Rhumatoid arthritis
33
-
Upload
monther-alkhawlany -
Category
Health & Medicine
-
view
96 -
download
0
Transcript of Rhumatoid arthritis

What is:-
Chronic symmetrical polyarthritis.
Characterized by:-
1- chronic pain,stiffness,swelling around joint and
tendon.
2- associate with extra- articular feature.
3- chronic inflammatory synovitis of peripheral
joint.
4- course of disease is prolong with exacerbation
and remission.

Incidence:-
- Female to male ratio 3:1
- peak age between 20-40 years.
Cause:-
1- genetic factor associate with HLA-DR4
2- autoimmunity for the following reasons:
a-present auto antibodies IgG,IgM.
b-immune complex in synovial fluid and circulation.
3- female gender.
Pathology:-Stage I:- preclinical characterized by..
immune pathology is beginning
increased ESR, C-reactive protein and rheumatoid factor.
Stage II:- synovitis characterized by..
thickening and cell rich synovial membrane.
painful and swelling.
joint and tendon still intact.
this disorder reversible.
Stage III:- destruction characterized by..
due to persist inflammation.
articular cartilage is eroded by proteolyses enzymes.
bone is eroded by granulation tissue invasion and osteoclast resorpation.
tenosynovitis lead to partially or complete rupture of tendons.
synovial effusion due to fibrinoid material also lead to swelling.
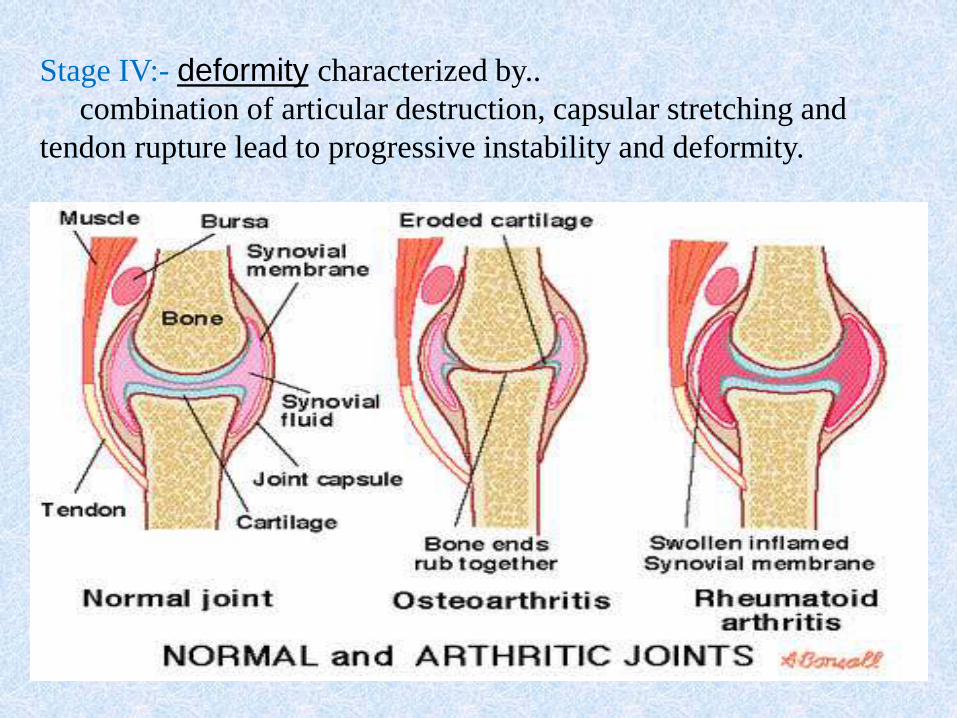
Stage IV:- deformity characterized by..
combination of articular destruction, capsular stretching and
tendon rupture lead to progressive instability and deformity.
Deformity of hands and wrist:-
1- spindling of fingers:- early stage, swelling of MCP joint.
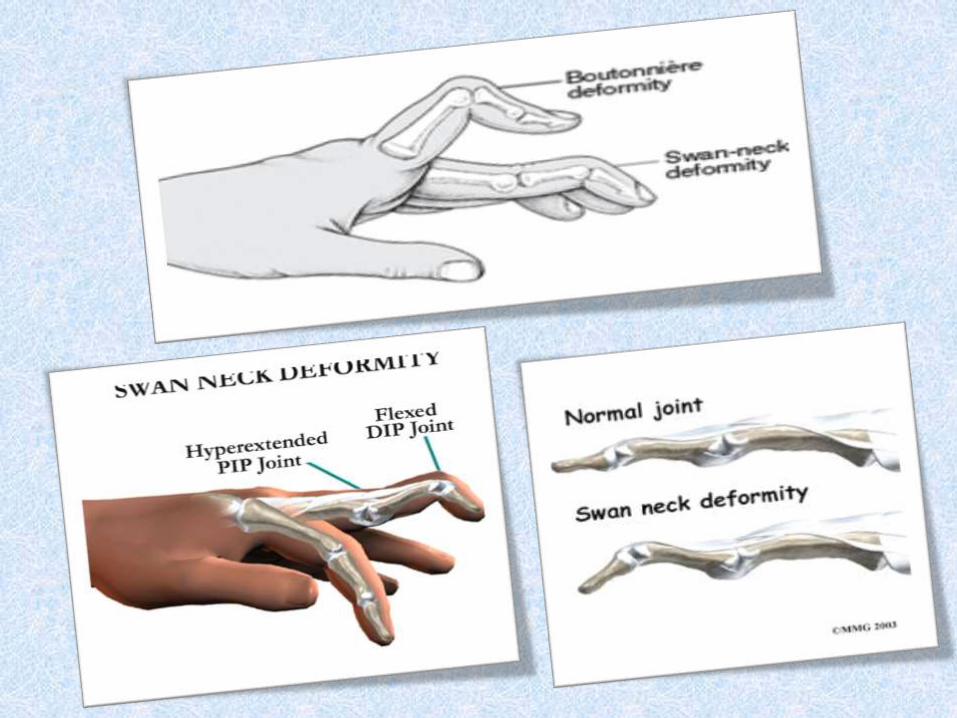
2-swan neck:- hyperextension at proximal interphalangeal joints
and fixed flexion at distal interphalangeal joints.
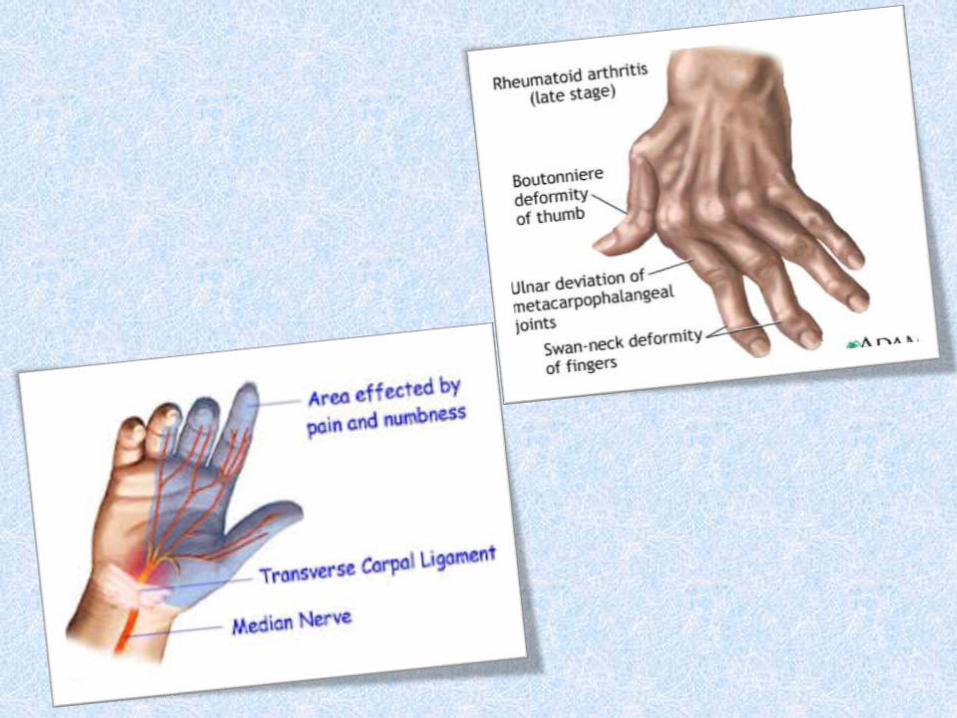
3-boutonniere :-fixed flexion of proximal interphalangeal joint and
extension of distal interphalangeal joints.
4- Z deformity of thumb:- hyperextension of 1st interphalangeal joint and
flexion of 1st MCP joint with consequent loss of thumb mobility.
5- carpal tunnel syndrome:- tenosynovitis at wrist entrap median nerve.
6-mallet finger:- flexion DIP joint due to rupture of extensor tendon.
Deformity of feet and ankle:-
1- Lateral deviation of toes and subluxation of
MTP joints.
2- Heads of MT become palpable in sole of feet.
3- Ankle develops valgus deformity.
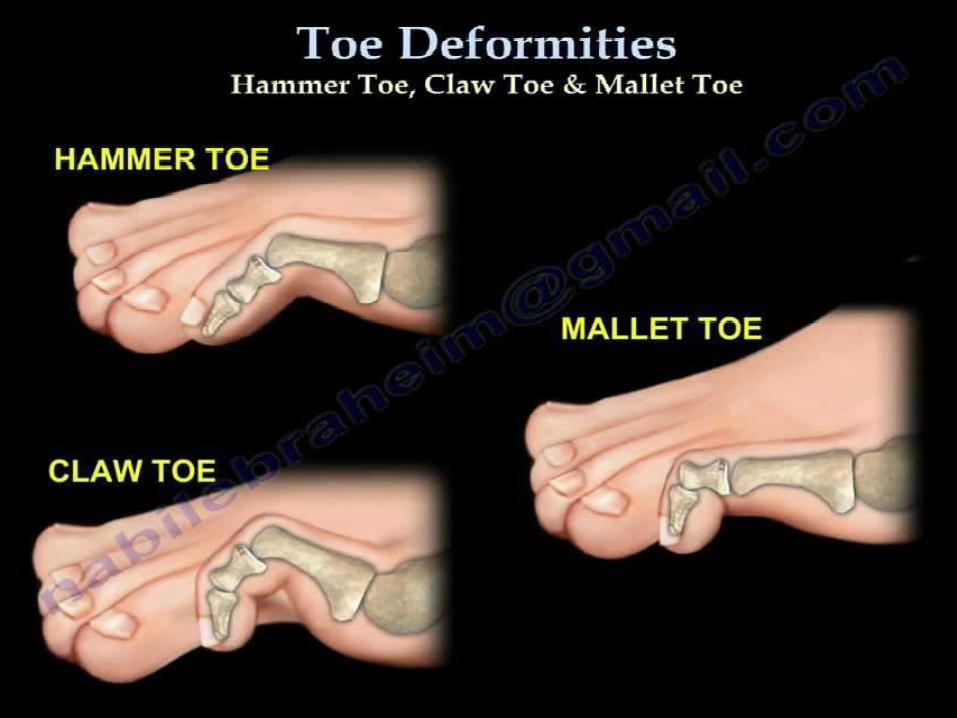
4- Hammer toe.
5- Clow toe.
6- mallet toe.
7- hallux valgus.
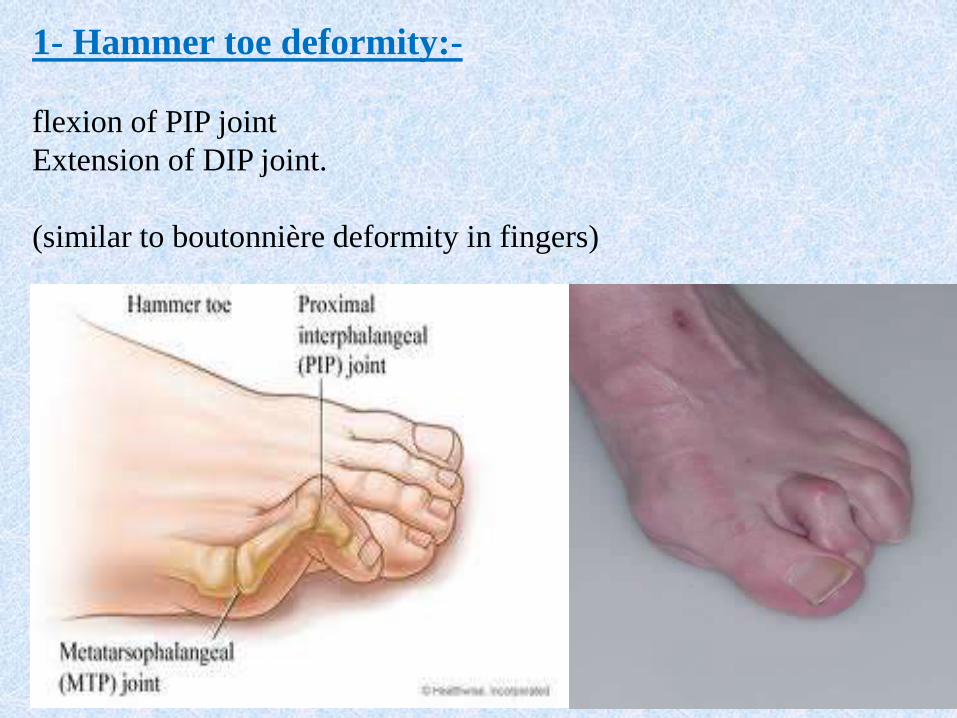
1- Hammer toe deformity:-
flexion of PIP joint
Extension of DIP joint.
(similar to boutonnière deformity in fingers)
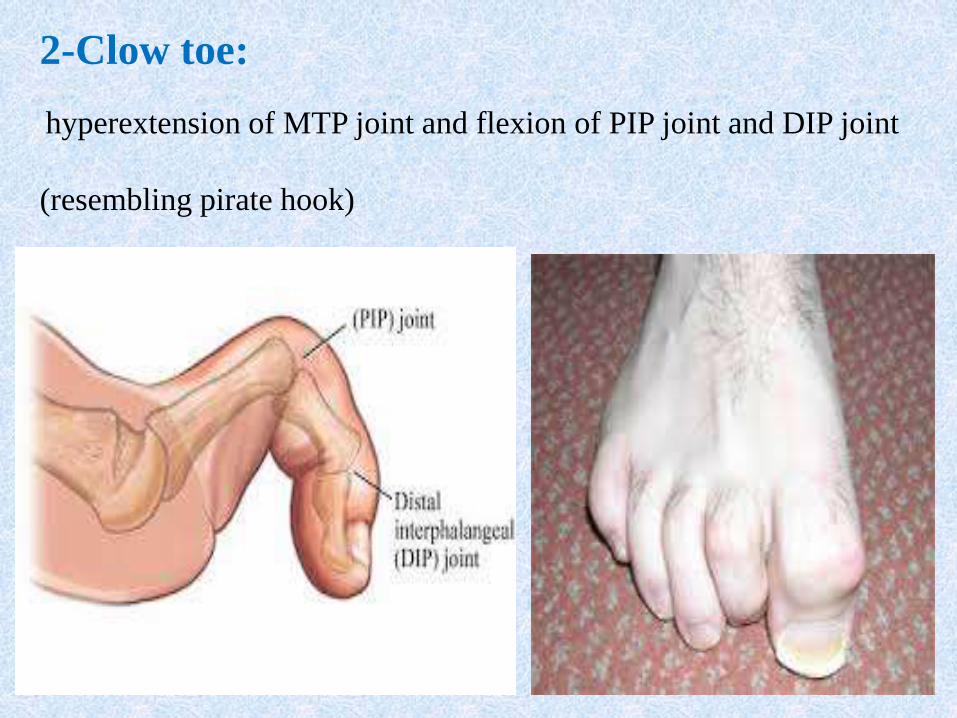
2-Clow toe:
hyperextension of MTP joint and flexion of PIP joint and DIP joint
(resembling pirate hook)
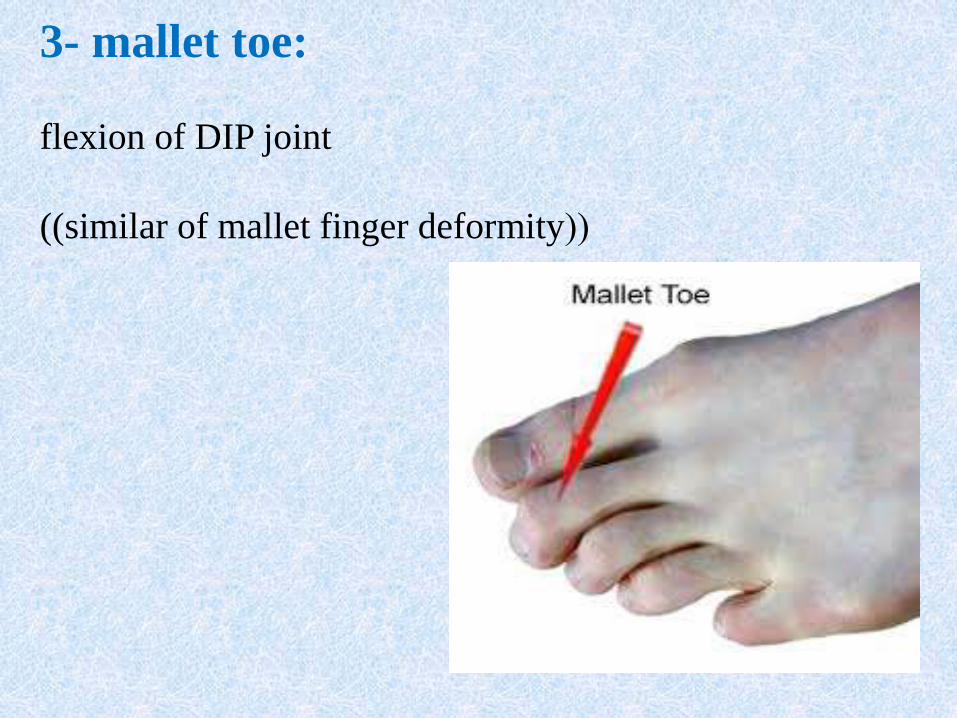
3- mallet toe:
flexion of DIP joint
((((similar of mallet finger deformity
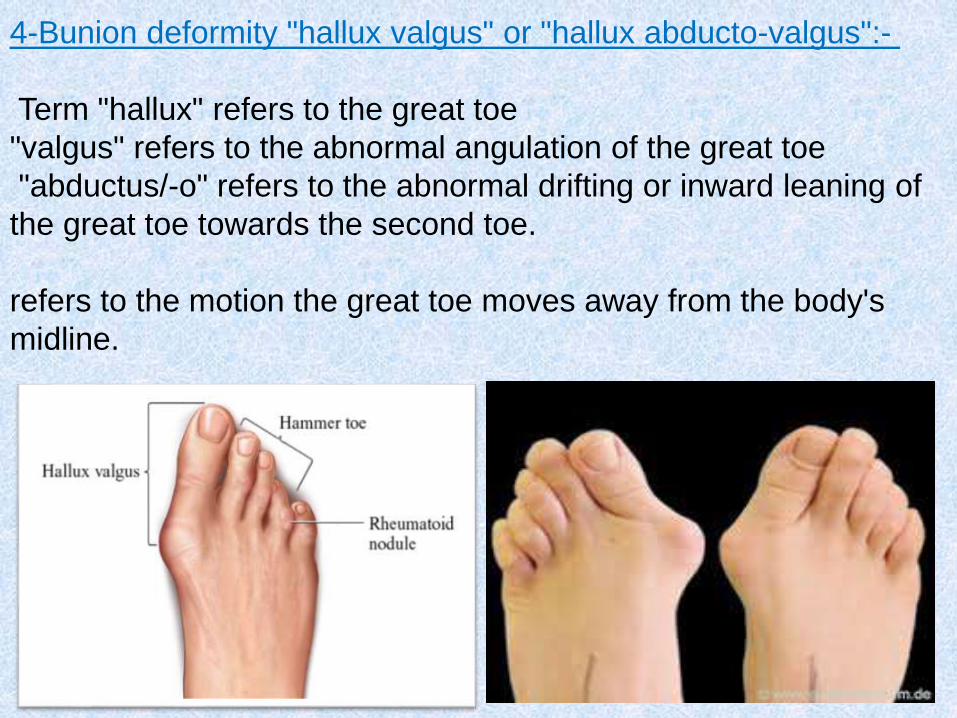
4-Bunion deformity "hallux valgus" or "hallux abducto-valgus":-
Term "hallux" refers to the great toe
"valgus" refers to the abnormal angulation of the great toe
"abductus/-o" refers to the abnormal drifting or inward leaning of
the great toe towards the second toe.
refers to the motion the great toe moves away from the body's
midline.
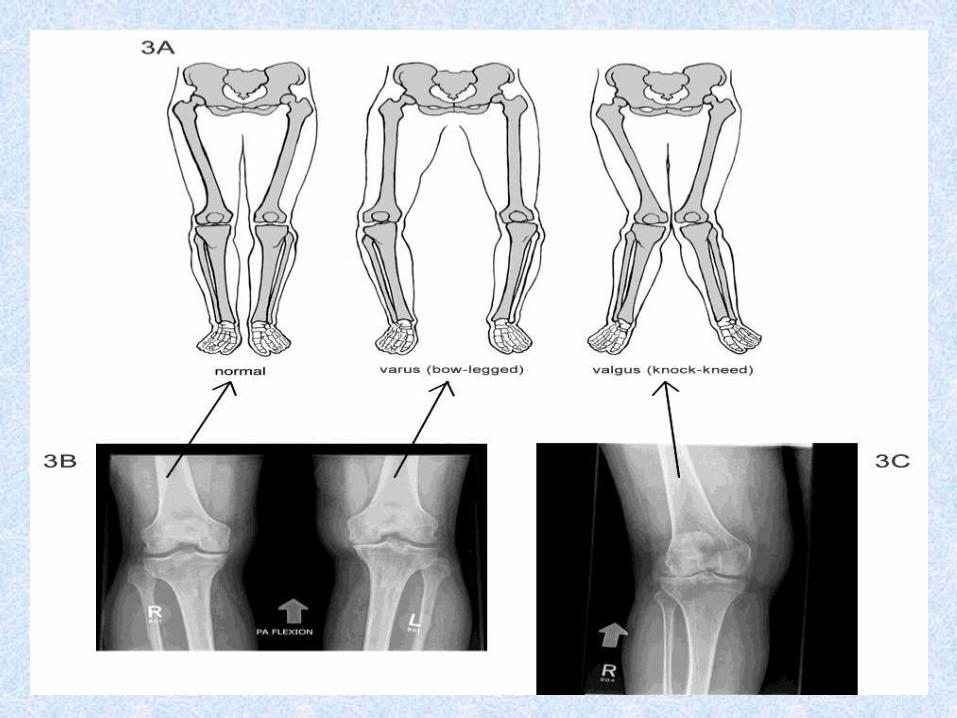
1-valgus deformity (bent outward), varus deformity
(bent inward) appear with joint instability.
2-synovial effusion (demonstrated with patellar tap).
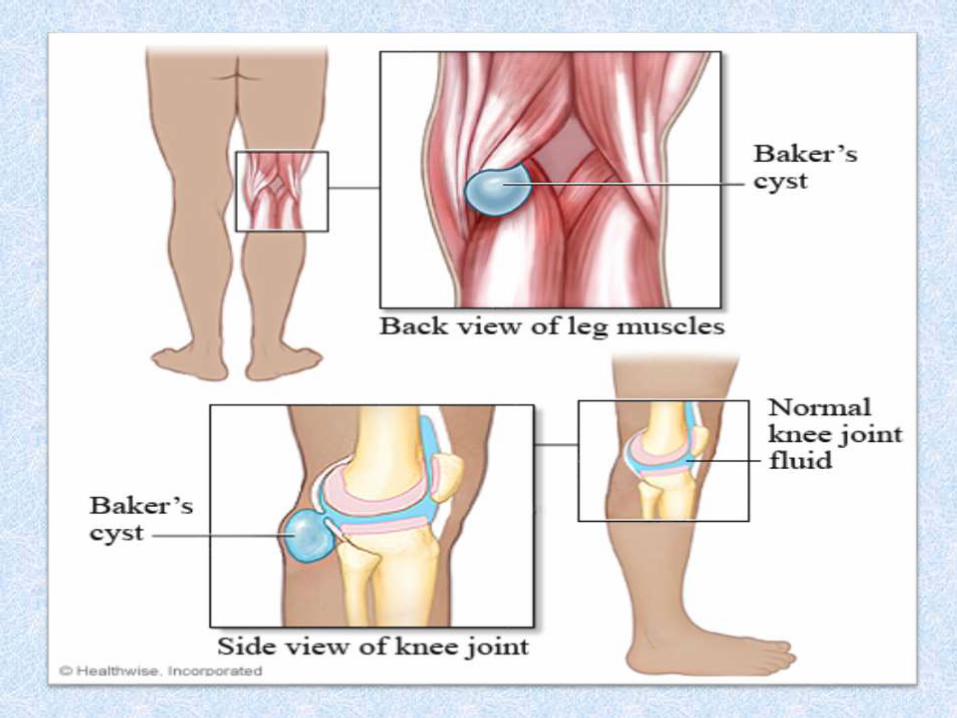
3- Baker cyst:- extension of inflamed synovium into
popliteal space, causing pain and swelling. high pressure
generated by flexion of knee can cause rupture of cyst into
calf, manifested as calf swelling, tenderness and pitting
edema.
Deformity of knee:-
Clinical feature:-
I- early stage:-swelling, stiffness, increased warmth,
tenderness proximal finger joint and wrist.
II-moderate stage:- restricted joint movement.
subcutaneous nodule.
isolated tendon rupture.
III-late stage: -constant ache of joint destruction.
-rheumatoid deformity.. Ulnar deviation of finger, valgus
knee, valgus feet, clowed toes.
-extra articular feature as muscle wasting,
lymphadenopathy, neuropathy….
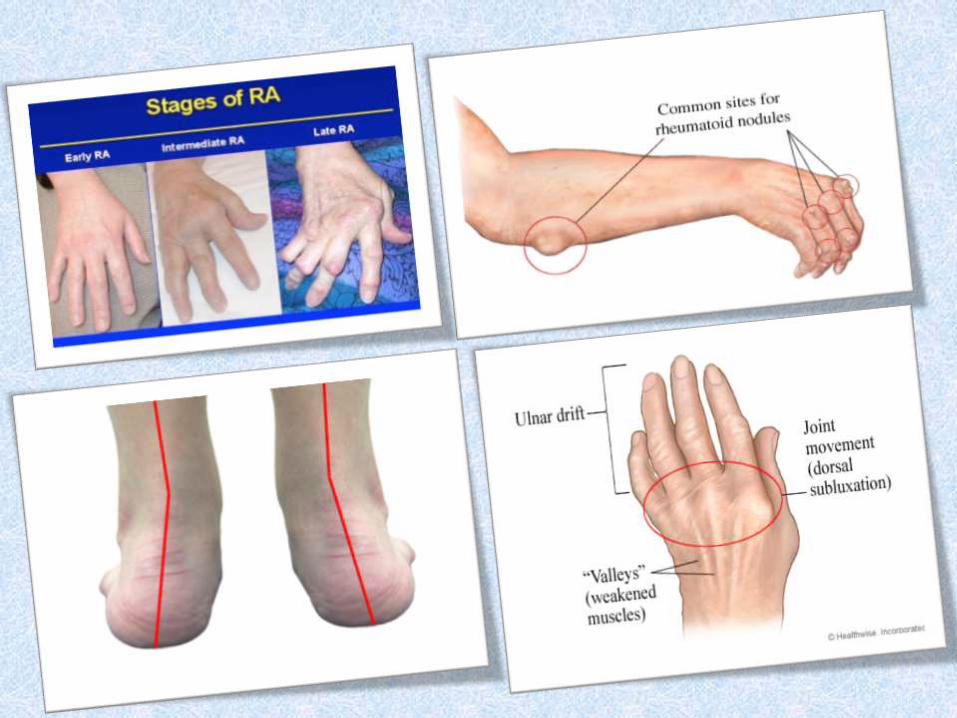
Extra- articular feature:-
1- MSS: subcutaneous nodules, muscle wasting.
2-ocular: sjogren’s syndrome, scleritis.
3-neurologic: carpal tunnel syndrome,
polyneuropathy.
4-hematology:anemia, thrombocytosis, esinophilia.
5- pulmonary: pleural effusion, rheumatoid nodules
in lung.
6-lymphadenopathy.
7-felty’s syndrome:- RA associate with
splenomegaly and neutropenia, in <1%.

Investigation:-
Note:- no test is specific for Dx of RA. Following
investigation may be helpful.
1-rhumatoid factor:- auto antibodies present in about 70% of
cases. not established Dx it for prognostic significance. Also
RA factor is positive in 10% of normal population.
2-ANA (Antinuclear antibodies):- is positive in 30% of
cases.
3- Blood:- anemia, thrombocytosis, ESR and C-reactive
protein are raised (inflammatory markers).

4- X-ray:-
- during first 6 months are read normal.
- early changes occur in the wrist or feet.
- 4 stages of x-ray progression in RA:-
I- periarticular osteoporosis (osteopenia).
II- loss of articular cartilage (joint space).
III- bony erosions on margins.
IV- subluxation and ankylosis.
5- MRI and bone scan detect early inflammatory
changes.

6- Synovial fluid aspiration:-
- fluid is usually turbid.
- reduced viscosity.
- increased protein content.
- decreased or normal glucose concentration.
- C3 and C4 markedly low.
- WBC count varies 5-50.000.
Criteria for the Dx of rheumatoid arthritis:-
(American Rheumatism Association 1987 Revised criteria)
1- morning stiffness (>1 hour).
2- arthritis of 3 or more joint areas.
3- arthritis of hand joints.
4- symmetrical arthritis,
5- rheumatoid nodules.
6- rheumatoid factor.
7-radiological changes.
When 4 or more of the above criteria are met, diagnosis of RA is made.
DDx:-
1- osteoarthritis.
2- gouty arthritis.
3-septic arthritis.
Management:-
1- non-pharmacology:-
- rest:- in mild inflammation.
-exercise:- to maintain joint mobility and muscle power.
-heat and cold :- for muscle relax.
-splint:- to provide rest joint, decreased pain,
-weight loss:- to reduce symptoms of weight bearing joint.

2-pharmacological treatment:-
I- NSAIDs:- select COX2 as anti-inflammatory effect.
II- corticosteroid:- Perdnisolone is the oral steroid of choice
III- disease modifying anti-rhumatoid drugs (DMARD):-
used in persist sing of inflammation with progressive damage.
a- methotrexate:-is ttt of choice.
b- antimalaria (hydroxychloroquine sulfate) use in mild cases.
c- pencillamine:- used combination with methotrexate in severe
RA active disease.
d-gold:-who fail improve.
e-immunosuppression therapy (as cyclophosphamide):-
Use in pt who failed therapy with DMARD.
IV-newer drugs as TNF inhibitors:-reduce inflammation during short
term, disadvantage:-local irritation and expensive.
V-IL1 and IL6 receptors blocker:- rapid anti-inflammatory effect.
3-surgical procedure:-
Indicated in patient with RA:-
1- severe joint destruction.
2- fixed deformity.
3- loss of function.
4- If a 6 months trail of medical treatment has been failed.
5- To reduce pain.
Types of surgical intervention:-
a-tendon repair.
b- synovectomy.
c- arthroplasty.
d- arthrodesis special for interphalangeal joint.
Follow up:-
1- Ask pt for severity of joint pain, morning stiffness, fever,
fatigue.
2- Look for joint swelling, deformity, wasting muscle around
joint.
3- Feel warmth, tenderness.
4- assess passive movement, muscle power.
Prognosis:- After 10 years, disease pattern is:-
1-complete remission 25%.
2-moderate impairment 40%.
3-severe disability 25%.
4-severly crippled 10%.

Poor prognosis:-
1-high titer of rheumatoid factor.
2-more >1year active disease without remission.
3-early develop nodules and erosion.
4-extra auricular manifested.
5- severe functional impairment of joint.
Complication:-
1- ruptured tendons.
2-rupture of backer cyst.
3-rupture joint.
4-spinal cord compression.
5-amyloidosis.
6-complication of drugs therapy.
7- secondary osteoarthritis.