wish to thank Mr. Stephen Lankton and Dr. EdwardFrischholz for their suggestions and remarks, and Drs. Jean Holroyd and Erik Woody fortheir comments and suggestions on an earlier version of this paper, in addition to the commentsof an anonymous reviewer. The contents of this presentation does not represent the viewsof the Department of Veterans Affairs nor the United States Government.

318
Suggestiblity, Expectancy, and Trance State Effects 2
1The PCI includes 5 items of similar or identical content that are used to generate a measure of howreliably participants completed the PCI. Scores above 2.3 are considered to be unreliable.
2Copies of the PCI (Pekala, 1982, 1991b), the PCI-HAP (Pekala, 1995a, 1995b), the therapistand self-report pre- and post-assessment forms, the administration (Pekala, Kumar, & Maurer,2009b) and interpretative (Pekala, 2009b) manuals, and the EXCEL scoring program are availableat www.quantifyingconsciousness.com.
3For the data analysis, the scoring for the finger raising item and the fell asleep item werereversed to allow for more intuitive interpretation of the results.
4Excluding the dummy variables: the finger response and negative effects items.
5Standardized coefficients, however, do not tell us of the unique variance accounted for by aparticular predictor. For this semi-partial correlation analyses are needed. The unique varianceattributable to a particular predictor is the change in R2 when this variable is added to theregression equation, called a squared semi-partial correlation. Hence, the standardized regressioncoefficients can only tell us of their relative influence on the dependent variable. Suchstandardized coefficients are useful “when assessing the effects of different variables within asingle regression equation or population” (Newton & Rudestam, 1999, p. 268) as was donehere; such regression coefficients are not useful when comparing across populations.
6Many theorists (see Schumaker, 1991) define suggestibility as more than just fantasy, imagery,or imagination. The aspect of suggestibility assessed by this study, imagoic suggestibility,we believe to be an important. However, we believe it is not the only aspect of suggestibility.
7Because this study used only the upper and lower portions of the Stanford C distribution tocompute this correlation, we believe the way the analyses were done inflated the correlation,and the correlation would have been lower had the full distribution been used.
8Because all variables were measured during one session, the results, we believe, are pertinentto clinical situations where such measurements are typically obtained in one session. Webelieve those aspects of subjective experience, as measured by the PCI/PCI-HAP, are afunction of organismic, contextual, and instructional variables, as the functionalintrospectionists (Angell, 1907; James, 1890/1950) have argued over a century ago.
9One can question the relevance of comparing the test-retest reliabilities of the (sub)dimensions ofthe PCI to that of trait instruments, since the PCI dimensions are assessing “state,” as opposed to“trait,” effects. However, this difference is highlighted since the PCI, as part of the PCI-HAP, ismeasuring different, i.e., phenomenological, processes than the usual hypnotizability trait instruments.
10The PowerPoint presentation can be obtained by emailing: [email protected].
Author’s Note
1Coatesville VA Medical Center, Coatesville, PA2West Chester University of Pennsylvania, West Chester, PA