Rights / License: Research Collection In Copyright - Non … · 2020. 4. 21. · task situation....
212
Research Collection Doctoral Thesis Cognitive-motor interventions A novel approach to improve physical functioning in older adults Author(s): Pichierri, Giuseppe Publication Date: 2014 Permanent Link: https://doi.org/10.3929/ethz-a-010104076 Rights / License: In Copyright - Non-Commercial Use Permitted This page was generated automatically upon download from the ETH Zurich Research Collection . For more information please consult the Terms of use . ETH Library
Transcript of Rights / License: Research Collection In Copyright - Non … · 2020. 4. 21. · task situation....

Research Collection
Doctoral Thesis
Cognitive-motor interventionsA novel approach to improve physical functioning in older adults
Author(s): Pichierri, Giuseppe
Publication Date: 2014
Permanent Link: https://doi.org/10.3929/ethz-a-010104076
Rights / License: In Copyright - Non-Commercial Use Permitted
This page was generated automatically upon download from the ETH Zurich Research Collection. For moreinformation please consult the Terms of use.
ETH Library

DISS. ETH NO. 21604
Cognitive-motor interventions
–
A novel approach to improve physical
functioning in older adults
A thesis submitted to attain the degree of
DOCTOR OF SCIENCES of ETH ZURICH
(Dr. sc. ETH Zurich)
Presented by
GIUSEPPE PICHIERRI
MSc ETH HMS
born on 06.07.1979
citizen of Niederglatt (Zurich) and Italy
accepted on the recommendation of
PD Dr. Eling D. de Bruin
Prof. Dr. Kurt Murer
Prof. Dr. David P. Wolfer
2014


Table of Contents
Chapter 1 General Introduction 7 – 24
Chapter 2 Use of virtual reality technique for the training of motor
control in the elderly – Some theoretical considerations
Article published in Z Gerontol Geriat 2010, 43:229–234
25 – 41
Chapter 3 Cognitive and cognitive-motor interventions affecting
physical functioning: a systematic review
Article published in BMC Geriatrics 2011, 11:29
43 – 87
Chapter 4 The effects of a cognitive-motor intervention on voluntary
step execution under single and dual task conditions in
older adults: a randomized controlled pilot study
Article published in Clinical Interventions in Aging 2012:7 175–184
89 – 113
Chapter 5 A cognitive-motor intervention using a dance video game
to enhance foot placement accuracy and gait under dual
task conditions in older adults: A randomized controlled
trial (ISRCTN05350123)
Article published in BMC Geriatrics 2012, 12:74
115 – 147
Chapter 6 Assessment of the test-retest reliability of a foot placement
accuracy protocol in assisted-living older adults
Article published in Gait & Posture 38 (2013) 784–789
149 – 166
Chapter 7 General Discussion 169 – 186
Chapter 8 Summary / Zusammenfassung 189 – 213
Danksagungen
PhD curriculum
Curriculum vitae


One
General Introduction
Ch
ap
ter

6
Chapter One
The improvement of physical functioning and the prevention of falls in the older population
have been of great interest since the 1980‘s [1-3]. ‘Physical functioning‘ refers to the ability to
conduct a variety of activities ranging from self-care (instrumental activities of daily living)
to more challenging mobility tasks that require balance abilities, strength or endurance, e. g.
walking or standing, important for achieving or maintaining an independent way of living [4,5].
A fall is defined as a situation in which a person unintentionally comes to the ground
or to some lower level other than as a consequence of sustaining a violent blow, a loss
of consciousness, or a sudden onset of paralysis as in stroke or epileptic seizure [6]. The
interest in this topic lies in the fact that the decline of physical functioning and above
all the increasing incidence of falls are under the many undesirable ancillary effects of
the natural aging process and can lead as the case may be to a premature admission
to care homes, the loss of independence or even to an increasing rate of morbidity, or
mortality [7, 8].
Fall prevention is of particular importance when considering the steady increase of
life expectancy of human beings. Thanks to better sanitation, higher standards of living
and a well-organized and efficient health care system, life expectancy has nearly doubled
during the last century. In Switzerland, for instance, from 1900 to 2011 life expectancy
increased from 49 to about 85 years in women and from 46 to about 80 years in men [9].
It has been observed that approximately one third of the population over 65 years of age
statistically experience a fall each year. The incidence of falls even increases to 50% in
people aged 85 and over [8,10]. Falls are by now the leading cause of hospitalization
related to injuries in older adults. The major injuries that result from a fall are, besides soft
tissues injuries, serious fractures of the wrist, the elbow, the trunk, the head and the
hips [11,12]. Fear of falling is a common reported concern in older adults, especially in
individuals who have already experienced a fall, and can lead to a further decrease in
activity of daily life, a further decline in physical functioning and to a general decrease in
quality of life [13, 14].

7
General Introduction
1.1. Causes of a fall
The causes of a fall are still in dispute. The increased incidence of falls has long been
attributed to the decline of physical abilities, reduced sensory functions, and to the
slowdown of psychomotor processing, all being common consequences of the natural
aging process [15–17]. The decline in muscle mass and strength is a natural process of
aging which already begins at the young age of 30. Muscle mass declines by 10% – 15% per
decade, and even accelerates at older ages [18, 19]. Additionally, the reduction in muscle
power (strength x velocity of movement) due to the decline in mass and contractile speed
of the skeletal muscles leads to relevant restrictions in activities of daily life [19, 20]. This
may cause slowing, and increases variability of gait patterns or gives rise to insecurities in
balance, representing a possible major cause of a fall [21–23].
The American Geriatrics Society has suggested risk factors that seem to be related
to the higher risk for falling in institutionalized or community-dwelling older adults [7].
The main proposals included factors related to poor physical functioning like muscle
weakness, gait and/or balance deficits, and associated factors like previous falls, together
with the use of assistive devices due to reduced abilities (Table 1.1). In the past these
aspects have long been regarded as the main factors for the occurrence of a fall in older
adults. Not surprisingly, to date fall prevention programs for older adults mainly focus
on improving physical functioning by conducting interventions including physical
exercise to rehabilitate muscle strength and postural balance skills. The solution of the
fall problem, however, is not that simple as it appears. The origin of a fall is more likely
to be an individual framework composed of various risk factors rather than the result
of one or two factors alone. In addition to physical and functional impairments, this
framework also includes cognitive impairments, the influence of prescribed medications
and environmental conditions [11].
1.2. The role of cognition
One particular potential risk factor for falls has been overlooked in the past, namely
the presence of cognitive impairments in older adults. Recent research suggests a link

8
Chapter One
between gait dysfunctions and cognitive impairments [4]. In fact older adults with
cognitive impairments have a higher susceptibility to falling than peers without cognitive
impairments [24]. Older adults or younger persons with neurological impairments, people
suffering from the consequences of traumatic brain injuries or a stroke event, together
with sufferers from dementia show similar impairments of walking abilities, i.e. slower gait
speed and an increased stride time variability, as well as limitations in postural balance
abilities [25,26]. Gait dysfunctions are included among the many risk factors for falls. Older
adults with slow gait velocity, gait instability, or increased step length variability have an
increased risk of falls [26].
Table 1.1 Results of univariate analysis of most common risk factors for falls identified in 16 studies that examined risk factors [7]
Risk Factor Significant/Total* Mean RR-OR# Range
Muscle weakness 10/11 4.4 1.5 – 10.3
History of falls 12/13 3.0 1.7 – 7.0
Gait deficit 10/12 2.9 1.3 – 5.6
Balance deficit 8/11 2.9 1.6 – 5.4
Use assistive device 8/8 2.6 1.2 – 4.6
Visual deficit 6/12 2.5 1.6 – 3.5
Arthritis 3/7 2.4 1.9 – 2.9
Impaired ADL 8/9 2.3 1.5 – 3.1
Depression 3/6 2.2 1.7 – 2.5
Cognitive impairment 4/11 1.8 1.0 – 2.3
Age > 80 years 5/8 1.7 1.1 – 2.5
* Number of studies with significant odds ratio or relative risk ratio in univariate analysis/total number of studies that included each factor; # Relative risk ratios (RR) calculated for prospective studies, odds ratios (OR) calculated for retros-pective studies; ADL = activities of daily living.
Until recently gait has been assumed to be an automated task without the need for
higher-level cognitive inputs. This holds true for younger or middle-aged individuals.
Walking is a complex cognitive task [27]. The impact of cognitive functions on gait in
the older population, however, can be easily observed in every day situations. Older
adults tend to stop walking while talking [28,29] or seem to walk around with blinders
on, focusing their attention on their walking path, blocking out what is going on around

9
General Introduction
themselves, e.g. other pedestrians or the traffic. This observation is explained by the
assumption that cognitive resources intended for regulating the gait cycle come into
conflict with cognitive resources needed to hold a conversation or to register the changing
environmental conditions. One of the tasks will automatically be preferred to the other.
So they either stop walking and hold the conversation or observe their surroundings, or
conversely they stop talking or stop observing in order to continue on their walk. This
phenomenon has been consistently observed throughout many studies and the poorer
performance of older adults in dual task conditions is one of the most typical symptoms
of the natural aging process [30].
The impact of cognitive deficiencies on gait or postural balance is extensively
underpinned by a very substantial number of studies investigating the abilities of
older adults to manage a situation in which they are told to perform a motor task
while simultaneously executing a cognitive task [31]. This situation is referred as a dual
task situation. For instance, we can observe slowing of gait speed and/or an increased
variability of gait patterns like stride time, step length, or step width when older adults are
told to execute a cognitive task like calculating backwards from a number in steps of seven
or list words with a specific initial letter [15,32–34]. In addition, increasing reaction times
were observed in stepping responses when older adults are challenged by simultaneous
cognitive tasks [35]. Walking on the street is nothing else then a typical dual task situation
that we encounter almost every day. Hence, it is not surprising that the most frequent
causes for a fall are tripping, slipping or misplacing steps whilst walking without any
hazardous behavior even on level surfaces [36–38]. It has been observed that older adults
are at particular risk to experience a fall while they walk in busy environments [15,39].
1.3. The special role of executive functions
A challenging problem related to falls is that they can potentially occur in different
situations during daily activities and, unfortunately, in most of cases without any notice.
They can occur while standing motionless, during the phase of gait initiation or during
walking itself, even on level surfaces. Our body is constantly challenged by different

10
Chapter One
internal influences (muscle weakness, illness, fatigue, mood, cognitive impairments, vision
problems) as well as by external ones (obstacles, crowds, traffic, weather) all of which
constitute a potential threat to postural stability. These circumstances demand intact
cognitive functions to register potential threatening situations at an early stage, to plan
and execute the correct motor answer to the special condition in order to prevent a trip
or a fall. In recent fall prevention research the decline of cognitive functions that regulate
these abilities has been suggested as a major cause of falls in addition to the decline of
physical functioning [40,41]. In fact, impaired cognitive functions that regulate these
skills may negatively affect the ability to plan and react to changing demands, possibly
increasing fall risk [26].
The ability to counteract these threats is regulated by specific cognitive functions
called executive functions. ‘Executive functions‘ is an umbrella term for higher-level
cognitive functions involved in the control, the regulation, and the management of lower-
level cognitive processes, such as planning, working memory, problem solving, initiation,
inhibition, mental flexibility, task switching, and attention [42]. There is still a heated
debate on the brain structures responsible for the regulation of the theses functions.
The frontal lobes have long been assumed to be the only brain structures responsible
for executive functions [43]. Increasing evidence, however, suggests that multiple brain
areas forming a specific network are involved in cognitive processes as complex as the
executive functions [42, 44]. It has been observed that older adults perform more poorly
than younger adults on many classic neuropsychological tests of executive function (e.g.
the Color-Word Stroop task or the Trail-Making test A & B) [45]. This suggests that natural
aging is associated with a decline of executive functions [46–48].
Neuropsychological studies have observed activation in the prefrontal cortex, the
anterior part of the frontal lobes, during dual task conditions but not under single task
situations [49, 50]. Further, even age-specific activation of prefrontal cortex in response
to a dual task challenge has been observed. In a study by Ohsugi et al. [51] young and
older adults performed a single motor task (stepping), a single cognitive task (performing
calculations) or a dual task, that was the performance of the motor and cognitive task

11
General Introduction
simultaneously. Both younger and older adults demonstrated an increased prefrontal
cortex activity during the dual task activity, though higher and longer activation of the
prefrontal cortex was observed in the older group. These results suggest that dual task
activity imposes a greater cognitive load on older adults compared to younger.
The observation that older adults show poorer performances in dual task situations
compared to younger adults, and that this may be in part attributable to the declines in
executive functions [40] led to the assumption that the focus of effective fall prevention
programs should possibly be the implementation of approaches that address the cognitive
decline and the dysfunctions in cognitive processes, especially of the executive functions.
There is growing evidence that rather than isolated physical or cognitive activity, the
combination of both better supports the healthy functions of executive function, working
memory, and the ability to divide and select attention [52–55]. Therefore, older adults
should be challenged and trained by a cognitive-motor approach that is the performance
of physical training with a simultaneous challenge of cognitive functions stimulating the
required abilities to control gait and postural balance in dual task situations, as experienced
in everyday life. The assumption that older adults could benefit to a greater extent from a
cognitive-motor approach than from physical training alone is the underlying hypothesis
of the present doctoral thesis.
1.4. How it all started
The story of the present doctoral thesis began with the performance of interventional
and observational pilot studies at the Institute of Human Movement Sciences and Sport
(IBWS) of the ETH (Swiss Federal Institute of Technology) Zurich. Projects in the context of
a master‘s thesis in the field of ‘Human Movement Science and Sport‘ laid the foundations
for the development of the study questions presented in this thesis. The research group
at the IBWS of the ETH Zurich knew early on that the combination of motor and cognitive
elements and its implementation in training programs for the elderly could constitute
an approach with a great potential for improving physical functioning in the older
population. Two interventional pilot studies were performed using the combination of

12
Chapter One
motor and cognitive elements. The settings of these studies were comparable. Whereas
the control groups received a traditional physical exercise program consisting of strength
and balance exercises, the cognitive-motor groups performed either a computer-
based training program that focused on selective and divided attention skills [56] or a
computerized dancing game in addition [57]. The results showed excellent rates of training
adherence and high levels of enjoyment among the participants. More significantly, in the
cognitive-motor groups compared to the control groups the interventions were observed
to produce greater reductions in the fear of falling, and stronger improvements in walking
abilities (i.e. decreased dual task costs of walking) or shortened foot reaction times. These
observations instigated the further development of the cognitive-motor approach and
finally the realization of this doctoral thesis.
1.5. The aims of this doctoral thesis
This doctoral thesis discusses approaches that require consideration with a view
to including a stimulating cognitive factor in fall prevention programs. Therefore it
investigates the current state of research into using cognitive elements in fall prevention
and collects data on interventions with the aim of improving physical functioning in
older adults. Further, in its experimental section this doctoral thesis presents a novel
training approach that combines traditional physical exercise, i.e. progressive strength
and balance exercise, with an interactive dance computer game as the cognitive factor,
especially adapted to the needs of older adults. The game as cognitive-motor element
simulates a dual task situation thus stimulating the ability to comprehend, plan, adapt
and execute specific movements, properties attributed to the executive function system.
The aim of the experiments was primarily to investigate if a cognitive-motor approach
with an additional attention-demanding dance computer game is feasible and accepted
by older adults. Additionally, the experiments examined if such an approach is better
suited to improving physical abilities related to gait, i.e. walking abilities and gait
initiation under dual task conditions, or the accuracy of foot placement during walking
compared to the usual care offered in senior hostels or through physical exercise alone.

13
General Introduction
The objective of the cognitive-motor element was to develop a training method that can
be easily performed in any senior hostel without the need of a laboratory setting or any
complicated or expensive technical equipment.
1.6. The outline of this thesis
In a first step (Chapter 2) this doctoral thesis offers some theoretical considerations based
on the findings of the previous cognitive-motor pilot studies conducted at the Institute
of Human Movement Sciences and Sport of the ETH Zurich. It is concerned with the
experiences made with computer-based approaches serving as a potential method for
the inclusion and stimulation of cognitive functions in exercise programs for older adults.
The importance and potential benefits of using virtual reality environments or interactive
video games as a novel approach to improve physical functioning in older adults under
attention-demanding circumstances are discussed and suggestions for the design of
future studies are made.
On the basis of this discussion a systematic review of literature on cognitive and
cognitive-motor interventions affecting physical functioning in older adults is presented
in Chapter 3. This review pursues the objective of examining the existing literature
regarding the use of cognitive or combined cognitive-motor interventions. The aim is to
evaluate the level of evidence for this approach in the older population, to determine the
methodological quality of the existing studies, and to identify strategies that might be
used in future intervention type studies for older adults.
Chapters 4, 5, and 6 constitute the experimental section of this doctoral thesis. These
chapters describe the application of the cognitive-motor approach in senior hostels
in the context of two randomized controlled trials performed in four senior hostels in
Switzerland. Chapter 6 constitutes a study, which investigates the test-retest reliability
of a protocol used in the experiment described in Chapter 5 to assess foot placement
accuracy during walking.
In Chapter 4 a randomized controlled pilot study is described which aims to explore
whether a cognitive-motor exercise program that combines traditional physical exercise

14
Chapter One
with a dance computer game is better suited to improve the voluntary stepping responses
of older adults under attention-demanding dual task conditions. Residents of two senior
hostels of the city of Zurich perform either twice-weekly cognitive-motor exercise for 12
weeks (n = 9) or continue with the usual care offered at their hostels (n = 6). As the main
outcome, a measure voluntary step execution under single and dual task conditions is
recorded at baseline and post intervention.
Chapter 5 describes a randomized controlled trial performed in two senior hostels in
the Canton of Zurich with the aim to compare two training groups that achieve similar
amounts of strength and balance exercise where one group receives an intervention
that includes additional computer game dancing. The dance group (n = 15) absolves a
twelve-week cognitive-motor exercise program twice weekly that comprises progressive
strength and balance training supplemented with additional computer game dancing.
The control group (n = 16) performs only the strength and balance exercises during
this period. Main outcome measures are foot placement accuracy performance during
walking, gait performance under dual task conditions, and falls efficacy.
In Chapter 6 this doctoral thesis offers the results of an experiment to analyze the test-
retest reliability of the protocol used to assess foot placement accuracy performance in the
context of the randomized controlled trial presented in Chapter 5. One observer assesses
twenty-five elderly subjects in two sessions with 48 hours as time interval between the
measurements. The main outcome measures are foot placement distance errors, intraclass
correlation coefficients (ICC), and the smallest detectable difference value (SDD).
This doctoral thesis concludes with a general discussion where the main results,
methodological issues, clinical implications, suggestions for future work, and the
conclusions are outlined (Chapter 7). Finally, a short summary of the doctoral thesis in
English and German is provided in Chapter 8.

15
General Introduction
References
1. Duthie EH, Jr.: Falls. Med Clin North Am 1989, 73(6):1321-1336.
2. Mossey JM: Social and psychologic factors related to falls among the elderly.
Clin Geriatr Med 1985, 1(3):541-553.
3. Livesley B: Falls in older age. Br Med J (Clin Res Ed) 1984, 289(6445):568-569.
4. Woollacott M, Shumway-Cook A: Attention and the control of posture and gait: a
review of an emerging area of research. Gait Posture 2002, 16(1):1-14.
5. Hays RD, Liu H, Spritzer K, Cella D: Item response theory analyses of physical
functioning items in the medical outcomes study. Med Care 2007, 45(5 Suppl
1):S32-38.
6. Gibson M, Andres R, Isaacs B, Radebaugh T, Worm-Peters J: The prevention of falls in
later life. A report of the Kellogg International Work Group on the prevention of falls
by the elderly. Danish Medical Bulletin 1987, 34(4):1-24.
7. Guideline for the prevention of falls in older persons. American Geriatrics Society,
British Geriatrics Society, and American Academy of Orthopaedic Surgeons Panel on
Falls Prevention. J Am Geriatr Soc 2001, 49(5):664-672.
8. Berg WP, Alessio HM, Mills EM, Tong C: Circumstances and consequences of falls in
independent community-dwelling older adults. Age Ageing 1997, 26(4):261-268.
9. Schweizerisches Bundesamt für Statistik. Statistisches Jahrbuch der Schweiz. In.
Neuchâtel; 1900 - 2011.
10. Gill T, Taylor AW, Pengelly A: A population-based survey of factors relating to the
prevalence of falls in older people. Gerontology 2005, 51(5):340-345.
11. Rubenstein LZ, Josephson KR: The epidemiology of falls and syncope. Clin Geriatr
Med 2002, 18(2):141-158.
12. Tinetti ME, Williams CS: Falls, injuries due to falls, and the risk of admission to a
nursing home. N Engl J Med 1997, 337(18):1279-1284.
13. Howland J, Peterson EW, Levin WC, Fried L, Pordon D, Bak S: Fear of falling among the
community-dwelling elderly. J Aging Health 1993, 5(2):229-243.
14. Yardley L, Beyer N, Hauer K, Kempen G, Piot-Ziegler C, Todd C: Development and

16
Chapter One
initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing 2005,
34(6):614-619.
15. Bock O: Dual-task costs while walking increase in old age for some, but not for other
tasks: an experimental study of healthy young and elderly persons. J Neuroeng
Rehabil 2008, 5:27.
16. Lajoie Y, Gallagher SP: Predicting falls within the elderly community: comparison
of postural sway, reaction time, the Berg balance scale and the Activities-specific
Balance Confidence (ABC) scale for comparing fallers and non-fallers. Arch Gerontol
Geriatr 2004, 38(1):11-26.
17. Tinetti ME, Speechley M: Prevention of falls among the elderly. N Engl J Med 1989,
320(16):1055-1059.
18. Lindle RS, Metter EJ, Lynch NA, Fleg JL, Fozard JL, Tobin J, Roy TA, Hurley BF: Age and
gender comparisons of muscle strength in 654 women and men aged 20-93 yr. J
Appl Physiol 1997, 83(5):1581-1587.
19. Paterson DH, Jones GR, Rice CL: Ageing and physical activity: evidence to develop
exercise recommendations for older adults. Can J Public Health 2007, 98 Suppl
2:S69-108.
20. Porter MM: Power training for older adults. Appl Physiol Nutr Metab 2006, 31(2):87-94.
21. Daley MJ, Spinks WL: Exercise, mobility and aging. Sports Med 2000, 29(1):1-12.
22. Hausdorff JM, Edelberg HK, Mitchell SL, Goldberger AL, Wei JY: Increased gait
unsteadiness in community-dwelling elderly fallers. Arch Phys Med Rehabil 1997,
78(3):278-283.
23. Inzitari M, Newman AB, Yaffe K, Boudreau R, de Rekeneire N, Shorr R, Harris TB,
Rosano C: Gait speed predicts decline in attention and psychomotor speed in older
adults: the health aging and body composition study. Neuroepidemiology 2007,
29(3-4):156-162.
24. Muir SW, Gopaul K, Montero Odasso MM: The role of cognitive impairment in fall
risk among older adults: a systematic review and meta-analysis. Age Ageing 2012,
41(3):299-308.

17
General Introduction
25. Allali G, van der Meulen M, Assal F: Gait and cognition: the impact of executive
function. Schweizer Archiv für Neurologie und Psychiatrie 2010, 161(6):195-199.
26. Taylor ME, Ketels MM, Delbaere K, Lord SR, Mikolaizak AS, Close JC: Gait impairment
and falls in cognitively impaired older adults: an explanatory model of sensorimotor
and neuropsychological mediators. Age Ageing 2012, 41(5):665-669.
27. Hausdorff JM, Yogev G, Springer S, Simon ES, Giladi N: Walking is more like catching
than tapping: gait in the elderly as a complex cognitive task. Exp Brain Res 2005,
164(4):541-548.
28. Lundin-Olsson L, Nyberg L, Gustafson Y: „Stops walking when talking“ as a predictor
of falls in elderly people. Lancet 1997, 349(9052):617.
29. Beauchet O, Annweiler C, Dubost V, Allali G, Kressig RW, Bridenbaugh S, Berrut G,
Assal F, Herrmann FR: Stops walking when talking: a predictor of falls in older adults?
Eur J Neurol 2009, 16(7):786-795.
30. Beurskens R, Bock O: Age-related deficits of dual-task walking: a review. Neural Plast
2012, 2012:131608.
31. Verhaeghen P, Steitz DW, Sliwinski MJ, Cerella J: Aging and dual-task performance: a
meta-analysis. Psychol Aging 2003, 18(3):443-460.
32. Laessoe U, Hoeck HC, Simonsen O, Voigt M: Residual attentional capacity
amongst young and elderly during dual and triple task walking. Hum Mov Sci
2008, 27(3):496-512.
33. Li KZ, Lindenberger U, Freund AM, Baltes PB: Walking while memorizing: age-related
differences in compensatory behavior. Psychol Sci 2001, 12(3):230-237.
34. Lindenberger U, Marsiske M, Baltes PB: Memorizing while walking: increase in dual-
task costs from young adulthood to old age. Psychol Aging 2000, 15(3):417-436.
35. Melzer I, Oddsson LI: The effect of a cognitive task on voluntary step execution in
healthy elderly and young individuals. J Am Geriatr Soc 2004, 52(8):1255-1262.
36. Talbot LA, Musiol RJ, Witham EK, Metter EJ: Falls in young, middle-aged and older
community dwelling adults: perceived cause, environmental factors and injury. BMC
Public Health 2005, 5:86.

18
Chapter One
37. Campbell AJ, Borrie MJ, Spears GF, Jackson SL, Brown JS, Fitzgerald JL: Circumstances
and consequences of falls experienced by a community population 70 years and
over during a prospective study. Age Ageing 1990, 19(2):136-141.
38. Berg WP, Alessio HM, Mills EM, Tong C: Circumstances and consequences of falls in
independent community-dwelling older adults. Age Ageing 1997, 26(4):261-268.
39. Holtzer R, Verghese J, Xue X, Lipton RB: Cognitive processes related to gait velocity:
results from the Einstein Aging Study. Neuropsychology 2006, 20(2):215-223.
40. Hsu CL, Nagamatsu LS, Davis JC, Liu-Ambrose T: Examining the relationship between
specific cognitive processes and falls risk in older adults: a systematic review.
Osteoporos Int 2012, 23(10):2409-2424.
41. Yogev-Seligmann G, Hausdorff JM, Giladi N: The role of executive function and
attention in gait. Mov Disord 2008, 23(3):329-342; quiz 472.
42. Alvarez JA, Emory E: Executive function and the frontal lobes: a meta-analytic review.
Neuropsychol Rev 2006, 16(1):17-42.
43. Royall DR, Lauterbach EC, Cummings JL, Reeve A, Rummans TA, Kaufer DI, LaFrance
WC, Jr., Coffey CE: Executive control function: a review of its promise and challenges
for clinical research. A report from the Committee on Research of the American
Neuropsychiatric Association. J Neuropsychiatry Clin Neurosci 2002, 14(4):377-405.
44. Duffy JD, Campbell JJ: Regional prefrontal syndromes: A theoretical and clinical
overview. In: The frontal lobes and neuropsychiatric illness. Edited by Salloway SP,
Malloy PF, Duffy JD. Washington, DC, US: American Psychiatric Publishing, Inc.;
2001: 113-123.
45. Daniels K, Toth J, Jacoby L: The Aging of Executive Functions. In: Lifespan Cognition:
Mechanisms of Change. Edited by Bialystok E, Craik FIM. New York, USA: Oxford
University Press, Inc.; 2006.
46. Crawford JR, Bryan J, Luszcz MA, Obonsawin MC, Stewart L: The executive decline
hypothesis of cognitive aging: do executive deficits qualify as differential deficits
and do they mediate age-related memory decline? Aging, Neuropsychology, and
Cognition 2000, 7(1):9-31.

19
General Introduction
47. Ardila A, Ostrosky-Solis F, Rosselli M, Gomez C: Age-related cognitive decline
during normal aging: the complex effect of education. Arch Clin Neuropsychol 2000,
15(6):495-513.
48. O‘Sullivan M, Jones DK, Summers PE, Morris RG, Williams SC, Markus HS: Evidence for
cortical „disconnection“ as a mechanism of age-related cognitive decline. Neurology
2001, 57(4):632-638.
49. D‘Esposito M, Detre JA, Alsop DC, Shin RK, Atlas S, Grossman M: The neural basis of
the central executive system of working memory. Nature 1995, 378(6554):279-281.
50. Koechlin E, Basso G, Pietrini P, Panzer S, Grafman J: The role of the anterior prefrontal
cortex in human cognition. Nature 1999, 399(6732):148-151.
51. Ohsugi H, Ohgi S, Shigemori K, Schneider EB: Differences in dual-task performance
and prefrontal cortex activation between younger and older adults. BMC Neurosci
2013, 14:10.
52. Baddeley A: Working memory: looking back and looking forward. Nat Rev Neurosci
2003, 4(10):829-839.
53. Della Sala S, Baddeley A, Papagno C, Spinnler H: Dual-task paradigm: a means to
examine the central executive. Ann N Y Acad Sci 1995, 769:161-171.
54. Klingberg T: Limitations in information processing in the human brain:
neuroimaging of dual task performance and working memory tasks. Prog Brain Res
2000, 126:95-102.
55. Silsupadol P, Shumway-Cook A, Lugade V, van Donkelaar P, Chou LS, Mayr U, Woollacott
MH: Effects of single-task versus dual-task training on balance performance in older
adults: a double-blind, randomized controlled trial. Arch Phys Med Rehabil 2009,
90(3):381-387.
56. de Bruin ED, van Het Reve E, Murer K: A randomized controlled pilot study
assessing the feasibility of combined motor-cognitive training and its effect on gait
characteristics in the elderly. Clin Rehabil 2013, 27(3):215-225.
57. de Bruin ED, Reith A, Dörflinger M, Murer K: Feasibility of Strength-Balance Training
Extended with Computer Game Dancing in Older People; Does it Affect Dual

20
Chapter One
Task Costs of Walking? J Nov Physiother 2011, 1(104): Accessible at http://www.
omicsgroup.org/journals/2165-7025/2165-7025-2161-2104.php?aid=3350.

21
General Introduction


Two
Use of virtual reality technique for the training of motor control in the elderly:
some theoretical considerationsde Bruin ED1, Schoene D2, Pichierri G1 and Smith ST2
1Institute of Human Movement Sciences and Sport, ETH Zurich, Switzerland
2Neuroscience Research Australia, Sydney
published in Z Gerontol Geriat 2010, 43:229–234C
ha
pte
r

24
Chapter Two
Abstract
Virtual augmented exercise, an emerging technology that can help to promote physical
activity and combine the strengths of indoor and outdoor exercise, has recently been
proposed as having the potential to increase exercise behavior in older adults. By creating
a strong presence in a virtual, interactive environment, distraction can be taken to greater
levels while maintaining the benefits of indoor exercises which may result in a shift from
negative to positive thoughts about exercise. Recent findings on young participants show
that virtual reality training enhances mood, thus, increasing enjoyment and energy.
For older adults virtual, interactive environments can influence postural control and
fall events by stimulating the sensory cues that are responsible in maintaining balance
and orientation. However, the potential of virtual reality training has yet to be explored
for older adults. This manuscript describes the potential of dance pad training protocols
in the elderly and reports on the theoretical rationale of combining physical game-like
exercises with sensory and cognitive challenges in a virtual environment.
Keywords: geriatric adults, virtual reality, virtual environment, physical activity, indoor
exercise

25
Use of virtual reality technique
2.1. Background
Decline in physical function is a common feature of older age and has important
outcomes in terms of physical health related quality of life, falls, health care use,
admission to residential care and mortality [1, 2]. The most common reason for loss in
functional capabilities in the aged, however, is inactivity or immobility [3–5]. Even in
the absence of overt pathology, motor functioning [cf. International Classification of
Functioning (ICF) by the World Health Organization, Geneva (see http://www.who.int/
classification/icf) can deteriorate, as is illustrated by the incidence and impact of falls
in ageing populations [6]. Falls are amongst the most common reasons for medical
intervention in the elderly and their occurrence might initiate a vicious circle that causes
fear of falling, nursing home admittance and loss of independence [7]. Falls among older
adult populations often occur during walking, and gait dysfunction is included among
the many risk factors for falls [8, 9].
Until recently, gait was considered an automated motor activity requiring minimal
higher-level cognitive input [10]. Maintenance of postural control during activities of
daily living does not usually place high demands on attention resources of healthy young
or middle-aged people. In contrast however, when sensory or motor deficits occur due
to natural ageing processes, the complex generation of movement may have to be
restructured, and movements may then be controlled and performed at an associative
or a cognitive stage [11]. When the benefits from the movement automation are lost,
the postural control of aged people can be expected to be more vulnerable to cognitive
distractions and additional tasks [11]. The link between cognition, gait, and the potential
for falls is indeed being increasingly recognized [12] and is for example reflected in a
special issue in the Journal of Gerontology: Biological Sciences and Medical Sciences (63A
(12), 2008).
Negative plastic changes in the brain often occur naturally in later life when people begin
to stereotype and simplify behaviors that previously were quite complex and elaborated.
As people age, a self-reinforcing, downwards spiral of reduced interaction with challenging
environments and reduced brain health significantly contribute to this cognitive decline [13].

26
Chapter Two
2.2. Physical exercise to restore postural balance and walking function
Because difficulties of walking are a key factor in loss of independence for older
individuals [14, 15] treatment of gait disorders is designed to optimize gait for the
purpose of improving function. Previous studies have shown that physical exercise is
effective [16] and may reduce gait variability in elderly [17]. Current evidence shows that
interventions that aim to improve locomotor function in older people should preferably
include strength training in combination with balance and coordination exercises [16,
18]. However, common interventions usually focus on the physical aspects of training
while overlooking the specific rehabilitation of executive functions [19], a set of cognitive
abilities that control and regulate other abilities and behaviors.
A central element of successful cognitive rehabilitation for older adults should be the
design of interventions that either re-activate disused or damaged brain regions, or that
compensates for decline in parts of the brain through the activation of compensatory
neural reserves [20]. Cognitive activity or stimulation could be a protective factor against
the functional losses in old age. Because spatial and temporal characteristics of gait are
also associated with distinct brain networks in older adults it can be hypothesized that
addressing focal neuronal losses in these networks may represent an important strategy
to prevent mobility disability [21]. Interventions should, as previous research suggests,
focus thereby on executive functioning processes [22] and should include enriched
environments that provide physical activities with decision-making opportunities because
these are believed to be able to facilitate the development of both motor performance
and brain functions [23]. Executive cognitive functions are involved in the control and
direction (planning, monitoring, activating, switching, inhibiting) of lower level, more
modular, or automatic functions [24].
2.3. Virtual augmented exercises
Involvement of real-time simulation in an environment, scenario or activity that allows
for user interaction via multiple sensory channels as an approach to user–computer
interface can be defined as virtual reality [25]. Virtual reality (VR) system complexity

27
Use of virtual reality technique
ranges from cheap, readily available video gaming consoles such as the Nintendo Wii,
Sony Playstation or Microsoft Xbox, through to dedicated, high costs systems such as the
GestureTek IREX. The less complex and cheaper systems that require physical movement
by the game player sometimes are referred to as exergames. VR techniques are rapidly
expanding across a variety of disciplines. The use of virtual reality environments for virtual
augmented exercise has recently been proposed as having the potential to increase
exercise behavior in older adults [26] and also has the potential to influence cognitive
abilities in this population segment [27]. The potential is based on strong presence (the
feeling of being there) which is achievable in an interactive virtual environment and that
is followed by greater distraction. Weiss and colleagues [28] suggest that virtual reality
platforms provide a number of unique advantages over conventional therapy in trying to
achieve rehabilitation goals.
First, virtual reality systems provide ecologically valid scenarios that elicit naturalistic
movement and behaviors in a safe environment that can be shaped and graded in
accordance to the needs and level of ability of the patient engaging in therapy. Second,
the realism of the virtual environments allows patients the opportunity to explore
independently, increasing their sense of autonomy and independence in directing their
own therapeutic experience. Third, the controllability of virtual environments allows for
consistency in the way therapeutic protocols are delivered and performance recorded,
enabling an accurate comparison of a patient’s performance over time. Finally, virtual
reality systems allow the introduction of „gaming“ factors into any scenario to enhance
motivation and increase user participation [29].
The use of gaming elements can also be used to take patients’ attention away from
any pain resulting from their injury or movement. This occurs the more a patient feels
involved in an activity and again, allows a higher level of participation in the activity, as
the patient is focused on achieving goals within the game [30]. In combination with the
benefits of indoor exercises such as safety or independence from weather conditions,
such a distraction may result in a shift from negative to positive thoughts about exercise.
Many different forms of equipment can be used in order to create different kinds of

28
Chapter Two
virtual environments. The basic components of all forms are a computer, usually with
a special graphics card for the fast computation and drawing of two- (2D) or three-
dimensional (3D) visual images, display devices through which the user views the virtual
environment, hardware devices used to monitor movement kinematics or that provide
haptic and force feedback to participants, and especially written software that enables all
of these components to work in synchrony [31]. There are both more immersive 3D and
less immersive 2D virtual environments. The latter are more kindred to looking through
a window at a scene. Immersion refers to the establishment of the feeling of being inside
and a part of the VR world.
2.4. VR and exergames as motor rehabilitation training
Although VR applications have been used in research and entertainment applications
since the 1980s, it was only during the late 1990s that VR systems began to be developed
and studied as potential tools to enhance and encourage participation in rehabilitation.
Several studies have since emerged suggesting the potential of virtual reality as a successful
treatment and assessment tool in a wide variety of applications, most notably in the fields
of motor and cognitive rehabilitation. In young subjects, it has already been shown that
exercising on a stationary bike combined with a virtual cycling race enhances enjoyment
and reduces tiredness [32], and promotes gains in cognitive function in brain-injured
individuals [33]. For older adults interactive virtual environments can influence postural
control and therefore fall events by stimulating the sensory cues that are responsible in
maintaining balance and orientation [34].
Exergaming interventions (dance pad stepping, Wii balance board) improved
parameters of static balance more than a traditional balance program in young healthy
adults after 4 weeks of training [35]. Merians and colleagues [36] found that exercise
conducted using a virtual reality interface enhanced the training of hand movements
in patients post stroke, resulting in improved function of the fingers, thumb, and overall
range of motion. These researchers also found that an improvement later transferred to
real world tasks, demonstrating that VR-based therapy has the potential to encourage

29
Use of virtual reality technique
a level of exercise intensity and participation that is comparable to conventional
interventions [36]. The special value of VR training paradigms is believed to be due to
the concordance of visual and proprioceptive information during training, thus updating
the way seniors perceive their body with their environment [37]. Beside this stimulation,
virtual environments provide salient feedback about the movement performance,
and the difficulty of the task can be adapted according to the subject’s ability, which is
particularly important for older adults. Virtual environments have also the potential to
specifically include motor learning enhancing features that activate motor areas in the
brain [38]. In addition the findings of You and colleagues suggest that VR training could
induce reorganization of the sensorimotor cortex in chronic stroke patients [39]. However,
the potential of such virtual reality trainings has yet to be explored for older adults.
In the following, to cite an example, we describe a low cost video game-based approach
to training and rehabilitation of stepping ability that can potentially be used to reduce the
risk of falls in older adults or for rehabilitation of balance control in stroke, spinal cord
injury or other motor-impaired patients. We describe the theoretical considerations that
indicate the potential of this technology for elderly together with some preliminary results
from our research groups.
2.5. Exergame use for motor control training in the elderly
Interactive, user input devices such as dance pads are a low cost, interactive method of
exergaming. These games, e.g. “Dance Dance Revolution” (DDR) or “Pump” are played on
a dance pad sensor, which measures about 1 m2 and has between four and eight step
panels (arrows). The pad is connected to a visual display screen such as a television or
computer screen that provides step direction instructions to the player via a system of
scrolling arrows that typically rise slowly from the bottom to the top of the screen. As
the arrows scroll up to the top of the screen, they cross over a set of four corresponding
arrow silhouettes. The player must step on the corresponding mat arrow as the scrolling
arrow crosses its silhouette (Figure 2.1). Sequences of steps can range in difficulty from
simple marching or walking patterns to those with varied rates and irregular patterns that

30
Chapter Two
challenge coordination and attention. It has been suggested that feed-forward planning
of gait and posture is diminished in older adults. Motor adaptation is one mechanism by
which feed-forward commands can be updated or fine-tuned [40].
The ability to make timely, appropriately directed steps underpins our ability to maintain
our balance and move unaided through our environment [41]. Stepping, which involves
changing the base of support (BOS) relative to our center of mass (COM), also provides
the means by which we are able to counter potentially destabilizing events such as slips,
trips and missteps and avoid obstacles. Protective stepping may be initiated volitionally
when a threat to balance is perceived, or induced reflexively when a disturbance moves
the COM relative to the BOS at a speed that prevents engagement of volitional strategies.
Initial studies suggest that both volitional and induced stepping abilities are significantly
impaired in older versus younger individuals and are good predictors of falls. Compared to
younger adults, older adults, particularly those with a history of falling, tend to be slower
in initiating volitional step responses [42], make inappropriately directed or multiple
short steps in response to an external perturbation of balance [43] and in response to
lateral perturbations have an increased chance of collision between the swing and
stance legs during compensatory stepping [44]. There is evidence, however, to suggest
that the timing of volitional stepping [45, 46], as well as the execution of successful steps
for recovery of balance following an induced slip [47], can be significantly improved in
older adults following repetitive training of stepping responses. Maki and colleagues [48]
have recently suggested a protocol for step training which specifically targets the kinds
of stepping abilities that contribute to falls such as collisions between legs during lateral
perturbation or the tendency for older adults to take multiple, short laterally directed steps
in response to an anterior-posterior perturbation. Although the training techniques they
suggest are well suited to specifically train compensatory stepping ability their approach
requires use of large devices (custom motion platforms [48], treadmills [47, 49], systems
employing weights and pulleys [46], low resistance slip platforms) or the supervision
of trained therapists [45]. None of these techniques could be easily or economically
incorporated into home-based training programs. Dance pad games require the player to

31
Use of virtual reality technique
make rapid step responses from either leg to a target location in response to a presented
visual stimulus. They not only involve controlled body weight transfers that are similar
to the step responses required to avoid many falls as well as requiring a narrow base of
support and well-coordinated quick movements. They further require cognitive work,
e.g. sensing of stimuli, paying attention and making quick decisions. This interaction
of sensory, information processing and neuromuscular systems is similar to the step
responses required to avoid many falls and is therefore suitable as an intervention in a
fall-specific context (Figure 2.2).
One hurdle facing the successful use of such exercise video games (or exergames) in
older adult and functionally impaired populations is that many off-the-shelf video games
are too complex for use by these groups. Video games must therefore be developed to
take into consideration the cognitive and physical limitations, as well as the interest sets,
of older adults. In the following we discuss the ways in which research groups in general
could address these issues and in which our respective research teams are presently
involved.
Figure 2.1: Training set-up for the dance pad game. The core game play involves the player moving his or her feet to a set pattern, stepping in time to the general rhythm or beat of a song. During normal game play, arrows scroll upwards from the bottom of the screen and pass over a set of stationary arrows near the top (upper red circle) referred to as the “guide arrows” or “receptors”. When the scrolling arrows overlap the stationary ones, the player must step on the corresponding arrows on the dance platform (lower red circle), and the player is given a judgement for their accuracy (Marvelous, Perfect, Great, Good, Boo/Almost, Miss/Boo) [51].

32
Chapter Two
PerceptionAction planExecution
Falls Dance pad stepping
2.6. The use of DDR to date
The Sydney-based research group at Neuroscience Research Australia (DS & STS) has
recently begun a research program aimed at developing age-appropriate DDR (Dance
Dance Revolution)-style video games. The aim of this group is to both engage older adults
in home-based step training exercises to reduce their falls rate as well as monitoring fall
risk. In particular they aim to develop a low-cost approach to engage older adults in fall
prevention training that can be placed into the houses of individuals, many of them
living in regional, remote parts of Australia. A recently published paper [50] describes a
series of studies conducted to develop and establish characteristics of DDR videogame
play in older adults. Participants aged 70 and above were asked to make simple step
movements in response to vertically drifting arrows presented on a video screen. Step
responses were detected by a modified USB DDR mat and characteristics of stepping
performance such as step timing, percentage of missed target steps and percentage of
correct steps, were recorded by purpose built software. Drift speed and step rate of visual
stimuli were modified to increase task difficulty. Performance of older adults decreased
as stimulus speed and step rate were increased. Optimal step performance occurred for
a stimulus speed of 17° of visual angle per second and a step rate of one step every 2
seconds. At fast drift speeds (up to 35°/second), participants were more than 200 ms too
slow in coordinating their steps with the visual stimulus. Younger adults were better able
to perform the stepping task across a wider range of drift speeds than older adults.
Data of another recently finished study from this group indicate that the dance pad
is a valid and reliable assessment instrument to measure the choice stepping reaction
Figure 2.2: Processes involved in avoiding a fall and in dance pad stepping.

33
Use of virtual reality technique
time in old and young people, a test that has shown to be predictive for falls in the elderly
[42]. This offers the opportunity to assess the fall risk of older adults on a regular basis
from the comfort of their own home. The aim of a recently finished study in Zurich was to
assess and compare the effects of a physical training program that included a VR dance
simulation computer game against usual care exercise interventions for elderly residential
care dwellers on relative dual tasking costs of walking [51]. These costs refer to the fact
that many older adults exhibit a reduced ability to perform two tasks at the same time,
e.g. walking at preferred speed is compared to walking at preferred speed whilst counting
backwards. This study showed that elderly who were training physically, in combination
with a VR dance game that required decision making, showed significant decreases in
the relative dual task costs (DTC) of walking. These walking parameters did not change
in individuals that trained with more traditional forms of training in usual care programs.
The possibility of improving gait while performing dual tasks has not been well
studied in general [10] and, to the best of our knowledge, this study [51] is one of the
first that showed an effect on DTC-related walking. This study, which has been submitted
for publication as a full text article, used dancing in a virtual environment as dual task
training, where subjects were expected to observe the environment for drifting arrows
and at the same time were initiating dance steps (Figure 2.1).
2. 7. Conclusions
For older adults virtual, interactive environments have large potential to influence postural
control and fall events by stimulating the sensory cues that are responsible in maintaining
balance and orientation and by improving stepping patterns. However, the potential of
virtual reality training has yet to be explored in sufficiently powered randomized controlled
trials. Dance pad games, where repetitive medio-lateral and anterior-posterior steps
are required offer a novel, yet effective, technique for training stepping ability in older
adults. Future research should develop, implement and evaluate VR exercise scenarios for
various sub-populations that can be identified within the elderly adult population. In such
projects an attempt could be made to get insight into the concept of motor learning in

34
Chapter Two
VR and the relationship between cognitive functions and balance and gait skills in elderly.
Conflict of interest
The corresponding author states that there are no conflicts of interest.

35
Use of virtual reality technique
References
1. Freedman VA, Martin LG, Schoeni RF: Recent trends in disability and functioning
among older adults in the United States: a systematic review. Jama 2002,
288:3137-3146.
2. Gill TM, Kurland B: The burden and patterns of disability in activities of daily living
among community-living older persons. J Gerontol A Biol Sci Med Sci 2003, 58:70-75.
3. Goldspink DF: Ageing and activity: their effects on the functional reserve
capacities of the heart and vascular smooth and skeletal muscles. Ergonomics
2005, 48:1334-1351.
4. Pluijm SM, Visser M, Puts MT et al: Unhealthy lifestyles during the life course:
association with physical decline in late life. Aging Clin Exp Res 2007, 19:75-83.
5. Taylor AH, Cable NT, Faulkner G et al: Physical activity and older adults: a review of
health benefits and the effectiveness of interventions. J Sports Sci 2004, 22:703-725.
6. Moreland J, Richardson J, Chan DH et al: Evidence-based guidelines for the secondary
prevention of falls in older adults. Gerontology 2003, 49:93-116.
7. Hausdorff JM, Edelberg HK, Mitchell SL et al: Increased gait unsteadiness in
community-dwelling elderly fallers. Arch Phys Med Rehabil 1997, 78:278- 283.
8. Campbell AJ, Borrie MJ, Spears GF: Risk factors for falls in a community-based
prospective study of people 70 years and older. J Gerontol 1989, 44:M112-117.
9. Rubenstein LZ, Robbins AS, Schulman BL et al: Falls and instability in the elderly. J Am
Geriatr Soc 1988, 36:266-278.
10. Yogev-Seligmann G, Hausdorff JM, Giladi N: The role of executive function and
attention in gait. Mov Disord 2008, 23:329-342; quiz 472.
11. Laessoe U, Hoeck HC, Simonsen O, Voigt M: Residual attentional capacity
amongst young and elderly during dual and triple task walking. Hum Mov Sci
2008, 27:496-512.
12. Alexander NB, Hausdorff JM: Guest editorial: linking thinking, walking, and falling. J
Gerontol A Biol Sci Med Sci 2008, 63:1325-1328.
13. Mahncke HW, Bronstone A, Merzenich MM: Brain plasticity and functional losses in

36
Chapter Two
the aged: scientific bases for a novel intervention. Prog Brain Res 2006, 157:81-109.
14. Alexander NB: Gait disorders in older adults. J Am Geriatr Soc 1996, 44:434-451.
15. Sauvage LR Jr, Myklebust BM, Crow-Pan J et al: A clinical trial of strengthening and
aerobic exercise to improve gait and balance in elderly male nursing home residents.
Am J Phys Med Rehabil 1992, 71:333-342.
16. Mian OS, Baltzopoulos V, Minetti AE, Narici MV: The impact of physical training on
locomotor function in older people. Sports Med 2007, 37:683-701.
17. Hausdorff JM, Rios DA, Edelberg HK: Gait variability and fall risk in community-living
older adults: a 1-year prospective study. Arch Phys Med Rehabil 2001, 82:1050-1056.
18. Skelton DA, Beyer N: Exercise and injury prevention in older people. Scand J Med Sci
Sports 2003, 13:77-85.
19. Studer M: Rehabilitation of executive function: to err is human, to be aware-divine. J
Neurol Phys Ther 2007, 31:128-134.
20. Hogan M: Physical and cognitive activity and exercise for older adults: a review. Int J
Aging Hum Dev 2005, 60:95-126.
21. Rosano C, Aizenstein H, Brach J et al: Special article: gait measures indicate underlying
focal gray matter atrophy in the brain of older adults. J Gerontol A Biol Sci Med Sci
2008, 63:1380-1388.
22. Rapport LJ, Hanks RA, Millis SR, Deshpande SA: Executive functioning and predictors
of falls in the rehabilitation setting. Arch Phys Med Rehabil 1998, 79:629-633.
23. Yan JH, Zhou CL: Effects of motor practice on cognitive disorders in older adults. Eur
Rev Aging Phys Act 2009, 6:67-74.
24. Cicerone K, Levin H, Malec J et al: Cognitive rehabilitation interventions for executive
function: moving from bench to bedside in patients with traumatic brain injury. J
Cogn Neurosci 2006, 18:1212-1222.
25. Adamovich SV, Fluet GG, Tunik E, Merians AS: Sensorimotor training in virtual reality:
a review. Neuro Rehabilitation 2009, 25:29-44.
26. Van Schaik P, Blake J, Pernet F et al: Virtual augmented exercise gaming for older
adults. Cyberpsychol Behav 2008, 11:103-106.

37
Use of virtual reality technique
27. Zelinski EM, Reyes R: Cognitive benefits of computer games for older adults.
Gerontechnology 2009, 8:220-235.
28. Kizony R, Raz L, Katz N et al: Video-capture virtual reality system for patients with
paraplegic spinal cord injury. J Rehabil Res Dev 2005, 42:595-608.
29. Holden M, Todorov E: Use of virtual environments in motor learning and rehabilitation.
In: Stanney K (ed) Handbook of virtual environments: design, implementation, and
applications. Mahwah, NJ, Erlbaum, 2002, pp 999-1026.
30. Sanchez-Vives MV, Slater M: From presence to consciousness through virtual reality.
Nat Rev Neurosci 2005, 6:332-339.
31. Holden MK: Virtual environments for motor rehabilitation: review. Cyberpsychol
Behav 2005, 8:187-211; discussion 212-189.
32. Plante T, Aldridge A, Bogden R, Hanelin C: Might virtual reality promote the mood
benefits of exercise? Computers in Human Behavior 2003, 19:495-509.
33. Grealy MA, Johnson DA, Rushton SK: Improving cognitive function after brain injury:
the use of exercise and virtual reality. Arch Phys Med Rehabil 1999, 80:661-667.
34. Virk S, McConville KM: Virtual reality applications in improving postural control and
minimizing falls. Conf Proc IEEE Eng Med Biol Soc 2006, 1:2694-2697.
35. Brumels KA, Blasius T, Cortright T et al: Comparison of efficacy between traditional
and video game based balance programs. Clinical Kinesiology: Journal of the American
Kinesiotherapy Association 2008, 62:26-31.
36. Merians AS, Poizner H, Boian R et al: Sensorimotor training in a virtual reality
environment: Does it improve functional recovery poststroke? Neurorehabil Neural
Repair 2006, 20:252-267.
37. Bisson E, Contant B, Sveistrup H, Lajoie Y: Functional balance and dual-task reaction
times in older adults are improved by virtual reality and biofeedback training.
Cyberpsychol Behav 2007, 10:16-23.
38. Cross ES, Kraemer DJ, Hamilton AF et al: Sensitivity of the action observation network
to physical and observational learning. Cereb Cortex 2009, 19:315-326.
39. You SH, Jang SH, Kim YH et al: Virtual reality-induced cortical reorganization and

38
Chapter Two
associated locomotor recovery in chronic stroke: An experimenter-blind randomized
study. Stroke 2005, 36:1166-1171.
40. Tseng SC, Stanhope SJ, Morton SM: Visuomotor adaptation of voluntary step
initiation in older adults. Gait Posture 2010, 31:180-184.
41. Shumway-Cook A, Woollacott MH: Motor control: theory and practical applications.
Baltimore, Williams & Wilkins, 1995.
42. Lord SR, Fitzpatrick RC: Choice stepping reaction time: a composite measure of falls
risk in older people. J Gerontol A Biol Sci Med Sci 2001, 56: M627-632.
43. McIlroy WE, Maki BE: Age-related changes in compensatory stepping in response to
unpredictable perturbations. J Gerontol A Biol Sci Med Sci 1996, 51:M289-296.
44. Maki BE, Edmondstone MA, McIlroy WE: Age-related differences in laterally directed
compensatory stepping behavior. J Gerontol A Biol Sci Med Sci 2000, 55:M270-277.
45. Jobges M, Heuschkel G, Pretzel C et al: Repetitive training of compensatory steps:
A therapeutic approach for postural instability in Parkinson's disease. J Neurol
Neurosurg Psychiatry 2004, 75:1682-1687.
46. Rogers MW, Johnson ME, Martinez KM et al: Step training improves the speed of
voluntary step initiation in aging. J Gerontol A Biol Sci Med Sci 2003, 58:46-51.
47. Pai YC, Bhatt TS: Repeated-slip training: an emerging paradigm for prevention of slip-
related falls among older adults. Phys Ther 2007, 87:1478-1491.
48. Mansfield A, Peters AL, Liu BA, Maki BE: A perturbation-based balance training
program for older adults: study protocol for a randomised controlled trial. BMC
Geriatr 2007, 7:12.
49. Shimada H, Obuchi S, Furuna T, Suzuki T: New intervention program for preventing
falls among frail elderly people: the effects of perturbed walking exercise using a
bilateral separated treadmill. Am J Phys Med Rehabil 2004, 83:493-499.
50. Smith ST, Sherrington C, Studenski S et al: A novel dance dance revolution (ddr)
system for inhome training of stepping ability: basic parameters of system use by
older adults. Br J Sports Med 2011, 45(5):441-445.
51. de Bruin ED, Reith A, Dörflinger M, Murer K Feasibility of strength-balance training

39
Use of virtual reality technique
extended with computer game dancing in older people; does it affect dual task cost
of walking?. J Nov Physiother 2011, 1(104): Accessible at http://www.omicsgroup.
org/journals/2165-7025/2165-7025-2161-2104.php?aid=3350.


Three
Cognitive and cognitive-motor interventions affecting physical
functioning: A systematic reviewPichierri G1, Wolf P2, Murer K1 and de Bruin ED1
1Institute of Human Movement Sciences and Sport, ETH Zurich, Switzerland
2Department of Mechanical and Process Engineering, ETH Zurich, Switzerland
published in BMC Geriatrics 2011, 11:29 (www.biomedcentral.com/1471-2318/11/29)
Ch
ap
ter

Chapter Three
42
Abstract
Background: Several types of cognitive or combined cognitive-motor intervention types
that might influence physical functions have been proposed in the past: training of dual-
tasking abilities, and improving cognitive function through behavioral interventions or
the use of computer games. The objective of this systematic review was to examine the
literature regarding the use of cognitive and cognitive-motor interventions to improve
physical functioning in older adults or people with neurological impairments that
are similar to cognitive impairments seen in aging. The aim was to identify potentially
promising methods that might be used in future intervention type studies for older adults.
Methods: A systematic search was conducted for the Medline/Premedline, PsycINFO,
CINAHL and EMBASE databases. The search was focused on older adults over the age of
65. To increase the number of articles for review, we also included those discussing adult
patients with neurological impairments due to trauma, as these cognitive impairments
are similar to those seen in the aging population. The search was restricted to English,
German and French language literature without any limitation of publication date or
restriction by study design. Cognitive or cognitive-motor interventions were defined as
dual-tasking, virtual reality exercise, cognitive exercise, or a combination of these.
Results: 28 articles met our inclusion criteria. Three articles used an isolated cognitive
rehabilitation intervention, seven articles used a dual task intervention and 19 applied a
computerized intervention. There is evidence to suggest that cognitive or cognitive-motor
methods positively affect physical functioning, such as postural control, walking abilities
and general functions of the upper and lower extremities, respectively. The majority of the
included studies resulted in improvements of the assessed functional outcome measures.
Conclusions: The current evidence on the effectiveness of cognitive or cognitive-motor
interventions to improve physical functioning in older adults or people with neurological
impairments is limited. The heterogeneity of the studies published so far does not

Cognitive and cognitive-motor interventions
43
allow defining the training methodology with the greatest effectiveness. This review
nevertheless provides important foundational information in order to encourage further
development of novel cognitive or cognitive-motor interventions, preferably with a
randomized control design. Future research that aims to examine the relation between
improvements in cognitive skills and the translation to better performance on selected
physical tasks should explicitly take the relation between the cognitive and physical skills
into account.
3.1. Background
Age-related deteriorations in physical functioning have been attributed to decreases in
sensory or motor system function [1]. 'Physical functioning' refers to the ability to conduct
a variety of activities ranging from self-care (instrumental activities of daily living) to
more challenging mobility tasks that require balance abilities, strength or endurance,
e.g. walking or standing, important for achieving or maintaining an independent way of
living [2,3]. Until recently, for example, gait was considered an automated motor activity
requiring minimal higher-level cognitive input [4]. Therefore, it seemed only logical that
prevention of falls was mainly focused on exercises that address the modifiable physical
aspects of fall related mobility impairments, e.g. strength and balance training [5–7].
Consistent evidence has been accumulated that regular physical training can improve
muscle strength, aerobic capacity and balance, and delay the point in time when older
adults need assistance to manage activities of daily living [5]. Maintenance of postural
control during activities of daily living does not usually place high demands on attentional
resources of healthy young or middle-aged people. In contrast, when sensory or motor
deficits occur due to the natural aging process, the complex generation of movement may
have to be adjusted. Movements may then be controlled and performed at an associative
or a cognitive stage. Consequently, the postural control of older adults might be more
vulnerable to cognitive distractions and additional tasks [8]. Recent research indicates
that the influence of motor and sensory impairments on falls is in part moderated by the
executive functions [9] and, thus, some of the causes of gait disturbances might also be

Chapter Three
44
attributed to changes in the executive functions [4], e.g., changes in divided attention
[10,11]. 'Executive function' refers to cognitive processes that control and integrate other
cognitive activities [12,13], and this term has been used to describe a group of cognitive
actions that include: dealing with novelty, planning and implementing strategies for
performance, monitoring performance, using feedback to adjust future responding,
vigilance, and inhibiting task-irrelevant information [12] of lower level, more modular,
or automatic functions [14]. Common tasks of daily life require attention, rapid motor
planning process, and effective inhibition of irrelevant or inappropriate details. Older
adults, however, experience increasing difficulties in maintaining multiple task rules in
working memory [15].
These findings imply that in addition to physical forms of training, we should possibly
also consider cognitive rehabilitation strategies that aim to influence physical functioning,
e.g., walking behavior of older adults [16]. The question remains, however, what the best
strategies are, that can support achieving this aim.
Several types of cognitive or cognitive-motor interventions that might be able to
improve physical functioning have been proposed in the past: cognitive rehabilitation
interventions, training of dual-tasking abilities, and the use of computer games or virtual
reality [4,17].
Cognitive rehabilitation, defined by the Brain Injury Interdisciplinary Special Interest
Group (BI-ISIG) of the American Congress of Rehabilitation Medicine as a „systematic,
functionally-oriented service of therapeutic cognitive activities, based on an assessment
and understanding of the person‘s brain-behavior deficits“ [18], has shown to be effective
in clinical practice [19,20].
Cognitive rehabilitation interventions have been developed to ameliorate cognitive
problems experienced by healthy older adults [21,22], and for adults suffering from
traumatic brain injury [19,23,24], with the goal of maximizing their current cognitive
functioning and/or reducing the risk of cognitive decline. Some of the cognitive
interventions, however, also show transfer effects to physical functioning. Specific motor
imagery protocols seem to improve mobility in people with stroke [25].

Cognitive and cognitive-motor interventions
45
Cognitive-motor interventions are interventions that combine a cognitive with a physical
rehabilitation task, e.g. strength and balance exercises together with cognitive exercises
or performing dual-tasking exercises. Interventions that used dual-tasking paradigms
demonstrated negative effects on postural control or gait while performing a concurrent
cognitive task in older adults [26,27], in patients with brain injury [28,29] and Alzheimer‘s
disease [30]. Several authors have suggested that procedures to improve the dual task
performance of elderly should be included in fall prevention programs [31].
Computerized interventions can be divided into biofeedback based systems or systems
that use elements of virtual reality. Becoming aware of various physiological functions
by using instruments that provide information on the activity of those same systems is
considered biofeedback training. The goal, thereby, is to be able to manipulate these
systems at will. Processes that can be controlled include for example dynamic balance
on a force platform where visual feedback gives information about the center of pressure
movements [32]. In virtual reality, in contrast to biofeedback training, environments are
created that allow users to interact with images and virtual objects that appear in the
virtual environment in real-time through multiple sensory modalities [32,33]. Playing of
computer games induced cognitive benefits in older adults [34], and is proposed as a
training strategy that may transfer to physical activity related tasks [4].
All three strategies, cognitive rehabilitation, training of dual-tasking abilities, and
computerized interventions, have mainly been applied to individuals with stroke, with
traumatic brain injury or elderly. Although it seems intuitive that these groups cannot be
compared because of the different underlying causes for their respective brain deficits,
this may not actually be the case [35,36]. Studies using a neuropsychological deficit profile
methodology suggest that the pattern and extent of cognitive decline associated with
these conditions is similar, at least partly, for both cognitive and motor deficits [36,37].
This implies that the treatment approaches needed to remediate the observed deficits are
theoretically also comparable.
The objective of this systematic review is to examine the literature regarding the
use of cognitive and cognitive-motor interventions to improve physical functioning in

Chapter Three
46
older adults and in adults with neurological impairments. The aim is to identify strategies
that have the potential to affect physical functioning and that might be used in future
intervention type studies for older adults. The specific questions that we asked were:
1. What types of cognitive and cognitive-motor intervention methods have been
used to influence physical functioning of older adults or adults with neurological
impairments?
2. What is the level of evidence for cognitive and cognitive-motor interventions to
influence physical functioning in these populations?
3. What is the methodological quality of these studies?
The underlying assumption that drives these questions is that (changes in) cognition also
has an impact on physical functioning.
3.2. Methods
3.2.1. Data sources and search strategies
In a first step we undertook a scoping review to gain an overview about existing
interventions or systematic reviews on this topic. In addition to studies conducted with
older adults, interventions with traumatic brain injury patients and patients with stroke
were found. Like older adults, people with brain injury or stroke show difficulties with
postural balance, exhibit gait insecurities when performing dual tasks and have cognitive
deficits evident in working memory, attention, and information processing [35,38].
Additionally it has been shown that people with brain injuries show similar characteristics
as older adults with an advanced aged-related cognitive decline. The patterns of cognitive
decline observed in patients after traumatic brain injury resembles that of classic aging
processes [35,39,40].
The search strategy was focused on older adults over the age of sixty-five. Although
we are aware that cognitive and physical deficits in patients with brain injury are not fully
comparable with the natural aging process we additionally searched further studies with
brain injured patients. We also decided to include studies conducted with stroke patients
arising from our search, because of their methodological importance for this review and

Cognitive and cognitive-motor interventions
47
the possible applicability of the applied methods in the general older population.
We developed an individualized electronic search strategy for the Medline/Premedline,
PsycINFO, CINAHL, and EMBASE databases in collaboration with a librarian from the
Medicinal Library of the University of Zurich. The search was restricted to English, German,
and French language literature. There was no limitation of publication date or restriction
by study design. The final search was performed in July 2010.
Table 3.1 Search strategy
Area Search terms
Population (aging or aged or elder*); exp Aged; exp Brain Injuries((injur* or trauma*) adj2 (brain or head or craniocerebral))
Outcomes/ Physical aspect ((quantify* or measure* or assess* or investigat* or examin* or evaluat*) adj5 (gait or walk* or balance or movement or mobility or posture or “motor function” or “physical functioning” or frailty)(balance adj3 (training or impair* or effect*))postural balance, gait, walking; Accidental Falls [Prevention and Control]equilibrium, postur*
Intervention (strateg* adj3 (training or learning or cognit* or metacognit*))((cognit* or metacognit*) adj3 (intervention or rehabilitation or task or strateg* or therap*)); (goal adj1 (setting or planning or attain* or achiev* or direct* or orient* or manag*)); (self adj3 (talk or evaluat*))(self adj3 (awareness or monitoring or control or instruction or regulation))(“executive functions” or metacognition or awareness or “problem solving” or metamemory or attention); biofeedback, user-computer interface(action game* or virtual reality or video game*); (computerized adj10 training); (computer* adj10 biofeedback); ((cognitive or dual) adj5 task“self-directed learning”, “task performance”, mental imager*
We used medical sub-headings as search terms, including the following main terms
for the population: aged, elder, old, aging, brain/head/craniocerebral injury, trauma; for
cognitive aspects: cognition, meta-cognition, learning, awareness, attention, self-directed
learning, executive function; for motor functions: gait, walking, balance, movement, mobility,
posture, motor function, accidental falls, training, exercise, physical functioning and for the
interventions of interest: cognitive therapy/rehabilitation/intervention, problem solving,
biofeedback, virtual reality, video game, action game, computerized training, user-computer
interface, dual task (Table 3.1). The search strategy was initially run in Medline/Premedline

Chapter Three
48
and then adapted to the search format requirements of the other databases included in
this review. The search results were supplemented by articles found through hand search
by scanning reference lists of identified studies.
3.2.2. Study collection
After duplicate citations were removed, two reviewers (GP, EDdB) determined which
articles should be included within the systematic review by scanning the titles, abstracts
and keywords applying the inclusion and exclusion criteria (Table 3.2). A study was
considered eligible for inclusion in the review when it was examining the results of a
cognitive or cognitive-motor intervention on physical functioning of older adults.
As mentioned in the introduction, we included any study that arose from our search
concerning people with traumatic brain injury or stroke patients. Cognitive and cognitive-
motor interventions were considered studies that included cognitive rehabilitation or a
combination of cognitive rehabilitation and physical exercise, respectively. We did not
include studies that solely carried out single tests without an intervention. We adopted
the definition of the Brain Injury Interdisciplinary Special Interest Group (BI-ISIG) of the
American Congress of Rehabilitation Medicine for cognitive rehabilitation to guide our
search. Studies evaluating the effectiveness of pharmacological therapy were excluded.
If title, abstract or key words provided insufficient information for a decision on inclusion,
the methods section of the full-text article was considered.
3.2.3. Data extraction and data synthesis
The following data were extracted from the studies: (1) characteristics of the studied
population: number of participants, disease and age, (2) characteristics of the interventions:
the design, frequency and duration of the intervention, co-interventions, and control
intervention; (3) characteristics of the outcomes: outcome measures and results (Tables
3.3 and 3.4).
The included studies were divided into three groups: a) cognitive rehabilitation, b)
dual task interventions and c) computerized interventions. Computerized interventions

Cognitive and cognitive-motor interventions
49
included every study using an electronic game or task that involves interaction with a
user interface to generate visual feedback on a display device. Because we expected the
interventions and reported outcome measures to be markedly varied, we focused on a
description of the studies and their results, and on qualitative synthesis rather than meta-
analysis.
Table 3.2 List of inclusion and exclusion details
Area Inclusion details
PopulationAny elderly subjects over 65 years, adult (aged > 18 years) brain trauma patients, studies with stroke patients
Study type Intervention studies of any type, including case studies and non-randomized trials
InterventionCognitive or cognitive-motor rehabilitation intervention (physical exercise must include a cognitive aspect)
Outcomes Outcomes focus on general physical functioning and mobility of upper or lower extremities
Exclusion details
Purely physical training, interventions without training period (tests), dual task intervention without concurrent cognitive task, animal studies, reviews, methodological, theoretical or discussion papers, studies that examine the effect of physical exercise on cognition.
3.2.4. Assessment of study quality
As the basis for our critical appraisal of the studies, a checklist designed for assessing the
methodological quality of both randomized and non-randomized studies of healthcare
interventions developed by Downs and Black [41] was used. The checklist assesses biases
related to reporting, external validity, internal validity, and power. Seven items concerning
follow-up analyses (items 9, 17 and 26), allocation concealment (items 14 and 24), adverse
effects (item 8), and representativeness of treatment places and facilities (item 13) were
not considered in this review. The items were excluded because we were not primarily
interested in possible long-term effects of cognitive or cognitive-motor interventions but
rather in short-term effects of the interventions on motor functioning.

Chapter Three
50
Table 3.3 Included studies reported by design and subject specifications
Study Design n Subjects Age: range or mean [years]
Cognitive Rehabilitation Interventions
Batson et al 2006 RCT 6 Community dwelling older adults 65–80
Dunsky et al 2008 Non-RCT 17 Community dwelling adults with hemiparetic stroke 44–79
Hamel & Lajoie 2005 RCT 20 Older adults 65–90
Dual task Interventions
Shigematsu et al 2008 RCT 63 Community dwelling older adults 65–74
Shigematsu et al 2008 RCT 39 Community dwelling healthy adults 65–74
Silsupadol et al 2006 Case study 3 Older adults with history of falls 82, 90 and 93
Silsupadol et al 2009 RCT 21 Older adults 75.0 ± 6.1
Vaillant et al 2006 RCT 68 Community dwelling older women with osteo-porosis
73.5 ± 1.6
You et al 2009 RCT 13 Older adults with history of falls 68.3 ± 6.5
Computerized Interventions
Bisson et al 2007 Pre-Post 24 Community dwelling older adults VR: 74.4 ± 3.65; BF: 74.4 ± 4.92
Broeren et al 2008 Pre-Post 22 Community dwelling adults with stroke 67.0 ± 12.5
Buccello-Stout et al 2008 RCT 16 Older adults 66–81
Clark et al 2009 Case study 1 Woman resident of a nursing home with unspecified balance disorders
89
de Bruin et al 2010 Two groups control
35 Older adults living in a residential care facility IG: 85.2 ± 5.5; CG: 86.8 ± 8.1
Deutsch et al 2009 Case study 2 Chronic phase post-stroke 34 and 48
Hatzitaki et al 2009 RCT 48 Community-dwelling healthy older women 70.9 ± 5.7
Hinman 2002 RCT 88 Community-dwelling older adults 63–87
Jang et al 2005 RCT 10 Patients with stroke 57.1 ± 4.5
Kerdoncuff et al 2004 RCT 25 Patients with stroke 59.5 ± 13.5
Lajoie 2003 RCT 24 Community-dwelling elderly IG: 70.3; CG: 71.4
Mumford et al 2010 Case study 3 Patients with TBI 20, 20 and 21
Sackley et al 1997 RCT 26 Patients with stroke 41–85
Srivastava et al 2009 Pre-Post 45 Patients with stroke 45.5 ± 11.2
Sugarman et al 2009 Case study 1 Patent with stroke 86
Talassi et al 2007 Case-control 54 Community-dwelling older adults with MCI or MD 42–91
Wolf et al 1997 RCT 72 Independently living older adults CBT: 77.7± 6.5; TC: 77.7±5.6;CG: 72.2.2±4.9
Yang et al 2008 RCT 20 Patients with stroke 30–74
Yong Joo et al 2010 Pre-Post 16 Rehabilitation inpatients within 3 months post-stroke
64.5 ± 9.6
Abbreviations: RCT = Randomized controlled trial; Non-RCT = Non-randomized controlled trial; TC = Tai Chi; VR = Virtual reality; BF = Biofeedback; IG = Intervention group; CG = Control group

Cognitive and cognitive-motor interventions
51
Tabl
e 3.4
Inclu
ded s
tudie
s rep
orte
d by s
ubjec
ts, ou
tcom
es m
easu
res,
inter
vent
ion, c
ontro
l and
resu
lts
Resu
lts
Cogn
itive
Inte
rven
tions
•Sig
nifica
nt re
sults
for T
UG on
ly fo
r the
grou
p as
a who
le•
No si
gnifi
cant
resu
lts fo
r eith
er gr
oup o
r for
the
grou
p as a
who
le fo
r rem
aining
mea
sure
s
•Sp
atiot
empo
ral p
aram
eter
s: sig
nifica
ntim
prov
emen
ts in
mea
n gait
spee
d at b
aseli
ne an
d fo
llow-
up; s
tride
leng
th, p
aret
ic an
d non
-par
etic
step l
engt
h inc
reas
ed si
gnifi
cant
ly at
post-
inter
vent
ion•
Signifi
cant
incre
ase o
f sag
ittal
ROM
of th
epa
retic
knee
joint
•Sig
nifica
nt in
creas
e of g
ait sy
mm
etry
afte
rint
erve
ntion
•Tre
atm
ent e
ffect
size w
as m
oder
ate f
or m
ost
of th
e var
iables
•M
I-gro
up be
cam
e mor
e sta
ble af
ter t
raini
ng,
while
sway
of co
ntro
l gro
up in
creas
ed w
hen
com
pare
d to p
re-te
st•
A-P p
ostu
ral o
scilla
tion s
ignifi
cant
ly de
creas
ed in
MI-g
roup
•Sig
nifica
nt de
creas
e in r
eacti
on ti
me t
ask f
orM
I-gro
up•
No si
gnifi
cant
outco
mes
on BB
S and
ABC s
cales
Cont
rol
Healt
h edu
catio
n plus
phys
ical
prac
tice
6 wee
ks: 2
x/we
ek fo
r 50m
in
None
No in
volve
men
tin
any t
ype o
f tra
ining
Inte
rven
tion
Men
tal im
ager
y plus
phys
ical
prac
tice;
6 wee
ks: 2
x/we
ek fo
r 50m
in
Mot
or im
ager
y tra
ining
;6 w
eeks
: 3 x
/wee
k for
20m
in
Men
tal im
ager
y tra
ining
;6 w
eeks
: dail
y pra
ctice
Outc
ome m
easu
res
•St
anda
rdize
d mea
sure
s of
balan
ce, g
ait sp
eed a
nd ba
lance
co
nfide
nce
•BB
S, AB
C•
TUG
•Sp
atiot
empo
ral a
ndkin
emat
ic ga
it pa
ram
eter
sTin
etti
POMA
•FM
A•
Mod
ified
FWCI
•A-
P & M
-L po
stura
los
cillat
ions
•Re
actio
n tim
e to a
udito
rysti
muli
•BB
S•
ABC
Subj
ects
n=6;
com
mun
ity-d
wellin
g eld
erly;
age r
ange
: 65–
80 ye
ars
n=17
; com
mun
ity dw
elling
ad
ults w
ith he
mipa
retic
str
oke;
age r
ange
: 44–
79 ye
ars
n=20
; olde
r adu
lts;
age r
ange
: 65–
90 ye
ars
Stud
y
Batso
n et
al, 20
07
Duns
ky et
al,
2008
Ham
el an
d Lajo
ie,
2005

Chapter Three
52
Tabl
e 3.4
Inclu
ded s
tudie
s rep
orte
d by s
ubjec
ts, ou
tcom
es m
easu
res,
inter
vent
ion, c
ontro
l and
resu
lts (c
ontin
ued)
Resu
lts
Dual
task
Inte
rven
tions
•Fu
nctio
nal fi
tnes
s of lo
wer e
xtre
miti
esim
prov
ed m
ore i
n SSE
than
in W
•No
sign
ifica
ntly
lower
rate
of fa
lls pe
r trip
for
SSE c
ompa
red t
o W
•SS
E: sig
nifica
nt w
ithin-
grou
p im
prov
emen
tin
one-
leg ba
lance
•SB
: Sign
ifica
nt im
prov
emen
t of f
uncti
onal
reac
h•
Perfo
rman
ces o
n rem
aining
test
were
signifi
cant
ly be
tter f
or bo
th gr
oups
•Ba
lance
impr
oved
in al
l 3 pa
rticip
ants,
BBS,
DGI a
nd AB
C sco
res i
ncre
ased
•Tim
e to c
omple
te TU
G de
creas
ed un
der b
oth
cond
ition
s (pa
rticip
ants
who
rece
ived
DT-Tr
aining
sh
owed
mor
e im
prov
emen
t in T
UG un
der D
T th
an un
der S
T and
vice
versa
)•
Subje
ct wh
o rec
eived
DT-tr
aining
using
VP,
show
ed im
prov
emen
ts on
oth
er d
ual t
asks
tha
t we
re no
t dire
ctly t
raine
d (no
vel t
ask)
•Fo
llow-
up (2
wee
ks):
time t
o per
form
TUG
decre
ased
for a
ll sub
jects
•Fo
llow-
up (3
mon
ths):
Clini
cal m
easu
res o
fba
lance
wer
e ret
ained
; TUG
in su
bject
with
FP
furth
er im
prov
ed (9
%)
Cont
rol
Supe
rvise
d walk
ing (W
);12
wee
k: 1x
wee
k for
70m
in
Stre
ngth
and b
alanc
e tra
ining
; 12
wee
ks: 2
x/we
ek fo
r 70m
in
Single
task
balan
ce tr
aining
;4 w
eeks
: 3x/
week
for 4
5min
Inte
rven
tion
Squa
re-S
tepp
ing Ex
ercis
e (SS
E);
12 w
eeks
: 2x/
week
for 7
0min
Squa
re-S
tepp
ing Ex
ercis
e (SS
E);
12 w
eeks
: 2x/
week
for 7
0min
Dual
task
bala
nce
traini
ng w
ith
fixed
- (FP
) or v
ariab
le-pr
iority
(VP)
;4 w
eeks
: 3x/
week
for 4
5min
Outc
ome m
easu
res
•Ph
ysica
l tes
ts of
balan
ce, le
gstr
engt
h and
coor
dinat
ion•
Self-
repo
rted o
ccur
renc
e of
falls
or tr
ips•
Step
-reco
rding
with
pedo
met
ers
•Ch
air st
ands
, leg e
xten
sion
powe
r, sing
le-leg
balan
ce
with
eyes
clos
ed, fu
nctio
nal
reac
h, st
andin
g up f
rom
a lyi
ng
posit
ion, s
tepp
ing w
ith bo
th
feet,
walki
ng ar
ound
two c
ones
, 10
m-w
alk, S
it &
Reac
h
•M
edio-
later
al CO
Mdis
place
men
t und
sing
le ta
sk
(ST)
and d
ual t
ask (
DT)
•BB
S, AB
C•
DGI
•TU
G
Subj
ects
n= 63
; com
mun
ity dw
elling
old
er ad
ults;
age r
ange
: 65–
74 ye
ars
n=39
; com
mun
ity-d
wellin
g he
althy
adult
s;ag
e ran
ge: 6
5–74
year
s
n=3;
older
adult
s wi
th
self-
repo
rted h
istor
y of f
alls
or co
ncer
ns ab
out i
mpa
ired
balan
ce;
age:
82, 9
0 and
93 ye
ars
Stud
y
Shige
mat
suet
al, 2
008
Shige
mat
su
et al
, 200
8
Silsu
pado
l et
al, 2
006

Cognitive and cognitive-motor interventions
53
Tabl
e 3.4
Inclu
ded s
tudie
s rep
orte
d by s
ubjec
ts, ou
tcom
es m
easu
res,
inter
vent
ion, c
ontro
l and
resu
lts (c
ontin
ued)
Resu
lts
•Ad
ding c
ognit
ive ta
sks d
id no
t sign
ifica
ntly
alter
the e
ffects
of th
e exe
rcise
prog
ram
•2 w
eeks
follo
w-up
: Sign
ifica
nt im
prov
emen
ts fo
rall
outco
me m
easu
res i
n bot
h gro
ups;
TUG
time
impr
oved
mor
e in s
ingle
task
grou
p tha
n in d
ual
task
grou
p•
3 mon
ths f
ollow
-up:
Impr
ovem
ents
in TU
G-DT
signifi
cant
ly gr
eate
r in du
al ta
sk gr
oup t
han i
n the
sin
gle ta
sk gr
oup
Cont
rol
Single
task
balan
ce tr
aining
;4 w
eeks
: 3x/
week
for 4
5min
Phys
ical e
xerci
ses (
single
task
);6 w
eeks
: 2x/
week
Inte
rven
tion
Dual
task
balan
ce tr
aining
with
fix
ed- (
FP) o
r var
iable-
prior
ity (V
P);
4 wee
ks: 3
x/we
ek fo
r 45m
in
Phys
ical
exer
cise
while
cou
nting
, m
emor
izing
or re
citing
(dua
l tas
k);
6 wee
ks: 2
x/we
ek
Outc
ome m
easu
res
•Se
lf-se
lecte
d gait
spee
d und
ersin
gle an
d dua
l tas
k con
dition
s•
Gait
tem
pora
l-dist
ance
mea
sure
men
ts•
BBS,
ABC
•Av
erag
e ang
le of
fron
tal p
lane
COM
posit
ion an
d ank
le joi
nt
cent
er (A
JC)
•TU
G &
TUG-
DT•
One L
eg Ba
lance
(OLB
) and
OLB
with
conc
urre
nt ta
sk (O
LB-D
T)
Subj
ects
n=21
; elde
rly ad
ults;
mea
n age
: 75 ±
6.1 y
ears
n=68
; com
mun
ity-
dwell
ing ol
der w
omen
with
os
teop
oros
ism
ean a
ge: 7
3.5 ±
1.6 y
ears
Stud
y
Silsu
pado
let
al, 2
009
Vailla
nt et
al,
2006
•Al
l par
ticipa
nts i
mpr
oved
gait
spee
d und
er ST
cond
ition
s •
DT-g
roup
s walk
ed si
gnifi
cant
ly fas
ter u
nder
DTco
nditi
ons.
No si
gnifi
cant
diffe
renc
e in g
ait sp
eed
unde
r DT c
ondit
ions f
or ST
-gro
up
•Al
l par
ticipa
nts i
mpr
oved
balan
ce un
der S
Tco
nditi
ons
•AB
C Sca
le: ST
grou
p inc
reas
ed th
eir le
vel o
fco
nfide
nce m
ore t
han D
T gro
ups
•BB
S Sca
le: im
prov
emen
ts in
BBS w
ere c
ompa
rable
acro
ss tra
ining
grou
ps•
Follo
w-up
: DT-
traini
ng w
ith VP
instr
uctio
nsde
mon
strat
ed a
traini
ng eff
ect o
n DT-
gait
spee
d at
the e
nd of
the s
econ
d wee
k of t
raini
ng an
d also
afte
r 3 m
onth
s foll
ow-u
p•
All g
roup
s sho
wed a
sign
ifica
ntly
small
er A
JC-a
ngle
afte
r tra
ining
whe
n walk
ing un
der S
T-co
nditi
ons
•Un
der D
T-co
nditi
ons r
educ
tion o
f AJC
-ang
le wa
ssig
nifica
nt fo
r all g
roup
s, bu
t was
grea
ter f
or th
e VP
-gro
up th
an fo
r the
ST-g
roup
and F
P-gr
oup
•No
sign
ifica
nt eff
ects
on A
JC-a
ngle
in a n
ovel
(unt
raine
d) DT
-con
dition
for a
ll gro
ups

Chapter Three
54
Tabl
e 3.4
Inclu
ded s
tudie
s rep
orte
d by s
ubjec
ts, ou
tcom
es m
easu
res,
inter
vent
ion, c
ontro
l and
resu
lts (c
ontin
ued)
Resu
lts
•No
sign
ifica
nt di
ffere
nce i
n the
M-L
COP o
r A-P
COP
devia
tion m
easu
res n
eithe
r in co
ntro
l nor
ex
perim
ent g
roup
•Sig
nifica
nt in
creas
e in g
ait sp
eed i
n con
trol g
roup
but n
ot in
expe
rimen
tal g
roup
Com
pute
rized
Inte
rven
tions
•M
ean C
B&M
scor
es fo
r bot
h gro
ups i
ncre
ased
signifi
cant
ly fro
m ba
selin
e to p
ost-t
raini
ng an
d re
tent
ion, n
o diff
eren
ce be
twee
n gro
ups
•St
atic
balan
ce: n
o diff
eren
ces b
etwe
en gr
oups
and n
o tra
ining
effec
t on v
ariab
ility o
f COP
dis
place
men
t; Sig
nifica
nt ta
sk eff
ect a
nd
inter
actio
n bet
ween
dire
ction
s of s
way a
nd ta
sks
•Re
actio
n tim
e: no
grou
p effe
ct; si
gnifi
cant
main
effec
t of t
ime;
reac
tion t
ime a
t bas
eline
sig
nifica
ntly
highe
r com
pare
d to p
ost-t
raini
ng an
d re
tent
ion; b
oth g
roup
s im
prov
ed th
eir re
actio
n tim
e equ
ally
•BB
T: In
creas
e in t
reat
men
t gro
up by
9%•
ABILH
AND:
No s
ignifi
cant
chan
ges i
n bot
h gro
ups
•TM
T-B:
med
ian ti
me d
ecre
ased
for c
omple
ting t
heta
sk in
both
grou
ps•
Kinem
atics
: Tim
e to c
omple
te th
e VR t
ask a
nd H
PRde
creas
ed si
gnifi
cant
ly in
treat
men
t gro
up•
Hand
traje
ctorie
s are
quali
tativ
ely m
ore r
estra
ined,
self-
cont
rolle
d, sm
ooth
er an
d les
s clut
ters
afte
r tra
ining
Cont
rol
Place
bo ve
rsion
of CG
I;6 w
eeks
: 5x/
week
for 3
0min
None
Cont
inued
parti
cipat
ion in
usua
l ph
ysica
l acti
vities
Inte
rven
tion
Cogn
itive
Gait
Inte
rven
tion (
CGI);
6 wee
ks: 5
x/we
ek fo
r 30m
in
Dyna
mic
balan
ce tr
aining
with
vis
ual b
iofee
dbac
k (BF
) or in
virtu
al re
ality
(VR)
;10
wee
ks: 2
x/we
ek fo
r 30m
in
3D co
mpu
ter g
ame p
lay w
ith
hapt
ic de
vice a
nd un
supp
orte
d up
per e
xtre
miti
es;
4 wee
ks: 3
x/we
ek fo
r 45m
in
Outc
ome m
easu
res
•Ga
it sp
eed
•A-
P & M
-L CO
P dev
iation
•St
atic
balan
ce
•Sim
ple au
ditor
y rea
ction
tim
eta
sk
•CB
&M
•M
anua
l Abil
ity m
easu
rem
ents
(BBT
and A
BILH
AND)
•Tra
il Mak
ing Te
st B
•Kin
emat
ics of
uppe
r ext
rem
ities
(veloc
ity, h
and-
path
ratio
, and
m
ore)
Subj
ects
n=13
; olde
r adu
lts w
ith
histo
ry of
falls
;m
ean a
ge: 6
8.3 ±
6.5 y
ears
n=24
; com
mun
ity dw
elling
old
er ad
ults;
mea
n age
: VR 7
4.4 ±
3.65
ye
ars,
BF 74
.4 ±
4.92
year
s
n=22
; com
mun
ity dw
elling
pe
rsons
with
stro
ke;
mea
n age
: 67 ±
12.5
year
s
Stud
y
You e
t al,
2009
Bisso
n et
al, 20
07
Broe
ren e
t al,
2008

Cognitive and cognitive-motor interventions
55
Tabl
e 3.4
Inclu
ded s
tudie
s rep
orte
d by s
ubjec
ts, ou
tcom
es m
easu
res,
inter
vent
ion, c
ontro
l and
resu
lts (c
ontin
ued)
Resu
lts
•Av
erag
e tim
e sco
res t
o com
plete
obsta
cle co
urse
and a
vera
ge pe
nalty
scor
es si
gnifi
cant
ly de
creas
ed
in ex
perim
enta
l gro
up af
ter in
terv
entio
n and
at
rete
ntion
(4 w
eeks
)
•Im
prov
emen
ts in
all ou
tcom
e mea
sure
s•
Self-
repo
rted i
mpr
ovem
ents
in ba
lance
,am
bulat
ion ab
ility a
nd co
nfide
nce
•DT
C: Sig
nifica
nt de
creas
e in D
TC of
walk
ingve
locity
and s
tride
tim
e in C
GD-g
roup
. No
signifi
cant
chan
ges i
n DTC
of ca
denc
e and
step
tim
e in b
oth g
roup
s•
ETGU
G: no
sign
ifica
nt ti
me e
ffect
in bo
th gr
oups
•FE
S-I: n
o sign
ifica
nt ti
me e
ffect
in bo
th gr
oups
•Ga
it sp
eed i
ncre
ased
for b
oth p
artic
ipant
s(re
taine
d at f
ollow
-up)
•Ga
it en
dura
nce i
ncre
ased
mod
estly
for b
oth
parti
cipan
ts•
DGI a
nd AB
C sco
res i
ncre
ased
for b
oth p
artic
ipant
s•
TUG
and T
UG-D
T tim
e dec
reas
ed fo
r bot
hpa
rticip
ants;
Cont
rol s
ubjec
t sho
wed f
urth
er
impr
ovem
ent a
t pos
t-tes
t
Cont
rol
Walk
ing st
raigh
t on a
trea
dmill
in a s
tatic
virtu
al ro
om; 4
wee
ks: 2
x/we
ek fo
r 20m
in
None
Usua
l car
e phy
sical
inter
vent
ion
(UC)
;12
wee
ks: 1
x/we
ek fo
r 30–
45m
in
Balan
ce an
d coo
rdina
tion a
ctivit
ies
in diff
eren
t con
dition
s; 4 w
eeks
: 3x/
week
for 6
0min
Inte
rven
tion
Walk
ing st
raigh
t on a
trea
dmill
in a
rota
ting v
irtua
l room
;4 w
eeks
: 2 x/
week
for 2
0min
Nint
endo
Wii B
owlin
g gam
e;2 w
eeks
: 3x/
week
for 6
0 min
Com
pute
r gam
e dan
cing (
CGD)
plus
pr
ogre
ssive
resis
tanc
e tra
ining
;12
wee
ks: 2
x/we
ek fo
r 45–
60m
in
Nint
endo
Wii S
ports
and W
ii Fit
Prog
ram
s; 4 w
eeks
: 3x/
week
for 6
0min
Outc
ome m
easu
res
•Tim
e to c
omple
te an
obsta
cle co
urse
with
13 so
ft ob
stacle
s•
Num
ber o
f pen
alties
onob
stacle
cour
se
•BB
S, AB
C•
DGI
•TU
G•
MM
SE
•Ga
it te
mpo
ral-d
istan
cem
easu
rem
ents
•Du
al ta
sk co
sts of
walk
ing•
ETGU
G•
FES-
I
•Ga
it sp
eed
•Six
-minu
te w
alk te
st (m
eter
s)•
BBS,
ABC
•DG
I•
TUG
and T
GU-D
T
Subj
ects
n=16
; olde
r adu
lts;
age r
ange
: 66–
81 ye
ars
n=1;
wom
an re
siden
t of
a nu
rsing
hom
e with
un
spec
ified
balan
ce di
sord
ers;
age:
89 ye
ars
n=35
; olde
r adu
lts liv
ing in
a re
siden
tial c
are f
acilit
y;m
ean a
ge: C
GD 85
.2 ±
5.5
year
s, UC
86.8
± 8.
1 yea
rs
n=2;
in ch
ronic
phas
e pos
t-str
oke p
atien
ts;ag
e: 48
and 3
4 yea
rs
Stud
y
Bucce
llo-S
tout
et
al, 2
008
Clark
et al
, 200
9
de Br
uin et
al, 20
10
Deut
sch et
al, 20
09

Chapter Three
56
Tabl
e 3.4
Inclu
ded s
tudie
s rep
orte
d by s
ubjec
ts, ou
tcom
es m
easu
res,
inter
vent
ion, c
ontro
l and
resu
lts (c
ontin
ued)
Resu
lts
•No
rmal
quiet
stan
ce: N
o sign
ifica
nt ch
ange
s in C
OPdis
place
men
t and
angu
lar ki
nem
atics
in ei
ther
of
the t
wo tr
aining
grou
ps.
•Sig
nifica
nt eff
ect o
f tra
ining
on in
terli
mb C
OPas
ymm
etry
in A-
P gro
up•
Shar
pene
d Rom
berg
Stan
ce: S
ignifi
cant
redu
ction
of CO
P disp
lacem
ent i
n A-P
grou
p, no
adap
tatio
ns
in M
-L gr
oup.
A-P g
roup
show
ed si
gnifi
cant
ly de
creas
ed pe
ak am
plitu
de an
d SD
of lo
wer l
eg
rota
tion i
n the
pitch
dire
ction
and o
f tru
nk’s
med
io-lat
eral
rota
tion.
No s
ignifi
cant
chan
ges i
n th
e M-L
grou
p
•Su
bjects
in bo
th tr
aining
grou
ps sh
owed
sligh
tim
prov
emen
ts in
all m
easu
res.
Subje
cts of
cont
rol
grou
p im
prov
ed to
a les
ser d
egre
e
•Sig
nifica
nt di
ffere
nce b
etwe
en th
e gro
ups, V
Rgr
oup i
mpr
oved
in m
otor
func
tions
, con
trol g
roup
did
not s
how
any c
hang
e•
Corti
cal a
ctiva
tion w
as re
orga
nized
from
cont
rales
ional
to ip
siles
ional
activ
ation
in th
e lat
erali
ty in
dex
•Im
prov
emen
ts in
gait
spee
d for
cont
rol g
roup
,de
creas
e for
inte
rven
tion g
roup
•Im
prov
emen
ts in
FMA,
MFI
and B
arth
el In
dex f
orbo
th gr
oups
•Im
prov
emen
ts of
force
plat
form
para
met
ers w
ithclo
sed e
yes
Cont
rol
No in
volve
men
t in a
ny ty
pe of
tra
ining
No in
volve
men
t in a
ny ty
pe of
tra
ining
No in
volve
men
t in a
ny ty
pe of
tra
ining
Tradit
ional
traini
ng;
3 wee
ks: 5
x/we
ek
Inte
rven
tion
Balan
ce tr
aining
on pl
atfo
rm w
ith
visua
l feed
back
in A-
P or M
-L
direc
tion;
4 wee
ks: 3
x/we
ek fo
r 25m
in
Com
pute
rized
Balan
ce Tr
aining
(C
BT) o
r Hom
e pro
gram
of ba
lance
ex
ercis
es (H
EP);
4 wee
ks: 3
x/we
ek fo
r 20m
in
VR ga
me e
xerci
se w
ith IR
EX sy
stem
fo
cusin
g on r
each
ing, li
fting
and
gras
ping;
4 wee
ks: 5
x/we
ek fo
r 60m
in
Prog
ressi
ve ba
lance
train
ing w
ith
visua
l biof
eedb
ack p
lus tr
aditi
onal
traini
ng;
3 wee
ks: 5
x/we
ek
Outc
ome m
easu
res
•St
atic
postu
ral s
way d
ata:
COP
displa
cem
ent i
n A-P
and M
-L
direc
tion
•An
gular
excu
rsion
of lo
wer l
eg,
pelvi
s and
trun
k
•BB
S•
MFE
S•
Timed
50-fo
ot w
alk te
st (T
WT)
•Sim
ple re
actio
n tim
e
•BB
T•
FMA
•M
anua
l Fun
ction
Test
•Se
vera
l fMRI
data
•FM
A•
Gait
evalu
ation
•Ba
rthel
Inde
x•
Mea
sure
men
t of f
uncti
onal
indep
ende
nce (
MFI)
•Sw
ay m
easu
rem
ents
on fo
rcepla
tform
Subj
ects
n=48
; com
mun
ity-d
wellin
g he
althy
olde
r wom
en;
mea
n age
: 70.8
9 ± 5.
67 ye
ars
n=88
; com
mun
ity-d
wellin
g eld
erly;
age r
ange
: 63-
87 ye
ars
n=10
; pat
ients
with
he
mipa
retic
stro
ke;
mea
n age
: 57.1
± 4.
5 yea
rs
n=25
; pat
ients
with
stro
ke;
mea
n age
: 59.5
± 13
.5
Stud
y
Hatzi
taki
et al
,20
09
Hinm
an,
2002
Jang
et
al, 20
05
Kerd
oncu
ff et
al20
04

Cognitive and cognitive-motor interventions
57
Tabl
e 3.4
Inclu
ded s
tudie
s rep
orte
d by s
ubjec
ts, ou
tcom
es m
easu
res,
inter
vent
ion, c
ontro
l and
resu
lts (c
ontin
ued)
Resu
lts
•BB
S: Sig
nifica
nt di
ffere
nce f
or CB
T-gr
oup a
fter
inter
vent
ion
•AB
C: No
sign
ifica
nt ch
ange
s•
Signifi
cant
decre
ase o
f rea
ction
tim
e in C
BT-g
roup
afte
r inte
rven
tion
•Po
stura
l swa
y: No
sign
ifica
nt ch
ange
s in b
oth
grou
ps
•Ac
cura
cy: Im
prov
emen
ts af
ter in
terv
entio
n and
main
taine
d in
2 of 3
patie
nts
•Sp
eed:
No i
mpr
ovem
ent a
fter in
terv
entio
n for
eithe
r han
d•
Efficie
ncy:
Impr
oved
perfo
rman
ce effi
cienc
y for
all
parti
cipan
ts af
ter in
terv
entio
n •
BBT:
mod
erat
e im
prov
emen
ts•
MAND
: mod
erat
e im
prov
emen
ts
•Tre
atm
ent g
roup
dem
onstr
ated
sign
ifica
ntly
bette
rpe
rform
ance
whe
n com
pare
d with
cont
rols
for
stanc
e sym
met
ry an
d for
func
tiona
l per
form
ance
(A
DL an
d Gro
ss Fu
nctio
n sco
res)
•Sw
ay va
lues s
howe
d a te
nden
cy to
grea
ter
impr
ovem
ent
•St
atist
ically
sign
ifica
nt di
ffere
nces
at th
e end
oftra
ining
for a
ll out
com
e mea
sure
s•
Stat
istica
lly si
gnifi
cant
diffe
renc
es fo
r all o
utco
mes
at 3
mon
ths f
ollow
-up
Cont
rol
No in
volve
men
t in a
ny ty
pe of
tra
ining
None
Balan
ce tr
aining
with
out v
isual
feedb
ack;
4 wee
ks: 3
x/we
ek fo
r 60m
in
None
Inte
rven
tion
Com
pute
rized
Balan
ce Tr
aining
;8 w
eeks
: 2x/
week
for 6
0min
Table
-top V
R-Sy
stem
for m
oving
ob
jects
to cu
ed lo
catio
ns w
ith
augm
ente
d mov
emen
t fee
dbac
k;12
wee
ks: 1
x/we
ek fo
r 60m
in
Balan
ce tr
aining
using
visu
al fee
dbac
k;4 w
eeks
: 3x/
week
for 6
0min
Balan
ce tr
aining
on fo
rce pl
atfo
rm
with
visu
al fee
dbac
k;4 w
eeks
: 5x/
week
for 2
0min
Outc
ome m
easu
res
•BB
S, AB
C•
Audit
ory-
verb
al re
actio
n tes
t•
Postu
ral s
way d
ata
•M
ovem
ent a
ccur
acy
•M
ovem
ent s
peed
•M
ovem
ent e
fficie
ncy
•BB
T•
MAND
•St
ance
sym
met
ry an
d swa
y•
Rive
rmea
d Mot
or A
ssessm
ent
•No
tting
ham
10 Po
int AD
L Sca
le
•BB
S•
Balan
ce In
dex
•Dy
nam
ic Lim
its of
Stab
ility
score
s•
Walk
ing ab
ility
•Ba
rthel
Inde
x
Subj
ects
n=24
; com
mun
ity-d
wellin
g eld
erly;
mea
n age
: IG 70
.3 ye
ars,
CG
71.4
year
s
n=3;
patie
nts w
ith TB
I;m
ean a
ge: 2
0.3 ye
ars
n=26
; stro
ke pa
tient
s;ag
e ran
ge: 4
1-85
year
s
n=45
; stro
ke pa
tient
s;m
ean a
ge: 4
5.51 ±
11.24
ye
ars
Stud
y
Lajoi
e,20
03
Mum
ford
et al
,20
10
Sack
leyet
al,
1997
Sriva
stava
et al
,20
09

Chapter Three
58
Tabl
e 3.4
Inclu
ded s
tudie
s rep
orte
d by s
ubjec
ts, ou
tcom
es m
easu
res,
inter
vent
ion, c
ontro
l and
resu
lts (c
ontin
ued)
Resu
lts
•M
odes
t im
prov
emen
ts in
BBS a
nd Fu
nctio
nal
Reac
h tes
ts•
TUG
time d
ecre
ased
•M
odes
t im
prov
emen
ts in
postu
ral s
tabil
ity te
sts
•Pa
rticip
ants
with
MCI
show
ed s
ignifi
cant
impr
ovem
ents
in PP
T•
Unsp
ecifi
c con
trol p
rogr
am sh
owed
no si
gnifi
cant
effec
ts
•CB
T: im
prov
ed po
stura
l sta
bility
•TC
: no i
mpr
ovem
ents
in po
stura
l sta
bility
, but
redu
ction
of fe
ar of
fallin
g occ
urre
d
•VR
-Gro
up: s
ignifi
cant
impr
ovem
ent i
n all
outco
mes
post-
traini
ng an
d sign
ifica
nt
impr
ovem
ents
in wa
lking
spee
d, CW
T and
WAQ
sco
re 1
mon
th af
ter c
omple
tion o
f pro
gram
•CG
: sign
ifica
nt im
prov
emen
ts in
CWT p
ost-t
raini
ngan
d in f
ollow
-up p
eriod
, sign
ifica
nt im
prov
emen
ts of
WAQ
scor
e at f
ollow
-up
•Sig
nifica
nt im
prov
emen
ts in
the F
MA an
d Mot
ricity
Inde
x sco
res
Abbr
eviat
ions:
BBS =
Berg
Balan
ce Sc
ale; A
BC =
Activ
ities
-spec
ific B
alanc
e Con
fiden
ce Sc
ale; C
B&M
= Fu
nctio
nal B
alanc
e and
Mob
ility;
COP =
Cent
re of
Pres
sure
; COM
= Ce
ntre
of M
ass;
DGI =
Dyn
amic
Gait
Inde
x; TU
G =
Tim
ed U
p an
d Go T
est; T
UG-D
T = Ti
med
Up a
nd G
o Tes
t Dua
l Tas
k; ET
GUG
= Ex
pand
ed Ti
med
Up a
nd G
o Tes
t; M
MSE
= M
ini M
enta
l Sta
te Ex
amina
tion;
ADL =
Activ
ities
of D
aily L
iving
; BBT
= Bo
x and
Bloc
k Tes
t; MA
ND =
Mc C
arro
n Asse
ssmen
t of
Neu
rom
uscu
lar D
ysfu
nctio
n; FM
A = Fu
gl-M
eyer
Asse
ssmen
t of U
pper
Lim
b Mot
or Fu
nctio
n; FE
S-I =
Falls
Effica
cy Sc
ale In
tern
ation
al; M
FES =
Tine
tti’s M
odifi
ed Fa
lls Effi
cacy
Scale
; POM
A = Pe
rform
ance
Orie
nted
Mob
ility
Asse
ssmen
t; FC
WI =
Func
tiona
l Walk
ing Ca
tego
ries I
ndex
; PPT
= Ph
ysica
l Per
form
ance
Test
Cont
rol
None
Sam
e pro
gram
with
phys
ical
reha
bilita
tion p
rogr
am (P
T)
inste
ad of
CCT
Educ
ation
al int
erve
ntion
(ED)
;15
wee
ks: 1
x/we
ek fo
r 60m
in
Tread
mill
traini
ng;
3 wee
ks: 3
x/we
ek fo
r 20m
in
None
Inte
rven
tion
Nint
endo
Wii F
it ba
lance
train
ing
plus s
tand
ard p
hysic
al th
erap
y with
em
phas
is on
func
tiona
l acti
vities
;4 x
45m
in
Com
pute
rized
cogn
itive
train
ing
(CCT)
, occ
upat
ional
ther
apy (
OT)
and b
ehav
ioral
traini
ng (B
T);
3 wee
ks: 4
x/we
ek fo
r 30–
45m
in
Com
pute
rized
Balan
ce Tr
aining
(C
BT) o
r Tai
Chi (
TC);
15 w
eeks
: CBT
1x/w
eek f
or 60
min,
TC
2x/w
eek f
or 60
min
Virtu
al re
ality
-bas
ed tr
eadm
ill tra
ining
;3 w
eeks
: 3x/
week
for 2
0min
Uppe
r lim
b exe
rcise
s with
Ni
nten
do W
ii in a
dditi
on to
usua
l re
habil
itatio
n;2 w
eeks
: 6x/
week
for 3
0min
Outc
ome m
easu
res
•BB
S•
Func
tiona
l Rea
ch•
TUG
•Po
stura
l Sta
bility
Inde
x (ST
I)•
Stab
ility S
core
(ST)
•PP
T•
Basic
and i
nstru
men
tal A
DL
•Po
stura
l sta
bility
mea
sure
men
tsun
der d
efine
d con
dition
s•
Fear
of Fa
lling Q
uesti
onna
ire
•W
alking
spee
d•
Com
mun
ity w
alk te
st (C
WT
•W
alking
Abilit
y Que
stion
naire
(W
AQ)
•AB
C
•FM
A•
Mot
ricity
Inde
x•
Mod
ified
Ash
worth
Scale
(MAS
)•
Visua
l Ana
logue
Scale
for u
pper
limb p
ain
Subj
ects
n=1;
wom
an 5
week
s afte
r str
oke;
age:
86 ye
ars
n=54
; com
mun
ity-d
wellin
g old
er ad
ults w
ith m
ild
cogn
itive
impa
irmen
t (M
CI) or
m
ild de
men
tia (M
D);
age r
ange
: 42–
91 ye
ars
n=72
; inde
pend
ently
living
old
er ad
ults;
mea
n age
: CBT
77.7±
6.5
year
s, TC 7
7.7±
5.6 ye
ars,
Cont
rol G
roup
75.2±
4.9 ye
ars
n=20
; adu
lts w
ith st
roke
;ag
e ran
ge: 3
0–74
year
s
n=16
; reha
bilita
tion
inpat
ients
with
in 3 m
onth
s po
st-str
oke;
mea
n age
: 64.5
± 9.
6 yea
rs
Stud
y
Suga
rman
et al
,20
09
Talas
si et
al,
2007
Wolf
et al
, 19
97
Yang
et al
, 20
08
Yong
Joo
et al
,20
10

Cognitive and cognitive-motor interventions
59
The blinding of participants and investigators, the assessment of adverse effects, and
the representativeness of the treatment places were also excluded. We considered these
as being of minor significance for this review.
The remaining 20 items were applied by two reviewers (GP, EDdB) to assess the
methodological quality of the studies. The total possible score was 22 points. The
scoring for statistical power (item 27) was simplified to a choice between 0, 1 or 2 points
depending on the level of power to detect a clinically important effect. The scale ranged
from insufficient (β < 70% = 0 points), sufficient (β = 70–80% = 1 point) or excellent (β >
80% = 2 points). To assess the level of agreement between the investigators a Cohen‘s
kappa analysis was performed on all items of the checklist. In accordance with Landis and
Koch‘s benchmarks for assessing the agreement between raters a kappa-score of 0.81–1.0
was considered 'almost perfect', 0.61–0.8 was 'substantial', 0.41–0.6 was 'moderate', 0.21–
0.4 was 'fair', 0.0–0.2 'slight' and scores < 0.0 'poor' [42]. Disagreements were resolved by
consensus.
The PRISMA-statement was followed for reporting items of this systematic review [43].
3.3. Results
3.3.1. Study selection
The search provided a total of 2349 references (Figure 3.1). After adjusting for duplicates,
1697 remained. Of these 1671 were discarded because they provided only physical exercise
(n = 159), did not discuss outcomes or population of interest (n = 89), constituted review
articles or were no interventional studies (n = 217), executed only single tests (n = 246) or
were clearly out of scope of this review (n = 944). The remaining 26 potentially relevant
articles were supplemented by 10 additional references retrieved by citations and author
tracking, resulting in a total of 36 articles being eligible for full-text reading. After full-text
reading eight articles were excluded because they did not report outcomes of interest
(n = 1), applied no intervention (n = 1), applied no training (n = 4), or were theoretical
articles (n = 2). One article appeared to be a written summary of a poster presentation and
represented an included article (n = 1).

Chapter Three
60
Figure 3.1 Study selection flow chart
CINAHL (n = 641)
References identi ed through database searching (n = 2‘349)
Additional records identi ed through citations and author tracking (n = 10)
Excluded duplicates (n = 652)
Articles screened on basis of title and abstract (n = 1‘697)
Excluded (n = 1‘671) • Not outcome or population of interest (n = 89) • Physical exercise ( n = 159) • E ects of physical exercise on cognition ( n = 16) • Reviews, discussions, no intervention etc. ( n = 217) • Tests ( n = 246) • Out of scope (n = 944)
Eligible for full-text reading (n = 26)
Full-text reading and application of inclusion criteria
Included (n = 28)
Excluded (n = 8) • No training (n = 4) • Not outcome of interest (n = 1) • Theortical article (n = 2) • Poster presentation of included article (n = 1)
Dual task strategy (n = 6)
Cognitive rehabilitation intervention
(n = 3 )
Computerized intervention (n = 19)
PsychINFO
(n = 103)
Medline (n = 626)
EMBASE (n = 979)

Cognitive and cognitive-motor interventions
61
3.3.2. Characteristics of included studies
Of the 28 studies finally selected for the review 27 were published in English [32,44–70]
and one in French [71]. The publication dates range from 1997 [67] to 2010 [48,56,69]. In
the selected studies participants were older adults partially with history of falls [47,70],
balance disorders [47,62], with mild cognitive impairments [65] or osteoporosis [66]. Ten
studies were concerned with patients after stroke [45,49,50,54,57,63,64,68,69,71] and one
study with traumatic brain injury patients [56].
From the 28 included articles three used an isolated cognitive rehabilitation
intervention [44,50,51], seven articles used a dual task intervention [58–62,66,70] and 19
applied a computerized intervention [32,45–49,52–57,63–65,67–69,71]. From the seven
articles concerning dual-tasking two articles arise from the same intervention [60,61]
leading us to regard it as one single study.
In 22 studies, a cognitive rehabilitation intervention, dual task training or a
computerized intervention were used as the only intervention for the participants [32,45–
47,49–52,54–63,66–70]. In six studies the interventions were applied as additional items
to a traditional physical or balance training [44,48,53,64,65,71]. The reported outcomes
involved different assessments of balance, gait or functional mobility.
Balance was assessed with the help of postural sway measurements
[32,44,51,52,57,62,67,71], with the Berg Balance Scale [44,47,49,51,53,55,60–64], with
the Activities-specific Balance Confidence Scale [44,47,49,51,55,60–62,68], with the
Functional Balance and Mobility test [32], with the Balance Index [63] and with one-leg-
stance tests [59,66]. Gait measurements included measurements of kinematic parameters
[44,48–50,60,61,68,70], the Timed Up & Go Test [44,47–49,62,64,66], the Dynamic Gait
Index [47,49,62], or step recording with pedometers [58]. Functional Mobility assessments
were determined by manual ability measurements [45,54], functional reach tests [64], the
Physical Performance Test [65], the Rivermead Motor Assessment [57], The Nottingham 10
Point ADL Scale [57], the Box and Block Test [45,54,56] and the Fugl-Meyer Assessment of
Upper Limb Motor Function [50,54,69,71].

Chapter Three
62
3.3.3. Methods used and their effects
3.3.3.1. Cognitive rehabilitation interventions
From the three articles evaluating the effects of a cognitive rehabilitation intervention on
motor outcomes, two examined the effects of mental imagery on physical functioning of
older adults aged between 65 and 90 years [44,51]. In the third study, the participants were
community-dwelling adults between 44 and 79 years of age suffering from hemiparetic
stroke [50]. The three studies investigated the effect of mental imagery training on postural
balance [44,51] and on gait [44,50]. Mental imagery training consisted of either visual
imagery training, i.e. participants are expected to view themselves from the perspective
of an external observer, or of kinesthetic imagery exercise, i.e. participants imagine
experiencing bodily sensations that might be expected in the exercise. The trainings
lasted six weeks with a training frequency ranging from daily [51], twice weekly [44] to three
times weekly [50]. Two studies used a pure cognitive rehabilitation method [50,51] whereas
one study combined mental practice with additional physical exercise [44].
The studies show reduction of postural sway [51], and improvements in gait speed [44]
and gait symmetry [50]. No improvements were shown for balance confidence [44].
Hamel and Lajoies‘ [51] results show a significant reduction of anterior-posterior
postural oscillations suggesting that mental imagery training over a six-week period helps
to improve postural control of the elderly. The study of Batson et al. [44] combined mental
imagery with physical exercise. The control group underwent a health education program
in addition to the physical training. Gait speed, expressed by improvement in Timed Up-
and-Go test performance, increased for all study participants. These results imply that
the improvement in gait speed were attaint through the physical practice regardless
of whether combined with mental imagery or not. This conjecture is supported by the
fact that the two groups under observation converge to each other for the Timed Up-
and-Go test measures following the intervention. In the pretest phase, there was a large,
meaningful difference for the Timed Up-and-Go test between the mental imagery and
physical practice subjects (Cohen‘s d = 1.2) that decreases to Cohen‘s d = 0.55 at the end
of intervention. The results showed no improvement in balance confidence, as expressed

Cognitive and cognitive-motor interventions
63
by non-significant results neither on the Berg Balance Scale nor on the Activities-specific
Balance Confidence Scale. The study of Dunsky et al. [50] showed improvements of
spatiotemporal gait parameters and gait symmetry in people with chronic poststroke
hemiparesis after mental imagery. There was no control group in this study to support
these results.
3.3.3.2. Dual task interventions
The methods varied from walking or balancing with a concurrent mental task like
memorizing words, reciting poems, or computing mental arithmetic tasks [60–62,66,70]
to a square-stepping exercise where participants executed forward, backward, lateral
and oblique step patterns on a thin felt mat [58,59]. The training lasted between 4 weeks
[60–62], 6 weeks [70] or 12 weeks [58,59,66]. No dual task study was found on stroke
patients or people with traumatic brain injury. The study of Shigematsu et al. [58] showed
improvements in functional fitness of lower extremities. The results on gait patterns
and postural sway are controversial. Silsupadol et al. [60–62] showed improvement of
gait speed under dual task conditions and a reduction of body sway, whereas You et al.
[70] and Vaillant et al. [66] found no improvements in gait and stability after a dual task
intervention. No other physical outcomes were reported.
The studies conducted by Silsupadol et al. [60–62] compared three different balance
training approaches: single task balance training, dual task balance training with fixed-
priorities and dual task balance training with variable-priority. Single task training
consisted of exercises for body stability with or without object manipulation and/or body
transport. In the dual task condition, concurrent auditory and visual discrimination tasks
and computing tasks were added to the balance training. In the fixed-priority condition
the subject was instructed to direct the attention with equal priority to both the postural
and additional tasks. In the variable-priority condition half the training was done with the
instruction to mainly prioritize the postural task and the other half with the instruction
to mainly prioritize the additional task. All participants improved self-selected gait speed
under single task testing conditions. Under dual task testing conditions, however, only

Chapter Three
64
participants who received dual task training showed significant improvements in self-
selected gait speed (with moderate effect sizes of 0.57 between single task and fixed-
priority and 0.46 between single task and variable-priority). All groups significantly
improved on the Berg Balance Scale under single task conditions. Participants in the
variable-priority training group additionally showed an average of 56% reduction in body
sway compared to only 30% of the fixed-priority and single task group. Overall, the study
showed that variable-priority instruction was more effective in improving both balance
and physical performance under dual task conditions than either the single task or the
fixed-priority training approaches. In contrast to the fixed-priority training group, the
variable-priority group showed long-term maintenance effects on dual task gait speed for
three months after the end of training.
In contrast to the results of Silsupadol et al., You and colleagues [70] found no
improvements in gait and stability after their dual task intervention that lasted six weeks.
Results of the gait tests showed a significant increase in gait velocity in the control group,
which underwent single task training, but not in the experimental group. No statistically
significant differences in the deviation of medio-lateral and anterior-posterior center
of pressure were found between the groups. Vaillant et al. [66] did not find additional
improvements through the addition of a cognitive task to the physical task either. The
exercise sessions were effective in improving performance on two balance tests,
improvements, however, were not attributable to the dual task training.
Shigematsu et al. [58,59] developed an alternative approach to exercise for dual
task abilities in community-dwelling older adults. A square-stepping exercise was
performed on a thin mat with the instruction to step from one end of the mat to
the other according to a step pattern provided, which could be made progressively
more complex. Results showed that square-stepping exercise was equally effective
as strength training to improve lower-extremity functional fitness. Compared to a
weekly walking session, however, participants of the square-stepping exercise group
showed a greater improvement in functional fitness of the lower-extremity.

Cognitive and cognitive-motor interventions
65
3.3.3.3. Computerized interventions
Nineteen studies investigated the effects of a computerized intervention to improve
physical abilities. The studies were distributed over the populations of interest as follows:
nine interventions treating older adults [32,46–48,52,53,55,65,67], nine interventions
treating patients with stroke [45,49,54,57,63,64,68,69,71] and one study treating young
adults with traumatic brain injury [56]. Fifteen studies investigated the effects on lower
extremities [32,46–49,52,53,55,57,63–65,67,68,71], whereas four studies analyzed the
effects on upper extremities [45,54,56,69]. The interventions included various methods
and ideas for the implementation of computers into a training session. Talassi et al. [65]
used a computerized cognitive program [72,73], to stimulate cognitive functions, e.g.
visual search, episodic memory or semantic verbal fluency, by a specific group of exercise
for older adults with mild cognitive impairments or mild dementia. Buccello-Stout et
al. [46] used a sensorimotor adaptation training to improve functional mobility in older
adults. Participants walked on a treadmill while viewing a rotating virtual scene providing
a perceptual-motor mismatch [46].
Seven studies used the method of computerized dynamic balance training with
visual feedback technique [52,53,55,57,63,67,71]. The tasks required to move a cursor
through weight-shifting on a screen representing the center of pressure (COP) position
to specified targets [32,53,55,63,67] or on a predefined sine wave trajectory [52]. In one
study, the feedback signal displayed the weight distribution and weight-shifting with
moving columns, showing stance symmetry [57]. In another study researchers designed
the task of visual feedback training in a more playful way, projecting the cursor for center
of pressure as a caterpillar moving on the screen [71].
A total of ten studies described an approach, which included interactive virtual reality
games or applications [32,45,47–49,54,56,64,68,69]. Seven studies out of this ten were
conducted on stroke patients [32,45,49,54,64,68,69], two studies on older adults [47,48]
and one on patients with traumatic brain injury [56]. The virtual reality applications
were varied. There were elaborated and expensive systems, enabling the participants
to see themselves in the virtual environment and to play games like juggling a virtual

Chapter Three
66
ball [32] or saving a ball as a soccer keeper [54]. Virtual devices consisting of a semi-
immersive workbench with which participants were able to reach and interact with three-
dimensional objects [45], a table-top virtual reality based system requiring the patients to
move an object to cued locations while receiving augmented movement feedback [56]
and virtual reality based treadmill training [68]. Furthermore, commercially available low-
cost interactive video game console systems [47,49,64,69] or dance simulation games [48]
were applied.
The computerized cognitive training program proposed by Talassi et al. [65] produced
an improvement in functional status, measured by the Physical Performance Test [74],
in patients with mild cognitive impairments, while a physical rehabilitation program did
not show any significant effects. The sensorimotor adaptation training for older adults
developed by Buccello-Stout et al. [46] resulted in better performance on an obstacle
course after the intervention compared to the control group, who walked on the treadmill
without rotation of the virtual scenario.
Some of the interventions providing balance training with visual feedback improved
simple auditory reaction time [32,55] postural balance and stability [32,55,57,63,67,71], gait
speed [63], functional status, and performance [55,57,63,71]. The intervention conducted
by Hatzitaki et al. [52] revealed that weight-shifting training in anterior-posterior direction
only induces improvements in standing balance of older adults. In contrast, the studies
of Lajoie et al. [55] and Bisson et al. [32] showed no improvements in postural sway after
computerized balance training in older adults. Hinman and colleagues [53] also found no
improvements neither in balance, gait speed nor in simple reaction time compared to the
control group. The results of Kerdoncuff et al. [71] even showed a reduction of gait speed
in stroke patients treated with visual biofeedback compared to an increase in gait speed
for the control group treated with a traditional physical rehabilitation program.
The methods using immersive computer technologies resulted in improved motor
functions of upper extremities and a cortical activation by the affected movements
from contralesional to ipsilesional activation in the laterality index after virtual reality
intervention in patients with chronic stroke [54]. Older adults benefited from training

Cognitive and cognitive-motor interventions
67
in terms of improved functional abilities, postural control and simple auditory reaction
times [32]. A virtual rehabilitation program with the help of a semi-immersive virtual
reality workbench, in a non-hospital environment, resulted in qualitatively improved
manual trajectories and increased movement velocity of the trained upper extremities for
patients with stroke, without any transfer to real-life activities [45].
A virtual reality based treadmill intervention conducted by Yang et al. [68] requested
patients with stroke to walk on a treadmill while observing a virtual scenario of the
typical regional community. The scenarios consisted of lane walking, street crossing,
striding across obstacles, and park stroll with increasing levels of complexity. Participants
improved their walking speed and walking ability at post-training as well as after one
month after the training.
Effects on motor functions were also observed in studies using so-called off the shelf
computer game systems. Four studies proposed a training program using the Nintendo
Wii console [47,49,64,69]. Three of them were case studies and exemplified that a training
with a commercially available computer game system can be applied for older adults [47]
and for the treatment of balance problems after stroke [49,64]. The participants performed
physical training using the Wii Fit system. Using the approach of the weight- shifting
method with visual feedback, the Wii Fit games were controlled by shifting body weight
on the platform combined with a challenging game [64]. The activities on the Nintendo
Wii console were selected to practice balance, coordination, strengthening, endurance
or bilateral upper extremity coordination [47,49]. Subjects very much enjoyed the
interventions resulting in better balance and mobility performance [47,64], improvements
in gait speed, gait endurance and balance [49]. A recently published study using the
Nintendo Wii console [69] resulted in improvements in upper extremity functions in post
stroke patients.
A study conducted by de Bruin et al. [48] studied the transfer effects on gait
characteristics of elderly who executed a traditional progressive physical balance and
resistance training with integrated computer game dancing. The task of the dancing
game consisted of stepping on arrows on a dance pad. Results indicated a positive effect

Chapter Three
68
of the computer game dancing training on relative dual task costs of walking, e.g., stride
time and step length. The more traditional physical training showed no transfer effects on
dual task costs related gait characteristics.
3.3.4. Quality evaluation
The agreement on study quality between the two reviewers was 'almost perfect'. The
estimated Kappa value was 0.96 with a confidence interval ranging between 0.95 and 0.98.
The percentage of agreement between the two reviewers was 98.18%. The quality scores
ranged from 7 to 22 points out of a maximum of 22. The mean quality score was 13.46
points (range: 7–22 points), the median value was 6.5 points and the mode was 12 points.
The mean score for reporting was 6.57 points (maximum: 9 points; range: 4–9 points), for
external validity 0.68 (maximum: 2 points; range: 0–2 points), for internal validity (bias)
3.71 points (maximum: 5 points; range: 2–5 points), for internal validity (confounding)
2.25 (maximum: 4 points; range: 0–4 points).
Table 3.5 summarizes the results of the quality assessment for the three intervention
types: cognitive rehabilitation interventions, dual task interventions, and computerized
interventions.
3.4. Discussion
An increased incidence of falls among older adults is one of the most serious problems
of mobility impairment. It has been suggested that effective programs to prevent falls in
older adults should focus on training both physical and cognitive aspects. The aim of this
systematic review was to examine the literature on the effects of cognitive and cognitive-
motor interventions to improve physical functioning of older adults with additional
insights from studies conducted with brain injured adults or patients with stroke.
Our search resulted in relatively few studies that evaluated a cognitive or a cognitive-
motor intervention. Twenty-eight articles were found including studies with older adults
or patients with neurological impairments. Our results show that the method of combining
physical exercise with cognitive elements to improve physical functioning is not yet

Cognitive and cognitive-motor interventions
69
Table 3.5 Assessment of methodological quality
Reporting External validity Internal validity Bias
Internal validityConfounding
Study Hypo
thes
is/aim
/obje
ctive
clea
rly de
scribe
d
Main
outco
mes
clea
rly de
scribe
d in t
he in
trodu
ction
or m
etho
ds se
ction
Parti
cipan
ts’ ch
arac
teris
tics c
learly
descr
ibed
Inte
rven
tion c
learly
descr
ibed
Dist
ribut
ion of
princ
ipal c
onfo
unde
rs cle
arly
descr
ibed
Main
findin
gs of
the s
tudy
clea
rly de
scribe
d
Estim
ation
of ra
ndom
varia
bility
for m
ain ou
tcom
es pr
ovide
d
Actu
al pr
obab
ility v
alues
repo
rted (
e.g. 0
.035 r
athe
r tha
n <0.0
5)
Tota
l (m
ax: 9
)
Subje
cts as
ked t
o par
ticipa
te re
pres
enta
tive f
or th
e ent
ire po
pulat
ion fr
om w
hich t
hey w
ere d
erive
d
Subje
cts pr
epar
ed to
parti
cipat
e rep
rese
ntat
ive of
the e
ntire
popu
lation
from
whic
h the
y wer
e rec
ruite
d
Tota
l (m
ax 2)
Atte
mpt
to bl
ind th
ose m
easu
ring t
he m
ain ou
tcom
es
No r
etro
spec
tive u
nplan
ned s
ubgr
oup a
nalys
es
Stat
istica
l tes
ts us
ed to
asse
ss th
e main
outco
mes
appr
opria
te
Com
plian
ce w
ith in
terv
entio
n/s r
eliab
le
Main
outco
me m
easu
res a
ccur
ate (
valid
and r
eliab
le)
Tota
l (m
ax: 5
)
Patie
nts i
n diff
eren
t int
erve
ntion
grou
ps
Patie
nts r
ecru
ited o
ver t
he sa
me p
eriod
of ti
me
Stud
y sub
jects
rand
omize
d to i
nter
vent
ion gr
oups
Adeq
uate
adjus
tmen
t for
conf
ound
ing
Tota
l (m
ax: 4
)
Powe
r (m
ax: 2
)
Tota
l Sco
re (m
ax: 2
2)
COG
Batson 1 1 1 1 0 1 0 0 5 0 0 0 0 1 1 1 1 4 1 1 1 0 3 0 12
Dunsky 1 1 1 1 0 1 1 0 6 1 1 2 0 1 1 1 1 4 0 0 0 0 0 2 14
Hamel & Lajoie
1 1 1 1 0 0 0 0 4 0 0 0 0 1 1 0 1 3 1 1 1 0 3 0* 10
DT
Shigematsua 1 1 1 1 2 1 1 1 9 1 1 2 1 1 1 1 1 5 1 1 1 1 4 2 22
Shigematsub 1 1 1 1 2 1 1 1 9 0 0 0 0 1 1 1 1 4 1 1 1 1 4 2 19
Silsupadol 2006
1 1 1 1 0 1 0 0 5 0 0 0 0 1 0 1 1 3 0 0 0 0 0 0 8
Silsupadol 2009
1 1 1 1 2 1 1 1 9 0 0 0 1 1 1 1 1 5 1 1 1 1 4 0 18
Vaillant 1 1 1 1 0 1 1 1 7 1 1 2 0 1 1 1 0 3 1 1 1 0 3 0 15
You 1 1 1 1 2 1 1 1 9 0 0 0 0 1 1 0 1 3 1 1 1 0 3 0 15
COM
Bisson 1 1 1 1 0 1 0 0 5 1 1 2 0 1 1 1 1 4 1 1 0 0 2 0* 13
Broeren 1 1 1 1 1 1 1 0 7 0 0 0 0 1 0 0 1 2 0 0 0 0 0 0 9
Buccello-Stout
1 1 1 1 1 1 0 0 6 1 0 1 0 1 1 1 1 4 1 1 1 0 3 0* 14
Clark 1 1 0 1 0 1 0 0 4 0 0 0 0 1 0 1 1 3 0 0 0 0 0 0 7
de Bruin 1 1 1 1 1 1 1 1 8 1 0 1 0 1 1 1 1 4 1 1 0 1 3 0 16
Deutsch 1 1 1 1 0 1 0 0 5 0 0 0 1 1 0 1 1 4 0 1 1 0 2 0 11
Hatzitaki 1 1 0 1 0 1 1 0 5 1 0 1 0 1 1 0 1 3 1 1 1 0 3 0 12
Hinman 1 1 0 1 0 1 1 1 6 1 0 1 0 1 1 0 1 3 1 1 1 0 3 0 13
Jang 1 1 1 1 2 1 1 0 8 0 0 0 1 1 1 1 1 5 1 1 1 1 4 0 17
Kerdoncuff 1 1 1 1 1 1 1 1 8 1 0 1 0 1 1 1 1 4 1 1 1 1 4 0 17
Lajoie 1 1 1 1 0 1 1 0 6 0 0 0 0 1 1 0 1 3 1 1 0 0 2 0* 11
Mumford 1 1 1 1 0 1 0 0 5 0 0 0 0 1 1 1 1 4 0 0 0 0 0 0 9
Sackley 1 1 1 1 2 1 1 0 8 1 0 1 1 1 1 1 1 5 1 1 1 1 4 1 19
Srivastava 1 1 1 0 0 1 1 0 5 0 0 0 0 1 1 1 1 4 0 0 0 0 0 0* 9
Sugarman 1 1 0 1 0 1 0 0 4 0 0 0 0 1 0 1 1 3 0 0 0 0 0 0 7
Talassi 1 1 0 1 1 1 1 1 7 1 0 1 0 1 1 1 1 4 1 1 0 0 2 0 14
Wolf 1 1 1 1 2 1 1 1 9 0 0 0 0 1 1 1 0 3 1 1 1 1 4 0 16
Yang 1 1 1 1 1 1 1 1 8 1 1 2 1 1 1 1 1 5 1 1 1 0 3 0 18
Yong Joo 1 1 1 1 0 1 1 1 7 1 1 2 0 1 1 0 1 3 0 0 0 0 0 0 12
Abbreviations: COG = Cognitive Rehabilitation Intervention; DT = Dual task Intervention; COM = Computerized Intervention; * unable to determine

Chapter Three
70
systematically part of the current interventions for older adults or patients with neurological
impairments. The methodological heterogeneity and the numerous feasibility studies are
indicators for a topic still being in its fledgling stage.
The results of the few studies identified in this review, however, justify larger studies
with older adults. There is evidence that cognitive or cognitive-motor interventions
positively affect physical functioning, such as postural control, walking abilities and
general functions of upper and lower extremities. The majority of the included studies
resulted in improvements of the assessed functional outcome measures. The next sections
will discuss the three different intervention types applied in more detail.
3.4.1. Cognitive rehabilitation interventions
The prevalent technique used was mental imagery, which involved the participants
imagining themselves in a specific environment or performing a specific activity, without
actually performing it [75]. Brain-imaging studies showed that comparable brain areas
are activated during actual performance and during mental rehearsal of the same tasks
[76,77]. Hamel and Lajoie [51] suggest that after mental imagery the motor control task
becomes more automatic, leading to a decrease in attentional demands directed toward
the control of the motor task.
Our search resulted in three relevant studies that applied mental imagery. In one study
[44] improvements in physical functioning were shown in both the intervention and the
control group and in a second study [50], a missing control group made it impossible to
assess whether improvements in physical functioning were attained through mental
practice or not. Thus, as for now it is not possible to determine whether an isolated
cognitive rehabilitation intervention based on mental imagery is able to improve
physical functioning in older adults. There is evidence about the effectiveness of
mental imagery in improving physical functioning of other populations than older
adults [25,75]. It seems fair to state that larger randomized control studies should
be performed in order to provide more insights in the impact of mental imagery in
older adults.

Cognitive and cognitive-motor interventions
71
3.4.2. Dual task interventions
Research has shown that dual task interventions may help participants to automate a
task, to focus on other tasks and consequently, to free the individual‘s processing capacity.
After dual task exercise more attention is available to process external information and
therefore to react faster on sudden disturbances [32]. The included studies showed that
it was generally feasible to apply dual task interventions, namely combining a traditional
physical intervention with a variety of cognitive tasks, in community-dwelling older
adults with balance impairments. During the selection stage of this review, numerous
studies were identified studying the dual task abilities of older adults, though only six
studies were found which integrated the method of dual-tasking in a program designed
to improve physical functioning. Two studies included relatively simple cognitive tasks
like computing or reciting poems. Both studies showed no improvements in physical
functioning that were clearly attributable to the dual task intervention.
Using dual task exercises with variable-priority or using a complex stepping task may
both be closer to real-life conditions as compared to computing while walking. The studies
of Silsupadol et al. [60-62] and Shigematsu et al. [58,59] applied a more challenging way
of attention-demanding tasks, and, presumably thus, offered advantages in terms of
rate of learning compared to more simple cognitive tasks. Results show improvements
in functional fitness of lower extremities, balance and gait speed. The latter has been
reported as a global indicator of functional performance in older adults and is a good
predictor of falls [78].
Shigematsu and colleagues in addition provided a challenging leg exercise, which was
suggested to enhance neural functions by reducing response latency and by effectively
recruiting postural muscles resulting in an improving of the interpretation of sensory
information. Caution seems to be indicated in relation to the transfer effects of this form
of training. The pre- and post-tests that were used to assess the effects of training were
similar to the cognitive and motor tasks assigned in the interventions. Thus, it cannot be
excluded that learning effects were observed instead of real improvements in underlying
functional motor skills. From this viewpoint, it is not surprising that participants in dual

Chapter Three
72
task groups performed better in the post-tests.
The dual task interventions showed satisfying study quality with a mean of 16.2
points out of a maximum of 22 points. However, the results about the effect of dual task
interventions on physical functioning are controversial. In addition, analogue to the
cognitive rehabilitation interventions, the limited number of studies performing dual task
training hampers a generalization of results.
3.4.3. Computerized interventions
Computerized interventions varied from force platforms with visual biofeedback with
relatively simple graphics [52,53,55,57,67,71], to video capture systems that enabled the
participant to see her/himself on a screen with attractive and realistic graphics allowing
to immerge into the virtual environment [32,46,54,68]. A third set of studies used
commercially available video game consoles that combined the simplicity of a weight-
shifting training on a platform with the elaborated graphics and motivating games of a
video capture system [47-49,64,69]. The study quality of the computerized interventions
articles was lower (mean value of 12.8 points out of a maximum of 22 points) as
compared with the value of the dual task studies (16.2 points). In contrast to the dual task
interventions, however, the results of the computerized interventions showed a consistent
positive effect on various physical abilities in older adults, patients with traumatic brain
injury, and stroke patients. Computerized interventions can also be effectively used in
clinical settings. Remarkable is that every study reported that participants were more
motivated and compliant with the computerized setting in comparison to conventional
physical training programs. Computerized interventions may have engaged people who
otherwise would lack interest to undergo a traditional exercise program.
The effects of the video games on cognitive aspects of the participants have,
remarkably, not been a specific focus of the various studies. It seems, however, that
computer games have the potential to also train cognitive functions [34], including
attention and executive functions [22]. Combined with physical exercise a video game or
a virtual environment requires sensory-motor function inputs as well as cognitive inputs.

Cognitive and cognitive-motor interventions
73
The participant is required to orientate her/himself, attend, comprehend, recall, plan
and execute appropriate responses to the visual cues provided on the screen [69]. The
visual aspect is crucial since with aging, vision remains important in maintaining postural
control [79]. Virtual environments have also the potential to specifically include motor
learning enhancing features that activate motor areas in the brain [80]. In addition You
and colleagues suggest that virtual reality training could induce reorganization of the
sensorimotor cortex in chronic patients [81].
As we know from the principles of motor learning, repetition is important for both
motor learning and the cortical changes that initiate it. The repeated practice must
be linked to incremental success at some task or goal. A computerized intervention
constitutes a powerful tool to provide participant repetitive practice, feedback about
performance and motivation to endure practice [82]. In addition, it can be adapted
based on an individual participant‘s baseline motor performance and be progressively
augmented in task difficulty. Weiss and colleagues [83] suggested that virtual reality
platforms provide a number of unique advantages over conventional therapy in trying to
achieve rehabilitation goals.
First, virtual reality systems provide ecologically valid scenarios that elicit naturalistic
movement and behaviors in a safe environment that can be shaped and graded in
accordance to the needs and level of ability of the patient engaging in therapy. Secondly,
the realism of the virtual environments gives patients the opportunity to explore
independently, increasing their sense of autonomy and independence in directing their
own therapeutic experience. Thirdly, the controllability of virtual environments allows for
consistency in the way therapeutic protocols are delivered and performance recorded,
enabling an accurate comparison of a patient‘s performance over time. Finally, virtual
reality systems allow the introduction of „gaming“ factors into any scenario to enhance
motivation and increase user participation [84]. The use of gaming elements can also
be used to take patients‘ attention away from any pain resulting from their injury or
movement. This occurs the more a patient feels involved in an activity and again, allows
a higher level of participation in the activity, as the patient is focused on achieving goals

Chapter Three
74
within the game [85]. In combination with the benefits of indoor exercises such as safety,
independence from weather conditions, this distraction may result in a shift from negative
to positive thoughts about exercise [17].
3.4.4. General methodological considerations
A central element of successful cognitive rehabilitation for older adults should be the
design of interventions that either re-activate disused or damaged brain regions, or that
compensates for decline in parts of the brain through the activation of compensatory
neural reserves [86]. Cognitive activity or stimulation could be a protective factor against
the functional losses in old age. Because spatial and temporal characteristics of gait are
also associated with distinct brain networks in older adults it can be hypothesized that
addressing focal neuronal losses in these networks may represent an important strategy
to prevent mobility disability [87]. Interventions should, as previous research suggests,
focus thereby on executive functioning processes [9], and in particular on the executive
function component divided attention [11], and should include enriched environments
that provide physical activities with decision-making opportunities because these
are believed to be able to facilitate the development of both motor performance and
brain functions [88]. This review encourages the further development of virtual reality
interventions, preferably with a randomized control design.
Future research that aims to examine the relation between virtual reality environments
and improvements in both cognitive and walking skills, and the translation to better
performance on selected physical tasks, should design the training content such that the
relation between the cognitive and physical skills are more explicitly taken into account,
e.g. specific elements of divided attention are integrated in the scenario. Many of the
studies of this review were small and may have lacked statistical power to demonstrate
differences, if such differences were present. In addition, the interventions were of relatively
short duration and heterogeneous in their design, and most subjects investigated were
stroke survivors. Most studies did not specifically focus on physical functioning outcomes
from which it is known that these relate to brain functioning. For example, spatial and

Cognitive and cognitive-motor interventions
75
temporal dual task cost characteristics of gait are especially associated with divided
attention in older adults [11], and are dependent of the nature of the task investigated
(preferred versus fast walking).
3.4.5. Future directions
Future research that aims to examine the relation between improvements in cognitive
skills and the translation to better performance on selected physical tasks should take
the relation between the cognitive and physical skills into account. The majority of the
authors, and above all this holds true for the studies using computerized interventions,
does not specifically mention or is even not aware of the potential cognitive aspects of
their interventions.
3.4.6. Limitations
We developed and utilized a structured study protocol to guide our search strategy, study
selection, extraction of data and statistical analysis. However, limitations of this review
should be noted. First, a publication bias may have been present, as well as a language
bias, given that we considered only interventions described in published studies and
restricted our search to English, French, and German language publications. Second, as
there were only few randomized trials, we also included observational studies, the results
of which may be affected by confounding bias due to the absence of random assignment.
An additional limitation is that we did not investigate the effect of the interventions in
separate populations. One study included in the analysis for example assessed subjects
with MCI and dementia [65]. It can very well be argued that the results of cognitive
interventions may be expected to be different between cognitively intact, MCI, and
demented subjects. This point should be considered in future reviews on this topic.
3.5. Conclusions
The current evidence on the effectiveness of cognitive or cognitive-motor interventions
to improve physical functioning in older adults or patients with traumatic brain injury is

Chapter Three
76
limited. Yet overall, as the most studies included in this review showed, these interventions
can enhance physical functioning. The heterogeneity of the studies published so far does
not allow defining the training methodology with the greatest effectiveness. This review
nevertheless provides important foundational information in order to encourage further
development of novel cognitive or cognitive-motor interventions, preferably with a
randomized control design. Future research that aims to examine the relation between
improvements in cognitive skills and the translation to better performance on selected
physical tasks should take the relation between the cognitive and physical skills into
account. The majority of the authors, and above all this holds true for the studies using the
computerized design, does not specifically mention or is even not aware of the potential
cognitive aspects of their interventions.
Acknowledgements
The authors would like to thank Dr. Martina Gosteli of the Medicinal Library of the
University of Zurich for her help in elaborating the search strategy.
Authors‘ contributions
Conception and design: GP, EDdB; screening: GP, EDdB, data abstraction: GP, EDdB; data
interpretation: GP, EDdB; manuscript drafting: GP, EDdB, PW; KM, GP, EDdB and PW critically
revised the manuscript for its content and approved its final version.
Competing interests
The authors declare that they have no competing interests.

Cognitive and cognitive-motor interventions
77
References
1. Woollacott M, Shumway-Cook A: Attention and the control of posture and gait: a
review of an emerging area of research. Gait Posture 2002, 16(1):1-14.
2. Hays RD, Liu H, Spritzer K, Cella D: Item response theory analyses of physical functioning
items in the medical outcomes study. Med Care 2007, 45(5 Suppl 1):S32-38.
3. Kane RL, Radosevich DM: Generic Health Outcomes Measures. In: Conducting Health
Outcomes Research. 1 edition. Edited by: Brown M, Heverling C. Sudbury: Jones
2011:91.
4. Yogev-Seligmann G, Hausdorff JM, Giladi N: The role of executive function and
attention in gait. Mov Disord 2008, 23(3):329-342, quiz 472.
5. Sherrington C, Whitney JC, Lord SR, Herbert RD, Cumming RG, Close JC: Effective
exercise for the prevention of falls: a systematic review and meta-analysis. J Am
Geriatr Soc 2008, 56(12):2234-2243.
6. McDermott AY, Mernitz H: Exercise and older patients: prescribing guidelines. Am
Fam Physician 2006, 74(3):437-444.
7. Paterson DH, Jones GR, Rice CL: Ageing and physical activity: evidence to develop
exercise recommendations for older adults. Can J Public Health 2007, 98(Suppl
2):S69-108.
8. Laessoe U, Hoeck HC, Simonsen O, Voigt M: Residual attentional capacity
amongst young and elderly during dual and triple task walking. Hum Mov Sci
2008, 27(3):496-512.
9. Rapport LJ, Hanks RA, Millis SR, Deshpande SA: Executive functioning and predictors
of falls in the rehabilitation setting. Arch Phys Med Rehabil 1998, 79(6):629-633.
10. Sheridan PL, Solomont J, Kowall N, Hausdorff JM: Influence of executive function
on locomotor function: divided attention increases gait variability in Alzheimer‘s
disease. J Am Geriatr Soc 2003, 51(11):1633-1637.
11. de Bruin ED, Schmidt A: Walking behaviour of healthy elderly: attention should be
paid. Behav Brain Funct 2010, 6:59.
12. Bryan J, Luszcz MA: Measurement of executive function: considerations for detecting

Chapter Three
78
adult age differences. J Clin Exp Neuropsychol 2000, 22(1):40-55.
13. Shallice T: Specific impairments of planning. Philos Trans R Soc Lond B Biol Sci 1982,
298(1089):199-209.
14. Cicerone K, Levin H, Malec J, Stuss D, Whyte J: Cognitive rehabilitation interventions
for executive function: moving from bench to bedside in patients with traumatic
brain injury. J Cogn Neurosci 2006, 18(7):1212-1222.
15. Rosano C, Aizenstein H, Cochran J, Saxton J, De Kosky S, Newman AB, Kuller LH, Lopez
OL, Carter CS: Functional neuroimaging indicators of successful executive control in
the oldest old. Neuroimage 2005, 28(4):881-889.
16. Scherder E, Eggermont L, Visscher C, Scheltens P, Swaab D: Understanding higher
level gait disturbances in mild dementia in order to improve rehabilitation: ‘Last in-
first out‘. Neurosci Biobehav Rev 2011, 35(3):699-714.
17. de Bruin ED, Schoene D, Pichierri G, Smith ST: Use of virtual reality technique for the
training of motor control in the elderly. Some theoretical considerations. Z Gerontol
Geriatr 2010, 43(4):229-234.
18. Harley JP, Allen C, Braciszewski TL, Cicerone KD, Dahlberg C, Evans S, Foto M,
Gordon WA, Harrington D, Levin W, et al: Guidelines for cognitive rehabilitation.
NeuroRehabilitation 1992, 2:62-67.
19. Cicerone KD, Dahlberg C, Malec JF, Langenbahn DM, Felicetti T, Kneipp S, Ellmo
W, Kalmar K, Giacino JT, Harley JP, et al: Evidence-based cognitive rehabilitation:
updated review of the literature from 1998 through 2002. Arch Phys Med Rehabil
2005, 86(8):1681-1692.
20. Rohling ML, Faust ME, Beverly B, Demakis G: Effectiveness of cognitive rehabilitation
following acquired brain injury: a meta-analytic reexamination of Cicerone et al.‘s
(2000, 2005) systematic reviews. Neuropsychology 2009, 23(1):20-39.
21. Acevedo A, Loewenstein DA: Nonpharmacological cognitive interventions in aging
and dementia. J Geriatr Psychiatry Neurol 2007, 20(4):239-249.
22. Jobe JB, Smith DM, Ball K, Tennstedt SL, Marsiske M, Willis SL, Rebok GW, Morris
JN, Helmers KF, Leveck MD, et al: ACTIVE: a cognitive intervention trial to promote

Cognitive and cognitive-motor interventions
79
independence in older adults. Control Clin Trials 2001, 22(4):453-479.
23. Faucounau V, Wu YH, Boulay M, De Rotrou J, Rigaud AS: Cognitive intervention
programmes on patients affected by Mild Cognitive Impairment: a promising
intervention tool for MCI? J Nutr Health Aging 2010, 14(1):31-35.
24. Thornton KE, Carmody DP: Efficacy of traumatic brain injury rehabilitation:
interventions of QEEG-guided biofeedback, computers, strategies, and medications.
Appl Psychophysiol Biofeedback 2008, 33(2):101-124.
25. McEwen SE, Huijbregts MP, Ryan JD, Polatajko HJ: Cognitive strategy use to enhance
motor skill acquisition post-stroke: a critical review. Brain Inj 2009, 23(4):263-277.
26. Brown LA, Shumway-Cook A, Woollacott MH: Attentional demands and postural
recovery: the effects of aging. J Gerontol A Biol Sci Med Sci 1999, 54(4):M165-171.
27. Maylor EA, Allison S, Wing AM: Effects of spatial and nonspatial cognitive activity on
postural stability. Br J Psychol 2001, 92 Part 2:319-338.
28. Haggard P, Cockburn J, Cock J, Fordham C, Wade D: Interference between gait
and cognitive tasks in a rehabilitating neurological population. J Neurol Neurosurg
Psychiatry 2000, 69(4):479-486.
29. McCulloch K: Attention and dual-task conditions: physical therapy implications for
individuals with acquired brain injury. J Neurol Phys Ther 2007, 31(3):104-118.
30. Camicioli R, Howieson D, Lehman S, Kaye J: Talking while walking: the effect of a dual
task in aging and Alzheimer‘s disease. Neurology 1997, 48(4):955-958.
31. Pellecchia GL: Dual-task training reduces impact of cognitive task on postural sway.
J Mot Behav 2005, 37(3):239-246.
32. Bisson E, Contant B, Sveistrup H, Lajoie Y: Functional balance and dual-task reaction
times in older adults are improved by virtual reality and biofeedback training.
Cyberpsychol Behav 2007, 10(1):16-23.
33. Sveistrup H: Motor rehabilitation using virtual reality. J Neuroeng Rehabil 2004,
1(1):10.
34. Zelinski EM, Reyes R: Cognitive benefits of computer games for older adults.
Gerontechnology 2009, 8(1):220-235.

Chapter Three
80
35. Bashore TR, Ridderinkhof KR: Older age, traumatic brain injury, and cognitive
slowing: some convergent and divergent findings. Psychol Bull 2002, 128(1):151-198.
36. Hinkebein JH, Martin TA, Callahan CD, Johnstone B: Traumatic brain injury and
Alzheimer‘s: deficit profile similarities and the impact of normal ageing. Brain Inj
2003, 17(12):1035-1042.
37. Goldstein G, Shelly CH: Similarities and differences between psychological deficit in
aging and brain damage. J Gerontol 1975, 30(4):448-455.
38. McDowd JM, Filion DL, Pohl PS, Richards LG, Stiers W: Attentional abilities and
functional outcomes following stroke. J Gerontol B Psychol Sci Soc Sci 2003,
58(1):P45-53.
39. Broglio SP, Tomporowski PD, Ferrara MS: Balance performance with a cognitive task:
a dual-task testing paradigm. Med Sci Sports Exerc 2005, 37(4):689-695.
40. Parker TM, Osternig LR, van Donkelaar P, Chou LS: Recovery of cognitive and
dynamic motor function following concussion. Br J Sports Med 2007, 41(12):868-873,
discussion 873.
41. Downs SH, Black N: The feasibility of creating a checklist for the assessment of the
methodological quality both of randomised and nonrandomised studies of health
care interventions. J Epidemiol Community Health 1998, 52(6):377-384.
42. Landis JR, Koch GG: An application of hierarchical kappa-type statistics in the
assessment of majority agreement among multiple observers. Biometrics 1977,
33(2):363-374.
43. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, Clarke M,
Devereaux PJ, Kleijnen J, Moher D: The PRISMA statement for reporting systematic
reviews and meta-analyses of studies that evaluate health care interventions:
explanation and elaboration. J Clin Epidemiol 2009, 62(10):e1-34.
44. Batson G, Feltman R, McBride C, Waring J: Effect of mental practice combined with
physical practice on balance in the community-dwelling elderly. Activities, Adaptation
& Aging 2007, 31(2):1-18.
45. Broeren J, Claesson L, Goude D, Rydmark M, Sunnerhagen KS: Virtual rehabilitation

Cognitive and cognitive-motor interventions
81
in an activity centre for community-dwelling persons with stroke. The possibilities of
3-dimensional computer games. Cerebrovasc Dis 2008, 26(3):289-296.
46. Buccello-Stout RR, Bloomberg JJ, Cohen HS, Whorton EB, Weaver GD, Cromwell RL:
Effects of sensorimotor adaptation training on functional mobility in older adults.
Journals of Gerontology Series B: Psychological Sciences & Social Sciences 2008,
63B(5):P295-300.
47. Clark R, Kraemer T: Clinical use of Nintendo Wii bowling simulation to decrease fall
risk in an elderly resident of a nursing home: a case report. J Geriatr Phys Ther 2009,
32(4):174-180.
48. de Bruin E, Dörflinger M, Reith A, Murer K: The effect of dance dance revolution
gaming compared to conventional physical training on dual task walking costs in
elderly. Parkinsonism and Related Disorders 2010, 16: S59.
49. Deutsch J, Robbins D, Morrison J, Guarrera Bowlby P: Wii-Based Compared to
Standard of Care Balance and Mobility Rehabilitation for Two Individuals Post-Stroke.
Virtual Rehabilitation International Conference 2009, 117-120.
50. Dunsky A, Dickstein R, Marcovitz E, Levy S, Deutsch J: Home-based motor imagery
training for gait rehabilitation of people with chronic poststroke hemiparesis.
Archives of Physical Medicine and Rehabilitation 2008, 89(8):1580-1588.
51. Hamel MF, Lajoie Y: Mental imagery. Effects on static balance and attentional
demands of the elderly. Aging - Clinical and Experimental Research 2005,
17(3):223-228.
52. Hatzitaki V, Amiridis IG, Nikodelis T, Spiliopoulou S: Direction-induced effects
of visually guided weight-shifting training on standing balance in the elderly.
Gerontology 2009, 55(2):145-152.
53. Hinman MR: Comparison of two short-term balance training programs for
community-dwelling older adults. J Geriatr Phys Ther 2002, 25(3):10.
54. Jang SH, You SH, Hallett M, Cho YW, Park C, Cho S, Lee H, Kim T: Cortical reorganization
and associated functional motor recovery after virtual reality in patients with
chronic stroke: an experimenter-blind preliminary study. Arch Phys Med Rehabil

Chapter Three
82
2005, 86(11):2218-2223.
55. Lajoie Y: Effect of computerized feedback postural training on posture and attentional
demands in older adults. Aging Clin Exp Res 2004,16(5):363-368.
56. Mumford N, Duckworth J, Thomas PR, Shum D, Williams G, Wilson PH: Upper limb
virtual rehabilitation for traumatic brain injury: initial evaluation of the elements
system. Brain Inj 2010, 24(5):780-791.
57. Sackley CM, Lincoln NB: Single blind randomized controlled trial of visual feedback
after stroke: effects on stance symmetry and function. Disabil Rehabil 1997,
19(12):536-546.
58. Shigematsu R, Okura T, Nakagaichi M, Tanaka K, Sakai T, Kitazumi S, Rantanen
T: Square-stepping exercise and fall risk factors in older adults: a single-blind,
randomized controlled trial. J Gerontol A Biol Sci Med Sci 2008, 63(1):76-82.
59. Shigematsu R, Okura T, Sakai T, Rantanen T: Square-stepping exercise versus strength
and balance training for fall risk factors. Aging Clin Exp Res 2008, 20(1):19-24.
60. Silsupadol P, Lugade V, Shumway-Cook A, van Donkelaar P, Chou LS, Mayr U,
Woollacott MH: Training-related changes in dual-task walking performance of
elderly persons with balance impairment: a doubleblind, randomized controlled
trial. Gait Posture 2009, 29(4):634-639.
61. Silsupadol P, Shumway-Cook A, Lugade V, van Donkelaar P, Chou LS, Mayr U, Woollacott
MH: Effects of single-task versus dual-task training on balance performance in older
adults: a double-blind, randomized controlled trial. Arch Phys Med Rehabil 2009,
90(3):381-387.
62. Silsupadol P, Siu KC, Shumway-Cook A, Woollacott MH: Training of balance under
single- and dual-task conditions in older adults with balance impairment. Phys Ther
2006, 86(2):269-281.
63. Srivastava A, Taly AB, Gupta A, Kumar S, Murali T: Post-stroke balance training: Role of
force platform with visual feedback technique. J Neurol Sci 2009, 287(1-2):89-93.
64. Sugarman H, Weisel-Eichler A, Burstin A, Brown R: Use of the Wii Fit system for the
treatment of balance problems in the elderly: A feasibility study. 2009, 111-116.

Cognitive and cognitive-motor interventions
83
65. Talassi E, Guerreschi M, Feriani M, Fedi V, Bianchetti A, Trabucchi M: Effectiveness of a
cognitive rehabilitation program in mild dementia (MD) and mild cognitive impairment
(MCI): a case control study. Arch Gerontol Geriatr 2007, 44(Suppl 1):391-399.
66. Vaillant J, Vuillerme N, Martigne P, Caillat-Miousse JL, Parisot J, Nougier V, Juvin
R: Balance, aging, and osteoporosis: effects of cognitive exercises combined with
physiotherapy. Joint Bone Spine 2006, 73(4):414-418.
67. Wolf SL, Barnhart HX, Ellison GL, Coogler CE: The effect of Tai Chi Quan and
computerized balance training on postural stability in older subjects. Atlanta FICSIT
Group. Frailty and Injuries: Cooperative Studies on Intervention Techniques. Phys
Ther 1997, 77(4):371-381, discussion 382- 374.
68. Yang YR, Tsai MP, Chuang TY, Sung WH, Wang RY: Virtual reality-based training
improves community ambulation in individuals with stroke: a randomized controlled
trial. Gait Posture 2008, 28(2):201-206.
69. Yong Joo L, Soon Yin T, Xu D, Thia E, Pei Fen C, Kuah CWK, Kong KH: A feasibility
study using interactive commercial off-the-shelf computer gaming in upper limb
rehabilitation in patients after stroke. J Rehabil Med 2010, 42(5):437-441.
70. You JH, Shetty A, Jones T, Shields K, Belay Y, Brown D: Effects of dual-task cognitive-
gait intervention on memory and gait dynamics in older adults with a history of falls:
a preliminary investigation. NeuroRehabilitation 2009, 24(2):193-198.
71. Kerdoncuff V, Durufle A, Petrilli S, Nicolas B, Robineau S, Lassalle A, Le Tallec H,
Ramanantsitonta J, Gallien P: Interest of visual biofeedback training in rehabilitation of
balance after stroke. Ann Readapt Med Phys 2004, 47(4):169-176, discussion 177-168.
72. Tonetta M: Il TNP, un software che opera in ambiente Windows. Atti del 4. Convegno
Nazionale Informatica, Didattica e Disabilità Napoli, (in Italian); 1995.
73. Tonetta M: Riabilitazione neuropsicologica e TNP (training neuropsicologico). Aspetti
teorici e pragmatici. New Magazine Publisher, Trento (in Italian); 1998.
74. Reuben DB, Siu AL: An objective measure of physical function of elderly outpatients.
The Physical Performance Test. J Am Geriatr Soc 1990, 38(10):1105-1112.
75. Mulder T: Motor imagery and action observation: cognitive tools for rehabilitation. J

Chapter Three
84
Neural Transm 2007, 114(10):1265-1278.
76. Ehrsson HH, Geyer S, Naito E: Imagery of voluntary movement of fingers, toes,
and tongue activates corresponding body-part-specific motor representations. J
Neurophysiol 2003, 90(5):3304-3316.
77. Mulder T, de Vries S, Zijlstra S: Observation, imagination and execution of an effortful
movement: more evidence for a central explanation of motor imagery. Exp Brain Res
2005, 163(3):344-351.
78. Hardy SE, Perera S, Roumani YF, Chandler JM, Studenski SA: Improvement in
usual gait speed predicts better survival in older adults. J Am Geriatr Soc 2007,
55(11):1727-1734.
79. Perrin PP, Jeandel C, Perrin CA, Bene MC: Influence of visual control, conduction,
and central integration on static and dynamic balance in healthy older adults.
Gerontology 1997, 43(4):223-231.
80. Cross ES, Kraemer DJ, Hamilton AF, Kelley WM, Grafton ST: Sensitivity of the action
observation network to physical and observational learning. Cereb Cortex 2009,
19(2):315-326.
81. You SH, Jang SH, Kim YH, Hallett M, Ahn SH, Kwon YH, Kim JH, Lee MY: Virtual reality-
induced cortical reorganization and associated locomotor recovery in chronic
stroke: an experimenter-blind randomized study. Stroke 2005, 36(6):1166-1171.
82. Holden MK: Virtual environments for motor rehabilitation: review. Cyberpsychol
Behav 2005, 8(3):187-211, discussion 212-189.
83. Kizony R, Raz L, Katz N, Weingarden H, Weiss PL: Video-capture virtual reality system
for patients with paraplegic spinal cord injury. J Rehabil Res Dev 2005, 42(5):595-608.
84. Holden MK, Todorov E: Use of virtual environments in motor learning and
rehabilitation. In: Handbook of virtual environments design implementation and
applications. Edited by: Stanney KM. Mahwah, NJ. Lawrence Erlbaum Associates;
2002:999-1026.
85. Sanchez-Vives MV, Slater M: From presence to consciousness through virtual reality.
Nat Rev Neurosci 2005, 6(4):332-339.

Cognitive and cognitive-motor interventions
85
86. Hogan M: Physical and cognitive activity and exercise for older adults: a review. Int J
Aging Hum Dev 2005, 60(2):95-126.
87. Rosano C, Aizenstein H, Brach J, Longenberger A, Studenski S, Newman AB: Special
article: gait measures indicate underlying focal gray matter atrophy in the brain of
older adults. J Gerontol A Biol Sci Med Sci 2008, 63(12):1380-1388.
88. Yan J, Zhou C: Effects of motor practice on cognitive disorders in older adults. Eur Rev
Aging Phys Act 2009, 6(2):67-74.


Four
The effect of a cognitive-motor intervention on voluntary step
execution under single and dual task conditions in older adults:
a randomized controlled pilot studyPichierri G1, Coppe A1, Lorenzetti S2, Murer K1 and de Bruin ED1
1Institute of Human Movement Sciences and Sport, ETH Zurich, Switzerland
2Institute for Biomechanics, Department of Health Sciences and Technology, ETH Zurich,
Switzerland
published in Clinical Interventions in Aging 2012:7 175–184
Ch
ap
ter

Chapter Four
88
Abstract
Background: This randomized controlled pilot study aimed to explore whether a cognitive-
motor exercise program that combines traditional physical exercise with dance video
gaming can improve the voluntary stepping responses of older adults under attention-
demanding dual task conditions.
Methods: Elderly subjects received twice weekly cognitive-motor exercise that included
progressive strength and balance training supplemented by dance video gaming for 12
weeks (intervention group). The control group received no specific intervention. Voluntary
step execution under single and dual task conditions was recorded at baseline and post
intervention (Week 12).
Results: After intervention between-group comparison revealed significant differences for
initiation time of forward steps under dual task conditions (U = 9, p = 0.034, r = 0.55) and
backward steps under dual task conditions (U = 10, p = 0.045, r = 0.52) in favor of the
intervention group, showing altered stepping levels in the intervention group compared
to the control group.
Conclusion: A cognitive-motor intervention based on strength and balance exercises with
additional dance video gaming is able to improve voluntary step execution under both
single and dual task conditions in older adults.
Keywords: fall prevention, exercise, dance, video game

Voluntary step execution
89
4.1. Introduction
Appropriate timing and execution of stepping responses is needed for the effective
avoidance of falls [1]. With age, the speed of these responses inevitably declines due to
changes in the sensory and motor systems [2,3]. Consequently, individuals who require
more time to initiate and execute a step to avoid a threat or to recover postural balance,
either during walking or performing postural transitions [4], may be at greater risk of
falling [5].
Considerable evidence has been accumulated showing that an additional secondary
cognitive dual task causes postural instability in older adults, and thus, a delay in step
execution [6,7]. Postural balance control requires, among other things, the integration of
visual, somatosensory, and vestibular inputs, as well as the adaptation of these inputs to
changes in tasks and environmental context [6]. Maintenance and regulation of postural
balance require a high information processing capacity, and a more difficult motor task
may demand an amount that exceeds the capacity of the available resources [8].
Reduced step execution capabilities can be mitigated by exercise, and improvements
in voluntary step execution after exercise interventions have been reported in older adults
[5,9–11] and patients after stroke [12]. However, these improvements have been tested
without any additional cognitive distraction, which questions the ecological validity of
the findings; that is, it can be questioned whether the action within the test condition
is equivalent to the motor performance requirements within the physical environment.
Physical exercise alone does not contribute to an improvement of voluntary stepping
performance under attention-demanding conditions [10].
A recently published systematic review supports the recommendation that a cognitive
element should be part of an exercise program for older adults since falls often occur
under attention-demanding circumstances [13]. A way to incorporate a cognitive element
into an exercise program is the use of virtual reality techniques in the form of dance video
gaming [14]. Games based on this technique require players to stand on a dance pad and
make rapid step responses from either leg to a target location in response to a presented
visual stimulus [15]. It involves controlled body weight transfer, which is similar to the step

Chapter Four
90
responses required to cope with external threats in everyday life; thus, we hypothesized
that the game has the potential to improve voluntary step execution under attention-
demanding circumstances. Previous dance pad studies have shown the feasibility of this
approach in the elderly and have reported positive contributions to self-reported balance
confidence and mental health in older adults [15,16]. Furthermore, there are strong
indications that the addition of dance video gaming has a positive effect on dual task
walking in older adults [17].
New treatments usually have to go through a series of pilot studies to test whether
they are safe and effective [18]. The aim of this pilot study was to perform a phase II trial
according the model for complex interventions, advocated by the British Medical Research
Council [19] to test a traditional strength and balance training program that also includes
dance video gaming in a group of elderly people in order to receive an estimation of the
treatment effect and its variations. The study aimed to explore whether this cognitive-
motor exercise program is able to improve the voluntary stepping responses of older
adults under attention-demanding dual task conditions.
4.2. Material and methods
4.2.1. Participants
The study was designed as a prospective, randomized, controlled pilot trial and was carried
out from October 2010 to January 2011 with participants recruited from two care homes
in Zurich, Switzerland. The study protocol was approved by the local ethics committee
(KEK-ZH-NR 2010-0337/0). The exercise intervention was conducted in suitable locations
at the care homes. The measurements of voluntary step execution were performed in the
laboratory of the Institute for Biomechanics of the ETH Zurich, Switzerland.
All residents of the care homes were invited to attend an information session in which
the intervention was explained. Thirty-four persons attended the information session, and
30 were interested in participating in the study. Participants were included if they were older
than 65 years, had a score of at least 22 points on the Mini-Mental State Examination [20],
were able to stand upright for at least 5 minutes, and were free of rapidly progressive or

Voluntary step execution
91
terminal illness, acute illness, or unstable chronic illness. If unsure, subjects were asked
to consult their primary care physician for medical clearance. Interested individuals were
contacted by the investigator seven days later for an individual appointment to clarify any
remaining questions and to sign an informed consent statement.
Three persons refused to participate due to insufficient motivation. Two interested
persons who used wheelchairs were excluded because they did not fulfill the inclusion
criteria. A total of 25 eligible residents signed informed consent statements and were
randomly assigned to either the usual care control group (CG) or the intervention
group (IG). Eleven participants were allocated to the CG and 14 participants to the IG
using a random numbers table. Blinding of investigators was not possible because the
investigators supervised and conducted the training sessions.
4.2.2. Intervention
The IG underwent a cognitive-motor intervention consisting of twice weekly progressive
resistance training, progressive postural balance training, and progressive dance video
gaming for twelve weeks. Intensity and duration of the program were chosen based on
guidelines published by the American College of Sports Medicine [21,22] and on a review
by Paterson et al describing exercise recommendations for older adults [23]. Training
sessions were conducted in groups of three or four participants to form group cohesion
and to encourage exercise class participation [24]. A training session lasted 60 minutes and
consisted of a warm-up (5 minutes), resistance training (25 minutes), balance exercises (10
minutes), and the dance video gaming (20 minutes).
The progressive resistance training focused on the muscle groups of the core and
lower extremities that are used in the functional activities of daily living, such as walking,
standing up from a chair, sitting down, or stair climbing. The goal of each session was to
perform two sets of ten to 15 repetitions of each exercise in a slow, controlled manner,
with a one minute sitting break after each set and between the series. Training intensity
was controlled by perceived exertion and intensity between "somewhat hard" and "hard
(heavy)" on Borg's perceived exertion scale. This corresponds to a point of instantaneous

Chapter Four
92
muscular fatigue at the end of a certain exercise [25]. To maintain the intensity of the
stimulus during the training period, the number of repetitions and the load were
progressively increased with weight vests (Kettler GmbH & Co KG, D-59469 Ense-Parsit), as
tolerated by the participants. The weight of the vests was adjusted with single sand-filled
elements of 1.125 kg each.
The progressive postural balance program consisted of static and dynamic functional
balance exercises [26]. Participants' balance skills were challenged through a variety of
activities performed with the help of air-filled balance cushions (diameter 32 cm and 16
cm) and grip balls (diameter 12 cm) (Ledraplastic S.p.a, I-33010 Osoppo).
Figure 4. 1 Dance video game: (a) participant on the dance pad secured by ropes fixed on the ceiling; (b–d) screenshots of the dance video game
The dance video game was performed on metal dance pads (Figure 4.1 a) (TX 6000

Voluntary step execution
93
Metal DDR Platinum Pro, 93 × 14.7 × 109 cm, Mayflash Limited, Baoan Shenzhen, China)
with a specially designed modifycation of the StepMania (Version 3.9) software [17]. The
dance pad was connected to a desktop computer using USB. The video game was then
projected on a white wall with a beamer. A scrolling display of arrows moving upwards
across the screen cued each move, and the participants were asked to execute the
indicated steps (forward, backward, right, or left) when the arrows reached the fixed raster
graphic at the top of the screen (Figure 4.1 b–d) and in time with different songs (32 to
137 beats per minute). In the first training session, a tutorial sequence was provided to
ensure understanding of the task. As the levels increased, additional distracting visual
cues, e.g., "bombs," were presented (Figure 4.1 c). Participants had to ignore these cues
and keep their attention focused on the arrows. Occasionally, some arrows were drawn-
out on the target locations, indicating that the trainees should remain for a while on the
dance pad button on one leg (Figure 4.1 d). The arrow sequences were generated using
the Dancing Monkey MATLAB script [27]. Electronic sensors in the dance pad detected
position and timing information that was then used to provide participants with real-time
visual feedback. For each training session, the participants performed for four songs of 2
to 3 minutes length each, with a short break of 30 seconds after each song. Progression of
performance was controlled through the beats per minute and the difficulty level.
When an exercise required the participants to stand, they were secured with ropes
fixed on the ceiling, which they could hold on to (Redcord AS, Staubo, Norway).
4.2.3. Usual care
The participants in the CG did not participate in the cognitive-motor program, but were
able to participate in the leisure time programs offered at the care homes at their own
will. These programs were non-specific, not targeted toward specific exercise goals, and
were representative of what is usually offered in assisted-living facilities [28]. Table 4.1
provides information regarding the physical activities of the CG during the intervention
period.

Chapter Four
94
Table 4.1 Physical activities of the control group during intervention
Participant Activity Duration (minutes)/frequency
1 WalkingSocial dancing
30–60/daily120/weekly
2 WalkingExercise program at care home*
60/daily45/irregularly
3 WalkingExercise program at care home*
90/weekly45/irregularly
4 WalkingAqua gym
45/daily45/weekly
5 WalkingExercise program at care home*
90/daily45/weekly
6 No activities -
Notes: * Exercise program at the care home: Exercise is conducted seated or/and in a standing position. Trained factors are flexibility, coordination of movements, strength, endurance, fine and gross motor skills, posture and memory.
4.2.4. Voluntary step execution
To estimate the performance of voluntary step execution, a test protocol was adopted that is able
to identify elderly individuals at risk for falls under attention-demanding conditions [29,32]. The
protocol assesses the change in the speed of voluntary step execution under the influence of a
secondary distractive cognitive task and the time to initiate and complete a step [7,8,24]. The test
was performed with all participants one week before and one week after the twelve-week training
period.
For the test, subjects stood upright on a force platform with feet abducted 10°, barefoot, and
heels separated medio-laterally by 6 cm. The stepping task required the execution of a step forward,
backward, or to the side as quickly as possible after a tap cue on the heel, which was provided by the
investigator with a cushioned hammer. The tap cue resembles the cutaneous stimulus experienced
by the foot when hitting an object prior to stumbling or tripping [29]. Six trials for each step direction
were recorded under single task and dual task conditions for a total of 36 trials. Step execution trials
always occurred with the dominant leg, as chosen by the subject. Two target force platforms were
used in front of (for forward steps) or behind (for backward steps) the main platform in order to
register the data from the landing of the moving leg (Figure 4.2 a). The force platforms (Kistler AG,

Voluntary step execution
95
(b)
(a)
Foot o�
Foot contact
Fy [N
]C
OP
x [m
m]
Fz [N
]
100
-100
0
-200
200
-200
0
400
600
50
-50
0
-100
100
Time [Seconds]
Tap cue
0
0
0
0.5 1.0
0.5 1.0
1.00.5
Initiation
swing leg
target forceplatform
zy
x
zy
x
Figure 4.2 Voluntary step execution test: (a) participant standing on the force platform and executing a backward step after tap cue on the heel by the supervisor; (b) example of force platform data for a single step to determine the occurrence of the step parameters. Abbreviations: COPx, medio-lateral deviation of body‘s center of pressure in millimeters; Fy, anterior-posterior ground force in Newton; Fz, vertical ground force in Newton.

Chapter Four
96
Switzerland, 400 × 600 mm) collected the ground reaction force data at a frequency of 2000 Hz.
In the single task condition, subjects focused on a white cross displayed at eye-level on
a black screen at a distance of 4.60 meters in front of them. Under dual task conditions, a
Stroop Color-Word task was displayed [30,31]. Participants were instructed to read the ink
color of the displayed words out loud. The performance of the participants was controlled
and corrected by the investigator if needed, but was not recorded as the Stroop Color-
Word task was used only for distractive purposes.
4.2.5. Data and statistical analysis
The criteria for success of this pilot was based on the primary feasibility objective
(adherence to the exercise plan), and methodological standards for being adherent to
training. A 75% attendance rate for the training sessions was set as the definition for being
adherent to the training program [34]. A total of 24 training sessions was scheduled for
each individual in the IG.
Force platform data was analyzed with a program written in MATLAB R2011a (Math
Works Inc., Cambridge, MA) to identify the following time points for each trial: tap cue,
response initiation (INI), foot off, and foot contact (Figure 4.2 b). These time points relate
to the definitions provided by Melzer et al [32,35]. Tap cue on the heel was detected as
a spike greater than three standard deviations from the average baseline noise in the
anterior-posterior direction of the ground force data. INI was defined as the first medio-
lateral deviation of center of pressure toward the stance leg (greater than 4 mm away from
the average baseline noise after the tap cue). Foot off was defined as a sudden change
of the center of pressure slope toward the stance leg in the medio-lateral direction. Foot
contact corresponds to the time when loading of the vertical ground reaction force on the
target force platform reaches more than 1% of a subject's body weight.
Statistical computations were carried out with SPSS 19 for a per-protocol strategy of
analysis in which only those subjects who adhered to the training counted toward the final
results. An average value for each temporal parameter in each stepping direction and for
both task conditions (single task and dual task) was calculated. A comparison at baseline

Voluntary step execution
97
was undertaken using a Mann-Whitney U test and a chi-squared test for dichotomous
variables. Due to non-normality of the data, a Mann-Whitney U test was used to estimate
group interaction effects in the form of between-groups differences, i.e., IG and CG after
the twelve-week time period. For this purpose, the difference of the values pre and post
intervention for each subject were calculated and then compared. The effect size, r, was
calculated as r = Z/√N (where Z is the approximation of the observed difference in terms of
the standard normal distribution and N is the total number of samples; r = 0.1, small effect;
r = 0.3, medium effect; and r = 0.5, large effect). A Wilcoxon signed rank test was used to
compare inner-group pre/post data. The significance level was set at p ≤ 0.05. A trend to
significance was defined as 0.10 ≤ p > 0.05.
Table 4.2 Demographic baseline data of participants
Group Intervention group Control group
No of participants 9 6
Age (mean, SD) 83.6, 3.4 86.2, 4.8
Sex (female/male) 6/3 3/3
Height in cm (mean, SD) 160.3, 9.9 160.9, 9.4
Weight in kg (mean, SD) 68.0, 17.5 65.5, 9.4
Mini-mental statusa (median, range) 28, 27–30 25.2, 22–29
Walking assistance
None/cane or crutches 5/4 5/1
Number of falls in the last 6 monthsb
None 7 4
One 1 1
>One 1 1
Diabetes 0 1
Hypertension 2 3
Cardiac insufficiency 3 1
Arthropathy 5 1
Osteoporosis 4 2
Notes: a Minimum score = 0, maximum score = 30 (higher scores indicate better functioning); b A fall was defined as an event, which results in a person coming to rest on the ground or other lower level [33]Abbreviation: SD, standard deviation

Chapter Four
98
4.3 Results
A flow chart (Figure 4.3) provides detailed information on the subjects included in
this study and on the subjects lost during the intervention phase. Demographic
data is summarized in Table 4.2. The participants were willing to be randomized.
Neither subjective nor objective side effects related to the used intervention were
reported. There were no significant differences at baseline in either demographic
data or temporal measurements of the voluntary step execution test between the
groups.
The average exercise program compliance was 86.9% (20.8 out of 24 sessions).
Two participants achieved a compliance of only 71% (17 out of 24) and 42% (10 out
of 24), respectively. As we expected the participants to attend at least 75% of the
exercise sessions, they were not considered for the analyses.
Temporal data of the voluntary step execution task is summarized in Table
4.3. Compared to the baseline data, the IG showed an overall time reduction of
-17.9% in all assessed temporal parameters after the training program (single task
condition: -15.7%; dual task condition: -20.1%). In comparison, the CG showed
an increase in time of +1.3% in all assessed temporal parameters (single task
condition: +1.5%; dual task condition: -4.1%). Data for the dual task condition
showed longer times for each of the three examined temporal parameters under
dual task conditions compared to single task conditions for all step directions in
both groups (IG: +42.7%; CG: +30.0%).
Between-group comparison revealed significant differences for INI of forward
steps under dual task conditions (U = 9, p = 0.034, r = 0.55) and for backward steps
under dual task conditions (U = 10, p = 0.045, r = 0.52) in favor of the IG.
Inner-group comparisons resulted in step directions with significance and step
directions with a trend to significance in pre/post-differences in the IG for INI, foot
off, and foot contact (Table 4.3). There were no changes detectable for the CG for
the inner-group comparisons.

Voluntary step execution
99
Asse
ssed
for e
ligib
ility
(n =
30)
Excl
uded
(n =
5)
• No
t mee
ting
incl
usio
n cr
iteria
(n =
2)
• De
clin
ed to
par
ticip
ate
(n =
3)
Com
plet
e da
ta se
ts (n
= 6
)
Rand
omiz
ed (n
= 2
5)
Allo
cate
d to
inte
rven
tion
grou
p (n
= 1
4)• R
ecei
ved
allo
cate
d in
terv
entio
n (n
= 1
1)• D
id n
ot re
ceiv
e fu
ll al
loca
ted
inte
rven
tion
(n =
-3)
beca
use
felt
asha
med
by
play
ing
the
com
pute
rga
me
(-1)
no
stud
y co
mpl
ianc
e (<
75%
) (-2
)
Allo
cate
d to
cont
rol g
roup
(n =
11)
Loss
es fo
r tes
ts (n
= -5
)Re
ason
s: to
o fra
il (-
1), i
njur
y du
e to
a fa
ll (-
1), p
erso
nal o
blig
atio
ns (-
3)
Com
plet
e da
ta se
ts (n
= 9
)
Loss
es fo
r tes
ts (n
= -2
)Re
ason
s: in
jury
due
to a
fall
(-2)
Figu
re 4.
3 The
stud
y flow
char
t

Chapter Four
100
Tabl
e 4.3
Tem
pora
l dat
a in s
econ
ds an
d sta
tistic
al ev
aluat
ion of
the v
olunt
ary s
tep e
xecu
tion t
est
r 0.03
0.55’’
0.12
0.27
0.27
0.18
Foot
off
0.30
0.24
0.09
0.37’
0.30’
0.00
Foot
cont
act
0.37’
0.24
0.18
0.52’’
0.15
0.03
Notes
: Valu
es ar
e in s
econ
ds an
d disp
layed
as gr
oup m
edian
s with
inte
rqua
rtile
rang
es (q
1; q3
) due
to no
n-no
rmal
distri
butio
n of d
ata.
* Sign
ifica
nt in
ner-g
roup
diffe
renc
es pr
e-po
st (p
inner
≤ 0.
05) c
alcula
ted w
ith W
ilcox
on si
gned
rank
te
st; ° T
rend
to si
gnifi
canc
e (p inn
er ≤
0.10
); +
Sign
ifica
nt be
twee
n-gr
oup d
iffer
ence
s afte
r inte
rven
tion p
hase
(pbe
twee
n ≤ 0.
05) c
alcula
ted w
ith M
ann-
Whit
ney U
test.
Abbr
eviat
ions:
p betw
een, p
-valu
e for
betw
een-
grou
ps co
mpa
rison
; pinn
er, p-v
alue f
or in
ner-g
roup
com
paris
on; D
T, du
al ta
sk; r
, effe
ct siz
e (r =
0.1:
small
effec
t, ’r =
0.3:
med
ium ef
fect,
”r =
0.5:
large
effec
t); ST
, sing
le ta
sk.
p betw
een
0.906
0.03
4+
0.637
0.289
0.289
0.480
0.239
0.346
0.724
0.157
0.239
1.000
0.157
0.346
0.480
0.04
5+
0.556
0.906
Cont
rol g
roup
(n =
6)
p inner
0.249
0.600
0.345
0.600
0.463
0.753
0.345
0.345
0.345
0.917
0.917
0.249
0.600
0.345
0.917
0.116
0.917
0.463
Post
0.180
(0.16
6; 0.1
94)
0.291
(0.24
7; 0.3
55)
0.170
(0.14
9; 0.1
85)
0.248
(0.20
9; 0.3
59)
0.195
(0.17
3; 0.2
12)
0.278
(0.21
1; 0.4
13)
0.611
(0.48
3; 0.7
44)
0.709
(0.61
4; 0.8
90)
0.577
(0.48
7; 0.6
32)
0.683
(0.57
5; 0.8
30)
0.468
(0.40
6; 0.5
22)
0.612
(0.50
4; 0.7
17)
0.975
(0.71
7; 1.1
51)
0.989
(0.90
6; 1.1
95)
0.894
(0.78
9; 1.1
10)
1.113
(0.98
4; 1.3
60)
1.113
(0.98
4; 1.3
60)
0.991
(0.78
0; 1.1
01)
Pre 0.1
90 (0
.174;
0.213
)
0.259
(0.19
6; 0.3
35)
0.175
(0.17
4; 0.1
90)
0.241
(0.21
4; 0.3
63)
0.187
(0.17
1; 0.1
98)
0.259
(0.20
5; 0.4
10)
0.602
(0.50
5; 0.7
77)
0.897
(0.58
6; 0.9
34)
0.629
(0.58
8; 0.6
61)
0.782
(0.58
3; 0.8
47)
0.461
(0.39
6; 0.5
45)
0.733
(0.46
5; 0.8
52)
0.906
(0.81
3; 1.1
22)
1.231
(0.89
9; 1.2
96)
0.966
(0.72
7; 1.0
83)
0.966
(0.72
7; 1.0
83)
0.820
(0.74
3; 0.9
01)
1.039
(0.78
6; 1.3
13)
Inte
rven
tion
grou
p (n
= 9)
p inner
0.260
0.051
°
0.066
°
0.110
0.173
0.374
0.01
5*
0.02
8*
0.02
8*
0.066
°
0.051
°
0.260
0.01
5*
0.02
8*
0.066
°
0.086
°
0.051
°
0.859
Post
0.163
(0.14
3; 0.1
86)
0.265
(0.19
5; 0.4
04)
0.168
(0.13
8; 0.2
01)
0.265
(0.20
4; 0.3
23)
0.161
(0.14
7; 0.1
81)
0.261
(0.24
4; 0.2
82)
0.437
(0.39
1; 0.6
18)
0.603
(0.53
0; 0.7
76)
0.445
(0.38
7; 0.6
05)
0.644
(0.55
6; 0.8
00)
0.338
(0.28
9; 0.5
41)
0.560
(0.50
6; 0.6
31)
0.676
(0.62
7; 1.0
57)
0.799
(0.76
5; 1.2
56)
0.738
(0.64
1; 1.0
56)
0.918
(0.84
3; 1.1
58)
0.619
(0.49
7; 0.9
11)
0.989
(0.76
0; 1.0
58)
Pre 0.1
62 (0
.144;
0.253
)
0.301
(0.26
9; 0.4
96)
0.197
(0.14
4; 0.2
08)
0.273
(0.21
9; 0.3
92)
0.179
(0.14
8; 0.1
97)
0.272
(0.19
2; 0.3
60)
0.489
(0.43
8; 0.9
86)
0.716
(0.65
2; 0.8
79)
0.538
(0.40
9; 0.8
38)
0.723
(0.57
0; 1.1
55)
0.431
(0.29
8; 0.6
45)
0.615
(0.49
2; 0.8
79)
0.836
(0.67
4; 1.5
76)
1.163
(0.89
0; 1.2
45)
0.782
(0.66
2; 1.2
46)
1.045
(0.92
5; 1.5
23)
0.941
(0.51
0; 1.1
10)
0.883
(0.68
5; 1.3
44)
Tem
pora
l Par
amet
ers
Initi
atio
n
Forw
ard S
T
Forw
ard D
T
Back
ward
ST
Back
ward
DT
Sidew
ay ST
Sidew
ay DT
Forw
ard S
T
Forw
ard D
T
Back
ward
ST
Back
ward
DT
Sidew
ay ST
Sidew
ay DT
Forw
ard S
T
Forw
ard D
T
Back
ward
ST
Back
ward
DT
Sidew
ay ST
Sidew
ay DT

Voluntary step execution
101
4.4 Discussion
The present pilot study aimed to develop and test a multimodal exercise intervention
and to deliver it to individuals living in care homes. The main focus was to evaluate the
feasibility of the multimodal intervention as a whole and the ability to recruit and retain
elderly subjects, as well as to assess the effects of the intervention. This study showed
that a cognitive-motor training program containing strength, balance, and computerized
cognitive training components is feasible and is able to improve voluntary step execution
under single task and dual task test conditions in older adults living in care homes. We
demonstrated the feasibility of acquiring acceptable compliance rates for care home
dwelling older people randomized to control and experimental training groups.
Our target of 75% compliance for this 12-week pilot project was attained. Two
individuals had a less than 75% attendance rate and were considered non-compliant
for the training. This non-compliance was mainly attributable to permanent sickness
and low motivation that prevented program adherence. Thus, compliance with the
exercise interventions and retesting was excellent. Adherence for group-based exercises
could be expected to be between 72% and 88% [34]. Our intervention is in the higher
range of adherence for group-based exercise. However, where we report on values after
three training months, Nyman and Victor [34] report values that may be expected by 12
months. In a future phase III trial, the follow-up period for the assessment of adherence
and attrition should, therefore, preferably be extended to a similar time frame to facilitate
comparability of this future study with reference values.
To our knowledge this is the first intervention study that demonstrates temporal
improvements in voluntary step execution under dual task conditions in older adults.
This study confirms previous findings that showed improvements in dual task motor
performance after an exercise program that included additional dance video gaming [17].
Although in previous literature, the deficiency of older adults in making rapid voluntary
steps under dual task conditions is well documented, there is still a lack of studies aiming
to improve the performance of voluntary step execution of older adults, specifically
under attention-demanding circumstances. The deficiency of coping with attention-

Chapter Four
102
demanding situations is well illustrated by the temporal delay of step execution in the
dual task condition of the voluntary step execution test used in this study. In line with
previous reports [29], we observed a temporal delay in step responses for all participants,
regardless of group allocation, under the influence of a concurrent cognitive task.
In the dance video game, subjects were expected to observe the virtual environment
for drifting arrows and initiate dance steps at the same time. When using an outward step,
participants needed to rapidly unload the leg they were falling toward to allow them
to take a step. This may be challenging from a cognitive, reaction time, and/or muscle
power generation perspective [36]. The crucial point is that dance video gaming not only
requires well-coordinated leg movements, but also requires cognitive work, e.g., sensing
of stimuli, paying attention, and making quick decisions [14].
The fact that this intervention had an impact on the initiation of the step response is
important since step or gait initiation is frequently repeated during daily activities, leading
to accidental falls during the step initiation phase in people with deficits in balance control
[37]. Important mechanisms for step initiation are the anticipatory postural adjustments
(APAs). The function of APAs is to prepare the body for the imminent movement and
possible changes in balance as a direct result of the movement caused by moving the
body center of mass toward the stance limb [38]. Falls during initiation of a step could
occur when the APAs are not performed efficiently enough prior to the unloading of the
swing leg, causing an unstable postural condition [4]. These mechanisms are complex and
require efficient peripheral sensory detection and afferent nerve conduction, followed by
central neural processing and efferent nerve conduction [29,39]. It is hypothesized that
these mechanisms are repeatedly trained by the use of a dance video game. Every step
on a dance pad has to be planned and executed with the proper timing while focusing
attention on the arrows on the screen.
Since our dance video game was based on the correct timing of the steps and not
on the maximal speed generation of the leg, we hypothesized that improvements in
step execution would be accountable in large part to the more efficient intramuscular
interplay, induced as well by the strength and balance training. The finding that a large

Voluntary step execution
103
part of the improvements in voluntary step execution seems to be attributable to the
earlier execution of APA movements during the initiation phase was somewhat surprising.
This leads to the question of whether the improvements we observed are attributable
to peripheral or to central adaptations. It is known that the supplementary motor area
contributes to the timing of the APAs during step initiation [40]. It would be interesting to
examine whether our cognitive-motor intervention has an influence on the activity of the
supplementary motor area in a future study to clarify this observation.
4.4.1. Related work
There are some reports on the use and effects of similar virtual reality training in various
populations. Methods using immersive computer technologies resulted in improved
motor functions of the upper extremities and a cortical activation after virtual reality
intervention in patients with chronic stroke [41]. Older adults benefited from training
in terms of improved functional abilities, postural control, and simple auditory reaction
times under dual task conditions [42]. Functional balance and dual task reaction times
in older adults are improved by virtual reality and biofeedback training. A virtual
rehabilitation program with the help of a semi-immersive virtual reality workbench,
in a non-hospital environment, resulted in qualitatively improved manual trajectories
and increased movement velocity of the trained upper extremities for patients with
stroke, but without any transfer to real-life activities [43]. A virtual reality based
treadmill intervention conducted by Yang et al [44] showed improved walking speed
and walking ability at post-training in patients with stroke. Preliminary evidence for
clinical effectiveness of virtual reality obstacle training post stroke has been reported
by Jaffe et al [45].
Although it seems more intuitive that more immersive virtual environments are to
be preferred for motor training, this may not actually be the case [46]. Less immersive
desktop or wall screen displays can be used for this purpose as well [14] and have
the advantage that no studies that used these two dimensional displays have been
associated with incidence of cyber-sickness [46].

Chapter Four
104
4.4.2. Limitations
Several limitations of this work should be discussed. Surely the fact that step direction and
the swing leg in the voluntary step execution test were known prior to the step execution
could possibly have influenced the initiation of the step. An impact on the generation of
APAs cannot be excluded since the subjects may try to lean on the supporting leg prior
to the tap cue. However, the subjects of the CG had the same conditions and showed
different reactions. Furthermore, we attempted to control for this potential disruptive
factor through careful observation of the center of pressure on the verge of the tap cue.
The point of application of the tap cue itself might be a limitation of the assessment
protocol. A trip stimulus under real life conditions would be expected on the front of the
foot and not the heel, and therefore, giving tap cues on the foot front might result in
different reactions. Another limitation was the rather small sample size.
This pilot study, therefore, only reveals first estimates for the measures of a consecutive
phase III study. This is an inherent property of a pilot study, and our findings warrant
further research in a larger phase III main study that includes a larger sample and clinically
relevant outcome measures. Differences regarding training intensities between the
groups were another limitation. Future studies with larger sample sizes are needed, which
compare training groups that achieve similar amounts of strength and balance training
and where one group receives additional game-like training. For a more substantial study,
monitoring the occurrence of falls post intervention is also recommended.
4.4.3. Future directions
The IG trained 60 minutes twice weekly for 12 weeks and the CG received the usual care. It
was thus expected that we would observe a difference in the development between the
two groups since it seemed obvious that the difference in the amount of training would
be the explanatory factor for the observed differences in the voluntary step execution
test. We did not expect an effect for usual care because it did not comply with training
recommendations to improve physical functions to prevent falls in the elderly [47].
Therefore, future studies should compare training groups that achieve similar amounts

Voluntary step execution
105
of strength and balance training, where the intervention group receives an additional
computerized cognitive component and the control group a placebo. In this case, we
expect, however, only marginal effects on voluntary step performance under dual task
conditions from the control group. The results of previous studies with similar groups
that performed progressive, machine-driven, resistance training complemented with
functional balance exercises revealed no improvement of performance under attention-
demanding circumstances [48,49].
In future studies, to clarify the additional influence of the dance video game on the
subjects in the IG, we should consider a study design with a control group that would
perform the strength and balance exercises without the additional dance video gaming.
Currently, we are performing such a trial registered under ISRCTN05350123 (www.
controlled-trials.com). In this study, however, we wanted to demonstrate the "proof of
concept" of the effect of a cognitive-motor intervention compared to usual care in care
homes in a pilot study.
4.5. Conclusion
We conclude that pilot studies with explicit feasibility objectives are important foundation
steps in preparing for large trials. Ongoing formal review of the multifaceted issues
inherent in the design and conduct of pilot studies can provide invaluable feasibility and
scientific data for rehabilitation specialists, e.g., physiotherapists, and may also be highly
relevant for furthering the development of theory based rehabilitation. For older
adults, the ability to take a quick step to prevent a fall is crucial, especially under
attention-demanding circumstances. We could demonstrate that a cognitive-motor
intervention based on strength and balance exercises with the addition of dance
video gaming is able to improve voluntary step execution under both single and dual
task conditions in older adults. The trainees were able to quicken step initiation and
total step completion time.
This study may constitute a reference for further studies in the topic of fall
prevention in older adults with the aim to improve physical performance under dual

Chapter Four
106
task conditions. This study encourages the further development of this intervention,
preferably with a randomized control design and a larger sample. The application in
a main study is deemed feasible with no need for protocol modifications.
Acknowledgments
A special thank goes to Turgut Gülay, research assistant at the Institute of Biomechanics,
for the assistance during the voluntary step execution test. We would also like to thank
Angela Naegeli and Amos Coppe for supervising the training program and Eva van het
Reve and Andrea Schärli for their help during the voluntary step execution test.
Authors' contributions
Conception and design: GP, EDdB, AC; manuscript drafting: GP, EDdB; critical revision of
manuscript for its content and approval of final version: GP, EDdB, AC, SL, KM.
Disclosure
The authors report no conflicts of interest in this work.

Voluntary step execution
107
References
1. Maki BE, McIlroy WE. Control of rapid limb movements for balance recovery: age
related changes and implications for fall prevention. Age Ageing. 2006;35 Suppl
2:ii12-ii18.
2. Inglin B, Woollacott M. Age-related changes in anticipatory postural adjustments
associated with arm movements. J Gerontol. 1988;43(4): M105-M113.
3. Rogers MW, Kukulka CG, Brunt D, Cain TD, Hanke TA. The influence of stimulus cue
on the initiation of stepping in young and older adults. Arch Phys Med Rehabil.
2001;82(5):619-624.
4. Rapp K, Becker C, Cameron ID, Konig HH, Buchele G. Epidemiology of falls in
residential aged care: analysis of more than 70,000 falls from residents of bavarian
nursing homes. J Am Med Dir Assoc. 2012;13(2): e181-e186.
5. Rogers MW, Johnson ME, Martinez KM, Mille ML, Hedman LD. Step training
improves the speed of voluntary step initiation in aging. J Gerontol A Biol Sci Med Sci.
2003;58(1):46-51.
6. Shumway-Cook A, Woollacott M. Attentional demands and postural control: the
effect of sensory context. J Gerontol A Biol Sci Med Sci. 2000;55(1):M10-M16.
7. Brauer SG, Woollacott M, Shumway-Cook A. The influence of a concurrent cognitive
task on the compensatory stepping response to a perturbation in balance-impaired
and healthy elders. Gait Posture. 2002;15(1):83-93.
8. Lajoie Y, Teasdale N, Bard C, Fleury M. Attentional demands for static and dynamic
equilibrium. Exp Brain Res. 1993;97(1):139-144.
9. Nnodim JO, Strasburg D, Nabozny M, et al. Dynamic balance and stepping versus tai
chi training to improve balance and stepping in at-risk older adults. J Am Geriatr Soc.
2006;54(12):1825-1831.
10. Melzer I, Marx R, Kurz I. Regular exercise in the elderly is effective to preserve the
speed of voluntary stepping under single-task condition but not under dual-task
condition. A case-control study. Gerontology. 2009;55(1):49-57.
11. Wong AMK, Pei Y-C, Lan C, Huang S-C, Lin Y-C, Chou S-W. Is Tai Chi Chuan effective

Chapter Four
108
in improving lower limb response time to prevent backward falls in the elderly? Age
(Dordr). 2009;31(2):163-170.
12. Marigold DS, Eng JJ, Dawson AS, Inglis JT, Harris JE, Gylfadottir S. Exercise leads
to faster postural reflexes, improved balance and mobility, and fewer falls in older
persons with chronic stroke. J Am Geriatr Soc. 2005;53(3):416-423.
13. Pichierri G, Wolf P, Murer K, de Bruin ED. Cognitive and cognitive-motor interventions
affecting physical functioning: a systematic review. BMC Geriatr. 2011;11:29.
14. de Bruin ED, Schoene D, Pichierri G, Smith ST. Use of virtual reality technique for the
training of motor control in the elderly. Some theoretical considerations. Z Gerontol
Geriatr. 2010;43(4):229-234.
15. Smith ST, Sherrington C, Studenski S, Schoene D, Lord SR. A novel Dance Dance
Revolution (DDR) system for in-home training of stepping ability: basic parameters
of system use by older adults. Br J Sports Med. 2011;45(5):441-445.
16. Studenski S, Perera S, Hile E, Keller V, Spadola-Bogard J, Garcia J. Interactive video
dance games for healthy older adults. J Nutr Health Aging. 2010;14(10):850-852.
17. de Bruin ED, Reith A, Dörflinger M, Murer K (2011) Feasibility of Strength-Balance
Training Extended with Computer Game Dancing in Older People; Does it Affect Dual
Task Costs of Walking?. J Nov Physiother 1:104. Accessible at http://www.omicsgroup.
org/journals/2165-7025/2165-7025-1-104.php?aid=3350
18. Thabane L, Ma J, Chu R, et al. A tutorial on pilot studies: the what, why and how. BMC
Med Res Methodol. 2010;10:1.
19. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and
evaluating complex interventions: the new Medical Research Council guidance.
BMJ. 2008;337:a1655.
20. Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading
the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198.
21. Kraemer WJ, Adams K, Cafarelli E, et al. American College of Sports Medicine position
stand. Progression models in resistance training for healthy adults. Med Sci Sports
Exerc. 2002;34(2):364-380.

Voluntary step execution
109
22. Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, et al. American College of
Sports Medicine position stand. Exercise and physical activity for older adults. Med
Sci Sports Exerc. 2009;41(7):1510-1530.
23. Paterson DH, Jones GR, Rice CL. Ageing and physical activity: evidence to develop
exercise recommendations for older adults. Can J Public Health. 2007;98 Suppl
2:S69-S108.
24. Estabrooks PA, Carron AV. Group cohesion in older adult exercisers: prediction and
intervention effects. J Behav Med. 1999;22(6): 575-588.
25. Borg G. Borg's Perceived Exertion and Pain Scales. Champaign, IL: Human Kinetics; 1998.
26. de Bruin ED, Murer K. Effect of additional functional exercises on balance in elderly
people. Clin Rehabil. 2007;21(2):112-121.
27. O'Keeffe K. Dancing Monkeys (Automated creation of step files for Dance Dance
Revolution). http://monket.net/files/dancingmonkeys/DancingMonkeys.pdf.
Accessed May 31, 2012. Imperial College London; 2003.
28. de Bruin E, Spence J, Hartman M, Murer K. Physical activity recommendations and
programmes offered in Swiss residential settings. Physio Science. 2008;4(4):154-162.
29. Melzer I, Oddsson LIE. The effect of a cognitive task on voluntary step execution in
healthy elderly and young individuals. J Am Geriatr Soc. 2004;52(8):1255-1262.
30. Stroop J. Studies of interference in serial verbal reactions. Journal of Experimental
Psychology. 1935; 18: 643-662.
31. Van der Elst W, Van Boxtel M, Van Breukelen G, Jolles J. The Stroop Color-Word Test -
Influence of Age, Sex, and Education; and Normative Data for a Large Sample Across
the Adult Age Range. Assessment. 2006; 13: 62-79.
32. Melzer I, Kurz I, Shahar D, Levi M, Oddsson L. Application of the voluntary step
execution test to identify elderly fallers. Age Ageing. 2007;36(5):532-537.
33. The Kellogg International Work Group on the Prevention of Falls by the Elderly. The
prevention of falls in later life. A report. Danish medical bulletin. 1987; 34 Suppl 4: 1-24.
34. Nyman SR, Victor CR. Older people's recruitment, sustained participation, and
adherence to falls prevention interventions in institutional settings: a supplement

Chapter Four
110
to the Cochrane systematic review. Age Ageing. 2011;40(4):430-436.
35. Melzer I, Shtilman I, Rosenblatt N, Oddsson LI. Reliability of voluntary step execution
behavior under single and dual task conditions. J Neuroeng Rehabil. 2007;4:16.
36. Egerton T, Brauer SG, Cresswell AG. Changes in stepping response to lateral
perturbations immediately following a single bout of physical activity. Physiother Res
Int. 2010 [epub ahead of print.]
37. Uemura K, Yamada M, Nagai K, Tanaka B, Mori S, Ichihashi N. Fear of falling is
associated with prolonged anticipatory postural adjustment during gait initiation
under dual-task conditions in older adults. Gait Posture. 2012:35(2):282-286.
38. Maki BE, McIlroy WE. The role of limb movements in maintaining upright stance: the
"change-in-support" strategy. Phys Ther. 1997;77(5): 488-507.
39. Goble DJ, Coxon JP, Van Impe A, et al. Brain activity during ankle proprioceptive
stimulation predicts balance performance in young and older adults. J Neurosci.
2011;31(45):16344-16352.
40. Jacobs JV, Lou JS, Kraakevik JA, Horak FB. The supplementary motor area contributes to
the timing of the anticipatory postural adjustment during step initiation in participants
with and without Parkinson's disease. Neuroscience. 2009;164(2):877-885.
41. Jang SH, You SH, Hallett M, et al. Cortical reorganization and associated functional
motor recovery after virtual reality in patients with chronic stroke: an experimenter-
blind preliminary study. Arch Phys Med Rehabil. 2005;86(11):2218-2223.
42. Bisson E, Contant B, Sveistrup H, Lajoie Y. Functional balance and dual-task reaction
times in older adults are improved by virtual reality and biofeedback training.
Cyberpsychol Behav. 2007;10(1):16-23.
43. Broeren J, Claesson L, Goude D, Rydmark M, Sunnerhagen KS. Virtual rehabilitation
in an activity centre for community-dwelling persons with stroke. The possibilities of
3-dimensional computer games. Cerebrovasc Dis. 2008;26(3):289-296.
44. Yang YR, Tsai MP, Chuang TY, Sung WH, Wang RY. Virtual reality-based training
improves community ambulation in individuals with stroke: a randomized controlled
trial. Gait Posture. 2008;28(2): 201-206.

Voluntary step execution
111
45. Jaffe DL, Brown DA, Pierson-Carey CD, Buckley EL, Lew HL. Stepping over obstacles
to improve walking in individuals with poststroke hemiplegia. J Rehabil Res Dev.
2004;41(3A):283-292.
46. Holden MK. Virtual environments for motor rehabilitation: review. Cyberpsychol
Behav. 2005;8(3):187-211; discussion 212-219.
47. Sherrington C, Whitney JC, Lord SR, Herbert RD, Cumming RG, Close JC. Effective
exercise for the prevention of falls: a systematic review and meta-analysis. J Am
Geriatr Soc. Dec 2008;56(12):2234-2243.
48. Hartmann A, Murer K, de Bie RA, de Bruin ED. The effect of a foot gymnastic exercise
programme on gait performance in older adults: a randomised controlled trial.
Disabil Rehabil. 2009;31(25): 2101-2110.
49. Hartmann A, Murer K, de Bie RA, de Bruin ED. The effect of a training program
combined with augmented afferent feedback from the feet using shoe insoles on
gait performance and muscle power in older adults: a randomised controlled trial.
Disabil Rehabil. 2010;32(9):755-764.


Five
A cognitive-motor intervention using a dance video game to enhance foot
placement accuracy and gait under dual task conditions in older adults:
a randomized controlled trialPichierri G1, Murer K1, de Bruin ED1
1Department Health Sciences and Technology (D-HEST),
Institute of Human Movement Sciences and Sport, ETH Zurich, Switzerland
published in BMC Geriatrics 2012, 12:74 (www.biomedcentral.com/1471-2318/12/74)
Ch
ap
ter

Chapter Five
114
Abstract
Background: Computer-based interventions have demonstrated consistent positive effects
on various physical abilities in older adults. This study aims to compare two training groups
that achieve similar amounts of strength and balance exercise where one group receives
an intervention that includes additional dance video gaming. The aim is to investigate the
different effects of the training programs on physical and psychological parameters in older
adults.
Methods: Thirty-one participants (mean age ± SD: 86.2 ± 4.6 years), residents of two Swiss
hostels for the aged, were randomly assigned to either the dance group (n = 15) or the control
group (n = 16). The dance group absolved a twelve-week cognitive-motor exercise program
twice weekly that comprised progressive strength and balance training supplemented
with additional dance video gaming. The control group performed only the strength and
balance exercises during this period. Outcome measures were foot placement accuracy, gait
performance under single and dual task conditions, and falls efficacy.
Results: After the intervention between-group comparison revealed significant differences for
gait velocity (U = 26, p = 0.041, r = 0.45) and for single support time (U = 24, p = 0.029, r = 0.48)
during the fast walking dual task condition in favor of the dance group. No significant between-
group differences were observed either in the foot placement accuracy test or in falls efficacy.
Conclusions: There was a significant interaction in favor of the dance video game group for
improvements in step time. Significant improved fast walking performance under dual task
conditions (velocity, double support time, step length) was observed for the dance video game
group only. These findings suggest that in older adults a cognitive-motor intervention may result in
more improved gait under dual task conditions in comparison to a traditional strength and balance
exercise program.
Trial registration: This trial has been registered under ISRCTN05350123 (www.controlled-
trials.com)
Keywords: dual task, dance video game, gait, older adults, cognitive-motor intervention

Foot placement accuracy and gait
115
5.1. Background
In the growing population of older people falling is a common problem. Approximately
30% of older adults over 65 years of age, experience a fall each year [1–3]. Fall incidence is
even higher (50%) in women aged 85 and above [4]. Individuals who require more time to
initiate and execute a step to avoid a threat or to recover postural balance, either during
walking or performing postural transitions, may be at greater risk for falling [5]. Similarly,
variable spatio-temporal gait characteristics may increase this risk [2]. For safe walking
the accuracy with which one places the foot on the walking surface is essential, especially
in challenging environments. Decreased foot placement accuracy [6,7] together with an
increased variability in spatio-temporal gait characteristics [8], and dual task deficits [9] are
typical symptoms of the ageing process and constitute critical factors that compromise
safe walking [10].
Common tasks of daily life such as walking are dependent on both sensorimotor
processes and higher-level cognitive functions [9]. Thus, the accurate foot placement
onto a footpath for instance, requires not only the appropriate planning and execution of
the movement. It also requires visual scanning, the extraction of visual information from
the environment, and cognitive skills related to so-called executive functioning processes
[7,11,12]. The term executive functioning processes refers to a group of cognitive actions
that include: dealing with novelty, planning and implementing strategies for performance,
using feedback to adjust future responding, vigilance, and inhibiting task-irrelevant
information [13]. There also is increasing evidence that an age-related decline in visuo-
motor control contributes to deficiencies in foot placement control [14]. Suboptimal visual
sampling strategies have been observed in older adults prone to falling when taught to
step into a target location [7,14,15].
Exercise interventions that incorporate exercises to improve muscle strength and
postural control have been often recommended for older adults [16]. However, with
physical exercise alone the additional cognitive requirements of safe walking cannot be
addressed. Two recent reviews discussed the interplay between physical functions and
cognition [17,18]. Both brought out the importance to combine physical and cognitive

Chapter Five
116
training into clinical practice to enable older adults to move safer in their physical
environment. Especially computerized interventions seem to be promising for this
purpose [17]. Thus, cognitive elements should be taken into account when designing an
exercise regimen with the aim to preserve or improve walking skills in older adults [19,20].
Interventions should thereby focus on executive functioning processes [19], in particular
on divided attention [21], and should provide physical activities with decision-making
opportunities because these are believed to be able to facilitate the development of both
physical performance and brain functions [22].
A simple and motivating way to incorporate a cognitive element into a physical exercise
program is the use of interactive video games. Interactive video games seem to have the
potential to train cognitive functions [23] such as executive functioning processes [24].
An interactive dance video game for example [25–27], requires the player to observe
the virtual environment for drifting cues and to concurrently execute well-coordinated
body movements, thus, challenging in particular divided attention skills. Previous dance
video games studies have shown the feasibility, defined through recruitment, attrition
and adherence to the exercise intervention [28], of this approach. Dance video games
studies in senior living settings [26,27,29,30] or with post-menopausal women [31] have
also shown that this approach is a safe, low-cost and motivating way to activate and
ensure continuation of physical exercise in middle-aged and older adults. Further, positive
contributions to self-reported balance confidence and mental health were observed
[26,29].
The results of two pilot studies conducted in care home settings, have shown that
the addition of dance video gaming may have a positive effect on relative dual task
costs of walking [30] and gait initiation under attention-demanding circumstances [27]
even in the oldest old (85 years and beyond). These latter two findings, however, should
be interpreted with caution. In both studies the control group did not train but rather
underwent usual care. To clarify the additional influence of the dance video game we
should consider a study design with a control group performing the same strength and
balance exercises, however, without the additional dance video gaming [27].

Foot placement accuracy and gait
117
This study compares two training groups that achieve similar amounts of physical
strength and balance exercise, where one group additionally performs dance video game
training. The aim is to investigate the additional effects of the dance video game training
on foot placement accuracy [7,15], gait under single and dual task conditions, and on fear
of falling.
5.2. Methods
5.2.1. Participants
The study was designed as a prospective randomized controlled trial (ISRCTN05350123)
and was carried out from June to September 2011. Participants were recruited from two
hostels for the aged in the Canton of Zurich, Switzerland. The study protocol was approved
by the local ethics committee (KEK-ZH-NR 2011-0005/0). All measurements and trainings
were performed in suitable locations at the hostels.
The residents of both hostels were invited to attend an information session. Thirty-five
(67.3%) out of 52 persons were interested in participating and were assessed for eligibility.
Participants were included if they were older than 65 years, had a score of at least 22 points
on the Mini-Mental State Examination (MMSE) [32], were able to walk for at least eight
meters with or without the need for a walking aid, and were free of rapidly progressive or
terminal illness, acute illness or unstable chronic illness. If unsure, subjects were asked to
consult their primary care physician for medical clearance. They were excluded if a severe
impairment of vision would impede to see projections on a wall screen as needed for the
intervention.
Four interested persons were excluded from the study before the randomization process. One
person changed his mind and declined to participate due to insufficient motivation. One person
suffered from hernia inguinalis before the start of the study and two other persons were excluded
for not fulfilling the inclusion criteria (MMSE < 22). A total of 31 (59.6%) eligible residents signed
informed consent statements and were randomly assigned to either the ‘Dance group‘ (DG, n =
15) or the ‘Control group‘ (CG, n = 16) using a random numbers table. Blinding of investigators
was not possible because the investigators supervised and conducted the training sessions.

Chapter Five
118
5.2.2. Intervention
The DG and the CG underwent a twice-weekly physical exercise program consisting of
progressive resistance and postural balance training for twelve weeks. Intensity and
duration of the program were chosen based on the guidelines published by the American
College of Sports Medicine [33,34] and on a review by Paterson et al. describing exercise
recommendations for older adults [35]. Training sessions were conducted in groups
of three or four participants to form group cohesion and to encourage exercise class
participation [36]. A training session lasted on average 40 minutes and consisted of a
warm-up (5 minutes), resistance training (25 minutes), and balance exercises (10 minutes).
In addition to the physical exercise program the DG performed a progressive video game
dancing program for 10-15 minutes throughout the study (‘cognitive-motor program‘).
When exercises required the participants to stand, they were requested to hold on to ropes
fixed on the ceiling for safety reasons (Figures 5.1 and 5.2) (Redcord AS, Staubo, Norway).
a b c
weight west
Redcords
air-filled cushion
Figure 5. 1 Exercise examples from the physical exercise program: strength exercises (a) sit-to-stand, (b) squat; (c) balance exercise: subject rolls the ball back and forth or from the left to the right with the left foot while balancing on the air-filled cushion.

Foot placement accuracy and gait
119
5.2.3. Physical exercise
The progressive resistance training focused on the muscle groups of the core and lower
extremities that are used in functional activities of daily living (Figure 5.1 a–b). Two sets
of ten to 15 repetitions of each exercise in a slow, controlled manner were performed.
One minute sitting breaks after each set and between the series were provided. Training
intensity was controlled by perceived exertion and intensity between „somewhat hard“
and „hard (heavy)“ on Borg‘s perceived exertion scale [37]. To maintain the intensity of
the stimulus during the training period, the number of repetitions and the load were
progressively increased with weight vests (Kettler GmbH & Co. KG, D-59469 Ense-Parsit),
as tolerated by the participants.
The progressive postural balance program (Figure 5.1 c) consisted of static and
dynamic functional balance exercises using air-filled cushions and grip balls (Ledraplastic
S.p.a, I- 33010 Osoppo) [38]. A more detailed description of the program can be found
elsewhere [38].
5.2.4. Cognitive-motor program
As an additional cognitive element the DG performed the dance video game after
the physical exercise in every training session. The dance video game was performed
on metal dance pads (Figure 5.2 a) (TX 6000 Metal DDR Platinum Pro, 93 x 14.7 x
109 cm, Mayflash Limited, Baoan Shenzhen, China) and with a specially designed
modification of the StepMania (Version 3.9) free-ware [27,30]. The dance video game
screen was projected on a white wall. A scrolling display of arrows moving upwards
across the screen cued each move, and the participants were asked to execute the
indicated steps (forward, backward, right, or left) when the arrows reached the fixed
raster graphic at the top of the screen (Figure 5.2 b–d), and in time with different
songs (32 to 137 beats per minute). In the first training session a tutorial sequence
was provided to ensure understanding of the task. As the levels increased additional
distracting visual cues, e.g., „bombs,“ were presented (Figure 5.2 c). Participants had
to ignore these cues and keep their attention focused on the arrows. Occasionally,

Chapter Five
120
some arrows were drawn-out on the target locations indicating that the trainees
should remain for a while on the dance pad button on one leg (Figure 5.2 d). The arrow
sequences were generated using the Dancing Monkey MATLAB script [39]. Electronic
sensors in the dance pad detected position and timing information that was then
used to provide participants with real-time visual feedback. For each training session,
the participants performed for four songs of two to three minutes length each, with a
short break of 30 seconds after each song. Progression of performance was controlled
through the beats per minute and the difficulty level.
Figure 5. 2 Dance video game: (a) participant on the dance pad secured by ropes fixed on the ceiling; (b–d) screenshots of the dance video game

Foot placement accuracy and gait
121
5.2.5. Baseline assessments of vision
To ensure that participants were free of vision impairments, which would have complicated
the performance of the video game dancing part, participants‘ vision skills were assessed
with the vision tests of the ‘Physiological Profile Assessment‘ (PPA) [40,41]. Tests of edge
contrast sensitivity (‘Melbourne Edge Test‘), and binocular dual-contrast visual acuity,
were considered for assessing vision.
5.2.6. Test procedures and outcomes
The following tests were performed in the week before and in the week after the twelve
weeks training period in suitable locations at the hostels.
5.2.6.1. Foot placement accuracy test
Foot placement accuracy (FPA) was assessed with an adapted version of the protocol
described by Chapman and Hollands in 2007 [7]. Subjects were instructed to walk at
self-selected walking speed along a path with three different walking conditions:
‘Condition 1‘ required placing the right foot into Target 1 (T1) (Figure 5.3 a); in ‘Condition
2‘ subjects placed the right foot into T1 and the left foot into Target 2 (T2) (Figure 5.3 b);
‘Condition 3‘ additionally required stepping over an obstacle placed between the two
targets (Figure 5.3 c). The targets and the obstacle were made of soft foam material. The
targets were rectangular (target area: 190 mm x 415 mm) and comprised a raised border
(40 mm x 40 mm x 40 mm). Dimensions of the obstacle were 170 mm x 670 mm x 25 mm
(height x length x depth). 170 mm corresponds to the ideal height of a staircase step as
defined by the Federal Authorities of the Swiss Confederation. The subjects performed
ten repetitions for each of the three walking conditions, resulting in a total of 30 trials
per person. To prevent task familiarization within each condition, the target(s) appeared
in two possible positions separated medio-laterally by 8 cm (Figure 5.3 d), an adaptation
to the protocol based on the results of Young and Hollands [15]. Prior to the start of
each trial subjects stood with their back against the walking path facing a wall to limit the
amount of attention towards the pathway during the adjustments of the target position

Chapter Five
122
by the investigator. After a light cue, triggered by the investigator, subjects turned towards
the walking path and began to walk from a labeled starting position over the path at
a self-selected pace. Subjects were verbally instructed prior to each change of walking
condition to place their foot as accurately as possible in the middle of the target area
and were allowed to perform two rehearsal walks for each condition. The presentation
of the target positions was randomized and of equal number for each condition. The
presentation of the walking conditions was not randomized.
To assess participants‘ foot placement performance into the targets, adhesive
labels were placed on both shoes on calcaneus level for anterior-posterior (A-P)
distance assessment and on the level of the head of the fifth metatarsal for medio-
lateral (M-L) assessment (Figure 5.3 e). During each trial the targets were recorded by
two stationary video cameras (Contour HD 1080p) at a sampling rate of 30 Hz. A fixed
image of the foot‘s stance phase into the target was then read into the analyzing
software (Vicon Motus 9.2, Vicon Motion Systems, Oxford, UK). The foam targets were
previously marked with two triangles (Figure 5.3 e), serving as calibration points to
read in the dimensions and to determine spatial orientation of the target by the video
analysis software.
The main outcome of the FPA test was the M-L and A-P deviation in mm of the
foot center to the center of the foam target. Further, walking velocity between T1
and T2 and quality aspects of the performance during the FPA test were assessed. For
the quality evaluation the number and percentage of contacts of the leading or the
subsequent foot with the target, and the use of the wrong foot were assessed.
5.2.6.2. Gait analysis
Spatio-temporal gait parameters were assessed with GAITRite® Platinum Version 4.0
software and the GAITRite® electronic walkway (CIR Systems, Havertown, USA) with
a sampling rate of 60 Hz [42–44]. The GAITRite® with an active area of 7.92 meters
length was extended with two 2.5 meters carpets at the beginning and at the end to
eliminate the effects of acceleration or deceleration and to allow for steady state gait

Foot placement accuracy and gait
123
Figure 5.3 Set-up of the foot placement accuracy protocol. Subjects were required to walk along the pathway at self-selected pace and place the right foot into target 1 (Condition 1 (a)), place the right foot into target 1 and the left foot into target 2 (Condition 2 (b)), and additionally step over an obstacle lying between the two targets (Condition 3 (c)). The target(s) appeared in two possible positions separated medio-laterally by 8 cm to prevent task familiarization (d). Video still of camera 2 during stance phase used to evaluate the lateral and posterior distance error (e).
116 cm
184 cm
260 cm
a
b
c
target 1
target 2
foot marker
camera 1
camera 2
d e
light marker
midline
10cm2cm0
x
y
P = posterior distance
PL
L = lateral distance
xy
calibration point

Chapter Five
124
assessment. Subjects were instructed to walk over the electronic walkway under four different
conditions: at self- selected comfortable walking speed (normal) and at a fast walking speed
(fast, as fast as possible without running) each with or without a concurrent cognitive task
(normalcog and fastcog), respectively. The additional cognitive task consisted in counting out
loud backwards by steps of seven from a three-digit number given by the investigator at the
start of each trial. For each walking condition three trials were collected, resulting in twelve
walks per participant. Subjects were allowed to wear their everyday footwear.
The temporal-spatial parameters recorded were: velocity (cm/s), cadence (steps/min), step
time (s), cycle time (s), stance time (s), single support time (s), double support time (s), and
step length (cm). Relative dual task costs (DTC) of walking were calculated as percentage of
loss relative to the single task walking performance, according to the formula DTC [%] = 100
x (single task score – dual task score)/single task score [45]. The effective DTC changes were
defined as the mean difference between pre and post intervention (∆DTC).
5.2.6.3. Gaze behavior
ASL Mobile Eye, a head-mounted eye-tracking system (Applied Science Laboratories, Bedford,
USA) was used to assess gaze behavior during the FPA test. Based on the observation that
older adults prone to falling look away from a target location prior to heel contact on the floor
[7], the temporal-spatial gaze parameters were defined as: a) location of gaze at heel contact
(on/off target), b) the subsequent duration (milliseconds) of target fixation after heel contact,
or in case of a premature gaze shift c) the time elapsed between the early gaze shift away
from target and the heel contact (milliseconds). Gaze fixation was defined as a stabilization of
gaze in the environment for longer than 120 milliseconds [7]. The light cue, serving as a start
signal for the FPA test, was filmed by the eye-tracking camera and served as a marker for the
synchronization of the eye-tracking camera with the stationary cameras pointed towards the
targets.
5.2.6.4. Fear of falling
The Falls Efficacy Scale International (FES-I) questionnaire was used as a measure of concern

Foot placement accuracy and gait
125
about falling to determine the transfer effects of training to activities of daily living [46].
5.2.6.5. Statistical methods
A 75% attendance rate for the training sessions was set as the definition for being adherent
to the training program [47]. There were a total of 24 training sessions scheduled for each
individual in the study. Only those subjects who adhered to the training counted towards the
final results (per protocol analysis).
An average value of the M-L and A-P distance errors for each walking condition and target
in the FPA test, as well as for each spatio-temporal gait parameter of the gait analysis for
each walking condition, was calculated. Due to non-normality of the data a comparison at
baseline was undertaken using a Mann-Whitney U test. The Mann-Whitney U test was also
used to estimate group interaction effects (between-groups differences), after the twelve-
week training period. For this purpose the difference of the values pre and post intervention
for each subject were calculated and then compared. The effects size, r, was calculated as r =
Z/√N (where Z is the approximation of the observed difference in terms of the standard normal
distribution and N is the total number of samples; r = 0.1, small effect; r = 0.3, medium effect;
and r = 0.5, large effect). A Wilcoxon signed rank test was used to compare within-group pre/
post data. The significance level was set at p ≤ 0.05. A trend to significance was defined as 0.05
< p ≤ 0.10. Statistical computations were carried out with SPSS 19.
5.3 Results
A total of 22 participants (mean ± SD age: 86.2 ± 4.6 years) received the full allocated
intervention. Detailed information on subjects’ recruitment and reasons for loss are
presented in the flow chart (Figure 5.4). Table 5.1 shows demographic and clinical
characteristics of the sample. Eleven (50%) subjects were classified as having a high risk for
falling based on the presence of at least four of eight possible risk factors according to di
Fabio et al. [48]. No significant differences at baseline, neither in demographic nor in the
outcome measurements, were observed between the groups. No subject manifested a
severe impairment of vision.

Chapter Five
126
An average exercise compliance of 90.6% (21.7 out of 24 sessions) was observed. The DG
showed a compliance of 94.7% (22.7 out of 24 sessions) whereas the CG visited 86.9% of the
exercise sessions (20.8 out of 24 sessions).
Figure 5.4 The Study Flow Chart
5.3.1 Foot placement accuracy
A summary of the FPA test is provided in Table 5.2. A more detailed illustration of the FPA
test data with the single target locations and conditions is provided in Table 5.3. The data of
17 participants were collected.
Between-group comparisons (all conditions and targets) resulted in no significant
differences of foot placement performance. Within-group comparison resulted in a
significant improvement in M-L foot placement performance (Z = -1.960, p = 0.05) in DG and
no changes in the CG.
The detailed results of the FPA test performance in A-P directions demonstrate an
increase in distance error for both the DG and CG. In Condition 3, for the CG even a significant
increase in A-P distance error from 8.34 to 18.75 mm was observed (Z = -2.100, p = 0.036).
Assessed for eligibility (n = 35)
Randomized (n = 31)
Allocated to Dance Group (n= 15)- Received full allocated intervention (n = 11)- Did not receive full allocated intervention (n = 4) Reasons: low exercise compliance (<75%) (n = 2), low motivation (n = 2)
Outcome Measurement: Walking (n = 11)- Losses for test: none
Outcome Measurement: Walking (n = 10)- Losses for test: (n = 1) Reason: low motivation
Outcome Measurement: Footplacement Accuracy (n = 8)- Losses for test (n = 3) Reason: reliant on walking device
Outcome Measurement: Footplacement Accuracy (n = 9)- Losses for test (n = 1) Reason: reliant on walking device
Allocated to Control Group (n= 16)- Received full allocated intervention (n = 11)- Did not receive full allocated intervention (n = 5) Reasons: low exercise compliance (<75%) (n = 2), stroke/death (n = 1), dizziness (n = 1), relocation (n = 1)
Excluded (n = 4)Reasons: Mini-Mental Status Examination Score < 22 points (n = 2), hernia inguinalis (n = 1), declined participation (n = 1)

Foot placement accuracy and gait
127
Median walking velocity during the FPA test significantly increased in the DG in ‘Condition 2’
from 53.0 to 62.0 cm/s (Z = -2.371, p = 0.018), and the between-group comparison revealed
significant differences in favor of the DG (U = -2.122, p = 0.034, r = 0.51).
Table 5.1 Demographic baseline data of participants
Group Dance group Control group
No. of participants 11 11
Age (mean, SD) 86.9, 5.1 85.6, 4.2
Sex (female/male) 8/3 10/1
Height in cm (mean, SD) 159.1, 10.0 154.5, 10.1
Weight in kg (mean, SD) 68.3, 14.3 58.8, 13.1
Mini-Mental Statusa (mean, SD) 27.2, 2.0 27.0, 2.6
Vision
Vision aid (n / %) 5 / 45.4 4 / 36.4
Visual acuityb [MAR] (high / low contrast) 0.48 / 0.66 0.53 / 0.67
Melbourne Edge Testc [dB] (mode, range) 19, 9-21 19, 5-24
Fall Risk factorsd (n / %)
Low BMI (< 23) 1 / 9 5 / 4
Slow walking speed (< 1.22 m/s) 11 / 100 11 / 100
Previous falls requiring medical attention none none
Falls in the last 6 months 1 / 9 3 / 27
3 or more prescription medications 7 / 64 10 / 91
Cardiovascular medications 11 / 100 10 / 91
Anti-Anxiety medication or sedatives 3 / 27 3 / 27
Medication for dizziness none 1 / 9
Categorized as ‘Faller’ 5 / 45 6 / 55
Notes: a Minimum score = 0, maximum score = 30 (higher scores indicate better cognitive functioning); b log10 of the minimum angle resolvable (MAR) in minutes of arc (-log10 (distance (3m)/lowest correct line)); c Minimum score = 1, maximum score = 24 (higher scores indicate better edge contrast sensitivity, 1dB = -10 log10); d Di Fabio et al 2001 [48]; A fall was defined as an event, which results in a person coming to rest on the ground or other lower level. Abbreviations: SD, standard deviation; arcmin, arcminute.

Chapter Five
128
Tabl
e 5.2
Resu
lts of
foot
plac
emen
t acc
urac
y
p betw
een
0.70
0.63
0.03
*
1.00
Notes
: Dist
ance
erro
r (ab
solut
e valu
es) a
nd w
alking
veloc
ity va
lues a
re di
splay
ed as
grou
p med
ians w
ith in
terq
uarti
le ra
nges
(q1;
q3) d
ue to
non-
norm
al dis
tribu
tion o
f dat
a. * S
ignifi
cant
with
in-gr
oup d
iffer
ence
s pre
-pos
t (p wi
thin ≤
0.0
5) ca
lculat
ed w
ith W
ilcox
on si
gned
rank
test.
Perce
ntag
e valu
es ar
e defi
ned a
s the
quot
ient b
etwe
en nu
mbe
r of c
onta
cts or
wro
ng fo
ot, re
spec
tively
, divi
ded b
y the
sum
of tr
ials o
f the
who
le gr
oup.
Abbr
eviat
ions:
p with
in, p-v
alue f
or w
ithin-
grou
p com
paris
on; p
betw
een, p
-valu
e for
betw
een-
grou
ps co
mpa
rison
.
p with
in
0.44
0.17
0.81
0.10
Cont
rol g
roup
(n=
9) Post
10.1
(8.7;
15.7)
24.4
(15.5
; 30.7
)
0.49 (
0.35;
0.58)
0.41 (
0.24;
0.64)
6 (1.3
)
10 (2
.2)
16 (3
.6)
2 (0.4
)
Pre
12.9
(9.9;
16.2)
21.7
(17.2
; 26.9
)
0.53 (
0.41;
0.68)
0.33 (
0.26;
0.60)
5 (1.1
)
21 (4
.7)
14 (3
.1)
5 (1.1
)
p with
in
0.05
*
0.33
0.02
*
0.31
Danc
e gro
up (n
=8)
Post
10.1
(8.8;
11.95
)
21.2
(15.1
; 28.7
)
0.62 (
0.57;
0.75)
0.47 (
0.45;
0.49)
3 (0.8
)
8 (2.0
)
14 (3
.5)
2 (0.5
)
Pre
13.4
(10.0
; 15.3
)
16.6
(14.9
; 29.2
)
0.53 (
0.45;
0.67)
0.42 (
0.34;
0.43)
11 (2
.8)
17 (4
.3)
16 (4
.0)
2 (0.5
)
Dist
ance
erro
rs [m
m]
Med
io-lat
eral
erro
r
Ante
rior-p
oste
rior e
rror
Wal
king
velo
city [
m/s]
Cond
ition
2
Cond
ition
3
Qual
ity ev
alua
tion
(n, %
)
Cont
act w
ith le
ading
foot
med
io-lat
eral
ante
rior-p
oste
rior
Cont
act w
ith su
bseq
uent
foot
Wro
ng fo
ot

Foot placement accuracy and gait
129
Tabl
e 5.3
Det
ailed
resu
lts of
foot
plac
emen
t acc
urac
y
p betw
een
0.77
0.15
1.00
0.39
0.29
0.21
0.63
0.77
0.63
0.56
Notes
: Valu
es ar
e disp
layed
as gr
oup m
edian
s with
inte
rqua
rtile
rang
es (q
1; q3
) due
to no
n-no
rmal
distri
butio
n of d
ata.
* Sign
ifica
nt w
ithin-
grou
p diff
eren
ces p
re-p
ost (
p with
in ≤ 0.
05) c
alcula
ted w
ith W
ilcox
on si
gned
rank
test;
°Tre
nd
to si
gnifi
canc
e (p wi
thin ≤
0.10
). Ab
brev
iation
s: p wi
thin, p
-valu
e for
with
in-gr
oup c
ompa
rison
; pbe
twee
n, p-v
alue f
or be
twee
n-gr
oups
com
paris
on; C
1, C2
, C3,
Cond
ition
1, 2,
and 3
; T1,
T2, T
arge
t 1 an
d 2.
p with
in
0.86
0.31
1.00
0.72
0.48
0.52
0.26
0.04
*
0.86
0.89
Cont
rol g
roup
(n=
9)
Post
10.92
(8.72
; 20.0
4)
13.71
(10.2
0; 17
.96)
8.27 (
6.78;
16.75
)
13.01
(8.37
; 2.08
)
9.16 (
6.78;
1.34)
21.40
(13.2
5; 34
.01)
23.55
(16.4
7; 30
.18)
18.75
(15.0
5; 26
.88)
24.97
(18.3
7; 31
.52)
14.97
(11.5
3; 20
.17)
Pre
12.96
(9.90
; 16.7
1)
11.72
(9.16
; 16.6
9)
11.00
(4.62
; 17.8
6)
12.52
(10.9
8; 20
.16)
9.62 (
3.16;
17.14
)
22.92
(17.2
2; 32
.28)
14.42
(10.2
1; 28
.49)
8.34 (
3.58;
23.23
)
18.60
(16.8
8; 34
.12)
19.84
(5.39
; 21.5
1)
p with
in
0.48
0.21
0.58
0.07°
0.16
0.58
0.58
0.26
0.67
0.40
Danc
e gro
up (n
=8)
Post
12.09
(8.95
; 17.6
3)
10.93
(8.92
; 12.5
2)
9.84 (
8.50;
15.09
)
9.93 (
5.65;
15.36
)
9.65 (
6.78;
10.93
)
19.59
(12.9
8; 26
.44)
22.32
(14.4
9; 31
.21)
27.86
(14.2
6; 39
.72)
21.17
(15.1
5; 26
.42)
18.52
(13.4
9; 29
.33)
Pre
15.00
(11.4
4; 17
.33)
12.27
(10.2
0; 14
.74)
10.42
(8.38
; 15.2
0)
13.51
(8.98
; 20.1
0)
12.97
(5.79
; 16.0
0)
19.82
(12.7
8; 29
.17)
17.76
(12.7
7; 29
.88)
16.80
(14.8
8; 26
.44)
22.85
(13.3
2; 28
.90)
16.56
(14.0
6; 27
.15)
Cond
ition
/Tar
get
Med
io-lat
eral
erro
r [m
m]
C1/T
1
C2/T
1
C3/T
1
C2/T
2
C3/T
2
Ante
rior-p
oste
rior e
rror [
mm
]
C1/T
1
C2/T
1
C3/T
1
C2/T
2
C3/T
2

Chapter Five
130
5.3.2 Gait analysis
The data of 21 subjects were collected for the gait analysis. The detailed results of the
spatio-temporal gait analysis are summarized in Tables 5.4 and 5.5. Significant between-
group differences where observed in the fastcog condition, where participants were
required to walk as fast as possible with a concurrent cognitive task. The DG showed a
significant increase in walking velocity (U = 26, p = 0.041, r = 0.45), and a decrease in
single support time (U = 24, p = 0.029, r = 0.48) compared to the CG. The within-group
comparison revealed significant walking performance improvements throughout all the
walking conditions for the DG. In contrast, in the CG improvements in walking performance
were only observable for the normal and normalcog conditions.
Table 5.5 summarizes the results of the DTC of walking analysis. Significant between-
group differences for ∆DTC were observed for the parameter single support time for
both normal (U = 27, p = 0.049, r = 0.43) and fast walking speed (U = 26, p = 0.041, r =
0.45). Further, in the DG the ∆DTC decreased throughout all parameters in both walking
conditions from pre to post intervention. In contrast the CG demonstrated an increase in
∆DTC values after the intervention when compared to baseline data.
5.3.3. Perceived fear of falling
The results of the FES-I questionnaire showed a reduction of concerns about falling in both
groups. In the DG the mean value (mean, SD) was lowered from 23.7 ± 6.4 to 21.8 ± 5.0 and in the
CG the mean value was reduced from 24.5 ± 4.2 to 19 ± 4.1. Between-group comparison after the
twelve-week regimen resulted in non-significant (U = 38, p = 0.134, r = 0.32) differences.
5.3.4. Gaze behavior
Substantial losses of participants for the analysis of the eye-tracking data were documented. From
the 17 participants who performed the FPA test only seven data sets were complete. Reasons for
the losses were mainly attributable to problems with the handling of the eye tracking system. For
the sake of completeness the gaze data is presented in Table 5.6 and not further referred to in
the following section.

Foot placement accuracy and gait
131
Tabl
e 5.4
Resu
lts of
spat
io-te
mpo
ral g
ait an
alysis
r 0.15
0.25
0.28
0.27
0.29
0.36+
0.25
0.08
0.06
0.03
0.01
0.01
0.02
0.09
0.05
0.13
Notes
: Valu
es ar
e disp
layed
as gr
oup m
edian
s with
inte
rqua
rtile
rang
es (q
1; q3
) due
to no
n-no
rmal
distri
butio
n of d
ata.
* Sign
ifica
nt w
ithin-
grou
p diff
eren
ces p
re-p
ost (
p with
in ≤
0.05
) calc
ulate
d with
Wilc
oxon
sign
ed ra
nk te
st; ° T
rend
to
sign
ifica
nce (
p with
in ≤
0.10
), * S
ignifi
cant
betw
een-
grou
p diff
eren
ces a
fter in
terv
entio
n pha
se (p
betw
een ≤
0.05
) calc
ulate
d with
Man
n-W
hitne
y U-te
st, ° T
rend
to si
gnifi
canc
e (p be
twee
n ≤ 0.
10).
Abbr
eviat
ions:
p with
in, p-v
alue f
or in
ner-g
roup
com
paris
on; p
betw
een,
p-va
lue fo
r bet
ween
-gro
ups c
ompa
rison
; r, e
ffect
size (
r = 0.
1: sm
all ef
fect,
+r=
0.3:
med
ium ef
fect);
norm
al, se
lf-se
lecte
d walk
ing sp
eed;
fast,
fast
walki
ng.
p betw
een
0.481
0.260
0.205
0.217
0.191
0.095
°
0.259
0.725
0.778
0.888
0.972
0.972
0.944
0.669
0.804
0.549
p with
in
0.059
°
0.02
2*
0.02
2*
0.02
2*
0.03
7*
0.01
3*
0.04
7*
0.203
0.285
0.203
0.139
0.139
0.169
0.169
0.203
0.575
Cont
rol G
roup
(n=
10) Po
st
82.2
(73.8
; 101
.8)
104.2
(89.9
; 112
.3)
0.58 (
0.54;
0.67)
1.15 (
1.07;
1.34)
0.75 (
0.70;
0.92)
0.39 (
0.36;
0.43)
0.36 (
0.32;
0.49)
48.8
(46.0
; 54.9
)
114.7
(99.6
; 136
.8)
126.0
(105
.7; 13
5.7)
0.48 (
0.44;
0.57)
0.96 (
0.88;
1.13)
0.60 (
0.55;
0.74)
0.36 (
0.33;
0.38)
0.24 (
0.22;
0.34)
55.3
(50.4
; 62.6
)
Pre
69.0
(61.1
; 82.7
)
93.9
(80.2
; 99.9
)
0.64 (
0.60;
0.75)
1.28 (
1.20;
1.49)
0.86 (
0.78;
1.03)
0.43 (
0.41;
0.47)
0.44 (
0.37;
0.56)
46.6
(43.7
; 52.2
)
112.1
(99.0
; 124
.0)
118.2
(106
.0; 12
9.1)
0.51 (
0.46;
0.57)
1.02 (
0.93;
1.13)
0.65 (
0.61;
0.72)
0.38 (
0.33;
0.39)
0.30 (
0.25;
0.32)
56.0
(52.1
; 61.0
)
p with
in
0.248
0.01
6*
0.01
6*
0.01
6*
0.02
1*
0.04
1*
0.062
°
0.477
0.091
°
0.03
3*
0.05
0*
0.062
0.04
1*
0.110
0.131
0.594
Danc
e Gro
up (n
=11
) Post
88.3
(69.2
; 106
.2)
97.5
(96.0
; 111
.8)
0.62 (
0.54;
0.63)
1.23 (
1.07;
1.24)
0.78 (
0.72;
0.84)
0.41 (
0.36;
0.43)
0.37 (
0.31;
0.43)
52.7
(42.6
; 56.3
)
132.7
(93.2
; 149
.8)
127.1
(118
.2; 13
4.5)
0.47 (
0.45;
0.51)
0.94 (
0.89;
1.02)
0.60 (
0.57;
0.66)
0.35 (
0.32;
0.39)
0.26 (
0.22;
0.31)
59.2
(50.5
; 69.8
)
Pre
80.4
(72.9
; 89.1
)
95.5
(93.3
; 102
.5)
1.26 (
1.17;
1.29)
0.63 (
0.59;
0.64)
0.82 (
0.80;
0.86)
0.42 (
0.39;
0.44)
0.41 (
0.38;
0.43)
50.7
(45.7
; 53.0
)
124.7
(89.9
; 147
.4)
122.6
(113
.8; 12
8.7)
0.49 (
0.47;
0.53)
0.98 (
0.93;
1.05)
0.62 (
0.58;
071)
0.37 (
0.34;
0.38)
0.25 (
0.23,
0.33)
58.4
(53.1
; 66.7
)
Cond
ition
/Par
amet
ers
norm
al
Veloc
ity [c
m/s]
Cade
nce [
steps
/min]
Step
tim
e [s]
Cycle
tim
e [s]
Stan
ce ti
me [
s]
Single
supp
ort t
ime [
s]
Doub
le su
ppor
t tim
e [s]
Step
leng
th [c
m]
fast Ve
locity
[cm
/s]
Cade
nce [
steps
/min]
Step
tim
e [s]
Cycle
tim
e [s]
Stan
ce ti
me [
s]
Single
supp
ort t
ime [
s]
Doub
le su
ppor
t tim
e [s]
Step
leng
th [c
m]

Chapter Five
132
Tabl
e 5.4
Resu
lts of
spat
io-te
mpo
ral g
ait an
alysis
(con
tinue
d)
r 0.09
0.15
0.03
0.12
0.09
0.26
0.03
0.07
0.45+
0.42+
0.41+
0.37+
0.34+
0.48+
0.25
0.22
Notes
: Valu
es ar
e disp
layed
as gr
oup m
edian
s with
inte
rqua
rtile
rang
es (q
1; q3
) due
to no
n-no
rmal
distri
butio
n of d
ata.
* Sign
ifica
nt w
ithin-
grou
p diff
eren
ces p
re-p
ost (
p with
in ≤ 0.
05) c
alcula
ted w
ith W
ilcox
on si
gned
rank
test;
° Tre
nd
to si
gnifi
canc
e (p wi
thin
≤ 0.
10),
* Sign
ifica
nt be
twee
n-gr
oup d
iffer
ence
s afte
r inte
rven
tion p
hase
(pbe
twee
n ≤ 0.
05) c
alcula
ted w
ith M
ann-
Whit
ney U
-test,
° Tre
nd to
sign
ifica
nce (
p betw
een ≤
0.10
). Ab
brev
iation
s: p wi
thin, p
-valu
e for
inne
r-gro
up co
mpa
rison
; pbe
twee
n, p-v
alue f
or be
twee
n-gr
oups
com
paris
on; r
, effe
ct siz
e (r =
0.1:
small
effec
t, +r=
0.3:
med
ium ef
fect);
norm
al, se
lf-se
lecte
d walk
ing sp
eed;
fast,
fast
walki
ng; n
orm
al-co
g, se
lf-se
lecte
d walk
ing sp
eed w
ith ad
dition
al co
gniti
ve ta
sk; fa
stcog
, fast
walki
ng sp
eed w
ith ad
dition
al co
gniti
ve ta
sk.
p betw
een
0.673
0.481
0.888
0.573
0.672
0.228
0.888
0.751
0.04
1*
0.057
°
0.062
°
0.091
°
0.121
0.02
9*
0.260
0.324
p with
in
0.02
8*
0.139
0.074
°
0.093
°
0.059
°
0.445
0.059
°
0.059
°
0.386
0.445
0.799
0.799
0.721
0.799
0.646
0.333
Cont
rol G
roup
(n=
10) Po
st
63.2
(55.8
; 84.4
)
96.8
(74.5
; 103
.6)
0.62 (
0.58;
0.81)
1.24 (
1.16;
1.61)
0.81 (
0.79;
1.08)
0.43 (
0.38;
0.50)
0.43 (
0.39;
0.59)
46.3
(38.1
; 54.6
)
87.1
(59.0
; 103
.2)
104.1
(76.7
; 114
.1)
0.58 (
0.53;
0.78)
1.15 (
1.05;
1.57)
0.76 (
0.70;
1.03)
0.39 (
0.37;
0.50)
0.38 (
0.31;
0.51)
51.2
(38.6
; 60.0
)
Pre
60.0
(51.7
; 71.8
)
82.7
(73.9
; 100
.9)
0.73 (
0.60;
0.84)
1.46 (
1.19;
1.64)
1.00 (
0.78;
1.15)
0.46 (
0.40;
0.48)
0.55 (
0.39;
0.67)
43.4
(37.5
; 52.4
)
80.1
(61.0
; 100
.0)
91.8
(88.0
; 108
.8)
0.65 (
0.55;
0.68)
1.31 (
1.10;
1.37)
0.86 (
0.72;
0.93)
0.42 (
0.38,
0.46)
0.39 (
0.35;
0.51)
50.7
(41.2
; 57.8
)
p with
in
0.05
0*
0.02
6*
0.01
3*
0.01
3*
0.01
0*
0.01
3*
0.01
6*
0.13
1
0.01
3*
0.00
6*
0.00
6*
0.00
6*
0.00
8*
0.00
6*
0.01
3*
0.110
Danc
e Gro
up (n
=11
) Post
82.8
(60.0
; 97.9
)
101.0
(97.2
; 103
.3)
0.60 (
0.58;
0.62)
1.19 (
1.17;
1.24)
0.79 (
0.75;
0.83)
0.41 (
0.39;
0.44)
0.39 (
0.35;
0.41)
50.5
(44.3
; 56.6
)
107.5
(74.1
; 115
.6)
109.7
(101
.7; 11
7.4)
0.55 (
0.51,
0.59)
1.09 (
1.02;
1.19)
0.71 (
0.64;
0.78)
0.38 (
0.37;
0.41)
0.32 (
0.28;
0.37)
55.2
(44.8
; 62.6
)
Pre
65.4
(57.3
; 87.4
)
87.0
(82.4
, 93.8
)
0.69 (
0.64;
0.73)
1.39 (
1.28;
1.45)
0.94 (
0.85;
0.99)
0.45 (
0.43;
0.47)
0.48 (
0.41;
0.55)
46.73
(40.3
; 51.1
)
87.9
(68.6
; 103
.2)
99.1
(94.8
; 105
.5)
0.61 (
0.57;
0.63)
1.21 (
1.14;
1.26)
0.78 (
0.71,
0.84)
0.43 (
0.39;
0.43)
0.38 (
0.32;
0.40)
53.0
(44.2
; 58.8
)
Cond
ition
/Par
amet
ers
norm
alco
g
Veloc
ity [c
m/s]
Cade
nce [
steps
/min]
Step
tim
e [s]
Cycle
tim
e [s]
Stan
ce ti
me [
s]
Single
supp
ort t
ime [
s]
Doub
le su
ppor
t tim
e [s]
Step
leng
th [c
m]
fastc
og
Veloc
ity [c
m/s]
Cade
nce [
steps
/min]
Step
tim
e [s]
Cycle
tim
e [s]
Stan
ce ti
me [
s]
Single
supp
ort t
ime [
s]
Doub
le su
ppor
t tim
e [s]
Step
leng
th [c
m]

Foot placement accuracy and gait
133
Table 5.5 Results of dual task costs of walking analysis
Condition/ParametersDance Group (n=11) Control Group (n=10)
ΔDTC % pwithin ΔDTC % pwithin pbetween r
Normal walking speed
Velocity - 8.22 0.16 + 0.90 0.96 0.29 0.23
Cadence - 4.92 0.13 + 2.85 0.80 0.15 0.32+
Step time - 5.80 0.09° + 2.00 0.88 0.25 0.27
Cycle time - 5.68 0.09° + 3.01 0.88 0.18 0.29
Stance time - 6.69 0.11 + 1.93 0.96 0.23 0.26
Single support time - 3.60 0.06° + 5.38 0.20 0.05* 0.43+
Double support time - 9.51 0.18 - 4.75 0.80 0.62 0.11
Step length - 3.54 0.21 - 2.52 0.65 0.86 0.04
Fast walking speed
Velocity - 7.07 0.04* - 3.05 0.88 0.29 0.23
Cadence - 4.35 0.09° + 0.62 0.72 0.16 0.31+
Step time - 6.27 0.08° + 5.03 0.58 0.16 0.31+
Cycle time - 6.02 0.08° + 4.74 0.58 0.16 0.31+
Stance time - 7.29 0.08° + 5.36 0.58 0.16 0.31+
Single support time - 3.51 0.21 + 4.18 0.51 0.04* 0.45+
Double support time - 13.42 0.03* + 9.23 0.33 0.18 0.29
Step length - 3.73 0.02* - 2.92 0.72 0.83 0.05
Notes: Dual task costs are illustrated as the percentage of the mean difference between pre and post intervention (ΔDTC %), negative values repre-sent a reduction of DTC, positive values represent an increase in DTC. * Significant within-group differences pre-post (pwithin ≤ 0.05) calculated with Wilcoxon signed rank test, ° Trend to significance (pwithin ≤ 0.10), * Significant between-group differences after intervention phase (pbetween ≤ 0.05) calculated with Mann-Whitney U-test, ° Trend to significance (pbetween ≤ 0.10). Abbreviations: pwithin, p-value for within-group comparison; pbetween, p-value for between-groups comparison; r, effect size (r = 0.1, small effect, +r= 0.3, medium effect).
5.4. Discussion
This randomized controlled trial was designed to test whether a twelve-week strength and
balance exercise regimen, that includes a dance video game as an additional cognitive
element, would lead to greater changes in measures of gait performance and fear of
falling, compared to strength and balance exercise alone. Although both groups attained
improvements in gait performance and were able to reduce their concerns about falling,
the results suggest positive interaction effects in favor of the dance video game group.
The finding of this study supports the notion that it is advantageous to combine physical
and cognitive training into clinical practice. The combination seems to have a positive

Chapter Five
134
Tabl
e 5.6
Resu
lts of
gaze
beha
vior a
ssessm
ent d
uring
FPA t
est
Gaze
on ta
rget
at h
eel c
onta
ct [%
] Pre
/ Po
st
C3
83 /
81
55 /
64
0 / 10
0
85 /
75
38 /
95
37 /
100
100 /
n.d.
Notes
: 1 acco
rding
to D
i Fab
io et
al 20
01 [4
8]; n
egat
ive fix
ation
value
s cor
resp
ond t
o pre
mat
ure g
aze s
hift f
rom
the t
arge
t prio
r to h
eel c
onta
ct, i.e
. tim
e fro
m ga
ze sh
ift to
heel
cont
act;
posit
ive fix
ation
va
lues c
orre
spon
d to t
he ti
me o
f per
siste
nt fix
ation
on ta
rget
afte
r hee
l con
tact;
the v
alues
‘gaz
e on t
arge
t’ pro
vide i
nfor
mat
ion on
the l
ocat
ion of
gaze
at he
el co
ntac
t (10
0 % =
gaze
on ta
rget
on ev
ery
trial)
; Ab
brev
iation
s: CG
, con
trol g
roup
; DG,
danc
e gro
up; C
1-3,
Cond
ition
s 1-3
; T1-
2, Ta
rget
1-2;
n.d.,
no da
ta av
ailab
le.
C2
75 /
65
70 /
73
0 / 95
100 /
85
59 /
90
0 / 73
100 /
60
C1 80 /
0
50 /
63
0 / 10
0
80 /
100
30 /
100
0 / 10
0
13 /
11
Gaze
fixa
tion
[ms]
Pre /
Pros
t
C3 - T
2
90 /
74
416 /
232
-510
/ 29
2
276 /
132
-780
/ 22
0
-98 /
400
369 /
n.d.
C2 - T
2
40 /
20
472 /
n.d.
-314
/ 24
4
320 /
188
160 /
240
-293
/ 24
8
449 /
260
C3 - T
1
132 /
140
-72 /
24
-100
5 / 18
8
148 /
52
-122
5 / 12
4
-140
/ 33
0
216 /
n.d.
C2 - T
1
180 /
87
22 /
40
-675
/ 12
4
240 /
102
6 / 14
5
-395
/ 87
84 /
-18
C1 - T
1
164 /
-171
4 / 15
3
-820
/ 15
1
228 /
380
-172
/ 21
6
-692
/ 33
6
-347
/-61
3
Clas
sifica
tion1
faller
faller
non-
faller
non-
faller
non-
faller
non-
faller
faller
Grou
p
CG CG DG DG DG DG DG
Subj
ect
1 2 3 4 5 6 7

Foot placement accuracy and gait
135
influence on older adults walking abilities under dual task conditions in comparison to
more traditional exercise forms [17,18].
The most prominent differences between the training groups were observable in the
gait analysis. The CG demonstrated significant positive within-group changes of several
spatio- temporal parameters, however, merely in the single task condition and at preferred
gait speed (normal). Furthermore, this group exhibited a gain in velocity in the normalcog
condition. This merely confirms findings from a systematic review that a strength
and balance exercise regimen is able to preserve or improve walking abilities, even in
advanced age [49]. The goal of this study, however, was to improve walking behavior
under dual task conditions. The results of previous studies with similar groups, which
were performing progressive machine-driven resistance training complemented with
functional balance exercises, revealed no improvement of performance under attention-
demanding circumstances; e.g. no changes in the dual task costs of walking [50,51]. Daily
activities pose high cognitive demands and safe walking should be practicable also under
cognitive distractive or otherwise challenging conditions. The results of the DG show
significant positive within-group differences for most gait parameters also in the dual task
conditions normalcog and fastcog, thus confirming findings from previous pilot studies
with similar results for dual task related costs [27,30]. Furthermore, significant between-
group differences in the dual task condition fastcog were observed for gait velocity and
single support time in favor of the DG. Fastcog is the condition with the most challenging
motor and cognitive demands. In the present study the positive effect on DTC of gait,
represented by the decrease in ∆DTC values in the DG (Table 5.5), may be attributed to
the additional input provided by the dance video game. Thus, this substantiates the
hypothesis that an additional cognitive challenge should be preferably part of a training
program aiming to improve physical functioning in older adults, especially under dual
task conditions. Unfortunately, how gait under these conditions should be improved has
not yet been well-studied in general [52] and this study is one of the first that shows that
an improvement in dual task walking with an exercise intervention supplemented by a
video game is achievable.

Chapter Five
136
In the FPA test both groups revealed a more accurate foot placement in M-L direction
over all the walking conditions, however, only the DG manifested significant within-group
differences after the intervention. The better performance may be in part attributable to
improvements in walking and balance skills gained by the strength and balance exercises.
A higher postural balance confidence during swing phase of the gait cycle has possibly
enabled a more accurate targeting. However, a more efficient movement planning
and a possible change in visual scanning of the walking path have possibly led to the
better performance in the FPA test in favor of the DG. Interactive video games, like the
dance video game used in this study, require precise visuo-motor control, that is to focus
attention on the screen and the concurrent execution of controlled body movement and
the regulation of postural control.
Interestingly in this context is that expert action video game players were found to have
an improved spatial distribution and resolution of visual attention, a more efficient visual
attention over time and were able to attend a higher number of objects simultaneously
compared to non-players [53,54], thus allowing a better allocation of the attentional
resources over a visuo-motor task.
Interestingly, in both exercise groups the mean distance error in A-P direction
increased after the intervention. Participants were able to navigate quicker through the
test path thereby controlling their M-L direction walking deviation, however, suffered the
loss of accuracy in mean distance error in A-P direction. The higher inaccuracy in the A-P
direction may be in part explained by the higher walking velocity in the second test. It can
be suggested, that participants gave more priority to their walking performance (greater
velocity, larger steps) and their navigation towards the target in M-L direction, so that
their foot placement accuracy in A-P direction decreased (speed-accuracy tradeoff ) [55].
The quality evaluation, however, shows in general a qualitative better performance in the
second FPA test with less shoe contacts with the targets (Table 5.2).
The reason to use a dance video game or video games in general, is mainly based
on the findings of a systematic review [17]. It is, however, also related to the numerous
advantages attributed to such a tool [25]. As known from the principles of motor learning,

Foot placement accuracy and gait
137
repetition is important for both motor learning and the cortical changes that initiate it
[56]. The repeated practice must be linked to incremental success at some task or goal.
A computerized intervention like the dance video game constitutes a powerful tool to
provide participant repetitive practice, feedback about performance and motivation to
endure practice [56]. In addition, it can be adapted based on the individual participant‘s
baseline motor performance and be progressively augmented in task difficulty. Further,
the addition of a challenging video game has the potential to engage people who
otherwise would lack of interest to participate in a physical exercise regimen. Especially
in the older population it is difficult to maintain high adherence to training programs
[57]. The participants of the present study showed excellent compliance rates. The losses
related to low exercise compliance or low motivation (n = 4) in the DG were caused by
animosities between the participants of one training group and in part by not perceiving
any changes in performance level at the half of the study. The reasons for discontinuation
of training were not because of rejection of the dance video game per se. The DG members
were motivated by the additional playing of the video game at the end of every training
session. The CG members were motivated by the assurance that after the end of the
intervention they had the opportunity to include the dance video game in their exercise
program as well. In both hostels, the training sessions with the additional dance video
game were pursued also after the study ended.
The high acceptance of the dance video game used in our study seems at variance with
reports of elderly being rather skeptical towards using commercially available games in
a hospital setting [58]. We think that this is partly explainable due to the modifications
made to the original dance video game free-ware StepMania. The information on the
screen was reduced to a minimum and the music was chosen according participants‘
taste. In general, commercially available video games are often not adapted to the
needs and preferences of older adults, since they are designed for children and young
adults. The games are not easy to comprehend and the screens are flashing. This might
be one of the reasons why some commercially available video games are rather disliked
by older adults [58].

Chapter Five
138
5.4.1. Limitations of the study
The present study contains some limitations that have to be discussed. A limitation of
the FPA test is that different shoe sizes of the participants are not accounted for. The
further development of the FPA test protocol should consider foot size by using different
sized foam targets. We assume that a subject with small feet has more free space in the
target area to place his/her foot before touching the border of the target resulting in a
potentially higher risk of becoming variable in the accuracy performance. On the other
hand the larger the foot the smaller the free space between foot and border of the target.
A subject with large feet will not have a comparable amount of potential variability of
distance errors as the person with small feet.
An obvious limitation of our study is the rather small sample size. This study, therefore,
only reveals first estimates for these measures and warrants further research in larger
populations. When evaluating the validity of a study it is important to consider both the
clinical and statistical significance of the findings [59]. Studies that claim clinical relevance
may lack sufficient statistical significance to make meaningful statements or, conversely,
may lack practicality despite showing a statistically significant difference in treatment
options. Researchers and clinicians should not focus on small p-values alone to decide
whether a treatment is clinically useful; it is necessary to also consider the magnitude(s)
of treatment differences and the power of the study [59]. Encouraging in this context is
the observation that the majority of the between-groups comparisons show medium or
medium-to-high magnitude(s) of treatment differences. This in mind, the relationship
between physical and cognitive training research and its effect on gait in elderly individuals
requires further exploration. Future adequately powered studies with similar populations
should, therefore, be performed to substantiate our assumption and findings.
The suggested link between the observed improvement in the physical tests after the
intervention and influences on cognitive processes in the brain is as of yet still speculative. A
necessary next step would be to investigate the isolated effects of the video game on measures
of cognitive functioning. Since improvements were observable in physical performance under
attention-demanding circumstances it seems plausible to hypothesize that these changes

Foot placement accuracy and gait
139
may rely, at least in part, on functional or even structural changes in the brain. A recently
published study protocol [60] might be able to provide some insights on this topic.
5.5. Conclusions
Our results support previous larger studies that strength and balance exercise may lead to better
walking performance in older untrained subjects. Integrating a cognitive training component
in addition, results in further improvements in those walking tasks that are related to cognitive
functions. Enhancements in walking performance under dual task conditions were observed
for the dance video game group only. Our findings suggest that the addition of this particular
program to traditional strength and balance exercises may result in improved outcomes for older
people. An exercise program that aims to improve physical functioning in older adults under
dual task conditions should also consider a cognitive challenging element, preferably in form of
an interactive video game adapted for older adults, in addition to strength and balance exercises.
Acknowledgements
We would like to acknowledge Manuela Nötzli, Melanie Ramp, Rosina Landolt and Susan
Brouwer for supervising the training sessions. We would also like to thank Marie-Louise
Sarraj and Gerhard Ineichen for giving us the opportunity to conduct the study in their
hostels in Stäfa and Rüti, Switzerland. Thanks also to Rolf van de Langenberg for his
creative ideas in answering technical questions.
Authors‘ contribution
Conception, design and manuscript drafting: GP, EDdB: Critical revision of manuscript for
its content and approval of final version: GP, EDdB, KM. All authors read and approved the
final manuscript.
Competing interests
The authors declare that they have no competing interests.
References

Chapter Five
140
1. Berg WP, Alessio HM, Mills EM, Tong C: Circumstances and consequences of falls in
independent community-dwelling older adults. Age Ageing 1997, 26(4):261-268.
2. Hausdorff JM, Rios DA, Edelberg HK: Gait variability and fall risk in community- living
older adults: a 1-year prospective study. Arch Phys Med Rehabil 2001, 82(8):1050- 1056.
3. Gill T, Taylor AW, Pengelly A: A population-based survey of factors relating to the
prevalence of falls in older people. Gerontology 2005, 51(5):340-345.
4. Blake AJ, Morgan K, Bendall MJ, Dallosso H, Ebrahim SB, Arie TH, Fentem PH, Bassey
EJ: Falls by elderly people at home: prevalence and associated factors. Age Ageing
1988, 17(6):365-372.
5. Rapp K, Becker C, Cameron ID, Konig HH, Buchele G: Epidemiology of falls in
residential aged care: analysis of more than 70,000 falls from residents of bavarian
nursing homes. J Am Med Dir Assoc 2012, 13(2):187. e181-186.
6. Chapman GJ, Hollands MA: Evidence for a link between changes to gaze behaviour
and risk of falling in older adults during adaptive locomotion. Gait and Posture 2006,
24(3):288-294.
7. Chapman GJ, Hollands MA: Evidence that older adult fallers prioritise the planning
of future stepping actions over the accurate execution of ongoing steps during
complex locomotor tasks. Gait Posture 2007, 26(1):59-67.
8. Hausdorff JM, Edelberg HK, Mitchell SL, Goldberger AL, Wei JY: Increased gait
unsteadiness in community-dwelling elderly fallers. Arch Phys Med Rehabil 1997,
78(3):278-283.
9. Laessoe U, Hoeck HC, Simonsen O, Voigt M: Residual attentional capacity amongst young
and elderly during dual and triple task walking. Hum Mov Sci 2008, 27(3):496- 512.
10. Chamberlin ME, Fulwider BD, Sanders SL, Medeiros JM: Does fear of falling influence
spatial and temporal gait parameters in elderly persons beyond changes associated
with normal aging? J Gerontol A Biol Sci Med Sci 2005, 60(9):1163-1167.
11. Alexander NB, Ashton-Miller JA, Giordani B, Guire K, Schultz AB: Age differences in
timed accurate stepping with increasing cognitive and visual demand: a walking trail
making test. J Gerontol A Biol Sci Med Sci 2005, 60(12):1558-1562.

Foot placement accuracy and gait
141
12. Neider MB, Gaspar JG, McCarley JS, Crowell JA, Kaczmarski H, Kramer AF: Walking and
talking: dual-task effects on street crossing behavior in older adults. Psychol Aging
2011, 26(2):260-268.
13. Bryan J, Luszcz MA: Measurement of executive function: considerations for detecting
adult age differences. J Clin Exp Neuropsychol 2000, 22(1):40-55.
14. Chapman GJ, Hollands MA: Age-related diffrences in visual sampling requirements
during adaptive locomotion. Exp Brain Res 2010, 204(3):467-78.
15. Young WR, Hollands MA: Can telling older adults where to look reduce falls? Evidence
for a causal link between inappropriate visual sampling and suboptimal stepping
performance. Exp Brain Res 2010, 204(1):103-113.
16. Anonymous: Guideline for the prevention of falls in older persons. American Geriatrics
Society, British Geriatrics Society, and American Academy of Orthopaedic Surgeons
Panel on Falls Prevention. J Am Geriatr Soc 2001, 49(5):664-672.
17. Pichierri G, Wolf P, Murer K, de Bruin ED: Cognitive and cognitive-motor interventions
affecting physical functioning: a systematic review. BMC Geriatr 2011, 11:29.
18. Segev-Jacubovski O, Herman T, Yogev-Seligmann G, Mirelman A, Giladi N, Hausdorff
JM: The interplay between gait, falls and cognition: can cognitive therapy reduce fall
risk? Expert Rev Neurother 2011, 11(7):1057-1075.
19. Rapport LJ, Hanks RA, Millis SR, Deshpande SA: Executive functioning and
predictors of falls in the rehabilitation setting. Arch Phys Med Rehabil 1998,
79(6):629- 633.
20. Scherder E, Eggermont L, Visscher C, Scheltens P, Swaab D: Understanding higher
level gait disturbances in mild dementia in order to improve rehabilitation: ‘Last in-
first out‘. Neurosci Biobehav Rev 2011, 35(3):699-714.
21. de Bruin ED, Schmidt A: Walking behaviour of healthy elderly: attention should be
paid. Behav Brain Funct 2010, 6:59.
22. Yan J, Zhou C: Effects of motor practice on cognitive disorders in older adults. Eur Rev
Aging Phys Act 2009, 6(2):67-74.
23. Zelinski EM, Reyes R: Cognitive benefits of computer games for older adults.

Chapter Five
142
Gerontechnology 2009, 8(1):220-235.
24. Jobe JB, Smith DM, Ball K, Tennstedt SL, Marsiske M, Willis SL, Rebok GW, Morris
JN, Helmers KF, Leveck MD, et al: ACTIVE: a cognitive intervention trial to promote
independence in older adults. Control Clin Trials 2001, 22(4):453-479.
25. de Bruin ED, Schoene D, Pichierri G, Smith ST: Use of virtual reality technique for the
training of motor control in the elderly. Some theoretical considerations. Z Gerontol
Geriatr 2010, 43(4):229-234.
26. Studenski S, Perera S, Hile E, Keller V, Spadola-Bogard J, Garcia J: Interactive video
dance games for healthy older adults. J Nutr Health Aging 2010, 14(10):850-852.
27. Pichierri G, Coppe A, Lorenzetti S, Murer K, de Bruin ED: The effect of a cognitive-
motor intervention on voluntary step execution under single and dual task conditions
in older adults: a randomized controlled pilot study. Clin Interv Aging 2012, 7:175-184.
28. Thabane L, Ma J, Chu R, Cheng J, Ismaila A, Rios LP, Robson R, Thabane M, Giangregorio
L, Goldsmith CH: A tutorial on pilot studies: the what, why and how. BMC medical
research methodology 2010, 10:1.
29. Smith ST, Sherrington C, Studenski S, Schoene D, Lord SR: A novel Dance Dance
Revolution (DDR) system for in-home training of stepping ability: basic parameters
of system use by older adults. Br J Sports Med 2011, 45(5):441-445.
30. de Bruin ED, Reith A, Dörflinger M, Murer K: Feasibility of Strength-Balance Training
Extended with Computer Game Dancing in Older People; Does it Affect Dual Task Costs
of Walking? J Nov Physiother 2011, 1(104). Accessible at http://www. omicsgroup.org/
journals/2165-7025/2165-7025-2161-2104.php?aid=3350.
31. Inzitari M, Greenlee A, Hess R, Perera S, Studenski SA: Attitudes of postmenopausal
women toward interactive video dance for exercise. J Womens Health (Larchmt) 2009,
18(8):1239-1243.
32. Folstein MF, Folstein SE, McHugh PR: Mini-mental state. A practical method for
grading the cognitive state of patients for the clinician. J Psychiatr Res 1975, 12(3):189-
198.
33. Kraemer WJ, Adams K, Cafarelli E, Dudley GA, Dooly C, Feigenbaum MS, Fleck SJ,

Foot placement accuracy and gait
143
Franklin B, Fry AC, Hoffman JR, et al: American College of Sports Medicine position
stand. Progression models in resistance training for healthy adults. Med Sci Sports
Exerc 2002, 34(2):364-380.
34. Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ,
Skinner JS: American College of Sports Medicine position stand. Exercise and physical
activity for older adults. Med Sci Sports Exerc 2009, 41(7):1510-1530.
35. Paterson DH, Jones GR, Rice CL: Ageing and physical activity: evidence to develop exercise
recommendations for older adults. Can J Public Health 2007, 98 (Suppl 2):S69- S108.
36. Estabrooks PA, Carron AV: Group cohesion in older adult exercisers: prediction and
intervention effects. J Behav Med 1999, 22(6):575-588.
37. Borg G: Borg‘s perceived exertion and pain scales. Champaign, IL: Human Kinetics; 1998.
38. de Bruin ED, Murer K: Effect of additional functional exercises on balance in elderly
people. Clin Rehabil 2007, 21(2):112-121.
39. O‘Keeffe K: Dancing Monkeys (Automated creation of step files for Dance
Dance Revolution). London: Imperial College; 2003. http://monketnet/files/
dancingmonkeys/ DancingMonkeyspdf Accessed May 31, 2012.
40. Lord SR, Clark RD, Webster IW: Visual acuity and contrast sensitivity in relation to falls
in an elderly population. Age Ageing 1991, 20(3):175-181.
41. Lord SR, Menz HB, Tiedemann A: A physiological profile approach to falls risk
assessment and prevention. Phys Ther 2003, 83(3):237-252.
42. Menz HB, Latt MD, Tiedemann A, Mun San Kwan M, Lord SR: Reliability of the GAITRite
walkway system for the quantification of temporo-spatial parameters of gait in
young and older people. Gait Posture 2004, 20(1):20-25.
43. Webster KE, Wittwer JE, Feller JA: Validity of the GAITRite walkway system for the
measurement of averaged and individual step parameters of gait. Gait Posture 2005,
22(4):317-321.
44. Kressig RW, Beauchet O: Guidelines for clinical applications of spatio-temporal gait
analysis in older adults. Aging Clin Exp Res 2006, 18(2):174-176.
45. Coppin AK, Shumway-Cook A, Saczynski JS, Patel KV, Ble A, Ferrucci L, Guralnik JM:

Chapter Five
144
Association of executive function and performance of dual-task physical tests among
older adults: analyses from the InChianti study. Age Ageing 2006, 35(6):619-624.
46. Yardley L, Beyer N, Hauer K, Kempen G, Piot-Ziegler C, Todd C: Development and
initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing 2005,
34(6):614-619.
47. Nyman SR, Victor CR: Older people‘s recruitment, sustained participation, and
adherence to falls prevention interventions in institutional settings: a supplement to
the Cochrane systematic review. Age Ageing 2011, 40(4):430-436.
48. Di Fabio RP, Emasithi A, Greany JF, Paul S: Suppression of the vertical vestibulo- ocular
reflex in older persons at risk of falling. Acta Otolaryngol 2001, 121(6):707-714.
49. Sherrington C, Whitney JC, Lord SR, Herbert RD, Cumming RG, Close JC: Effective
exercise for the prevention of falls: a systematic review and meta-analysis. J Am
Geriatr Soc 2008, 56(12):2234-2243.
50. Hartmann A, Murer K, de Bie RA, de Bruin ED: The effect of a training program
combined with augmented afferent feedback from the feet using shoe insoles on
gait performance and muscle power in older adults: a randomised controlled trial.
Disabil Rehabil 2010, 32(9):755-764.
51. Hartmann A, Murer K, de Bie RA, de Bruin ED: The effect of a foot gymnastic exercise
programme on gait performance in older adults: a randomised controlled trial.
Disabil Rehabil 2009, 31(25):2101-2110.
52. Yogev-Seligmann G, Hausdorff JM, Giladi N: The role of executive function and
attention in gait. Mov Disord 2008, 23(3):329-342. quiz 472.
53. Green CS, Bavelier D: Action video game modifies visual selective attention. Nature
2003, 423(6939):534-537.
54. Achtman RL, Green CS, Bavelier D: Video games as a tool to train visual skills. Restor
Neurol Neurosci 2008, 26(4-5):435-446.
55. Fitts PM: The information capacity of the human motor system in controlling the
amplitude of movement. J Exp Psychol 1954, 47(6):381-391.

Foot placement accuracy and gait
145
56. Holden MK: Virtual Environments for Motor Rehabilitation: Review. Cyberpsychol
Behav 2005, 8(3):187-211.
57. Yardley L, Donovan-Hall M, Francis K, Todd C: Attitudes and beliefs that predict older
people‘s intention to undertake strength and balance training. J Gerontol B Psychol
Sci Soc Sci 2007, 62(2):P119-P125.
58. Laver K, Ratcliffe J, George S, Burgess L, Crotty M: Is the Nintendo Wii Fit really
acceptable to older people? A discrete choice experiment. BMC Geriatr 2011, 11:64.
59. Bhardwaj SS, Camacho F, Derrow A, Fleischer AB Jr, Feldman SR: Statistical significance
and clinical relevance: the importance of power in clinical trials in dermatology. Arch
Dermatol 2004, 140(12):1520-1523.
60. Jovancevic J, Rosano C, Perera S, Erickson KI, Studenski S: A protocol for a randomized
clinical trial of interactive video dance: potential for effects on cognitive function.
BMC Geriatr 2012, 12(1):23.


Six
Assessment of the test-retest reliability of a foot placement accuracy protocol
in assisted-living older adults
Pichierri G1, Diener T1, Murer K1, de Bruin ED1
1Institute of Human Movement Sciences and Sport, ETH Zurich, Switzerland
published in Gait & Posture 38 (2013) 784–789.
Ch
ap
ter

148
Chapter Six
Abstract
Introduction: This study assessed the test-retest reliability of a foot placement accuracy
protocol in assisted-living elderly. The goal is to evaluate the execution of foot placement
performance with increasing complexity of the walking condition.
Methods: Twenty-five elderly (5 males, 20 females, 80.4 ± 8.6 years) were assessed by
one observer in two sessions with 48 hours as time interval between the measurements.
Participants walked at self-selected pace along a pathway with three different walking
conditions composed by two rectangular foam target locations and an obstacle on
the walking surface. The main outcome measures were foot placement distance error,
intraclass correlation coefficients (ICC), and the smallest detectable difference (SDD).
Results: Mean absolute values of the foot placement distance errors were 14.0 ± 4.5 mm for
medio-lateral deviation and 27.2 ± 2.1 mm for anterior-posterior deviation, respectively.
ICC values for test-retest reliability showed ‘fair to good’ to ‘excellent’ reliability across all
conditions with values ranging from 0.63 to 0.94. SDD values lie between 3.6 and 37.3 mm.
Conclusion: The protocol showed good reliability for test-retest measurements of foot
placement accuracy, thus making this protocol a reliable and location-independent tool
to assess performance of foot placement in elderly in assisted-living settings. In the future,
measurements with elderly fallers and non-fallers should be conducted to assess validity
of the protocol.
Keywords: test-retest, reliability, foot placement, elderly, video analysis

149
Assessment of the test-retest reliability
The majority of falls in the elderly occur during activities of postural transition such as
walking [1]. Controlled placement of the foot on the walking surface is essential for safe
walking, especially in challenging environments. Because increased stride- to-stride
variability [2] and decreased foot placement accuracy [3,4] are typical features of the
aging process, the elderly are at greater risk of tripping or falling.
Accurate positioning of the foot requires appropriate planning and execution of the
movement, as well as cognitive skills such as visual scanning, attention and problem solving
[5]. It has been demonstrated that elderly people that are prone to falling generally show
greater foot placement variability compared to younger adults [3]. The elderly apparently
need more time to plan accurate steps into a target due to longer eye fixation times on
the target compared to younger adults [4]. In the past there have been some attempts
to assess foot placement accuracy in elderly populations [5–8], however these have not
included quantification of the performance. Foot placement accuracy performance was
defined by whether or not the participant stepped onto a target area on the floor [5–7], or
by measuring the foot placement accuracy error in the anterior-posterior (A-P) direction
only [8].
Chapman and Hollands [3,4] in contrast, designed a protocol that enabled the
assessment of foot placement accuracy in both A-P and medio-lateral (M-L) directions.
The goal of their protocol was to evaluate the planning and execution of foot placement
with increasing complexity of the walking condition. This foot placement protocol proved
to be able to discriminate between elderly with a low-risk and a high-risk for falling.
However, the use of this protocol is dependent on dedicated gait analysis infrastructure
and, therefore, restricted to gait analysis laboratories. Further, the time required to
complete the protocol limits the use of this protocol in clinical practice [9].
Critical to the further development of therapies and interventions are easy-to-use devices
that can be applied in clinical and (care) home settings [10]. Compared to other motion
measurement devices, digital cameras have the advantage of being lightweight and
portable, thus permitting data collection in a home environment. Consequently, they
seem ideal for extending our understanding of foot placement and gait, and the causes

150
Chapter Six
of elderly gait problems in real-life conditions, and ultimately facilitate the choice or the
development of appropriate physical treatment.
To be clinically useful, an assessment procedure must have a small measurement error
to detect a real change in an individual. A test-retest difference in a patient with a value
smaller than the standard error of the measurement (SEM) is likely to be the result of mea-
surement noise and is unlikely to be detected reliably in practice; a difference greater
than the smallest detectable difference (SDD) is highly likely (with 95% confidence) to
be a real difference [11].
We conducted this study to investigate the reliability of a foot placement accuracy
protocol in an assisted-living elderly population with mobile equipment, to identify
the SEM, and the SDD. To the best of our knowledge no evaluation of reliability of the
foot placement protocol in assisted-living settings has been published so far.
6.2. Methods
6.2.1. Study design
This study was designed as a test-retest study where all subjects were tested by the
same observer. Two trials were executed on two different days with 48 h between
the measurements. The study protocol was approved by the local ethics committee.
All participants received written and oral information and were requested to sign an
informed consent statement.
6.2.2. Subjects recruitment
Letters with an explanation of the study process and its aims were sent to the residents
of two senior hostels (total: 155). 31 residents (20%) evinced interest and were
assessed for eligibility. Inclusion criteria were age over 65 years, residential status, the
ability to walk independently for at least 10 m. Exclusion criteria were severe cognitive
impairments (Mini-Mental Status Examination Score (MMSE) < 22 points), rapidly
progressive or terminal illness, acute illness or presence of an unstable chronic illness.
6.2.3. Test procedures

151
Assessment of the test-retest reliability
The protocol used to assess foot placement accuracy was a modification of
a previously described protocol [4,12]. Subjects were instructed to walk at self-
selected pace along a path with three different obstacle conditions (Figure 6.1 a–c):
‘Condition 1’ (C1) required subjects to place their right foot onto target 1 (T1); in
‘Condition 2’(C2) subjects were required to place their right foot onto T1 and the
left foot onto target 2 (T2); ‘Condition 3’ (C3) additionally required stepping over an
obstacle placed between the two targets. The targets and the obstacle were made
of soft foam material. The targets were rectangular (target area (TA): 190 mm × 415
mm) and comprised a raised border (40 mm × 40 mm × 40 mm). Dimensions of the
obstacle were 170 mm × 670 mm × 25 mm. 170 mm corresponds to the ideal height
of a staircase step as defined by the Federal Authorities of the Swiss Confederation.
Subjects performed ten repetitions for each walking condition, resulting in a total
of 30 trials per person. Compared to the original protocol the number of trials was
halved since we expected to have older participants with on average less optimal
physical abilities compared to the elderly in the reference studies [4,12].
Prior to the start of each trial subjects stood with their back to the walking path,
facing a wall, to limit knowledge of the pathway during adjustments of the target
position by the investigator. The target(s) appeared in two possible positions (A or B)
separated medio-laterally by 8 cm (Figure 6.1 d), an adaptation to the protocol based
on the results of Young and Hollands [12]. The presentation of the target positions
was randomized and of equal number for each condition. The presentation of the
walking conditions was not randomized.
After a verbal signal by the supervisor, subjects turned toward the pathway.
From a labeled starting position they began to walk over the path at a self-selected
pace. Subjects were verbally instructed prior to each change of walking condition to
place their foot as accurately as possible in the middle of the TA and were allowed to
perform two rehearsal walks for each condition.

152
Chapter Six
6.2.4. Data acquisition
To assess participants’ foot placement performance on the targets, adhesive labels
were placed on both shoes at calcaneus level for A-P estimation and on the level of
the head of the fifth metatarsal for M-L estimation (Figure 6.1 e). During each trial, the
targets were recorded by two stationary video cameras (Contour HD 1080p, chosen for
shooting sharp, high resolution 1080p HD video) at a sampling rate of 30 Hz. Video data was
analyzed with Vicon Motus (Version 9.2) with an accuracy of 4.30 mm (A-P)/ 1.12 mm (M-L),
and a precision of 3.39 mm (A-P)/0.87 mm (M-L), respectively. Short video sequences (4
to 5 frames) of the heel strike moment onto the target were imported into the software
(Figure 6.1 e).
First, the spatial coordinates of the TA were determined for spatial calibration. Following
this, four reference points (P0–P3) were selected, where P0 represents the point of origin. P1
and P3 represent the extension of the medial and frontal boarder of the target, respectively.
Second, the M-L and A-P distance of the foot markers to the previously defined
coordinates of the TA were calculated by the software. Finally, for the assessment of foot
placement performance, the M-L and A-P deviation of the foot center to the center of the
foam target was determined. For this purpose, the contour of the participants’ shoe sole
were traced on a sheet of paper, thus allowing identification of the foot center, which was
defined as the midpoint between heel and toe for A-P error and the midpoint between the
lateral marker and the proximal shoe border for M-L error. The foam targets were marked
with two black triangles (Figure 6.1 e), serving as calibration points to read in the dimensions
and to determine spatial orientation of the target by the video analysis software. The shape
of a triangle was chosen to facilitate identification and marking of the calibration points on
the video file.
6.2.5. Statistical analysis
The mean M-L and A-P absolute distance errors of the foot center to the target center
were calculated for each target under each condition. Normality of the data was analyzed
with the one sample Kolmogorov-Smirnov test.

153
Assessment of the test-retest reliability
Figure 6.1. Set-up of the foot placement accuracy protocol. Subjects were required to walk along the pathway at self-selected pace and place the right foot into target 1 (Condition 1 (a)), place the right foot into target 1 and the left foot into target 2 (Condition 2 (b)), and additionally step over an obstacle lying between the two targets (Condition 3 (c)). The target(s) appeared in two possible positions (A or B) separated medio-laterally by 8 cm to prevent task familiarization (d). Video still of camera 2 during stance phase used to evaluate the lateral (la) and posterior (po) distance error (e).
116 cm
184 cm
260 cm
a
b
c
target 1
target 2
foot marker
camera 1
camera 2
d e
target 2target 1
midli
ne
10cm2cm0x
y
po = posterior distance
pola
la = lateral distance
xy= calibration points P0
P1
P2
P3
A B
A B

154
Chapter Six
Heteroscedasticity of the data was assessed by calculating the square value of Pearson’s
correlation coefficient (r2) between the absolute measurement differences (measurement
1 – measurement 2) and the respective means. Values of r2 above 0.1 indicate
heteroscedasticity. Negative values or values below 0.1 indicate homoscedasticity.
Bland-Altman plots were created for the visual inspection of heteroscedasticity
[13,14]. If heteroscedasticity was present, data was transformed to the logarithms of
base 10 for the calculation of the reliability parameters [15]. For the relative measures of
test-retest reliability the two-way random intraclass correlation coefficients (ICC2,k) with
absolute agreement were calculated. 95% confidence intervals (95% CI) for each target
and condition were determined. The interpretation of the ICC2,k values was based on the
benchmarks suggested by Shrout and Fleiss (>0.75 excellent reliability, 0.4–0.75 fair to
good reliability, <0.4 poor reliability) [16].
To examine if a significant systematic bias existed between the test and retest and
as needed for the subsequent calculation of the absolute indices of reliability a two-
way analysis of variance (ANOVA) was performed [17]. SEM was estimated with: SEM
= SD√1 – ICC2,k) where SD is the standard deviation of the scores from all subjects
(determined from the ANOVA: √SStotal /(n – 1)) and ICC2,k is the reliability coefficient.
SStotal is the total sum of squares derived from the ANOVA. SDD was calculated with
the formula SDD = SEM x 1.96 x √2 [18]. All statistical analyses were performed with SPSS
Statistics 19. Significance level was set at α = 0.05 (2-tailed).
6.3. Results
25 subjects were recruited and signed informed consent statements. The participants’
characteristics are summarized in Table 6.1. 25 subjects, with a mean age of 80.4 years
(range 66 to 94 years), completed both measurements. From the thirty subjects who
evinced interest to participate, four were excluded for not meeting the inclusion criteria
(walking device (n = 2), MMSE score < 22 (n = 1) or too frail (n = 1)) and one person declined
to participate after the first measurement.
Data sets for A-P distance error for T1 in C1, M-L distance error for T1 in C3, and A-P

155
Assessment of the test-retest reliability
distance error for T2 in C2 were heteroscedastic and were log-transformed to base 10 for
calculation of the reliability parameters.
Mean absolute values and ranges of both measurements, their mean difference
with corresponding limits of agreement and 95% CI, and the results of the ANOVA are
reported in Table 6.2. Data for A-P distance error for T1 in C3 (p = 0.04) and for M-L distance
errors for T2 in C2 (p = 0.05) revealed significant differences between the measurements.
Mean absolute values of the foot placement distance errors combining all experimental
conditions and both measurements were 14.0 ± 4.5 mm for M-L deviation and 27.2 ± 2.1
mm for A-P deviation, respectively.
The results of the reliability measures and agreement parameters are shown in
Table 6.3. ICC2,k values show ‘fair to good’ to ‘excellent’ reliability results across all
conditions with values ranging from ICC2,k 0.63 to 0.94. SDD values lie between 3.6
and 37.3 mm. In proportion to the size of the TA, the SDD values range from 1.9% (3.6
mm) to 7.0% (13.3 mm) for M-L distance error, and from 0.87% (3.6 mm) to 9.0% (37.3
mm) for A-P distance error. The Bland-Altman plots are presented in Figure 6.2.
Table 6.1 Demographic data of participantsNo. of participants 25
Age (mean, range) 80.4, 66–94
Sex (female/male) 20/5
Height (m) (mean, range) 1.61, 1.37–1.78
Weight (kg) (mean, range) 67.0, 47.1–92.7
Mini-Mental statusa (median, range) 28, 24–30
FES-Ib (median, range) 17, 16–24
Walking assistance (cane) n (%) 3 (12%)
Fallsc in the last 6 months n (%)
One 7 (28%)
More than one 2 (8%)
Previous falls requiring medical attention 1
Hypertension n (%) 13 (52%)
Arthropathy n (%) 8 (32%)
Osteoporosis n (%) 4 (16%)
Diabetes n (%) 4 (16%)
Cardiac insufficiency n (%) 3 (12%)a Minimum score = 0, maximum score = 30; higher scores indicate better cognitive functioning.b FES-I: falls efficacy scale-international; minimum score = 16, maximum score = 64; lower scores indicate less fear of falling.c A fall was defined as an event, which results in a person coming to rest on the ground or other lower level.

156
Chapter Six
Tabl
e 6. 2
Dist
ance
erro
rs (fo
ot ce
nter
to ta
rget
cent
er),
mea
n diff
eren
ce d,
and A
NOVA
value
s (sa
mple
size
n =
25)
ANOV
A
p 0.53
0.26
0.49
0.89
0.05
*
0.71
0.71
0.04
*
0.69
0.92
Abbr
eviat
ions:
Cond
ition
1: on
e tar
get;
Cond
ition
2: tw
o tar
gets;
Cond
ition
3: tw
o tar
gets
plus o
bsta
cle; T
1, T2
: tar
get 1
or 2;
M-L
, A-P
: med
io-lat
eral
or an
terio
r–po
sterio
r dist
ance
erro
r of c
ente
r foo
t to
targ
et ce
nter
; d: d
iffer
ence
betw
een
the v
alue o
f mea
sure
men
t one
minu
s mea
sure
men
t two
; LoA
: lowe
r and
uppe
r lim
it of
agre
emen
t (d
± 1.
96 st
and d
eviat
ion of
d); 9
5% CI
: 95%
conf
idenc
e int
erva
l (lo
wer l
imit,
uppe
r lim
it).
F
0.401
1.333
0.494
0.019
4.272
0.139
0.145
4.583
0.162
0.010
Diffe
renc
e d 95%
CI of
d (m
m)
-3.2,
1.7
-0.5,
8.2
-3.5,
1.7
-3.3,
3.8
0.0, 4
.9
-1.8,
4.9
-2.5,
2.5
0.2, 9
.9
-1.4,
1.8
-7.1,
6.4
Mea
n (Lo
A) (m
m)
-0.7
(-12.2
, 10.7
)
3.8 (-
16.9,
24.6)
-0.9
(-13.3
, 11.6
)
0.2 (-
16.6,
17.1)
2.4 (-
9.1, 1
4.0)
1.5 (-
14.4,
17.5)
0.0 (-
11.9,
11.9)
5.0 (-
18.0,
28.0)
0.3 (-
7.0, 7
.6)
-0.3
(-32.4
, 31.8
)
Mea
sure
men
t 2
Mea
n (ra
nge)
(mm
)
13.5
(5.2,
27.3)
23.5
(9.0,
45.9)
14.1
(5.1,
41.5)
27.5
(1.2,
52.7)
14.0
(4.5,
51.3)
23.8
(8.4,
57.2)
14.3
(6.6,
49.3)
30.4
(8.2,
60.7)
13.6
(5.1,
42.2)
25.7
(0.8,
86.8)
Mea
sure
men
t 1
Mea
n (ra
nge)
(mm
)
12.8
(7.3,
30.6)
27.3
(7.6,
57.3)
13.2
(4.4,
41.2)
27.7
(8.2,
54.6)
16.4
(6.1,
44.7)
25.4
(9.7,
66.5)
14.3
(7.2,
33.1)
35.4
(0.3,
68.2)
13.9
(5.2,
36.0)
25.4
(2.1,
65.3)
Dire
ctio
n
M-L A-P
M-L A-P
M-L A-P
M-L A-P
M-L A-P
Targ
et
T1 T1 T1 T1 T2 T2 T1 T1 T2 T2
Cond
ition
1 1 2 2 2 2 3 3 3 3

157
Assessment of the test-retest reliability
0.5
1.0
1.5
2.0
2.5
3.0
-2.0
-1.00.0
1.0
2.0
Cond
ition
1, t
arge
t 1 (M
-L)
Mea
n la
tera
l dist
ance
[cm
]
Mean difference of lateral distance [cm]
+1.9
6 SD
-1.9
6 SD
mea
n
1.0
2.0
3.0
4.0
5.0
-2.0
-1.00.0
1.0
2.0
3.0
4.0
Mean difference of posterior distance [cm]
Cond
ition
1, t
arge
t 1 (A
-P)
Mea
n po
ster
ior d
istan
ce [
cm]
0.0
1.0
2.0
3.0
4.0
5.0
-2.0
-1.00.01.0
2.0
Mean difference of lateral distance [cm]
Mea
n la
tera
l dist
ance
[cm
]
Cond
ition
2, t
arge
t 1 (M
-L)
Mea
n po
ster
ior d
istan
ce [
cm]
Mean difference of posterior distance [cm]
1.0
2.0
3.0
4.0
5.0
6.0
-2.0
-1.00.0
1.0
2.0
Cond
ition
2, t
arge
t 1 (A
-P)
Mea
n la
tera
l dist
ance
[cm
]
Mean difference of lateral distance [cm]Co
nditi
on 3
, tar
get 1
(M-L
)
1.0
2.0
3.0
4.0
-2.0
-1.00.0
1.0
2.0
1.0
2.0
3.0
4.0
5.0
6.0
Mea
n po
ster
ior d
istan
ce [
cm]
Mean difference of posterior distance [cm]
Cond
ition
3, t
arge
t 1 (A
-P)
1.0
2.0
-1.0
-2.0
Figu
re 6
. 2 B
land-
Altm
an p
lots w
ith th
e mea
n lat
eral
/ pos
terio
r dist
ance
[cm
] plot
ted
again
st th
e cor
resp
ondin
g m
ean
differ
ence
bet
ween
mea
sure
men
t 1 an
d m
easu
rem
ent 2
[cm
]. M
ean
differ
ence
(d
otte
d line
s) an
d upp
er an
d low
er lim
its of
agre
emen
t (da
shed
lines
) are
show
n.

158
Chapter Six
Mea
n la
tera
l dis
tanc
e [c
m]
0.0
1.0
2.0
3.0
4.0
5.0
-1.5
-0.50.5
1.5
Mean difference of lateral distance [cm]C
ondi
tion
2, ta
rget
2 (M
-L)
Mea
n po
ster
ior d
ista
nce
[cm
]1.
02.
03.
04.
05.
06.
07.
0
Mean difference of posterior distance [cm] -2.5
-1.5
-0.50.5
1.5
2.5
Con
ditio
n 2,
targ
et 2
(A-P
)
Mea
n la
tera
l dis
tanc
e [c
m]
Mean difference of lateral distance [cm]
0.0
1.0
2.0
3.0
4.0
-1.0
-0.5
0.0
0.5
1.0
Con
ditio
n 3,
targ
et 2
(M-L
)
Mea
n po
ster
ior d
ista
nce
[cm
]
Mean difference of posterior distance [cm]
1.0
2.0
3.0
4.0
5.0
6.0
-8.0
-6.0
-4.0
-2.0
0.0
2.0
4.0
Con
ditio
n 3,
targ
et 2
(A-P
)
Figu
re 6
. 2 (c
ontin
ued)
Blan
d-Al
tman
plot
s with
the m
ean l
ater
al / p
oste
rior d
istan
ce [c
m] p
lotte
d aga
inst t
he co
rresp
ondin
g mea
n diff
eren
ce be
twee
n mea
sure
men
t 1 an
d mea
sure
men
t 2 [c
m].
Mea
n dif
feren
ce (d
otte
d line
s) an
d upp
er an
d low
er lim
its of
agre
emen
t (da
shed
lines
) are
show
n.

159
Assessment of the test-retest reliability
Table 6.3 Reliability measures and agreement parameters (sample size n = 25)
Condition Target Direction
Reliabilitymeasures
Agreementparameters
ICC2,k
95% CIfor ICC2,k
SEM(mm)
SDD(mm)
1 T1 M-L 0.70 0.31, 0.87 4.7 13.0
1 T1 A-P 0.66 0.24, 0.85 1.7 4.8
2 T1 M-L 0.85 0.66, 0.93 4.8 13.3
2 T1 A-P 0.89 0.74, 0.95 6.3 17.5
2 T2 M-L 0.88 0.71, 0.95 4.7 13.0
2 T2 A-P 0.85 0.65, 0.93 1.3 3.6
3 T1 M-L 0.78 0.50, 0.90 1.3 3.6
3 T1 A-P 0.83 0.61, 0.93 9.5 26.4
3 T2 M-L 0.94 0.85, 0.97 2.7 7.4
3 T2 A-P 0.63 0.14, 0.84 13.4 37.3
Abbreviations: Condition 1: one target; Condition 2: two targets; Condition 3: two targets plus obstacle; T1 & T2: target 1 or 2; M-L & A-P: medio-lateral or anterior-posterior distance error of foot center to target center; ICC2,k: intraclass correlation coefficient (two-way random with absolute agreement); SEM: standard error of measurements in mm; SDD: smallest detectable difference in mm.
6.4. Discussion
The purpose of this study was to determine the test–retest reliability of the
modified foot placement accuracy test with mobile equipment applied with a
healthy elderly population in assisted-living settings. The results show ‘fair to
good’ to ‘excellent’ reliability parameters, thus making this protocol a reliable tool
to assess performance of foot placement in healthy elderly people in assisted-
living settings.
Our study population was representative of a typical population in senior care
homes when the demographic variables are considered. A wide age range (66–94
years), high percentage of women (80%), and MMSE scores ranging from 24 to
30 points, that is from the edge to mild cognitive impairments to no cognitive
impairments. This indicates our results can be generalized to comparable
populations of elderly people in clinical settings.

160
Chapter Six
In this study we used the ICC2,k with corresponding 95% CI to estimate relative
reliability. We observed prevalently ‘excellent’ ICC2,k values for C2 (ICC2,k = 0.85–0.89)
with narrow 95% CI values ranging from 0.65 to 0.95. In contrast C1 and C3 showed
ICC2,k values between ‘fair to good’ and ‘excellent’ (ICC2,k = 0.63–0.94) but wider ranges
of corresponding 95% CI (range from 0.14 to 0.97). Therefore it seems plausible to
assume that C2 is the more reproducible condition for elderly people.
The reason for these results could be that participants made use of C1 to acclimatize
to the test. This could be interpreted as a need for more rehearsal trials ahead of the
actual testing. C3 was more complex than C2 since participants were required to
decelerate, take a step over the obstacle and accelerate toward T2. Since the mean
age of our participants was 80.4 years it is plausible to think that C3 posed a more
challenging condition for some of the participants compared to others, explaining
the high variability of the results and the low reproducibility of the performance. It
could also be argued that some participants, especially the older ones, felt tired after
the first two conditions, which may have caused inaccuracies during walking. C2 on
the other hand, represented a more constant and rhythmical condition since it did not
require any changes in pace.
To detect relevant changes in performance of foot placement accuracy on an
individual level in clinical practice, the changes should exceed the SDD values
presented in Table 6.3. However, it is difficult to say whether the SDD values are
adequate to detect clinically meaningful differences on an individual level following
an intervention. At present the data used to categorize individuals as being at high-
risk for falls based on their foot placement accuracy, is poor and reported somewhat
contradictorily. Chapman and Hollands observed similar high values for foot placement
distance errors for both young adults and for elderly people prone to falling [3]. Their
values are in line with the values in our study over all test conditions. Interestingly,
elderly people with a low-risk for falls manifested lower values for distance errors,
which could be interpreted as a more accurate performance. In contrast, in the study
published in 2007, high-risk elderly people showed lower values for distance error

161
Assessment of the test-retest reliability
compared to both the low-risk and the young group [4]. This is one of the reasons why
further research should aim to acquire a broader collection of data in clinical settings.
One limitation of the protocol was that participants’ different foot sizes were not
accounted for. We assumed that a subject with smaller feet had more free space in the
TA to place his foot before touching the border, resulting in a potentially higher risk
of becoming variable in accuracy performance. On the other hand the larger the foot,
the smaller the free space between the foot and the border of the target. Therefore, a
subject with large feet may not have a comparable amount of variability in distance
errors as a person with smaller feet. A further development of the test protocol should
consider foot size by using different sized foam targets for instance. The small bias
from test to retest suggests learning effects of the protocol and can therefore be
considered as another limitation. Learning effects negatively influence reliability and
might be prevented by increasing the number of practice trials [19]. In frail elderly
people however, extensive testing might also cause systematic bias. A solution for this
problem might be the performance of several trials taken over several days in order
to control for learning effects. Furthermore, the occurrence of trial-to-trial learning
effects should be limited by a randomized presentation of the walking conditions.
6.5. Conclusion
This study showed good reliability for test–retest measurements of the foot placement
accuracy protocol, thus making this protocol a reliable and location-independent tool
to assess performance of foot placement in groups of elderly people in assisted-living
settings. However, the study should be repeated, taking into account the improvements
of the protocol as suggested in the limitations, and preferably with a sample of non-fallers
and frequent fallers to assess the ability to differentiate between these groups.

162
Chapter Six
Funding
No external funding.
Acknowledgements
Special thanks go to Gerhard Ineichen and Hans van het Reve for giving us the
opportunity to conduct this study in their hostels in Rüti and Feusisberg, Switzerland.
We also acknowledge Eva van het Reve’s and Rosina Landolt’s efforts for organizing the
measurements and for motivating the participants for this study.
Conflict of interest statement
The authors declare that they have no competing interests.

163
Assessment of the test-retest reliability
References
1 Berg WP, Alessio HM, Mills EM, Tong C. Circumstances and consequences of falls in
independent community-dwelling older adults. Age & Ageing. 1997; 26: 261-8.
2 Hausdorff JM, Edelberg HK, Mitchell SL, Goldberger AL, Wei JY. Increased gait
unsteadiness in community-dwelling elderly fallers. Archives of Physical Medicine &
Rehabilitation. 1997; 78: 278-83.
3 Chapman GJ and Hollands MA. Evidence for a link between changes to gaze
behaviour and risk of falling in older adults during adaptive locomotion. Gait &
Posture. 2006; 24: 288-294.
4 Chapman GJ and Hollands MA. Evidence that older adult fallers prioritise the
planning of future stepping actions over the accurate execution of ongoing steps
during complex locomotor tasks. Gait & Posture. 2007; 26: 59-67.
5 Alexander NB, Ashton-Miller JA, Giordani B, Guire K, Schultz AB. Age differences in
timed accurate stepping with increasing cognitive and visual demand: a walking trail
making test. Journals of Gerontology Series A-Biological Sciences & Medical Sciences.
2005; 60: 1558-62.
6 Yamada M, Higuchi T, Tanaka B, Nagai K, Uemura K, Aoyama T, Ichihashi N.
Measurements of stepping accuracy in a multitarget stepping task as a potential
indicator of fall risk in elderly individuals. Journals of Gerontology Series A-Biological
Sciences & Medical Sciences. 2011; 66: 994-1000.
7 Yamada M, Higuchi T, Mori S, Uemura K, Nagai K, Aoyama T, Ichihashi N. Maladaptive
turning and gaze behavior induces impaired stepping on multiple footfall targets
during gait in older individuals who are at high risk of falling. Archives of Gerontology
& Geriatrics. 2012; 54: e102-8.
8 Berg WP and Murdock LA. Age-related differences in locomotor targeting
performance under structural interference. Age & Ageing. 2011; 40: 324-9.
9 Simon SR. Quantification of human motion: gait analysis-benefits and limitations to
its application to clinical problems. J Biomech. 2004; 37: 1869-80.

164
Chapter Six
10 Wade E and Mataric MJ. Design and testing of lightweight inexpensive
motion-capture devices with application to clinical gait analysis in Pervasive
Computing Technologies for Healthcare, 2009. 3rd International Conference on
PervasiveHealth 2009. p. 1-7.
11 Hartmann A, Knols R, Murer K, de Bruin ED. Reproducibility of an isokinetic strength-
testing protocol of the knee and ankle in older adults. Gerontology. 2009; 55: 259-68.
12 Young WR and Hollands MA. Can telling older adults where to look reduce falls?
Evidence for a causal link between inappropriate visual sampling and suboptimal
stepping performance. Experimental Brain Research. 2010; 204: 103-13.
13 Bland JM and Altman DG. Statistical methods for assessing agreement between two
methods of clinical measurement. Lancet. 1986; 1: 307-10.
14 Ageberg E, Flenhagen J, Ljung J. Test-retest reliability of knee kinesthesia in healthy
adults. BMC Musculoskeletal Disorders. 2007; 8: 57.
15 Tabachnick BG and Fidell LS. Using multivariate statistics. California State University,
Northridge: Harper Collins College Publishers; 1996.
16 Shrout PE and Fleiss JL. Intraclass correlations: uses in assessing rater reliability.
Psychol Bull. 1979; 86: 420-8.
17 Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient
and the SEM. Journal of Strength & Conditioning Research. 2005; 19: 231-40.
18 de Bruin ED, Rozendal RH, Stussi E. Reliability of phase-velocity measurements of
tibial bone. Physical Therapy. 1998; 78: 1166-74.
19 Atkinson G and Nevill AM. Statistical methods for assessing measurement error
(reliability) in variables relevant to sports medicine. Sports Med. 1998; 26: 217-38.

165
Assessment of the test-retest reliability


Seven
General Discussion
Ch
ap
ter

168
Chapter Seven
Physical and cognitive decline are amongst the many factors that are thought to be
responsible for the increased fall risk in the older population. In the last few years the
awareness of the link between cognitive decline and the decline of physical functioning,
i.e. the decrease of walking abilities or impaired postural control, has given rise to novel
approaches for the prevention or reduction of the occurrence of falls in older adults.
In particular, cognitive decline that affects complex cognitive structures such as the
executive functions has been made responsible for the higher fall rate in older adults. The
many observations made in dual task experiments comparing younger with older adults
has led to the suggestion that a cognitive-motor approach should preferably be part of an
effective fall prevention training program.
This doctoral thesis discusses approaches that require consideration with a view to
including a stimulating cognitive factor to fall prevention training programs. Further, this
thesis aims to investigate the current state of research into using cognitive elements in
fall prevention or interventions with the aim of improving physical functioning in older
adults. Based on these findings, two intervention trials with a randomized controlled
study design that used a cognitive-motor approach with residents of four senior hostels in
Switzerland were performed. The objective of these studies was to examine the feasibility
and acceptance of the cognitive-motor approach, and to assess the benefits to the
participants of the cognitive-motor training program of including additional computer
game dancing in progressive strength and balance exercises, compared with those who
only received usual care or performed only strength and balance exercises. In this chapter
the main findings of the literature investigation and of the experiments are summarized
and discussed. In a second step methodological issues and clinical implications are
addressed. To conclude, future perspectives and conclusions are presented.
7.1. Main findings
7.1.1. The current use of cognitive-motor techniques for rehabilitation (Chapter 2 & 3)
There is limited current evidence on the effectiveness of cognitive or cognitive-motor
approaches on physical functioning with the objective of reducing the occurrence

169
General Discussion
of falls in older adults. The many pilot or case studies traced by the systematic review
(Chapter 3) clearly indicate that the use of cognitive or cognitive-motor approaches
to influence physical functioning in older adults is still in its fledgling state. Although
numerous studies have detected the dual task performance deficiency of older adults in
the past, surprisingly, there seems to be an inexistent practical use of dual task methods
in the context of intervention studies for rehabilitation purposes. The systematic review,
together with the conclusions of the theoretical discussion offered in Chapter 2, conclude
that approaches using computerized gaming techniques are the most convenient
methods to be used for the implementation of cognitive elements in a training program
with the aim of simulating a dual task condition. As early as the late 1990s, computerized
gaming techniques had begun to be developed and to be considered as a potential tool
for physical rehabilitation. Computerized gaming techniques were suggested to be able
to enhance the way older adults perceive their bodies within their environment, due to
the concordance of visual and proprioceptive information during training [1].
Computer games offer almost unlimited possibilities to implement into a training
program challenges that are close to reality. They provide scenarios that stimulate and
induce naturalistic movement and behaviors in a safe manner and they can be easily
shaped and adapted to the individual needs of the target subjects. Further, they provide
sufficient gaming experience to distract the subject’s attention from motor insecurities or
pain. To date the majority of the computer games for motor rehabilitation purposes are
found in the treatment and care of stroke patients, people with acquired brain injury, and
Parkinson’s disease sufferers [2, 3]. The aim of these studies in general is to rehabilitate
movements of upper and lower extremities that are important for activities of daily
life. With the help of computerized interventions the therapy sessions are motivating,
improvements in performance can be easily recorded and the level of difficulty can be
adjusted individually. The main finding of the systematic review is that to date there is
an insufficient application of cognitive or cognitive-motor interventions with the aim
of improving physical functioning. Further, computerized interventions for older adults
have to date seldom been applied or reported. Thus, the performance of experiments

170
Chapter Seven
and interventions using a cognitive or a cognitive-motor approach that uses interactive
computerized technologies is a justifiable and desirable objective.
7.1.2. The effects of a cognitive-motor intervention on voluntary step execution in
older adults (Chapter 4)
The execution of a timed voluntary stepping response is essential for tasks that demand
avoidance of a threat or recovery of balance during walking or whilst performing postural
transitions. It has been observed that individuals who require more time to initiate and
execute a step are at greater risk of falling [4–6]. In older adults the ability to execute a
quick step response further decreases in attention-demanding situations [7, 8].
The randomized controlled pilot study presented in Chapter 4 focused on the
evaluation of the effects of a twice-weekly exercise program enhanced by supplemental
computer game dancing for 12 weeks (n = 9) in comparison to usual care (n = 6) in older
adult residents of two senior hostels in the city of Zurich. Furthermore, the study examined
the feasibility and the potential to recruit and retain elderly subjects.
For the first time this intervention study revealed temporal improvements in voluntary
step execution under dual task conditions in older adults. The between-group comparison
resulted in a significant decrease of step initiation time (U = 9, p = 0.034, r = 0.55)
and step completion time (U = 10, p = 0.045, r = 0.52) in favor of the cognitive-
motor group. Additionally, the study participants showed an excellent mean compliance
rate of approximately 87%, thus substantiating the suggestion that a cognitive-motor
intervention that includes progressive strength and balance exercises supplemented by
an interactive dance video game is feasible and appreciated by older adults.
7.1.3. The effects of a cognitive-motor intervention on foot placement accuracy and
gait under dual task conditions and falls efficacy in older adults (Chapter 5)
Intact walking abilities are certainly one of the most important factors for the preservation
of autonomy and independence in everyday life. The accurate positioning of the foot onto
a footpath, for instance, is a crucial ability to ensure safe walking. It enables the avoidance of

171
General Discussion
missteps and the handling of potential threats to postural stability. Furthermore, reduced
gait abilities under attention-demanding conditions, and the slowing of usual gait velocity
are associated with a higher risk of falls and with a decline in attention and psychomotor
speed [9, 10]. It has even been suggested that improvements in usual gait velocity predict
a substantial reduction in mortality [11]. Both the decreased foot placement accuracy and
the general reduced walking abilities are often reported as common symptoms of the
natural aging process. In this regard, fear of falling is a frequently reported concern in
older adults, especially in individuals who have already experienced a fall, and can lead to
a further decrease in activity of daily life, a further decline in physical functioning and to a
general decrease in quality of life [12, 13].
Chapter 5 highlights the effects of a 12-week randomized controlled intervention
study of residents of two senior hostels regarding foot placement accuracy and gait under
dual task conditions, coupled with fear of falling. The participants either performed a
cognitive-motor program that comprised twice-weekly progressive strength and balance
exercises with supplemental computer game dancing (n = 15) or progressive strength
and balance exercises alone (n = 16). Although both groups attained improvements in
foot placement and gait performance and both were able to reduce their concerns about
falling, the results of this study suggest positive interaction effects in favor of the cognitive-
motor group. The cognitive-motor group achieved significant positive within-group
differences for most gait parameters assessed under both single and dual task conditions.
Furthermore, significant between-group differences for gait velocity (U = 26, p = 0.041,
r = 0.45) and single support time (U = 24, p = 0.029, r = 0.48) under dual task conditions
in favor of the cognitive-motor group were observed. However no significant between-
group differences were found for foot placement accuracy after the intervention − only
the cognitive-motor group exhibited significant positive within-group differences after
12 weeks. The results suggest that a cognitive-motor intervention may have a positive
influence on dual task walking abilities in older adults compared to a traditional exercises
regimen. The addition of a cognitive training component results in further improvements
in those walking tasks that are related to cognitive functions.

172
Chapter Seven
7.1.4. The test-retest reliability of the foot placement accuracy test (Chapter 6)
Knowledge of data reliability allows the use of a system in observational and interventional
type studies. The study presented in Chapter 6 assessed the test-retest reliability of a foot
placement accuracy protocol performed with mobile equipment in assisted-living elderly.
One observer assessed twenty-five elderly residents of two senior hostels in two sessions
with a 48-hour time interval between measurements. Participants walked at a self-
selected pace along a pathway with three different walking conditions composed of two
rectangular foam target locations and an obstacle on the walking surface. The analysis of
the foot placement performance was performed by the help of commercially available
digital video cameras and software able to identify the spatial position of objects and to
calculate relative distances to other objects based on video data. The results show ‘fair to
good’ to ‘excellent’ reliability parameters and SDD values in a small range, thus making
the foot placement accuracy test protocol a reliable tool to assess performance of foot
placement in healthy elderly in assisted-living settings.
However, it is difficult to say whether the SDD values are adequate to detect clinically
meaningful differences on an individual level following an intervention. Therefore, further
research should aim to acquire a broader collection of data, especially with groups of non-
fallers and frequent fallers, in clinical settings.
7.2. Methodological issues
7.2.1. Systematic review (Chapter 3)
Although the primary objective of the review was to identify intervention studies
using cognitive or cognitive-motor interventions affecting physical functioning in an
older population, studies including people with neurological deficits were considered
as a methodological supplement with the intention of receiving useful inputs for the
application in studies with older adults. People with neurological deficits as a cause of
brain dysfunctions behave very similarly to older adults, although the causes of the deficits
are different. Whether brain functions are lost through a sudden accident or through slow
and gradual decline, as it is in older adults, both result in more or less the same behavioral

173
General Discussion
symptoms and deficits, that is slowing of gait together with variability of temporal
and spatial gait parameters under single and dual task situations. The consideration of
other groups for the systematic literature search turned out to be fundamental for the
methodological content and the completeness of the review, since a majority of the
studies were conducted with older adults not in full health.
8.2.2. Randomized controlled pilot study (Chapter 4)
The small sample size definitely hinders the generalization of the results reported for the
pilot study presented in Chapter 4. Presumably, a larger sample size in both the cognitive-
motor and usual care group would have led to different results. The rationale for the
performance of this pilot study was purely scientific. Besides estimating possible effects
on physical functioning and the feasibility of a cognitive-motor approach the study was
concerned with the assessment of treatment safety, the determination of dose levels and
response. As Thabane, L. et al., stated [14]: “Pilot studies can be very informative, not only
to the researchers conducting them but also to others doing similar work. However, many
of them never get published, often because of the way the results are presented. Quite
often the emphasis is wrongly placed on statistical significance, not on feasibility – which
is the main focus of the pilot study.”
Certainly, an effective replication of the study should not only consider a larger number
of participants but also additional clinical meaningful measures of physical performance
such as the Expanded Timed Get-Up-and-Go test (ETGUG) [15], the Berg Balance Scale
[16], or the Activities-specific Balance Confidence Scale (ABC) [17]. These assessments may
contribute to a better and more comprehensible estimation of the effects observed on
the voluntary step execution task.
The comparison of the cognitive-motor group with a control group that received
only usual care is not recommendable by implication. It remains unclear whether
the positive results were a consequence of the additional dance computer game
alone, or of the cognitive-motor intervention as a whole. Therefore, the randomized
controlled study presented in Chapter 5 focused on separating the contribution of

174
Chapter Seven
the isolated training parameters, i.e. progressive strength and balance exercise and
interactive computer game dancing.
Nevertheless, the comparison reveals obvious deficiencies in the usual care
management in senior hostels. The two hostels considered for this pilot study lacked a
systematic physical exercise program as well as appropriate infrastructures to perform
physical activity for the resident older adults. This is a common problem in Swiss residential
settings [18].
7.2.3. Randomized controlled study (Chapter 5)
From the viewpoint of the assessments performed in the context of the study presented
in Chapter 5, some methodological issues need to be discussed. One major limitation
of the study is the absence of complete gaze behavior data during the foot placement
accuracy test. This substantial data deficiency makes it impossible to draw a relationship
between the improvements in the foot placement accuracy task and a possibly changed
gaze behavior as suggested by the reference studies [19–21]. Not only were technical
problems experienced, but also several age-related difficulties (vision problems) that
hampered the use of the eye-tracking system, thus bringing up the question whether
such an eye-tracking system is suitable for adults in this age category. In a future study
subjects who are not able to walk without glasses, subjects suffering from head tremor, or
those who have hanging eyelids should be excluded from the measurements.
Furthermore, some modifications in the foot placement accuracy test are necessary.
Participants were told to face a wall prior to the start of the test to prevent pre-walking
adjustments when aware of the targets’ medio-lateral position. After the visual start signal
appeared they performed a body turn of 180° towards the walking path. This body turn
could have been the origin of unwanted vestibular effects and may have influenced
the performance of the foot placement accuracy test. Nonetheless, as the time needed
to perform the body turn and perform the first step was not limited, the occurrence of
unwanted vestibular effects and its influence on performance can be disregarded. In
contrast, the participants in the reference studies [19–21] were told to close their eyes to

175
General Discussion
prevent catching a premature view of the walking path. Closing and opening the eyes may
also have an influence on the vestibular system, since participants begin to walk during
the light adaptation phase of the eye. A possible method of avoiding both unwanted pre-
start effects is the use of an easily removable wall on wheels between the participant and
the walking path.
From the viewpoint of the exercise program there is no need to change the design of
the cognitive-motor intervention used in this study. Participants very much enjoyed the
physical exercise as well as playing the dance video game. Some participants involved
in the performance of the dance video game suggested that the music could have been
more diversified, but this was reported as a minor issue. However, suggestions of this kind
should be taken seriously, since they may influence adherence to the training program
and the results of the study.
As in the pilot study offered in Chapter 4 the randomized controlled trial presented
in Chapter 5 showed small sample sizes although numerous residents attended the
recruitment events. For future studies the participant recruitment process should
be more focused on establishing a personal relationship between the investigators
and the residents of the senior hostels, right from the start. The support of the hostel
staff is therefore crucial, as they know the residents and are able to convince potential
participants in case of concerns about the participation to the study. The presentation of
videos and pictures of previous studies showing participants during the performance of
the training program is definitely helpful to provide confidence and assure that the study
is safe and especially designed for the older population. Having been more conscious of
these aspects possibly would have resulted in a larger study population.
7.2.4. The test-retest reliability study (Chapter 6)
The study that examined the test-retest reliability of the foot placement accuracy test
(Chapter 6) did not account for test to retest learning effects. To control for these learning
effects, the performance of several trials taken over several days is recommended. Further,
the trial-to-trial learning effects should be limited by a randomized presentation of the

176
Chapter Seven
walking conditions. As a matter of convenience the walking conditions were presented in
order of their complexity, i.e. one target, two targets, two targets with the obstacle.
7.2.5. Falls ascertainment
The fact that we did not ascertain falls after the intervention periods of both studies is a
point that needs to be discussed. Participants should be followed up for a certain period,
preferably 12 months, in order to assess the incidence of falls. In both intervention studies
only a retrospective data assemblage of falls data was performed. Participants were asked
how many times they had fallen in the last year or the last six months. Such an approach
is misleading because of failings in a participant’s memory of fall events over such a long
period of time. For future studies a prospective report of falls experiences should be
considered. This can be done by a self-reported bi-weekly or monthly falls diary, where
the participants report a fall event, its cause, and can note the environmental conditions
in which the fall happened. The accuracy of the fall reports increases when staff in senior
hostels are involved in the collection of falls data. Information on prospective falls data is
important to evaluate the long-term effects of an intervention.
7.3. Using computer games for older adults
The dance video game setting used in the context of this thesis is one possible approach to
using computerized methods. The advantage of using dance pads is that stepping on the
pad requires repetitive, well-coordinated leg movements and the regulation of postural
balance during the course of the training. The motivating component ‘music’ and the
performance of a step choreography on the dance pad in synchronization with music is
a complex sensorimotor action. Further, the continuous feedback on performance of the
dance computer game is very important for the participants since older adults may show
age-related deficits in self-monitoring [22, 23]. The feedback encourages the participants
to persevere with the game.
The most important aspect when using computer games for older adults is the
consideration of their preferences and needs for an aged-based adaptation of these games

177
General Discussion
[24]. This was shown by a recent study from Australia that investigated the acceptability of
a commercially available interactive video games as a therapeutic tool in health and aged
care settings [25]. The conclusion was that the usefulness of a commercially interactive
mainstream video game, in their case the Nintendo Wii Fit, is limited. Although the
Nintendo Wii Fit has become a popular tool in rehabilitation settings the applicability to
the older population is not warranted. Contemporary mainstream computer games are
designed for children or younger adults, they do not cope with the needs, interests and
abilities of older adults. The animation on the screen is colorful, blinking and overloaded
with information.
Computer games for older adults with the aim of improving physical functioning under
dual task conditions should focus on the stimulation of executive functions, especially on
divided attention and should preferably implement strength and balance exercises.
7.4. Clinical implications
Cognitive impairment should be regarded as one important point of future fall
prevention programs. Actual guidelines that prescribe adequate fall risk assessments
still do not propose the assessment of cognitive impairments for fall prevention. The
guidelines for the prevention of falls published by the American Geriatrics Society,
the British Geriatrics Society, and the American Academy of Orthopedic Surgeons
Panel on Falls Prevention propose the assessment of fall history, medication,
vision, gait and balance, lower limb joints, neurological (sensory neuron and
motor responses) and cardiovascular factors [26]. Although these assessments
cover a diversified list of potential fall risk factors, cognitive impairments such as
impaired executive functions, dementia, cognitive dysfunctions following traumatic
brain injuries or stroke are not considered. A complete fall risk assessment should
consider the cognitive domain. Cognitive tests for executive functions and the
assessment of physical performance, e.g. gait under dual task conditions, should be
considered in routine assessments for older adults. Many other researchers support
this suggestion [11, 27–29].

178
Chapter Seven
Progressive physical activity that comprises strength exercises focusing on muscle
groups that are used in everyday situations and the improvement of postural balance
enriched with a cognitive element should be part of any training program for older adults.
Thereby the aspect of group exercise is very important, especially in institutionalized
older adults where people tend to live their own lives regardless of the cohabitants. An
exercise program should be considered as a regular social event where people meet and
enjoy the common activity. The addition of a computer game such as the dance video
game used in the experiments in the context of this doctoral thesis integrates not only
physical activity and cognitive challenges but also offers emotional inputs to support
social cohesion between the inhabitants of a senior hostel.
When planning intervention studies for improving physical functioning in older adults
one should not be too cautious or blinded by too many prejudices. The perception that
computer games in general cannot be adapted to older adults' abilities and needs is fatal,
since aged people can be young at heart. Introducing a gaming effect and a healthy
portion of competition is important also in the old age. This could possibly be an argument
for higher participation rates in future studies. Low participation rates are a big problem in
exercise studies with older adults.
Further, the adequate design of computerized gaming techniques that focus on
improving physical functioning in older adults should be easily and economically
incorporated into home-based training programs without the need of any expensive and
unfamiliar settings.
7.5. Suggestions for future research
In a next step the effective contribution of the computer dance game on the
observed improvements in physical performance under dual task conditions
should be evaluated. The study would thus compare one group that performs
physical exercise alone, one group that performs the cognitive-motor program,
and a third group that performs only the computer dance game during the whole
study period of twelve weeks. Main outcome measures would be the assessment

179
General Discussion
of gait and of other relevant fall-related physical performances under dual task
conditions.
A model where cognitive stimuli are suggested to have an impact on physical
functioning could be examined. The question would be whether improvements in
gait under dual task conditions can be observed when the dance computer game is
played with a hand-held controller
(HC) only (Figure 7.1) instead of
whole-body step training (WBT) on
the original dance pad. The HC- and
WBT-group would exercise twice
weekly or more for 12 weeks. Main
outcome measures would be pre-
and post-tests of gait performance
or of other relevant fall-related
physical performances under dual task conditions. The hypothesis is that the WBT-
group will show better performances in dual task walking compared to the HC-group.
This would speak in favor of the suggestion that the cognitive and the motor element
have to be performed together. In case of improvements in dual task performance
of the HC-group after the purely cognitive training, such a design could possibly be
applied in the workout of rather frail older adults, who are not yet able to take part in
a WBT-training.
In fact, the dance computer game implies that participants are standing on the
dance pad for several minutes. Even with the help of the hanging ropes, this is an
ability that cannot be taken for granted for a great part of institutionalized older
adults. Unfortunately, some individuals interested in participating had to be excluded
from the training program, including those who required the use of a wheelchair, or
suffered from muscle weakness that restricted the ability to stand for such a long time,
or who just felt too insecure while standing without device support. An adaptation of
the training program specifically for this group of older adults that are overlooked
Figure 7. 1 Hand-held controller ( 20 x 20 x 60 cm)

180
Chapter Seven
in the majority of training studies should be designed. Strength and balance
exercises that can be performed in a seated position should be implemented. The
dance computer game could be performed by stepping on the dance pad in a sitting
position or by performing the game with the hands using an appropriately designed
hand controller constituting a miniature dance pad (Figure 7.1). This approach would
constitute a valuable opportunity for weaker and physically impaired older adults to
start with physical exercise in a safe manner. As main outcome measures in these
groups simple or choice reaction time of upper and lower extremities under dual task
conditions are suggested.
The next step should be the investigation of the dance computer game on a
neuropsychological level. It is still unclear what the underlying factors are that lead
to the improvements in physical functioning under dual task conditions in older
adults. We can only speculate that the dance computer game has an influence on
executive functions. However, first pilot findings suggest that interactive computer
dance gaming is associated with increased fronto-parietal network activation [30].
The further investigation of the dance computer game should focus on whether and
how the game stimulates and affects brain activity, with a focus on prefrontal brains
structures. Measurement of brain activity with electroencephalogy (EEG) during the
performance of the computer task or functional magnetic resonance imaging (fMRI)
before and after the cognitive-motor intervention could reveal which and to what
extent specific brain functions are active or affected during and after the performance
of the dance computer game. An interesting point would be to explore whether
the possibly observed changes in brain activity are achieved by structural and/or
functional changes in the brain. Three groups would be tested after a training regimen
of either computer game dancing, computer game dancing with a hand-held controller
(Figure 7.1), traditional stepping exercises and compared to a non-intervention group.
In addition, with the integration of the possibly new insights regarding the effect
of an interactive dance video game on brain level, new types of interactive computer
games especially designed and adapted for older adults should be developed.

181
General Discussion
7.6. Conclusions
This doctoral thesis highlights the fact that the use of cognitive-motor approaches
is still in its fledgling state, thus justifying the need for further research in the use
of cognitive-motor approaches for the improvement of physical functioning and
fall prevention in older adults. The suggested link between cognitive functions and
physical functioning should be taken into account in future studies aiming to improve
the ability of older adults to counteract threats to their postural stability. Furthermore,
cognitive impairments and decreased dual task performances in older adults should
be considered in routine assessments to identify at an early stage dysfunctions in this
context. The findings arising from the interventions performed in the experimental
context of this thesis substantiate the hypothesis that physical exercise enriched by
supplemental cognitive stimuli, in the form an interactive and attention-demanding
computer game, has an essential positive benefit on the physical performance
of older adults under attention-demanding circumstances when compared to
previously applied physical exercise regimen. However, it remains unclear to what
extent the additional cognitive input is responsible for the observed improvements
of performance.
To conclude, the design of future training approaches and interventional studies
should consider the needs, interests and abilities of the older population to ensure
adherence and persistence.

182
Chapter Seven
References
1. Bisson E, Contant B, Sveistrup H, Lajoie Y: Functional balance and dual-task
reaction times in older adults are improved by virtual reality and biofeedback
training. Cyberpsychol Behav 2007, 10(1):16-23.
2. Holden MK: Virtual environments for motor rehabilitation: review. Cyberpsychol
Behav 2005, 8(3):187-211; discussion 212-189.
3. Sveistrup H: Motor rehabilitation using virtual reality. J Neuroeng Rehabil 2004, 1(1):10.
4. Maki BE, McIlroy WE: Control of rapid limb movements for balance recovery: age-
related changes and implications for fall prevention. Age Ageing 2006, 35 Suppl
2:ii12-ii18.
5. Rapp K, Becker C, Cameron ID, Konig HH, Buchele G: Epidemiology of falls in
residential aged care: analysis of more than 70,000 falls from residents of
bavarian nursing homes. J Am Med Dir Assoc 2012, 13(2):187 e181-186.
6. Rogers MW, Kukulka CG, Brunt D, Cain TD, Hanke TA: The influence of stimulus cue
on the initiation of stepping in young and older adults. Arch Phys Med Rehabil
2001, 82(5):619-624.
7. Brauer SG, Woollacott M, Shumway-Cook A: The influence of a concurrent
cognitive task on the compensatory stepping response to a perturbation in
balance-impaired and healthy elders. Gait Posture 2002, 15(1):83-93.
8. Shumway-Cook A, Woollacott M: Attentional demands and postural control: the
effect of sensory context. J Gerontol A Biol Sci Med Sci 2000, 55(1):M10-16.
9. Montero-Odasso M, Verghese J, Beauchet O, Hausdorff JM: Gait and cognition:
a complementary approach to understanding brain function and the risk of
falling. J Am Geriatr Soc 2012, 60(11):2127-2136.
10. Inzitari M, Newman AB, Yaffe K, Boudreau R, de Rekeneire N, Shorr R, Harris TB,
Rosano C: Gait speed predicts decline in attention and psychomotor speed in
older adults: the health aging and body composition study. Neuroepidemiology
2007, 29(3-4):156-162.
11. Hardy SE, Perera S, Roumani YF, Chandler JM, Studenski SA: Improvement in

183
General Discussion
usual gait speed predicts better survival in older adults. J Am Geriatr Soc 2007,
55(11):1727-1734.
12. Howland J, Peterson EW, Levin WC, Fried L, Pordon D, Bak S: Fear of falling among
the community-dwelling elderly. J Aging Health 1993, 5(2):229-243.
13. Yardley L, Beyer N, Hauer K, Kempen G, Piot-Ziegler C, Todd C: Development and
initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing 2005,
34(6):614-619.
14. Thabane L, Ma J, Chu R, Cheng J, Ismaila A, Rios LP, Robson R, Thabane M,
Giangregorio L, Goldsmith CH: A tutorial on pilot studies: the what, why and
how. BMC Med Res Methodol 2010, 10:1.
15. Wall JC, Bell C, Campbell S, Davis J: The Timed Get-up-and-Go test revisited:
measurement of the component tasks. J Rehabil Res Dev 2000, 37(1):109-113.
16. Berg K, Wood-Dauphinee S, Williams JI: The Balance Scale: reliability assessment
with elderly residents and patients with an acute stroke. Scand J Rehabil Med
1995, 27(1):27-36.
17. Schott N: [German adaptation of the „Activities-Specific Balance Confidence
(ABC) scale“ for the assessment of falls-related self-efficacy. Z Gerontol Geriatr
2008, 41(6):475-485.
18. de Bruin ED, Spence JC, Hartmann M, Murer K: Physical Activity Recommendations and
Programmes Offered in Swiss Residential Settings. physioscience 2008, 4:154-162.
19. Chapman GJ, Hollands MA: Evidence for a link between changes to gaze
behaviour and risk of falling in older adults during adaptive locomotion. Gait
Posture 2006, 24(3):288-294.
20. Chapman GJ, Hollands MA: Evidence that older adult fallers prioritise the
planning of future stepping actions over the accurate execution of ongoing
steps during complex locomotor tasks. Gait Posture 2007, 26(1):59-67.
21. Young WR, Hollands MA: Can telling older adults where to look reduce falls?
Evidence for a causal link between inappropriate visual sampling and suboptimal
stepping performance. Exp Brain Res 2010, 204(1):103-113.

184
Chapter Seven
22. Dunlosky J, Kubat-Silman AK, Hertzog C: Training monitoring skills improves
older adults‘ self-paced associative learning. Psychol Aging 2003, 18(2):340-345.
23. Studer M: Rehabilitation of executive function: to err is human, to be aware-
divine. J Neurol Phys Ther 2007, 31(3):128-134.
24. Herman H, de Kort YAW, Ijsselsteijn WA: Senior gamers: Preferences, motivations
and needs. Gerontotechnology 2009, 8(4):247-262.
25. Laver K, Ratcliffe J, George S, Burgess L, Crotty M: Is the Nintendo Wii Fit really
acceptable to older people? A discrete choice experiment. BMC Geriatr 2011, 11:64.
26. Guideline for the prevention of falls in older persons. American Geriatrics Society,
British Geriatrics Society, and American Academy of Orthopaedic Surgeons
Panel on Falls Prevention. J Am Geriatr Soc 2001, 49(5):664-672.
27. Allali G, van der Meulen M, Assal F: Gait and cognition: the impact of executive
function. Schweizer Archiv für Neurologie und Psychiatrie 2010, 161(6):195-199.
28. Mirelman A, Herman T, Brozgol M, Dorfman M, Sprecher E, Schweiger A, Giladi N,
Hausdorff JM: Executive function and falls in older adults: new findings from a
five-year prospective study link fall risk to cognition. PLoS One 2012, 7(6):e40297.
29. Muir SW, Gopaul K, Montero Odasso MM: The role of cognitive impairment in
fall risk among older adults: a systematic review and meta-analysis. Age Ageing
2012, 41(3):299-308.
30. Jovancevic J, Rosano C, Perera S, Erickson KI, Studenski S: A protocol for a
randomized clinical trial of interactive video dance: potential for effects on
cognitive function. BMC Geriatr 2012, 12:23.

185
General Discussion


Eight
Summary / Zusammenfassung Danksagungen
PhD CurriculumCurriculum Vitae
Ch
ap
ter


Summary / Zusammenfassung

190
Chapter Eight
Summary
Our body is constantly challenged not only by different internal influences (muscle
weakness, illness, fatigue, mood, cognitive impairments, vision problems) but also by
external ones (obstacles, crowds, traffic, weather) all of which constitute a potential threat
to our postural stability. These demand intact cognitive functions to register potentially
threatening situations at an early stage, to plan and execute the correct motor response to
the special circumstance in order to avoid a misstep or a fall. Besides the decline of physical
functions, a decline of cognitive functions that regulate these abilities has been suggested
as a major cause for falls in the older population. It has been extensively observed that older
adults show poorer performances in dual task situations compared to younger adults, and
this deficiency is thought to be in part attributable to declines in executive functioning.
The thesis aims to answer the question of whether effective fall prevention programs
for older adults should implement approaches that address the cognitive decline and the
dysfunctions in cognitive processes, especially of the executive functions. The assumption
is based on the growing evidence that rather than isolated physical or cognitive activity, the
combination of both better supports the healthy functions of executive function, working
memory, and the ability to divide and select attention. The results of a systematic review
of literature (Chapter 3) reveal that the current evidence on the effectiveness of such
approaches on physical functioning under single and dual task conditions in older adults is
still limited, thus warranting the performance of experiments and interventions using such
a cognitive-motor approach for this population.
The thesis proposes the use of interactive computer games as a supplement to traditional
physical exercise procedures, that is strength and/or balance exercise. The special value of
interactive computer game training paradigms is believed to be due to the concordance
of visual and proprioceptive information during training. Further, interactive computer
games provide salient feedback about the movement performance and the task difficulty
can be easily adapted according to the subject’s ability and needs. The computer game
used in the experiments is an interactive dance game (a specially designed modification
of StepMania, Version 3.9) based on the performance of precise and timed steps on a metal

191
Summary / Zusammenfassung
pad in response to visual and acoustic stimuli. Subjects are expected to observe the virtual
environment on a screen indicating moving arrows and concurrently initiate appropriate
dance steps (forwards, backwards and to the side, respectively). The dance game challenges
body coordination and attention at the same time.
In two intervention studies (Chapter 4 and 5) older adults in care home settings in
Switzerland performed for twelve weeks either a cognitive-motor program that comprised
twice-weekly progressive strength and balance exercises with supplemental interactive
computer game dancing (dance group) or twice-weekly strength and balance exercise alone
(Chapter 5) or usual care offered a their homes (Chapter 4), respectively (control groups).
At baseline and after the intervention period of twelve weeks the groups were compared in
reference to their performance on walking (Chapter 4 and 5), their voluntary step execution
under single and dual task conditions (Chapter 4), and on their foot placement accuracy
during walking (Chapter 5). In both experiments the results revealed positive effects on
the performance of the tasks in favor of the dance group: a significant decrease of step
initiation time and step completion time in a voluntary step execution test under dual task
conditions (Chapter 4), a significant increase of gait velocity under dual task conditions,
and a significant positive within-group difference for foot placement accuracy in the dance
group (Chapter 5).
The findings arising from the interventions substantiate the hypothesis that physical
exercise enriched by an interactive and attention-demanding computer game can lead
to essential positive benefits in the physical performance of older adults under dual task
conditions when compared to traditional physical exercise. An exercise program that aims
to improve the physical performance under attention demanding circumstances should
consider a cognitively challenging element in addition to strength and balance exercise,
preferably in the form of an interactive computer game that is adapted to the participants’
abilities and needs. However, it still remains unclear to what extent the additional cognitive
input is responsible for the observed positive changes in physical performance in the
presented studies, which offers an incentive for further research on this topic.

192
Chapter Eight
Zusammenfassung
Unser Körper ist ständig sowohl mit inneren (Muskelschwäche, Erkrankungen, Müdigkeit,
Gemütslage, kognitive Beeinträchtigungen, Sehschwächen) als auch mit äusseren
Einflussfaktoren (Hindernisse, Menschenmassen, Strassenverkehr, Wetter) konfrontiert.
Diese Faktoren stellen eine potentielle Gefahr für die Erhaltung des Körpergleichgewichts
dar. Der Einfluss dieser Faktoren verlangt von unserem Körper intakte kognitive Funktionen
um so potentielle Gefahrensituationen frühzeitig erkennen und eine angemessene
motorische Antwort auf die speziellen Gegebenheiten planen und auszuführen zu können.
Nur so ist es möglich einen Fehltritt oder gar einen Sturz zu verhindern. Nebst dem
Rückgang der körperlichen Funktionen wird ein Rückgang der kognitiven Funktionen,
welche diese Fähigkeiten steuern, als eines der Hauptgründe für Stürze bei älteren
Menschen vermutet. Es wurde bereits nachgewiesen, dass ältere Menschen im Vergleich zu
jüngeren Erwachsenen eine beeinträchtigte Leistungsfähigkeit unter Dual-Task-Situationen
aufweisen. Es wird vermutet, dass diese Beeinträchtigung teilweise einem Rückgang der
exekutiven Funktionen zuzuschreiben ist.
Ziel dieser Dissertation ist es herauszufinden, ob effektive Programme zur Sturzprävention
bei älteren Menschen Methoden einsetzen sollten, welche den kognitiven Rückgang
aufhalten und auf die Beeinträchtigungen der kognitiven Prozesse, mit Schwerpunkt auf
den exekutiven Funktionen, eingehen. Diese Frage basiert auf die wachsende Anzahl
der Studienergebnisse, die darauf hinweisen, dass die Kombination von kognitiver und
motorischer Aktivität, gegenüber der rein isolierten Ausübung der beiden Aktivitäten die
exekutiven Funktionen, insbesondere das Arbeitsgedächtnis und die Fähigkeit der geteilten
und selektiven Aufmerksamkeit, stärker fördern. Die Ergebnisse der Literaturübersicht
(Kapitel 3) machen deutlich, dass das Wissen über die Wirkung der kognitiv-motorischen
Methoden auf die körperliche Leistungsfähigkeit unter Single- und Dual-Task-Bedingungen
bei älteren Menschen noch sehr gering ist, was die Durchführung von Experimenten und
Interventionen mit einem kognitiv-motorischen Charakter in dieser Population rechtfertigt.
Zur Ergänzung des traditionellen körperlichen Trainings (Kraft- und
Gleichgewichtsübungen) wird in dieser Dissertation der Einsatz von interaktiven

193
Summary / Zusammenfassung
Computerspielen vorgeschlagen. Der Einsatz dieser Spiele ist aufgrund des
Zusammenspiels zwischen visuellen und propriozeptiven Informationen während des
Trainings äusserst wertvoll. Die Spieler erhalten wertvolle Rückmeldungen zur Qualität der
Bewegungsausführung und der Schwierigkeitsgrad kann relativ einfach an die Fähigkeiten
und Bedürfnisse der Trainierende angepasst werden. Das Computerspiel, welches in den
Interventionen dieser Dissertation zu Verwendung kam, ist ein interaktives Computer-
Tanzspiel (eine speziell modifizierte Version von StepMania, Version 3.9), welches auf
die Ausführung von präzisen und zeitlich getimten Schrittfolgen auf einer metallischen
Tanzplatte, aufgrund visueller und akustischer Reize basiert. Der Spieler beobachtet die
virtuelle Umgebung auf einem Bildschirm, auf welchem sich Pfeile vom unteren zum
oberen Ende bewegen und führt gemäss der angezeigten Pfeilrichtung Tanzschritte aus
(vorwärts, rückwärts oder zur Seite). Das Computer-Tanzspiel fördert die Koordination
der Körperbewegungen und schult gleichzeitig aber auch die Fähigkeit der geteilten
Aufmerksamkeit.
In zwei Interventionsstudien (Kapitel 4 und 5) absolvierten Senioren aus Schweizer
Altersheimen ein 12-wöchiges kognitiv-motorisches Trainingsprogramm, welches zweimal
pro Woche progressives Kraft- und Gleichgewichtsübungen und zusätzlich interaktives
Computer-Tanztraining beinhaltete (Tanzgruppe). Die Senioren der Kontrollgruppen
hingegen, absolvierten entweder ein rein motorisches Programm mit Kraft- und
Gleichgewichtsübungen zweimal pro Woche (Kapitel 5) oder besuchten weiterhin die
in den Altersheimen angebotenen Aktivitätsprogramme (Kapitel 4). Vor Beginn und
nach Beendigung der 12-wöchigen Trainingsphase wurden die Gruppen jeweils auf
ihre Gehleistung (Kapitel 4 und 5), ihre Fähigkeit der willentlichen Ausführung eines
Schrittes unter Single- und Dual-Task-Bedingungen (Kapitel 4) und die Genauigkeit ihrer
Fussplatzierung beim Gehen (Kapitel 5) getestet und miteinander verglichen.
Die Resultate beider Interventionsstudien zeigten positive Effekte in der Ausführung
der körperlichen Tests zugunsten der Tanzgruppe. Es resultierten eine signifikante
Verminderung der Schrittinitiierungs- und Schrittausführungszeit bei der willentlichen
Ausführung eines Schrittes unter Dual-Task-Bedingungen (Kapitel 4), eine signifikante

194
Chapter Eight
Zunahme der Gehgeschwindigkeit unter Dual-Task-Bedingungen und eine signifikant
positive Veränderung der Genauigkeit der Fussplatzierung innerhalb der Tanzgruppe
(Kapitel 5).
Die Beobachtungen aus den beiden Interventionen bekräftigen die Hypothese, dass ein
körperliches Trainingsprogramm, welches durch ein interaktives und Aufmerksamkeit
förderndes Computerspiel im Vergleich zu traditionellem Training zu einem wichtigen
positiven Nutzen für die körperliche Leistungsfähigkeit von älteren Menschen unter Dual-
Task-Bedingungen führen kann. Ein Trainingsprogramm, welches zum Ziel hat die körperliche
Leistungsfähigkeit unter Aufmerksamkeit fördernden Bedingungen zu verbessern, sollte
ein zusätzliches kognitiv anspruchsvolles Element in die Kraft- und Gleichgewichtsübungen
integrieren. Dies idealerweise in Form eines interaktiven Computerspiels, welches auf die
Fähigkeiten und Bedürfnisse der älteren Menschen zugeschnitten ist. Allerdings bleibt noch
unklar in welchem Ausmass der zusätzliche kognitive Input für die beobachteten positiven
Veränderungen der körperlichen Leistungsfähigkeit der Teilnehmer in den vorgestellten
Studien verantwortlich ist, was eine Legitimation für weitere Forschung in diesem
Themengebiet ist.

195
Summary / Zusammenfassung


Danksagungen

198
Chapter Eight

199
Danksagungen
Viele Leute haben zum Gelingen dieser Dissertation beigetragen. Im Folgenden möchte
ich mich bei denjenigen Leuten bedanken, die mich während der Zeit meines Doktorats
am Institut für Bewegungswissenschaften und Sport der ETH Zürich begleitet,
unterstützt und die Zeit so angenehm gestaltet haben.
Ein besonderer Dank gilt meinem Betreuer PD Dr. Eling de Bruin. Ich möchte mich bei
Dir für die einzigartige Unterstützung bedanken. Du hattest immer ein offenes Ohr für
alle Arten von Fragen und Problemen, ganz besonders auch in der letzten Phase meiner
Arbeit, in der ich nicht mehr am Institut anwesend war. Auch hast Du mich immer
wieder mit Deinem unerschöpflichen Optimismus angesteckt wenn es darum ging
schwierigen Reviewern entgegenzutreten und eine passende Lösung zu finden. Danke
für die Ermöglichung an zahlreichen internationalen Kongressen teilzunehmen und
die Einbindung in das alljährliche MOBEX Meeting, welches mir ermöglicht hat, meine
ersten Schritte in der Präsentation der eigenen Resultate vor einem fachkundigen,
aber toleranten und hilfsbereiten Publikum zu vollführen. Danke auch für Deine
unkomplizierte Art, die es einem ermöglicht auch bei der Arbeit viel Spass zu haben
und nicht immer alles so ernst zu nehmen.
Beim Institutsleiter und meinem Co-Referenten Prof. Dr. Kurt Murer möchte ich mich
dafür bedanken, dass er mir die Möglichkeit gegeben hat, am IBWS meine Doktorarbeit
zu schreiben. Kurt, insbesondere möchte ich mich bei Dir bedanken, dass Du am
IBWS eine lockere, freundschaftliche und verständnisvolle Atmosphäre unter allen
Mitarbeitern ermöglichst, wa ich sehr schätze.
Herr Prof. Dr. David P. Wolfer, bei Ihnen bedanke ich mich, dass Sie sich bereit erklärt
haben als Co-Referent für meine Doktorarbeit zu fungieren. Danke für Ihre Offenheit
sich auch mit Themen, welche ausserhalb Ihres Fachgebietes liegen zu begeistern.
Ohne die Mitarbeiter des IBWS wären die letzten vier Jahre nur halb so angenehm
gewesen:
Regula und Yvonne: Danke für die tolle Administrationsarbeit und eure Hilfsbereitschaft
– auch schon in den guten ‘alten’ Zeit im Kellersekretariat im ETH-Hauptgebäude.

200
Chapter Eight
Rolf: Danke für Deine Unterstützung bei technischen und statistischen Fragen im Rahmen
meiner Studien. Ich bewundere Dich für Deine kreative Herangehensweise bei solchen
Dingen. Laura: Danke für Deine Gastfreundschaft und den vielen selbstgemachten
Leckereien mit denen Du uns regelmässig verwöhnt hast. Brigitte: Danke für Deine
Unterstützung bei wissenschaftlichen Fragen und Dein leckeres Johannisbeerkuchen-
Rezept. Jessica: Danke, dass ich Dir gleich am ersten Arbeitstag den Fensterplatz
„klauen“ durfte. Danke für die gute Zeit als Nachbarn und auch für die Zeit, in der uns
ein hohes Bücherregal trennte. Simon: Danke für unsere manchmal sinnvolle, aber auch
sinnlose Diskussionen über Gott und die Welt. Dank Dir werde ich nie mehr vergessen die
Hintergrundebene im Photoshop zu duplizieren. Der Dank geht auch an Sara, Monika,
Roger, Roli und Oli, die zum guten Arbeitsklima am IBWS beigetragen haben.
Ganz besonders möchte ich mich bei meinen ‘Doktoratsgspänlis’ bedanken:
Andrea wir haben die Hochs und Tiefs des ‘Doktorandendaseins‘ fast vom selben Tag
an zusammen durchlebt. Wir haben immer versucht, uns gegenseitig so gut es ging zu
helfen. Ich danke Dir für die tolle Zeit, die wir miteinander am Institut erleben durften.
Dank für Deine Hilfsbereitschaft, Deine Echtheit und Dein Vertrauen Sam während Deinen
Experimenten hüten zu dürfen und Deine Offenheit während unseren Gesprächen über
Dinge, die das Leben so mit sich bringt. Ich hoffe Du konntest von mir eine kleine Portion
‘Ironie’ mit auf den Weg nehmen. Liebe Eva, heute denke ich nicht mehr, dass wir als die
‘dümmsten’ Doktoranden in der Geschichte der ETH eingehen werden, denn wir haben in
den gemeinsamen Jahren am IBWS viel erarbeitet und geleistet. Bewundert habe ich dabei
immer Deine Zielstrebigkeit und Dein Organisationstalent. Ein grosses Dankeschön für
Deine Mithilfe bei den Tests und für das Einspringen beim Leiten von Trainingslektionen.
Danke für Deine Mithilfe in der Organisation der Probanden und Räumlichkeiten für
die Durchführung der Reliabilitätsstudie in Feusisberg, das weiss ich sehr zu schätzen.
Ich wünsche Dir für Deine Zukunft als Mami und Geschäftsfrau von Herzen alles Gute.
Rahel Du warst der sichere Wert am IBWS. Wenn alle schon den Feierabend genossen
oder frei machten, warst Du noch mit mir im Büro. In der Zeit am Institut haben wir viele

201
Danksagungen
Gemeinsamkeiten entdeckt, z. B. das Ärgernis von ‘Nespresso-Kapseln-stecken-lassen-
bis-sie-so-fest-kleben-dass-sie-nicht-mehr-von-alleine-runterfallen’. Du hattest in Deinem
ersten Jahr leider etwas Pech mit Deinem Thema, ich wünsche Dir für Deinen zweiten
Anlauf alles Gute und viel Erfolg. Danke auch Dir Seline für die gemeinsame Zeit am
IBWS. In der kurzen Zeit konnte ich Dich als eine warmherzige, aufgestellte und fleissige
Person kennenlernen. Unsere Aufenthalte in Trondheim und Manchester und unseren
Ghetto-Gruss am Morgen und am Abend werde ich in guter Erinnerung behalten. Auch
Dir viel Erfolg bei Deiner Arbeit und ‘keep on running’. Lieber Patrick, leider hatten wir
nicht oft die Gelegenheit uns besser kennenzulernen. Ich wünsche Dir alles Gute für
Deine Doktorarbeit und danke, dass Du meine Arbeit mit den Tanzplatten am Institut
weiterverfolgst.
Ein spezieller Dank geht auch an Andrew Fraser. Ich bin Dir sehr dankbar für das englische
‘proof-reading‘ des Manuskripts dieser Doktorarbeit. Bleibe weiterhin so interessiert und
begeistert für neue Themen.
Danke auch an alle, die im Rahmen der Studien mitgeholfen haben, sei es bei der Mithilfe
bei der Durchführung der Tests, bei der Leitung der Trainingsstunden oder bei der
Bereitstellung der Räumlichkeiten: Amos Coppe, Angela Nägeli, Tatjana Diener, Simone
Karmann, Turgut Gülay, Manuela Nötzli, Melanie Ramp, Rosina Landolt, Susan Brouwer,
Gerhard Ineichen, Marie-Louise Sarraj, Hans van het Reve und danke allen Teilnehmern
und Mitarbeitern des Alterszentrum am Etzel in Feusisberg, des Zentrum Breitenhof in
Rüti, des Alterszentrum Lanzeln in Stäfa, der Altersheime Limmat und Stampfenbach in
der Stadt Zürich.


PhD Curriculum

204
Chapter Eight

205
PhD Curriculum
PhD Curriculum
Peer-reviewed publications:
de Bruin ED, Schoene D, Pichierri G, Smith ST. Use of virtual reality technique for the
training of motor control in the elderly. Some theoretical considerations. Z Gerontol
Geriatr. 2010 Aug; 43(4):229-34.
Pichierri G, Wolf P, Murer K, de Bruin ED. Cognitive and cognitive-motor interventions
affecting physical functioning: A systematic review. BMC Geriatrics 2011,11:29.
Pichierri G, Coppe A, Lorenzetti S, Murer K, de Bruin ED. The effect of a cognitive-motor
intervention on voluntary step execution under single and dual task conditions in
older adults: a randomized controlled pilot study. Clinicial Interventions in Aging,
2012:175–184.
Pichierri G, Murer K, de Bruin ED. A cognitive-motor intervention using a dance video
game to enhance foot placement accuracy and gait under dual task conditions in older
adults: a randomized controlled trial. BMC Geriatrics 2012,12:74.
Pichierri G, Diener T, Murer K, de Bruin ED. Assessment of the test-retest reliability of a
foot placement accuracy protocol in assisted-living older adults. Gait & Posture 38 (2013)
784–789.
Other publications:
Slavko R, Pichierri G, de Bruin ED. Denk-Sport – Dual-Tasking-Training mindert
Sturzrisiko. Physiopraxis 2011, 10:34-37 & Ergopraxis 2012, 3/12.

206
Chapter Eight
Presentations:
Oral presentation at the 1st Joint World Congress ISPGR and GMF in Trondheim (Norway),
June 28th, 2012: “The effects of computer game dancing on voluntary step execution in
older adults”.
Oral presentation at the 15th MOBEX Meeting 2012 in Zurich, Switzerland, January 13th,
2012: “The effects of a cognitive motor exercise intervention on voluntary step execution
and step accuracy in older adults”.
Oral presentation at the 14th MOBEX Meeting 2011 in Glasgow, Scotland UK, January 14th,
2011: “Cognitive and cognitive-motor interventions affecting motor functioning of older
adults: a systematic review”.
Poster presentation at the 16th annual Congress of the European College of Sport Science
(ECSS) in Liverpool UK, July 7th, 2011: “Cognitive and cognitive-motor interventions affec-
ting motor functioning of older adults: a systematic review”.
Poster presentation at the 4. Jahrestagung der Sportwissenschaftlichen Gesellschaft der
Schweiz (SGSS) in Magglingen, Switzerland, March 1–2, 2012: “The effect of a cognitive-
motor intervention on voluntary step execution under single and dual task conditions in
older adults: a randomized controlled pilot study”.
Visited congresses:
3rd International Congress on Gait & Mental Function – The interplay between walking,
behavior and cognition. Washington D.C., USA, February 26–28, 2010.
14th MOBEX Meeting 2011 in Glasgow, Scotland UK, January 14–15, 2011.
16th annual Congress of the European College of Sport Science (ECSS), Liverpool,
England UK, July 6–9, 2011.
15th MOBEX Meeting 2012 in Zurich, Switzerland, January 13–14, 2012.
1st Joint World Congress ISPGR and GMF in Trondheim (Norway), June 24–28, 2012.
16th MOBEX Meeting 2013 in Manchester, England UK, January 13–14, 2013.

207
PhD Curriculum


Curriculum vitae

210
Chapter Eight

211
Curriculum vitae
About the author
Name Giuseppe Pichierri
Date of birth July 6th 1979 in Bülach, Switzerland
Citizen of Niederglatt, Zurich, Switzerland
Sava, Taranto, Italy
Education
2009 – 2014 PhD in Science at the Institute of Human Movement Sciences and
Sport, ETH Zurich, Switzerland
2006 – 2008 Master of Science Degree in Human Movement Sciences and Sport ETH
Zurich with Major in Motor Control and Motor Learning
2002 – 2006 Bachelor of Science Degree in Human Movement Sciences and Sport,
ETH Zurich
1995 – 2000 Academic Upper Secondary School, Matura Type D (modern languages)
Master thesis and academic internships
01 – 07/2008 Master thesis ETH Zurich, Switzerland
“Factors related to the reduced physical activity in patients with
hematological malignancies”
In collaboration with the University Hospital Zurich
09 – 12/2007 Academic internship II in oncological rehabilitation in the Clinic for
Rheumatic Diseases and Physical Medicine at the University Hospital
Zurich, Switzerland
03 – 06/2007 Academic internship I in neuropsychology at the Institute for Neuro-
psychology of the University of Zurich, Switzerland








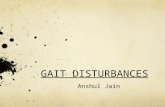


![Speed Invariance vs. Stability: Cross-Speed Gait ...makihara/pdf/accv2016_xu.pdf · gait energy image (GEI) [7], frequency-domain feature [8], chrono-gait image [9], gait flow image](https://static.fdocuments.in/doc/165x107/5f305a4d15c68c7b7c70ceb7/speed-invariance-vs-stability-cross-speed-gait-makiharapdfaccv2016xupdf.jpg)