Romanian Journal of Ophthalmology · Ovidiu Musat, M.D., Ph.D. Bucharest, Romania . ... Zurac...
89
Romanian Journal of Ophthalmology Romanian Society of Ophthalmology www.rjo.ro Volume 61, Issue 3, 2017 INDEXED BY: MEDLINE/PUBMED
Transcript of Romanian Journal of Ophthalmology · Ovidiu Musat, M.D., Ph.D. Bucharest, Romania . ... Zurac...

RomanianJournal ofOphthalmology
Romanian Society of Ophthalmologywww.rjo.ro
Volume 61, Issue 3, 2017
INDEXED BY: MEDLINE/PUBMED

Romanian Journal of Ophthalmology
EDITOR-IN-CHIEF Mihail Zemba, M.D., Ph.D. Bucharest, Romania
E-mail: [email protected]
ASSOCIATE EDITOR Ovidiu Musat, M.D., Ph.D. Bucharest, Romania
E-mail: [email protected]
EXECUTIVE EDITOR Prof. Victor Lorin Purcarea, Ph.D. Bucharest, Romania
E-mail: [email protected]
ASSISTANT EDITORS Horia Stanca, M.D., Ph.D. Bucharest, Romania
E-mail: [email protected] Daniel Branisteanu, M.D., Ph.D. Iasi, Romania
E-mail: [email protected]
INTERNATIONAL EDITORIAL ADVISORY BOARD Prof. Khaled al Rakhawy, M.D., Ph.D. Cairo, Egipt Daniel Baron M.D., Ph.D. Nantes, France Prof. Zsolt Biro M.D., Ph.D. Pecs, Hungary Prof. Derald Brackmann M.D., Ph.D. Los Angeles, USA Thierry Chazalon M.D., Ph.D. Nantes, France Prof. Gabriel Coscas M.D., Ph.D. Paris, France Prof. J.J. De Laey M.D., Ph.D. Gent, Belgium Prof. Fabian Hoehn M.D., Ph.D. Pforzheim, Germany
Prof. Christian Paul Jonescu-Cuypers M.D., Ph.D. Berlin, Germany Prof. Slobodanka Latinovic M.D., Ph.D. Novi Sad, Serbia Prof. Dan Milea M.D., Ph.D. Angers, France Gabor Rado M.D., Ph.D. Budapest, Hungary Prof.Gabor Scharioth M.D., Ph.D. Recklinghausen, Germany Prof. Wolfgang Schrader M.D., Ph.D. Wuerzburg, Germany Prof. Fankhauser Franz M.D., Ph.D. Bern, Switzerland
NATIONAL EDITORIAL ADVISORY BOARD Assoc.Prof. Florian Balta, M.D., Ph.D. Bucharest, Romania Prof. Dorin Chiselita M.D., Ph.D. Iasi, Romania Assoc. Prof. Mircea Filip M.D., Ph.D. Bucharest, Romania Prof. Mihnea Munteanu M.D., Ph.D. Timisoara, Romania Daniela Selaru M.D., Ph.D. Bucharest, Romania
Assoc.Prof. Cristina Stan M.D., Ph.D. Cluj Napoca, Romania Prof. Adriana Stanila M.D., Ph.D. Sibiu, Romania Cornel Stefan M.D., Ph.D. Bucharest, Romania Prof. Dr. Calin Tataru M.D.,Ph.D. Bucharest, Romania Prof.Dr. Cristina Vladutiu M.D., Ph.D. Cluj Napoca, Romania
NATIONAL EDITORIAL BOARD Gheorghe Anghel M.D., Ph.D. Bucharest, Romania Eugen Bendelic M.D., Ph.D. Chisinau, Republic of Moldova Camelia Bogdanici M.D., Ph.D. Iasi, Romania Daniel Branisteanu M.D., Ph.D. Iasi, Romania Marian Burcea M.D., Ph.D. Bucharest, Romania Catalina Corbu M.D., Ph.D. Bucharest, Romania Mihaela Coroi M.D., Ph.D. Oradea, Romania Valeria Coviltir M.D., Ph.D. Bucharest, Romania Valeriu Cusnir M.D., Ph.D. Chisinau, Republic of Moldova Danut Costin M.D., Ph.D. Iasi, Romania Monica Gavris M.D., Ph.D. Cluj Napoca, Romania Karin Horvath M.D., Ph.D. Tg. Mures, Romania Sanda Jurja M.D., Ph.D. Constanta, Romania
Carmen Mocanu M.D., Ph.D. Craiova, Romania Cristina Nicula M.D., Ph.D. Cluj Napoca, Romania Monica Pop M.D., Ph.D. Bucharest, Romania Mihai Pop M.D., Ph.D. Bucharest, Romania Alina Popa-Cherecheanu M.D., Ph.D. Bucharest, Romania Vasile Potop M.D., Ph.D. Bucharest, Romania Speranta Schmitzer M.D., Ph.D. Bucharest, Romania Horia Stanca M.D., Ph.D. Bucharest, Romania Ioan Stefaniu M.D., Ph.D. Bucharest, Romania Simona Talu M.D., Ph.D. Cluj Napoca, Romania Liliana Voinea M.D., Ph.D. Bucharest, Romania Mihail Zemba, M.D., Ph.D. Bucharest, Romania
PUBLISHING EDITORS Consuela Madalina Gheorghe, Bucharest, Romania Dodu Petrescu, Bucharest, Romania Petrut Radu, Bucharest, Romania
EDITORIAL OFFICE "Dr. Carol Davila"Central Military University Emergency Hospital 134 Calea Plevnei Street, District 1, Bucharest, Romania Phone number/Fax: +40.21.3137189 E-mail:[email protected], Typesetting and cover graphic: P. Radu
Volume 61, Issue 3 July-September 2017
© All the rights on the journal belong to the Romanian Society of Ophthalmology. The partial reproduction of the articles or of the figures is possible only with the written consent of the Romanian Society of Ophthalmology. The responsibility of the articles’ originality belongs entirely to the authors.
Print ISSN 2457 – 4325 ISSN-L 2457 - 4325
Online ISSN 2501-2533 ISSN–L 2457-4325
Printed at ''Carol Davila'' University Press, 8 Eroilor Sanitari Blvd., 050474 Bucharest, Romania

Romanian Journal of Ophthalmology Volume 61, Issue 3, July-September 2017
Contents
Editorial
Mihail Zemba 151
Reviews Citicoline – a neuroprotector with proven effects on glaucomatous disease Iulia Chitu, Ruxandra Tudosescu, Costin Leasu-Branet, Liliana-Mary Voinea
152
Glaucoma after penetrating keratoplasty Zemba Mihail, Stamate Alina-Cristina
159
Management of diplopia Iliescu Daniela Adriana, Timaru Cristina Mihaela, Alexe Nicolae, Gosav Elena, De Simone Algerino, Batras Mehd, Stefan Cornel
166
Update on retinal vascular caliber Dumitrescu Alina Gabriela, Voinea Liliana, Badarau Ioana Anca, Paun Vanessa Andrada, Schowe Marilena, Ciuluvica Radu
171
General articles
Investigating the perception of Romanian adults on ophthalmology services from an experiential marketing perspective Gheorghe Consuela-Mădălina, Gheorghe Iuliana-Raluca, Purcărea Victor Lorin
181
Transnasal endoscopic assisted dacryocystorhinostomy Hainăroșie Răzvan, Ioniță Irina, Pietroșanu Cătălina, Pițuru Silviu, Hainăroșie Mura, Zainea Viorel
188
Transnasal endoscopic orbital decompression Hainăroșie Răzvan, Ioniță Irina, Pietroșanu Cătălina, Pițuru Silviu, Hainăroșie Mura, Zainea Viorel
192
Cataract surgery outcome in patients with non-glaucomatous pseudoexfoliation Sastry Praveen Venkatesha, Singal Anuj Kumar
196
Functional results of cataract surgery in the treatment of phacomorphic glaucoma Moraru Andreea, Pînzaru Gabriela, Moţoc Anca, Costin Dănuţ
202
Incidence of ocular hypertension after intravitreal injection of anti-VEGF agents in the treatment of neovascular AMD Moraru Andreea, Pînzaru Gabriela, Moţoc Anca, Costin Dănuţ, Brănişteanu Daniel
207
Non-parametric tests in detecting glaucoma progression Pantalon Anca, Feraru Crenguța
212
Modeling the consumer’s perception of experiential marketing in the Romanian private ophthalmologic services Gheorghe Consuela-Mădălina, Gheorghe Iuliana-Raluca, Purcărea Victor Lorin
219
Case reports
Iris juvenile xanthogranuloma in an infant - spontaneous hyphema and secondary glaucoma Pantalon Anca, Ștefănache Tudor, Danciu Mihai, Zurac Sabina, Chiseliță Dorin
229

Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:151
EDITORIAL
151 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.28
Editorial
The Fourth Congress of the Romanian Society of Cataract and Refractive Surgery, connected with the Annual Conference of the Romanian Retina Society took place in the period 22-25 of June 2017, in Eforie Nord.
The association of these two conferences, already a tradition, was again a great success, with an audience of more than five hundred ophthalmologists from Romania and from abroad.
The event started on Thursday with an interesting symposium about the role of aflibercept in retinal pathology. Horia Stanca, MD, PhD, and Prof. Mihnea Munteanu, MD, PhD, shared their experience with this type of treatment.
The Conference continued with three very interesting lectures: Assoc. Prof. Florian Balta talked about vitamin D and retina, Daniel Branisteanu, MD, PhD, presented an update about the surgical treatment in retinology and Horia Stanca, MD, PhD, approached a very difficult issue: education in ophthalmology, talking about his experience with the educational system for residents in the USA.
The following day, the Congress of Romanian Society of Cataract and Refractive Surgery began. There were two days with a very dense schedule, very interesting topics being approached during the sessions: Ngenuity 3D Visualization System Platform, both for anterior and posterior pole surgery, new types of premium intraocular lenses, the role of vitreoretinal surgeon in managing ocular trauma, premium personalized intraocular lens and others.
The session about nightmares in ophthalmology was very much appreciated, during which, experienced surgeons shared their experience with very complicated cases.
The international participation was important, with interesting presentations of Prof. Usha Chakravarthy - Belfast – on OCT, Juergen Beierl on Refractive Corneal Topography and Prof. Sorcha Ni Dhunhgheill – Antwerp - on cataract surgery in children, bag in the lens technique.
An important event that also took place during this Congress was the election for the Board of Romanian Society of Cataract and Refractive Surgery. Prof. Calin Tataru, MD, PhD, the leader of this Society the last four years, presented a scientific and financial audit. The overall conclusion was that this was a remarkable period, with many achievements: four Congresses of the Society, the joint with the Conference of Romanian Retina Society, the print of the Guide for Cataract Surgery and many others.
The delegates appreciated very much the activity of the former President, so, after the voting, Prof. Calin Tataru, MD, PhD, remained President of Romanian Society of Cataract and Refractive Surgery for the next four years. He suggested and the delegates approved that the former Secretary and Treasurer would remain in duty. Musat Ovidiu, MD, PhD, and Madalina Serban, MD, PhD, were confirmed as Secretary and Treasurer by the delegates.
Finally, a vote for two vice presidents established that Dorin Nicula, MD, PhD, and Mihail Zemba, MD, PhD, would join the Board of Romanian Society of Cataract and Refractive Surgery for the next four years.
The Editorial Board of Romanian Journal of Ophthalmology wishes great success to all of them. Editor-in-Chief
Mihail Zemba, MD, PhD

Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:152-158
REVIEW
152 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.29
Citicoline – a neuroprotector with proven effects on glaucomatous disease
Iulia Chitu, Ruxandra Tudosescu, Costin Leasu-Branet, Liliana-Mary Voinea Department of Ophthalmology, University Emergency Hospital, Bucharest, Romania Correspondence to: Iulia Chițu Department of Ophthalmology, University Emergency Hospital, Bucharest, 169 Splaiul Independenței Street, Code 050098, Bucharest, Romania Mobile phone: +40746 010 314, E-mail: [email protected] Accepted: September 9th, 2017
Abstract Citicoline is the generic name of cytidine-5’-diphosphocholine (CDP-choline), an endogenous compound that is able to increase the levels of neurotransmitters in the central nervous system by interacting with the synthesis of cellular membranes phospholipids, especially phosphatidylcholine. Exogenous Citicoline, administered by ingestion or injection, is hydrolyzed and dephosphorylated in order to form cytidine and choline, which resynthesize CDP-choline inside brain cells. It has proven neuroprotective effects in Alzheimer disease, stroke, and Parkinson’s disease, as well as in glaucoma and amblyopia. Citicoline acts as a neuroprotector for those patients with progressive glaucomatous disease in spite of well-controlled intraocular pressure. The purpose of this review was to outline the main features of Citicoline and the evidences of its effect in glaucoma. Keywords: Citicoline, neuroprotection, glaucoma
Pharmacology and effects
Cytidine-5’-diphosphocholine (CDP-choline, CDPCho) or Citicoline is a pharmaceutical substance identical with the natural compound, and has an important role in the phospholipid synthesis. In 1050s, Kennedy and collaborators showed that Citicoline is a precursor of phosphatidylcholine (PC), one of the most important phospholipid of the cell membrane [1].
Phospholipids are major constituents of cell membrane, with a high turnover rate, thus the continuous synthesis of these substances ensure the optimal structure and function of the cell.
CDP-Choline is a mononucleotide made of ribose, pyrophosphate, cytosine and choline, and its chemical structure is illustrated in Fig. 1 [2].
The CDP-choline pathway is the pathway of the novo synthesis of phosphatidylcholine and includes the enzymes cytidine kinase (CK), choline phosphate cytidilyltransferase (CCT) and
Fig. 1 Chemical structure of Citicoline

Romanian Journal of Ophthalmology 2017; 61(3): 152-158
153
Romanian Society of Ophthalmology © 2017
CDP-choline:1,2-diacylglicerol choline phosphotransferase (CTP). In this pathway, choline is provided by PC turnover and transport into the cell (Fig. 2) [1].
The term “Citicoline” was first introduced in the 1970s when the substance was used as a drug. Manaka et al. from Japan administered Citicoline for the first time in 1974 for Parkinson’s disease.
When administered (orally or parenterally), Citicoline is quickly metabolized (minutes) and transformed in pyrimidinergic and cholinergic catabolites. It is a safe molecule, with only few adverse effects, such as digestive intolerance after oral administration. The therapeutic dosage in humans is 500-2000 mg Citicoline daily (7-28 mg/ kg) [1].
The most important phospholipids are phosphatidylinositol, phosphatidylethanolamine, phosphatidylcholine, and sphingomyelin. They are part of cell membrane and ensure its function, like enzymatic processes of membrane, linking receptors and intracellular signals, and maintaining the cell homeostasis. The mechanism of some neurodegenerative diseases, such as vascular dementia, Alzheimer disease, and cognitive impairment involve specific changes in neuronal membrane and metabolism of structural phospholipids. The apoptotic cascade is triggered by phosphatidylcholine metabolism changes. CDP-choline is also linked to acetylcholine metabolism. Thus, exogenous Citicoline administration provides choline for acetylcholine synthesis [2].
Pharmacokinetics
When administered orally or intravenous, Citicoline is converted to cytidine and choline, its main circulating metabolites. Plasmatic cytidine is then converted to uridine, and, this results in
uridine phosphate inside the brain. At neuronal level, this is transformed to cytidine triphosphate. After administration, Citicoline rapidly diffuses to the tissues and is actively used. It can be found in liver, brain, and kidney. The excretion of CDP-choline is by urinary or fecal route and in expired CO2.
Citicoline provides neuroprotection by few mechanisms such as the following: maintains sphingomyelin and cardiolipin levels (constituent of inner mitochondrial membrane), restores the phosphatidylcholine (PtdCho) levels, increases the activity of glutathione reductase activity and the glutathione synthesis, decreases lipid peroxidation, and restores the activity of Na+/K+ ATPase. It is also involved in acetylcholine synthesis, providing choline [3].
Cytidine and choline are the two parts of Citicoline connected by a diphosphate bridge. After being absorbed, cytidine and choline are re-phosphorylated, and Citicoline is recreated from choline monophosphate and cytidine triphosphate.
In the course of PtdCho synthesis, choline monophosphate is added to PtdCho, releasing cytidine 5’-monophosphate (CMP). CMP can be used for DNA or RNA synthesis. The acetylation of choline part of Citicoline leads to acetylcholine.
Studies have shown that Citicoline is almost completely absorbed when it is orally administered and only a small part of it is excreted. Citicoline metabolites reach the brain in about 30 minutes after administration, but the blood level has a slow increase, with a peak at 6 hours after the oral intake.
The choline is used by cholinergic neurons in two metabolic pathways: synthesis of PtdCho and the neurotransmitter acetylcholine. The two pathways compete for the available choline, which is used preferentially for acetylation. When choline is depleted, phospholipids (PtdCho) are hydrolyzed in order to restore choline levels. Acetylcholine synthesis is favored when the available amount of choline is limited. Therefore, Citicoline is a source of choline, avoiding PtdCho hydrolysis and cholinergic neurons death.
Choline liberated from Citicoline can be metabolized to glutathione, one of the most important endogenous antioxidant defense systems in the brain. Glutathione has a
Fig. 2 The CDP-choline pathway
Romanian Journal of Ophthalmology 2017; 61(3): 152-158
154 Romanian Society of Ophthalmology
© 2017
neuroprotective role by decreasing lipid peroxidation. Citicoline has proven effects in cerebral edema reduction by restoring Na+/K+-ATPase activity in traumatic brain injury and transient focal or global ischemia [3].
Having these properties, Citicoline has been studied as a promising therapeutic agent in brain ischemia, Parkinson’s disease, Alzheimer’s disease and ocular diseases such as glaucoma, non-arteritic ischemic neuropathy and amblyopia.
Use of Citicoline in neurological diseases – evidence
Many experimental studies have proven the protective effects of Citicoline in stroke models by reducing the infarct volume and brain edema, leading to improvement of neurological deficits. In these studies, Citicoline was used as a single therapy or in combination with others agents [4]. Moreover, the benefic role of Citicoline was reported in clinical stroke trials when administered soon after ischemia.
In Alzheimer’s disease, Citicoline may inhibit the deposition of beta-amyloid, a neurotoxic protein involved in the pathophysiology of the disease [5]. It is believed to be an interaction between the formation of amyloid peptides and membrane phospholipids disintegration.
Alvarez et al. [6] revealed in a study performed on 30 patients with Alzheimer’s disease that after 12 weeks of treatment with Citicoline, the cognitive performance increased, and this was more pronounced in patients with mild dementia. It was also an increase of cerebral blood flow velocity and of brain bioelectrical activity.
The improvement in mental performance and brain electrical activity was also proven by Franco et al. [7] after one month of treatment with Citicoline in patients with an early onset of Alzheimer’s disease.
Many authors have studied the role of Citicoline in Parkinson’s disease [8-10] and concluded that the basis of symptoms improvement is the stimulation of the dopaminergic system.
Agnoli et al. [8] administered Citicoline to patients with Parkinson disease already treated with L-dopa + dopa decarboxylase inhibitor and revealed that Citicoline determined an important
improvement of bradykinesia and rigidity. Citicoline could decrease the incidence of side effects and slow down the loss of efficacy of levodopa in the long-term treatment [9].
Use of Citicoline in Amblyopia and Non-arteritic Ischemic Optic Neuropathy
In amblyopia, Citicoline may improve the retinal and postretinal visual pathways by stimulating the dopaminergic system. It has been proven that it enhances contrast sensitivity, visual acuity, visual evoked responses and the effect of part-time occlusion.
Campos et al. [11] treated children with amblyopia (anisometropic or strabismic amblyopia) with oral Citicoline in addition to patching. After 30 days of treatment, the conclusion was that Citicoline was not more effective than patching alone but was able to stabilize the effect obtained during the treatment. They maintained the same visual acuity after 90 days compared to those who had only patching and who showed a decrease of visual acuity [12,13].
Another study made by Porciatti et al. [14] also showed the benefic role of Citicoline in amblyopia. He treaded 10 amblyopic patients with intramuscular Citicoline for 15 days. The visual acuity improved in both eyes with 1.4-1.5 lines and with 0.4 lines in the control group. The contrast sensitivity and the visual evoked potential also improved.
In 2008, Parisi et al. [15] proved the positive role of Citicoline treatment on patients with non-arteritic ischemic optic neuropathy. He evaluated the visual function before and after a 60 days treatment with oral Citicoline. There was an improvement of visual acuity, Pattern Electroretinogram (PERG), visual evoked potential (VEP) parameters, compared with pre-treatment values. The results persisted after the wash out period, compared to baseline.
Neuroprotective role of Citicoline in glaucoma – Current Evidence
Physiopathology of glaucoma and neuroprotection
Glaucoma is a group of optic neuropathies characterized by death of retinal ganglionar cells (RGC), which leads to structural and functional abnormalities of the optic nerve. It is the second cause of blindness in the world with 111.8

Romanian Journal of Ophthalmology 2017; 61(3): 152-158
155
Romanian Society of Ophthalmology © 2017
million people estimated to be affected in 2040. The most important factor is an elevated intraocular pressure (IOP), but hypotensive therapy alone is not sufficient in some cases to preserve the visual function, and the disease continues to progress despite a well-controlled IOP. It is currently recognized as a chronic neurodegenerative disease, which alters the whole visual pathways running from the eye to the visual cortex. This suggests that the pharmacological approach used in different degenerative brain disorders can also be useful in glaucoma.
In 2006, Gupta first demonstrated the presence of degenerative changes in lateral geniculate nucleus and visual cortex in glaucoma patients. The eye could be part of the central nervous system and glaucoma could be a neurodegenerative disease. There are also common cell death mechanisms of glaucoma and neurological progressive diseases [16].
The death of RGC is the main pathophysiological event in glaucoma and neuroprotection has the aim to prevent, delay, or reduce the cell death by targeting the neurons.
One of the mechanisms involved is the deprivation of neurotrophins. Acute or chronic IOP elevation can cause a blockade of the axonal transport of neurotrophins from the superior colliculus to the optic nerve head. Apoptosis can be the result of neurotrophic factors deprivation, such as brain derived neurotrophic factor (BDNF), which are important for cell survival and growth. Glutamate-mediated toxicity is another mechanism that has been investigated; blocking glutamate cascade could represent a neuroprotective strategy.
Experimental studies
In recent years, experimental studies have proven the protective role of Citicoline on RGCs.
In 2002, Rejadak et al. [17] showed the impact of Citicoline on retinal catecholamine levels. He injected intraperitoneally adult male Albino rabbits and measured the concentration of catecholamines in the retina, showing a higher level of dopamine in the animal treated with Citicoline, a slightly higher adrenaline concentration, while noradrenaline was unmodified.
Citicoline could also have an anti-apoptotic effect in the mitochondria-dependent cell death mechanism and could help the axon regeneration. Shuettauf et al. [18] studied the anti-apoptotic effect of Citicoline in adult rats by treating them with lithium, Citicoline or a mixture of lithium and Citicoline by intraperitoneal injections. The results indicated a higher density or RGC connected with the superior colliculus in those treated with Citicoline compared with the others.
Some authors demonstrated the neuroprotective role of Citicoline in glutamate-mediated cell death by using a model of Kainic acid (KA)-induced retinal damage in rats, which is an analogue of glutamate. They injected KA in the vitreous space and Citicoline intraperitoneally in some of the rats. Compared to the control group that received only KA, in which a reduction of retinal thickness was noticed gradually, the group treated with Citicoline showed an attenuated reduction (Fig. 3) [19].
The neuroprotective effect of Citicoline on retinal nerve fibers in hyperglycemia conditions has also been proven by using Citicoline eye drops in a mouse model of diabetes [20].
Clinical studies
Many studies have investigated the neurotrophic effect of Citicoline in glaucoma. The
Fig. 3 Transverse sections in rat retina at 7 days after KA injection using H-E staining. In control retina, five, well organized retinal layers are seen (A). In the KA-injected group, the thickness of retina is markedly reduced due to loss of internal nuclear (INL) and internal plexiform layers (IPL) (B). Conserved retinal layers in KA-injected group treated with Citicoline (C)

Romanian Journal of Ophthalmology 2017; 61(3): 152-158
156 Romanian Society of Ophthalmology
© 2017
effects of Citicoline treatment in glaucoma were analyzed by perimetry using Humphrey Field Analyzer and electrophysiological methods. The last can describe the structures that contribute to the visual function. The function or retinal ganglionar cells are analyzed by pattern electroretinogram (ERGp). Visual evoked potentials (VEP) describe the whole visual pathways.
In 1999, Parisi et al. [21] investigated the effect of Citicoline by using electrofunctional tests (VEP and ERGp) in order to assess the retinal and cortical response in patients with glaucoma. The intramuscular dose of Citicoline or placebo was added to their hypotensive treatment, followed by a washout period. The Citicoline-treated group showed an improvement of VEP and ERGp parameters when compared to placebo that was treatment-dependent.
In 2005, Parisi et al. [22] evaluated the long-term treatment effect of Citicoline treatment in a 8 years study adding Citicoline to the hypotensive therapy followed by a washout period and repeated the protocol for the whole period. The results obtained at the end of each period were compared to baseline. Citicoline improved the VEP and ERGp parameters compared to pre-treatment conditions and to placebo patients. An increase in the visual field mean deviation was also observed at the end of the follow up, and this was linked to the electrofunctional results. This improvement could be determined by dopamine increase in the central nervous system.
All the above studies refer to Citicoline administered by intramuscular injection. In 2003, Rejadak et al. [23] made the first clinical study by using Citicoline tablets containing 500 mg of active ingredient, given twice a day. VEP measurement showed an improvement of conduction along the visual pathways.
In 2008, Parisi et al. [24] studied the effect of oral suspension of Citicoline versus the intramuscular administration over visual function in patients with moderate visual field defects. They noticed an improvement of VEP and ERGp parameters after both treatments, with no difference between the two administration routes. After washout, a partial regression was noticed (Fig. 4).
Citicoline can also be administered as eye drops in order to increase the patient compliance and adherence. In an experimental study, Citicoline has been detected in the vitreous when administered topically [25]. In this study, five mice were treated with Citicoline eye drops 1% and 2%, two drops per day. The molecule was detected in vitreous at the end of the treatment. When 2% Citicoline was administered, a systemic absorption was also noted. This study had a clinical part too. The authors added Citicoline eye drops to the hypotensive therapy of glaucoma patients for 2 months followed by one month of washout. After the first 2 months of treatment, an improvement in RGC function was noted on electrofunctional tests, but regressed after 30 days of washout.
The positive effects of Citicoline on the retinal function and neural conduction in glaucoma patients was also reported by Parisi et
Fig. 4 Electrophysiological examination at baseline, after 60 days of treatment with Citicoline and after the last washout period. Improvement of visual field and electrophysiological parameters after treatment followed by regression or stabilization after washout [24]

Romanian Journal of Ophthalmology 2017; 61(3): 152-158
157
Romanian Society of Ophthalmology © 2017
al. [26]. They treated a group of patients with beta-blocker monotherapy and Citicoline eye drops 3 times per day for 4 months followed by a 2 months washout period, and the other group with beta-blocker monotherapy for the whole period. The electrofunctional measurements were done at the baseline, at four and six months. An improvement was noticed after the 4 months of Citicoline treatment compared to baseline, and the increase of VEP P100 was correlated with the increase of ERGp parameters. The results went back to the baseline levels after washout period. The group treated with beta-blockers only maintained the same electrophysiological level during the whole study.
Conclusions and Future Perspectives
There are 3 steps of neuroprotection in glaucoma: to protect unaffected axons and RGC, to save minimally damaged axons and RGC and to regenerate them. Citicoline may play a role in the second step, acting between the dysfunction and the apoptosis of RGC. In animal models, the steps of RGC death were demonstrated, which occur later in the disease course: a decrease in axonal transport, a split of axons and the death of RGC later [27]. The time between neuronal dysfunction and death could be used as a good moment to introduce therapies in order to increase the retinal function (neuroenhancement), and Citicoline may play a role in this process.
The scientific literature regarding the Citicoline role in glaucoma is growing and the studies differ in terms of patients’ characteristics, outcomes measures, schedule of treatment (dosage, administration route, length). The conclusion of all the studies made so far is that Citicoline is a safe molecule with positive effects on the visual function.
In the future, more clinical trials are needed with a larger population involved and more investigations need to be done (optical coherence tomography measurement of retinal nerve fiber layer, ganglion cell complex thickness) in order to obtain a dose-response relation and to sustain the clinical effect of Citicoline demonstrated until now.
Disclosures None
References
1. Grieb P. Neuroprotective Properties of Citicoline: Facts, Doubts and Unresolved Issues. CNS Drugs. 2014; 28(3):185–193.
2. Secades JJ. Citicoline: Pharmacological and clinical review, 2010 update. Revista de neurologie. March 2011; 52 Suppl 2(Suppl 2):S1-S62.
3. Muralikrishna Adibhatla R, Hatcher JF, Dempsey RJ. Citicoline: neuroprotective mechanisms in cerebral ischemia. Journal of Neurochemistry. 2002; 80,12±23.
4. Gutiérrez-Fernández M, Rodríguez-Frutos B, Fuentes B, Vallejo-Cremades MT, Alvarez-Grech J, Expósito-Alcaide M, Díez-Tejedor E. CDP-choline treatment induces brain plasticity markers expression inexperimental animal stroke. Neurochem. Int. 2012; 60,310–317.
5. Cacabelos R, Caamaño J, Gómez MJ, Fernández-Novoa L, Franco-Maside A, Alvarez XA. Therapeutic effects of CDP-choline in Alzheimer’s disease. Cognition, brain mapping, cerebrovascular hemodynamics, and immune factors. Ann. N. Y. Acad. Sci. 1996; 777,399–403.
6. Alvarez XA, Mouzo R, Pichel V, Pérez P, Laredo M, Fernández-Novoa L, Corzo L, Zas R, Alcaraz M, Secades JJ et al. Double-blind placebo-controlled study with citicoline in APOE genotyped Alzheimer’s disease patients. Effects on cognitive performance, brain bioelectrical activity and cerebral perfusion. Methods Find Exp. Clin. Pharmacol. 1999; 21,633–644.
7. Franco-Maside A, Caamaño J, Gómez MJ, Cacabelos R. Brain mapping activity and mental performance after chronic treatment with CDP-choline in Alzheimer’s disease. Methods Find Exp. Clin. Pharmacol. 1994; 16,597–607.
8. Agnoli A, Ruggieri S, Denaro A, Bruno G. New strategies in the management of Parkinson’s disease: A biological approach using a phospholipid precursor (CDP-choline). Neuropsychobiology. 1982; 8,289–296.
9. Saligaut C, Daoust M, Moore N, Boismare F. Circling behaviour in rats with unilateral lesions of the nigrostriatum induced by 6-hydroxydopamine: Changes induced by oral administration of cytidine-51-diphosphocholine. Neuropharmacology. 1987; 26,1315–1319.
10. Eberhardt R, Birbamer G, Gerstenbrand F, Rainer E, Traegner H. Citicoline in the treatment of Parkinson’s disease. Clin. Ther. 1990; 12,489–495.
11. Campos EC, Bolzani R, Schiavi C, Baldi A, Porciatti V. Cytidin-51-diphosphocholine enhances the effect of part-time occlusion in amblyopia. Doc. Ophthalmol. 1996–1997; 93,247–263.
12. Fresina M, Dickmann A, Salerni A, de Gregorio F, Campos EC. Effect of oral CDP-choline on visual function in young amblyopic patients. Graefes Arch. Clin. Exp. Ophthalmol. 2008; 246,143–150.
13. Pawar PV, Mumbare SS, Patil MS, Ramakrishnan S. Effectiveness of the addition of citicoline to patching in

Romanian Journal of Ophthalmology 2017; 61(3): 152-158
158 Romanian Society of Ophthalmology
© 2017
the treatment of amblyopia around visual maturity: A randomized controlled trial. Indian J. Ophthalmol. 2014; 62,124–129.
14. Porciatti V, Schiavi C, Benedetti P, Baldi A, Campos EC. Cytidine-51-diphosphocholine improves visual acuity, contrast sensitivity and visually-evoked potentials of amblyopic subjects. Curr. Eye Res. 1998; 17,141–148.
15. Parisi V, Coppola G, Ziccardi L, Gallinaro G, Falsini B. Cytidine-51-diphosphocholine (Citicoline): A pilot study in patients with non-arteritic ischaemic optic neuropathy. Eur. J. Neurol. 2008; 15,465–474.
16. Gupta N, Ang LC, Noël de Tilly L, Bidaisee L, Yücel YH. Human glaucoma and neural degeneration in intracranial optic nerve, lateral geniculate nucleus, and visual cortex. Br. J. Ophthalmol. 2006; 90,674–678.
17. Rejdak R, Toczolowski J, Solski J, Duma D, Grieb P. Citicoline treatment increases retinal dopamine content in rabbits. Ophthalmic Res. 2002; 34,146–149.
18. Schuettauf F, Rejdak R, Thaler S, Bolz S, Lehaci C, Mankowska A, Zarnowski T, Junemann A, Zagorski Z, Zrenner E et al. Citicoline and lithium rescue retinal ganglion cells following partial optic nerve crush in the rat. Exp. Eye Res. 2006; 83,1128–1134.
19. Park CH, Kim YS, Noh HS, Cheon EW, Yang YA, Yoo JM, Choi WS, Cho GJ. Neuroprotective effect of citicoline against KA-induced neurotoxicity in the rat retina. Exp. Eye Res. 2005; 81,350–358.
20. Zerbini G, Bandello F, Lattanzio R, Gabellini D, Zucchiatti I, Spinello A, Capuano V, Preziosa C, Maestroni S. In vivo evaluation of retinal and choroidal structure in a mouse model of long-lasting diabetes. Effect of topical treatment with citicoline. J. Ocul. Dis. Ther. 2015; 3,1–8.
21. Parisi V, Manni G, Colacino G, Bucci MG. Cytidine-5′-diphpsphocholine (citicoline) improves retinal and cortical responses in patients with glaucoma. Ophthalmology. 1999; 106,1126–1134.
22. Parisi V. Electrophysiological assessment of glaucomatous visual dysfunction during treatment with cytidine-5′-diphosphocholine (citicoline): A study of 8 years of follow-up. Doc. Ophthalmol. 2005; 110,91–102.
23. Rejdak R, Toczolowski J, Krukowski J, Kaminski M, Rejdak K, Stelmasiak Z, Grieb P. Oral citicoline treatment improves visual pathway function in glaucoma. Med. Sci. Monit. 2003; 9,PI24–PI28.
24. Parisi V, Coppola G, Centofanti M, Oddone F, Angrisani AM, Ziccardi L, Ricci B, Quaranta L, Manni G. Evidence of the neuroprotective role of citicoline in glaucoma patients. Prog. Brain Res. 2008; 173,541–554.
25. Roberti G, Tanga L, Parisi V, Sampalmieri M, Centofanti M, Manni G. A preliminary study of the neuroprotective role of Citicoline eye drops in glaucomatous optic neuropathy. Indian J. Ophthalmol. 2014; 62,549–553.
26. Parisi V, Centofanti M, Ziccardi L, Tanga L, Michelessi M, Roberti G, Manni G. Treatment with Citicoline eye drops enhances retinal function and neural conduction along the visual pathways in open angle glaucoma. Graefes Arch. Clin. Exp. Ophthalmol. 2015; 253,1327–1340.
27. Chang EE, Goldberg JL. Glaucoma 2.0: Neuroprotection, neuroregeneration,
neuroenhancement. Ophthalmology. 2012; 119,979–986.

Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:159-165
REVIEW
159 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.30
Glaucoma after penetrating keratoplasty
Zemba Mihail* **, Stamate Alina-Cristina** *** *Department of Ophthalmology, “Dr. Carol Davila” Central Military Emergency University Hospital, Bucharest, Romania **“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania ***Arena Med Clinic, Bucharest, Romania Correspondence to: Stamate Alina-Cristina, MD, Arena Med Clinic, Bucharest, 68 Basarabia Boulevard, Ap. 1, District 2, Bucharest, Romania, Mobile phone: +40737 027 067, E-mail: [email protected] Accepted: September 7th, 2017
Abstract Penetrating keratoplasty is a surgical intervention that despite the progress of surgical techniques and of postoperative treatment continues to have numerous complications. Many of them, such as graft rejection, significant astigmatism, cystoid macular edema, or cataract lead to important limitations of the visual function. Glaucoma is possibly the most dangerous complication following PK, leading to loss of the visual potential of the eye due to irreversible damage to the optic nerve. Identifying the risk factors permits an attentive follow-up and rapid treatment of the postoperative IOP rises. Maybe the most important is that preexisting glaucoma should be rightly diagnosed and controlled before PK, medically or, if necessary, surgically. Keywords: penetrating keratoplasty, high intraocular pressure, glaucoma post penetrating keratoplasty, antiglaucomatous therapy Abbreviations: PK = penetrating keratoplasty, IOP = intraocular pressure, PAS = peripheral anterior synechiae, TM = trabecular meshwork, DM = Descemet membrane, GAT = Goldmann applanation tonometry, MMC = mitomycin C, CAI = carbonic anhydrase inhibitors, 5-FU = 5-fluorouracil
Introduction
Penetrating keratoplasty (PK) is a surgical intervention that despite the progress of surgical techniques and of postoperative treatment continues to have numerous complications. Many of them, such as graft rejection, significant astigmatism, cystoid macular edema, or cataract lead to important limitations of the visual function. Glaucoma is possibly the most dangerous complication following PK, leading to loss of the visual potential of the eye due to irreversible damage to the optic nerve, contrary
to other complications, in which visual recovery can be expected.
Glaucoma following PK has a relatively high frequency, it can appear early, as well as late in the evolution of the transplant, it is very hard to diagnose and also to follow-up and the medical or surgical treatment can interfere negatively with the evolution of the corneal graft [1].
Incidence
In 1969, Irvine and Kaufman were the first to publish a study that emphasized the increased incidence of high intraocular pressure (IOP) after

Romanian Journal of Ophthalmology 2017; 61(3): 159-165
160 Romanian Society of Ophthalmology
© 2017
PK. The maximum mean IOP in the first postoperative week was 24 mmHg in phakic eyes, 40 mmHg in aphakic eyes and 50 mmHg in eyes that underwent combined surgery - cataract and transplant [2]. Subsequently, different studies showed a variable incidence of glaucoma after PK, ranging from 9 to 31% early postoperatively and from 18 to 35% in the late postoperative period [3,4]. One of the reasons for this great variation of incidence is the different manner in which glaucoma after PK is defined in various studies [5].
Definition
Glaucoma is defined as a chronic progressive optic neuropathy that has characteristic morphological changes of the optic nerve and of the retinal nerve fiber layer in the absence of other ocular diseases and congenital anomalies. Starting from this classical statement, defining glaucoma after PK implies numerous difficulties: difficulty in performing a preoperative examination of the optic nerve, visual field and even of the IOP (the cornea is usually opaque); the postoperative examination can also be troublesome (high astigmatism, reduced transparency of the cornea).
Therefore, multiple studies define post-PK glaucoma as an elevation of IOP greater than 21 mmHg, independent of the optic nerve or visual field modifications. The definition obviously has scientific deficiencies, but has an important practical component [3,6].
A problem appears in the cases with preexisting glaucoma. Some studies enclose all these cases in post-KP glaucoma, meanwhile others include only the cases that require additional antiglaucomatous therapy (i.e. medications, laser or surgical treatment) to maintain IOP at adequate values (escalation of glaucoma therapy).
Risk factors
Recognition of risk factors is important for the prevention, diagnosis, and early treatment of post-PK glaucoma.
The most significant risk factors are preexisting glaucoma, lens status (i.e. aphakia,
pseudophakia) and the disease for which PK is performed [7].
In a study from 2014, Hemanth et al. compared the incidence of glaucoma after PK in phakic, pseudophakic, and aphakic eyes. The aphakic group had the highest risk, followed by the pseudophakic and phakic group; there was no statistically significant difference between the last two groups [3].
Kirkness and Ficker published one of the greatest studies on the incidence and risk factors associated with post-PK glaucoma, that included 1122 PKs, performed at Moorfields Eye Hospital, London. The incidence of post-PK glaucoma was 14%. Corneal dystrophies and keratoconus had the lowest risk of glaucoma, contrary to bullous keratopathy, anterior segment trauma, iridocorneal endothelial syndrome and corneal perforations that had an increased risk [8,9]. In another study, Kirkness and Mashegov demonstrated an increased incidence of post-PK glaucoma after corneal perforations, especially those after bacterial ulcers, due to the formation of peripheral anterior synechiae (PAS). The longer the period between the perforation and the transplant, the higher the risk of glaucoma [10].
Pathogenesis
The pathophysiology of post-PK glaucoma is multifactorial, including among the causes the compression of the angle’s anatomical elements with the trabecular meshwork’s (TM) collapse, incorrect suture of the graft, postoperative inflammation and prolonged use of corticosteroids in the postoperative treatment.
Other causes are not specific to post-PK glaucoma, also appearing after other types of surgical interventions; they should be promptly recognized and treated: pupillary blockage, lens induced glaucoma, hyphaema and viscoelastic retention [5].
Zimmerman et al. demonstrated how the TM’s collapse, especially in aphakic eyes, is the main cause of glaucoma; they advocated that for an easy access through the anterior chamber angle to the trabecular meshwork, the trabeculum needs a posterior fixation, sustained by the ciliary body-lens complex and an anterior fixation at the level of Descemet membrane

Romanian Journal of Ophthalmology 2017; 61(3): 159-165
161
Romanian Society of Ophthalmology © 2017
(DM). In aphakic and pseudophakic eyes the posterior support is relaxed due to lens removal. On the other side, the incision through DM in PK relaxes the anterior support, the DM being capable of displacing towards the angle [11].
In 1975, using a mathematical model, Olson and Kaufman pointed out the factors that contribute to the distortion of the angle and so to the reduction of the outflow: tight sutures (widen the gap between the margins of the incision in the DM), lengthy sutures (compress even more the tissues), large grafts and thick peripheral corneas [12].
One of the causes of late glaucoma after PK is the formation of PAS. They can appear if the anterior chamber is shallow prior to the intervention (e.g. corneal perforation) or postoperatively (e.g. wound dehiscence or iris incarceration at the graft-host junction).
Long-term use of corticosteroids, necessary for graft rejection prevention, can lead to IOP elevation. Corticosteroids that increase the IOP to a lower extent (e.g. fluorometholone) can be used, but these are less effective in rejection prophylaxis.
Diagnosis
Measuring the IOP, optic disc and visual field evaluation are in the most occasions difficult to perform preoperatively, because of the corneal disease, which makes it impossible to establish a starting point for the postoperative period.
Changes in the corneal thickness, high astigmatism and other refractive errors, that also harden a proper evaluation, appear after PK.
In the immediate postoperative period, the diagnosis is based principally on measuring the IOP; later, to the extent possible (transparency of the cornea and ocular media), the classical evaluation is approached [1].
High astigmatism, graft edema, thick fluorescein meniscus and inappropriate mires (especially for grafts smaller than 7.5 mm) make Goldmann applanation tonometry (GAT) practically impossible [1]. In cases of irregular surface, IOP can be measured with the Mackay-Marg electronic tonometer, the pneumotonometer [13] or the Tono-Pen [14]. Comparing the iCare tonometer with the GAT,
Salvetat et al. demonstrated that the values are comparable in cases of anterior and posterior lamellar keratoplasty, but are different in cases of PK, the iCare tonometer underestimating pressure compared to the GAT [15]. Epithelial and stromal edema lead to the under evaluation of IOP and the measurement on a scarred tissue can give false raised values. Dynamic contour tonometer was imagined for measuring IOP independent of the mechanical properties of the cornea, which theoretically makes it very useful in eyes with keratoplasty, in which these properties are profusely modified. A digital piezoelectric pressure transducer is directly coupled to the ocular surface contour and directly measures the IOP transcorneally. More studies showed that this tonometer’s measurements are closer to the true manometric measurements than the other ones are [5]. Comparing the dynamic contour tonometer and the GAT in cases with keratoplasty, Ceruti et al. proved that the tonometer was not influenced by thickness, curvature, and corneal astigmatism [16].
Treatment
Prophylaxis Preexistent glaucoma should be well
controlled prior to the surgical intervention. If the IOP is difficult to control with drugs or if the control imposes maximal therapy, the IOP can decompensate after keratoplasty. Therefore, it is recommended that in these cases, the glaucoma should be controlled surgically and afterwards the transplant should be performed [5], because multiple studies revealed a higher incidence of graft failure if the intervention for glaucoma was performed after keratoplasty [17]. Other authors recommend trabeculectomy with mitomycin C (MMC) application or artificial drainage systems concomitantly with PK [17-19].
In the case of PK, certain elements of the surgical technique can lower the risk of postoperative glaucoma. A graft 0.5 mm larger than the host opening is associated with a lower frequency of glaucoma after PK [20,21]. Deep sutures allow a better coalescence of the host and graft DM [11] and relatively short and equal sutures between graft and host compress the tissues to a lesser extent, both elements

Romanian Journal of Ophthalmology 2017; 61(3): 159-165
162 Romanian Society of Ophthalmology
© 2017
attenuating the TM’s tendency to collapse. In case of PAS, goniosynechialysis can be performed. Viscoelastic substances should be removed as completely as possible at the end of the intervention. In case of atrophic iris or floppy-iris syndrome, iridoplasty can be performed to tension the iris and to remove it from the angle [22]. Graft suture should be tight, avoiding iris incarceration at the graft-host junction, as well as the dehiscence of the plague postoperatively.
A frequent instillation of corticosteroids in the immediate postoperative period controls inflammation, reducing the risk of PAS. Dosage must be carefully monitored, because in the mean and long term, corticosteroid induced elevation of pressure can appear. Also, in the early postoperative period, mydriatics can also be used to prevent pupillary blockage.
Medical treatment
Medical treatment represents the first line of therapy in preventing glaucoma after PK. Fortunately, many classes of drugs are at our disposal as compared to 20 years ago: beta-blockers, alpha-2 agonists, carbonic anhydrase inhibitors (CAI) and topical prostaglandin analogues, as well as systemic CAI. Miotics and adrenergic agents have historical value at the most, being no longer used. Therapy must be thought in such a manner that is efficient, but with the lowest rate of adverse effects on the graft and on the patient’s quality of life.
Beta-blockers are effective in lowering IOP and the effect installs rapidly. This group of agents can be utilized for IOP spikes in the perioperative period, but also for long-term therapy. In prolonged use, the adverse effects are punctate epithelial keratopathy and corneal anesthesia that can affect the graft’s epithelium, compromising it [23].
Alpha-2 agents also act promptly, are efficient and have few systemic adverse effects. Approximately one quarter of patients have allergies that lead to discontinuation of treatment.
Topical CAI are well tolerated, do not have the systemic adverse reactions of the systemic administration and can be combined with other topical antiglaucomatous drugs. However, carbonic anhydrase has a role in the pump
function of the corneal endothelium. Some studies showed endothelial decompensation with corneal edema in cases of borderline endothelial function. For this reason, it is recommended to stop therapy when edema of the corneal graft appears [5].
Prostaglandin analogues efficacy is renowned, are administered once daily and have few systemic adverse effects. Because the effect installs relatively slow, these agents are suited for chronic forms of post-PK glaucoma. They should be avoided in PK for herpetic keratitis, because recurrence of herpetic keratitis has been reported and also the possibility of inducing cystoid macular edema should be taken into account [24,25].
Systemic CAI are very efficient, have the advantage of not having any direct toxic effect on the graft, but are difficult to utilize on the long term, 30-50% of the patients manifesting side-effects such as: paraesthesia, tinnitus, fatigue, muscular weakness, nausea, depression and cutaneous allergies. They are very useful in the treatment of sudden IOP spikes in the immediate postoperative period.
Laser treatment
Nd:YAG laser iridotomy can be used in pupillary blockage, but in the majority of the cases cannot be performed properly, because the patient’s peripheral cornea is not sufficiently transparent. For the same reason, neither Argon laser iridoplasty can be performed, which is useful in peripheral iris retraction and obtaining an easier access to the trabeculum.
Argon or selective laser trabeculoplasty can be used in selected cases, with transparent graft, open angle, moderate pressure (25-30 mmHg) with medical treatment at a few months after keratoplasty, that allow the application of the lens. Van Meter et al. reported IOP control with Argon laser trabeculoplasty in 10 out of 14 cases for 2 years [26]. Considering that the effect of Argon laser trabeculoplasty is limited in time, that it can lower IOP with a maximum of 8-10 mmHg and that in the majority of cases, the angle of PK patients has PAS and a tendency for collapse of the TM, with difficult visibility, we consider that this option of therapy should be avoided in the treatment of glaucoma after PK.

Romanian Journal of Ophthalmology 2017; 61(3): 159-165
163
Romanian Society of Ophthalmology © 2017
Surgical treatment Trabeculectomy Standard trabeculectomy has a low rate of
success due to extensive subconjunctival fibrosis (after prior interventions) and the presence of PAS that numerous times are extended towards the graft-host junction and make the functioning of the fistula difficult. A study performed on 35 PK patients showed that 92% of them required medication after trabeculectomy and 53% necessitated further surgical interventions [27].
5-fluorouracil (5-FU) can be administered for many days postoperatively via subconjunctival injections. It has a toxic effect on the corneal epithelium and can compromise the graft. The incidence of epithelial toxicity can be as much as 50% of the cases [28].
Because of the corneal toxicity of 5-FU, most surgeons prefer MMC [7]. It is applied for 1 to 4 minutes intraoperatively and does not appear to have toxicity on the corneal epithelium. In a retrospective study on patients with glaucoma after PK, trabeculectomy with MMC had a higher success rate concerning IOP control (73%) in comparison to standard trabeculectomy (25%) for a follow-up period of 22 months [29]. Clarity of the graft was present in 69.2% of the cases from the lot with MMC and in 37.5% of the cases from the standard trabeculectomy lot. On the other side, the MMC group had a greater incidence of choroidal detachment, macular edema and fistula of the filtering bleb.
All measures for preventing anterior chamber collapse intra- and postoperatively should be taken. Endothelial cell loss after trabeculectomy is of 7-12% in case of iridocorneal contact and of 40-50% in case of corneolenticular contact [30]. This loss of endothelial cells can compromise the graft. In order to assure a relatively deep postoperative chamber, an over-tight suturing of the scleral flap and subsequent laser lysis of these sutures can be considered.
Another element that should be monitored after trabeculectomy in cases with a more prominent bleb is the dellen effect that can lead to epithelial defect and appearance of a corneal ulceration in the suture area.
Artificial drainage devices From a theoretical standpoint, inserting an
artificial drainage device has some advantages compared to trabeculectomy. The filtering bleb is located posteriorly, possibly avoiding perilimbal fibrosis. Overfiltration with postoperative hypotony and collapse of the anterior chamber can be avoided either by using devices with valves (i.e. Ahmed implant) or by provisory suturing of the tube (i.e. Molteno implant). The success rate in reducing IOP after PK is 60 to 80% [31,32].
Artificial drainage devices have their disadvantages. They are more expensive, require a higher surgical experience and the most important, have a relatively higher risk of graft failure than trabeculectomy [31-33].
A mechanism of graft failure in eyes with artificial drainage devices could be immunological; the tube apparently allows the access of inflammatory cells from the subconjunctival space into the anterior chamber that could contribute to graft rejection [34]. The most important mechanism is the mechanic one, the tube being implanted in the anterior chamber and even though at the moment of implantation it is distant from the graft’s endothelium, it can displace afterwards.
To avoid injuring the endothelium, the valve’s tube can be implanted at the level of the pars plana. The success rate in the control of IOP is similar, but there is a higher rate of retinal complications (e.g. cystoid macular edema, epiretinal membranes, retinal detachment, suprachoroidal hemorrhage) [35].
Cyclodestructive procedures Cyclocryotherapy has been used from the
1950s in the treatment of refractory glaucoma. The success rate in the control of IOP is satisfying (60-90%), but is mainly replaced by cyclophotocoagulation, because of the great rate of serious complications [36,37].
Nd:YAG laser cyclophotocoagulation is a more predictable method, less painful and with a lower rate of complications [38,39]. The success rate in IOP control varied from 69 to 77% with a follow-up period of 2 years. However, a high rate of graft failure (23-46%) appears and also, other severe complications such as: hypotony, phthisis bulbi [38,39].

Romanian Journal of Ophthalmology 2017; 61(3): 159-165
164 Romanian Society of Ophthalmology
© 2017
Diode laser cyclophotocoagulation with a 810 nm wavelength has some advantages: the laser is portable, easier to manipulate and as effective as the Nd:YAG laser. Okacoglu et al. showed a rate of success of 92% in IOP control at 6 months and of 72% at 12 months in patients with post-PK glaucoma. 44% of the patients had to be retreated to obtain the control of the IOP, but no graft rejection was reported in the 32 patients of this study [40].
It is difficult to assess which surgical treatment option - trabeculectomy with antimetabolites, implantation of an artificial drainage device or cyclophotocoagulation - is the most useful in the treatment of glaucoma after PK. As demonstrated, there are numerous studies on series of cases, generally retrospective, but there are no prospective, randomized studies that compare the treatment options.
From our point of view, the future belongs to cyclophotocoagulation. Trabeculectomy with antimetabolites, as well as artificial drainage devices interfere with the anterior chamber and any intervention at this level increases the risk of graft failure. Probably a perfected variant of the existing cyclophotocoagulation lasers that would reduce the rate of complications related to hypotony, even if the intervention was periodically repeated, would theoretically have the highest chances of success.
Conclusions
Glaucoma is a complication of PK very difficult to treat. Identifying the risk factors allows an attentive follow-up and rapid treatment of the postoperative IOP rises. Possibly, the most important fact is that preexisting glaucoma should be rightly diagnosed and controlled before PK, medically or, if necessary, surgically.
Certain technical details can reduce the incidence of TM’s collapse and implicitly the appearance of glaucoma after PK.
Once the glaucoma has installed, the medical treatment can control the IOP in certain cases and antiglaucomatous surgical interventions also contribute to the control of IOP.
Graft failure can appear relatively frequently after surgical interventions, especially in those in which important inflammation at the level of the anterior chamber or mechanical injury of the corneal endothelium develop.
Disclosures
None of the authors has any financial or proprietary interests to disclose.
References
1. Ayyala RS. Penetrating keratoplasty and glaucoma. Surv. Ophthalmol. 2000; 45:91-105.
2. Irvine AR, Kaufman HE. Intraocular pressure following penetrating keratoplasty. Am. J. Ophthalmol. 1969; 68:835-44.
3. Hemanth Raj MN, Bhanushree G, Hlinaykor RM, Vijayanath V. Preoperative risk factors and incidence of glaucoma after penetrating keratoplasty. Int. J Clin. Trials. 2014 Aug; 1(2):55-61.
4. Franea ET, Araeri ES, Roche FJ. A study of glaucoma after penetrating keratoplasty. Cornea. 2002; 21:284-8.
5. Lim MC, Brandt JD, O’Duny DG. Glaucoma after penetrating keratoplasty. Cornea. 2011, Mosby, Elsevier Inc, 1441-54.
6. Dada T, Aggarwal A, Minudeth KB, Vanathy M, Choudhary S, Gupta V. Post-penetrating keratoplasty glaucoma. Indian J. Ophthalmol. 2008; 56(4):269-77.
7. Gupta P, Sharma A, Ichhpujani P. Post penetrating keratoplasty glaucoma. Nepal J Ophthalmol. 2014; 6(11):80-90.
8. Kirkness CM, Ficker LA. Risk factor for the development of postkeratoplasty glaucoma. Cornea. 1992; 11(5):427-432.
9. Kirkness CM, Moshegov C. Postkeratoplasty glaucoma. Eye. 1998; 2:19-26.
10. Keroday O, Kugu S, Erdogan G, Kandenir B, Odzil SE. Incidence of and risk factors for increased intraocular pressure after penetrating keratoplasty. Cornea. 2010; 29:278-82.
11. Zimmerman TJ, Krupin T, Grodzki W. The effect of suture depth on outflow facility in penetrating keratoplasty. Arch Ophthalmol. 91:505-6.
12. Olson RJ, Kaufman HE. Prognostic factors of intraocular pressure after aphakic keratoplasty. Am J Ophthalmol. 1975; 86:510-515.
13. West CE, Capello JA, Kaufma HE. Measurement of intraocular pressure with pneumatic applanation tonometer. Am J Ophthalmol. 1972; 505-9.
14. Rootman DS, Insler MS, Thomson HV. Accuracy and precision of the Tonopen in measuring IOP after keratoplasty and epikeratophakia and on scarred corneas. Arch Ophthalmol. 1988; 106:1697-700.
15. Salvetat ML, Zeppori M, Miani F, Tosoni C, Parisi L, Brusini P. Comparison of I Care tonometer and Goldmann applanation tonometry in normal corneas and in eyes with automated lamelar and penetrating keratoplasty. Eye. 2011; 25:642-50.

Romanian Journal of Ophthalmology 2017; 61(3): 159-165
165
Romanian Society of Ophthalmology © 2017
16. Geruti P, Morbib R, Marraffe M, Marchini G. Comparison of dynamic contour tonometry and Goldmann applanation tonometry in deep lamellar and penetrating keratoplasties. Am. J Ophthalmol. 2008; 145(2):215-221.
17. Rapuano CJ, Scmidt CM, Chen EJ. Results of alloplastic tube shunt procedure before, during or after penetrating keratoplasty. Cornea. 1995; 14:26-32.
18. Figuerida RS, Arranjo SV, Cohen EJ. Management of coexisting corneal disease and glaucoma by combined penetrating keratoplasty and trabeculectomy with mitomycin C. Ophthalmic Surg. Lasers. 1996; 27:903-9.
19. Insler MS, Cooper HD, Kasti PR, Caldwell DR: Penetrating keratoplasty with trabeculectomy. Am J Ophthalmol. 1985; 100:593-5.
20. Bourne WM, Davison JA, O’Fallon WM. The effect of oversize donor buttons on postoperative intraocular pressure and corneal curvature in aphakic penetrating keratoplasty. Ophthalmology. 1982; 88:242-6.
21. Zimmerman T, Olson R, Waltman S. Transplant size and elevated intraocular pressure postkeratoplasty. Arch Ophthalmol. 1978; 96:2231-3.
22. Cohen EJ, Kenyon KR, Dohlman CH. Iridoplasty for prevention of postkeratoplasty angle-closure and glaucoma. Ophthalmic Surg. 1982; 13:994-6.
23. Zimmerman TJ, Baumann JD, Hetherington J Jr. Side effects of timolol. Surv Ophthalmol. 1983; 28 (suppl):243-51.
24. Kaufman HE, Varnell ED, Thompson HW. Latanoprost increases the severity and recurrence of herpetic keratitis in the rabbit. Am J Ophthalmol. 1999; 127:51-6.
25. Wand M, Gilbert CM, Liesegang TY. Latanoprost and herpes simplex keratitis. Am J Ophthalmol. 1999; 127:602-4.
26. Van Meter WS, Allen RS, Waring GO. Laser trabeciloplasty for glaucoma in aphakic and pseudophakic eyes after penetrating keratoplasty. Arch Ophthalmol. 1988; 106:185-8.
27. Gilvarry AM, Kirkness CM, Steele AD, Rice NS, Ficker LA. The management of postkeratoplasty glaucoma by trabeculectomy. Eye. 1989; 3(Pt. 6):713-718.
28. Heuer DK, Parrish RK, Gresse MG. 5 Fluorouracil and glaucoma filtering surgery. Intermediate follow-up of a pilot study. Ophthalmology. 1986; 93:1537-46.
29. Ishioka M, Schimezaki J, Jamagami J, Fujishima H, Shimmura S, Tsubota K. Trabeculectomy with mitomycin C for postkeratoplasty glaucoma. Br. J Ophthalmol. 2000; 84(7):714-717.
30. Smith DL, Skuta GL, Lindenmuth KA. The effect of glaucoma filtering surgery o corneal endothelial cell density. Ophthalmic Surg. 1991; 22:251-5.
31. Kwon YH, Taylon JM, Hory S. Long term results of eyes with penetrating keratoplasty and glaucoma drainage tube implant. Ophthalmology. 2001; 108:272-278.
32. Sherwood MB, Smith MF, Driebe WT Jr., Stern GA, Beneke JD, Zaum ZS. Drainage tube implants in the treatment of glaucoma following penetrating keratoplasty. Ophthamic Surg. 1993; 24(3):185-189.
33. Zallaum JN, Ahuja RN, Shin D, Weiss JS. Assessment of corneal decompensation in eyes having undergone Molteno shunt procedure compared to eyes having undergone trabeculectomy. CLAOJ. 1999; 25(1)57-60.
34. Kirkness CM, Ling Y, Rice NS. The use of silicone drainage tubing to control postkeatoplasty glaucoma. Eye. 1988; 2(Pt.5):583-590.
35. Sidoti PA, Masny AY, Ritterband DC, Seedor JA. Pars plana tube insertion of glaucoma drainage implants and penetrating keratoplasty in patients with coexisting glaucoma and corneal disease. Ophthalmology. 2001; 108(6):1050-1058.
36. Bindar PS, Abel Jr., Kaufman HE. Cyclocryotherapy for glaucoma after penetrating keratoplasty. Am J Ophthalmol. 1975; 79:489-92.
37. West CE, Wood TO, Kaufman HE. Cyclocryotherapy for glaucoma pre or post penetrating keratoplasty. Am J Ophthalmol. 1973; 75:77-81.
38. Herdlen DR, Brown JD. Transscleral Nd:YAG cyclophotocoagulation: comparison of 180 degree and 360 degree initial treatment. Ophthalmol Surg. 1993; 24(3):181-184.
39. Weatcroft S, Singh A, Casey T, Mc Allister J. Treatment of glaucoma following penetrating keratoplasty with transscleral YAG cyclophotocoagulation. Int. Ophthalmol. 1992; 16(4-5):347-400.
40. Ocakoglu O, Arslan OS, Kaynan A. Diode laser transscleral cyclophotocoagulation for the treatment of refractory glaucoma after penetrating keratoplasty. Curr Eye Ref. 2005; 30(7):569-574.
Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:166-170
REVIEW
166 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.31
Management of diplopia
Iliescu Daniela Adriana, Timaru Cristina Mihaela, Alexe Nicolae, Gosav Elena, De Simone Algerino, Batras Mehdi, Stefan Cornel Ophthalmology Department, “Dr. Carol Davila” Central Military University Emergency Hospital, Bucharest, Romania Correspondence to: Iliescu Daniela Adriana, MD, Ophthalmology Department, “Dr. Carol Davila” Central Military University Emergency Hospital, Bucharest, 134 Calea Plevnei Street, District 1, Bucharest, Bucharest, Romania, Phone/ fax: +4021 313 71 89, E-mail: [email protected] Accepted: September 9th, 2017
Abstract Diplopia (seeing double) is an ophthalmologic complaint found mainly in elder patients. It can have both ocular and neurological causes. A careful history and clinical examination must detail the type of diplopia (monocular/ binocular), onset, and progression, associated and relieving factors. In case of monocular diplopia, refraction and biomicroscopic examination of the ocular media are mandatory. The cause of ocular misalignment for binocular diplopia must be determined and life-threatening conditions (such as posterior communicating artery aneurysm) must imply an immediate treatment. Management and treatment is always according to the specific cause of diplopia. Keywords: diplopia, binocular vision, strabismus
Introduction
Diplopia - simultaneous perception of two images of a single object or seeing double is a common symptom identified in ophthalmological and neurological patients. It has many underlying causes. An efficient management implies an accurate diagnosis that can be made with a detailed history and a careful clinical examination. The assessment of the patient’s perception of diplopia must exclude other symptoms that can be misunderstood by the patient, such as image distortion, vision field defects, after images, hemianopia. The first aspect that must be determined is whether the diplopia is monocular or binocular. The difference is made by covering one eye. If the diplopia persists after one eye occlusion, then the diplopia is monocular. If the diplopia
disappears after the eye is occluded, then it is binocular and an extensive investigation must make the differential diagnosis between multiple etiologies that can cause the misalignment of the visual axes [1].
Monocular diplopia
Monocular diplopia is often caused by uncorrected refractive errors (astigmatism) and cataract. It is usually due to intraocular pathology that requires a detailed ophthalmological evaluation. Monocular diplopia or polyopia (> 2 images), unilateral or bilateral, are rarely of cerebral cause, determined by primary and secondary visual cortex lesions. Associated symptoms such as decreased visual acuity and haze can appear in diplopia caused by cataract. Macular disorders can associate

Romanian Journal of Ophthalmology 2017; 61(3): 166-170
167
Romanian Society of Ophthalmology © 2017
metamorphopsia (Amsler grid evaluation). Other causes of monocular diplopia include dry eye syndrome, wrong-fitting contact lens, irregular corneal surface, keratoconus, abnormalities of the iris (iridodialysis, polycoria, and large iridotomies), and vitreous opacities. The pinhole test will differentiate between an optical cause and other forms of monocular diplopia. The optical causes can then be treated with glasses, contact lenses, refractive or cataract surgery and artificial tears.
Physiological diplopia is the phenomenon in which targets that are not in the area of focus, but in front or behind the point of fixation, are seen as double. It is more common in children; in adults, it is usually centrally suppressed. The test of looking at a distant object while fixation is directed to a near target must demonstrate the phenomenon and no other eye movement abnormalities or underlying neurological disorder must be reassured.
Binocular diplopia
History of binocular diplopia A detailed history of diplopia has a very
important role in establishing the diagnosis. The assessment must include the onset, quality, direction, comitancy, variability or fatigability, associated symptoms or diseases. The onset of diplopia is most often sudden, but it can also be gradual, determined by trauma, or spontaneous. While the acute onset is more suggestive of a vascular event but is not very specific, the gradual progression or diplopia that has changed the pattern is more indicative of a compressive lesion. The direction of diplopia can be horizontal, vertical, and oblique. When right and left rectus muscles are affected either by impaired nervous control or by muscle function, the diplopia is horizontal. The most common causes of horizontal diplopia are VIth nerve palsy and internuclear ophthalmoplegia. Horizontal diplopia that appears only after a prolonged near vision is highly pointing towards a convergence insufficiency (most common in patients with Parkinson’s disease). Diplopia is worst (the patient has a maximal separation of images) in the region of action of the paralyzed muscle and the false image (the image that belongs to the eye with the impaired muscle) is
always peripherally situated. Vertical diplopia can appear in thyroid eye disease (inferior rectus muscle is most commonly affected), orbital floor fracture, trochlear nerve palsy, supranuclear or infranuclear lesions. Oblique and torsional (tilted image) diplopia are seen in superior and inferior muscle impairment and lateral medullary syndrome. Comitant deviations will be equal in all directions. Usually, comitant deviations do not induce diplopia due to cortical suppression (patients with congenital strabismus). Variations of diplopia during the day, with an exacerbation in the second half, improvement after rest and associated ptosis that is also intermittent are suggestive of myasthenia gravis (autoimmune neuromuscular junction disease) [2].
Evaluation for binocular diplopia
The examination of binocular diplopia must assess the presence or absence of local findings (eyelid position, facial sensation, orbicularis oculi strength, and exophthalmos) and ocular motility. An important displacement of the ocular globe must be determined if resulting from exophthalmos or enophthalmos. Spontaneous (exophthalmos, congestion) or posttraumatic local findings must include tonometry, ultrasound, CT scan, MRI, neurologic and neuro-surgery examination in their evaluation. The alignment of the eyes starts with the observation of the eyes in primary position, upgaze, downgaze, lateral gaze, and cover-uncover test. Cross-cover test will identify the presence of latent deviation (phoria). Hess test, Maddox rod and red glass testing are useful for the measurement of ocular deviation. Parks-Bielschowsky test is used for the identification of the paretic muscle in vertical diplopia. Forced duction test can identify if the restricted movement of the eye is due to mechanical restriction (important to assess in blow out fractures) or agonist muscle weakness. The misalignment of visual axes is most often due to the dysfunction of extraocular muscles.
Cranial nerve palsies
Oculomotor nerve palsy Complete oculomotor nerve palsy is
revealed when superior, inferior, medial recti, oblique inferior and superior levator palpebral

Romanian Journal of Ophthalmology 2017; 61(3): 166-170
168 Romanian Society of Ophthalmology
© 2017
are affected giving a dysfunction that will generate ptosis and downgaze with lateral gaze position of the eye. Paralysis of ciliary muscle and pupillary sphincter will associate fixed dilated pupil. Describing the pupil as spared or involved is very important. Pupil sparing will show a normal size and reactivity to light, contrary to the pupillary involvement that indicates mydriasis and hyporesponsiveness to light and accommodation. In case of relative pupillary sparing, the pupil is affected, but more than 0.5 mm and up to 2 mm remains reactive to light. Due to the anatomical placement of the pupillary fiber along the superficial layer of the nerve, pupil involvement is present when there is external compression (especially posterior communicating artery aneurysm). In this case, emergency MRI or CT of the brain is required, followed by catheter angiography. Neuroimaging is not necessary in complete, pupil-sparing oculomotor palsies that appear in older patients over 50 with multiple vascular risk factors (diabetes, hypertension, and atherosclerosis). Moreover, the third nerve palsy is secondary to vascular microinfarction. If after 3 months from third nerve palsy onset, the recovery is not complete, or there are other cranial nerve involvements, neuroimaging must be indicated. If the pupil is dilated and unresponsive but there is no extraocular movement or eyelid impairment, the patient does not present with a third nerve palsy [3].
Trochlear nerve palsy
Trochlear nerve palsy will impair the function of superior oblique muscle. It causes vertical, oblique, or torsional diplopia that is more pronounced in downgaze. These patients usually develop a contralateral head tilt as a reaction to counteract the vertical diplopia. If ipsilateral oculomotor nerve palsy is also present, testing the superior oblique muscle function can be difficult because the muscle acts as a depressor only if adduction is present. In this situation, if the eye can do intorsion on attempted downgaze, the muscle may have a normal function. Ocular motility testing will show ipsilateral hypertropia that is emphasized on ipsilateral head tilt and contralateral gaze. Thyroid eye disease and myasthenia gravis must be excluded for apparent trochlear nerve palsy. Besides microvascular disease, a frequent cause
of trochlear nerve palsy is head trauma. Intermittent diplopia can appear in decompensated congenital trochlear nerve palsy (patients present with long-standing head tilt) or superior oblique myokymia that is a rare monocular disorder, in which high frequency burst will contract the muscle those last seconds and occurs multiple times per day. The fourth cranial nerve has a short course, and, in isolated palsies, is usually not affected by aneurysm, tumors or demyelinating processes [4].
Abducens nerve palsy
The abducens nerve palsy (has the longest intracranial course) is the most common nerve palsy, followed by trochlear and oculomotor in second and third place. Due to its long path, it is sensitive to direct and indirect lesions. The sixth nerve palsy will generate lateral rectus muscle paresis (esotropia) and horizontal diplopia that is worse at distance. The causes of sixth nerve palsy may include microvascular ischemia that requires neuroimaging (MRI with gadolinium) if there is progression or absence of improvement, and raised intracranial pressure if the dysfunction is transient, frequently bilateral but asymmetric. Raised intracranial pressure requires neuroimaging and sometimes lumbar puncture. Myasthenia gravis and Duane retraction syndrome must be excluded in abducens nerve palsy thyroid eye disease [5].
Convergence insufficiency
Convergence insufficiency is a sensory and neuromuscular disorder of the binocular visual system that causes horizontal diplopia after prolonged near vision. It is present in children and adults, and is of idiopathic cause or can be developed after head trauma. Moreover, convergence insufficiency is more common in Parkinson’s disease patients. Medication can also influence convergence disorders by exacerbating the symptoms, like antidepressants, through their anticholinergic action on accommodation. Patients usually present with diplopia, asthenopia, headache, letters that “mix together” after sustained near tasks (reading, writing, computer working) and making eye contact. Examination will reveal high exophoria at near. Symptoms cease after resting periods but return
Romanian Journal of Ophthalmology 2017; 61(3): 166-170
169
Romanian Society of Ophthalmology © 2017
with near activities. Treatment of convergence insufficiency aims to improve convergence thought exercises by pencil push-ups therapy, changing fixation from distance to near, stereograms or computer orthoptics. In addition, orthoptic training with prisms or even strabismus surgery is occasionally indicated [6].
Divergence insufficiency
Divergence insufficiency is a disorder present in older adults that manifests itself by horizontal diplopia at distance. Examination will show esodeviation that is comitant in all gazes at distance but profoundly reduced or even presenting exophoria at near. High myopia with long anterior-posterior axis is associated with divergence insufficiency probably due to the anatomical insertion and modified angles of extraocular muscles. Patients usually present with gradual onset, variable horizontal diplopia at distance, asthenopia, and motion sickness. The pattern of sudden onset will redirect the diagnosis towards sixth nerve palsy. Moreover, papilledema and endpoint nystagmus are important in the differential diagnosis of divergence insufficiency pointing the clinician towards finding a neurological disorder. In these cases, neuroimaging should be considered. In many cases, divergence insufficiency will resolve spontaneously. Treatment options include base-out prisms correction for distance that may cause diplopia if they are worn at near, orthoptic exercises and surgery if the misalignment is stable, long-standing and the patients do not tolerate prism glasses.
Thyroid ophthalmopathy
The most common muscle involved in thyroid-associated ophthalmopathy is the inferior rectus that causes vertical diplopia. This symptom is defined by a chin-up face position. Nevertheless, all the extraocular muscles may be affected in various degrees (in the following decreasing frequency: medial rectus, superior rectus and lateral rectus). For thyroid ophthalmopathy, diplopia is worse in the morning, unlike myasthenia gravis that characteristically has double vision in the second half of the day. 5% of Graves disease patients
associate myasthenia gravis. In thyroid ophthalmopathy, exotropia is rare, and should determine the clinician to search for coexisting myasthenia gravis. Pseudo-abducens nerve palsy may be present in medial rectus involvement that will cause abduction restriction [7]. Forced duction test will assess the direction of restriction, while orbital imaging (echography, MRI or CT scan) will show enlargement of extraocular muscles. Thyroid function testing is usually normal (TSH, T3, and T4). Autoimmune markers for thyroid dysfunction include thyroid stimulating immunoglobulin (TSI), thyroglobulin antibody, and thyroid peroxidase antibody. Treatment includes thyroid dysfunction therapy, ocular occlusion for diplopia (prismatic lenses are more inconvenient because they require frequent changes), corticosteroid therapy (for acute and severe phases), surgery, radiotherapy. To stop smoking is also very important for therapeutic improvement [8].
Myasthenia gravis
Myasthenia gravis is an autoimmune disease of the neuromuscular junction, mainly found in the older population. Patients complain of uni- or bilateral ptosis and diplopia along with other systemic manifestations (dysphagia, dysarthria, dysphonia, and dyspnea). Symptoms tend to get worse in the second half of the day and improve with rest. The pupil examination is normal and sensory symptoms and pain is usually not present. Myasthenia gravis can make a differential diagnosis with any oculomotor palsy. A simple clinical diagnostic test is the ice test that is highly sensitive and specific for myasthenia. The ice test implies an ice block that is applied on the eyelid for 5 minutes. The test is positive when improvement of ptosis is more than 2 mm. Edrophonium test remains the standard for myasthenia gravis diagnosis and therapy with pyridostigmine and immunosuppressive treatments are necessary [9].
Internuclear ophthalmoplegia
Internuclear ophthalmoplegia is a conjugate lateral gaze disorder. The patients cannot adduct the eye when it looks at

Romanian Journal of Ophthalmology 2017; 61(3): 166-170
170 Romanian Society of Ophthalmology
© 2017
contralateral gaze (relative to the affected eye). The unaffected eye abducts but with nystagmus. Symptoms include horizontal diplopia when the eyes are in divergence. This disorder is caused by medial longitudinal fasciculus dysfunction.
Postoperative diplopia
Some patients may develop diplopia after surgical procedures, such as cataract, glaucoma, strabismus, or retinal detachment surgery. For cataract surgery, the causes may be anisometropia more than 3-4 D (cover test indicates orthophoria), astigmatism, trauma of the extraocular muscles after peribulbar injections and myotoxicity induced by the anesthetic agent (that resolves usually in weeks or develops towards restrictive strabismus) and IOL malposition. Binocular diplopia may develop after glaucoma surgery that uses implants, especially Baerveldt implants (the 350 Baerveldt model has most cases) and much less frequent for Ahmed valve or trabeculectomy. The use of scleral buckle for retinal detachment may cause diplopia due to injury of the extraocular muscles. Diplopia can be present following strabismus surgery in patients who are overcorrected. Younger patients can suppress the deviated eye unlike adults or if the suppression was before surgery, they may not be able to shift it [10].
Treatment of diplopia
The management of diplopia must be according to the cause that determined it. Common sense will indicate the treatment of the pathology that caused it whenever this is possible. Symptomatic treatment is often used in patients with diplopia who have a significant morbidity rate associated with loss of orientation and confusion. The goal in these patients is to regain single binocular vision. Unilateral occlusion of the poorer eye may be used as treatment when other measures are not successful. In younger patients, the occlusion should be alternative because they have the risk of developing amblyopia. In this case, options include eye patch, frosting of eyeglass lens or semi-opaque tape and contact lens with opaque center. Temporary monocular occlusion is usually necessary in patients who have diplopia
as a cause of ischemic cranial nerve palsies, until diplopia resolves by itself. Fresnel prisms for the realignment of visual axis may also be used in case of vertical and horizontal diplopia but not in torsional diplopia or in the resolving stages, when ocular misalignment may frequently change. Surgical treatment of strabismus is indicated in long-standing, unchanged misalignment for more than 12 months, when other therapies have not been successful. Another option includes botulinum injection in the antagonist of the paralyzed muscle with an effect of 3 to 6 months for a single dose [11].
References
1. Gräf M, Lorenz B. How to deal with diplopia. Rev Neurol. 2012; 168(10):720-728.
2. Dinkin M. Diagnostic approach to diplopia. Continuum. 2014; 20(4 Neuro-ophthalmology):942-965.
3. O'Colmain U, Gilmour C, MacEwen CJ. Acute-onset diplopia. Acta Ophthalmol. 2014; 92(4):382-6.
4. Morillon P, Bremner F. Trochlear nerve palsy. Br J Hosp Med. 2017; 78(3):C38-C40.
5. Elder C, Hainline C, Galetta SL, Balcer LJ, Rucker JC. Isolated Abducens Nerve Palsy: Update on Evaluation and Diagnosis. Curr Neurol Neurosci Rep. 2016; 16(8):69.
6. Kaski D, Bronstein AM. Functional eye movement disorders. Handb Clin Neurol. 2016; 139:343-351.
7. Rao R, MacIntosh PW, Yoon MK, Lefebvre DR. Current trends in the management of thyroid eye disease. Curr Opin Ophthalmol. 2015; 26(6):484-490.
8. Harrad R. Management of strabismus in thyroid eye disease. Eye. 2015; 29(2):234-237.
9. Smith SV, Lee AG. Update on Ocular Myasthenia Gravis. Neurol Clin. 2017; 35(1):115-123.
10. Bailey AK, Sarkisian SR Jr. Complications of tube implants and their management. Curr Opin Ophthalmol. 2014; 25(2):148-53.
11. Rucker JC, Tomsak RL. Binocular diplopia. A practical approach. Neurologist. 2005; 11(2):98-110.

Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:171-180
REVIEW
171 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.32
Update on retinal vascular caliber
Dumitrescu Alina Gabriela* **, Voinea Liliana***, Badarau Ioana Anca**, Paun Vanessa Andrada***, Schowe Marilena****, Ciuluvica Radu***** *Coltea Clinical Hospital, Bucharest, Romania **Physiology Department I, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania ***Ophthalmology Department, University Emergency Hospital; “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania ****Ophthalmology Hospital, Langenfeld, Dortmund, Germany *****Anatomy Department, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania Correspondence to: Dumitrescu Alina Gabriela, MD, Coltea Clinical Hospital, Bucharest, 1 I. C. Bratianu Boulevard, Code 030171, District 3, Bucharest, Romania, Mobile phone: +40721 284 561, E-mail: [email protected] Accepted: September 9th, 2017
Abstract Retinal vessels are the only blood vessels that can be viewed directly, in vivo, repetitively and non-invasively. Retinal vessel caliber is influenced by physiological (age, sex, race, blood pressure, blood glucose, body mass index) and pathological (atherosclerosis, dyslipidemia, smoking) determinants. There are studies on large population groups that demonstrate the associations between retinal vasculature and subclinical or clinical changes in systemic diseases (hypertension, diabetes, stroke, renal or cardiac diseases). The assessment of retinal vessels can provide information about the pathophysiology of many diseases, but it also has a direct applicability in clinic, being used as a screening method that predicts the risk of their occurrence. Keywords: retinal vascular caliber, vessel diameter, hypertension, diabetes, optical coherence tomography, fundus photography
Introduction
The development of ophthalmoscopy in the 19th century has allowed the in vivo, non-invasive study of the retina and its microcirculation. Thus, numerous correlations have been made between changes in the appearance of retinal vessels and the various systemic diseases involving vascular alterations. The most frequent changes in retinal vasculature were observed in hypertensive patients, attempting to make a classification for hypertensive retinopathy. There are several such classifications, but the most well-known and used is that of Keith from 1974 [1].
Table 1. Keith-Wagner-Barker classification of hypertensive retinopathy Grade Retinal vessel morphology I Mild to moderate narrowing or sclerosis of
the arterioles II Moderated to marked arteriolar sclerosis,
arteriovenous nicking, generalized and/ or focal arteriolar narrowing
III Marked arteriolar narrowing and focal constriction, retinal edema, cotton wool spots, hemorrhage
IV Grade III plus papilledema
The disadvantage of this method is the degree of subjectivity and variability among examiners, as well as the difficulty of an

Romanian Journal of Ophthalmology 2017; 61(3): 171-180
172 Romanian Society of Ophthalmology
© 2017
objective assessment of incipient changes that may allow the early therapeutic interventions able to reduce the risk of long-term complications.
The emergence of new retinal imaging methods, such as retinal photographs and optical coherence tomography, allowed a more objective and reproducible assessment of the vascular caliber. Hubbard and collaborators have developed computational formulas for CRAE (central retinal arteriolar equivalent) and CRVE (central retinal venular equivalent) through retinal photography [2]. Based on these coefficients, the AVR (arteriovenous ratio) used in many studies is calculated because its value is not dependent on the optical properties of the eye or the camera. But, this method also has limitations because it does not allow a direct measurement of the vascular caliber, it is based on a single image and does not provide information about the three-dimensional geometry of the vessel [3]. The appearance of OCT (optical coherence tomography) offers three-dimensional images of vessels, easy to obtain and independent of magnification. Thus, Goldenberg used a horizontal cube scan at the optic disc margin for retinal vessel diameter measurement with SD-OCT (spectral domain OCT) [4]. Moreover, Muraoka used a circular scan to detect the cross section image of the retinal vessel and the measured retinal vessel diameter, the lumen diameter and the wall thickness in zone A [5] and Zhu used a line scan perpendicular to the vessel to measure the vessel diameter and the lumen diameter in zone B [6].
There are new vascular parameters that began to be measured in relation to the cardiovascular changes. These are the branching angle of vessels, retinal vessel tortuosity, and fractal dimensions. Thus, the local topographic features of retinal vessels may provide information on the appearance of systemic and cerebral microcirculation. The development of new technologies will allow the dynamic and functional examination of the retinal vasculature by the flickering light response used by the Doppler flowmeter and the dynamic vessel analyzer [7,8]. There is still insufficient data on the information provided by these innovative methods.
With all these methods available, studies have been conducted on large groups of individuals to find correlations between the retinal vessel diameter and the demographic characteristics and the associated systemic pathology of people.
Determinants of retinal vascular caliber Age
A first study on 20 newborns reported an average value of 85.5 μm retinal arterioles and a 130 μm retinal diameter without gender differences [9]. In the first 6 years of life, when the body weight increases about 5-fold, the arteriolar and retinal caliber doubles [10]. By adulthood, the venular diameter remains constant, while the arteriolar caliber continues to increase [11]. Then, after the age of 45, both the arteriolar and the venular caliber begin to slowly decrease by 1.8-4.8 μm for each decade of age [12]. Therefore, by the age of 80 years, the vascular caliber is with 10-12 μm, smaller than at 55-60 years [13]. Sex
In the Cardiovascular Health Study group and MESA (The Multi-Ethnic Study of Atherosclerosis), higher values of retinal arteriolar caliber and AVR were found in women compared to men, linking these values to the protective effect of estrogens on coronary circulation [14,15]. Race
Both arteriolar and venular caliber have higher values in African-American and Hispanic races than in Caucasians and Chinese. These values may correlate with the differences in the distribution of cardiovascular risk factors among populations of different ethnicity, but the data are insufficient [15,16]. Birth weight
Mitchell measured the retinal vascular diameter in a study on 1,369 children and estimated that the average arteriolar diameter was lower by 2 μm for every kilo in minus to the birth weight [10]. A twin study in Tasmania found a direct correlation between the birth weight and the retinal arteriolar caliber [17]. These changes may suggest a structural

Romanian Journal of Ophthalmology 2017; 61(3): 171-180
173
Romanian Society of Ophthalmology © 2017
adaptation of microcirculation to nutrition and growth restriction. Also, children with a small weight at birth are at a greater risk of developing a cardiovascular disease in adulthood. Genetics
Data from the Beaver Dam Eye Study, based on genome analysis, demonstrates a genetic contribution to the variation of the retinal vasculature, with similar values for individuals in the same family [18]. In another large cohort study, four genes responsible for retinal vasculature variation (19q13, 6q24, 12q24, and 5q14) were identified. In nearby regions, genes for essential hypertension, coronary heart disease, endothelial dysfunction, and angiogenesis are located [19]. These new data suggest the importance of studying retinal microcirculation to understand the pathogenesis of the cardiovascular disease. Modifiable factors that influence retinal vasculature Blood pressure (BP)
There is a clear association between hypertension and peripheral arterial narrowing [20]. Initially, it was believed that the impaired sodium homeostasis is responsible for the fluid expansion that leads to cardiac overload and the BP increase with secondary structural changes on peripheral circulation [21]. New hypotheses consider the arterial changes responsible for arterial hypertension [22]. Studies on laboratory animals have shown decreases in retinal arteriolar diameters prior to arterial hypertension in rats [23] and studies in humans showed that people with a family history of hypertension have lower arteriolar diameters than those with no history [24]. Blood glucose
Many studies have correlated the presence of hyperglycemia with a higher retinal vein diameter [25]. Hyperglycemia and secondary retinal ischemia increase blood flow, while altered glucose metabolism generates inflammatory cytokine and nitric oxide release, processes leading to endothelial dysfunction with secondary venular dilation [26].
Body mass index (BMI) Studies such as MESA and ARIC (The
Atherosclerosis Risk in Communities Study) have found an association between the increased retinal vein caliber and the obesity indicators (high body mass index and increased waist-hip ratio). The Blue Mountain Eye Study reports that an increased retinal diameter may predict the incidence of obesity in 5 years, suggesting that the microcirculation dysfunction is involved in the pathogenesis of obesity [27]. The Singapore Prospective Study Program also found a link between the lack of physical activity and the larger retinal venular caliber [28]. Dyslipidemia
Both, MESA and ARIC have demonstrated a correlation between the increased retinal venular caliber and dyslipidemia defined as elevated plasma levels of triglycerides and LDL cholesterol and low HDL cholesterol [29,30]. Atherosclerosis
A link between low AVR and the presence of carotid artery atheromatosis was demonstrated in the ARIC study [16]. Moreover, the Rotterdam study correlated the small AVR with the intima-mean thickness of the carotid artery wall as well as the increased stiffness of the arterial wall (marker of atherosclerosis) [29]. MESA related a retinal arterial narrowing with a concentric remodeling of the left ventricle and the myocardial blood flow, while the larger venous caliber is associated with the low index ankle arm [31,32].
In Beaver Dam Eye Study, the indicators of endothelial dysfunction (soluble intercellular adhesion molecule-1 and E-selectin serum) and the inflammatory markers (PCR and leukocyte counts) were associated with an increased retinal venous diameter [33]. Thus, atherosclerosis, inflammation, and endothelial dysfunction play an important role in demonstrating the link between the retinal venular dilatation and the systemic cardiovascular disease. Smoking
The ARIC study demonstrated an association between low AVR and cigarette smoking in middle-aged individuals. In the Rotterdam study, higher values of arteriolar and

Romanian Journal of Ophthalmology 2017; 61(3): 171-180
174 Romanian Society of Ophthalmology
© 2017
retinal venular caliber were correlated with smoking [16,29]. Alcohol
Recent studies have linked alcohol consumption to the risk of cardiovascular disease, but few have also analyzed the relationship with retinal vasculature [16]. The ARIC study found lower AVR values for alcohol consumers and MESA narrower arteriolar caliber [14]. Longitudinal studies are required to establish the mechanism by which alcohol consumption influences the retinal vascular size. Drug administration
The Beaver Dam Eye Study reported an association between the topical beta blocking agents for the treatment of glaucoma and the narrow retinal arterioles and venules; Beta blockers administered orally do not have the same effect [34]. According to the Blue Mountain Eye Study, retinal vascular diameters remain constant over time, suggesting the protective effect of estrogens on the long term in women who receive substitution hormone therapy for more than 10 years [35]. This study also reported a possible association between the combined aspirin-antihypertensive therapy and the larger diameters of retinal arterioles, which confirms the anti-inflammatory effect of aspirin on microcirculation [36]. Associations between retinal vasculature and systemic diseases Hypertension
It is well known that the narrowing of the retinal arteriolar caliber is an early sign of hypertension secondary to chronic exposure to high blood pressure. A meta-analysis that comprised 5 large studies with a total of 19,633 patients reported that for every 10 mmHg of BP increase there was a decrease of 2.0-2.4 μm of the retinal arteriolar caliber [37]. The Rotterdam study reported a greater influence of BP on the retinal vascular size in younger and more prominent on arterioles than venules [22]. This hypothesis can be supported by the fact that, in the elderly, the stiffness and the arterial wall sclerosis prevent vascular adaptation to higher blood pressures. Thus, the narrow arteriolar caliber may be a marker for the assessment of
the chronic effects of hypertension (aortic wall stiffness, hypertrophy and remodeling of the left ventricle) [38]. Beaver Dam, ARIC, Blue Mountains, and Rotterdam have found lower values of retinal arteriolar diameter and AVR in patients who subsequently developed hypertension in 3 years than in those with a normal blood pressure. These new data make the arteriolar caliber and AVR a pre-clinical marker of hypertension. A raised peripheral vascular resistance in small vessels, including retinal vessels, is the initial condition for the development of essential hypertension [22,39]. Diabetes Mellitus
Microvascular pathology has an important role in the pathophysiology of diabetes mellitus [40]. Since the retinal vessels are the only small vessels that can be readily available, we can study the effect of hyperglycemia on the retinal vascular caliber [41]. Some studies (ARIC and Beaver Dam Eye) showed a link between the low AVR and the higher risk of developing Diabetes Mellitus independent of the cardiovascular risk factors [42]. In the Rotterdam Eye Study, the increased venular diameter was correlated with the impaired fasting glucose. In subsequent studies (MESA, Australian Diabetes, Obesity and Lifestyle and Blue Mountains Eye Study), an association was also reported between Diabetes and the increased retinal arteriolar caliber [43-45]. In WESDR (Wisconsin Epidemiologic Study of Diabetic Retinopathy), in patients with type 1 diabetes mellitus, a higher glycosylated hemoglobin was associated with a higher retinal vascular caliber, both venules and arterioles [46]. Coronary heart disease
Studies have found an association between the retinal microvascular morphology and the incidence of coronary pathology [47]. The ARIC study correlated a small AVR with the high risk of coronary artery disease in women, and CHS demonstrated that small AVR is generated by both, narrow arteriolar caliber and increased venular caliber [48]. The Blue Mountains Eye Study and the Beaver Dam Eye study correlated small AVR (due to larger venular caliber) with the double risk of coronary heart disease mortality in persons under 75 years old. For women, an additional 1.5-fold increase in risk is

Romanian Journal of Ophthalmology 2017; 61(3): 171-180
175
Romanian Society of Ophthalmology © 2017
associated with a narrow arteriolar caliber [49]. In his meta-analysis of 22,159 people, McGeechan revealed a correlation between the narrow arteries and the larger venules and the risk for coronary artery disease in women [50]. In WESDR, in patients with type I diabetes mellitus, the risk of cardiovascular mortality is higher in those with low AVR. In some studies, the smaller retinal arteriolar caliber was associated with signs of concentric remodeling of the left ventricle, seen on magnetic resonance imaging (MRI). Thus, the retinal microvascular changes may provide information on subclinical myocardial abnormalities, especially in middle-aged women (49-75 years) [15,31,46]. Brain diseases
It has been hypothesized that the impaired cerebral microcirculation is a major risk factor for stroke [51]. Since small cerebral vessels are quite similar in embryological origin, structure and function to retinal vessels, an attempt is being made to link the appearance of retinal vessels with brain pathologies [52]. Cardiovascular Health Study (CHS) and ARIC reported an association between an increased risk of ischemic stroke and low AVR; Rotterdam study demonstrated that people with a larger retinal venular caliber have a 12% higher risk of developing cerebral infarction [53]. McGeechan also concluded that the stroke risk is associated with an increased retinal venular diameter and there is no correlation with the arteriolar caliber [54]. There is only one study demonstrating the correlation between the increased venular caliber and the risk of intracerebral hemorrhage [55]. In WESDR, in patients with type II diabetes mellitus, both narrow arterioles and the dilated venules are correlated with a high mortality caused by stroke after 22 years [46]. Also, in ARIC, CHS and Rotterdam Study, subclinical changes in MRI (lacunar infarcts, white matter lesions and cortical atrophy) were found in healthy individuals with a larger venular caliber [56,57]. Patients without stroke retinal venular changes were associated with a poorer cognitive function and an increased risk of developing vascular dementia [58]. In conclusion, there are numerous links between the retinal microvascular changes and clinical cerebral pathologies, such as stroke, or sub-clinical, respectively, small vessels disease.
Kidney diseases There are fewer studies on kidney diseases
and vascular morphology, many of them on groups of patients with diabetes, in whom retinopathy and nephropathy are thought to have a common pathogenic pathway (endothelial dysfunction due to inflammation) [59,60]. WESDR demonstrated that in patients with type I Diabetes, the larger retinal venular diameter predicted proteinuria and renal impairment on the long run, and in those with type II diabetes, the venular retinal dilatation occurred before nephropathy [61]. ARIC revealed that low AVR was correlated with higher serum creatinine levels in both diabetic and non-diabetic patients [60]. In a study from 2017, Daien concluded that both CRAE and CRVE were negatively correlated with urinary albumin excretion and did not correlate with the estimated glomerular filtration rate [62]. Further, studies are needed to demonstrate correlations between retinal microvascular changes and renal dysfunctions. It is known that microvascular changes are important in the pathophysiology of diabetic nephropathy [60]. Ocular diseases
In the pathophysiology of many ocular diseases, changes in retinal vessels are caused by cardiovascular pathologies. Diabetic retinopathy
The MESA study, conducted on approximately 6,000 people of different ethnicities with normal blood sugar, hyperglycemia or diagnosed with Diabetes, evaluated retinal microcirculation. Thus, higher CRAE values were found in patients with Diabetes while CRVE was higher in those with impaired fasting glucose and those with Diabetes. Only large venous caliber was correlated with changes in glycemic and glycosylated hemoglobin, as well as the presence of diabetic retinopathy [44]. The combination of increased venular diameters with diabetes was also demonstrated by ARIC, Rotterdam and WESDR [63]. The WESDR study on patients with type II diabetes mellitus found an association between small CRAE and the increased risk of lower limb amputations and stroke mortality. Large CRVE was associated with an increased incidence of nephropathy and stroke mortality.

Romanian Journal of Ophthalmology 2017; 61(3): 171-180
176 Romanian Society of Ophthalmology
© 2017
Also in WESDR, large venular caliber at the onset of diabetes was associated with a higher incidence of proliferative diabetic retinopathy on the long run [61]. According to the Diabetic Retinopathy Study, the increase in the retinal venular caliber is a predictor of a low visual acuity due to the progression of diabetic retinopathy. Arterial and venular changes may be caused by the presence of endothelial dysfunction due to the inflammation and retinal hypoxia caused by hyperglycemia [64,65]. Age-related macular degeneration (AMD)
Epidemiological studies have shown that both AMD and the cardiovascular disease have similar risk factors (smoking, high blood pressure, atherosclerosis), as well as an increased risk of stroke and myocardial infarction [66]. Due to these data, hypotheses were made that the pathological processes involved in the occurrence of AMD may lead to changes in the retinal vasculature. Longitudinal studies on Caucasians, Beaver Dam Eye Study, Blue Mountains Eye Study (BMES), and Rotterdam Study have found no association between the retinal vascular caliber and AMD [67]. A study on the Asian population, the Singapore Malay Eye Study, concluded that a higher retinal venular diameter is associated with retinal pigment abnormalities and early stage AMD. Although a smaller arterial diameter was associated with retinal pigmentation abnormalities, there is no significant correlation between arteriolar caliber and AMD occurrence [68]. In contrast, the Handan Eye Study showed that a narrow arteriolar diameter is associated with incipient forms of AMD, while the venular caliber is not [69]. Primary Open-Angle Glaucoma (POAG)
Glaucomatous optic neuropathy is defined by reduced retinal nerve fiber layer (RNFL) thickness, increased Cup Disc ratio and characteristic visual field defects [70]. There are many hypotheses regarding the correlations between the retinal arteriolar caliber reduction and RNFL loss. These hypotheses are supported by the fact that the loss of retinal ganglion cells decreases local metabolic and vascular requirements, leading to arteriolar
vasoconstriction [71]. Various study hypotheses have been outlined. In a group of patients with asymmetric glaucoma, De Leon found lower values of CRAE and CRVE in the eye with severe glaucomatous impairment [72]. In BMES, lower arteriolar caliber values were found in POAG patients than in non-glaucoma patients [73]. The Singapore Malay Eye study found significant associations between the retinal vascular size and glaucoma prevalence as well as a larger cup disc ratio [74]. The Beijing Eye Study showed that POAG patients had a smaller retinal arteriolar caliber and a similar venular caliber compared to those without glaucoma [75]. In the Handan Eye Study, both POAG and PCAG (primary closed angle glaucoma) patients have a retinal arteriolar and a retinal venular caliber smaller than the non-glaucoma control group [76]. Hall found a significant correlation between the retinal arteriolar diameter and the visual field defects in POAG patients [77]. Both Beaver Dam Eye Study and Rotterdam Study have not found correlations between the retinal vascular caliber and glaucoma prevalence, increased Cup Disc ratio or high IOP. Further studies are needed to define the role of retinal vasculature in the pathogenesis of POAG. Retinal vein occlusion
There was only one study in Korea, on 10890 people, of which 0.8% were diagnosed with branch retinal vein occlusion, which measured CRAE and CRVE. The results showed that BRVO eyes had lower mean CRAE and CRVE values compared to normal eyes [78].
Conclusions
In conclusion, there are links between retinal vasculature and the large number of physiological or pathological changes in the human body. Narrow retinal arteries and, possibly, a small AVR are found in elderly, hypertensive, with vascular atherosclerosis and alcohol-consuming patients. Moreover, patients with POAG have a small arteriolar caliber. There are cases of increased arteriolar diameter, such as females (possibly because of hormone replacement therapy), African-American or Hispanic race, smokers, or people who have antihypertensive and aspirin-associated

Romanian Journal of Ophthalmology 2017; 61(3): 171-180
177
Romanian Society of Ophthalmology © 2017
treatment. An increased retinal venular caliber is found in African-American and Hispanic patients, in those with a large BMI, dyslipidemia, atherosclerosis, who smoke, have an impaired fasting glucose, or diabetes and with cerebrovascular disease (stroke or vascular dementia). In patients with diabetes mellitus, a larger venous caliber suggests an increased risk of retinopathy and diabetic nephropathy. Combined large venular and narrow arteriolar caliber can predict an increased risk of coronary artery disease, especially in women, or may suggest a higher mortality caused by stroke in patients with Diabetes.
Retina examination offers information about many systemic disorders. The fact that it can be explored directly, in vivo and noninvasively, makes eye examination a mandatory investigation in all patients. The new imaging techniques of the last decade allow an easy exploration of retinal circulation. Retinal vascular caliber is a quantitative assessment of microvascular structural changes that can be correlated with the cardiovascular risk factors or the glycemic profile. Numerous studies have demonstrated that the value of retinal vascular caliber can also be used as a noninvasive biomarker for the most important 21st century diseases (cardiovascular disease and diabetes). More and more rapid and easy examination methods of retinal vasculature will be developed and used in the coming years.
Conflict of interests The authors declare no conflict of interest.
References
1. Wong TY, Knudtson MD, Klein R, Klein BE, Meuer SM, Hubbard LD. Computer-assisted measurement of retinal vessel diameters in the Beaver Dam Eye Study: methodology, correlation between eyes, and effect of refractive errors. Ophthalmology. 2004.
2. Hubbard LD, King WN, Clegg LX, Lein R, Cooper LS, Sharett AR, Davis MD, Cai J. Methods for evaluation of retinal microvascular abnormalities associated with hypertension/sclerosis in the Atherosclerosis Risk in Communities Study. Ophthalmology. 1999; (106):2269-80.
3. Knudtson MD, Lee KE, Hubbard LD, Wong TY, Klein R, Klein BE. Revised formulas for summarizing retinal vessel diameters. Current Eye Research. 2003; (27):143-9.
4. Goldenberg D, Shahar J, Loewenstein A, Goldstein M. Diameters of retinal blood vessels in a healthy cohort as measured by spectral domain optical coherence tomography. Retina. 2013; (33):1888-94.
5. Muraoka Y, Tsujikawa A, Kumagai K, Akiba M, Ogino K, Murakami T, Yoshimura N. Age-and hypertension-dependent changes in retinal vessel diameter and wall thickness: an optical coherence tomography study. American Journal of Ophthalmology. 2013; (156):706-14.
6. Zhu TP, Tong YH, Zhan HJ, Ma J. Update on retinal vessel structure measurement with spectral-domain optical coherence tomography. Microvascular Research. 2014; (7-14).
7. Guan K, Hudson C, Flanagan JG. Variability and repeatability of retinal blood flow measurements using the Canon Laser Blood Flowmeter. Microvascular Research. 2003; 65(3):145-51.
8. Blondal R, Sturludottir MK, Hardarson SH, Halldorsson GH, Stefánsson E. Reliability of vessel diameter measurements with a retinal oximeter. Graefe's Archive for Clinical and Experimental Ophthalmology. 2011; 249(9)(1311-1317).
9. Kandasamy Y, Smith R, Wright IM. Retinal microvasculature measurements in full-term newborn infants. Microvascular Research. 2011; 82(3):381-4.
10. Mitchell P, Liew G, Rochtchina E, Wang JJ, Robaei D, Cheung N, Wong TY. Evidence of arteriolar narrowing in low-birth-weight children. Circulation. 2008; 118(5):518-24.
11. Wong TY, Knudtson MD, Klein R, Klein BE, Meuer SM, Hubbard LD. Computer-assisted measurement of retinal vessel diameters in the Beaver Dam Eye Study: methodology, correlation between eyes, and effect of refractive errors. Ophthalmology. 2004; 111(6):1183-90.
12. Leung H, Wang JJ, Rochtchina E, Tan AG, Wong TY, Klein R et al. Relationships between age, blood pressure, and retinal vessel diameters in an older population. Investigative Ophthalmology & Visual Science. 2003; 44(7):2900-4.
13. Wong TY, Klein R, Klein BE, Meuer SM, Hubbard LD. Retinal vessel diameters and their associations with age and blood pressure. Investigative Ophthalmology & Visual Science. 2003; 44(11):4644-50.
14. Wong TY, Islam FM, Klein R, Klein BE, Cotch MF, Castro C et al. Retinal vascular caliber, cardiovascular risk factors, and inflammation: the multi-ethnic study of atherosclerosis (MESA). Investigative Ophthalmology & Visual Science. 2006; 47(6):2341-50.
15. Wong TY, Klein R, Sharrett AR, Manolio TA, Hubbard LD, Marino EK et al. The prevalence and risk factors of retinal microvascular abnormalities in older persons: The Cardiovascular Health Study. Ophthalmology. 2003; 110(4):658-66.
16. Klein R, Sharrett AR, Klein BE, Chambless LE, Cooper LS, Hubbard LD et al. Are retinal arteriolar abnormalities related to atherosclerosis?: The Atherosclerosis Risk in Communities Study. Arteriosclerosis, thrombosis, and vascular biology. 2000; 20(6):1644-50.
17. Sun C, Ponsonby AL, Wong TY, Brown SA, Kearns LS, Cochrane J et al. Effect of birth parameters on retinal

Romanian Journal of Ophthalmology 2017; 61(3): 171-180
178 Romanian Society of Ophthalmology
© 2017
vascular caliber: the Twins Eye Study in Tasmania. Hypertension. 2009; 53(3):487-93.
18. Lee KE, Klein BE, Klein R, Knudtson MD. Familial aggregation of retinal vessel caliber in the beaver dam eye study. Investigative Ophthalmology & Visual Science. 2004; 45(11):3929-33.
19. Ikram MK, Sim X, Jensen RA, Cotch MF, Hewitt AW, Ikram MA et al. Four novel Loci (19q13, 6q24, 12q24, and 5q14) influence the microcirculation in vivo. PLoS Genetics. 2010; 6(10):e1001184.
20. Mulvany MJ. Are vascular abnormalities a primary cause or secondary consequence of hypertension?. Hypertension. 1991; 18(3 Suppl):I52-7.
21. Levy BI, Ambrosio G, Pries AR, Struijker-Boudier HA. Microcirculation in hypertension: a new target for treatment?. Circulation. 2001; 104(6):735-40.
22. Ikram MK, Witteman JC, Vingerling JR, Breteler MM, Hofman A, de Jong PT. Retinal vessel diameters and risk of hypertension: the Rotterdam Study. Hypertension. 2006; 47(2):189-94.
23. le Noble JL, Tangelder GJ, Slaaf DW, van Essen H, Reneman RS, Struyker-Boudier HA. A functional morphometric study of the cremaster muscle microcirculation in young spontaneously hypertensive rats. Journal of Hypertension. 1990; 8(8):741-8.
24. Muraoka YTA, Kumagai K, Akiba M, Ogino K, Murakami T, Yoshimura N. Age-and hypertension-dependent changes in retinal vessel diameter and wall thickness: an optical coherence tomography study. American Journal of Ophthalmology. 2013; (156):706-14.
25. Ciulla TA, Amador AG, Zinman B. Diabetic retinopathy and diabetic macular edema: pathophysiology, screening, and novel therapies. Diabetes Care. 2003; 26(9):2653-64.
26. Nguyen TT, Wang JJ, Wong TY. Retinal vascular changes in pre-diabetes and prehypertension: new findings and their research and clinical implications. Diabetes Care. 2007; 30(10):2708-15.
27. Wang JJ, Taylor B, Wong TY, Chua B, Rochtchina E, Klein R et al. Retinal vessel diameters and obesity: a population-based study in older persons. Obesity (Silver Spring). 2006; 14(2):206-14.
28. Anuradha S, Healy GN, Dunstan DW, Tai ES, Van Dam RM, Lee J et al. Associations of physical activity and television viewing time with retinal vascular caliber in a multiethnic Asian population. Investigative Ophthalmology & Visual Science. 2011; 52(9):6522-8.
29. Ikram MK, de Jong FJ, Vingerling JR, Witteman JC, Hofman A, Breteler MM et al. Are retinal arteriolar or venular diameters associated with markers for cardiovascular disorders?. The Rotterdam Study. Investigative Ophthalmology & Visual Science. 2004; 45(7):2129-34.
30. Sun C, Wang JJ, Mackey DA, Wong TY. Retinal vascular caliber: systemic, environmental, and genetic associations. Survey of Ophthalmology. 2009; 54(1):74-95.
31. Cheung N, Bluemke DA, Klein R, Sharrett AR, Islam FM, Cotch MF et al. Retinal arteriolar narrowing and left ventricular remodeling: the multi-ethnic study of atherosclerosis. Journal of the American College of Cardiology. 2007; 50(1):48-55.
32. Wang L, Wong TY, Sharrett AR, Klein R, Folsom AR, Jerosch-Herold M. Relationship between retinal arteriolar narrowing and myocardial perfusion: multi-ethnic study of atherosclerosis. Hypertension. 2008; 51(1):119-26.
33. Klein R, Klein BE, Knudtson MD, Wong TY, Tsai MY. Are inflammatory factors related to retinal vessel caliber?. The Beaver Dam Eye Study. Arch Ophthalmol. 2006; 124(1):87-94.
34. Wong TY, Knudtson MD, Klein BE, Klein R, Hubbard LD. Medication use and retinal vessel diameters. Am J Ophthalmol. 2005; 139(2):373-5.
35. Wong TY, Knudtson MD, Klein BE, Klein R, Hubbard LD. Estrogen replacement therapy and retinal vascular caliber. Ophthalmology. 2005; 112(4):553-8.
36. Liew G, Mitchell P, Leeder SR, Smith W, Wong TY, Wang JJ. Regular aspirin use and retinal microvascular signs: the Blue Mountains Eye Study. Journal of Hypertension. 2006; 24(7):1329-35.
37. Chew SK, Xie J, Wang JJ. Retinal arteriolar diameter and the prevalence and incidence of hypertension: a systematic review and meta-analysis of their association. Current Hypertension Reports. 2012; 14(2):144-51.
38. Wong TY, Shankar A, Klein R, Klein BE, Hubbard LD. Prospective cohort study of retinal vessel diameters and risk of hypertension. BMJ. 2004; 329(7457):79.
39. Smith W, Wang JJ, Wong TY, Rochtchina E, Klein R, Leeder SR et al. Retinal arteriolar narrowing is associated with 5-year incident severe hypertension: the Blue Mountains Eye Study. Hypertension. 2004; 44(4):442-7.
40. Tooke JE. Microvascular function in human diabetes. A physiological perspective. Diabetes. 1995; 44(7):721-6.
41. Caballero AE, Arora S, Saouaf R, Lim SC, Smakowski P, Park JY et al. Microvascular and macrovascular reactivity is reduced in subjects at risk for type 2 diabetes. Diabetes. 1999; 48(9):1856-62.
42. Wong TY, Klein R, Sharrett AR, Schmidt MI, Pankow JS, Couper DJ et al. Retinal arteriolar narrowing and risk of diabetes mellitus in middle-aged persons. Jama. 2002; 287(19):2528-33.
43. Wong TY, Shankar A, Klein R, Klein BE, Hubbard LD. Retinal arteriolar narrowing, hypertension, and subsequent risk of diabetes mellitus. Archives of Internal Medicine. 2005; 165(9):1060-5.
44. Nguyen TT, Wang JJ, Sharrett AR, Islam FM, Klein R, Klein BE et al. Relationship of retinal vascular caliber with diabetes and retinopathy: the Multi-Ethnic Study of Atherosclerosis (MESA). Diabetes Care. 2008; 31(3):544-9.
45. Tikellis G, Wang JJ, Tapp R, Simpson R, Mitchell P, Zimmet PZ et al. The relationship of retinal vascular calibre to diabetes and retinopathy: the Australian Diabetes, Obesity and Lifestyle (AusDiab) study. Diabetologia. 2007; 50(11):2263-71.
46. Hirai FE, Moss SE, Klein BE, Klein R. Relationship of glycemic control, exogenous insulin, and C-peptide levels to ischemic heart disease mortality over a 16-year period in people with older-onset diabetes: the Wisconsin Epidemiologic Study of Diabetic

Romanian Journal of Ophthalmology 2017; 61(3): 171-180
179
Romanian Society of Ophthalmology © 2017
Retinopathy (WESDR). Diabetes Care. 2008; 31(3):493-7.
47. McClintic BR, McClintic JI, Bisognano JD, Block RC. The relationship between retinal microvascular abnormalities and coronary heart disease: a review. The American Journal of Medicine. 2010; 123(4):374 e1-7.
48. Wong TY, Klein R, Nieto FJ, Klein BE, Sharrett AR, Meuer SM et al. Retinal microvascular abnormalities and 10-year cardiovascular mortality: a population-based case-control study. Ophthalmology. 2003; 110(5):933-40.
49. Wang JJ, Liew G, Wong TY, Smith W, Klein R, Leeder SR et al. Retinal vascular calibre and the risk of coronary heart disease-related death. Heart. 2006; 92(11):1583-7.
50. McGeechan K, Liew G, Macaskill P, Irwig L, Klein R, Klein BE et al. Meta-analysis: retinal vessel caliber and risk for coronary heart disease. Annals of Internal Medicine. 2009; 151(6):404-13.
51. Wong TY. Is retinal photography useful in the measurement of stroke risk?. The Lancet Neurology. 2004; 3(3):179-83.
52. Wong TY, Klein R, Klein BE, Tielsch JM, Hubbard L, Nieto FJ. Retinal microvascular abnormalities and their relationship with hypertension, cardiovascular disease, and mortality. Survey of Ophthalmology. 2001; 46(1):59-80.
53. Ikram MK, De Jong FJ, Van Dijk EJ, Prins ND, Hofman A, Breteler MM et al. Retinal vessel diameters and cerebral small vessel disease: the Rotterdam Scan Study. Brain: a Journal of Neurology. 2006; 129(Pt 1):182-8.
54. McGeechan K, Liew G, Macaskill P, Irwig L, Klein R, Klein BE et al. Prediction of incident stroke events based on retinal vessel caliber: a systematic review and individual-participant meta-analysis. American Journal of Epidemiology. 2009; 170(11):1323-32.
55. Wieberdink RG, Ikram MK, Koudstaal PJ, Hofman A, Vingerling JR, Breteler MM. Retinal vascular calibers and the risk of intracerebral hemorrhage and cerebral infarction: the Rotterdam Study. Stroke. 2010; 41(12):2757-61.
56. Wong TY, Klein R, Sharrett AR, Couper DJ, Klein BE, Liao DP et al. Cerebral white matter lesions, retinopathy, and incident clinical stroke. Jama. 2002; 288(1):67-74.
57. Mutlu U, Cremers LG, de Groot M, Hofman A, Niessen WJ, van der Lugt A et al. Retinal microvasculature and white matter microstructure: The Rotterdam Study. Neurology. 2016; 87(10):1003-10.
58. Baker ML, Marino Larsen EK, Kuller LH, Klein R, Klein BE, Siscovick DS et al. Retinal microvascular signs, cognitive function, and dementia in older persons: the Cardiovascular Health Study. Stroke. 2007; 38(7):2041-7.
59. Edwards MS, Wilson DB, Craven TE, Stafford J, Fried LF, Wong TY et al. Associations between retinal microvascular abnormalities and declining renal function in the elderly population: the Cardiovascular Health Study. American Journal of Kidney Diseases: the Official Journal of the National Kidney Foundation. 2005; 46(2):214-24.
60. Wong TY, Coresh J, Klein R, Muntner P, Couper DJ, Sharrett AR et al. Retinal microvascular abnormalities and renal dysfunction: the atherosclerosis risk in communities study. Journal of the American Society of Nephrology: JASN. 2004; 15(9):2469-76.
61. Klein R, Klein BE, Moss SE, Wong TY. Retinal vessel caliber and microvascular and macrovascular disease in type 2 diabetes: XXI: the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Ophthalmology. 2007; 114(10):1884-92.
62. Daien V, Granados L, Kawasaki R, Villain M, Ribstein J, Du Cailar G et al. Retinal vascular caliber associated with cardiac and renal target organ damage in never-treated hypertensive patients. Microcirculation. 2017; 24(4).
63. Wong TY, Duncan BB, Golden SH, Klein R, Couper DJ, Klein BE et al. Associations between the metabolic syndrome and retinal microvascular signs: the Atherosclerosis Risk In Communities study. Investigative Ophthalmology & Visual Science. 2004; 45(9):2949-54.
64. Grunwald JE, Riva CE, Baine J, Brucker AJ. Total retinal volumetric blood flow rate in diabetic patients with poor glycemic control. Investigative Ophthalmology & Visual Science. 1992; 33(2):356-63.
65. Saldivar E, Cabrales P, Tsai AG, Intaglietta M. Microcirculatory changes during chronic adaptation to hypoxia. American Journal of Physiology Heart and Circulatory Physiology. 2003; 285(5):H2064-71.
66. Feke GT. Cardiovascular disease, its risk factors and treatment, and age-related macular degeneration: women's health initiative sight exam ancillary study. Am J Ophthalmol. 2007; 144(3):482-3; author reply 3.
67. Klein R, Klein BE, Tomany SC, Wong TY. The relation of retinal microvascular characteristics to age-related eye disease: the Beaver Dam eye study. Am J Ophthalmol. 2004; 137(3):435-44.
68. Jeganathan VS, Kawasaki R, Wang JJ, Aung T, Mitchell P, Saw SM et al. Retinal vascular caliber and age-related macular degeneration: the Singapore Malay Eye Study. Am J Ophthalmol. 2008; 146(6):954-9 e1.
69. Yang K, Zhan SY, Liang YB, Duan X, Wang F, Wong TY et al. Association of dilated retinal arteriolar caliber with early age-related macular degeneration: the Handan Eye Study. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2012; 250(5):741-9.
70. Gupta N, Weinreb RN. New definitions of glaucoma. Current Opinion in Ophthalmology. 1997; 8(2):38-41.
71. Flammer J, Konieczka K, Flammer AJ. The primary vascular dysregulation syndrome: implications for eye diseases. The EPMA Journal. 2013; 4(1):14.
72. De Leon JM, Cheung CY, Wong TY, Li X, Hamzah H, Aung T et al. Retinal vascular caliber between eyes with asymmetric glaucoma. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2015; 253(4):583-9.
73. Mitchell P, Leung H, Wang JJ, Rochtchina E, Lee AJ, Wong TY et al. Retinal vessel diameter and open-angle glaucoma: the Blue Mountains Eye Study. Ophthalmology. 2005; 112(2):245-50.
Romanian Journal of Ophthalmology 2017; 61(3): 171-180
180 Romanian Society of Ophthalmology
© 2017
74. Amerasinghe N, Aung T, Cheung N, Fong CW, Wang JJ, Mitchell P et al. Evidence of retinal vascular narrowing in glaucomatous eyes in an Asian population. Investigative Ophthalmology & Visual Science. 2008; 49(12):5397-402.
75. Wang S, Xu L, Wang Y, Jonas JB. Retinal vessel diameter in normal and glaucomatous eyes: the Beijing eye study. Clinical & Experimental Ophthalmology. 2007; 35(9):800-7.
76. Gao J, Liang Y, Wang F, Shen R, Wong T, Peng Y et al. Retinal vessels change in primary angle-closure glaucoma: the Handan Eye Study. Scientific Reports. 2015; 5:9585.
77. Hall JK, Andrews AP, Walker R, Piltz-Seymour JR. Association of retinal vessel caliber and visual field defects in glaucoma. Am J Ophthalmol. 2001; 132(6):855-9.
78. Youm DJ, Ha MM, Chang Y, Song SJ. Retinal vessel caliber and risk factors for branch retinal vein occlusion. Current Eye Research. 2012; 37(4):334-8.
Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:181-187
GENERAL ARTICLE
181 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.33
Investigating the perception of Romanian adults on ophthalmology services from an experiential
marketing perspective
Gheorghe Consuela-Mădălina, Gheorghe Iuliana-Raluca, Purcărea Victor Lorin Department of Marketing and Medical Technology, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania Correspondence to: Consuela-Mădălina Gheorghe, PhD student, Department of Marketing and Medical Technology, “Carol Davila” University of Medicine and Pharmacy, Bucharest, 8 Eroii Sanitari Blvd., Code 050474, District 5, Bucharest, Romania, Mobile phone: +40729 935 485, E-mail: [email protected] Accepted: September 5th, 2017
Abstract Nowadays, we live in a world in which we are daily bombed by hundreds of advertisements. Specialists have to discover other channels or embed attractive elements in the advertisements’ messages to cut through the clutter and catch the consumers’ attention. The evolution of the concept of service has changed from the commercial status to determining a lifestyle. Buying a service has led to a change in the consumer behavior. Consumers want to buy services that dazzle their senses, touch their hearts, and stimulate their minds, not as before, excellent or satisfying. Ophthalmology is the medical specialty that is the most oriented toward outpatient care, as hospitalization is required only in a small percentage of cases. The objective of this case study was to investigate the perception of Romanian adult consumers on ophthalmology services from an experiential marketing perspective, by using the Focus Group method. Ophthalmology requires a wide range of skills due to the diversity of consumers who demand specialized consultations. Experiential marketing is a valuable strategy that ophthalmologic organizations may use to target specific consumers. The purpose of this case study was to identify the perceptions of Romanian adults on experiential marketing campaigns and determine the degree to which these campaigns influenced their decisions of buying an ophthalmologic service. Using a snowball sampling technique we have sent a filter questionnaire to 40 people on the internet. The filter questionnaire consisted of questions about wearing eyeglasses, the period of wearing them, the last ophthalmologic consultation, the type of ophthalmologic clinic they were going to, age and education. The respondents revealed there is almost no visibility on promoting services even if there is an upsurge of organizations offering this type of health service in the Romanian ophthalmology sector. Keywords: perception, ophthalmology services, experiential marketing, snowball sampling technique, ophthalmology sector

Romanian Journal of Ophthalmology 2017; 61(3): 181-187
182 Romanian Society of Ophthalmology
© 2017
1.Introduction
Nowadays, we live in a world in which we are daily bombed by hundreds of advertisements. Moreover, as consumers found new methods of avoiding advertisements, the impact of sending the ad’s message on traditional channels has diminished. Consequently, specialists have to discover other channels or embed attractive elements in the advertisements’ messages to cut through the clutter and catch the consumers’ attention.
Further, the evolution of the concept of service has changed from the commercial status to determining a lifestyle [1]. More exactly, buying a service has led to a change in the consumer behavior, as they became more educated, experienced, sophisticated, demanding and discerning in their purchasing process, which developed into greater requirements for the marketing experts. At the same time, consumers have started to consider the purchasing process a relationship established between them and the service itself [2]. In addition, consumers want to buy services that dazzle their senses, touch their hearts and stimulate their minds, not as before, excellent or satisfying [3]. This is where, more and more often, the interest of marketing experts to provide service experiences with a unique sensation has risen, rather than provide a list of features and benefits that remain engrained in the consumers’ minds for a long period of time, through experiential marketing.
Health care is a service that most people need but do not want, in other words, it is an unwanted service. In addition, health care services are highly troublesome but critically important for a population’s wellbeing [4]. From a marketing perspective, it is the most customized service that the consumers can buy; however, its variability in solving health problems stands as proof that there is an undeniable difference between health care services and the other services. For instance, Berry and Beaudapudi (2007) [4] pinpointed that consumers are sick, relinquish privacy and are reluctant in disclosing their most intimate thoughts, perceiving a high risk in the service delivery, as it also happens in ophthalmology.
Ophthalmology is the medical specialty that is the most oriented toward outpatient care, as hospitalization is required only in a small percentage of cases, when surgery is conducted. Further, many ophthalmologic patients have no disease, but require preventive check-ups and eyeglasses for benign refractive conditions, being self-referred or referred non-specifically by other physicians for a specialized consultation. Ophthalmologic practice is like primary care, with a large throughput of patients, many of whom are normal [5].
Since ophthalmology services are credence oriented and consumers are self-referred, marketing experts use an experience to attract a target audience with the intention of triggering an emotion or action at a cognitive level [4]. The experiential approach is the new currency of the modern marketing landscape, because experiences are life and people talk about life experiences day-by-day [6].
The objective of this case study was to investigate the perception of Romanian adult consumers on ophthalmology services from an experiential marketing perspective, by using the Focus Group method.
2.Ophthalmology specialty from a marketing perspective
Ophthalmology requires a wide range of skills due to the diversity of consumers who demand specialized consultations. Thus, patients who need an ophthalmic consultation range from pediatric to geriatric segments. Patient care usually takes place on an outpatient basis on a long period of time, allowing the development of a true report. Moreover, surgeries are usually performed on a day care basis and under local anesthesia.
According to Thomas (2010), many ophthalmologic consumers are different from other service consumers in some aspects. The main differences between the ophthalmologic consumers are highlighted in Table 1.

Romanian Journal of Ophthalmology 2017; 61(3): 181-187
183
Romanian Society of Ophthalmology © 2017
Table 1. Differences between ophthalmologic and other services consumers Ophthalmologic services Other services Seldom are the last decision makers Usually are the ultimate decision makers Often make decisions subjectively Usually make decisions objectively Seldom know the price Always know the price Seldom make decisions based on price Usually make decisions based on price Usually make nondiscretionary purchases Usually make discretionary purchases Usually require a professional referral Rarely require a professional referral Have limited knowledge of service attributes Have significant knowledge of service attributes Have limited ability to judge the quality of the service Are usually able to judge the quality of the service Have limited ability to evaluate the outcome Are usually able to evaluate the outcome Are not susceptible to standard marketing techniques Are susceptible to standard marketing techniques
Source: adapted from Thomas RK. Marketing Health Care Services. 2010, Oxford, Oxford University Press, 157. 3.Experiential marketing in ophthalmologic services
Experiential marketing is a valuable strategy that ophthalmologic organizations may use to target specific consumers, which delivers a compelling service experience that is appealing to the wants and needs of its consumers. Moreover, experiential marketing connects with consumers through the participation and tangible nature of a personally relevant and memorable experience [7].
The concept of experiential marketing was first introduced in 1999 by Bernd Schmitt, who defined it as the consumer’s process of recognition or intention to purchase a service only after they have had an experience with the organization, through which the value perceived by the consumer has increased. Nevertheless, experiential marketing does not refer to the quality, the benefits, and the functions of the service, but is rather emotionally oriented as it conveys to the consumer and the senses it activates.
The core values of emotional marketing are the following [8]: 1. Communicate by using the sense of touch
and emotions more while helping consumers visualize the way the service will bring a benefit to their lives.
2. Demonstrate the use and benefit by employing photography and other illustration techniques, showing the application, use and service benefits in an “aspirational” manner.
3. Infuse emotional selling messages, as the consumers’ buying decisions are more emotionally oriented than logic.
By relying on the strategic experiential model, Schmitt divided the types of marketing into 5 categories: Sense Experience, Feel Experience, Think Experience, Act Experience, and Relate Experience [9]. - Sense Experience refers to the experience
consumers gain while using their senses such as sight, hear, touch, smell and taste. As such, through sensory experience, consumers will be able to develop experience logic and, subsequently, using the experience logic, they will form attitudes to differentiate services [10]. In fact, Sense Experience appeals to the five basic human senses, as it follows [11]: a. Visual Experience. Sight is the most
commonly used sense in marketing because it is the most stimulated by the environment. Due to this fact, the ophthalmologic organizations use many colors and forms to attract consumers, because they are memorized easier in the audience’ mind. Moreover, the colors of the surroundings, lights, materials, or layout are also important criteria to take into consideration in selling points.
b. Auditory experience uses music or sounds to promote a message in order for the consumer to remember it easier.
c. Tactile experience. d. Olfactory experience is connected to the
emotions and ophthalmologic organizations use natural or artificial smells.
- Feel Experience is referred to the consumer’s inner emotion, mood and feeling, which is derived from the consumption experience [12]. Feel experience can only

Romanian Journal of Ophthalmology 2017; 61(3): 181-187
184 Romanian Society of Ophthalmology
© 2017
work if there is a deep understanding of which stimuli trigger certain emotions.
- Think Experience refers to the stimulation of the consumer’s creativity on a cognitive level so that they engage in solving real problems. Moreover, think experience uses surprise, intrigue, and provocation to appeal to problem solving capabilities.
- Act Experience involves the consumer’s activities related to changing a certain behavioral habit or lifestyle. These experiences sometimes occur in a private environment, but are most often the result of interactions between several persons. According to Schmitt, act experience enables consumers to develop experiences that deal with the consumer’s physical body, behavior and lifestyle and the experience gained from
the social interaction with other people. Through the experience action, consumers develop a sense of sensation, influence, and relationship with the services offered.
- Relate Experience refers to an experience that allows the consumer to establish ties with various entities and communities through the process of buying and consuming. Relate experience allows consumers to build their connection with the social communities and social entities through the process of purchasing and service consumption [13].
The ultimate strategy of experiential marketing is to build holistic experiences with intense, broad, and interconnected experiences by using advertising.
4. Research objectives
The purpose of this case study was to identify the perceptions of Romanian adults on experiential marketing campaigns and determine the degree to which these campaigns influenced their decisions of buying an ophthalmologic service. The objectives of the research were the following:
1. Determine the respondents’ degree of knowledge on the concept of experiential marketing.
2. Determine the respondents’ degree of knowledge of the concept of experiential marketing applied in ophthalmologic services.
3. Identify the respondents’ perception of experiential marketing in ophthalmology.
Experiential marketing advertising
Sense
Feel
Think Act
Relate
Fig. 1 Experiential marketing advertising and the 5 senses

Romanian Journal of Ophthalmology 2017; 61(3): 181-187
185
Romanian Society of Ophthalmology © 2017
4. Examine the factors that made experiential marketing efficient in ophthalmologic services.
5. Investigate whether the respondents would go to a consultation in an ophthalmologic clinic advertised with the help of experiential marketing messages.
5. Research methodology
The focus group method was used in order to assess the established objectives. The focus group is a method specifically used in exploratory research. Moreover, focus groups are small groups of people brought together with the aim of gaining information on a relevant topic, such as generating ideas, learning the respondents’ vocabulary when relating to a certain type of service, or gaining some insight into basic needs and attitudes [14]. On one hand, the main advantages of focus groups are that they generate fresh ideas, allow moderators to observe their respondents, may be directed towards understanding a wide variety of issues and allow a fairly easy access to special respondent groups, and, on the other hand, the major disadvantages of focus groups are that they are not representative samples, it is difficult to interpret the results of focus groups, as the moderator’s report is based on a subjective evaluation of what was said during the focus group, and the cost per participant is high [14].
We decided that 25 people would give us enough insight to assess the objectives. Using a snowball sampling technique we have sent a filter questionnaire to 40 people on the internet. The filter questionnaire consisted of questions about wearing eyeglasses, the period of wearing them, the last ophthalmologic consultation, the type of ophthalmologic clinic they were going to, age and education. We selected only the persons who wore eyeglasses for a period longer than 5 years, who went to a consultation not more than 2 months before the research took place in a private clinic, were aged 25 to 35 years and graduated from university. The selected sample size consisted of 20 participants. Consequently, the participants received 2 invitations with dates, hours and the places where the focus groups took place. The location selected was in a room specially designed for these kinds of
research methods, in a marketing research institution in Bucharest, which was rented for a couple of hours. The room also required a projector, because the experiential marketing technique consisted of an advertisement of an ophthalmologic clinic, which needed visualization on a screen. The advertisement can be found on the internet, at https://www.youtube.com/watch?v=bE4eiuoMmAE. It embedded elements that covered all 5 experiences described as being part of the experiential marketing, with a focus on the feel, think and act experiences.
The focus groups took place during 2 consecutive days and lasted not more than 2 hours. Moreover, the answers were recorded with the help of a mobile phone. The first group consisted of 10 participants and, the second group, of only seven, because one respondent quit in the last minute, and others did not show up even if they confirmed their participation. Hence, 17 persons were included in the focus groups. A questionnaire was administered at the end of every focus group, in case there were respondents who did not have the chance to express themselves or were not very talkative. The recorded conversations were transcribed in a text format and a content analysis was conducted.
6. Findings
Both focus groups took place in a relaxed atmosphere and the 17 participants were friendly and brief on the provided answers, eager to share their knowledge and experiences. The demographic profile of the respondents revealed 4 males and 13 females, the mean period of wearing eyeglasses was of 8 years and the mean period since the respondents went to their last ophthalmologic consultation was of about 5 months.
After watching the advertisement, the moderator presented the main objective of the research to the respondents, assured them that their answers will be confidential, that they were going to be recorded and if they felt embarrassed while answering a question they could avoid it.
The first discussion subject approached was about the degree of knowledge of the respondents on experiential marketing. 4
Romanian Journal of Ophthalmology 2017; 61(3): 181-187
186 Romanian Society of Ophthalmology
© 2017
participants answered that it was related to experience and others (10 persons) used words such as testing, trying and selling a service with the sense of experience. 3 respondents did not know what experiential marketing meant. Further, the moderator explained what experiential marketing was, as acknowledged in the scientific literature.
The second subject approached was whether the participants had any knowledge about the application of experiential marketing in ophthalmologic services. All respondents replied they have not seen any advertisement on ophthalmologic services on Romanian TV or over the internet. However, 2 participants have seen an ad for ophthalmologic services during a dedicated event but they did not use experiential marketing elements. The vast majority of respondents (15 persons) agreed on the lack of advertising in health care services, and implicitly, on ophthalmologic services.
The third subject covered the factors that would make experiential marketing efficient in ophthalmologic services. The vast majority of respondents took into consideration what the moderator explained about the significance of the concept of experiential marketing and pointed out the following particularities of experiential marketing advertising for ophthalmologic services: - All respondents agreed that the
advertisement should be visually attractive and tell a story.
- 13 respondents emphasized the importance of emotions in advertising, gaining more attention if used properly.
- All respondents mentioned the word “empathy” in relation to the advertisement watched. What should be added is that empathy presupposes the relate experience, as part of experiential marketing. Moreover, consumers have to be engaged in the process decisions regarding their health and so, organizations have to empower them and offer a benefit to their experience with the provider.
The fourth subject discussed focused on the respondents’ intention to go to a consultation of an ophthalmologic organization advertised and which used experiential marketing elements. The vast majority of respondents (13 persons) answered that they would go to a consultation if
they could watch the advertisement on TV first. However, a few participants were rather skeptical on trusting the organization when making health care decisions and answered they would rather prefer a recommendation from family and peers, or even the general practitioner instead.
7. Discussion
It is acknowledged that marketers use experience to influence a target audience. Regardless of the field, there is always the intention to use an experience to distribute a message or content which trigger an emotion or action (a behavioral response) [4].
Moreover, when developing a marketing plan, especially an experiential marketing plan, it is important for the organizations to focus on several factors such as the following [7]: - Choosing an appropriate location or venue
where the ad would be distributed; - Targeting the appropriate audience
(Consumer emotional attitudes vary depending on age, gender, culture, socioeconomic status);
- Creating a fun and memorable experience by using multiple media platforms, visual and print ads;
- Offering consumers what they want to see and hear.
Health care is still a sensitive subject and, when advertising their services, most medical organizations concentrate on a description of indoor components of their building and equipment. Thus, most consumers would not consider this kind of advertisement interesting even if it uses some experiential marketing strategies. As our research findings suggested, the advertising message should enclose emotional elements and add value to the consumers’ experiences. If consumers were influenced by the emotional marketing advertisement they would recommend it to other peers, would build on loyalty and stimulate a purchasing behavior.
The respondents revealed there is almost no visibility on promoting services even if there is an upsurge of organizations offering this type of health service in the Romanian ophthalmology sector. Moreover, organizations should conceive their advertisements around a story that the consumer could identify with.

Romanian Journal of Ophthalmology 2017; 61(3): 181-187
187
Romanian Society of Ophthalmology © 2017
References
1. Owyang J. Disruptive technology—the new reality will be augmented. Consum Related Manag Mag. 2010; 32(2):32-33.
2. Caru A, Cova B. Consuming Experience, 2007, New York, Taylor and Francis Group.
3. Pine J, Gilmore JH. The experience economy: work is theatre and every business a stage. 1999, Boston, Harvard Business School Press.
4. Smith K, Hanover D. Experiential Marketing. 2016, United States, Wiley.
5. Safir A. Ophthalmology’s characteristics as a specialty, from an information science viewpoint. Ophthalmology. 1981 Sep; 88(9):41A-45A.
6. Smilansky S. Experiential marketing. A practical guide to interactive brand experiences. 2009, London, Kogan Publishing House.
7. Adweek. Entrepreneur magazine, Emerald insight, 2009, Proceedings of the 41st Hawaii International Conference on System Sciences.
8. Nigam A. Experiential Marketing: Changing Paradigm for Marketers. International Journal of Computer Science and Management Studies. 2011; 11(2),200-204.
9. Schmitt B. Experiential Marketing: How to get customers to sense, feel, think, act, relate. 1999, New York, The Free Press.
10. Vargo SL, Lusch RF. Evaluating to a new dominant logic for marketing. Journal of Marketing. 2004; 68(1),1-17.
11. Canneterre J, Mou N, Moul S, Bernadac M, Ghor A. International Conference of Scientific Paper, AFASES. In: How Do Companies Innovate and Attract Consumers through Experiential Marketing?, Brasov, 2012.
12. Yang ZY, He LY. Goal, customer experience and purchase intention in a retail context in China: An empirical study. African Journal of Business Management. 2011; 5(16),6738-6746.
13. Chou HJ. The effect of experiential and relationship marketing on customer value: A case study of international American casual dining chains in Taiwan. Social Behavior and Personality. 2009; 37(7),998.
14. Burns AC, Bush RF. Marketing Research, 5th Ed., 2010, New Jersey, Pearson Prentice Hall, Upper Saddle River.

Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:188-191
GENERAL ARTICLE
188 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.34
Transnasal endoscopic assisted dacryocystorhinostomy
Hainăroșie Răzvan* **, Ioniță Irina* **, Pietroșanu Cătălina* **, Pițuru Silviu*, Hainăroșie Mura* **, Zainea Viorel* **
*”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania **“Prof. Dr. Dorin Hociotă” Institute of Phonoaudiology and Functional ENT surgery, Bucharest, Romania Correspondence to: Silviu Pițuru, ”Carol Davila” University of Medicine and Pharmacy, Bucharest, 8 Eroii Sanitari Blvd., Code 050474, District 5, Bucharest, Romania, Mobile phone: +40722 488 675, E-mail: [email protected] Accepted: September 6th, 2017
Abstract Transnasal endoscopic dacryocystorhinostomy is a good alternative for external DCR. It is considered a safe and efficient technique with successful results, comparable or even better than the external technique. Advanced knowledge of the endoscopic anatomy and the lacrimal system is necessary to perform the procedure safely, and to obtain good surgical outcomes. The aim of the paper is to analyze the changes of the endoscopic technique and to improve it. The transnasal endoscopic dacryocystorhinostomy surgical technique is described in a “step by step” manner. Also the surgical technologies that can be used for this intervention are presented, focusing on the cold instruments. Keywords: endoscopic, transnasal, dacryocystorhinostomy
Introduction
In the last 20 years, an avalanche of developments, mainly in the endoscopic field, has taken place in ENT. Endoscopic sinus surgery developments were outstanding. Optical technologies and video chip advancements offered a perfect view of the endoscopic surgical field. Surgeons can perform more complex operations, safely and minimally invasive.
Dacryocystorhinostomy (DCR) is the procedure that aims to create a direct drainage of the tears, opening the lacrimal sac directly into the nasal cavity in cases of nasolacrimal duct (NLD) blockage.
The procedure is over 100 years old, and it was described in the first century by Celsus. He created a new passage for the tears using a
cautery at the level of the lacrimal bone. In the second century, Galen described the same procedure.
In the eighteenth century, Woolhouse imagined a technique to open the lacrimal sac into the maxillary sinus. That method is somehow similar to the modern DCR. He removed the lacrimal sac and placed a stent of gold or silver. Some of the authors reported success in almost 70-85% of the cases.
The first modern description of an external DCR was published in 1904, while the modified version of Dupuy-Dutemps and Bourguet remain the gold standard for the treatment of NLD obstruction [1].
In 1893, Caldwell described for the first time the endonasal approach of an endoscopic DCR [2]. In 1989, Meiring and Mc Donogh
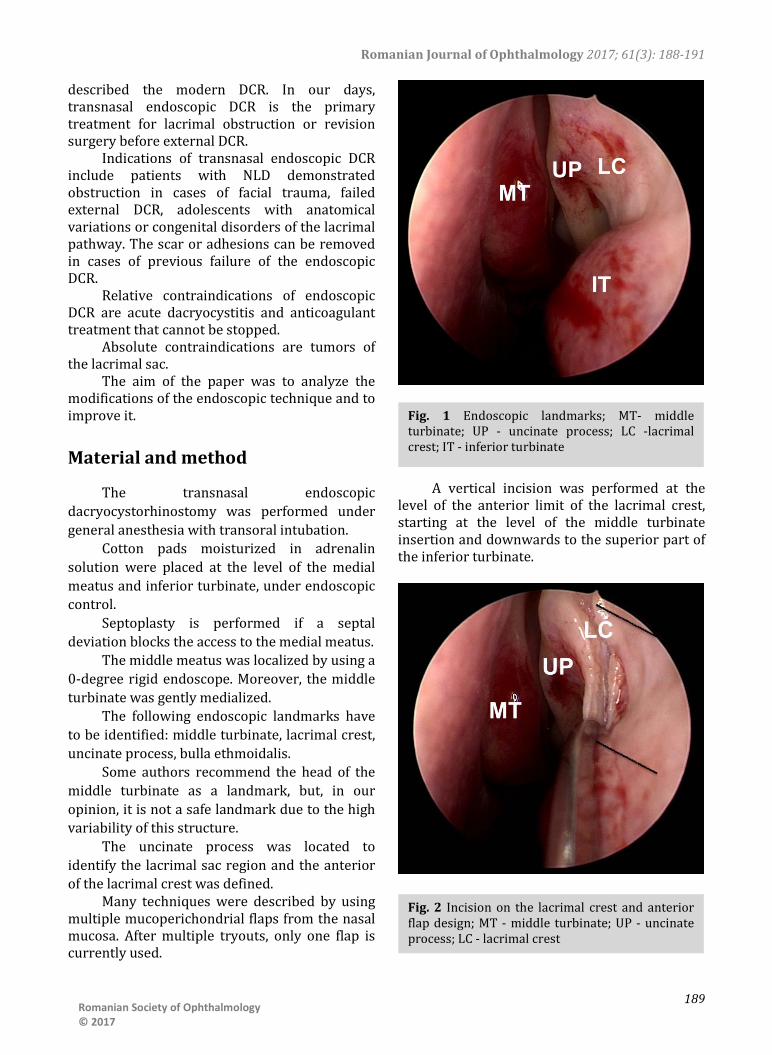
Romanian Journal of Ophthalmology 2017; 61(3): 188-191
189
Romanian Society of Ophthalmology © 2017
described the modern DCR. In our days, transnasal endoscopic DCR is the primary treatment for lacrimal obstruction or revision surgery before external DCR.
Indications of transnasal endoscopic DCR include patients with NLD demonstrated obstruction in cases of facial trauma, failed external DCR, adolescents with anatomical variations or congenital disorders of the lacrimal pathway. The scar or adhesions can be removed in cases of previous failure of the endoscopic DCR.
Relative contraindications of endoscopic DCR are acute dacryocystitis and anticoagulant treatment that cannot be stopped.
Absolute contraindications are tumors of the lacrimal sac.
The aim of the paper was to analyze the modifications of the endoscopic technique and to improve it.
Material and method
The transnasal endoscopic dacryocystorhinostomy was performed under general anesthesia with transoral intubation.
Cotton pads moisturized in adrenalin solution were placed at the level of the medial meatus and inferior turbinate, under endoscopic control.
Septoplasty is performed if a septal deviation blocks the access to the medial meatus.
The middle meatus was localized by using a 0-degree rigid endoscope. Moreover, the middle turbinate was gently medialized.
The following endoscopic landmarks have to be identified: middle turbinate, lacrimal crest, uncinate process, bulla ethmoidalis.
Some authors recommend the head of the middle turbinate as a landmark, but, in our opinion, it is not a safe landmark due to the high variability of this structure.
The uncinate process was located to identify the lacrimal sac region and the anterior of the lacrimal crest was defined.
Many techniques were described by using multiple mucoperichondrial flaps from the nasal mucosa. After multiple tryouts, only one flap is currently used.
A vertical incision was performed at the level of the anterior limit of the lacrimal crest, starting at the level of the middle turbinate insertion and downwards to the superior part of the inferior turbinate.
Fig. 1 Endoscopic landmarks; MT- middle turbinate; UP - uncinate process; LC -lacrimal crest; IT - inferior turbinate
Fig. 2 Incision on the lacrimal crest and anterior flap design; MT - middle turbinate; UP - uncinate process; LC - lacrimal crest

Romanian Journal of Ophthalmology 2017; 61(3): 188-191
190 Romanian Society of Ophthalmology
© 2017
Two parallel horizontal incisions were made at the extremities of the vertical incisions from the anterior up to the posterior part of the lacrimal crest.
The mucoperiosteal flap was elevated anteriorly and the lacrimal bone was exposed.
The bone removed was represented by the maxillary branch and lacrimal bone. In cases of agger nasi rich pneumatization, some anterior ethmoidal cells can be removed as well.
A high-speed drill was used to remove the bone. Some authors recommend the use of piezotome, a device that removes only bone and does not harm the soft tissue, with minimal thermal effect.
We removed as much bone as we could vertically.
A Bowman cannula was inserted into the inferior canaliculus to identify the medial wall of the lacrimal sac.
The medial wall of the lacrimal sac was incised with the endoscopic knife in an “H” shape.
The two vertical flaps from the lacrimal sac were exposed until the posterior flap came in close contact with the nasal mucosa located at the posterior limit of the lacrimal crest.
The nasal mucosal anterior flap was shortened with the shaver until it reached the anterior flap from the lacrimal sac.
A piece of Gelaspone was placed to stabilize the flaps.
No stenting was performed. No nasal packing was necessary. Postoperative care was done by using
saline solution and oil drops to clean the nose. The first visit was at 14 days, then at one
month and two months.
Results and discussions
Our success rate in 37 patients was 91.89% after the first surgery and 97.3% after the second surgery. No external DCR was performed.
First, it was believed that the external DCR would obtain better results than the endoscopic DCR, but recent studies showed that the results are comparable, maybe better in endoscopic DCR [3].
The advantages in endoscopic DCR include the fact that it does not disturb the lacrimal pump system [4]. Also, all surrounding structures were visualized.
Fig. 3 Drilling the lacrimal bone
Fig. 4 Bowman cannula insertion will better identify the projection of the lacrimal sac. An incision can be performed safely
Fig. 5 Wide opening of the lacrimal sac, no stenting required

Romanian Journal of Ophthalmology 2017; 61(3): 188-191
191
Romanian Society of Ophthalmology © 2017
Better esthetic results are obtained without a skin incision.
Less operative bleeding was reported together with no scar to the external canthus area and orbicularis muscle.
A disadvantage of the endoscopic DCRS is that a lacrimal neoplasia cannot be excluded; if a suspicion is raised, a biopsy must be performed [5].
LASER or radiofrequency assisted DCR was described, but we do not recommend that technique because of the thermal damage produced to the tissue and the additional cost of the procedure. We recommend using “cold” instruments.
Taking into account that endoscopic and external DCR have comparable results, from an ethical point of view, the surgeon has to present both options (with advantages, disadvantages, risks, benefits, possible complications) to the patient. The esthetic result of the procedure must be addressed, and the patient can choose the most convenient procedure. The informed consent is obtained before surgery.
Also, the surgeon has to be aware of the limits imposed by his/ her medical specialty, and always have in mind an improvement of the patients’ health as a result of the treatment.
Conclusion
Transnasal endoscopic dacryocystorhinostomy is a safe and efficient technique with a success result comparable or even better than external DCR.
Advanced knowledge of endoscopic anatomy and lacrimal system is necessary to perform the procedure safely. In case of failure, the procedures can be repeated, or external DCR can be conducted.
In our opinion, “cold” instruments are the best choice to perform the surgery.
Further studies must be made concerning the use of piezoelectric surgery in lacrimal bone removal. That technology offers a “cold” removal of the bone without damaging the soft tissue, reducing scar formation, but the operation will take longer since the speed is low with that type of technology.
Acknowledgement All the authors have contributed equally to
this paper.
References 1. Dubey SP, Munjal VR. Endoscopic DCR: How To
Improve The Results. Indian Journal of Otolaryngology and Head & Neck Surgery. 2014; 66(2):178-181. doi:10.1007/s12070-014-0702-x.
2. Muscatello L, Giudice M, Spriano G, Tondini L. Endoscopic dacryocystorhinostomy: personal experience. Acta Otorhinolaryngologica Italica. 2005; 25(4):209-213.
3. Tsirbas A, Wormald PJ. Endonasal dacryocystorhinostomy with mucosal flaps. Am J Ophthalmol. 2003 Jan; 135(1):76-83.
4. Marcet MM, Kuk AK, Phelps PO. Evidence-based review of surgical practices in endoscopic endonasal dacryocystorhinostomy for primary acquired nasolacrimal duct obstruction and other new indications. Curr Opin Ophthalmol. 2014 Sep; 25(5):443-8.
5. Jawaheer L, MacEwen CJ, Anijeet D. Endonasal versus external dacryocystorhinostomy for nasolacrimal duct obstruction. Cochrane Database Syst Rev. 2017 Feb 24; 2:CD007097.
https://www.ncbi.nlm.nih.gov/pubmed/?term=Wormald%20PJ%5BAuthor%5D&cauthor=true&cauthor_uid=12504701
https://www.ncbi.nlm.nih.gov/pubmed/?term=Jawaheer%20L%5BAuthor%5D&cauthor=true&cauthor_uid=28231605
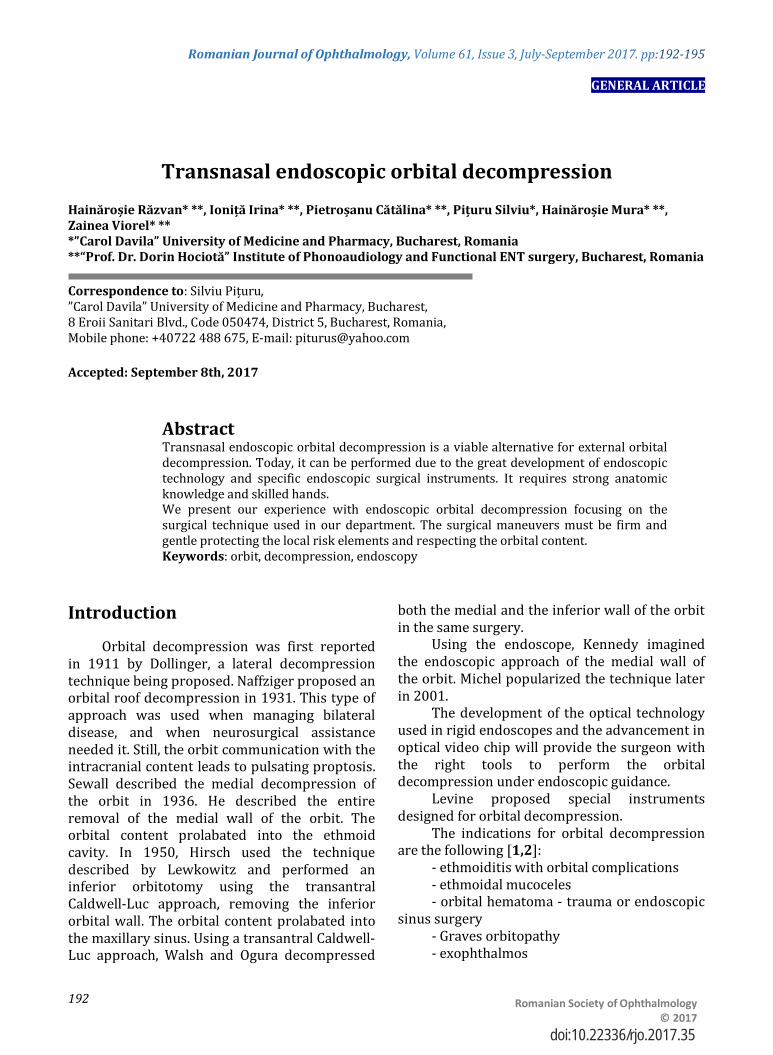
Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:192-195
GENERAL ARTICLE
192 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.35
Transnasal endoscopic orbital decompression Hainăroșie Răzvan* **, Ioniță Irina* **, Pietroșanu Cătălina* **, Pițuru Silviu*, Hainăroșie Mura* **, Zainea Viorel* **
*”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania **“Prof. Dr. Dorin Hociotă” Institute of Phonoaudiology and Functional ENT surgery, Bucharest, Romania Correspondence to: Silviu Pițuru, ”Carol Davila” University of Medicine and Pharmacy, Bucharest, 8 Eroii Sanitari Blvd., Code 050474, District 5, Bucharest, Romania, Mobile phone: +40722 488 675, E-mail: [email protected] Accepted: September 8th, 2017
Abstract Transnasal endoscopic orbital decompression is a viable alternative for external orbital decompression. Today, it can be performed due to the great development of endoscopic technology and specific endoscopic surgical instruments. It requires strong anatomic knowledge and skilled hands. We present our experience with endoscopic orbital decompression focusing on the surgical technique used in our department. The surgical maneuvers must be firm and gentle protecting the local risk elements and respecting the orbital content. Keywords: orbit, decompression, endoscopy
Introduction
Orbital decompression was first reported in 1911 by Dollinger, a lateral decompression technique being proposed. Naffziger proposed an orbital roof decompression in 1931. This type of approach was used when managing bilateral disease, and when neurosurgical assistance needed it. Still, the orbit communication with the intracranial content leads to pulsating proptosis. Sewall described the medial decompression of the orbit in 1936. He described the entire removal of the medial wall of the orbit. The orbital content prolabated into the ethmoid cavity. In 1950, Hirsch used the technique described by Lewkowitz and performed an inferior orbitotomy using the transantral Caldwell-Luc approach, removing the inferior orbital wall. The orbital content prolabated into the maxillary sinus. Using a transantral Caldwell-Luc approach, Walsh and Ogura decompressed
both the medial and the inferior wall of the orbit in the same surgery.
Using the endoscope, Kennedy imagined the endoscopic approach of the medial wall of the orbit. Michel popularized the technique later in 2001.
The development of the optical technology used in rigid endoscopes and the advancement in optical video chip will provide the surgeon with the right tools to perform the orbital decompression under endoscopic guidance.
Levine proposed special instruments designed for orbital decompression.
The indications for orbital decompression are the following [1,2]:
- ethmoiditis with orbital complications - ethmoidal mucoceles - orbital hematoma - trauma or endoscopic
sinus surgery - Graves orbitopathy - exophthalmos

Romanian Journal of Ophthalmology 2017; 61(3): 192-195
193
Romanian Society of Ophthalmology © 2017
- exposure keratopathy - diplopia - optic neuropathy - tumors located medial to the optic nerve - sinonasal or skull base tumors with
orbital compartment extension From an ethical point of view, there are two
ways to obtain the informed consent depending on the patients’ general health status. When dealing with a scheduled surgery, the patient needs to be thoroughly presented the surgical plan with its advantages, disadvantages, risks, benefits, possible complications and prognostic, and afterwards the informed consent can be obtained. When facing an emergency situation, the informed consent is not a priority, the surgical and medical gestures have to be performed to save the patient’s life or prevent permanent damages. After the surgery, an emergency report will be written to justify the absence of the informed consent.
Materials and method
We analyzed the cases that underwent endoscopic orbital decompression in the IIIrd ENT and Head and Neck Surgery Department of “Prof. Dr. Dorin Hociota” Institute of Phonoaudiology and Functional ENT Surgery in the period 2007-2010. The patients who underwent purely endoscopic orbital decompression were included in the study. In one case, inferior wall orbital decompression was associated to the medial decompression of the orbit. Table 1. Endoscopic orbital decompression
Orbital decompression Number of patients Ethmoiditis with orbital complications
19
Ethmoidal mucoceles 14 Orbital hematoma - trauma/ endoscopic sinus surgery
5/ 12
Optic neuropathy 4 Graves orbitopathy 3 Tumors located medial to the optic nerve
2
Sinonasal tumors with orbital compartment extension
27
The technique used was performed under general anesthesia with orotracheal intubation. Pieces of cotton moisturized in adrenaline solution were mounted along the inferior turbinate and into the medial meatus.
If a major septal deviation was encountered, septoplasty was performed to achieve a good exposure of the ethmoidal bulla.
After 5 minutes, we gently medialized the medial turbinate. The uncinate process and the bulla ethmoidalis were exposed. Inferior uncinectomy was performed. The surgeon had to assess the insertion of the uncinate process preoperatively to avoid harming the orbital contents when uncinectomy was performed.
Medial meatotomy was performed; if needed meatotomy orifice could be enlarged, and inferior wall decompression could be conducted.
Anterior ethmoidectomy was done by removing the ethmoidal cells until the lamina papyracea was reached. Lamina papyracea represents the insertion of the medial turbinate on the lateral wall of the nasal cavity. It separates the anterior ethmoid from the posterior one.
Posterior ethmoidectomy was continued until the skull base was reached. The procedure can be completed when sphenoidotomy is
Fig. 1 Inspecting the middle meatus. UP – uncinate process; BE – bulla ethmoidalis; MT – middle turbinate

Romanian Journal of Ophthalmology 2017; 61(3): 192-195
194 Romanian Society of Ophthalmology
© 2017
needed, in addition, a total sphenoethmoidectomy was achieved.
The medial wall of the orbital cavity was exposed widely. The medial wall of the orbit was penetrated with a particular pyramidal tip instrument. The lamina papyracea was removed by using special dissectors with aspiration.
The periorbit was exposed and two or
three horizontal incision lines were performed with a blunt tip endoscopic knife. One or two sliding of fascia had to be preserved in patients without optic neuropathy to protect the medial rectus muscle to minimize postoperative diplopia.
Fig. 2 Ethmoidal cavity inspection after anteroposterior ethmoidectomy; LP – lamina papyracea; SB - skull-base
Fig. 3 Exposing the medial orbital wall
Fig. 4 Elevating the bone of the medial orbital wall; LP - lamina papyracea; PO -periorbit
Fig. 5 Incising the periorbit with OF (orbital fat) protruding into the ethmoidal cavity

Romanian Journal of Ophthalmology 2017; 61(3): 192-195
195
Romanian Society of Ophthalmology © 2017
Result and discussion
Medial orbital decompression was performed successfully. Still, in Graves orbitopathy, we considered that a 360-degree decompression is the gold standard [6,7].
The orbit is a cone-shaped compartment made up of bony walls circumferentially and the orbital septum anteriorly. The intact orbital septum can manage pressures up to 50 mmHg. The term “orbital compartment syndrome” was presented in 1990 by Kratky. Increased pressure in the intraorbital compartment may compromise the vascularisation of the optic nerve that will lead to irreversible blindness [3,4].
If the blood flow in the posterior ciliary arteries, central retinal artery, or vasa nervorum of the optic nerve is obstructed, optic neuropathy may appear due to ischemia. In orbital abscesses or orbital hematoma, the orbit must be decompressed in the first 8 hours [5].
Conclusions
Endoscopic medial orbital decompression is a safe and reliable technique. Advanced anatomic knowledge is necessary to perform the decompression safely. If needed, it can completed with inferior decompression, which can also be performed endoscopically.
The procedure must be performed by surgeons who can also perform medial canthotomy or decompress the orbit externally. The endoscopic approach offers an excellent visualization and control of the skull base area and orbital apex.
Acknowledgement
All the authors have equally contributed to this paper.
References 1. Chandler JR, Langenbrunner DJ, Stevens ER. The
pathogenesis of orbital complications in acute sinusitis. Laryngoscope. 1970; 80(9):1414-1428.
2. Pandian DG, Babu RK, Chaitra A, Anjali A, Rao VA et al. Nine years’ review on preseptal and orbital cellulitis and emergence of community-acquired methicillin-resistant Staphylococcus aureus in a tertiary hospital in India. Indian J Ophthalmol. 2011; 59(6):431-435.
3. Thiagarajan NE, Cherian T. An Orbital Cellulitis Demanding Multispecialty Management. The Internet Journal of Ophthalmology and Visual Science. 2009; 8(1).
4. Chaha K, Chinda D, Ajike SO. Management of bilateral orbital cellulitis in a 41-year-old man. Niger J Ophthalmol. 2014; 22(1):50-55.
5. Liu IT, Kao SC, Wang AG, Tsai CC, Liang CK et al. Preseptal and Orbital Cellulitis: A 10-Year Review of Hospitalized Patients. J Chin Med Assoc. 2006; 69(9):415-422.
6. Lal P, Thakar A, Tandon N. Endoscopic orbital decompression for Graves’ orbitopathy. Indian Journal of Endocrinology and Metabolism. 2013; 17(2):265-270.
7. Paridaens D, Lie A, Grootendorst RJ, van den Bosch WA. Efficacy and side effects of “swinging eyelid” orbital decompression in Graves’ orbitopathy: a proposal for standardized evaluation of diplopia. Eye. 2006; 20,154–162.

Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:196-201
GENERAL ARTICLE
196 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.36
Cataract surgery outcome in patients with non-glaucomatous pseudoexfoliation
Sastry Praveen Venkatesha, Singal Anuj Kumar Department of Ophthalmology, JSS Hospital, Mysore, India Correspondence to: Anuj Kumar Singal, MD, MS, Junior Resident, Department of Ophthalmology, JSS Hospital, Mysore, Code 570004, Karnataka, India Phone: 9212 762 478/ 7219 877 735, E-mail: [email protected] Accepted: September 9th, 2017
Abstract Aim. To study the outcome of cataract surgery in eyes with pseudoexfoliation without signs of glaucoma. Methods. This prospective study was done over nine months on patients with pseudoexfoliation undergoing small incision cataract surgery. Only patients with normal intraocular pressure (Central Corneal Thickness Corrected), normal cup disc ratio and open angles were included. Patients on anti-glaucoma medication were excluded. Patients underwent surgery performed by a single senior surgeon. Intraoperative and postoperative day (POD) 1 findings were noted. Results. The mean age of the patients was 61.60 years +/ - 10.21 years. Males were 46% (n=16). Right eye was operated upon in 60% of the cases (n=21). The mean pupil dilation was 5.1 mm +/ - 1.47 mm. The postoperative day 1 visual acuity of the patients was logMar 1.02 +/- 0.64 and the mean POD 1 intraocular pressure was noted to be 26.23 mmHg +/ - 11.40 mmHg. Five cases had a zonular dialysis intraoperatively due to weak zonules. 11 cases had high anterior chamber reaction of 2+ or more. Four cases had unavoidable sphincter tears and two cases had iridodialysis superiorly during nucleus delivery. Conclusions. Intraoperative complications should be anticipated in patients with pseudoexfoliation even without glaucomatous changes due to poor pupillary dilation and zonular weakness. First postoperative day visual acuity in pseudoexfoliation patients undergoing cataract surgery was found to be low due to severe anterior chamber inflammation causing elevated intraocular pressure and corneal edema. Keywords: corneal edema, exfoliation, intraocular pressure, glaucoma, visual acuity Abbreviations. POD = Postoperative day, PEX = Pseudoexfoliation syndrome, LOXL 1 = Lysyl oxidase-like 1, IOP = Intraocular pressure, AC = Anterior chamber, IOL = Intraocular lens
Introduction
The Pseudoexfoliation syndrome (PEX) was first described by Lindberg in 1917 in Finnish patients. The histological studies done by Davork-Theobald differentiated between the
exfoliation seen in glass blowers and senile exfoliation. Senile exfoliation was then termed as Pseudoexfoliation [1].
Pseudoexfoliation is characterized by production and deposition of abnormal fibrillar extracellular material in the ocular adnexa, Iris

Romanian Journal of Ophthalmology 2017; 61(3): 196-201
197
Romanian Society of Ophthalmology © 2017
and Lens Capsule and has also been observed in other tissues such as blood vessels, skin, gallbladder, kidneys, lungs, and heart. It has been linked to dysregulation of lysyl oxidase-like 1 (LOXL1) gene in PEX tissues [2].
Nordic countries tend to have a higher rate of pseudoexfoliation with up to 22.4% in Finland, above 60 years of age [3,4]. Rates in most other populations around the world are less but have been found to be as high as in American Navajo Indians (38.0%), to the very low rate in ethnic Chinese of Singapore (0.7%) [5,6].
Due to its manifestations, pseudoexfoliation can have a deleterious effect intraoperatively and significant effects on visual prognosis, postoperatively. Pseudoexfoliation Patients undergoing cataract surgery have been associated with various intraoperative cataract surgery complications such as zonular weakness, non-dilating pupil, Iris atrophy, and corneal edema [7]. Studies of unilateral exfoliation syndrome have found about a 5% decrease in the number of endothelial cells in the affected eye and about a 14% decrease in endothelial counts when compared to normal eyes [8-10]. Mild increase in polymegathism and pleomorphism of endothelial cells has also been noted [8,9].
PEX is the commonest identifiable cause of secondary glaucoma and most of these complications are thought to be secondary to glaucoma and associated to raised intraocular pressure rather than pseudoexfoliation itself [7].
In this first of a kind study, the effect of pseudoexfoliation without glaucomatous changes on the outcome of cataract surgeries has been studied. We aimed to find a correlation between postoperative visual acuity and pseudoexfoliation and try to understand the ocular manifestations of pseudoexfoliation and its resulting clinical and surgical complications.
Material and Methods
The study was done over nine months in a tertiary hospital in south India. Over 900 patients attended for cataract surgery during this period but only 35 met the inclusion and exclusion criteria and were taken for the study. All the patients with pseudoexfoliative material seen on slit lamp examination on Iris/ Corneal endothelium/ pupillary ruff/ Lens Capsule along with lens opacities were included but if
associated glaucomatous changes such as raised intraocular pressure and Glaucomatous Optic Disc were found, those patients were rejected. All the patients with history of secondary glaucoma, post refractive surgery were also excluded and so were the patients with obvious zonular weakness and phacodonesis or iridodonesis. A written informed consent was obtained for participation in the study from all the cases, according to Helsinki Declaration of 1975, as revised in 2000 and 2008.
A complete ophthalmic evaluation was done, including the recording of relevant ocular history; best corrected visual acuity with Snellen’s chart, examination of the pupillary reaction, and slit lamp evaluation of the anterior segment with a careful search for pseudoexfoliative deposits. Intraocular pressure (IOP) was recorded by Goldman’s applanation tonometry along with Gonioscopy by using a Goniolens in complete sterile condition in sitting position by a single fellow (blinded for patient details). Only subjects with open angles were included. Lens changes were graded by using Lens Opacities Classification System III (LOCS III) system and presence of subluxation of lens/ Phacodonesis was noted.
For easy reference, authors used a clinical grading system for classification, which was the following:
M1-MILD-Those with Pseudoexfoliative deposits on pupillary margin and anterior capsule.
M2-MODERATE-Those with M1 Iris changes (such as Iris atrophy).
M3-SEVERE-Those with M1/ M2 + Pseudoexfoliative deposits on endothelium and angle or other anterior segment structures.
Detailed stereoscopic evaluation of the fundus and the optic disc with the indirect ophthalmoscope and the +90 D lens was performed. Patients with dense cataracts, with no fundus view, underwent fundus examination postoperatively and if found to have a glaucomatous optic disc then were excluded from the study.
Glaucomatous optic nerve damage was considered as one or more of the following features:
(i) Vertical cup-disc ratio of 0.5 or more (physiological cups were excluded);
(ii) Vertical cup-disc asymmetry of 0.2 or more between the two eyes;
(iii) Characteristic glaucomatous excavation of the neuroretinal rim.

Romanian Journal of Ophthalmology 2017; 61(3): 196-201
198 Romanian Society of Ophthalmology
© 2017
Cataract surgery by phacoemulsification was performed for all the patients by a single senior consultant trained in the surgery. All the patients were prescribed topical ketorolac 0.3% for one day preoperatively to decrease the intraoperative miosis. Topical Tropicacyl Plus eye drops (Tropicamide 0.8% w/ v+ Phenylephrine 5% w/ v) was used the same morning to achieve mydriasis. Maximum pupil dilation pre-operative was noted.
During surgery, intracameral adrenaline along with copious amounts of viscoelastic material was used to achieve mydriasis in cases with inadequate mydriasis. Few cases required Iris hooks (8 mm* 0.8mm BD Visitec™ micro iris hooks) to achieve sufficient mydriasis. Phacoemulsification within the bag placement of foldable intraocular lens (Hydrophobic Acrylic Sensar® IOL) was done. In five cases an in the bag placement was not possible due to zonular dialysis and thus the lens was placed in the sulcus in three cases, whereas scleral fixation of the lens was done in the remaining two cases.
Intraoperative and first day postoperative complications along with best-corrected visual acuity were noted. IOP measurement was done on postoperative day 1 by Goldmann Applanation tonometry in complete sterile condition in sitting position by a single fellow (blinded for patient details). A detailed assessment of the anterior segment including the anterior chamber reaction, corneal edema, IOL position, iris tissue, as well as detailed fundus examination was done. Statistical tools used were regression analysis and paired t test. A P value less than or equal to 0.05 was considered significant. Microsoft Excel 2013 was used for data collection, tabulation, and chart preparation.
Results
The prospective study was done over nine months, in which 35 patients with pseudoexfoliation underwent phacoemulsification by a single surgeon trained in the same. The mean age of the patients was 61.60 years +/ - 10.21 years with the maximum number of patients being in the 61-70 years age group (n=14) as depicted in Table 1.
Table 1. Age groups of patients AGE GROUPS No. of Patients (%) 31-40 2 (5.71%) 41-50 3 (8.57%) 51-60 11 (31.43%) 61-70 14 (40%) 71-80 4 (11.43%) 81-90 1 (2.86%)
Males represented 46% (n=16). Right eye
was operated upon in 60% of the cases (n=21). 19 cases (54.29%) were immature cataract while 16 (45.71%) were mature cataract. Different types of cataract grading are depicted in Table 2.
Table 2. Grades of cataract
Cataract Grading No. of Patients (%) Grade II Nuclear Sclerosis 6 (17.14%) Grade III Nuclear Sclerosis 4 (11.43%) Grade IV Nuclear Sclerosis 6 (17.14%) Mature cataract 11 (31.43%) Hypermature cataract 5 (14.29%) Intumescent cataract 1 (2.86%) Posterior subcapsular cataract 2 (5.71%)
Eighteen patients (51.43%) had mild
pseudoexfoliation (M1), while five (14.29%) had moderate (M2) and twelve patients (34.29%) had severe pseudoexfoliation (M3).
Fig. 1 demonstrates the different amounts of pupil dilation observed. The mean pupil dilation was 5.1 mm +/ - 1.47 mm with 86% of the patients (n=30) having a maximum dilation of less than 6 mm as depicted in Table 3.
Fig. 1a Normal Pupil dilation, Fig. 1b Poor Mydriasis on the day of surgery, Fig. 1c Moderate Mydriasis on the day of surgery with pseudoexfoliative material visible on pupillary margin, Fig. 1d Good Mydriasis on the day of surgery
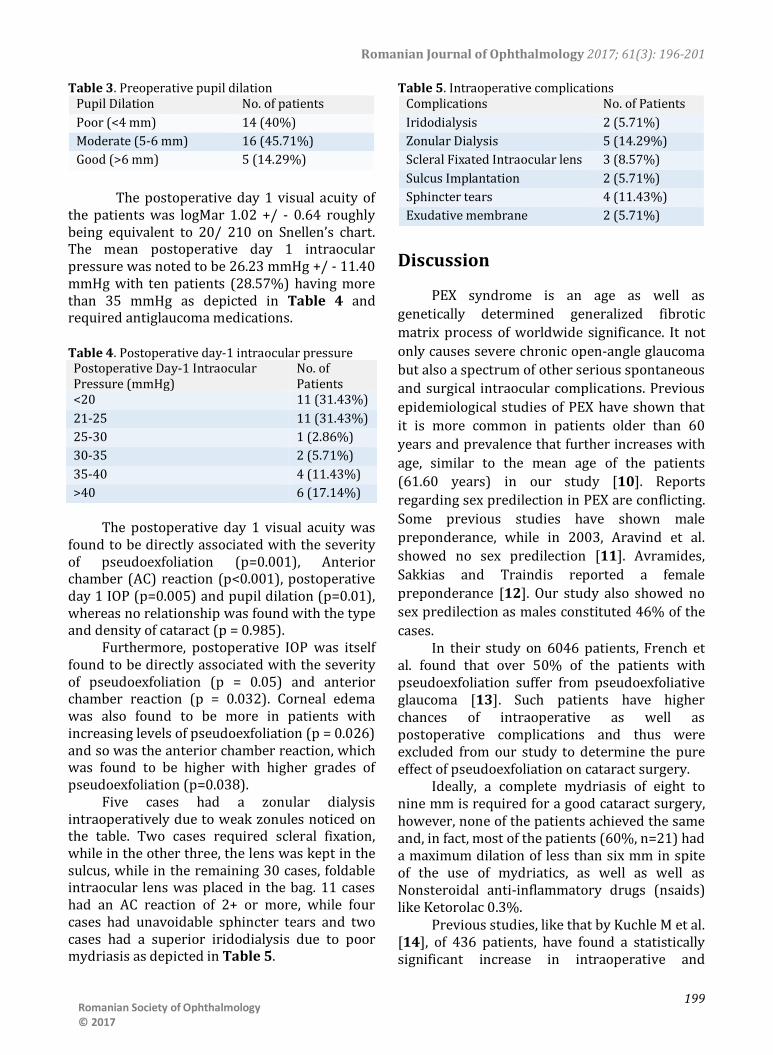
Romanian Journal of Ophthalmology 2017; 61(3): 196-201
199
Romanian Society of Ophthalmology © 2017
Table 3. Preoperative pupil dilation Pupil Dilation No. of patients Poor (<4 mm) 14 (40%) Moderate (5-6 mm) 16 (45.71%) Good (>6 mm) 5 (14.29%)
The postoperative day 1 visual acuity of
the patients was logMar 1.02 +/ - 0.64 roughly being equivalent to 20/ 210 on Snellen’s chart. The mean postoperative day 1 intraocular pressure was noted to be 26.23 mmHg +/ - 11.40 mmHg with ten patients (28.57%) having more than 35 mmHg as depicted in Table 4 and required antiglaucoma medications.
Table 4. Postoperative day-1 intraocular pressure Postoperative Day-1 Intraocular Pressure (mmHg)
No. of Patients
<20 11 (31.43%) 21-25 11 (31.43%) 25-30 1 (2.86%) 30-35 2 (5.71%) 35-40 4 (11.43%) >40 6 (17.14%)
The postoperative day 1 visual acuity was
found to be directly associated with the severity of pseudoexfoliation (p=0.001), Anterior chamber (AC) reaction (p<0.001), postoperative day 1 IOP (p=0.005) and pupil dilation (p=0.01), whereas no relationship was found with the type and density of cataract (p = 0.985).
Furthermore, postoperative IOP was itself found to be directly associated with the severity of pseudoexfoliation (p = 0.05) and anterior chamber reaction (p = 0.032). Corneal edema was also found to be more in patients with increasing levels of pseudoexfoliation (p = 0.026) and so was the anterior chamber reaction, which was found to be higher with higher grades of pseudoexfoliation (p=0.038).
Five cases had a zonular dialysis intraoperatively due to weak zonules noticed on the table. Two cases required scleral fixation, while in the other three, the lens was kept in the sulcus, while in the remaining 30 cases, foldable intraocular lens was placed in the bag. 11 cases had an AC reaction of 2+ or more, while four cases had unavoidable sphincter tears and two cases had a superior iridodialysis due to poor mydriasis as depicted in Table 5.
Table 5. Intraoperative complications Complications No. of Patients Iridodialysis 2 (5.71%) Zonular Dialysis 5 (14.29%) Scleral Fixated Intraocular lens 3 (8.57%) Sulcus Implantation 2 (5.71%) Sphincter tears 4 (11.43%) Exudative membrane 2 (5.71%)
Discussion
PEX syndrome is an age as well as genetically determined generalized fibrotic matrix process of worldwide significance. It not only causes severe chronic open-angle glaucoma but also a spectrum of other serious spontaneous and surgical intraocular complications. Previous epidemiological studies of PEX have shown that it is more common in patients older than 60 years and prevalence that further increases with age, similar to the mean age of the patients (61.60 years) in our study [10]. Reports regarding sex predilection in PEX are conflicting. Some previous studies have shown male preponderance, while in 2003, Aravind et al. showed no sex predilection [11]. Avramides, Sakkias and Traindis reported a female preponderance [12]. Our study also showed no sex predilection as males constituted 46% of the cases.
In their study on 6046 patients, French et al. found that over 50% of the patients with pseudoexfoliation suffer from pseudoexfoliative glaucoma [13]. Such patients have higher chances of intraoperative as well as postoperative complications and thus were excluded from our study to determine the pure effect of pseudoexfoliation on cataract surgery.
Ideally, a complete mydriasis of eight to nine mm is required for a good cataract surgery, however, none of the patients achieved the same and, in fact, most of the patients (60%, n=21) had a maximum dilation of less than six mm in spite of the use of mydriatics, as well as well as Nonsteroidal anti-inflammatory drugs (nsaids) like Ketorolac 0.3%.
Previous studies, like that by Kuchle M et al. [14], of 436 patients, have found a statistically significant increase in intraoperative and
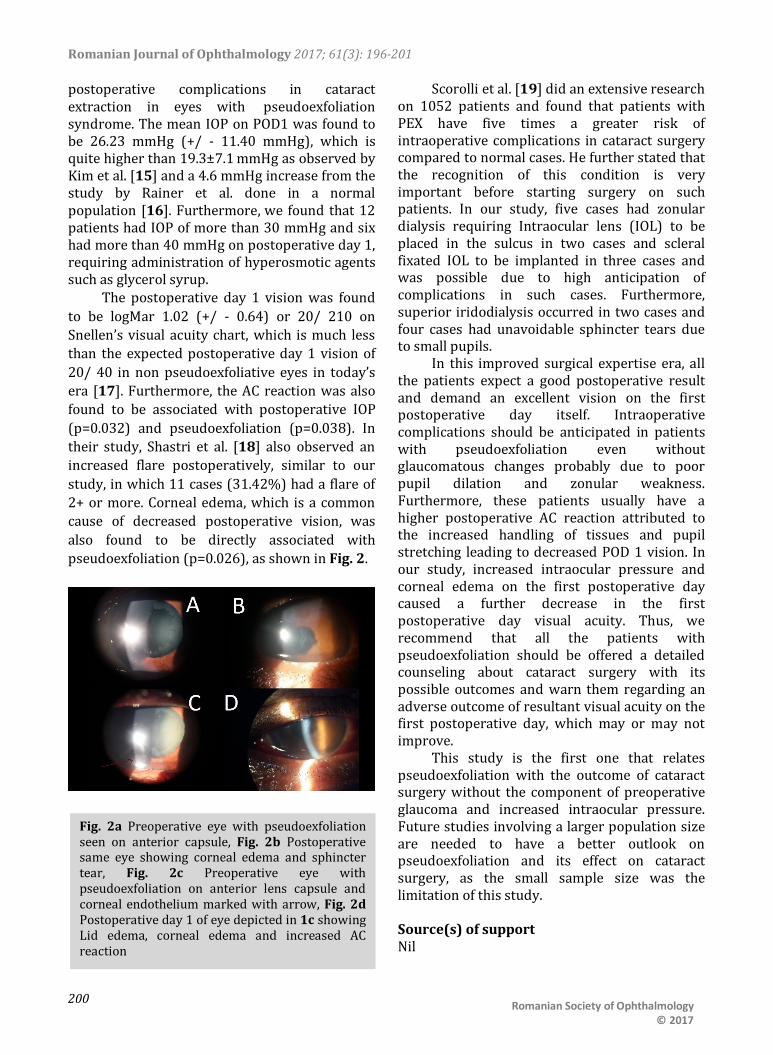
Romanian Journal of Ophthalmology 2017; 61(3): 196-201
200 Romanian Society of Ophthalmology
© 2017
postoperative complications in cataract extraction in eyes with pseudoexfoliation syndrome. The mean IOP on POD1 was found to be 26.23 mmHg (+/ - 11.40 mmHg), which is quite higher than 19.3±7.1 mmHg as observed by Kim et al. [15] and a 4.6 mmHg increase from the study by Rainer et al. done in a normal population [16]. Furthermore, we found that 12 patients had IOP of more than 30 mmHg and six had more than 40 mmHg on postoperative day 1, requiring administration of hyperosmotic agents such as glycerol syrup.
The postoperative day 1 vision was found to be logMar 1.02 (+/ - 0.64) or 20/ 210 on Snellen’s visual acuity chart, which is much less than the expected postoperative day 1 vision of 20/ 40 in non pseudoexfoliative eyes in today’s era [17]. Furthermore, the AC reaction was also found to be associated with postoperative IOP (p=0.032) and pseudoexfoliation (p=0.038). In their study, Shastri et al. [18] also observed an increased flare postoperatively, similar to our study, in which 11 cases (31.42%) had a flare of 2+ or more. Corneal edema, which is a common cause of decreased postoperative vision, was also found to be directly associated with pseudoexfoliation (p=0.026), as shown in Fig. 2.
Scorolli et al. [19] did an extensive research on 1052 patients and found that patients with PEX have five times a greater risk of intraoperative complications in cataract surgery compared to normal cases. He further stated that the recognition of this condition is very important before starting surgery on such patients. In our study, five cases had zonular dialysis requiring Intraocular lens (IOL) to be placed in the sulcus in two cases and scleral fixated IOL to be implanted in three cases and was possible due to high anticipation of complications in such cases. Furthermore, superior iridodialysis occurred in two cases and four cases had unavoidable sphincter tears due to small pupils.
In this improved surgical expertise era, all the patients expect a good postoperative result and demand an excellent vision on the first postoperative day itself. Intraoperative complications should be anticipated in patients with pseudoexfoliation even without glaucomatous changes probably due to poor pupil dilation and zonular weakness. Furthermore, these patients usually have a higher postoperative AC reaction attributed to the increased handling of tissues and pupil stretching leading to decreased POD 1 vision. In our study, increased intraocular pressure and corneal edema on the first postoperative day caused a further decrease in the first postoperative day visual acuity. Thus, we recommend that all the patients with pseudoexfoliation should be offered a detailed counseling about cataract surgery with its possible outcomes and warn them regarding an adverse outcome of resultant visual acuity on the first postoperative day, which may or may not improve.
This study is the first one that relates pseudoexfoliation with the outcome of cataract surgery without the component of preoperative glaucoma and increased intraocular pressure. Future studies involving a larger population size are needed to have a better outlook on pseudoexfoliation and its effect on cataract surgery, as the small sample size was the limitation of this study.
Source(s) of support Nil
Fig. 2a Preoperative eye with pseudoexfoliation seen on anterior capsule, Fig. 2b Postoperative same eye showing corneal edema and sphincter tear, Fig. 2c Preoperative eye with pseudoexfoliation on anterior lens capsule and corneal endothelium marked with arrow, Fig. 2d Postoperative day 1 of eye depicted in 1c showing Lid edema, corneal edema and increased AC reaction
Romanian Journal of Ophthalmology 2017; 61(3): 196-201
201
Romanian Society of Ophthalmology © 2017
Conflicting Interest Nil Acknowledgement
Dr. Parijat Joshi for relentless proofing of the manuscript. Mr. Ankush Singhal for his useful inputs in the statistical analysis.
References 1. Lindberg JGMD. Clinical studies of depigmentation of
the pupillary margin and transillumination of the iris in cases of senile cataract and also in normal eyes of the aged. Thesis, 1917, Diss Helsingfors, Finland.
2. Schlötzer-Schrehardt U, Pasutto F, Sommer P, Hornstra I, Kruse FE, Naumann GOH, Zenkel M. Genotype-Correlated Expression of Lysyl Oxidase-Like 1 in Ocular Tissues of Patients with Pseudoexfoliation Syndrome/Glaucoma and Normal Patients. The American Journal of Pathology. 2008; 173(6),1724–1735. Http://doi.org/10.2353/ajpath.2008.080535.
3. Krause U, Alanko HI, Karna J, Miettinen R, Larmi T, Jaanio E, Ollila OI, Takala J. Prevalence of exfoliation syndrome in Finland. Acta Ophthalmol. 1988; 66(Suppl 184):120.
4. Backhaus B, Lorentzen SE. Prevalence of pseudoexfoliation in non glaucomatous eyes in Denmark. Acta Ophthalmol. 1966; 44:1.
5. Faulkner HW. Pseudo exfoliation of the lens among the Navajo Indians. Am J Ophthalmol. 1971; 72:206.
6. Foster PJ, Seah SK. The prevalence of pseudoexfoliation syndrome in Chinese people: the Tanjong Pagar Survey. Br J Ophthalmol. 2005; 89:239–240.
7. Repo LP, Teräsvirta ME, Tuovinen EJ. Generalized peripheral iris transluminance in the pseudoexfoliation syndrome. Ophthalmology. 1990; 97:1027–1029.
8. Vannas A, Setälä K, Ruusuvaara P. Endothelial cells in capsular glaucoma. Acta Ophthalmol. 1977; 55:951.
9. Miyake K, Matsuda M, Inaba M. Corneal endothelial changes in pseudoexfoliation syndrome. Am J Ophthalmol. 1989; 108:49.
10. Inoue K, Okugawa K, Oshika T, Amano S. Morphological study of corneal endothelium and corneal thickness in pseudoexfoliation syndrome. Eur J Ophthalmol. 2003; 47:235–239.
11. Sekeroglu MA, Bozkurt B, Irkec M, Ustunel S, Orhan M, Saracbasi O. Systemic associations and prevalence of exfoliation syndrome in patients scheduled for cataract surgery. Eur JOphthalmol. 2008; 18:551-5.
12. Avramides S, Traianidis P, Sakkias G. Cataract surgery and lens implantation in eyes with exfoliation syndrome. J Cataract Refract Surg. 1997; 23:583-7.
13. French DD, Margo CE, Harman LE. Ocular Pseudoexfoliation and Cardiovascular Disease: A National Cross-Section Comparison Study. North American Journal of Medical Sciences. 2012; 4(10),468–473. Http://doi.org/10.4103/1947-2714.101987.
14. Küchle M, Schönherr U, Dieckmann U. Risk factors for capsular rupture and vitreous loss in extracapsular
cataract extraction. The Erlangen Ophthalmology Group. Fortschr Ophthalmol. 1989; 86(5):417-21.
15. Kim JY, Jo MW, Brauner SC, Ferrufino-Ponce Z, Ali R, Cremers SL, An Henderson B. Increased intraocular pressure on the first postoperative day following resident-performed cataract surgery. Eye. 2011; 25(7),929–936. Http://doi.org/10.1038/eye.2011.93.
16. Rainer G, Menapace R, Findl O, Kiss B, Petternel V, Georgopoulos M. Intraocular pressure rise after small incision cataract surgery: a randomized intraindividual comparison of two dispersive viscoelastic agents. Br J Ophthalmol. 2001; 85:139-142 doi:10.1136/bjo.85.2.139.
17. Thanigasalam T, Reddy SC, Zaki RA. Factors associated with complications and postoperative visual outcomes of cataract surgery; A study of 1,632 cases. J Ophthalmic Vis Res. 2015; 10:375-84.
18. Shastri L, Vasavada A. Phacoemulsification in Indian eyes with pseudoexfoliation. J Cataract Refract Surg. 2001; 27:1629-37.
19. Scorolli L, Campos EC, Bassein L, Meduri RA. Pseudoexfoliation syndrome. A cohort study on intraoperative complications in cataract surgery. Ophthalmologica. 1998; 212:278-80.

Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:202-206
GENERAL ARTICLE
202 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.37
Functional results of cataract surgery in the treatment of phacomorphic glaucoma
Moraru Andreea* **, Pînzaru Gabriela**, Moţoc Anca**, Costin Dănuţ* **
* “Grigore T. Popa” University of Medicine and Pharmacy, Iaşi, Romania ** “Prof. N. Oblu” Emergency Hospital, Iaşi, Romania Correspondence to: Andreea Moraru, MD, PhD, “Prof. N. Oblu” Emergency Hospital, Iaşi, 2 Ateneului Street, Iaşi, Romania, Mobile phone: +40723 504 701, E-mail: [email protected] Accepted: September 8th, 2017
Abstract Purpose. Analysis of functional outcome and complications reported in patients diagnosed with phacomorphic glaucoma, in which phacoemulsification or extracapsular extraction of the lens was performed. Methods. The retrospective study included 38 eyes diagnosed with phacomorphic glaucoma. In 25 cases, group 1, the lens was removed by phacoemulsification and in 13 cases, group 2, by extracapsular extraction. Intraocular pressure, visual acuity, and anterior chamber depth were evaluated preoperative and postoperative. The incidence of intra and postoperative complications was analyzed. The minimum follow-up period was 12 months. Results. The mean IOP decreased from the preoperative value of 38.4 +/ - 11.3 mmHg to 13.5 +/ - 3.4 mmHg in group 1 and 11.5 +/ - 3.2 mmHg in group 2. Persistent corneal edema was observed in 32% patients from group 1 and 23% of the patients from group 2. The inflammatory reaction of anterior chamber prevailed in patients from group 2 (46.1%). ACD modified from the preoperative mean of 1.3 +/- 0.5 mm to 2.3 +/- 0.2 mm in both groups. At the end of follow-up in both groups, the average BCVA was 0.6. 18.42% of the cases required long-term topical hypotensive therapy. Conclusions. Both phacoemulsification and extracapsular extraction were safe and effective procedures in the treatment of phacomorphic glaucoma, ensuring a rapid functional recovery and a satisfactory long-term IOP control. Although the rate of immediate postoperative complications and the final functional outcome were better in patients treated with phacoemulsification, not all the cases could be subjected to this type of surgery. Keywords: cataract surgery, phacomorphic, glaucoma
In 2013, the estimated number of people with eyesight deficiencies worldwide was 285 million people, out of which 39 million were blind. 65% of the patients diagnosed with eyesight deficiencies are over 50 years old and the cataract alone constitutes 51% of the causes that lead to blindness [1].
Phacomorphic glaucoma is defined as secondary angle-closure glaucoma due to lens thickness increase, which is obstructing the drainage angle. It is characterized by a sudden rise in the intraocular pressure (IOP), which compromises the function of the optic nerve and
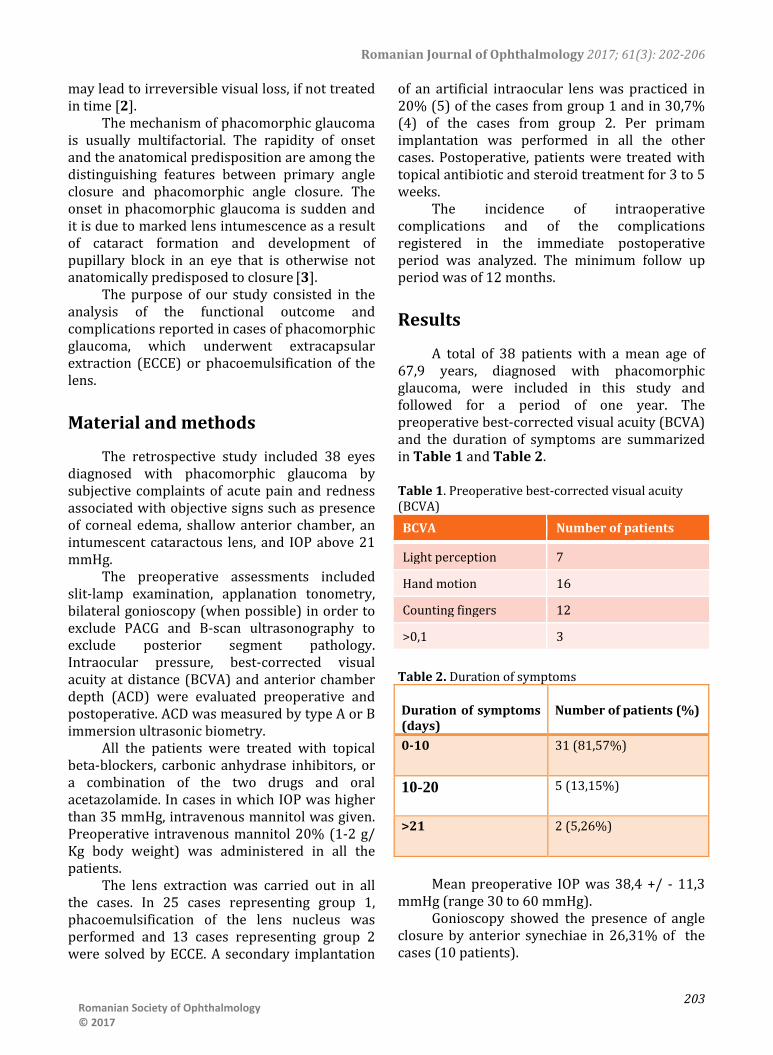
Romanian Journal of Ophthalmology 2017; 61(3): 202-206
203
Romanian Society of Ophthalmology © 2017
may lead to irreversible visual loss, if not treated in time [2].
The mechanism of phacomorphic glaucoma is usually multifactorial. The rapidity of onset and the anatomical predisposition are among the distinguishing features between primary angle closure and phacomorphic angle closure. The onset in phacomorphic glaucoma is sudden and it is due to marked lens intumescence as a result of cataract formation and development of pupillary block in an eye that is otherwise not anatomically predisposed to closure [3].
The purpose of our study consisted in the analysis of the functional outcome and complications reported in cases of phacomorphic glaucoma, which underwent extracapsular extraction (ECCE) or phacoemulsification of the lens.
Material and methods
The retrospective study included 38 eyes diagnosed with phacomorphic glaucoma by subjective complaints of acute pain and redness associated with objective signs such as presence of corneal edema, shallow anterior chamber, an intumescent cataractous lens, and IOP above 21 mmHg.
The preoperative assessments included slit-lamp examination, applanation tonometry, bilateral gonioscopy (when possible) in order to exclude PACG and B-scan ultrasonography to exclude posterior segment pathology. Intraocular pressure, best-corrected visual acuity at distance (BCVA) and anterior chamber depth (ACD) were evaluated preoperative and postoperative. ACD was measured by type A or B immersion ultrasonic biometry.
All the patients were treated with topical beta-blockers, carbonic anhydrase inhibitors, or a combination of the two drugs and oral acetazolamide. In cases in which IOP was higher than 35 mmHg, intravenous mannitol was given. Preoperative intravenous mannitol 20% (1-2 g/ Kg body weight) was administered in all the patients.
The lens extraction was carried out in all the cases. In 25 cases representing group 1, phacoemulsification of the lens nucleus was performed and 13 cases representing group 2 were solved by ECCE. A secondary implantation
of an artificial intraocular lens was practiced in 20% (5) of the cases from group 1 and in 30,7% (4) of the cases from group 2. Per primam implantation was performed in all the other cases. Postoperative, patients were treated with topical antibiotic and steroid treatment for 3 to 5 weeks.
The incidence of intraoperative complications and of the complications registered in the immediate postoperative period was analyzed. The minimum follow up period was of 12 months.
Results
A total of 38 patients with a mean age of 67,9 years, diagnosed with phacomorphic glaucoma, were included in this study and followed for a period of one year. The preoperative best-corrected visual acuity (BCVA) and the duration of symptoms are summarized in Table 1 and Table 2. Table 1. Preoperative best-corrected visual acuity (BCVA) BCVA Number of patients
Light perception 7
Hand motion 16
Counting fingers 12
>0,1 3
Table 2. Duration of symptoms Duration of symptoms (days)
Number of patients (%)
0-10 31 (81,57%)
10-20 5 (13,15%)
>21 2 (5,26%)
Mean preoperative IOP was 38,4 +/ - 11,3
mmHg (range 30 to 60 mmHg). Gonioscopy showed the presence of angle
closure by anterior synechiae in 26,31% of the cases (10 patients).

Romanian Journal of Ophthalmology 2017; 61(3): 202-206
204 Romanian Society of Ophthalmology
© 2017
The extraction of the lens was carried out after lowering the IOP under 21 mmHg, between 2 and 5 days after presentation.
In 25 cases representing group 1, phacoemulsification of the lens nucleus was performed by using higher quantities of viscoelastics in a “soft shell” technique, in order to deepen the anterior chamber. The nucleus was fragmented by using “stop and chop” technique and a single- piece hydrophobic foldable IOL was injected into the capsular bag or ciliary sulcus in 80% of the cases.
In 13 cases representing group 2, phacoemulsification could not be performed. In these cases, extracapsular cataract extraction was successfully carried out. IOL was injected in sulcus in 70% of the cases. In 20% of the cases (5 eyes) of group 1 and in 30% of the cases (4 eyes)
of group 2, secondary implantation of an IOL was performed.
The most important intraoperative challenges were: miosis - 11 eyes (28,94%), fluctuation of the anterior chamber depth - 20 eyes (52,63%), posterior capsular rupture - 3 eyes (7,89%), zonular dehiscence – 4 eyes (10,52%), anterior synechiae > 180º - 10 eyes (26,31%), posterior positive pressure - 2 eyes (5,26%).
In the first postoperative day, severe to moderate corneal edema was present in 8 (32%) patients from group 1 and 3 (23%) patients from group 2. Also, 6 patients (46%) from group 1 and 2 patients (8%) from group 2 presented with severe iritis and a fibrinous pupillary membrane. Two cases from group 2 had mild hyphema (Table 3). The complications were solved by administering topical medication.
Table 3. Early postoperative complications in Group 1 and 2
Late postoperative complications observed
were opacification of the posterior capsule in one eye from group 1 and cystoid macular edema in 3 eyes from group 2. Also, 7 eyes, 2
from group 1 and 5 from group 2 developed glaucomatous optic neuropathy (Table 4).
Table 4. Late postoperative complications in Group 1 and 2
No. Late postoperative complications Group 1 (%of patients)
Group 2 (%of patients)
1 Opacification of the posterior capsule
4% (1 eye) -
2 Cystoid macular edema 23% (3 eyes) 44% (11 eyes)
3 Glaucomatous optic neuropathy 8% (2 eyes) 38,4% (5 eyes)
BCVA status was improved during the first
week postoperative. At 3 months after surgery, the mean BCVA in group 1 was 0,4, while that of group 2 was 0,2. At the end of the follow-up in group 1, the average BCVA was 0,6 and 0,55 in
group 2. The mean postoperative BCVA values are summarized in Fig. 1.
No. Early postoperative complications Group 1 (%of patients)
Group 2 (%of patients)
1 Severe to moderate corneal edema 32% (8 cases) 23% (3 cases) 2 Severe iritis with fibrin membrane 8% (2 cases) 46,1% (6 cases)
3 Hyphema - 15,3% (2 cases)

Romanian Journal of Ophthalmology 2017; 61(3): 202-206
205
Romanian Society of Ophthalmology © 2017
The mean preoperative anterior chamber depth (ACD) was 1,3+/ -0,5 mm. ACD after surgery in both groups had a mean value of 2,3+/ - 0,2 mm, measured by type A or B immersion ultrasonic biometry. The mean postoperative IOP in group 1 was 13,5 +/ - 3,4 mmHg and in group 2, a value of 11,5+/ - 3,2 mmHg was registered. 18,42% of the cases (7 patients) required postoperative topical hypotensive long-term therapy, but none of the cases required glaucoma surgery.
Discussions
Phacomorphic glaucoma is a type of secondary angle-closure glaucoma, due to a mature and intumescent cataract [4]. Historically, this entity has been called phacomorphic glaucoma, but Tham and colab. have pointed out that the use of the word “glaucoma” implies an optic neuropathy and, since the majority of these patients do not have a glaucomatous optic neuropathy, the disease is currently called phacomorphic angle closure [5].
The risk factors for phacomorphic angle closure are: age > 60 years, axial length ≤ 23,7 mm, shallow anterior chamber [6,7].
Control of the high IOP is the first line treatment in a phacomorphic angle closure case, followed by the reduction of corneal edema and cataract surgery. Initial antiglaucomatous medication usually includes beta-blockers, alpha agonists, and carbonic anhydrase inhibitors. Prostaglandin analogues use in such cases has not been reported on a large scale, most likely to avoid their pro-inflammatory effect [8]. Many cases require iv mannitol 20% and oral acetazolamide in order to lower the IOP and safely extract the cataractous lens.
Phacoemulsification was attempted in all the eyes included in this study and it has been successfully completed in 25 eyes – group 1. 20 eyes included in group 1 benefited from per primam implantation of the IOL in the capsular bag or the sulcus. Due to the hard nucleus and intraoperative difficulties, we decided to convert the surgery to extracapsular extraction in 13 eyes, included in group 2. 9 of these eyes benefited from per primam implantation of the IOL.
Corneal edema and AC inflammation with fibrinous reaction during the first few days after surgery are complications frequently found in the early postoperative period [9]. In our study, moderate to severe postoperative corneal edema was observed in 32% of the patients from group 1 and in 23% of the patients form group 2, severe iritis with fibrous membrane in 8% of the patients from group 1 and in 46,6% of the patients from group 2, but were successfully treated with topical treatment.
Studies showed there was a statistically significant association between the duration of the symptoms and the final visual prognosis. A delay higher than 5-10 days from onset to surgery is an important risk factor for an unsatisfactory final VA [10].
In our study, 85,57% of the patients reporting a duration of the symptoms of less than 10 days presented a mean BCVA of 0,3, at one month postoperative. In 13,15% of the patients, who reported a duration of the symptoms of 10-20 days, the mean BCVA was 0,15. The worst functional result was registered in the cases in which the delay between the onset and the treatment was more than 20 days. The mean BCVA in this group was 0,05.
Literature data also reported that a duration of symptoms from the onset of more than 10 days is linked with alterations of C/ D ratio [5]. At 3 months postoperative, 7 patients included in our study showed an enlargement of the C/ D ratio. 2 of these patients were diagnosed between 10 to 20 days from the onset and 5 after more than 20 days. All these cases required chronic topical hypotensive treatment. This result confirms that a delay of more than 10 days from the diagnosis is a significant risk factor for the development of glaucomatous optic neuropathy.
The final visual prognosis was influenced by late postoperative complications. In 12 cases, the mean final BCVA was less than 0,05 due to opacification of the posterior capsule requiring
Fig. 1 Mean postoperative BCVA values

Romanian Journal of Ophthalmology 2017; 61(3): 202-206
206 Romanian Society of Ophthalmology
© 2017
YAG capsulotomy (1 eye), glaucomatous optic neuropathy (7 eyes), cystoid macular edema (4 eyes).
Data provides postoperative normal reference range values for IOP in both groups analyzed in our study. At the end of the study, the IOP in more than 80% of the cases was maintained under control without needing long-term therapy. Literature data shows that there is a statistically significant difference between the IOP at the first visit and the IOP at the last visit, without any correlations between the IOP at the first visit and the final VA [10].
Conclusions
Lens removal through phacoemulsification or ECCE is a safe and effective procedure in the treatment of phacomorphic glaucoma, ensuring a rapid functional recovery and a satisfactory long-term IOP control. Although the rate of immediate postoperative complications and the final functional outcome were better in patients treated by phacoemulsification, not all the cases could be subjected to this type of surgery due to intraoperative difficulties linked to the angle closure.
The final visual outcome is influenced by the delay between the onset of symptoms and the establishment of the diagnosis and by the presence of late postoperative complications, but over 80% of the patients are expected to have a favorable visual outcome. The development of glaucomatous optic neuropathy depends on how soon the treatment is initialized, after the onset of the phacomorphic angle closure.
References
1. Rajkumari V, Khongbantabam S, Rajkumari D, Rajkumur V. Manual Small Incision Cataract Surgery in Phacomorphic Glaucoma: Surgical Technique and Outcome in North-Eastern India. J Curr Glaucoma Pract. 2013 May-Aug; 7(2):43-48.
2. Shibal B, Mahesh KHM, Jain M. Phacomorphic Glaucoma: Evolving Management Strategies. Journal Current Glaucoma Practice. May-August 2009; 3(2):39-46.
3. Lee JW, Lai JS, Yick DW, Tse RK. Retrospective case series on the long-term visual and intraocular pressure outcomes of phacomorphic glaucoma. Eye. 2010 Nov; 24(11):1675-80.
4. Tham CCY, Lai JSM, Poon ASY, Chan JCH, Lam SW, Chua JKH, Lam DSC. Immediate argon laser peripheral
iridoplasty as initial treatment for acute phacomorphic angle-closure before cataract extraction: a preliminary study. Eye. 2005; 19:778-783.
5. Kaplowitz KB, Kapoor KG. An Evidence–Based Approach to Phacomorphic Glaucoma. J Clinic Experiment Ophthalmol. 2011; S:1.
6. Sowka J. Phacomorphic glaucoma: case and review. Optometry. 2006 Dec; 77(12):586-9.
7. Barkana Y, Shihadeh W, Oliveira C, Tello C, Liebmann JM. Angle closure in highly myopic eyes. Ophthalmology. 2006; 113:247-254.
8. Schumer RA, Camras CB, Mandahl AK. Putative side effects of prostaglandin analogs. Surv Ophthalmol. 2002; 47 Suppl 1:S219.
9. Lee SJ, Lee CK, Kim WS. Long-term therapeutic efficacy of phacoemulsification with intraocular lens implantation in patients with phacomorphic glaucoma. J Cataract Refract Surg. 2010 May; 36(5):783-9.
10. Ramakrishanan R, Devendra M, Mohideen AK, Singh R, Neelam P, Bharathi MJ. Visual prognosis, intraocular pressure control and complications in phacomorphic glaucoma following manual small incision cataract surgery. Indian J Ophthalmol. Jul-Aug 2010; 58(4):303-306.

Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:207-211
GENERAL ARTICLE
207 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.38
Incidence of ocular hypertension after intravitreal injection of anti-VEGF agents in the treatment of neovascular AMD
Moraru Andreea* **, Pînzaru Gabriela**, Moţoc Anca**, Costin Dănuţ* **, Brănişteanu Daniel* ***
* “Grigore T. Popa” University of Medicine and Pharmacy, Iaşi, Romania **“Prof. N. Oblu” Hospital, Iaşi, Romania ***Retina Center Iaşi, Romania Correspondence to: Andreea Moraru, MD, PhD, “Prof. N. Oblu” Emergency Hospital, Iaşi, 2 Ateneului Street, Iaşi, Romania, Mobile phone: +40723 504 701, E-mail: [email protected] Accepted: September 9th, 2017
Abstract Purpose. The assessment of the incidence of ocular hypertension over a period of 1 year in patients treated with multiple intravitreal injections of anti-VEGF agents for neovascular AMD. Methods. The study comprised 58 eyes diagnosed with neovascular age-related macular degeneration and receiving PRN intravitreal treatment with anti-VEGF agents (bevacizumab or aflibercept). The follow-up period was 1 year. Intraocular pressure was measured by using the Goldmann applanation tonometry before the intravitreal injection, at 24 hours after the administration of the anti-VEGF agent and at 1 and 4 weeks. Patients diagnosed with glaucoma or who underwent ophthalmic surgery were excluded. Results. The patients received an average of 7.54 intravitreal injections. The mean baseline intraocular pressure was 15.3 mm Hg; 19.8 mm Hg at 24 hours; 17,4 mmHg at 1 week and 14.8 mmHg at 4 weeks after the administration of the anti-VEGF agent. 4 patients required long-term topical hypotensive treatment. Raised intraocular pressure was related to increased frequency of treatment. At 1 year follow up, an average difference of 2.1 mmHg compared to baseline was registered in the cases that have received more than 6 intravitreal injections. By comparison, in the cases treated with a reduced number of doses of intravitreal anti VEGF agent, the difference from baseline was 0,9 mmHg. There were no significant differences in mean IOP depending on the anti VEGF (bevacizumab or aflibercept) agent used. Conclusions. Intravitreal treatment with anti VEGF agents produces a transient increase in intraocular pressure, predominantly immediately following administration, without causing long-term increased values. Keywords: intraocular pressure, intravitreal injection, neovascular AMD, anti-VEGF
Intravitreal anti-vascular endothelial growth factor (VEGF) agents usage is widely spread as primary treatment of many vitreoretinal diseases such as neovascular age-related macular degeneration, diabetic macular edema, macular edema secondary to retinal vein
occlusion and other macular edemas [1]. The introduction of additional fluid into the vitreous cavity by intravitreal therapy could cause an immediate rise in intraocular pressure (IOP). This transient, short-term IOP elevation (lasting

Romanian Journal of Ophthalmology 2017; 61(3): 207-211
208 Romanian Society of Ophthalmology
© 2017
up to 30 minutes) after intravitreal anti-VEGF therapy has been studied by many authors [2].
Bevacizumab (Avastin), a monoclonal antibody targeting vascular endothelial growth factor (VEGF), was approved by the Food and Drug Administration (FDA) for systemic administration in patients with metastatic colon cancer. Bevacizumab was first injected intravenously to treat age-related macular degeneration (AMD). The use of intravitreal bevacizumab in treating ocular diseases was first reported in 2005 for choroidal neovascularization (CNV) caused by AMD. One of the side effects is related to the rise of intraocular pressure (IOP), which can be transient or permanent [3].
Aflibercept (Eylea) is a fully human fusion protein consisting of portions of VEGF receptors 1 and 2, which binds all forms of VEGF-A, along with the related placental growth factor, which the drug blocks. FDA approved aflibercept for the treatment of neovascular (“wet”) age-related macular degeneration (AMD) in 2011 [4].
In all cases, an effective therapy with anti-VEGF antibodies can only be achieved by repeated intravitreal anti-VEGF injections. In general practice, three intravitreal injections of anti-VEGF antibodies are given at every 4 weeks in the initial upload phase, followed by further intravitreal injections of anti-VEGF antibodies if the lesion persists or increases. Therefore, a monthly ophthalmologic checkup is needed to ensure a correct treatment interval with anti-VEGF antibodies [5]. The recommended dose for Aflibercept administered by intravitreal injection is once at every 4 weeks for the first 3 months, followed by intravitreal injection once at every 8 weeks [6].
Material and methods
58 eyes diagnosed with neovascular age-related macular degeneration and receiving „Pro Re Nata” (PRN) intravitreal treatment with anti-VEGF agents (bevacizumab or aflibercept) were
included in this study. The follow-up period was 1 year.
Inclusion criteria consisted in age between 65 and 85 years, initial IOP < 21 mmHg, ability to understand and sign the consent form, and ability to follow the scheduled visit protocol. The exclusion criteria consisted in: open-angle or angle-closure glaucoma, suspected glaucoma (IOP > 21 mmhg and/ or cup to disc ratio > 0.5), currently receiving a systemic beta blocker, previously receiving intravitreal injection of any medication (steroid, ganciclovir, and anti-VEGF agent), current use of steroid eye drops, and any ocular surface disease precluding a reliable IOP measurement.
The follow-up protocol of patients with exudative AMD treated with anti-VEGF required strict monthly follow-up visits with complete ocular examinations, including IOP measurements.
Intraocular pressure was measured by using the Goldmann applanation tonometry before the intravitreal injection, at 24 hours after the administration of anti-VEGF agent at 1 and 4 weeks. Ocular hypertension was defined as intraocular pressure over 21 mmHg. Patients diagnosed with glaucoma or who underwent ophthalmic surgery were excluded. All the patients received a loading dose, which consisted of one monthly-administered injection, for three months.
The patients were divided into two groups according to the injection type: • 50 (86%) patients received bevacizumab 36 (72%) patients received the injection
at an interval of less than 8 weeks (range 4-7 weeks) after the initial loading dose
14 (28%) patients received the injection at an interval of more than 8 weeks (range 8-12 weeks) after the initial loading dose
• 8 (14%) patients received aflibercept (once at every 2 months after the initial loading dose).
Results
58 eyes of 58 patients diagnosed with neovascular age related macular degeneration were analyzed in the present study. The mean age was 69 years (ranging from 65–85 years of

Romanian Journal of Ophthalmology 2017; 61(3): 207-211
209
Romanian Society of Ophthalmology © 2017
age) and most of the patients were women. The study included 36 phakic eyes (62%) and 22 pseudophakic eyes (38%).
Most patients received intravitreal bevacizumab injection (86%) and the rest were treated with intravitreal aflibercept (14%). All the patients were treated with the standard dose of Avastin or Eylea administered intravitreally. Most patients, 72%, received the bevacizumab injection at an interval of less than 8 weeks after the initial loading dose. The patients receiving aflibercept were treated according to the recommended protocol (once at every two months after the initial loading dose) (Fig. 1).
The patients received an average of 7.54 intravitreal injections during the study period, with limits between 3 and 10 injections. The only complications seen post injection were discreet corneal edema, conjunctival congestion, subconjunctival hemorrhage.
IOP was monitored for all patients prior to treatment and at all follow-up visits. Sustained IOP elevation was defined as an IOP of 21 mmHg or greater, combined with a rise of 6 mmHg or more lasting for 30 days or more, compared to baseline. The average IOP rose from 15.3 mmHg (range 8-15 mmHg) before the initiation of injections to 19.8 mmHg (range 16-28 mmHg) after the treatment.
No significant differences were found in IOP elevations between the two groups depending on the anti VEGF agent used (bevacizumab or aflibercept) (Fig. 2), although bevacizumab seemed to induce a slightly higher IOP level than aflibercept.
The raised intraocular pressure was related
to an increased frequency of treatment. Increased levels of the IOP were observed in patients who received more than six injections and those in whom the frequency of the treatment was of less than eight weeks. The interval between injections was the most remarkable risk factor for the IOP elevation identified in this study. The IOP elevation was greater when the average interval between the injections was of less than eight weeks compared to the average intervals of eight weeks or more.
Fig. 1 Frequency of treatment after the administration of the initial loading dose of bevacizumab/ aflibercept
Fig. 2 Variation of mean IOP values after the intravitreal injection
Fig. 3 Number of patients in relation with the number of intravitreal injections of bevacizumab/ aflibercept received

Romanian Journal of Ophthalmology 2017; 61(3): 207-211
210 Romanian Society of Ophthalmology
© 2017
At 1 year follow up, an average difference of 2.1 mmHg compared to baseline was registered in the cases that have received more than 6 intravitreal injections. By comparison, in the cases treated with a reduced number of doses of intravitreal anti VEGF agent, the difference from baseline was 0,9 mmHg.
None of the patients had to undergo glaucoma surgery or discontinue the participation in the study following uncontrolled IOP. Four patients needed topical hypotensive treatment during the follow up period due to the maintenance of IOP at levels higher than 25mmHg.
Discussions
The intravitreal injection of anti-angiogenic agents has assumed an important leading role in the treatment of a growing number of ophthalmologic conditions since 2005, when the intravitreal use of bevacizumab was first reported [7].
Evidence collected in recent years has demonstrated that intravitreal injections may produce short- and/ or long-term elevations in IOP. The possible mechanisms for a sustained IOP elevation after the intravitreal injection of anti-VEGF agents are not very well understood. Anti-VEGF agents may directly damage the trabecular meshwork, so one possible mechanism of IOP elevation is inflammation, such as drug-induced trabeculitis or uveitis [8].
Another mechanism of anti-VEGF-induced IOP elevation is considered an underlying inflammatory mechanism or an immunological reaction that damages the aqueous humor outflow pathways. Besides that, a traumatic mechanism after frequent injections may lead to a disruption of the anterior hyaloid or zonules and allow access for high molecular weight proteins to enter the anterior chamber, resulting in increased IOP [9].
The IOP spike that occurs after the intravitreal injection of anti-VEGF agents is usually transient, with IOP returning to a safer range (< 25–30 mmHg) within 1 hour, without topical hypotensive medications, in most patients [10].
A prolonged elevation was found in 4 out of 58 patients treated with recurrent intravitreal
Eylea or Avastin who needed topical hypotensive treatment during the follow up period. None of the patients who suffered from IOP elevations had a history of glaucoma or ocular hypertension.
Some authors reported an increased risk of IOP elevation in patients receiving >29 injections compared to patients with <12 injections [11]. Moreover, an increased risk of IOP elevation was also found in the groups with a higher number of injections.
Initial IOP elevation varied from 1 hour, 1 week, and 3 months after treatment. In 3 eyes, the IOP returned to baseline levels after 1 month, even when receiving monthly injections. A possible explanation for the low rate of sustained IOP elevation could be that 64% of the patients in our study did not receive monthly injections, but rather, received an extended treatment regimen. It is possible that the increase of the interval between injections will allow the anti-VEGF medication to be cleared from the eye [12].
The type of injected drug (Avastin versus Eylea) did not have a statistically remarkable influence on the difference in IOP, but a slightly higher IOP was found in eyes receiving bevacizumab. The limitations of this study include its retrospective nature and a short follow-up period, which implied a limited number of injections.
Conclusion
In conclusion, most eyes in our study achieved a normalization of IOP within 24 hours without the need for any immediate intervention.
A close monitoring of IOP is required in patients undergoing intravitreal Avastin injections, especially in those patients receiving frequent injections, to prevent further ocular damage, in addition to the underlying retinal disease. A prompt diagnosis and treatment can prevent the potential loss of vision.
References
1. Nuzzi R, Tridico F. Complications of Intravitreal Anti-VEGF Drugs: A Report on Our Personal Experience. J Clin Exp Ophthalmol. 2015; 6:4.

Romanian Journal of Ophthalmology 2017; 61(3): 207-211
211
Romanian Society of Ophthalmology © 2017
2. Falkenstein IA, Cheng L, Freeman WR. Changes of intraocular pressure after intravitreal injection of bevacizumab (Avastin). Retina. 2007; 27:1044–1047.
3. Shima C, Sakaguchi H, Gomi F et al. Complications in patients after intravitreal injection of bevacizumab. Acta Ophthalmol. 2008; 86:372–376.
4. Heier JS, Brown DM. Intravitreal Aflibercept (VEGF Trap-Eye) in wet age-related macular degeneration. Ophthalmology. December 2012; 119(12).
5. Yu AL, Schaumberger M. Evaluation of intraocular pressure elevation after multiple injections of intravitreal ranibizumab. Clinical Ophthalmology. 2014; 8:743–747.
6. Schmidt-Erfurth U, Kaiser PK, Korobelnik JF. Intravitreal aflibercept injection for neovascular age-related macular degeneration: ninety-six-week results of the VIEW studies. Ophthalmology. 2014 Jan; 121(1):193-201. (2):10.1016/j.ophtha.2013.08.011.
7. Lemos-Reis R, Moreira-Gonçalves N, Melo AB, Carneiro AM, Falcão-Reis FM. Immediate effect of intravitreal injection of bevacizumab on intraocular pressure. Clinical Ophthalmology. 2014; 8:1383–1388.
8. Kiddee W, Montriwet M. Intraocular Pressure Changes in Non-Glaucomatous Patients Receiving Intravitreal Anti-Vascular Endothelial Growth Factor Agents. Rosenbaum JT. PLoS ONE. 2015; 10(9):e0137833. doi:10.1371/journal.pone.0137833.
9. Bakri SJ, McCannel CA, Edwards AO, Moshfeghi DM. Persisent ocular hypertension following intravitreal ranibizumab. Graefes Arch Clin Exp Ophthalmol. 2008; 246:955–958.
10. Avery RL. Pieramici DJ, Rabena MD, Castellarin AA. Intravitreal bevacizumab (Avastin) for neovascular age-related macular degeneration. Ophthalmology. 2006; 113(3):363-372.e5.
11. Grismond M, Salati C, Salvetat ML. Short-term effect of intravitreal injection of ranibizumab (Lucentis) on intraocular pressure. J Glaucoma. 2009; 18:658-661.
12. Wehrli SJ, Tawse K, Levin MH, Zaidi A, Pistilli M, Brucker AJ. A lack of delayed intraocular pressure elevation in patients treated with intravitreal injection of bevacizumab and ranibizumab. Retina. 2012; 32:1295–1301.

Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:212-218
GENERAL ARTICLE
212 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.39
Non-parametric tests in detecting glaucoma progression
Pantalon Anca*, Feraru Crenguța**
*Ophthalmology Clinic, “Sf. Spiridon” University Hospital, Iași, Romania **Surgery Department, Ophthalmology Unit, “Gr. T. Popa” University of Medicine and Pharmacy, Iași, Romania Correspondence to: Pantalon Anca, MD, PhD, Ophthalmology Clinic, “Sf. Spiridon” University Hospital, Iaşi, 1 Independenței Square, Code 700115, Iaşi, Romania, Mobile phone: +40740 686 865, E-mail: [email protected] Accepted: September 8th, 2017
Abstract Automated perimetry still represents the gold standard in long term glaucoma monitoring. On a daily practice basis, glaucoma progression analysis could be difficult due to the long time needed to detect, confirm, and quantify the progression rate. Moreover, “trend” and “event” analysis require a good theoretical basis to perform and interpret. Aim of study was to present an alternative method to conventional Glaucoma Progression Analysis (Humphrey Visual Field Analyzer, Carl Zeiss® Inc.) applied for the early detection of glaucoma progression. Such an “event” analysis orients the clinician in a fast manner on the progression profile in glaucoma patients and might adapt the follow up visits accordingly. Method and material: 41 eyes from 41 patients with open angle glaucoma were studied in a longitudinal manner, over a 24 months’ time interval from diagnosis. Results: in the GPA analysis, a positive “event” (progression) was detected in 11/ 41 eyes (26.82%). Non-parametric analysis confirmed progression in all GPA cases, and additionally found 8 more eyes with positive progression (46.34% studied eyes). Mc Nemar concordance analysis between tests was good and relevant (kappa index k=0.596, p=0.000), with positive correlation (r=0.652, p=0.008). In conclusion, NPA tends to overestimate the number of progression cases in a cohort, but it can easily orient the clinician on the profile of the followed patients. In the first years, the GPA analysis can be highly inaccurate, but there is a great need to detect which patients are at significant risk for vision loss (fast progressors). Yet, combining the two methods of detection of glaucoma progression, the practitioners might direct their selected interest and attention towards observing a larger than expected number of patients who are at risk for vision loss over time due to glaucoma, but not necessarily in a fast manner. Keywords: glaucoma, progression, non-parametric analysis
Introduction
Standard automated perimetry (SAP) remains the “gold standard” method to assess functional glaucomatous damage and
progressive disease. Recent improvements in the Swedish interactive thresholding algorithm (SITA) strategy and the guided progression analysis (GPA) have further settled it as the

Romanian Journal of Ophthalmology 2017; 61(3): 212-218
213
Romanian Society of Ophthalmology © 2017
preferred method for diagnosis and follow-up of glaucomatous functional loss [1].
On a daily practice basis, glaucoma progression analysis could be difficult due to the long time needed to detect, confirm, and quantify the progression rate. Moreover, “trend” and “event” analysis require a good theoretical basis to “integrate into the clinical context” and interpret the information. As such, clinical decisions are based on more aspects than a visual field output. In this respect, more and more research is directed towards adjunctive methods of visual function assessment and progression detection (such as the non-parametric tests) in eyes with visual field loss. These types of alternative analysis could earlier direct the attention towards a selected category of patients with higher progression risk and could also enable a faster profiling for progression in some cases or “modulate” clinical decisions for the doctors in terms of good clinical practice.
“Event” analysis detects progression and it is developed from all the re-test values measured in the follow up visual field (VF) examinations, in locations with a given baseline value. Because patients included in a clinical trial are usually highly variable in response, significant deviation from the baseline is often met. Applying the non-parametric tests helps ensuring that progression is not flagged because of deviant values in highly variable individuals, improving the overall specificity [2].
The aim of the study was to present an alternative method to conventional Glaucoma Progression Analysis (Humphrey Visual Field Analyzer, Carl Zeiss® Inc.) applied for the early detection of glaucoma progression. Such an “event” algorithm (NPA) applied to the mean deviation (MD) orients the clinician in a fast manner on the progression profile in glaucoma patients and might adapt the follow up visits accordingly.
Study design: longitudinal prospective study on 41 eyes from 41 patients with primary open angle glaucoma. Subjects were enrolled over a period of 2 years (2012-2014), and then followed for the next 2 years (2014-2016) in our Glaucoma Unit at “Sf. Spiridon” University Hospital, Iasi, Romania.
Ethics: our study was performed in respect with the Declaration of Helsinki. The Ethical
Review Board of “Gr. T. Popa” University of Medicine and Pharmacy approved the study and each patient signed an informed consent.
Material and method
We included only patients newly diagnosed with primary open angle glaucoma (POAG), according to EGS criteria European Glaucoma Society [3]. POAG was defined in the presence of open anterior chamber angle on gonioscopy, glaucomatous optic disc damage on clinical examination (focal or diffuse neuroretinal rim thinning, localized notching, or nerve fiber layer defect) and corresponding visual field (VF) defects. Glaucoma severity was graded according to Hodapp criteria [4].
In Standard Automated Perimetry (24-2 SITA Standard SAP, Humphrey Field Analyzer II, Carl Zeiss Meditec Inc., Dublin, CA, USA), VF changes for glaucoma were defined if at least two of the three Anderson’s criteria were fulfilled (three or more non-edged points in a cluster depressed to P<5% and one of which depressed to P<1%, Glaucoma Hemifield Test outside normal limits and pattern standard deviation depressed to P<5%). Reliability of tests was assessed. Tests with fixation losses, false-positive or false-negative rates >20% were considered unreliable and excluded from the analysis. A minimum number of 5 valid VF tests were required for each patient in our study.
All reliable VF tests were analyzed for progression by Glaucoma Progression Analysis (GPA) software, which provides both an event-based and a trend-based progression analysis. Both analyses took the first two reliable VF tests as baseline landmark. For GPA, visual field progression was based on glaucoma change probability maps [5]. In glaucoma change probability maps, the threshold value of each test point location in every follow-up field is compared with a mean of the values from the same test point in 2 baseline fields. Points that have changed more than might be expected from random variability at P<0.05 are flagged as significantly changing. To limit the effect of increasing media opacities, GPA uses pattern deviation probability plots [6]. Likely progression is reached when 3 or more test point locations at any location in the field, not necessarily contiguous, show a significant deterioration in 3 consecutive tests. Possible progression occurs when 3 or more such locations have been identified in 2 consecutive
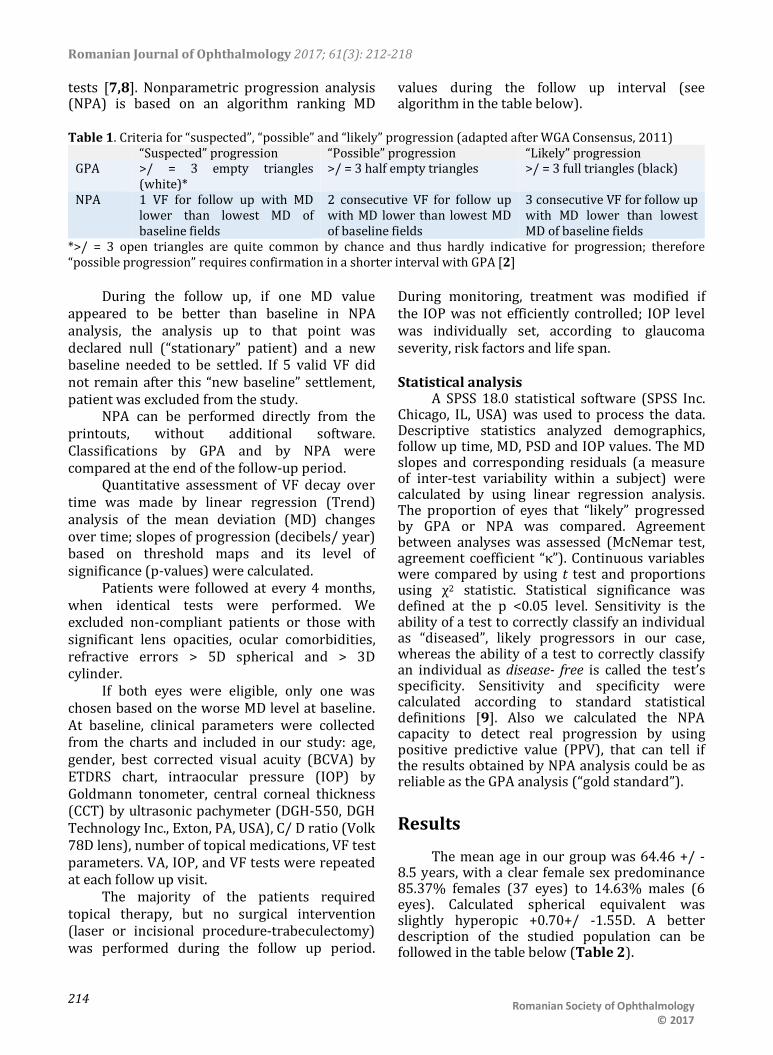
Romanian Journal of Ophthalmology 2017; 61(3): 212-218
214 Romanian Society of Ophthalmology
© 2017
tests [7,8]. Nonparametric progression analysis (NPA) is based on an algorithm ranking MD
values during the follow up interval (see algorithm in the table below).
Table 1. Criteria for “suspected”, “possible” and “likely” progression (adapted after WGA Consensus, 2011)
“Suspected” progression “Possible” progression “Likely” progression GPA >/ = 3 empty triangles
(white)* >/ = 3 half empty triangles >/ = 3 full triangles (black)
NPA 1 VF for follow up with MD lower than lowest MD of baseline fields
2 consecutive VF for follow up with MD lower than lowest MD of baseline fields
3 consecutive VF for follow up with MD lower than lowest MD of baseline fields
*>/ = 3 open triangles are quite common by chance and thus hardly indicative for progression; therefore “possible progression” requires confirmation in a shorter interval with GPA [2]
During the follow up, if one MD value appeared to be better than baseline in NPA analysis, the analysis up to that point was declared null (“stationary” patient) and a new baseline needed to be settled. If 5 valid VF did not remain after this “new baseline” settlement, patient was excluded from the study.
NPA can be performed directly from the printouts, without additional software. Classifications by GPA and by NPA were compared at the end of the follow-up period.
Quantitative assessment of VF decay over time was made by linear regression (Trend) analysis of the mean deviation (MD) changes over time; slopes of progression (decibels/ year) based on threshold maps and its level of significance (p-values) were calculated.
Patients were followed at every 4 months, when identical tests were performed. We excluded non-compliant patients or those with significant lens opacities, ocular comorbidities, refractive errors > 5D spherical and > 3D cylinder.
If both eyes were eligible, only one was chosen based on the worse MD level at baseline. At baseline, clinical parameters were collected from the charts and included in our study: age, gender, best corrected visual acuity (BCVA) by ETDRS chart, intraocular pressure (IOP) by Goldmann tonometer, central corneal thickness (CCT) by ultrasonic pachymeter (DGH-550, DGH Technology Inc., Exton, PA, USA), C/ D ratio (Volk 78D lens), number of topical medications, VF test parameters. VA, IOP, and VF tests were repeated at each follow up visit.
The majority of the patients required topical therapy, but no surgical intervention (laser or incisional procedure-trabeculectomy) was performed during the follow up period.
During monitoring, treatment was modified if the IOP was not efficiently controlled; IOP level was individually set, according to glaucoma severity, risk factors and life span. Statistical analysis
A SPSS 18.0 statistical software (SPSS Inc. Chicago, IL, USA) was used to process the data. Descriptive statistics analyzed demographics, follow up time, MD, PSD and IOP values. The MD slopes and corresponding residuals (a measure of inter-test variability within a subject) were calculated by using linear regression analysis. The proportion of eyes that “likely” progressed by GPA or NPA was compared. Agreement between analyses was assessed (McNemar test, agreement coefficient “κ”). Continuous variables were compared by using t test and proportions using χ2 statistic. Statistical significance was defined at the p <0.05 level. Sensitivity is the ability of a test to correctly classify an individual as “diseased”, likely progressors in our case, whereas the ability of a test to correctly classify an individual as disease- free is called the test’s specificity. Sensitivity and specificity were calculated according to standard statistical definitions [9]. Also we calculated the NPA capacity to detect real progression by using positive predictive value (PPV), that can tell if the results obtained by NPA analysis could be as reliable as the GPA analysis (“gold standard”).
Results
The mean age in our group was 64.46 +/ -8.5 years, with a clear female sex predominance 85.37% females (37 eyes) to 14.63% males (6 eyes). Calculated spherical equivalent was slightly hyperopic +0.70+/ -1.55D. A better description of the studied population can be followed in the table below (Table 2).

Romanian Journal of Ophthalmology 2017; 61(3): 212-218
215
Romanian Society of Ophthalmology © 2017
Table 2. Baseline parameters in the study Parameters (baseline) POAG VA (decimal) 0.82+/ -0.21 IOP baseline (mmHg) 16.69+/ -4.58 No. medications 1.68+/ -1.19 CCT (µm) 537.73+/ -27.20 C/ D ratio (clinical assessment)
0.66+/ -0.17
OCT examination C/ D ratio (vertical) 0.7+/ -0.13 Disk area (mm2) 2.02+/ -0.38 Neural rim area (mm2) 0.93+/ -0.26 RNFL thickness (µm) 78.88+/ -12.94 CGL thickness (µm) 74.44+/ -10.20 VF examination MD (db) -2.37+/ -3.24 PSD (db) 2.56+/ -1.83
Later evolution of parameters and
comparison between baseline and final values can be followed in Table 3. Table 3. Baseline vs. final parameters in the study
Parameter Initial Final p (test t) VA (decimal)
0.82+/ -0.21 0.73+/ -0.24 0.000
IOP (mmHg)
16.69+/ -4.58 14.04+/ -3.70 0.000
No. medications
1.68+/ -1.19 2.26+/ -1.28 0.001
MD (dB) -2.37+/ -3.24 -3.96+/ -4.04 0.013 PSD (dB) 2.56+/ -1.83 3.65+/ -2.63 0.007
The overall visual field decay calculated
after 24 months of follow up was -0.63 +/ - 1.12 dB/ year. The histogram of all MD values for the 41 eyes included in the study is represented in Fig. 1. MD slopes are depicted in Fig. 2 for all followed eyes.
A simple calculation of VF decline does not also reflect the degree of clinical and statistical significance. Therefore, we evaluated the presence of “likely” glaucoma progression (“event” analysis), through two different methods, independently and saw the agreement between them. For this, we followed the algorithm described in the “Material and Method” section above (Table 1). Applying the above-mentioned criteria, we found in our study that there was a considerable higher proportion of likely progressive cases by NPA analysis than GPA analysis (see Fig. 3-4).
Fig. 1 Histogram of MD values in the studied POAG patients
Fig. 2 MD slopes in all 41 eyes in the study
Fig. 3 “Likely” progression flagged by NPA analysis

Romanian Journal of Ophthalmology 2017; 61(3): 212-218
216 Romanian Society of Ophthalmology
© 2017
11 eyes were flagged as “likely progressive” by GPA analysis (26.8% eyes), whereas 19 eyes were found as “likely progressive” glaucoma damage by NPA analysis (46.34% eyes); percentages were statistically different, p<0.01. 9 eyes with a “likely” progression by GPA analysis were flagged similarly by NPA analysis, whereas 2 cases were not confirmed by NPA. A better understanding of the “likely progression” cases may be followed in the Venn diagrams below (Fig. 5).
The mean MD slope for the 11 progressive cases by GPA was -1.74+/ -1.87 dB/ year, compared to -1.83+/ -1.96 dB/ year with a positive progression by NPA analysis. The
difference was not statistically significant, p>0.05.
Kappa agreement index between the two methods (GPA/ NPA) was k=0.596, p=0.000 (Mc Nemar test), with positive medium-strong correlation (Pearson test): r=0.652, p=0.008.
Since for detecting progression SAP remains the “gold standard”, we calculated the sensitivity and specificity of NPA in relation to this. For the present study, we found that in the first two years of follow up, GPA sensitivity was 84.61% and specificity was 66.66% in our glaucoma patients. In a similar manner, we calculated the NPA sensitivity= 65.09% and NPA specificity= 90%. Positive predictive value (PPV) for GPA was 52.38%, compared to 90.47% NPA.
Discussions
In this study, we prospectively observed 41 eyes of 41 patients with POAG who were followed up by using SAP. We compared a nonparametric ranking method applied to the MD (NPA) with GPA. Most eyes flagged as showing likely progression by GPA were detected by NPA as well. In addition, some eyes were flagged as showing progression by NPA but not by GPA. Because of its design, GPA is insensitive to a general decrease in sensitivity. The development of cataract is presumably a common cause of a general decrease in sensitivity. Insensitivity to cataract is obviously an advantage in a glaucoma trial. However, in a clinical setting, patients may benefit from the fact that a clinician has to evaluate the lens before he or she can interpret perimetry results. Yet, glaucoma deficit might include diffuse loss in addition to localized deterioration, case in which GPA will not detect the changes. As such, NPA detects what GPA cannot. Some eyes were flagged by GPA without being flagged by NPA. This is not an unexpected finding because agreement between different progression detection algorithms has been shown to be less than perfect [12-16]. The agreement in this study is in line with previously published values (k=0.37 for the EMGT vs. subjective assessment [13] and k=0.40 for the Advanced Glaucoma Intervention Study vs. glaucoma change probability [15].
Fig. 4 “Likely” progression flagged by GPA analysis
Fig. 5 “Likely” progression analyzed by NPA and GPA methods in the study

Romanian Journal of Ophthalmology 2017; 61(3): 212-218
217
Romanian Society of Ophthalmology © 2017
Other drawbacks of GPA are that additional software is needed, all visual fields involved must be stored in a single perimeter (which is often challenging), and it is only available for more recent versions of the Humphrey field analyzer (Carl Zeiss Meditec Inc). For these reasons, a subjective evaluation of a series of fields is still the most widely used approach today. However, inter-observer agreement for this approach is moderate at best [10,11]. Therefore, a new approach that is simple to use and understand, objective, not dependent on software, applicable for all (static-automated) perimeters, and applicable at all disease stages, was introduced herein. This method applies nonparametric ranking to the global index mean deviation (MD) - “nonparametric progression analysis” (NPA).
The mean rate of progression in our study was -0.63 +/ - 1.12 db/ year, which is in good agreement with the rate of progression in other studies [17-20]. This rate of progression was reached with a mean intraocular pressure of 15 mm Hg during our follow-up period, similar to the intraocular pressure values in the treated arm of the EMGT study. Neither GPA nor NPA provides information regarding the speed of deterioration. Hence, after progression was diagnosed by using either technique, the amount of deterioration and its localization (toward fixation or not) should be evaluated. The algorithms warn the clinician that something is going wrong rather than telling the whole story.
In clinical practice, we advice combining the two methods discussed above in order to increase both sensitivity and specificity. In the current study, the “gold standard” in perimetric progression – GPA is more sensitive in detecting an event similar to progression than specific enough to eliminate the “false alarms”. A false positive is essentially a false alarm, which could lead to subjects being incorrectly referred, causing them unnecessary anxiety and wasting clinical time and resources, or worse still, in other pathologies, potentially having to undergo unnecessary treatment if the correct diagnosis is not made in the clinic. A false negative can have equally dire consequences; if a patient has the pathology but is not diagnosed, then this would lead to him being falsely reassured that all is well and not receiving appropriate treatment at the earliest stage of his disease [21].
In this respect, for the current study, an easy manual method – NPA might help improve this aspect and increase the specificity in detection glaucoma progression.
Conclusions
NPA tends to overestimate the progressive number in a cohort, but its purpose is to alert and orient the clinician towards the possibility of progression in the followed population. As shown in this study, NPA is an easy tool for screening likely progression in glaucoma; it can be used with any perimeter at any disease stage, without the need for additional software. NPA cannot substitute the GPA methods, but GPA analysis can be highly inaccurate, especially in the first two years due to marked learning effects and high variability in responses during tests. As such, authors suggest combining the two methods for a better glaucoma management. Since nonparametric progression analysis seems to flag more eyes as showing progression than GPA, clinicians should carefully consider their decisions before any decisions and obtain confirmations through the same method and also additional ones.
References
1. Alencar LM, Medeiros FA. The role of standard automated perimetry and newer functional methods for glaucoma diagnosis and follow-up. Indian Journal of Ophthalmology. 2011; 59(Suppl1):S53-S58. doi:10.4103/0301-4738.73694.
2. Weinreb R et al. WGA Consensus. 2011; 29. 3. Terminology and Guidelines for Glaucoma, 4rd ed.,
2008, Savona: Italy, 21,138-141. 4. Heijl A, Alm A, Bengtsson B et al. Riktlinjer för
glaukomsjukvården. 2010, Bäcklunds Media, Malmö: Sveriges Ögonläkarförening.
5. Heijl A, Lindgren G, Lindgren A et al. Extended empirical statistical package for evaluation of single and multiple fields in glaucoma: StatPac2. Perimetry Update 1990/1. New York, 1990, NY Kugler Publications, 305-315.
6. Bengtsson B, Lindgren A, Heijl A et al. Perimetric probability maps to separate change caused by glaucoma from that caused by cataract. Acta Ophthalmol Scand. 1997; 75(2)184-188.
7. Heijl A, Leske MC, Bengtsson B et al. Early Manifest Glaucoma Trial Group. Measuring visual field progression in the Early Manifest Glaucoma Trial. Acta Ophthalmol Scand. 2003; 81(3)286-293.
Romanian Journal of Ophthalmology 2017; 61(3): 212-218
218 Romanian Society of Ophthalmology
© 2017
8. Bengtsson HA, Chauhan BC et al. A comparison of visual field progression criteria of 3 major glaucoma trials in early manifest glaucoma trial patients. Ophthalmology. 2008; 115(9)1557-1565.
9. Parikh R, Mathai A, Parikh S et al. Understanding and using sensitivity, specificity and predictive values. Indian Journal of Ophthalmology. 2008; 56(1):45-50.
10. Viswanathan AC, Crabb DP, McNaught AI et al. Interobserver agreement on visual field progression in glaucoma: a comparison of methods. Br J Ophthalmol. 2003; 87(6):726-730.
11. Werner EB, Bishop KI, Koelle J et al. A comparison of experienced clinical observers and statistical tests in detection of progressive visual field loss in glaucoma using automated perimetry. Arch Ophthalmol. 1988; 106(5):619-623.
12. Heijl A, Bengtsson B, Chauhan BC et al. A comparison of visual field progression criteria of 3 major glaucoma trials in early manifest glaucoma trial patients. Ophthalmology. 2008; 115(9):1557-1565.
13. Katz J, Congdon N, Friedman DS. Methodological variations in estimating apparent progressive visual field loss in clinical trials of glaucoma treatment. Arch Ophthalmol. 1999; 117(9):1137-1142.
14. Lee AC, Sample PA, Blumenthal EZ et al. Infrequent confirmation of visual field progression. Ophthalmology. 2002; 109(6):1059-1065.
15. Nouri-Mahdavi K, Hoffman D, Ralli M et al. Comparison of methods to predict visual field progression in glaucoma. Arch Ophthalmol. 2007; 125(9):1176-1181.
16. Vesti E, Johnson CA, Chauhan BC. Comparison of different methods for detecting glaucomatous visual field progression. Invest Ophthalmol Vis Sci. 2003; 44(9):3873-3879.
17. De Moraes CG, Juthani VJ, Liebmann JM, Teng CC, Tello C, Susanna R, Ritch R. Risk factors for visual field progression in treated glaucoma patients. Arch Ophthalmol. 2011; 129:562–568.
18. Forchheimer I, de Moraes CG, Teng CC, Folgar F, Tello C, Ritch R, Liebmann JM. Baseline mean deviation and rates of visual field change in treated glaucoma patients. Eye. 2011; 25:626–632.
19. Chauhan BC, Mikelberg FS, Balaszi AG, Le Blanc RP, Lesk MR, Trope GE. Canadian Glaucoma Study - Risk factors in the progression of open angle glaucoma. Arch Ophthalmol. 2008; 126:1030-1036.
20. De Moraes CG, Liebmann J, Liebmann CA, Susanna R Jr., Tello C, Ritch R. Visual field progression outcomes in glaucoma subtypes. Acta Ophthalmol. 2013; 91:288-293.
21. Saunders LJ, Zhu H, Bunce C et al. Ophthalmic statistics note 5: diagnostic tests—sensitivity and specificity. British Journal of Ophthalmology Published Online First: 08 December 2014. doi: 10.1136/bjophthalmol-2014-306055.

Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:219-228
GENERAL ARTICLE
219 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.40
Modeling the consumer’s perception of experiential marketing in the Romanian private
ophthalmologic services Gheorghe Consuela-Mădălina, Gheorghe Iuliana-Raluca, Purcărea Victor Lorin Department of Marketing and Medical Technology, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania Correspondence to: Consuela-Mădălina Gheorghe, PhD student, Department of Marketing and Medical Technology, “Carol Davila” University of Medicine and Pharmacy, Bucharest, 8 Eroii Sanitari Blvd., Code 050474, District 5, Bucharest, Romania, Mobile phone: +40729 935 485, E-mail: [email protected] Accepted: September 8th, 2017
Abstract Introduction. The importance of experience in marketing grew, as the concept itself is very personal and difficult to measure. Experience turns out to be complicated but once placed in a context it gets significant features. As the health care competitive environment increases, marketers are looking for new and effective methods of engaging consumers by using experiential marketing strategies. Moreover, little is known about the consumers’ perceptions related to ophthalmologic services. Aim. The objective of this paper was to measure the consumer’s perception of experiential marketing in the Romanian private ophthalmologic services by using structural equation modeling. Materials and Methods. The Experiential Marketing model consisted of the following components: Sense Experience, Feel Experience, Think Experience, Act Experience and Relate Experience as well as the consequences of applying Experiential Marketing in the form of willingness to purchase a service, generating word-of-mouth communication and building consumer loyalty. The sampling method was non-probabilistic, using the snowball technique and the sample was made up of 190 people who wore eyeglasses for more than 3 years. The instrument for data collection was a self-administered questionnaire, which consisted of 2 parts: the first section contained several demographic questions and the second section encompassed closed end questions related to the perception of private ophthalmologic services from an experiential marketing perspective. All the second section questions were measured on a 5-point Likert scale ranging from 1 with Strongly Disagree to 5 to Strongly Agree. The data analysis was conducted in SPSS and the structural equation modeling was performed in WarpPLS version 6.0. Findings. There were 71.05% respondents, who appreciated the application of experiential marketing in private ophthalmologic services, followed by 18.95%, who were confused. The demographic profile of respondents encompassed the following features: females with the ages between 36 and 45, from the rural area and with a middle level of education, their private ophthalmologic consultation frequency was at every 3 months and they also declared having a stable physician.

Romanian Journal of Ophthalmology 2017; 61(3): 219-228
220 Romanian Society of Ophthalmology
© 2017
Going further with the analysis, 89.63% of the respondents admitted they were willing to buy a private ophthalmologic service based on the experiential marketing application strategies. The design of a model containing both the constituent elements of the experimental marketing and its consequences in ophthalmologic services was conducted by modeling with structural equations in WarpPLS version 6.0 software. Thus, the validity of the model was assessed with the Cronbach’s alpha coefficients, Composite reliability values, as well as with the Average Variance Extracted coefficients, and the fitness of the model was determined by using the ARS, APC, and AVIF values, respectively. According to the beta coefficients and levels of statistical significance (p<0.05), some hypotheses have been rejected or negative relationships have been established between dependent and independent variables. Conclusions. Sense experience had a negative impact on WOM and consumer loyalty, Think Experience had a negative influence on the WOM, Relate Experience had a negative impact on consumer Loyalty, as well as Relate Experience had a negative impact on willingness to purchase an ophthalmologic service. In contrast, the following positive relationships were established: Feel Experience established a positive relationship with WOM and consumer loyalty, Think Experience presented a positive impact both on consumer loyalty and on willingness to purchase an ophthalmologic service, Act Experience presented a positive impact on WOM and willingness to purchase and last, willingness to purchase an ophthalmologic service presented a positive influence on consumer loyalty and WOM. However, managers in Ophthalmology can successfully use experimental marketing strategies if they promote a story, meaning a life experience. Keywords: consumer perception, experiential marketing, private ophthalmologic services, word-of-mouth communication.
Introduction
Experience has played a core role in health care services, as today most global economies are related to the consumption of experiences. Moreover, the importance of experience in marketing grew, as the concept itself is very personal and difficult to measure. Clearly, experience turns out to be complicated but placed in a context it gets a significant feature as for example an interaction between a physician and a patient. Many specialists consider experience to be subjectively assessed as it involves a wide range of feelings and sensorial stimuli and it implies involvement at different levels [1].
As the health care competitive environment increases, marketers are looking and trying to find new and effective methods of engaging consumers.
The concept of service itself has also evolved from being considered commercial to being something that defines a lifestyle [2]. The process of purchasing a service has also led to changes in consumer’s behavior, namely, consumers are becoming more educated and demanding. In the same vein, Lindstrom stated
that most people would always want to experience touch, smell, sound, and taste, as well as visual appeal, before they buy a service, as it helps them tangibilize it [3]. At the same time, consumers have begun to frequently establish relationships between themselves and the service they desire [4]. Health care services are no exception from these features. Further, this is where, more and more often, the interest of marketing specialists for experiential marketing grows, in order to provide the service experiences that awaken all their senses and offer them a unique sensation and will remain engrained in their minds for a long period of time [5].
According to Kotler [6], there are two types of marketing: traditional marketing and modern marketing. As far as modern marketing is concerned, it overtook the traditional approach, as it focuses on both customer experience and experiential marketing. Moreover, Holbrook [7] believed that when organizations start implementing experiential marketing principles, the major focus would turn from service performance to experiences, as illustrated in Table 1.

Romanian Journal of Ophthalmology 2017; 61(3): 219-228
221
Romanian Society of Ophthalmology © 2017
Table 1. Traditional marketing versus modern marketing [8] Traditional
Marketing Modern Marketing (Experiential Marketing)
Focus Service features and benefits
Consumer experience
Scope Narrow definition of service categories and consumption
Broader consumption situation and socio-cultural context
The consumer model is based on
Rational decisions
Rational and emotional decisions
Marketer’s Approach
Analytical, verbal and quantitative
Eclectic, verbal, visual and intuitive
The main objective of this paper was to
measure the consumer’s perception of experiential marketing in the Romanian private ophthalmologic services by using structural equation modeling. As such, the following objectives have been settled: - Identifying the demographic profile of the
respondents who appreciate the application of experiential marketing in private ophthalmologic services.
- Determining the proportion of consumers who have the willingness to buy a private ophthalmologic service after they appreciate the application of experiential marketing principles.
- Elaborating a model that will encompass both the elements of experiential marketing as well as the consequences of applying its principles in private ophthalmologic services.
Conceptual framework a. Experiential marketing
The idea of experiential marketing relies on the assumption that the main strategic policies and marketing decisions concentrate not only on supply, but also on the consumption and the experience that can be shaped based on designing an entire physical environment and an operational process for its consumers to experience [9].
The vast majority of scientific literature on experiential marketing focuses on the following dimensions, which are known as strategic experiential modules (SEMs) [10]: - Sense is the dimension which refers to the
experience as perceived through the five human senses;
- Feel dimension is concerned with the consumer’s emotional engagement but how to trigger certain positive emotions in consumers may be difficult as there are differences between consumption cultures;
- Think dimension is linked to the cognitive elements of the service’s features and attributes. It relates to stimulating the service consumption by using technology and innovativeness and make consumers associate it with something different;
- Act dimension refers to consumer’s actions and their physical engagement;
- Relate dimension concentrates on the social dimension of the experience, meaning that the experience allows the consumer, through the process of consumption, to establish ties with various peers and communities.
However, most Schmitt’s work (1999) focused on the following key features of experiential marketing: - Consumer experience should replace the
functional values of services with sensory, emotional, cognitive, behavioral and relational values;
- The consumption experience should be adjusted to the socio-cultural context;
- Consumers should be considered both as rational and emotional beings and so, the consumption experience is often driven by emotions, fantasies and creativity;
- Methods and tools are eclectic, meaning that experiential marketing offers specialists the opportunity to address the consumption experience from different perspectives by using both analytical and intuitive methods.
b. Experiential marketing and consumer loyalty
Bowen and Chen (2011) [11] define consumer loyalty as the degree to which a consumer shows repeated purchasing behavior of a service as well as has a positive attitudinal behavior towards the provider. Moreover, Oliver (1999) [12] defines loyalty as a deeply held commitment to rebuy a preferred service in the
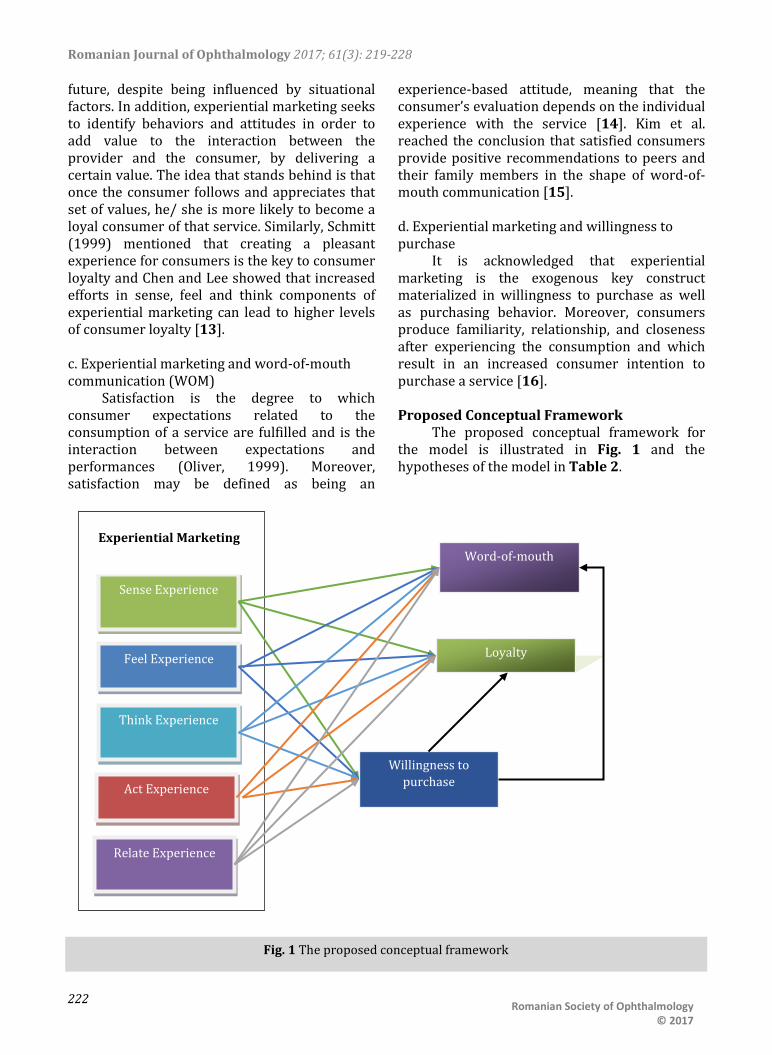
Romanian Journal of Ophthalmology 2017; 61(3): 219-228
222 Romanian Society of Ophthalmology
© 2017
future, despite being influenced by situational factors. In addition, experiential marketing seeks to identify behaviors and attitudes in order to add value to the interaction between the provider and the consumer, by delivering a certain value. The idea that stands behind is that once the consumer follows and appreciates that set of values, he/ she is more likely to become a loyal consumer of that service. Similarly, Schmitt (1999) mentioned that creating a pleasant experience for consumers is the key to consumer loyalty and Chen and Lee showed that increased efforts in sense, feel and think components of experiential marketing can lead to higher levels of consumer loyalty [13]. c. Experiential marketing and word-of-mouth communication (WOM)
Satisfaction is the degree to which consumer expectations related to the consumption of a service are fulfilled and is the interaction between expectations and performances (Oliver, 1999). Moreover, satisfaction may be defined as being an
experience-based attitude, meaning that the consumer’s evaluation depends on the individual experience with the service [14]. Kim et al. reached the conclusion that satisfied consumers provide positive recommendations to peers and their family members in the shape of word-of-mouth communication [15]. d. Experiential marketing and willingness to purchase
It is acknowledged that experiential marketing is the exogenous key construct materialized in willingness to purchase as well as purchasing behavior. Moreover, consumers produce familiarity, relationship, and closeness after experiencing the consumption and which result in an increased consumer intention to purchase a service [16]. Proposed Conceptual Framework
The proposed conceptual framework for the model is illustrated in Fig. 1 and the hypotheses of the model in Table 2.
Sense Experience
Feel Experience
Relate Experience
Think Experience
Act Experience
Word-of-mouth
Loyalty
Willingness to purchase
Experiential Marketing
Fig. 1 The proposed conceptual framework

Romanian Journal of Ophthalmology 2017; 61(3): 219-228
223
Romanian Society of Ophthalmology © 2017
Table 2. The hypotheses of the model No. Hypotheses H1 Sense Experience is positively related to the
WOM communication in private ophthalmologic services.
H2 Sense Experience is positively related to consumer loyalty in private ophthalmologic services.
H3 Sense Experience is positively related to the willingness to purchase a private ophthalmologic service.
H4 Feel Experience is positively related to the WOM communication in private ophthalmologic services.
H5 Feel Experience is positively related to consumer loyalty in private ophthalmologic services.
H6 Feel Experience is positively related to the willingness to purchase a private ophthalmologic service.
H7 Think Experience is positively related to the WOM communication in private ophthalmologic services.
H8 Think Experience is positively related to consumer loyalty in private ophthalmologic services.
H9 Think Experience is positively related to the willingness to purchase a private ophthalmologic service.
H10 Act Experience is positively related to the WOM communication in private ophthalmologic services.
H11 Act Experience is positively related to consumer loyalty in private ophthalmologic services.
H12 Act Experience is positively related to the willingness to purchase a private ophthalmologic service.
H13 Relate Experience is positively related to the WOM communication in private ophthalmologic services.
H14 Relate Experience is positively related to consumer loyalty in private ophthalmologic services.
H15 Relate Experience is positively related to the willingness to purchase a private ophthalmologic service.
H16 The willingness to purchase a private ophthalmologic service is positively related to WOM communication.
H17 The willingness to purchase a private ophthalmologic service is positively related to consumer loyalty.
Material and methods
The sampling method was non-probabilistic, using the snowball technique and the sample was made up of 190 people who wore eyeglasses for more than 3 years.
The instrument for data collection was a self-administered questionnaire which consisted of 2 parts: the first section contained several demographic questions and the second section encompassed closed end questions related to the perception of private ophthalmologic services from an experiential marketing perspective through its components. All the second section questions were measured on a 5-point Likert scale ranging from 1 with Strongly Disagree to 5 to Strongly Agree, as shown in Table 3 but modified for measuring a health care service. Table 3. The questionnaire design Construct Measurement No. of
items Source
Experiential Marketing
Sense Experience
7 Schmitt (1999)
Feel Experience
7 Schmitt (1999)
Think Experience
4 Gentile et al. (2007) [17]
Act Experience
5 Maghnati et al. (2012) [18]
Relate Experience
3 Schmitt (1999)
Consumer loyalty
4 Chen et al. (2009) [19] Chou et al. (2010) [20]
WOM 2 - Willingness to purchase
3 Soderlund and Ohman (2005) [21]
The data analysis was conducted in SPSS
and the modeling was performed in WarpPLS version 6.0. More exactly, the Structural Equation Modeling was used to test the measurement and the structural design of the model as well as the research hypotheses presented in Table 2.

Romanian Journal of Ophthalmology 2017; 61(3): 219-228
224 Romanian Society of Ophthalmology
© 2017
Findings
There were 71.05% respondents, who appreciated the application of experiential marketing in private ophthalmologic services, followed by 18.95%, who were confused. The demographic profile was that the respondents were females with the ages between 36 and 45, from the rural area and with a middle level of education. Moreover, their private ophthalmologic consultation frequency was at every 3 months and they also declared having a stable physician.
Going further with the analysis, 89.63% of the respondents admitted they were willing to buy a private ophthalmologic service based on the experiential marketing application.
The structural equation model a. Reliability measurement A review of Table 4 and Table 5 shows
several results concerning the reliability in a PLS measurement model. As such, Table 4 illustrates the Cronbach’s alpha coefficients and the composite reliability coefficients. The cutoff point for these 2 types of coefficients is recommended to be more than 0.7, however, values of 0.6 were also admitted. The average variance extracted should exceed the suggested value of 0.5 for all measures [22]. Taking into consideration the results in Table 4, it was concluded that the internal consistency of the model was assessed.
Table 4. The internal reliability of the model Construct Cronbach’s Alpha
Coefficient Values Composite Reliability
(CR) Average Variance Extracted (AVE)
Sense Experience 0.86 0.91 0.72 Feel Experience 0.81 0.89 0.73 Think Experience 0.92 0.96 0.92 Act Experience 0.87 0.91 0.73 Relate Experience 0.83 0.92 0.86 Willingness to purchase 0.72 0.84 0.74 Word-of-Mouth Communication 0.72 0.88 0.78 Consumer Loyalty 0.75 0.86 0.77
In Table 5, the Pattern Matrix confirms the existence of 8 dictinct factors that are the equivalents of the 8 latent constructs of experiential marketing. In addition, the resulted matrix also confirmed that not all the items were
still included in the model. However, the resulted Pattern Matrix from the WrapPLS analysis supports the fact that the selection of variables was optimal.
Table 5. The Pattern Matrix of the Model
sense affect think act rel int wom loi
es_it1 0.781 -0.050 -0.154 0.083 0.020 0.131 -0.152 0.086 es_it3 0.849 -0.003 0.001 -0.018 -0.061 -0.014 0.042 -0.109 es_it4 0.890 0.031 0.047 -0.018 0.013 -0.042 0.040 0.060 es_it5 0.870 0.017 0.091 -0.040 0.027 -0.063 0.057 -0.034 ea_it1 -0.058 0.809 -0.050 0.048 -0.112 0.035 0.041 0.040 ea_it3 0.098 0.869 -0.042 -0.069 0.022 -0.060 -0.019 0.019 ea_it4 -0.041 0.893 0.087 0.022 0.082 0.025 -0.020 -0.055 eg_it3 0.032 -0.023 0.963 0.014 -0.018 0.018 0.025 0.007 eg_it4 -0.032 0.023 0.965 -0.014 0.018 -0.018 -0.025 -0.007 eact_it1 -0.091 -0.036 -0.027 0.901 -0.073 0.023 0.038 0.019
eact_it3 -0.011 -0.002 -0.006 0.916 -0.043 -0.003 -0.115 0.021 eact_it4 0.021 -0.014 0.025 0.795 0.137 -0.003 0.026 -0.020 eact_it5 0.085 0.055 0.008 0.810 -0.025 -0.017 0.060 -0.021 erel_it1 -0.012 0.034 0.044 0.026 0.917 -0.016 0.063 -0.029

Romanian Journal of Ophthalmology 2017; 61(3): 219-228
225
Romanian Society of Ophthalmology © 2017
erel_it3 0.012 -0.034 -0.044 -0.026 0.939 0.016 -0.063 0.029 int_it1 -0.011 0.042 -0.111 -0.003 0.060 0.854 -0.092 -0.002 int_it2 -0.053 -0.071 0.129 -0.009 -0.086 0.715 0.035 -0.015 int_it3 0.060 0.025 -0.011 0.011 0.021 0.830 0.058 0.016 wom_it1 0.089 -0.071 -0.041 0.056 -0.135 0.070 0.891 0.000 wom_it2 -0.089 0.071 0.041 -0.056 0.135 -0.070 0.881 -0.000 loi_it1 0.030 -0.023 0.083 0.041 -0.134 -0.079 0.119 0.837 loi_it3 -0.044 -0.003 -0.022 0.006 0.072 -0.069 -0.014 0.783 loi_it4 0.009 0.026 -0.063 -0.046 0.068 0.140 -0.106 0.841
b. The fitness of the model
The goodness of fit of a PLS-based model is measured with three indices: the average path coefficient (APC), the average-R squared (ARS) and the average variance inflation factor (AVIF). For assessing the fitness of a model, the APC and ARS indices should have p values lower than 0.05, and secondly, AVIF should be lower than 5 [23] (Table 6). Table 6. The fitness indices of the model
The value of the coefficient
Level of statistical significance
The ideal value for validation
APC=0.13 P<0.01 P<0.05 ARS=0.13 P<0.01 P<0.05 AARS=0.11 P<0.02 P<0.05 AVIF=1.12 - <=3.3 AFVIF=1.17 - <=3.3
Since the validity, the reliability and the
fitness of the model have proved that it is correctly defined, the hypotheses of the model using structural equation modeling were investigated.
c. Structural Equation Modeling The PLS-Structural Equation Modeling is
based on the Partial Least Squares method and measures the connection between latent variables using beta standardize d coefficients and R square values. The PLS-SEM model, the path coefficients, their associated p values and the hypotheses’ testing are illustrated in Table 7 and Fig. 2. A refined model is presented in Fig. 3.
Table 7. Hypotheses’ statuses
No. Hypotheses β Level of statistical
significance Validation
H1 Sense experience -> WOM -0.11 0.056 NO H2 Sense experience -> consumer loyalty -0.12 0.037 YES H3 Sense experience -> willingness to purchase -0.19 0.003 YES H4 Feel experience -> WOM 0.18 0.004 YES H5 Feel experience -> consumer loyalty -0.03 0.336 NO H6 Feel experience -> willingness to purchase 0.13 0.027 YES H7 Think experience -> WOM -0.12 0.045 YES H8 Think experience -> consumer loyalty 0.31 <0.001 YES H9 Think experience -> willingness to purchase 0.12 0.041 YES H10 Act experience -> WOM 0.12 0.036 YES H11 Act experience -> consumer loyalty -0.12 0.034 YES H12 Act experience -> willingness to purchase 0.12 0.039 YES H13 Relate Experience -> WOM -0.02 0.383 NO H14 Relate experience -> consumer loyalty 0.01 0.422 NO H15 Relate experience-> willingness to purchase -0.12 0.046 YES H16 Willingness to purchase -> WOM 0.24 <0.001 YES H17 Willingness to purchase -> consumer loyalty 0.18 0.005 YES

Romanian Journal of Ophthalmology 2017; 61(3): 219-228
226 Romanian Society of Ophthalmology
© 2017
Sense Experience
Feel Experience
Relate Experience
Think Experience
Act Experience
WOM
Consumer loyalty
Willingness to purchase
Experiential Marketing
Legend:
Positive relationship
Negative relationship
Fig. 2 The resulted model in Warp PLS
Fig. 3 The refined model

Romanian Journal of Ophthalmology 2017; 61(3): 219-228
227
Romanian Society of Ophthalmology © 2017
The R2 coefficient for willingness to purchase construct was of 0.08, meaning that the experiential marketing components explain 8% of its variance, which is classified as acceptable, whereas the R2 coefficient for the WOM construct was of 0.14, meaning that the experiential marketing constructs and the willingness to purchase a private ophthalmologic service explain 14% of its variance, and the consumer loyalty construct is explained in a proportion of 20% by experiential marketing and the willingness to purchase. Overall, the model proved to be satisfactory in the context of private ophthalmologic services.
Conclusions
The respondents who appreciated the application of experiential marketing in ophthalmologic services were 71.05%, 18.95% being confused. Moreover, the participants’ demographic profile was the following: age between 36 and 45 years, females with college studies and with a frequency of ophthalmologic consultations at every 3 months.
Further, there were 89.63% of the respondents who appreciated the application of experiential marketing in ophthalmologic services and also expressed their willingness of buying the service.
The design of a model containing both the constituent elements of the experimental marketing and its consequences in ophthalmology services was conducted by modeling with structural equations in WarpPLS version 6.0 software. Thus, the validity of the model was assessed with the Cronbach’s alpha coefficients, Composite reliability values, as well as with the Average Variance Extracted coefficients and the fitness of the model was determined by using the ARS, APC, and AVIF values, respectively.
According to beta coefficients and levels of statistical significance, some hypotheses have been rejected or negative relationships have been established between dependent and independent variables. Therefore, negative relationships have been established between sensory experience and consumer loyalty, as well as sensory experience and willingness to purchase an ophthalmologic service. One
possible explanation would be that an ophthalmologic consultation does not imply a high degree of customization, the vast majority of ophthalmic organizations offer specific services under excellent conditions, and consumers no longer value the environmental elements but the perceived value of the service. Further, consumers are no longer attracted by technical and technological equipment but by other elements that give them a sense of respect, integrity, and dignity, as well as by empowering them to take part in the health decision-making process.
Moreover, affective experience influences the consumer of ophthalmic services at the level of purchasing intention and generating recommendations. The health service remains a typology that requires a lot of patient confidence but also he perceives very high risks, such as psychological risk through fear, social risk through manifestation of social aversion and marginalization of sick people, physical risk, and of course, the functional risk, namely the long waiting for the outcome to be observed. All these risks may be solved if the physician adopts an empathic attitude, as consumers of ophthalmologic services lack the necessary knowledge of understanding the specialized language. An appropriate attitude of the physician will generate a positive intention to purchase the ophthalmologic service and would raise the level of recommending the service to relatives and peers as well as on the Internet in virtual patient communities.
It is difficult to position on the ophthalmology market in Romania, as the vast majority of consumers choose the service provider according to the location. In these circumstances, the ophthalmologist managers can successfully use experimental marketing strategies if they promote a story, meaning a life experience.
References
1. Shaw C, Ivens J. Building great customer experiences, 2005, New York, MacMillan.
2. Owyang J. Disruptive technology - The new argument. Consumer relationship management magazine. 2010; 32(2),32-33.
3. Lindstrom M. Brand Sense, 2005, New York, Free Press.
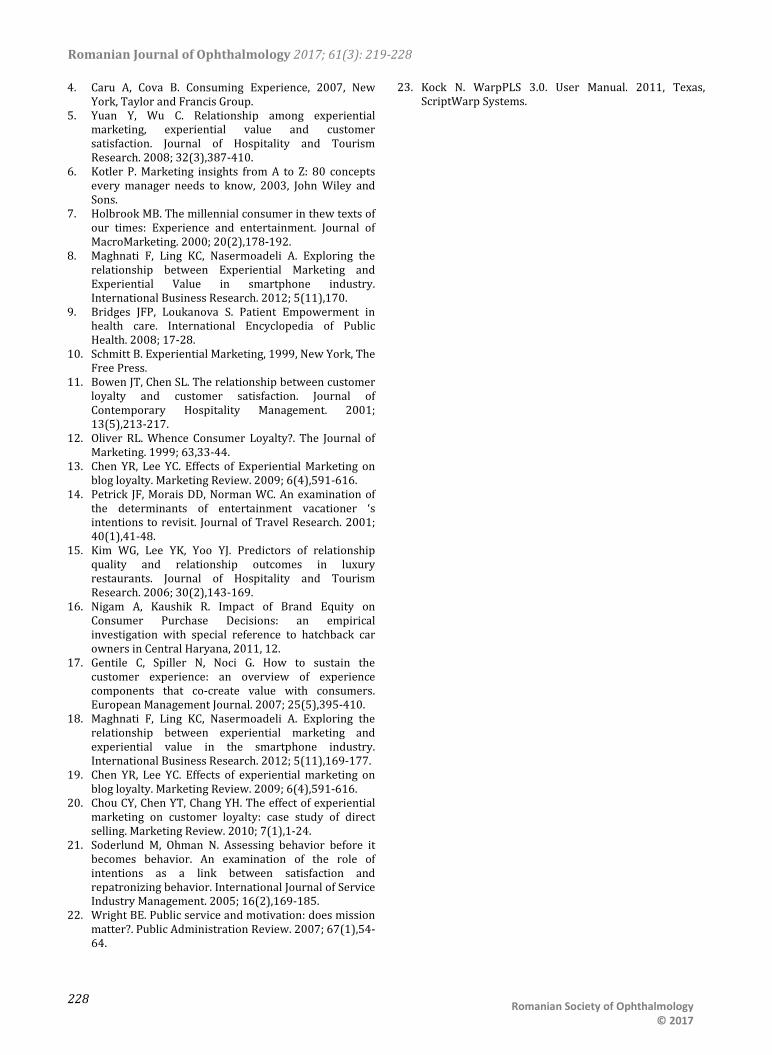
Romanian Journal of Ophthalmology 2017; 61(3): 219-228
228 Romanian Society of Ophthalmology
© 2017
4. Caru A, Cova B. Consuming Experience, 2007, New York, Taylor and Francis Group.
5. Yuan Y, Wu C. Relationship among experiential marketing, experiential value and customer satisfaction. Journal of Hospitality and Tourism Research. 2008; 32(3),387-410.
6. Kotler P. Marketing insights from A to Z: 80 concepts every manager needs to know, 2003, John Wiley and Sons.
7. Holbrook MB. The millennial consumer in thew texts of our times: Experience and entertainment. Journal of MacroMarketing. 2000; 20(2),178-192.
8. Maghnati F, Ling KC, Nasermoadeli A. Exploring the relationship between Experiential Marketing and Experiential Value in smartphone industry. International Business Research. 2012; 5(11),170.
9. Bridges JFP, Loukanova S. Patient Empowerment in health care. International Encyclopedia of Public Health. 2008; 17-28.
10. Schmitt B. Experiential Marketing, 1999, New York, The Free Press.
11. Bowen JT, Chen SL. The relationship between customer loyalty and customer satisfaction. Journal of Contemporary Hospitality Management. 2001; 13(5),213-217.
12. Oliver RL. Whence Consumer Loyalty?. The Journal of Marketing. 1999; 63,33-44.
13. Chen YR, Lee YC. Effects of Experiential Marketing on blog loyalty. Marketing Review. 2009; 6(4),591-616.
14. Petrick JF, Morais DD, Norman WC. An examination of the determinants of entertainment vacationer ‘s intentions to revisit. Journal of Travel Research. 2001; 40(1),41-48.
15. Kim WG, Lee YK, Yoo YJ. Predictors of relationship quality and relationship outcomes in luxury restaurants. Journal of Hospitality and Tourism Research. 2006; 30(2),143-169.
16. Nigam A, Kaushik R. Impact of Brand Equity on Consumer Purchase Decisions: an empirical investigation with special reference to hatchback car owners in Central Haryana, 2011, 12.
17. Gentile C, Spiller N, Noci G. How to sustain the customer experience: an overview of experience components that co-create value with consumers. European Management Journal. 2007; 25(5),395-410.
18. Maghnati F, Ling KC, Nasermoadeli A. Exploring the relationship between experiential marketing and experiential value in the smartphone industry. International Business Research. 2012; 5(11),169-177.
19. Chen YR, Lee YC. Effects of experiential marketing on blog loyalty. Marketing Review. 2009; 6(4),591-616.
20. Chou CY, Chen YT, Chang YH. The effect of experiential marketing on customer loyalty: case study of direct selling. Marketing Review. 2010; 7(1),1-24.
21. Soderlund M, Ohman N. Assessing behavior before it becomes behavior. An examination of the role of intentions as a link between satisfaction and repatronizing behavior. International Journal of Service Industry Management. 2005; 16(2),169-185.
22. Wright BE. Public service and motivation: does mission matter?. Public Administration Review. 2007; 67(1),54-64.
23. Kock N. WarpPLS 3.0. User Manual. 2011, Texas, ScriptWarp Systems.

Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:229-236
CASE REPORT
229 Romanian Society of Ophthalmology
© 2017 doi:10.22336/rjo.2017.41
Iris juvenile xanthogranuloma in an infant - spontaneous hyphema and secondary glaucoma
Pantalon Anca*, Ștefănache Tudor* **, Danciu Mihai***, Zurac Sabina****, Chiseliță Dorin* ** *Opthalmology Clinic, “Sf. Spiridon” University Hospital, Iași, Romania **Ophthalmology Unit, “Gr. T. Popa” University of Medicine and Pharmacy, Iași, Romania ***Department of Pathology, “Gr. T. Popa” University of Medicine and Pharmacy, Iași, Romania ****Department of Pathology, Faculty of Dental Medicine, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania Correspondence to: Pantalon Anca, MD, PhD, Ophthalmology Clinic, “Sf. Spiridon” University Hospital, Iaşi, 1 Independenței Square, Code 700115, Iaşi, Romania, Mobile phone: +40740 686 865, E-mail: [email protected]
Accepted: September 9th, 2017
Abstract Juvenile xanthogranuloma (JXG) is a benign histiocytic skin disorder mainly encountered during infancy and childhood. Although with multiple potential localizations, less than 1% of the cases exhibit ocular manifestations. Some of these might lead to serious complications, specifically, secondary glaucoma that can result in severe and blinding eye disease. The aim of the present case report was to demonstrate typical clinical features, emphasize the difficulties attributed when managing these patients and literature review. We present the case of 4 months old female baby with spontaneous hyphema and secondary unilateral glaucoma due to ocular JXG. The natural history and treatment of the condition were extremely difficult to handle due to multiple opinions in histopathology related to other severe conditions that resembled with the lesions detected in this case: myelomonocytic leukemia and Langerhans cell histiocytosis. Although a minority of patients with JXG have ocular involvement, recognition of this condition is important because a treatment delay can lead to serious complications, such as glaucoma and spontaneous hyphema, as in our case. A thorough differential diagnosis represents the key to a proper management plan in these patients, both on short and long term. “Triple disease” defined as JXG plus neurofibromatosis type 1 (NF-1) and juvenile chronic myelogenous leukemia (JCML) has been reported, but it was not confirmed in our patient. Keywords: juvenile xanthogranuloma, secondary glaucoma, infant, spontaneous hyphema
Introduction
Juvenile xanthogranuloma (JXG) is a benign non-Langerhans histiocytic skin disorder mainly affecting infants and children, 75% of the cases
occurring in the first 9 months of life [1]. In 5–17% of the cases, the skin lesions may appear soon after birth [2]. About 10% of the cases can manifest in adulthood, being known as “adult xanthogranuloma” [1]. The etiology is unknown,

Romanian Journal of Ophthalmology 2017; 61(3): 229-236
230 Romanian Society of Ophthalmology
© 2017
although it may represent a reactive process (physical or infectious) [3,4]. Cutaneous lesions are asymptomatic and generally appear spontaneously during the first year of life as reddish-yellow nodules, most often in the head and neck region. The general tendency is towards spontaneous resolution until the age of 3-6 years old [3]. Extra-cutaneous JXG most commonly affects the eye but can involve the brain, lungs, liver, spleen, and other sites. Eye involvement (iris, choroid, retina, optic nerve, and orbit) has been reported to occur in approximately 0.3% to 10% of the children with cutaneous JXG [5]. Solitary lesions are found in 60–82% of the cases [1]. Among ocular sites, iris has been most commonly involved; some cases might lead to serious complications, from spontaneous intraocular hemorrhages, secondary glaucoma to blinding eye disease.
Contrary to other xanthomatous diseases, JXG has not been associated with lipid disturbances or metabolic disorders [6], but a variety of systemic diseases, including neurofibromatosis type 1 and juvenile chronic myelogenous leukemia, which may be associated with juvenile xanthogranuloma. Patients with this combination of findings require special management.
Case report
We present the case of a 4 months old female baby referred to our ophthalmology unit by a fellow colleague for unilateral red eye, photophobia, epiphora, and spontaneous hyphema (OD). As a personal history, soon after birth (at 2 weeks), the mother recalled the appearance of few red-orange cutaneous nodules (thorax, head, neck); in time, lesions became more numerous and some changed aspect due to crust formation or mild superficial hemorrhages. As such, a dermatologist was consulted and skin biopsies from the lesions were indicated. The diagnosis established by several pathologists varied greatly, from Langerhans cells histiocytosis to myelomonocytic leukemia or juvenile xanthogranuloma (JXG). Due to this situation, the baby underwent a bone marrow biopsy that excluded any malignant process and pleaded for cutaneous JXG. At this stage, no treatment was indicated, except for observation.
At 3 months, the mother noticed a color change in the OD appearance in her baby and
addressed an ophthalmologist, who found the above-mentioned changes (photophobia, epiphora, and spontaneous hyphema) at the clinical examination and sent the child to a tertiary center for further investigations.
The general clinical examination was completely normal, except for the numerous cutaneous nodules (Fig. 1a,b,c), varying in color from yellowish to bright red, mostly spread onto the head/ neck region and thorax. Fewer lesions were noted on the arms and legs. All further investigations (complementary exams, laboratory findings, and imaging scans) were within the normal limits and revealed neither lesions onto the internal organs, nor the presence of any other systemic alteration.
In the ophthalmology exam, we found visual acuity in both eyes “fixes and follows” and, under general anesthesia, IOP-OD = 25 mmHg and IOP OS =12 mm Hg. Corneal diameter was increased in OD (12 mm) and normal in OS (10 mm), aspect which coincided with increased axial lengths in OD (19.12 mm) compared to OS (18.49 mm) by “A” scan ultrasound methods.
Anterior segment examination found all structures with normal appearance in OS, while in OD there were visible changes such as: mild epithelial corneal edema, peripheral iris synechiae/ 360*, thick fibrinoid membrane on the surface of the iris, 2mm hyphema and a wide blood clot on the surface of the iris (11-4 o’clock meridians) – Fig. 2. Fundus examination could not be performed in OD due to low visibility, whereas OS aspect was normal. B scan ultrasound examination in OD detected no abnormalities in the choroid, retina, or optic nerve (Fig. 3).
Fig. 1 a,b,c Numerous cutaneous nodules, varying in color from yellowish to bright red, mostly spread onto the head/ neck region and thorax; fewer lesions were noted on the arms and legs

Romanian Journal of Ophthalmology 2017; 61(3): 229-236
231
Romanian Society of Ophthalmology © 2017
Based on all these findings we established the diagnosis of OD - Pediatric secondary inflammatory glaucoma in the context of juvenile xanthogranuloma with ocular (iris) involvement. Short course of topical corticosteroids (dexamethasone) and close monitoring for the next 3 weeks was indicated. Since no improvement was detected within this interval and persistent hyphema, fibrinoid iris membrane (more dense in inferonasal quadrant) were present, surgical intervention became
mandatory in order to avoid future and more severe complications in this child.
In this respect, augmented trabeculectomy with mitomycin C (0.02%, 3 minutes) and trabeculotomy were performed in November 2016. Fig. 4 depicts the most important surgical steps. Surgery was uneventful and the outcome is presented in Fig. 5.
The thick plaque extracted from the surface
of the iris together with the tissue resulted from the peripheral iridectomy (at 12 o’clock) were sent to histology examination, including immunohistochemistry markers.
Fig. 2 Anterior segment (OD)
Fig. 3 OD-B scan revealed normal structures; no JXG suggestive lesions appeared in the retina, choroid, optic nerve Fig. 4 OD Augmented trabeculectomy with
mitomycin C (0.02%, 3 minutes) and trabeculotomy; difficult rotation in the anterior chamber of the trabeculotomes due to the fibrinoid membrane adherent to the iris root in the AC angle; removal of the iris fibrinoid membrane, mild hemorrhage after removal, patient 12 o’clock peripheral iridectomy
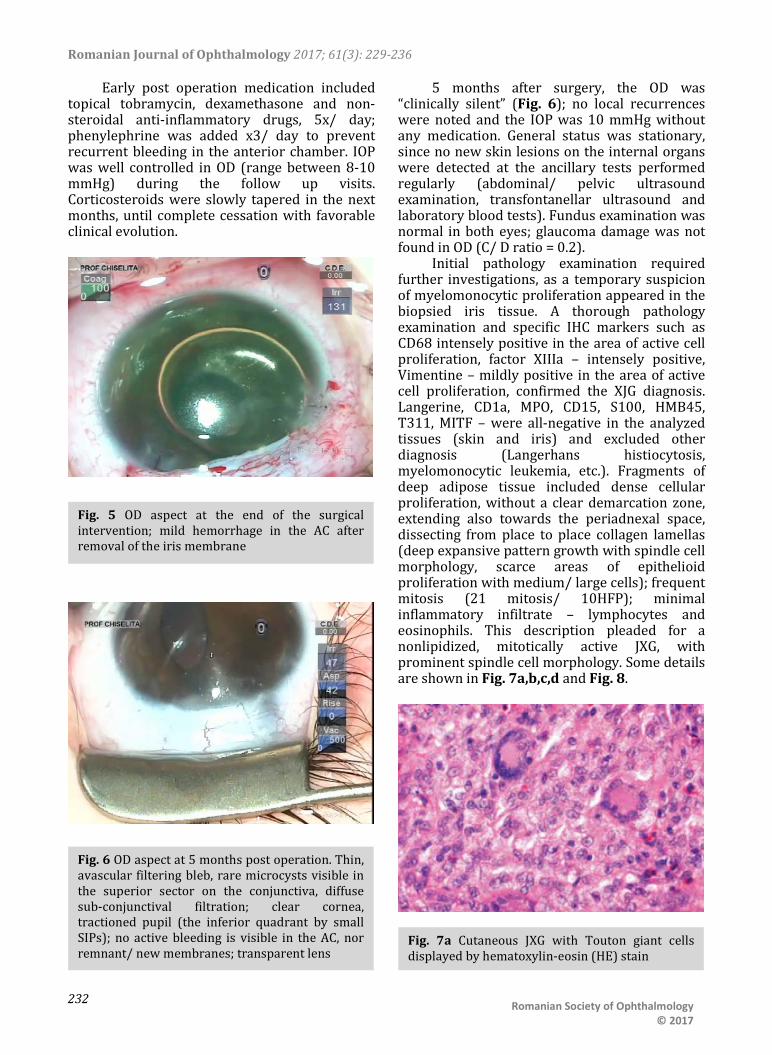
Romanian Journal of Ophthalmology 2017; 61(3): 229-236
232 Romanian Society of Ophthalmology
© 2017
Early post operation medication included topical tobramycin, dexamethasone and non-steroidal anti-inflammatory drugs, 5x/ day; phenylephrine was added x3/ day to prevent recurrent bleeding in the anterior chamber. IOP was well controlled in OD (range between 8-10 mmHg) during the follow up visits. Corticosteroids were slowly tapered in the next months, until complete cessation with favorable clinical evolution.
5 months after surgery, the OD was “clinically silent” (Fig. 6); no local recurrences were noted and the IOP was 10 mmHg without any medication. General status was stationary, since no new skin lesions on the internal organs were detected at the ancillary tests performed regularly (abdominal/ pelvic ultrasound examination, transfontanellar ultrasound and laboratory blood tests). Fundus examination was normal in both eyes; glaucoma damage was not found in OD (C/ D ratio = 0.2).
Initial pathology examination required further investigations, as a temporary suspicion of myelomonocytic proliferation appeared in the biopsied iris tissue. A thorough pathology examination and specific IHC markers such as CD68 intensely positive in the area of active cell proliferation, factor XIIIa – intensely positive, Vimentine – mildly positive in the area of active cell proliferation, confirmed the XJG diagnosis. Langerine, CD1a, MPO, CD15, S100, HMB45, T311, MITF – were all-negative in the analyzed tissues (skin and iris) and excluded other diagnosis (Langerhans histiocytosis, myelomonocytic leukemia, etc.). Fragments of deep adipose tissue included dense cellular proliferation, without a clear demarcation zone, extending also towards the periadnexal space, dissecting from place to place collagen lamellas (deep expansive pattern growth with spindle cell morphology, scarce areas of epithelioid proliferation with medium/ large cells); frequent mitosis (21 mitosis/ 10HFP); minimal inflammatory infiltrate – lymphocytes and eosinophils. This description pleaded for a nonlipidized, mitotically active JXG, with prominent spindle cell morphology. Some details are shown in Fig. 7a,b,c,d and Fig. 8.
Fig. 5 OD aspect at the end of the surgical intervention; mild hemorrhage in the AC after removal of the iris membrane
Fig. 6 OD aspect at 5 months post operation. Thin, avascular filtering bleb, rare microcysts visible in the superior sector on the conjunctiva, diffuse sub-conjunctival filtration; clear cornea, tractioned pupil (the inferior quadrant by small SIPs); no active bleeding is visible in the AC, nor remnant/ new membranes; transparent lens
Fig. 7a Cutaneous JXG with Touton giant cells displayed by hematoxylin-eosin (HE) stain

Romanian Journal of Ophthalmology 2017; 61(3): 229-236
233
Romanian Society of Ophthalmology © 2017
Discussions
Histiocytic disorders consist mainly in two types: Langerhans cell histiocytosis (LCH) and non-Langerhans cell histiocytosis (non-LCH). JXG is a rare disorder, but it is the most common among the non-LCH forms, with benign evolution [5]. Lesions appear spontaneously, during the 1st year of life; as it was the case of our patient, and resolve spontaneously later in childhood. The most frequent areas involved are the head and neck region, but extracutaneous lesions are also described [3,5]. Organ involvement is very rare and happens predominantly in patients with multiple skin nodules, as the case we presented hereby [7]. The majority of the patients with ocular lesions are young children typically younger than 1 year, similar to the 4 months old baby, subject of this case report. Ocular lesions usually involve the iris, but have also been reported in the orbit, optic nerve, retina, and choroid [8,9]. Iridocyclitis, hyphema, and secondary glaucoma are frequent presenting signs [10] and represent serious complications that may cause blindness if unrecognized or left untreated [11]. Zimmerman identified 5 clinical patterns for intraocular involvement in infants and young children: asymptomatically localized or diffuse iris tumor, unilateral glaucoma, spontaneous hyphema, red eye with signs of uveitis and congenital/ acquired iris
Fig. 7b Cutaneous JXG with CD68 +++ IHC stain
Fig. 7c Cutaneous JXG with S-100 negative IHC stain
Fig. 7d Cutaneous JXG with CD1a negative IHC stains
Fig. 8 Histology exam (iris) biopsy. Hematoxylin-Eosin (HE) staining, ×25; detail, ×200). Diffuse iris infiltration of lymphocytes (monocytes); nodular aggregates on the anterior surface of the iris (histiocytes)

Romanian Journal of Ophthalmology 2017; 61(3): 229-236
234 Romanian Society of Ophthalmology
© 2017
heterochromia. All these signs [12] were found in our patient.
Microscopically, the ocular tumor cells are rich in cytoplasm, which is light and eosinophilic or fine granular-like. The nucleoli are round or kidney-shaped. Most of the cells are mononuclear, and some can see two or three unclear nucleoli. The number of Touton cells is decreased compared to skin JXG lesions or even missing; inflammatory cells are also rare [13]. This could lead to some degree of confusion for inexperienced pathologists.
Microscopy of skin lesions in JXG describes a diffuse invasion of numerous tissue cells accompanied by a small amount of lymphocytes and eosinophils that can be seen in the early stage of JXG. Some tissue cells have light and hollow cytoplasm, and the nucleus is small in round or ovoid shape without atypia. In some cells, the nuclear groove and an unclear nucleus can be seen, which are often absent in Touton cells. Invasion of foam cells, foreign body giant cells and Touton giant cells can be seen in mature stage. The nucleus of Touton cell is garland-like, which is the typical characteristic of juvenile xanthogranuloma. A lot of fibroblasts are visible at the late stage, and fibrosis replaces the infiltration [13]. Collecting tissue samples from different stages of the skin lesions might lead to different descriptions in the same patient, as it was in our case.
The differential diagnosis relies on the immunohistochemical study. JXG lesions classically stain with macrophage markers including CD68 or Ki-M1P and anti F XIIIa, vimentin and often anti-CD4. As such, JXG expresses CD68, lysozyme and FXIIIa, but not CD1a. LCH expresses S-100 protein and CD1a, but not CD68, lysozyme and FXIIIa. CD1a is a relatively specific marker for LCH and it is not expressed in non-LCH diseases [14].
In our case, multiple biopsies were collected and various interpretations were given. According to Dehner, neither factor XIIIa negativity, nor S-100 positivity should preclude the diagnosis of JXG [15]. Therefore, the first attempt to characterize the skin biopsy fragments was made, a diagnosis of Lanherhans Cells Histiocytosis was discussed, based on CD68+++, CD 45+, MPO+, CD1a-, S-100-, desmin -, MY14-. Further IHC exams stated that elements such as positive markers for histiocytes and
monocytes (CD68+++ and CD14+), Langerine- and CD1a – could exclude HCL or another tumor with dendritic undetermined cells, that are usually Langerine -, but CD1a+. Spindle cell morphology, corroborated with fascein+, FXIIIa- could exclude a myelomonocytic proliferation. Third and most comprehensive IHC evaluation showed positive markers such as CD 68 (+++), factor XIIIa(++), Vimentine (+), whereas Langerine, CD1a, MPO, CD15, S-100, HMB45, T311, MITF were all negative. All the above-mentioned IHC markers are consistent with JXG characteristics.
In most cases with JXG, S-100 protein is non reactive, but scattered cells may show weak cytoplasmic reactivity, unlike the more diffuse and intense reaction of Langerhans cells [16]. Probably this was the reason for the initial confusion that was made with malignancies that required a bone marrow biopsy in this child at 3-4 weeks after birth.
JXG lesions beyond skin have different histological characteristics with cutaneous JXG, and are easy to be confused with Langerhans cell histiocytosis (LCH) [17], therefore the confusion in this case, when an iris fragment was analyzed; yet, JXG and LCH might be found simultaneous in the same patient [18]. A “triple disease” (18% of the cases) defined as JXG plus neurofibromatosis type 1 (NF-1) and juvenile chronic myelogenous leukemia (JCML) has been reported, but it was not confirmed in our patient.
From the three characteristic histologic patterns of JXG: early JXG (EJXG), classic JXG (CJXG), and transitional JXG (TJXG) [19,20], we found elements consistent for all forms in our patient: CJXG due to abundant vacuolated, foamy histiocytes with Touton giant cells, TJXG due to predominance of spindle-shaped cells resembling benign fibrous histiocytoma with foamy histiocytes and EJXG forms due to cells with little lipid and relatively more mitoses than the others. The high number of mitosis found in our case of non-lipidized JXG could be explained by the immature or evolving character of this histologic subtype.
Regarding the therapeutic options, patients with a single or only a few lesions need no therapy; excisional biopsy can be considered, but only for cosmetic reasons. Due to potential blinding complications, treatment of iris JXG should be promptly considered. Usually,

Romanian Journal of Ophthalmology 2017; 61(3): 229-236
235
Romanian Society of Ophthalmology © 2017
corticosteroids are the main stay of treatment, but refractory cases have been described, therefore an escalation of treatment needs to be approached, if the patient’s status deteriorates and the disease progresses despite conventional treatment. Surgery serves both diagnosis and treatment, since it provides a tissue specimen and excisional biopsy is curative, since the lesions once excised do not recur [21]. Refractory cases or for the patients who have systemic disease require radiotherapy (low dose) or chemotherapy similar to LCH protocols [22]. Glaucoma surgery (trabeculectomy and trabeculotomy) was “curative” for the iris JXG in this patient, and prevented complications of intraocular inflammation and increased IOP. Postoperatory management included only topical corticosteroids and NSAID with positive outcome during the follow up period. We recorded no recurrence, either local or systemic in this patient, but still, a close monitoring is needed in this child.
Conclusions
We presented a difficult case of a mitotically active JXG in iris and skin that requested multidisciplinary approach, involving an ophthalmologist, pathologist, pediatrician, dermatologist, etc. After treating the ocular complication, the situation was declared temporarily stable, but the long-term prognosis is yet guarded and further monitoring is needed.
Although JXG is described as a benign tumor, some histological aspects might be confounders for inexperienced pathologists; therefore, the definitive diagnosis should be made only by IHC markers just to avoid errors.
As general recommendation we advice the ophthalmology fellows to consider the JXG diagnosis in every case of spontaneous hyphema they find in infants and young children, since spontaneous hyphema is the most common presentation in ocular JXG in this range of age. Treatment should be promptly considered to avoid potential blinding complications.
References
1. Batista AC, Mendonc EF, Arantes Elias LS et al. Nonlipidized juvenile xanthogranuloma: An unusual
variant with a potential diagnostic pitfall. International Journal of Pediatric Otorhinolaryngology. 2012; 76:295–299.
2. Cohen BA, Hood A. Xanthogranuloma: report on clinical and histological findings in 64 patients. Pediatr Dermatol. 1989; 6:262–6.
3. Seo IS, Min KW, Mirkin LD. Juvenile xanthogranuloma. Ultrastructural and immunocytochemical studies. Arch Pathol Lab Med. 1986; 110:911–5.
4. Esterly NB, Sahihi T, Medenica M. Juvenile xanthogranuloma. An atypical case with study of ultrastructure. Arch Dermatol. 1972; 105:99–102.
5. Samara Wasim A et al. Juvenile Xanthogranuloma Involving the Eye and Ocular Adnexa. Ophthalmology. 122(10):2130–2138.
6. Szczerkowska-Dobosz A, Kozicka D, Purzycka-Bohdan D et al. Juvenile xanthogranuloma: a rare benign histiocytic disorder. Advances in Dermatology and Allergology/PostȩpyDermatologii i Alergologii. 2014; 31(3):197-200.
7. Chang MW, Frieden IJ, Good W. The risk intraocular juvenile xanthogranuloma: survey of current practices and assessment of risk. J Am Acad Dermatol. 1996; 34:445–9.
8. Shields CL, Shields JA, Buchanon HW. Solitary orbital involvement with JXG. Arch Ophthalmol. 1990; 1081587-1589.
9. Wertz FD, Zimmerman LE, McKeown CA et al. JXG of the optic nerve, disc, retina, and choroid. Ophthalmology. 1982; 891331-1335.
10. Zimmerman LE. Ocular lesions of JXG. Am J Ophthalmol. 1965; 601011-1035.
11. Chang MW, Frieden IJ, Good W. The risk intraocular juvenile xanthogranuloma: survey of current practices and assessment of risk. J Am Acad Dermatol. 1996; 34:445–9.
12. Zimmerman LE. Ocular lesions of juvenile xanthogranuloma. Nevoxanthoedothelioma. Am J Ophthalmol. 1965 Dec; 60(6):1011-35.
13. Parmley VC, George DP, Fannin LA. Juvenile Xanthogranuloma of the Iris in an Adult. Arch Ophthalmol. 1998; 116(3):377–379.
14. Carstensen H, Ornvold K, Ugeskr L. Langerhans-cell histiocytosis (histiocytosis X in children). 1993 Jun 7; 155(23):1779-83.
15. Tomaszewski MM, Lipton GP. Unusual expression of S-100 protein in histiocytic neoplasms. J Cutan Pathol. 1998; 25:129–135.
16. Dehner LP. Juvenile xanthogranuloma in the first decades of life. A clinicopathologic study of 174 cases with cutaneous an extracutaneous manifestations. Am J Surg Pathol. 2003; 5:579–593.
17. Kuo FY, Eng HL, Chen SH, Huang HY. Intramuscular juvenile xanthogranuloma in an adult: a case report with immunohistochemical study. Arch Pathol Lab Med. 2005 Feb; 129(2):e31-4.
18. Fassina A, Olivotto A, Cappellesso R, Vendraminelli R, Fassan M. Fine-needle cytology of cutaneous juvenile xanthogranuloma and langerhans cell histiocytosis. Cancer Cytopathology. 2011; 119:134–140.
19. Janssen D, Harms D. Juvenile xanthogranuloma in childhood and adolescence: a clinicopathologic study of

Romanian Journal of Ophthalmology 2017; 61(3): 229-236
236 Romanian Society of Ophthalmology
© 2017
129 patients from the kiel pediatric tumor registry. Am. J Surg. Pathol. 2005c; 29,21-28.
20. Janssen D, Harms D. Juvenile xanthogranuloma in childhood and adolescence: a clinicopathologic study of 129 patients from the kiel pediatric tumor registry. Am. J Surg. Pathol. 2005d; 29,21-28.
21. Janssen D, Harms D. Juvenile xanthogranuloma in childhood and adolescence: a clinicopathologic study of 129 patients from the kiel pediatric tumor registry. Am. J Surg. Pathol. 2005a; 29,21-28.
22. Stover DG. Treatment in juvenile xantogranuloma. Pediatr Blood Cancer. 51(1),130-133.