Role of Stem Cell Transplantation in the Treatment of Ulcerative Colitis
180
Introduction and Aim of the Work - 1 - Introduction Inflammatory bowel disease (IBD) represents a group of idiopathic chronic inflammatory intestinal conditions. The two main disease categories are Crohn's disease (CD) and ulcerative colitis (UC), with both overlapping and distinct clinical and pathological features (Charles, et al., 2009). Ulcerative colitis is a chronic disease leading to inflammation of the colon and in more severe degrees even causing painful ulcers in the colon which can bleed, cause mucous production and infection. Symptoms can recur or be minimal for months and years. Common symptoms include bloody diarrhea, abdominal pain and weight loss which may be mild to severe and affect individual's quality of life (Lakatos PL, et al., 2007). In a meta-analysis performed by Mayo Clinic, incidence of ulcerative colitis was reported as 2 to 14 per thousand person-years (Mahid, et al., 2006). The disease pathogenesis is still incompletely understood. The genetic and environmental factors such as altered luminal bacteria and enhanced the intestinal permeability play a role in the dysregulation of intestinal immunity, leading to the gastrointestinal injury (Ricart E, et al., 2010).
-
Upload
mohammed-fathy -
Category
Health & Medicine
-
view
90 -
download
3
Transcript of Role of Stem Cell Transplantation in the Treatment of Ulcerative Colitis

Introduction and Aim of the Work
- 1 -
Introduction
Inflammatory bowel disease (IBD) represents
a group of idiopathic chronic inflammatory intestinal
conditions. The two main disease categories are
Crohn's disease (CD) and ulcerative colitis (UC),
with both overlapping and distinct clinical and
pathological features (Charles, et al., 2009).
Ulcerative colitis is a chronic disease leading to
inflammation of the colon and in more severe degrees even
causing painful ulcers in the colon which can bleed, cause
mucous production and infection. Symptoms can recur or
be minimal for months and years. Common symptoms
include bloody diarrhea, abdominal pain and weight loss
which may be mild to severe and affect individual's quality
of life (Lakatos PL, et al., 2007).
In a meta-analysis performed by Mayo Clinic,
incidence of ulcerative colitis was reported as 2 to 14 per
thousand person-years (Mahid, et al., 2006).
The disease pathogenesis is still incompletely
understood. The genetic and environmental factors
such as altered luminal bacteria and enhanced the
intestinal permeability play a role in the dysregulation
of intestinal immunity, leading to the gastrointestinal injury
(Ricart E, et al., 2010).

Introduction and Aim of the Work
- 2 -
Standard medical therapy is directed against the
inflammatory and immune processes that are known to play
an important role in the disease process. Medical therapy is
of variable success in ameliorating cardinal symptoms of
the disease (diarrhea, abdominal pain), in treating extra
intestinal manifestations, and in preventing complications
(Ricart E, et al., 2010).
Currently, therapy is most often implemented in
a stepwise fashion, progressing through amino salicylates
[sulfasalazine, mesalazine (mesalamine)], corticosteroids,
immunosuppressive medications including tioguanine
(thioguanine) compounds (mercaptopurine, azathioprine),
methotrexate, and ciclosporin, and finally anti-TNF drugs.
This common approach is predicated on the addition of
more potent medications to agents that are believed
to be safer but that may also be less effective
(Ricart E, et al., 2010).
Primary and secondary failure to respond to
approved therapies and, in some cases, inability to provide
a surgical solution to a particular patient due to extension
and \ or location of lesions represents unmet needs in the
treatment of IBD (Ricart E, et al., 2010).
A novel and exciting approach could be offered
through the current development in the field of
stem cell biology (Masson, et al, 2004).
Consequently, bone marrow stem cells have been
sought of as a promising new approach capable of
addressing mostly unmet medical needs (Weissman, 2000).

Introduction and Aim of the Work
- 3 -
The considerable excitement surrounding the stem
cell field is based on the unique biological properties of
these cells and their capacity to self-renew and regenerate
tissue and organ systems, a flurry of studies reported bone
marrow derived stroma to brain, bone marrow to
liver, skin to brain, brain to heart and other such
stem cells differentiation (Morrison, 2000).
Two streams of research, experimental and clinical,
are the origin of the increasing utilization of stem cell
therapies for severe immune-mediated diseases (IMIDs)
including IBD. The considerable excitement surrounding
the stem cell field was initially based on the unique
biological properties of these cells; later, the
immunomodulatory ability of stem cell therapy has become
also apparent (Ricart E, et al., 2010).

Introduction and Aim of the Work
- 4 -
Aim of the Work
To investigate the role of autologous bone marrow
stem cells intravenous injection in treatment for cases of
ulcerative colitis disease.

Ulcerative Colitis Chapter 1
- 5 -
Ulcerative Colitis
Inflammatory bowel disease:
Inflammatory bowel disease (IBD) commonly refers
to ulcerative colitis (UC) and Crohn's disease (CD), which
are chronic inflammatory diseases of the GI tract of
unknown etiology (Hyams, 2002).
Ulcerative colitis is characterized by diffuse mucosal
inflammation limited to the colon. It is classified according
to the maximal extent of inflammation observed at
colonoscopy, while Crohn's disease is characterized by
patchy, trans mural inflammation, which may affect any
part of the gastrointestinal tract, it may be defined by: age
of onset, location, or behavior (Silverberg, et al., 2005).
In particular, the definitions of ulcerative colitis
and Crohn's disease acknowledge the revised
Montreal classification which attempts to more
accurately characterize the clinical patterns of IBD
(Satsangi, et al., 2006).
Unclassified (IBDU) is the term best suited for the
minority of cases where a definitive distinction between
UC, CD, or other cause of colitis cannot be made after
considering clinical, radiological, endoscopic and
pathological criteria, because they have some features of
both conditions. Indeterminate colitis (IC) is a term
reserved for pathologists to describe overlapping features in
IBDU (Satsangi, et al., 2006).

Ulcerative Colitis Chapter 1
- 6 -
Ulcerative colitis:
Ulcerative colitis is a lifelong disease arising from an
interaction between genetic and environmental factors,
observed predominantly in the developed countries of the
world. The precise etiology is unknown and therefore
medical therapy to cure the disease is not yet available
(Dignass, et al., 2012).
It is a chronic inflammatory condition causing
continuous mucosal inflammation of the colon without
granulomas on biopsy, affecting the rectum and a variable
extent of the colon in continuity, which is characterized by
a relapsing & remitting course (Silverberg, et al., 2005).
Clinical disease activity is grouped into remission,
mild, moderate and severe. This refers to biological
activity and not to treatment responsiveness
(Rice-Oxley and Truelove, 1950).
The term severe colitis (or „acute severe colitis‟) is
preferred to „fulminant‟ colitis, because the term
„fulminant‟ is ill-defined. Severe colitis as defined
according to Truelove and Witt's' criteria is easy to apply in
outpatients, mandates hospital admission for intensive
treatment and defines an outcome (only 70% respond to
intensive therapy) (Dignass, et al., 2012).
Response is defined as clinical and endoscopic
improvement, depending on the activity index used.
In general, this means a decrease in the activity index
of >30%, plus a decrease in the rectal bleeding and
endoscopy sub scores, but there are many permutations
(D'Haens, et al., 2007).

Ulcerative Colitis Chapter 1
- 7 -
The term relapse is used to define a flare of
symptoms in a patient with established UC who is in
clinical remission, either spontaneously or after medical
treatment. It is considered when a combination of rectal
bleeding with an increase in stool frequency and abnormal
mucosa at sigmoidoscopy are present. It may be infrequent
(≤1/year), frequent (≥2 relapses/year), or continuous
(persistent symptoms of active UC without a period of
remission) (D'Haens G et al., 2007).
The term „chronic active disease‟ has been used in
the past to define a patient who is dependent on, refractory
to, or intolerant of steroids, or who has disease activity
despite immunomodulators. Since this term is ambiguous it
is best avoided. Instead, arbitrary, but more precise
definitions are preferred, including steroid-refractory or
steroid-dependence (Van Assche, et al., 2010).
Steroid-refractory colitis if patients have active
disease despite prednisolone up to 0.75 mg/kg/day over a
period of 4 weeks. Steroid-dependent colitis patients who
are either unable to reduce steroids below the equivalent of
prednisolone 10 mg/day within 3 months of starting
steroids, without recurrent active disease, or who have
a relapse within 3 months of stopping steroids
(Van Assche, et al., 2010).
Immunomodulator-refractory colitis patients who
have active disease or relapse in spite of thiopurines at an
appropriate dose for at least 3 months (i.e. azathioprine 2–
2.5 mg/kg/day or mercaptopurine 1– 1.5 mg/kg/day in the
absence of leucopenia) (Dignass, et al., 2012).

Ulcerative Colitis Chapter 1
- 8 -
Classifications:
A. Classification according to disease extent
The preferred classification is an endoscopic
classification as outlined in the Montréal classification
into ulcerative proctitis (limited to the rectum), left-sided
colitis (up to the splenic flexure) and extensive colitis, and
by maximal extent upon follow up (Dignass, et al., 2012).
There are several reasons why patients with UC
should be classified according to disease extent. The extent
of inflammation will influence the patient's management
and the choice of delivery system for a given therapy. For
instance, topical therapy in the form of suppositories (for
proctitis) or enemas (for left-sided colitis) is often the first
line choice, but oral therapy often combined with
topical therapy is appropriate for extensive colitis.
Also, it influences start and frequency of surveillance
(Dignass, et al., 2012).
Table (1): The Montreal classification of UC (Silverberg, et al., 2005).
E1 Proctitis
Involvement limited to the rectum (i.e.
proximal extent of inflammation is distal to
recto-sigmoid junction)
E2 Left-sided
Involvement limited to the proportion of the
colon distal to the splenic flexure
(analogous to „distal‟ colitis)
E3 Extensive Involvement extends proximal to the
splenic flexure, including pan colitis

Ulcerative Colitis Chapter 1
- 9 -
B. Classification according to disease severity
Classification of UC based on disease severity is
useful for clinical practice and dictates the patient's
management. Many disease activity indices or criteria have
been proposed, but none have been adequately validated.
Although modifications of the original Truelove and Witts'
criteria are used in daily practice, the modified Mayo score
is used more frequently in current clinical trials.
For clinical practice a combination of clinical
features, laboratory findings, imaging modalities and
endoscopic parameters including histopathology will
all assist physicians in their patients' management
(Dignass, et al., 2012).
A distinction should be made between disease
activity at a point in time (remission, mild, moderate,
severe) and the response of disease to treatment. Moderate
colitis has become necessary to distinguish from mildly
active disease, because the efficacy of some treatments may
differ. The simplest clinical measure to distinguish
moderate from mildly active colitis is the presence of
mucosal friability (bleeding on light contact with the rectal
mucosa at sigmoidoscopy) (D'Haens, et al., 2007).
There is no fully validated definition of remission.
The best way of defining remission is a combination of
clinical parameters (i.e. stool frequency ≤ 3/day with no
bleeding) and a normal mucosa at endoscopy. Absence of
an acute inflammatory infiltrate at histology is helpful
(Dignass, et al., 2012).

Ulcerative Colitis Chapter 1
- 10 -
Table (2): Disease severity index of UC (Truelove and Witts, 1995).
Mild Moderate Severe Bloody stools/day < 4 4 - 6 ≥ 6
Pulse < 90 bpm ≤ 90 bpm > 90 bpm
Temperature < 37.5 °C ≤ 37.8 °C > 37.8 °C
Hemoglobin > 11.5 g/dL ≥ 10.5 g/dL < 10.5 g/dL
ESR < 20 mm/h ≤ 30 mm/h > 30 mm/h
CRP Normal ≤ 30 mg/L > 30 mg/L
Table (3): Mayo activity scoring index (D'Haens, et al., 2007).
0 1 2 3 Stool
frequency Normal
1-2/day
> normal
3-4/day
> normal
5/day
> normal
Rectal
bleeding None Streaks Obvious
Mostly
blood
Endoscopic
finding Normal
Mild
friability
Moderate
friability
Spontaneous
bleeding
Global
assessment Normal Mild Moderate Severe
The Mayo score ranges from
0 to 12, with higher scores
indicating more severe disease.
0 to 1: Remission
2 to 5: Mild disease
6 to 9: Moderate disease
10 to 12: Severe disease
Table (4): Endoscopic scores for UC (Dignass, et al., 2012).
Baron Score (Baron JH, et al., 1964)
0 Normal: matt mucosa, ramifying vascular pattern clearly
visible, no spontaneous bleeding, no bleeding to light touch
1 Abnormal, but non-hemorrhagic: appearances between 0 and 2
2 Moderately hemorrhagic: bleeding to light touch,
but no spontaneous bleeding seen on initial inspection
3 Severely hemorrhagic: spontaneous bleeding seen ahead of
instrument at initial inspection and bleeds to light touch
Schroeder Score (Schroeder KW, et al., 1987)
0 Normal or inactive disease
1 Mild (erythema, decreased vascular pattern, mild friability)
2 Moderate (marked erythema, absent vascular pattern, friability, erosions)
3 Severe (spontaneous bleeding, ulceration)
Feagan Score (Feagan BG, et al., 2005)
0 Normal, smooth, glistening mucosa, with vascular pattern visible; not friable
1 Granular mucosa; vascular pattern not visible; not friable; hyperemia
2 As 1, with a friable mucosa, but not spontaneously bleeding
3 As 2, but mucosa spontaneously bleeding

Ulcerative Colitis Chapter 1
- 11 -
Pathophysiology:
Increasing evidence suggests that there is a defect in
the function of the intestinal immune system.
As a consequence, there is a breakdown of the defense
barrier of the gut, which, in turn, results in exposure of the
mucosa to microorganisms or their products. The result is
a chronic inflammatory process mediated by T-cells.
Hence, therapy should be directed at improving the
intestinal immune system. It has been postulated that
genetic factors may predispose certain individuals to
developing a "leaky gut" (William Tremaine, et al., 2008).
In ulcerative colitis, inflammation always begins in
the rectum, extends proximally a certain distance, and then
abruptly stops. A clear demarcation exists between
involved and uninvolved mucosa and no "skip areas" are
present. It primarily involves the mucosa and submucosa,
with formation of crypt abscesses and mucosal ulceration.
The mucosa typically appears granular and friable. The
small intestine is never involved, except when the distal
terminal ileum is inflamed in a superficial manner, referred
to as backwash ileitis (William Tremaine, et al., 2008).
In severe cases, pseudo polyps form, consisting of
areas of hyperplastic growth with swollen mucosa
surrounded by inflamed mucosa with shallow ulcers.
Necrosis can extend below the lamina propria to involve
the submucosa and the circular and longitudinal muscles,
although this is unusual. As the disease becomes chronic,
the colon becomes a rigid foreshortened tube that
lacks its usual haustral markings, leading to the
lead pipe appearance observed on barium enema
(William Tremaine, et al., 2008).

Ulcerative Colitis Chapter 1
- 12 -
Etiology:
The etiology of IBD is unknown. Environmental,
infectious, genetic, autoimmune, and host factors have
been suspected. Interactions among these factors may be
more important (Buhner, et al., 2006).
A. Genetic Factors
IBD is seen two to four times greater in the Jewish
population as compared with other ethnic groups.
Ashkenazi Jews have the greatest risk within the Jewish
population. Other epidemiologic studies have shown higher
rates in whites, lower rates in African Americans, and the
lowest rates in Asians (Ahmad, et al., 2001).
The prevalence of IBD is also increased in relatives
of those who have CD and UC. For patients who have UC,
the occurrence of IBD in their offspring was 6.26%; for
patients who have CD, the occurrence was 9.2%
(Orholm, et al., 1999).
Epidemiologic studies demonstrate familial
similitude for disease type, extent and extra-intestinal
manifestations for siblings with UC, but the concordance
rates are smaller than for CD. All studies that included the
evaluation of concordance rates between monozygotic and
dizygotic twins indicate that the genetic contribution to
disease susceptibility is smaller for UC than for CD
(Halfvarson, et al., 2003).
The region of the major histocompatibility complex
(MHC) locus on chromosome 6p that contains the genes
encoding the HLA Class I and II histocompatibility
molecules has been implicated in susceptibility to UC by
both association and linkage studies; however, the linkage

Ulcerative Colitis Chapter 1
- 13 -
studies do not discriminate between risk for UC and CD.
Specifically, UC has been most consistently associated with
HLA Class II alleles (Satsangi, et al. 2003).
For example, in some populations the HLA-
DRB1*1502 allele (representing HLA-DR2) is positively
associated with UC and the HLA-DR4 and DR6 alleles
negatively associated; the differences in association among
populations may be accounted for by racial and ethnic
variability. The infrequent HLA-DRB1*0103 allele is
associated with extensive and severe UC and often
associated with the requisite for colectomy. Although there
is conflicting data in differing populations, other potential
genetic associations for UC include the interleukin-1 family
of genes on chromosome 2q13. Another potential
'functional candidate gene' is the multidrug resistance gene
(MDR1) that is located in an area of linkage on
chromosome 7 (Pallone; Silverberg; Ahmad, et al. 2003).
In addition, there is a strong likelihood that genetics
also impact on the incidence of extra-intestinal
complications of UC. In particular, the association between
HLA-B27 and the development of ankylosing spondylitis
and sacroiliitis in patients with UC has been reproduced
and approaches 100%. Peripheral arthropathies (type I and
II) accompanying UC are also associated with HLA
polymorphisms that associate with erythema nodosum and
uveitis (Orchard, et al. 2002).
Of note, the association of UC with primary
sclerosing cholangitis is also related to the presence of
several HLA Class II alleles and is modified (prevented)
by the environmental factor of cigarette smoking
(Mitchell, et al. 2002).

Ulcerative Colitis Chapter 1
- 14 -
B. Environmental Factors
Cigarette smoking:
There are several environmental clues to
susceptibility and development of UC (Krishnan and
Korzenik, 2002).
The long-standing finding that cigarette smoking
protects against the development of ulcerative colitis has
withstood the test of time. Indeed, case series continue to
demonstrate a protective effect of smoking on both the
development and course of UC (Abraham, et al., 2003).
Although smokers are less likely to develop UC, however,
ex-smokers are more likely to develop extensive or severe
colitis. Others believe that ex-smokers account for the
preponderance of the second age peak for UC in
patients > 40 years (Halme, et al., 2002).
The protective effect of smoking also extends to
the extra-intestinal manifestations and the post-surgical
complications of UC. For example, smoking protects
against the development of PSC, smoking, or non-smoking,
accounts for the differing incidence of PSC associated
with UC (Mitchell, et al., 2002).
Appendectomy:
Another consistent epidemiologic clue to the
pathogenesis of UC is the observation that appendectomy,
particularly at a younger age, both reduces the likelihood of
developing and the severity of disease. It seems to be an
additive protective factor to cigarette smoking against the
development of UC. In contrast to UC, prior appendectomy
does not seem to be protective against development of PSC
(Feeney et al.; Cosnes, et al.; Mitchell, et al., 2002).

Ulcerative Colitis Chapter 1
- 15 -
Bacteria:
One ubiquitous factor in animal models of colitis and
in human disease is the relationship with bacteria. In
experimental models of IBD, colitis does not develop in
animals that are raised in germ-free environments
(Sartor, 2004).
Commensal bacteria, not pathogens, are sufficient to
induce colitis, but this is determined by both host and
bacterial specificities. Also, different phenotypic patterns of
colitis are seen with specific bacterial species. Commensal
bacteria can induce a protective effect that can be
transmitted by bacteria-responsive regulatory CD4+ T-cells
(Cong, et al. 2002).
Although it has not been possible to identify bacterial
strains that are specific to UC, there are increased numbers
of mucosa-associated (adherent) Bacteroides species and
Enterobacteriaceae species in patients with inflamed
segments (Swidsinski, et al. 2002).
Whether early exposure to common environmental
microbes is protective against UC as it is with other
autoimmune disorders, in line with the so-called hygiene
hypothesis, remains to be determined (Weiss, 2002).
Alternatively, functional activity of microbial strains
may also lead to 'DYSBIOSIS' and affect the metabolic
activity of colonocytes or enterocytes, leading to the
development of UC. The potential inductive or protective
role of bacteria has also led to considerable interest in
prebiotic or probiotic therapies for UC and its
complications (Sartor, 2004).

Ulcerative Colitis Chapter 1
- 16 -
C. Immunologic Factors
From an immunologic perspective, UC has less of a
Th1 response pattern than CD (Pallone, et al. 2003).
In IBD there are chronic inflammatory changes in the
GIT. These are mediated by different immunologic factors
for each disease, although they are both a consequence of
T-cell activation (Pallone and Monteleone, 1998).
The cytokine expression is different comparing
ulcerative colitis and Crohn's disease. In ulcerative colitis,
the inflammation is thought to be regulated by Th2-cells,
which mediate B cells and antibody responses; however
this has not been proven. It has been shown that there is
increased expression of IL-5, which is a Th2 cytokine,
but IL-4, another Th2 cytokine, is not increased
(Fuss, et al., 1996).
The Th2 contribution may be helping the antibody
response, because in UC, there is an increase in IgG plasma
cells presumably mediated by T-cells (Macdonald, 2000).
Recent evidence indicates that, in contrast to the Th1
cytokines that are associated with the pathogenesis of
Crohn's disease (interferon-γ, TNF-α and IL-12),
animal models of ulcerative colitis may be associated
with increased natural killer cell activity and IL-13
(Heller, et al. 2002).
In addition, attention is being directed at the down
regulatory role of transforming growth factor-ß in colitis
and the possibility that defective signaling of transforming
growth factor-ß may account for inadequate tissue repair
(Pallone, et al. 2003).

Ulcerative Colitis Chapter 1
- 17 -
Diagnosis:
A gold standard for the diagnosis of UC is not
available. The diagnosis is made on the basis of clinical
suspicion supported by appropriate macroscopic findings
on colonoscopy, typical histological findings on biopsy
and negative stool examinations for infectious agents
(Dignass, et al., 2012).
There is some evidence to suggest that patients with
UC stratified by age have different outcomes. Patients
diagnosed before the age of 16 had a more aggressive
initial course, while older age at diagnosis was found
to be associated with a lower risk of colectomy
(Barreiro-de-Acosta, et al., 2010).
There is also some evidence that UC diagnosed in
the very young has a different etiology and prognosis. This
is taken into consideration by the pediatric modification to
the Montréal classification (Levine, et al., 2011).
It is a disease that used to carry a high mortality and
major morbidity. With modern medical and surgical
management, the disease now has a slight excess of
mortality in the first 2 years after diagnosis, but little
subsequent difference from the normal population. The
clinical course is marked by exacerbation and remission.
About 50% of patients have a relapse in any year. An
appreciable minority has frequently relapsing or chronic,
continuous disease and overall, 20-30% of patients with
pancolitis come to colectomy. After the first year
approximately 90% of patients are fully capable of work
(defined by < 1 month off work/year), although significant
employment problems remain an issue for a minority
(Langholz, et al., 1994).

Ulcerative Colitis Chapter 1
- 18 -
Clinical picture
The onset may be gradual or sudden. The course is
variable, with periods of exacerbation, improvement, and
remission that may occur with or without specific medical
therapy (William Tremaine, 2008).
Symptoms of UC are dependent upon extent and
severity of disease. The cardinal symptom of ulcerative
colitis is bloody diarrhea. Diarrhea may vary from 1 to 20
or more loose or liquid stools a day, usually worse in the
morning and immediately after meals, and patients with
moderate or severe symptoms often have nocturnal stools.
Constipation with rectal bleeding is a presenting symptom
in about 25% of patients with disease limited to the rectum.
Abdominal pain is usually cramping, which is worse after
meals or bowel movements. Anorexia, weight loss, and
nausea in the absence of bowel obstruction are common
with severe and extensive disease but uncommon with mild
to moderate disease or disease limited to the left colon. In
children, urgency, incontinence, and upper gastrointestinal
tract symptoms are more frequent and growth failure is
common. It is associated with an equivalent increased risk
of colonic carcinoma (Friedman, et al., 2008).
A full medical history should include detailed
questioning about the onset of symptoms, particularly the
stool frequency and consistency, recurrent episodes of
rectal bleeding or bloody diarrhea, urgency, tenesmus,
abdominal pain, incontinence, nocturnal diarrhea, weight
loss, features of extra-intestinal manifestations, and
systemic symptoms of malaise, anorexia, or fever are
features of a severe attack (Dignass, et al., 2012).

Ulcerative Colitis Chapter 1
- 19 -
History should include recent travel, food
intolerances, contact with enteric infectious illnesses,
medication (antibiotics and NSAIDs drugs), smoking habit,
sexual practice, vaccination, family history of IBD,
Colorectal cancer, and previous appendictomy should be
explored (Dignass, et al., 2012).
However, severe colitis is still a potentially
life-threatening illness. Immediate admission to
hospital is warranted for all patients fulfilling
Truelove and Witts' criteria for severe colitis to
prevent delayed decision making which may lead
to increased perioperative morbidity and mortality
(Dignass, et al., 2012).
In mildly active ulcerative colitis, physical
examination findings are often normal or there
may be abdominal tenderness, particularly with
palpation over the sigmoid colon. Patients with
more severe disease may have pallor, dehydration,
tachycardia, fever, diminished bowel sounds,
and diffuse abdominal tenderness with rebound.
Tenderness with rebound is ominous and suggests toxic
dilatation or perforation (Sands, 2004).
Also, it should include general well-being, pulse rate,
body temperature, blood pressure, measurement
body weight and height, calculation of BMI, abdominal
examination for distention and tenderness, palpable
masses, perianal inspection, digital rectal examination,
oral inspection, check for anemia, fluid depletion,
and check for eye, skin and/or joint involvement
(Sands, 2004).

Ulcerative Colitis Chapter 1
- 20 -
Ulcerative colitis is associated with a wide variety of
systemic complications which classically called extra-
intestinal manifestations, immune-mediated phenomena
that affect the joints, eye, skin, or hepatobiliary tract, but
they can be defined more broadly to include complications
in other organ systems and complications that arise as a
direct pathophysiologic consequence of extensive bowel
inflammation or resection. It occurs in up to 36% of
patients (Edward, 2008).
Arthritis affecting the axial skeleton can be classified
into the more common, frequently asymptomatic,
sacroiliitis and the less common, more progressive,
ankylosing spondylitis. Symptomatic sacroiliitis manifests
as low back pain and stiffness, typically worse in the
morning and with rest while spondylitis resulting in
progressive stiffness and lordosis of the spine. The
symptoms usually accompany exacerbations but may
appear before the disease and don't necessarily follow its
course (Johns Hopkins, 2013).
About 19% of patients with UC experience
dermatological changes. The two most common
dermatologic manifestations are pyoderma gangrenosum
and erythema nodosum. Other dermatological sequelae
include dermatitis, erythematous rash, psoriasis, carcinoma,
urticaria, pityriasis, lupus erythematosus, vitiligo and
ecchymosis (Edward, 2008).
Ocular complications occur in 1-13% of patients
with IBD. The most common forms are anterior uveitis
(also known as iritis) and scleritis. An inflammatory
retinopathy or keratitis (corneal inflammation) may occur
less frequently. Symptoms include headache, photophobia
and blurred vision (Johns Hopkins, 2013).

Ulcerative Colitis Chapter 1
- 21 -
The most important hepatobiliary condition
associated with IBD is primary sclerosing cholangitis. This
idiopathic chronic cholestatic liver disease is characterized
by inflammation and fibrosis of the biliary tree.
Autoimmune hepatitis is associated rarely with IBD, but
when it is, it usually is associated with ulcerative colitis.
Some patients may have features of both autoimmune
hepatitis and primary sclerosing cholangitis (the so-called
overlap syndrome) (Edward, 2008).
In most situations, extra-intestinal manifestations
respond to standard medical therapy. On rare occasions,
a total proctocolectomy may be necessary to control
severe extra intestinal manifestations of this disease
(Edward, 2008).
Fig.(1): Extra-colonic manifestations of UC (Johns Hopkins, 2013)

Ulcerative Colitis Chapter 1
- 22 -
Endoscopy
Flexible proctosigmoidoscopy or colonoscopy with
multiple biopsies (at least two biopsies from five sites
including the distal ileum and rectum) is the first line
procedure for diagnosing colitis. It allows classification of
disease based on endoscopic extent, severity of mucosal
disease and histological features. Active disease
confirmed sigmoidoscopy as a first line procedure
(Dignass, et al., 2012).
No endoscopic feature is specific for UC. The most
useful endoscopic features of UC are considered to be
continuous and confluent colonic involvement with clear
demarcation of inflammation and rectal involvement.
Endoscopic severity of UC may be best reflected by the
presence of mucosal friability, spontaneous bleeding and
deep ulcerations (Dignass, et al., 2012).
There are mucosal changes including loss of
the normal vascular markings, mucosal granularity,
mucosal friability, mucous exudate, and focal ulceration
(William Tremaine, 2008).
Fig.(2): Endoscopic image of ulcerative colitis (Samir, 2004)

Ulcerative Colitis Chapter 1
- 23 -
With colonoscopy, the extent of disease can be
determined and the terminal ileum can be examined for
evidence of backwash ileitis in UC or ileal involvement in
CD. Patients with left-sided UC may have inflammatory
changes around the appendix, called a cecal patch,
as a manifestation of the disease; this finding should
not be confused with segmental colitis due to CD
(William Tremaine, 2008).
In acute severe colitis, full colonoscopy is rarely
needed and may be contraindicated, because of the risk of
perforation or hemorrhage. Patients should have abdominal
radiography. Also, phosphate enema is considered safe,
except with colonic dilatation (Terheggen, et al., 2008).
Endoscopic findings are predictive of outcome at for
patients with UC in remission. Endoscopic reassessment is
appropriate at a relapse, or for steroid-dependent or -
refractory UC or when considering colectomy. Patients
with UC (extending proximal to the rectum), the risk of
malignancy is increased above that for the general
population after 8-10 years of disease. So, periodic
colonoscopy with biopsies for surveillance for dysplasia is
indicated after 8-10 years of disease. The risk for patients
with less extensive UC (with involvement of the colon
distal to the splenic flexure) also is increased, but the
magnitude of the risk is not defined. There doesn't appear
to be an increased risk of the rectal cancer for ulcerative
proctitis without colitis above the rectum. Patients with
left-sided UC of 8-10 years‟ duration, or longer, should
undergo periodic surveillance biopsies. The optimal
interval between surveillance examinations has not been
defined, and the examinations usually are performed
at 1-2 year intervals (William Tremaine, 2008).

Ulcerative Colitis Chapter 1
- 24 -
Table (5): UC Endoscopic Index of Severity (UCEIS) (Travis, et al., 2012)
Vasc
ula
r p
att
ern
Normal (0)
Normal vascular pattern with
arborisation of capillaries clearly
defined, or with blurring or patchy
loss of capillary margins
Patchy obliteration
(1) Patchy obliteration of vascular pattern
Obliterated (2) Complete obliteration of vascular pattern
Ble
edin
g
None (0) No visible blood
Mucosal (1)
Some spots or streaks of coagulated blood on
the surface of the mucosa ahead of the scope,
which can be washed away
Mild (2) Some free liquid blood in the lumen
Moderate
or severe (3)
Frank blood in the lumen ahead of
endoscope or visible oozing from mucosa
after washing intra-luminal blood, or visible
oozing from a hemorrhagic mucosa
Ero
sio
ns
& U
lcer
s None (0) Normal mucosa, no visible erosions or
ulcers
Erosions (1) Tiny (≤5 mm) defects in the mucosa, of a
white or yellow color with a flat edge
Superficial
ulcer (2)
Larger (N5 mm) defects in the mucosa,
which are discrete fibrin-covered
ulcers when compared to erosions,
but remain superficial
Deep ulcer (3) Deeper excavated defects in the mucosa,
with a slightly raised edge
Fig. (3): Histology of
normal colon and UC
(Johns Hopkins, 2013)

Ulcerative Colitis Chapter 1
- 25 -
Histology
Histopathological examination of biopsy specimens
should be carried out according to the BSG guideline, „A
Structured Approach to Colorectal Biopsy Assessment‟
(Jenkins, et al., 1997).
For a reliable diagnosis of ulcerative colitis multiple
biopsies from five sites around the colon (including the
rectum) and the ileum should be obtained. Multiple implies
a minimum of two samples. Repeat biopsies after an
interval may help to solve differential diagnostic problems
and establish a definitive diagnosis especially in adults, by
showing additional features (Dignass, et al., 2012).
There should be an attempt to define the type of IBD,
to mention other coexistent diagnoses or complications and
to mention the absence or presence of any dysplasia and its
grade. Medical and surgical therapy may modify the
histological appearances of IBD and these should be taken
into account when assessing IBD biopsy pathology
(Hyde, et al., 2002).
Also, mucosal biopsy specimens from involved areas
of the gastrointestinal tract are useful for excluding self-
limited colitis and other infections and non-infectious
colitis due to ischemia, collagenous and lymphocytic
colitis, drug effect, radiation injury, and solitary rectal ulcer
syndrome. Non-caseating granulomas are a feature of CD
and can be helpful for distinguishing it from UC
(William Tremaine, 2008).
A hallmark of active UC is the presence of a
polymorphonuclear cell infiltration into the epithelial crypts
(cryptitis) and lamina propria (Beckmann, et al., 2007).

Ulcerative Colitis Chapter 1
- 26 -
Radiologic Features
Imaging can be helpful in diagnosis, assessment of
disease extent and severity and for investigation of
suspected complications. Each modality has its own
advantages and drawbacks and the tests are often
complimentary (Hall and Brenner, 2008).
Barium fluoroscopy (Double contrast barium
enema) allows for exquisite detail of the colonic mucosa,
and also allows bowel proximal to strictures to be assessed.
It is however contraindicated if acute severe colitis is
present due to the risk of perforation. Mucosal
inflammation lends a granular appearance to the surface of
the bowel. Mucosal ulcers are undermined (button-shaped
ulcers). When most of the mucosa has been lost, islands of
mucosa remain giving it a pseudo-polyp appearance. In
chronic cases the bowel becomes featureless with loss of
normal haustral markings, luminal narrowing and bowel
shortening (lead pipe sign). Small islands of residual
mucosa can grow into thin worm like structures (so-called
filiform polyps) (Roggeveen, et al., 2005).
A. Pseudo-polyp-------- B. Target sign ------- C. Loss of haustration
Fig.(4): Radiological features in UC (Gore, et al., 1996)

Ulcerative Colitis Chapter 1
- 27 -
Computed Tomography (CT) will reflect the same
changes that are seen with a barium enema, with the
additional advantage of being able to directly visualize the
colonic wall, the terminal ileum and identify extra-colonic
complications, such as perforations or abscess formation. It
is important to note however that CT is insensitive to early
mucosal disease (Gore, et al., 1996).
A cross section of the inflamed and thickened bowel
is having a target appearance, due concentric rings of
varying attenuation, also known as mural stratification. In
chronic cases, submucosal fat deposition is seen
particularly in the rectum (fat halo sign). Strictures are also
common, and are not all malignant. Colorectal carcinoma is
often sessile. Focal loss of mural stratification or
excessive mural thickness (1.5 cm) should prompt
endoscopic evaluation (Gore, et al., 1996).
The current status of Magnetic Resonance Imaging
(MRI) in UC is that of a promising, noninvasive technique
for imaging extent of more severe disease. The most
striking abnormalities in UC are wall thickening and
increased enhancement. The median wall thickness in UC
ranges from 4.7-9.8 mm. In general, the more is severe the
inflammation, the thicker the colonic wall. A colonic wall
thickness <3 mm is usually considered as normal, 3-4 mm
as a "gray zone," and >4 mm as pathological. Enhancement
of the mucosa with no or less enhancement of
the submucosa is producing a low SI strip the
so-called submucosal stripe. Other features are the loss
of haustral markings, backwash ileitis shows
mild enhancement and no wall thickening and
there is increased SI of the pericolonic fat noted
(Gore, et al., 1996).

Ulcerative Colitis Chapter 1
- 28 -
Plain film is nonspecific but may show evidence of
mural thickening. Ultrasound cannot comprehensively
assess the gut when used in isolation. Doppler are useful in
the assessing the degree of disease activity. It has
reasonable sensitivity for documenting presence of
complicating abscess, particularly in thinner patients and is
a useful first line test in this context (Dietrich, 2009).
Virtual colonography is an evolving technology.
The limited data currently available do not demonstrate a
diagnostic value for assessing the disease extent in patients
with suspected or proven UC (Dignass, et al., 2012).
Recent studies assess the assessment of the severity
of ulcerative colitis using endorectal ultrasonography
(ERUS) corresponds with clinical severity of the disease.
ERUS is a valuable, relatively cost-effective diagnostic tool
of high overall accuracy, which may be helpful in clinical
evaluation and monitoring of ulcerative colitis
(Dignass, et al., 2012).
A variety of nuclear medical techniques can be used
in the assessment of IBD, but they have no role in primary
diagnosis. Technetium-99m labelling of WBCs remain a
widely acceptable scintigraphic method for the evaluation
of disease extension and severity. Positron emission
tomography alone or with CT using fluorine-18
fluorodeoxy glucose is a promising method of measuring
inflammation in IBD. These techniques considered when
colonoscopy is not completed successfully or other imaging
modalities are negative (Stathaki, et al., 2009).
Ulcerative Colitis Chapter 1
- 29 -
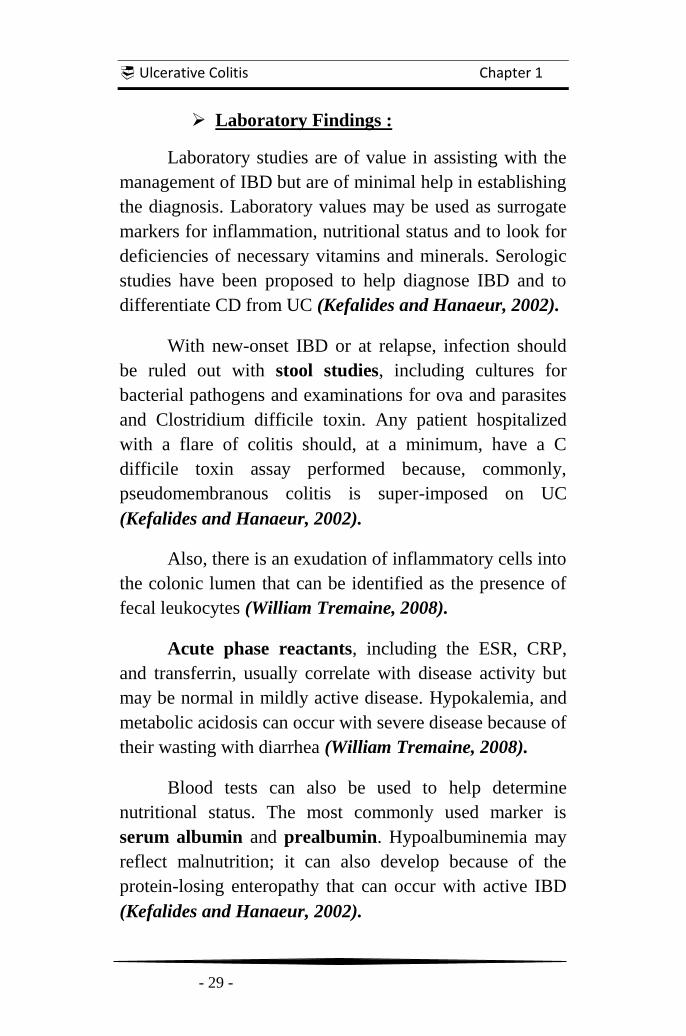
Laboratory Findings :
Laboratory studies are of value in assisting with the
management of IBD but are of minimal help in establishing
the diagnosis. Laboratory values may be used as surrogate
markers for inflammation, nutritional status and to look for
deficiencies of necessary vitamins and minerals. Serologic
studies have been proposed to help diagnose IBD and to
differentiate CD from UC (Kefalides and Hanaeur, 2002).
With new-onset IBD or at relapse, infection should
be ruled out with stool studies, including cultures for
bacterial pathogens and examinations for ova and parasites
and Clostridium difficile toxin. Any patient hospitalized
with a flare of colitis should, at a minimum, have a C
difficile toxin assay performed because, commonly,
pseudomembranous colitis is super-imposed on UC
(Kefalides and Hanaeur, 2002).
Also, there is an exudation of inflammatory cells into
the colonic lumen that can be identified as the presence of
fecal leukocytes (William Tremaine, 2008).
Acute phase reactants, including the ESR, CRP,
and transferrin, usually correlate with disease activity but
may be normal in mildly active disease. Hypokalemia, and
metabolic acidosis can occur with severe disease because of
their wasting with diarrhea (William Tremaine, 2008).
Blood tests can also be used to help determine
nutritional status. The most commonly used marker is
serum albumin and prealbumin. Hypoalbuminemia may
reflect malnutrition; it can also develop because of the
protein-losing enteropathy that can occur with active IBD
(Kefalides and Hanaeur, 2002).

Ulcerative Colitis Chapter 1
- 30 -
Complete blood cell count (CBC) can be useful
indicators of disease activity and iron or vitamin
deficiency. An elevated WBC count is common in patients
with active inflammatory disease or due to a complicating
abscess but it does not necessarily indicate infection.
Anemia is common and may be an anemia of chronic
disease, presumably due to cytokine effects on the bone
marrow or an iron deficiency anemia due to blood loss that
is confirmed by serum iron studies or as a result of
malabsorption of vitamin B12 or folate especially with CD
(Kefalides PT and Hanaeur SB, 2002)
Cytomegalovirus (CMV) should be considered in
severe or refractory colitis, as reactivation is common in
patients with IBD on immunosuppression. Additional tests
may need for patients who have travelled abroad
(William Tremaine, 2008).
Several new fecal tests have become available that
assist, initially, with the diagnosis of IBD in general, but
not specifically UC. Perhaps in the future they will
contribute to measurements of disease activity. For
example, elevated concentrations of calprotectin,
a neutrophil granulocyte-derived Ca++
binding protein,
have been evaluated as both a diagnostic assay to
identify inflammatory diarrhea and as measurement of
inflammatory activity (Beckmann, et al., 2007)
Similarly, the concentration of lactoferrin, another
neutrophil granulocyte-derived protein, can be quantified,
most recently by using a polyclonal antibody-based enzyme
linked immunoassay that can discriminate between active
IBD and IBS. It can quantify disease activity but has yet to
be incorporated into clinical trials as a disease-activity
endpoint (Summerton, et al., 2002; Kane, et al., 2003).

Ulcerative Colitis Chapter 1
- 31 -
The peri-nuclear antineutrophil cytoplasmic
antibody (pANCA) is positive in about 2/3 of patients with
UC and about 1/3 of patients with CD while the
anti-Saccharomyces cerevisiae antibody (ASCA) is
positive in about 2/3 of patients with CD and about 1/3 of
patients with UC. These tests used together to help
distinguish UC from CD. However, the positive predictive
value of the two tests together is 63.6% for UC and 80%
for CD; thus, distinguishing the two diseases with these
tests is less than ideal (William Tremaine, 2008).
There are several potential roles for serologic
markers in UC. The most desirable would be as a
pathognomonic marker of disease specificity or prognosis,
the second as a screening tool to discriminate IBD
from other digestive disorders, and the third to assist in
the understanding of disease mechanisms or
immune interactions (Dubinsky, et al., 2002).
In adult populations the ability to diagnose UC by
flexible sigmoidoscopy or colonoscopy is less of an issue
and offers immediate confirmation and access to histology.
So, serologic markers have, thus far, not been necessary to
screen or exclude UC compared with conventional
investigations. The potential for serologic studies to
discriminate between UC & CD, particularly for patients
with 'indeterminate colitis' has been evaluated by
(Joossens, et al., 2002).
They found that the presence of pANCA does not
help to discriminate between UC and CD in patients with
IC. By contrast, the presence of anti-Saccharomyces
cerevisiae antibodies is more helpful, but their sensitivity in
indeterminate colitis is so low that a positive or negative
predictive value will be low (Vasiliauskas, 2003).

Ulcerative Colitis Chapter 1
- 32 -
Nutritional aspects in UC
The inflammation of the GIT with the associated
symptoms of pain, nausea, and diarrhea is leading to
reduced food intake and uptake leading to malnutrition.
The prevalence of nutritional deficiencies and malnutrition
is higher in patients with CD than in patients with UC
(Lochs, et al., 2006).
The etiology of malnutrition is multifactorial.
Medication, increased exudative losses of protein or small
bowel bacterial overgrowth is additional causes of
malabsorption (Han, et al., 1999).
Anemia and iron deficiencies are more prevalent in
patients with UC. In patients with severe diarrhea,
low levels of potassium, magnesium, calcium and
phosphate can be encountered. The levels of fat
soluble vitamins correlate with the severity of steatorhea
(Remy Meier, 2008).
Table (6): Nutritional deficiencies in IBD (Remy Meier, 2008).
Ulcerative Colitis Chapter 1
- 33 -
The diagnosis of malnutrition is done by using
several anthropometric and biochemical parameters as
weight, height, skinfold thickness, body composition
analysis, and serum albumin. It is also important to record
the food intake in the last 1-2 weeks. Patients often
consume an unbalanced diet which may lead to nutritional
deficiencies (Vagianos, et al., 2007).
Resting energy expenditure varies depending on
inflammatory activity. The Energy requirements have been
calculated with the Harris-Benedict equation. However,
physical activity, inflammatory activity, malabsorption and
the degree of obesity should be taken into account. The
more obese the less energy/kg is required and vice versa.
Consequently requirements may be calculated on the basis
of ideal BW (or adjusted BW) and may amount to 25-30
Cal/kg ideal BW/24h (Lochs, et al., 2006).
Protein requirements in patients with IBD are
generally increased. Inflammation induces a catabolic
response with endogenous proteolysis and ensuing negative
nitrogen balance. To limit nitrogen losses in patients with
active IBD, 1.5 g/kg BW protein per day should be
provided. It is recommended to increase protein intake to
2g protein/kg BW/24 h in infectious or severely
malnourished patients (Han, et al., 1999).
The nutritional support required during an acute
exacerbation differs from the nutritional regimen during
remission. The aims of nutritional support in IBD are to
treat or to prevent nutritional deficits, to reduce disease
activity, to improve growth and development in children
and adolescents, to reduce the need for surgery or
aggressive medical treatment, and to maintain remission
(Remy Meier, 2008).
Ulcerative Colitis Chapter 1
- 34 -
There are no specific data available for ulcerative
colitis to improve or to maintain nutritional status with oral
supplements. Specific nutritional support is more beneficial
in Crohn's disease than in ulcerative colitis. Enteral
nutrition is the preferred route for nutritional repletion
because of the potential trophic effects on the intestinal
mucosa, the preservation of gastrointestinal function, the
beneficial effects on the intestinal flora and mucosal barrier
integrity (Harries, et al., 1983).
In addition, complication rates and costs have been
reported to be lower than with parenteral nutrition. For a
long time, it was suggested that bowel rest with TPN may
reduce intestinal inflammation and decrease disease activity
in patients with IBD. Parenteral nutrition is of limited
benefit in ulcerative colitis. Sometimes parenteral nutrition
is instituted to decrease a debilitating defecation frequency,
when patients are hospitalized with acute toxic colitis
(Remy Meier, 2008).
Enteral tube feeding has shown to be ineffective in
patients with active UC. The remission rates are not higher
than the rate of spontaneous remission when patients
consume normal food. A comparison of TPN with EN in
acute UC showed similar effects on nutritional status,
disease activity and complications, but neither TPN
nor EN had a positive effect on inflammatory activity
(González-Huix, et al., 1993).
Pre- and probiotics have been shown to be beneficial
in gastrointestinal diseases. Prebiotics are soluble poli- or
oligo-saccharides and serve in the intestine as substrates for
fermentation (Johannsson, et al., 1997).
Ulcerative Colitis Chapter 1
- 35 -
Probiotics are non-pathogenic bacteria which are
able to exert positive health benefits in the gastrointestinal
tract. They are able to adhere to the intestinal mucosa and
can stimulate the secretion of serum IgA and mucus
production. They may reduce the levels of pro-
inflammatory cytokines and increase levels of anti-
inflammatory cytokines. Also, they can produce defenses
and heat shock proteins (Johannsson, et al., 1997).
Pre- and probiotics can interact with the commensal
bacteria and may therefore influence the intestinal
ecosystem. This effect is eminent in the colon, where
anaerobic bacteria can ferment non-absorbable dietary
carbohydrates. Through fermentation, the intestinal pH
decreases, which is stimulates the growth of non-
pathogenic bacteria and liberate short chain fatty acids.
Butyrate is the main energy source for the colonic epithelial
cells. This prevents the expression of specific genes
encoding cytokines intensifying inflammatory response.
Also, it increases apoptosis of inflammatory cells. So far,
the use of pre-and probiotics was found to be more
beneficial in UC than in CD. The use of a fermentable
Plantago ovate (dietary fibre) supplementation
achieved similar relapse rates in UC as Mesalazine
(Buda, et al., 2003; Gionchetti, et al., 2000).
Most patients with IBD in remission have a normal
nutritional status. There are no specific diets recommended
if the patients are in remission and can eat normally. A
normal "healthy" diet rich in fruits, vegetables and fish can
be recommended. In patients with ileum resection or
sulfasalazine treatment, vitamin B12 levels have to be
monitored. Ca++
and vitamin D status should be controlled
in patients treated with steroids (Belluzzi, et al., 1996).
Ulcerative Colitis Chapter 1
- 36 -
Traditional pharmacological treatment of UC:
Therapy for IBD is a rapidly evolving field, with
many new biological agents under investigation that are
likely to change therapeutic strategies radically in the next
decade (Mowat, et al., 2011). Details of the principal drugs
can only be summarized in this document.
Amino salicylates
5-Aminosalicylic acid (5-ASA) or mesalazine
(„mesalamine‟ in the USA) can be delivered in millimolar
concentrations to the gut lumen by a variety of oral tablets,
sachets or suspensions using pH-dependent release
mechanism, multi-matrix delivery systems, or conjugation
via a diazo bond to a variety of carrier molecules with
release of 5-ASA after splitting by bacterial enzymes in
the large intestine. They can also be used as topical agents
in the form of liquid or foam enemas, or suppositories
(Sandborn and Hanauer, 2003).
They act on epithelial cells by a variety of
mechanisms to moderate the release of lipid mediators,
inflammatory cells, cytokines and reactive oxygen species
(Sutherland and Macdonald, 2006).
The choice of 5-ASA is debated, but is influenced by
tolerability (mesalazine is tolerated by 80% of those
unable to tolerate sulfasalazine), dose schedule (single or
twice daily dosing with better compliance), route of
delivery, availability and cost are relevant factors in
choice (Dignass, et al., 2009).
Ulcerative Colitis Chapter 1
- 37 -
For UC, greater clinical improvement is associated
with doses of ≥ 2.0 g/day are more effective than < 2.0
g/day. Clinical improvement characteristically occurs at
twice the remission rate (Bergman and Parke, 2006).
There is now robust evidence to suggest that single
daily dosing is as effective as multiple dosing, and may
even be superior. Maintenance with all 5-ASA drugs may
reduce the risk of colorectal cancer by up to 75%
(Eaden, et al., 2000).
Side effects of 5-Aminosalicylic acid occur in
10-45% of patients, depending on the dose. Headache,
nausea, epigastric pain, diarrhea, thrombocytopenia,
rash and oligospermia in men are most common. Serious
idiosyncratic reactions (including Stevense Johnson
syndrome, pancreatitis, agranulocytosis, or alveolitis)
are rare (Van Staa, et al., 2004).
Also, they associated with nephrotoxicity (including
interstitial nephritis and nephrotic syndrome), which
appears both to be idiosyncratic and, in part, dose related
(Muller, et al., 2005).
For patients on maintenance 5-ASA, many clinicians
believe that creatinine and full blood count should be
monitored every 3–6 months and it should be stopped if
renal function deteriorates (Muller, et al., 2005).
Ulcerative Colitis Chapter 1
- 38 -
Corticosteroids
Corticosteroids are used in the form of oral
prednisolone, prednisone, budesonide, or intravenous
hydrocortisone and methylprednisolone. Topical
suppositories, foam or liquid enemas also used. Many
strategies attempt to maximize topical effects
while limiting the systemic side effects of steroids
(Seow, et al., 2009).
Corticosteroids are potent anti-inflammatory agents
for moderate to severe relapses of UC. They have no role in
maintenance therapy (Manguso and Balzano, 2007).
They act through inhibition of several inflammatory
pathways: suppressing interleukin transcription,
suppression of arachidonic acid metabolism and stimulation
of apoptosis of lymphocytes within the lamina propria of
the gut (Benchimol, et al., 2008).
A combination of oral and rectal steroids is better
than either alone. Adverse events are significantly more
frequent at a dose of 60 mg/day compared to 40 mg/day,
without added benefit, so 40 mg/day appears optimal for
outpatient management of acute UC (Lee, et al., 1996).
Budesonide (colonic release preparation) is a poorly
absorbed corticosteroid with limited bioavailability and
extensive first-pass metabolism that has therapeutic benefit
with reduced systemic toxicity in ileo-caecal CD, or UC.
Beclometasone dipropionate has been studied in oral and
enema forms in UC, and is no better than 5-ASA also, it
appears as effective as prednisolone for mild - moderate
left-sided and extensive colitis (Campieri, et al., 2003).

Ulcerative Colitis Chapter 1
- 39 -
Regimens of steroid therapy are various. There is no
evidence to support any particular regimen. The commonly
used regimen is done by a starting dose of 40 mg
prednisolone per day, reducing by 5 mg/d at weekly
intervals. A standard weaning strategy helps identify
patients who relapse rapidly or do not respond and
need adjunctive therapy. Shorter courses (< 3 weeks)
are associated with early relapse and doses of
prednisolone ≤ 15 mg day are ineffective for active disease
(Kane, et al., 2002).
Steroid resistance or unresponsiveness should
lead to escalation of treatment, or consideration of
surgery. Medical therapies include an immunosuppressive
appropriate to the acuteness and type of the disease
(Kane, et al., 2002).
Side effects of corticosteroids due to supra-
physiological doses include cosmetic (acne, moon face,
edema), sleep and mood disturbance, dyspepsia or glucose
intolerance (Subramanian, et al., 2008). Prolonged use
(usually >12 weeks, but sometimes less) include cataracts,
osteoporosis, osteonecrosis of the femoral head, myopathy
and susceptibility to infection (Newby, et al., 2005).
Efficacy should be balanced against side effects, but
decisive treatment of active disease in conjunction with a
strategy for complete withdrawal of steroids is often
appreciated by a patient suffering miserable symptoms
during withdrawal acute adrenal insufficiency and
corticosteroid withdrawal syndrome may occur
(Lichtenstein, et al., 2006). Guidelines recommend
monitoring for eye, bone and other side effects particularly
in patients on steroids for more than 3 months
(Abreu, et al., 2006).

Ulcerative Colitis Chapter 1
- 40 -
Thiopurines
Azathioprine (AZA) or mercaptopurine (MP) is
widely used in UC and CD as adjunctive and sparing
therapy. Purine antimetabolites inhibit ribonucleotide
synthesis, but mechanism of immunomodulation is by
inducing T-cell apoptosis by modulating cell (Rac1)
signaling (Tiede, et al., 2003).
AZA is non-enzymatically metabolized to MP,
which involves loss of a nitro-imidazole side chain; this is
thought to explain some of the side effects seen with AZA
and which may be less of a problem with MP. MP is
subsequently metabolized to 6-thioguanine nucleotides (6-
TGN). 6-TGN has been used for treatment of IBD with
caution because of potential hepatotoxicity
(McGovern, et al., 2002; Bowen and Selby, 2000).
AZA is more effective than mesalazine at induction
of clinical and endoscopic remission in steroid dependent
ulcerative colitis and should be first-choice therapy in this
situation providing other causes of persistent symptoms
such as CMV or cancer have been excluded. Thiopurines
are effective maintenance therapy for patients with UC who
has failed or who cannot tolerate mesalazine and for
patients who require repeated courses of steroids. The
evidence for using thiopurines in UC is weaker than in CD
(Ardizzone, et al., 2006; Timmer, et al., 2007).
Tailoring or optimization can occur prior to or during
treatment. The appropriate maintenance dose of AZA is 2-
2.5 mg/kg/day and of MP is 0.75-1.5 mg/kg/day. The
„maximum‟ dose will differ between individuals and
effectively means that level at which leucopenia develops
(Gilissen, et al., 2005).

Ulcerative Colitis Chapter 1
- 41 -
Adverse events occur in up to 20%. The commonest
are allergic reactions (fever, arthralgia, rash) that
characteristically occur after 2-3 weeks and cease
rapidly when the drug is withdrawn. Hepatotoxicity and
pancreatitis are uncommon (Gisbert and Gomollon, 2008).
Bone marrow toxicity has been reported to occur up
to 11 years after starting AZA and blood monitoring should
continue throughout thiopurine therapy. Manufacturers
recommend monitoring thiopurine therapy weekly by full
blood counts (FBCs) for the first 8 weeks of therapy
followed by blood tests at least every 3 months
(Colombel, et al., 2000).
Although a significant proportion of patients
experience adverse effects with thiopurines when the drug
is tolerated for 3 weeks, long-term benefit can be expected
(Macdonald, et al., 2009). In absolute terms, the risk
remains very small (<1% risk after 10 years of thiopurine
use) and the benefits of AZA outweigh any risks
(Lewis, et al., 2000).
In IBD, large population-based studies have shown
no increased risk. Whereas a second suggested a fourfold
increased risk of lymphoma in patients with IBD treated
with AZA/MP compared with background population
(Kandiel, et al., 2005).
There is an increased risk of non-melanoma skin
cancer in patients treated with thiopurines. Patients should
be advised to avoid excessive sun exposure and use a high-
strength sun block (Fraser, et al., 2002).

Ulcerative Colitis Chapter 1
- 42 -
Methotrexate
Polyglutamated metabolites of methotrexate (MTX)
inhibit dihydrofolate reductase, but this cytotoxic effect
does not explain its anti-inflammatory effect. Inhibition of
cytokine and eicosanoid synthesis probably plays a role. It
is positioned as a second-line immunosuppressive agent in
patients resistant or intolerant of AZA, although it is
currently unclear whether thiopurines are any more
efficacious than MTX for induction or maintenance of
remission in IBD (Oren, et al., 1996).
A low dose (12.5 mg once weekly) was not shown to
be efficacious at inducing or maintaining remission. Using
larger weekly doses show higher response or remission
rates resistant or intolerant of AZA or MP. Parenteral
administration (either subcutaneous or intramuscular) may
be more effective that oral therapy and is recommended.
Monitoring therapy by measurement of FBC and liver
function tests are advisable before and within 4 weeks of
starting therapy, then monthly (Ei-Matary; Wahed, et al.,
2009; Nathan, et al., 2008).
Side effects are reported by 27- 49% of patients.
Early toxicity from MTX is primarily gastrointestinal
(nausea, vomiting, diarrhea and stomatitis). Co-prescription
of folic acid 5 mg (once a week, taken 3 days after MTX)
limits side effects. Long-term concerns are hepatotoxicity,
pneumonitis and opportunistic infections (Fraser, 2003).
MTX is teratogenic and should not be used if
conception considered. It may persist in tissues for long
periods; therefore conception should be avoided for 3-6
months after withdrawal. Breastfeeding isn't recommended
(Mahadevan and Kane, 2006)

Ulcerative Colitis Chapter 1
- 43 -
Calcineurin inhibitors
Ciclosporin (CsA) is an inhibitor of calcineurin,
which prevents clonal expansion of T cell subsets
(Shibolet, et al., 2005). It is rapidly effective as a salvage
therapy for patients with refractory UC, who would
otherwise face colectomy, but its use is controversial
because of the narrow therapeutic index of it (including
mortality rates of 3–4%), toxicity and long-term failure
rate. The drug should rarely be continued for more than 3-6
months and its main role is a bridge to thiopurine therapy
(Lichtiger, et al., 1994).
Measurement of blood pressure, FBC, renal
function and CsA concentration (aim for 100-200 ng/ml)
are advisable at 0, 1 and 2 weeks, then monthly. Blood
cholesterol and Mg++
should be checked before starting due
to risk of seizures (McDonald, et al., 2005).
Minor side effects occur in 31-51%, including
tremor, paraesthesiae, malaise, headache, abnormal liver
function, gingival hyperplasia and hirsutism. Major
complications are reported in 17%, including renal
impairment, pneumonia, infections and neurotoxicity (Van
Assche, et al., 2003). Toxicity can be reduced by using
lower doses (2 mg/kg/day IV), by oral micro emulsion
CsA, or by mono-therapy without corticosteroids
(D’Haens, et al., 2001).
Tacrolimus is another calcineurin inhibitor often
preferred in the transplant setting to CsA. Data from trials
show that it is effective in treatment of steroid refractory
thiopurine naïve UC. A dose is of 0.025 mg/kg twice a day
should achieve trough levels of 10-15 ng/ml (Ogata;
Herrlinger, et al., 2006).
Ulcerative Colitis Chapter 1
- 44 -
Anti-TNF therapies
There are presently two biological agents licensed
for the treatment of IBD in UK; both are monoclonal
antibodies against TNF α (anti-TNF) (Mowat, et al., 2011).
Infliximab (IFX) is a chimeric anti-TNF antibody,
consisting of 75% human IgG and 25% murine component
that actively binds membrane-bound and soluble TNFα.
IFX is given by IV infusion only (Mowat, et al., 2011).
Adalimumab (ADA) is a humanized anti-TNF
antibody, given by sub-cutaneous injection only. At the
present time both agents are licensed for the treatment of
Crohn's disease that has failed to respond to standard
immunosuppression (Mowat, et al., 2011).
Three intravenous infusions of IFX at 0, 2 and 6
weeks were effective in inducing clinical remission;
inducing endoscopic remission and clinical response at 8
weeks. The efficacy of infliximab for treating patients with
moderate to severe UC refractory to corticosteroids and
immunomodulators concluded that it was effective for
inducing clinical remission, clinical response, promoting
mucosal healing, and reducing the need for colectomy in
the short term (Lawson, et al., 2006).
Most recently, the anti-TNF antibody golimumab
has been shown to induce clinical remission and mucosal
healing. Treatment at weeks 0 and 2 (400/200 mg, 200/100
mg) significantly induced clinical remission and mucosal
healing at week 6 suggesting that several anti-TNF
antibodies favor mucosal healing in ulcerative colitis
(Sandborn, et al., 2012).

Ulcerative Colitis Chapter 1
- 45 -
Treatment with anti-TNF therapy is relatively safe if
used for appropriate indications. It should be balanced with
the potential curative option of surgery in UC. Due to the
nature of their effects on TNF, all anti-TNF therapies share
a similar profile of adverse events, including increased risk
of infections from intracellular pathogens, most notably,
TB, other opportunistic infections, autoimmunity,
infusion reactions, and other more rare side-effects
(Mowat, et al., 2011).
Pre-treatment screening for exposure to TB is
important via a history, chest x-ray and tuberculin skin test
if applicable in patients who are about to begin anti-TNF
therapy (Theis and Rhodes, 2008).
The combination of IFX and a thiopurine analogue
or corticosteroids is probably justified to decrease
immunogenicity, which is the source of infusion reactions
and loss of response (Tekkis, et al., 2010).
There is insufficient evidence at present to
recommend the use of interferon γ release assays. Re-
activation of chronic hepatitis B has been reported in
patients treated with IFX. There are no data to suggest it
has any effect on course of chronic hepatitis C.
Pre-treatment screening for exposure to hepatitis B is
important; vaccination should be considered in the non-
immune high-risk patient (Esteve, et al., 2004).
Antibodies formation to infliximab (ATI) can
trigger both acute infusion reactions and delayed serum-
sickness-like reactions. Minor acute reactions usually
respond to slowing the infusion rate or treatment with
antihistamines, paracetamol and sometimes corticosteroids.
Episodic therapy and consequent „drug holiday‟ is
Ulcerative Colitis Chapter 1
- 46 -
associated with increased formation of ATIs, and should be
avoided. ATI formation is associated with increased
incidence of infusion reactions and loss of response (Baert,
et al., 2003). Although ADA is a fully humanized antibody,
it is also associated with the formation of antibodies to
adalimumab (ATA) which have been shown to reduce
efficacy in rheumatoid arthritis and CD (West, et al., 2008).
Prolonged medical therapy for a potentially
pre-malignant condition with anti-TNF therapy creates its
own anxieties. The Mayo Clinic practice and Edinburgh
series confirmed the relatively rare occurrence of
malignancy including basal & squamous cell cancers
(Lees, et al., 2009).
Anti-TNF therapy was associated with an increased
risk of NHL when compared to the general population, but
the risk remained small (6.1 per 10000 patient-years). Anti-
TNF therapy also led to an increased rate of NHL
compared to those treated with immunosuppressants
alone, although this did not reach significance
(Kandiel, et al., 2005).
Reports of optic neuritis, seizure, and new onset or
exacerbation of central nervous system demyelinating
disorders, including multiple sclerosis, have been reported
with the use of all anti-TNFs. Also, Anti-TNF agents are
contraindicated for patients with class III-IV congestive
heart failure due to evidence of increased risks of death
from several clinical trials (Mowat, et al., 2011).

Ulcerative Colitis Chapter 1
- 47 -
UC Management Guidelines
Active ulcerative colitis
When deciding the appropriate treatment strategy for
active ulcerative colitis one should consider the activity,
distribution and pattern of disease. The disease pattern
includes relapse frequency, course of disease, response
to previous medications, side-effect profile of
medication and extra-intestinal manifestations. The age
at onset and disease duration may also be important factors
(Silverberg, et al.,2005).
It is most important to distinguish patients with
severe ulcerative colitis necessitating hospital admission
from those with mild or moderately active disease
who can generally be managed as outpatients
(Schroeder, et al., 1987).
Patients should be encouraged to participate actively
in therapeutic decisions which should be tailored to the
individual (Munkholm, et al., 2010).
The choice of therapeutic strategy should be
influenced by the balance between drug potency and
side-effect profile; previous response to treatment
(especially when considering treatment of a relapse,
treatment of steroid-dependent or refractory disease, or
immunomodulator refractory disease); and the presence of
extra intestinal manifestations which may require
systemic therapy (Su, et al., 2007).

Ulcerative Colitis Chapter 1
- 48 -
Treatment according to site of disease and disease activity
PROCTITIS
Choice of topical formulation should be determined
by the proximal extent of the inflammation (suppositories
for disease to the recto-sigmoid junction, foam or liquid
enemas for more proximal disease) along with patient
preference, such as ease of insertion or retention of enemas
(Safdi, et al., 1997).
A mesalazine 1 g suppository once daily is the
preferred initial treatment for mild or moderately active
proctitis. There is no dose response for topical therapy
above a dose of 1 g daily. Mesalazine foam enemas are an
alternative. Suppositories may deliver drug more
effectively to the rectum and are better tolerated than
enemas. Topical mesalazine is more effective than topical
steroids; consequently topical steroids should be reserved
as second line therapy for patients who are intolerant of
topical mesalazine (Dignass, et al., 2012).
Combining topical with oral mesalazine or topical
steroid is more effective than either alone and should be
considered for escalation of treatment. Oral mesalazine
alone is less effective. Patients who fail to improve on
oral/topical mesalazine and topical corticosteroids should
be treated with the addition of oral prednisolone.
Refractory proctitis may require treatment with
immunosuppressants or biologics (Dignass, et al., 2012).
Fig. (5): Extent of bowel
involvement in UC
(Johns Hopkins, 2013)

Ulcerative Colitis Chapter 1
- 49 -
LEFT SIDED COLITIS
Left-sided colitis of mild-moderate severity should
initially be treated with an amino-salicylate enema 1
g/day combined with oral mesalazine >2 g/day. Foam
enemas are not inferior to liquid enemas for inducing
remission. Also, low volume enemas are not inferior to
high volume enemas and may be better tolerated. Topical
therapy with steroids or 5ASA alone as well as mono-
therapy with oral 5ASA is less effective than oral plus
topical 5ASA therapy. Topical mesalazine is more effective
than topical steroid (Dignass, et al., 2012).
Systemic corticosteroids are appropriate if a patient's
symptoms deteriorate, rectal bleeding persists beyond 10-
14 days, or sustained relief from all symptoms has not been
achieved after 40 days of appropriate mesalazine therapy
(Dignass, et al., 2012).
EXTENSIVE COLITIS
Extensive UC of mild-moderate severity should
initially be treated with oral 5ASA >2 g/day, which should
be combined with topical mesalazine to increase remission
rates if tolerated. Systemic corticosteroids are appropriate if
symptoms of active colitis do not respond to mesalazine by
oral prednisolone combined with steroid enemas. An
appropriate regimen for active disease is prednisolone 40
mg/day for 1 week, reducing by 5 mg/day/week resulting in
an 8 week course, and many different regimes are used
(Dignass, et al., 2012).
Ulcerative Colitis Chapter 1
- 50 -
SEVERE UC OF ANY EXTENT
Acute severe UC is a potentially life-threatening
condition. In 1933, 75% patients died within the first year
after acute presentation with UC and in 1950 a mortality of
22% was reported amongst cases in the first year after
diagnosis. The response rate to appropriately dosed
intravenous steroids has not changed over the last 30 years
(Turner, et al., 2007).
Patients with bloody diarrhea ≥6/day and any signs
of systemic toxicity (tachycardia >90 bpm, fever >37.8 °C,
Hb <10.5 g/dL, or an ESR >30 mm/h) have severe colitis
and should be admitted to hospital for intensive treatment.
All patients admitted with severe colitis require appropriate
investigations to confirm the diagnosis and exclude enteric
infection (Van Assche, et al., 2011).
Corticosteroids are generally given intravenously
using methyl-prednisolone 60 mg/24 h or hydrocortisone
100 mg four times daily. Higher doses are no more
effective, but lower doses are less effective. Bolus injection
is as effective as continuous infusion. Treatment should be
given for a defined period as extending therapy
beyond 7 to 10 days carries no additional benefit
(Rosenberg, et al., 1990).
Consideration of mono-therapy with CsA or IFX if
there is no improvement by day 3, there is subsequent
deterioration or when steroids are best avoided, but for
patients already on immunosuppressive therapy, colectomy
is the first option. Other measures that may considered as
subcutaneous prophylactic low molecular weight heparin,
IV fluid, electrolyte replacement and blood transfusion
(Dignass, et al., 2012).
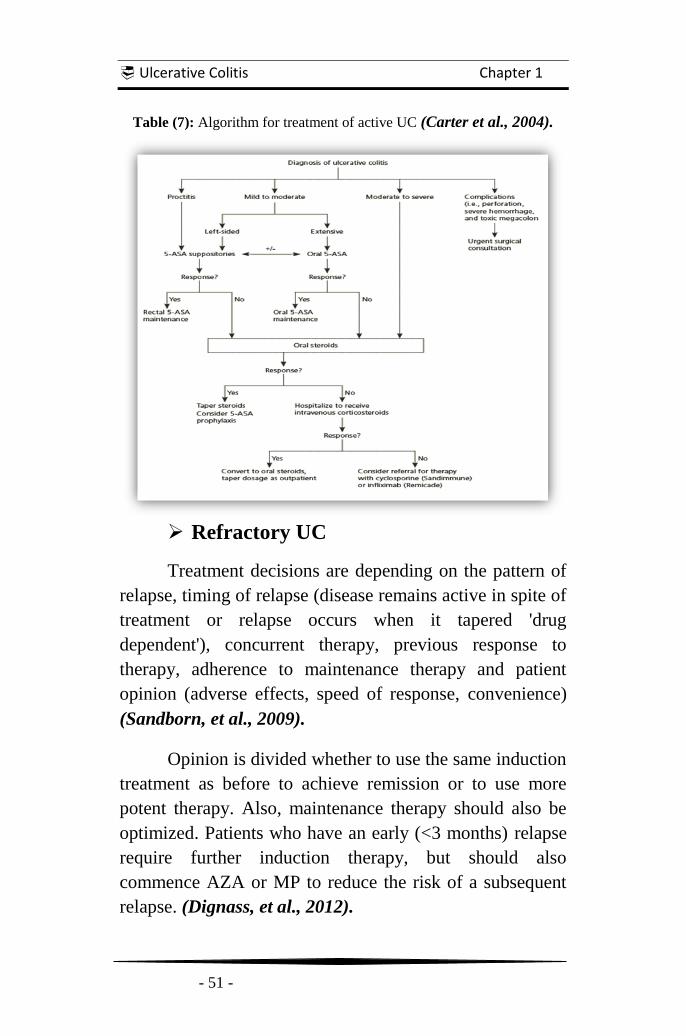
Ulcerative Colitis Chapter 1
- 51 -
Table (7): Algorithm for treatment of active UC (Carter et al., 2004).
Refractory UC
Treatment decisions are depending on the pattern of
relapse, timing of relapse (disease remains active in spite of
treatment or relapse occurs when it tapered 'drug
dependent'), concurrent therapy, previous response to
therapy, adherence to maintenance therapy and patient
opinion (adverse effects, speed of response, convenience)
(Sandborn, et al., 2009).
Opinion is divided whether to use the same induction
treatment as before to achieve remission or to use more
potent therapy. Also, maintenance therapy should also be
optimized. Patients who have an early (<3 months) relapse
require further induction therapy, but should also
commence AZA or MP to reduce the risk of a subsequent
relapse. (Dignass, et al., 2012).

Ulcerative Colitis Chapter 1
- 52 -
‘Steroid-dependent’, active ulcerative colitis
Thiopurines is the first choice of therapy for patients
who flare when steroids are withdrawn. Patients with active
disease despite steroid therapy require appropriate
induction therapy, including consideration of anti-TNF
therapy. Azathioprine is significantly more effective than
mesalazine at achieving clinical and endoscopic
remission in the treatment of steroid-dependent UC
(Ardizzone, et al., 2006).
Oral steroid-refractory ulcerative colitis
For active UC that is refractory to steroids, other
causes of persistent symptoms should be considered. If
active steroid-refractory UC is confirmed, alternative
therapy to induce steroid-free remission is required. Anti-
TNF therapy has clear evidence of benefit in this patient
group (Dignass, et al., 2012).
Adalimumab is now licensed for treatment of
severely active UC in Europe. Moderately active disease
outpatients have the surgical options or admission for IV
steroid therapy (Dignass, et al., 2012).
It should be noted that none of the treatments
discussed above have achieved steroid-free remission at
any time point in the majority of patients. The sequence (or
hierarchy) of therapy has to depend on the individual
circumstances and acceptability to the patient
(Ogata, et al., 2006).

Ulcerative Colitis Chapter 1
- 53 -
Intravenous-steroid refractory UC of any extent
The response to intravenous steroids is best assessed
objectively around the third day. Treatment options
including colectomy should be discussed with patients with
severely active UC not responding to IV steroids. Second
line therapy with ciclosporin, infliximab or tacrolimus may
be appropriate. If there is no improvement within 4-7 days
of salvage therapy, colectomy is recommended. The timing
of colectomy for severe colitis remains one of the most
difficult decisions that a gastroenterologist has to make.
Delaying will increase the morbidity and mortality
associated with subsequent surgery (Dignass, et al., 2012;
Randall, et al., 2010).
Immunomodulator-refractory ulcerative colitis
Patients should be treated with anti TNF therapy or
tacrolimus although colectomy should also be considered.
Continued medical therapy that does not achieve a
clear clinical benefit is not recommended. It is best
reassessed to confirm diagnosis and exclude complications
(Dignass, et al., 2012).
Infliximab at either dose used (5 mg/kg or 10 mg/kg)
achieved clinical remission in a significantly greater
proportion of patients. Using infliximab (three IV infusions
at 0, 2, and 6 weeks) was effective in inducing clinical
remission in patients with moderate to severe UC refractory
to corticosteroids and/or immunomodulators (Lawson, et
al., 2006).Adalimumab also induced clinical remission with
standard induction dose of 160 mg, followed by 80 mg
after 2 weeks. Maintenance doses are then scheduled at 40
mg every other week (Gies, et al., 2010).

Ulcerative Colitis Chapter 1
- 54 -
Refractory proctitis and distal colitis
They present common clinical dilemmas. It is clearly
important to consider and identify the etiology of the
refractory course. One obvious explanation is that the
disease is refractory to medication being prescribed.
However, alternative explanations include poor adherence
to prescribed therapy, delivery of an inadequate
concentration of drug to inflamed mucosa, unrecognized
complications (constipation or infection), and Inappropriate
diagnosis. Therefore, the initial step is to review current
symptoms and treatment to date, with a careful discussion
about adherence followed by reassessment of the diagnosis.
Next step is to ensure that conventional therapy has been
used appropriately. Attention in particular should be paid to
the formulation of topical therapy and whether it was used
in conjunction with an adequate dose of oral therapy.
Endoscopically documented patients have therapeutic
options include admission for IV steroid therapy.
Alternatively, there is open label evidence supporting the
use of salvage medical therapies (Dignass, et al., 2012;
Hebden, et al., 2000; Sandborn, et al., 1994).
An abdominal X-ray can be useful to diagnose
proximal constipation, since abnormal intestinal motility
induces proximal colonic stasis in patients with distal
colitis which may affect drug delivery. If there is visible
faecal loading, a laxative should be considered
(Järnerot, et al., 1985).
There is evidence from studies that appendicectomy
may improve outcome in patients with refractory proctitis.
The outcome of colectomy and pouch formation for distal
colitis is usually good (Brunel, et al., 1999).

Ulcerative Colitis Chapter 1
- 55 -
Maintenance of remission
The goal of maintenance therapy in UC is to
maintain steroid-free remission, clinically and
endoscopically defined. More than half of patients with
UC have a relapse in the year following a flare. The
endpoint is the absence of relapse after 6 or 12 months
(Edwards and Truelove, 1963).
Maintenance treatment is recommended for all
patients. Intermittent therapy is acceptable in a few patients
with disease of limited extent. Choice of maintenance
treatment in UC is determined by disease extent, disease
course (frequency of flares), failure of previous
maintenance treatment, severity of the most recent flare,
treatment used for inducing remission during the most
recent flare, safety of maintenance treatment, and cancer
prevention. Options for a stepwise escalation of
maintenance therapy include dose escalation of oral/rectal
amino salicylates, the addition of azathioprine/
mercaptopurine or Infliximab/anti TNF therapy. Short term
use of systemic or topical steroids may be required when a
rapid response is needed (Dignass, et al., 2012).
Oral 5-ASA containing compounds are the first line
maintenance treatment in patients responding to 5-ASA or
steroids (oral or rectal). Rectal 5-ASA is the first line
in maintenance in proctitis and an alternative in
left-sided colitis. A combination of oral and rectal 5-ASA
can be used as a second line maintenance treatment
(Dignass, et al., 2012).
The minimum effective dose of oral 5-ASA is 1.2 g
per day. For rectal treatment 3 g/week in divided doses is
sufficient to maintain remission (Dignass, et al., 2012).
Ulcerative Colitis Chapter 1
- 56 -
The dose can be tailored individually according to
efficacy. In some cases higher doses ± topical 5-ASA is
useful. There is no robust evidence to support the choice of
any specific preparation for maintenance. Although
sulfasalazine is equally or slightly more effective, other 5-
ASA preparations are preferred for toxicity reasons
(Dignass, et al., 2012).
E. Coli Nissle is an effective alternative to 5-ASA
for maintenance. No evidence has yet been reported that
any other probiotic is effective for maintaining of UC
remission. Also, insufficient data were regarded to
recommend antibiotics for maintenance of remission in UC
(Dignass, et al., 2012).
Azathioprine/mercaptopurine is recommended for
patients with mild to moderate disease activity who have
experienced early or frequent relapse whilst taking 5-ASA
at optimal dose or who are intolerant to 5-ASA, patients
that are steroid-dependent and for patients responding to
ciclosporin (or tacrolimus) for induction of remission
(Dignass, et al., 2012).
In patients responding to anti-TNF agents, both
maintaining remission with AZA/ MP and continuing anti-
TNF therapy with or without thiopurines are appropriate. In
patients with severe colitis responding to IV steroids, IV
CsA or IFX, AZA / MP should be considered to maintain
remission. However, in patients responding to INX
continuing it is also appropriate. The prior failure of
thiopurines favors maintenance with anti-TNF therapy. Due
to limited evidence, no recommendation can be given for
the duration of treatment with AZA or IFX, although
prolonged use of these medications may be considered if
needed (Dignass, et al., 2012).
Ulcerative Colitis Chapter 1
- 57 -
Surgical options in UC
Up to 30% of patients will ultimately require
colectomy for ulcerative colitis. The decision to operate is
best taken by the gastroenterologist and colorectal surgeon
in conjunction with the patient (Hoie, et al., 2007).
Delay in appropriate surgery is associated with an
increased risk of surgical complication. A staged procedure
(colectomy first) is recommended in the acute case when
patients do not respond to medical therapy, or if a patient
has been taking 20 mg daily or more of prednisolone for
more than 6 weeks. If the appropriate laparoscopic skills
are available, a minimally invasive approach is feasible and
may convey some advantages (Dignass, et al., 2012).
The operation of choice in patients with acute severe
colitis failing to respond to intensive medical treatment is a
subtotal colectomy, end ileostomy and preservation of a
long rectal stump. Ileo-anal pouch is anther procedure that
involves panproctocolectomy with permanent end
ileostomy or ileoanal pull through procedure (IAPP)
(Brown, et al., 2008).
To aid decision-making many factors that predict the
need for colectomy in acute severe colitis can broadly be
divided into clinical markers such as stool frequency
(>12/day), pyrexia (>38◦C) and steroid-dependent disease
course, biochemical markers include a high CRP, low
albumin, and pH and radiological/endoscopic criteria
include the presence of colonic dilatation (>5.5 cm), the
depth of colonic ulceration, or mucosal islands on a plain
abdominal radiograph (Roussomoustakaki, et al., 1997).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 58 -
Stem Cells and Stem Cell therapy for UC
Discovery of Stem Cells:
. Stem cells are how we all begin. They are
undifferentiated cells that go on to develop into any of
more than 200 types of cell an adult human body holds
(Becker AJ, et al., 1963).
The stem cell is the origin of life, as stated first by
the great pathologist Rudolph Virchow, “All cells come
from cells”, and “All the cells of the human body arise
from a preexisting stem cell, the fertilized egg”
(Sell, 2004).
Fig. (6): Stem cells (Bloomberg News, 2012)

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 59 -
Introduction to Stem Cells:
The zygote is the ultimate stem cell produced from
fertilization. It is totipotent with the ability to produce all
the cell types of the species including the trophoblast and
the embryonic membranes. The zygote undergoes a process
of cell divisions and cell migrations known as cleavage. It
begins when several successive cell divisions resulting in a
doubling of the cell number and a reduction in the cell size.
At the 32 - 64 cell stage each cell is called a blastomere
(Sell, 2004).
The blastomeres stick together to form a tight ball of
cells called a morula. Each of these cells retains
totipotential. The next stage is the blastocyst which
consists of a hollow ball of cells; trophoblast cells along
the periphery develop into the embryonic membranes and
placenta while the inner cell mass develops into the fetus.
Beyond the blastocyst stage, development is characterized
by cell migration in addition to cell division
(Kuehnle and Goodell, 2002).
The gastrula is composed of three germ layers: the
ectoderm, mesoderm and endoderm. As development
proceeds, there is a loss of potential and a gain of
specialization, a process called determination. The cells of
the germ layers are more specialized than the fertilized egg
or the blastomere. The germ layer SCs give rise to
progenitor cells (precursor cells) which can further divide
to produce the terminally differentiated cell. The ectoderm
(outer layer) gives rise to the future nervous system and the
epidermis. The mesoderm (middle layer) gives rise to the
connective tissue, muscles, bones and blood, and the
endoderm (inner layer) forms the gastrointestinal tract and
the respiratory system (Kuehnle and Goodell, 2002).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 60 -
Fig. (7): Development of Preimplantation Blastocyst in Humans(Terese Winslow, 2001).
Early in embryogenesis, some cells migrate to the
primitive gonad or genital ridge. These are the precursors to
the gonad of the organism and are called germinal cells.
These cells are not derived from any of the three germ
layers but appear to be set aside earlier. In adults, ovum and
sperm are derived from these cells by special cell division
called meiosis (Sell, 2004).
Fig. (8):Pluripotent stems cells (Mike Jones, 2006).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 61 -
Definitions and Characteristics of SCs:
Stem cells (SCs) are undifferentiated cells that have
the capability of both Self-regeneration (self-renewal) and
Potency (differentiation) into mature specialized cells
through replication (Ricart E, et al., 2010).
Self-regeneration is the ability of stem cells to
divide and produce more stem cells. During early
development, the cell division is symmetrical i.e. each cell
divides to give rise to daughter cells each with the same
potential. Later in development, the cell divides
asymmetrically with one of the daughter cells produced is
also a stem cell and the other is a more differentiated cell
(Piscaglia, et al., 2008).
Potency is the ability to differentiate or the potential
to develop into different cell types. A totipotent stem cell
(e.g. fertilized egg) can develop into all cell types including
the embryonic membranes. A pluripotent stem cell can
develop into cells from all three germinal layers. A
multipotent stem cells could produce only cells of a
closely related family of cells (e.g. hematopoietic SCs).
Other cells can be oligopotent, bipotent or unipotent
depending on their ability to develop into few, two or one
other cell type(s) (Sell, 2004).
There are differences in how progenitor cell division
is described. For instance, according to one source (Robey,
2000), when a SC divides at least one of the daughter cells
it produces is also a SC; when a progenitor cell undergoes
cell division it produces two specialized cells. A different
source (Sell, 2004), explains that a progenitor cell
undergoes asymmetrical cell division, while a SCs
undergoes symmetrical cell division.

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 62 -
The apparent inconsistency of these two versions
illustrates the diversity and complexity of progenitor cells
and their role in differentiation. This diversity is reflected
in the nomenclature as well; progenitor cells are also called
Transit-amplifying cells, Precursor cells, Progenitors,
Lineage stem cells, and Tissue - determined stem cells
(Kuehnle and Goodell, 2002).
Table (8):Stem cells during differentiation at each stage (Sell, 2004).
Table (9): Types of cell division (Lindblad, 2004)
Early in development
Late in development: type 1
Late in development: type 2

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 63 -
Types of SCs:
A. Embryonic Stem Cells:
Embryonic stem cells (ESCs) are defined by
its origin. They are generally isolated from the
inner cell masses (ICMs) of blastocysts, which consist
of pluripotent cell populations that are able to
generate primitive ectoderm during embryogenesis.
More specifically the primitive ectoderm gives rise
during the gastrulating process to the primary germ
layers, including ectoderm, mesoderm, and endoderm
(Yao, et al., 2006).
They possess the dual ability to undergo unlimited
self-renewal and to differentiate in all fetal and
adult stem cells and their more differentiated
progenitors. They are pluripotent cells, capable of
forming tissues from all three germ layers in vitro and vivo
(Swenson and Theise, 2010).
Therefore, they represent a useful source of stem
cells for investigating the molecular events that are
involved in normal embryogenesis and generating a large
number of specific progenitors for cellular therapies. It
could use in studies of congenital birth defects,
chromosomal abnormality effects and childhood tumors
development (Trounson; Karp et al., 2006).
Stem Cells and Stem Cell Therapy for UC Chapter 2
- 64 -
Advantages & Disadvantages of Embryonic SCs:
Advantages: They are
Flexible: They have the potential to make
anybody cell.
Immortal: One cell line can potentially supply
endless amounts of cells with carefully defined
characteristics.
Easily available: human embryos can be obtained
from fertility clinics in developed countries.
Disadvantages: They could be
Difficult to control: ESCs may be tumorigenic
when transplanted in vivo. The method for
inducing the cell type needed to treat a particular
disease must be defined and optimized
(Fujikawa, et al., 2005).
At odds with a patient's immune system: It is
possible that transplanted cells would differ in
their immune profile from that of the recipient
and so would be rejected. But this could be
avoided through genetic engineering them to
express MHC antigen of the recipient.
(Kuehnle and Goodell, 2002).
Ethically controversial: as life begins at
conception, doing research on human embryos is
unethical.

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 65 -
B. Adult Stem Cells:
The term adult stem cells (ASCs) refers to any cell
which is found in a developed organism that has two
properties: the ability to divide and create another cell like
itself and also divide and create a cell more differentiated
than itself. Also known as somatic (from Greek "of the
body") stem cells and germ line (giving rise to gametes)
stem cells, they can be found in children, as well as adults
(Doyonnas and Blau, 2004).
ASCs allow specific tissues to regenerate throughout
life. They also have the ability for self-renewal and multi-
lineage differentiation. In fact, the list for
identifying ASCs and lineage specific progenitor cells is
growing. A great deal of ASCs research has
focused on clarifying their capacity to divide or
self-renew indefinitely and their differentiation potential
(Preston, et al., 2003).
Distinct stem cell types have been established in
specific niches in many adult mammalian tissues and
organs, such as brain, skin, eyes, heart, kidneys,
lungs, gastrointestinal tract, pancreas, liver, breast,
ovaries, prostate, and testis(Griffiths, et al., 2005;
Liu, et al., 2004).
The replenishment of epithelial cell lineages within
the gastrointestinal tract (GIT) is a frequent process,
occurring every 2-7 days under physiological conditions.
This process may contribute to the generation of
new cell progenitors, which repopulate the damaged tissues
during diverse pathological disorders, such as inflammation
and ulceration (Schier and Wright, 2005).
Stem Cells and Stem Cell Therapy for UC Chapter 2
- 66 -
This process is regulated by multipotent SCs, which
give rise to all gastrointestinal epithelial cell lineages and
can regenerate whole intestinal crypts and gastric glands.
The SCs of the GIT are localized within the
niches in the intestinal crypts and gastric glands
(Brittan and Wright, 2002).
These SCs can give rise to all cell types within the
crypt, including absorptive, goblet, entero-endocrine and
Paneth cells. Similarly, the SCs in the large intestine or
colon, which are localized at the bottom of crypts, may also
give rise to the proliferative progenitors that differentiate
toward all lineages during epithelium regeneration
(Reya and Clever, 2005).
Fig. (9): Embryonic stem cells (Kuehnle and Goodell, 2002).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 67 -
Advantages & Disadvantages of Adult SCs:
Advantages: They are
Already somewhat specialized: the inducement
may be simpler.
Immune hardy: Recipients who receive products
of their own SCs will not experience immune
rejection.
Flexible: it may be used to form other tissue
types.
Mixed degree of availability: Some ASCs are
easy to harvest and others, such as neural (brain)
stem cells, can be dangerous to the donor.
Disadvantages: They could be
Minimal quantity: difficulty in obtaining it in
large quantities
Finite: They don't live as long in a culture as
ESCs.
Genetically unsuitable: The harvested SCs may
carry genetic mutations for disease or become
defective during experimentation (Kuehnle and
Goodell, 2002).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 68 -
Progenitor cells:
Stem cells generate an intermediate cell type or types
before they achieve their fully differentiated state. The
intermediate cell is called precursor or progenitor cell.
Progenitor cells in fetal or adult tissues are partially
differentiated cells that divide and give rise to differentiated
cells. Such cells are usually regarded as “committed” to
differentiate along a particular cellular pathway
(Robey, 2000).
The concept of a progenitor cell is difficult to define.
Like SCs, progenitor cells have a capacity to differentiate
into a specific type of cells. However, in contrast to SCs,
they are already far more specific than SCs: they are
pushed to differentiate into their “target” cell. Despite the
difficulty of defining progenitors, the term is frequently
used in researches (Noctor, et al., 2007).
Most progenitors are described as unipotant or
multipotant. In this point of view, they may be compared to
ASCs, on the other hand, they are said to be in a farther
stage of cell differentiation. They are in the “center”
between stem cells and fully differentiated cell. The kind of
potency they have depends on the type of their “parent”
stem cell and also on their niche (Noctor, et al., 2007).
Progenitors exhibit slow growth and their main role
is to replace cells lost by normal attrition. Growth factors
and cytokines trigger the progenitors towards the damage
tissue. At the same time, they differentiate to the target cell
to recover the injured tissue (Noctor, et al., 2007).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 69 -
Plasticity of SCs:
Recently, several examples have been reported
which demonstrate that these stem cells, under certain
conditions, can be induced to form other cell types. This
property is called plasticity. For example neural stem cells
(NSCs) can give rise to blood and skeletal muscle. Also
BM cells can give rise to muscle, liver cells, and astrocytes
(Kuehnle and Goodell, 2002)
Therefore, they are considered multipotent, since
they can produce mature cell types of one or more lineages.
What determines SC potency largely depends on intrinsic
properties of SCs provided by the niche, microenvironment
where SCs reside, (Baharvand, et al., 2007).
Plasticity is the ability of stem cells to expand their
potential beyond the tissue from which they are derived.
For example, Dental pulp stem cells develop into tissue of
the teeth but can also develop into neural tissue (Nosrat, et
al., 2004). There are at least 2 alternative pathways to be
kept in mind when discussing mechanisms of SC plasticity:
i- Tran's differentiation is the direct conversion of one
cell type to another completely different one(Shen, et
al., 2003), e.g. Tran's differentiation of pancreatic
cells into hepatic cells and vice versa (Priller, 2004).
ii- Cell fusion: ESCs can fuse in vitro with a very small
proportion of BM stem cells, the fusion product, seen
as a new cell type, expressed genes of both fusion
partners in various degrees. Here the chromosomes of
the fused cells mosaic, presenting as a
mixture of chromosomes of different origin
(Doyonnas and Blau, 2004).
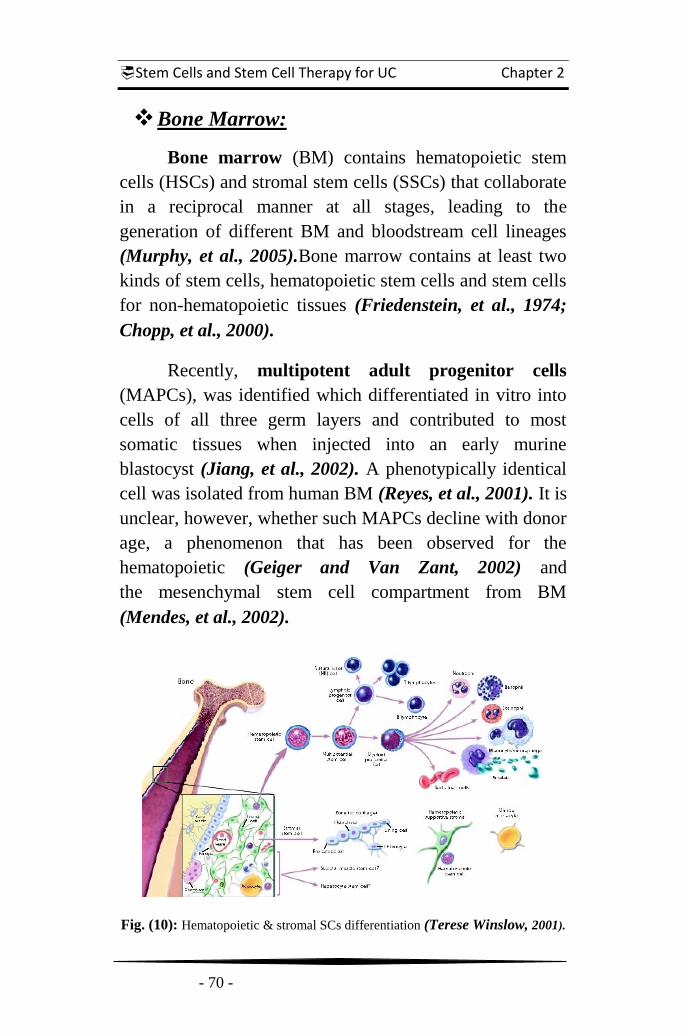
Stem Cells and Stem Cell Therapy for UC Chapter 2
- 70 -
Bone Marrow:
Bone marrow (BM) contains hematopoietic stem
cells (HSCs) and stromal stem cells (SSCs) that collaborate
in a reciprocal manner at all stages, leading to the
generation of different BM and bloodstream cell lineages
(Murphy, et al., 2005).Bone marrow contains at least two
kinds of stem cells, hematopoietic stem cells and stem cells
for non-hematopoietic tissues (Friedenstein, et al., 1974;
Chopp, et al., 2000).
Recently, multipotent adult progenitor cells
(MAPCs), was identified which differentiated in vitro into
cells of all three germ layers and contributed to most
somatic tissues when injected into an early murine
blastocyst (Jiang, et al., 2002). A phenotypically identical
cell was isolated from human BM (Reyes, et al., 2001). It is
unclear, however, whether such MAPCs decline with donor
age, a phenomenon that has been observed for the
hematopoietic (Geiger and Van Zant, 2002) and
the mesenchymal stem cell compartment from BM
(Mendes, et al., 2002).
Fig. (10): Hematopoietic & stromal SCs differentiation (Terese Winslow, 2001).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 71 -
Types of ASCs:
A. Hematopoietic Stem Cells:
The ability of HSCs to self-renew continuously in the
marrow and to differentiate into the full complement of cell
types found in blood qualifies them as the premier ASCs.
HSCs are among the few SCs to be isolated in adult
humans. They reside in the BM localized near endosteal
bone surface and sinusoidal endothelium and under some
conditions migrate to other tissues through the blood. HSCs
are also normally found in the fetal liver, spleen, umbilical
cord and placenta blood (Kiel, et al., 2005).
HSCs can migrate from endosteal surface into
vascular niche under specific stimuli such as injury and
after treatment with myeloablative agents. Hence, the
localization of HSCs and their progenitors within BM
vascular niche may allow their rapid release into
circulation. In addition, HSCs were also localized at the
sinusoidal endothelium on the spleen tissue sections,
it has been proposed that this site could also
constitute an extra medullary niche for HSC homing
(Wilson and Trumpp, 2006).
There is a growing body of evidence that HSCs are
plastic that, at least under some circumstances, they are
able to participate in the generation of tissues other than
those of the blood system. The expectations have risen that
HSCs will be able to give rise to multiple cell types from
all three germ layers. If HSCs are truly multipotant, their
potential for life-saving regenerative therapies may be
considerably expanded in the future (Murphy, et al., 2005)
.

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 72 -
B. Mesenchymal Stem Cell:
The BM stroma is a highly vascularized, complex
structure containing mesenchymal stem cells and
extracellular matrix elements supporting for hematopoiesis
(Neiva et al., 2005). They are variously referred to as
mesenchymal stem cells or marrow stromal cells. The term
"mesenchymal stem cells" has been used only relatively
recently. MSCs provide the stromal cells constituting the
microenvironment within the marrow cavities.
More recent data indicate broader potential for MSCs
(Jiang, et al., 2002).
Mesenchymal stem cells are an entirely different
type of adult stem cell. MSCs can be derived from bone
marrow, fat, or other tissues. MSCs are perhaps more
restricted in their differentiation potential to mesodermal
tissues such as fat, cartilage and bone. Transplanted MSCs
do not reconstitute hematopoietic lineages, but can alter the
host immune response. (Swenson and Theise, 2010).
Depending upon the environment, MSCs give rise to
many cell lineages including epithelial cells, astrocytes,
osteoblasts, chondrocytes, adipocytes and muscle,
promoting regeneration of damaged tissue in vivo
(Uccelli, et al., 2008).
In vitro, MSCs have vast proliferative potential, can
clonally regenerate and can give rise to differentiated
progeny. They also exhibit anti proliferative and anti-
inflammatory properties in vitro/vivo, making them
candidates for treatment of Immunomodulatory drugs
(IMiDs) (Dazzi, et al., 2007).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 73 -
Among the BM stromal stem cells, there are
primitive mesodermal progenitor cells (MPCs) and
multipotent adult progenitor cells, which have been co-
purified with other mesenchymal stem cells, also as known
as bone marrow stromal cells (BMSCs). MPCs might
differentiate into different mesenchymal cell types
including bone-forming cells, osteoblasts, chondrocytes, &
adipocytes (Reyes, et al., 2001), as well as neuron-like cells
& glial cells, as in well-defined culture mediums in vitro
(Sanchez-Ramos, et al., 2000).
Furthermore, MAPCs and MSCs also show the
ability to migrate extensively throughout the circulation.
For instance, it has been reported that the transplantation of
MAPCs leads to their engraftment and differentiation into
the hematopoietic lineages and the epithelium of the liver,
lungs, and gut in non irradiated mice, which were further
enhanced in an irradiated host (Jiang, et al., 2002).
The injection of stromal BM cells was also
accompanied by their migration throughout the forebrain
and cerebellum, where they differentiated into astrocytes
(Kopen, et al., 1999).
Regardless of whether or not MSCs are true stem
cells, clinical benefit from MSCs may not require sustained
engraftment of large numbers of cells or differentiation into
specific tissues. It is possible that a therapeutic benefit can
be obtained by local paracrine production of growth factors
and by the provision of temporary antiproliferative and
immune-modulatory properties (Panes and Salas, 2009).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 74 -
Role of Stem Cells in tissue regeneration:
If body tissue is damaged, stem cells head for the
damaged area and advance the process of healing.
However, day-to-day processes in the human body also rely
on stem cells: our erythrocytes only live for about 120 to
130 days, by which time they have become too old, cannot
transport enough oxygen and have to be replaced. This task
is taken over by the HSCs that can be found in the bone
marrow. According to theoretical calculations, about 350
million new erythrocytes are formed every minute. Most of
the other somatic cells are also replaced regularly: liver
cells after 10 to 15 days, white blood cells after 1 to 3 days
(Tuch, 2006).
During development, stem cells divide and produce
more specialized cells. Stem cells are also present in the
adult in far lesser numbers. Adult stem cells are observed in
continually-replenished cells such as blood cells and skin
cells, stem cells have recently been found in other issues
such as neural tissues (Hans Schöler, 2007).
Organ regeneration has long been believed to be
through organ-specific and tissue-specific stem cells.
Hematopoietic stem cells were believed to replenish blood
cells, stem cells of the gut to replace cells of the gut and so
on. Recently, using cell lineage tracking, stem cells from
one organ have been discovered that divide to form cells of
another organ. Hematopoietic stem cells can give rise to
liver, brain and kidney cells. This plasticity of adult stem
cells has been observed not only under experimental
conditions, but also in people who have received bone
marrow transplants (Hans Schöler, 2007).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 75 -
If the goal of medicine has been to treat symptoms of
diseases and possibly remove their causes, scientists and
physicians point now to a more ambitious target. The
primary objective of regenerative medicine is the complete
structural and functional recovery of the damaged organ
(Koh and Atala, 2004).
Regeneration coincides with tissue homeostasis and
involves the replacement of cells lost by normal
weal and tear and, ideally, following injury
(Ferguson and O'Kane, 2004).
Tissue regeneration is achieved by two mechanisms:
(1) Circulating stem cells divide and differentiate under
appropriate signaling by cytokines and growth factors, e.g.
blood cells; and
(2) Differentiated cells which are capable of division can
also self-repair, e.g. hepatocytes, endothelial cells, smooth
muscle cells, keratinocytes and fibroblasts. These fully
differentiated cells are limited to local repair. For more
extensive repair, stem cells are maintained in the quiescent
state, and can then be activated and mobilized to the
required site (Forbes, et al., 2002).
For wound healing in the skin, epidermal stem cells
and bone-marrow progenitor cells both contribute. Thus it
is likely that organ-specific progenitors and hematopoietic
stem cells are involved in repair, even for other organ repair
(Asahara and Isner, 2004).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 76 -
Stem Cells Therapies:
There is great interest in the biology of ASCs
because of their capacity to self-renew and their high
plasticity. These traits enable ASCs to produce diverse
mature cell progenitors that actively participate in the
maintenance of homeostatic processes by replenishing the
cells that repopulate the tissues/organs during a lifespan
and regenerate damaged tissues during injury
(Leri, et al., 2005).
In general, embryonic, fetal and adult stem cells
show several common functional properties. Common
properties include their high self-renewal capacity and
potential to generate differentiated cell progenitors of
different lineages under simplified culture conditions in
vitro and after transplantation in host in vivo
(Trounson, 2006).
Therefore, the use of stem cells and their progenitors
is a promising strategy in cellular and genetic therapies for
multiple degenerative disorders, as well as adjuvant
immunotherapy for diverse aggressive cancer types
(Lindvall, et al., 2004).
Stem cell-based therapies hold great promise for
many diseases (Swenson and Theise, 2010).
The main clinical application of stem cells is as a
source of donor cells to be used to replace cells in
transplantation therapy. Parkinson and Alzheimer diseases,
muscular degenerative disorders, chronic liver and heart
failures, type 1 and 2 diabetes, arthritis, as well as skin, eye,
kidney, and hematopoietic disorders, could be treated by
the stem cell-based therapies (Hesdorffer, et al., 1998).
Stem Cells and Stem Cell Therapy for UC Chapter 2
- 77 -
Induced pluripotent stem cells (iPSCs) can be
derived from adult somatic cells forced to reprogram to an
ES-like state in culture. iPSCs can be redirected toward
other phenotypes under specific culture conditions. iPSCs
are not derived from embryos, avoiding ethical concerns
regarding the use of human embryos. iPSCs can
also be made from any patient, allowing the production
of patient-specific and disease-specific cells for
research treatment. Undifferentiated ESCs and iPSCs can
both give rise to teratomas after transplantation, so
complete eradication of undifferentiated cells is a critical
step toward the clinical use of cell therapy when
they are used to produce differentiated cells for therapy
(Swenson and Theise, 2010).
Adult stem cells exist in all types of tissues
throughout the body and function as a reservoir to replace
damaged or ageing cells (Ricart E, et al., 2010). They are
derived from mature organs and are much more limited in
differentiation potential compared with ESCs or iPSCs.
Also, ASCs might be better considered as
multipotent “progenitor” cells rather than stem cells
(Swenson and Theise, 2010).
Due to the inability to harvest or expand SCs from
most adult organs efficiently and safely (e.g. liver, GIT,
heart), a majority of human stem cell trials have focused on
clinical applications for HSCs, MSCs, or both, which can
be easily obtained in clinically sufficient numbers from
peripheral blood, bone marrow, or umbilical cord blood and
placenta (Chamberlain, et al., 2007).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 78 -
Stem cell transplantation in treatment of IBD
Applications of stem cells into autoimmune diseases
(AID) are currently being actively sought. Autoimmune
diseases result in the patient's own immune system
attacking its own tissues. The symptoms of the particular
autoimmune disease match the type of tissue that is under
attack. For example, autoimmune antibodies to a nerve
receptor can result in progressive paralysis
(Tyndall and Saccardi, 2002).
For stem cell therapeutics, one approach is to try to
suppress the patient's native immune system, which is
attacking the patient, and then replacing bone marrow with
other grafted stem cells. Human clinical trials using high
dose immunosuppression and chemotherapy, combined
with auto graft hematopoietic cell transplants have
been used in several autoimmune diseases including:
systemic sclerosis, rheumatoid arthritis, myasthenia gravis,
systemic lupus erythematosus and multiple sclerosis
(Burt, et al., 2003).
Intensive myelosuppressive or myeloablative
chemotherapy followed by transplantation of stem cells
derived directly from the bone marrow or from peripheral
blood after suitable conditioning, has revolutionized the
management of haematological malignancy and
haemoglobinopathies. Because these maneuvers cause
significant and prolonged alterations in the body's immune
system and function, SCT has been used for severe cases of
diseases that are believed to have an autoimmune basis
(Marmont and Van Bekkum, 1995).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 79 -
Some diseases seem to have longer remissions while
others have more frequent recurrences. Furthermore, for
those patients in whom there is a relapse of the autoimmune
disease, may responded to agents that were ineffective
before the stem cell therapy (Tyndall and Saccardi, 2002).
Stem cell transplantation can either be allogeneic
(from a donor, usually HLA matched sibling)
(Soutar and King, 1995), or autologous (harvested from
the individual undergoing treatment with later reinfusion)
(Duncombe, 1997), also syngeneic transplantation
(from an identical twin) is possible (Snowden, et al., 1998).
HSCs have been proposed as a novel form of cell
therapy for damaged organs (Anversa and Nadal-Ginard,
2002). Hematopoietic stem cell transplantation (HSCT) has
been used to treat patients with other autoimmune diseases
that include loss of immune tolerance or a Th1-
predominant immune response (Lowenthal, et al., 1993).
Most patients with AID have a near-normal life
expectancy. Nevertheless, some patients suffer severe,
therapy-resistant progressive autoimmunity. HSCT is a
potential therapy for people with such severe refractory
diseases. HCT involves the administration of HSC, which
are capable of giving rise to all mature haematopoietic
cell types and some non haematopoietic cell types
(Sykes, et al., 2005).
IBD is an acute or chronic inflammation of the
mucosal layers of the intestine. It may be considered
an autoimmune disease, resulting from inappropriate
immune reactivity against one‟s own tissues in the GIT
(Swenson and Theise, 2010).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 80 -
The epithelial lining of the intestinal tract is
constantly being shed and renewed, using a stem cell
lineage system similar to the bone marrow's hematopoietic
stem cell system. The stem cells lie at the bottom crypts
of villi that line the intestinal wall and daughter
cells then differentiate as the migrate up the villi
(Marshman, et al., 2002).
The mainstay of clinical treatment is a combination
of anti-inflammatory agents and immunosuppressive
medications. Newer agents, including monoclonal
antibodies directed against TNF, are available for patients
who are unable to achieve remission with standard
immunosuppression. Despite treatment, the morbidity and
cost of IBD remain high. Corticosteroids are not effective
for maintaining remission of IBD and induce well-known
adverse side effects. New treatment approaches are needed
(Swenson and Theise, 2010).
Recent advances reveal a primary role of
dysregulation of the immune system in the pathogenesis of
IBD. Sophisticated genome-wide association studies
implicate maladaptive signaling of a number of cytokines
and their receptors (Abraham and Cho, 2009).
Stem cell therapy for inflammatory bowel disease
(IBD) is still in its very early stages. It is known that
isolated hematopoietic stem cells in vitro can reconstitute,
among other things, epithelial cells of the GIT
(Theise, 2005).
The advantage with IBD is that it is an inflammatory
process, and inflamed tissue is one of the triggers that
appear to recruit circulating SCs. From a therapeutic
standpoint for IBD, this raises the possibility of treating

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 81 -
patient with SCs that are able to secrete an IBD alleviating
medication such as antibodies that can neutralize tumor
necrosis factor (TNF). The SCs would then be recruited
into the intestinal wall, locally secrete the TNF antibodies,
soothe the inflammation of the bowel and thus control the
symptoms of IBD (Brittan and Wright, 2002).
Recent studies on the use of HSCT for refractory
Crohn's disease and evaluations of patients who have
undergone HSCT for other reasons show remission of CD
following the transplantation. HSCTs were either
allogeneic or autologous. Allogeneic transplants may help
by overcoming CD's genetic predisposition to circulate
leukocytes, while autologous transplants may clear the
body of committed lymphocyte clones and restore the
lymphocytic imbalance. Most patients responded well and
some were in complete clinical remission 10 years after
transplantation (Hawkey, 2004).
BM transplant therapy for refractory IBD remains
experimental. This approach should be limited to patients
with severe disease who have exhausted standard
treatment options, and is best performed in the
context of an appropriately designed clinical trial
(Swenson and Theise, 2010).
Results from phase I and phase II clinical trials
indicate that the approach is feasible and may result in a
remission with regard to tumor formation. Phase III trials
currently underway in Europe and the USA should help
clarify these issues (Swenson and Theise, 2010).
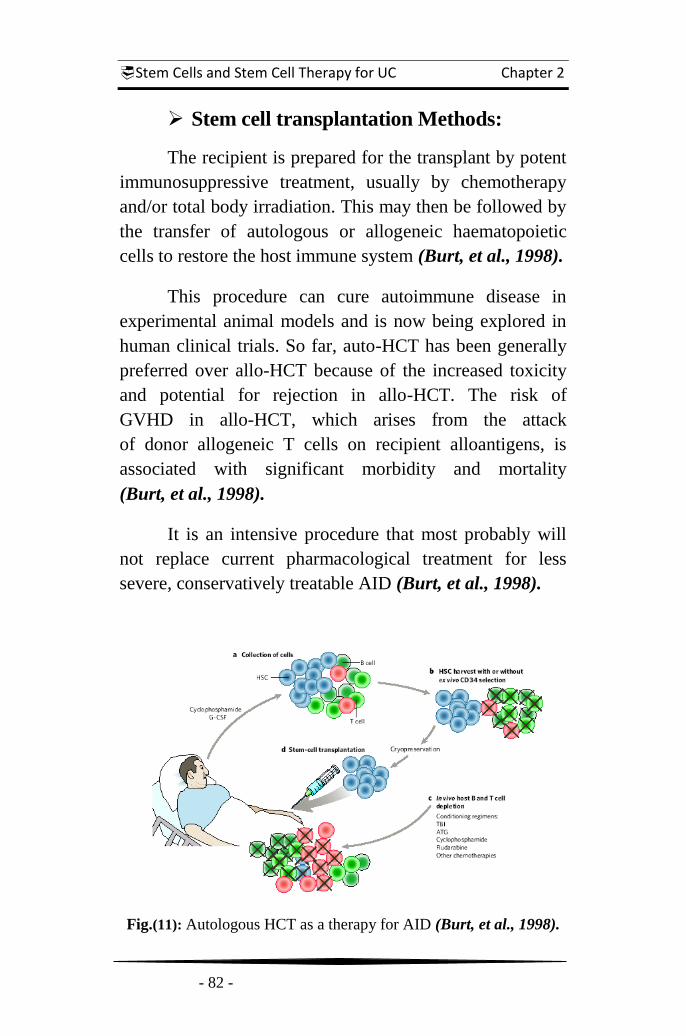
Stem Cells and Stem Cell Therapy for UC Chapter 2
- 82 -
Stem cell transplantation Methods:
The recipient is prepared for the transplant by potent
immunosuppressive treatment, usually by chemotherapy
and/or total body irradiation. This may then be followed by
the transfer of autologous or allogeneic haematopoietic
cells to restore the host immune system (Burt, et al., 1998).
This procedure can cure autoimmune disease in
experimental animal models and is now being explored in
human clinical trials. So far, auto-HCT has been generally
preferred over allo-HCT because of the increased toxicity
and potential for rejection in allo-HCT. The risk of
GVHD in allo-HCT, which arises from the attack
of donor allogeneic T cells on recipient alloantigens, is
associated with significant morbidity and mortality
(Burt, et al., 1998).
It is an intensive procedure that most probably will
not replace current pharmacological treatment for less
severe, conservatively treatable AID (Burt, et al., 1998).
Fig.(11): Autologous HCT as a therapy for AID (Burt, et al., 1998).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 83 -
The steps in autologous HCT (Sykes, et al., 2005):
a. Stem-cell collection: HSCs are either harvested from the
bone marrow under anesthesia or collected after
mobilization to the peripheral blood by treating the
patient with growth factor (for example, G-CSF).
b. HSC harvest, with or without ex vivo selection using
antibody specific for CD34 (a marker of HSCs): efforts
may or may not be made to deplete T and B cells from
the marrow or mobilized peripheral blood cells. This is
usually achieved by HSC positive selection on the basis
of CD34 expression. The HSC preparation is
cryopreserved.
c. In vivo lymphocyte depletion: various conditioning
regimens with the goal of minimizing the burden of auto
reactive B and T cells are given to patients. These
include combinations of chemotherapeutic agents, total-
body irradiation (TBI) and in vivo lymphocyte depletion
by antibodies, such as anti-thymocyte globulin (ATG),
and these treatments often deplete host HSC as well.
d. Stem-cell transplantation: after conditioning, the
cryopreserved HSC preparation is thawed and returned
to the recipient to reconstitute hematopoiesis

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 84 -
The steps in allogeneic HCT (Sykes, et al., 2005):
a. Mobilization regimen: these are similar to the methods
employed for autologous HCT, except that
chemotherapies are not used. Mobilization is achieved
using the growth factor G-CSF.
b. HSC harvest: This step is similar to that used for auto-
HCT.
c. In vivo lymphocyte depletion: this step depletes host T
and B cells to prevent rejection and treat the AID; it
may also be aimed at depleting donor T cells (to prevent
GVHD).
d. Stem - cell transplantation: as for auto-HCT.
e. Post - transplantation immunosuppression: as
prophylaxis against both rejection mediated by residual
host T cells and GVHD mediated by contaminating
donor T cells, allo-HCT usually requires additional post-
transplantation immunosuppression with agents such as
cyclosporine A.
Fig. (12):SCs transplant
using patient’s own cells
(Preeti Gokal Kochar, 2004)

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 85 -
Mechanisms by which HCT treat autoimmunity:
Several mechanisms for correction of autoimmunity
may apply to HCT (Burt, et al., 1998).
a. Immunomodulation by immunosuppressive
conditioning: potent immunosuppressive treatments
such as total body irradiation (TBI), cyclophosphamide
(CY), anti-CD2 antibodies (anti-CD2), anti-CD52
antibodies (anti-CD52), fludarabine & anti-thymocyte
globulin (ATG) can eliminate the majority of B and T
cells. In addition to alloreactive and auto reactive
memory B and T cells, others are depleted.
b. Immune-mediated destruction of auto reactive cells
(graft-versus-autoimmune host T and B cells). Donor T
cells recognize alloantigens and destroy residual
memory B and T cells. This mechanism is applicable to
allo-HCT only.
c. Deletion of alloreactive and auto reactive T cells in
thymus. If both donor and host cells contribute to
hematopoiesis and to the antigen-presenting cell (APC)
pool in the thymus, the new T-cell repertoire generated
in the recipient thymus is deleted of T cells recognizing
both allo- and autoantigens expressed by HSC of both
origins.
d. Induction of energy and deletion of auto reactive and
alloreactive T cells in the periphery. Costimulatory
blockade of the CD40−CD154 and CD28−CD80−CD86
pathways in concert with allogeneic BMT can overcome
the T-cell barrier to allo-HSC engraftment, which in
turn quickly produces donor-specific tolerance and
could tolerize cross-reactive auto reactive lymphocytes
as well. This mechanism plays a role only in allo-HCT.

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 86 -
e. Tolerization of peripheral auto reactive/alloreactive
T cells by regulatory T cells. CD4+CD25
+ regulatory
T cells have been implicated in the maintenance of
peripheral tolerance to organ-specific self-antigens as
well as alloantigens. The secretion of TGF- and IL-10
by regulatory T cells has been suggested to mediate this
process. Both allo-HCT and auto-HCT could
incorporate this mechanism.
f. Tolerization of auto reactive and alloreactive B cells. In
addition to alloantigens, haematopoietic chimaerism
could potentially tolerize pre-existing recipient B cells
to autoantigens expressed by donor haematopoietic
cells. This mechanism plays a role only in allo-HCT.
Fig.(13): Mechanism by which HCT ameliorate AID (Burt, et al., 1998).
Donor-derived cells are shown in green and host-derived cells are shown in red.

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 87 -
Potential risks of stem cell therapies
The risks of autologous or allogeneic hematopoietic
stem cell transplantation are well known, and include
hemorrhage, sepsis and GVHD. Allogeneic bone marrow
donors are thoroughly screened to prevent transmission of
infectious diseases, though acute infections may be
missed and laboratory errors are always possible
(Swenson and Theise, 2010).
As well as the intrinsic dangers of SCT, which
include mucositis (a painful inflammation and ulceration of
the mucous membranes lining the digestive tract), there are
also some data suggesting that SCT may either worsen or at
least not prevent IBD in some patients. Some patients have
been reported to develop UC or colonic ulceration after
allogeneic SCT (Murayama, et al., 1995).
It would appear that the risk of infectious disease or
malignancy with autologous MSC therapy should be low.
As with allogeneic hematopoietic or whole-organ
transplantation, there is a small risk of transmission of
malignancy from donor to recipient. MSC themselves may
give rise to tumors, though evidence for this is limited
(Swenson and Theise, 2010).
Reports suggest that MSC-derived tumor formation
may be a concern, and long-term MSC culture is best
avoided. Suppression of GVHD by allogeneic MSC may
also be coincident with reduction in the beneficial graft-vs.-
tumor effect, therefore it is essential to follow the long-term
incidence of hematologic disease recurrence in patients
treated with MSC (Swenson and Theise, 2010).

Stem Cells and Stem Cell Therapy for UC Chapter 2
- 88 -
A clinical trial in stem cell therapies for UC
In 2010, a study included 44 patients with ulcerative
colitis (UC), which was implemented MSC transplantation
to determine the efficacy and safety of mesenchymal
stromal cells of bone marrow in the treatment of patients
with UC. 40 patients with UC who received standard
therapy and 12 patients treated by infliximab therapy.
The patients were observed for 24 months after
transplantation and evaluated using the average values of
indices of Rahmilevich clinical activity, indices of
endoscopic and histological activity scales Mayo and Gebs.
BM cells were obtained from the donor's sternum or iliac
crest and culture of it injected in the drip IV single dose.
The results show that in 34 patients after the
induction of MSCs was statistically significant compared
with the group of patients treated with drugs only 5-
aminosalicylic acid and corticosteroids, reducing the
clinical and morphological indices of inflammatory
activity. In 12 patients with UC include MSCs in the
treatment program did not have a therapeutic effect.
Application of MSC allowed canceling corticosteroids in
most patients with hormone-dependent and steroid
resistance forms of UC, and in 7 to reduce the dose of
prednisolone to 5 mg/day.
Finally researchers said that using of MSCs can be
evaluated as a new strategic direction for therapy UC.
MSC, have powerful immunomodulatory effects, reduce
the activity and stimulate regeneration of intestinal mucosa,
thereby increasing the duration of remission, reduces risk
of recurrence of disease (Lazebnik, et al., 2010).

Patients and Methods
- 89 -
Patients and Methods
This pilot study was a phase II randomized add-on
clinical trial that was done for the first time in EGYPT and
in Ain Shams University to investigate the role of bone
marrow stem cell transplantation as a potential line of
treatment in ulcerative colitis patients.
It was conducted on 10 patients with confirmed
diagnose of ulcerative colitis. Cases were collected from
Internal Medicine Departments and Out Patient Clinics
from Ain Shams, Nasser Institute and Electricity Hospitals.
This study hypothesized that infusion of HSCs may
help to reverse the inflammatory process in patients with
ulcerative colitis. Thus, we conducted a human trial to
evaluate safety and feasibility of autologous bone marrow
HSC transplantation in Egyptian patients with ulcerative
colitis and to evaluate the HSC transplantation as a
therapeutic option.
All patients assessed initially at January 2013 and
three months later at April 2013 after autologous
hematopoietic stem cells transplantation and follow up
includes comparison the changes in the patient's clinical
assessment, nutritional status, biochemical profile,
endoscopic findings, medication requirement, and quality
of life of those patients before and after potential therapy.
The patients of this study continued on the same
medications they were on previously but changes in their
use and dose were done according to the clinical
assessment throughout the follow up period.
Patients and Methods
- 90 -
All patients will be selected according to:
Inclusion criteria:
Adult Middle Eastern patients below 60 years old.
Documented diagnosed Ulcerative Colitis.
Written consent from every patient in our study.
Exclusion criteria:
Patients with Crohn's disease.
Patients with advanced systemic disease.
Patients with any malignancies or blood diseases.
Patients with other autoimmune diseases.
Refusal to sign a written consent.
All patients will be subjected to :
Clinical assessment :
Complete history taking.
Thorough medical examination.
Body mass index.
Investigations :
Laboratory markers (HB% - ALB - ESR - CRP).
Endoscopy : Lower GI Endoscopy (Colonoscopy).
Staging:(Mayo Scoring for Assessment of UC Activity)
Treatment modifications : Any changes in the type, form
or dose of different traditional pharmacological lines of
treatment according to case status.

Patients and Methods
- 91 -
Stem Cells Transplantation:
Stem cells transplantation was done in Nozha
International Hospital. All steps were performed within
complete sterile field in the following sequence:
A- Bone marrow aspiration:
1. The patient is placed in prone position on the
operating table.
2. Visual access is created to iliac crest by making a
puncture in the right iliac crest.
3. Penetrate bone marrow of ilium using standard
BM aspiration needle with needle length of
about 4 cm.
4. Upon penetration approximately 1 cm into
marrow cortex, the aspiration needle is advanced
forward gently through the marrow until the
needle contacts the cortical bone surface.
5. Spike with heparin solution (2000 µ/mL).
Ensure heparin solution has coated the entire
marrow contacting surfaces.
6. Procedure is complete after 100 ml of BM has
been aspirated from the penetration in the
right ilium.
B- Bone marrow transferring:
1. Remove Processing Disposables (PDs) from
packaging and place on an appropriate
workspace.
2. Slowly dispense 50 ml of bone marrow aspirate
(BMA) into the marrow chamber of each PD
through the RED access site.

Patients and Methods
- 92 -
C- Bone marrow processing:
1. Load centrifuge by placing the fully PDs into the
Smart PReP2 System (the Harvest instrument).
2. Close lid machine and press ʻSTARTʼ button to
start the process which takes 14 min. to be
finished. Then remove PDs from the Harvest
when cycle completed.
3. The plasma volume used for cell resuspension is
about 50 ml in chamber of each PD. a syringe is
used to withdraw unwanted plasma from the
chamber by being careful not to disturb the lower
cell layer.
4. To resuspend the BM cells into the plasma we
withdraw remaining plasma via a 50 ml syringe
with blunt needle, and gently inject it back and
forth into the plasma chamber. We repeat this 2-3
times till cells visibly suspend in plasma then we
withdraw total volume into the syringe.
5. Transfer full plasma volume which contains the
SCs (100ml) back in sterile field to a 350 ml
plastic bag (JMS Single Blood Bag).
D- Bone marrow injection:
1. A puncture of peripheral vein was performed by
using wide pore cannula.
2. IV infusion is performed through an infusion set
connects cannula with plastic bag to transfer
100ml of autologous BM mononuclear cell layer
contains SCs.
3. After that, the cannula was flushed with 10 ml of
normal saline and the procedure was finished.
After the stem cell infusion the catheter
was removed.

Patients and Methods
- 93 -
All patients take 500 ml saline 0.9% contains 1gm
cefoperazone (cefobid®) before starting the injection. They
were kept under medical observation for their vital data for
6 hours after that they discharged and reassessment
3 months later.
Bone marrow aspiration
Bone marrow transferring
Bone marrow processing
Bone marrow injection
Fig. (14): Stem Cells Transplantation for Patient No. 2
at Nozha International Hospital

Patients and Methods
- 94 -
Statistical Method
Statistical presentation and analysis of the present
study was conducted, using the mean, standard deviation,
Paired t-test, Chi- by SPSS V17.
Mean = n
x
Where: = sum & n = number of observations.
Standard Deviation [SD]:
SD 1
x-x 2
n
Standard Error [SE]:
n
SD SE
Paired t-test:
SE
dX
d
t
Where:
dX = Mean's difference between pre and post
SEd = Standard error of difference between pre and post.
Unpaired Student T-test was used to compare
between related samples.
Chi-square:
The hypothesis that the row and column variables are
independent, without indicating strength or direction of the
relationship. Pearson chi-square and likelihood-ratio chi-
square. Fisher's exact test and Yates' corrected chi-square
are computed for 2x2 tables.

Results
- 95 -
Results
This study was conducted on 10 patients with
confirmed diagnose of ulcerative colitis. The cases
chosen of those had a resistant active disease with
variable degrees of severity.
All cases were evaluated according to the
"Mayo Scoring System for Assessment of UC Activity"
which ranges from 0 to 12, with higher scores indicating
more severe disease (D'Haens, et al., 2007). This score
was used for both initial evaluation and 3 months post
therapy re-evaluation.
They are diagnosed and managed according to
European Crohn's and Colitis Organization (ECCO). They
were selected randomly of various extents and severity
assessed according to the Montreal classification and
Truelove & Witts criteria (Dignass, et al., 2012).
The patients included in this study are males (40%)
and females (60%). Their ages ranged from 24-50 years
with mean of (39.2 ± 10.2) and their BMI score ranged
from 20-33 with mean of (25.0 ± 4.7). All the patients
undergo to the autologous stem cell transplantation, and all
the patients tolerated the treatment protocol well without
any complications or side effects related to the procedure.

Results
- 96 -
Table (10): Showing comparison between patients
before and after the SCT as regard the presence of diarrhea
Diarrhea Negative Positive Total
Before N 0 10 10
% 0.00 100.00 100.00
After N 9 1 10
% 90.00 10.00 100.00
Chi-square
X2 4.9
P-value 0.026*
There were statistically significant differences as
regard the presence of diarrhea as 10 patients complained
of diarrhea associated with loose, mucus and bloody stool
in the initial clinical assessment but only one of them
continue complaining of this complaint in the final clinical
assessment after the procedure during the follow up period.
Fig. (15): Assessment of the presence of diarrhea
in patients pre and post the SCT procedure

Results
- 97 -
0
10
20
30
40
50
60
70
80
Before After
Negative
Positive
Rectal bleeding
Table (11): Showing comparison between patients
before and after the SCT as regard the rectal bleeding
Rectal bleeding Negative Positive Total
Before N 4 6 10
% 40.00 60.00 100.00
After N 8 2 10
% 80.00 20.00 100.00
Chi-square X2 2.37
P-value 0.124
There were statistically none significant differences
as regard the presence of rectal bleeding as 6 patients
complained of rectal bleeding in the initial clinical
assessment, 4 of them become free of rectal bleeding in the
final clinical assessment after the procedure during the
follow up period.
Fig. (16): Assessment of the rectal bleeding
in patients pre and post the SCT procedure

Results
- 98 -
0
10
20
30
40
50
60
70
80
Before After
Negative
Positive
Abdominal pain
Table (12): Showing comparison between patients
before and after the SCT as regard the abdominal pain
Abdominal pain Negative Positive Total
Before N 2 8 10
% 20.00 80.00 100.00
After N 8 2 10
% 80.00 20.00 100.00
Chi-square
X2 1.011
P-value 0.315
There were statistically none significant differences
as regard the presence of abdominal pain as8 patients
complained of abdominal pain in the initial clinical
assessment, 6 of them become free in the final clinical
assessment after the procedure during the follow up period.
Fig. (17): Assessment of the abdominal pain
in patients pre and post the SCT procedure

Results
- 99 -
Table (13): Showing comparison between patients
before and after the SCT as regard the disease extent
Disease extent E1 E2 E3 Total
Before N 0 4 6 10
% 0.00 40.00 60.00 100.00
After N 4 6 0 10
% 40.00 60.00 0.00 100.00
Chi-square
X2 0.277
P-value 0.599
There were statistically none significant differences
as regard the disease site and extent as 4 patients having
left sided colitis and 6 have pancolitis in the initial
endoscopic assessment but by the end of the study
6patientshave left sided colitis and 4 have proctitis as
recorded in the final endoscopic assessment after the
procedure during the follow up period.
Fig. (18): Assessment of the disease extent
in patients pre and post the SCT procedure

Results
- 100 -
Table (14): Showing comparison between patients
before and after the SCT as regard the disease severity
Disease severity
After Total cases (before) Mild
Mild to moderate
Moderate
Be
fore
Moderate N 2 2 0 4
% 20.00 20.00 0.00 40.00
Moderate to sever
N 2 0 2 4
% 20.00 0.00 20.00 40.00
Sever N 0 2 0 2
% 0.00 20.00 0.00 20.00
Total cases (after)
N 4 4 2 10
% 40.00 40.00 20.00 100.0
Chi-square X2 10.008 P-
value 0.040*
There were statistically significant differences as
regard the disease degree and severity as patients were:
4 moderate, 4 moderate to severe and 2 severe cases
in the initial assessment but by the end of the study
we have only 2 moderate case and 8 cases
evaluated as a mild or mild to moderate cases in
the final assessment after the procedure during the
follow up.
Fig. (19): Assessment of the disease severity
in patients pre and post the SCT procedure
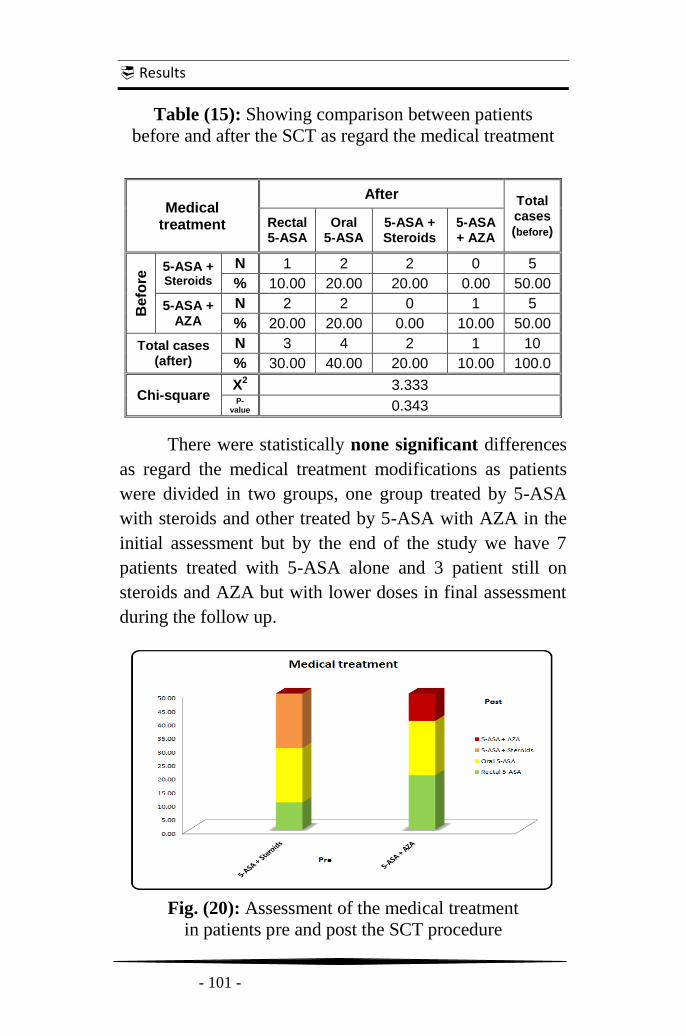
Results
- 101 -
Table (15): Showing comparison between patients
before and after the SCT as regard the medical treatment
Medical treatment
After Total cases (before)
Rectal 5-ASA
Oral 5-ASA
5-ASA + Steroids
5-ASA + AZA
Be
fore
5-ASA + Steroids
N 1 2 2 0 5
% 10.00 20.00 20.00 0.00 50.00
5-ASA + AZA
N 2 2 0 1 5
% 20.00 20.00 0.00 10.00 50.00
Total cases (after)
N 3 4 2 1 10
% 30.00 40.00 20.00 10.00 100.0
Chi-square X2 3.333 P-
value 0.343
There were statistically none significant differences
as regard the medical treatment modifications as patients
were divided in two groups, one group treated by 5-ASA
with steroids and other treated by 5-ASA with AZA in the
initial assessment but by the end of the study we have 7
patients treated with 5-ASA alone and 3 patient still on
steroids and AZA but with lower doses in final assessment
during the follow up.
Fig. (20): Assessment of the medical treatment
in patients pre and post the SCT procedure

Results
- 102 -
Table (16): Showing comparison between patients before and after the SCT as regard the disease outcome
There were statistically significant differences as regard the disease degree and severity as patients were
divided in 5 cases of moderate, moderate to severe and severe pancolitis; and 5 cases of moderate and moderate
to severe left sided colitis in the initial global assessment but we end the study with having only 2 cases of
moderate left sided colitis case while other 8 cases evaluated between mild proctitis and left sided colitis in the
final global assessment during the follow up period.
Disease outcome After Total
cases (before)
Mild proctitis
Mild left sided colitis
Mild to moderate proctitis
Mild to moderate left sided colitis
Moderate left sided colitis
Be
fore
Moderate active left sided colitis
N 1 1 0 0 0 2
% 10.00 10.00 0.00 0.00 0.00 20.00
Moderate active pancolitis
N 0 0 1 1 0 2
% 0.00 0.00 10.00 10.00 0.00 20.00
Moderate to severe active left sided colitis
N 1 1 0 0 1 3
% 10.00 10.00 0.00 0.00 10.00 30.00
moderate to severe active pancolitis
N 0 0 1 0 0 1
% 0.00 0.00 10.00 0.00 0.00 10.00
Sever active pancolitis N 0 0 0 1 1 2
% 0 0 0 10.00 10.00 20.00
Total cases (after) N 2 2 2 2 2 10
% 20.00 20.00 20.00 20.00 20.00 100.0
Wilcoxon Signed Ranks Test
Z 17.27 P-
value 0.038*

Results
- 103 -
Fig. (21): Assessment of the disease outcome in patients pre and post SCT procedure

Results
- 104 -
Fig. (22): Endoscopic picture of a patient before and after SCT procedure.
Before After
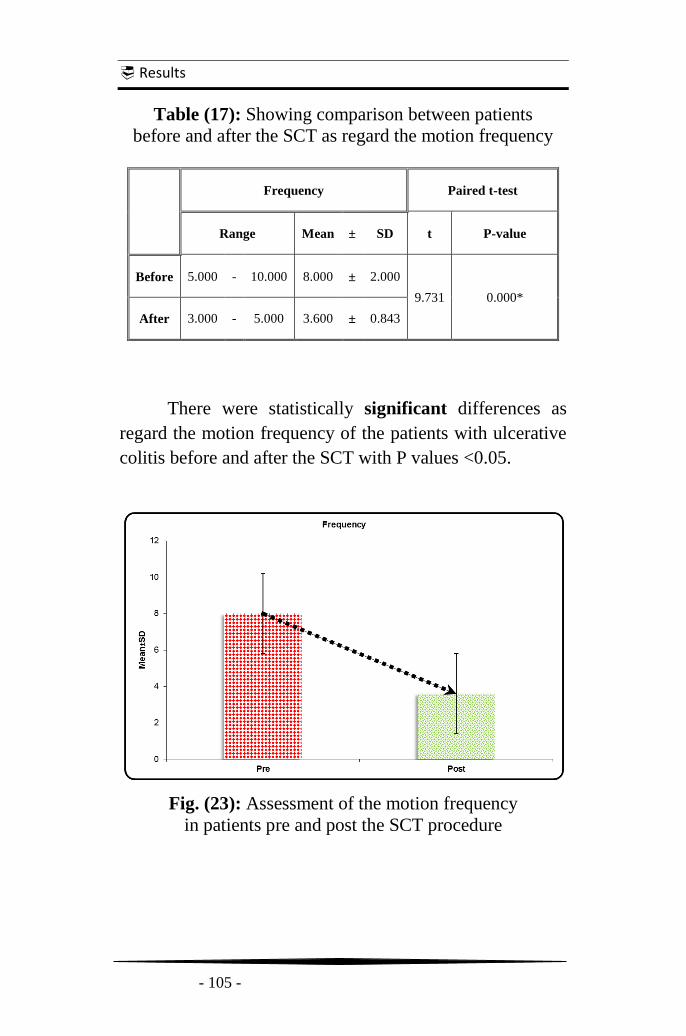
Results
- 105 -
Table (17): Showing comparison between patients
before and after the SCT as regard the motion frequency
Frequency Paired t-test
Range Mean ± SD t P-value
Before 5.000 - 10.000 8.000 ± 2.000
9.731 0.000*
After 3.000 - 5.000 3.600 ± 0.843
There were statistically significant differences as
regard the motion frequency of the patients with ulcerative
colitis before and after the SCT with P values <0.05.
Fig. (23): Assessment of the motion frequency
in patients pre and post the SCT procedure

Results
- 106 -
Table (18): Showing comparison between patients
before and after the SCT as regard the body temperature
Temperature Paired t-test
Range Mean ± SD t P-value
Before 37.000 - 37.900 37.440 ± 0.381
1.354 0.209
After 36.900 - 37.500 37.220 ± 0.262
There were statistically non significant differences
as regard body temperature of the patients with ulcerative
colitis before and after the SCT with P values >0.05.
Fig. (24): Assessment of the body temperature
in patients pre and post the SCT procedure

Results
- 107 -
Table (19): Showing comparison between patients
before and after the SCT as regard the heart rate
Heart rate Paired t-test
Range Mean ± SD T P-value
Before 73.000 - 100.000 86.600 ± 10.679
3.321 0.009*
After 65.000 - 90.000 80.400 ± 8.809
There were statistically significant differences as
regard the heart rate of the patients with ulcerative colitis
before and after the SCT with P values <0.05.
Fig. (25): Assessment of the heart rate
in patients pre and post the SCT procedure

Results
- 108 -
Table (20): Showing comparison between patients
before and after the SCT as regard the body mass index
BMI Paired t-test
Range Mean ± SD t P-value
Before 19.800 - 33.200 25.040 ± 4.739
0.178 0.863
After 20.500 - 32.300 24.980 ± 4.468
There were statistically non significant differences
as regard the BMI of the patients with ulcerative colitis
before and after the SCT with P values >0.05.
Fig. (26): Assessment of the body mass index
in patients pre and post the SCT procedure

Results
- 109 -
Table (21): Showing comparison between patients
before and after the SCT as regard the serum albumin
ALB Paired t-test
Range Mean ± SD t P-value
Before 3.100 - 5.100 4.000 ± 0.772
-0.309 0.764
After 3.100 - 4.700 4.040 ± 0.659
There were statistically non significant differences
as regard the serum albumin of the patients with ulcerative
colitis before and after the SCT with P values >0.05.
Fig. (27): Assessment of the serum albumin
in patients pre and post the SCT procedure
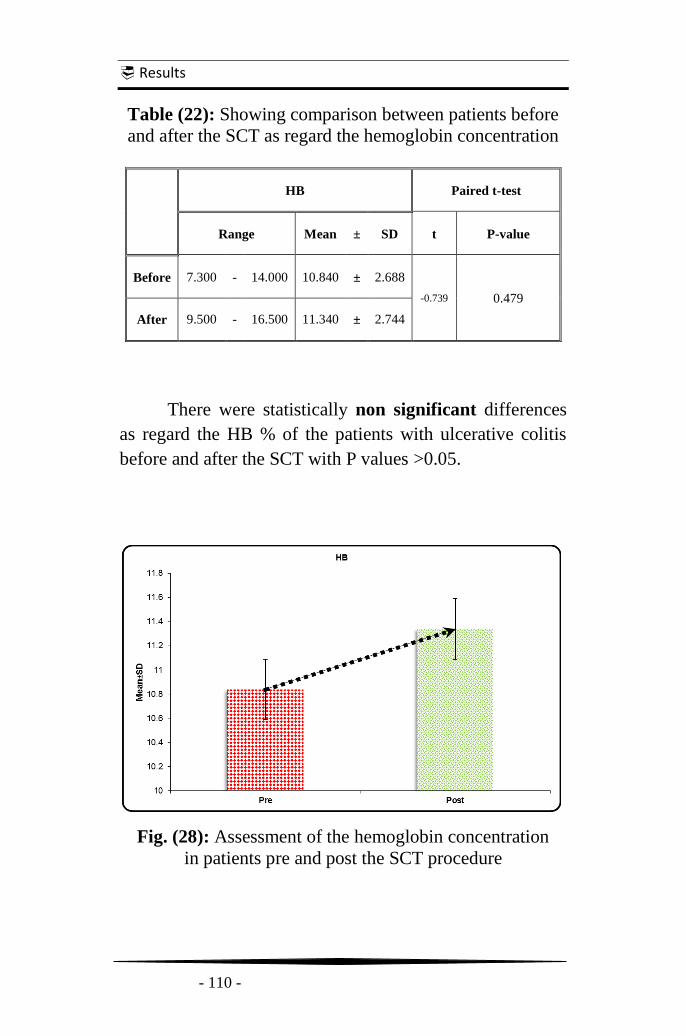
Results
- 110 -
Table (22): Showing comparison between patients before
and after the SCT as regard the hemoglobin concentration
HB Paired t-test
Range Mean ± SD t P-value
Before 7.300 - 14.000 10.840 ± 2.688
-0.739 0.479
After 9.500 - 16.500 11.340 ± 2.744
There were statistically non significant differences
as regard the HB % of the patients with ulcerative colitis
before and after the SCT with P values >0.05.
Fig. (28): Assessment of the hemoglobin concentration
in patients pre and post the SCT procedure

Results
- 111 -
Table (23): Showing comparison between patients before
and after the SCT as regard erythrocyte sedimentation rate
ESR Paired t-test
Range Mean ± SD T P-value
Before 20.000 - 140.000 75.400 ± 49.332
3.628 0.006*
After 13.000 - 100.000 49.200 ± 32.913
There were statistically significant differences as
regard the ESR of the patients with ulcerative colitis before
and after the SCT with P values <0.05.
Fig. (29): Assessment of the erythrocyte sedimentation rate
in patients pre and post the SCT procedure

Results
- 112 -
Table (24): Showing comparison between patients
before and after the SCT as regard the C-reactive protein
CRP Paired t-test
Range Mean ± SD t P-value
Before 16.000 - 24.000 20.667 ± 3.724
3.273 0.012*
After 11.000 - 19.000 14.500 ± 12.124
There were statistically significant differences as
regard the CRP of the patients with ulcerative colitis before
and after the SCT with P values <0.05.
Fig. (30): Assessment of the C-reactive protein
in patients pre and post the SCT procedure
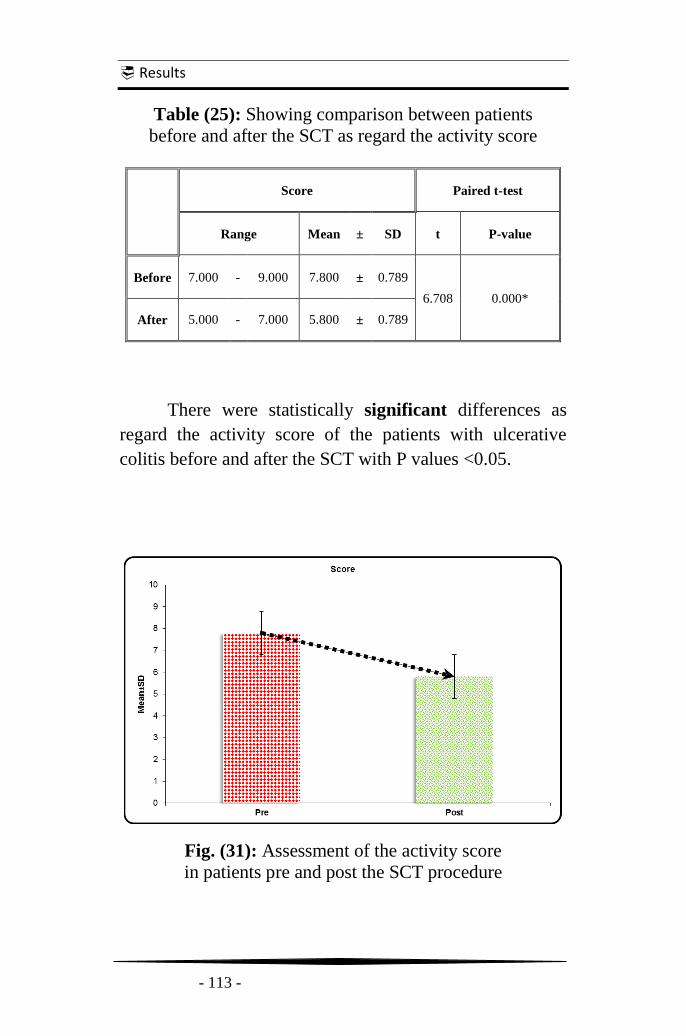
Results
- 113 -
Table (25): Showing comparison between patients
before and after the SCT as regard the activity score
Score Paired t-test
Range Mean ± SD t P-value
Before 7.000 - 9.000 7.800 ± 0.789
6.708 0.000*
After 5.000 - 7.000 5.800 ± 0.789
There were statistically significant differences as
regard the activity score of the patients with ulcerative
colitis before and after the SCT with P values <0.05.
Fig. (31): Assessment of the activity score
in patients pre and post the SCT procedure

Discussion
- 114 -
Discussion
„„Whatever deserves to exist deserves to be known‟‟
(Francis Bacon)
So much has been written and rewritten on stem
cells, their potentials, their properties, their possible uses
and their risks. Protagonists of a new scientific era, SCs are
promising tools for treating diseases of any sort, from
degenerative disorders to inborn errors of metabolism, to
organ failures. SCs represent the key to tissue genesis,
regeneration and homeostasis. This has led to the concept
of regenerative medicine, which is based on their potential
for therapies aimed to facilitate the repair of degenerating
or injured tissues (Piscaglia et al., 2008).
SCs can be obtained from various sources, including
embryos, fetal tissues, umbilical cord blood, and also
terminally differentiated organs. Once isolated, these cells
may be forced - ex vivo or in vivo - to expand and
differentiate into functional progenies suitable
for the cell replacement and the tissue engineering
(Mimeault et al., 2007).
Recent progress in cell biology resulting in the
isolation and characterization of bone marrow SCs and
progenitor cells further increases the expectation for a new
approach to the treatment of genetic and chronic diseases
(Sakaida et al.;2005).

Discussion
- 115 -
It is well known that ESCs may give rise to tumors,
while cancers derived from ASC-therapies haven‟t been
reported. Nonetheless, the long-term safety of ASC
infusion has not been adequately tested. Preclinical
studies and clinical trials with longer follow up
periods should be recommended prior to large-scale
clinical applications of such cell-based therapies
(Piscaglia, 2008).
The manipulation of adult stem cells (ASCs) seems to
be particularly promising, as it could improve the
endogenous regenerative potential without risk of
rejection and overcome the ethical and political
issues related to embryonic stem cell research
(Mimeault et al., 2007).
There are at least two types of SCs in the human
BM; mesenchymal SCs, and hematopoietic SCs.
HSC are continuously moving between the
bone marrow and peripheral blood. This movement is
critical for hematopoietic homeostasis & is hypothesized to
contribute to homeostasis and tissue repair
(Schachinger et al., 2006).
SC-based therapies could be used to cure
inherited or genetic degenerative alterations associated
with the loss of adult SC functions, such as cancers,
immune system and hematopoietic disorders,
cardiovascular, muscular and neurological diseases,
gastrointestinal pathologies, diabetes mellitus and
chronic hepatopathies (Mimeault et al., 2007).
Discussion
- 116 -
This pilot study was a phase II randomized add-on
cross-over clinical trial that was done in Ain Shams
University to investigate the role of bone marrow stem cell
transplantation as a potential line of treatment in ulcerative
colitis patients.
It was conducted on 10 patients with confirmed
diagnose of ulcerative colitis. Cases were collected from
Internal Medicine Departments and Out Patient Clinics
from Ain Shams, Nasser Institute and Electricity Hospitals.
This study hypothesized that infusion of HSCs may
help to reverse the inflammatory process in patients with
ulcerative colitis. Thus, we conducted a human trial to
evaluate safety and feasibility of autologous bone marrow
HSC transplantation in Egyptian patients with ulcerative
colitis and to evaluate the HSC transplantation as a
therapeutic option compared to the conventional treatment.
All patients assessed before and 3 months after
autologous hematopoietic stem cells transplantation and
follow up includes comparison the changes in the patient's
clinical assessment, nutritional status, biochemical profile,
endoscopic findings, medication requirement, and quality
of life of those patients before and after potential therapy.
This study goes with agreement with Lazebnik, et
al., (2010), who initiated a pilot study to assess the safety
and efficacy of mesenchymal stromal cells of bone marrow
in the treatment of patients with UC. The patients were
observed for 24 months after transplantation and evaluated
using the average values of indices of Rahmilevich clinical
activity, indices of endoscopic and histological activity
scales Mayo and Gebs.

Discussion
- 117 -
In this study, there was improvement in the quality of
life in most of the patients after the procedure. Such
improvement was recorded according to the clinical,
laboratory and endoscopic assessment. This goes with the
trial of Lazebnik, et al., (2010), in which there was
improvement in the quality of life of 34 patients of the 44
patients included in their study at the end of follow up.
As regard clinical symptomatology, there was
significant improvement in most of the 10 patients
regarding the presence of diarrhea but in rectal bleeding,
abdominal pain and other associated symptoms includes
weight loss, anorexia, and urgency the improvement was
partially and statistically insignificant. Generally, most of
the patients regain their normal bowl habits with well-
formed stool and shifted form positive records at initial
clinical evaluation before the SCT to negative records at
the final clinical evaluation as they stopped complaining of
diarrhea, pain, bleeding, etc., after 3 months the SCT. This
goes with results of clinical trial of Lazebnik, et al., (2010).
There were statistically significant differences
regarding the motion frequency of the patients before SCT
with mean of (8.000 ± 2.000) and after SCT with mean of
(3.600 ± 0.843), with (P value <0.05) with improvement of
the frequency to the normal ranges. However, individual
non statistical analysis of each patient showed sustained
decline in most of patients over follow up period. Patients
No.1 and 3 decline from 9-10 to 3-4 times daily while
patients' No. 7, 8, 9 and 10 decline from 6-7 to 4-5 times
daily. This goes with results of Lazebnik, et al., (2010).

Discussion
- 118 -
This reflects that SCT has made improvement in the
quality of life to patients of UC but the mechanism for
the effect isn't clear but may reflect activation of
genes corresponding to an enterocyte differentiation
program in the transplanted SCs upon exposure to
injured colon environment.
Also, it found that heart rate was significantly
different before and after SCT while body temperature
was statistically insignificant. Vital data are considered as
supporting factors in assessment especially because it is
recorded in the former evaluation scoring systems of UC
but we didn't entitle them alone as they might be affected
by other several factors.
The body mass index (BMI) and serum albumin
which is an important laboratory marker that reflect the
nutritional status of the patients with ulcerative colitis
showed statistically non-significant differences in their
levels before and after the SCT in patients over the follow
up period. Analyzing the results of each patient without
statistical analysis showed limited increase in the level of
the s. albumin by about 0.5gm/dl in patients' No. 1 and 6
while slight decrease in patient No. 2 detected. Other
patient s. albumin didn't remarkably change. On the other
hand, BMI wasn't changed though out the study in the all of
the patient except patient No. 9 who gain about two
kilograms over his weight that recorded in his final
assessment which may be due to improved anorexia or
from the effect of the corticosteroids therapy. Results
regarding the BMI and s. albumin weren't evaluated in
study of Lazebnik, et al., (2010).

Discussion
- 119 -
Regarding the hemoglobin concentration level of
patients, there were statistically non-significant differences
before and after the SCT. Patient No. 3 showed elevation in
her HB% levels from 7.3g/dL before procedure to 9.5g/dL
after it in later follow up visits without blood transfusion.
This may be related to disease activity improvement. This
goes with results of clinical trial of Lazebnik, et al., (2010).
As regard the C-reactive protein (CRP), there was
statistically significant improvement in its level in patients
with Mean of (20.667 ± 3.724) before the SCT and a Mean
of (14.50 ± 12.124) 3 month after SCT. This also goes with
the results of the study of Lazebnik, et al., (2010).When
analyzing the results of each patient alone from the Master
Sheet; we found that the decreased was remarkable in some
patients as in patients' No. 1, 3, 4, 5, 6, 7 and 9. Other
patients showed not more than slight decrease as in patient
No. 2 showed no decrease at all. This difference between
the CRP results couldn't be confirmed due to small number
of patients. We need to have larger groups of patients to be
reevaluated upon with long-term follow-up.
Erythrocyte sedimentation rate (ESR) showed
statistically significant decrease in its results in patients 3
months after the SCT as differences regarding the ESR of
the patients before SCT with mean of (75.400 ± 49.332)
and 3 months after SCT with mean of (49.200 ± 32.913),
with (P value <0.05). When analyzing the results of each
patient alone from the Master Sheet, we found that the
decreased was in parallel with that in the CRP values as
mentioned and goes with results of Lazebnik, et al., (2010).

Discussion
- 120 -
Although the medical treatment changes
were statistically non-significant, it was considerable in
the individual non statistical analysis which showed
changes over the follow up period in the prescription, form
and dose of the used drugs for treatment of the patients in
our study. This also goes with the results of the study of
Lazebnik, et al., (2010).
There were significant differences regarding the
medications used in all the patients before and after the
SCT, as seven of them stopped using of steroids and
immune suppurations through gradual withdrawal of them
with sustained clinical and endoscopic response after SCT
throughout the follow up period.
On the other hand, two patients still on steroids that
planned to be stopped but in much slower rate than the
planned period of our study. Only one case remained using
azathioprine (AZA) after 3 months after SCT but in
lower dose as it decreased to100mg instead
of 150mg before it.
One of the targets in this study was to assess the
effect of SCT on the disease extent and severity. The result
analysis showed that SCT had significant effect on both.
Colonoscopy showed significant differences in distribution
and degree of inflammation after 3 months after the SCT.
This may be due to the complex pathophysiological
mechanisms of SCT that involved in the treatment of
ulcerative colitis. This also goes with the results of the
study of Lazebnik, et al., (2010).

Discussion
- 121 -
When analyzing the results of each patient alone
from the Master Sheet, it found that the improvement was
significant in most of the patients as they were having
moderate or moderate to severe, left sided or extensive
colitis in the initial assessment before SCT and become
mild or mild to moderate, proctitis or left sided colitis
after 3 months after SCT.
As regard the activity score index, there is
statistically significant difference between the score before
the SCT with mean of (7.800 ± 0.789) and 3 month after
the SCT with mean of (5.800 ± 0.789).
Patients No. 2, 4, 6 and 7 showed sustained decrease
in the activity score index from 8 to 6 over the whole
follow up period. The same occurred with
Patient No. 3 and 5 whose score decreased from 9 to 6 for
more than 3 months. Rest of patients showed slight
decrease in their score after SCT. Lazebnik, et al., (2010),
used different scoring indices to evaluated patients.
Disease outcome was promising in this study as
patients pass in a degree of inactivity but the correlation
between the procedure and the patients' improvements still
completely unclear. It could be analyzed as stems cells
effect by their dual action through induction mucosa
regeneration and immune system remodeling. In the study
of Lazebnik, et al., (2010), patients also showed
improvement at end of follow up period.
SCT may be able to improve the general condition of
patients with ulcerative colitis disease, at least temporarily;
until a curative treatment is available or other SCT is done.
Conclusions
- 122 -
Conclusions
Hematopoietic Stem Cell transplantation to patients
of ulcerative colitis disease is a safe and feasible procedure
without recorded complications like bleeding, thrombosis
or any system failure.
It can improve the quality of life of the patients as
well as the clinical illness, laboratory markers,
inflammatory process extent, activity degrees, and multiple
usage of medical treatment.
This improvement may be transient needs for longer
period of follow up to assess if SCT can consider as an
induction therapy of remissions or acts only as adjuvant
one helps to deliver the patient to inactivity much easier.

Recommendations
- 123 -
Recommendations
One of the limitations of our work was the fact that we
didn't track the infused HSCs in the patients‟ bodies. It
is very important to understand the way SCs act to
improve UC disease.
Evaluating the effect of SCT using different clinical trial
protocol as randomized controlled clinical trial study as
it has the strongest evidence of the clinical efficacy of
preventive and therapeutic procedures in the
clinical setting.
Clarify its effect on the other medications and
vice versa. Also, put it in comparison with
anti-TNF therapies.
Compare the use of Hematopoietic and Mesenchymal
stem cell therapy as regard the efficacy and side effects.
Larger number of patients and longer period of follow
up are needed to assess long lasting effects
and complications.
Evaluating the SCT as a maintenance therapy and
compare it with other available maintenance therapeutic
options as regard efficacy, cost and side effects.
Try different routes for SCT as local injection of stem
cells and whether it is better than intravenous injection.
Evaluating the SCT in patients of IBD due to other
causes rather than ulcerative colitis to see if there are
better results with other diseases or not.

Summary
- 124 -
Summary
Ulcerative colitis is an inflammatory bowel disease
leading to inflammation of the colon and causing painful
ulcers which can bleed, cause mucous production and
infection. Common symptoms include bloody diarrhea,
abdominal pain and weight loss which may be mild to
severe and affect individual's quality of life.
Currently, therapy is most often implemented in
a stepwise fashion, progressing through amino salicylates,
corticosteroids, immunosuppressives, and anti-TNF drugs.
Primary and secondary failure to respond to
approved therapies represents unmet needs in the
treatment of IBD.
A novel and exciting approach could be offered
through the current development in the field of
stem cell biology. Two streams of research, experimental
and clinical, are the origin of the increasing utilization of
stem cell therapies for severe immune-mediated diseases
(IMIDs) including IBD.
Other medical researches reflect that SCT has made
improvement in the quality of life to patients of UC but the
mechanism for the effect isn't clear but it interpreted
through the powerful immunomodulatory effects of
SCs and its ability to stimulate regeneration of
intestinal mucosa.

Summary
- 125 -
The present pilot study is a clinical trial that was
done in Ain Shams University to investigate the role of
bone marrow stem cell transplantation as a potential line of
treatment in ulcerative colitis patients. It was conducted on
10 patients diagnosed and managed according to European
Crohn's and Colitis Organization. They were selected
randomly of various extents and severity, and they
were assessed according to The Montreal classification,
Truelove & Witts severity scoring system and
Mayo activity score index.
This study hypothesized that infusion of HSCs may
help to reverse the inflammatory process in patients with
ulcerative colitis. Thus, we conducted a human trial to
evaluate safety and feasibility of autologous bone marrow
HSC transplantation in Egyptian patients with ulcerative
colitis and to evaluate the HSC transplantation as a
therapeutic option compared to the conventional treatment.
All patients assessed before and 3 months after
autologous hematopoietic stem cells transplantation and
follow up includes comparison the changes in the patient's
clinical assessment, nutritional status, biochemical profile,
endoscopic findings, medication requirement, and quality
of life of those patients before and after potential therapy.
The study results showed that there was
improvement in the severity of the disease and the quality
of life in most of the patients over the 3 months after the
procedure. Also, results showed that the procedure was
well tolerated with no observed procedure-related
complications.

References
- 126 -
References
Abraham C and Cho JH (2009): Inflammatory Bowel
Disease. N Engl J Med; 361(21):2066–2078
Abraham N, Selby, W, Lazarus R, et al. (2003): Is
smoking an indirect risk factor for the development of
UC? An age- and sex-matched case-control study. J.
Gastroenterol Hepatol; 18: 139-146.
Abreu MT, Lichtenstein GR, Cohen R, et al. (2006):
American Gastroenterological Association Institute
medical position statement on corticosteroids,
immunomodulators, and infliximab in IBD.
Gastroenterology; 130:935-9.
Ahmad T, Marshall S, Jewell D, et al. (2003): Genotype-
based phenotyping heralds a new taxonomy for IBD.
Curr. Opin. Gastroenterol; 19: 327-335.
Ahmad T, Satsangi J, et al. (2001): Review article:
genetics of IBD. Aliment Pharmacol Ther; 15:731–48.
Anversa P and Nadal-Ginar B (2002): “Myocyte renewal
and ventricular remodeling”. Nature; 415:240-43.
Ardizzone S, Maconi G, Russo A, et al. (2006):
Randomized controlled trial of azathioprine and
5-aminosalicylic acid for treatment of steroid dependent
UC. Gut; 55:47-53.
References
- 127 -
Asahara T and Isner JM (2004):״Endothelial Progenitor
Cells״. Stem Cell Handbook (ed.): by Sell; 221-27.
Baert F, Noman M, Vermeire S, et al. (2003): Influence of
immunogenicity on the long-term efficacy of infliximab
in Crohn's disease. N Engl J Med; 348:601-8.
Baharvand H, Ali F, Dennis VH and Ghasem HS
Concise Review: Trends in Stem Cell״:(2007)
Proteomics״. Stem Cells; 25:1888-903.
Baron JH, Connell AM and Lennard-Jones JE. (1964):
Variation between observers in describing mucosal
appearances in proctocolitis. Br Med J1964; 1:89–92.
Barreiro-de-Acosta M, Magro F, Carpio D, et al. (2010):
Ulcerative colitis in Northern Portugal and Galicia in
Spain. Inflamm Bowel; 16:1227–38.
Becker AJ, McCulloch EA, Till JE (1963), Mouse
Embryonic Stem (ES) Cell Culture-Current Protocols in
Molecular Biology Nature 197: 452-454.
Beckmann J, Scheitza S, Wernet P, Fischer JC and
Giebel B (2007): "Asymmetric cell division within the
human HSC and progenitor cell compartment:
identification of asymmetrically segregating proteins".
Blood; 109(12):5494-5501.
Belluzzi A, Grignoa C, Campieri M, et al. (1996): Effect
of an enteric-coated fish-oil preparation on relapses in
Crohn's Disease. N Engl J Med; 334:1557-1560.

References
- 128 -
Benchimol EI, Seow CH, Steinhart AH, et al. (2008):
Traditional corticosteroids for induction of remission
in Crohn's disease. Cochrane Database Syst; (2):
CD006792.
Bergman R and Parkes M. (2006): Systematic review: the
use of mesalazine in IBD. Aliment Pharmacol Ther;
23:841-55.
Bloomberg News (2012): http://topics.nytimes.com/top/
news/health/diseasesconditionsandhealthtopics/stem
cells/index.html?inline=nyt-classifier) - Bloomberg
news.
Bowen DG and Selby WS. (2000): Use of 6-mercaptopurine
in patients with IBD previously intolerant of
azathioprine. Dig Dis Sci2000; 45: 1810-13.
Brittan M and Wright NA (2002): Gastrointestinal stem
cells. J Pathol; 197:492–509.
Brown SR, Haboubi N, Hampton J, et al. (2008): The
management of acute severe colitis: ACPGBI position
statement. Colorectal Dis; (10 Suppl 3):8-29.
Brunel M, Penna C, Tiret E, Balladur P and Parc R.
(1999): Restorative proctocolectomy for distal UC.
Gut; 45:542-5
Buda A, Qualthrough D, et al. (2003): Butyrate down
regulates alpha-beta1 integrin: a possible role in
induction of apoptosis in colorectal cancer lines.
Gut; 52:729-734.

References
- 129 -
Buhner S, Buning C and Genschel J (2006): Genetic
basis for increased intestinal permeability in families
with CD: role of CARD15 3020insC mutation. Gut;
55(3):342-347.
Burt RK, Traynor AE, Craig R and Marmont AM
(2003): The promise of hematopoietic stem cell
transplantation for autoimmune diseases. Bone Marrow
Transplant: 31; 521-524.
Burt RK, Traynor AE, Pope R, et al. (1998): Treatment
of autoimmune disease by intense immunosuppressive
conditioning and autologous hematopoietic stem cell
transplantation. Blood; 92:3505-3514.
Campieri M, Adamo S, Valpiani D, et al. (2003): Oral
beclometasone dipropionate in the treatment UC: a
multicentre randomized study. Aliment Pharmacol
Ther; 17:1471-80.
Carter MJ, Lobo AJ and Travis SP (2004): IBD Section,
British Society of Gastroenterology. Guidelines for the
management of IBD in adults. Gut.; (53 suppl 5):V1–16.
Chamberlain G, Fox J, Ashton B and Mid-dleton J.
(2007): Concise review: MSC: their phenotype,
differentiation capacity, immunological features, and
potential for homing. Stem Cells; 25: 2739–49.
Charles N. Bernstein, Michael Fried and J.H.
Krabshuis (2009): Inflammatory bowel disease: a
global perspective - World Gastroenterology
Organization Global Guidelines,(1): 1-24

References
- 130 -
Chopp M, Zhang XH, Li Y, Wang L, Chen J, Lu D, Lu
M and Rosenblum M (2000): Spinal cord injury in
Rat: treatment with BMSCT. Neuro report;
11:3001-3005.
Colombel JF, Ferrari N, Debuysere H, et al. (2000):
Genotypic analysis of thiopurine S-methyltransferase in
patients with Crohn's disease and severe
myelosuppression during azathioprine therapy.
Gastroenterology; 118:1025-30.
Cong Y, Weaver C.T, Lazenby A, et al. (2002):
Bacterial-reactive T regulatory cells inhibit
pathogenic immune responses to the enteric flora. J.
Immunol; 169: 6112-6119.
Cosnes J, Carbonnel F, Beaugerie L, et al. (2002):
Effects of appendicectomy on the course of ulcerative
colitis. Gut; 51: 803-807.
D’Haens G, Lemmens L, Geboes K, et al. (2001): IV
cyclosporine vs. IV corticosteroids as single therapy for
severe attacks of ulcerative colitis. Gastroenterology;
120:1323-9.
D'Haens G, Sandborn WJ, Feagan BG, Geboes K,
Hanauer SB, Irvine EJ, et al. (2007):A review of
activity indices and efficacy end points for clinical
trials of medical therapy in adults with UC.
Gastroenterology; 132:763–86.
Dazzi F, van Laar JM, Cope A and Tyndall A. (2007):
Cell therapy for AID. Arthritis Res Ther; 9: 206.

References
- 131 -
Dietrich CF (2009): Significance of abdominal ultrasound
in inflammatory bowel disease. Dig Dis; 27:482-93.
Dignass AU, Bokemeyer B, Adamek H, et al. (2009):
Mesalamine once daily is more effective than twice
daily in patients with quiescent UC. Clin Gastroenterol
Hepatol; 7:762-9.
Dignass A, Eliakim R, Magro F, et al. (2012): Review
article: Second European evidence-based Consensus on
the diagnosis and management of ulcerative colitis:
Definitions, diagnosis and Current management. Journal
of Crohn's and Colitis.
Doyonnas R and Blau HM (2004):״What is the Future of
Stem Cell Research?״ Stem Cell Handbook by Sell;
491-99.
Dubinsky MC, Johanson, J.F., Seidman, E.G., et al.
(2002): Suspected inflammatory bowel disease -- the
clinical and economic impact of competing diagnostic
strategies. Am. J. Gastroenterol; 97: 2333-2342.
Duncombe A (1997): ABC of clinical haematology. Bone
marrow and stem cell transplantation. BMJ. 314; 1179-
1182.
Eaden J, Abrams K, Ekbom A, et al. (2000): Colorectal
cancer prevention in ulcerative colitis: a case-control
study. Aliment Pharmacol Ther; 14:145-53.
Edwards FC and Truelove SC (1963): The course and
prognosis of ulcerative colitis. Gut; 4:299–315.

References
- 132 -
Edward V. Loftus, Jr., MD (2008): IBD: Extra intestinal
Manifestations. Mayo Clinic. Gastroenterology and
Hepatology. Board Review - Third Edition Ch 16
Ei-Matary W, Vandermeer B and Griffiths AM(2009):
Methotrexate for maintenance of remission in ulcerative
colitis. Cochrane Database Syst Rev; (3):CD007560
Esteve M, Saro C, Gonzalez-Huix F, et al. (2004): Chronic
hepatitis B reactivation following infliximab therapy in
CD patients: need for primary prophylaxis. Gut;
53:1363-5.
Feagan BG, Greenberg GR, Wild G, et al. (2005):
Treatment of UC with a humanized antibody to the
alpha4beta7 integrin. N Engl J Med; 352:2499–507.
Feeney MA, Murphy F, Clegg AJ, et al. (2002): A case-
control study of childhood environmental risk factors
for the development of IBD. Eur. J. Gastro. Hepatol;
14: 529-534.
Ferguson MW and O’Kane S (2004): “Scar-free healing:
from embryonic mechanisms to adult therapeutic
intervention”. Philos Trans R Soc Lond B Biol Sci;
359:839-50.
Forbes SJ, Vig P and Poulsom R (2002): "Bone marrow-
derived liver stem cells: their therapeutic potential".
Gastroenterology; 123:654-55.
Fraser AG. (2003): Methotrexate: first-line or second-line
immunomodulator? Eur J Gastro Hepatol; 15:225-31.

References
- 133 -
Fraser AG, Orchard TR and Jewell DP. (2002): The
efficacy of azathioprine for the treatment of IBD: a 30
year review. Gut; 50:485-9.
Friedenstein AJ, Chailakhyan RK and Latsinik NV
(1974): "Stromal cells responsible for transferring the
microenvironment of the haemopoietic tissues:
Cloning in vitro and retransplantation in vivo".
Transplantation; 17:331-40.
Friedman S, Rubin PH, Bodian C, et al. (2008):
Screening and surveillance colonoscopy in chronic
Crohn's colitis: results of a surveillance program
spanning 25 years. Clin Gastroenterol Hepatol;
6:993e8; quiz 53-4.
Fujikawa T, Oh SH and Pi L (2005): "Teratoma
formation leads to failure of treatment for type I
diabetes using embryonic stem cell-derived insulin-
producing cells". Am J Pathol; 166:1781-91.
Fuss I, Neurath M, Boirivant M, et al. (1996): Disparate
CD4þ lamina propria (LP) lymphokine secretion
profiles in inflammatory bowel disease. J Immunol;
157:1261–70.
Ricart E, Garcı´a-Bosch and Pane´s J (2010): Review
article: stem cell therapies for inflammatory bowel
disease (efficacy and safety). Aliment Pharmacol
Ther; 32:939–952
Geiger H and Van Zant G (2002): "The aging of lympho-
hematopoietic stem cells". Nat Immunol; 3:329-33.

References
- 134 -
Gies N, Kroeker KI, Wong K and Fedorak RN. (2010):
Treatment of ulcerative colitis with adalimumab or
infliximab: long-term follow-up of a single-Centre
cohort. Aliment Pharmacol Ther; 32:522–8.
Gilissen LP, Bierau J, Derijks LJ, et al. (2005): The
pharmacokinetic effect of discontinuation of mesalazine
on mercaptopurine metabolite levels in IBD patients.
Aliment Pharmacol Ther; 22:605-11.
Gisbert JP and Gomollon F. (2008): Thiopurine-induced
myelotoxicity in patients with inflammatory bowel
disease: a review. Am J Gastroenterol; 103:1783-800.
Gionchetti P, Rizzello F, Venturi A, et al. (2000): Oral
bacterio-therapy as maintenance treatment in patients
with chronic pouchitis: a double-blind, placebo-
controlled trial. Gastroenterology; 119:305-309.
González-Huix F, Fernández Bañares F, et al. (1993):
Enteral versus parenteral nutrition as adjunct therapy
in acute UC. Am J Gastroenterol; 88:227-232.
Gore RM, Balthazar EJ, et al. (1996): CT features of UC
and CD. AJR Am J Roentgenol; 167 (1): 3-15.
Griffiths MJ, Bonnet D and Janes SM (2005): "Stem
cells of the alveolar epithelium". Lancet; 366:249-60.
Halfvarson J, Bodin L, Tysk C, et al. (2003):
Inflammatory bowel disease in a Swedish twin cohort:
a long-term follow-up of concordance and clinical
characteristics. Gastroenterology; 124: 1767-1773.

References
- 135 -
Hall EJ and Brenner DJ (2008): Cancer risks from
diagnostic radiology.Br J Radiol; 81:362-78.
Halme L, Turunen U, Heliö T, et al. (2002): Familial and
sporadic inflammatory bowel disease: comparison of
clinical features and serological markers in a
genetically homogeneous population. Scand J.
Gastroenterol; 37: 692-698.
Han PD, Burke A, Baldassano RN, et al. (1999):
Nutrition and IBD. Gastroentrol Clin North Am;
28:423-443.
Hans R. Schöler (2007): "The Potential of Stem Cells: An
Inventory". in Nikolaus Knoepffler, Dagmar
Schipanski, and Stefan Lorenz Sorgner. Human
biotechnology as Social Challenge, Ashgate
Publishing, Ltd. p.28.
Harries AD, Jones LA, Danis V, et al. (1983): trial of
supplemented oral nutrition in Crohn's disease. Lancet;
1:887-890.
Hawkey CJ (2004): Stem cell transplantation for Crohn's
disease. Best. Pract. Res. Clin. Haematol;
17(2):317-325.
Hebden JM, Blackshaw PE, Perkins AC, et al. (2000):
Limited exposure of the healthy distal colon to orally-
dosed formulation is further exaggerated in active left-
sided ulcerative colitis. Aliment Pharmacol Ther;
14:155–61.

References
- 136 -
Heller F, Fuss IJ, Niewenhuis EE, et al. (2002):
Oxazolone colitis, a Th2 colitis model resembling
ulcerative colitis, is mediated by IL-13-producing
NK-T cells. Immunity; 17: 629-638.
Herrlinger KR, Fellermann K and Stange EF. (2006):
Tacrolimuse finally! Gut; 55:1224-5.
Hesdorffer C, Ayello J and Ward M (1998): "Phase I
trial of retroviral-mediated transfer of the human
MDR1 gene as marrow chemoprotection in patients
undergoing high-dose chemotherapy and autologous
SCT". J Clin Oncol; 16:165-72.
Hoie O, Wolters FL, Riis L, et al. (2007): Low colectomy
rates in ulcerative colitis in an unselected European
cohort followed for 10 years. Gastroenterology;
132:507-15.
Hyams JS (2002): Inflammatory bowel disease. Pediatr Rev;
21(9):291-295.
Hyde GM, Jewell DP, Warren BF. (2002): Histological
changes associated with the use of IV cyclosporin in
treatment of severe UC may mimic dysplasia.
Colorectal Dis; 4:455-8.
Järnerot G, Rolny P and Sandberg-Gertzen H. (1985):
Intensive IV treatment of UC. Gastroenterology;
89:1005–13.

References
- 137 -
Jenkins D, Balsitis M, Gallivan S, et al. (1997):
Guidelines for the initial biopsy diagnosis of
suspected chronic idiopathic inflammatory bowel
disease. The British Society of Gastroenterology
Initiative. J Clin Patho; 50:93-105.
Jiang Y, Jahagirdar BN, Reinhardt RL, Schwartz RE,
Keene CD, Ortiz-Gonzalez XR, Reyes M, Lenvik
T, Lund T and Blackstad M (2002): "Pluripotency
of mesenchymal stem cells derived from adult
marrow". Nature; 418:41-49.
Johns Hopkins (2013): Gastroenterology and Hepatology.
IBD – Ulcerative Colitis – Introduction.
Johannsson ML, Molin G, et al. (1997): Administration
of different Lactobacillus strains in fermented oatmeal
soup: in vivo colonization of human intestinal mucosa
and effect on the indigenous flora. Appl Environ
Microbiol; 59:15-20.
Joossens S, Reinisch W, Vermeire S, et al. (2002): The
value of serologic markers in indeterminate colitis: a
prospective follow-up study. Gastro; 122: 1242-1247.
Kandiel A, Fraser AG, Korelitz BI, et al. (2005): Increased
risk of lymphoma among IBD patients treated with
azathioprine and 6-mercaptopurine. Gut; 54:1121-5.
Kane SV, Sandborn WJ, Rufo PA, et al. (2003): Fecal
lactoferrin is a sensitive and specific marker in
identifying intestinal inflammation. Am. J.
Gastroenterol; 98: 1309-1314.

References
- 138 -
Kane SV, Schoenfeld P, Sandborn WJ, et al. (2002): The
effectiveness of budesonide therapy for Crohn's disease.
Aliment Pharmacol Ther; 16:1509-17
Karp JM, Ferreira LS and Khademhosseini A (2006):
"Cultivation of human ESCs without the embryoid
body step enhances osteogenesis in vitro". Stem Cells;
24:835-43.
Kefalides PT and Hanaeur SB (2002): Ulcerative colitis:
diagnosis and management. Hospital Physician;
38(6):53.
Kiel MJ, Yilmaz OH and Iwashita T (2005): "SLAM
family receptors distinguish hematopoietic stem and
progenitor cells and reveal endothelial niches for
SCs". Cell; 121:1109-21.
Koh CJ and Atala A (2004): “Tissue engineering, stem
cells & cloning: Opportunities for regenerative
medicine. J Am Soc Nephrol; 15:1113-25.
Kopen GC, Prockop DJ and Phinney DG (1999):
"Marrow stromal cells migrate throughout forebrain
and cerebellum and they differentiate into astrocytes
after injection into neonatal mouse brains". Proc Natl
Acad Sci, USA; 96:10711-16.
Krishnan A and Korzenik JR (2002): IBD and
environmental influences. Gastro Clin. North Am; 31: 21-39
Kuehnle I and Goodell MA (2002): The therapeutic
potential of SCs from adults. BMJ; 325: 372–376.
References
- 139 -
Lakatos PL, Czegledi Z, Szamosi T, et al., (2007):
Smoking in IBD: Good, bad or ugly? World J.
Gastroenterology, 13(46): 6134-6139.
Langholz E, Munkholm P, Davidsen M, et al. (1994):
Course of ulcerative colitis: analysis of changes in
disease activity over years.Gastroenterology;107:3-11.
Lawson MM, Thomas AG and Akobeng AK. (2006):
Tumor necrosis factor alpha blocking agents for
induction of remission in UC. Cochrane Database Syst
Rev; 3:CD005112
Lazebnik LB, Kniazev OV, Konopliannikov AG, et al.
(2010): Allogeneic mesenchymal stromal cells in
patients with ulcerative colitis: two years of observation.
Article in Russian - Eksp Klin Gastroenterol; (11):3-15.
Lee FI, Jewell DP, Mani V, et al. (1996): A randomised trial
comparing mesalazine and prednisolone foam enemas
in patients with acute distal ulcerative colitis. Gut;
38:229-33.
Lees CW, Ali AI, Thompson AI, et al. (2009): The safety
profile of anti-tumor necrosis factor therapy in
inflammatory bowel disease in clinical practice: analysis
of 620 patient-years follow-up. Aliment Pharmacol
Ther; 29:286-97.
Leri A, Kajstura J and Anversa P (2005): Cardiac SCs
and mechanisms of regeneration. Physiol Rev;
85:1373-416.

References
- 140 -
Levine A, Griffiths A, Markowitz J, et al. (2011):
Pediatric modification of the Montreal classification
for IBD: the Paris classification. Inflam Bowel Dis;
17:1314–21.
Lewis JD, Schwartz JS and Lichtenstein GR. (2000):
Azathioprine for maintenance of remission in CD:
benefits outweigh the risk of lymphoma.
Gastroenterology; 118:1018-24.
Lichtenstein GR, Feagan BG, Cohen RD, et al. (2006):
Serious infections and mortality in association with
therapies for CD: TREAT registry. Clin Gastroenterol
Hepatol; 4:621-30.
Lichtiger S, Present DH, Kornbluth A, et al. (1994):
Cyclosporine in severe ulcerative colitis refractory to
steroid therapy. N Engl J Med; 330:1841-5.
Lindblad WJ (2004): Stem cells in Dermal Wound
Healing. Stem Cell Handbook (ed.) by Sell; 101-105.
Lindvall O, Kokaia Z and Martinez-Serrano A (2004):
Stem cell therapy for human neurodegenerative
disorders-how to make it work. Nat Med; 10
(Suppl.):S42-S50.
Liu X, Driskell RR and Engelhardt JF (2004): "Airway
glandular development and SCs". Curr Top Dev Biol;
64:33-56.
Lochs H, Dejong C, et al. (2006): ESPEN guidelines on
enteral nutrition: gastro. Clin Nutr; 25:260-274.
References
- 141 -
Lowenthal RM, Cohen ML, Atkinson K, et al. (1993):
Apparent cure of rheumatoid arthritis by bone marrow
transplantation. J Rheumatol; 20(1):137-140.
Macdonald JK, Prefontaine E and Sutherland LR.
(2009): Azathioprine or 6-mercaptopurine for induction
of remission in CD. Cochrane Database Rev; (4):
CD000545.
Macdonald TT, Monteleone G and Pender SLF. (2000):
Recent developments in the immunology of
inflammatory bowel disease. Scand J Immunol; 51:2–9.
Mahadevan U and Kane S. (2006):AGA
gastroenterological association institute technical review
on the use of gastrointestinal medications in pregnancy.
Gastroenterology; 131:283-311.
Mahid SS, Minor, KS, Stromberg, AJ et al.,
(2006):Smoking and Inflammatory Bowel Disease: A
Meta-analysis. Mayo clinic. Proc., 81(11): 1462-1471.
Manguso F and Balzano A. (2007): Meta-analysis: the
efficacy of rectal beclomethasone dipropionate vs. 5-
aminosalicylic acid in mild to moderate distal ulcerative
colitis. Aliment Pharmacol Ther; 26:21-9.
Marmont AM and Van Bekkum DW (1995): SCT for
severe AID: new proposals but still unanswered
questions. Bone Marrow Transplant 16:497-498.
Marshman E, Booth C and Potten CS (2002): The
intestinal epithelial stem cell. Bioessays; 24:91–98.
References
- 142 -
Masson D, Harrison J, John N, et al (2004): Newsome
potential of HSCT in hepatology. Stem cell; 22:897-
907.
McDonald JW, Feagan BG, Jewell D, et al. (2005):
Cyclosporine for induction of remission in Crohn's
disease. Cochrane Database Syst Rev; (2):CD000297.
McGovern DP, Travis SP, Duley J, et al. (2002):
Azathioprine intolerance in patients with IBD may be
imidazole-related and is independent of TPMT activity.
Gastro; 122:838-9.
Mendes SC, Tibbe JM, Veenhof M, et al. (2002): "Bone
tissue-engineered implants using human BMSCs:
Effect of culture conditions & donor age".
Tissue Eng; 8:911-20.
Mike Jones (2006): The source of pluripotent SCs from
developing embryos - http://en.wikipedia.org/wiki/Stem_cell.
Mimeault M, Hauke R and Batra SK (2007): Stem cells:
A revolution in therapeutics-recent advances in stem
cell biology and their therapeutic applications in
regenerative medicine & cancer therapies. Clin
Pharmacol Ther; 82:252-64.
Mitchell SA, Thyssen, M, Orchard, TR, et al. (2002):
Cigarette smoking, appendectomy, and tonsillectomy
as risk factors for the development of primary
sclerosing cholangitis: a case control study. Gut;
51: 567-573.

References
- 143 -
Morrison S (2000): Stem cell potential can anything make
anything? Current biology; 11: 7-9.
Mowat C, Cole A, Windsor A, et al. (2011): Guidelines for
management of IBD in adults. doi: 10.1136/gut. 224154.
Muller AF, Stevens PE, McIntyre AS, et al. (2005):
Experience of 5-aminosalicylate nephrotoxicity in the
United Kingdom. Aliment Pharmacol Ther; 21:1217-24.
Munkholm P, Michetti P, Probert CS and Elkjaer M,
Marteau P. (2010): Best practice in the management of
mild-to-moderately active UC and achieving
maintenance of remission using mesalazine. Eur J
Gastroenterol Hepatol; 22:912–6.
Murayama T, Nakagawa T, Matsushita K, et al. (1995):
Hemorrhagic colitis with unusual colonoscopy features,
complicated with chronic GVHD after allogeneic bone
marrow transplantation. BMT; 15:141-143.
Murphy MJ, Wilson A and Trumpp A (2005):"More
than just proliferation: function in stem cells". Trends
Cell Biol; 15:128-37.
Neiva K, Sun YX and Taichman RS (2005): "The role of
osteoblasts in regulating HSC activity and tumor
metastasis". Braz J Med Biol Res; 38:1449-54.
Nathan DM, Iser JH and Gibson PR. (2008): A single
center experience of methotrexate in the treatment of
Crohn's disease and ulcerative colitis: a case for SC
administration. J Gastro Hepatol; 23:954-8.

References
- 144 -
Newby EA, Sawczenko A, Thomas AG, et al. (2005):
Interventions for growth failure in childhood Crohn's
disease. Cochrane Database Syst Rev; (3):CD003873.
Noctor S, Martinez-Cerdeno V and Kriegstein A (2007):
Contribution of intermediate progentors cells to cortical
histogenesis. Arch. Neural.; 64 : 639-42.
Nosrat IV, Smith CA, Mullally P, Olson L and Nosrat
CA (2004): Dental Pulp Cells Provide Neurotrophic
Support for Dopaminergic Neurons and Differentiate
into Neurons in vitro; implications for Tissue
Engineering and Repair in the Nervous System. Eur J
of Neurosci; 19:2388-98.
Ogata H, Matsui T, Nakamura M, Iida M, et al. (2006): A
randomised dose finding study of oral tacrolimus
(FK506) therapy in refractory ulcerative colitis. Gut;
55:1255–62.
Orchard TR, Chua, CN, Ahmad, T, et al. (2002): Uveitis
and erythema nodosum in IBD: clinical features &
role of HLA genes. Gastro; 123: 714-718.
Oren R, Arber N, Odes S, et al. (1996): Methotrexate in
chronic active ulcerative colitis: a double-blind,
randomized, Israeli multicenter trial. Gastroenterology;
110:1416-21.
Orholm M, Fonager K, Sorensen HT (1999): Risk of
ulcerative colitis and Crohn's disease among offspring
of patients with chronic inflammatory bowel disease.
Am J Gastroenterol; 94(11):3236–8.
References
- 145 -
Pallone F, Blanco Gdel V, Vavassori P, et al. (2003):
Genetic and pathogenetic insights into IBD. Curr.
Gastroenterol. Rep; 5: 487-492.
Pallone F and Monteleone G. (1998): Interleukin 12 and
Th1 responses in IBD. Gut; 43:735–6.
Panes J and Salas A. (2009): Mechanisms underlying the
beneficial effects of SC therapies for IBD. Gut; 58:
898–900
Piscaglia AC, Novi ML, Campanale MC and Antnio G
Stem cell-based therapy in gastroenterology״:(2008)
and hepatology״. Minimally Invasive Therapy;
17:100-18.
Preeti Gokal Kochar, 2004: SCT using patient‟s own cells
- http://gslc.genetics.utah.edu/units/stemcells/scfuture/
Preston SL, Alison MR and Forbes SJ (2003): "The new
SCs biology: Something for everyone". Mol Pathol;
56:86-96.
Priller J (2004): From Marrow to Brain. Adult Stem Cells
(ed.) by Turksen K; 215-33.
Randall JSB, Warren BF, Travis SP, et al. (2010):
Delayed surgery for acute severe colitis is associated
with increased risk of postoperative complications. B J
Surg; 97:404–9.
Remy Meier (2008): nutritional support in GI diseases.
Nutrition in IBD. ESPEN guidelines. Module 12.4
References
- 146 -
Reyes M and Verfaillie CM (2001): "Characterization of
multipotent adult progenitor cells, a subpopulation of
MSC". Ann N Y Acad Sci; 938:231-35.
Reya T and Clevers H (2005): "What signal stem cells
and cancer". Nature; 434:843-50.
Rice-Oxley JM and Truelove SC. (1950):Ulcerative
colitis course and prognosis. Lancet; 255:6636.
Robey PG (2000): Stem cells near the century mark. J Clin
Invest; 105:1489-91.
Roggeveen MJ, Tismenetsky M and Shapiro R. (2005):
Best cases from the AFIP: UC. Radiographics. 26 (3):
947-51. doi:10.1148/rg.263055149 - Pubmed citation.
Rosenberg W, Ireland A and Jewell DP. (1990): High-
dose methyl prednisolone in the treatment of active
ulcerative colitis. J Clin Gastroenterol 1990;12:40–1.
Roussomoustakaki M, Satsangi J, Welsh K, et al. (1997):
Genetic markers may predict disease behavior in
patients with UC. Gastroenterology; 112: 1845–53.
Safdi M, DeMicco M, Sninsky C, et al. (1997): A double-
blind comparison of oral versus rectal mesalamine
versus combination therapy in the treatment of distal
ulcerative colitis. Am J Gastroenterol; 92:1867-71
Sakaida I, Terai S, Nishima H and Ckita K (2005):
Development of cell therapy using autologous bone
marrow cells for liver cirrhosis. Med Mal Morphol;
38:197-202.

References
- 147 -
Samir T (2004): Endoscopic image of UC released with
permission of patient into public domain; 07:39, 7 -
http://en.wikipedia.org/wiki/File:Ulcerative_colitis.jpg
Sanchez-Ramos J, Song S, Cardozo-Pelaez F (2000):
"Adult bone marrow stromal cells differentiate into
neural cells in vitro". Exp Neurol; 164:247-56.
Sandborn WJ, Feagan B, Marano C, Strauss R, Johanns
J, Zhang H, et al. (2012): A phase 2/3 randomized
study to evaluate the safety & efficacy of golimumab
induction therapy in patients with severe UC: Gastro;
142(Suppl 1):S161.
Sandborn WJ and Hanauer SB. (2003): Systematic
review: the pharmacokinetic profiles of oral mesalazine
formulations and mesalazine pro-drugs used in the
management of ulcerative colitis. Aliment Pharmacol
Ther; 17:29-42.
Sandborn WJ, Rutgeerts P, Feagan BG, et al. (2009):
Colectomy rate comparison after treatment of ulcerative
colitis with placebo or infliximab. Gastroenterology;
137:1250–60 [quiz 1520–1250–1260; quiz 1520].
Sandborn WJ, Tremaine WJ, Schroeder KW, et al.
(1994): A placebo-controlled trial of cyclosporine
enemas for mildly to moderately active left-sided UC.
Gastro; 106:1429–35.
Sands BE (2004): From symptom to diagnosis: clinical
distinctions among various forms of intestinal
inflammation. Gastroenterology; 126:1518-32.

References
- 148 -
Sartor RB (2004): Microbial influences in inflammatory
bowel disease: role in pathogenesis and clinical
implications. In Kirsner's Inflammatory Bowel
Diseases (eds Sartor RB and Sandborn WJ)
Philadelphia: WB Saunders, 138-162.
Satsangi J, Morecroft J, Shah NB, et al. (2003): Genetics
of IBD: scientific and clinical implications. Best.
Pract. Res. Clin. Gastro; 17: 3-18.
Satsangi J, Silverberg MS, Vermeire S, et al. (2006):
The Montreal classification of IBD: controversies,
consensus, and implications. Gut; 55:74953.
Schachinger V, Erbs S, et al. (2006): Intracoronary bone
marrow-derived progenitor cells in acute myocardial
infarction. N Engl J Med; 355:1210-21.
Schier S and Wright NA (2005): "SC relationships and
origin of gastrointestinal cancer". Oncology; 69:9-13.
Schroeder KW, Tremaine WJ and Ilstrup DM (1987):
Coated oral 5-aminosalicylic acid therapy for mildly
to moderately active ulcerative colitis. A randomized
study. N Engl J Med; 317:1625–9.
Sell Stewart (2004): Stem Cells: In stem cell handbook.
Humana Press Inc. 999 Riverview Drive, Suite 208.
Totowa, New Jersey 07512.
Seow CH, Benchimol EI, Steinhart AH, et al. (2009):
Budesonide for CD. Expert Opin Drug Metab Toxicol;
5:971-9.

References
- 149 -
Shen CN, Horb ME, Slack JMW and Tosh D (2003):
Transdifferentiation of Pancreas to Liver. Mech;
120:107-16.
Shibolet O, Regushevskaya E, Brezis M, et al. (2005):
Cyclosporine A for induction of remission in severe
ulcerative colitis. Cochrane Database Syst Rev;
(1):CD004277.
Silverberg MS, Mirea L, Bull SB, et al. (2003): A
population- and family-based study of Canadian
families reveals association of HLA DRB1*0103 with
colonic involvement in IBD. IBD; 9: 1-9.
Silverberg MS, Satsangi J, Ahmad T, et al. (2005):
Toward an integrated clinical, molecular and
serological classification of inflammatory bowel
disease: report of a working party of the 2005
Montreal World Congress of Gastroenterology. Can J
Gastroenterol; 19(Suppl A):5–36.
Snowden JA, Kearney P, Kearney A, et al. (1998): Long-
term outcome of autoimmune disease following
allogeneic bone marrow. Transplantation Arthritis
Rheum; 41: 453-459.
Soutar RL and King DJ (1995): Bone marrow
transplantation. BMJ; 310: 31-36.
Stathaki MI, Koukouraki SI, Karkavitsas NS, et al.
(2009): Role of scintigraphy in inflammatory bowel
disease. World J Gastroenterol; 15:2693-700.

References
- 150 -
Su C, Lewis JD, Goldberg B, Brensinger C and
Lichtenstein GR. (2007): A meta-analysis of the
placebo rates of remission and response in clinical trials
of active ulcerative colitis. Gastroentero; 132:516–26.
Subramanian V, Saxena S, Kang JY, et al. (2008):
Preoperative steroid use and risk of postoperative
complications in patients with IBD undergoing
abdominal surgery. Am J Gastroenterol; 103:2373-81.
Summerton CB, Longlands MG, Wiener K, et al. (2002):
Faecal calprotectin: a marker of inflammation
throughout the intestinal tract. Eur. J. Gastroenterol.
Hepatol; 14: 841-845.
Sutherland L and Macdonald JK. (2006): Oral 5-ASA for
induction of remission in ulcerative colitis. Cochrane
Database Syst Rev; (2):CD000543.
Swenson ES and Theise ND (2010): SCT: potential in the
treatment of IBD. Clinical & Experimental Gastro; 31– 10
Swidsinski A, Ladhoff A, Pernthaler A, et al. (2002):
Mucosal flora in inflammatory bowel disease.
Gastroenterology; 122: 44-54.
Sykes M, Nikolic B, et al. (2005): Treatment of severe
autoimmune disease by SCT Nature; 435, 620-627.
Tekkis PP, Lovegrove RE, Tilney HS, et al. (2010): Long-
term failure and function after restorative proctocol
ectomyda multi-Centre study of patients from the UK
national ileal pouch registry. Colorectal Dis; 12:433-41.

References
- 151 -
Terese Winslow (2001): Medical and scientific
illustrations-http://www.teresewinslow.com/index.asp
Terheggen G, Lanyi B, Schanz S, et al. (2008): Safety,
feasibility, and tolerability of ileocolonoscopy in
inflammatory bowel disease. Endoscopy; 40:656-63.
Theis VS and Rhodes JM. (2008): Review: minimizing
tuberculosis during anti-tumor necrosis factor-alpha
treatment of IBD. Aliment Pharmacol Ther; 27:19-30.
Theise ND (2005): Stem cell plasticity: tools for
investigation and repair. Session V. Inverting the IBD
therapeutic triangle through genomics and proteomics.
J. Pediatr. Gastroenterol. and Nutr; 40: 48-49.
Tiede I, Fritz G, Strand S, et al. (2003): CD28-dependent
Rac1 activation is the molecular target of azathioprine
in primary human CD4+ T lymphocytes. J Clin Invest;
111:1133-45.
Timmer A, McDonald JW and Macdonald JK. (2007):
Azathioprine and 6-mercaptopurine for maintenance of
remission in UC. Cochrane Database Syst Rev;
(1):CD000478.
Travis SPL, Schnell D, Krzeski P, et al. (2012):
Validation of the UC Endoscopic Index of Severity
(UCEIS): a randomized, blinded, validation study in
an independent cohort. Gastroenterology in press.
Trounson A (2006): The production and directed
differentiation of human ESCs. Endocr Rev; 27:208-19.

References
- 152 -
Truelove SC and Witts LJ. (1995):Cortisone in UC; final
report on a therapeutic trial.Br Med J; 2:1041–8.
Tuch BE (2006): "Bone Marrow Transplant ". Australian
family physician; 35 (9): 719-721.
Turner D, Walsh CM, Steinhart AH and Griffiths AM.
(2007): Response to corticosteroids in severe UC: a
review of the literature and a meta-regression. Clin
Gastro Hepatol; 5:103–10.
Tyndall A and Saccardi R (2002): HSCT in the treatment
of severe autoimmune disease - results from phase I/II
studies, prospective randomized trials and future
directions. Clin. Exp. Immunol.
Yao S, Chen S and Clark J (2006): "Long-term self-
renewal and directed differentiation of human ESCs in
chemically defined conditions". Proc Natl Acad Sci.
USA; 103:6907-12.
Uccelli A, Moretta L and Pistoia V. (2008):
Mesenchymal stem cells in health and disease. Nat
Rev Immunol; 8:726–36.
Vagianos K, Bector S, McConnell J and Bernstein CN.
(2007): Nutrition assessment of patients with IBD.
J Parent Enteral Nutrition; 31:311-319.
Van Assche G, D’Haens G, Noman M, et al. (2003):
Randomized, double-blind comparison of 4 mg/kg vs. 2
mg/kg IV cyclosporine in severe UC. Gastroenterology;
125:1025-31.

References
- 153 -
Van Assche G, Dignass A, Panes J, et al. (2010): The
second European evidence-based diagnosis and
management of CD. J Crohn's Colitis; 4:7–27.
Van Assche G, Vermeire S and Rutgeerts P (2011):
Management of acute severe UC. Gut; 60:130–3.
Van Staa TP, Travis S, Leufkens HG, et al. (2004): 5-ASA
and the risk of renal disease: a large British
epidemiologic study. Gastroenterology; 126:1733-9.
Vasiliauskas E (2003): Recent advances in diagnosis &
classification of IBD. Curr. Gastroenterol. Rep; 5: 493-500
Wahed M, Louis-Auguste JR, Baxter LM, et al. (2009):
Efficacy of methotrexate in Crohn's disease and UC
patients unresponsive or intolerant to azathioprine
/mercaptopurine. Aliment Pharmacol Ther; 30:614-20.
Weiss ST (2002): Eat dirt -- the hygiene hypothesis and
allergic diseases. N. Engl. J. Med; 347: 930-931.
Weissman L (2000): Translating SCs biology to the clinic
barrier and opportunities. Science; 287: 1442-1446.
West RL, Zelinkova Z, Wolbink GJ, et al. (2008):
Immunogenicity negatively influences the outcome of
adalimumab in CD. Aliment Pharmacol Ther; 28:1122-6.
William J. Tremaine, MD (2008): IBD: Clinical Aspects.
Mayo Clinic. Gastro. Board Review - Third Edition Ch 14
Wilson A and Trumpp A (2006): "Bone-marrow HSC
niches". Nat Rev Immunol; 6:93-106.

Arabic summary
- 154 -
:هقدهة الرسالة
ؤد أحذ أيشاع انزبثبد انمن انضيخ انزبة انمن انزمشح
أ رزظ إفشاصاد أ رضف رمشحبد يؤنخ ك ظبحجإن انزبة انمن
أػشاع يب غؼم شبؽ خل يزفبرخ يخبؽخ ، ش انشع ثفزشاد
سثب ساد ،زض زا انشع أنؼذح أشش رخزفانشع رزكشس أ
ثبإلػبفخ إن آالو ف انجط ، فمذا ثبنص ، يرشم اإلسبل انذثأػشاع
أػشاع أخش.
حز ا، لذ أظشد انؼذذ ي كهب يسججبد زا انشع غش يؼشف
هؼذ ك ن ف ظس ، سثب انجئخ هؼايم انساصخنا انذساسبد رأصش
انجكزشخ دس ف رنك أؼب ، إال أ أغهت انظشبد رشعح أ يشع يبػ
يسزشف يب ث لبيذ ثحش لذ شش ثبنذسعخ األن ، يشع بدس سجب ،
.سب زا انشع ث شخض ي كم أنف شخض 44 - 2ي إطبثخػح كهك
انسشش، ؼزذ رشخض زا انشع ػه ػذح ػايم رشم انفحض
انزحبنم انخجشخ ، إػبفخ إن انظبس انزشخظ ػ ؽشك انمن ، انز
زح أخز ػبد نفحظب يكشسكثب رأكذ انزشخض ،إػبفخ إن رنك زى
ثشايظ يزؼذدح يؼزذح دنب ،زلف رمى انحبالد رظفب رجؼب ألسبنت
يكب حذح انشع ، ف انؼزبد انز رج ػه زبئظ انزمى نشػا ػالط
، ػمبساد انسبنفب يضم ثبنؼمبساد انزمهذخ يؼظى األؽجبء ػالط يشػبى جذأ
بػخ فؼبنزب انيضجطبد ػمبساد صجذلذ أ انكسرضبد انؼبداد انحخ ،
طبق د ي اسزخذايب ػه لذ حذ زب س أؼب ، إال ا انشع زا ف ػالط
انز اصجزذ انؼمبساد انجنعخ األعسبو انؼبدح ظشد حذضب كباسغ ،
.نك اسرفبع ركبنف انؼالط ثب حذ ي ازشبسب كزنك ، أؼبػبنخ خ فؼبن
حممب زبة انمن انزمشح يب ضال شكم رحذب نػالط ا ف انالغ إ
نهؼالط رك أكضش فبػهخ سهخ عذذحزمذى ، يب غؼهى ف ثحش دائى ن نألؽجبء
االثحبس انطجخ زظش انزطم نؼالط عذذ ألم س خ ، يغ رمذو انؼهى رطس
بعح نزا انشع.
ذػ نالزبو ، انغزػخ س انحبطم ف يغبل ثنعب انخالبانزط إ
اػذح نهكضش ي ثذأ ؼط إشبساد كؼالط خكب أ ارسبع اسزخذاو ز انزم
انؼه نؼالط شبف نب انجحش ، انز نى زطم االيشاع انضيخ انسزؼظخ
انكجشح انحطخ ثغبل انؼالط ثبنخالب انغزػخ رسزذ انؼغخسثب حز ا.
ػه لذسرب انزارخ ػه انزغذد انضح انفشذح ثنعب ، ػه خظبئظب
ذساسبد انيعخ ي لذ ازششد، األػؼبء انخزهفخػه رغذذ األسغخ
يخزهف مم خبع انؼظى إن إيكبخ حلششد االثحبس انؼهخ ، انز
نؼالط األيشاع. األػؼبء
-أ-

Arabic summary
- 155 -
انخالب انغزػخ ف يغبل ثنعب ظشد ثادس انزطس انحذش انزم
با خؼؼ كانز يز ألم ي ػمذ ي انضي، حش نحع أ ثؼغ انشػ
انز كب ؼب أؼب ػخ ثسجت أيشاع سشؽب انذيزنهؼالط ثبنخالب انغ
الحظا رحسب ف حبنزى اخزفبء ي يشع انزبة انمن انزمشح انضي
نألػشاع انظبحجخ نزا انشع ، يب عؼم انجبحض فكش ف اسزخذاو ز
يفظم.انزمخ ف ػالط زا انشع ثشكم
انغزػخ بنخال أبلخ ػه لذ اصجزذ انؼذذ ي االثحبس انؼبنخ ثأدنخ
ػضنب ك عدح ف انؼذذ ي أعضح عسى انجبنغانيزؼذدح انم
بض زحش راالشخبص انجبنغ، يؼبنغزب خبسعب صسػب يشح أخش ف
، لذ رى رفز ز انطشمخ نؼالط انخزهفخ أسغخ األعضح نزؼم ثشكم يبست ف
انز ح ثظذد -ػذح أيشاع، يب يشع انزبة انمن انزمشح انضي
اظشد انزبئظ دالالد يجششح. لذ –انجحش ف ػالع
طرق وأسالب البحث:
كانزحم ذفب شس ػ عبيؼخف رزى انز انزغشجخ انذساسخ ز
انذيخ انخالب انغزػخ نخبع انؼظى داخم األػخحم انكشف ػ دس
انمن انزبة ي ؼب انز انشػ ف يحزم ػالط كخؾ انفشػخ
رأصش ػه ي خالل زا اإلعشاء ف انؼالط رمى يذ فبػهخ انضي انزمشح
انزحبنم ، انزغزخ انحبنخ ، انسشش انزمى رحس انحبالد ي بحخ
سفغ ، انسزخذيخ األدخ ع عشػخ ، نظبسا زبئظ ، انؼهخ
عدح حبح انشػ.
ؼب ي انزبة انمن انزمشحيشػ 41ز انذساسخ ػه أعشذ
رى رشخظى ػالعى فمب نهزطبد انشسح ي يظخ )إك( األسثخ ،
انحبالد ؼذع رمى حبالرى فمب نألظخ انؼبش انؼزذح دنب ،لذ
يؼذ ، شس ػ يسزشفبد ف انؼبداد انخبسعخ انجبؽخ وبلسأ ي ػشائب
. انكشثبء، بطش
:ى وفقا لوا ل تن اختار جوع الورض
اإلدراج هعار:
.سخ 61شخض ششق أسط ثبنغ ألم ي .4
.يشغ انزبة انمن انزمشح ثزشخض يصك .2
.يافمخ خطخ ي انشغ ػه انزطع ف دساسزب .3
-ب-

Arabic summary
- 156 -
هعار االستبعاد:
كشض.ع انشػ انز ؼب ي يش .4
.خيزمذي انشػ انز ؼب ي أيشاع أخش يضيخ .2
.انشػ انز ؼب ي األساو انخجضخ أ أيشاع انذو .3
.أخش انشػ انز ؼب ي أيشاع يبػخ رارخ .4
.افمخ انخطخ نهزطع ثبنذساسخانسفغ انزلغ ػه .5
هزمى ن أخش عغ انحبالد ف دساسزب نزمى أن كبيم إػبدح ذخؼؼ
أشش ي حم انخالب انغزػخ ي خالل يؤشش شبؽ انزبة ثؼذ يشس صالصخ
.ػه حبنخ انشػ انمن انزمشح نزسغم رأصش صسع انخالب انغزػخ
:خضع جوع الورضى إلى ها ل
:التقن السرري .1
شبيمانأخز انزبسخ انشػ انكبيم انفحض انطج
الفحوصات: .2
(- %ESR – CRP –ALB -HBرحبنم يخجش )
:التنظر .3
فحض االسغخ ػه انمن ( انزظش انسفه)يظبس
لتقن نشاط الورض( "Mayoالتدرج )نظام " .4
سزى اسزخذاو زا انظبو ف كم ي انزمى األن انزكه
.42إن 1نشطذ االسزغبثخ نهؼالط حسبة دسعخ انشع ي
:تعدالت العالج .5
ؽشمخ أ عشػخ انؼــــــــالط فأ رغشاد ف ع أ
.فمب نحبنخ انشغ يخزهف خطؾ انؼالط انذائ انزمهذخ
بنخالب انغزػخ انزارخ ث رهمذ انؼالطانحبالد اناسدح ف دساسزب عغ
ثؼذ انذيخ ، رنك انغش يزبضح نخبع انؼظى ػ ؽشك انحم داخم األػخ
يؼمخ ثبنكبيم ، رمبد خالل عبص خبصيؼبنغزب ثبنطشد انشكض ثاسطخ
ف أسثغ خطاد سئسخ : انغزػخ نهشػ انخالب صسع ػهخلذ رذ
عهسخ احذح ف ذ عؼبر ، االسزخالص ، انمم ، انؼبنغخ، انحم
.انذن انضخ سزشفث
-ج-

Arabic summary
- 157 -
االستنتاج :
انزبة شػن انغزػخ انخالب صسعي خالل زبئظ ب انجحش عذب أ
خطشح يؼبػفبد ذث يك ، آي إعشاء انضي انزمشح انمن
.يسغهخ
عدح سفغ أ رؤد إن ككب عذب أ اسزخذاو ز انطشمخ نهؼالط
انزبة حذح ،انؼهخ ؼاليبدان ، نهشع ، األػشاع انؼبيخ انشػ حبح
إػبفخ إن خفغ اسزخذاو انؼمبساد انذائخ ، انشع شبؽ دسعخ ، انشع
انزمهذخ.
زبثؼخان ي أؽل فزشحن لز أ ػبثش نزنك حزبط انزحس زا ك لذ
ػالط اػزجبس حمب كإرا كب انؼالط ثبنخالب انغزػخ يب نزم نهشػ
يب إن انشغ إظبل ػه أ فمؾ لذ سزخذو كؼالط يسبػذ يفشد نهشع ، أو
.سمثظسح أ انشع خلس ثفزشح
التوصات:
شعان زا رحس ػه انغزػخ انخالب كفخ ػم نفى ؼكثانجحش.
يخزهفخ ثشركالد ثحش ػه ثبسزخذاو انغزػخرأصش انؼالط ثبنخالب رمى.
انؼكس. األخش األدخ انؼالط ػهرأصش زا رػح
ف ػالط زا انشع. انغزػخ ثبنخالب اسزخذاو األاع انخزهفخ ي يمبسخ
نهزمى ثظسح أػح.ل أؽ فزشح انشػ ي أكجش ػذد إن حبعخان
كؼالط رحفظ ؽم انفؼل. انغزػخرمى انؼالط ثبنخالب
انغزخ ف ػالط انشع.اسزخذاو ؽشق أخش نحم انخالب
نألاع األخش ي ايشاع انزبة انمن. كؼالط رمى انخالب انغزػخ
……..
-د-

Role of Stem Cell
Transplantation in the
Treatment of Ulcerative Colitis
Thesis
Submitted for the Partial Fulfillment
of Master Degree in Internal Medicine
By
Mohammed Fathy Sayed Mohammed Zaky
M.B.B.Ch.
Faculty of Medicine - Ain Shams University
Supervised by
Prof. Dr . Mohsen Mostafa Maher
Professor of Internal Medicine
Faculty of Medicine - Ain Shams University
Ass. Prof. Dr . Wesam Ahmed Ibrahim
Assistant Professor of Internal Medicine
Faculty of Medicine - Ain Shams University
Dr . Shereen Abou Bakr Saleh
Lecturer of Internal Medicine
Faculty of Medicine - Ain Shams University
Faculty of Medicine - Ain Shams University
2014

بسم هللا الرحمن الرحيم
(111سورة طه )
صدق هللا العظيم

Acknowledgement
At first and foremost thanks to “Allah” the most
merciful who gave me the power to finish this work.
I wish to express my deepest appreciation and
sincere gratitude to Prof. Dr. Mohsen Mostafa Maher,
Professor of Internal Medicine, Ain Shams University,
for his precious help throughout all stages of this work,
outstanding kind support and valuable instructions.
My greatest respect, appreciation and thanks to
Prof. Dr. Wesam Ahmed Ibrahim, Assistant Professor
of Internal Medicine, Ain Shams University, for her
valuables help, planning and supervision of this study.
It was a great honor to me to work under her guidance.
It is a great honor to express my thanks to
Prof. Dr. Shereen Abou Bakr Saleh, Lecturer of
Internal Medicine, Ain Shams University, who was very
kind, supportive and helpful throughout all the stages of
this work. She had such a great influence on my character
and behavior.

I owe many thanks, respect and appreciation to
Prof. Dr. Alaa El Din Ismail, Professor of General
Surgery, Ain Shams University, for offering me much of
his time and experience throughout the practical part of
this work and for help me to overcome the obstacles and
difficulties that arose along the way until finally the
project was completed.
Also, I am great fully indebted to
Prof. Dr. Doaa Zakaria Zaki, Lecturer of Tropical
Medicine, Ain Shams University, for her help, guidance
and revision of this work that helped me to finish this
project.
I am deeply grateful to my Mother, Father and
Brother, for their great support and help throughout my
life not only this great study….
Mohammed Fathy Sayed Zaky

List of Contents
Title Page
Introduction and Aim of the Work 1
Review of Literature
Chapter I
Chapter II
5
58
Patients and Methods 89
Results 95
Discussion 114
Conclusions 122
Recommendations 123
Summary 124
References 126
Arabic Summary -أ-

List of Abbreviations
ADA Adalimumab
AID Autoimmune Diseases
ALT Alanine Aminotransferase
ALB Albumin
APC Antigen Presenting Cell
ASA Amino salicylic Acid
ASCA Anti-Saccharomyces Cerevisiae Antibodies
ASCs Adult Stem Cells
ATA Antibodies formation to Adalimumab
ATI Antibodies formation to Infliximab
ATG Anti-thymocyte Globulin
AZA Azathioprine
BM Bone Marrow
BMA Bone Marrow Aspirate
BMI Body mass index
BMSCs Bone Marrow Stromal Cells
bpm Beat per minute
BSG British Society of Gastroenterology
BW Bodyweight
Cal Calories
CBC Complete Blood Cell Count
CD Crohn's Disease
CK Cytokeratin
CMV Cytomegalovirus
CRC Colorectal Cancer
CNS Central Nervous System
CRP C Reactive Protein
CsA Ciclosporin
CT Computed Tomography
CY Cyclophosphamide

List of Abbreviations (cont.)
DNA Deoxyribonucleic Acid
E1 Proctitis
E2 Left-sided Colitis
E3 Extensive Ulcerative Colitis
E. coli Escherichia Coli
ECCO European Crohn's and Colitis Organization
EIS Endoscopic Index of Severity
EN Enteral Nutrition
ERUS Endorectal Ultrasonography
ESCs Embryonic Stem Cells
ESR Erythrocyte Sedimentation Rate
FBCs Full Blood Counts
G-CSF Granulocyte Colony Stimulating Factor
g/dL gram/deciliter
GIT Gastro Intestinal Tract
GVHD Graft Versus Host Disease
HB Hemoglobin
HCT Haematopoietic Cell Transplantation
HLA Human Leukocyte Antigen
HSCs Hematopoietic Stem Cells
HSCT Hematopoietic Stem Cell Transplantation
IC Indeterminate Colitis
ICMs Inner Cell Masses
IBD Inflammatory Bowel Disease
IBDU Unclassified Inflammatory Bowel Disease
IBS Irritable Bowel Syndrome
IFN Interferon
IFX Infliximab
IL Interleukin
IMIDs Immune-mediated Diseases

List of Abbreviations (cont.)
IMiDs Immunomodulatory Drugs
iPSCs Induced Pluripotent Stem Cells
IV Intravascular
MAPCs Multipotent Adult Progenitor Cells
MDR Multidrug Resistance Gene
MHC Histocompatibility Complex
MTX Methotrexate
MP Mercaptopurine
MPCs Mesodermal Progenitor Cells
MRI Magnetic Resonance Imaging
MSCs Mesenchymal Stem Cells
NSAID Non-Steroidal Anti-Inflammatory Drug
NSC Neural Stem Cells
NHL Non Hodgkin Lymphoma
PD Processing Disposable
PSC Primary Sclerosing Cholangitis
SCT Stem Cell Therapy
SCs Stem Cells
SLE Systemic Lupus Erythematosus
SSCs Stromal Stem Cells
TB Tuberculosis
TBI Total Body Irradiation
TGF Transforming Growth Factor
TGN Thioguanine Nucleotides
TNF Tumor Necrosis Factor
TPN Total Parenteral Nutrition
UC Ulcerative Colitis
UK United Kingdom
USA United State of America
WBCs White Blood Cells

List of Figures
Fig. Subjects Page
(1) Extra-colonic manifestations of UC. 21
(2) Endoscopic image of ulcerative colitis. 22
(3) Histology of normal colon and UC 24
(4) Radiological features of ulcerative colitis. 26
(5) Extent of bowel involvement in UC. 48
(6) Stem cells. 58
(7) Development of Preimplantation Blastocyst 60
(8) Pluripotent stems cells. 60
(9) Embryonic stem cells. 63
(10) Hematopoietic & stromal SCs differentiation. 69
(11) Autologous HCT as a therapy for AID. 81
(12) SCs transplant using patient‟s own cells. 84
(13) Mechanism by which HCT ameliorate AID. 86
(14) Stem Cells Transplantation for Patients. 93
(15) Assessment of the presence of diarrhea. 96
(16) Assessment of the rectal bleeding. 97
(17) Assessment of the abdominal pain. 98
(18) Assessment of the disease extent. 99
(19) Assessment of the disease severity. 100
(20) Assessment of the medical treatment. 101
(21) Assessment of the disease outcome. 103
(22) Endoscopic picture of patient before and after SCT. 104
(23) Assessment of the motion frequency. 105
(24) Assessment of the body temperature. 106
(25) Assessment of the heart rate. 107
(26) Assessment of the body mass index. 108
(27) Assessment of the serum albumin. 109
(28) Assessment of the hemoglobin level. 110
(29) Assessment of the erythrocyte sedimentation rate. 111
(30) Assessment of the C-reactive protein. 112
(31) Assessment of the activity score. 113

List of Tables
Table Subjects Page
(1) The Montreal classification of UC. 8
(2) Disease severity index of UC 10
(3) Mayo activity scoring index. 10
(4) Endoscopic scores for UC. 10
(5) UC Endoscopic Index of Severity. 24
(6) Nutritional deficiencies in IBD. 32
(7) Algorithm for the treatment of UC. 51
(8) SCs during differentiation at each stage. 62
(9) Types of cell division. 62
(10) Comparison between patients as regard the presence of diarrhea 96
(11) Comparison between patients as regard the rectal bleeding. 97
(12) Comparison between patients as regard the abdominal pain. 98
(13) Comparison between patients as regard the disease extent. 99
(14) Comparison between patients as regard the disease severity. 100
(15) Comparison between patients as regard the medical treatment 101
(16) Comparison between patients as regard the disease outcome. 102
(17) Comparison between patients as regard the motion frequency 105
(18) Comparison between patients as regard the body temperature 106
(19) Comparison between patients as regard the heart rate. 107
(20) Comparison between patients as regard the body mass index. 108
(21) Comparison between patients as regard the serum albumin. 109
(22) Comparison between patients as regard the hemoglobin level 110
(23) Comparison between patients as regard the ESR. 111
(24) Comparison between patients as regard the CRP. 112
(25) Comparison between patients as regard the activity score. 113

Introduction

Aim of the Work

Review of Literature

Chapter I

Chapter II

Patients and Methods

Results

Discussion

Conclusion and
Recommendations

Summary

References

Arabic Summary