Rohan R. Walvekar
9
1 UCSF Salivary Endoscopy Course 2014 Basic Set Up and Instruments Rohan R. Walvekar, MD Department of Otolaryngology & Head Neck Surgery Louisiana State University Health Sciences Center New Orleans, LA Disclosure I have the following relationship(s) with commercial interests. Hood Laboratories *Walvekar Salivary Stent Cook Industries Medtronic Xome A commercial interest is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients. Instruments for Exposure of the Oral Cavity Anesthesia – Nasal Intubation is preferred Epistaxis • Pre-op nasal endoscopy to document spurs, deviated septum or other abnormality • Afrin and lubricated nasal trumpet while patient is in preoperative holding area Disposable Plastic cheek retractor Dental splints Jennings's mouth gag Minnesota and Sweetheart retractors Basic Sialendoscopy Set Dilator System Marchal Dilator System Probes No.0000 to No.8 Schaitkin’s Fluted Dilators \ No.0 – 5 Conical Dilator Helps to transition between dilators Useful usually once papilla is dilated up to Marchal No.1 or 2 dilator Bougies (increasing diameter) Compatible with 0.4 mm guide wire COOK Dilator System with Operating Sheath Guide Wire Cook Dilators 1-8 Basic Sialendoscopy Set
Transcript of Rohan R. Walvekar

1
UCSF Salivary Endoscopy Course 2014
Basic Set Up and Instruments
Rohan R. Walvekar, MD
Department of Otolaryngology & Head Neck Surgery
Louisiana State University Health Sciences Center
New Orleans, LA
DisclosureI have the following relationship(s) with commercial interests.
Hood Laboratories *Walvekar Salivary Stent
Cook Industries
Medtronic Xome
A commercial interest is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients.
� Instruments for Exposure of the Oral Cavity� Anesthesia – Nasal Intubation is preferred
� Epistaxis• Pre-op nasal endoscopy to document spurs,
deviated septum or other abnormality• Afrin and lubricated nasal trumpet while
patient is in preoperative holding area � Disposable Plastic cheek retractor� Dental splints � Jennings's mouth gag � Minnesota and Sweetheart
retractors
Basic Sialendoscopy Set
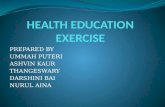
� Dilator System � Marchal Dilator System
� Probes No.0000 to No.8� Schaitkin’s Fluted Dilators \
� No.0 – 5� Conical Dilator � Helps to transition between dilators� Useful usually once papilla is dilated up to Marchal
No.1 or 2 dilator� Bougies (increasing diameter)
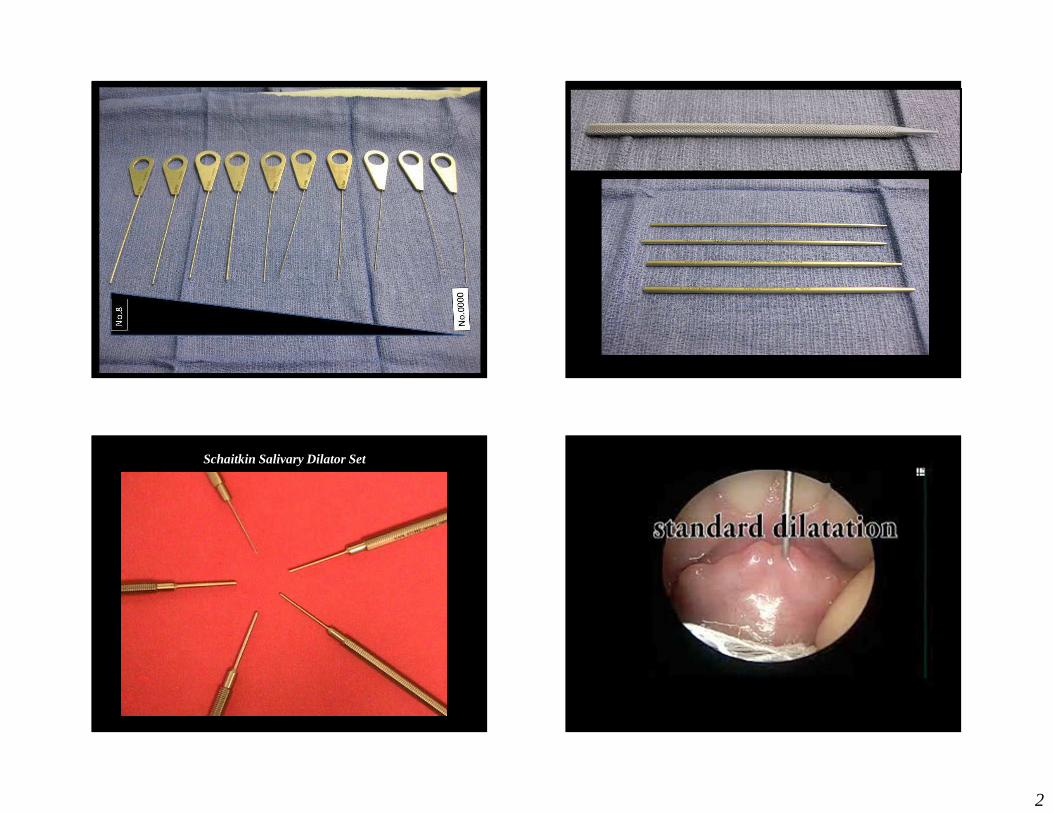
� Compatible with 0.4 mm guide wire� COOK Dilator System with Operating Sheath
� Guide Wire � Cook Dilators 1-8
Basic Sialendoscopy Set
2
Schaitkin Salivary Dilator Set
3
Sialendoscopy
Kolenda Introducer Set (COOK)
Sialendoscopy
Sialendoscopy
Sialendoscopes
Geisthoff UW. Basic sialendoscopy techniques. Otolaryngol Clin N Am 42 (2009) 1029-1052
� 1.3 mm Marchal*
� 1.1 mm Erlangen*
� 1.6 mm Erlangen*
*Karl Storz, Tuttlingen, Germany
Fiberoptic channel Irrigation Port
Interventional Port
4
� Fifth generation endoscopes
� Original was flexible
� 1.3 mm semi rigid scope with 6000 pixels, 0.25mm rinsing channel and 0.65mm working channel
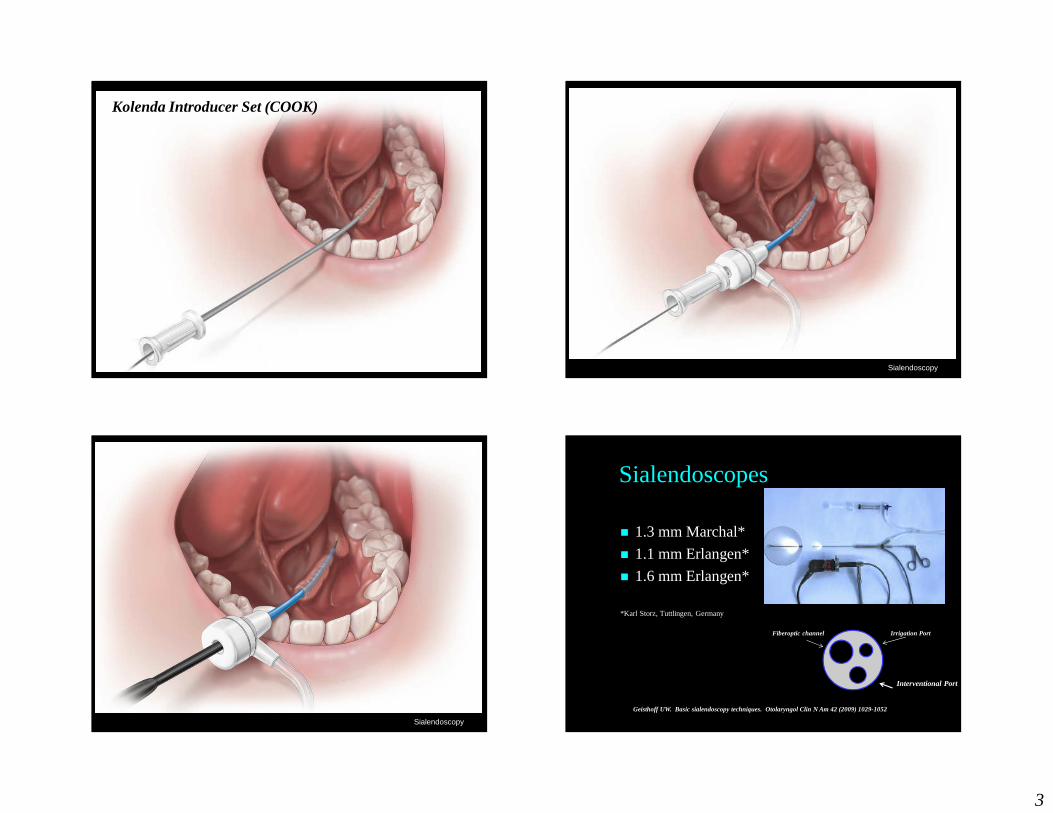
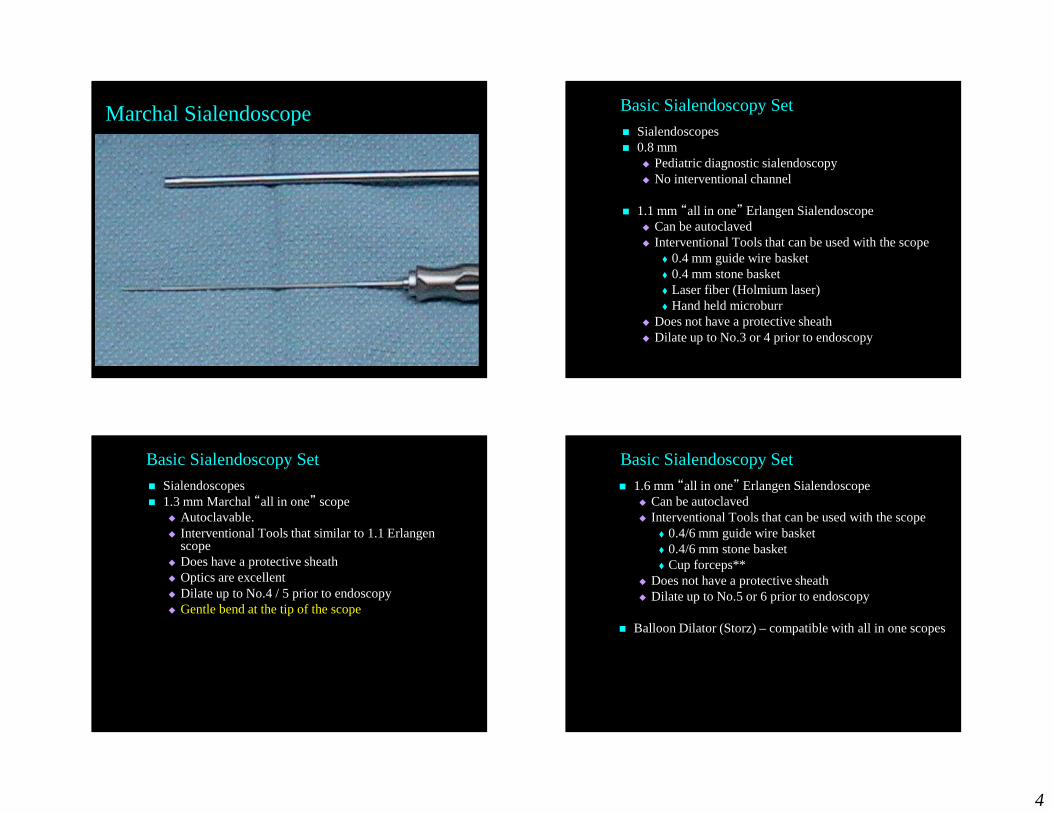
Marchal Sialendoscope� Sialendoscopes� 0.8 mm
� Pediatric diagnostic sialendoscopy� No interventional channel
� 1.1 mm “all in one” Erlangen Sialendoscope� Can be autoclaved� Interventional Tools that can be used with the scope
� 0.4 mm guide wire basket� 0.4 mm stone basket � Laser fiber (Holmium laser)� Hand held microburr
� Does not have a protective sheath� Dilate up to No.3 or 4 prior to endoscopy
Basic Sialendoscopy Set
� Sialendoscopes� 1.3 mm Marchal “all in one” scope
� Autoclavable. � Interventional Tools that similar to 1.1 Erlangen
scope� Does have a protective sheath� Optics are excellent� Dilate up to No.4 / 5 prior to endoscopy� Gentle bend at the tip of the scope
Basic Sialendoscopy Set
� 1.6 mm “all in one” Erlangen Sialendoscope� Can be autoclaved� Interventional Tools that can be used with the scope
� 0.4/6 mm guide wire basket� 0.4/6 mm stone basket � Cup forceps**
� Does not have a protective sheath� Dilate up to No.5 or 6 prior to endoscopy
� Balloon Dilator (Storz) – compatible with all in one scopes
Basic Sialendoscopy Set

5
Sialendoscopy
� IV Extension Tubing� 20 cc syringe � Vessel loops� Angled Forces with and without teeth� Standard Endoscopy Tower and Monitor with recording
capabilities**Accessories� Disposables
� Stone baskets� Guide wires� Cleaning brushes� Stents (Hood Laboratories)*� Balloon Dilator
� Not Disposable� Hand-held micro burr� Stone forceps
Basic Sialendoscopy Set
Three way stopcock/valve
STORZ WIRE BASKETS COOK WIRE BASKETS - - N Gage
6
LSU Sialendoscopy Course
Diagnostic Sialendoscopy
Rohan R. Walvekar, MD
Department of Otolaryngology & Head Neck Surgery
Louisiana State University Health Sciences Center
New Orleans, LA
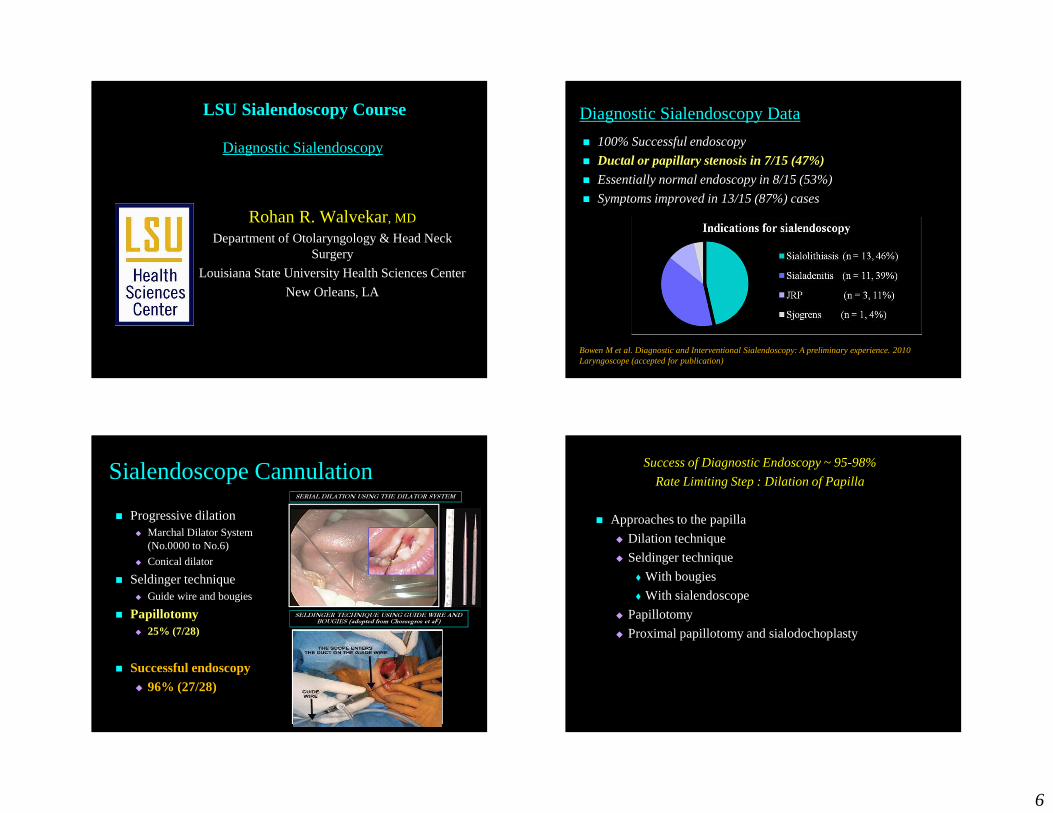
� 100% Successful endoscopy
� Ductal or papillary stenosis in 7/15 (47%)
� Essentially normal endoscopy in 8/15 (53%)
� Symptoms improved in 13/15 (87%) cases
Diagnostic Sialendoscopy Data
Bowen M et al. Diagnostic and Interventional Sialendoscopy: A preliminary experience. 2010 Laryngoscope (accepted for publication)
� Progressive dilation� Marchal Dilator System
(No.0000 to No.6)
� Conical dilator
� Seldinger technique� Guide wire and bougies
� Papillotomy� 25% (7/28)
� Successful endoscopy� 96% (27/28)
Sialendoscope CannulationSERIAL DILATION USING THE DILATOR SYSTEM
SELDINGER TECHNIQUE USING GUIDE WIRE AND BOUGIES (adopted from Chossegros et al2)
Success of Diagnostic Endoscopy ~ 95-98%
Rate Limiting Step : Dilation of Papilla
� Approaches to the papilla
� Dilation technique
� Seldinger technique
� With bougies
� With sialendoscope
� Papillotomy
� Proximal papillotomy and sialodochoplasty
7
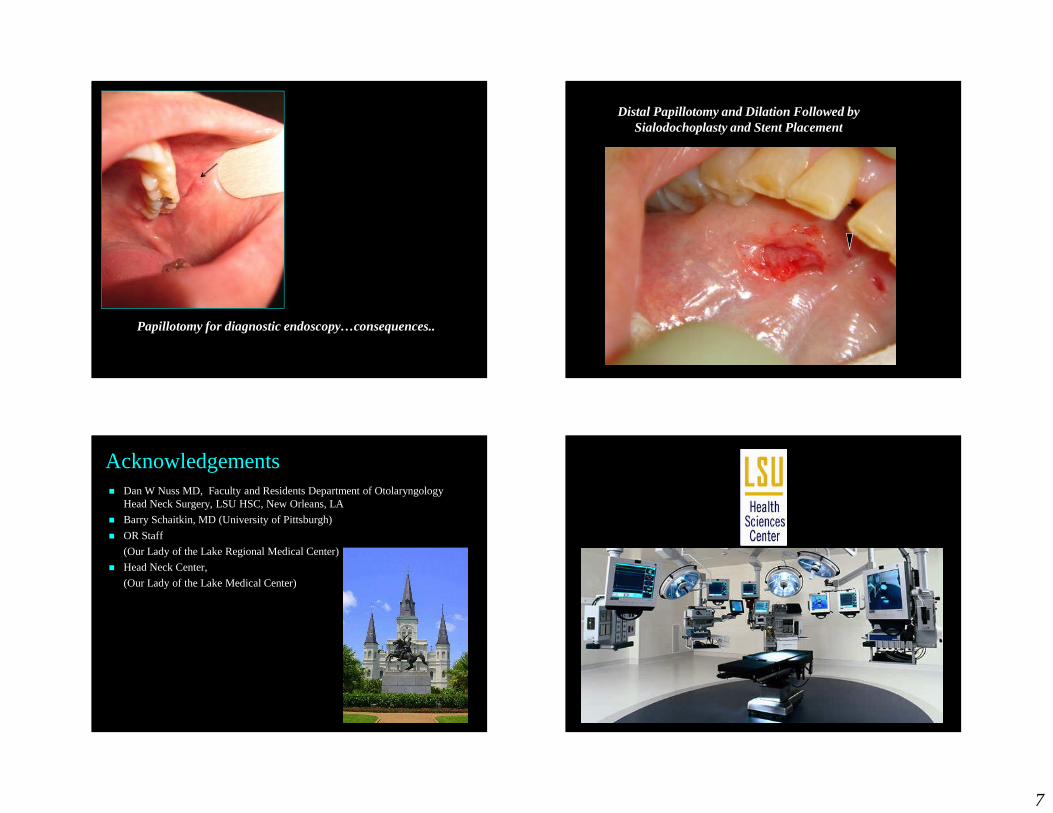
Papillotomy for diagnostic endoscopy…consequences..
Distal Papillotomy and Dilation Followed by Sialodochoplasty and Stent Placement
Acknowledgements� Dan W Nuss MD, Faculty and Residents Department of Otolaryngology
Head Neck Surgery, LSU HSC, New Orleans, LA
� Barry Schaitkin, MD (University of Pittsburgh)
� OR Staff
(Our Lady of the Lake Regional Medical Center)
� Head Neck Center,
(Our Lady of the Lake Medical Center)
8
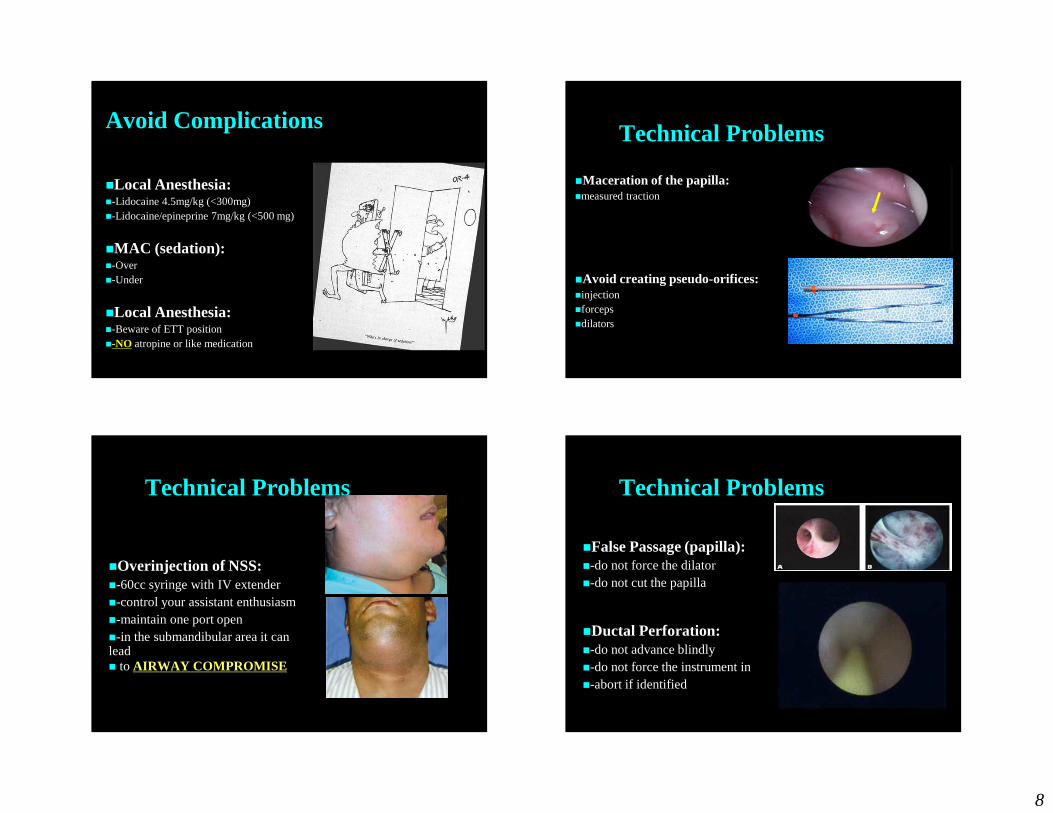
Avoid Complications
�Local Anesthesia:�-Lidocaine 4.5mg/kg (<300mg)�-Lidocaine/epineprine 7mg/kg (<500 mg)
�MAC (sedation):�-Over�-Under
�Local Anesthesia:�-Beware of ETT position�-NO atropine or like medication
Technical Problems
�Maceration of the papilla:�measured traction
�Avoid creating pseudo-orifices:�injection�forceps�dilators
Technical Problems
�Overinjection of NSS:�-60cc syringe with IV extender�-control your assistant enthusiasm�-maintain one port open�-in the submandibular area it can lead � to AIRWAY COMPROMISE
Technical Problems
�False Passage (papilla):�-do not force the dilator�-do not cut the papilla
�Ductal Perforation:�-do not advance blindly�-do not force the instrument in�-abort if identified

9
Equipment Failure
�Be cognizant of the turns:�-scope is semi-rigid (it is fragile) �-straighten the duct using manual traction
and pressure
�Be cognizant of the teeth
�Have back up gear
The Learning Curve


















