Rob Storey Reader and Honorary Consultant in Cardiology, University of Sheffield
36
Rob Storey Reader and Honorary Consultant in Cardiology, University of Sheffield The changing world of adjunctive pharmacology
description
Rob Storey Reader and Honorary Consultant in Cardiology, University of Sheffield. The changing world of adjunctive pharmacology. Disclosures. Company Name Relationship AstraZenecaResearch grants, speaker fees, consultant, travel - PowerPoint PPT Presentation
Transcript of Rob Storey Reader and Honorary Consultant in Cardiology, University of Sheffield

Rob Storey
Reader and Honorary Consultant in Cardiology, University of Sheffield
The changing world of adjunctive pharmacology

2
Disclosures
Company Name Relationship• AstraZeneca Research grants, speaker
fees, consultant, travel
• Eli Lilly / Daiichi Sankyo Research grant, speaker fees, consultant, travel
• Schering-Plough Research grant, consultant
• Teva Consultant
• Novartis Consultant
• The Medicines Company Consultant
• Dynabyte Research consumables

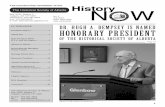
GP = glycoprotein; PAR = protease-activated receptor; TP = thromboxane A2 / prostaglandin H2.Storey RF. Curr Pharm Des. 2006;12:1255-1259.
Targets for Platelet Inhibition
ThromboxaneA2
5HT
P2Y12
ADP ADPADP
5HT
PLATELETACTIVATION
P2Y15HT2A
PAR-1
PAR-4
Densegranule
Thrombingeneration
Shapechange
IIb3
IIb3
FibrinogenIIb3
Aggregation
AmplificationAmplificationAlpha
granule
Coagulation factorsInflammatory mediators
TP
Coagulation
GPVI
Collagen
ATPATP
P2X1
ASPIRIN
x TICLOPIDINECLOPIDOGRELPRASUGREL
ACTIVE METABOLITE
x TICAGRELOR CANGRELOR
GP IIb/IIIa ANTAGONISTS
xx
SCH 530348SCH 530348E5555
x
TERUTROBAN
x
HEPARINSFONDAPARINUXBIVALIRUDINRIVAROXABANAPIXABANDABIGATRAN Thrombin
x

GP = glycoprotein; PAR = protease-activated receptor; TP = thromboxane A2 / prostaglandin H2.Storey RF. Curr Pharm Des. 2006;12:1255-1259.
P2YP2Y1212 as a therapeutic target as a therapeutic target
ThromboxaneA2
5HT
P2Y12
ADP ADPADP
5HT
PLATELETACTIVATION
P2Y15HT2A
PAR-1
PAR-4
Densegranule
Thrombingeneration
Shapechange
IIb3
IIb3
FibrinogenIIb3
Aggregation
AmplificationAmplificationAlpha
granule
Coagulation factorsInflammatory mediators
TP
Coagulation
GPVI
Collagen
ATPATP
P2X1
TICLOPIDINECLOPIDOGRELPRASUGREL
ACTIVE METABOLITE
x TICAGRELOR CANGRELOR
ThrombinThrombin

5
Activation/inactivation of clopidogrel
CYP = cytochrome P450.Farid NA, et al. Clin Pharmacol Ther. 2007;81:735-741.
S
N
O
Cl SO
N
O
Cl
N
SH
COOHO
Cl
S
N
OHO
Cl
Clopidogrel
CYPs
Esterases
CYPs
2-Oxo-clopidogrel R-130964
SR26334 (Inactive)
OCH3 OCH3OCH3

Platelet aggregation before and 4 hours after clopidogrel 600 mg in patients undergoing PCIWhole blood single platelet counting in response to ADP 10 uM
Baseline Post clopidogrel0
20
40
60
80
100
% a
gg
reg
ati
on
Patient with subacute stentthrombosis
Smith SMG et al. Platelets 2006; 17: 250-258

VerifyNow P2Y12 assay
7

Multiplate MEA
8

Clinical outcomes according to platelet aggregometry results with MEA
Sibbing, D. et al. JACC 2009; 53: 849-56

Sibbing, D. et al. Eur Heart J 2009 30:916-922
Clopidogrel, CYP 2C19 and stent thrombosisClopidogrel, CYP 2C19 and stent thrombosis

11
Prasugrel

Comparison of prasugrel with higher dose clopidogrel
P<0.0001 for each
IPA (%; 20 M ADP)
Hours 14 Days
IPA (%; 20 M ADP)
P<0.0001
Prasugrel 10 mg
Clopidogrel 150 mg
Wiviott et al Circ 2007
N=201
Prasugrel 60 mg
Clopidogrel 600 mg

TRITON Study Design
Double-blind
ACS (STEMI or UA/NSTEMI) & Planned PCI
ASA
PRASUGREL60 mg LD/ 10 mg MD
CLOPIDOGREL300 mg LD/ 75 mg MD
1o endpoint: CV death, MI, Stroke2o endpoints: CV death, MI, Stroke, Rehosp-Rec Isch, CV death, MI, UTVR Stent Thrombosis (ARC definite/prob.) Safety endpoints: TIMI major bleeds, Life-threatening bleedsKey Substudies: Pharmacokinetic, Genomic
Median duration of therapy - 12 months
N= 13,600

0
5
10
15
0 30 60 90 180 270 360 450
HR 0.81(0.73-0.90)P=0.0004
Prasugrel
Clopidogrel
Days
En
dp
oin
t (%
)
12.1
9.9
HR 1.32(1.03-1.68)P=0.03
Prasugrel
Clopidogrel1.82.4
138 events
35 events
TRITON-TIMI study TRITON-TIMI study Balance of Efficacy and SafetyBalance of Efficacy and Safety
CV Death / MI / Stroke
TIMI Major NonCABG Bleeds
NNT = 46
NNH = 167

TRITON-TIMI study TRITON-TIMI study Stent Thrombosis (ARC Definite + Probable)
0
1
2
3
0 30 60 90 180 270 360 450
HR 0.48P <0.0001
Prasugrel
Clopidogrel2.4(142)
NNT= 77
1.1 (68)
Days
En
dp
oin
t (%
)
Any Stent at Index PCIAny Stent at Index PCI N= 12,844 N= 12,844

TRITON Diabetic Subgroup
0
2
4
6
8
10
12
14
16
18
0 30 60 90 180 270 360 450
HR 0.70P<0.001
Days
En
dp
oin
t (%
)
CV Death / MI / Stroke
TIMI Major NonCABG Bleeds
NNT = 46
N=3146N=3146
17.0
12.2
Prasugrel
Clopidogrel
Prasugrel
Clopidogrel 2.6
2.5

TRITON STEMI cohortPrimary EP (CV death, MI and stroke at 15 months)
Montalescot et al. ESC 2008
Time (Days)
5
10
15
00 50 100 150 200 250 300 350 400 450
Pro
po
rtio
n o
f p
atie
nts
(%
)
9.5
6.5
12.4
10.0
HR=0.79 (0.65–0.97) NNT=42
p=0.02RRR=21%
p=0.002RRR=32%
Clopidogrel
Prasugrel
Age-adjusted HR=0.81 (0.66-0.99)

TRITON Net Clinical BenefitBleeding Risk Subgroups
OVERALL
>=60 kg
< 60 kg
< 75
>=75
No
Yes
0.5 1 2
Prior Stroke / TIA
Age
Wgt
Risk (%)
+ 37
-16
-1
-16
+3
-14
-13
Prasugrel Better Clopidogrel BetterHR
Pint = 0.006
Pint = 0.18
Pint = 0.36
Post-hoc analysisPost-hoc analysis

Ticagrelor Ticagrelor The first oral reversible P2YThe first oral reversible P2Y1212 antagonist antagonist

Time (hours) Onset Maintenance Offset
100
90
80
70
60
50
40
30
20
10
0
IPA
%Ticagrelor 180mg LD / 90 mg bd (n=54)Clopidogrel 600mg LD / 75 mg od (n=50)
0 .5 1 2 4 8 24 6 weeks 0 2 4 8 24 48 72 120 168 240
*
*
* * *
*
*
*
*
‡
†
†
ONSET/OFFSET Study IPA with ADP 5uM (final extent)
Gurbel PA et al. Circulation 2009

PLATO PLATELET – VerifyNow P2Y12 assay comparing maintenance therapy with
clopidogrel (C) vs ticagrelor (T)
C T C T0
100
200
300
400
500
Trough Peak
**** ****
235PRU
PL
AT
EL
ET
RE
AC
TIO
N U
NIT
S (
PR
U)
Storey RF et al. Presented at American Heart Association annual scientific sessions Nov 2009

No. at risk
Clopidogrel
Ticagrelor
9,291
9,333
8,560
8,678
8,405
8,520
8,177
Days after randomisation
6,703
6,796
5,136
5,210
4,109
4,191
0 60 120 180 240 300 360
6
5
4
3
2
1
0
7
Cum
ula
tive
inci
denc
e (%
)
Clopidogrel
Ticagrelor
5.8
6.9
8,279
HR 0.84 (95% CI 0.75–0.95), p=0.005
0 60 120 180 240 300 360
6
4
3
2
1
0
Clopidogrel
Ticagrelor
4.0
5.1
HR 0.79 (95% CI 0.69–0.91), p=0.001
7
5
9,291
9,333
8,865
8,294
8,780
8,822
8,589
Days after randomisation
7079
7119
5,441
5,482
4,364
4,4198,626
Myocardial infarction Cardiovascular death
Cum
ula
tive
inci
denc
e (%
)
Secondary efficacy endpoints over time

Total major bleeding
NS
NS
NS
NS
NS
0K-M
est
imat
ed r
ate
(% p
er y
ear)
PLATO major bleeding
1
2
3
4
5
6
7
8
9
10
12
11
13
TIMI major bleeding
Red cell transfusion*
PLATO life-threatening/fatal bleeding
Fatal bleeding
Major bleeding and major or minor bleeding according to TIMI criteria refer to non-adjudicated events analysed with the use of a statistically programmed analysis in accordance with definition described in Wiviott SD et al. NEJM 2007;357:2001–15; *Proportion of patients (%); NS = not significant
11.611.2
7.9 7.7
8.9 8.9
5.8 5.8
0.3 0.3
TicagrelorClopidogrel

Non-CABG and CABG-related major bleeding
p=0.026
p=0.025
NS
NS
9K
-M e
stim
ated
rat
e (
% p
er y
ear)
Non-CABGPLATO majorbleeding
8
7
6
5
4
3
2
1
0Non-CABGTIMI major bleeding
CABGPLATO major bleeding
CABG TIMI major bleeding
4.5
3.8
2.8
2.2
7.4
7.9
5.3
5.8
TicagrelorClopidogrel

PLATO - Dyspnoea
All patientsTicagrelor(n=9,235)
Clopidogrel(n=9,186) p value*
Dyspnoea, %
Any
With discontinuation of study treatment
13.8
0.9
7.8
0.1<0.001
<0.001
*p values were calculated using Fischer’s exact test

PLATO Conclusions• Reversible, more intense P2Y12 receptor inhibition for one year with ticagrelor in
comparison with clopidogrel in a broad population with ST- and non-ST-elevation
ACS provides
– Reduction in myocardial infarction and stent thrombosis
– Reduction in cardiovascular and total mortality
– No change in the overall risk of major bleeding
• Ticagrelor is a more effective alternative than clopidogrel for the continuous prevention of
ischaemic events, stent thrombosis and death in the acute and long-term treatment of
patients with ACS• Clinicians will need to learn how to identify and manage dyspnoea associated with ticagrelor

Cangrelor Cangrelor Intravenous reversible P2YIntravenous reversible P2Y1212 antagonist antagonist

HOO
OH OH
N
N
N S F
FF
N
HNS
_
O_
P
O_
O Cl
ClP
O
O
OP
O
_O
OO
OH OH
N
N
N S F
FF
N
HNS
4Na+
Inactivation by Dephosphorylation

BRIDGE study design (provisional) ACS treated with clopidogrel, scheduled for CABG
Stop clopidogrel x days prior to CABG
Cangrelor infusionPlacebo infusion
1o end point: Bleeding2o end points: Inhibition of platelet function, ischaemic events
Primary objective: To assess safety of cangrelor compared to placebo prior to CABG surgery
Stop x hours prior to CABG surgery
PD measurements

Elinogrel Elinogrel Intravenous and oral reversible Intravenous and oral reversible
P2YP2Y1212 antagonist antagonist

Elinogrel
• Reversible P2Y12 inhibitor in phase 2/3 development
• IV and oral formulations
• Half-life ~12 hours
• Competitive mechanism of action – competes with ADP for binding to receptor, greater IPA for low vs high concentrations of ADP

32
Targeting PAR-1

GP = glycoprotein; PAR = protease-activated receptor; TP = thromboxane A2 / prostaglandin H2.Storey RF. Curr Pharm Des. 2006;12:1255-1259.
Targets for Platelet Inhibition
ThromboxaneA2
5HT
P2Y12
ADP ADPADP
5HT
PLATELETACTIVATION
P2Y15HT2A
PAR-1
PAR-4
Densegranule
Thrombingeneration
Shapechange
IIb3
IIb3
FibrinogenIIb3
Aggregation
AmplificationAmplificationAlpha
granule
Coagulation factorsInflammatory mediators
TP
Coagulation
GPVI
Collagen
ATPATP
P2X1
ASPIRIN
x TICLOPIDINECLOPIDOGRELPRASUGREL
ACTIVE METABOLITE
x TICAGRELOR CANGRELOR
GP IIb/IIIa ANTAGONISTS
xx
SCH 530348SCH 530348E5555
x
TERUTROBAN
x
HEPARINSFONDAPARINUXBIVALIRUDINRIVAROXABANAPIXABANDABIGATRAN Thrombin
x

No significant compromise to haemostasis with SCH 530348
Surgical blood loss (ml/hr)
Vehicle T-1 T-2 T-30
1
2
3
* *
Treament
Blo
od
Lo
ss (m
ls)
Bleeding time
Vehicle T-1 T-2 T-30
10
20
30 * *
TreatmentT
emp
late
ble
edin
gti
me
(min
)T-1 = SCH 530348 1 mg/kgT-2 = Aspirin (10 mg/kg) plus Clopidogrel (2 mg/kg)T-3 = SCH 530348, Aspirin plus Clopidogrel
Cynomolgus monkey model.
Chintala M et al. Arterioscl Thromb Vasc Biol. 2008; 28: e138–e139

Study started December 2007
Estimated study completion July 2011
TRACER Study Design
Primary end point: CV death/MI/stroke/recurrent ischaemia
with rehospitalisation/urgent coronary revascularisation
12-month minimum exposure
(N=10,000)
Standard therapy + placebo
Standard therapy + SCH 530548
40 mg LD then 2.5 mg od
Moderate- to High-Risk ACS patients (UA/NSTEMI, PCI,
Medically-Managed, or CABG)

GP = glycoprotein; PAR = protease-activated receptor; TP = thromboxane A2 / prostaglandin H2.Storey RF. Curr Pharm Des. 2006;12:1255-1259.
ThromboxaneA2
5HT
P2Y12
ADP ADPADP
5HT
P2Y15HT2A
PAR-1
PAR-4
Densegranule
Thrombingeneration
Shapechange
IIb3
IIb3
FibrinogenIIb3
Aggregation
AmplificationAmplificationAlpha
granule
Coagulation factorsInflammatory mediators
TP
Coagulation
GPVI
Collagen
ATPATP
P2X1
ASPIRIN
x TICLOPIDINECLOPIDOGRELPRASUGREL
ACTIVE METABOLITE
x TICAGRELOR CANGRELOR
GP IIb/IIIa ANTAGONISTS
xx
SCH 530348E5555
x
TERUTROBAN
x
HEPARINSFONDAPARINUXBIVALIRUDINRIVAROXABANAPIXABANDABIGATRAN Thrombinx
?
QuestionsQuestions