Rick 2004 Omscna
22
Adenomatoid odontogenic tumor Gordon M. Rick, DDS, MS a,b, * a Loma Linda University, School of Dentistry, Loma Linda, CA, USA b Scripps Oral Pathology Service, 5190 Governor Drive, Suite 106, San Diego, CA 92122-2848, USA The adenomatoid odontogenic tumor (AOT) is included in classifications of odontogenic tumors because it occurs only in the tooth-bearing area of the jaws and because of its histomorphologic resem- blance to components of the dental organ (tooth germ). Although numerous cases have been reported, AOT generally is considered to be an uncommon tumor. Its distinctive, although not pathognomonic, clinicopathologic profile is unique among odonto- genic tumors because most lesions occur in associa- tion with an unerupted maxillary cuspid in teenage girls. Although the so-called ‘‘duct-like structures’’ are a unique (although not always present) micro- scopic feature of AOT, a diagnostic pitfall has been delineated. No unequivocal recurrences have been reported despite known incomplete removal of some tumors. History and terminology The AOT, like many odontogenic tumors, has an interesting history. The search for the first identifiable case is challenging because many names have been used for it, some early cases were grouped with other superficially similar tumors, and especially because photomicrographic documentation was not available in that era. The earliest irrefutable case that I found was reported from Norway by Harbitz [1] in 1915 as ‘‘adamantoma’’; however, the case reported by James and Forbes [2] from England in 1909 as an ‘‘epithe- lial odontome’’ is almost certainly an AOT. The first acceptable American case that I found was reported in 1916 as ‘‘tooth germ (or chorioblastomatous) cyst of the jaw’’ by Wohl [3] of Omaha, Nebraska. Although he did not propose a specific name for it, Stafne [4] reported the first series of AOT in 1948 under the title ‘‘epithelial tumors associated with developmental cysts of the maxilla’’. Presumably, he chose not to use ‘‘adenoadamantoblastoma’’ or ‘‘adamantoblastoma, adenoma type’’ because none of his three cases resembled the case that was illustrated under those terms in the first several editions of Thoma’s [5] Oral Pathology textbook. Thoma’s con- cept of this tumor obviously was influenced by his earlier work in salivary gland embryology as seen in his explanation of the derivation of this lengthy term [6]. He believed that in this variant of the adamanto- blastoma ‘‘the epithelium in its differentiation may tend toward glandular structure and arrangement. This is due to the fact that the oral epithelium has the potential ability to form glandular as well as dental structures.’’ In a later case report he goes to even greater lengths to defend this belief [7]. Bernier and Tiecke [8] were the first to publish a case using the name ‘‘adeno-ameloblastoma.’’ The superb photomicrographs in their later series of nine cases from the Armed Forces Institute of Pathology undoubtedly made a profound contribution to the eventual recognition that AOT is not merely a type of ameloblastoma [9]. Although they emphasized the younger average age of affected patients, the fre- quent association with impacted teeth, and the lack of recurrence (with follow-up ranging up to nearly 15 years), they did not divest this innocent lesion of its taxonomic link to the ameloblastoma. A classification of odontogenic tumors that listed ‘‘simple ameloblastoma’’ and ‘‘adenoameloblastoma’’ as separate entities ‘‘was presented for further consid- 1042-3699/04/$ – see front matter D 2004 Elsevier Inc. All rights reserved. doi:10.1016/j.coms.2004.04.001 This work was supported partially by Fellowship No. 1FO6 TW00820-01 from the National Institutes of Health. * Scripps Oral Pathology Service, 5190 Governor Drive, Suite 106, San Diego, CA 92122-2848. E-mail address: [email protected] Oral Maxillofacial Surg Clin N Am 16 (2004) 333 – 354
Transcript of Rick 2004 Omscna

Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354
Adenomatoid odontogenic tumor
Gordon M. Rick, DDS, MSa,b,*
aLoma Linda University, School of Dentistry, Loma Linda, CA, USAbScripps Oral Pathology Service, 5190 Governor Drive, Suite 106, San Diego, CA 92122-2848, USA
The adenomatoid odontogenic tumor (AOT) is lial odontome’’ is almost certainly an AOT. The first
included in classifications of odontogenic tumors
because it occurs only in the tooth-bearing area of
the jaws and because of its histomorphologic resem-
blance to components of the dental organ (tooth
germ). Although numerous cases have been reported,
AOT generally is considered to be an uncommon
tumor. Its distinctive, although not pathognomonic,
clinicopathologic profile is unique among odonto-
genic tumors because most lesions occur in associa-
tion with an unerupted maxillary cuspid in teenage
girls. Although the so-called ‘‘duct-like structures’’
are a unique (although not always present) micro-
scopic feature of AOT, a diagnostic pitfall has been
delineated. No unequivocal recurrences have been
reported despite known incomplete removal of
some tumors.
History and terminology
The AOT, like many odontogenic tumors, has an
interesting history. The search for the first identifiable
case is challenging because many names have been
used for it, some early cases were grouped with other
superficially similar tumors, and especially because
photomicrographic documentation was not available
in that era. The earliest irrefutable case that I found
was reported from Norway by Harbitz [1] in 1915 as
‘‘adamantoma’’; however, the case reported by James
and Forbes [2] from England in 1909 as an ‘‘epithe-
1042-3699/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.coms.2004.04.001
This work was supported partially by Fellowship No.
1FO6 TW00820-01 from the National Institutes of Health.
* Scripps Oral Pathology Service, 5190 Governor
Drive, Suite 106, San Diego, CA 92122-2848.
E-mail address: [email protected]
acceptable American case that I found was reported
in 1916 as ‘‘tooth germ (or chorioblastomatous) cyst
of the jaw’’ by Wohl [3] of Omaha, Nebraska.
Although he did not propose a specific name for
it, Stafne [4] reported the first series of AOT in 1948
under the title ‘‘epithelial tumors associated with
developmental cysts of the maxilla’’. Presumably,
he chose not to use ‘‘adenoadamantoblastoma’’ or
‘‘adamantoblastoma, adenoma type’’ because none of
his three cases resembled the case that was illustrated
under those terms in the first several editions of
Thoma’s [5] Oral Pathology textbook. Thoma’s con-
cept of this tumor obviously was influenced by his
earlier work in salivary gland embryology as seen in
his explanation of the derivation of this lengthy term
[6]. He believed that in this variant of the adamanto-
blastoma ‘‘the epithelium in its differentiation may
tend toward glandular structure and arrangement.
This is due to the fact that the oral epithelium has
the potential ability to form glandular as well as
dental structures.’’ In a later case report he goes to
even greater lengths to defend this belief [7].
Bernier and Tiecke [8] were the first to publish a
case using the name ‘‘adeno-ameloblastoma.’’ The
superb photomicrographs in their later series of nine
cases from the Armed Forces Institute of Pathology
undoubtedly made a profound contribution to the
eventual recognition that AOT is not merely a type
of ameloblastoma [9]. Although they emphasized the
younger average age of affected patients, the fre-
quent association with impacted teeth, and the lack
of recurrence (with follow-up ranging up to nearly
15 years), they did not divest this innocent lesion of
its taxonomic link to the ameloblastoma.
A classification of odontogenic tumors that listed
‘‘simple ameloblastoma’’ and ‘‘adenoameloblastoma’’
as separate entities ‘‘was presented for further consid-
s reserved.

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354334
eration but was not adopted’’ at the fifth annual
American Academy of Oral Pathology meeting in
1951 [10]. This failed to prevent the subsequent path
to a more universally accepted term that reflected the
lesion’s true nature from being strewn with numerous
rejected terms with varying degrees of nosologic
merit. An abbreviated list of the discarded terms
includes ‘‘cystic complex composite odontome’’ from
England [11], ‘‘an unusual pleomorphic adenoma-like
tumor in the wall of a dentigerous cyst’’ from Singa-
pore [12], ‘‘tumor of enamel organ epithelium’’ from
London [13], ‘‘adenomatoid ameloblastoma’’ from
Japan [14], and ‘‘adenomatoid odontoma’’ from the
United States [15].
In an attempt to ‘‘remove unjust stigma from this
lesion’’ and to eliminate the risk of unnecessarily
mutilating surgery for patients who had the tumor that
seemed to be occurring because of use of the term
‘‘adenoameloblastoma,’’ in 1961, Gorlin et al [16]
introduced the term ‘‘ameloblastic adenomatoid tu-
mor.’’ Shafer et al [17] provided additional support
for this moniker by adopting it in the second edition
of their widely used Textbook of Oral Pathology in
1963. Admitting that this term was an improvement,
and yet, concerned about the remaining ‘‘spector of
ameloblastoma,’’ in 1968, Abrams et al [18] sug-
gested consideration of the term ‘‘odontogenic adeno-
matoid tumor.’’ This paper was in press and was not
available to Philipsen and Birn [19] when they
proposed the name ‘‘adenomatoid odontogenic tu-
mor’’ in 1969. Shortly thereafter, the latter term was
adopted in the initial edition of the World Health
Organization’s (WHO) Histological Typing of Odon-
togenic Tumors, Jaw Cysts and Allied Lesions in
1971 [20] and was retained in the second edition in
1992 [21]. It subsequently became the generally
accepted nomenclature and apparently has facilitated
effective management of patients who have the lesion
ever since.
Therefore, although their concern about keeping
‘‘disease name’’ terminology current is laudable, I
disagree with the following statements by the re-
spected American surgeon-pathologist team, Marx
and Stern [22], in their recent 10-pound tome. They
state that ‘‘the catchy abbreviation AOT prevailed,
which unfortunately is also incorrect’’ and an ‘‘out-
dated term’’ and ‘‘therefore, the more appropriate term
is adenomatoid odontogenic cyst or AOC.’’ For a
lesion that generally is not a fluid-filled pathologic
cavity and often has a predominantly solid compo-
nent, it is difficult to understand how this change can
be considered an improvement or how it will contrib-
ute to better clinical management of patients who have
this bland tumor.
In the nearly 90 years since Harbitz clearly de-
scribed and illustrated his case, more than 800 cases
have been reported—most as individual case reports
because only 10 series with seven or more previously
unreported cases were found in the English-language
literature [9,18,23–30]. In 1991, Philipsen et al [31]
thoroughly reviewed the extensive world literature
and, on the basis of the 499 cases that they considered
acceptable, provided a clinical, radiographic, and
microscopic profile of the tumor that leaves few
remaining questions as to its diagnosis, biologic
behavior, and management. A subsequent update that
was based on more than 600 cases was published in
1998 [32] and AOT warrants an entire chapter in
Reichart and Philipsen’s [33] recent reference work
Odontogenic Tumors and Allied Lesions. It will be
interesting to compare this book with the chapter on
odontogenic tumors in the latest WHO ‘‘Blue Book’’
series, Pathology and Genetics of Tumours of the
Head and Neck that is expected later this year.
Classification
The classification of odontogenic tumors has been
the source of endless fascination and frustration for
microscopists for more than a century. Gabell et al
seem to be the first investigators to divide this group
of complex tumors into categories based on the
embryonal tissue of origin—epithelial, composite
(epithelial and mesoblastic), and connective tissue
(mesoblastic) [34]. The refinement of their scheme,
suggested by Thoma and Goldman [35], forms the
basis of most classifications to the present. Although
it is not known how closely odontogenic tumors
mimic the complicated process of odontogenesis, a
classification of odontogenic tumors that is based on
the inductive influences between epithelial and mes-
enchymal tissues during odontogenesis was proposed
by Pindborg and Clausen [36] and was modified
slightly by Gorlin et al [37,38]. Although the position
of AOT has varied in subsequent versions of the
classification [20,21,33], it always has been included
in the epithelial category rather than the mixed group,
despite the presence of abnormal hard tissue elements
within the tumor. Its subclassification by some inves-
tigators as a tumor of ‘‘odontogenic epithelium with-
out odontogenic ectomesenchyme’’ may need to be
reconsidered in view of the cases that are discussed
later that contain significant amounts of dentin, and
rarely, enamel matrix. The classification of AOT
simply as an epithelial tumor, however, also was sup-
ported in a recent immunohistochemical study that
used bone morphogenetic protein (BMP) to divide

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354 335
odontogenic tumors into those that were purely
epithelial (ie, negative for BMP) and those that
formed enamel, dentin, cementum, or bone (ie, posi-
tive for BMP) [39]. As new tumor-related proteins are
discovered [40] and gene-expression profiles are
developed for odontogenic tumors, more meaningful
classifications of these neoplasms may become avail-
able. However, it is likely to be some time before
the results of these studies will lead to more specific
diagnoses, more rational therapy, or more reliable
prognostication for patients that suffer from these
uncommon tumors.
Hamartoma versus neoplasm
The long-term debate as to whether AOT is an
anomalous developmental hamartomatous growth or
a true benign neoplasm has not been settled and it
likely never will be. This is due, in part, to difficulties
with precise definitions of what seem to be, at least
superficially, simple terms and concepts. Lucas and
Pindborg [41] eloquently discussed this problem as it
pertains to odontogenic tumors.
Meanwhile, investigators who prefer to consider
AOT to be a hamartoma [18,20,24,32,42–44] point
to the limited size of most cases (attributed to its
minimal growth potential) and to the lack of recur-
rence (even following definitely incomplete removal)
to support their belief. Those who prefer to consider
AOT to be a nonaggressive noninvasive benign
neoplasm [9,13,45–48] presumably believe that the
limited size of most cases stems from the fact that
most are detected early (often on a routine dental
radiograph) and removed before the slow-growing
tumor reaches a clinically noticeable size. They also
point to the considerable size of some reported cases
that had gone undetected or untreated for many years
and resulted in facial asymmetry and distortion that
rival many ameloblastomas [48–51]. Additional sup-
port comes from the microscopic features of the
lesional tissue that show greater departure from the
arrangement of the normal odontogenic apparatus
than should be expected in a developmental anomaly.
Based on currently available evidence, I agree with
Gardner [52] that AOT is ‘‘most appropriately con-
sidered a benign embryonal neoplasm.’’
Histogenesis
Like all other odontogenic tumors, the specific
stimulus that triggers proliferation of the progenitor
cells of AOT is unknown. Because of its exclusive
occurrence within the tooth-bearing areas of the jaws
(most often associated closely with an unerupted or
impacted tooth) and its cytologic resemblance to the
dental lamina and components of the enamel organ,
there is no disagreement that the AOT is of odonto-
genic origin. Since its earliest recognition as an entity,
however, many investigators have debated the histo-
genesis of AOT and the nature of the acellular
materials within the tumor. Even though their argu-
ments were based solely on routine light microscopy
and nonspecific histochemistry, their speculations
are interesting, and in some cases, farsighted. Be-
cause these theories have been discussed exhaustively
in the literature, they will not be reiterated here.
Although the precise progenitor cell or tissue of
AOT has not been settled, the development of the
transmission electron microscope (TEM) and the
availability of an ever-increasing variety of specific
antibodies for immunohistochemical (IHC) studies
have engendered considerable progress during the
past 30 to 40 years. Studies that used these tools
have confirmed that some AOT tumor cells are
equipped metabolically similar to ameloblasts during
particular stages of amelogenesis and are capable of,
and responsible for, generating the variety of extra-
cellular materials that commonly are observed in
these microscopically-fascinating tumors.
Thirteen ultrastructural studies [53–65] and 10 im-
munohistochemical studies [39,66–75] of AOT exist
in the English-language literature. Because formalin
fixation is prone to cause tissue artifacts at the TEM
level of observation, it should be mentioned that only
9 of the 17 tumors that were examined had been fixed
optimally for TEM. Also, because of the histomor-
phologic variation that exists between and within
examples of this tumor, it is possible that some of
the various tumor constituents may not have been
scrutinized fully (tissue samples for TEM study are
1-mm cubes). I have attempted to compare and har-
monize the results of these two branches of investi-
gation (TEM and IHC) but this proved challenging,
partially because of the different terminology that is
used. Some interesting observations have emerged,
however, and for the sake of brevity, the following
update concentrates on decisive findings although
equivocal observations also may be important.
Generally, TEM studies have confirmed the
resemblance of the various AOT tumor cells to
counterparts in the enamel organ. The presence of
hemidesmosomes and basal lamina at the luminal
pole of the cells that form the ductlike structures
conclusively rules out Thoma’s notion of a dual
salivary and odontogenic origin for AOT [57]. This

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354336
was corroborated by the negative reactivity of these
cells to lactoferrin and a1-antichymotrypsin anti-
bodies [74]. The duct-forming cells also exhibit
secretory granules and coated vesicles near the lumi-
nal pole which renders them highly reminiscent of
preameloblasts; these structures also were reported in
the nonduct-forming columnar cells in various pat-
terns [57–59,61]. IHC studies revealed differences
between the duct- and nonduct-forming cells; the
nonduct-forming columnar cells expressed ameloge-
nin reactivity, whereas the duct-forming cells showed
no reactivity to amelogenin [71] or the other enamel
matrix protein (enamelin and sheathlin) antibodies
[68,69,72]. Additionally, the eosinophilic material
that lines the periluminal surface (the so-called ‘‘hya-
line ring’’) resembled basal lamina by way of TEM
[53,56,57,60] and coexpressed basement membrane
extracellular matrix proteins (laminin, type IV colla-
gen, heparan sulfate proteoglycan, fibronectin) and
enamel matrix proteins (amelogenin, enamelin) [66,
68,71,75]. The same pattern of reactivity was seen
in the occasionally more abundant intraluminal ma-
terial. The droplets of eosinophilic material (the so-
called ‘‘hyaline’’ or ‘‘tumor droplets’’) between the
cuboidal, low columnar, and polygonal cells that
form the cell-rich tumor nodules exhibit TEM fea-
tures that are consistent with enamel matrix-like ma-
terial [59,60,65]. They also colocalized enamel matrix
and basement membrane antibodies and enamely-
sin (a tooth specific protease) antibodies [66,68,69,
71–73,75]. The tumor cells immediately adjacent to
the droplets also demonstrate cytoplasmic positivity to
the enamel protein, sheathlin [72]. These findings
provide additional support for the odontogenic origin
of AOT and indicate that some of the epithelial tumor
cells display features that are consistent with neoplas-
tic (pre)ameloblasts in a state of arrested development,
yet they apparently are metabolically active enough to
produce basement membrane and enamel matrix pro-
teins. It was suggested that the accumulation and
eventual (enamelysin) degradation of these secretory
products are responsible for the development of the
ductlike structures [71] that some investigators prefer
to think of as enclosed spherical microcysts, whether
they are considered as completely intraepithelial or
stromal in nature.
The spindle cells that are between the cell-rich
nodules resemble ultrastructurally the stellate reticu-
lum and those that are immediately adjacent to the
nodules resemble the stratum intermedium of the
enamel organ. The juxtanodular spindle cells are
amelogenin positive [68], whereas the internodular
spindle cells are nonreactive to amelogenin, ename-
lin, and sheathlin [69,72] which confirms the lesser
degree of differentiation of the latter cells that some
investigators suggested may be the progenitor cells of
the duct-forming cells [59].
The ultrastructural suggestion that the small, irreg-
ular calcifications may be partially composed of atypi-
cal enamel [60] is supported by positive reactivity of
this material to amelogenin, enamelin, and enamelysin
although it is sheathlin negative [69,71–73]. A TEM
study reported that the concentrically-laminated calci-
fied bodies were indistinguishable from calcified amy-
loid [64]. The ultrastructural morphologic variability
that is seen in this class of proteinaceous materials and
the similarity of the b-pleated sheet conformation of
amyloid and enamel must be kept in mind when
amyloid is being discussed. The fine structure of the
large, irregular, globular masses was reported in only
one study where it was conjectured to be atubular
dentin [60]. This must be evaluated further, especially
in view of reported positivity (especially at the pe-
riphery of the masses) to amelogenin and enamelin,
although they were enamelysin negative [69,73].
The gubernaculum dentis
Philipsen et al [76] argued that the AOT arises
from remnants of the successional dental lamina or
the accessional dental lamina (a distal extension of
the dental lamina in the permanent molar region).
Disintegration of the dental lamina complex leads to
numerous epithelial remnants that persist (presum-
ably indefinitely) in the jaws and gingiva following
completion of odontogenesis. According to Hodgson
[77] and expanded and explained by Philipsen et al
[76] and Reichart and Philipsen [33], these epithelial
rests are not distributed haphazardly but are confined
to the gubernaculum dentis—the fibrous connective
tissue that runs in intrabony gubernacular canals from
the bony crypts of all developing permanent tooth
buds to the overlying gingival lamina propria and
which is believed to guide or direct the course of
erupting succedaneous teeth and permanent molars.
Theoretically, eruption of a permanent tooth/teeth
adjacent to an odontogenic tumor may be halted when
the tumor envelopes the crown of the tooth and
disrupts the gubernaculum dentis or the developing
tooth erupts into a hamartomatous or neoplastic mass
and loses the guiding influence of the gubernaculum
dentis—hence a pericoronal lesion associated with an
unerupted tooth. Similarly, if the odontogenic tumor
were to arise from epithelial rests outside the eruptive
path, eruption of the adjacent tooth/teeth would not be
impaired and, following normal eruption, the tumor
would be located lateral, or possibly even apical, to
the erupted tooth/teeth.

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354 337
Epidemiology
The incidence and prevalence of odontogenic
tumors is unknown, largely because most of them
are benign and are not reported to local, regional, or
national tumor registries that compile and track
malignant tumors. AOT accounts for approximately
3% to 7% of odontogenic tumors that are accessioned
by a variety of institutions around the world which
makes it the fourth most frequent odontogenic tumor
[31,32].
Demographic features
Age
Although AOT has been reported in patients from
3 to 82 years of age, its predilection for young
patients is well-established. It is unique among odon-
togenic tumors and unexplainable that more than two
thirds (69%) are diagnosed between the ages of
10 and 19 years; more than half (53%) are diagnosed
in teenagers; 21% are diagnosed between ages 20 and
29; and altogether, 88% are diagnosed in the second
and third decades. Pericoronal (dentigerous, follicu-
lar) AOTs are diagnosed at an earlier age than lesions
that are not in a pericoronal relationship to a tooth,
probably because affected patients seek consultation
concerning failure of the associated tooth to erupt.
The early detection of gingival (peripheral, extraos-
seous) AOTs is likely due to the discovery of a
variably obvious anterior maxillary gingival mass.
Although the average age at the time of excision
of gingival lesions is 13 years (and ranges from 3 to
19 years), the fact that some lesions had already been
present for 3 to 5 years suggests that gingival AOTs
develop at an early age [31,32].
Gender
Overall, the tumor is diagnosed approximately
twice as frequently in women. Although in the third
decade AOT is nearly four times more frequent in
women, in patients who are older than age 30 it is
diagnosed nearly twice as commonly in men. It also
is interesting and unexplainable that the female:male
ratio for gingival lesions is 14:1 [31,32].
Race
Like ameloblastoma, the AOT may be more
common in blacks, but this may be just a ‘‘harvest-
ing’’ phenomenon rather than a true racial difference.
The significant female:male predominance of about
3:1 for reported cases from Sri Lanka and Japan
remains unexplained [31,32].
Clinical features
Anatomic site
Like most odontogenic tumors, AOT may occur
within the jawbones or the gingiva. Radiographic
findings are of more value than clinical findings for
the more than 95% of AOTs that develop within the
maxilla or mandible. Before age 30, nearly twice as
many maxillary lesions are diagnosed, whereas after
age 30, almost twice as many lesions are diagnosed
in the mandible [31].
Clinical signs
Most central lesions are discovered on routine
dental radiographic examination; however, delayed
eruption of (especially an anterior maxillary) perma-
nent tooth or slow-growing bony expansion (with or
without displacement of adjacent teeth) that overlies
the lesion commonly lead to the discovery of the
intragnathic AOTs. Mobility of teeth [42,78–80],
swelling of the cheek [51], and asymmetrical facial
swelling have been reported less frequently. Periph-
eral lesions present as a gingival-colored mass that
ranges from 1 to 1.5 mm in diameter (the size was
listed in only 4 of 18 reported cases). They are
10 times more prevalent in the maxillary gingiva
than in the mandibular gingiva; all but 3 of the 18 re-
ported cases were located adjacent to an incisor—
usually the maxillary central incisor [32].
Clinical symptoms
Usually, AOTs are asymptomatic; however pa-
tients may be aware of a gingival swelling or an
area of jaw enlargement. Rarely, infection of the
tumor or fracture of the mandible [11] has led to
discovery of the condition. Nasal obstruction was
reported in conjunction with rarely encountered
large maxillary lesions [50,51]. Gingival lesions most
often are painless.
Clinical differential diagnosis
Because the diffuse swelling that can accompany
central lesions is clinically indistinguishable from the
maxillary or mandibular enlargement that may occur
with central odontogenic cysts and tumors as well as

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354338
benign fibro-osseous lesions and benign mesenchy-
mal neoplasms; radiographic evaluation is indicated
to narrow the differential diagnostic considerations.
Gingival lesions cannot be differentiated clinically
from gingival fibromas, peripheral cemento-ossifying
fibromas, peripheral giant cell lesions, or from other
peripheral odontogenic tumors, such as odontogenic
fibroma, ameloblastoma, calcifying odontogenic cyst,
and calcifying epithelial odontogenic tumor.
Fig. 2. A 13-year-old girl presented because of delayed
eruption a maxillary lateral incisor and the surgeon de-
scribed an overlying ‘‘fluctuant bulge.’’ This corticated
unilocular radiolucent lesion was superimposed partially
on the unerupted tooth. (Courtesy of R.E. Barsan, DDS,
El Centro, CA.)
Radiographic features
Anatomic site
A significant number of AOTs are discovered
radiographically because more than 95% occur intra-
osseously (centrally), usually as small asymptomatic
lesions [32].
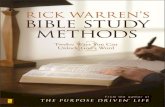
Pericoronal
About 71% of AOTs are associated with the
crown of an unerupted permanent tooth (Fig. 1),
including about 6% that are associated with two or
more unerupted teeth. Nearly 60% of AOTs are
associated with cuspids—40% with the maxillary
cuspids. Only rarely (f3% or 7/220) is AOT asso-
ciated with permanent molars and reported cases
have been almost exclusively related to third molars
but at a mean age of 9 years greater than those
associated with cuspids (i.e. 25.6 vs. 16.5) presum-
ably due to the later biologic development of molars
than anterior teeth. This age difference also is related
to the fact that unerupted/impacted posterior teeth
are diagnosed later than unerupted/impacted anterior
teeth, at least partially because of their lesser cosmetic
Fig. 1. Distribution of pericoronal (dentigerous, follicular)
AOT associated with unerupted permanent teeth (n = 341).
(Data from Philipsen HP, Reichart PA. Adenomatoid
odontogenic tumor: facts and figures. Oral Oncol 1998;35:
125–31.)
impact [76]. Only two reported cases involved pri-
mary teeth [31,81].
Extracoronal
Nearly 30% of the central AOTs are not pericoro-
nal and demonstrate a relationship to the roots of
adjacent or nearby teeth that ranges from lateral or
interproximal to periapical to no relationship at all.
Among the extracoronal cases where the exact loca-
tion was reported, 89% of AOTs occurred adjacent to
a permanent cuspid. Four of 86 lesions appeared in a
periapical position but some likely were superim-
posed on the apex radiographically [31,82].
Radiographic signs
Central AOTs almost invariably display the radio-
graphic features of a benign intrabony odontogenic
lesion by presenting as a well-demarcated, almost
always unilocular radiolucency that generally exhibits
a smooth corticated (and sometimes sclerotic) border.
Most lesions are pericoronal or juxtacoronal (Fig. 2)
but the radiolucency may extend apically beyond the
cemento-enamel junction on at least one side of the
root (Fig. 3) [18,47]. Rare, multilocular cases have
been reported [48,83,84] and a scalloped border is
observed occasionally [9,45]. Most cases are between
1 and 3 cm in greatest diameter and are associated
with only one impacted tooth; however, several much
larger cases were reported, including one that was
12 cm in diameter and was associated with seven

Fig. 3. A 16-year-old girl presented with a 3-cm hard bony
expansion of unknown duration. The corticated unilocular
pericoronal radiolucency does not ‘‘respect’’ the cemento-
enamel junction and there is displacement of the adjacent
teeth and apical resorption of the second bicuspid. (Courtesy
of J.J. Moses, DDS, MD, Encinitas, CA.)
Fig. 4. This 2-cm soft mass from the maxillary lateral incisor
area of a 12-year-old girl had a capsule of varying thickness
and was composed of soft granular tan material without
evidence of a cyst cavity or lining. (Courtesy of R.S.
Mowry, DDS, Chula Vista, CA.)
G.M. Rick / Oral Maxillofacial Surg
impacted teeth (including some deciduous teeth) [48].
About 65% of reported cases also demonstrate faintly
detectable radiopaque foci within the radiolucent
lesion. Because this feature often is not visible on
panoramic films, obtaining good quality periapical
views of the lesional area of suspected cases is
advisable [85]. Occasionally, a more obvious intrale-
sional radiopacity may be identified, usually eccentri-
cally positioned within the lesion. Although not
mentioned often in case reports, divergence of roots
and displacement of teeth [47,48,50,51] occurs more
frequently than root resorption [47,86–90]. Several
reported cases have encroached on [12] or filled or
expanded the maxillary sinus [4,9,51,80,91–95], in-
cluding one case that contained a calcified, craterlike
mass of dentinoid material [96]. Orbital encroachment
also has been mentioned occasionally [12,80,95].
Gingival lesions rarely are detectable radiograph-
ically but there may be slight erosion of the underly-
ing alveolar bone cortex. One reported case [97]
demonstrated central and peripheral involvement; it
could not be determined whether the bilobed lesion
was primarily a gingival lesion that had eroded into
the underlying alveolar bone or if a superficial,
primarily intraosseous lesion had expanded out into
the overlying gingiva. I saw a case in a 9-year-old girl
who had been aware of an asymptomatic firm gingi-
val swelling adjacent to a maxillary central incisor for
a year. A periapical radiograph revealed slight peri-
radicular widening of the periodontal ligament space
as the only radiographic finding.
Radiographic differential diagnosis
Pericoronal
The differential diagnosis of dentigerous (follicu-
lar) AOTs includes the following radiolucent lesions
that range from frequently to rarely identified in a
pericoronal relationship to a tooth: dentigerous (fol-
licular) cyst, odontogenic keratocyst, calcifying
odontogenic cyst, unicystic ameloblastoma, amelo-
blastic fibroma, early ameloblastic fibro-odontoma,
odontogenic fibroma, and calcifying epithelial odon-
togenic tumor.
Extracoronal
The differential diagnosis of extracoronal AOTs
includes most of the aforementioned odontogenic
cysts and tumors because they also may occur in a
nonpericoronal relationship to an unerupted or erup-
ted tooth (some dentigerous cysts are lateral rather
than pericoronal). Additional considerations include
central giant cell lesion (granuloma, tumor), benign
fibro-osseous lesions (eg, early cemento-ossifying
fibroma), lateral periodontal cyst, lateral radicular
cyst, apical radicular cyst and much rarer central
benign mesenchymal neoplasms (eg, neurilemoma).
Clin N Am 16 (2004) 333–354 339
Macroscopic features
Unmagnified gross examination of most excision-
al surgical specimens of central AOTs reveal a soft,
roughly spherical mass with a discernible fibrous
capsule. Upon gross sectioning, the tumor may ex-
hibit white to tan solid to crumbly tissue or one or

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354340
more cystic spaces of varying size; minimal yellow-
brown fluid to semisolid material; fine, hard ‘‘gritty’’
granular material; and one to several larger calcified
masses. Additionally, intact dentigerous specimens
demonstrate the crown of a tooth embedded in the
solid tumor mass or projecting into a cystic cavity
(Fig. 4).
Routine light microscopic features
The AOT exhibits diverse histomorphologic fea-
tures but the light microscopic findings are remark-
Fig. 5. (A) The characteristic clusters of cell-rich nodules are identi
magnification �40). (B) Droplets of eosinophilic material are seen
layering of the juxtanodular spindle cells is discernible (hematoxyl
of some of the ‘‘peridroplet’’ tumor cells (hematoxylin-eosin, orig
ably consistent from tumor to tumor. Although present
in varying proportions, the tumor is made up of a
cellular multinodular proliferation of spindle, cuboi-
dal, and columnar cells in a variety of patterns; usually
scattered ductlike structures, eosinophilic material,
and calcifications in several forms; and a fibrous
capsule of variable thickness. Although the literature
contains multiple histochemical, ultrastructural, and
immunohistochemical analyses, these special tests are
not needed to establish a reliable diagnosis of this
distinctive neoplasm. They have been used almost
exclusively in research attempts to determine the cell
of origin or the nature of the lesional products.
fied easily in this scanning view (hematoxylin-eosin, original
between the spindle to polygonal cells and vague concentric
in-eosin, original magnification �100). (C) Vague clustering
inal magnification �250).

Fig. 6. (A) Microcysts (‘‘ducts’’ or ‘‘tubules’’) lined by cuboidal to low-columnar cells with some pale basophilic fibrillar and
floccular material (consistent with basement membrane and enamel matrix proteins) in the lumen in addition to a residual
droplet of eosinophilic material (enameloid?) (arrow) (hematoxylin-eosin, original magnification �400). (B) An eosinophilic
rim of varying thickness lines several ducts one of which shows more prominent nuclear polarization (hematoxylin-eosin,
original magnification �250).
Fig. 7. Tall eosinophilic columnar cells resembling func-
tional ameloblasts abutting a partially calcified mass of
eosinophilic material and an adjacent focus of CEOT-
like polygonal cells with intercellular bridges (hematoxylin-
eosin, original magnification �250).
G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354 341
Cell-rich epithelial nodules
Examination at scanning or low magnification
usually is dominated by variably sized, cell-rich nests
or nodules that are composed of spindle to cuboidal
to polygonal epithelial cells. At higher magnification,
it is apparent that some of the cells are arranged in
clusters, frequently around small foci of eosinophilic
material (so-called ‘‘hyaline droplets’’ or ‘‘tumor
droplets’’) (Fig. 5).
Microcysts
Although not present in all tumors, the most
distinctive microscopic feature of AOT is varying
numbers of ductlike structures with lumina of varying
size that are lined by a single layer of cuboidal to
columnar epithelial cells that have nuclei that fre-
quently are polarized away from the lumen. Follow-
ing examination of several tumors, it is not difficult to
develop the impression that there is a continuous
spectrum from the cells of the peridroplet clusters to
the cuboidal to progressively more columnar cells
that line lumina of gradually increasing diameter
(Fig. 6). One study of serial sections supports an
earlier contention that these structures are closed
spherical microcysts rather than ducts or tubules
[98], whereas another study purported a direct con-
nection from the tumor stoma into the duct lumina
[14]. These ductlike or microcyst lumina frequently
are lined by an eosinophilic rim of varying thickness
(the so-called ‘‘hyaline ring’’) and they may be empty
or contain finely fibrillar or flocculent material of
variable staining quality. Extremely tall columnar
cells with intensely eosinophilic cytoplasm and mark-
edly polarized nuclei are seen occasionally (espe-
cially near calcifying epithelial odontogenic tumor
[CEOT]-like areas) abutting a solid mass of usually
partially calcified eosinophilic material (Fig. 7). Usu-
ally, the columnar cells demonstrate clear cytoplasm
and form rosettes as well as linear, curved, convo-
luted, invaginated, and occasionally branching rows
of opposing cells. A strip or band of noncalcified

Fig. 8. Rosette (hematoxylin-eosin, original magnification �250) (A) and convoluted double row (B) of columnar cells
(hematoxylin-eosin, original magnification �400).
G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354342
eosinophilic material (that resembles the hyaline ring)
usually is present between the opposing rows of
columnar cells that also may demonstrate separations
of varying width at irregular intervals (Figs. 8–10).
Internodular epithelial cells
Swirling streams of variably stellate reticulum-
like spindle cells to occasionally round or polygonal
epithelial cells that can demonstrate zones of intense
basophilia dominate the tissue between the cell-rich
nodules. Small amounts of eosinophilic material or
calcifications also may be present between these cells
(Fig. 11). The spindle cells that are immediately
adjacent to the cell-rich nodules are sometimes ar-
ranged with their long axis parallel to the periphery of
the nodule which results in a vague layered appear-
ance (Fig. 5B).
Fig. 9. Curved rows of columnar cells with a tubular ap-
pearance (hematoxylin-eosin, original magnification �100).
Basaloid epithelial cells
Variably-sized areas that are composed of one-
to two-cell wide anastomosing strands of basaloid
epithelial cells that are arranged in a plexiform,
trabecular, cribriform, or latticework configuration
occasionally extend between the cell-rich nodules
and usually are present in the peripheral subcapsular
area of most tumors (Fig. 12). These small, round to
cuboidal cells with small round dark nuclei, and often
clear cytoplasm, resemble cells or rests of the den-
tal lamina.
Calcifying epithelial odontogenic tumor-like foci
Many AOTs contain up to a few clusters of well-
defined eosinophilic polyhedral squamous epithelial
Fig. 10. Branching rows of tall columnar cells with a band
of eosinophilic material between the rows that periodi-
cally separate to varying degrees (hematoxylin-eosin, origi-
nal magnification �100).

Fig. 11. (A) The stellate reticulum-like spindle cells between the cell-rich nodules and microcysts/duct-like structures may
demonstrate areas of intense hyperchromasia (hematoxylin-eosin, original magnification �100). (B) Small droplets of
eosinophilic material and more basophilic calcifications may be present between these internodular cells (hematoxylin-eosin,
original magnification �400).
G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354 343
cells with prominent intercellular bridges and, occa-
sionally, mild nuclear pleomorphism. Usually, pools
of amorphous, amyloid-like material and globular
masses of calcified substances also are present in or
near these squamous islands that bear considerable
histopathologic resemblance to the CEOT (Pindborg
tumor) (Fig. 13). Although some investigators refer to
these foci as areas of squamous metaplasia, ultra-
structural evidence confirms their metabolic capabil-
ity and similarity to CEOT tumor cells [99].
Cystic space
Although a considerable number of AOTs dem-
onstrate an identifiable cystic component, it is not
clear whether this represents pooling of the mucoid
stroma due to rupture of the thin lattice-work pattern
Fig. 12. Thin anastomosing strands of basaloid epithelial
cells in a plexiform, cribriform, or lattice-work pattern
(hematoxylin-eosin, original magnification �40).
or if the tumor developed within or adjacent to a pre-
existing cyst—presumably either could occur. Al-
though the cyst lining occasionally may resemble
that seen in dentigerous cysts, it more often is similar
to the basaloid cells that form the plexiform pattern
that was described above and may demonstrate bud-
like extensions into the adjacent stroma (Fig. 14).
Reduplicated basement membrane
Some tumors exhibit pools of finely fibrillar
eosinophilic material at the epithelial–connective
tissue interface; this was immunoreactive for the
basement membrane component laminin in the first
IHC study of AOT (Fig. 15) [66].
Dysplastic dentin/dentinoid
In addition to the droplets, bands, and globules of
amorphous eosinophilic material, some AOTs contain
varying amounts of usually paler and nonmineralized
fibrillar eosinophilic material that also may contain a
few entrapped cells. It has been labeled dysplastic
dentin, dentinoid, and osteodentin (Fig. 16) and
identification of dentinal tubules was reported occa-
sionally. A few cases with significant amounts of
dentinoid also were reported (see later discussion).
Calcified bodies
Varying amounts of calcified material in differing
forms is present in most AOTs. Most common are
irregular to round calcified bodies that may be seen
in parenchymal or stromal zones (Fig. 17) and may
exhibit areas with a concentric layered pattern

Fig. 13. (A) One to several small foci of eosinophilic polygonal cells with intercellular bridges resembling the CEOT are not
present infrequently in the cell-rich nodules or less frequently in the internodular areas of many AOT (hematoxylin-eosin,
original magnification �100). (B) The squamoid cells also may demonstrate intracellular amyloid-like material and admixed
or adjacent calcifications with or without concentric laminations generally are present (hematoxylin-eosin, original magnifica-
tion �250).
G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354344
(so-called ‘‘Liesegang rings’’). Larger, globular
masses often appear to be a fused conglomeration
of smaller masses that also may display Liesegang
rings (Fig. 18).
Stroma
Generally, the supporting stroma of AOTs is
loose, parvicellular, fibrovascular connective tissue
that may show considerable dilatation and congestion
of a prominent vascular component (Fig. 14).
Fibrous capsule
Invariably, the tumor has a fibrous capsule of
varying thickness and demonstrates no evidence of
local infiltration or invasion of the surrounding tissues.
Fig. 14. (A) Cell-rich nodules in loose fibrous stroma adjacent to cy
original magnification �100). (B) Basaloid cells lining cystic
(hematoxylin-eosin, original magnification �400).
Cytologic atypia
Although occasional foci of epithelial mitotic
activity have been reported, it never is a prominent
feature. Neither epithelial nor stromal cytologic
atypia has ever been reported, apart from the slight
nuclear pleomorphism that is observed in some
CEOT-like foci.
Microscopic differential diagnosis and diagnostic
pitfall
Typically, most AOTs are distinctive enough that
no other tumor or lesion needs to enter the patholo-
gist’s microscopic differential diagnostic considera-
tion. The problem of misdiagnosing an AOT with
a highly vascular stroma as a vascular ameloblas-
stic cavity along top of photomicrograph (hematoxylin-eosin,
cavity demonstrate an area of budding into the stroma

Fig. 15. (A) Thick aggregates of fibrillar eosinophilic material occasionally accumulate at the periphery of the tumor epithelial
cell masses (periodic acid-Schiff, original magnification �250). (B) This fibrillar material has been shown by electron micros-
copy and in this photomicrograph by immunohistochemistry to represent reduplicated basement membrane material. (antilaminin
immunoperoxidase stain, original magnification �250).
G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354 345
toma (‘‘adamantohemangioma’’ [100], ‘‘ameloblasto-
hemangioma’’ [101], ‘‘hemangioameloblastoma’’
[102], ‘‘vascular ameloblastoma’’ [103]) that oc-
curred around the time that the AOT was being
recognized as an entity was identified early and dealt
with promptly [45,104,105].
In the past several years we have become aware
of a new diagnostic pitfall. Rarely, ameloblastomas
with a plexiform pattern may exhibit a highly mucoid
stroma that can result in an adenoid appearance. The
similarity to AOT can be striking when the cells
that border the pale-staining to apparently empty,
round to ovoid stromal spaces demonstrate amelo-
blastic differentiation with nuclei that are polarized
away from the pseudolumen. This situation is well-
illustrated by the Armed Forces Institute of Pathol-
Fig. 16. Irregular islands of pale fibrillar eosinophilic material that
few entrapped cells and varying numbers of adjacent tumor epith
(hematoxylin-eosin, original magnification �250).
ogy (AFIP) Registry of Oral Pathology Case of
the Month for January 1994. The respondents to
the monthly, diagnostically-challenging cases are
almost exclusively oral and maxillofacial patholo-
gists; 42% returned a diagnosis of AOT (many
mentioned that it was atypical), 40% favored a
diagnosis of ameloblastoma, and 12% diagnosed it
as one of several other odontogenic tumors. The
AFIP interpretation was ‘‘adenoid ameloblastoma
with dentinoid’’ on the basis that: (1) the intraepithe-
lial ductlike spaces were lined by cuboidal to low-
columnar cells with some nuclei polarized away
from the (pseudoluminal) basement membrane and
occasionally contained blood vessels indicating that
the adenoid spaces likely contain connective tissue
mucoid matrix and (2) the presence of dentinoid
is consistent with dysplastic dentin or ‘‘dentinoid’’ contains a
elial cells (hematoxylin-eosin, original magnification �40)

Fig. 17. (A) Small round and larger irregular conglomerates of basophilic calcifications within the stroma (hematoxylin-eosin,
original magnification �100). (B) Multiple rounded and irregular globules with varying calcification within the tumor pa-
renchyma (hematoxylin-eosin, original magnification �400).
G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354346
material with focal dentin tubules [106] (Fig. 19).
Waldron [107] reported ‘‘an identical case’’ that had
recurred twice in less than nine years, one of the
reportedly recurrent AOTs (see prognosis section)
likely was an adenoid ameloblastoma [108], two
similar cases were reported from Japan [96,109], we
recently reviewed a case in consultation from another
institution, and we have several similar cases in our
archives. Altogether, these cases demonstrate a po-
tential diagnostic pitfall that can be avoided by
careful evaluation of the epithelium at the tumor–
stroma interface. In the adenoid ameloblastoma, the
ameloblast-like epithelial cells at the subcapsular
interface exhibit varying degrees of nuclear polariza-
Fig. 18. (A) Irregular stromal calcified body containing aggregate
magnification �125). (B) Calcified stromal globules of varying siz
(hematoxylin-eosin, original magnification �250).
tion away from the basement membrane (a feature
that is not present in AOT) and the other distinctive
features of AOT are not present (ie, rosettes, variably
convoluted opposing rows of columnar cells, and a
distinct capsule).
Treatment
Surgical findings
Although there may be expansion of the alveolar
bone overlying central lesions, the cortex is almost
invariably intact; however, on rare occasions, pene-
s of smaller rounded globules (hematoxylin-eosin, original
e with focal areas of concentric laminations (liesgang rings)

Fig. 19. (A) Plexiform ameloblastoma with cuboidal to columnar cells that exhibit varying nuclear polarization at the stromal
interface, including around ovoid ‘‘adenoid’’ spaces that contain abundant mucoid stroma (hematoxylin-eosin, original
magnification �100). (B) High power view of same features as well as a few small blood vessels in the adenoid stromal spaces
(hematoxylin-eosin, original magnification �400).
G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354 347
tration of the cortical plate has been reported. Essen-
tially all cases have a smooth, well-defined capsule of
varying thickness [31].
Enucleation and curettage
Because of the uniformly benign biologic behav-
ior of nearly all typical AOTs and the consistent
presence of a well-developed fibrous capsule, con-
servative complete surgical excision—usually ac-
complished by enucleation and curettage—is the
treatment of choice.
Incisional biopsy only
Although not considered to be the preferred treat-
ment, several reported cases resolved or failed to
progress following incomplete removal of varying
extent [98]. In one case, following complete removal
of a solid mass that had destroyed about one half of
the distal bone adjacent to an unerupted maxillary
cuspid, the ‘‘slightly loose’’ tooth was allowed to
erupt some before it was orthodontically-guided into
position; there was no evidence of recurrence during
6 years of observation [110]. Another similar case
that was managed by subtotal excision (presumably
following confirmatory incisional biopsy) showed no
evidence of persistence or recurrence during several
years of follow-up [111]. Finally, a 22-year-old Japa-
nese man who had swelling of the cheek, unilateral
nasal obstruction, a ‘‘large’’ unilocular radiolucency
that contained a displaced maxillary third molar, and
expansion of the maxillary sinus was presumed to
have a dentigerous cyst following aspiration of
40 mL of brown fluid that contained cholesterol
crystals. Although the lesion decreased in size during
the first 6 months of marsupialization, it showed
no change in the next 7 months and cystectomy
was performed. A mural AOT was diagnosed upon
microscopic examination of the 6-cm postmarsupial-
ization specimen, the sinus returned to normal ap-
pearance, and there were no signs of recurrence
7 months postoperatively [51].
Prognosis
Growth rate
AOT almost is always referred to as ‘‘slow’’ or
‘‘very-slowly growing’’ but no report of measure-
ments of growth rate over a course of time could be
located. The large size of a few of the reported cases
in young children from underdeveloped countries
indicate that some cases have shown at least a
moderate rate of growth [48,50]. Rarely, a period of
rapid growth is reported in a lesion of considerable
duration [112].
Recurrence rate
I was not able to find a single unequivocal case of
recurrence of an AOT. The five reportedly recurrent
cases that I located are summarized below in the
chronologic order in which they were published.
Case 1. Case report of adenoadamantoblastoma
This case [113,114] was rejected as a recurrent
AOT because no photomicrographs are available

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354348
for diagnostic confirmation, clinicoradiographic evi-
dence is more consistent with a unicystic ameloblas-
toma or an ameloblastoma that arose in a dentigerous
cyst, and the described microscopic features of the
1944 biopsy and excisional specimens are more
consistent with a plexiform or adenoid ameloblas-
toma. However, the enamel deposition that was
mentioned in the 1944 biopsy specimen is not
consistent with an ameloblastoma.
Case 2. Ameloblastic adenomatoid tumors: a report
of four new cases
Case 1 in this series of 4 cases was rejected as a
recurrent AOT because the age and gender of the
patient and the site of the tumor are not typical of
AOT, but it cannot be ruled out on that data alone.
The initial partial excision resulted in a microscopic
diagnosis of ‘‘adamantinoma’’ in 1916 and the
single published photomicrograph portrays a few
ductlike structures that are lined by cuboidal cells.
The lack of nuclear polarization in the ductal cells
and the cellularity and possible cytologic atypia of
the interductal epithelial cells preclude ruling out a
primarily solid ameloblastoma with mucoid stroma,
however [42]. If the tumor was not atypical or
malignant before treatment, the extensive radiation
treatments likely promoted the malignant transforma-
tion to which the patient eventually succumbed in
1925 [115].
Case 3. A case report of adenoameloblastoma of the
maxilla
This case in a 10-year-old Japanese girl [116] is
the most likely bona fide recurrent case; however, it is
not completely unequivocal. The published photo-
micrographs of the reportedly recurrent lesion are
typical for AOT as are the patient’s age at the time of
original treatment and the location of the lesion;
therefore, the original diagnosis likely is correct.
The possibility that the original ‘‘cyst’’ was some-
thing other than an AOT cannot be excluded on the
basis of the material that is available for analysis,
however. The nature and completeness of the original
cystectomy also is unknown. Because this may be the
only bona fide case of AOT recurrence, it would be
interesting to review the radiographs of the original
lesion and at the time of the apparent recurrence at
age 13 to 15. It also would be especially helpful to
review the microslides of the original surgical speci-
men. It is my understanding that this material prob-
ably is not available and it may never be known for
certain whether the microscopic features of the origi-
nal surgical specimen are similar enough to the final
specimen to qualify it as a genuine recurrence.
Case 4. Odontogenic adenomatoid tumor of the
mandible (adenoameloblastoma)
This case [108] cannot be accepted as an unequiv-
ocal recurrent AOT for several reasons. Although the
age of the patient and the site of the tumor are not
typical of AOT (like case 2, above) it cannot be
excluded on that basis alone. There is no photo-
micrograph of the original surgical specimen and no
histopathology report is available. Additionally, the
description of the radiographic features of the recur-
rent lesion that was noted 5 years following the initial
curettage fits the clinician’s published radiographic
impression of ameloblastoma. Finally, the three pub-
lished photomicrographic images of the recurrent
tumor are similar to the adenoid ameloblastoma that
was described above. Other investigators who
reviewed this case favor a diagnosis of adenoid cystic
carcinoma [31].
Case 5. A case of adenomatoid odontogenic tumor
with intracranial extension
The paper is written in Japanese [117] with a brief
English abstract and it cannot be accepted as an
unequivocal recurrent AOT for several reasons. Al-
though AOT cannot be ruled out on the basis of the
patient’s age, the plain radiographic, tomographic, and
CT scan descriptions of the large lesion with involve-
ment of several paranasal sinuses, extensive destruc-
tion of the base of the skull, and intracranial extension
do not conform to any previously reported AOT. The
fact that it ‘‘recurred several times’’ before intracranial
extension does not coincide with the behavior of any
other reported AOT. Most importantly, however, be-
cause the single published photomicrograph does not
demonstrate the classic microscopic features of AOT,
this recurring aggressive case cannot be accepted as
such unless more evidence is provided. I believe that
the features that are seen in the only available photo-
micrograph are more suggestive of an ameloblastoma.
Association of adenomatoid odontogenic tumor
with other odontogenic cysts and tumors
Over the years, several odontogenic tumors of
various types were reported to occur in association
with odontogenic cysts, or, more rarely, in association
with other odontogenic tumors. In addition to its
frequently reported association with a dentigerous

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354 349
(follicular) cyst, the AOT occasionally was reported
in conjunction with other odontogenic tumors.
Dentigerous cyst
The AOT may demonstrate, grossly and micro-
scopically, one or more associated cystic cavities.
Some of these cysts may be lined by nonkeratinized,
stratified, squamous epithelium that is similar to the
lining of dentigerous cysts, whereas others may be
lined by a less structured membrane that may dem-
onstrate budlike extensions into the supporting stroma.
Although most central AOTs occur in a pericoronal
relationship with an associated tooth, there is noway to
be certain whether the lining of an associated cyst
represents a true dentigerous cyst or cystic change
within the AOT.
Combined epithelial odontogenic tumor
Several investigators mentioned foci of squamous
metaplasia among the tumor cells in some of the
AOTs that they reported [18,24,58]. Following a
report of scattered ‘‘CEOT-like foci’’ within other-
wise typical AOTs and the introduction of the term
‘‘combined epithelial odontogenic tumor’’ [118], at
least 24 cases with this combination of features have
been reported [32]. In the largest series reported to
date, all AOTs (with paraffin blocks available for
additional sections) that were accessioned (within an
unspecified period of time) by three dental school
diagnostic oral pathology services in Mexico were
reviewed; CEOT-like foci were found in all 12 cases
[119]. All of the patients fell within the usual profile
of AOT and the conclusion that this feature forms part
of the usual histomorphologic spectrum of AOT
apparently is shared by most oral and maxillofa-
cial pathologists.
Odontoma (and similar tumors)
In 1951, Miles [11] reported an AOT from the left
posterior mandible as ‘‘a cystic complex composite
odontome’’ because hard tissue that he interpreted as
dentin and enamel matrix was identified within the
tumor. His descriptions of these materials and the
single photomicrograph raise the possibility that he
observed calcified bodies that now are recognized as
commonly present in AOT. Similar cases were
reported later by other investigators who used the
term ‘‘adenoameloblastic odontoma’’ [120,121] or
descriptive terminology [122]. The most recent simi-
lar cases were published as ‘‘adenomatoid odontoma’’
[123–125]. Additionally, at least seven similar cases
have been reported that include, in addition to areas of
typical AOT, varying amounts of dentin, apparently
without any associated formation of atypical ename-
loid or prismatic enamel matrix [83,90,126,127]. Five
of the seven cases were described as having a pe-
ripheral rim of dentin [90,127], six of them occurred
in the mandibular bicuspid-molar area of 29- to
82-year-old adults [83,90,127], and no recurrences
were reported. Although Allen et al [127] suggested
that ‘‘the term adenomatoid dentinoma should be
applied’’ to this tumor, until there is evidence that
these histomorphologic features are accompanied by
altered biologic behavior, it seems advisable to in-
clude them tentatively under the ‘‘AOT umbrella.’’ It
also is prudent to obtain long-term follow-up before
permanently accepting them into the ‘‘AOT fold.’’
A similar situation was reported in conjunc-
tion with other odontogenic tumors, including the
ameloblastoma, as evidenced by such terms as ‘‘ame-
loblastoma with dentinoid induction (dentinoamelo-
blastoma)’’ [128] and unicystic ameloblastoma with
dentinogenesis [129]. This brings to mind another
recently reported case that may illustrate the point
more easily to an audience of oral and maxillofacial
surgeons—an ‘‘odontogenic keratocyst with dentinoid
formation’’ [130]. Although the temptation to intro-
duce a new name (such as ‘‘dentinogenic odontogenic
keratocyst’’ or ‘‘odontogenic dentinokeratocyst’’) for
such a unique lesion can be almost overwhelming, it
always is wise to refrain from creating new entities
until distinctive clinicopathologic parameters are es-
tablished and have been confirmed.
Ameloblastoma
Raubenheimer et al [131] cited two cases of
unicystic ameloblastoma that showed focal mural
‘‘microscopic changes resembling an AOT.’’ No fol-
low-up information was provided; however, it proba-
bly can be assumed safely that these AOT foci had no
effect on the clinical course of the ameloblastomas.
Calcifying odontogenic cyst
Although a variety of odontogenic tumors have
been reported in association with calcifying odonto-
genic cysts (COC), the first reported association with
AOT was from Saudi Arabia in 1996. A ‘‘prominent
area’’ of AOT-like tissue was noted in the luminal
lining of a typical COC from the anterior mandible of
a 35-year-old man; there was no evidence of recur-
rence 18 months later [132]. Just as foci of CEOT do
not seem to alter the biologic behavior of AOT, a
focus of AOT should not be expected to alter the

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354350
clinical behavior of COC. A reportedly similar case in
the Japanese literature has not been obtained and
translated [133].
A mini-plea
Although it is a potentially valuable endeavor to
continue to collect, document, and report the demo-
graphic, clinical, radiographic, microscopic, and fol-
low-up information on these potential variants of
AOT, it seems unlikely that minor foci resembling
one odontogenic tumor or another will have any
significant effect on the clinical behavior of a dif-
ferent associated odontogenic tumor that makes up
the majority of a given lesion. Until proven other-
wise, it seems to be safe to manage an affected
patient in accordance with the majority lesion or the
worst-acting lesion if lesions of disparate behavior
are present.
Unusual cases
Melanotic adenomatoid odontogenic tumor
Three reported cases of otherwise typical AOTs (all
in nonwhites) showed varying numbers of melanin-
containing epithelial and stromal cells and admixed
melanocytes; so far, this has had no reported effect on
the innocent behavior of the tumor [134–136]. This
finding also was reported in several other odonto-
genic tumors (eg, ameloblastoma, COC, ameloblastic
fibroma, ameloblastic fibro-odontoma).
Multifocal adenomatoid odontogenic tumor
A most unusual case was reported recently from
Sweden in which a 12-year-old girl, over the course of
5 years, developed about a dozen separate radiolucent
lesions that were removed surgically on seven differ-
ent occasions along with about 20 associated tooth
germs and multiple erupted and unerupted malformed
teeth. The excised encapsulated soft tissue lesions
resembled AOT microscopically and invariably were
associated with the roots of the developing teeth
rather than their crowns as are most AOTs [137].
Future research and reporting of cases
Modern research methods have facilitated the
advancement of our understanding of the histogenesis
of this intriguing tumor but unanswered questions
remain. We eagerly await the results of in situ
hybridization, DNA microarray analysis, gene re-
arrangement studies, and other developing molecular
biology techniques to solve the remaining mysteries.
For these research efforts to move forward there is a
continuing need for tissue from these rare tumors.
Because this in the one exclusive area of oncology
that our two dental specialties can claim, I suggest
that the American Academy of Oral and Maxillo-
facial Pathology and the American Association of
Oral and Maxillofacial Surgeons appoint a joint
committee on Odontogenic Tumor Research to work
with the National Institutes of Health or academic
institutions. In addition to prioritizing a list of impor-
tant remaining questions concerning odontogenic
tumors, the group could set up protocols for obtain-
ing, transporting, and storing fresh tumor tissue from
these rare tumors to establish a research tissue bank
that could help to advance our understanding of these
fascinating lesions.
On a more practical level, I agree with following
recommendations of Philipsen et al [31] to discon-
tinue reporting ‘‘classic’’ pericoronal cases of AOT
but to continue to report well-documented cases that
are associated with primary teeth, extracoronal intra-
osseous cases, gingival cases, and, especially, all fully
documented recurrences.
Summary
The AOT is one of the most unique and thor-
oughly profiled odontogenic tumors; however, oral
and maxillofacial surgeons also must be familiar with
its unusual variants to provide optimal patient care.
They also should be aware of a rarely encountered
potential diagnostic pitfall at the light microscopic
level that was delineated herein. The association of
AOT with other established and recently proposed
odontogenic tumors was reviewed and analyzed and
reportedly recurrent AOTs were evaluated case by
case. Because of its consistently benign behavior, in
selected cases it may be possible to preserve the tooth
or teeth associated with the tumor provided on-going
follow-up is assured. Clinicians are encouraged to
publish only case reports of completely documented
nonclassic cases.
Acknowledgments
The author gratefully acknowledges the kind
assistance of the following individuals: the late
Professor Jens Pindborg for most enthusiastic en-
couragement to undertake odontogenic tumor re-

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354 351
search; Professor Jesper Reibel for incredibly patient
support during tedious research procedures; Dr. Lee
Slater for superb collegial discussions, manuscript
review, advice, and extended practice coverage;
Drs. Lane Thomsen and Phil Sapp for library research
assistance; and Dr. Mamiko Kuriya for translation of
the Japanese case report. My special thanks to my
wife, Judy, for her understanding and patience.
References
[1] Harbitz F. On cystic tumors of the maxillae, and es-
pecially on adamantine cystadenomas (adamanto-
mas). Dent Cosmos 1915;57:1081–93.
[2] James W, Forbes JG. An epithelial odontome. Proc R
Soc Med 1909;2:166–75.
[3] Wohl MG. Tooth germ cysts of the jaw. Ann Surg
1916;64:672–9.
[4] Stafne EC. Epithelial tumors associated with devel-
opmental cysts of the maxilla. Report of three cases.
Oral Surg 1948;1:887–94.
[5] Thoma KH. Tumors of odontogenic origin. In: Oral
pathology. St. Louis (MO): Mosby; 1941. p. 945–6.
[6] Thoma KH. A contribution to the knowledge of the
development of the submaxillary and sublingual sali-
vary glands in human embryos. J Dent Res 1919;1:
95–142.
[7] Thoma KH. Adenoameloblastoma. Oral Surg 1955;8:
441–4.
[8] Bernier JL, Tiecke RW. Adeno-ameloblastoma. J Oral
Surg 1950;8:259–61.
[9] Bernier JL, Tiecke RW. Adenoameloblastoma: report
of nine cases. Oral Surg 1956;84:304–17.
[10] Robinson HBG. Proceedings of the Fifth Annual
Meeting of the American Academy of Oral Pathol-
ogy. Oral Surg 1952;5:177–8.
[11] Miles AEW. A cystic complex composite odontome.
Proc R Soc Med 1951;44:51–5.
[12] Oehlers FAC. An unusual pleomorphic adenoma-like
tumor in the wall of a dentigerous cyst: report of a
case. Oral Surg 1956;9:411–7.
[13] Lucas RB. A tumor of enamel epithelium. Oral Surg
1957;10:652–6.
[14] Ishikawa G, Mori K. A histopathological study on
the adenomatoid ameloblastoma—report of four
cases. Acta Odont Scand 1962;20:419–32.
[15] Smith JF. The controversial ameloblastoma. Oral
Surg 1968;26:45–75.
[16] Gorlin RJ, Chaudhry AP, Pindborg JJ. Odontogenic
tumors: classification, histopathology, and clinical be-
havior in man and domesticated animals. Cancer
1961;14:73–101.
[17] Shafer WG, Hine MK, Levy BM. Tumors and cysts
of odontogenic origin. In: A textbook of oral pathol-
ogy. 2nd edition. Philadelphia: WB Saunders; 1963.
p. 218–9.
[18] Abrams AM, Melrose RJ, Howell FV. Adenoamelo-
blastoma. A clinical pathologic study of ten new
cases. Cancer 1968;22(1):175–85.
[19] Philipsen HP, Birn H. The adenomatoid odon-
togenic tumor. Acta Pathol Microbiol Scand 1969;
75:375–98.
[20] Pindborg JJ, Kramer IRH. Histological typing of
odontogenic tumors, jaw cysts and allied lesions. (In-
ternational Histological Classification of Tumours,
No. 5). Geneva (Switzerland): World Health Organi-
zation; 1971.
[21] Kramer IRH, Pindborg JJ, Shear M. Histological typ-
ing of odontogenic tumours. 2nd edition. Heidelberg
(Germany): Springer-Verlag; 1992.
[22] Marx RE, Stern D. Oral and maxillofacial pathology.
Chicago: Quintessence; 2003.
[23] Bhaskar SN. Adenoameloblastoma: its histogenesis
and report of 15 new cases. J Oral Surg 1964;22:
218–26.
[24] Courtney RM, Kerr DA. The odontogenic adenoma-
toid tumor. Oral Surg 1975;39:424–35.
[25] Ajagbe HA, Daramola JO, Junaid TA, Ajagbe AO.
Adenomatoid odontogenic tumor in a black African
population: report of thirteen cases. J Oral Maxillofac
Surg 1985;43(9):683–7.
[26] Siar CH, Ng KH, Murugasu P. Adenomatoid odonto-
genic tumour: gross and histological examination of
45 cases. Singapore Med J 1987;28(2):180–9.
[27] Mendis BR, MacDonald DG. Adenomatoid odonto-
genic tumour. A survey of 21 cases from Sri Lanka.
Int J Oral Maxillofac Surg 1990;19(3):141–3.
[28] Awange DO. Adenomatoid odontogenic tumour
(adenoameloblastoma) – a review. East Afr Med J
1991;68(3):155–63.
[29] Odukoya O. Odontogenic tumors: analysis of 289 Ni-
gerian cases. J Oral Pathol Med 1995;24:454–7.
[30] Arotiba GT, Arotiba JT, Olaitan AA, Ajayi OF. The
adenomatoid odontogenic tumor: an analysis of
57 cases in a black African population. J Oral Maxil-
lofac Surg 1997;55(2):146–8.
[31] Philipsen HP, Reichart PA, Zhang KH, Nikai H, Yu
QX. Adenomatoid odontogenic tumor: biologic pro-
file based on 499 cases. J Oral Pathol Med 1991;20:
149–58.
[32] Philipsen HP, Reichart PA. Adenomatoid odonto-
genic tumor: facts and figures. Oral Oncol 1998;
35:125–31.
[33] Reichart PA, Philipsen HP. Odontogenic tumors and
allied lesions. London: Quintessence; 2004.
[34] Gabell D, James WW, Payne JL. Report on Odon-
tomes. London, 1914 as cited by Sprawson E. Odon-
tomes. Brit Dent J 1937;74:178–201.
[35] Thoma KH, Goldman HM. Odontogenic tumors. A
classification based on observations of the epithelial,
mesenchymal, and mixed varieties. Am J Pathol 1946;
22:433–71.
[36] Pindborg JJ, Clausen F. Classification of odontogenic
tumors: a suggestion. Acta Odont Scand 1958;16:
293–301.
[37] Gorlin RJ, Chaudhry AP, Pindborg JJ. Odontogenic

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354352
tumors. classification, histopathology, and clinical
behavior in man and domesticated animals. Cancer
1961;14:73–101.
[38] Gorlin RJ, Meskin LH, Brodey R. Odontogenic
tumors in man and animals: pathologic classification
and clinical behavior—a review. Ann N Y Acad Sci
1963;108:722–71.
[39] Gao YH, Yang LJ, Yamaguchi A. Immunohistochemi-
cal demonstration of bone morphogenetic protein in
odontogenic tumors. J Oral Pathol Med 1997;26(6):
273–7.
[40] Snead ML, Luo W, Hsu DD, Melrose RJ, Lau EC,
Stenman G. Human ameloblastoma tumors express
the amelogenin gene. Oral Surg 1992;74(1):64–72.
[41] Lucas RB, Pindborg JJ. Odontogenic tumours and
tumour-like lesions. In: Cohen B, Kramer IRH,
editors. Scientific foundations of dentistry. Lon-
don: William Heinemann Medical Books; 1976.
p. 240–50.
[42] Cina MT, Dahlin DC, Gores RJ. Ameloblastic adeno-
matoid tumors. A report of four new cases. Am J Clin
Pathol 1963;39:59–65.
[43] Spouge JD. The adenoameloblastoma. Oral Surg
1967;23(4):470–82.
[44] Baden E. Odontogenic tumors. Pathol Ann 1971;6:
475–568.
[45] Gorlin RJ, Chaudhry AP. Adenoameloblastoma. Oral
Surg 1958;11:762–8.
[46] Shear M. The histogenesis of the ‘‘tumor of enamel
organ epithelium. Br Dent J 1962;112(12):494–8.
[47] Giansanti JS, Someren A, Waldron CA. Odontogenic
adenomatoid tumor (adenoameloblastoma). Survey of
3 cases. Oral Surg 1970;30(1):69–88.
[48] Tsaknis PJ, Carpenter WM, Shade NL. Odontogenic
adenomatoid tumor: report of case and review of the
literature. J Oral Surg 1977;35(2):146–9.
[49] Geist SM, Mallon HL. Adenomatoid odontogenic
tumor: report of an unusually large lesion in the man-
dible. J Oral Maxillofac Surg 1995;53(6):714–7.
[50] Raubenheimer EJ, Seeliger JE, van Heerden WF,
Dreyer AF. Adenomatoid odontogenic tumour: a re-
port of two large lesions. Dentomaxillofac Radiol
1991;20(1):43–5.
[51] Takahashi K, Yoshino T, Hashimoto S. Unusually
large cystic adenomatoid odontogenic tumour of the
maxilla: case report. Int J Oral Maxillofac Surg 2001;
30(2):173–5.
[52] Gardner DG. The concept of hamartomas: its rele-
vance to the pathogenesis of odontogenic lesions.
Oral Surg 1978;45(6):884–6.
[53] Tagaki M. Adenomatoid ameloblastoma: an analysis
of nine case by histopathological and electron micro-
scopic study. Bull Tokyo Med Dent Univ 1967;14:
487–506.
[54] Lee KW. A light and electron microscopic study of
the adenomatoid odontogenic tumor. Int J Oral Surg
1974;3(4):183–93.
[55] Khan MY, Kwee H, Schneider LC, Saber I. Adeno-
matoid odontogenic tumor resembling a globulomax-
illary cyst: light and electron microscopic studies.
J Oral Surg 1977;35(9):739–42.
[56] Hatakeyama S, Suzuki A. Ultrastructural study of
adenomatoid odontogenic tumor. J Oral Pathol 1978;
7(5):295–300.
[57] Smith RR, Olson JL, Hutchins GM, Crawley WA,
Levin LS. Adenomatoid odontogenic tumor: ultra-
structural demonstration of two cell types and amy-
loid. Cancer 1979;43(2):505–11.
[58] Schlosnagle DC, Someren A. The ultrastructure of the
adenomatoid odontogenic tumor. Oral Surg Oral Med
Oral Pathol 1981;52(2):154–61.
[59] Yamamoto H, Kozawa Y, Hirai G, Hagiwara T, Naka-
mura T. Adenomatoid odontogenic tumor: light and
electron microscopic study. Int J Oral Surg 1981;
10(4):272–8.
[60] Moro I, Okamura N, Okuda S, Komiyama K, Ume-
mura S. The eosinophilic and amyloid-like materials
in adenomatoid odontogenic tumor. J Oral Pathol
1982;11(2):138–50.
[61] Poulson TC, Greer Jr RO. Adenomatoid odontogenic
tumor: clinicopathologic and ultrastructural concepts.
J Oral Maxillofac Surg 1983;41(12):818–24.
[62] Shimono M, Iguchi Y, Hashimoto S, Yamane H,
Tanaka Y, Yamamura T, et al. Intercellular junctions
in an adenomatoid odontogenic tumor. Bull Tokyo
Dent Coll 1984;25(4):145–57.
[63] El-Labban NG, Lee KW. Vascular degeneration in
adenomatoid odontogenic tumour: an ultrastructural
study. J Oral Pathol 1988;17(6):298–305.
[64] El-Labban NG. The nature of the eosinophilic and
laminated masses in the adenomatoid odontogenic
tumor: a histochemical and ultrastructural study.
J Oral Pathol Med 1992;21(2):75–81.
[65] Philipsen HP, Reichart PA. The adenomatoid odonto-
genic tumour: ultrastructure of tumour cells and non-
calcified amorphous masses. J Oral Pathol Med 1996;
25(9):491–6.
[66] Rick GM, Reibel J, Wewer U. Basement mem-
brane proteins in adenomatoid odontogenic tumors
[abstract No. 40]. Abstracts of the 38th Annual
Meeting of the American Academy of Oral Pa-
thology. Boston: American Academy of Oral Pa-
thology; 1984.
[67] Tatemoto Y, Tanaka T, Okada Y, Mori M. Adenoma-
toid odontogenic tumour: co-expression of keratin
and vimentin. Virchows Arch A Pathol Anat Histo-
pathol 1988;413(4):341–7.
[68] Mori M, Yamada K, Kasai T, Yamada T, Shimokawa
H, Sasaki S. Immunohistochemical expression of
amelogenins in odontogenic epithelial tumours and
cysts. Virchows Arch A Pathol Anat Histopathol
1991;418(4):319–25.
[69] Saku T, Okabe H, Shimokawa H. Immunohistochemi-
cal demonstration of enamel proteins in odontogenic
tumors. J Oral Pathol Med 1992;21(3):113–9.
[70] Nagai N, Yamachika E, Nishijima K, Inoue M, Shin
HI, Suh MS, et al. Immunohistochemical demon-
stration of tenascin and fibronectin in odontogenic

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354 353
tumours and human fetal tooth germs. Eur J Cancer B
Oral Oncol 1994;30B(3):191–5.
[71] Murata M, Cheng J, Horino K, Hara K, Shimokawa
K, Saku T. Enamel proteins and extracellular matrix
molecules are co-localized in the pseudocystic stro-
mal space of adenomatoid odontogenic tumor. J Oral
Path Med 2000;29:483–90.
[72] Takata T, Zhao M, Uchida T, Kudo Y, Sato S, Nikai
H. Immunohistochemical demonstration of an enamel
sheath protein, sheathlin, in odontogenic tumors.
Virchows Arch 2000;436(4):324–9.
[73] Takata T, Zhao M, Uchida T, Wang T, Aoki T,
Bartlett JD, et al. Immunohistochemical detection
and distribution of enamelysin (MMP-20) in hu-
man odontogenic tumors. J Dent Res 2000;79(8):
1608–13.
[74] Takahashi H, Fujita S, Shibata Y, Yamaguchi A.
Adenomatoid odontogenic tumour: immunohisto-
chemical demonstration of transferrin, ferritin and
alpha-one-antitrypsin. J Oral Pathol Med 2001;
30(4):237–44.
[75] Nagatsuka H, Siar CH, Nakano K, Tsujigiwa H,
Gunduz M, Choufuku H, et al. Differential expres-
sion of collagen Iva1 to a6 chains in basement mem-
branes of benign and malignant odontogenic tumors.
Virchows Arch 2002;441:392–9.
[76] Philipsen HP, Samman N, Ormiston IW, Wu PC,
Reichart PA. Variants of the adenomatoid odonto-
genic tumor with a note on tumor origin. J Oral
Pathol Med 1992;21(8):348–52.
[77] Hodson JJ. The gubernaculum dentis. Dent Pract
1971;21:423–8.
[78] Topazian RG, Simon GT. Adenoameloblastoma. Re-
port of three cases. Oral Surg Oral Med Oral Pathol
1960;13:1038–45.
[79] Das AK, Cooper WK, Medak H. Adenoameloblas-
toma: report of case. J Oral Surg 1964;22:434–8.
[80] Bell WM. Adenoameloblastoma in the maxilla. Re-
port of a case. N Z Dent J 1965;61:271–4.
[81] Toida M, Hyodo I, Okuda T, Tatematsu N. Adenoma-
toid odontogenic tumor: report of two cases and sur-
vey of 126 cases in Japan. J Oral Maxillofac Surg
1990;48(4):404–8.
[82] Philipsen HP, Srisuwan T, Reichart PA. Adenomatoid
odontogenic tumor mimicking a periapical (radicular)
cyst: a case report. Oral Surg 2002;94:246–8.
[83] Meyer I, Giunta JL. Adenomatoid odontogenic tumor
(adenoameloblastoma): report of case. J Oral Surg
1974;32(6):448–51.
[84] Khanna S, Khanna NN, Shrivastava AB, Gupta IM.
Adenomatoid odontogenic tumor. Ear Nose Throat J
1977;56(12):468–72.
[85] Dare A, Yamaguchi A, Yoshiki S, Okano T. Limita-
tion of panoramic radiography in diagnosing adeno-
matoid odontogenic tumors. Oral Surg Oral Med Oral
Pathol 1994;77(6):662–8.
[86] Tiecke RW, Shira RB. Adenoameloblastoma: report
of case. J Oral Surg Anesth Hosp Dent Serv 1961;
19:252–4.
[87] Link JF. Adenoameloblastoma of the maxilla: report
of case. J Oral Surg Anesth Hosp Dent Serv 1963;21:
432–4.
[88] Fahim MS, Elmofty SK, el-Attar AA. Adenoamelo-
blastoma: report of three cases. J Oral Surg 1969;
27(6):409–14.
[89] Layton SA. Adenomatoid odontogenic tumour. Re-
port of an unusual lesion in the posterior maxilla.
Dentomaxillofac Radiol 1992;21(1):50–2.
[90] Nomura M, Tanimoto K, Takata T, Shimosato T. Man-
dibular adenomatoid odontogenic tumor with unusual
clinicopathologic features. J Oral Maxillofac Surg
1992;50(3):282–5.
[91] Ghosh LSH. Adamantinoma of the upper jaw. Report
of a case. Am J Pathol 1934;10:773–89.
[92] Iwata K. The so-called adenoameloblastoma. Report
of a case. Acta Med Okayama 1967;21(3):121–32.
[93] Martis CS, Karakasis DT. Adenoameloblastoma.
Case report. Plast Reconstr Surg 1972;50(4):409–11.
[94] Goracy E, Stratigos GT. Adenoameloblastoma: report
of case. J Am Dent Assoc 1973;86(3):672–4.
[95] Khin U, Sanders B, Kasper E, Adilman H. Adeno-
matoid odontogenic tumor. J Oral Surg 1973;31(8):
607–12.
[96] Tajima Y, Sakamoto E, Yamamoto Y. Odontogenic
cyst giving rise to an adenomatoid odontogenic tu-
mor: report of a case with peculiar features. J Oral
Maxillofac Surg 1992;50(2):190–3.
[97] Bedrick AE, Solomon MP, Ferber I. The adenomatoid
odontogenic tumor: an unusual clinical presentation.
Oral Surg 1979;48:143–5.
[98] Oehlers FA. The so-called adenoameloblastoma. Oral
Surg Oral Med Oral Pathol 1961;14:712–25.
[99] Miyake M, Nagahata S, Nishihara J, Ohbayashi Y.
Combined adenomatoid odontogenic tumor and
calcifying epithelial odontogenic tumor: report of
case and ultrastructural study. J Oral Maxillofac Surg
1996;54(6):788–93.
[100] Aisenberg MS. Adamantinohemangioma. Oral Surg
1950;3:798–801.
[101] Thoma KH. The pathogenesis of the odontogenic
tumors. Oral Surg 1951;4:1262–80.
[102] Aisenberg MS. Histopathology of ameloblastomas.
Oral Surg 1953;6:1111–28.
[103] Shklar G, Cataldo E. Vascular ameloblastoma of
periodontium. Periodontics 1965;3:190–2.
[104] Lucas RB. A vascular ameloblastoma. Oral Surg
1957;10:863–8.
[105] Bernier JL. Benign tumors of the jaws. In: Tumors of
the odontogenic apparatus and jaws. (Atlas of Tumor
Pathology, Section IV—Fascicle 10a). Washington,
DC: Armed Forces Institute of Pathology under the
auspices of National Academy of Sciences—National
Research Council; 1960. p. 47.
[106] Brannon RB. Adenoid ameloblastoma with dentinoid.
Registry of Oral Pathology: case of the month 1–94.
Washington, DC: Armed Forces Institute of Pathol-
ogy; 1994.
[107] Waldron CA. The importance of histologic study of

G.M. Rick / Oral Maxillofacial Surg Clin N Am 16 (2004) 333–354354
the various radiolucent areas of the jaws. Oral Surg
1959;12:19–30.
[108] Andrade Sobrinho J, Carvalho MB, Rapoport A, Saba
LM. Odontogenic adenomatoid tumor of the mandi-
ble (adenoameloblastoma). Inter Surg 1978;63(1):
39–42.
[109] Matsumoto Y, Mizoue K, Seto K. Atypical plexiform
ameloblastoma with dentinoid: adenoid ameloblas-
toma with dentinoid. J Oral Pathol Med 2001;30(4):
251–4.
[110] Root RW. Adenoameloblastoma: report of case. J
Oral Surg Anesth Hosp Dent Serv 1963;21:515–8.
[111] Melrose RJ. Benign epithelial odontogenic tumors.
Semin Diagn Pathol 1999;16(4):271–87.
[112] Mallon HL, Sabes WR, Monaco F. Ameloblastic
adenomatoid tumor. Report of a case occurring in
the mandible. Oral Surg 1968;25:143–9.
[113] Sturgis SH, Holland DJ. Case reports from the max-
illofacial team, 6th General Hospital. Amer J Ortho-
dont Oral Surg 1946;32:635–55.
[114] Thoma KH. Benign central tumors of jaws of odon-
togenic origin. In: Oral surgery. St. Louis (MO):
Mosby; 1963. p. 987.
[115] Cina MT, Dahlin DC, Gores RJ. Odontogenic mixed
tumors: a review of the Mayo Clinic series. Staff
Meetings of the Mayo Clinic 1961;36:664–78.
[116] Fukaya M, Satoh H, Imai T, Umakoshi H, Kurauchi
T, Hanji J. A case report of adenoameloblastoma of
the maxilla. Jpn J Oral Surg 1971;17:155–7.
[117] Takigami M, Uede T, Imaizumi T, Ohtaki M, Tanabe
S, Hashi K. A case of adenomatoid odontogenic tu-
mor with intracranial extension. Neurol Surg 1988;
16(6):775–9.
[118] Damm DD, White DK, Drummond JF, Poindexter JB,
Henry BB. Combined epithelial odontogenic tumor:
adenomatoid odontogenic tumor and calcifying epi-
thelial odontogenic tumor. Oral Surg Oral Med Oral
Pathol 1983;55(5):487–96.
[119] Ledesma CM, Taylor AM, de Leon ER, Garze MP,
Jaukin PG, Robertson JP. Adenomatoid odontogenic
tumour with features of calcifying epithelial odonto-
genic tumor (the so-called combined epithelial odon-
togenic tumour): clinico-pathological report of
12 cases. Eur J Cancer B Oral Oncol 1993;29B:
221–4.
[120] Bernier JL. Tumors of the odontogenic apparatus.
In: The management of oral disease. 2nd edition.
St. Louis (MO): The CV Mosby Company; 1959.
p. 575.
[121] Dunlap CL, Fritzlen TJ. Cystic odontoma with con-
comitant adenoameloblastoma (adenoameloblastic
odontoma). Oral Surg 1972;34:450–6.
[122] Takeda Y. Induction of osteodentin and abortive
enamel in adenomatoid odontogenic tumor. Ann Dent
1995;54:61–3.
[123] Copete MA, Stakiw JE. Adenomatoid odontoma:
a case report of a rare lesion. Oral Surg 2001;92:543.
[124] Ide F, Kusama K. Adenomatoid odontoma. Oral Surg
2002;94:149–50.
[125] Tajima Y, Sakamoto E, Yamamoto T. Odontogenic
cyst giving rise to an adenomatoid odontogenic tu-
mor. J Oral Maxillofac Surg 1992;50:190–3.
[126] Takeda Y, Shimono M. Adenomatoid odontogenic
tumor with extensive formation of tubular dentin.
Bull Tokyo Dent Coll 1996;37:189–93.
[127] Allen CM, Neville BW, Hammond HL. Adenomatoid
dentinoma: report of four cases of an unusual odonto-
genic lesion. Oral Surg 1998;86:313–7.
[128] Slabbert H, Altini M, Crooks J, Uys P. Ameloblas-
toma with dentinoid induction: dentinoameloblas-
toma. J Oral Pathol Med 1993;21:46–8.
[129] Orlowski WA, Doyle JL, Salb R. Unique odonto-
genic tumor with dentinogenesis and features of uni-
cystic plexiform ameloblastoma. Oral Surg 1991;72:
91–4.
[130] Ng KH, Siar CH. Odontogenic keratocyst with denti-
noid formation. Oral Surg 2003;95:601–6.
[131] Raubenheimer EJ, van Heerden WFP, Noffke CEE.
Infrequent clinicopathological findings in 108 amelo-
blastomas. J Oral Pathol Med 1995;24:227–32.
[132] Zeitoun IM, Dhanrajani PJ, Mosadomi HA. Adeno-
matoid odontogenic tumor arising in a calcifying
odontogenic cyst. J Oral Maxillofac Surg 1996;54:
634–7.
[133] Ando T, Noguche I, Ide F. A case of calcifying
odontogenic cyst with ameloblastomatous prolifera-
tion and adenomatoid odontogenic tumor-like pro-
liferation. Jpn J Oral Maxillofac Surg 1985;30:
930–41.
[134] Takeda Y. Pigmented adenomatoid odontogenic tu-
mor: report of an undescribed case and review of
the literature of pigmented intraosseous odontogenic
lesions. Virchows Arch A Pathol Anat 1989;415:
571–5.
[135] Aldred MJ, Gray AR. A pigmented adenomatoid
odontogenic tumor. Oral Surg 1990;70:86–90.
[136] Warter A, George-Diolombi G, Chazal M, Ango A.
Melanin in a dentigerous cyst and associated adeno-
matoid odontogenic tumor. Cancer 1990;66:786–8.
[137] Larson A, Swartz K, Heikinheimo K. A case of mul-
tiple AOT-like jawbone lesions in a young patient—
a new odontogenic entity? J Oral Pathol Med 2003;
32:55–62.










![04-Notation How to write it down?adrion/520-f04/PDF/Lecture04.pdf · 2004. 12. 27. · CMPSCI520/620 Fall 2004- Lecture 04-Notation-II 9/19/04 „ Rick Adrion 2004 [except where noted]](https://static.fdocuments.in/doc/165x107/61289caea3d9df50e7608027/04-notation-how-to-write-it-down-adrion520-f04pdf-2004-12-27-cmpsci520620.jpg)