Risk Or, Hippocrates was wrong P. Mukherji. Primum non nocerum -HIPPOCRATES.
62
Risk Or, Hippocrates was wrong P. Mukherji
-
Upload
arron-booth -
Category
Documents
-
view
227 -
download
1
Transcript of Risk Or, Hippocrates was wrong P. Mukherji. Primum non nocerum -HIPPOCRATES.

RiskOr, Hippocrates was wrong
P. Mukherji
Primum non nocerum-HIPPOCRATES
First do no harm FIRST: implies that this is a
cardinal and overarching tenet of medicine
The statement also implies that this is possible.
Better motto:
Please try and kill as few patients as possible, while hopefully healing and helping as many as possible.

Please stop me Please interrupt Please look it up
91 yo WM s/p trip and fall +head injury: abrasion NT head/spine, full ROM No concerning sx, no
ASA/Coumadin
CT?
RULES to help us? Canadian Head CT
NEXUS II
New Orleans Criteria

To scan or not to scan?
Spin
em
all
and le
t Go.
..
Nope,
he
mig
ht get
a ..
.
0%0%
a. Spin em all and let God sort em out
b. Nope, he might get a brain tumor

CT shows small SAH
SDH is
mor
e co
...
Epid
ural i
s m
o...
He
has a
n aneu
...
He
needs
ICU t.
..
He
needs
a m
on...
0% 0% 0%0%0%
a. SDH is more common in trauma
b. Epidural is more common in trauma
c. He has an aneurysm
d. He needs ICU timee. He needs a monitor

Pt. admitted for observation Falls off the bed(!) When transferred back to
stretcher stops breathing Regains VS, is transported to CT Stops breathing again!

CT shows? C-spine is crumply at C2
CT head is clean Attending read later finds initial CT
finding to be motion artifact
Did we do wrong? Pt. was admitted for his own safety Harm came to patient Admission led to harm
Should we change practice? CO- vs. O-MISSION

Would you do it differently next time?
Hea
d CT
plea
se
How a
bout
jus.
..
0%0%
a. Head CT pleaseb. How about just
good instructions

Doctors are biased*
Routinely overestimate benefits of intervention
Routinely minimize risks of intervention
*Surgeons!

House of God? FAT MAN’s RULE #13
“The delivery of good medical care is to do as much nothing as possible”

But it’s not just about doctors We all routinely underestimate
everday risks High frequency, unlikely events
We tend to demonize and overestimate rare events Low frequency, very unlikely events
Did you ever fall? Over your lifetime, falling is a
significant risk
Falls in the elderly are a problem, should you be attentive to it already?
What’s most likely to kill ya?
Shar
k at
tack
MRSA
Flu
Fal
l
25% 25%25%25%a. Shark attackb. MRSAc. Flud. Fall
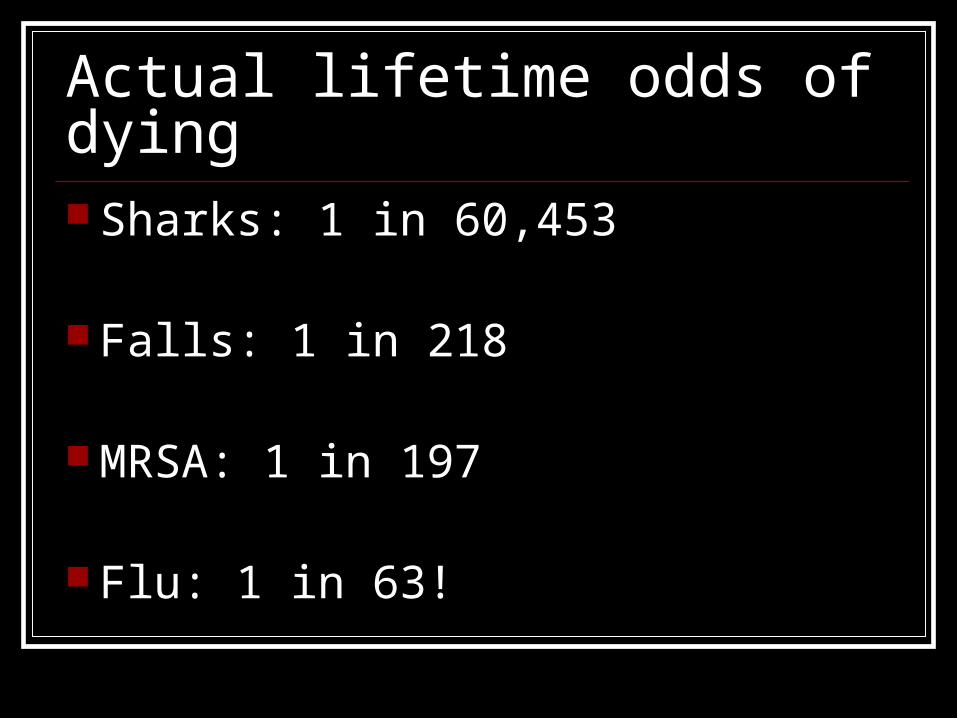
Actual lifetime odds of dying Sharks: 1 in 60,453
Falls: 1 in 218
MRSA: 1 in 197
Flu: 1 in 63!
Risk vs. Benefit We accept the risk of anaphylaxis
when prescribing antibiotics,
AS LONG AS
We think there is some benefit to the antibiotics for the pt.

Overutilization? Overuse is defined by multiple
federal overseers and review boards as: Testing for which no (or minimal)
benefit to the patient exists
Who has prescribed Abx?
…for sinus pressure? …for cough/bronchitis? …for sore throat?
31M with fever and sore throat, has exudates, tender ant. nodes, and no cough a. Bicillin shot!b. Z-packc. Rapid strep, Cx
if negd. Rapid strep, do
what is sayse. Suck it up, wuss

It’s cool, you haven’t killed (Probably)
But you haven’t helped
…and you might have killed

Sore throats 14 million visits in U.S./yr. Steroids/NSAIDS >> Abx NO evidence that it helps abscess ONLY evidence on rheumatic heart
from worst military outbreak ever
NNT? 40,000 NNH? 5 minor rxn, 6 to recur, 2500
majorSmartem.org, David Newman, AEM 2010
Let’s talk about Our cognitive errors
Assessing and communicating risk
Balancing risk and intervention


Unintended Consequences**
Interventions ALWAYS have the potential to create unanticipated and unforeseen events Perverse
Every intervention/test carries RISK and UNCERTAINTY RULE #1
LAW of UNINTENDED CONSEQUENCES
We are expected to detail these risks to our patients Informed consent: risk/benefit-
uncertainty on both ends
Risk assessment
We suck at this
Probability of Occurrence x Impact of Risk Event

We suck at probability, too. Statistics, anyone?
You test a bunch of people for HIV
1 is positive Likelihood of true positive?
Math! Test is 99.99% sensitive AND
specific
Out of 10,001 men, 1 has HIV
So what do you do with your positive guy?
Sir, your rapid test was positive, you need a repeat test but…
It’s
ver
y lik
e...
It’s
ver
y unli.
..
Pro
bable
, but .
..
Pro
bably
wro
ng
25% 25%25%25%a. It’s very likely correct
b. It’s very unlikely to be correct
c. Probable, but could be wrong
d. Probably wrong
Great for negatives (screen)
One pt. with HIV will be positive.
One other pt. will have a positive test.
50% chance that this is a true positive** PPV = 50% (RULE #2)
Testing?
On low prevalence groups leads to higher rates of false positives**
RULE #2
Screening Hgb A1C
Mammography
PSA
PSA
Screening PSA will result in an absolute mortality reduction of 33%
PSA 17 of 100 men will get a dx of CA
3 will die if untreated Treatment will save the life of 1 of
3* Treatment will kill 1 of the 17 10 of the 17 will be incontinent
and/or impotent
How you present the data matters
“98.5% safety from a particular disease”
That is exactly 1 in 63, the odds that you’ll be killed by flu in your lifetime.
How likely are you to pass the inservice?
50%
90%
95%
98%
99%
20% 20% 20%20%20%a. 50%b. 90%c. 95%d. 98%e. 99%
You did not grow a brain that likes small or huge numbers
All your brain sees is either a really high (98%, 99%) likelihood and rounds up
or a really low (1%, 2%) and rounds down
Probabilities are percentages
But real numbers work MUCH better RULE #3: USE REAL NUMBERS Want someone to go home?
“98% you’re ok!” Want someone admitted?
“1 out of 50 you’re dead!”

How do some docs manage risk?
TESTS We’re even told that pts. WANT tests.
Testing does not reduce legal action and might increase it

Every test is an additional intervention** RULE #1 Failure to follow up Failure to interpret correctly Failure to pursue to the correct test Alteration of the presenting frame Incidentaloma Radiation
Prevalence of incidental findings in trauma patients detected by computed tomography imaging
>3000 pts. 990 (32%) had Type I findings 1274 (41%) had Type II findings
631 incidentalomas concerning for nodules, masses

Incidence and Predictors of Repeated CT-PA in ED patients
Longitudinal study of 675 pts. 33% had repeat CT-PA 5% had >5 repeat CT-PA 75% had some CT scanning
Limitations: possible under-reporting
Don’t just stand there… Inherent predisposition to
intervening
Lack of tolerance for uncertainty
Errors of comission and omission are treated differently
Testing does not transfer risk
Most “high utilizers” are not driven by litigation fears
Most cite diagnostic concerns, “best for the pt.”, “don’t want to miss anything”

“Not missing anything” Implies need for diagnostic
certainty Relays fears of sudden unexpected
morbidity
Outcome based practice Low risk patients may not get a dx
Who’s the most conservative Jacobi attdg?
Per
rera
Gru
ber
Corc
iari
Hau
ghey
Jones
Sufa
i
17% 17% 17%17%17%17%a. Perrerab. Gruberc. Corciarid. Haugheye. Jonesf. Sufai
Most clinically cowboyish?
Per
rera
Gru
ber
Corc
iari
Hau
ghey
Jones
Sufa
i
17% 17% 17%17%17%17%a. Perrerab. Gruberc. Corciarid. Haugheye. Jonesf. Sufai
What if all the cowboyish guys worked fasttrack and main?
And the most conservative attdgs worked resus/trauma?
Poker, anyone?
Know thyself
Questions? We a low level of comfort with
uncertainty; it makes us want to do stuff
Testing low risk groups has problems
Discussion of risk and benefit (to whom and of what) is ongoing. Minimalists will win this discussion.
Take home We should expect much clearer
thinking about risk to our pts.
We should accept that we are responsible for both our actions and inactions, and tailor approach to pt.
Thank you
Dr. Schriger, UCLADr. Gallagher, MontefioreDr. Newman, Sinai
choosingwisely.orgTheNNT.combestbets.orgCochrane Review
@ercowboy