Robert J. Walters, Senior Assistant Attorney General ... · Robert J. Walters, Senior Assistant...
91
Robert J. Walters, Senior Assistant Attorney General Wyoming Attorney General’s Office June 5, 2014
Transcript of Robert J. Walters, Senior Assistant Attorney General ... · Robert J. Walters, Senior Assistant...
Robert J. Walters, Senior Assistant Attorney General Wyoming Attorney General’s Office
June 5, 2014

Introduction
:
Introduction
:
The prescription drug abuser, or drug seeker, represents a serious and constant problem for the health care professional in the United States.
These people, through a variety of methods, are successful in obtaining an enormous amount of pharmaceutical drugs from health care professionals. These drugs then perpetuate personal addictions, or provide a very valuable product to the prescription drug trafficker.

Introduction
the health care professional is a nurse?

Introduction
THE FACTS • Reliable statistics on the prevalence of drug diversion
by nurses ARE NOT available • By its nature, drug diversion is a clandestine activity • Methods in place in many hospitals, facilities and
institutions leave cases undiscovered or unreported • Drug diversion by health care providers, including
nurses, is universal among hospitals, facilities and institutions in the United States
Introduction
Drug diversion may actually be under-reported.
: Presentation: “Health Facility Drug Diversion: Essential Compliance & Auditing Measures,” by Kimberly S. New JD BSN RN, and Kelly C. Loya CPC-I, CHC, CPhT, CRMA
• Fear of negative publicity • Fear of State and Federal agency involvement • Uncertainty about reporting requirements and avenues • Justification that terminating the employee is enough • Possible inadequate investigative systems in place

Introduction
Consequences When Diverter is dismissed/employment terminated or allowed to quit: • May disregard the well being of the diverter • Opportunity for rehabilitation may be precluded • Potential violation of laws and regulations • No reported history will bypass preventive screening at next employer : Presentation: “Health Facility Drug Diversion: Essential
Compliance & Auditing Measures,” by Kimberly S. New JD BSN RN, and Kelly C. Loya CPC-I, CHC, CPhT, CRMA
Introduction
Are drug diversion cases complicated?

Introduction
Can drug diversion cases look more like medication error and/or documentation
substandard practice cases?

Introduction

Introduction
Is it easy to PROCRASTINATE in drug diversion cases?

Introduction
Is it ever too early to develop a STRATEGY in drug diversion cases?

BASIC RULE:
NOTICE AND OPPORTUNITY TO BE
HEARD
DUE PROCESS 101

Due Process 101
indicating the charges or GROUNDS FOR DISCIPLINE upon which proposed disciplinary action will be based
The Wyoming Administrative Procedure Act describes the notice requirement as follows: No revocation, suspension, annulment or withdrawal of any license is lawful unless, prior to the institution of agency proceedings, the agency gave notice by mail to the licensee of facts or conduct which warrant the intended action, and the licensee was given an opportunity to show compliance with all lawful requirements for the retention of the license. Wyo. Stat. Ann. § 16-3-113(c).

Due Process 101
CONTESTED CASE HEARING

Due Process 101
Music to a drug diverter’s ears They think they are covered or that you can’t prove he/she diverted
Due Process 101
Accused nurse has the legal right for opportunity to dispute the charges of diversion

Due Process 101
Usually not going to catch nurse with his/her “hand in the cookie jar”

Due Process 101
Nurses oftentimes will deny diversion or any role in any suspected drug diversion

Due Process 101
“I think you’d be surprised the lengths a drug addict will go to keep it a secret.” Nurse Jackie, “Lost Girls,” Season 5 (2013).

Due Process 101
Going to need strong or solid EVIDENCE of
diversion

BURDEN OF PROOF
DUE PROCESS 101 -- EVIDENCE

Due Process 101 -- Evidence
Due Process 101 -- Evidence

Due Process 101 -- Evidence
or what are the ELEMENTS that must be proven?
FRAMES NOT ONLY WHAT EVIDENCE MUST BE PRESENTED AT A HEARING BUT WHAT EVIDENCE ALSO
MUST BE OBTAINED IN INVESTIGATION!

Due Process 101 -- Evidence
“Drug Diversion” Defined
Diverting (or taking/removal of) a prescription drug for other than its intended purpose.
Theft of medication, including “waste,” from patients or health care facilities for personal use.
Wyo. Stat. Ann. § 33-21-146(a)(v): “Has engaged in any unauthorized possession or unauthorized use of a controlled substance as defined in the Wyoming Controlled Substances Act[.]”

Due Process 101 -- Evidence
“Misappropriation” Defined
Negligently or deliberately taking, misusing, exploiting, using or selling property belonging
to another, whether temporarily or permanently, and without regard to consent.

Due Process 101 -- Evidence
Emergency/Summary Suspension vs. Hearing on the Merits
� Elements of the underlying ground(s) (e.g., drug diversion, misappropriation, theft)
� Substantial likelihood of prevailing at hearing on merits
� Nurse presents a clear and immediate danger to public health and safety if permitted to practice.
� Elements of the underlying ground(s) (e.g., drug diversion, misappropriation, theft)
� Clear and convincing evidence standard
� Sanction imposed by Board is not arbitrary or capricious (i.e., reasonable under circumstances considering mitigating and aggravating factors)

Case Digest
Tale of Two Cases

Case Digest Administrative complaint alleged: Ø According to Pyxis reports, nurse (LPN) removed twenty-six (26) Fentanyl patches over the course of three (3) months that were unaccounted for or not signed out on a resident Medication Administration Report (“MAR”). Ø Fentanyl patches were pulled day after day or on days that they were not due to be changed. Ø Three (3) instances where nurse refilled the Pyxis machine with Fentanyl patches and only refilled nine (9), which left one patch unaccounted for each time refills occurred. Ø Greater administration of Percocet and Vicodin when nurse was working, indicating a pattern in which five (5) residents were receiving multiple doses of PRN narcotics and in which corresponding documentation of administration was not reflected on the MAR or the pain tracking sheet.

Case Digest Initial recommendation by Disciplinary Committee: Ø Reprimand for unsafe practice – i.e., medication errors, lack of appropriate documentation (even though suspicious for drug diversion) Ø Remedial training in medication errors and documentation
Nurse was sent a proposed settlement agreement (consent decree) for reprimand and training, which she “happily” executed.
Board DID NOT approve proposed settlement agreement (consent decree) for reprimand and training, and suggested some level of supervision (worksite monitor for an appropriate period with reporting).

Case Digest
In preparation for hearing, became more evident that drug diversion ACTUALLY could be proven.
Nurse retained counsel who communicated dispute of alternative recommendation and requested a hearing.

Case Digest
FACILITY’S INTERNAL AUDIT (data of three-month period from Pyxis reports and corresponding medical records) reflected: Ø NUMEROUS incidents of single nurse REMOVAL of significant quantities Vicodin, Norco, Percocet, and Fentanyl, related to several patients, and Ø VAST MAJORITY (approximately 85%) in which ADMINISTRATION NOT DOCUMENTED, and Ø NO JUSTIFICATION for removal and lack of appropriate care (assessment/reassessment) and failure to document.
Case Digest
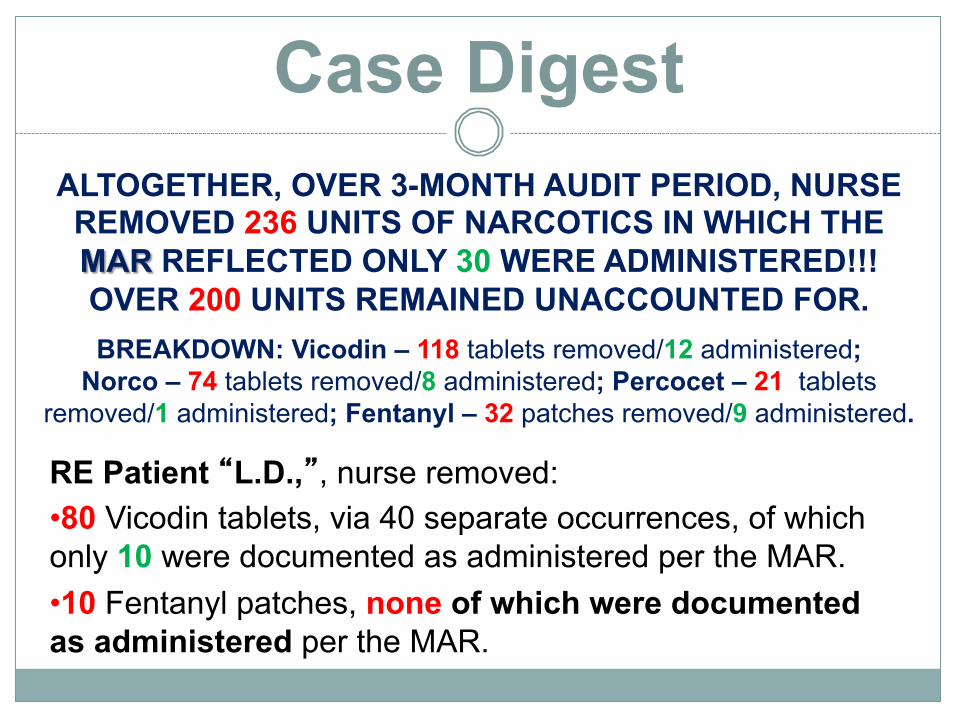
RE Patient “L.D.,”, nurse removed: • 80 Vicodin tablets, via 40 separate occurrences, of which only 10 were documented as administered per the MAR. • 10 Fentanyl patches, none of which were documented as administered per the MAR.
ALTOGETHER, OVER 3-MONTH AUDIT PERIOD, NURSE REMOVED 236 UNITS OF NARCOTICS IN WHICH THE MAR REFLECTED ONLY 30 WERE ADMINISTERED!!! OVER 200 UNITS REMAINED UNACCOUNTED FOR. BREAKDOWN: Vicodin – 118 tablets removed/12 administered;
Norco – 74 tablets removed/8 administered; Percocet – 21 tablets removed/1 administered; Fentanyl – 32 patches removed/9 administered.

Case Digest RE Patient “D.L.,”, nurse : • Removed 21 Fentanyl patches, and ONLY 9 were documented as administered per the MAR. • Removed 8 Percocet tablets and ONLY 4 were documented as administered per the MAR. • Refilled/Inventoried 9 Fentanyl patches (one missing)
RE Patient “W.R.,”, nurse : • Removed 19 Vicodin tablets and ONLY 2 were documented as administered per the MAR. • Removed 8 Norco tablets and ONLY 2 were documented as administered per the MAR.

Case Digest RE Patient “T.R.,”, nurse : • Removed 9 Vicodin tablets and none of which were documented as administered per the MAR. • MAR reflected that Vicodin was not a prescribed medication for this patient. • Removed 12 Norco tablets and ONLY 1 was documented as administered per the MAR. • Removed 8 Ambien tablets and none of which were documented as administered per the MAR. • MAR reflected that Ambien was not a prescribed medication for this patient.

Case Digest RE Patient “D.S.,”, nurse : • Removed 54 Norco tablets and ONLY 5 were documented as administered per the MAR.
RE Patient “A.K.,”, nurse : • Removed 1 Fentanyl patch, which was not documented as administered per the MAR. • This patient no longer at facility when patch removed.
RE Patient “C.T.,”, nurse : • Removed 4 Percocet tablets, none of which were documented as administered per the MAR. • This patient was not assigned to nurse.
Case Digest RE Patient “R.K.,”, nurse : • Refilled/Inventoried 9 Fentanyl patches (one missing)
RE Patient “D.C.,”, nurse : • Refilled/Inventoried 9 Fentanyl patches (one missing)
Case Digest As part of disclosure requirements, and about two weeks prior to hearing, communicated with nurse’s attorney regarding evidence to be presented and strength of case. Suggested that nurse consider a voluntary surrender in lieu of hearing.
Nurse agreed to voluntary surrender and Board approved a settlement agreement (consent decree) for voluntary surrender.




WHAT was diverted?
WHAT do we know (or need to know) about the diverter?
WHAT are the potential explanations (or defenses) to accusations?
WHAT systems were in place (are there issues regarding reliability)?

HOW was the situation discovered?
HOW did the suspected diversion occur?
HOW often were substances diverted – i.e., was there a pattern?
HOW were patients impacted?

HOW extensive was investigation by hospital, facility or institution? HOW many other nurses or persons were considered or investigated?

WAS suspected employee interviewed to explain discrepancy (and what was explanation)?
WAS suspected employee drug tested?
WAS suspected employee suspended or terminated?

What was diverted?
Most Commonly Diverted Controlled Substances
v Hydrocodone v Oxycodone v Hydromorphone v Morphine Sulfate v Fentanyl v Alprazolam v Diazepam

What do we know about the diverter?
of a “Drug Diverter”
• High achiever or Model Nurse
• “Team Player”
• The last person you would suspect

of a “Drug Diverter”
• Medication removed on the controlled substances sign-out sheets but not transferred to or charted as administered on patients’ medical records • Charts more controlled substances than other nurses • Noticeable increase of PRN or “as needed” controlled substances charted • Charts out larger doses of controlled substances than ordered when the appropriate dose is available
What do we know about the diverter?
(Possible red flags)

of a “Drug Diverter”
• Excessive amounts of time spent near a drug supply, such as a cart or medicine room • Waits for other staff to leave controlled substances unit before accessing medications • Frequently checks supply of controlled substances • Preoccupied with medications • “Disappears” at work (e.g., takes break or visits restroom especially after accessing controlled substances)
What do we know about the diverter?
(Possible red flags)

of a “Drug Diverter”
• “Forgetfulness” in routine duties, including decline in documentation • Record keeping is sloppy -- some records falsification is possible with drug shortages • Changes evident in handwriting and charting • Frequent overrides in automated dispensing systems (ADS) • Frequently accessing the ADS after coworker fails to log off the system • Heavy “wastage” of drugs
What do we know about the diverter?
(Possible red flags)
of a “Drug Diverter”
• Makes unusual comments about usage/ disposal of controlled substances • Defensive responses when questioned about errors or poor patient care • Asks coworkers for their user lD and password • Asks coworker to sign for opioid wastage without actually witnessing it • Asks for help accessing controlled substances • Seen accessing ADS while off duty
What do we know about the diverter?
(Possible red flags)

of a “Drug Diverter”
• Night shift • Critical care or other unit where nursing staff have increased autonomy • Volunteers for overtime, weekend or extra shifts • Willingly “floats” to other units • Works on a job lower than his/her educational level
What do we know about the diverter?
(Possible red flags)

of a “Drug Diverter”
• Patients and staff make complaints about the co-worker’s attitude or behavior • Significant stress in personal life • Frequent hospitalization or accidents • Personal history of being on pain medications • Legitimate prescription for drug being diverted • Wears long sleeves in appropriately, such as in very hot weather • Slight hand tremors • Pupillary size change and/or bloodshot eyes
What do we know about the diverter?
(Possible red flags)

What are the potential explanations/defenses) to accusations?

10. Prejudice or bias by management or other coworkers
9. The Pyxis machine or ADS malfunctioned 8. Someone else had access to the Pyxis
machine and used my access information 7. Mistakenly administered to another patient
and did not (or forgot to) document/chart 6. Administered the medication but did not/
forgot to chart
What are the potential explanations/defenses) to accusations?

5. Chart portions missing or altered by someone else
4. Someone else did it 3. Occurrence report filed but disappeared 2. I have no motive because I already
receive prescribed medication for pain
What are the potential explanations/defenses) to accusations? I JUST DIDN’T DO IT!

Methods of Diversion Removal from secure storage areas without any documentation
Removal from storage area and falsification of an order for administration
Removal and substitution in administration or wasting
• Substitution of look-alike pills • Saline substituted for injectable medication • Potential for tampering
How did the suspected diversion occur?

Methods of Diversion Removal of medication without order • Medication override • Falsification of “verbal order”
Removal of medication when not needed • Often initial method of diversion • Very difficult to detect • Falsification of records • Medication errors • No documentation of administration
How did the suspected diversion occur?

Methods of Diversion Removal for discharged patient
Removal of duplicate dose • May not be assigned to care for patient
Removal under sign-on of colleague • Stolen password • Left alone when colleague is signed in
Removal and use from inconspicuous vessel
How did the suspected diversion occur?

Methods of Diversion Removal of/diversion from fentanyl patches
• Removal of gel with syringe and needle • Keeping new patch for self and putting used
patch on patient
Removal from PCA and drip lines
Removal of unspent syringes from sharps containers
• Nurse steals sharps containers and removes syringes to collect remnants of syringes
How did the suspected diversion occur?

Methods of Diversion Failure to waste (properly)
• Claims he/she was too busy or others unavailable to have a wasted dose witnessed
• Unwasted medication kept for self • Waste thrown into the general trash and later
picked up by the diverter
Frequent wasting of entire doses (should be returned)
Falsification of wastage record (to show a drug was wasted, but may have wasted water)
How did the suspected diversion occur?

Methods of Diversion Charting of administration but patient was not given quantity documented
Pilfering patient medications brought from home
Nurse places drugs in coat, purse or car
How did the suspected diversion occur?

Patient indications that drugs have been diverted
• Patient who had been well controlled with pain medication has marked change and increasingly states pain is poorly controlled or exhibits signs of increased pain.
• Response to pain medication varies with different caregivers.
• Request for prescription refills are made with increasing frequency.
How were patients impacted?

Patient indications that drugs have been diverted
• Appearance of drugs (pills, capsules) has changed (indicating they may have been replaced with non-opioid drugs).
• Patient may show signs of neglect (poor hygiene, pressure sores, weight loss).
• Patient may exhibit fear or anxiety, especially in the presence of a suspect caregiver.
How were patients impacted?

Preparation of Drug Diversion Cases

Preparation of Drug Diversion Cases

Preparation of Drug Diversion Cases
Can a PATTERN of drug diversion by subject nurse be demonstrated? v Is supporting evidence sufficient? v What are possible explanations or counter-indications? v Is the nurse’s “side of the story credible” – can it be rebutted? v Is there a smoking gun?

Preparation of Drug Diversion Cases
How strong is your

Preparation of Drug Diversion Cases
Preparation for Drug Diversion Cases
Evidence Needed (MINIMUM)
• Automated system audit (e.g., Pyxis report of removal of substances by suspected employee over meaningful period of time) • Corresponding patient medical records (reflecting orders, charting of pain assessments, medication administration, etc.) • Medication Administration Record (MARS) or Daily Medication Log (DML) • Chart audits comparing physician’s orders, MARS or DML, nurse’s notes & Pyxis reports (to determine if there is a discrepancy from audits to show drug diversion – especially if there is a clear pattern)

Preparation for Drug Diversion Cases
OTHER IMPORTANT EVIDENCE • Copy of hospital’s or facility’s internal investigation documents • Patient complaints and survey results relating to pain management • Drug test (if done and particularly if positive for substance(s) diverted) • Personnel disciplinary action (particularly if issues re substance abuse or past medication errors or failure to document) • Prescription Drug Monitoring Program (PDMP) report/prescription profile (particularly if the profile indicates a substance use disorder) • Medical records of subject (particularly if being treated for chronic pain – pain management contract; noncompliant drug tests) • Employee time records

Preparation for Drug Diversion Cases
OTHER IMPORTANT EVIDENCE • Testimony of pharmacist, DON/CNO or other head of facility/hospital, prescribing physicians, or other witnesses (persons most knowledgeable – possibly also for rebuttal purposes) • Testimony of other nurses (possibly also for rebuttal purposes) • Law enforcement investigative reports (if available) • Disciplinary action by another state BON or other licensing authority – especially if substance abuse issue or suspicion of or actual diversion (inference of past behavior indicating present – goes more to recommendation for disciplinary sanction)

Preparation for Drug Diversion Cases
OTHER IMPORTANT EVIDENCE • Testimony of nurse (possible credibility issues) • Psychological and /or treatment records of nurse (e.g., substance abuse evaluations, discharge summaries from treatment facilities -- particularly if information reveals admissions to diversion) • Employment records of nurse from former employment (particularly if reveal personnel action related to actual or suspected diversion of controlled substances, or indications of substance use disorder) • Documentation of occurrences since facility investigation completed • Testimony/statements from patients (if available and strong recollection of Rx nonadministration)

Preparation for Drug Diversion Cases
What to look for in Chart/Pyxis Audits:
• Frequent removal by override in Pyxis • Withdrawal then cancels action in Pyxis • Appropriate documentation of wasting or lack of documentation • Waste and frequency of waste • Waste without witness • Frequency of medication and amount • Correlation of removal activity with documentation • Physician orders match medication administration to patient • Documentation of pain assessment and control or failure to control pain despite continued administration of medication • Date and time of medication administration comparison to MAR and nurse’s notes may vary

Preparation for Drug Diversion Cases
What to look for in Chart/Pyxis Audits:
• Frequent new physician orders for different or stronger pain medication • Administration of pain medications at frequent intervals above and beyond expected • If range is ordered for medication, look for upper limits being administered and documented • Review patient's pain range and usage on previous and following shifts • Drug removal occurs at or shorter intervals as ordered • Drug removal from other patients that nurse is not assigned or caring for • Drugs are removed for patients no longer on unit or in hospital (e.g., patient moves from ED to inpatient unit or is discharged)

Preparation for Drug Diversion Cases
Evaluating Medication Orders and the Nurse Who Administered Medication
• Is a controlled substance (CS) signed out for a patient who has no order for the medication? • Does order authorize the amount of CS removed? • Does patient chart reflect assessment for administration of CS? • Do withdrawal times on sign out sheets or Pyxis report match the administration time on the MAR? • Was the patient/resident present when the medications were administered? • Did the nurse medicate another nurse’s patient? • Are another nurse’s initials forged on a MAR?

Preparation for Drug Diversion Cases
Evidence of TYPES of Diversion
• Signing out controlled substance but not administering to patient • Nurse ordering PRN controlled substances takes entire container when delivered • Switching tablets • Emptying capsules (substituting other substances) • Diluting oral liquid controlled substance with water • Diluting injectables with water or saline • Theft from emergency kits • Theft of discontinued controlled substances awaiting destruction by pharmacist or nurses • Dropped medication

Preparation for Drug Diversion Cases
Investigate the Pyxis or Automatic Dispensing System
POTENTIAL ISSUES
• Lack of reliability of automated system • Lack of reliability of how automated system is used • Lack of security or controls • Lack of regular or routine checks and balances • Lack of training for nurses using • Lack of familiarity or investigation of “issues” related to malfunctions, etc. • Lack of “triggers” to prompt review for possible discrepancies or irregularities

Preparation for Drug Diversion Cases
Investigate the Pyxis or Automatic Dispensing System
• What are the recommended settings for the system used?
• Understand the programming and options available
• What functions are “on”? • What is available that is “off”?
• Why is it “off”? (how can this be detected?) • Understand the end user’s view
• Who authorizes access?
• What are the settings on access and exit? • What are the different access levels?
• How do these differ in different care areas? • Who can override (and how/why)?
• Who can waste? (what system is in place?)*

Preparation for Drug Diversion Cases
Possible Areas of Systemic Weaknesses • User passwords not changed (bioprinting system available?) • Users not terminated from system (access limited promptly?) • Discharged patient list remaining available for hours or days after
discharge (are alerts available?) • Built in system controls “turned off” (too cumbersome) • Overrides that permit removals without justification (documented in
MAR?) • Lack of internal controls over controlled substances stored in
emergency kits for trauma or urgent needs • Pain response documentation not regularly reviewed for patterns
• Inadequate segregation of duties
• Staff with no or little training/competency on system (poor practices)

Preparation for Drug Diversion Cases

Preparation for Drug Diversion Cases
Additional Litigation Considerations
v Will formal discovery be required to obtain needed evidence?
• Objections to prosecution evidence v What constraints may be faced in presenting at the hearing? • Time constraints • Limitations or availability of witnesses
v What creative methods can be used to present evidence? • Use of demonstrative exhibits • Power Point in closing v Can a theme (theory of the case) be developed?

Preparation for Drug Diversion Cases

Preparation for Drug Diversion Cases
Demonstrative Exhibits

Preparation for Drug Diversion Cases
CHARACTERISTICS
ü Theory must be credible / believable " Consistent with facts " Explain away bad facts
ü Theory must be interesting / entertaining " Non-abrasive or demeaning " Balanced with seriousness or sensitivity
ü Theory must be consistent with common sense / human experience ü Theory must reveal the true nature / character of the major players ü Theory must lend itself to outcome

Preparation for Drug Diversion Cases

Preparation for Drug Diversion Cases

Preparation for Drug Diversion Cases
Ø Investigating staff/Board member
Ø Attorney Ø Hospital/Facility
Personnel (DONs/CNOs, Drs., other nurses and Pharmacists)
Ø Other agencies (law enforcement, Board of Pharmacy)
Ø Other Boards of Nursing

Robert J. Walters Senior Assistant Attorney General Wyoming Attorney General’s Office 2424 Pioneer Avenue, 2nd Floor Cheyenne, Wyoming 82002 307-777-8662 [email protected]