Risk Pooling to Achieve Universal Coverage: Ghana ’ s National Health Insurance Scheme
26
Abt Associates Inc. In collaboration with: I Aga Khan Foundation I BearingPoint I Bitrán y Asociados I BRAC University I Broad Branch Associates I Forum One Communications I RTI International I Training Resources Group I Tulane University’s School of Public Health Risk Pooling to Achieve Universal Coverage: Ghana’s National Health Insurance Scheme Slavea Chankova
-
Upload
seth-perkins -
Category
Documents
-
view
26 -
download
1
description
Risk Pooling to Achieve Universal Coverage: Ghana ’ s National Health Insurance Scheme. Slavea Chankova. I. BACKGROUND. The National Health Insurance Scheme (NHIS). Established by legislation in 2003 Goal: equitable and universal access to health care Coverage reached 66% in 2010 - PowerPoint PPT Presentation
Transcript of Risk Pooling to Achieve Universal Coverage: Ghana ’ s National Health Insurance Scheme

Abt Associates Inc. In collaboration with:I Aga Khan Foundation I BearingPoint I Bitrán y Asociados I BRAC University I Broad Branch Associates I Forum One Communications I RTI International I Training Resources Group I Tulane University’s School of Public Health
Risk Pooling to Achieve Universal Coverage: Ghana’s National Health
Insurance Scheme
Slavea Chankova
I. BACKGROUND

The National Health Insurance Scheme (NHIS)
Established by legislation in 2003 Goal: equitable and universal access to health care Coverage reached 66% in 2010 Evaluation of NHIS
Designed in anticipation of NHIS implementation Collaboration between Health Systems 20/20 project and
Health Research Unit - Ghana Health Service

Key Features of the NHIS
Managed by district-level mutual health insurance schemes
Providers: all public health facilities and accredited private providers
Benefits: 95% of disease conditions, essential drugs Enrollment
Open to all with sliding-scale premium contributions starting at about $5 per adult
Premium exemptions for children (under 18), elderly (70+), indigent, and pregnant women (as of 2008)

II. EVALUATION DESIGN

Evaluation Questions
Who has enrolled in the NHIS? Do enrollment rates differ among different socio-economic groups? Is there evidence of adverse selection in NHIS enrollment? How well-targeted have premium exemptions been?
What is the impact of the NHIS on the utilization of health services?
What is the impact of the NHIS on out-of-pocket expenditures for health care?

Evaluation Design
Pre-post study design Baseline in September 2004 Endline in September 2007 Implementation of NHIS in study sites started in 2005
Cross-sectional household surveys in 2 districts Nkoranza (had CBHI at baseline) Offinso

Study Sample
Baseline2004
Endline2007
Number of households 1,805 2,520
Number of individuals 9,554 11,770
Individuals reporting illness/injury in past 2 weeks
413 411
Individuals reporting hospitalization in past 12 months
203 208
Women reporting delivery in past 12 months
298 312
Analytic Methods
Pre-post comparison of means for key indicators Regression models
Control for differences in socio-economic characteristics between baseline and endline samples
Probit and logistic regression models Results were robust to analytic methods

III. RESULTS

Sample Characteristics
Poor rural population General improvements in socio-economic characteristics between 2004 and 2007 Health insurance coverage:
Baseline 2004(Nkoranza CBHI)
Endline 2007(NHIS)
Nkoranza 35% 45%
Offinso 0% 25%
Total sample 23% 35%

Who Enrolls in NHIS?
Enrollment increases with wealth quintile Poorest are 3 times less likely to enroll compared to the richest
18%
40% 39%
52%
30%
0%
10%
20%
30%
40%
50%
60%
Poorest Middle-poor Middle Middle-rich Richest
% o
f w
ealt
h q
uin
tile
en
rolle
d in
NH
IS

Who Enrolls in NHIS?
Factors associated with higher likelihood of NHIS enrollment* Richer wealth quintile Education of household head Female headed household Female gender Age: children and the elderly more likely to enroll, compared to
18-49 yr old Self-reported chronic illness At least one household member is part of a community solidarity
scheme
* Results from multivariate regression (variables with statistically significant coefficients)
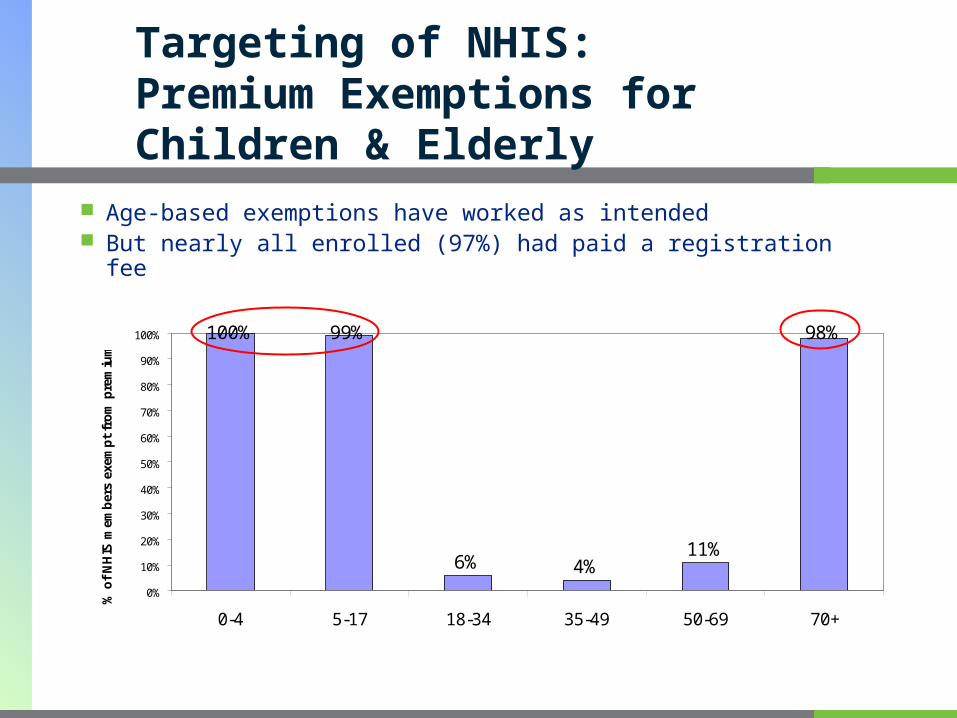
Targeting of NHIS: Premium Exemptions for Children & Elderly
Age-based exemptions have worked as intended But nearly all enrolled (97%) had paid a registration fee
100%
6% 4%11%
98%99%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-4 5-17 18-34 35-49 50-69 70+
% o
f N
HIS
mem
ber
s ex
emp
t fr
om
pre
miu
m

Targeting of NHIS: Premium Exemptions for the Poor
Exemptions have not benefited primarily those in the lowest wealth quintile
64%59% 62% 60% 62%65%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Poorest Middle-poor Middle Middle-rich Richest Total
% o
f N
HIS
mem
ber
s ex
emp
t fr
om
pre
miu
m

Adverse Selection in Enrollment
Strong evidence of adverse selection based on health status
NHIS-insured almost 3 times as likely to report illness in past 2 weeks, compared to uninsured
55% of those with chronic illness insured, compared to 34% of those without
No evidence of self-selection in enrollment related to pregnancy
36% of women with delivery in the past 12 months were insured at time of delivery, compared to 33% of women who did not have a delivery

Utilization of Care for Recent Illness or Injury
50%
37%
70%76%
44%36%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Used medication at home (p=0.009) Sought care from informalproviders (p<0.0001)
Sought care at a modern healthcare provider (p<0.0001)
Per
cen
t o
f in
div
idu
als
sick
in
pas
t 2
wee
ks
2004
2007

Utilization of Maternal Health Care
No significant changes between 2004 and 2007 in proportion of pregnant women receiving key maternal health services
73%
6% 6%
54%
68%
55%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
4 or more ANC visits (p>0.10) Delivery in health facility (p>0.10) Delivery by c-section (p>0.10)
% o
f w
om
en w
ith
del
iver
y in
pas
t 1
2 m
on
ths
2004
2007

Likelihood of OOP Expenditures for Care
Significant decrease in probability of incurring OOP expenditures for recent curative care, hospitalization, antenatal care (ANC), and delivery
87% 88%
74%
55%
47%
87%
43%
57%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Recent curative care (p<0.01) Hospitalization (p<0.01) ANC (p<0.01) Delivery (p<0.01)
% w
ith
po
sit
ive
OO
P e
xp
en
dit
ure
s f
or
ca
re
2004
2007

Changes in OOP Expenditures for Care
Average expenditures for treatment declined significantly for most services: 41% decrease for curative care (from $2 at baseline) 44% decrease for hospitalization (from $25 at baseline) No significant decrease for ANC (remained at about $3) 30% decrease for delivery (from $8 at baseline)
No significant changes in average amount paid by those who had positive OOP expenditures
Limitations
Results from 2 districts (out of 138) so cannot be generalized to whole country
Changes between 2004 and 2007 likely reflect impact of NHIS, but may also be influenced by other factors (e.g. other socioeconomic or policy changes occurring simultaneously)
Small samples for some indicators (e.g. hospitalization) limit the ability of the study to detect significant changes

IV. CONCLUSIONS & POLICY IMPLICATIONS
NHIS Enrollment
Age-based exemptions from NHIS premiums for children and the elderly have worked as intended But this may have potential implications for NHIS sustainability
Strong wealth effects observed for NHIS enrollment Exemptions for the poorest groups need to be strengthened to ensure
equitable enrollment in NHIS
Evidence of adverse selection: those with poorer health status are more likely to enroll and more likely to utilize care Implications for DMHIS sustainability

Utilization and OOP Expenditures
Substantial increase in use of formal medical services for illness; decrease in self-treatment and informal care-seeking
However, no improvement in maternal care-seeking Need to explore non-financial barriers for seeking care
Insurance has been very effective at reducing out-of-pocket expenditures for curative care and hospitalization, as well as for maternal care
Acknowledgements
Abt Associates -- Health Systems 20/20: Laurel Hatt, Sara Sulzbach, Hong Wang, Ha Nguyen
Ghana Health Service/Health Research Unit: Dr. John Gyapong, Bertha Garshong
USAID: Yogesh Rajkotia, Karen Cavenaugh, Mary Ellen Stanton
Abt Associates Inc. In collaboration with:I Aga Khan Foundation I BearingPoint I Bitrán y Asociados I BRAC University I Broad Branch Associates I Forum One Communications I RTI International I Training Resources Group I Tulane University’s School of Public Health
Reports related to this presentation are available at: www.HS2020.org
Presentation will be posted at: http://www.abtassociates.com/HSRsymposium