
Richard Schuster: Life Lessons and Legacy
166
Lifetime Lessons Learned The Legacy of Richard O Schuster Stephen M. Pribut, D.P.M., FAAPSM, FACFAS Past President, AAPSM Clinical Assistant Professor of Surgery George Washington University Medical School
-
Upload
steve-pribut -
Category
Health & Medicine
-
view
272 -
download
3
Transcript of Richard Schuster: Life Lessons and Legacy

Lifetime Lessons
Learned
The Legacy of Richard O Schuster
Stephen M. Pribut, D.P.M., FAAPSM, FACFAS
Past President, AAPSMClinical Assistant Professor of Surgery
George Washington University Medical School

Financial and Conflict Disclosure
I have no relevant financial relationships or
conflicts to disclose.
I have no conflicts of interest.

Thanks
• NYCPM for education, Fellowship,
Residency
• special thanks to the Department of
Orthopedics and Dr. D’Amico


Where Are We
Headed
• Introduction
• Schuster
• Lessons
• Case Studies
• Models, What’s real, what’s not

Thoughts
• “If in the last few years you haven’t discarded a
major opinion or acquired a new one, your
critical thinking capacity may be broken.”
• “All models are wrong, but some are useful.”
(George Box)
• Master the art of “what works”


Fellows in Jimbo’s Getting
Coffee

Wisdom of the Ages
• Over 600 years of experience
• Average over 35 years of experience
per practitioner
• Wisdom of the ages or wisdom of the
aged
• Eyes to the future

Searching For The
Truth
Richard O. Schuster,
DPM:
A Biomechanics IconAn up-close look at a man who helped shape this discipline
by Joseph C. D’Amico, DPM
Mandatory background reading
Biomechanics
Podopediatrics
Sports Medicine

Fellowship Lessons
• Learning and Leading By Example
• Case Studies
• Learn what works
• Be curious
Learn from treatment successes and failures

Looking Back

Podiatric Sports
Medicine was
Starting To Take
Off
Telstar I 1962
Springsteen 1974-75

1960’s-1970’s
Billy Martin with Catfish Hunter 19793 HRs in World Series Game

Shot heard round the world (1951)
Whitey Ford Rookie 1950
562 Foot Homer, No steroids.
Mostly 1950’s

Into The 70’s and Forward

When you want to give your feet
a rest, the NY Subway is the
very best.

Knowledge
Gathering: Sports
Medicine 1977• Journal articles - few on specific sport related topics
• Conferences
• Biomechanics Fellowships
• Preceptorships
• Orthopedic/Biomechanics Residency
• Reading Runner/Runners World
• Reading Physician & Sports Medicine
• AAPSM / ACSM

NYCPM & AAPSM
1977“Post Graduate Course in Sports Medicine”

Early Articles
• Runner’s Knee - Sheehan
• Survey of running injuries -
Stanley James
• Immunity to heart disease
for marathoners - Tom
Bassler
–Jim Fixx ultimately
disproved an incorrect
theory.
What does legacy mean?

Definition of LEGACY
1
: a gift by will especially of money or other personal property :bequest
2
: something transmitted by or received from an ancestor or predecessor or from the
past <the legacy of the ancient philosophers>
3
:
anything contributed or created by someone who is no longer living or active and which continues to be
of influence or impact.
Examples: This esteemed university is the great legacy of its enlightened founder.The introduction of the term "rock 'n' roll" is part of the legacy of famous disc jockey Alan Freed.
Synonyms
bequest, birthright, heritage, inheritance, patrimony
Related Words
heirloom; bestowal, gift, offering, present
Origin:

Wisdom: the ability to identify truth and
make correct judgments on the bases of
previous knowledge, experience and
insight.
The Wisdom Pyramid

Podiatric Sports Medicine
Podiatric sports medicine was an important force in
putting modern podiatric medicine on the map.

Richard Schuster receives the Robert Barnes Service Award
Dr. Schuster’s Special Role In Sports Medicine


Great Moments In Running History
“Dr. Schuster gives George
Sheehan his first pair of
orthotics.” (1971)

“Never trust a thought that comes to you while
sitting.”

Lore of Running: Tim Noakes
“Only when I attended the 1976
New York Academy of Science
Conference on the Marathon
and heard the presentations by
George Sheehan, Richard
Schuster, and Steven
Subotnick did I begin to
appreciate that attention to my
running shoes and the use of
an orthotic might cure my injury.
These measures worked.”

New York Academy of Science:
1976 Symposium on the Marathon
Schuster
Subotnick
Sheehan
Bassler
Noakes
Over 30 Years Later: Still Legendary

Runner’s Handbook: Bob Glover
...George Sheehan’s writings
about podiatrist Dr. Richard
Schuster’s pioneer work with
orthotics for runners led me to
Schuster’s office.
“Then came the great
discovery: My knee pain didn’t
need surgery, just exercises
and orthotics.
It Worked!”

Many go too far too fast too soon. Then, explains
Schuster, 62, "the body begins to break down. It's
like an old jalopy: good enough to get you to the
supermarket, but if you try to run it in the Grand
Prix, it'll fall apart."
Schuster also has worked extensively with brain-damaged children
whose balance system is not functioning properly. His shoe
modifications and inserts allow many afflicted children to walk with
increased stability. "That's the exciting work," he says.
Working out of a small office in Queens,
Schuster uses a tape measure, a
carpenter's level and a mirror, among
other tools, to amass 80 pieces of
information about the ailing foot.

The Runner Magazine 1978-1987

The Runner Magazine 1978-1987
Dr. Schuster was the “Podiatric Editor” and Dr. Sheehan
was the “Medical Editor”.
Also featured: George Hirsch, David Costill, Hal Higdon,
Tom Fleming, Edwin Moses, Bill Rodgers, Frank Shorter,
Craig Virgin, Nina Kusick, and Marty Liquouri.
Sold by Ziff-Davis to CBS to Rodale which merged it with
Runner’s World.
Many hoped the April, 1987
issue was an April Fool’s Issue.

The Runner Magazine: Foot Works
Case studies, tips on injuries, analysis of new
features in shoes, insoles, socks, running trends.
If you did everything as Schuster did 30 years ago,
you’d be a great clinical practitioner.
If you made clinical observations as he did, you’d
do far better than you do now.

The Runner Magazine: Foot Work
Bad habits of running
Morton’s neuralgia
Tarsal tunnel syndrome
Ankle sprains
Blisters
Stress fractures
Forefoot running
Shoe changes
Shoe cushioning
Shoe insoles
Women’s injuries
Children’s injuries
Recurrent stress
fractures
Stretching
Topics:

The Runner Magazine: Foot Work (April 1984)
Bad Habits of
Running:
Too much, too soon.
Changing running
style.
Not stretching.
Faulty stretching.

Compared pre-1978 and post 1978
• Second metatarsal most often
• Moments of force (bending
forces)
• Practical means of treatment
• Early diagnosis - bone scan
Still used term
“pre-stress
fracture”.
Stress Fractures 1972-1982

"Runners with low-arched feet generally don't
have to worry," says Schuster. "The runner
with high-arched feet is usually the one with
more problems.”
Authored many “Body Works” columns
Overtraining
Limb length discrepancy
Practical & educational


Biomechanical Forces of Good and Bad
Did pop culture have an impact in1977?
What did long experience imply in this mysterious field?

The Force:
Newton v. Lucas
• Forces may be good or
evil
• Injunction to measure
and determine abnormal
forces
• Train sense of intuition
• An eternal battle
Forces of Good and Evil

Moving On: The Clinician

Full Definition of CLINICIAN
1 : a person qualified in the clinical practice of medicine, psychiatry, or psychology as distinguished from one specializing in laboratory or research techniques or in theory
2 : a person who conducts a clinic
Origin: 1870-1875; from “clinic” + ian
Word Origin & History
clinician1875, from Fr. clinicien, from L. clinicus (see clinic).
Schuster: Respected For
His
Clinical Expertise• Patients and Athletes
• Print media
• Running Books
• Running Magazines and Columns
–Runner Magazine
–Runner’s World
• Inspired athletes to become podiatrists
Ideal Clinician
• Dr. Schuster exhibited many of the
characteristics of an ideal clinician
• His example stood as a life lesson to
many
Character
• Humble
• Attentive
• Focused
• Clear thinking
• Honest
• Sincere
• Goal directed
• Results oriented
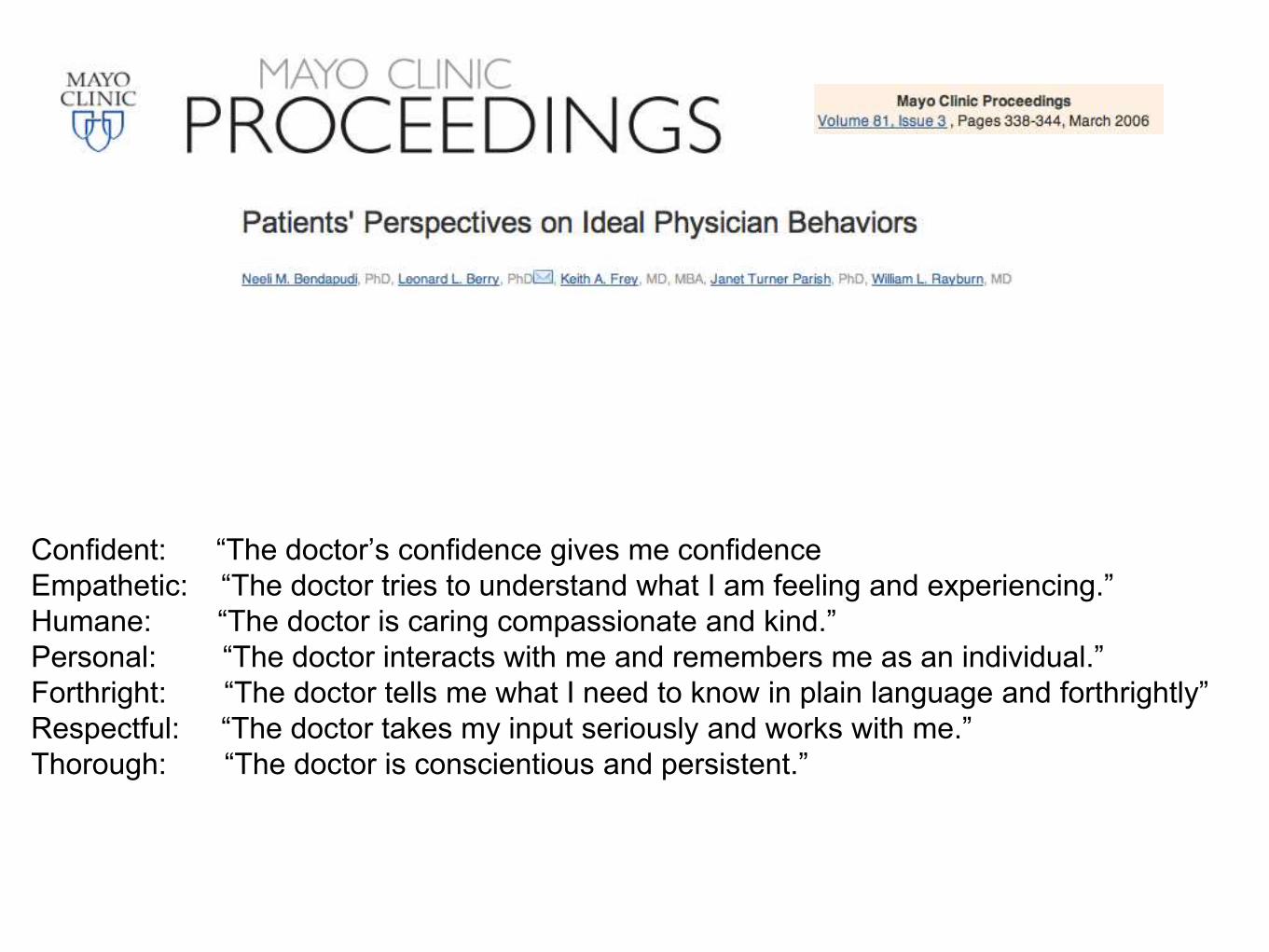
Confident: “The doctor’s confidence gives me confidence
Empathetic: “The doctor tries to understand what I am feeling and experiencing.”
Humane: “The doctor is caring compassionate and kind.”
Personal: “The doctor interacts with me and remembers me as an individual.”
Forthright: “The doctor tells me what I need to know in plain language and forthrightly”
Respectful: “The doctor takes my input seriously and works with me.”
Thorough: “The doctor is conscientious and persistent.”

Standards in Clinical
SkillsProject Professionalism of the American Board of Internal Medicine
has outlined:
specific values, including humanistic and communication
behaviors expected of their membership
The Outcome Project of the Accreditation Council for Graduate
Medical Education requires all accredited residency programs:
to address the training of physicians in 6 core competency
domains:
patient care
medical knowledge
practice-based learning and improvement
interpersonal and communication skills, professionalism
systems-based practice

Seven Habits of Highly Effective Clinicians
Demonstrate aspects of ideal
physician behaviors.
The traits described are from
the interview transcripts and
patient focus groups.
Personal observations of the
research team are included.


Confident
• Makes use of state-of-the-art medical practices
• Applies experience in treating specific medical
conditions or performing procedures
• Is not disturbed by patient's queries about
medical information acquired from other
sources (regardless of accuracy or inaccuracy)
Is at ease in the presence of patient, family
members, and medical colleagues

Empathetic• Makes eye contact with the patient as
well as family members
• Correctly interprets patient's verbal and
nonverbal concerns
• Repeats patient's concerns
• Shares personal stories that are
relevant
Speaks in a sympathetic and calm tone of
voice
• Makes eye contact with the patient as
well as family members


Humane
• Uses appropriate physical contact
• Is attentive, present to the patient and
the situation
• Indicates willingness to spend adequate
time with patient through unhurried
movements


Personal
• Asks patients about their lives
• Discusses own personal interests
• Uses appropriate humor
• Acknowledges patient's family
• Remembers details about the patient's
life from previous visits

Forthright
• Doesn't sugarcoat or
withhold information
• Doesn't use medical
jargon
• Explains pros and cons of
treatment
• Asks patient to recap the
conversation to ensure
understanding

Respectful• Offers explanation or apology if patient is kept
waiting
• Listens carefully and does not interrupt when the
patient is describing the medical concern
• Provides choices to the patient as appropriate but is
also willing to recommend a specific course of
treatment
• Solicits patient's input in treatment options and
scheduling
• Takes care to maintain patient's modesty during the
physical examination

Thorough
(most often mentioned)
• Provides detailed explanations
• Gives instructions in writing
• Follows up in a timely manner
• Expresses to patient desire to consult
other clinicians or research literature on
a difficult case
Handwrite
highlights and
directions and use
handouts as
needed.
Patients as Detectives:
Clues About The
Office• Functional clues
–Lab reports - accurate, not “missing”
–Check on allergies before Rx
• Mechanical clues
–Comfort, sights, sounds, smells, textures
• Humanistic
–Behavior and appearance of physician
• Word choice, tone, enthusiasm, body language,
appearance
These Clues
create the
service
experience.

Practical Suggestions
1. Eye contact—is a basic sign of connecting, listening and caring.
2. Partnership—in a healthcare relationship is not a one-way proposition.
3. Communication—also works in two directions. Understanding needs. Understanding solutions.
4. Time—is what physicians have little of, and what patients want from physicians. They do not want to feel rushed.
Rapport begins before you say hello…
Shake hands
Apologize if you are late
Introduce yourself by first and last name “Good
morning Mr. Smith, I’m Billy Ray Cyrus.”

On To The Next
One? Jay-Z

One Toolkit Is Always
Available
• Brain
• Eyes
• Ears
• Hands

Devices
• Goniometer
• Kurzweil device
• Postage scale

Old School
Computers (pre
1980’s)

Supercomputer
Equivalent
Other Tools:
Old & New• EDG - Father of EDG - M. Polchaninoff/Langer Labs (1977 -
NYCPM Fellow)
–F Scan
–Dartfish
• Internet forums
–PM Magazine, Podiatry Online, Podiatry-Arena, Bartold
–Social media: bane or blessing?
• iPhone
–Data & programs in your hand
• Online forums
• Traditional Journals
Schuster:
Used Careful and Methodical
Evaluation
• Skepticism of unsubstantiated research
–Bayes theorem
• First to note problems of over-stretching

Clinical Observations
& Problem Solving
• Listen
• Observe
• Think
• Solve
• Fix
“If I had an hour to solve a problem, I’d spend 55 minutes
thinking about the problem and 5 minutes thinking about the
solutions” – Einstein

If WD-40 doesn’t fix it, duct tape is the answer.

Gait Analysis: Out Of The Box Thinking
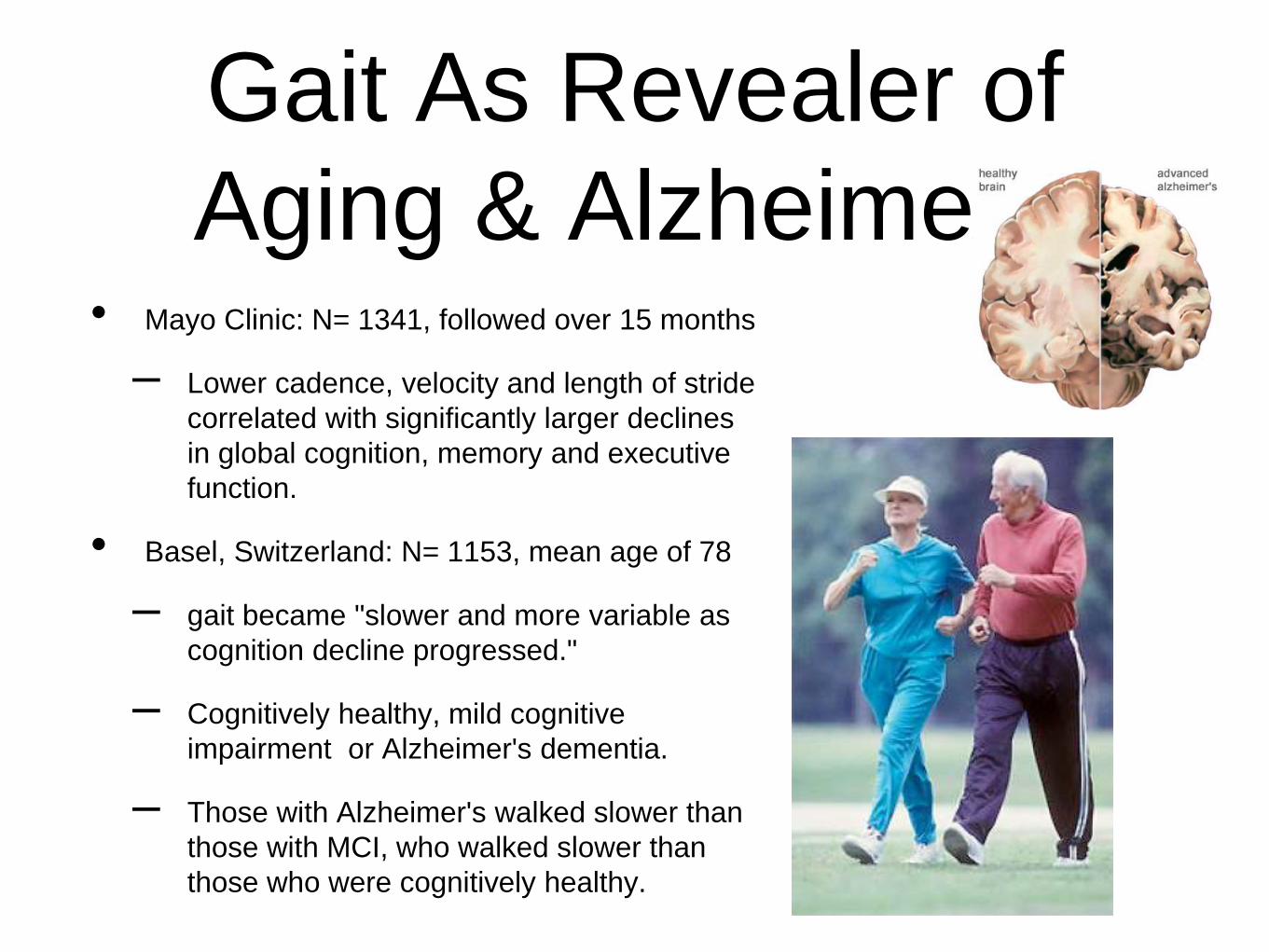
Gait As Revealer of
Aging & Alzheimer's• Mayo Clinic: N= 1341, followed over 15 months
– Lower cadence, velocity and length of stride
correlated with significantly larger declines
in global cognition, memory and executive
function.
• Basel, Switzerland: N= 1153, mean age of 78
– gait became "slower and more variable as
cognition decline progressed."
– Cognitively healthy, mild cognitive
impairment or Alzheimer's dementia.
– Those with Alzheimer's walked slower than
those with MCI, who walked slower than
those who were cognitively healthy.

Simplicity &
Simplexity• Scale Test
– Shoe flexibilty
• Scaled down
– Finger Test
• Diagnostics Use Occam’s Razor. Select the
simplest of all competing hypotheses. The one
with the fewest assumptions.

Measurements
• Navicular drop
• Total varus (Dr. Skliar
discussed earlier)
• Shoe flexibility
–Peter Cavanaugh
–Richard Schuster

Orthotics:
What are they? How do they work?
“An in-shoe medical device which is
designed to alter the magnitude and
temporal patterns of the reaction
forces acting on the plantar aspect of
the foot”
Kevin Kirby

Kirby on Schuster
• Kirby mentioned R O Schuster as a
major influence on his choosing
podiatric biomechanics as a field of
interest.
• Kirby calls Schuster one of the important
historians of the profession. (Schuster
1974. JAPA History of Orthopedics in
Podiatry)

Orthotics:
What are they? How do they work?
How do they work? By altering force application, direction,
magnitude.
Thoughts: Kinematics (motion) or Kinetics (forces)
Conformity of orthotic to foot (foot orthotic conformity and
orthotic topography)
Frictional characteristics
Deformation of device under load

Are these Orthotics?
They changed the thinking of many in one journal article...
But, I look to Magritte for the answer!


Old Orthotic Rx
• Material
• Top-cover
• RF Posting
• FF Posting
• Accommodations and modifications

Old School Root
Orthotic:
Rohadur• The cast is altered significantly during
manufacturing process
• Too narrow to be truly effective
• Very often there was too much arch fill
• Forefoot balancing
–With bad casting technique
Modern Orthotic: Features
(What Dr. Schuster Used In His Orthotics)
• Deep heel cup
• Minimal cast correction
• Good contour to foot
• Wide enough to do the job
• Functions also at talo-navicular and C-C joint and midfoot
• Anatomically correct accommodations
–Sesamoid/1st Met
–Sweet spots - navicular/heel
• Bevel rear foot post when needed

The Clash of the
Cast(ing) Technique
Text
Old: Semi weight bearing or non-weight bearing
New: Wipe out or enhance a plantar flexed first ray

Negative
Impression
Capture
Earlier: Tracings, Trays of Plaster or
Grease.
Plaster Bandage
Casting
Reed E.N.: A simple method for making
plaster casts of feet. JBJS (1933).
17:1007

New Orthotic Rx
• Kirby Skive
• Inversion of cast (Blake or less than Blake)
• RF posting material
• RF post
• Thickness of shell, material choice
• Additions/Modifications
• Plantar fascial groove

Schuster: Impact
On Orthotic
Modifications
Modifications below polypropylene shell. Adding felt or other
material to increase “arch support” and firmness. (Kirby:
Newsletter (Aug 2013))
Thinning shell by grinding in area of arch to make it more
flexible.
(Medial or lateral) Decrease bevel of heel.
Orthotic design has ultimately swung around to many of what
Schuster proposed and practiced


3 Things That Don’t
Exist
(as described)
• Unicorns
• Metatarsalgia as a Condition (It is a
symptom not a diagnosis.)
• Cuboid Syndrome
Or are less commonly seen than diagnosed
Unicorns

Metatarsalgia

3 Things Not To Miss
• Plantar plate injury - symptomatic, low
grade
• Peroneal tendinopathy brevis behind fibula
& longus tendinopathy (below foot)
• Lisfrank injury - symptomatic, low grade
• Today: Skipping Lisfrank and looking at
Sever’s

Internet Research:
MetatarsalgiaDefinition
Metatarsalgia is a condition marked by pain and inflammation in the
ball of your foot.
Metatarsalgia is caused by the compression of a small toe nerve
between two displaced metatarsal bones. Inflammation occurs when
the head of one displaced metatarsal bone presses against another
and they catch the nerve between them. With every step, the nerve is
pushed together by the bones and then rubbed, pressed again, and
irritated without relief. Consequently, the surrounding nerve tissue
becomes enlarged, with a sheath of scar tissue that forms to protect
the nerve fibers.
We can do better than this.

Reality
• Morton’s Neuroma
• Flexor tendinopathy
• Lumbricale tendinopathy
• Plantar plate injury
–Under-diagnosed entity
–Steroid injection or not?

Cuboid Syndrome
Don’t forget
everything else that
is right nearby!
Speed Cases: Better Than Speed
Dating

Case Study: Forefoot
Pain
• 57 year old master triathlete, 5k and
martial arts competitor. 9 months of
forefoot pain interfering with sports and
ADL.
Clinical History &
Evaluation• Chief complaint: 9 months of
undiagnosed and unresolved pain
below his second metatarsal.
• HPI: 2nd MTP & 2nd digit pain,
weakness at toe off. Trail running and
martial arts are difficult and painful for
this long time high level athlete.

Physical Examination
• Thorough examination - check planes
of deformity and MTPJ instability.
• Look for predisposing factors
• Provocative tests: push-up, book-curl
test, Lachman, max-toe
flexion/extension & toe-off.
suggested readings: Gerard Yu (2002), Rich
Bouche lecture on MTPJ instability


Take Aways
• It isn’t always “just a hammertoe”
• Pay attention to signs, symptoms, exam
• Metatarsalgia is a symptom (like angina)
not a diagnosis

MTPJ Instability
• Related MTPJ instability:
–overlapping toes, crossover toes, pre-
dislocation syndrome, splay toes
• Planes affected
–Sagittal
–Transverse
–Combined
Pre-dislocation
Syndrome
Gerard Yu et. al., JAPMA 2002
“idea of idiopathic pain and instability of the
metatarsophalangeal joint is relatively new”
“can develop following jogging, tennis and
basketball or minor trauma.”
Can be viewed as intermediate level plantar plate
injury

Presentation
Yu et. al. 2002Late antalgic gait
Mistaken diagnoses are common
Feel “lump” or bruise at met head
Plantar plate involved (rather than “bursa”)

Pathomechanics
Review• Anatomy: Second Digit - 2 dorsal interossei, no
plantar interossei, medial first lumbricale
• Primary (chronic) deforming force: EDL
• Primary digital flexor: Interossei
• Dynamic digital stabilizers: Interossei and
lumbricales
• Static digital stabilizers: PLANTAR PLATE,
collateral ligaments (also capsule and plantar
fascia)
Key: Role of Plantar
Plate
• Plantar plate is the primary static
stabilizer
• Dynamic stabilization is by intrinsic and
extrinsic muscles
–But is dependent upon intact plantar
plate
Must Read: Yu JAPMA April 2002 182-199

Function of Digits
• Assist balance, proprioception
• Aid in force transfer forward

Plantar
plate/Predislocation
Syndrome
• Pain localized to plantar MTPJ
• Negative tuning fork test
• X-rays - no change in early stage
• Bone scan can show uptake at MTPJ

• Minor trauma may be recalled
• Onset acute or subacute (occ. chronic)
• Digital contracture - late stage
• Positive vertical drawer test
• Absent Moulder sign
• Subtle malalignment of toe
Evaluative Process
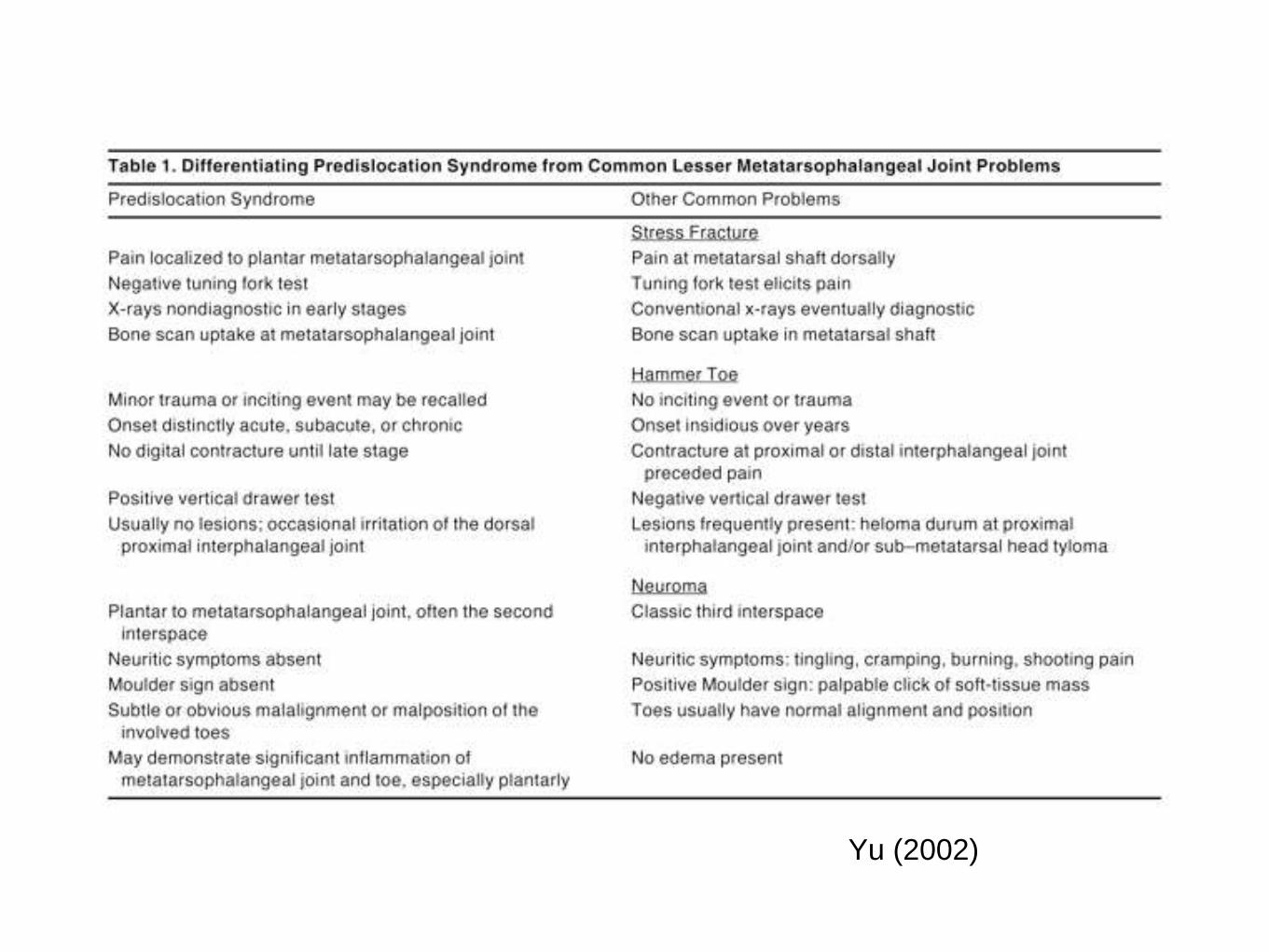
Yu (2002)
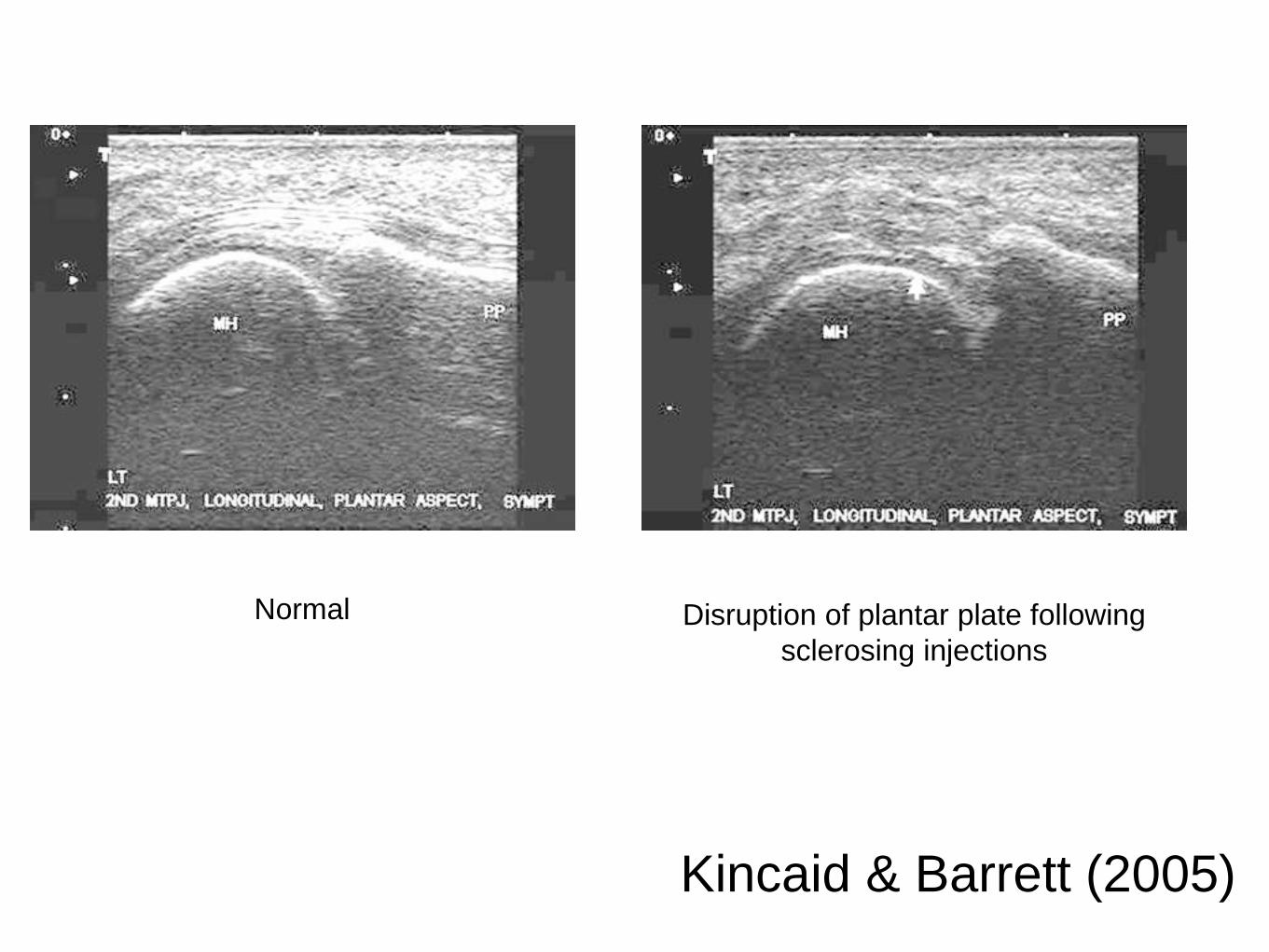
Kincaid & Barrett (2005)
Normal Disruption of plantar plate following
sclerosing injections

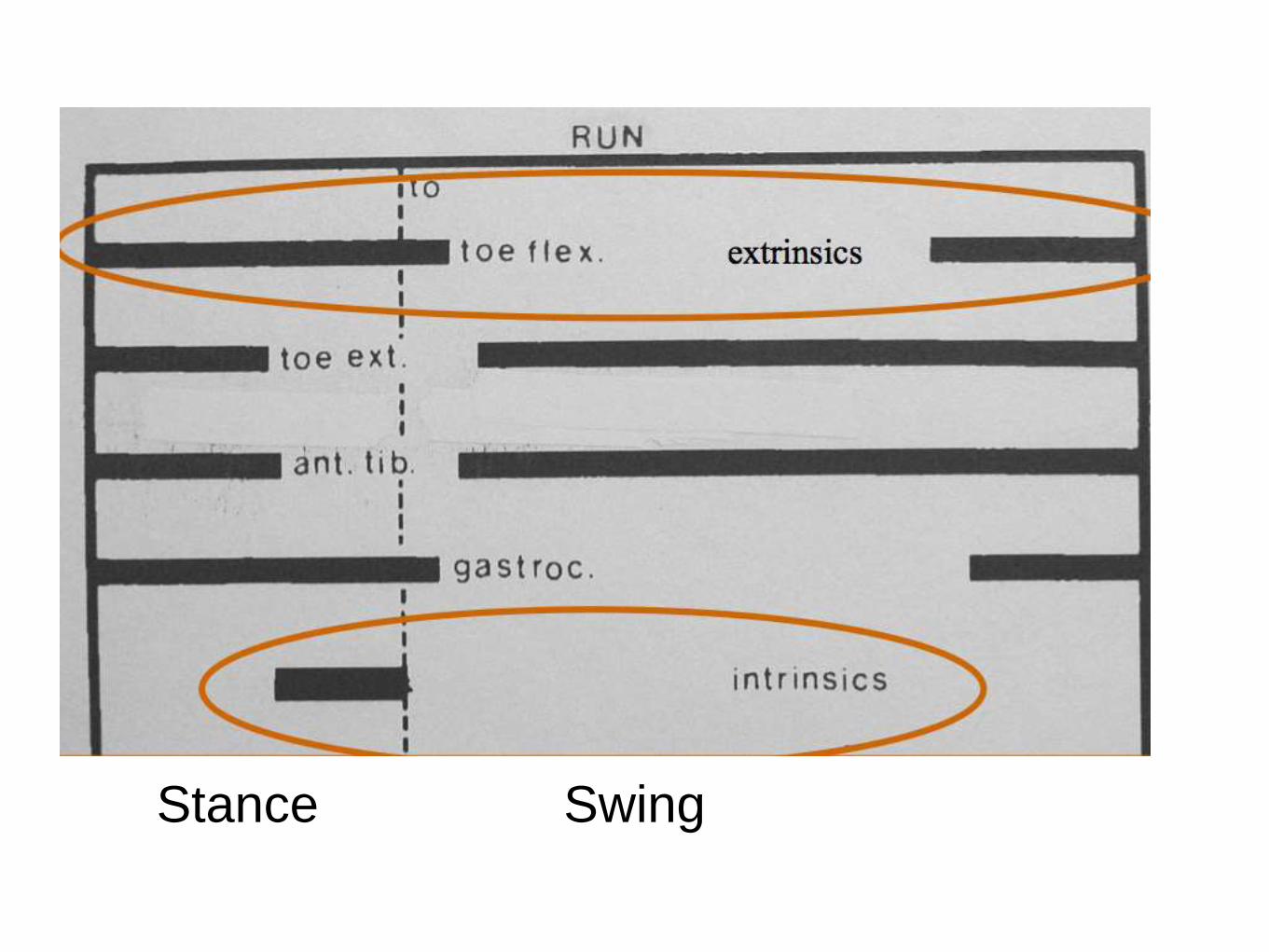
Stance Swing

Intermediate Stage
Plantar Plate Injury: Tx
• Immobilization
–6 to 12 weeks
• Plantar flexion exercises
• Splinting
• Orthotic
–Control abnormal biomechanics
–No anterior bevel
–Poron added from mets to sulcus
• Surgery
Resolved with conservative
therapy. Resumed 5Ks and
martial arts.

Case 2: Mild Plantar Plate
Injury57 year old female runner with a 30 year running
streak.
Pain below right 2, 3 metatarsals
Began after sprint training. Worsened by toe pull
ups and toe press against wall stretch.
Negotiated Treatment
(Case 2)Relative rest. Decrease running from 6 to 4
miles.
Toe curls - strengthen flexors, intrinsics
No sprints, speed work
Avoid awful stretches
Midfoot/heel contact - not forefoot
400’s in future: at sustainable speed with
rest between 400’s not sprint straightaways,
walk curves.

Summary:
Metatarsalgia
• Less than optimal diagnosis
• “Like saying ‘headache’ - S. Bartold
• Under-diagnosed: Plantar Plate Injury
• Lumbricale tendinopathy

Enthesopathy
• Spondyloarthropathies
• Achilles
• Plantar fascia
–Plantar fasciopathy

Case Study: Juvenile
Heel Pain
• Presentation: 8 year old child, student,
and basketball player presents with 6
months of pain in both heels, with the
right foot more symptomatic than the
left.
• He is hoping for an NBA career.

Is Sever’s Disease
Properly Named?

Clinical History &
Evaluation• Chief complaint: 6 months of undiagnosed
and unresolved pain both posterior and
plantar heels.
• HPI: Reports pain during jumping and
running. It has minimally improved with
short term rest, but returns.
• Mom will not let him run cross country due
to pain and fear of he may need orthotics.
Dad thinks it may be Achilles tendinopathy.

Physical Examination
• Thorough examination - examine area
of chief complaint and nearby
structures.
• Look for biomechanical risk factors
• Evaluate for equinus, Achilles and
hamstring tightness and pronatory
forces. suggested readings: JAPMA September
2013

Left foot
Right foot
“Sclerosis is
often seen but
not
diagnostic.
Likewise
fragmentation
.”

Sever’s “Injury”, Disease, or Phenomena?
Inadequate Classical treatment:
Wait until growth plate fuses
Rest
Heel Lift
Growth center abnormality
is not always present
may be present in normals
associated with athletic activity
recent articles call it a “clinically diagnosed disorder”
Seaver the phenomena

Juvenile Osteochondroses, Stammel,
CA Radiology Oct 1940
Lifespan of Misinformation: Endless
The opportunity for education, is always present.

Is Sever’s likely another -opathy not an -itis?
Calcaneal Apophysopathy
No biopsy material
No evidence of “inflammation”
Clearly traction related
After tendinopathy, fasciopathy, why not?


Calcaneal Apophysopathy
Heel pain on one or both sides with 60% having bilateral symptoms
Heel pain with running, jumping
Antalgic gait
Pain elicited when the heel is compressed medially and laterally at
the apophysis
Often classical radiographic signs are present
Growth center appears in boys aged 7-8 and fuses at 15-17
Growth center appears in girls aged 4-6 and fuses at 12-14

Calcaneal Apophysopathy
Acute Care:
Rest, Ice, Elevation.
Relative rest - allow pain free activity
Limit motion using: Heel lift or Pneumatic Walker
In The Long Run:
Evaluate biomechanics carefully
Heel lift
Gentle calf stretching
Intrinsic muscle group strengthening (toe crunch)
Tibialis anterior strengthening
Custom orthotics may be needed
Gradual return to activity

Case Comparison: The Runner
March 1984
cc: 25 yo♀Lateral ankle and leg pain while running
•Ankle sprain - untreated 10 days
•Brief use of soft cast
•5-6 week rest
•Pain

Schuster (Footwork Column):
•Warned of the danger of waiting for
treatment of ankle injury.
•Used lateral wedge below insole.
•Lateral buttress on counter and lateral
aspect of shoe.
•Recommended exercises for the ankle.
•Felt further evaluation and surgery might
be needed if this did not work.
Case Comparison: The Runner
March 1984

Case Comparison: The Runner
March 1984
30 years later..
The lateral wedge holds up and the buttress also.

Case Comparison: The Runner
March 1984
Areas for improvement:
• Improved assessment of ankle injury via better
physical examination, anterior drawer test,
imaging.
• Pneumatic cast boot = better immobilization
• Longer immobilization
•Wobble board training - muscle strength,
balance, proprioception
Case Comparison: The Runner
March 1984
Orthotic Improvements
No lateral bevel
Forefoot - Valgus wedge 3°
Orthotic for contour to foot not insole
(Reverse Kirby skive and -Inversion casting)
Exercise Improvements
Wobble board not just rubber bands and ROM
Bracing or taping
Shoes - avoid mushy, over-cushioned shoes

Case Study:
Lateral Ankle Pain in Olympic Triple
Jumper
• 26 year old elite Triple Jumper
• Lateral foot and ankle pain for nearly a
year

Case Study:
Lateral Ankle
• Symptoms present in training shoes,
running on grass
• Shoe role in pain causation - Mizuno -
soft & squishy
• Previous treatment: Injection at PB
tendon behind ankle: FAIL

Case Study:
Lateral Ankle
• Physician suggestion via phone: Sinus
tarsi injection
• My suggestion before examination:
“Let’s check it out and see if it is
something else and we can do
something mechanically.”

Case Study:
Lateral Ankle• Somewhat tender at peroneus brevis below
ankle
• My suspicion: Training Shoes
• Symptoms present in training shoes, running
on grass
• Symptoms not present in competition flats and
track work.
• Shoe role in pain causation - soft & squishy
(miz)

Treatment
• Change to more solid shoe, different brand
• Add 1/8 to 1/4” heel lift to decrease forces
on PB tendon
• Wobble board therapy + Calf/Posterior
muscle group stretching
• Consider orthotic as discussed above:
–No lateral bevel, 2 degree valgus post to
sulcus for training shoe only


Belief Systems
“Beliefs held by patients about their health and
illness are central to how they present, (and)
respond to treatment”...
Peter Halligan, (2007) The Psychologist, 20:6 358
Beliefs are pre-existing notions and typically
involve strong personal endorsement for a
proposition considered true and beyond
further inquiry.e.g. Mom of 8 year old whose “feet are still growing”

Competing Belief Systems

Models & Principles
• Schuster - clinically oriented
• Root - neutral position
• Kirby - STJ Axis
• Dananberg - Sagittal plane
• Nigg - muscle tuning

Schuster on Root– “...research by Inman, Strauss, Elftman,
Manter, Hicks, Hibbs, and many others
was put together in a meaningful
biomechanical concept by Dr. Merton L.
Root”
– “Root...emphasized the relationship of the
forefoot to the rearfoot and provided
..validity for the comparatively hazy
balance concepts of earlier years.
Misunderstanding
Root
• There is a difference between the
Aristotelian average and the Platonic
ideal.
• Ideal normal is different from average
findings.
• The ideal was lost to the mundane.

Kirby• Foot orthoses have effects
on Midtarsal/Midfoot Joints
• Plantar Ligaments and
muscles cause a
longitudinal arch raising
moment
• Longitudinal arch stops
lowering at position of
rotational equilibrium
• Foot orthosis acts to
reduce tensile stress on
plantar soft tissue
structuresillustration: Kevin Kirby

Endless Debates on
MTJ Axis

And More
Simon Spooner trying to make
Kevin Kirby think hard
cop: position 1; mtj: position a; STJ axis i =?cop position 2; mtj: position a; STJ axis i =?cop position 3; mtj: position a; STJ axis i =?cop position 1; mtj: position b; STJ axis i =?cop position 1; mtj: position c; STJ axis i =?



New paradigms in shoe design lead to new injuries.
Don’t wear more shoe than you need or less
shoe than works.
What would Dr. Schuster say today?

Schuster on The Future of Running
Shoes
“running injuries vary year to
year in response to the latest
“advances” in running shoes. “
Changes in flexibility of the
shoe and the rigidity of the
heel counter may help some
runners but cause problems
for others.

Schuster on The Future of Running
Shoes
“As shoes get lighter with the use
of new materials, injuries may
result from less support and
cushioning.”
“Shoes must offer flexibility,
cushioning, support and they must
fit your feet.” (feel comfortable)

Schuster on Running
InjuriesOver cushioned shoes can create
problems.
Shorter strides can help hip and
gluteal problems.
Calcium balance and hormonal
issues contribute to women’s
stress fractures.
Heel lifts are not evil.
Stretch wisely.

Meme of “Shoes Bad, Barefoot Good”

Soil Classification

If we are going to use minimalist shoes, we need
maximal analysis of what we are running on.
Concrete is not the answer.

RESPECT &
RESULTS
Do your own casting and don’t use foam!

THE END IS HERE




















