Roadmap to 2014: Subsidized Insurance Workgroup Update
29
Commonwealth of Massachusetts Executive Office of Health and Human Services Roadmap to 2014: Subsidized Insurance Workgroup Update Stakeholder Meeting December 21, 2011
-
Upload
cyrus-livingston -
Category
Documents
-
view
32 -
download
0
description
Roadmap to 2014: Subsidized Insurance Workgroup Update. Stakeholder Meeting December 21, 2011. Guiding Principles and Key Concepts. Guiding Principles. - PowerPoint PPT Presentation
Transcript of Roadmap to 2014: Subsidized Insurance Workgroup Update
Commonwealth of MassachusettsExecutive Office of Health and Human Services
Roadmap to 2014:Subsidized Insurance Workgroup Update
Stakeholder MeetingDecember 21, 2011
2
EOHHS
Guiding Principles and Key Concepts
3
EOHHS
Guiding Principles
As we prepare for providing health insurance coverage to Massachusetts’ subsidized population under national health care reform in 2014, these guiding principles were developed by inter-agency leaders
1. Creating a consumer-centric approach to ensuring that all eligible Massachusetts residents avail themselves of available health insurance subsidies to make health care affordable to as many people as possible.
2. Creating a single, integrated process to determine eligibility for the full range of health insurance programs including Medicaid, CHIP, potentially the Basic Health Program and premium tax credits and cost-sharing subsidies.
3. Offering appropriate health insurance coverage to eligible individuals by defining both the populations affected and the health benefits that meet their needs.
4. Working within state fiscal realities, maximizing and leveraging financial resources, such as FFP.
5. Focusing on simplicity and continuity of coverage for members by streamlining coverage types, thereby making noticing and explanation of benefits more understandable, and also minimizing disruptions in coverage.
6. Creating an efficient administrative infrastructure that leverages technology and eliminates administrative duplication.
7. Building off the lessons learned since passage of Chapter 58.
8. Creating opportunities to achieve payment and delivery system reforms that ensure continued coverage, access, and cost containment and improve the overall health status of the populations served.
4
EOHHS
ACA Key Concepts
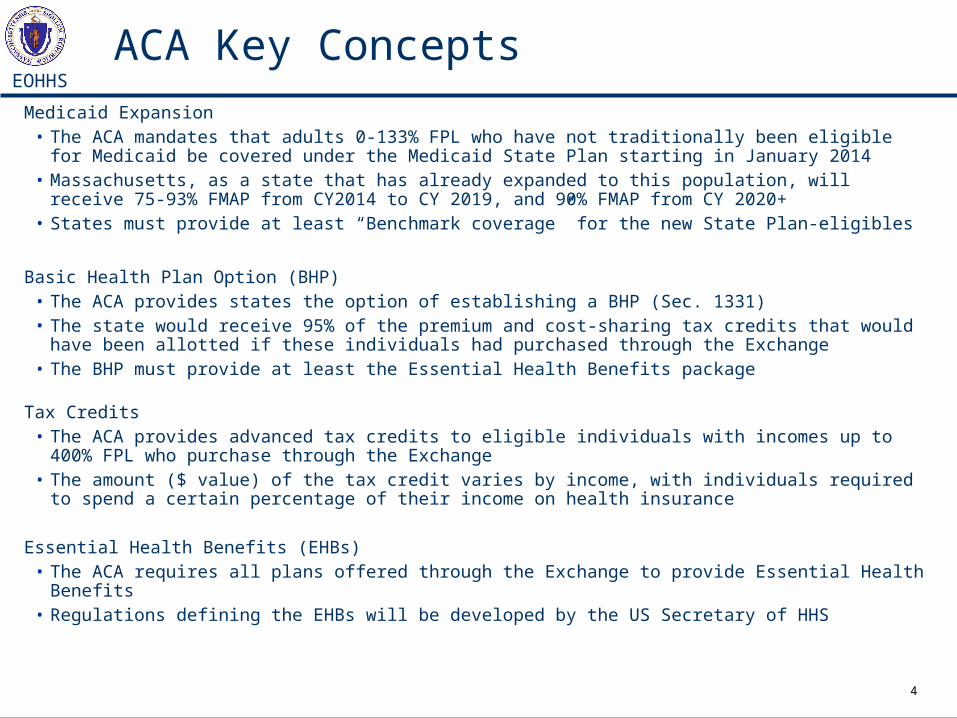
Medicaid Expansion• The ACA mandates that adults 0-133% FPL who have not traditionally been eligible for Medicaid be
covered under the Medicaid State Plan starting in January 2014• Massachusetts, as a state that has already expanded to this population, will receive 75-93% FMAP
from CY2014 to CY 2019, and 90% FMAP from CY 2020+• States must provide at least “Benchmark coverage” for the new State Plan-eligibles
Basic Health Plan Option (BHP)• The ACA provides states the option of establishing a BHP (Sec. 1331)• The state would receive 95% of the premium and cost-sharing tax credits that would have been
allotted if these individuals had purchased through the Exchange• The BHP must provide at least the Essential Health Benefits package
Tax Credits• The ACA provides advanced tax credits to eligible individuals with incomes up to 400% FPL who
purchase through the Exchange• The amount ($ value) of the tax credit varies by income, with individuals required to spend a certain
percentage of their income on health insurance
Essential Health Benefits (EHBs)• The ACA requires all plans offered through the Exchange to provide Essential Health Benefits• Regulations defining the EHBs will be developed by the US Secretary of HHS
5
EOHHS
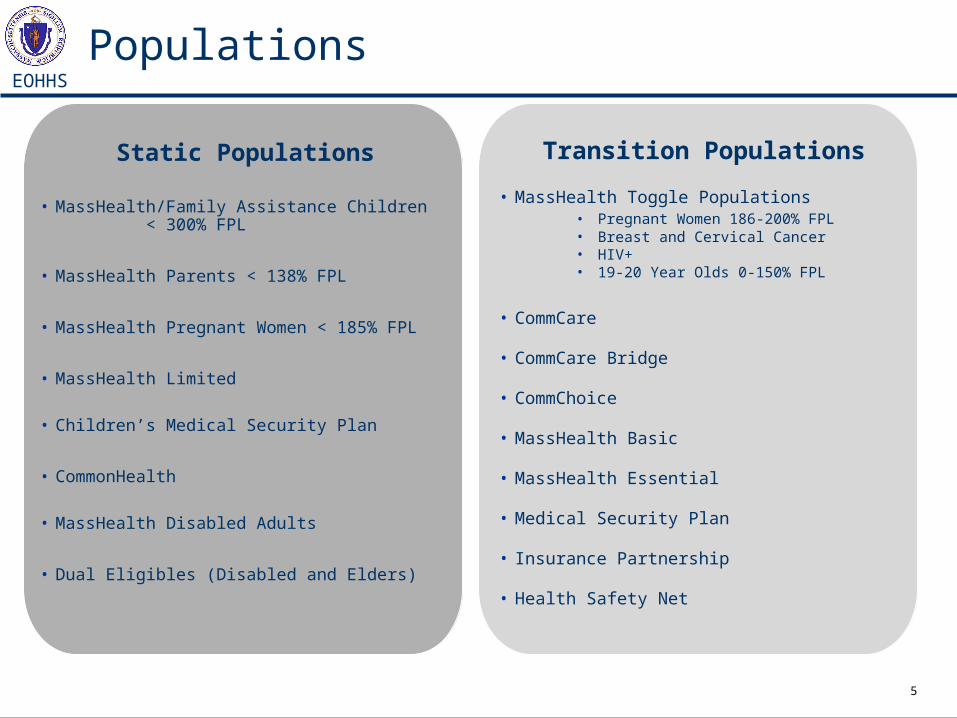
Transition Populations
• MassHealth Toggle Populations• Pregnant Women 186-200% FPL• Breast and Cervical Cancer• HIV+• 19-20 Year Olds 0-150% FPL
• CommCare
• CommCare Bridge
• CommChoice
• MassHealth Basic
• MassHealth Essential
• Medical Security Plan
• Insurance Partnership
• Health Safety Net
Static Populations
• MassHealth/Family Assistance Children < 300% FPL
• MassHealth Parents < 138% FPL
• MassHealth Pregnant Women < 185% FPL
• MassHealth Limited
• Children’s Medical Security Plan
• CommonHealth
• MassHealth Disabled Adults
• Dual Eligibles (Disabled and Elders)
Populations
6
EOHHS
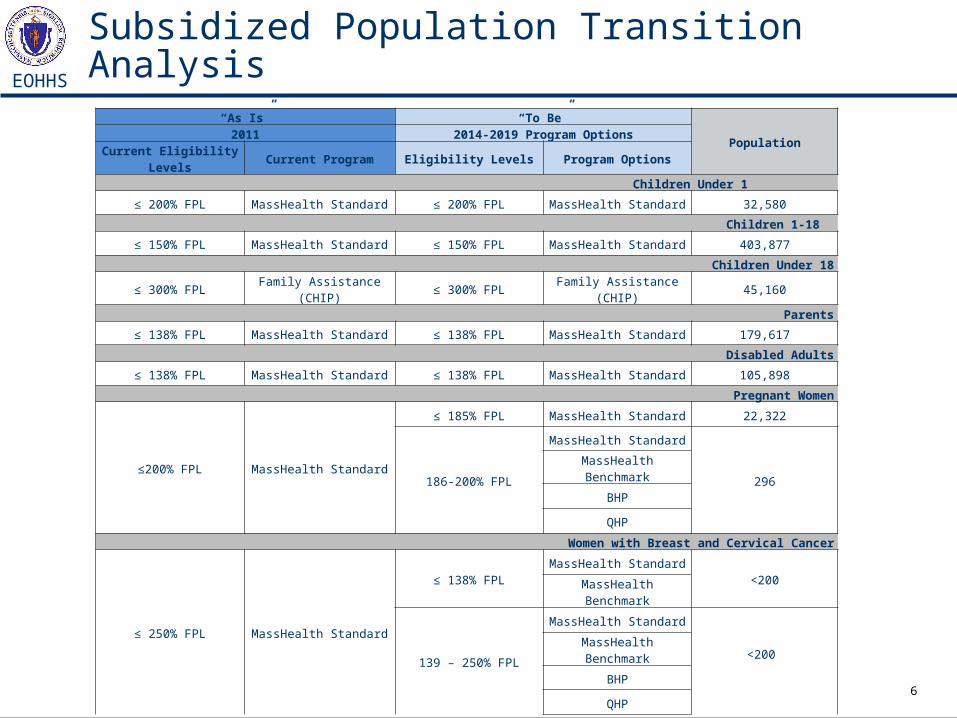
Subsidized Population Transition Analysis
“As Is” “To Be”
Population2011 2014-2019 Program Options
Current Eligibility Levels
Current Program Eligibility Levels Program Options
Children Under 1
≤ 200% FPL MassHealth Standard ≤ 200% FPL MassHealth Standard 32,580
Children 1-18
≤ 150% FPL MassHealth Standard ≤ 150% FPL MassHealth Standard 403,877
Children Under 18
≤ 300% FPL Family Assistance (CHIP) ≤ 300% FPL Family Assistance (CHIP) 45,160
Parents
≤ 138% FPL MassHealth Standard ≤ 138% FPL MassHealth Standard 179,617
Disabled Adults
≤ 138% FPL MassHealth Standard ≤ 138% FPL MassHealth Standard 105,898
Pregnant Women
≤200% FPL MassHealth Standard
≤ 185% FPL MassHealth Standard 22,322
186-200% FPL
MassHealth Standard
296MassHealth Benchmark
BHP
QHP
Women with Breast and Cervical Cancer
≤ 250% FPL MassHealth Standard
≤ 138% FPLMassHealth Standard
<200MassHealth Benchmark
139 – 250% FPL
MassHealth Standard
<200 MassHealth Benchmark
BHP
QHP
7
EOHHS
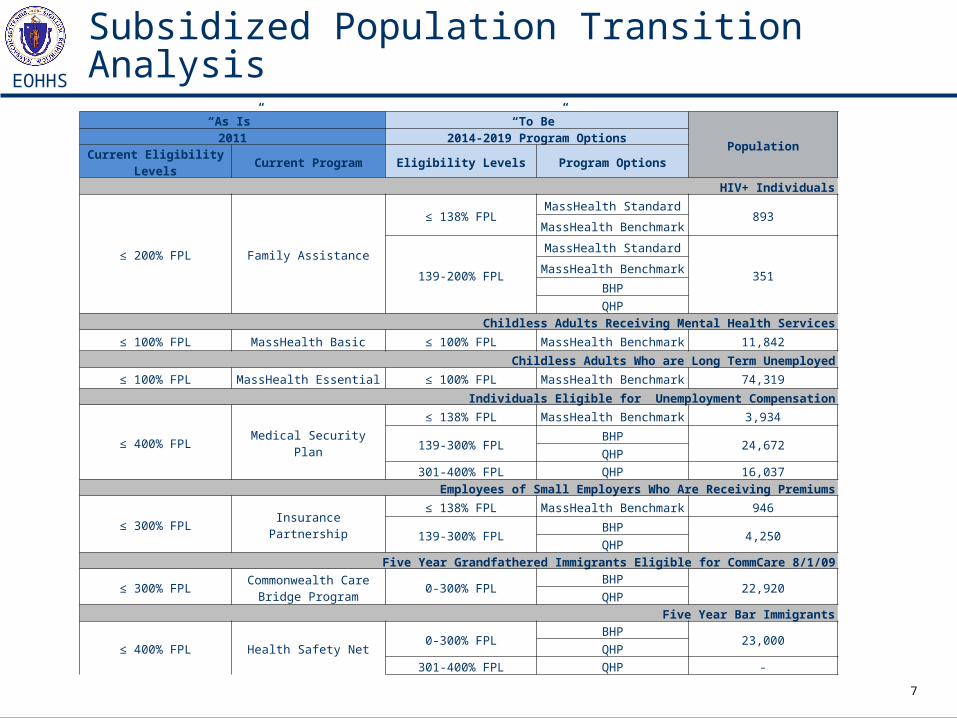
Subsidized Population Transition Analysis
“As Is” “To Be”
Population2011 2014-2019 Program Options
Current Eligibility Levels Current Program Eligibility Levels Program Options
HIV+ Individuals
≤ 200% FPL Family Assistance
≤ 138% FPLMassHealth Standard
893MassHealth Benchmark
139-200% FPL
MassHealth Standard
351MassHealth Benchmark
BHP
QHP
Childless Adults Receiving Mental Health Services
≤ 100% FPL MassHealth Basic ≤ 100% FPL MassHealth Benchmark 11,842
Childless Adults Who are Long Term Unemployed
≤ 100% FPL MassHealth Essential ≤ 100% FPL MassHealth Benchmark 74,319
Individuals Eligible for Unemployment Compensation
≤ 400% FPL Medical Security Plan
≤ 138% FPL MassHealth Benchmark 3,934
139-300% FPLBHP
24,672QHP
301-400% FPL QHP 16,037
Employees of Small Employers Who Are Receiving Premiums
≤ 300% FPL Insurance Partnership
≤ 138% FPL MassHealth Benchmark 946
139-300% FPLBHP
4,250QHP
Five Year Grandfathered Immigrants Eligible for CommCare 8/1/09
≤ 300% FPLCommonwealth Care
Bridge Program0-300% FPL
BHP22,920
QHP
Five Year Bar Immigrants
≤ 400% FPL Health Safety Net0-300% FPL
BHP23,000
QHP
301-400% FPL QHP -
8
EOHHS
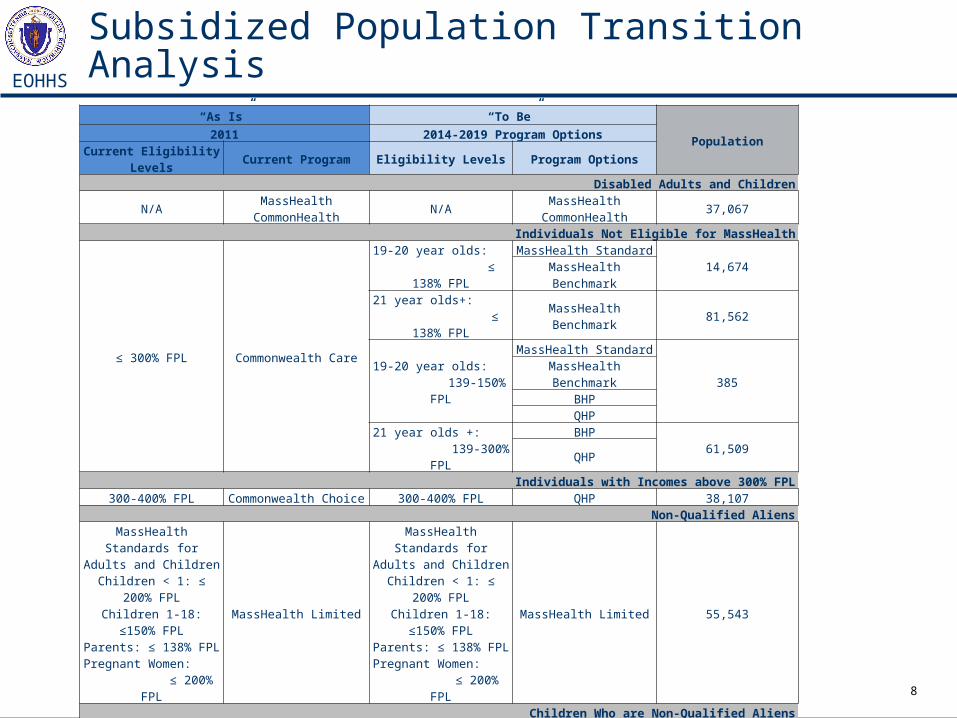
Subsidized Population Transition Analysis
“As Is” “To Be”
Population2011 2014-2019 Program Options
Current Eligibility Levels
Current Program Eligibility Levels Program Options
Disabled Adults and Children
N/AMassHealth
CommonHealthN/A
MassHealth CommonHealth
37,067
Individuals Not Eligible for MassHealth
≤ 300% FPL Commonwealth Care
19-20 year olds: ≤ 138% FPL
MassHealth Standard14,674
MassHealth Benchmark21 year olds+:
≤ 138% FPLMassHealth Benchmark 81,562
19-20 year olds: 139-150% FPL
MassHealth Standard
385MassHealth Benchmark
BHPQHP
21 year olds +: 139-300% FPL
BHP61,509
QHPIndividuals with Incomes above 300% FPL
300-400% FPL Commonwealth Choice 300-400% FPL QHP 38,107Non-Qualified Aliens
MassHealth Standards for Adults and ChildrenChildren < 1: ≤ 200%
FPLChildren 1-18: ≤150%
FPLParents: ≤ 138% FPL
Pregnant Women: ≤ 200% FPL
MassHealth Limited
MassHealth Standards for Adults and ChildrenChildren < 1: ≤ 200%
FPLChildren 1-18: ≤150%
FPLParents: ≤ 138% FPL
Pregnant Women: ≤ 200% FPL
MassHealth Limited 55,543
Children Who are Non-Qualified Aliens
N/AChildren’s Medical
Security PlanN/A
Children’s Medical Security Plan
<200
HSN0-138% FPL Health Safety Net 0-138% FPL MassHealth Benchmark 49,000
9
EOHHS
Subsidized Coverage Options
10
EOHHS
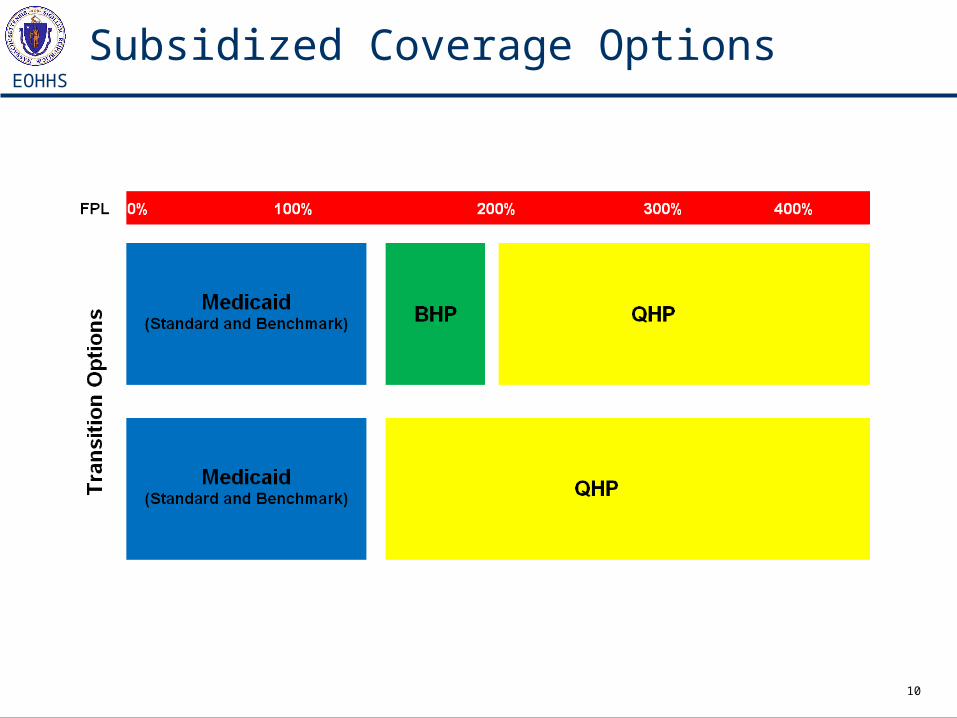
Subsidized Coverage Options
11
EOHHS
Coverage OptionsInitial Modeling
12
EOHHS
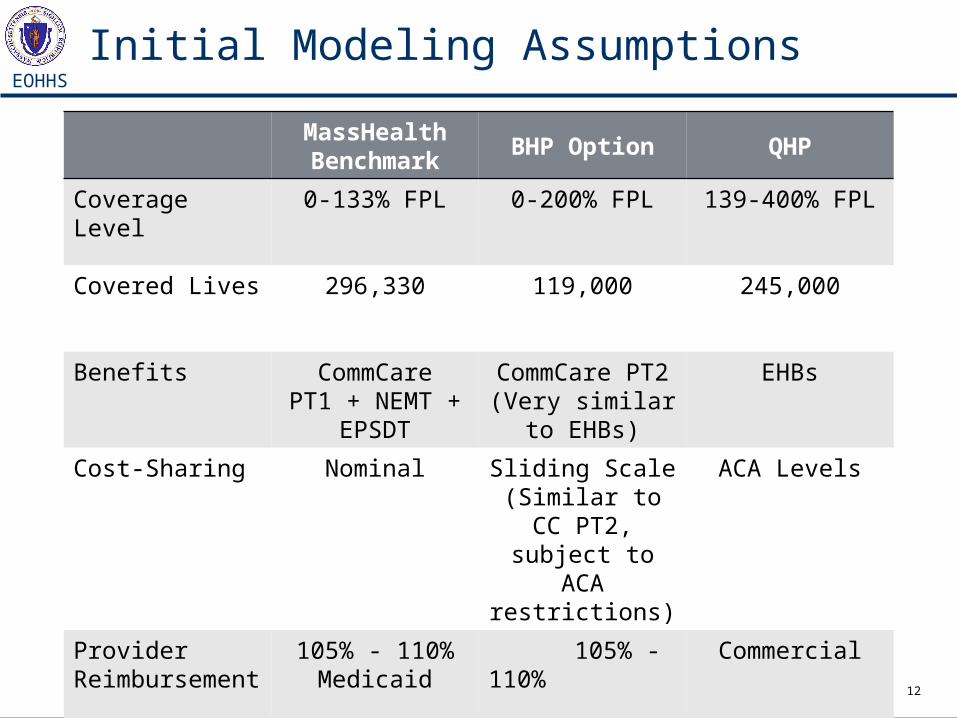
Initial Modeling Assumptions
MassHealthBenchmark
BHP Option QHP
Coverage Level 0-133% FPL 0-200% FPL 139-400% FPL
Covered Lives 296,330 119,000 245,000
Benefits CommCarePT1 + NEMT +
EPSDT
CommCare PT2(Very similar to
EHBs)
EHBs
Cost-Sharing Nominal Sliding Scale(Similar to CC PT2, subject to
ACA restrictions)
ACA Levels
Provider Reimbursement
105% - 110% Medicaid
105% - 110% Medicaid
Commercial
13
EOHHS
Key Issues in Evaluating Options
14
EOHHS
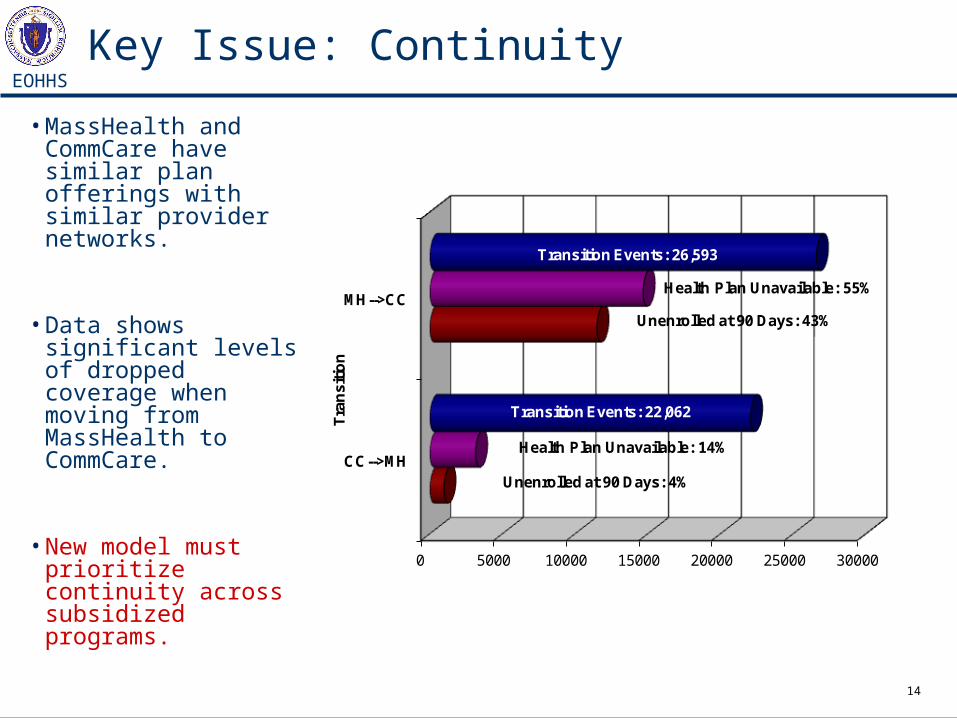
Key Issue: Continuity
• MassHealth and CommCare have similar plan offerings with similar provider networks.
• Data shows significant levels of dropped coverage when moving from MassHealth to CommCare.
• New model must prioritize continuity across subsidized programs.
0 5000 10000 15000 20000 25000 30000
CC-->MH
MH-->CC
Tra
nsi
tion
Transition Events: 22,062
Transition Events: 26,593
Health Plan Unavailable: 55%
Health Plan Unavailable: 14%
Unenrolled at 90 Days: 4%
Unenrolled at 90 Days: 43%
15
EOHHS
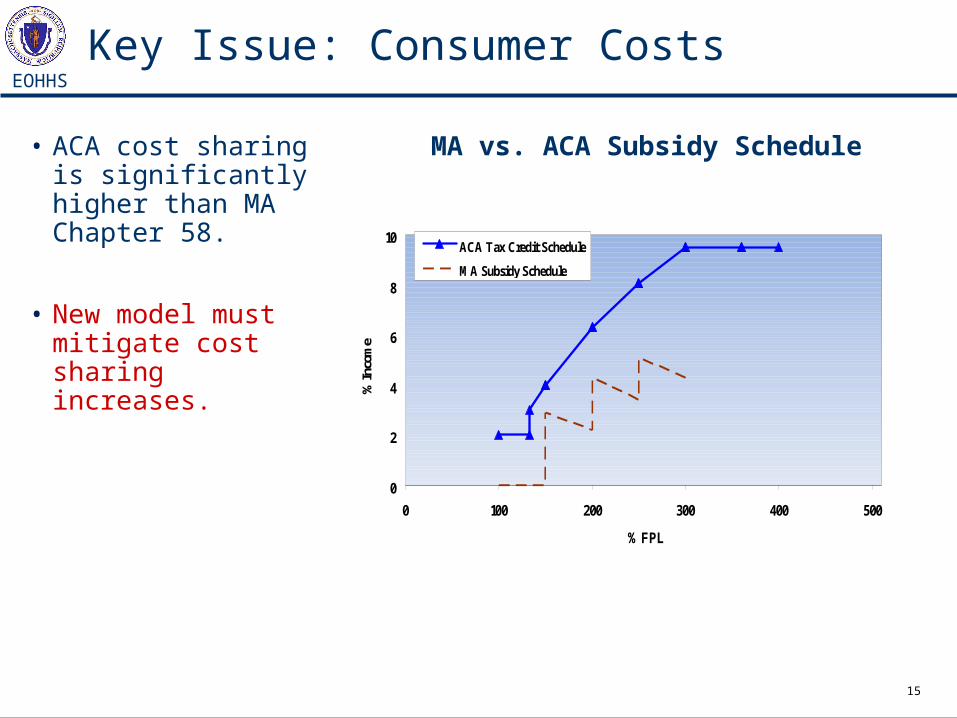
Key Issue: Consumer Costs
• ACA cost sharing is significantly higher than MA Chapter 58.
• New model must mitigate cost sharing increases.
MA vs. ACA Subsidy Schedule
0
2
4
6
8
10
0 100 200 300 400 500
% FPL
% In
com
e
ACA Tax Credit Schedule
MA Subsidy Schedule
16
EOHHS
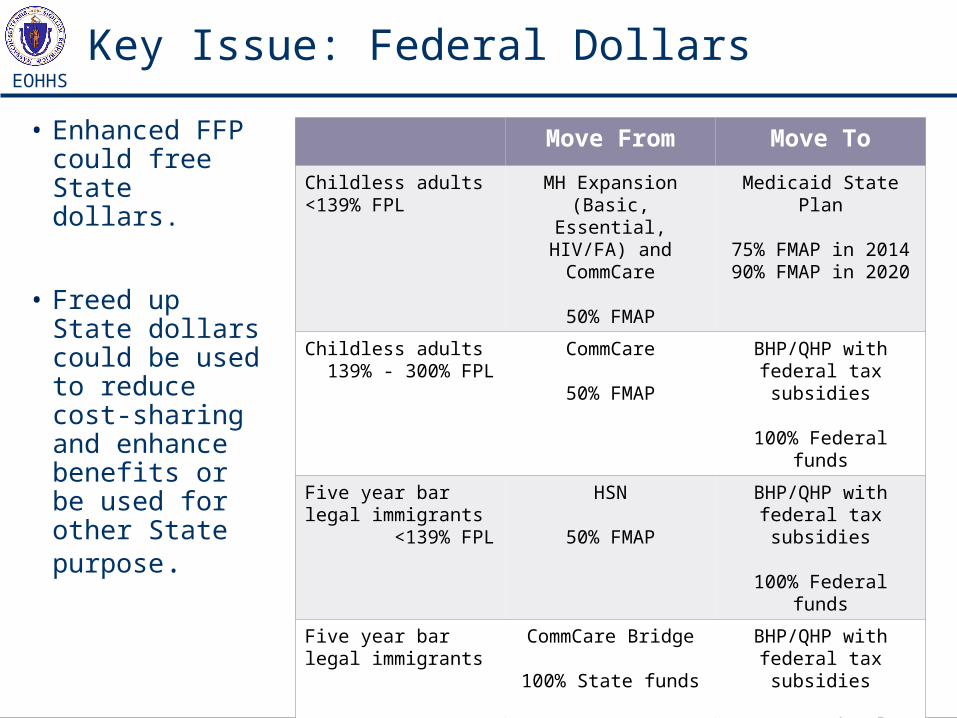
Key Issue: Federal Dollars
• Enhanced FFP could free State dollars.
• Freed up State dollars could be used to reduce cost-sharing and enhance benefits or be used for other State purpose.
Move From Move To
Childless adults <139% FPL
MH Expansion (Basic, Essential, HIV/FA) and
CommCare
50% FMAP
Medicaid State Plan
75% FMAP in 201490% FMAP in 2020
Childless adults 139% - 300% FPL
CommCare
50% FMAP
BHP/QHP with federal tax subsidies
100% Federal funds
Five year bar legal immigrants <139% FPL
HSN
50% FMAP
BHP/QHP with federal tax subsidies
100% Federal funds
Five year bar legal immigrants
CommCare Bridge
100% State funds
BHP/QHP with federal tax subsidies
100% Federal funds
17
EOHHS
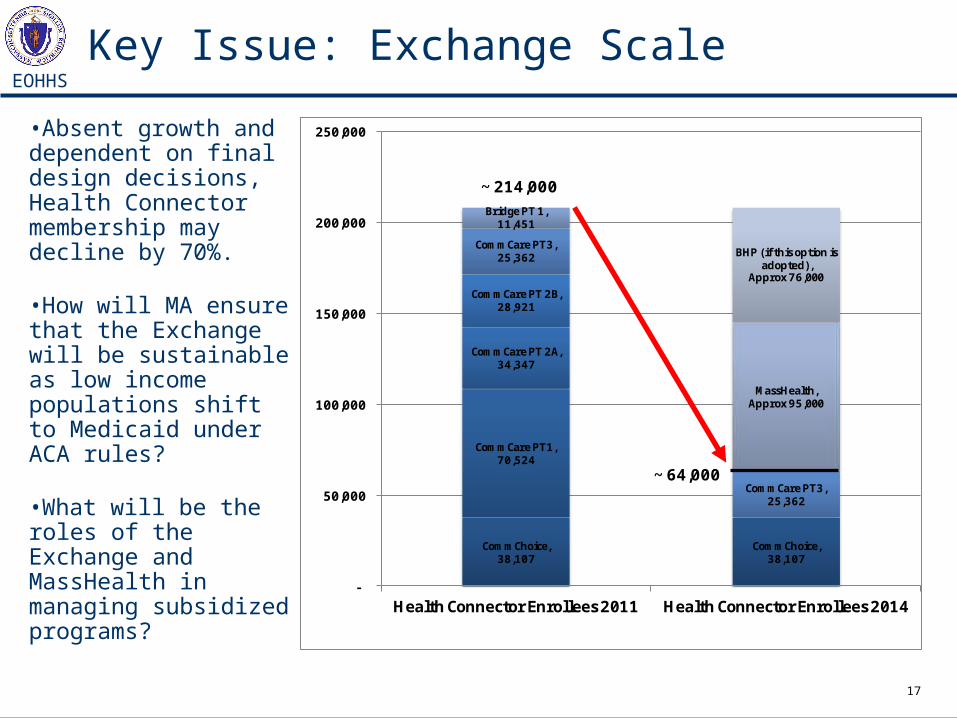
Key Issue: Exchange Scale
•Absent growth and dependent on final design decisions, Health Connector membership may decline by 70%.
•How will MA ensure that the Exchange will be sustainable as low income populations shift to Medicaid under ACA rules?
•What will be the roles of the Exchange and MassHealth in managing subsidized programs?
CommChoice, 38,107
CommChoice, 38,107
CommCare PT1, 70,524
CommCare PT 2A, 34,347
CommCare PT 2B, 28,921
CommCare PT3, 25,362
CommCare PT3, 25,362
Bridge PT 1, 11,451
MassHealth, Approx 95,000
BHP (if this option is adopted),
Approx 76,000
-
50,000
100,000
150,000
200,000
250,000
Health Connector Enrollees 2011 Health Connector Enrollees 2014
~ 214,000
~ 64,000
18
EOHHS
Takeaways from Initial Modeling
• ACA requires higher levels of consumer cost sharing as compared to cost-sharing currently imposed in CommCare.
• State savings could be used to reduce cost sharing for consumers up to 300% FPL.
• BHP may offer opportunity to reduce cost sharing in 2014 for consumers between 139% and 200% FPL with no state investment.
• BHP modeling includes some federal revenue uncertainties, including premium value of 2nd lowest cost silver plan and EHBs, which could impact State cost (since State receives 95% of premium amount).
• BHP has risk for Connector related to scale, leverage and sustainability
19
EOHHS
Follow up Modeling
To further refine Cost and FFP Estimates
20
EOHHS
Population Variances
Enrollment Assumptions• Model using upper and lower bounds of enrollment in
Medicaid Benchmark, and BHP/QHP to 200% FPL.
Acuity Assumptions• Model using higher acuity for certain BHP members
(MSP and Bridge).
21
EOHHS
Cost-sharing and Take-up Rates
Premium and Cost-Sharing Assumptions• Model the BHP with premiums and cost-sharing as under the ACA and as in CommCare Plan Type 1 and Type 2.
Take-up Rates• Model differential coverage take-up rates of the BHP, QHP, and subsidized QHP related to member cost sharing bounds.
22
EOHHS
Cost/Revenue Variances
Trend Assumptions• Model the impact of different Medicaid-Commercial trend scenarios (current modeling assumes 4% Medicaid and 6% Commercial) to illustrate the revenue and cost implications of reasonable combinations.
Benefit Assumptions• Model the impact of a narrower set of Essential Health Benefits (current modeling assumes CommCare Plan Type 1 benefits) for BHP and subsidized QHP members to reflect “typical small employer.” Impact includes cost of “adding” benefits and the change in state revenue for a BHP (due to a lower premium price).
23
EOHHS
Benefit ConfigurationDecisions To Be Made
24
EOHHS
New Medicaid State Plan Populations
Benchmark Coverage
• What are the covered services?
• What will the premium assistance component look like? (ESI requirements, minimum benefit levels, FFS wrap?)
Who are the truly new enrollees? How many?
What enrollment options will be used for the expanded Medicaid population?
25
EOHHS
Basic Health Plan (BHP) Option – 138-200% FPL and AWSS
Will there be a BHP? If so,
• What benefits and cost-sharing?
• How will it be administered?
• What will it cost members?
• What will it cost the State?
26
EOHHS
Qualified Health Plans (QHP)Essential Health Benefits and Tax Credits
Will there be a “wrapped” QHP? If so,
• To what % FPL?
• How will it be operationalized in regard to copays, premiums, and additional benefits?
• What will it cost members?
• What will it cost the State?
How will tax credits work for members?
• What is their financial exposure for incorrect subsidy amounts (due to errors or income changes)?
27
EOHHS
Movement Between Subsidized Programs
Where are the transition points?
• at 138% FPL, at 200% FPL, both?
How many people are expected to move between programs?
What are the benefit “cliffs”?
What are the cost sharing “cliffs”?
How does movement between programs affect continuity of: coverage, providers, care?
28
EOHHS
General Questions
• How do options align with Guiding Principles?
• How will budgets be aligned across programs (MassHealth, Connector, MSP, HSN)?
• Will health plans be required to participate across Medicaid, (BHP), QHP?
• When will enrollments begin?
• How will members be notified?
• What Statute changes are needed?
• What State Plan changes are needed?
• What MassHealth 1115 Waiver changes are needed?
29
EOHHS
Next Steps for Subsidized Insurance Options
• Manatt/Mercer to provide final evaluation results, including sensitivity analysis.
• Stakeholder engagement relative to findings anticipated in January.