RICHARD O. SCHAMP MD GEORGE W. BRETT MD CHIEF EXECUTIVE OFFICER CHIEF MEDICAL OFFICER ©AAHCM1.
100
Understanding HCC Coding in Home-based Primary Care RICHARD O. SCHAMP MD GEORGE W. BRETT MD CHIEF EXECUTIVE OFFICER CHIEF MEDICAL OFFICER ©AAHCM 1
-
Upload
conrad-hamilton -
Category
Documents
-
view
218 -
download
5
Transcript of RICHARD O. SCHAMP MD GEORGE W. BRETT MD CHIEF EXECUTIVE OFFICER CHIEF MEDICAL OFFICER ©AAHCM1.

©AAHCM 1
Understanding HCC Coding in Home-based
Primary Care
RICHARD O. SCHAMP MD GEORGE W. BRET T MD
CHIEF EXECUT IVE OFF ICER CH IEF MEDICAL OFF ICER

©AAHCM
Presenter: Richard Schamp, MD
• Family Medicine & Geriatrics x 30 yrs (rural PA with active home care practice, then urban St. Louis)
• Clinical Professor of FM & Geriatrics at Saint Louis University School of Medicine – started home visit program for residents & students
• Medical Director experience: Hospice, Home Health, Long Term Care and PACE
Disclosures• CEO of Capstone Performance Systems -- support
organizations/providers that care for vulnerable patients
• Risk Adjustment training for providers, Managed Care & PACE organizations x 10 yrs
2

©AAHCM 3

©AAHCM 4
• Discuss the Risk Adjustment methodology and relevance to home-based primary care practice
• Understand how complete and accurate documentation and coding supports good patient care
• Introduction to Official Coding Guidelines and comments on ICD-10
• Tips for accurate and complete documentation and coding of common conditions seen in typical home-based primary care practice
Objectives for Today

5
• NEVER submit false data or data (codes) that are not supported by documentation
• ALWAYS seek to be complete and accurate
• NEVER attempt to game the system
• ALWAYS attempt to systemize your game
Honesty is the best Policy
Disclaimer
©AAHCM

Triple Aim: 3 Value Vectors
©AAHCM 6

Quality vs. Quantity Value-based compensation Healthcare is shifting from FFS model to
pay-for-performance methods Payers will reward value and care
coordination- rather than volume and duplication
HHS testing and expanding new healthcare payment models
©AAHCM 7

HHS Payment Models
Category 1: FFS no link to quality Category 2: FFS with quality link Category 3: Alternative Models built on
FFS architecture Category 4: Population Based Payment
Value-Based Payment is Here to Stay
Source:
http://www.hhs.gov/news/press/2015pres/01/20150126a.html
©AAHCM 8
FFS Museum

Shifting Provider Payment Environment Two Shifts1. Increasing accountability for quality and total
cost of care2. Timeline:
1. 30% of Medicare payments in alternative payment models (categories 3 & 4) by the end of 2016
2. 50% of Medicare payments in alternative payment models (categories 3 & 4) by the end of 2018
3. Overall, 85% of payments in categories 2 through 4 by 2016 and 90% by 2018
3. Most contracted arrangements will involve risk-adjusted payments
©AAHCM 9

©AAHCM 10
Payment Mechanism Shift
FFS
Time
Shared Risk/Savings

©AAHCM 11
How does this make you feel so far?

How Does Risk-based Payment Model Work?CMS MONTHLY MEDICARE PAYMENT
• Capitated Payment for A&B costs• Benchmarks established for each County
~$750 -- $1300/mo
• Risk Adjusted amount for each member/enrollee
• Amount Changes Yearly
©AAHCM 12

Significance to Providers•Traditional: seriousness and severity of patient care indicated by E&M CPT® codes
•Higher level E&M codes identify serious encounters•utilizing more medical decision making•reimbursed at a higher rate
•In Risk Adjustment scenarios, these CPT® codes have no significance•Instead, diagnosis codes communicate the seriousness of medical decision-making
Risk-adjusted Plans are paid based on ICD-9 Codes,
based on DIAGNOSES, not on procedures.©AAHCM 13

Significance to Providers Documenting involves three main points:① Identify diagnosis as a current problem as opposed to a previous condition② Choose specific ICD-9 diagnosis code and ③ Support the diagnosis fully by documentation
14©AAHCM

15
• Medicare pays based on severity of illness for each enrollee
• ICD-9 is the specific language that is used to inform CMS the extent and severity of disease present
• Like any language, ICD-9 must be spoken properly.
• Failure to document and code correctly can lead to ◦ underpayment for your plan; i.e., Lost Revenue
◦ overpayment and violations of the False Claims Act
ICD-9 (10) is its own Language
©AAHCM

16
Risk Adjustment and
The False Claims Act
The False Claims Act prohibits: a) knowingly presenting (or causing to be
presented) to the federal government a false or fraudulent claim for payment or approval; and
b) knowingly concealing or knowingly and improperly avoiding or decreasing an obligation to pay or transmit money or property to the Government.
31 U.S.C. §3729(a)(1)
©AAHCM

17
The False Claims Act
• Any person who violates the FCA is liable for a civil penalty of up to $11,000 for each violation, plus three times the amount of the damages sustained by the United States.
31 U.S.C. §3729(a)(1)
©AAHCM

18
• Coding from a problem list (not current problems)• Submitting diagnoses (e.g. cachexia) with no support in
medical records for existence in that year.• Claiming current treatment for conditions better
characterized by “history of.” (e.g. acute stroke)• Submitting diagnostic codes from Labs/Radiology
Rpts/Rx’s without further documentation• Improperly linking complications and conditions to
increase risk score (e.g. linking diabetes and CKD without proper documentation)
• Targeted Coding: Pressuring coders to focus on high value diagnoses (e.g. malnutrition, Major Depression)
Improper Upcoding
©AAHCM

ICD-10• The ICD-10 transition date is October 1, 2015.
Get ready now for ICD-10.
• You don’t have to use 68,000 codes.As you do now, your practice will use a very small subset of the codes.
• You will look up ICD-10 codes just like you look up ICD-9.Alphabetic index and electronic tools available to help with code selection.
• Outpatient procedure codes aren’t changing.Transition to ICD-10 does not affect the use of CPT for outpatient coding.
• All FFS providers can conduct testing before ICD-10 transition.Contact Medicare Administrative Contractor for details about testing plans.
©AAHCM 19

ICD-10 v ICD-9 Comparison
©AAHCM 20
Tobacco Abuse
ICD-9-CM: 1 Code
ICD-10-CM: 5 Codes
Diabetes Mellitus
ICD-9-CM: 10 Codes
ICD-10-CM: 318 Codes
Fracture of Radius
ICD-9-CM: 33 Codes
ICD-10-CM: 1,818 Codes
Source: AHLA Institute on Medicare and Medicaid Payment issues

Coder’s Employment Relief Act? Between ICD-10 and the changes
associated with changing payment models, medical coding has never been more valuable.
Should your practice use a coder?◦ Depends on provider interest, skills and time◦ Out-sourcing coder is an option◦ Fresh models bring fresh scrutiny – compliance
with rules and regulations supported by coder/audits
©AAHCM 21

“Close Enough for Gummint Work” Doesn’t Cut it Anymore
©AAHCM 22

Under the Hood of RA How does the Risk Adjustment Model work? What are the key characteristics of the
Model? How is a risk score calculated? How much impact does a risk score have? How does incomplete documentation affect
it?
©AAHCM 23

24
• RA is a mathematical model designed for more accurate payments to Medicare Advantage and other capitated health plans
• Payment based upon health status of enrollees plus demographic data.
• Designed to predict illness costs covered by Parts A and B (Part C)
• Sicker members generate higher payments (to cover the costs of care)
Big Picture of Risk Adjustment
©AAHCM

25
• In March 2002, CMS chose CMS Hierarchical Condition Category Model (“CMS-HCC Model”) groups similar serious chronic medical conditions with similar costs of treatment into Hierarchical Condition Categories (HCCs), each with a “risk score”
• RA methodology has two inputs: ◦ Demographics◦ Diagnoses
• One output = HCCs (driving risk scores) • MA Plans and most other models (except PACE /
ESRD) use Version 22 (79 HCCs) for 2016 payments
Big Picture of Risk Adjustment
©AAHCM

CMS HCC Model is Prospective
• CURRENT demographics and diagnoses predict FUTURE expenses.
• Ultimately, payment in a given year is based on diagnoses submitted the PREVIOUS year.
• ICD-9 codes for dates of service in CY 2015 will be basis of payment in CY 2016
• (Health Exchanges use a concurrent model.)
©AAHCM 26

Risk Adjustment System (RAS)
All RAS factors are regressed SO THATAverage Medicare Risk Score = 1.000
(Based on FFS costs)
©AAHCM 27

28
Demographics: (approx. 0.330)◦ Gender◦ Age◦ How entered Medicare (disabled or age)◦ Medicaid status
HCC Component: (approx. 0.670)◦ Determined by diagnosis codes (ICD-9)
Risk Score ComponentsAverage Risk Score = 1.000
©AAHCM

29
Demographic FactorsDescription Score
Female70-74 Years 0.348 75-79 Years 0.437 80-84 Years 0.539 85-89 Years 0.667 90-94 Years 0.815
Male 70-74 Years 0.356 75-79 Years 0.442 80-84 Years 0.543 85-89 Years 0.683 90-94 Years 0.848
Medicaid Female Aged 0.151 Medicaid Female Disabled 0.085
Medicaid Male Aged 0.177 Medicaid Male Disabled 0.086
Originally Disabled Female 0.239 Originally Disabled Male 0.163
©AAHCM
• Gender• Age• OREM (disabled or
age)• Medicaid status

©AAHCM 30
Where do HCCs come from?
ICD-9 Codes(13,000)
Qualifying Dx Codes(~3400)
Diagnostic Groups(804)
Condition Categories
(189)
HCCs (79) Hierarchies
imposed

31©AAHCM
Examples of HCCsHCC Description Score
1 HIV/AIDS 0.470 2 Septicemia, Sepsis, SIRS/Shock 0.535 8 Metastatic Cancer and Acute Leukemia 2.484
12Breast, Prostate, and Other Cancers and Tumors 0.154
18 Diabetes with Chronic Complications 0.368 19 Diabetes without Complication 0.118 21 Protein-Calorie Malnutrition 0.713 22 Morbid Obesity 0.365 55 Drug/Alcohol Dependence 0.420 57 Schizophrenia 0.490
58Major Depressive, Bipolar, and Paranoid Disorders 0.330
75 Polyneuropathy 0.408 108 Vascular Disease 0.299 137 Chronic Kidney Disease, Moderate (Stage 4) 0.224 Note: these are not diagnoses, but categories that contain
diagnoses

32
Hierarchical◦ Payment based on more severe form of disease when
less severe form is also present in reporting period (e.g., PVD vs PVD w/complications)
Interactive◦ When certain diseases coexist, the model assigns
additional payment to recognize higher morbidity and costs than just adding the separate conditions
Additive◦ When unrelated diseases co-exist, the risk factors are
added together
The HCC model rewards: specificity and completeness
HCC Model Characteristics
©AAHCM

Hierarchy (Trump) Examples
33©AAHCM

34©AAHCM
• 78 yo woman,• Lives in 2-story row home
for past 50 years• Bi-polar daughter lives in
home with her (with her 2 children)
• Oxygen dependent• Personally catered annual
block party x 20 years• Multiple cats with fleas• Personal goal to survive to
80th birthday
Example of the HCC Model

35©AAHCM
Example of the HCC Model
o 491.21 COPDo 518.83 Respiratory Fail.
with O2o 327.3 Sleep Apneao 440.2 PVDo 585.4 CKD 4o 404.11 HTN w/CKD and HFo 416.8 Pulmonary Htno 428.3 Diastolic CHFo 427.89 SVTo 358.8 Neuropathyo 274.0 Gouto 285.29 Anemia o 721.9 Cervical spondylosiso 295.30 Major Depressiono 366.9 Cataracto 530.81 GERDo 389.9 Hearing losso 250.00 Diabetes Mellituso 250.40 Diabetes w. CKDo 250.70 Diabetes w PVDo 250.60 Diabetes w/Neuro
HCC Version 22
111 - COPD
84 - Cardiorespiratory Failure
108 - Peripheral Vascular Disease
137 – CKD Stage IV
85 - Congestive Heart Failure
96 - Specified Heart Arrhythmia
58 - Major Depression
18 - Diabetes With Complications
19 - Diabetes W/O Complications
Acti
ve P
rob
lem
s

©AAHCM 36
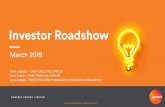
Risk Score Calculatio
n
Version 22Coefficients

37
Adjusted HCC Risk Score: 4.053 Beaver County Rate $790.24
PAYMENT/MO: ($750 * 4.053) =$3,040
Calculating Her PaymentAssume our Patient is living in Beaver County, PA, enrolled in MA Plan with a 4.5 Star Rating and a bid of $750
©AAHCM

Financial Impact Example
38©AAHCM

39
DIAGNOSISICD9 CODE
RXHCC NUMBER
RXHCC Score
Hypertension 401.9 88 0.244
Hypothyroidism 244.0 20 0.056
Hyperlipidemia 272.4 23 0.150
Osteoporosis 733.0 45 0.121
Depression (NEC) 311.0 62 0.122
Glaucoma (NOS) 365.00 113 0.232
Coronary Artery DisHistory of MI
414.01412.0
8989
0.1800.180
Diagnoses Unique to RxHCC Model(Document and submit all active diagnoses)
©AAHCM

©AAHCM 40
RA Model Run Timetable

Practical Matter – need to submit ALL diagnoses/year Only room for 4 codes on paper claim (or 8
if file electronically) Key – maintain good active problem list
and track which are submitted in calendar year
Annual assessment is another way – the MA plan collects the diagnoses on separate form and submits (no limit)
MA Plan may perform chart review and collect codes (no limit)
41©AAHCM

Face-to-Face To be eligible for risk adjustment, a
diagnosis must be documented in the context of a face-to-face visit.
42©AAHCM

Documentation Guidelines What are CMS expectations for medical
records? How do Official Coding Guidelines impact
us? Which common documentation pitfalls?
©AAHCM 43

44
• Importance of clear, complete, accurate documentation cannot be overstated.
• Each visit note • Reason for the visit• Findings from physical exam• Diagnosis (single or multiple) established with
medical decision making• Plan of care
• Note dated and signed by PCP w/credentials.• SOAP note form is common and acceptable • “Impression/Plan” approach better for
comprehensive assessments
Documentation in Medical Records
©AAHCM

Question 1 The following assessment is found in a note:
What is/are the proper code(s) for the assessment above?
a) 305.1, 272.4, 401.9, 250.00b) 272.4, 401.9, 250.00c) 272.4, 401.9d) 401.9
45©AAHCM

Answer 1
1. Answer: d) 401.9
Rationale: The HTN is only code that can be obtained from this example. Positive history of smoking cannot translate to tobacco
dependence (it must be stated), so 305.1 is incorrect. Diabetes is questionable due to legibility, so not coded.
The cholesterol is listed as “↑ chol”. (Cannot code from arrows)
This example illustrates coding clinic rules on up and down arrows, illegible notes, and clinical documentation specificity.
46©AAHCM

Problem Lists
Problem list should be maintained to include:◦ Each condition and the start date.◦ The end date if the condition no longer exists.◦ The reason why the patient is disabled (Medicare
beneficiary and under 65 years).
Current (active) problem list important ◦ Other providers can know patient’s condition ◦ Reminder to address each chronic condition at least
once a year
47©AAHCM

48
Show a clear, causal relationship between any condition and its respective manifestation(s).
Use linking verbiage such as “due to,” “because of” or “related to” to establish this relationship. The word “with” does not establish a cause-and-effect relationship except in the case of “diabetes with neuropathy”
Coding guidelines prohibit medical coders from assuming any cause and effect relationships
Document Causality if possible
©AAHCM

49
Official ICD-9 Coding Guidelines Diagnosis may only coded when
explicitly spelled out in medical record Medical record documentation that
supports each coded diagnosis must be obtainable
Must demonstrate adherence to coding guidelines
Documentation Critical in Capturing Risk Adjustment Data
©AAHCM
http://www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm

50
Mantra #1 - All conditions documented by a PCP that co-exist at the time of the encounter/visit, and require or affect patient care or management should be coded.
• Do not continue to code conditions that were previously treated and no longer exist.
• History codes may be used as secondary codes IF the historical condition or family history has an impact on current care or influences treatment (V10-V19 are not in HCC model but are important).
Official Coding Guidelines
©AAHCM

Mantra #2 - Documentation should reflect medical decision-makingExamples:◦ DM currently stable on medication◦ Condition worsening - medications adjusted◦ Reviewed history and use of inhaler
w/patient◦ Condition improving◦ Interpret test results/confirm diagnosis in
note
51
Official Coding Guidelines
©AAHCM

52
Monitored: current or planned
Evaluated: testing, physical finding or symptom
Assessed: conclusion that describes diagnosis
Treated: medications, exercise, advice, diet, etc
Put MEAT in your notes
©AAHCM
Best if each problem/diagnosis is addressed explicitly with an “Impression/Plan” format, instead of SOAP format for complex patients.

53
Mantra #3 – Treatment is prima facie evidence of a diagnosis
◦ If treating, then a working diagnosis has usually been made, so write it down
◦ Don’t state “rule out” and then start treatment ◦ Document as “will treat for _______” or similar◦ Clinician should be as specific as possible when
documenting to allow for the most accurate/highest level code to be assigned (especially for ICD-10).
Coding Guidelines
©AAHCM

Avoid Qualifiers, if Possible
Using qualifying language disqualifies codes◦ OK to use qualifying terms, if diagnosis not established◦ If treating condition, diagnose/code for what you are treating
54
Cannot Code in Outpatient Records: May Code in Outpatient Records:
Suggestive of / Symptoms of / Likely Early / Underlying
Consistent With / Compatible With Evidence of
Suspicious for / Pending Element of
Probable / Suspect / Tendency / Possible Component of
Presumed / Sign(s) of / Suspect Significant
Pre‐ / or vs. Compensated
Rule‐Out / Perhaps / Questionable Results show
©AAHCM

Incomplete Diagnoses Work-up in progress? Fine to state “rule-
out”, etc When results point to either firm/working
diagnosis OR when treating definitively (not symptoms only), then record the working diagnosis for coding.
Addendum to original face-to-face visit note is fine to record new diagnosis based on work-up.
55©AAHCM

Question 2Ms. Maibock came in for follow up visit with her PCP. A full SOAP note was documented and signed by the treating MD.CC/HPI: Ms. Maibock is here for follow-up of RLL painMedications: CoumadinPMH: Compartmental syndrome status post surgery 2 years ago.Assessment: 1. Rt. Leg pain (NOTE: Duplex Doppler report of lower extremities from radiologist shows findings of: “consistent with DVT”.May the coder code DVT mentioned as an active diagnosis?a) Yesb) No
56©AAHCM

Answer 2
2. Answer: b) No
Rationale: A Coding Clinic* ruling states that any diagnosis described as “consistent with” cannot be coded as active or current as a specific diagnosis is not being made with this wording choice.
This example highlights the rules around coding unspecific diagnoses when described as “consistent with”.
*The Coding Clinic (a department within the AHA‐ American Hospital Association) issues rulings on diagnosis coding.
57©AAHCM

58
• Diagnosis specificity is paramount.• E.g., “chronic” can change the chosen
diagnosis code (and its risk score value)•Chronic Renal Disease vs. Renal insufficiency•Chronic Hepatitis B vs. Hepatitis B•Chronic Bronchitis vs. Bronchitis•Chronic cor pulmonale vs. cor pulmonale
Specificity Matters
©AAHCM

Evaluate and document chronic quiescent conditions, such as:
o Amputation, toe loss (V-code) (Z89.4xxx)
o Ostomy (V-code) (Z93.x)o HIV status (V-code) (B20)o Dialysis status (V-code) (Z99.2)
Each of these triggers an HCC.
59
“Status” Conditions
©AAHCM

Standard abbreviations
Avoid abbreviations in medical record documentation
Use only standard abbreviations
Do not create abbreviations Check with local hospital for
list if your organization doesn’t have an approved standard
60©AAHCM

Use “history of” only when appropriate
Per ICD-9-CM guidelines, the term “history of” means the patient no longer has the condition
Examples:◦ “history of congestive heart failure” to indicate
compensated congestive heart failure◦ “history of atrial fibrillation” to indicate atrial
fibrillation controlled by medication Avoid using the words “history of” to
document a current condition
61©AAHCM

©AAHCM 62
Signature Issues
Unacceptable Signature/ Authentication
Acceptable Signature/ Authentication
“Signed but not read”Handwritten signature or initials of treating provider
“Dictated but not signed/ read”, etc.
Electronic signature/ authentication (e.g. “authenticated by”, “completed by”, “finalized by”, “validated by”, “attested by”, “sealed by”, etc.
Signed by someone other than the treating provider (nurse, transcriptionist, etc.) on providers behalf
Signature stamps were phased out effective 12/31/2008. (EMR systems that affix a JPEG that looks like a signature stamp are approved)

EHR Shortcuts Beware “copy and paste” without updates Auditors are not stupid
©AAHCM 63

• Diabetes & complications• Vascular Disease• Chronic Kidney Disease• Chronic Heart Failure
©AAHCM 64
Common Documentation and Coding Issues in Home-
based Primary Care• Malnutrition• Stroke & Sequela• Major Depression• Dependencies

65
• There are two HCC’s for Chronic Diabetes Mellitus◦Uncomplicated
HCC 19 (Community) 0.182◦Complicated
HCC 18 (Community) 0.368• Most patients with diabetes for a long time
have complications • Evaluating and documenting diabetic
complications does increase revenue, and is just plain Good Medicine.
Documenting Diabetes Mellitus
©AAHCM

Coding Diabetes Mellitus
66©AAHCM

Documenting Diabetic Complications• Common Diabetic Complications include
• Nephropathy (250.4x) (E11.22)
• Neuropathy (250.6x) (E11.4x)
• Diabetic Vascular Disease/angiopathy (250.7x) (E11.5x)
• Diabetic retinopathy (250.5x) (E11.3x)
• Lipidemiopathies (250.8x) (E11.69)
• Each diabetic complication represents a separate diagnosis itself
• Support both diagnoses in your narrative – signs, symptoms, test results and link the two together.
67©AAHCM

Coding Diabetes Mellitus First, document DM type with 250.xx code(s) These codes always require a 4th and 5th character
◦ 4th Character: Diabetic Complication◦ 5th Character: Type I v Type II and controlled (actually is “not stated as
uncontrolled”) v uncontrolled 0 = type 2, not stated as uncontrolled 1 = type 1, not stated as uncontrolled 2 = type 2, uncontrolled 3 = type 1, uncontrolled
Type 2 is default, if documentation doesn’t state Type 1 Uncomplicated diabetes requires just one code Multiple complications require multiple (250.xx) codes
◦ Example: DM2 with renal and neuro manifestations: 250.40 and 250.60 (E11.21 and E11.4x)
68©AAHCM

Coding Diabetes Mellitus
Second, document/code all complications◦ Document/code at least one manifestation for
each 250.xx code that applies.◦ Ex: DM2 with diabetic retinopathy & diabetic
neuropathy would be coded as: 250.50, 250.60, 366.41, 357.2 (E11.36, E11.42)
◦ Document the linkages between complications and Diabetes (“due to”, “caused by”, etc)
69©AAHCM

Question 3Ms. Lager came in for follow up visit with her PCP. A SOAP note is documented and signed by the treating MD.Assessment: 1. Diabetes (DM) Type II 2. Peripheral Neuropathy 3. HypertensionWhat are the proper codes for the diabetes & neuropathy above?a) 250.00, 357.2 -- DM2, uncompl + Polyneuropathy in diabetes
b) 250.60, 356.9 – DM2 w/neuro manif + Unspec peripheral neuropathy
c) 250.00, 356.9 -- DM2, uncompl + Unspec peripheral neuropathy
d) 250.60, 357.2 -- DM2 w/neuro manif + Polyneuropathy in diabetes
70©AAHCM

Answer 3
3. Answer: c) 250.00, 356.9
Rationale: In this example, cause & effect is not demonstrated between the diabetes and the peripheral neuropathy. If the provider had documented the cause & effect relationship such as: “DM with peripheral neuropathy”, “Peripheral neuropathy due to diabetes”, “Diabetic peripheral (or poly) neuropathy”, etc., then the codes would be justified for 250.60 and 357.2.
This example illustrates the importance of documenting all cause & effect relationships, especially in diabetes.
71©AAHCM

DM w/Renal Manifestations 250.4x (E11.2-)
Most common Renal Manifestations: CKD with Nephropathy in DM (583.81) (N05.9)
◦ DM and Microalbuminuria (>30mg in 24 hr or urine albumin/Cr> 30 x 2 in >3 mo), or
◦ Proteinuria (evidence of protein on UA >/=1+)◦ Nephrotic syndrome (581.81) sometimes present
and/or
CKD (585.x ) (N18.x) without Nephropathy(stage based on eGFR alone if <60ml/min/1.83m2)
72©AAHCM

CKD Documentation & Coding CKD 1 - 2◦ eGFR> 60, requires documented evidence
of renal disease◦ document microalbuminuria, polycystic
kidney, hydronephrosis, etc. CKD 3 - 5
◦ eGFR <60 is presumed CKD (at least stage 3)
If >70 y/o, use Cockcroft-Gault equation (age, ideal wt, Cr) vs lab report (MDRD: age, gender, race Cr, BUN, Albumin)Example: 79 y/o BM, Cr 1.4, BUN 20, Alb 4.0
MDRD = 63but CG = 53
Don’t forget about Renal Hyperparathyroidism (588.81) – common in CKD 3 or worse – order PTH
73©AAHCM
DX eGFR ICD-9
CKD I 90+ 585.1CKD 2 60-89 585.2CKD 3 30-59 585.3
CKD 4 15-29 585.4CKD 5 0-15 585.5
ESRD Dialysis 585.6
CKD unspecified
NOS 585.9

Question 4
Mr. Dubble came in for follow up visit with his PCP. A SOAP note was documented and signed by the treating MD.Assessment: 1. Diabetes, 2. Hypertension, 3. Kidney Disease
What is (are) the right code(s) for kidney disease noted above?a)585.9 Chronic kidney disease, unspecifiedb)593.9 Unspecified disorder of kidney and ureterc)584.9 Acute Kidney Failure, unspecifiedd)585.1 CKD Stage 1
74©AAHCM

Answer 44. Answer: b) 593.9 Unspecified disorder of kidney and ureter
Rationale: Provider did not use specific documentation for the kidney disease. Had the provider noted it as “chronic”, then 585.9 would be correct for unspecified. Without the description of the kidney disease, default code is 593.9, “unspecified disorder of kidney and ureter”. This is the same default code when “chronic” is not used to describe a renal insufficiency as well.
This example covers the needed specificity in kidney disease coding.
75©AAHCM

DM w/Neuro Manifestations 250.6x (E11.4)
Document and code:
• Polyneuropathy in diabetes (357.2) (E11.42)
• Peripheral autonomic neuropathy (337.1) (E11.43)
• Mononeuropathy (354.0 - 355.9) (E11.41)
• Diagnosis does not require NCT, etc. Can document • Positive findings on physical exam• Numbness• Tingling• Burning sensations • Gastroparesis• What about ED?
76©AAHCM

Diabetes Mellitus with Peripheral Circulatory Disease 250.7x (E11.51)
Document and code manifestations, such as arterial insufficiency: Peripheral angiopathy due to other disease
(443.81) (Preferred over unspecified PVD - 443.9)
(I70.209)
77©AAHCM

Documenting Vascular Disease Easy to diagnose, but over-looked, since not symptomatic in
early/middle stages. Look for:◦ Claudication if present
◦ Diminished pedal pulses common (avoid documenting pulse “present” or “palpable” – use gradations like“+2”
◦ Other stigmata Ankle-Brachial Index (ABI) is preferred diagnostic study if
claudication or other manifestations absent Document ulceration/gangrene if present. Also Large vessel disease – AAA, atherosclerotic aorta, etc
◦ May be discovered on CXR, for example◦ Is usually being treated (risk factor modification)◦ So, add to assessment/problem list
78©AAHCM

Vascular Disease
HCC 108 – Atherosclerosis of Extremities ◦ 440.20 (I70.20x) Atherosclerosis of Extremities, unspecified◦ 443.9 (I73.9) PVD, unspecified◦ 443.81 Angiopathy in diabetes
HCC 107 – Vascular w/complications ◦ 454 (I83.0) Document varicose veins of LE w/ulcer◦ Renovascular disorders, ruptured aneurysms, arterial emboli
HCC 106 - Atherosclerosis of Extremity with Ulcer/Gangrene
◦ 785.4 (I96) Gangrene◦ 440.24 (I70.269) Atherosclerosis of ext artery w/gangrene ◦ 440.23 (I70.2x) Atherosclerosis of ext artery w/ulcer
79©AAHCM

DM with Ophthalmic Manifestations 250.5x (E11.3xx)
Document and code, such as:• Proliferative Diabetic Retinopathy (362.02) * (E11.35)
• Vitreous hemorrhage (379.23)* (H43.10)
• Microaneurysm/background retinopathy (362.01) (E11.329)
• Macular edema (362.07), (must include a diabetic retinopathy code also) (E11.311 only code needed)
If linked by specialist…• Diabetic Cataract (366.41) (rare: not senile cataract) (e11.36)
• Glaucoma with systemic syndromes (365.44) (E34.9)
*generates separate HCC (122)
80©AAHCM

Diabetic Coding Examples A person with documented controlled diabetes
with the following diabetic complications: ◦ Polyneuropathy◦ Nephropathy (microalbuminuria x 2 over 3 mo)◦ Stage III chronic kidney disease (eGFR = 30-60 x 3 mo)
Would use the following diagnosis codes:◦ 250.40 (DM2 w/renal manifestations) (E11.22)
◦ 250.60 (DM2 w/neuro manifestation) (E11.4x)
◦ 357.2 (Neuropathy in DM) (no code in ICD10)
◦ 583.81 (nephropathy in oth dis) (E11.21)
◦ 585.3 (CKD 3) (N18.3)
81©AAHCM

Diabetic Coding ExampleUnder-documenting DM communicates a less serious DM case, which affects value of careAny manifestations must be documented as a cause and effect relationship, for example:
①Assessment: 1. DM 2. Polyneuropathy
Can only code: 250.00 and 356.9 (ICD-9)
E11.9 and G62.9 (ICD-10)
[Lower Value DM]
②Assessment: 1. Diabetic Polyneuropathy
Can code: 250.60 and 357.2
E11.42 (ICD-10)
[Higher Value DM]
82©AAHCM

Chronic Heart Failure Many new patients have quiescent disease Develop high index of suspicion for CHF
◦ Clue: May be on diuretic, ACEI, Beta-blocker, etc◦ Abnormal EKG should prompt echocardiogram
EF and PA Pressure Diastolic dysfunction is common
◦ (Normal EKG =high predictive value for normal Echo) Remember: Stage B CHF = anatomic
changes without symptoms; e.g.,◦ Non-valvular AF ◦ LVH, wall motion abnormalities◦ Diastolic dysfunction◦ Elevated PA Pressure
83©AAHCM

Ischemic Cardiomyopathy Clinicians use this term to refer to CHF from
various forms of coronary artery disease◦ 414.xx (I25.89) “Other forms of Ischemic Heart
Disease.”◦ 414.8 (I25.5): Ischemic Cardiomyopathy◦ Also includes Chronic Coronary Insufficiency, and
Chronic Ischemia, myocardial This Presents a Problem: None of the ICD9
414.xx (I25.x) codes map to the HCC 85 CHF.
84©AAHCM

Documenting Ischemic Cardiomyopathy Does the patient have history/evidence of
coronary artery disease (CAD) or old MI? Does the participant have evidence
of CHF documented? In your medical opinion, is CHF a
result from the CAD? If “yes” to all three, then document and code
BOTH◦414.8 (I25.5) Ischemic Cardiomyopathy
(Genotype)◦428.xx (I50.xx) Heart Failure (Phenotype)
85©AAHCM

Stable AnginaCAD (414.0x) (I25.10) and ASCVD (429.2) (I25.x)
do not risk-adjust Angina Pectoris does risk adjust (HCC 88)Document Stable Angina:◦Known diagnosis of CAD?◦Current use of Nitrates or beta-blockers?◦Past history of chest pain, now controlled?◦Treatment is prima facie evidence of disease
If definitively treated with CABG/stent and no further medical Tx, then Dx is “History of” Angina.
86
AMI
Unstable
Angina
Stable Angina
CAD/ASCVD
Hierarchy of HCCs:
©AAHCM

COPD Be specific if possible, otherwise
use “COPD” 496 (J44.9)
Code pneumoconiosis separately Be careful how document/code
Asthma◦ 493.9x (J45.90x) – Unspecified Asthma
(is non-specific)◦ 493.2x (J44.9) – Chronic Obstructive
Asthma (abnormal PFTs between exacerabations)
Look for rescue inhalers, etc as clue to dx
87©AAHCM

Respiratory Failure
TWO types – Hypercapnic or Hypoxemic If requiring continuous O2 (hypoxemic)
then also document Chronic Resp Failure (518.83)◦ Oxygen dependence (>15 hrs/day)◦ Document Hypoxemia at rest (not only with
exercise or sleep)◦ Usually CHF or COPD as etiology
ICD10 Respiratory failure (NEC) (J96.xx) ◦ Acute and Chronic Resp Failure map to the same HCC◦ Can designate Hypoxia (J96.11) vs Hypercapnia (J96.12)
88©AAHCM

Nutritional Diagnoses
Malnutrition generally under-diagnosed ◦ No clear diagnostic criteria for community-
dwelling elders◦ Acute hospitalization often causes malnutrition◦ Common with end-stage conditions like COPD,
CA, Dementia◦ Are you treating it with supplements, etc?
Mini-Nutritional Assessment (MNA®) to screen or diagnose for malnutrition
89©AAHCM

©AAHCM 90

Malnutrition Diagnoses
• 263.1 (E44.1) Malnutrition of mild degree ◦BMI 16-17.9 or loss of 21% to 30% of ideal weight and mildly low albumin, 3.5g/dL, <75% of EER intake for >mo
• 263.0 (E44.0) Malnutrition of moderate degree◦BMI <16 or loss of 30% or more of ideal body weight, and moderately low albumin, 2.5g/dl◦Weight loss of 5%/mo, 7.5%/3mo or 10%/6 mo
• 262 (E43) Malnutrition of severe degree ◦Weight loss of >5%/mo, >7.5%/3 mo
• 799.4 (R64) Cachexia
91©AAHCM

Morbid Obesity• Morbid Obesity (BMI >40) (WHO definition)
◦ 278.01 (E66.01) Morbid Obesity
◦ 278.03 (E66.2) Obesity hypoventilation synd
◦ V85.4x (Z68.4x) BMI >40 and over
• “Overweight,” and “Obesity due to excess calories” do not risk adjust.
• Some authorities suggest BMI >35 with obesity-related complications of chronic illness or functional decline (indications for bariatric surgery) meets criteria for Morbid Obesity Dx –
• We suggest sticking with WHO definition
92©AAHCM

Neoplasm Coding Neoplasm is coded as malignant if documented
as 1. Active (visible, measurable, growing, present)2. Receiving treatment (even if not measurable active)3. In Palliative care
History of cancer (V codes) (Z85.xx) should be used for all cancers that are not active at the time of coding.
If neoplasm has become metastatic disease carefully document and code as such (much higher RAF.)
93©AAHCM

Cerebral Infarction, Stroke or Cerebrovascular Accident (CVA) Above terms are interchangeable = 434.91
(I63.9) = Cerebral artery occlusion, unspecified, with infarction.◦ These are ACUTE codes – not for sequelae◦ Once out of the hospital, code for late effects
Acute vs. Late Effects of CVD◦Use 438 (I69.3-) codes for neurologic deficits that persist after onset of acute condition from categories 430-437
96©AAHCM

Late Effect
If appropriate, document presence of “plegia” or “paresis” modified with “mono” or “hemi”
◦ If associated with a CVA, document association.◦ If associated with Cerebral Hemorrhage,
subarachnoid hemorrhage◦ If present but not due to known cerebral event,
document as such◦ All of these conditions Risk Adjust (HCC 103 or HCC
104) “Weakness” and “Gait abnormality” are
symptoms, not diagnoses and code to different ICD9 codes that do not risk adjust.
97©AAHCM

Major Depression If write “depression”, then coder must us 311 (Depressive
Disorder NEC) ◦ Non-specific◦ There are NO diagnostic criteria for 311◦ Coding convention used when there is poor documentation
Major Depression is common in home-bound population
100
(Use Single Episode unless you have clear evidence of recurrent episodes.)
©AAHCM

Finally, Know the “Rules of the Road”
◦ Become familiar with the coding conventions and follow all instructions related to specific codes.
◦ Be aware of “includes” and “excludes” instructions and inclusion terms, as well as “use additional code” and other code-related instruction in the Official ICD-9-CM Guidelines for Coding and Reporting.
◦ If use ICD code book, locate the code first in the alphabetic index, then verify the code in the tabular index. (Reliance on only the alphabetic index or tabular index can lead to coding errors.)
◦ American Hospital Association Coding Clinic is approved resource for clarification of ICD-9-CM.
102
©AAHCM

Summary Accurate risk adjusted payment relies on
diagnosis documentation completeness and specificity
Accurate medical record documentation is essential as it leads to accurate ICD-9 coding
Document and submit all relevant codes annually at least
Prepare for ICD-10 and increased specificity Consider coding assistance
103
©AAHCM

Helpful Websites
CSSC operations- Customer Service & Support Center -- RAPS information and Prescription Drug Information Center◦ www.csscoperations.com
Official Guidelines for Coding and Reporting
http://www.cdc.gov/nchs/data/icd9/icd9cm_guidelines_2012.pdf
Medicare Advantage Website:◦
www.cms.gov/Medicare/Health-Plans/MedicareAdvtgSpecRateStats
104
©AAHCM

Questions
Capstone Performance Systems
Richard O. Schamp MD, Chief Executive OfficerGeorge W. Brett MD, Chief Medical Officer
6255 San Bonita Ave.
Saint Louis, MO 63105
314-477-3685
[email protected]@cpstn.com
105
©AAHCM