
Role of Pharmacists in HIV Care under NACP III Tamilnadu State AIDS Control Society.
21
Role of Pharmacists in HIV Care under NACP III Tamilnadu State AIDS Control Society
-
Upload
eugene-baker -
Category
Documents
-
view
216 -
download
0
Transcript of Role of Pharmacists in HIV Care under NACP III Tamilnadu State AIDS Control Society.

Role of Pharmacists in HIV Care under NACP III
Tamilnadu State AIDS Control Society

Districts by category:
A – 141
B – 46
C – 309
D – 114
HIV/AIDS Epidemic in India (2007)
Tamilnadu
• National India0.48 %
• State Tamilnadu0.25 %

Category of Districts
More than 1% ANC/ PPTCT prevalence in district in any time in any of the sites in the last 3 years
A
Less than 1% ANC/PPTCT prevalence in all the sites during last 3 years Associated with More than 5% prevalence in any HRG group (STD/ FSW/ MSM/ IDU)
B
Less than 1% in ANC prevalence and Less than 5% in all STD clinic attendees or any HRG WITH KNOWN HOT SPOTS (Migrants, Truckers, Large aggregation of, Factory workers, Tourist etc)
C
Less than 1% in ANC prevalence in all sites during last 3 years with Less than 5% in all STD clinic attendees or any HRG OR No or Poor HIV Data With No Known Hot Spots/ Unknown
D
Categorization of districts

National AIDS Control Program Phase III

GOAL
To reverse the epidemic in India over the next 5 years through integration of prevention & treatment programs.
• Objectives Prevention of new infections in high risk groups and vulnerable
populations througha) Saturation of coverage of high risk groups with Targeted
Interventions (TI)b) Scaled up interventions in other vulnerable populations
Increasing the proportion of persons living with HIV/AIDS receiving care and treatment
Strengthening the infrastructure, systems and human resources in prevention and treatment programs at the district, state and national levels
Establishing nation wide strategic planning, programme management, monitoring and evaluation system.

Key features
• Prevention• Up-scaling of activities • Classification of districts by risk category• TIs more focused approach on HRGs• Empowering and capacity strengthening of CBOs to
manage TIs • Introduction of Link Workers in A and B districts (more
focus on IPC)• Focused efforts on women, youth and children

Key features ....
• Emphasis on quality of care
• Increased access to ART, including resistance surveillance
• Increased focus of pediatric ART care
• Special efforts to address GIPA, impact mitigation
• Mainstreaming and partnerships with private sector
• Leveraging resources for sustainable response
• Performance Oriented Programme Management

Guiding principles• Three Ones
one agreed action framework; one National HIV/ AIDS coordinating authority, one agreed National Monitoring & Evaluation system
• Equity
• Respect for the rights of the PLHA
• Civil society representation and participation
• Creation of enabling environment
• Improved access to services
• Effective HRD strategy
• Evidence based and result oriented programme implementation

CST component under NACP III
To ensured access to OI treatment including free drugs. First line ART is to be provided to eligible PLHA free of cost. Ensuring adherence and monitoring ART drug resistance.
Through e.g.: medical colleges, district hospitals with fully functional medicine department.
Community outreach for home based care and livelihood support.
PCP prophylaxis, nutritional advice and treatment of TB The national target for first line ART is 2,00,000
Care, Support and Treatment

Care, Support and Treatment
Improved treatment access for OIs
There would be a referral system for appropriate management
Supply of major OI drugs under government hospitals free of cost
Doctors in private sector will have access to training and referral linkages
Development of guidelines on OI management for different levels of service delivery and referral linkages
Development of guidelines and capacities for establishing standards of care
Establishment linkages with DOTS programme for HIV/TB co-infection

Care, Support ... Increased Number of PLWHA on ART
More ART centres and link ART centres Arrangements for CD4 testing either through direct provision or
linkages with central units Identification of referral centres and orientation of doctors Identification of NGOs to provide community outreach, home
based care and psycho social support Establishment of facilities for paediatric ART, including viral load
testing facilities and procurement of paediatric drug formulations Assessing the need for and setting up community care and
support centres Improve public private partnership to achieved specific targets
every year.

Care, Support ... Expansion of VCTC, PPTCT and PEP programs
Integration of VCTC and PPTCT centres (and if feasible blood bank and STI services also). If loads permit it, the programmes can share counseling and testing services.
Long term follow up of mother and child for OI and ART and facilitate access to RCH services
States with poor testing load need to ascertain reasons for poor use and take remedial measures.
Establish district model ICTCs as training and referral centres Staggered approach to scale up based on identified need and
capacity over the project period (Capacity building) Set up EQAS for ICTC testing and quality
assurance systems for counselling services

Care, Support ...Community care and support programs
Identify and develop partnership with NGOs/CBOs Community care centres where needed
Integration of prevention and treatment measures and linkages Linkages established between ART centres, PLHA networks and
TIs/Workplace interventions Prevention education for positive persons Risk reduction strategies for PLHA and their partners Prevention case management integrated into OI and ART Partner referrals through counselling Screening for TB/STI of PLHA Capacity building of PLHA networks to participate in prevention
programmes (IEC, Advocacy, Workplace, School AIDS programme, Youth friendly services)
Strengthening positive prevention programmes

Care, Support ... Collaboration with PLHA networks
Facilitating the formation of PLHA CBOs/networks Capacity building of PLHA Advocacy and technical support for policy changes to enable GIPA Development and implementation of policies to create an enabling
environment to enhance the involvement of PLHA and affected people at all levels
Linking livelihood support Advocacy with government and private sector to support PLHA, Through membership of SHGs, savings fund, corpus fund, vocational
trainings for IGP Capacity building of PLHA to advocate for livelihood support, design and
manage micro credit/ IGP Reducing stigma and discrimination
Advocacy for enactment of State-specific anti discriminatory laws Providing and supporting community based programs especially in the
workplace Supporting formation of PLHA networks at district levels

Centres of support under the CST component in the State
Programs Number of facilities
Anti Retero viral centres 37PPP Anti Retero viral centres 1Link Anti Retero viral centres 46 ( target 90)Integrated Counselling & testing centres 783Mobile 11Community Care Centres 40 + 1Child focussed Community Care Centres 5Drop in Centres 37
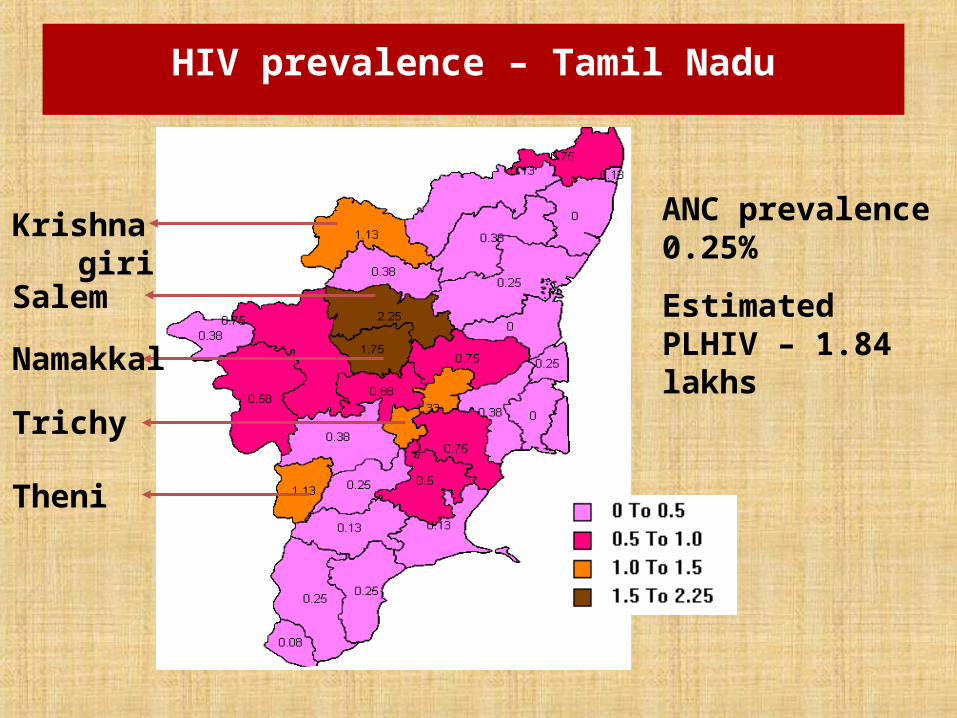
HIV prevalence – Tamil Nadu
Salem
Namakkal
Krishnagiri
Trichy
Theni
ANC prevalence 0.25%
Estimated PLHIV – 1.84 lakhs

1
1.13
0.87
0.75
0.65
0.5
0.375
0.25
0
0.2
0.4
0.6
0.8
1
1.2
2000 2001 2002 2003 2004 2005 2006 2007
Year
Per
cen
tHIV Prevalence - ANC (%)

Role of Pharmacists
Prevention
Care & treatment

Prevention
• Promotion of safe and healthy sexual behaviour • Improve the management and control of STIs• Reduce parental transmission • Provide appropriate post exposure prophylaxis

Care & Treatment• Provide treatment, care & support services in health facilities
– Supply of appropriate drugs for OI management and HIV related infections
– Budgeting and forecasting the demands for dispensing – Advise on rational drug usage
• Nutrition • Antibiotics• ART• TB drugs • Prophylaxis • Anti fungal drugs
– ART • Adherence• Resistance • Efficacy • Side effects
– Help in referral services• Provide adequate treatment, care and support services in
communities – since their public interaction is more, vital information can be spread

Role of Pharmacist in Institutional DOT Provider
• Check the TB identity card for CPT prescription• Provide monthly supply of CPT to the HIV-infected TB patients,
who have been prescribed CPT by the attending MO and record the date of delivering on the TB treatment card.
• Encourage the HIV-infected TB patients, during their monthly visit to PHI for collecting CPT, to meet the Medical Officer for routine examination
• Ensure confidentiality of HIV status of the TB patients remains confidential with in the health system
• Monthly basis indent (from MO-TC) and maintain stock of Cotrimoxazole for the HIV-infected
• TB patients prescribed CPT for the entire duration of their TB treatment


















