
Risks of Death and Stroke in Patients Undergoing ... Atrial fibrillation ... Database (NHIRD)....
31
DOI: 10.1161/CIRCULATIONAHA.115.018294 1 Risks of Death and Stroke in Patients Undergoing Hemodialysis With New- Onset Atrial Fibrillation: A Competing-Risk Analysis of a Nationwide Cohort Running title: Shih et al.; Death and stroke in patients with dialysis and AF Chia-Jen Shih, MD 1,2,3* ; Shuo-Ming Ou, MD 1,4,5* ; Pei-Wen Chao, MD 6,7 ; Shu-Chen Kuo, MD, PhD 1,8,9 ; Yi-Jung Lee , MD 1,10 ; Chih-Yu Yang, MD, PhD 1,4 ; Der-Cherng Tarng MD, PhD 1,4 ; Chih-Ching Lin, MD, PhD 1,4 ; Po-Hsun Huang, MD, PhD 1,11 ; Szu-Yuan Li, MD, PhD 1,4 ; Yung-Tai Chen, MD 1,5,12 1 School of Medicine, National Yang-Ming University, Taipei, Taiwan; 2 Dept of Medicine, Taipei Veterans General Hospital, Yuanshan Branch, Yilan, Taiwan; 3 Deran Clinic, Yilan, Taiwan; 4 Division of Nephrology, Dept of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; 5 Institute of Clinical Medicine, National Yang-Ming University, Taipei, Taiwan; 6 Dept of Anesthesiology, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan; 7 School of Medicine, Taipei Medical University, Taipei, Taiwan; 8 National Institute of Infectious Diseases and Vaccinology, National Health Research Institutes, Miaoli County, Taiwan; 9 Division of Infectious Diseases, Taipei Veterans General Hospital, Taipei, Taiwan; 10 Dept of Neurology, Taipei City Hospital, Ren Ai Branch, Taipei, Taiwan; 11 Division of Cardiology, Dept of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; 12 Division of Nephrology, Dept of Medicine, Taipei City Hospital, Heping Fuyou Branch, Taipei, Taiwan *contributed equally Address Correspondence: Yung-Tai Chen, MD Szu-Yuan Li, MD, PhD Dept of Nephrology Division of Nephrology, Dept of Medicine Taipei City Hospital Heping Fuyou Branch Taipei Veterans General Hospital Taipei, Taiwan, 112 Taipei, Taiwan, 112 Tel: 886-2-2388-9595 Tel: 886-2- 2871 2121 Fax: 886-2-2876-5215 Fax: 886-2- 2871 2121 E-mail: [email protected] E-mail: [email protected] Journal Subject Terms: Epidemiology; Atrial Fibrillation; Arrhythmias; Electrophysiology; Risk Factors Szu-Yuan Li, MD, PhD ; Yung-Tai Chen, MD 1 School of Medicine, National Yang-M ing University, Taipei, Taiwan; 2 Dept of Medicine, Taipei Veterans General Hospital, Yuanshan Branch, Yilan, Taiwan; 3 Deran Clinic, Yilan, Ta a aiw iw iwan an an; ; ; 4 4 4 Di Di Divi v si i ion on on of Nephrology, Dept of Medi di dici ci cin n ne, Ta ipei Veterans Ge G G neral Hospital, Taipei, Ta Ta Taiw iw iwan; 5 In n ns st stitut e of C Cli l ni nical Me Medicine, Nationa l l Y Y Yang -M Ming Un Un Uni i iversity , Taip ei , Taiwan ; 6 De pt of f f Anesthesiol ol olog og o y, W W Wan an an F F Fan an ang g g Ho Ho Hos sp spit t tal l, Ta a aip p p ei M Me e edic c cal al al U U Uni ni niver rsit t ty, T T Tai a a p pei, , , T T Ta aiwa wa wan n; n; 7 7 7 Sc S S ho ho hool ol ol o o of Me Me Medicine, Taipe ei Me ed di ical U U Un n n iversity, , , T Taipe e ei, , , Taiw iw wan; ; 8 8 Na Na Natio o ona al I I Institu u ut e o o of I I Infect ct tio o ous D D Disea a ase es an an and d d Vacc cc cin in inolog og ogy, N N Na at ationa a al l He He Heal al alth th th R R Res es esea ea ar r rch h h Ins n ti i itut t tes, s, s, M M Mia a aol o o i i i Co Co Coun u u t t ty, , , Ta a aiw iw iwan a ; 9 9 9 D D Divi i isi i ion o o of Infe f f t ct cti io ious Dis i i eases, T Taipei Ve Ve V t t terans G G Gener eral H H Hospita l l l, T Tai i ipei, T T Taiwan; 10 1 De t pt pt of f Neur l l ology, T T Tai i ip i i ei C C Ci i ity H H Hospi i it l l al, R R Ren Ai Ai Ai B B Branch h h, T T T i i aipei i i, T T T i i aiwan; 11 11 11 Di Di Di i i vi i i sion of f f C C Ca d d rdi i iol l logy, D D Dept of f f by guest on April 21, 2017 http://circ.ahajournals.org/ Downloaded from by guest on April 21, 2017 http://circ.ahajournals.org/ Downloaded from by guest on April 21, 2017 http://circ.ahajournals.org/ Downloaded from by guest on April 21, 2017 http://circ.ahajournals.org/ Downloaded from by guest on April 21, 2017 http://circ.ahajournals.org/ Downloaded from by guest on April 21, 2017 http://circ.ahajournals.org/ Downloaded from by guest on April 21, 2017 http://circ.ahajournals.org/ Downloaded from by guest on April 21, 2017 http://circ.ahajournals.org/ Downloaded from by guest on April 21, 2017 http://circ.ahajournals.org/ Downloaded from
Transcript of Risks of Death and Stroke in Patients Undergoing ... Atrial fibrillation ... Database (NHIRD)....

DOI: 10.1161/CIRCULATIONAHA.115.018294
1
Risks of Death and Stroke in Patients Undergoing Hemodialysis With New-
Onset Atrial Fibrillation: A Competing-Risk Analysis of a Nationwide Cohort
Running title: Shih et al.; Death and stroke in patients with dialysis and AF
Chia-Jen Shih, MD1,2,3*; Shuo-Ming Ou, MD1,4,5*; Pei-Wen Chao, MD6,7;
Shu-Chen Kuo, MD, PhD1,8,9; Yi-Jung Lee, MD1,10; Chih-Yu Yang, MD, PhD1,4;
Der-Cherng Tarng MD, PhD1,4; Chih-Ching Lin, MD, PhD1,4; Po-Hsun Huang, MD, PhD1,11;
Szu-Yuan Li, MD, PhD1,4; Yung-Tai Chen, MD1,5,12
1School of Medicine, National Yang-Ming University, Taipei, Taiwan; 2Dept of Medicine, Taipei Veterans General Hospital, Yuanshan Branch, Yilan, Taiwan; 3Deran Clinic, Yilan,
Taiwan; 4Division of Nephrology, Dept of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; 5Institute of Clinical Medicine, National Yang-Ming University, Taipei, Taiwan; 6Dept of Anesthesiology, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan; 7School of Medicine, Taipei Medical University, Taipei, Taiwan; 8National Institute of Infectious Diseases
and Vaccinology, National Health Research Institutes, Miaoli County, Taiwan; 9Division of Infectious Diseases, Taipei Veterans General Hospital, Taipei, Taiwan; 10Dept of Neurology,
Taipei City Hospital, Ren Ai Branch, Taipei, Taiwan; 11Division of Cardiology, Dept of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; 12Division of Nephrology, Dept of
Medicine, Taipei City Hospital, Heping Fuyou Branch, Taipei, Taiwan *contributed equally
Address Correspondence:Yung-Tai Chen, MD Szu-Yuan Li, MD, PhD Dept of Nephrology Division of Nephrology, Dept of Medicine Taipei City Hospital Heping Fuyou Branch Taipei Veterans General Hospital Taipei, Taiwan, 112 Taipei, Taiwan, 112 Tel: 886-2-2388-9595 Tel: 886-2- 2871 2121 Fax: 886-2-2876-5215 Fax: 886-2- 2871 2121 E-mail: [email protected] E-mail: [email protected] Journal Subject Terms: Epidemiology; Atrial Fibrillation; Arrhythmias; Electrophysiology; Risk Factors
Szu-Yuan Li, MD, PhD ; Yung-Tai Chen, MD
1School of Medicine, National Yang-Ming University, Taipei, Taiwan; 2Dept of Medicine, Taipei Veterans General Hospital, Yuanshan Branch, Yilan, Taiwan; 3Deran Clinic, Yilan,
Taaaiwiwiwananan;;; 444DiDiDiviv siiiononon of Nephrology, Dept of Medididicicicinnne, Taipei Veterans GeGG neral Hospital, Taipei,TaTaTaiwiwiwan; 5Innnsststitutte e of CClil ninical MeMedicine, , Nationall YYYangg-MMing UnUnUniiiversitytyy, Taipppeie ,,, Taiwann; 6DeD ptofff Anesthesiololologogo y, WWWananan FFFanananggg HoHoHospspspitttall, Taaaipppei MMeeedicccalalal UUUnininiverrsittty, TTTaiaa ppei,,, TTTaaiwawawann;n; 777ScSS hohohoololol ooof MeMeMedicine, Taipeei Meeddiical UUUnnniversity,,, TTaipeeei,,, Taiwiwwan;;; 888NaNaNatiooonaal IIInstituuutte ooof IIInfectcttiooous DDDiseaaasees
ananand dd Vacccccinininologogogy,y NNNaatationaaal l HeHeHealalalththth RRReseseseaeaarrrchhh Insn tiiitutttes,s,s, MMMiaaaoloo i i i CoCoCounuu ttty,, , Taaaiwiwiwana ;;; 999DDDiviiisiiion ooof ffInfeff tctctiioious Disii eases, TTaipei VeVeV ttterans GGGenereral HHHospitat lll, TTaiiipei, TTTaiwan; 101 De tptpt of f Neur llology,
TTTaiiip iiei CCCiiity HHHospiiit llal, RRRen AiAiAi BBBranchhh, TTT iiaipeiii, TTT iiaiwan; 111111DiDiDi iivi iision offf CCCa ddrdiiiolllogy, DDDept offf
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on A
pril 21, 2017http://circ.ahajournals.org/
Dow
nloaded from
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on A
pril 21, 2017http://circ.ahajournals.org/
Dow
nloaded from
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on A
pril 21, 2017http://circ.ahajournals.org/
Dow
nloaded from
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on A
pril 21, 2017http://circ.ahajournals.org/
Dow
nloaded from
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
2
Abstract
Background—Whether oral anticoagulant (OAC) use should be considered in patients
undergoing hemodialysis with atrial fibrillation (AF) remains controversial due to uncertainty
regarding risk-benefit assessments. The purpose of this study was to investigate the risk of
ischemic stroke in patients undergoing hemodialysis with new-onset AF, compared with those
without arrhythmia.
Methods and Results—This nationwide, population-based, propensity score-matched cohort
study used data from Taiwan’s National Health Insurance Research Database during 1998–2011
for patients on hemodialysis with new-onset non-valvular AF and matched subjects without
arrhythmia. The clinical endpoints were ischemic stroke (fatal or non-fatal), all-cause death, and
other serious adverse cardiovascular events. Compared with the matched cohort, patients with
AF (n = 6,772) had higher risks of ischemic stroke (adjusted hazard ratio [aHR] 1.27, 95%
confidence interval [CI] 1.13–1.43), all-cause death (aHR 1.59, 95% CI 1.52–1.67), in-hospital
cardiovascular death (aHR 1.83, 95% CI 1.71–1.94), myocardial infarction (aHR 1.33, 95% CI
1.17–1.51), and hospitalization for heart failure (aHR 1.90, 95% CI 1.76–2.05). After considering
in-hospital death as a competing risk, AF significantly increased the risk of heart failure (HR
1.56, 95% CI 1.45–1.68), but not those of ischemic stroke and myocardial infarction.
Additionally, the predictive value of the CHA2DS2 –VASc score for ischemic stroke was
diminished in the competing risk model.
Conclusions—The risk of stroke was only modestly higher in patients undergoing hemodialysis
with new-onset AF than in those without AF, and it became insignificant when accounting for the
competing risk of in-hospital death.
Key words: epidemiology; lipids; population; risk factor
other serious adverse cardiovascular events. Compared with the matched cohort, papapatititienenntststs wwwititith h h
AF (n = 6,772) had higher risks of ischemic stroke (adjusted hazard ratio [aHR] 1.1 272727, 959595% % %
confidence interval [CI] 1.13–1.43), all-cause death (aHR 1.59, 95% CI 1.52–1.67), in-hospital
carddioioiovavavascscscululularaa dddeaeaeath (aHR 1.83, 95% CI 1.71–1.1..949494),)) myocardial infarctctctioioion (aHR 1.33, 95% CI
1...1777–1.51), ananand d hohohospppitititalalalizizizatatation n n fofoforrr heheeararart tt faaailililururure (aaHHHR 1.9.9.90,0,0, 9995%%% CCCIII 1.1.1 767676–2–– .05)5)5)... AfAfAftett r cococonsnsn idididererering
nnn-hhhospital deathhh aas a cccoompeeetiiinngn risk, AFAAF sigggnninificaannntly iiincncncrerereasssed thhhe riskkk of heheheart fafaaillluuuree (HHHR
1.565656,,, 959595%%% CICICI 1.4.4.45–––1.1..686868),),), bututt nnnototot ttthohoh seee ooofff isisischhchemememiiic ssstrtrrokokokeee aana d d d mymymyocococararardddialalal infnfnfarararctctctioioionnn.
AdAdAddididitititionononalalallylly, thththeee prprpredededicicictititiveeve valalalueeue ooofff thththeee CHCHCHAAA2DSDSDS2 –VAVAVAScScSc ssscococorerere fffororor iiiscscschehehemimimiccc stststrororokekeke wasasas
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
3
Introduction
Atrial fibrillation (AF) is an increasing prevalent heart rhythm disorder1-3 for patients with end-
stage renal disease (ESRD) undergoing hemodialysis, and associated with adverse outcomes and
death in these patients.4-6 Given the routine administration of heparin during hemodialysis and
the bleeding tendency associated with ESRD, reports about whether the risk of thromboembolic
stroke is notably higher in patients undergoing dialysis with AF than in those without AF remain
inconsistent.7-9
Current American College of Cardiology/American Heart Association AF guidelines10 do not
provide strong recommendations for patients with non-valvular AF undergoing dialysis; they
suggest only the consideration of warfarin prescription for those with higher stroke risk
(CHA2DS2-VASc 2), based on limited findings from observational studies.11 However, recent
large-scale registry studies12-16 involving patients with AF undergoing dialysis found that
warfarin use was insignificantly or positively associated with ischemic stroke, major bleeding
events, and mortality. These controversial findings have raised concern about the actual clinical
impact of AF-related cardioembolic events in patients undergoing dialysis, especially as the
perceived risk of death is considerably higher than the risk of stroke in these patients. Death is a
potential competing risk for stroke, as many patients on dialysis may die before initial stroke;
this issue has not been fully addressed,8, 17, 18 and previous studies likely overestimated the true
excess stroke risk. In addition, these studies have been limited primarily by small samples, and
prevalent cohort biases (i.e., AF diagnosed before dialysis). Thus, taking advantage of
nationwide data from Taiwan, we evaluated the actual risk of incident ischemic stroke in patients
on dialysis with new-onset AF, compared with a propensity score–matched cohort without
arrhythmia, with consideration of the competing risk of death.
uggest only the consideration of warfarin prescription for those with higher strokekeke rrrisisisk k k
CHA2DS2-VASc 2), based on limited findings from observational studies.11 However, recent
arggge-e-e-scscscalalale e e rereregistttryyy studies12-16 involving patientttss s wiww th AF undergoing dddiaiaialysis found that
wwwarrrfarin use wasasas innssigigignininififificacacantntntlylyly ooor popop siss ttivelylyly aassoociiiateeed d d wiwiwiththth iscscscheeemimimiccc sttrokekeke,, , mamamajojojor rr blblbleeeeeedididingngng
evvvenenentstt , and momm rtttalllity. Thheh see cononontrovovoverrssis aala ffininindddingggs hhhaveveve raiiisesesed d cocoonnncerere n abbouuut ttthe aaactctctuual cllinicccall t
mmmpapapactctct ooofff AFAFAF rr-relelelatatatededed cccararardididioeoeoembmbmbolololicicic eeeveeventntntsss ininin pppaaatititienenentststs undndndererergogogoinininggg dididialalalyssysisisis, esesespepepecicicialalallylly aaasss thththeee
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
4
Methods
Data Source
For this retrospective population-based cohort study, we retrieved all medical records of patients
with ESRD undergoing chronic dialysis from Taiwan’s National Health Insurance Research
Database (NHIRD). Taiwan’s National Health Research Institutes (NHRI) released the NHIRD
for research purposes, with data encrypted to protect privacy. The national health insurance
(NHI) program offers comprehensive medical care coverage to more than 99% of the country’s
population of 23 million people. All information on clinical visits, hospitalization, and prescribed
drugs is included in the NHI system. We have described the NHIRD in detail in previous
works.19, 20 Disease diagnoses for all individuals were classified according to the International
Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). The Institutional
Review Board of Taipei City Hospital exempted this study from full review (TCHIRB-1030407-
W) because the sample comprised de-identi ed secondary data.
Study Cohort
All patients aged 20 years with ESRD undergoing maintenance hemodialysis between 1
January 1998 and 31 December 2011 were identified. ESRD diagnoses were confirmed by ICD-
9-CM code 585 and inclusion in the NHIRD’s catastrophic illness dataset. According to NHI
rules, only patients with ESRD undergoing chronic dialysis can be registered in this dataset.
Based on internal report of Taiwan Society of Nephrology, unfractionated heparin, the most
widely used anticoagulant in Taiwan, was usually administered as a bolus at the start of dialysis
(1000–3000 U) followed by a continuous infusion (500–1000 U per hour) until 15 to 60 minutes
before the end of dialysis.21, 22
The AF cohort comprised all patients with ESRD and incident AF after dialysis. The
works.19, 20 Disease diagnoses for all individuals were classified according to the IIIntntntererernananatititionononalalal
Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). The Institutional
Reviviiewewew BBBoaoaoardrdr of f f TaTT ipei City Hospital exempteddd ttthihihis study from full reviviviewee (TCHIRB-1030407-m
WWW) because thehee sssammmplplple cococompmpmpriririssesed dd dedede-i-i-ideenttiii eeed seecoondadadarryry dddaaata.a
Stttudududy y y Cohooortrtr
AlAlAllll papapatititienenentststs aaagegegeddd 222000 yeeyearararsss wiiwiththth EEESRSRSRDDD unnundededergrgrgoioioingngng mmmaiaiaintntntenenenananancecece hhhemememodododiaiaialyllysisisisss bebebetwttweeeeeennn 111
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
5
index date was defined as the date of AF diagnosis. To ensure accuracy, the diagnosis of AF was
established based on one inpatient or two outpatient records of ICD-9-CM code 427.31 in the
database, which has been validated.23-25 As the main aim of the present study was to investigate
the risk of ischemic stroke in patients undergoing dialysis with new-onset non-valvular AF, we
excluded patients with diagnoses of AF before dialysis and those with histories of valvular heart
disease. Patients without arrhythmia were included in the control cohort. Index dates for subjects
in the control cohort were randomly assigned and corresponded to those of patients in the AF
cohort, and the same exclusion criteria were applied to both cohorts.
Baseline Characteristics and Score Calculation
For each subject, information on baseline demographic characteristics, including age, gender,
monthly income (NT$ <19,100, 19,100 41,999, and 42,000), urbanization level and dialysis
vintage (i.e. time between onset of ESRD and index date), were extracted. Urbanization levels in
Taiwan are divided into four strata according to the NHRI, with level 1 corresponding to the
most urbanized and level 4 corresponding to the least urbanized areas. The Charlson
Comorbidity Index (CCI) score was used to determine overall systemic health. Each increase in
score indicates a stepwise increase in cumulative mortality.26 Other systemic diseases and risk
factors for cardiovascular disease not included in the CCI were also examined; these included
hypertension, prior major bleeding, alcohol or drug use history, and dyslipidemia. Concomitant
mediation data associated with the outcomes of interest, including data on use of alpha blockers,
beta blockers, calcium channel blockers, diuretics, angiotensin-converting enzyme inhibitors,
angiotensin II receptor blockers, other anti-hypertensive drugs, anti-hyperglycemic drugs,
aspirin, clopidogrel, ticlopidine, dipyridamole, nitrate, statins, proton pump inhibitors, and
nonsteroidal anti-inflammatory drugs, were extracted. The CHA2DS2-VASc score was calculated
For each subject, information on baseline demographic characteristics, including aaagegege, gegegendndndererer,
monthly income (NT$ <19,100, 19,100 41,999, and 42,000), urbanization level and dialysis
vintttagagagee e (((iii.e.e.e. titt meee bbbetween onset of ESRD and indndnde ), were extracteteteddd. Urbanization levels inxxx date
TTTaiwwwan are divvidididedd iiintntntooo fofofoururur ssstttrar tatata aaaccccorrdingngg tto thhee NHHHRRRI, wwwith hh leleevel l 111 ccorrresesespppondndndinining gg totto ttthehehe
momoosttt uuurbannizizizedee aaanndn leevveele 4 cccorororrererespspsponoo dddingngng tttooo tthhehe leaeaeast uuurbrbrbanannizzzededed arrereasasa . ThThThe ChChCharaa lsononon
CCComo bbrbidididiitity IIIndddex (C(C(CCICICI))) score was us dded to dddetermiiine over llallll systemiiic hhhealltlthhh. EEEachhh iiincrease iiin
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
6
for each patient by adding 1 point each for age between 65 and 74 years, history of hypertension,
diabetes, congestive heart failure, vascular disease (myocardial infarction or peripheral artery
disease), and female sex; and 2 points each for history of stroke/transient ischemic attack and age
75 years. The CHADS2 score was calculated for each patient by adding 1 point each for history
of congestive heart failure, hypertension, diabetes, and age 75 years; and 2 points for history of
stroke/transient ischemic attack.
Propensity score matching
Given the differences in baseline characteristics and risk of cardiovascular disease between the
AF and control cohorts, we used 1:1 propensity score matching and calculated propensity scores,
which predicted the probability of AF occurrence conditional on baseline covariates, by
multivariable logistic regression (Supplementary Table 1). We attempted to match each patient in
the AF cohort with a patient in the control cohort with a similar propensity score, based on
nearest-neighbor matching without replacement, using a caliper width equal to 0.1 of the
standard deviation of the logit of the propensity score.
Outcomes
The primary outcome was hospitalization or death with a principal diagnosis of ischemic stroke
(ICD-9-CM code 433.x, 434.x, or 436). The secondary outcomes were all-cause death, in-
hospital cardiovascular death, and hospitalization or death for hemorrhagic stroke (ICD-9-CM
code 431 or 432), myocardial infarction (ICD-9-CM code 410.x), or heart failure (ICD-9-CM
code 428.x). The accuracy of stroke and myocardial infarction diagnoses recorded in the
database has been validated with a positive predictive value of 88.4 to 94% and 92%
respectively, and a negative predicted values of these diagnoses have been reported to be over
90%.27-29 All subjects were followed until death or 31 December 2012.
which predicted the probability of AF occurrence conditional on baseline covariatatateseses, bybyby
multivariable logistic regression (Supplementary Table 1). We attempted to match each patient ina
he AFAFAF cccohohohororort t wiiiththth a patient in the control cohorrrtt t wiwiw th a similar propennnsisisitytt score, based on
nnnearararest-neighbh ororor mmatatatcchchininingg g wiwiwithththououut tt rerr plpp aacemmmeenent, uusiing g g a a a cacaalililippeper r wiwiwidtdtdth hh eqeqe ual tototo 000.1.1.1 ooof thththe
tttaanandadad rd devvviaiaiationonon of thththe logggiti ooof thhhe ee prrropopopennnssittyty scocoore..
OOuOutctctcomomomeseses
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
7
Statistical Analysis
Descriptive statistics were used to characterize baseline demographic and clinical variables of the
study cohort. Standardized differences were used to check for balance between the AF and
control cohorts after matching. Propensity scores for the likelihood of AF occurrence were
determined by multivariate logistic regression analysis, conditional on baseline covariates
(Supplementary Table 1). The incidence rates of outcomes of interest in the two groups were
calculated using Poisson distribution. Adjusted hazard ratios (aHRs) and 95% confidence
intervals (CIs) were calculated for the outcomes of interest in each group. Warfarin use was
calculated as a time-varying covariate. Due to the high mortality rate in patients with ESRD,
competing-risk regression using Fine and Gray’s model was also performed.30 In-hospital death
that is not part of the outcome of interest was the competing risk. Given lack of data from
autopsies to characterize the exact cause of out-of-hospital death, out-of-hospital death was not
regarded as the competing risk for respective mortality outcomes of interest to ensure accuracy.
To validate the robustness of our results, we performed sensitivity analyses including Cox
regression models adjusted for propensity scores in quintile before propensity score matching
and different stroke risk stratification by CHA2DS2-VASc score. The SQL Server 2012
(Microsoft Corporation, Redmond, WA, USA) was used for data linkage, processing, and
sampling. Propensity scores were calculated using SAS version 9.3 (SAS Institute, Cary, NC,
USA). All other statistical analyses were conducted with STATA statistical software (version
12.0; StataCorp, College Station, TX, USA). Statistical significance was defined as two-sided P
< 0.05.
competing-risk regression using Fine and Gray’s model was also performed.30 In---hohohospspspitititalalal dddeaeaeathtt
hat is not part of the outcome of interest was the competing risk. Given lack of data from G
autoopspspsieieies ss tototo cccharraractcc erize the exact cause of out-oooff-f-hohh spital death, out-ooofff-hohh spital death was not
eeegaaarded as thhe ee cocc mpmpmpeeetininingg g rrrisksksk fffororor rrresese peppectivivivee mmmorrt . aaality y y oououtctctcomomomeseses ooofff ininintteterrest ttto o o enenensususurerr aaaccccccurururacacacyyy
ToToo vvvalaa idate thththe roorobbub sttneneness ooff f ououour reeesssultltts,,, weee ppeperfoormmemeddd sess nsnsnsitttivvvittty annnalysysyses iiincccludiiingngng Coxxx
eeegrgrgresesessisisiononon mmmodododelelelsss adadadjujjustststededed fffororor prprpropopopenenensisisitytty ssscococorereresss ininin qqquiiuintntntililileee bebebefofoforerere ppprororopepepensnsnsititity scscscorororeee mamamatctctchihihingngng
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
8
Results
Characteristics of the Study Population
For the study period of January 1998 to December 2011, a total of 6,772 patients with ESRD and
AF and 70,625 control subjects met the inclusion criteria (Supplementary Figure 1). The mean
age of the AF cohort was 68.8 ± 11.3 years, and the majority (53.2%) of patients were female.
The median timing of AF occurrence was 38 (quartiles 13–76) months after ESRD. The mean
CHA2DS2-VASc score was 4.8 ± 2.2. A total of 566 patients (8.4%) used warfarin during the
follow-up period. After propensity score matching, we identified 6,494 patients with AF and
6,494 matched controls with similar baseline characteristics. Detailed demographic information
for these cohorts is provided in Table 1.
Long-Term Risks of Ischemic Stroke and Adverse Cardiovascular Events
During the follow-up period (mean [standard deviation] years: 3.2 [2.7]; median [quartiles] years:
2.3 [1.3–4.4]), the AF cohort had higher risks of ischemic stroke (aHR 1.27, 95% CI 1.13–1.43),
all-cause death (aHR 1.59, 95% CI 1.52–1.67), in-hospital cardiovascular death (aHR 1.83, 95%
CI 1.71–1.94), myocardial infarction (aHR 1.33, 95% CI 1.17–1.51), and heart failure (aHR 1.90,
95% CI 1.76–2.05) compared with the matched non-AF cohort (Table 2). However, after adjusting
for in-hospital death from causes other than outcomes of interest as a competing risk, AF was
associated significantly only with in-hospital cardiovascular death (HR 1.65, 95% CI 1.55–1.76)
and heart failure (HR 1.56, 95% CI 1.45–1.68), but not those of ischemic stroke and myocardial
infarction. Sensitivity analyses conducted before propensity score matching (Table 2) and
stratified by different stroke risk according to CHA2DS2-VASc score (Supplementary Table 2)
yielded consistent results.
Association between CHA2DS2-VASc Score and Risks of Ischemic Stroke and Death in
for these cohorts is provided in Table 1.
Long-Term Risks of Ischemic Stroke and Adverse Cardiovascular Events
Duririingngng ttthehehe fffoloo low-w-w-up period (mean [standard deeviviviatatation] years: 3.2 [2.7]7]]; memm dian [quartiles] years
222.3 [1.3–4.4])), thththe AFAFF cohohohororort t t hahahaddd hihihighghgherere riskskk of iscscchemimimiccc stststrororokekek (aHaHaHR RR 1.27,, 959595%%% CICICI 11.1.1.13–––11.1 434343),
allll-l-l-cacacause deeatatath h (aa(aHHRH 111.5559, 9995%5%5% CI I I 111.5552––1– .6667))), , in-hhhospipipitttal cacacardrddiooovvavascscsculllarr ddeeeatthth (aHHHRRR 1.83, 95%%
CICICI 111 77.7111–111.949494))), mmmyooyocacacardrdrdiaiaialll inininfafafarcrcrctititiononon (((aHaHaHRRR 111.333333, 959595%%% CICICI 111 11.1777–111.515151))), aaandndnd hhheaeaearrrttt fafafailililurrureee (a(a(aHRHRHR 111 99.90000
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
9
Patients on Hemodialysis with new-onset AF
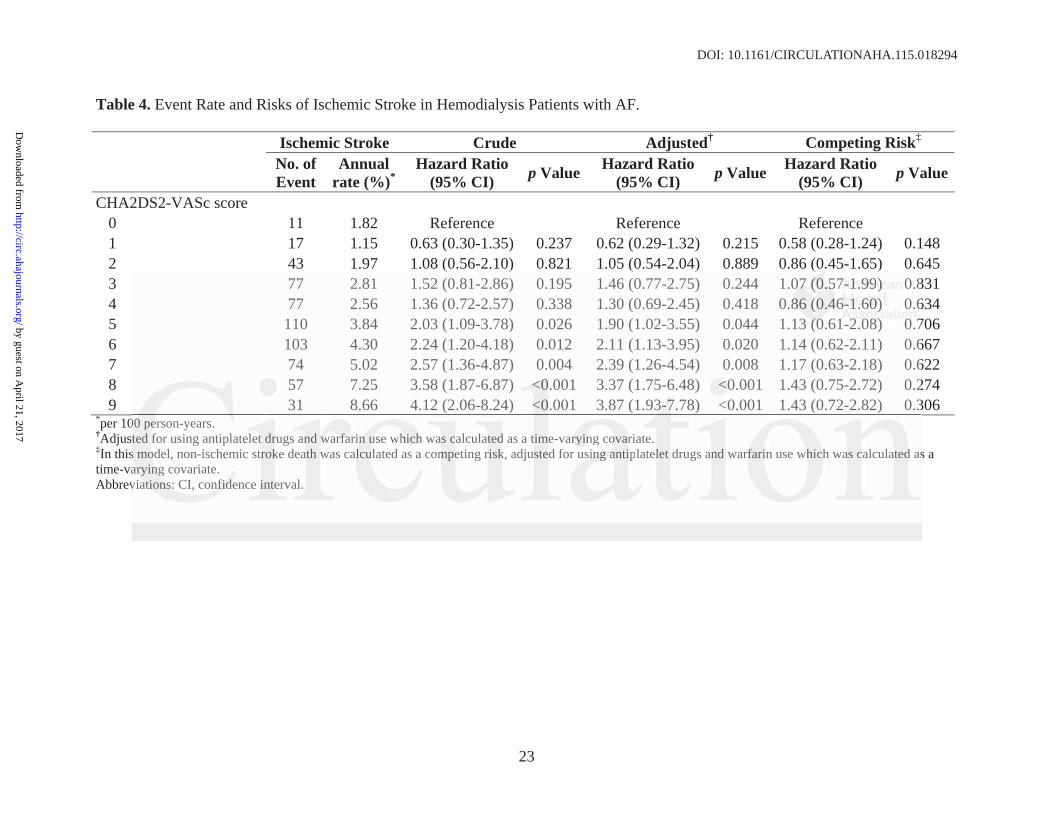
Of 6,772 patients with AF, 600 patients experienced ischemic stroke (3.35 per 100 person-years)
and 4,642 patients died (24.7 per 100 person-years) during the follow-up period. The annual risks
of ischemic stroke and all-cause death were 1.82% and 10.03%, respectively, for patients with a
CHA2DS2-VASc score of 0 and 8.66 % and 63.10 %, respectively, for those with a CHA2DS2-
VASc score of 9 (Table 3). Annual stroke and death rates according to CHADS2 score were also
shown in Table 3. In the Cox model, warfarin use was not associated with reducing stroke (aHR
1.24, 95% CI 0.91–1.69). CHA2DS2-VASc score showed good predictive ability for ischemic
stroke (Harrell's c statistic = 0.622). CHA2DS2-VASc scores 3 increased the risk of ischemic
stroke relative to scores of 0, although the difference was significant only for CHA2DS2-VASc
scores 5 (aHR 1.90, 95% CI 1.02–3.55 for score 5; aHR 2.11, 95% CI 1.13–3.95 for score 6;
aHR 2.39, 95% CI 1.26–4.54 for score 7; aHR 3.37, 95% CI 1.75–6.48 for score 8; aHR 3.87, 95%
CI 1.93–7.78 for score 9). However, when in-hospital death was treated as a competing risk in the
Cox model, higher CHA2DS2-VASc score was not associated with an increased risk of ischemic
stroke (Table 4).
Discussion
In this analysis of a large “real-world” contemporary nationwide cohort, we found that patients
undergoing hemodialysis with new-onset AF have a high incidence of ischemic stroke,
cardiovascular and all-cause death, and other serious adverse cardiovascular events (myocardial
infarction and heart failure). However, compared with the matched cohort without arrhythmia,
patients with AF had only a modestly (1.3-fold) higher risk of ischemic stroke, which became
insignificant after accounting for the competing risk of in-hospital death. The predictive value of
troke relative to scores of 0, although the difference was significant only for CHAHAA222DSDSDS222-V-V-VASASASccc
cores 5 (aHR 1.90, 95% CI 1.02–3.55 for score 5; aHR 2.11, 95% CI 1.13–3.95 for score 6;
aHR R R 2.2.2.393939, , , 959595% CICICI 1.26–4.54 for score 7; aHR 3.3.3.373737, 95% CI 1.75–6.488 fffooor score 8; aHR 3.87, 95
CCCI 111.93–7.78 fororor scooorerere 999).).) HHHowowowevevvererr,,, wwhw een iiinn-n hhoh sppitttal dededeatatath hh wawawas trrreaeaeateteteddd aas a cococompmpmpetetetininingg g iriisksksk iiin nn thtt
CoCoox momm del,l,, hhhigi hheh rr r CHHHAAA2DSSS222-V-VVASSSccc scccorrre wwwasss not aaassoooccciattededed wwwititthhh aan nn innnccreaaasesesed dd riskskk oof iisccchemmmicc hh
tttrororokekeke (((TaTaTablblbleee 444))).
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
10
the CHA2DS2 –VASc score for ischemic stroke was also diminished in analyses considering the
competing risk of in-hospital death.
The incidence of ischemic stroke in patients on dialysis with new-onset AF was lower in the
present study (3.28/100 person-years) than in a Danish study17(5.61/100 person-years) of 901
patients undergoing dialysis with AF, including outcomes of mild stroke or transient ischemic
attack, and in a population-based study2 (9.9/100 person-years) using United States Renal Data
System (USRDS) data from 1995–2007, including patients of older age (mean age 75.9 years).
Overall, stroke rates according to CHADS2 score for patients with AF in our study were
comparable with the findings from Dialysis Outcomes and Practice Patterns Study15,but not as
high as that observed in non-dialysis general population with AF31, 32, which implicitly assumed
that AF had less impact on stroke risk in dialysis population as it did in general population. Most
notably, the USRDS data2 indicated that more than 60% of patients on dialysis with incident AF
died before the occurrence of stroke. In Danish national registries of patients on dialysis who
were discharged with a diagnosis of AF, the death rate (29.35/100 person-years) was more than
five-fold higher than the stroke rate during the follow-up period.17 These findings are similar to
those of the present study, suggesting that the risk of death overwhelms the risk of AF-related
stroke in patients undergoing dialysis. Also, Murray et al.7 reported that AF appeared not to
aggravate the risk of incident stroke in US Medicare-insured patients on dialysis. Overall, the
discrepancy that exists between competing and non-competing risk analyses in our study could
be attributed to high mortality rate in patients on dialysis with incident AF and majority of them
who died before a stroke. In addition to the competing risks between death and stroke, another
proposed explanation may be reduced risk of thrombus formation or embolization, and even
subsequent stroke due to systemic heparinization during dialysis sessions.
high as that observed in non-dialysis general population with AF31, 32, which implllicicicitititlylyly aaassssssumumumedee
hat AF had less impact on stroke risk in dialysis population as it did in general population. Most
notaaablblbly,y,y, ttthehehe UUUSRRRDSDD data2 indicated that more thahahannn 606 % of patients on dididialaa ysis with incident AF
ddidieddd before thhe e ooco ccuurrrrrrennncecece ooof f f stststrorookekeke. InInIn DDannnissshh naatiionaaalll rrregigigissstririiesee ooofff papapatieentsss ooonnn dididialalalysysysisisis wwwhohoho
weweereee discharararggeg d wwiw th aa diagngnnosososisi ooof f f AFFF, the e e deeeathh raaate e (2229.33535/1/1100000 pppererersooonn-yeaeaearsrsrs) ) waaas s s mooreee thaaann
fififiveeve ff-folololddd hihihighghghererer ttthahahannn thththeee stststrororokekeke rrratatateee dudduririringngng ttthehehe fffololollololow-uppup ppperererioioioddd.1717 TTThehehesesese fffininindididingngngsss ararareee sisisimimimilalalarrr tototo
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
11
By contrast, other studies8, 9, 33 showed that AF increased the risk of ischemic stroke 3.1–
9.8-fold in patients undergoing dialysis, resulting in a higher stroke risk than observed in our
study. However, the results of these studies must be interpreted cautiously due to selection bias
(single centers), small samples, uncontrolled baseline risk of stroke, and lack of adjustment for
the competing risks of stroke and death. Although correspondence between a higher CHA2DS2 –
VASc score and a higher risk of stroke in patients with ESRD was observed in the present cohort
and by Chao et al.,34 no such relationship was found after accounting for the competing risk of
death, which further strengthens our results. Thus, our findings better reflect the real estimated
risk of ischemic stroke in a nationwide, unselected dialysis population. We demonstrated that
new-onset AF did not amplify stroke risk in this population to a greater extent than previously
expected. Our findings may indirectly explain the unsatisfactory outcome of warfarin treatment
in patients on dialysis with AF in most recent studies.12-16 However, we need to acknowledge that
the efficacy of warfarin treatment for stroke prevention in dialysis patients with AF is beyond the
scope of the present study due to unavailable information about warfarin use in our claims
database, such as adherence to prescribed warfarin and therapeutic values of international
normalized ratio that may confound the estimation of stroke risk.16 Thus, further prospective
randomized trials are warranted to clarify this issue.
Some limitations of our study should be addressed. First, because of its observational
nature, bias due to unmeasured confounding could not be completely ruled out, although we used
propensity score–matched analysis to balance major baseline comorbidities associated with
stroke occurrence between cohorts. Second, the precision of the disease diagnoses, which was
based on ICD-9-CM code from administrative data reported by physicians, may be a concern
although diagnostic accuracy of main events of interest such as atrial fibrillation23-25, stroke27, 28
new-onset AF did not amplify stroke risk in this population to a greater extent thaaannn prprprevevevioioiousususlylyly
expected. Our findings may indirectly explain the unsatisfactory outcome of warfarin treatment
n pppatatatieieientntnts s s ononon diaaalylylysis with AF in most recent stuuudididieees.12-16 However, weee nnneed to acknowledge tha
hhhe efficacy of wwwarrfararariinin tttrerereaatatmemementntnt fffooor ssstrr kokke ee prrreveentttionnn iiinnn dididialaa ysysisi pppatatatieieientts wiwiwiththth AAAF F F isii bbbeyeyeyononond dd thththe
cccopopopeee of theee pppresses nntn stttuddyd duuue totot uuunanan vavaailllablelele iiinformmmatititioonon aaaboboboutuu wawawarfrffara iiin useee iiinnn ourrr ccclaimsmm
dadadatatatabababasesese, sussuchchch aaasss adadadheheherererencncnceee tototo ppprererescscscririribebebeddd waawarfrfrfarararininin aaandndnd tttheheherararapepepeuttuticicic valalalueeuesss ofofof iiintntntererernananatititionononalalal ffff
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.115.018294
12
and myocardial infarction29 and other important covariates such as diabetes35 or hypertension27,
has been validated. Third, the cause of out-of-hospital death may be variable and uncertain
without autopsy confirmation, whereas it is very unlikely to perform autopsies on patients with
ESRD because they are more likely to die of cardiovascular disease. According to one Japanese
study of 93 autopsied chronic dialysis patients, there were only 5.7% of out-of-hospital deaths
due to ischemic stroke.36 Thus, this confounding may less bias the risk estimate of ischemic
stroke than expected. Besides, while all out-of-hospital deaths were excluded from competing
risk mortality outcome for ischemic stroke as our main analysis, the potential misclassification
(i.e. non-ischemic stroke related out-of-hospital deaths) would lead the estimated HR for
ischemic stroke away from the null in the competing-risk analysis and further strengthen our
main findings. Fourth, we could not include some patient data (including body weight, smoking,
alcohol consumption, and physical activity) or heparin use during hemodialysis in the adjusted
analysis because the NHIRD does not contain these data. Fifth, underestimation of true incidence
of AF was possible in our national registry cohort in which ambulatory arrhythmia monitoring
(24-hour Holter monitoring or cardiac event recorders) was not routinely performed for every
patient. However, our estimates of the incidence of new-onset AF are similar to that of previous
studies2, 15 and, therefore, support that the underestimation may be minimal. Besides, given that
the true incidence of AF and subsequent stroke risk would be less biased on low-risk patients
than high-risk patients, we further stratified the cohort into low-risk (0-1) and high-risk ( 2)
groups by CHA2DS2-VASc score. The result remained consistent in the low-risk group in
addition to the high-risk group. Thus, we believed that this underestimation was less likely to
influence the robustness of our results. Additionally, we could not specify AF type (paroxysmal
or non-paroxysmal), which was also not recorded in the database, but the risks of stroke and
schemic stroke away from the null in the competing-risk analysis and rrr further streeengngngthththenenen oooururur
we could not include somain findings. Fourth, me patient data (including body weight, smoking,
alcoohohohol l l cococonsnsnsumuu ptptptioioion, and physical activity) or hhhepepepaaarin use during hemodododialysis in the adjusted
anananalalalysis becausesese thhee NNNHIHIHIRDRDRD dddooeoesss nnonottt coonttaiaiainnn theseee daaatatata. FiFiFiftftfth, uuundndnderereresesestiimatititiononon ooof f f trtrtrueuee incncncidididenenence
offf AAAF FF was popoposssibbbleee in ouuur naaatitt onononal rrreeegiiisttrtry y cccohhhort innn whwhwhiiich h ammmbububulaaatoooryry arrrhyhyythhhmia a a mmmonnitoooringngg
222444-hohohourrur HHHolololteteterrr momomonininitototoririringngng ooorrr cacacardrdrdiaiaiaccc eveevenenenttt rererecococordrdrdererers)s)s) wasasas nnnototot rrrouooutititinenenelylly ppperererfofoformrmrmededed fffororor eeeveeveryrry
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
13
survival do not differ between patients with paroxysmal and non-paroxysmal AF.9, 37, 38 Last,
whether the underlying cause of ischemic stroke is AF-related thromboembolism or
atherosclerosis and thrombosis of the cerebral artery is not available, whereas neither other
prospective clinical trials had this information.39, 40
Conclusions
The risk of stroke was only modestly higher in this contemporary population of hemodialysis
patients with new-onset AF than in those without AF, and the risk became insignificant after
adjustment for the competing risk of in-hospital death. Thus, the net clinical benefit of stroke
prevention for patients on dialysis with AF needs to be re-evaluated, especially considering the
impact of the high mortality burden. Of note, our results emphasize the need to re-prioritize the
list of AF-related comorbidity risk estimates, especially with targeting of the outcome of death.
Acknowledgments: This study was based in part on data from the NHIRD provided by Bureau
of National Health Insurance (BNHI) of the Department of Health and managed by the NHRI.
The conclusions presented in this study are those of the authors and do not necessarily reflect the
views of the BNHI, the Department of Health, or the National Health Research Institute.
Conflict of Interest Disclosures: None.
References:
1. Winkelmayer WC, Patrick AR, Liu J, Brookhart MA, Setoguchi S. The increasing prevalence of atrial fibrillation among hemodialysis patients. J Am Soc Nephrol. 2011;22:349-57. 2. Goldstein BA, Arce CM, Hlatky MA, Turakhia M, Setoguchi S, Winkelmayer WC. Trends in the incidence of atrial fibrillation in older patients initiating dialysis in the United States. Circulation. 2012;126:2293-301. 3. Liao JN, Chao TF, Liu CJ, Wang KL, Chen SJ, Lin YJ, Chang SL, Lo LW, Hu YF, Tuan TC,
prevention for patients on dialysis with AF needs to be re-evaluated, especially conononsisisidededeririringngng ttthehehe
mpact of the high mortality burden. Of note, our results emphasize the need to re-prioritize the
ist ooofff AFAFAF-r-r-relelelataa eddd cccomorbidity risk estimates, espppecececiiially with targeting ofofof the outcome of death.
AcAcAcknknknowledgdgdgmmementntnts: ThThThis stuuudydydy wasasas baaaseede iiinnn ppapart onn dddattta fffrrrommm ththheee NHNN IRIIRD prprprooovidededed byy y BBBureauu a
of National Health Insurance (((BNHI))) of the Depapp rtment of Health and managgged by yy the NHRI.
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
14
Chung FP, Chen TJ, Chen SA. Incidence and risk factors for new-onset atrial fibrillation among patients with end-stage renal disease undergoing renal replacement therapy. Kidney Int. 2015;87:1209-15. 4. Genovesi S, Vincenti A, Rossi E, Pogliani D, Acquistapace I, Stella A, Valsecchi MG. Atrial fibrillation and morbidity and mortality in a cohort of long-term hemodialysis patients. Am J Kidney Dis. 2008;51:255-62. 5. Vázquez E, Sánchez-Perales C, Borrego F, Garcia-Cortés MJ, Lozano C, Guzmán M, Gil J-M, Borrego MJ, Pérez V. Influence of atrial fibrillation on the morbido-mortality of patients on hemodialysis. Am Heart J. 2000;140:886-890. 6. Zimmerman D, Sood MM, Rigatto C, Holden RM, Hiremath S, Clase CM. Systematic review and meta-analysis of incidence, prevalence and outcomes of atrial fibrillation in patients on dialysis. Nephrol Dial Transplant. 2012;27:3816-22. 7. Murray AM, Seliger S, Lakshminarayan K, Herzog CA, Solid CA. Incidence of stroke before and after dialysis initiation in older patients. J Am Soc Nephrol. 2013;24:1166-73. 8. Vazquez E, Sanchez-Perales C, Garcia-Garcia F, Castellano P, Garcia-Cortes MJ, Liebana A, Lozano C. Atrial fibrillation in incident dialysis patients. Kidney Int. 2009;76:324-30. 9. Chou CY, Kuo HL, Wang SM, Liu JH, Lin HH, Liu YL, Huang CC. Outcome of atrial fibrillation among patients with end-stage renal disease. Nephrol Dial Transplant. 2010;25:1225-30. 10. January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Jr., Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW, Members AATF. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071-104. 11. Winkelmayer WC, Liu J, Setoguchi S, Choudhry NK. Effectiveness and safety of warfarin initiation in older hemodialysis patients with incident atrial fibrillation. Clin J Am Soc Nephrol. 2011;6:2662-8. 12. Shah M, Avgil Tsadok M, Jackevicius CA, Essebag V, Eisenberg MJ, Rahme E, Humphries KH, Tu JV, Behlouli H, Guo H, Pilote L. Warfarin use and the risk for stroke and bleeding in patients with atrial fibrillation undergoing dialysis. Circulation. 2014;129:1196-203. 13. Chen JJ, Lin LY, Yang YH, Hwang JJ, Chen PC, Lin JL. Anti-platelet or anti-coagulant agent for the prevention of ischemic stroke in patients with end-stage renal disease and atrial fibrillation--a nation-wide database analyses. Int J Cardiol. 2014;177:1008-11. 14. Sood MM, Larkina M, Thumma JR, Tentori F, Gillespie BW, Fukuhara S, Mendelssohn DC,
and after dialysis initiation in older patients. J Am Soc Nephrol. 2013;24:1166 73.
8. Vazquez E, Sanchez-Perales C, Garcia-Garcia F, Castellano P, Garcia-Cortes MMMJ,J,J, LLLieieiebababananana AAA,,,Lozano C. Atrial fibrillation in incident dialysis patients. n Kidney Int. 2009;76:324-30.
9. CChohohou u u CYCYCY,,, KuKK ooo HLHH , Wang SM, Liu JH, Lin HH,H,H, LLLiu YL, Huang CC. OOOutcome of atrial fibrbrbrililillal tion aaammmongg patients with end-stage renal diiiseeease. Nephrol l l DiDD al Transplant. 2010;25:1225-3330.
1000. . JaJaJanuary y y CTCC , WaWW nnnn LLLS, AAAlplplpeere t JSJSJS, CaCaCalkll innns HHH, CCigggarrrroooa JJJE,E,E, CCCleleevvvelalalanddd JJC, Jrr.r.,, Cooontntnti JBB,,, ElliinnorPT, EzEzEzekekekowowowitz MDMDMD, FiFFielleld dd MEEE, MuMuMurray KKKTTT, SSSaaaccocco RRRL,LL SSSteteteveveennsnson WWWGGG, TTTchhchoou PPPJJJ, TTTrar cyyy CCMMM, YaYaYancncncy CWCWCW, MeMeMembmbmbererersss AAAAAATFTFTF. 202020141414 AAAHAHAHA/A/A/ACCCCCC/H/H/HRSRSRS ggguiiuidededelililinenene fffororor ttthehehe mmmanananagagagemememenenenttt ofofof pppatatatieieientntntsss
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
15
Chan K, de Sequera P, Komenda P, Rigatto C, Robinson BM. Major bleeding events and risk stratification of antithrombotic agents in hemodialysis: results from the DOPPS. Kidney Int. 2013;84:600-8. 15. Wizemann V, Tong L, Satayathum S, Disney A, Akiba T, Fissell RB, Kerr PG, Young EW, Robinson BM. Atrial fibrillation in hemodialysis patients: clinical features and associations with anticoagulant therapy. Kidney Int. 2010;77:1098-106. 16. Chan KE, Lazarus JM, Thadhani R, Hakim RM. Warfarin use associates with increased risk for stroke in hemodialysis patients with atrial fibrillation. J Am Soc Nephrol. 2009;20:2223-33. 17. Olesen JB, Lip GY, Kamper AL, Hommel K, Kober L, Lane DA, Lindhardsen J, Gislason GH, Torp-Pedersen C. Stroke and bleeding in atrial fibrillation with chronic kidney disease. NEngl J Med. 2012;367:625-35. 18. Reinecke H, Brand E, Mesters R, Schabitz WR, Fisher M, Pavenstadt H, Breithardt G. Dilemmas in the management of atrial fibrillation in chronic kidney disease. J Am Soc Nephrol. 2009;20:705-11. 19. Shih CJ, Chu H, Chao PW, Lee YJ, Kuo SC, Li SY, Tarng DC, Yang CY, Yang WC, Ou SM, Chen YT. Long-term clinical outcome of major adverse cardiac events in survivors of infective endocarditis: a nationwide population-based study. Circulation. 2014;130:1684-91. 20. Chao PW, Shih CJ, Lee YJ, Tseng CM, Kuo SC, Shih YN, Chou KT, Tarng DC, Li SY, Ou SM, Chen YT. Association of postdischarge rehabilitation with mortality in intensive care unit survivors of sepsis. Am J Respir Crit Care Med. 2014;190:1003-11. 21. Fischer KG. Essentials of anticoagulation in hemodialysis. Hemodial Int. 2007;11:178-89. 22. Davenport A. What are the anticoagulation options for intermittent hemodialysis? Nat Rev Nephrol. 2011;7:499-508. 23. Chang CH, Lee YC, Tsai CT, Chang SN, Chung YH, Lin MS, Lin JW, Lai MS. Continuation of statin therapy and a decreased risk of atrial fibrillation/flutter in patients with and without chronic kidney disease. Atherosclerosis. 2014;232:224-30. 24. Lin LJ, Cheng MH, Lee CH, Wung DC, Cheng CL, Kao Yang YH. Compliance with antithrombotic prescribing guidelines for patients with atrial fibrillation--a nationwide descriptive study in Taiwan. Clin Ther. 2008;30:1726-36. 25. Tsai WC, Chen CY, Kuo HF, Wu MT, Tang WH, Chu CS, Lin TH, Su HM, Hsu PC, Jhuo SJ, Lin MY, Lee KT, Sheu SH, Lai WT. Areca nut chewing and risk of atrial fibrillation in Taiwanese men: a nationwide ecological study. Int J Med Sci. 2013;10:804-11. 26. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373-83.
2009;20:705 11.
19. Shih CJ, Chu H, Chao PW, Lee YJ, Kuo SC, Li SY, Tarng DC, Yang CY, Yang gg WCWCWC,,, OuOuOu SSSM,M,M, Chen YT. Long-term clinical outcome of major adverse cardiac events in survivors of infective endocarditis: a nationwide population-based study. Circulation. 2014;130:1684-91.
2000. CCChao PW,W,W, Shih CJ, Lee YJ, Tseng CM, Kuo SCSCSC, Shih YN, Chohohou KT, Tarng DC, Li SY, Ou SMSMSM, Chen YT. AAAsssoccciaiaiatiitiononon oof f f ppopostststdididisccchahhargee reeehabbbiliitatititiononon wwwititith h momomortrtrtalalalititity in iiintntntenenensisisiveveve cccaara eee unununititit auuurvvvivors of sepsssiss. Ammm J Reesespppir Crit CCCaare MeMeMed. 220114;111909090:1:1:100003---1111.
21. FiFiFiscscscheheherr KGGG. EEsEssesesentntiaialslsl of ananantititicccoagulululatatatioioion nn iinin hhhememodododiaiaialylylysisisisss. HeHeemmomodididialal IIIntnn . 202020070707;;11:17117888-898989.
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
16
27. Cheng CL, Kao YH, Lin SJ, Lee CH, Lai ML. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol Drug Saf. 2011;20:236-42. 28. Hsieh CY, Chen CH, Li CY, Lai ML. Validating the diagnosis of acute ischemic stroke in a National Health Insurance claims database. J Formos Med Assoc. 2015;114:254-9. 29. Cheng C-L, Lee C-H, Chen P-S, Li Y-H, Lin S-J and Yang Y-HK. Validation of Acute Myocardial Infarction Cases in the National Health Insurance Research Database in Taiwan. JEpidemiol. 2014;24:500-507. 30. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. JAm Stat Assoc. 1999;94:496–509. 31. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285:2864-70. 32. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137:263-72. 33. Quinn RR, Naimark DM, Oliver MJ, Bayoumi AM. Should hemodialysis patients with atrial fibrillation undergo systemic anticoagulation? A cost-utility analysis. Am J Kidney Dis. 2007;50:421-32. 34. Chao TF, Liu CJ, Wang KL, Lin YJ, Chang SL, Lo LW, Hu YF, Tuan TC, Chung FP, Liao JN, Chen TJ, Lip GY, Chen SA. Incidence and prediction of ischemic stroke among atrial fibrillation patients with end-stage renal disease requiring dialysis. Heart Rhythm. 2014;11:1752-9. 35. Lin CC, Lai MS, Syu CY, Chang SC, Tseng FY. Accuracy of diabetes diagnosis in health insurance claims data in Taiwan. J Formos Med Assoc. 2005;104:157-63. 36. Takeda K, Harada A, Okuda S, Fujimi S, Oh Y, Hattori F, Motomura K, Hirakata H, Fujishima M. Sudden death in chronic dialysis patients. Nephrol Dial Transplant. 1997;12:952-5. 37. Hart RG, Pearce LA, Rothbart RM, McAnulty JH, Asinger RW, Halperin JL. Stroke with intermittent atrial fibrillation: incidence and predictors during aspirin therapy. Stroke Prevention in Atrial Fibrillation Investigators. J Am Coll Cardiol. 2000;35:183-7. 38. Hohnloser SH, Pajitnev D, Pogue J, Healey JS, Pfeffer MA, Yusuf S, Connolly SJ, Investigators AW. Incidence of stroke in paroxysmal versus sustained atrial fibrillation in patients taking oral anticoagulation or combined antiplatelet therapy: an ACTIVE W Substudy. J Am Coll Cardiol. 2007;50:2156-61.
Fibrillation. JAMA. 2001;285:2864 70.
32. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk strrratatatififificicicatatatioioion n n fofofor r r predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137:263-72.
3333. QQQuinn RRRRRR, Naimark DM, Oliver MJ, Bayoummi AAAM. Should hhhemee odialysis patients with atrial fififibrrriillation undnddererergo sssyysy tetetemimimicc ananantititicococoagaga uluu aatioion?n?n? A ccossst-utututilililititityyy aaanalallysyssiisis. AmAmAm J KKKidididneneneyyy DiDD sss. 2022 0070 ;50:421-32.
34. ChChChaoaoao TTTFFF, LLiuiuiu CCCJ,JJ WWWananng KLKLKL, LiLiLin YJJJ, ChChChananangg SLSLSL, LoLLo LLLWWW, HHHu YFYFYF, TuTuTuanan TTTC, CCChuhuhunng FFFP,PP LLLiaiaiaoo JNNJNChChChenenen TTTJJJ, LLLipipip GGGYYY, CCChehehennn SASASA. InInIncicicidededencncnceee anananddd prprpredededicicictititiononon ooofff isisischchchemememicicic ssstrtrtrokokokeee amamamonononggg atatatriririalalal fffibibibriririllllllatatatioioionnnn
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.115.018294
17
39. Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, Breithardt G, Halperin JL, Hankey GJ, Piccini JP, Becker RC, Nessel CC, Paolini JF, Berkowitz SD, Fox KA, Califf RM, Investigators RA. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883-91. 40. Giugliano RP, Ruff CT, Braunwald E, Murphy SA, Wiviott SD, Halperin JL, Waldo AL, Ezekowitz MD, Weitz JI, Spinar J, Ruzyllo W, Ruda M, Koretsune Y, Betcher J, Shi M, Grip LT, Patel SP, Patel I, Hanyok JJ, Mercuri M, Antman EM, Investigators EA-T. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369:2093-104.
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
18
Clinical Perspective
There is no strong evidence regarding the use of oral anticoagulants for stroke prevention in
patients undergoing hemodialysis with atrial fibrillation (AF). A better risk estimate of AF-
related stroke in this population was required to set the realistic treatment goals while majority of
hemodialysis patients with AF would die before a stroke. Previous small studies may
overestimate the stroke risk from the Kaplan-Meier approach because of potential of competing
risk bias, especially in frail populations. The present nationwide population-based propensity
score–matched study analysed the risk of ischemic stroke in 6,772 patients undergoing
hemodialysis with new-onset AF during 1998–2011, compared with those without arrhythmia in
the Cox model and the Fine and Gray competing-risk model, respectively. In the Cox model, we
found that AF patients was associated with increased risk of death or poor cardiovascular
outcomes. However, in the competing-risk model, the risk of ischemic stroke became
insignificant. The similar findings were observed in outcomes of hemorrhagic stroke and
myocardial infarction with the exception of in-hospital cardiovascular death and heart failure that
remained significant when taking into account the competing risk of in-hospital death. Thus, this
study suggests that the association of new-onset AF with subsequent ischemic stroke was weaker
than as previously expected in patients on chronic hemodialysis. Our results have implications
for reconsideration the need of oral anticoagulants for stroke prevention and choice of primary
outcomes in trials on hemodialysis patients with AF.
during 1998–2011hemodialysis with new-onset AF , compared with those withouuuttt arararrhrhrhytytythmhmhmiaiaia in
he Cox model and the Fine and Gray competing-ri sk model, respectively. In the Cox model, we
founnnddd thththatatat AAAFFF paaatititiene ts was associated with in r creaeaeasesesed risk of death or poooooor cardiovascular
oooutcccomes. Howeweweveer, iiin n thththeee cocoompmpm etetetinining-g-g-riiskkk mmmoodo el, ttthe riririsksksk ooof f f isschchchemememicicc strrokeee bebebecacacammme
nnnsiss gngngnificannt.t.t. Theh ssimmiiilaara finnndididingngngs weww rerere ooobsseeer d vvved innn ouuutcccommemess ofofof hhhememmorrrrhhagggicicic strokkkeee annd
mymmyocococararardididialalal iiinfnfnfarararctctctioioionnn wiiwiththth ttthehehe eeexccxcepepeptititiononon ooofff ininin hh-hososospipipitatatalll cacacardrdrdioioiovaavascscscullulararar dddeaeaeaththth aaandndnd hhheaeaeartrtrt fffaiaiailullurerere ttthahahaa
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
19
Table 1. Baseline Characteristics of Hemodialysis Patients.
Before Propensity Score-Matching Propensity Score-Matched Characteristics AF Non-AF StD AF Non-AF StD†
Patient (no.) 6,772 70,625 6,494 6,494 Mean age (SD), year 68.8 (11.3) 62.0 (13.8) 0.539 68.6 (11.3) 68.4 (11.6) 0.017 Male 3,166 (46.8) 35,417 (50.1) -0.068 3,030 (46.7) 3,030 (46.7) 0.000 Monthly income, NT dollars Dependent 2,628 (38.8) 23,927 (33.9) 0.103 2,511 (38.7) 2,525 (38.9) -0.004 <19,100 1,465 (21.6) 16,503 (23.4) -0.042 1,398 (21.5) 1,366 (21.0) 0.012 19,100 41,999 2,538 (37.5) 27,617 (39.1) -0.033 2,448 (37.7) 2,470 (38.0) -0.007
42,000 141 (2.1) 2,578 (3.7) -0.094 137 (2.1) 133 (2.0) 0.004 Urbanization
Level 1 2,195 (32.4) 22,574 (32.0) 0.010 2,113 (32.5) 2,172 (33.4) -0.019Level 2 4,200 (62.0) 44,466 (63.0) -0.019 4,018 (61.9) 3,960 (61.0) 0.018 Level 3 314 (4.6) 3,002 (4.3) 0.019 303 (4.7) 299 (4.6) 0.003 Level 4 (rural area) 63 (0.9) 583 (0.8) 0.011 60 (0.9) 63 (1.0) -0.005
Outpatient Visits of Cardiologist, in the past one year
0 5 visits 2,981 (44.0) 43,659 (61.8) -0.362 2,931 (45.1) 2,881 (44.4) 0.015 6 10 visits 2,698 (39.8) 20,640 (29.2) 0.225 2,550 (39.3) 2,613 (40.2) -0.020 11 15 visits 701 (10.4) 4,501 (6.4) 0.144 661 (10.2) 678 (10.4) -0.009 >15 visits 392 (5.8) 1,825 (2.6) 0.161 352 (5.4) 322 (5.0) 0.021 Charlson Comorbidity Index Score (SD)
7.2 (2.9) 6.7 (3.0) 0.159 7.2 (2.9) 7.3 (3.0) -0.013
Dialysis vintage, months (quartiles)
38 (13-76) 27 (9-65) 0.151 38 (13-76) 37 (13-75) 0.007
Medication for hypertension Alpha-blocker 249 (3.7) 3,077 (4.4) -0.035 243 (3.7) 238 (3.7) 0.004 Beta-blocker 1,555 (23.0) 14,499 (20.5) 0.059 1,460 (22.5) 1,483 (22.8) -0.008 Calcium channel blocker 2,081 (30.7) 20,516 (29.0) 0.037 1,957 (30.1) 1,998 (30.8) -0.014 Diuretics 855 (12.6) 8,240 (11.7) 0.029 805 (12.4) 806 (12.4) 0.000 ACEI or ARB 1,295 (19.1) 12,887 (18.2) 0.022 1,224 (18.8) 1,259 (19.4) -0.014
Other anti-hypertensive drug 214 (3.2) 2,076 (2.9) 0.013 198 (3.0) 170 (2.6) 0.026 Other Medications
Anti-hyperglycemic drugs 1,551 (22.9) 18,238 (25.8) -0.068 1,503 (23.1) 1,555 (23.9) -0.019Aspirin 1,423 (21.0) 10,104 (14.3) 0.177 1,319 (20.3) 1,312 (20.2) 0.003 Clopidogrel 529 (7.8) 3,437 (4.9) 0.121 512 (7.9) 513 (7.9) -0.001Ticlopidine 144 (2.1) 733 (1.0) 0.087 133 (2.0) 140 (2.2) -0.008Dipyridamole 571 (8.4) 3,882 (5.5) 0.115 514 (7.9) 510 (7.9) 0.002 Nitrate 1,471 (21.7) 8,561 (12.1) 0.258 1,327 (20.4) 1,315 (20.2) 0.005 Statin 522 (7.7) 7,165 (10.1) -0.086 508 (7.8) 544 (8.4) -0.020PPI 554 (8.2) 4,356 (6.2) 0.078 526 (8.1) 517 (8.0) 0.005 NSAID 923 (13.6) 6,671 (9.4) 0.131 867 (13.4) 871 (13.4) -0.002
Comorbid disease Congestive heart failure 4,394 (64.9) 32,804 (46.4) 0.378 4,196 (64.6) 4,174 (64.3) 0.007 Hypertension 4,394 (64.9) 32,804 (46.4) 0.378 4,196 (64.6) 4,174 (64.3) 0.007 Diabetes mellitus 3,953 (58.4) 41,873 (59.3) -0.019 3,826 (58.9) 3,852 (59.3) -0.008Previous Stroke/TIA 2,234 (33.0) 19,803 (28.0) 0.108 2,151 (33.1) 2,151 (33.1) 0.000 Vascular diseases 5,176 (76.4) 41,453 (58.7) 0.386 4,937 (76.0) 5,005 (77.1) -0.025
p y5 visits 2,981 (44.0) 43,659 (61.8) -0.362 2,931 (45.1) 222,8,8,8818181 (((444444.4.4.4) 0) 0) 0.010 visits 2,698 (39.8) 20,640 (29.2) 0.225 2,550 (39.3) 2,2,2,61113 3 3 (4(440.0.0.2)2)2) -0-0-0.0.0.0
1 15 visits 701 (10.4) 4,501 (6.4) 0.144 661 (10.2) 6778 (10.4) -0.015 visits 392 (5.8) 1,825 (2.6) 0.161 352 (5.4) 322 (5.0) 0.02
harlson Comorbidididity Index orrreee (S(S(SDDD)
7.2 (2.9) 6.7 7 7 (3(( .0) 0.159 7..2 2 2 (2( .9) 7.3 (3.0) -0.0
aalalysysysis vintageee, momomontnn hss uuau rrrtiles)
383838 (((131313-7-776))) 27 (999-65)5)) 00.1515151 38 8 (1(1(13-76) ) ) 37373 (133-7-7-75)5)5) 000.0
eeediiicacc tion for hypperrtennssioon Allphphpha-a-a-blb ockekekerrr 2424249 (((3.7.7.7))) 3,3 0777777 (44.4.4))) -000.0.0.0335 24443 (3.7)7)7) 22233838 (33.3 77)7) 0.0.Beta-bbblololockckckere 111,555 (2(22333.000) 1114,4449999 ((2000 55.5) 0) 0) 0.05999 1,4446060 (((2222.555))) 111,4483 (2(2( 22.8))8) 0-0 00.0CCCalllciiium hhchannelll blblblockkker 222,080808111 (3(3(3000.7)7)7) 202020 55,5161616 (((292929 00.0) 0) 0) 0 00.0373737 111 99,9575757 (((303030 11.1))) 111,999999888 (3(3(3000.8)8)8) 00-0 00.00
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
20
Liver Disease 2,422 (35.8) 25,676 (36.4) -0.012 2,345 (36.1) 2,387 (36.8) -0.013Prior Major Bleeding 3,708 (54.8) 35,392 (50.1) 0.093 3,580 (55.1) 3,584 (55.2) -0.001Alcohol or drug abuse 150 (2.2) 2,540 (3.6) -0.082 148 (2.3) 165 (2.5) -0.017
Myocardial infarction 992 (14.6) 6,169 (8.7) 0.185 941 (14.5) 912 (14.0) 0.013 Peptic ulcer disease 4,312 (63.7) 42,617 (60.3) 0.069 4,172 (64.2) 4,161 (64.1) 0.004 Dyslipidemia 3,170 (46.8) 38,613 (54.7) -0.158 3,096 (47.7) 3,096 (47.7) 0.000 Cancer 1,638 (24.2) 14,429 (20.4) 0.090 1,572 (24.2) 1,589 (24.5) -0.006 Autoimmune disease 264 (3.9) 3,850 (5.5) -0.074 260 (4.0) 262 (4.0) -0.002CHA2DS2-VASc
0 130 (1.9) 4,476 (6.3) -0.223 129 (2.0) 129 (2.0) 0.000 1 322 (4.8) 9,383 (13.3) -0.301 311 (4.8) 311 (4.8) 0.000 2 578 (8.5) 9,273 (13.1) -0.148 562 (8.7) 562 (8.7) 0.000 3 836 (12.3) 9,762 (13.8) -0.044 808 (12.4) 808 (12.4) 0.000 4 1,072 (15.8) 10,751 (15.2) 0.017 1,029 (15.8) 1,029 (15.8) 0.000 5 1,156 (17.1) 8,989 (12.7) 0.122 1,098 (16.9) 1,098 (16.9) 0.000 6 1,086 (16.0) 7,681 (10.9) 0.152 1,028 (15.8) 1,028 (15.8) 0.000 7 784 (11.6) 5,468 (7.7) 0.130 760 (11.7) 760 (11.7) 0.000 8 520 (7.7) 3,290 (4.7) 0.126 499 (7.7) 499 (7.7) 0.000 9 288 (4.3) 1,552 (2.2) 0.117 270 (4.2) 270 (4.2) 0.000
* All data were descripted as number (%), except mean age, Charlson Comorbidity Index Score, dialysis vintage, and propensity score. † Imbalance defined as absolute value greater than 0.034. Abbreviations: AF, atrial fibrillation; SD, standard deviation; StD, Standardized difference; NT$, new Taiwan dollars; ACEI, angiotensin-converting-enzyme inhibitors; ARB, Angiotensin II receptor blockers; PPI, proton-pump inhibitor; NSAIDs, Non-steroidal anti-inflammatory drugs; TIA, Transient ischemic attack.
All data were descripted as number (%), except mean age, Charlson Comorbidity Index Score, dialylyysisisis vivivintntagagage,e,, aand opensity score.mbalance defined as absolute value greater than 0.034. breviations: AF, atrial fibrillation; SD, standard deviation; StD, Standardized difference; NT$, new Taiwan dollars
CEI, angiotensin-converting-enzyme inhibitors; ARB, Angiotensin II receptor blockers; PPI, proton-pump inhibitorSAIDs, Non-steroidadaal l anti-inflammatory drugs; TIA, Transienenent ischemic attack.
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
21
Table 2. Incidence and Risk of Stroke, Myocardial Infarction, and Major Bleeding among Hemodialysis Patients With and Without AF.
AF Non-AF Crude Adjusted† Competing Risk‡
No. ofEvent
Annualrate
No. of Event
Annualrate
Hazard Ratio(95% CI)
pValue
Hazard Ratio(95% CI)
pValue
Hazard Ratio(95% CI)
pValue
Before Propensity Score Matching All-cause death 4,642 24.72 22,008 9.56 2.57
(2.49-2.66) <0.001 1.64 (1.59-1.70) <0.001 -
In-hospitalcardiovascular death 2,461 13.11 10,403 4.52 2.88
(2.76-3.01) <0.001 1.89 (1.80-1.99) <0.001 1.71
(1.63-1.80) <0.001
Ischemic stroke 600 3.35 3,963 1.77 1.88 (1.73-2.05) <0.001 1.25
(1.15-1.37) <0.001 1.03 (0.94-1.12) 0.558
Hemorrhagic stroke 278 1.40 2,101 0.92 1.52 (1.34-1.72) <0.001 1.28(
1.12-1.46) <0.001 1.03 (0.90-1.18) 0.683
Myocardial infarction 517 2.84 3,312 1.46 1.94 (1.76-2.12) <0.001 1.30
(1.18-1.44) <0.001 1.14 (1.03-1.27) 0.010
Hospitalization for heart failure 1,719 10.88 7,822 3.58 2.95
(2.80-3.11) <0.001 1.95 (1.84-2.06) <0.001 1.63
(1.54-1.72) <0.001
After Propensity Score Matching All-cause death 4,380 24.33 3,548 14.84 1.59
(1.52-1.66) <0.001 1.59 (1.52-1.67) <0.001 -
In-hospitalcardiovascular death 2,322 12.90 1,629 6.81 1.82
(1.71-1.94) <0.001 1.83 (1.71-1.94) <0.001 1.65
(1.55-1.76) <0.001
Ischemic Stroke 563 3.28 573 2.50 1.27 (1.13-1.42) <0.001 1.27
(1.13-1.43) <0.001 1.01 (0.90-1.14) 0.832
Hemorrhagic stroke 245 1.38 254 1.07 1.24 (1.04-1.49) 0.015 1.24
(1.04-1.48) 0.015 0.99 (0.83-1.18) 0.882
Myocardial infarction 499 2.86 483 2.07 1.33 (1.18-1.51) <0.001 1.33
(1.17-1.51) <0.001 1.06 (0.94-1.21) 0.327
Hospitalization for heart failure 1,636 10.77 1,153 5.25 1.90
(1.76-2.05) <0.001 1.90 (1.76-2.05) <0.001 1.56
(1.45-1.68) <0.001 † Adjusted for propensity score quintile and warfarin use which was calculated as a time-varying covariate. ‡Adjusted for propensity score quintile, using antiplatelet drugs, and warfarin use which was calculated as a time-varying covariate. Abbreviations: CI, confidence interval.
mic stroke 600 3.35 3,963 1.77 1.88 (1.73-2.05) <0.001 1.25
(1.15-1.37) <0.001 1.0333 (0(0(0.9994-4-4 1.1.1.121212) ) ) 0.00 55
orrhagic stroke 278 1.40 2,101 0.92 1.52 (1.34-1.72) <0.001 1.28(
1.12-1.46) <0.001 1.1.1 03033 (00.90-1.18) 000.6868688
ardial infarction 517 2.84 3,312 1.46 1.94 (1.76-2.12) <0.001 1.30
(1.18-1.44) <0.001 1.14 (1.03-1.27) 0.01
talizatiooonnn fofofor rfailililurururee e 1,1,1 11719 10.88 7,822 3.58 2.959595
(2 88.80-0-0-3.1111 ) <0.001 1.95 (1.8.8.84-2. 6606))) <0.001 1.63
(1.54-1.72) <0.0
PrPrPropopopensity S ocorerere Matchingaaausuu e e e death 4,44 8380 2444 33.3333 3,33 54888 1411 88.84 1.5955
(1(( .5 --2-1.6666 ) <0< 00.0 1101 111.59595 (1(( 55.52-1. 7767) <000.0.0.00100 -
ssspipp atatalovavava ccsculuu ar deathhh ,22 2322 2212.90 1,11 629 6.66 8188 1.8288
(1(( .7 --1-1.9499 ) <0<< 00.001 1.83 (1(( 77.71-1.1 4494) <0<0< 00.0010 1. 5655
(1(1( .5.5.55- .1 6676) 00<0.0
mic SSStrtrtrokokokeee 565656333 333.282828 555737373 22 55.5000 1.1.1.27272 (1.13-1.42) <0<0<0.00010101 1.1.1.2722
(1.13-1.43) <0 0.0010101 1..010101 (0.90-1.14) 000.838383
rrhagic stroke 245 1.38 254 1.07 1.24 (1 04 1 49) 0.015 1.24
(1 04 1 48) 0.015 0.99(0 83 1 18) 0. 8888
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.115.018294
22
Table 3. Incidence Rate of Ischemic Stroke and Death in Hemodialysis Patients with AF.
Ischemic Stroke Death No. of Event Annual rate (%)* No. of Event Annual rate (%)*
CHA2DS2-VASc 0 11 1.82 64 10.03 1 17 1.15 168 11.06 2 43 1.97 332 14.65 3 77 2.81 532 18.63 4 77 2.56 721 22.93 5 110 3.84 806 26.43 6 103 4.30 798 31.47 7 74 5.02 577 36.80 8 57 7.25 408 49.51 9 31 8.66 236 63.10
Total patients 600 3.35 4,642 24.72 CHADS2 Score 0 56 1.60 415 11.48 1 61 2.70 519 22.11 2 79 2.22 716 19.35 3 182 4.01 1294 26.64 4 70 4.23 612 35.44 5 101 5.97 657 36.34 6 51 7.37 429 59.58
Total patients 600 3.35 4,642 24.72 *per 100 person-years.
CHADS2 Score 0 56 1.60 415 1111.4448881 61 2.70 519 222.11 2 79 2.22 716 19.35 3 182 4.4.4.010101 1294 26.64 444 70 4.23233 6166 2 35.44 555 11010111 5.97977 665657 7 363636.333444666 51 7.37377 44429 55959.588
Tootatatalll papapatitit enenentststs 606060000 3..353535 444,66,642424 222444.7222 per 100 person-years.
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.115.018294
23
Table 4. Event Rate and Risks of Ischemic Stroke in Hemodialysis Patients with AF.
Ischemic Stroke Crude Adjusted† Competing Risk‡
No. ofEvent
Annualrate (%)*
Hazard Ratio (95% CI) p Value Hazard Ratio
(95% CI) p Value Hazard Ratio (95% CI) p Value
CHA2DS2-VASc score 0 11 1.82 Reference Reference Reference 1 17 1.15 0.63 (0.30-1.35) 0.237 0.62 (0.29-1.32) 0.215 0.58 (0.28-1.24) 0.148 2 43 1.97 1.08 (0.56-2.10) 0.821 1.05 (0.54-2.04) 0.889 0.86 (0.45-1.65) 0.645 3 77 2.81 1.52 (0.81-2.86) 0.195 1.46 (0.77-2.75) 0.244 1.07 (0.57-1.99) 0.831 4 77 2.56 1.36 (0.72-2.57) 0.338 1.30 (0.69-2.45) 0.418 0.86 (0.46-1.60) 0.634 5 110 3.84 2.03 (1.09-3.78) 0.026 1.90 (1.02-3.55) 0.044 1.13 (0.61-2.08) 0.706 6 103 4.30 2.24 (1.20-4.18) 0.012 2.11 (1.13-3.95) 0.020 1.14 (0.62-2.11) 0.667 7 74 5.02 2.57 (1.36-4.87) 0.004 2.39 (1.26-4.54) 0.008 1.17 (0.63-2.18) 0.622 8 57 7.25 3.58 (1.87-6.87) <0.001 3.37 (1.75-6.48) <0.001 1.43 (0.75-2.72) 0.274 9 31 8.66 4.12 (2.06-8.24) <0.001 3.87 (1.93-7.78) <0.001 1.43 (0.72-2.82) 0.306
*per 100 person-years. †Adjusted for using antiplatelet drugs and warfarin use which was calculated as a time-varying covariate. ‡In this model, non-ischemic stroke death was calculated as a competing risk, adjusted for using antiplatelet drugs and warfarin use which was calculated as a time-varying covariate. Abbreviations: CI, confidence interval.
( ) ( ) ( )77 2.81 1.52 (0.81-2.86) 0.195 1.46 (0.77-2.75) 0.244 1.000777 (0(0(0.5.5.57-7-7-1.1.1.999999) 0)) .877 2.56 1.36 (0.72-2.57) 0.338 1.30 (0.69-2.45) 0.418 0 88.86 (0(( 44.46-6-6-11.1.606060) 0) 0) 0.6110 3.84 2.03 (1.09-3.78) 0.026 1.90 (1.02-3.55) 0.044 1. 313 (((0.00 1611 22-2 0.008)8)8) 00.0 777103 4.30 2.24 (1.20-4.18) 0.012 2.11 (1.13-3.95) 0.020 1.14 (0.62-2.11) 0.674 5.02 2.57 (1.36-4.87) 0.004 2.39 (1.26-4.54) 0.008 1.17 (0.63-2.18) 0.657 7.25 3.58 (1.87-6.87) <0<0<0.001 3.37 (1.75-6.48) <0<< .001 1.43 (0.75-2.72) 0.231 8.66 4.12 (2.06-8.24) <0<0<0.001 3.87 (1.93-3-3-7.77 78) <0.001 1.43 (0.72-2.82) 0.3
000 00 eeperson-years. ttted ffor using antiplatelel t tt rdrugs nnand wawaw rfrfrfaraa ninin uuuse hhwhich h h aawas ac lcul tata dded as a titt emem -v rraryiyiy ngnn covoo rarariate. s s s oomodel, non-ischemic tstror kek d aaeath wwas c lalal uuculated as a compmm etee ing rirr kksk, ad uujust dee for usisisingngng aaantipii la etelel t drugs nnand wa frfrfarinii use wwwhihh hhch wasaa cccalcu alaated dd asnarararyingngng covariate. v aaiatititi nnons:s:s: CI, connnfififideded nce inii eeterval.
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from

Der-Cherng Tarng, Chih-Ching Lin, Po-Hsun Huang, Szu-Yuan Li and Yung-Tai ChenChia-Jen Shih, Shuo-Ming Ou, Pei-Wen Chao, Shu-Chen Kuo, Yi-Jung Lee, Chih-Yu Yang,
Fibrillation: A Competing-Risk Analysis of a Nationwide CohortRisks of Death and Stroke in Patients Undergoing Hemodialysis With New-Onset Atrial
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2015 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation published online December 17, 2015;Circulation.
http://circ.ahajournals.org/content/early/2015/12/17/CIRCULATIONAHA.115.018294World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2015/12/17/CIRCULATIONAHA.115.018294.DC1Data Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on April 21, 2017
http://circ.ahajournals.org/D
ownloaded from
SUPPLEMENTAL MATERIAL
A concise listing of the variables used in the propensity score model is provided
below.
1. Demographic factors included age, gender, year and month of index date,
monthly income, urbanization level, dialysis vintage, outpatient visits of diabetes
specialist, nephrologist and cardiologist in the past one year.
2. Comorbid factors included Charlson Comorbidity Index score, diabetes
mellitus, congestive heart failure, coronary artery disease, myocardial infarction,
prior stroke/transient ischemic accident, liver diseases, peptic ulcer disease, prior
major bleeding, alcohol or drug abuse, dyslipidemia, proteinuria, cancer and
autoimmune disease.
3. Concomitant medications included anti-hyperglycemic drugs, aspirin,
clopidogrel, ticlopidine, dipyridamole, nitrate, statin, proton pump inhibitors,
non-steroidal anti-inflammatory drugs, and anti-hypertensive drugs such as
alpha-blockers, beta-blockers, calcium channel blockers, diuretics,
angiotensin-converting-enzyme inhibitors/angiotensin II receptor blockers, and
others.

Table 1. Propensity Score Model Results of Probability of Arterial Fibrillation.
Table 2. Incidence and Risk of Stroke among Hemodialysis Patients with and without
AF, Stratified by CHA2DS2-VASc Score
Figure legends
Figure 1. Flow Chart of Patient Selection.

Supplementary Table 1. Propensity Score Model Results of Probability of Arterial
Fibrillation.
95% CI
Parameter Estimate Odds Ratios Lower Upper P value
Age, per year 0.0449 1.046 1.043 1.049 <.0001
Male 0.00583 1.006 0.952 1.063 0.8365
Year of Index Date
1998 1
1999 -0.4464 0.64 0.499 0.821 0.0005
2000 -0.7656 0.465 0.368 0.588 <.0001
2001 -1.0307 0.357 0.284 0.449 <.0001
2002 -1.1986 0.302 0.241 0.378 <.0001
2003 -1.4703 0.23 0.183 0.288 <.0001
2004 -1.7181 0.179 0.143 0.224 <.0001
2005 -1.9033 0.149 0.12 0.186 <.0001
2006 -2.0537 0.128 0.103 0.16 <.0001
2007 -2.214 0.109 0.088 0.136 <.0001
2008 -2.4096 0.09 0.072 0.112 <.0001
2009 -2.6466 0.071 0.057 0.088 <.0001
2010 -3.0255 0.049 0.039 0.06 <.0001
2011 -3.4682 0.031 0.025 0.039 <.0001
Month of Index Date
January 1
February -0.0703 0.932 0.818 1.063 0.2932
March -0.0267 0.974 0.857 1.106 0.681
April -0.0667 0.935 0.822 1.065 0.3138
May -0.1129 0.893 0.786 1.015 0.0843
June -0.1523 0.859 0.754 0.978 0.0221
July -0.1163 0.89 0.783 1.012 0.0766
August -0.148 0.862 0.756 0.984 0.0274
September -0.2467 0.781 0.684 0.893 0.0003
October -0.1529 0.858 0.753 0.979 0.0223
November -0.236 0.79 0.693 0.9 0.0004
December -0.2762 0.759 0.669 0.861 <.0001
Monthly income, NT dollars
Dependent 1
<19,100 0.0115 1.012 0.94 1.089 0.7574
19,10041,999 0.0441 1.045 0.982 1.112 0.1665

42,000 0.03 1.03 0.855 1.242 0.753
Urbanizationa
Level 1 1
Level 2 0.0395 1.04 0.982 1.102 0.1829
Level 3 0.0401 1.041 0.911 1.189 0.5553
Level 4 (rural area) 0.0228 1.023 0.772 1.356 0.8742
Outpatient Visits of diabetes
specialist, in the past one year
05 visits 1
610 visits -0.0457 0.955 0.866 1.054 0.361
1115 visits -0.0234 0.977 0.79 1.207 0.8289
>15 visits -0.056 0.946 0.741 1.206 0.6518
Outpatient Visits of Nephrologist, in
the past one year
05 visits 1
610 visits 1.5246 4.593 3.658 5.768 <.0001
1115 visits 1.3921 4.023 3.235 5.004 <.0001
>15 visits 1.4245 4.156 3.428 5.038 <.0001
Outpatient Visits of Cardiologist, in
the past one year
05 visits 1
610 visits 0.4281 1.534 1.445 1.629 <.0001
1115 visits 0.4258 1.531 1.387 1.69 <.0001
>15 visits 0.5025 1.653 1.453 1.88 <.0001
Dialysis vintage 0.00861 1.009 1.008 1.009 <.0001
Charlson Comorbidity Index Scoreb 0.0264 1.027 1.008 1.046 0.0056
Anti-hypertensive drug
Alpha-blocker -0.1615 0.851 0.736 0.984 0.029
Beta-blocker 0.1483 1.16 1.079 1.246 <.0001
Calcium channel blocker 0.1172 1.124 1.051 1.203 0.0007
Diuretics 0.317 1.373 1.258 1.498 <.0001
Other anti-hypertensive drug 0.0388 1.04 0.888 1.217 0.6295
ACEI or ARB -0.0013 0.999 0.925 1.078 0.9736
Other concomitant medications
Anti-hyperglycemic drugs -0.0915 0.913 0.848 0.982 0.015
Aspirin 0.1786 1.196 1.111 1.286 <.0001
Clopidogrel 0.2292 1.258 1.126 1.404 <.0001
Ticlopidine 0.2374 1.268 1.04 1.545 0.0187

Dipyridamole -0.0915 0.913 0.848 0.982 0.015
Nitrate 0.0583 1.06 0.958 1.172 0.257
Statin 0.1537 1.166 1.082 1.257 <.0001
PPI -0.1991 0.819 0.739 0.909 0.0002
NSAID 0.3355 1.399 1.263 1.548 <.0001
Comorbidities
Diabetes mellitus -0.0793 0.924 0.855 0.998 0.0456
Congestive heart failure 0.5242 1.689 1.585 1.8 <.0001
Previous Stroke/TIA 0.0402 1.041 0.941 1.152 0.4375
Vascular disease 0.1002 1.105 0.93 1.314 0.2553
Liver disease 0.0157 1.016 0.955 1.08 0.6163
Prior Major Bleeding 0.1755 1.192 1.121 1.267 <.0001
Alcohol or drug abuse -0.0744 0.928 0.777 1.11 0.4136
Proteinuria 0.0495 1.051 0.954 1.158 0.3171
Coronary artery disease 0.3891 1.476 1.25 1.742 <.0001
Peptic ulcer disease -0.055 0.946 0.885 1.013 0.1098
Myocardial infarction -0.0828 0.921 0.865 0.98 0.0096
Dyslipidemia -0.0037 0.996 0.92 1.079 0.9283
Cancer 0.217 1.242 1.141 1.353 <.0001
Autoimmune disease -0.1636 0.849 0.742 0.972 0.0175
a Urbanization levels in Taiwan are divided into four strata according to the Taiwan National
Health Research Institute publications. Level 1 designates the most urbanized areas, and level
4 designates the least urbanized areas. b
Charlson Comorbidity Index score is used to determine overall systemic health. With each
increased level of CCI score, there are stepwise increases in the cumulative mortality.
Abbreviations: NT dollars, new Taiwan dollars; ACEI, Angiotensin-converting-enzyme
inhibitors; ARB, Angiotensin II receptor blockers; PPI, Proton-pump inhibitor; NSAIDs,
Non-steroidal anti-inflammatory drugs; TIA, Transient ischemic attack
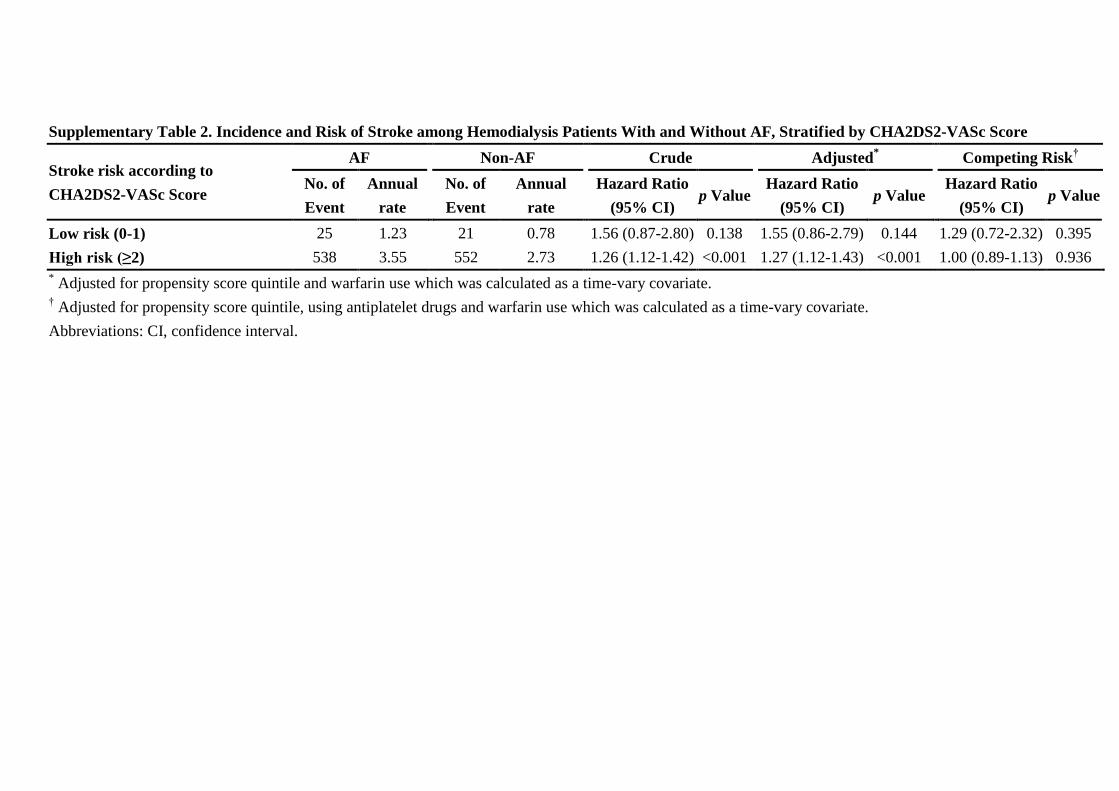
Supplementary Table 2. Incidence and Risk of Stroke among Hemodialysis Patients With and Without AF, Stratified by CHA2DS2-VASc Score
Stroke risk according to
CHA2DS2-VASc Score
AF Non-AF Crude Adjusted* Competing Risk
†
No. of
Event
Annual
rate
No. of
Event
Annual
rate
Hazard Ratio
(95% CI) p Value
Hazard Ratio
(95% CI) p Value
Hazard Ratio
(95% CI) p Value
Low risk (0-1) 25 1.23 21 0.78 1.56 (0.87-2.80) 0.138 1.55 (0.86-2.79) 0.144 1.29 (0.72-2.32) 0.395
High risk (≥2) 538 3.55 552 2.73 1.26 (1.12-1.42) <0.001 1.27 (1.12-1.43) <0.001 1.00 (0.89-1.13) 0.936
* Adjusted for propensity score quintile and warfarin use which was calculated as a time-vary covariate. † Adjusted for propensity score quintile, using antiplatelet drugs and warfarin use which was calculated as a time-vary covariate.
Abbreviations: CI, confidence interval.

Supplementary Figure 1. Flow Chart of Patient Selection.


















