Role of disease-associated tolerance in infectious superspreaders · Role of disease-associated...
6
Role of disease-associated tolerance in infectious superspreaders Smita Gopinath a , Joshua S. Lichtman b , Donna M. Bouley c , Joshua E. Elias b , and Denise M. Monack a,1 Departments of a Microbiology and Immunology, b Chemical and Systems Biology, c Comparative Medicine, Stanford University School of Medicine, Stanford, CA 94305 Edited by Ruslan Medzhitov, Yale University School of Medicine, New Haven, CT, and approved September 15, 2014 (received for review May 30, 2014) Natural populations show striking heterogeneity in their ability to transmit disease. For example, a minority of infected individuals known as superspreaders carries out the majority of pathogen transmission events. In a mouse model of Salmonella infection, a subset of infected hosts becomes superspreaders, shedding high levels of bacteria (>10 8 cfu per g of feces) but remain asymptom- atic with a dampened systemic immune state. Here we show that superspreader hosts remain asymptomatic when they are treated with oral antibiotics. In contrast, nonsuperspreader Salmonella- infected hosts that are treated with oral antibiotics rapidly shed superspreader levels of the pathogen but display signs of morbid- ity. This morbidity is linked to an increase in inflammatory myeloid cells in the spleen followed by increased production of acute- phase proteins and proinflammatory cytokines. The degree of co- lonic inflammation is similar in antibiotic-treated superspreader and nonsuperspreader hosts, indicating that the superspreader hosts are tolerant of antibiotic-mediated perturbations in the in- testinal tract. Importantly, neutralization of acute-phase proinflam- matory cytokines in antibiotic-induced superspreaders suppresses the expansion of inflammatory myeloid cells and reduces morbid- ity. We describe a unique disease-associated tolerance to oral anti- biotics in superspreaders that facilitates continued transmission of the pathogen. host-to-host transmission | carriers | pathogenesis | acute phase response A growing body of work has demonstrated that a minority of infected hosts is responsible for the majority of new infec- tions within the population. Woolhouse et al. first formulated the 80/20 rule of host–pathogen interactions, wherein 20% of the infected hosts (“superspreaders”) are responsible for 80% of the infections (1). For example, analysis of cattle herds infected with Escherichia coli O157:H7 has demonstrated that high-shedding individuals (8–20% of the infected herd) are responsible for the majority of the pathogen transmission to uninfected members of the herd (2–5). The identification of these superspreaders is of key importance for disease treatment and clearance (1, 6–8). However, comparatively little is known about the host immune response that contributes to the superspreader state. An infected host can fight pathogenic infection by two distinct processes—resistance and tolerance. Resistance encompasses a diverse set of mechanisms used by the host to control pathogen invasion and replication. Tolerance, conversely, employs differ- ent mechanisms that help the host organism tolerate the damage caused by both the pathogenic infection and the resulting im- mune response, thereby maintaining host health (9–11). Al- though very little is known about the full spectrum of tolerance mechanisms, the few studies in animals suggest that, because pathogens and immunopathology can potentially affect almost any physiological process, tolerance is not restricted to a single protective pathway (9, 12, 13). Unlike resistance mechanisms, tolerance strategies do not have direct negative consequences for the pathogen and therefore should place no selective pressures upon the pathogen (12, 14, 15). For these reasons, tolerance mechanisms have been hypothesized to play a role in the main- tenance of the asymptomatic superspreader state (11, 12, 15). However, an experimental link between tolerance and trans- mission has not been demonstrated. Upon oral infection with Salmonella enterica serovar Typhimurium, in our mouse model of Salmonella transmission, 30% of infected hosts shed the pathogen at high levels (>10 8 Salmonella per gram of feces). These superspreader hosts are able to efficiently infect naive cagemates (16) and possess a dis- tinct immune phenotype compared with the majority of the infected hosts [which shed the pathogen at lower levels and are nonsuperspreaders (17)]. Importantly, both superspreader and nonsuperspreader hosts carry identical pathogen burdens across all tissues except the intestinal tract. The host microbiota plays an important role in protecting the host from acute Salmonella infection (18, 19) and in the establishment of the superspreader state (16). Frequent subtherapeutic antibiotic use is common among livestock animals, and the resulting disruption of host gut flora or dysbiosis has long-lasting effects on the health of the host (20). Here, we demonstrate that superspreader hosts are uniquely able to tolerate antibiotic treatment and importantly, this tolerance is not maintained in nonsuperspreader hosts. Results Superspreaders Are Tolerant of Oral Antibiotic Treatment. We have previously shown that administration of a single dose of 5 mg of streptomycin to nonsuperspreader hosts results in the increase of intestinal Salmonella burden to superspreader levels overnight (>10 8 cfu/g) (16, 17). We observed, however, that, unlike naturally occurring superspreaders, these antibiotic-induced superspreaders Significance A minority of infected hosts is thought to be responsible for the majority of pathogen transmission events. Surprisingly little is known about what distinguishes superspreader hosts from the rest of the infected population. Using a mouse model of Salmonella infection, we show that levels of Salmonella are equivalent between antibiotic-treated superspreader and nonsuperspreader hosts; however, superspreader hosts are uniquely able to tolerate antibiotic treatment, unlike non- superspreader hosts. We find that nonsuperspreaders have a hyperinflammatory response to antibiotic treatment, result- ing in increased inflammatory myeloid cells that contribute to the morbidity observed. Superspreaders display neither an increased frequency of inflammatory myeloid cells nor mor- bidity upon antibiotic treatment. Our data describe tolerance mechanisms unique to superspreader hosts that enable sus- tained pathogen transmission. Author contributions: S.G. and D.M.M. designed research; S.G. performed research; J.S.L. and J.E.E. contributed new reagents/analytic tools; S.G., J.S.L., and D.M.B. analyzed data; and S.G. and D.M.M. wrote the paper. The authors declare no conflict of interest. This article is a PNAS Direct Submission. 1 To whom correspondence should be addressed. Email: [email protected]. This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10. 1073/pnas.1409968111/-/DCSupplemental. 15780–15785 | PNAS | November 4, 2014 | vol. 111 | no. 44 www.pnas.org/cgi/doi/10.1073/pnas.1409968111 Downloaded by guest on July 27, 2021
Transcript of Role of disease-associated tolerance in infectious superspreaders · Role of disease-associated...

Role of disease-associated tolerance ininfectious superspreadersSmita Gopinatha, Joshua S. Lichtmanb, Donna M. Bouleyc, Joshua E. Eliasb, and Denise M. Monacka,1
Departments of aMicrobiology and Immunology, bChemical and Systems Biology, cComparative Medicine, Stanford University School of Medicine, Stanford,CA 94305
Edited by Ruslan Medzhitov, Yale University School of Medicine, New Haven, CT, and approved September 15, 2014 (received for review May 30, 2014)
Natural populations show striking heterogeneity in their ability totransmit disease. For example, a minority of infected individualsknown as superspreaders carries out the majority of pathogentransmission events. In a mouse model of Salmonella infection,a subset of infected hosts becomes superspreaders, shedding highlevels of bacteria (>108 cfu per g of feces) but remain asymptom-atic with a dampened systemic immune state. Here we show thatsuperspreader hosts remain asymptomatic when they are treatedwith oral antibiotics. In contrast, nonsuperspreader Salmonella-infected hosts that are treated with oral antibiotics rapidly shedsuperspreader levels of the pathogen but display signs of morbid-ity. This morbidity is linked to an increase in inflammatory myeloidcells in the spleen followed by increased production of acute-phase proteins and proinflammatory cytokines. The degree of co-lonic inflammation is similar in antibiotic-treated superspreaderand nonsuperspreader hosts, indicating that the superspreaderhosts are tolerant of antibiotic-mediated perturbations in the in-testinal tract. Importantly, neutralization of acute-phase proinflam-matory cytokines in antibiotic-induced superspreaders suppressesthe expansion of inflammatory myeloid cells and reduces morbid-ity. We describe a unique disease-associated tolerance to oral anti-biotics in superspreaders that facilitates continued transmission ofthe pathogen.
host-to-host transmission | carriers | pathogenesis | acute phase response
Agrowing body of work has demonstrated that a minority ofinfected hosts is responsible for the majority of new infec-
tions within the population. Woolhouse et al. first formulatedthe 80/20 rule of host–pathogen interactions, wherein 20% of theinfected hosts (“superspreaders”) are responsible for 80% of theinfections (1). For example, analysis of cattle herds infected withEscherichia coli O157:H7 has demonstrated that high-sheddingindividuals (8–20% of the infected herd) are responsible for themajority of the pathogen transmission to uninfected membersof the herd (2–5). The identification of these superspreaders isof key importance for disease treatment and clearance (1, 6–8).However, comparatively little is known about the host immuneresponse that contributes to the superspreader state.An infected host can fight pathogenic infection by two distinct
processes—resistance and tolerance. Resistance encompasses adiverse set of mechanisms used by the host to control pathogeninvasion and replication. Tolerance, conversely, employs differ-ent mechanisms that help the host organism tolerate the damagecaused by both the pathogenic infection and the resulting im-mune response, thereby maintaining host health (9–11). Al-though very little is known about the full spectrum of tolerancemechanisms, the few studies in animals suggest that, becausepathogens and immunopathology can potentially affect almostany physiological process, tolerance is not restricted to a singleprotective pathway (9, 12, 13). Unlike resistance mechanisms,tolerance strategies do not have direct negative consequences forthe pathogen and therefore should place no selective pressuresupon the pathogen (12, 14, 15). For these reasons, tolerancemechanisms have been hypothesized to play a role in the main-tenance of the asymptomatic superspreader state (11, 12, 15).
However, an experimental link between tolerance and trans-mission has not been demonstrated.Upon oral infection with Salmonella enterica serovar
Typhimurium, in our mouse model of Salmonella transmission,30% of infected hosts shed the pathogen at high levels (>108
Salmonella per gram of feces). These superspreader hosts areable to efficiently infect naive cagemates (16) and possess a dis-tinct immune phenotype compared with the majority of theinfected hosts [which shed the pathogen at lower levels and arenonsuperspreaders (17)]. Importantly, both superspreader andnonsuperspreader hosts carry identical pathogen burdens acrossall tissues except the intestinal tract. The host microbiota playsan important role in protecting the host from acute Salmonellainfection (18, 19) and in the establishment of the superspreaderstate (16). Frequent subtherapeutic antibiotic use is commonamong livestock animals, and the resulting disruption of hostgut flora or dysbiosis has long-lasting effects on the health of thehost (20). Here, we demonstrate that superspreader hosts areuniquely able to tolerate antibiotic treatment and importantly,this tolerance is not maintained in nonsuperspreader hosts.
ResultsSuperspreaders Are Tolerant of Oral Antibiotic Treatment. We havepreviously shown that administration of a single dose of 5 mg ofstreptomycin to nonsuperspreader hosts results in the increase ofintestinal Salmonella burden to superspreader levels overnight(>108 cfu/g) (16, 17). We observed, however, that, unlike naturallyoccurring superspreaders, these antibiotic-induced superspreaders
Significance
A minority of infected hosts is thought to be responsible forthe majority of pathogen transmission events. Surprisinglylittle is known about what distinguishes superspreader hostsfrom the rest of the infected population. Using a mouse modelof Salmonella infection, we show that levels of Salmonellaare equivalent between antibiotic-treated superspreader andnonsuperspreader hosts; however, superspreader hosts areuniquely able to tolerate antibiotic treatment, unlike non-superspreader hosts. We find that nonsuperspreaders havea hyperinflammatory response to antibiotic treatment, result-ing in increased inflammatory myeloid cells that contributeto the morbidity observed. Superspreaders display neither anincreased frequency of inflammatory myeloid cells nor mor-bidity upon antibiotic treatment. Our data describe tolerancemechanisms unique to superspreader hosts that enable sus-tained pathogen transmission.
Author contributions: S.G. and D.M.M. designed research; S.G. performed research; J.S.L.and J.E.E. contributed new reagents/analytic tools; S.G., J.S.L., and D.M.B. analyzed data;and S.G. and D.M.M. wrote the paper.
The authors declare no conflict of interest.
This article is a PNAS Direct Submission.1To whom correspondence should be addressed. Email: [email protected].
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.1409968111/-/DCSupplemental.
15780–15785 | PNAS | November 4, 2014 | vol. 111 | no. 44 www.pnas.org/cgi/doi/10.1073/pnas.1409968111
Dow
nloa
ded
by g
uest
on
July
27,
202
1

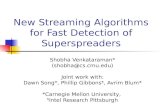
displayed signs of morbidity and even death. It has been shownthat streptomycin alone can induce gastrointestinal inflammation(21). Thus, we treated superspreaders with antibiotics to controlfor potential effects of the antibiotic on the microbiota and hostimmune response. After streptomycin treatment, both super-spreaders and nonsuperspreaders had identical levels of fecalSalmonella (Fig. 1A). Surprisingly, superspreader hosts treatedwith antibiotics did not lose weight, remaining at 98% (±2.5%)of their initial weight. In contrast, nonsuperspreader hosts trea-ted with antibiotics lost an average of 15% (±9.7%) of their bodyweight (Fig. 1B). Indeed, nonsuperspreaders lost significantlymore weight compared with superspreaders at 5 d after antibiotictreatment (Fig. 1C).To determine the cause of this weight loss, we first inves-
tigated the pathogen and commensal bacterial burden in theseantibiotic-induced superspreaders. We measured the levels of
Salmonella in systemic tissues, such as the spleen and mesentericlymph nodes, and determined that the bacterial burden didnot differ significantly between antibiotic-treated superspreaderand nonsuperspreader hosts (Fig. 1D). Commensal outgrowth, asmeasured by anaerobic growth on brain and heart infusion bloodagar, did not differ significantly between the groups. Finally,neither Salmonella Typhimurium (Fig. 1D) nor commensal bac-teria was detected in the blood, confirming that weight loss wasnot due to bacterial sepsis mediated by Salmonella or culturablecommensal outgrowth.Because the Salmonella Typhimurium strain we use is resistant
to streptomycin, it was possible that the weight loss observedin streptomycin-treated nonsuperspreaders was induced by theovernight increase (100- to 100,000-fold) in Salmonella numbersin the gastrointestinal tract. To control for this increase, wetreated superspreader and nonsuperspreader hosts orally withneomycin, an antibiotic to which the Salmonella Typhimuriumstrain is sensitive. Upon treatment with a single dose (5 mg) ofneomycin, the fecal Salmonella levels in nonsuperspreaders stillrose to superspreader levels (Fig. 1E). Two weeks after oralantibiotic treatment, nonsuperspreaders lost significantly moreweight (up to 12 ± 10% of their initial body weight; Fig. 1F).These results indicate that superspreaders are protected fromantibiotic-induced gastrointestinal disruptions.
Salmonella-Infected Hosts Are Not Tolerant to Antibiotic TreatmentDuring the First Week of Infection. Superspreaders have a distinctimmune phenotype compared with hosts that are not colonizedwith high levels of Salmonella in the intestinal tract (17). Thesuperspreader immune phenotype consists of an active, pro-longed innate immune response that is characterized by higherlevels of neutrophils in intestinal and systemic sites and a sup-pressed systemic adaptive CD4 T-cell response. In contrast,nonsuperspreaders have lower levels of gastrointestinal andsystemic inflammation, but an active, robust CD4 T-cell response(17). Our previous studies demonstrated that the immune stateof superspreaders is fully established by 2 wk after infection. Thisfinding raises the question: Is the tolerance to antibiotic treat-ment gained by superspreaders? To test this possibility, wetreated hosts with an oral antibiotic before the adaptive immuneresponse was initiated. Because we had shown previously that theadaptive CD4 T-cell response is not activated until 7–9 d afterinfection (17), the treatment of hosts with an antibiotic 4 d afterSalmonella infection would eliminate the potential contributionof Salmonella-specific CD4 T-cell responses. Mice treated withstreptomycin at day 4 after infection lost significantly moreweight than PBS-treated cagemates (Fig. 1G), suggesting thata Salmonella-specific T-cell response is not required for theweight loss observed after antibiotic treatment. Together, theseresults indicate that the superspreader-specific tolerance to an-tibiotic treatment develops later during infection.
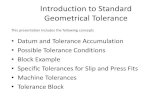
Antibiotic-Treated Nonsuperspreaders Have Increased Acute-PhaseResponse. Having established that antibiotic-driven weight losscould occur before the onset of Salmonella-specific adaptiveT-cell responses, we next characterized the inflammatory re-sponse in these hosts. We examined cytokine levels in theserum and intestinal wash of antibiotic-treated superspreadersand nonsuperspreaders. There was no significant difference inthe average serum cytokine level between the two groups.However, there was a wide variation in the levels of proin-flammatory cytokines in antibiotic-treated nonsuperspreaders (Fig.2 A and B), which was influenced by the two hosts with the largestweight loss (>20% of their initial body weight). Indeed, the onlymice that had detectable levels of serum IL-1β and TNF-α weremoribund (Fig. 2A). This pattern was also seen in intestinal washes,with the most moribund mice having the highest levels of proin-flammatory cytokines, especially IL-1β, TNF-α, and IL-6 (Fig. 2B).
A
E
Days post streptomycin treatment
B
F
ns nsD ns
D1 D6 D1470
80
90
100
110
120
130
Days post neomycin treatment
**
Pe
rce
nta
ge
of i
nit
ial w
eig
ht
Non-SS +Antibiotic
SS + Antibiotic
Spleen mLN Blood
10
100
1000
10000
10
20
30
40
50
CF
U/g
m T
issu
e
CF
U/ m
l
1 2 3 4 570
80
90
100
110
Pe
rce
nta
ge
of i
nit
ial w
eig
ht
****
0 1 2 3 4 510
10
10
10
10
10
10
10
10
CF
U/g
m F
ece
s
Days post streptomycin treatment
C ****p<0.0001
Non-superspreader
Streptomycin
Superspreader
Streptomycin
D0 D1 D14101010101010101010
10
CF
U/g
m
Days post neomycin treatment
Pe
rce
nta
ge
of i
nit
ial w
eig
ht
70
80
90
100
110
*****
**
Non-SS +Antibiotic
SS + Antibiotic
Non-SS +Antibiotic
SS + Antibiotic
Non-SS +Antibiotic
SS + Antibiotic
Non-SS +Antibiotic
SS + Antibiotic
Day 1 Day 2 Day 4 Day 5 Day 670
80
90
100
110
120
Pe
rce
nta
ge
of i
nit
ial w
eig
ht
StreptomycinPBS
** ** ** * **
Days post streptomycin treatment
G
Fig. 1. Superspreaders are tolerant to oral antibiotic treatment. Micewere infected for 30 d, and their transmission status was identified. (A–F)Superspreaders (SS; black circles) and nonsuperspreaders (non-SS; red squares)were treated with 5 mg of streptomycin (A–D) or neomycin (E and F) via oralgavage. Weight and fecal Salmonella burden were recorded for the indicatedperiod. Data shown is representative of a minimum of two experiments witha total of 10–15 mice per condition. (A and B) Each data point represents anindividual mouse. (C) Mice from two independent experiments were pooledwith a total of 10–15 mice per condition, and weight data are shown from 5 dafter streptomycin treatment. (D) Salmonella bacterial burden of indicatedorgans (left y axis) and whole blood (right y axis) in streptomycin-treatedsuperspreaders and nonsuperspreaders. (E and F) Fecal Salmonella burdenwas quantified in neomycin treated superspreader and nonsuperspreaderhosts (E), and weight data were recorded at indicated times (F). (G) Micewere infected for 4 d (shedding status cannot be confirmed at this timepoint) and treated with 5 mg of streptomycin (red squares) or PBS (blacksquares), and weight was recorded for the time period indicated. *P < 0.05;**P < 0.005; ****P < 0.0001. ns, not significant.
Gopinath et al. PNAS | November 4, 2014 | vol. 111 | no. 44 | 15781
IMMUNOLO
GYAND
INFLAMMATION
Dow
nloa
ded
by g
uest
on
July
27,
202
1

Together, these data suggest that a severe inflammatory re-sponse may underlie the morbidity observed in antibiotic-treatednonsuperspreaders.To confirm that morbidity was linked to an inflammatory re-
sponse, we used a nontargeted proteomics approach to analyzehost-secreted proteins in the feces. We found a large numberof proteins belonging to the acute-phase response. Of the 17identified acute-phase proteins, 10 were significantly positivelycorrelated to weight loss (Fig. 2C). These results indicate thatthe morbidity observed in antibiotic-treated nonsuperspreaderhosts (Fig. 2D) is linked to activation of the acute-phase response.
Antibiotic-Treated Nonsuperspreaders Have Increased Splenic Inflam-matory Myeloid Cells. Next, we investigated the inflammatoryresponse by analyzing the frequency of Ly6C+ CD11b+ inflam-matory myeloid cells in the mesenteric lymph nodes and spleen.These cells encompass both inflammatory monocytes and neu-trophils (Fig. S1A), cell types that have been shown to secreteIL-1β and TNF-α (22, 23). We found that antibiotic-treatednonsuperspreaders had significantly more inflammatory myeloidcells in the spleen compared with antibiotic-treated super-spreaders 6 d after treatment (Fig. 3 A and B). Upon analysis of
the subsets of inflammatory myeloid cells, we found that thespleens from all of the antibiotic-treated nonsuperspreader micecontained significantly more inflammatory monocytes than an-tibiotic-treated superspreaders (Fig. S1B). A similar trend wasseen for splenic neutrophil frequencies (Fig. S1C), with the dif-ference in neutrophil frequencies between antibiotic-treatedsuperspreader and nonsuperspreaders being significant afterremoving the sickest mice (mice that lost >20% of their initialbody weight; Fig. S1C).This increase in inflammatory cells is not limited to systemic
sites. Indeed, naturally occurring superspreaders and antibiotic-induced superspreaders have cecal and colonic inflammatory cellinfiltrates. In contrast to the spleen, the levels of cecal and co-lonic inflammation were the same in both groups of mice, asrevealed by histopathological analysis (Fig. 3 C and D). Addi-tionally, the frequency of colonic neutrophils in antibiotic-trea-ted superspreaders and nonsuperspreaders was identical anddid not vary with morbidity (Fig. 3E), further confirming thatsuperspreaders and nonsuperspreaders have similar levels ofintestinal and colonic inflammatory cells after antibiotic treat-ment. Together, our results indicate that the increased morbidityin nonsuperspreader mice is linked to increased inflammatorymyeloid cells in the spleen, but not the gut.
CD4 T Cells Contribute to Antibiotic-Induced Morbidity but NotSuperspreader Tolerance. Although antibiotic-mediated morbiditycan occur before the development of Salmonella-specific adaptiveimmune responses (Fig. 1G), we wondered whether CD4 T cellscontribute to morbidity in antibiotic-treated nonsuperspreaders.
SS + Strep Non-SS + Strep
High protein spectral counts
A B Weight
Day 6 post streptomycin
IFNγ IL-1β TNFα IL-6 IL-101
10
100
1000
10000
pg
/ml
Non-superspreader
Streptomycin
70
80
90
100
110
Pe
rce
nta
ge
of i
nit
ial w
eig
ht
IFNγ IL-1β TNFα IL-6 IL-10
0.1
1
10
100
1000
10000
pg
/ml
**
C
Serum albumin
Ceruloplasmin
Alpha-1-antitrypsin 1-3
Serotransferrin
PK-120
Haptoglobin
Alpha-2-HS-glycoprotein
Fibrinogen gamma chain
Fibrinogen
Serine protease inhibitor A3N
Hemopexin
Fibrinogen beta chain
Putative uncharacterized protein
Inter-alpha-trypsin inhibitor heavy chain H3
Complement C5
Complement component 4B
Fn1 protein
*
*
*
*
*
*
*
*
Host Weight
*
*
Superspreader
Streptomycin
Non-superspreader
Streptomycin
**
Pe
rce
nta
ge
of i
nit
ial w
eig
ht
80
90
100
110D
Increased host weight
Fig. 2. Antibiotic-mediated weight loss is correlated with activation of theacute-phase response. Mice were infected for 30 d, and their transmissionstatus was identified. Superspreaders (black circles) and nonsuperspreaders(red squares) were treated with 5 mg of antibiotic via oral gavage. Super-spreaders and nonsuperspreaders were treated with streptomycin and sac-rificed 6 d after antibiotic treatment. Data shown are representative of twoexperiments with a total of 8–10 mice in each condition. (A and B) Serum (A)and intestinal cytokine (B) levels were measured by ELISA. Each point rep-resents an individual mouse, and data are representative of two experimentswith 10–15 mice per group. Nonsuperspreader hosts that lost >20% of theirtotal body weight are represented by filled squares (Inset). (C) Fecal samplesfrom streptomycin-treated superspreaders and nonsuperspreaders wereprocessed, and host-derived proteins were identified by using mass spec-trometry. Data show normalized spectral counts from the 17 identifiedproteins in the acute-phase response pathway depicted in a heat map whereintensity was normalized within each protein and warmer colors representincreased spectral counts as depicted in the key. Host weight was normalizedfrom red to blue with warmer colors depicting increased host weight. Allproteins were correlated to host weight loss using Spearman’s correlation.*Significant correlations. (D) Host weight data from C is quantified, andsignificance is calculated by using the two-tailed Mann–Whitney test.**P < 0.005.
B
0 102 103 104 105
0
102
103
104
105
16.6 6.2
0 102 103 104 105
0
102
103
104
105
CD
11
b
Ly6C
Non-superspreaders
Streptomycin
Superspreaders
Streptomycin
A
% N
eu
tro
ph
ils
E
0
20
40
60
80
100
His
top
ath
olo
gic
al s
core
Non-superspreaders
Streptomycin
Superspreaders
Streptomycin
C D
0
5
10
15
% L
y6C
+C
D1
1b
+
*
Non-superspreaders
Streptomycin
Superspreaders
Streptomycin
1000μm 1000μm
Transmural
Mucosal and submucosal
0
5
10
15
Non-SS
Streptomycin
SS
Streptomycin
Non-superspreaders + Streptomycin Superspreaders + Streptomycin
Fig. 3. Antibiotic-treated nonsuperspreaders have increased inflammatorymyeloid cells in the spleen, but not the gut. Mice were infected for 30 d,and their shedding status was identified. Superspreaders (black) and non-superspreaders (red) were treated with 5 mg of antibiotic via oral gavage.(A and B) Splenic cells were collected from streptomycin-treated super-spreaders and nonsuperspreaders 6 d after antibiotic treatment. (A) Repre-sentative FACS plot shows frequency of CD11b+ Ly6C+ inflammatory myeloidcells gated on nonlymphocytes. (B) Total frequency of myeloid inflammatorycells expressed as a percentage of nonlymphocytes. (C and D) Ceca werefixed, and hematoxylin/eosin-stained sections were scored for histopatho-logical changes. A representative figure of a cecal section from each group isdisplayed in C, and histopathological scores are represented in D. (E) Barsrepresent colonic neutrophils measured as a frequency of CD11b+ cells 6 dafter streptomycin treatment. *P < 0.05.
15782 | www.pnas.org/cgi/doi/10.1073/pnas.1409968111 Gopinath et al.
Dow
nloa
ded
by g
uest
on
July
27,
202
1

Neutralization of CD4 T cells in mice that had been infectedwith Salmonella for 30 d was sufficient to rescue antibiotic-treated nonsuperspreaders from significant weight loss (Fig. 4Aand Fig. S2). There was a concurrent decrease in the numbers ofsplenic CD11b+Ly6C+ inflammatory myeloid cells and the con-stituent groups of inflammatory monocyte and neutrophils inCD4 T-cell–depleted mice (Fig. 4B). However, bacterial burdensin the spleen were significantly increased in CD4-neutralizedmice compared with controls (Figs. 1D and 4C). Importantly,superspreader hosts treated with CD4 T-cell–neutralizing anti-body did not lose weight and remained asymptomatic after an-tibiotic treatment, indicating that CD4 T cells are not requiredfor maintenance of superspreader tolerance (Fig. 4A).
Neutralizing IL-1β and TNF-α Alleviates Antibiotic-Treated Non-superspreader Morbidity. Based on the links between the levelsof inflammatory myeloid cells, proinflammatory cytokines, fecalacute-phase proteins, and morbidity in antibiotic-treated non-superspreader mice, we hypothesized that suppression of theacute-phase cytokines might restore tolerance in antibiotic-treatednonsuperspreaders. To test this hypothesis, we neutralized IL-1βand TNF-α—the two acute-phase cytokines detected in mori-bund antibiotic-treated nonsuperspreader hosts. Nonsuperspreaderstreated with neomycin or streptomycin were injected with neutral-izing antibodies against IL-1β and TNF-α or with the isotypecontrol antibody. The mice that received the IL-1β– and TNF-α–neutralizing antibodies lost significantly less weight com-pared with antibiotic-treated nonsuperspreaders injected withthe isotype control antibodies (Fig. 5 A and B). As expected,the neutralizing antibodies did not affect the weights of antibiotic-treated superspreader hosts (Fig. 5A). Importantly, the frequenciesof inflammatory myeloid cells and neutrophils in antibiotic-treatednonsuperspreader hosts were significantly reduced (Fig. 5 C andD). This decrease in frequency was mirrored by significantdecreases in the numbers of total inflammatory myeloid cells,inflammatory monocytes, and neutrophils in the spleens ofacute-phase cytokine-neutralized hosts (Fig. 5E). Thus, neutral-ization of acute-phase cytokines was sufficient to suppress the
expansion of the inflammatory myeloid cell population and bringthem to levels comparable to those observed in superspreaderhosts. Systemic and fecal Salmonella levels were not affected bytreatment with neutralizing antibodies (Fig. 5 F and G), con-firming that neutralization of acute-phase cytokines resulted inincreased tolerance of the bacterial burden.
DiscussionDisease tolerance to pathogen infection has been characterizedin genetically distinct mouse and Drosophila strains (14, 24, 25),as well as in a mouse model of viral and bacterial coinfection(26). Our results demonstrate that tolerance can also be inducedin a subset of individuals infected with the same pathogen ina genetically similar host population. Unlike resistance, toler-ance has been proposed to not have negative consequences forthe pathogen (9–11, 15). However, recent theoretical work haspredicted that the use of therapeutic mechanisms that alleviatesymptoms of illness in infected hosts but do not alter pathogenburden can have negative epidemiological consequences for host
Day 1 Day 2 Day 3 Day 4 Day 560
80
100
120
140
Pe
rce
nta
ge
of i
nit
ial
we
igh
t
Non-SS Streptpmycin Isotype
Non-SS Streptomycin CD4 DepletedSS Streptomycin CD4 Depleted
**
A
CD45+ CD11b+Ly6C+ Neutrophils
10
10
10
10** * ** * **
Nu
mb
er
of c
ells
Infl. Mon.
B
Non-SS
Isotype
Non-SS
Neut.
SS
Neut.
103
104
105
CF
U/g
m
*C
Fig. 4. CD4 T cells contribute to antibiotic-induced morbidity but notsuperspreader tolerance. Mice were infected for 30 d, and their sheddingstatus was identified. Superspreaders (black circles) and nonsuperspreaders(red squares) were treated with 5 mg of streptomycin via oral gavage. Micewere treated with CD4-neutralizing antibodies or the isotype control (n = 4or 5 in each group) 1 d before antibiotic treatment and at 2 and 4 d afterantibiotic treatment. (A) Each point represents an individual mouse, and theweight data were collected daily. (B) Splenocytes were collected and rep-resentative cell populations were enumerated. In the isotype group, a singlemouse was excluded due to morbidity. (C) Splenic Salmonella burden wasquantified. *P < 0.05; **P < 0.005.
A
C
B
% L
y6C+
CD11
b+
Non-SSIsotype
Non-SSNeutralized
SSNeutralized
SSIsotype
Non-SSIsotype
Non-SSNeutralized
**
85
90
95
100
105
110
Perc
enta
ge o
f ini
tial w
eigh
t
*
% N
eutro
phils
D *
0
5
10
15
20
25
0
5
10
15
20
25
Non-SSIsotype
Non-SSNeutralized
SSNeutralized
SSIsotype
70
80
90
100
110
120
Non-SSIsotype
Non-SSNeutralized
SSNeutralized
SSIsotype
** ns
Perc
enta
ge o
f ini
tial w
eigh
t
F
G
Isotype Neutralized
E
0
2×10
4×10
6×10
8×10
1×10 ** ***
CD11b+Ly6C+ Infl. Mon. NeutrophilsSpleen mLN Feces
1010101010101010
CFU
/gm
Spleen mLN Feces101010101010101010
CFU
/gm
Isotype Neutralized
Num
ber o
f cel
ls
ns ns
ns ns
ns
ns
Fig. 5. Neutralization of acute-phase cytokines ablates weight loss in an-tibiotic-treated nonsuperspreaders. Mice were infected for 30 d, and theirtransmission status was identified. Superspreaders (SS; black circles) andnonsuperspreaders (Non-SS; red squares) were treated with 5 mg of neo-mycin (A and C–F) or streptomycin (B and G) via oral gavage. Data shown arerepresentative of two experiments with a total of 8–10 mice in each con-dition. Along with the antibiotic, mice were injected intraperitoneally withneutralizing antibodies against IL-1β and TNF-α (filled shapes) and the iso-type control (open shapes). (A and B) Each point represents an individualmouse, and the weight data were measured at 12 d after neomycin treat-ment (A) and 6 d after streptomycin treatment (B). Splenocytes were col-lected from mice in A, and inflammatory myeloid cells (C) and neutrophils(D) were quantified as a frequency of nonlymphocytes. Cell populationswere enumerated in E. Bacterial burden of selected tissues was quantified at12 d after neomycin treatment (F) and 6 d after streptomycin treatment (G)*P < 0.05; **P < 0.005. ns, not significant.
Gopinath et al. PNAS | November 4, 2014 | vol. 111 | no. 44 | 15783
IMMUNOLO
GYAND
INFLAMMATION
Dow
nloa
ded
by g
uest
on
July
27,
202
1

populations (13). We have identified a disease-associated toler-ance mechanism that is specific to superspreaders and enablesthe host to tolerate inflammation mediated by oral antibiotics,thereby facilitating continued pathogen transmission. Non-superspreaders, however, display morbidity upon antibiotic treat-ment. This morbidity is correlated with the activation of theacute-phase inflammatory response and the increase in sys-temic inflammatory myeloid cells. Neutralization of the acute-phase response cytokines in these nonsuperspreader hosts reducesmorbidity while leaving pathogen burden unchanged, therebyenabling continued pathogen transmission. Our results furtherunderline the importance of identification and treatment ofhighly infectious superspreader hosts.We have previously shown that superspreader hosts have
more systemic inflammation compared with nonsuperspreaderhosts, yet appear perfectly healthy. However, upon antibiotictreatment, superspreader hosts have a relatively reduced in-flammatory response compared with nonsuperspreaders. Ourdata suggest that the previously described superspreader-specificimmune phenotype allows superspreaders to tolerate antibioticinsult and resulting inflammation. For example, superspreadershave dampened responses to some cytokines (IL-6 in particular)and lower basal phosphorylated STAT proteins (17). Thus,superspreader hosts may be better equipped to tolerate higherlevels of proinflammatory cytokines, and we speculate that thesetolerance mechanisms protect the host from morbidity associ-ated with antibiotic-driven dysbiosis. One hypothesis we testedwas whether superspreaders had higher levels of IL-1 receptoragonist, thereby inhibiting the effect of IL-1β via competitivebinding to the IL-1 receptor (27). However, we found thatsuperspreaders did not have higher levels of IL-1 receptor ago-nist in serum or intestinal wash (Fig. S3), indicating an alternatemechanism(s) of tolerance of acute-phase cytokines. Intriguingly,acute-phase cytokine neutralization in antibiotic-treated super-spreaders did not result in suppression of the neutrophils orinflammatory monocytes, suggesting that proliferation of thesecell types may be differentially regulated in superspreaders. Al-though inflammatory monocytes (28) are observed during chronicSalmonella infection, little is known about their functionality in thecontext of transmission. We wonder whether induction and regu-lation of inflammatory monocytes and neutrophils may differ basedon the transmission status of the infected host.We observed that moribund antibiotic-treated nonsuperspreaders
had lower frequencies of neutrophils in the spleen, potentiallyindicating a belated attempt to control antibiotic-driven inflam-mation. For example, we show that at 7 d after streptomycintreatment, surviving nonsuperspreader hosts have lower levels ofsplenic neutrophils compared with 3 d after streptomycin treat-ment (Fig. S4A). In contrast, there was a sustained increase incolonic neutrophils in all of the antibiotic-treated nonsuper-spreaders (Fig. S4B). We have shown previously that an influx ofsystemic neutrophils is sufficient to suppress Tbet+ CD4 T cells.Consistent with our previous findings, we saw lower frequenciesof TH1 cells in antibiotic-treated nonsuperspreaders (Fig. S5 Aand B). This suppression is inadequate for protection, becausedepletion of CD4 T cells is required to rescue antibiotic-treatednonsuperspreaders from weight loss. The mechanism thatmediates this rescue remains unclear. We observed fewer in-flammatory monocytes and neutrophils in CD4-depleted mice,providing an independent line of evidence that these cells arelinked to the morbidity observed in antibiotic-treated non-superspreaders. However, unlike the neutralization of acute-phase cytokines, we observed increased splenic bacterial loadsin CD4-depleted mice. Although naturally occurring super-spreaders have a blunted CD4 T-cell response, we show here thatCD4-depleted superspreaders continue to be tolerant of antibiotics,suggesting that CD4 T cells are not required for tolerance.
The mice used in our study are siblings and cagemates, po-tentially indicating that intracage microbiota variation does notimpact development of disease-associated tolerance in super-spreaders. A month-long infection with Salmonella Tyhpimuriummay result in differential modulation of the gut microbiota insuperspreaders and nonsuperspreaders, resulting in a super-spreader-specific microbiota that is protective against antibiotictreatment. However, because superspreader and nonsuperspreaderhosts were housed in the same cage before antibiotic treatment,our results suggest that disease-associated tolerance develops in-dependent of cage effects. To confirm that the protective nature ofthe microbiota is not transferrable, we cohoused superspreadersand nonsuperspreaders after antibiotic treatment; however, thiscohousing did not prevent morbidity in the nonsuperspreaderhosts (Fig. S6). It is possible that the components of the micro-biota that mediate tolerance are not transferrable by cohousingand instead require a more direct method of transfer. Becauseuninfected mice treated with neomycin or streptomycin do notdisplay morbidity and have only transient inflammation (21),presence of a pathogen is still required. This finding raises thequestion of whether Salmonella in superspreaders mediates tol-erance. Although we have previously published the finding thatthe Salmonella cultured from superspreaders does not have heri-table differences in virulence compared with nonsuperspreaders(16), there could be nonheritable differences in Salmonellathat mediate tolerance within superspreaders. These transcrip-tional differences could be driven by interactions with a super-spreader-specific microbiota or differential localization withinthe superspreader gut.Some host-adapted pathogens are capable of establishing
longstanding carrier states in specific hosts, which can lead topathogen shedding for extended periods of time. However,the long-term effects on the host remain to be determined. Itis possible that the tolerance to antibiotic-induced inflammationobserved in superspreader hosts could have a deleterious effectin other cases of immune challenge, such as a secondary in-fection or potential induction of autoimmunity. Here we showthat superspreader tolerance is acquired sometime between 4 dand 4 wk after infection. The determination of the host immuneand microbiota effects mediating this tolerance will likely lead tonew modalities of treatment of proinflammatory diseases, suchas inflammatory bowel disease and ulcerative colitis.
Materials and MethodsInfections. The 129 × 1/SvJ (strain 000691) or 129S1/SvImJ (strain 002448) micewere purchased from Jackson Laboratories and infected at 6–8 wk of age.Mice were infected with Salmonella Typhimurium strain SL1344 grownshaking overnight in Luria broth supplemented with streptomycin at a finalconcentration of 100 μg/mL. Bacteria were spun down, washed, and resus-pended in PBS at a concentration of 1010 cfu/mL and 108 cfu in a volume of10 μL fed to mice via pipet tip. Food was removed, and mice were starved16 h before infection. Mice were placed into a fresh cage after infection andantibiotic treatment. Superspreader and nonsuperspreader status was con-firmed by plating fecal pellets on antibiotic-selective plates, and sheddingstatus was determined as described (17). All animal experiments were con-ducted in accordance with the Association for Assessment and Accreditationof Laboratory Animal Care guidelines and approved by the Stanford Uni-versity Institutional Animal Care and Use Committee.
Antibiotic Administration. Mice were oral gavaged with 5 mg of the appro-priate antibiotic suspended in 100 μL of distilled water at either 30 or 4 dafter infection. After antibiotic treatment, mice were moved to fresh cagesand weighed daily by using the Dune electrical balance (Braintree; DCT201).Mice were weighed at the same time of day to control for circadian-relatedvariations in feeding behavior. Typically after antibiotic treatment, micefrom the same group were housed together, with the exception of thecohousing experiment in which three nonsuperspreaders and two super-spreaders mice were placed in a cage together.
15784 | www.pnas.org/cgi/doi/10.1073/pnas.1409968111 Gopinath et al.
Dow
nloa
ded
by g
uest
on
July
27,
202
1

Single Cell Isolation. Single cell solutions were obtained as described (17).Briefly, splenocytes were obtained by grinding spleens between two glassslides, mesenteric lymph nodes were dissociated by using a pestle grinder,and all solutions were passed through a 70-μm strainer. Colonic tissue wasthoroughly cleaned, cut into small pieces, and digested in a RPMI mediumcontaining 10% (vol/vol) fetal calf serum, 0.5% Hepes, 0.1% β-Mercapto-methanol, and 1 mg/mL each of Collagenase A and Trypsin Inhibitor(C9891; T6522; Sigma) and DNase I (Roche; 1010415900).
Fluorescence-Activated Cell Staining. Cells were fixed with paraformaldehyde(Electron Microscopy Sciences; 15710) at a final concentration of 1.6% for10 min at room temperature. Cells were permeabilized with methanol,washed twice with FACS buffer (0.5% BSA, 0.02% sodium azide, and PBS,with a pH of 7.2), and stained with the granulocyte or T-cell panel ofmarkers. The granulocyte panel included CD11b (PE-CF594), Ly6G (FITC),Ly6C (PE), MHC-II (APC), F4/80 (APCCy7), CD11c (PerCPCy5.5), and CD3, B220(PacBlue). The T-cell panel included CD4 (PE-CF594), Tbet (PE), FoxP3(PacBlue), CD11b (APCCy7), CD44 (APC), Gr1 (PECy5.5), and CD19 (FITC). Cellnumbers were obtained by using CountBright beads (Invitrogen; 11570066).
Cytokine Neutralization. Neutralizing antibodies against TNF-α (clone TN3-19.12;BE0244), anti–IL-1β (clone B122; BE0246), and isotype control (hamster poly-clonal IgG; BE0091) were all obtained from Bio-X-Cell. Mice were injectedintraperitoneally with 5 μg of each antibody or 10 μg of the isotype con-trol. Injections were performed daily for streptomycin experiments orevery second day for neomycin experiments for a total of six or seveninjections per experiment.
For CD4 neutralization experiments, mice were injected with 150 μg ofCD4-neutralizing antibody (clone GK1.5; BE00031) or isotype control (RatIgG2b; BE0090) intraperitoneally 1 d before antibiotic treatment and againat days 2 and 4 after antibiotic treatment.
Cytokine Analysis. TNF-α (88-7324), IFN-γ (88-7314), IL-10 (88-7804), and IL-6(88-7064) ELISA kits were purchased from eBiosciences. IL-1β (DY401) andIL-1 receptor agonist (DY408) kits were purchased from R&D Systems. Serum
was obtained via cardiac puncture, and intestinal wash was obtained byflushing 1 mL of phospho-buffered saline containing protease inhibitor(Roche; 05892953001) through the length of the intestine over a 70-μmcell strainer.
Histology. Tissues evaluated histologically were fixed in 10% buffered neutralformalin and routinely processed for paraffin embedding and stained withhematoxylin and eosin. A semiquantitative scoring system of 0 to +6, (0 = nosignificant lesion, +1 =minimal, +2 =mild, +3 =moderate, +4 =marked, +5 =severe, and +6 = massive) was used to evaluate the severity of pathologicalchanges in the ceca of infected mice including inflammation, edema,ulceration, and necrosis. The distribution (focal, multifocal, regionallyextensive, or diffuse) and location (i.e., limited to lamina propria, laminapropria + submucosa, or transmural, through all layers of the cecal wall)of pathology was also noted in addition to assigning severity scores.
Proteomics. Protein was extracted from fecal pellets, digested with trypsin,and analyzed by liquid chromatography tandem mass spectrometry as de-scribed (29). Two fractions from the C4 chromatography (40% and 60%acetonitrile) were analyzed, and no technical replicates were collected. Datawere filtered to a 1% peptide false discovery rate (FDR) and 5% protein FDRby using in-house software (30). Acute-phase response proteins were iden-tified through the use of IPA (Ingenuity Systems), and Spearmann correla-tions were calculated in Prism 6.
Statistics. Significance was calculated by using the Mann–Whitney U two-tailed test unless otherwise mentioned.
ACKNOWLEDGMENTS. We thank Dr. David Schneider for several thought-provoking conversations on tolerance and Katherine Ng for her insightand help with experiments. S.G. was supported by National Institutes ofHealth Grant R01 A1095396. This work was supported by a Burroughs Well-come Fund Investigator in the Pathogenesis of Infectious Diseases award(to D.M.M.).
1. Woolhouse ME, et al. (1997) Heterogeneities in the transmission of infectious agents:Implications for the design of control programs. Proc Natl Acad Sci USA 94(1):338–342.
2. Chase-Topping ME, et al. (2007) Risk factors for the presence of high-level shedders ofEscherichia coli O157 on Scottish farms. J Clin Microbiol 45(5):1594–1603.
3. Chase-Topping M, Gally D, Low C, Matthews L, Woolhouse M (2008) Super-sheddingand the link between human infection and livestock carriage of Escherichia coli O157.Nat Rev Microbiol 6(12):904–912.
4. Matthews L, et al. (2006) Heterogeneous shedding of Escherichia coli O157 in cattleand its implications for control. Proc Natl Acad Sci USA 103(3):547–552.
5. Matthews L, et al. (2009) Exploiting strain diversity to expose transmission hetero-geneities and predict the impact of targeting supershedding. Epidemics 1(4):221–229.
6. Lloyd-Smith JO, Schreiber SJ, Kopp PE, Getz WM (2005) Superspreading and the effectof individual variation on disease emergence. Nature 438(7066):355–359.
7. Courtenay O, Quinnell RJ, Garcez LM, Shaw JJ, Dye C (2002) Infectiousness in a cohortof brazilian dogs: Why culling fails to control visceral leishmaniasis in areas of hightransmission. J Infect Dis 186(9):1314–1320.
8. Galvani AP, May RM (2005) Epidemiology: Dimensions of superspreading. Nature438(7066):293–295.
9. Schneider DS, Ayres JS (2008) Two ways to survive infection: What resistance andtolerance can teach us about treating infectious diseases. Nat Rev Immunol 8(11):889–895.
10. Ayres JS, Schneider DS (2012) Tolerance of infections. Annu Rev Immunol 30:271–294.11. Medzhitov R, Schneider DS, Soares MP (2012) Disease tolerance as a defense strategy.
Science 335(6071):936–941.12. Boots M (2008) Fight or learn to live with the consequences? Trends Ecol Evol 23(5):
248–250.13. Vale PF, Fenton A, Brown SP (2014) Limiting damage during infection: Lessons from
infection tolerance for novel therapeutics. PLoS Biol 12(1):e1001769.14. Råberg L, Sim D, Read AF (2007) Disentangling genetic variation for resistance and
tolerance to infectious diseases in animals. Science 318(5851):812–814.15. Råberg L, Graham AL, Read AF (2009) Decomposing health: Tolerance and resistance
to parasites in animals. Philos Trans R Soc Lond B Biol Sci 364(1513):37–49.16. Lawley TD, et al. (2008) Host transmission of Salmonella enterica serovar Typhimurium is
controlled by virulence factors and indigenous intestinal microbiota. Infect Immun 76(1):403–416.
17. Gopinath S, Hotson A, Johns J, Nolan G, Monack D (2013) The systemic immune stateof super-shedder mice is characterized by a unique neutrophil-dependent blunting ofTH1 responses. PLoS Pathog 9(6):e1003408.
18. Stecher B, et al. (2006) Chronic Salmonella enterica serovar Typhimurium-inducedcolitis and cholangitis in streptomycin-pretreated Nramp1+/+ mice. Infect Immun74(9):5047–5057.
19. Barthel M, et al. (2003) Pretreatment of mice with streptomycin provides a Salmonellaenterica serovar Typhimurium colitis model that allows analysis of both pathogen andhost. Infect Immun 71(5):2839–2858.
20. Cho I, et al. (2012) Antibiotics in early life alter the murine colonic microbiome andadiposity. Nature 488(7413):621–626.
21. Spees AM, et al. (2013) Streptomycin-induced inflammation enhances Escherichia coligut colonization through nitrate respiration. mBio 4:e00430–13.
22. Mazlam MZ, Hodgson HJ (1992) Peripheral blood monocyte cytokine production andacute phase response in inflammatory bowel disease. Gut 33(6):773–778.
23. Cho JS, et al. (2012) Neutrophil-derived IL-1β is sufficient for abscess formation inimmunity against Staphylococcus aureus in mice. PLoS Pathog 8(11):e1003047.
24. Bessede A, et al. (2014) Aryl hydrocarbon receptor control of a disease tolerancedefence pathway. Nature 511(7508):184–190.
25. Ayres JS, Freitag N, Schneider DS (2008) Identification of Drosophila mutants alteringdefense of and endurance to Listeria monocytogenes infection. Genetics 178(3):1807–1815.
26. Jamieson AM, et al. (2013) Role of tissue protection in lethal respiratory viral-bacterialcoinfection. Science 340(6137):1230–1234.
27. Arend WP, Malyak M, Guthridge CJ, Gabay C (1998) Interleukin-1 receptor antago-nist: Role in biology. Annu Rev Immunol 16:27–55.
28. Tam JW, Kullas AL, Mena P, Bliska JB, van der Velden AWM (2014) CD11b+ Ly6ChiLy6G- immature myeloid cells recruited in response to Salmonella enterica serovarTyphimurium infection exhibit protective and immunosuppressive properties.Infect Immun 82(6):2606–2614.
29. Lichtman JS, Marcobal A, Sonnenburg JL, Elias JE (2013) Host-centric proteomics ofStool: a novel strategy focused on intestinal responses to the gut microbiota. Mol CellProteomics 12:3310–3318.
30. Huttlin EL, et al. (2010) A tissue-specific atlas of mouse protein phosphorylation andexpression. Cell 143:1174–1189.
Gopinath et al. PNAS | November 4, 2014 | vol. 111 | no. 44 | 15785
IMMUNOLO
GYAND
INFLAMMATION
Dow
nloa
ded
by g
uest
on
July
27,
202
1