
Rivaroxaban: efficacia e sicurezza dei NAO · Dose totale giornaliera 120 mg * ... AF who are...
39
Stefano Carugo Università degli Studi di Milano Rivaroxaban: efficacia e sicurezza dei NAO Alba 15 novembre 2014
Transcript of Rivaroxaban: efficacia e sicurezza dei NAO · Dose totale giornaliera 120 mg * ... AF who are...

Stefano Carugo
Università degli Studi di Milano
Rivaroxaban: efficacia e sicurezza dei NAO
Alba 15 novembre 2014

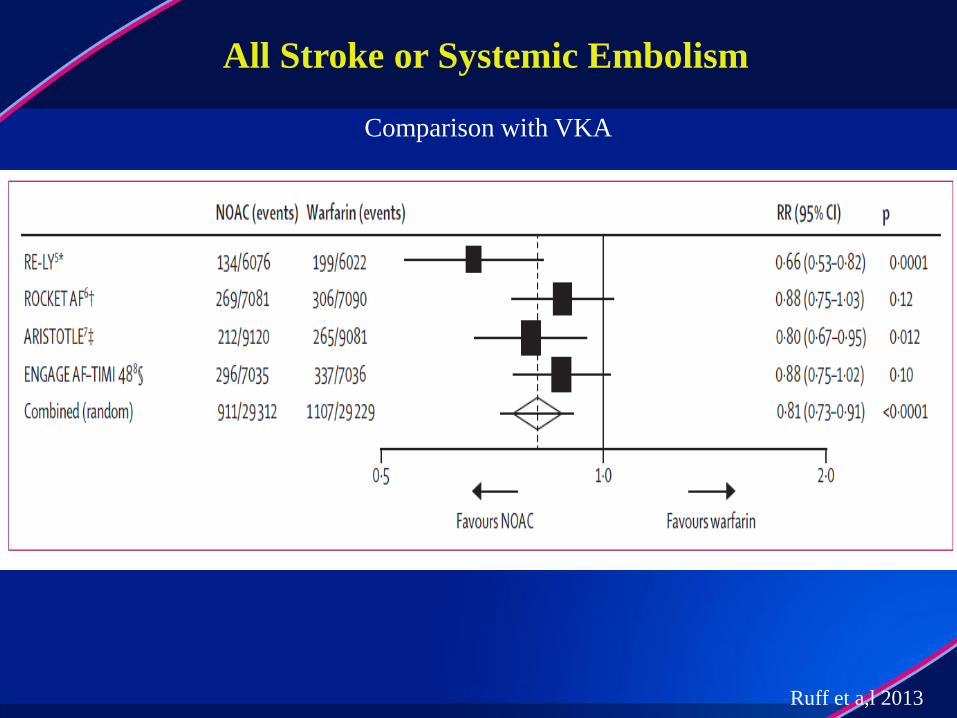
• All four novel anticoagulants are non-inferior to warfarin in reducing the
risk of stroke and systemic embolization
• All four novel anticoagulants are associated with a reduction of
haemorrhagic stroke
• All four agents reduce the risk of bleeding (fatal and in critical organ for
Rivaroxaban, major for Apixaban and Edoxaban, major at 110 mg for
Dabigatran, ) and intracranial hemorrhage
• The directionality and magnitude of the mortality reduction is consistent
and approximates a RRR of 10% / year
“Class effects”

• Dabigatran (at the dose of 150 mg bid) is associated with a reduction of
ischemic stroke
• Rivaroxoban is associated with a reduction the risk of fatal and in
critical organ bleeding
• Apixaban is associated with a reduction of mortality
• Both doses of edoxaban are associated with a reduction of major bleeding
AF studies: main clinical differences
Ruff et a,l 2013
All Stroke or Systemic Embolism
Comparison with VKA

Ruff et al 2013
Major bleeding

Ruff et al 2013
Secondary efficacy and safety outcomes
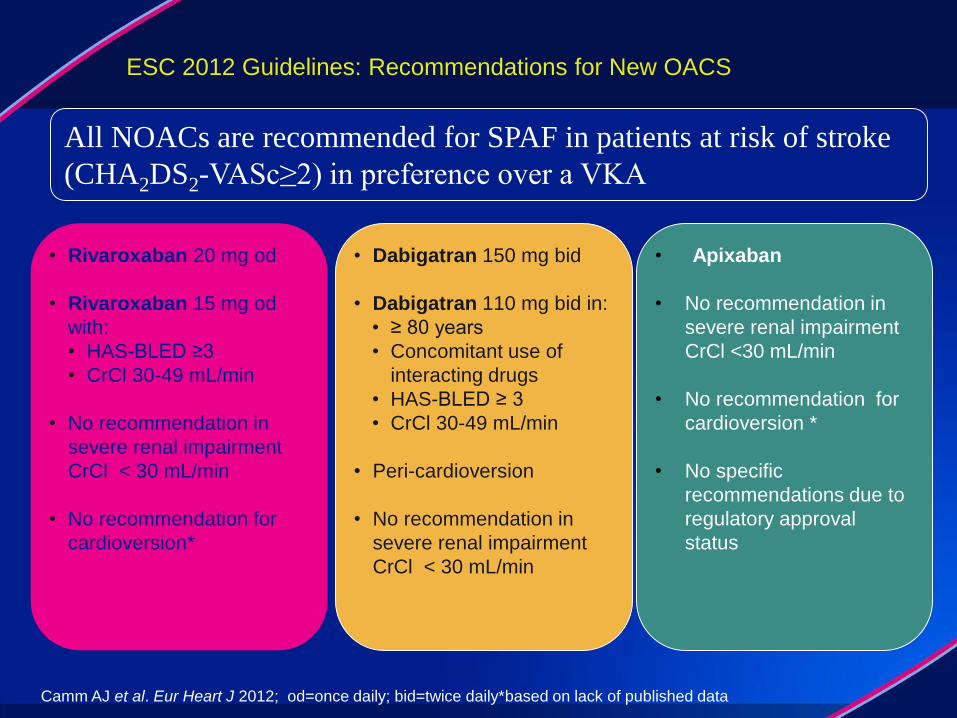
ESC 2012 Guidelines: Recommendations for New OACS
• Dabigatran 150 mg bid
• Dabigatran 110 mg bid in:
• ≥ 80 years
• Concomitant use of
interacting drugs
• HAS-BLED ≥ 3
• CrCl 30-49 mL/min
• Peri-cardioversion
• No recommendation in
severe renal impairment
CrCl < 30 mL/min
• Apixaban
• No recommendation in
severe renal impairment
CrCl <30 mL/min
• No recommendation for
cardioversion *
• No specific
recommendations due to
regulatory approval
status
All NOACs are recommended for SPAF in patients at risk of stroke
(CHA2DS2-VASc≥2) in preference over a VKA
• Rivaroxaban 20 mg od
• Rivaroxaban 15 mg od
with:
• HAS-BLED ≥3
• CrCl 30-49 mL/min
• No recommendation in
severe renal impairment
CrCl < 30 mL/min
• No recommendation for
cardioversion*
Camm AJ et al. Eur Heart J 2012; od=once daily; bid=twice daily*based on lack of published data

ESC 2012 Guidelines: Selection of Patients for OACs
Non-valvular atrial fibrillation Valvular atrial fibrillation
< 65 years and lone AF including women
Stroke risk assessment using CHA2DS2-VASc
0 1 ≥2
Assess bleeding risk (HAS-BLED score);
consider patient values/preferences
New oral anticoagulant;
rivaroxaban, dabigatran
apixaban
Vitamin K antagonistNo antithrombotic therapy
Oral anticoagulant
Yes
Camm AJ et al. Eur Heart J 2012 Slide line preferred; dotted line alternative

Dati farmacodinamici e clinici
Aspetti pratici (aderenza)
Monosomministrazione
quotidiana: vantaggi

Dati farmacodinamici e clinici
Aspetti pratici (aderenza)
Monosomministrazione
quotidiana: vantaggi

Rivaroxaban (MW 436 1 nM = 0.436 ng/mL)
inibisce:
– attività FXa libero = IC50 0.7 nM
– attività protrombinasi = IC50 2.1 nM
Ctrough (concentrazioni dopo 24 h) con 10 mg
0.45–0.73 ng/ml [≈1-1.7 nM] Ctrough (concentrazioni dopo 24 h) con 20 mg
1.5–2.4 ng/ml [≈3.5-5.5 nM]
Rivaroxaban:
farmacodinamica regime OD
La concentrazione minima nelle 24 h è sempre
sufficiente a inibire adeguatamente il FXa

• La somministrazione monogiornaliera (OD) si associa a una superiore
concentrazione massima (Cmax) e a una minore concentrazione minima
(Ctrough) rispetto alla somministrazione bigiornaliera (BID), con
sovrapposizione tuttavia degli intervalli di variabilità al 90%.
• La somministrazione OD risulta pertanto simile a quella BID relativamente
alla concentrazione plasmatica (e quindi all’effetto farmacologico), ma più
conveniente per il paziente.
Riv
aro
xa
ba
n C
max
(µg
/l)
Dose giornaliera totale di rivaroxaban (mg) Dose giornaliera totale di rivaroxaban (mg)
Riv
aro
xaban C
max
(µg
/l) Riv
aro
xa
ba
n C
troug
h (µ
g/l) R
iva
roxa
ba
n C
troug
h (µ
g/l)
Studio BID Cmax
Studio OD Cmax
Studio BID Ctrough
Studio OD Ctrough
Dosaggio di rivaroxaban od versus bidin pazienti sottoposti a protesi d’anca
Mueck, Thromb Haemost, 2008

AUC, area under the plasma
concentration-time curve from
0 to 24 hours at steady-state;
Cmax, maximum steady-state
plasma concentration;
Cmin, minimum steady-state
concentration;
QD, once daily;
BID, twice daily
300
250
200
150
100
50
0
ng/m
L
30
QD
60
QD
30
BID
60
BID
30
QD
60
QD
30
BID
60
BID
30
QD
60
QD
30
BID
60
BID
4000
3000
2000
1000
Ng*h
/mL
150
100
50
0
ng/m
L
Cmax, 88 AUC, 88 Cmin, 88
35
30
25
20
15
10
5
0Ble
ed
ing incid
ence, %
30
QD
60
QD
30
BID
60
BID
Edoxaban
Weitz, Thromb Haemost, 2010
I valori a valle piuttosto che al picco sono i migliori indicatori di rischio di sanguinamento

Anche i risultati dello studio di fase II con edoxaban
sostengono la selezione del dosaggio od nella AF
Weitz, Thromb Haemost, 2010
35
30
15
25
20
10
5
0
Dose di edoxaban ed intervallo di dosaggio
Inc
iden
za d
i san
gu
inam
en
to (
%)
30 mg od 60 mg od 30 mg bid 60 mg bid
Dose totale giornaliera
60 mg
Dose totale giornaliera
30 mg
Dose totale giornaliera
120 mg *
*Stopped prematurely by the DSMB
Dati farmacodinamici e clinici
Aspetti pratici (aderenza)
Monosomministrazione
quotidiana: vantaggi

A systematic review of the association between dose
regimens and medication compliance
Claxton, Clin Ther , 2001

0
5
10
15
20
25
La compliance del regime od rispetto al regime bid è
generalmente migliore in condizioni croniche
Numero di studi che valutano direttamente la complianceN
um
ero
di
stu
di
od > bid* od = bid# od < bid‡
* La compliance del paziente (valutata nello studio) con regime od è significativamente migliore rispetto al
regime bid# Nessuna differenza significativa nella compliance del paziente (valutata nello studio) tra regime od e bid‡ La compliance del paziente (valutata nello studio) con regime bid è significativamente migliore rispetto al
regime od
Ricerca Pubmed; Marzo 2001–2011
Barriers to adherence (patients survey):
Forget
Other priorities
Decision to quit dose
Lack of information
Emotional reasons
Improve adherence:
Emphasizing value of regimen
Simple regimen
Adapt regimen to patient´s lifestyle
Quali fattori causano una scarsa aderenza alla
terapia e quali la potrebbero migliorare
Osterberg et al. N Engl J Med 2005;353:487-97; Song et al. Am J Cardiovasc Drugs 2012; 12 (4): 245-253.

93,1
84,9
76,3
86,2
73,8
50,4
0
20
40
60
80
100
Taking Adherence Regimen
Adherence
Timing Adherence
Ad
here
nce (
%)
Once-daily
Twice-daily
Il regime OD è associato a una maggior aderenza alla
terapia
- 6.9 (-11.2,-2.6)
P<0.01- 14.0 (-19.9,-8.1)
P<0.01
- 22.9 (-33.1,-12.7)
P<0.01
Coleman CI et al. Curr Ned Res Opin. 2012;28(5):669-80.
Dosing Frequency
Adherence to Chronic Cardiovascular Disease Medication
Definition of adherenceLess stringent More stringent

Nei pazienti con FA la compliance alla terapia
è migliore con un regime OD rispetto a BID

EHRA Practical Guide, Europace, 2013

I nuovi studi

3030
XANTUS: study design
Interventional observational study in patients with non-valvular AF who are prescribed rivaroxaban under routine treatment conditions to prevent stroke or non-central nervous system
systemic embolism
Rivaroxaban dose and duration of
drug used at discretion of
attending physician
Study population:
patients with non-valvular AF (N~ 6000)
who start treatment
with rivaroxaban to prevent stroke or non-CNS systemic
embolism
Investigators to collect dataat initial visit, at hospital discharge (if
applicable) and quarterlya
N~ 6000
Final visit: 1 yearb
Clinicaltrials.gov NCT01606995
a: protocol does not define exact referral dates for follow up visits or reports (every 3 months recommended)b: in patients discontinuing rivaroxaban before 1 year, the end of observation period is 30 days after last dose

3131
XANTUS: endpoints
Primary endpoints:
• Adjudicated major bleeding events
• Adverse events
Clinicaltrials.gov NCT01606995
Secondary endpoints:
• All-cause mortality
• Adjudicated symptomatic thromboembolic events (collected as adverse events)
• Persistence with rivaroxaban treatment
Anticipated timelines: first patient visit: June 2012
last patient visit: Dec 2014

3232
XALIA: study design
Prospective non-interventional cohort field study to collect real-life data on adverse events, bleeding, thromboembolic events
and mortality in patients diagnosed with acute DVT treated with rivaroxaban or standard of care
Rivaroxaban for ≥ 3 months
Type, dose and duration of drug
used at discretion of attending
physician
Study population:
Pts (N~4800) with
disgnosis of acute DVT
(not PE) and with an
indication for
anticoagulant therapy for ≥ 3 months
Investigators to collect dataat initial visit, at 1 month
and then quarterlya
N~ 2400
N~ 2400
SoC: e.g. initial treatment with LMWH orfondaparinux, followed by VKA for ≥ 3 months Final assessment
(1 month after end oftreatment)
Clinicaltrials.gov NCT01619007
a: protocol does not define exact referral dates for follow up visits

3333
XALIA: endpoints
Primary endpoints:
• Major bleeding events
• Symptomatic recurrent venous thromboembolic events
• All-cause mortality
Clinicaltrials.gov NCT01619007
Secondary endpoints:
• Adverse cardiac events
• Other symptomatic thromboembolic events
• Treatment satisfaction (patient-reported outcomes)
Anticipated timelines: first patient visit: June 2012
last patient visit: Dec 2014

3434
X-PLORER: study design
Prospective multi-center, randomized, heparin controlled dose finding trial to evaluate the efficacy and safety of rivaroxaban
on the background of standard dual antiplatelet therapy to support elective PCI
Rivaroxaban 20 mg1
Study population: patients with
symptomatic CAD undergoing an elective (non
emergent) PCI on one of the two lesions in the
native coronary vessels3
N= 105
Follow up call
Clinicaltrials.gov NCT01442792
1: single dose 2-4 hours before index PCI procedure2: 5 minutes before PCI (after insertion of catheter sheath) until end of PCI procedure3: all patients on stable DAPT≥5 days before PCI procedure
2:2:2:1
R
Rivaroxaban 10 mg1
Rivaroxaban 10 mg1+ UFH 50 IU/kg bolus2
UFH 70-100 IU/kg bolus2
Index
PCI30+7 days

3535
X-PLORER: endpoints
Primary endpoints: anticoagulant effect determined based on percentage of patients who:
• Require ball-out anticoagulant therapy in the context of an ischemic coronary event, and/or
• Experience an angiopraphic flow-limiting thrombotic event, and/or
• Experience thrombus formation on the PCI equipment, and/or
• Experience a procedural myocardial infarction
Clinicaltrials.gov NCT01442792
Secondary endpoints:
• Bleeding events
• Composite of clinical ischemic events up to 30 days after index PCI
• Coagulation profile and plasma concentrations of rivaroxaban
Anticipated timelines: first patient visit: Oct 2011
last patient visit: Q1 2013

3636
X-VERT: study design
Prospective , phase IIIb, randomized, open label, parallel group, active controlled study exploring efficacy and safety of rivaroxaban (20 mg
OD) compared with dose adjusted VKA for the prevention of CV events in patients with NVAF scheduled for cardioversion
Rivaroxaban 20 mg OD1
Study population: patients with
NVAF lasting >48 hours or of
unknown duration and scheduled for
electrical or pharmacologic cardioversion
Follow up callClinicaltrials.gov NCT01674647
1: CrCl 30-49 ml/min:15 mg OD
R
card
iove
rsio
n
Sufficient anti-
coagulation OR
immediate TEE
YES: direct cardioversion
NO: delayed cardioversion
2:1
VKA (INR 2-3)
1-5 days
Rivaroxaban 20 mg OD1
42 days
VKA (INR 2-3)
2:1
R
Rivaroxaban 20 mg OD1
VKA (INR 2-3)
≥21(+4) days(max 56[+4] days)
card
iove
rsio
n
Rivaroxaban 20 mg OD1
42 days
VKA (INR 2-3)
SOC
SOC
SOC
SOC
30 days
30 days
N=1500
3737
X-VERT: endpoints
Primary endpoints:
EFFICACY
• Composite of stroke, TIA, non-CNS systemic embolism, MI, cardiovascular death
SAFETY
• Major bleeding
Clinicaltrials.gov NCT01674647
Secondary endpoints:
• Composite of stroke and non-CNS systemic embolism
• Composite of stroke, TIA, non-CNS systemic embolism, MI and all-cause mortality
• All bleeding events
Anticipated timelines: first patient visit: Oct 2012
last patient visit: Q1 2014

3838
VENTURE-AF: study design
Randomized, open label, active controlled multi-center study to evaluate the safety of rivaroxaban and VKA in subjects
undergoing catheter ablation for atrial fibrillation
Rivaroxaban 20 mg OD
Study population: patients with paroxysmal or
persistent NVAF scheduled to undergo first ever
catheter ablation for their AF
≥ 4 weeks30 ± 5 days
follow up
Clinicaltrials.gov NCT01729871
R
N=250
1:1
VKA (INR 2-3) Cat
het
erab
lati
on
pro
ced
ure
Rivaroxaban 20 mg OD
VKA (INR 2-3)
Day 1 ≥ 4 weeks ≥ 8 weeks

3939
VENTURE-AF: endpoints
Primary endpoints:
•Incidence of major bleeding events 30 ± 5 days after catheter
ablation procedure
Clinicaltrials.gov NCT01729871
Secondary endpoints:
•Incidence of the composite and individual components of myocardial infarction, ischemic stroke, NC-systemic embolism, and vascular death, 30 ±5 days after procedure
Anticipated timelines: first patient visit: end of 2012
last patient visit: Q1 2014

4040
PIONEER AF-PCI: study design
Open label, randomized, controlled, multi-center study exploring two treatment strategies of rivaroxaban and a dose adjusted oral VKA treatment strategy in patients with AF who undergo
PCI
Clinicaltrials.gov: NCT01830543
Rivaroxaban 15 mg OD*#+ clopidogrel
Study population: patients with paroxysmal, persistent or
permanent AF
N= 2100
End of treatment
(12 months)
*: reduced to 10 mg OD in patients with CrCl 30-50 ml/min#: first dose administered 72-96 h after sheath removal§: first dose administered 12-72 h after sheath removal
1:1:1
R
Rivaroxaban 2.5 mg BID§
+DAPTPCI (with
stent placeme
nt
VKA (target INR 2-3)§
+DAPT
Rivaroxaban 15 mg OD*+ low dose ASA
VKA + low dose ASA
Intended DAPT durationOf 1,6 or 12 months

PIONEER AF-PCI: endpoints
4141
Primary endpoints:
• Composite of TIMI major bleeding, minor bleeding and bleeding requiring medical attention (known collectively as clinically significant bleeding at 12 months
Secondary endpoints:
• Separate components of the primary endpoint
• Composite of adverse CV events (cardiovascular death, MI, stroke) at the end of the prespecified duration of DAPT and at month 12
• Stent thrombosis
Anticipated timelines: first patient visit: Apr 2014
last patient visit: Q2 2015
Clinicaltrials.gov: NCT01830543

4242
COMPASS: study design
Randomized, controlled trial of rivaroxaban for the prevention of major CV events in patients with coronary or peripheral
artery disease
Clinicaltrials.gov: NCT01776424
This study will evaluate the efficacy and the safety of rivaroxaban alonecompared with low rivaroxaban+ ASA or ASA alone for the prevention ofmajor adverse cardiac outcomes in patients with established CAD or PAD
• Rivaroxaban: 2.5 mg bid+ ASA 100 mg OD
• Rivaroxaban: 5 mg bid
• ASA: 100 mg od

COMPASS: endpoints
4343
Primary endpoints:
• Composite of CV death, MI and stroke
Secondary endpoints:
• Major bleeding
Anticipated timelines: first patient visit: Feb 2013
last patient visit: Q1 2018
Clinicaltrials.gov: NCT01776424

4444
X-TRA: study design
Open label, international, multi-center, interventional study exploring rivaroxaban for the treatment of a left atrial (LA)/left
appendage (LAA) thrombus in subjects with NVAF or atrial flutter
4444
Study population: patients with NVAF or
atrial flutter with LA/LAA thrombus detected via TEE
Rivaroxaban 20 mg OD1
N~ 60
End of follow up
1: CrCl 15-49 ml/min: 15 mg OD
6-8 weeks
Standard of care
30 days
Clinicaltrials.gov: NCT01839357

4545
X-TRA: endpoints
Primary endpoints:
• The percentage of subjects with complete resolution of left atrial
or left atrial appendage thrombus at the end of treatment
Secondary endpoints:
• Categories of thrombus outcome in subjects: resolved, reduced, unchanged, enlarged or new
• The composite number of stroke and non-central nervous system systemic embolism events
• The number of all bleeding events
Anticipated timelines: first patient visit: May 2013
last patient visit: Jul 2014
Clinicaltrials.gov: NCT01839357

Grazie per l’attenzione

![Single Dose Bioequivalence Study of Two Rivaroxaban Tablet ...€¦ · drug [3], rivaroxaban did not fulfil the waiver criteria for crushed bioequivalence testing. Therefore, after](https://static.fdocuments.in/doc/165x107/5f024c737e708231d403933a/single-dose-bioequivalence-study-of-two-rivaroxaban-tablet-drug-3-rivaroxaban.jpg)
















